Submitted:
17 July 2023
Posted:
18 July 2023
You are already at the latest version
Abstract
: Background and objectives: One of the most severe symptoms of extrapulmonary tuberculosis (TBEP) is tuberculous meningitis (TBM) which is linked to significant morbidity and high mortality. It is well recognized that HIV-positive people are more likely to develop TBEP, including TBM, especially if they have severe immunodeficiencies. Material and methods: We conducted a retrospective clinical study based on hospital medical records of the diagnosed patients with HIV/AIDS and Tuberculous Meningitis in North-eastern Romania, hospitalized at "Sf. Parascheva" Clinical Hospital of Infectious Diseases from Iasi. We aim to highlight the profile and the caracteristics of the HIV/AIDS and Tuberculous Meningitis coinfection cases. The time frame under study was from January 1st, 2010, to December 1st, 2022. Results: Our Center has a total number of patients on record of 1692. Patients co-infected with HIV- TB were 195 of which 19 cases were HIV- TBM coinfection and it was more common in women. From this total, 6 cases were late presenters and 13 patients were already in the center's records with a deficient immunological viral status, non-compliant, and non-adherent to antiretroviral therapy. The average age in the study group was 27 years old. The mean admission day number was 17.73 days. CSF findings (qualitative and quantitaitve examination, biochemestry) were in accordance with the literature. Conclusions: The key to the management of the HIV-positive patient is the multidisciplinary approach and access to antiretroviral therapy. We must find and eliminate obstacles affecting patients and the healthcare system. In order to increase ART uptake among HIV-infected TB patients and to put an end to the TB and HIV epidemics.
Keywords:
HIV infection
; Tuberculous meningitis
; TB-DOTS
; Mycobacterium tuberculosis
1. Introduction
HIV (Human Immunodeficiency Virus) attacks the immune system, which can lead to AIDS (Acquired Immunodeficiency Syndrome) a condition that results in the weakening of the immune system and increased susceptibility to other infections. HIV/AIDS is a global public health issue, with an estimated 38 million people living with HIV/AIDS worldwide as of 2019. Since the virus was first identified in the early 1980s, HIV/AIDS has become one of the deadliest pandemics in human history, with over 36 million people dying from AIDS-related illnesses [1,2].
The majority of new HIV diagnoses in Europe are among MSM, who accounted for 42% of new diagnoses in 2019. Other key populations with higher rates of HIV/AIDS in Europe include PWID (People who Inject Drugs), migrants, and sex workers. According to the World Health Organization (WHO), there were approximately 2.2 million people living with HIV/AIDS in Europe in 2019, with an estimated 136,000 new diagnoses that year [3].
Romania has a relatively low prevalence of HIV/AIDS compared to some other countries in Europe, but the epidemic has been growing in recent years. According to UNAIDS, there were approximately 16,000 people living with HIV/AIDS in Romania as of 2020, with an estimated 1,000 new infections that year [4].
One of the most severe symptoms of extrapulmonary tuberculosis (TBEP) is tuberculous meningitis (TBM) which is linked to significant morbidity and high mortality. It is well recognized that HIV-positive people are more likely to develop TBEP, including TBM, especially if they have severe immunodeficiencies. Additionally, it has been demonstrated that TBM among HIV-positive patients died at higher rates than HIV-negative people in the time before receiving combination antiretroviral therapy [5,6].
TBM symptoms have reportedly ranged in length from one day to six months prior to presentation, and as a result, the condition may manifest as either acute or chronic meningitis. Fatigue, malaise, anorexia, vomiting, fever, and headache are among the symptoms of TBM's nonspecific prodrome; symptom variation throughout this time is frequent. Occasionally, TBM may manifest as gradual dementia, with social retreat and personality abnormalities. Active pulmonary tuberculosis coexists with TBM in 30% to 60 % of cases. Acute presentations may be difficult to distinguish from bacterial meningitis [6,7].
The diagnosis of TBM heavily relies on CSF analysis. A lymphocytic pleocytosis frequently coexists with low glucose and increased protein levels. Clinical and CSF findings-based diagnostic guidelines have been devised and evaluated in a variety of settings, however, it is unclear if these rules can be used outside of their source populations. The timing of the introduction of ART in relation to anti-tuberculous medication is complicated, even if the use of ART during the treatment of tuberculosis may improve clinical outcomes. In addition to the previously mentioned known drug-drug interactions, starting ART and anti-tuberculous therapy at the same time results in overlapping drug toxicities. The paradoxical reaction, which is a temporary exacerbation of the signs and symptoms of infection, has been linked to the start of anti-tuberculous medication in the absence of ART. The paradoxical reaction in TBM instances may manifest as the development of several tuberculomas following the start of effective treatment. The paradoxical response that occurs during the treatment of TBM may be made worse by ART's immunological reconstitution [8].
In conclusion, significant immune suppression and an unacceptably high mortality rate are characteristics of HIV-positive patients with TBM. Patients who have advanced HIV infection have a particularly poor prognosis after TBM, which urgently calls for public health interventions to improve patient management in terms of earlier HIV infection diagnosis, timely and accurate TB diagnosis, optimal TB treatment, and access to cART [9].
2. Materials and Methods
2.1. Database description
In order to highlight the profile and associated comorbidities of the HIV/AIDS cases with TBM, we conducted a retrospective clinical study based on hospital medical records of the diagnosed patients with HIV/AIDS in Northeastern Romania, hospitalized at "Sf. Parascheva" Clinical Hospital of Infectious Diseases from Iasi. The time frame under study was from January 1, 2010, to December 1, 2022.
Two ELISA tests were used to serologically diagnose those suspected of having HIV, and a Western blot test was used to confirm the diagnosis. The epidemiologists working for the area public health management network completed all of this. The Mycobacterium tuberculosis infection was confirmed with PCR ADN Mycobacterium tuberculosis and cultures for Mycobacterium spp. from the CSF with positive results.
The information gathered covered demographic factors (age, sex), personal pathological antecedents, clinical traits, blood tests (viro-immunological testing), evaluation of potential associated opportunistic infections, patient staging, initiation of antiretroviral treatment, as well as the development and prognosis following therapy of patients who had just received an HIV/AIDS infection diagnosis.
According to the Centers for Disease Control and Prevention (CDC) Atlanta, the HIV infection stage was determined using a specific CD4+ T-lymphocyte count or CD4+ T-lymphocyte percentage of total lymphocytes*CD4 T cells level. HIV infection and AIDS are classified into three stages: stage 1 when CD4+ T-lymphocyte levels are below 500 cells/l; stage 2, when they are between 200 and 499 cells/l; and stage 3 when they are below 200 cells/l. HIV infection is represented by stages 1 and 2, and AIDS is represented by stage 3. (https://www.cdc.gov/hiv/statistics/surveillance/terms.html).
The hospital's central laboratory completed all blood tests, and the molecular biology lab measured the patient's CD4+ T cell count and HIV plasmatic viral load. RT-PCR HIV 1 using Cepheid's GeneX-pert® was utilized to measure the viral load used for determining HIV viremia and monitoring the viral load levels.
All patients with MTB were biologically evaluated for CSF findings, quantitative qualitative examination, and biochemistry examination (glycorrhagia, albuminorrhagia, chlororrhagia) of cerebrospinal fluid.
2.2. Statistical Analysis
The Pearson test in the XLSTAT version 2019 software was used to correlate demographic factors, clinical data, and the outcome. There were calculated Kendall's Tau correlation coefficients. Statistical Software for Excel (XLSTAT) version 2019 was used to conduct the statistical analysis.
3. Results
Our Center has a total number of patients on record of 1692. Patients co-infected with HIV- TB, 195 of which 19 cases were HIV TBM coinfection, from January 1, 2010, to December 1, 2022.
HIV infection was more common in women (10 cases, or 53%) than in men (9 cases, or 47%) in the Northeastern region of Romania from 2010 to 2022, where there was a total of 19 cases (Figure 1). From this total, 6 cases were late presenters and 13 patients were already in the center's records with a deficient immunological viral status, non-compliant, and non-adherent to antiretroviral therapy.
The majority of cases were young adults, aged between 21-30 years old – 10 patients (26.31%), followed by the age group 31-40 – 5 patients (40.12%), 41-50 years – 2 patients (10.52%), 51-60 years old– 1 patient (5.26%), 0-20 years old – 1 patient (5.26%), (Table 1). The average age in the study group was 27 years old.
The distribution of our study group based on county showed that almost a third of the patients were from Suceava (7 cases, 31%), followed by Iasi (4 cases, 21%), Botosani (4 cases, 21%), Bacau (2 cases, 11%), Neamt (1 case, 5%) and Vaslui (1 case, 5%), (Table 2).
From urban areas in North East Romania, were 7 patients (37%), and the remaining 12 cases (63%) were from rural areas (Figure 2).
Considering the route of transmission, only 18 cases (94.73%) have reported a possible cause. For the remaining 1 case (5.26%), the route of transmission remains unknown (Table 3). For those with a known route of transmission, the most frequent was sexual transmission (MSM and heterosexual contact) (89.47%), with only one known case of intravenous drug usage (5.26%) and none perinatal cases recorded.
All of the admitted patients from the Iasi HIV/AIDS Regional Center between January 1st, 2010, and December 1st, 2022 were virologically and immunologically evaluated.
The patients presented a deficient viro-immunological status. It was observed that 89.47% (17 cases) had a CD4+ T-lymphocytes level between 1-199 cells/μl, 10.52% (2 cases) had CD4+ T-lymphocytes value between 200-499 cells/μl, with an average CD4+ T-lymphocytes level of 106.05 cells/μl. Cases with Ly T CD4+ >500 cells/μl were not recorded (Table 4, Figure 3, Figure 4).
Based on sex correlated with CD4+ T-lymphocytes level, the most affected were females, with a lower CD4+ T-lymphocytes level overall. The average HIV viral load was 403 844.2 copies/ml.
Most of the patients needed more than 20 days of admission in 10 cases (52.63), 7 cases (36.84%) were admitted between 11 and 20 days, and 2 cases (10.52%) were admitted between 0 and 10 days (Figure 5). The mean admission day number was 17.73 days.
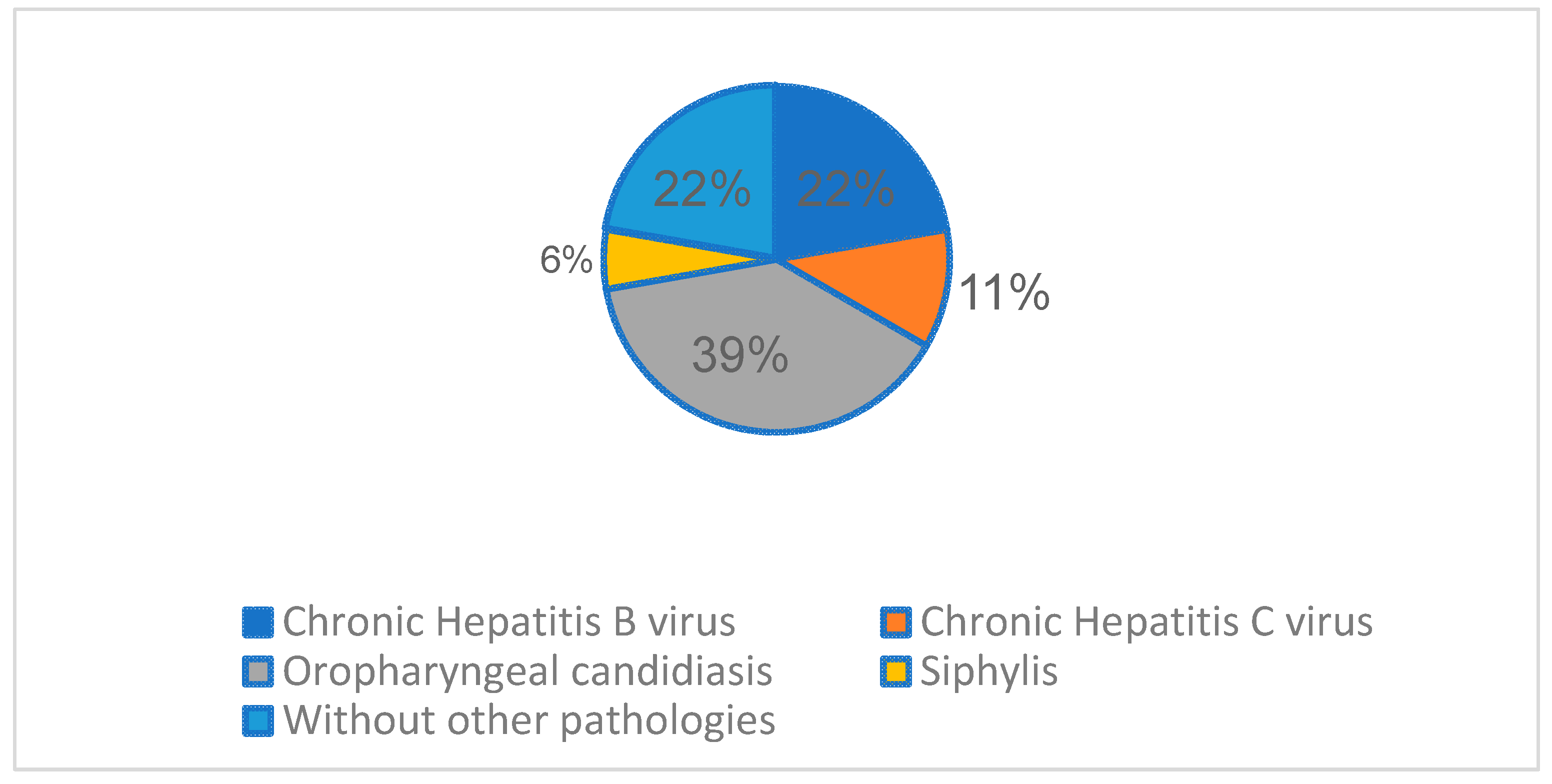
The most frequent associated infectious pathology registered, besides HIV and TB, was Oropharyngeal candidiasis (7 cases,36.84%), followed by chronic hepatitis B virus (4 cases, 21.05%), chronic hepatitis C virus (2 cases, 10.52%), and 1 syphilis co-infection case (5.26%).
Figure 6.
Other associated infectious pathology registered.
From the perspective of the laboratory features, in our study, we investigated CSF findings, Cytological examination (quantitatively and qualitatively), and biochemistry (glycorrhagia, albuminorrhagia, and chlororrhagia). The quantitatively cytological examination of the CSF showed that the majority of the patients had pleocytosis of the order of "tens" (16 cases, 84.21%) and 3 cases had pleocytosis of the order of "hundreds" (20.22) (Figure 7). The mean value of the nuclear cellular elements was 83.73 cells/ mmc.
The qualitatively cytological examination showed us that the patients had lymphocytic predominance with low neutrophils and macrophages. The lymphocyte range was between 70% and 92% with a mean value of 79.21%. The neutrophil level was between 7% and 27%, the mean value was 15.21%. Macrophages were contained between 1% and 4%, the average value was 2.42% (Figure 8).
The evaluation of the CSF biochemistry showed an increased albuminorrhagia value between 1.0 g/L and 2.1 g/L, with a mean value of 1.65 g/L. Glycorrhagia was also increased, between 0.14 g/L to 0.43 g/L, the average value was 0.30 g/L. Chlororrhagia was decreased with values between 5.2 g/L and 6.8 g/L, the mean value was 6.14 g/L (Figure 9).
In the study group, it was observed that a third of the males had an abnormal ALT (15.78%) and almost a half had abnormal AST (21.05%); as for the females, almost a third had an increased value of ALT or AST respectively (15.78% and 21.05%). Of the 15.78% of the males with an abnormal ALT/AST value, 5.26% (1 case) had hepatitis B, 5.26% (1 case) had hepatitis C, and only 5.26 (1 case) declared occasional alcohol consumption. Of 15,78% of female patients with abnormal AST/ ALT, 15.78% (3 cases) had hepatitis B, 5.26% (1 cases) had hepatitis C, and only 10.52% (2 cases) declared occasional alcohol consumption. The rest of the patients did not have an identified cause of elevated transaminase values (Table 5).
The patients that were already in our evidence, before the admission, had different ARV regiments. Most of the patients had protease inhibitors (7 cases, 46.15%), others had integrase inhibitors regimens (5 cases, 38.46%) and 1 case (7.69%) had classic combined therapy (2 non-nucleoside reverse transcriptase inhibitors+ 1 nucleoside reverse transcriptase inhibitors) (Table 6).
7/7 DOTS assessment and initiation were established in collaboration with the pneumology service. At 2-3 weeks, antiretroviral therapy was initiated for late-presenting cases, depending on the clinical evolution.
Interruption of ART was made for the patients already in the center's records during antituberculosis therapy to avoid immune reconstitution inflammatory syndrome, later with the resumption of the regimen adapted according to the clinical evolution in accordance with the guidelines' recommendations.
Rearrangement of ARV therapy for patients on record with drug interaction checker, drug-drug interaction Liverpool (https://www.hiv-druginteractions.org/checker).
From the point of view of the evolution of the cases, 31.57% of cases had deceased (6 cases), 36.84% of patients (7 cases) were lost from our evidence, and 32% are still in our present evidence (Figure 10).
The patients were evaluated after one year, and the viro-immunological status showed (Table 7, Table 8) an increased CD4+ T-lymphocytes level and a significant decrease in HIV viremia. As such, from the 13 patients that remained alive, 1 patient (7.69%) had a CD4 value between 1 and 199 cells/μl, 4 patients (30.76%) had a value between 200-499 cells/μl, and 8 patients (61.53%) had a value above 500 cells/μl. The median CD4 value was 537.92 cells/μl. The average HIV viral load was 20.61 copies/ml, 2 patients (15.38%) were with detectable viremia. In both sexes, most cases had a CD4+ T-lymphocyte level >500 cells/μl (Table 7, Table 8 and Figure 11).
4. Discussion
TB remains one of the most significant socially neglected diseases because of its associations with prejudice, delayed diagnosis, limited access to therapies, and subpar follow-up. When linked to HIV infection, it significantly challenges the global and national health systems [10].
Lawn et al. concluded that although early ART has been proven to be beneficial in various approach trials looking at the best timing of ART during opportunistic infections, the exceptions include those studies including patients with severe CNS infections in resource-constrained settings. Thus, it is evident that there are multiple correct responses to the question of the ideal timing. The timing of ART is simply one part of a complicated package of care that must also include the best possible care for the opportunistic infection in question, the best possible care for any concomitant conditions, and the best possible care for preventing the development of subsequent opportunistic infections. The unfortunate truth may be that in the instance of TB meningitis in Vietnam, the prognosis of the patients is so bad that changes in the scheduling of ART are mainly pointless. As a result, even though efforts must be made to improve the delivery of the present level of care and diagnose patients earlier, new solutions are urgently required [11].
Cresswell et al. enrolled 61 adults, 92% were living with HIV in their study with the median CD4 count being 50 cells/L. Rifampicin minimal inhibitory concentration (MIC) was exceeded in 11% (2/18) of standard-of-care individuals, 93% (14/15) of IV-20 participants, and 95% (18/19) of PO-35 participants. At day 14, higher serum and CSF levels were still present. Adverse reactions were not dose-dependent. They showed reassuring proof that high-dose rifampicin increases CSF and serum exposures in a population mostly made up of HIV-positive individuals without causing any additional harm. Together with data from Indonesian research, these findings support the need for a phase III trial to look into safety in a larger population and assess the effects of high doses of rifampicin on death and disability. Whether high-dose rifampicin will ever be a part of the optimal TBM treatment regimen is not decided yet [12].
Anggraini et al. studied the differences in clinical manifestations, cerebrospinal fluid (CSF) findings, and chest X-ray results between HIV-positive and HIV-negative TBM patients. Only the CSF results had statistical differences. HIV-positive subjects had higher CSF to blood glucose ratios (0.42 vs. 0.18) and fewer leukocyte cells (41 vs. 199), whilst clinical manifestations and chest x-ray results showed no differences [13].
Thwaites et al. showed that despite the fact that extrapulmonary tuberculosis was more likely to develop in HIV-infected patients, the neurological manifestation of tuberculous meningitis was unaffected by HIV infection. The 9-month survival rate was significantly lower in HIV-infected patients (relative risk of death from any cause, 2.91 [95%]). Although HIV infection considerably lowers survival rates, it has little effect on the neurological characteristics of tuberculous meningitis [14].
Croda et al contained 108 cases (72% men, 36 years was the median age). Fever, headache, and meningeal symptoms were only present in 15% of patients. The extra meningeal TB rate was 48%. The median number of CD4+ cells per microL was 65 cells. Nine percent of the 90 cases showed primary isoniazid resistance, and seven percent had multidrug-resistant strains. Overall mortality was 29% while in the hospital and 41% after 9 months. Mortality at 9 months was correlated with tachycardia and a history of HAART. The 9-month survival rate was 22%. They concluded that clinical and laboratory symptoms lacked specificity. Severe immunosuppression and widespread TB were prevalent. High mortality and a low 9-month survival rate were observed. [15].
Boonyagars et al. did a retrospective cohort analysis on adult patients who received treatment at Thailand's Navamindradhiraj University's Vajira Hospital between January 2005 and December 2016 and whose final diagnosis was TBM. The final number of participants in the study was 174. 97 of them (55.75%) tested positive for HIV. There were larger percentages of patients under 40, those with low body mass indexes, those with a history of tuberculosis infection, and those who were also co-infected with the hepatitis C virus in HIV-infected TBM patients. Compared to HIV-uninfected TBM patients, the success rate of treatment was lower in HIV-infected TBM patients. Future research is required to identify the clinical markers for worse survival outcomes in HIV-positive TBM patients since HIV infection reduces the likelihood that TBM patients would respond favorably to treatment. They concluded that the findings of the present investigation show that HIV infection does not affect TBM radiological signs, CSF profiles (apart from increased CSF protein in HIV-infected patients), or neurological characteristics. Their results enable the elimination of clinical variables that were similar in HIV-infected and HIV-uninfected TBM patients. HIV infection lowers the likelihood of successful treatment and survival from an outcome standpoint. We advise early diagnosis and treatment to improve the outcome of TBM treatment. To enhance the caliber and success of TBM care, doctors may use this finding to establish early intervention plans and more potent therapeutic modalities for TBM patients, especially those who are HIV-positive [16].
Maitre et al. did a phase III, multicenter, randomized controlled, factorial plan superiority experiment. The study was open-label for anti-TB treatment and double-blind placebo-controlled for aspirin treatment, and it contains four arms that combine the two experimental therapies (intensified TBM regimen and aspirin) with the two reference treatments (WHO standard TB treatment and placebo). This study is carried out in four African nations: Ivory Coast, Madagascar, Uganda, and South Africa, in adults or adolescents aged 15 years with TBM characterized as "definite," "probable," or "possible" using Tuberculosis Meningitis International Research Consortium criteria. All-cause mortality between inclusion and week 40 is the main result. Even while some other studies supported the intravenous method to boost rifampicin CSF exposure, we purposefully chose to limit the use of this route to malabsorption in order to evaluate the effectiveness of a widely repeatable and practical high-dose oral strategy on a global scale. We chose an aspirin dose that is readily available (200 mg daily) because it is closest to the one (150 mg daily) that lowers TBM mortality. Through a strong European and African partnership, the INTENSE-TBM trial offers a significant chance to improve the efficacy of TBM treatment with widely accessible old medications, particularly in high-incidence areas for both TB and HIV. The trial's design is practical, and the findings would allow for quick and efficient applications in the treatment of TBM patients, which would be simple to implement in nations with high rates of both TB and HIV [17].
Pormohammad et al. included twenty studies in their review. In adult TBM patients, the combined HIV prevalence was 38.0% HIV infection was present in 6.0% of children (under the age of 15). In patients with bacterial meningitis other than TBM, the prevalence of HIV infection was 36.0%. They concluded that adults with HIV have a much higher case fatality rate than adults without the virus. One of the most significant elements that may have contributed to the high case fatality rate in HIV-infected patients with TBM is resistance to anti-TB medicines. More M. tuberculosis isolates from HIV-positive patients had more than one first-line TB medication resistance. Additionally, there is an ongoing debate over whether antiretroviral medication (ART) should be started in individuals who are also infected with TB and HIV. Drug toxicity may be linked to early ART initiation with TB treatment, whereas delayed ART initiation may cause HIV disease progression and death [18].
Vinnard et al. concluded that despite the beginning of effective anti-tuberculous therapy, the mortality rates of TBM remain high. The risk of TBM in an HIV-positive person increases, especially when immunosuppression is further established. Clinical traits include altered level of consciousness, cerebral infarctions, and a positive M. tuberculosis CSF culture may be more prevalent in HIV-infected people with TBM [19].
Garg et al. stated tuberculous meningitis is more common among HIV-positive people. Given that it is a significant predictor of death, infection by multidrug-resistant bacteria presents a significant challenge. Clinicians should be knowledgeable about the pathogenesis of infection and disease, rapid diagnosis, identification of resistant strains, ideal antituberculosis treatment regimens, adjunctive corticosteroid regimens, and the ideal time to start antiretroviral therapy in order to combat this deadly combination. The 3Is policy (intensified tuberculosis case finding, infection control, and isoniazid preventive therapy) continues to be the most effective strategy for eradicating this threat [20].
From May 2000 to August 2003, Karande et al. did a prospective hospital-based investigation. The study included each subsequent child who was diagnosed with TBM and was admitted, ranging in age from 1 month to 12 years. It was evaluated how two outcomes—disabled survivor or death—relate to 35 features, including two demographic factors, nine clinical features, 13 neurological features, five laboratory parameters (including cerebrospinal fluid), six radiological parameters (including computed tomography scan brain), and 13 neurological features. Eight (6.5%) of the 123 TBM cases in total who were enrolled had HIV. The results were similar between the two groups. In conclusion, the only factor related to HIV infection was the presence of Hb 8 gm/dl. The presence of HIV did not influence the results [21].
Martino et al. examined the information on 13,802 cases of TB identified in Harare, Zimbabwe, between 2013 and 2017. 9,725 (70.5%) of the 13,802 TB patients examined were HIV positive. The likelihood of being diagnosed with TB/HIV coinfection was shown to be considerably greater in females, patients aged 25 to 64, previously treated cases, and acid-fast bacillus sputum smear-negative cases. Miliary TB and TB meningitis both exhibited significantly higher odds of TB/HIV coinfection compared to nondisseminated pulmonary TB, but pleural TB and all other extrapulmonary TB had significantly lower risks. The sociodemographic and clinical variables of patients in Harare significantly affected the risk for TB/HIV coinfection. The information base about clinical markers for TB/HIV coinfection has been expanded as a result of our discovery that various kinds of EPTB have various connections with HIV coinfection. This finding can have a stronger public health influence on the elimination of TB/HIV infection [22].
Mukuku O et al. did a cross-sectional analysis of children under 15 years who had TB treatment between January 1, 2013, and December 31, 2015. HIV-infected TB children who died and those who survived were compared statistically. There were 840 TB-positive kids in total. HIV infection was prevalent in 20.95% of people. HIV-positive children had a greater mortality rate (47.73%) than HIV-negative children (17.02%). Death during anti-TB medication was associated with age 5 years, poor nutritional condition, and a negative acid-fast bacilli test. They concluded that In Lubumbashi, pediatric settings frequently see co-infections with TB and HIV, and the significance of early management is highlighted by high mortality [23].
5. Conclusions
The key to the management of the HIV-positive patient is the multidisciplinary approach and access to antiretroviral therapy. Patient adherence and compliance with antiretroviral therapy are also very important. Despite adequate antiretroviral coverage, HIV infection has continued to be found in our nation for a considerable amount of time. The promotion of voluntary testing must be the main objective, especially among those who are most at risk of contracting an infection (those who have intercourse with other males, those who inject drugs, those under 24 years old, sex workers, and those who are economically disadvantaged) [24,25].
Additionally, we must improve access to HIV testing, with community outreach initiatives being especially valuable. Always provide assistance with counseling and fast referrals to medical facilities to start ART in order to support these outreach initiatives. Promptness and speed of therapeutic intervention are essential elements for the patient's prognosis [26].
We must find and eliminate obstacles affecting patients and the healthcare system. In order to increase ART uptake among HIV-infected TB patients and to put an end to the TB and HIV epidemics, these hurdles must be removed [27].
Early initiation of antiretroviral therapy (ART) for the treatment of tuberculosis (TB) carries the risk of medication toxicity, drug-drug interactions, patients' perception of a high pill load, and immunological reconstitution inflammatory syndrome (IRIS), all of which have the potential to reduce patient adherence and retention in care [28,29].
Furthermore, HIV infection is linked to a higher risk of mortality, according to the majority of observational studies of TBM. Future studies on pharmacokinetics and clinical effects will help to refine the guidelines for ART and dual anti-tuberculous therapy [30].
Author Contributions
Conceptualization, I.I.L. M.C. and C.D.M.; Data curation, I.I.L., M.C. and G.S.; Formal analysis, G.S. and Ş.A.R.; Investigation, M.C. and I.I.L.; Methodology, I.I.L. and C.M.D..; Resources, I.I.L. Ş.A.R and G.S.; Software, I.I.L. and Ș.A.R.; Supervision, C.M.D.; Validation, M.C., I.I.L. and C.M.D.; Visualization, M.C., I.I.L. and C.M.D..; Writing—original draft, I.I.L. C.M.D and Ș.A.R; Writing—review & editing, I.I.L and M.C. All authors have read and agreed to the published version of the manuscript.
Funding
No funding was received.
Institutional Review Board Statement
The study was a retrospective one, conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Commission of “St. Parascheva” Clinical Hospital of Infectious Diseases, Iasi, Romania. (Decision no 28/April 10, 2022)
Informed Consent Statement
Not applicable.
Data Availability Statement
All data generated or analyzed during this study are included in this published article and its supplementary files.
Acknowledgments
To HIV/AIDS Department of “St. Parascheva” Clinical Hospital of Infectious Diseases Iasi, Romania, for providing institutional access and assistance in developing this study.
Conflicts of Interest
The authors declare no conflict of interest.
Ethics Approval and Consent to Participate
Ethics approval was obtained according to the internal Ethical Commission of Institute “St. Parascheva” Clinical Hospital of Infectious Diseases Iasi, Romania. (Decision no 3/March 20, 2023).
References
- Viviana Simon, David D Ho, and Quarraisha Abdool Karim, HIV/AIDS epidemiology, pathogenesis, prevention, and treatment, Lancet. 2006 Aug 5; 368(9534): 489–504. [CrossRef]
- Justiz Vaillant AA, Gulick PG. HIV Disease Current Practice. [Updated 2022 Sep 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-.
- Govender RD, Hashim MJ, Khan MA, Mustafa H, Khan G. Global Epidemiology of HIV/AIDS: A Resurgence in North America and Europe. J Epidemiol Glob Health. 2021 Sep;11(3):296-301. [CrossRef]
- HIV/AIDS surveillance in Europe: 2022 – 2021 data, 30 November 2022| Joint Infectious Diseases Unit (JID) World Health Organization. Regional Office for Europe & European Centre for Disease Prevention and Control. EVOLUȚIA HIV ÎN ROMÂNIA - 30 SEPTEMBRIE 2022, Institutul Național de Boli Infecțioase "Prof. Dr. Matei Balș"; Bucuresti, 2022 Sept. 5. https://www.cnlas.ro/images/doc/01122022.pdf.
- Slane VH, Unakal CG. Tuberculous Meningitis. [Updated 2022 Nov 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK541015/.
- Vinnard C, Macgregor RR. Tuberculous meningitis in HIV-infected individuals. Curr HIV/AIDS Rep. 2009 Aug;6(3):139-45. [CrossRef]
- Wilkinson, R., Rohlwink, U., Misra, U. et al. Tuberculous meningitis. Nat Rev Neurol 13, 581–598 (2017). [CrossRef]
- Huynh J, Donovan J, Phu NH, Nghia HDT, Thuong NTT, Thwaites GE. Tuberculous meningitis: progress and remaining questions. Lancet Neurol. 2022 May;21(5):450-464. [CrossRef] [PubMed]
- Updated recommendations on HIV prevention, infant diagnosis, antiretroviral initiation and monitoring [Internet]. Geneva: World Health Organization; 2021 Mar. 4, CLINICAL GUIDELINES: TIMING OF ANTIRETROVIRAL THERAPY.
- Sultana, Z.Z., Hoque, F.U., Beyene, J. et al. HIV infection and multidrug resistant tuberculosis: a systematic review and meta-analysis. BMC Infect Dis 21, 51 (2021). [CrossRef]
- Stephen D. Lawn , Robin Wood, Poor Prognosis of HIV-Associated Tuberculous Meningitis Regardless of the Timing of Antiretroviral Therapy, Clinical Infectious Diseases, Volume 52, Issue 11, 1 June 2011, Pages 1384–1387. [CrossRef]
- Fiona V Cresswell and others, High-Dose Oral and Intravenous Rifampicin for the Treatment of Tuberculous Meningitis in Predominantly Human Immunodeficiency Virus (HIV)-Positive Ugandan Adults: A Phase II Open-Label Randomized Controlled Trial, Clinical Infectious Diseases, Volume 73, Issue 5, 1 September 2021, Pages 876–884. [CrossRef]
- Ita Anggraini, Yovita Hartantri, Ahmad Rizal. A Phenotypic Comparison between HIV Positive and HIV Negative Tuberculous Meningitis Patients, Makara Journal of Health Research, Vol. 21 > Iss. 3 (2017). [CrossRef]
- Thwaites, Guy E., et al. “The Influence of HIV Infection on Clinical Presentation, Response to Treatment, and Outcome in Adults with Tuberculous Meningitis.” The Journal of Infectious Diseases, vol. 192, no. 12, 2005, pp. 2134–41. JSTOR, http://www.jstor.org/stable/30086418. Accessed 21 May 2023.
- Croda MG, Vidal JE, Hernández AV, Dal Molin T, Gualberto FA, de Oliveira AC. Tuberculous meningitis in HIV-infected patients in Brazil: clinical and laboratory characteristics and factors associated with mortality. Int J Infect Dis. 2010 Jul;14(7):e586-91. [CrossRef]
- Boonyagars L, Sangketchon C, Pholtawornkulchai K. Presentation, Clinical Characteristics, and Treatment Outcomes among Tuberculous Meningitis Patients with and Without HIV Infection at Vajira Hospital, Thailand: A Retrospective Cohort Study. Journal of the International Association of Providers of AIDS Care (JIAPAC). 2021;20. [CrossRef]
- Maitre, T., Bonnet, M., Calmy, A. et al. Intensified tuberculosis treatment to reduce the mortality of HIV-infected and uninfected patients with tuberculosis meningitis (INTENSE-TBM): study protocol for a phase III randomized controlled trial. Trials 23, 928 (2022). [CrossRef]
- Pormohammad A, Nasiri MJ, Riahi SM, Fallah F. Human immunodeficiency virus in patients with tuberculous meningitis: systematic review and meta-analysis. Trop Med Int Health. 2018 Jun;23(6):589-595. [CrossRef]
- Vinnard, C., Macgregor, R.R. Tuberculous meningitis in HIV-infected individuals. Curr HIV/AIDS Rep 6, 139–145 (2009). [CrossRef]
- Garg RK, Sinha MK. Tuberculous meningitis in patients infected with human immunodeficiency virus. Journal of Neurology. 2011 Jan;258(1):3-13. [CrossRef]
- Karande, S., Gupta, V., Kulkarni, M. et al. Tuberculous meningitis and HIV. Indian J Pediatr 72, 755–760 (2005). [CrossRef]
- Martino RJ, Chirenda J, Mujuru HA, Ye W, Yang Z. Characteristics Indicative of Tuberculosis/HIV Coinfection in a High-Burden Setting: Lessons from 13,802 Incident Tuberculosis Cases in Harare, Zimbabwe. Am J Trop Med Hyg. 2020 Jul;103(1):214-220. [CrossRef]
- Mukuku O, Mutombo AM, Kakisingi CN, Musung JM, Wembonyama SO, Luboya ON. Tuberculosis and HIV co-infection in Congolese children: risk factors of death. Pan Afr Med J. 2019 Aug 27;33:326. [CrossRef]
- Management of opportunistic infections in HIV/ AIDS Clinical protocol for the WHO European Region, Denmark, 2007.
- Feinberg J, Keeshin S. Prevention and Initial Management of HIV Infection. Ann Intern Med. 2022 Jun;175(6):ITC81-ITC96. [CrossRef]
- Naidoo K, Rampersad S, Karim SA. Improving survival with tuberculosis & HIV treatment integration: A mini-review. Indian J Med Res. 2019 Aug;150(2):131-138. [CrossRef]
- Aung, N.H.H.L.; Soe, K.T.; Kumar, A.M.V.; Saw, S.; Aung, S.T. What Are the Barriers for Uptake of Antiretroviral Therapy in HIV-Infected Tuberculosis Patients? A Mixed-Methods Study from Ayeyawady Region, Myanmar. Trop. Med. Infect. Dis. 2020, 5, 41. [Google Scholar] [CrossRef]
- Burke, R. M., Rickman, H. M., Singh, V., Corbett, E. L., Ayles, H., Jahn, A., Hosseinipour, M. C., Wilkinson, R. J. and MacPherson, P. What is the optimum time to start antiretroviral therapy in people with HIV and tuberculosis coinfection? A systematic review and meta-analysis. J Int AIDS Soc. 2021; 24(7):e25772. [CrossRef]
- Hamada Y, Getahun H, Tadesse BT, Ford N. HIV-associated tuberculosis. Int J STD AIDS. 2021 Aug;32(9):780-790.
- Purmohamad A, Azimi T, Nasiri MJ, Goudarzi M, Zangiabadian M, Sedighian H, Fooladi AAI. HIV-Tuberculous Meningitis Co-Infection: A Systematic Review and Meta-Analysis. Curr Pharm Biotechnol. 2021;22(7):960-968. [CrossRef]
Figure 1.
Distribution of TBM HIV cases by sex.
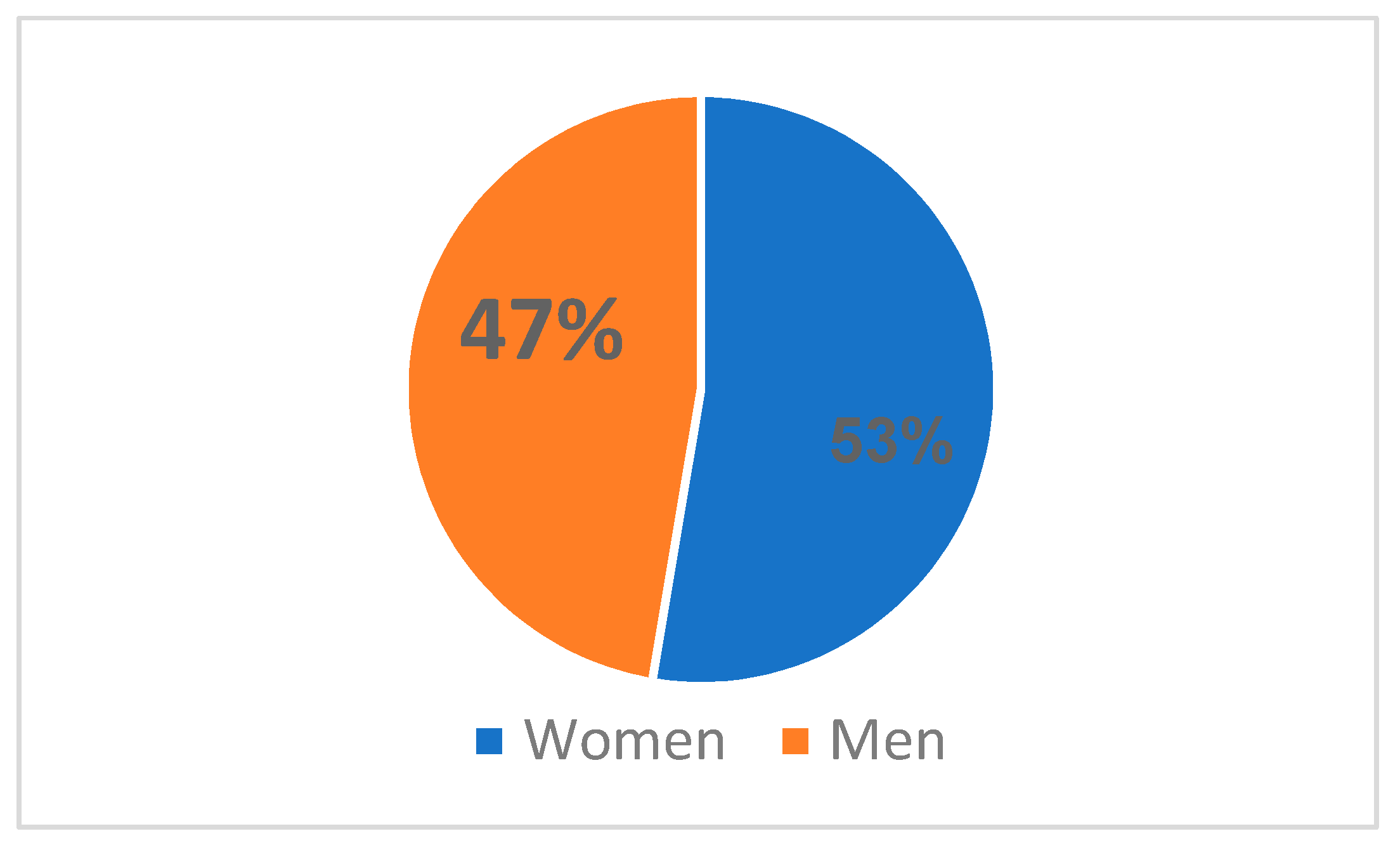
Figure 2.
TBM HIV cases distribution by area.
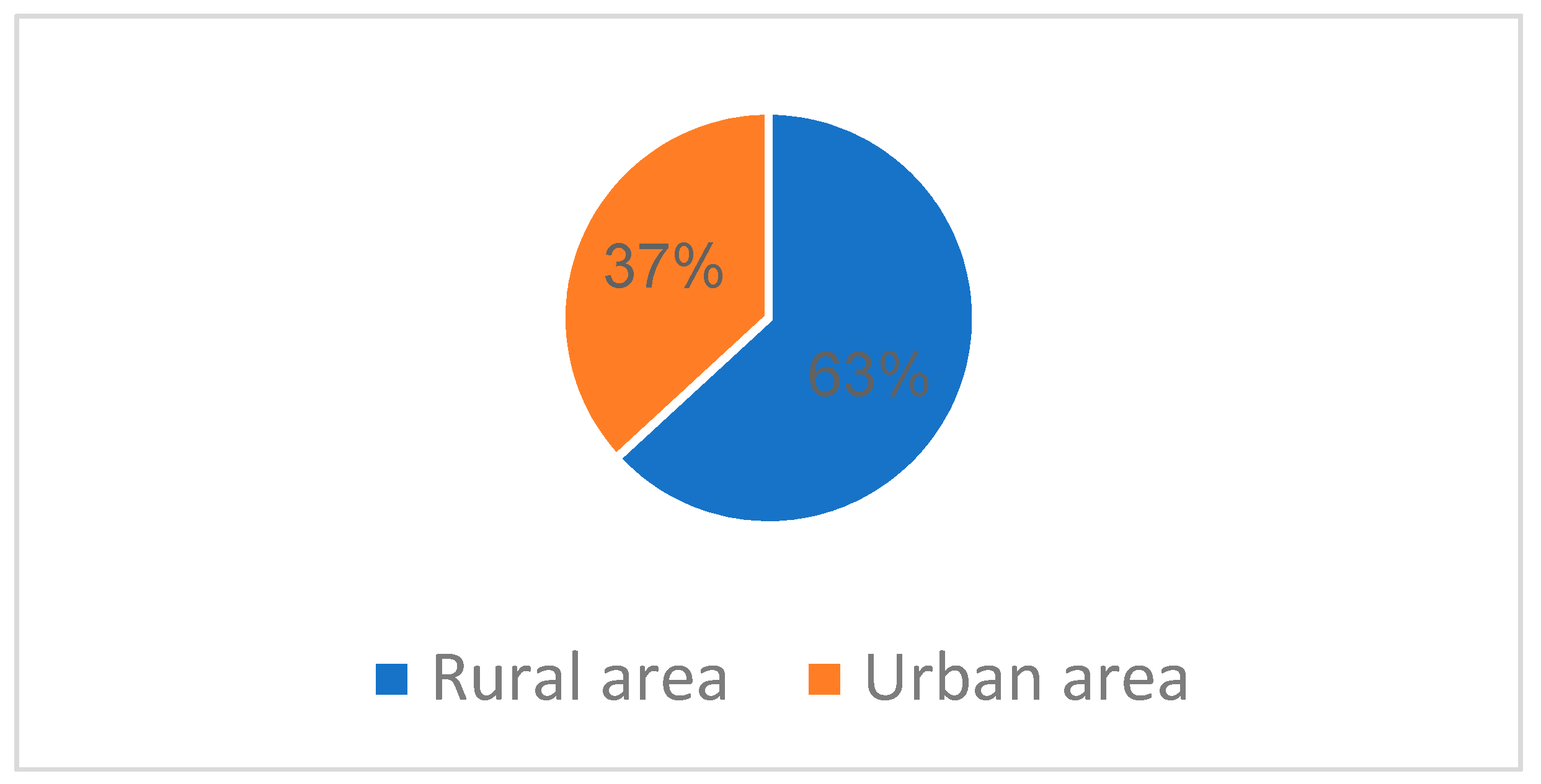
Figure 3.
Distribution of cases by CD4+ T-lymphocytes level (cells/μl).
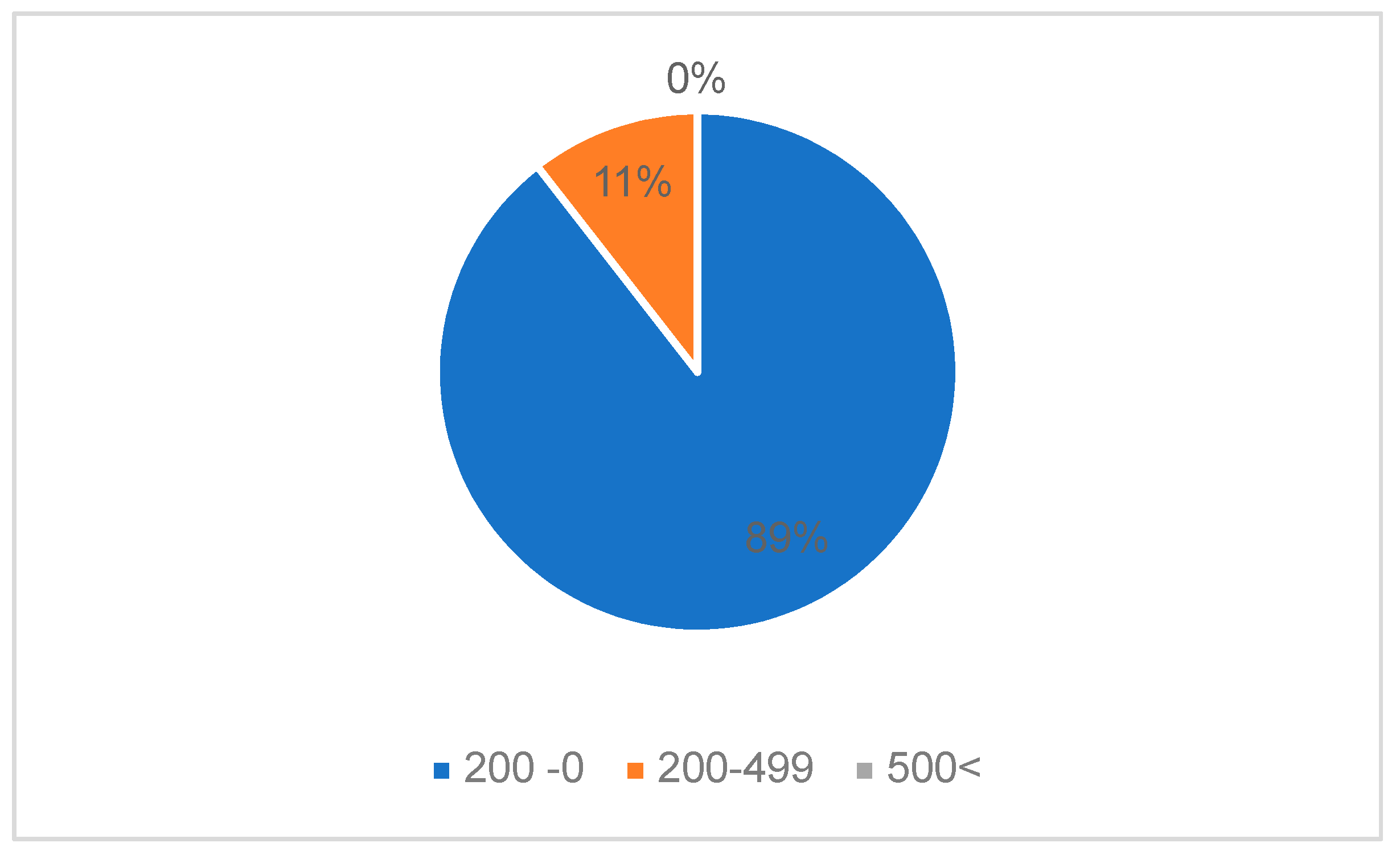
Figure 4.
Distribution of HIV cases by CD4+ T-lymphocytes level and HIV viral load.
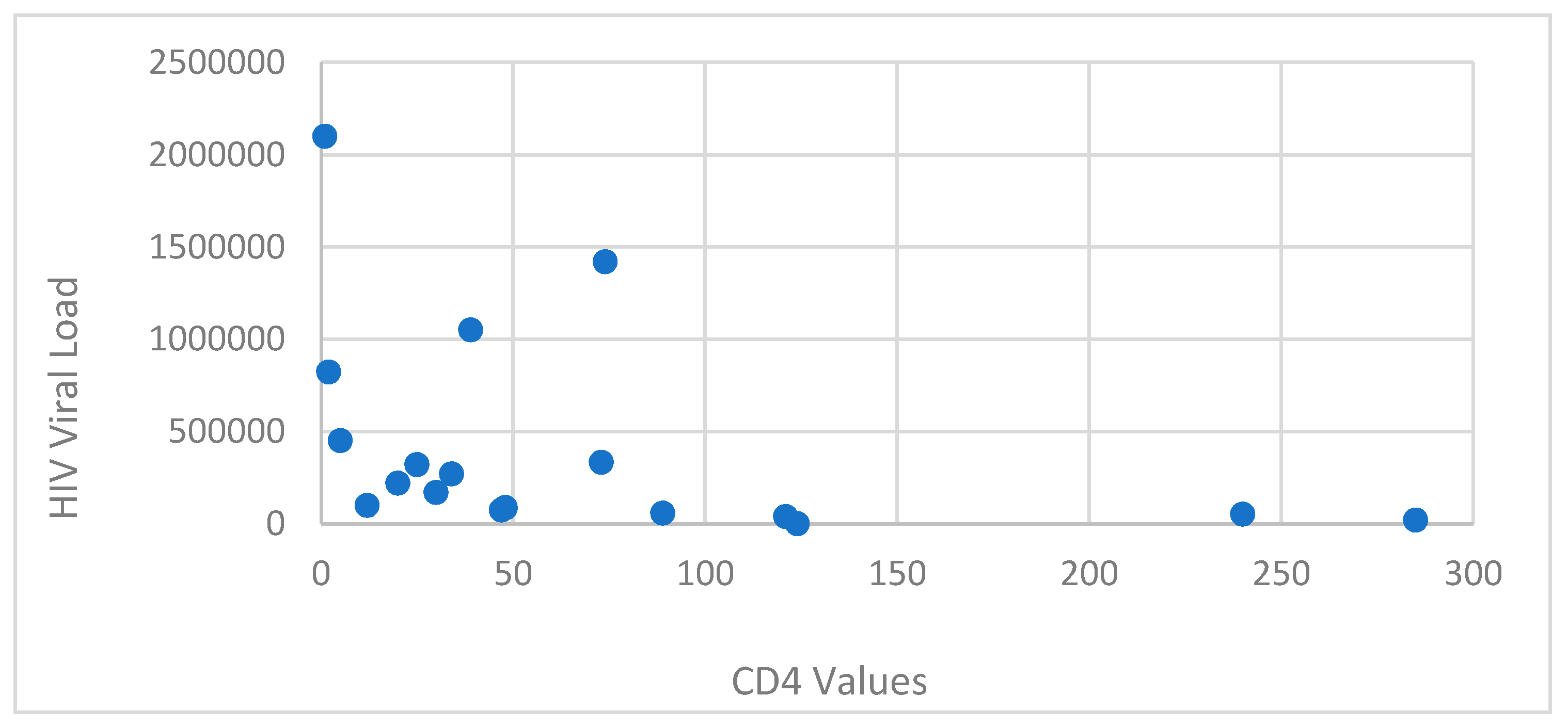
Figure 5.
Distribution of TBM HIV cases by number of admission days.
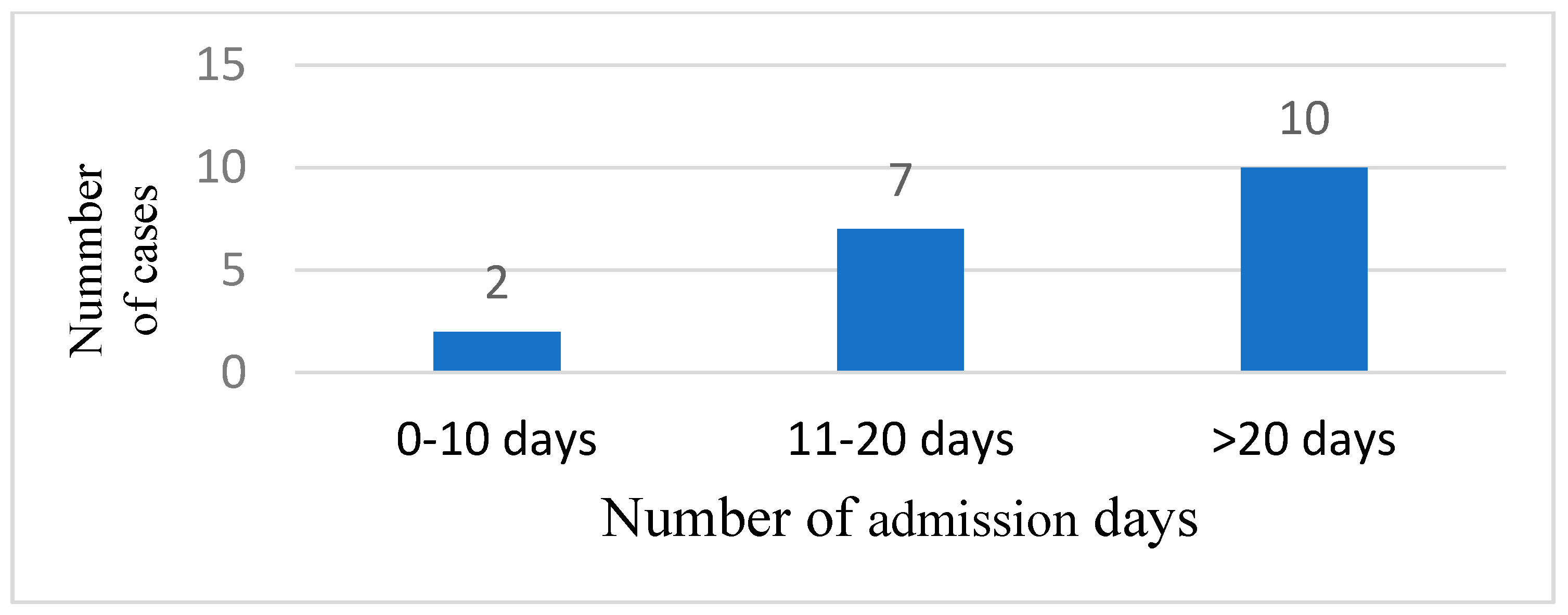
Figure 7.
The quantitative examination of cerebrospinal fluid.
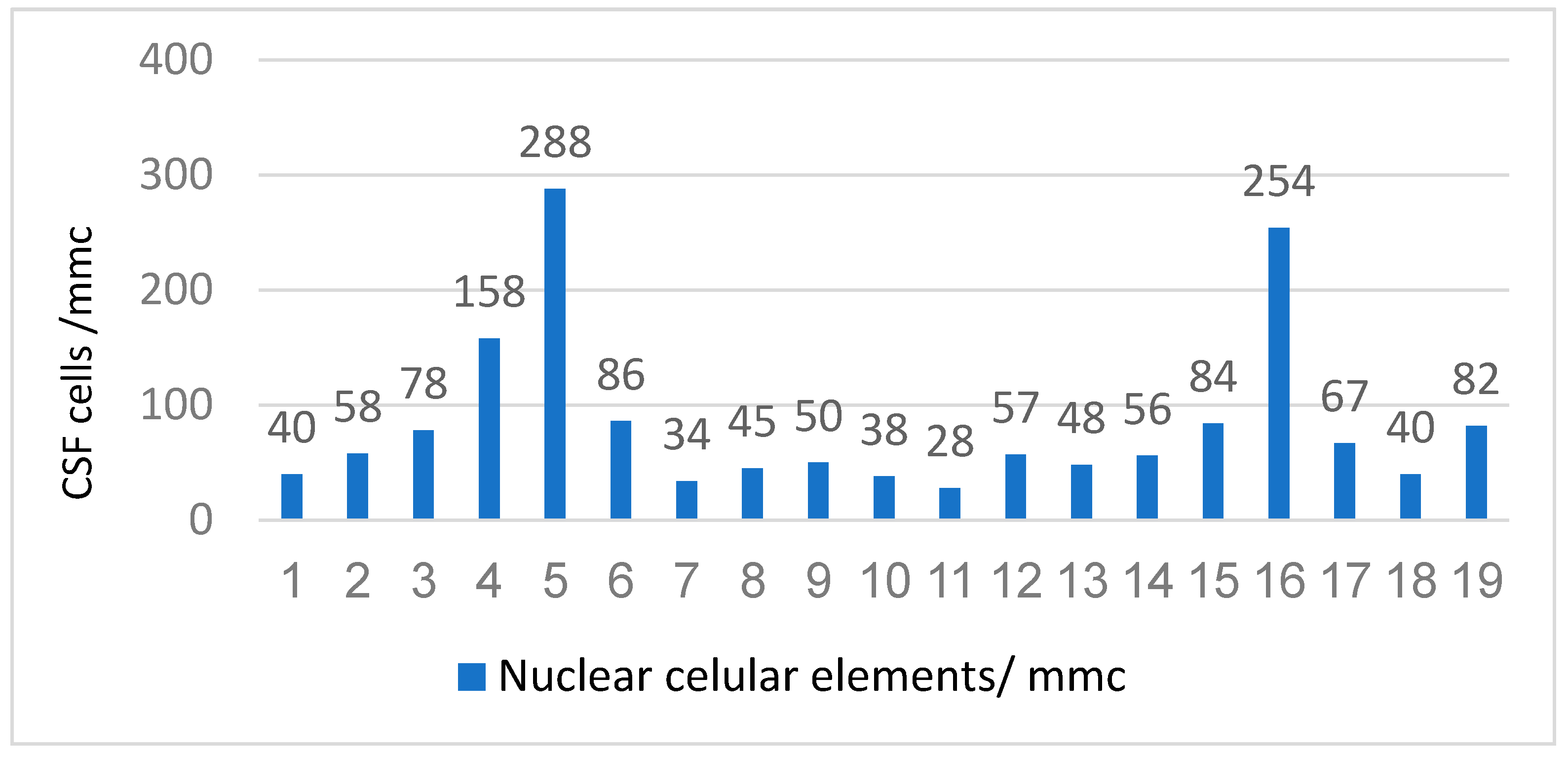
Figure 8.
The qualitative examination of cerebrospinal fluid.
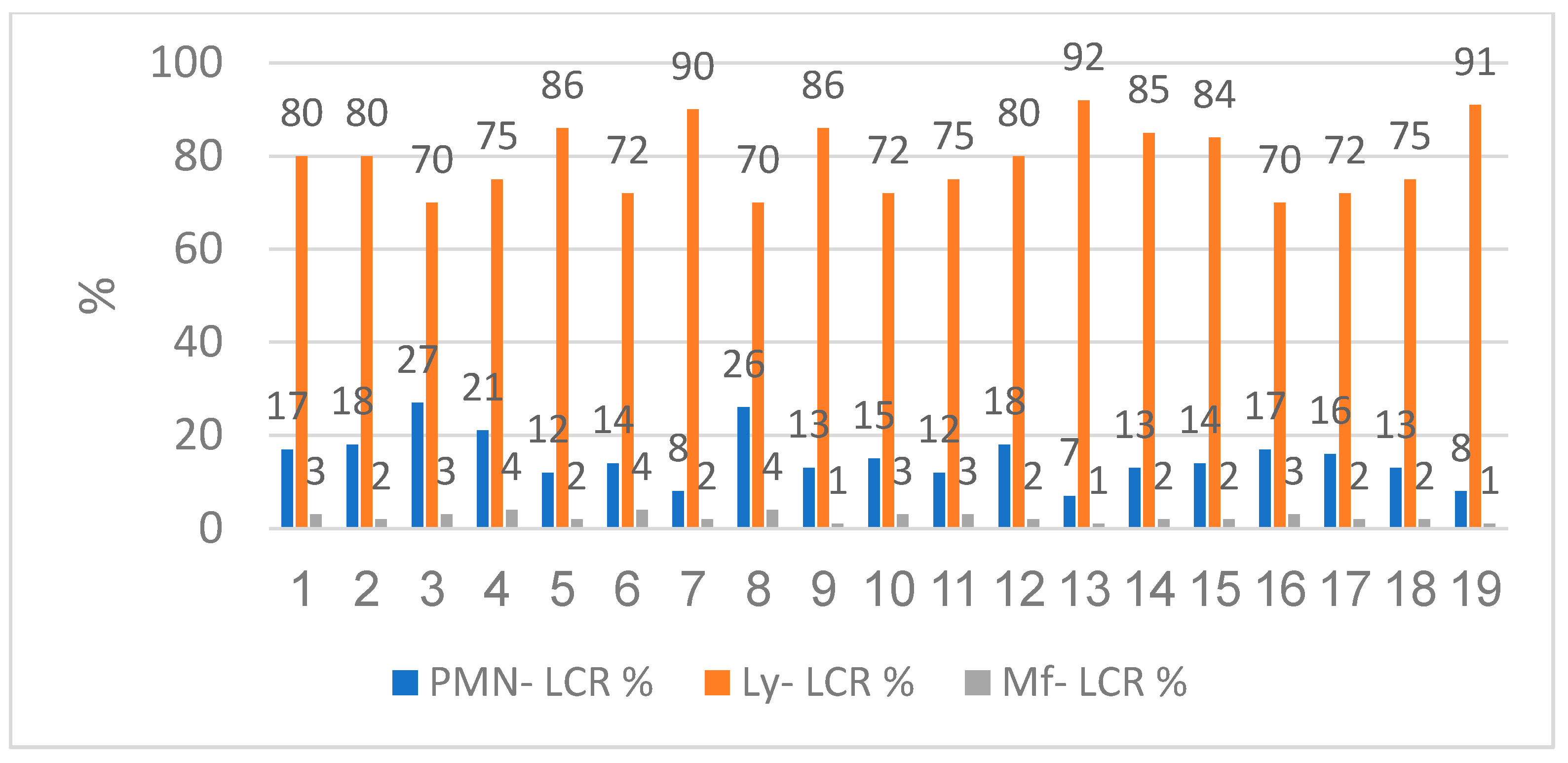
Figure 9.
Biochemistry examination of cerebrospinal fluid- increased glycorrhagia, albuminorrhagia and decreased chlororrhagia.
Figure 9.
Biochemistry examination of cerebrospinal fluid- increased glycorrhagia, albuminorrhagia and decreased chlororrhagia.
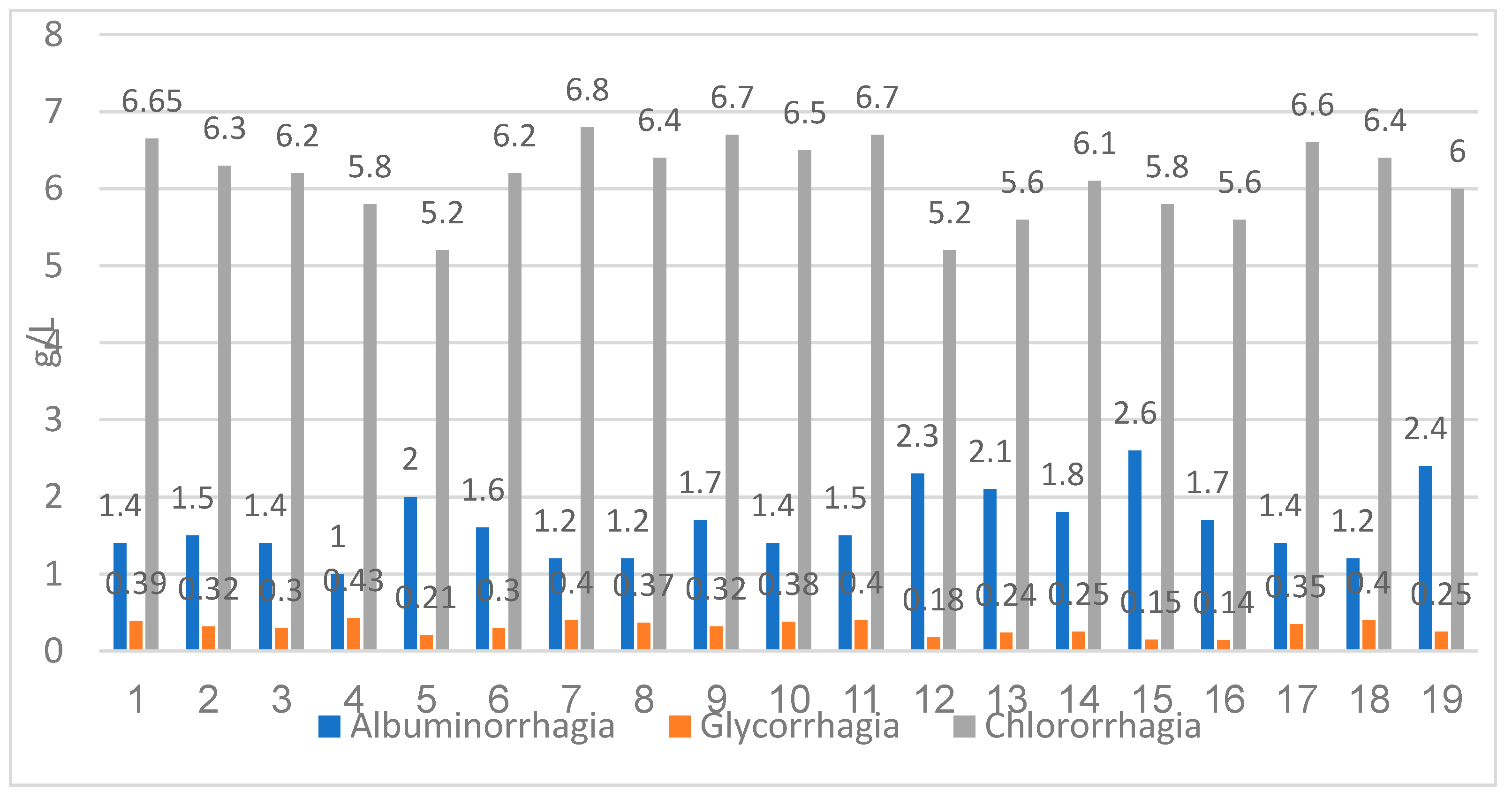
Figure 10.
Evolution of our TBM HIV coinfected patients.
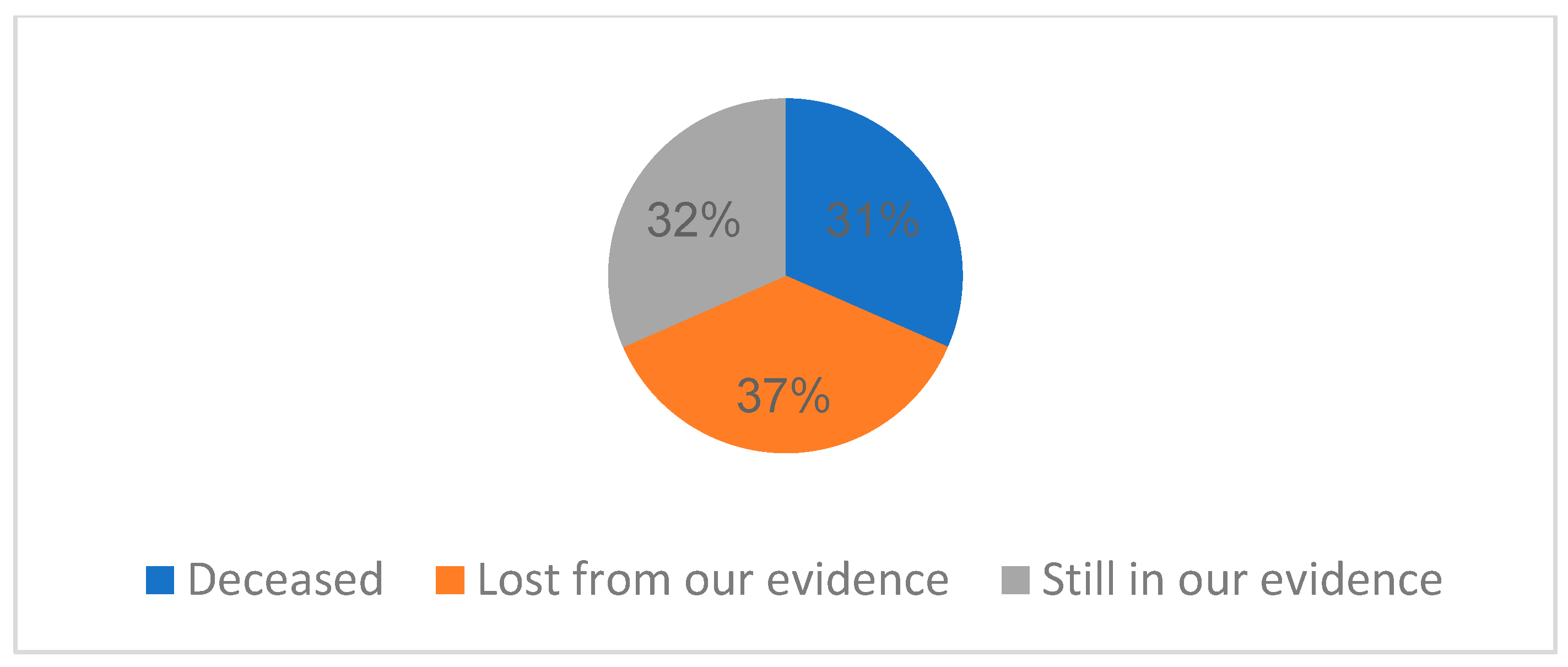
Figure 11.
Distribution of HIV cases by CD4+ T-lymphocytes level and HIV viral load at one-year evaluation.
Figure 11.
Distribution of HIV cases by CD4+ T-lymphocytes level and HIV viral load at one-year evaluation.
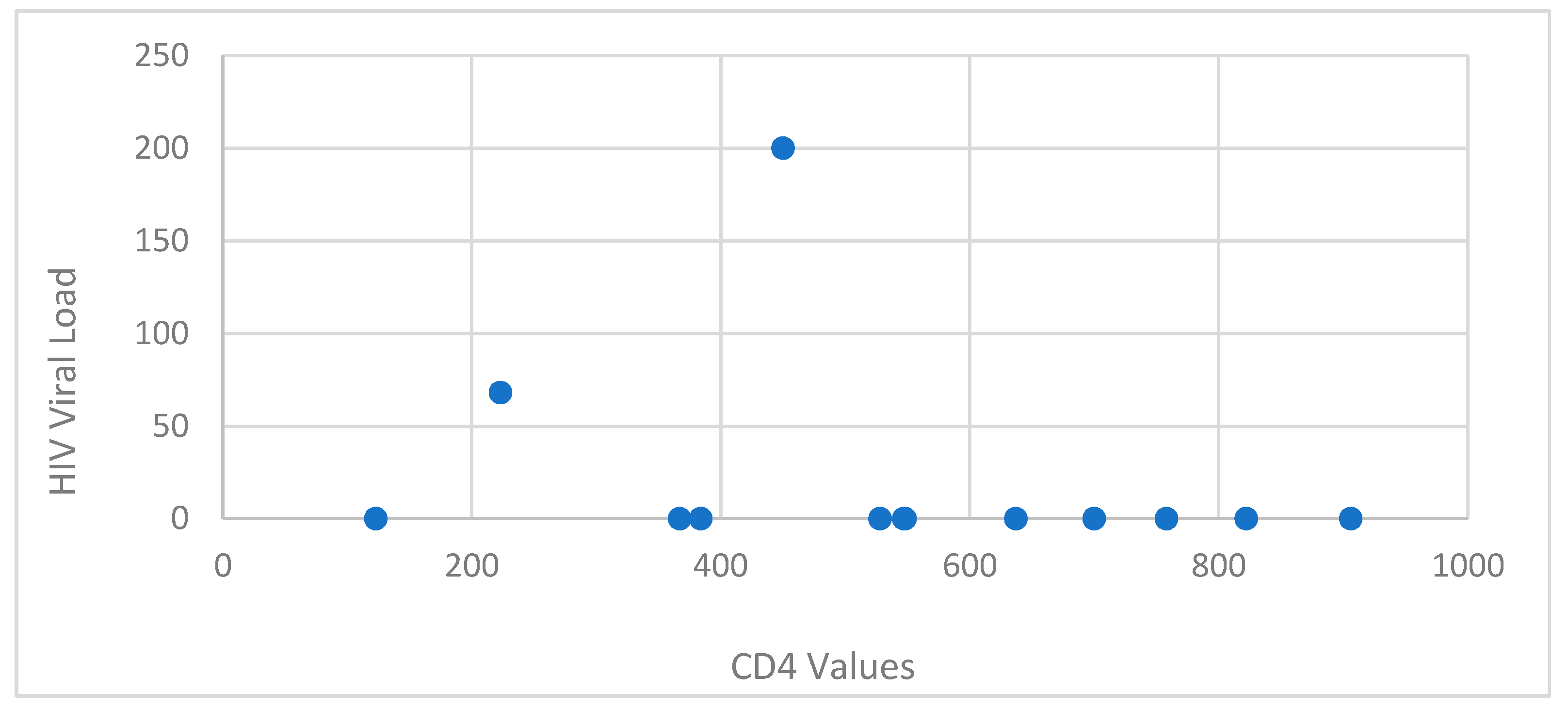

Table 1.
Distribution of TBM HIV cases by age.
| Age (years) | n | % |
|---|---|---|
| 0-20 | 1 | 5.26 |
| 21-30 | 10 | 26.31 |
| 31-40 | 5 | 40.12 |
| 41-50 | 2 | 10.52 |
| 51-60 | 1 | 5.26 |
Table 2.
Distribution of TBM HIV cases by county in North East Romania.
| County | n | % |
|---|---|---|
| Iasi | 4 | 21 |
| Neamt | 1 | 5 |
| Vaslui | 1 | 5 |
| Bacau | 2 | 11 |
| Botosani | 4 | 21 |
| Suceava | 7 | 37 |
Table 3.
Route of transmission of the study group.
| n | % | |
|---|---|---|
| Known route of transmission | 18 | 94.73 |
| Sexual transmission | 17 | 89.47 |
| Drug-use transmission | 1 | 5.26 |
| Perinatal transmission | 0 | 0 |
| Unknown route of transmission | 1 | 5.26 |
Table 4.
Distribution of TBM HIV cases by CD4+ T-lymphocytes level and sex.
| CD4+ T-lymphocytes level p=0.065 |
male | female | total | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| 0-199 cells/μl | 8 | 42.10 | 9 | 47.37 | 17 | 89.47 |
| 200-499 cells/μl | 1 | 5.26 | 1 | 5.26 | 2 | 10.52 |
| >500 cells/μl | 0 | 0 | 0 | 0 | 0 | 0 |
Table 5.
Distribution of cases based on sex and metabolic syndrome and liver enzymes.
| Laboratory Marker |
Value |
Male | Female | Total | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| ALT |
normal | 6 | 31.57 | 7 | 36.84 | 13 | 68.41 |
| abnormal | 3 | 15.78 | 3 | 15.78 | 6 | 31.56 | |
| AST |
normal | 5 | 26.31 | 6 | 31.57 | 11 | 57.88 |
| abnormal | 4 | 21.05 | 4 | 21.05 | 8 | 42.10 | |
| GGT |
normal | 3 | 15.78 | 6 | 31.57 | 9 | 47.35 |
| abnormal | 6 | 31.57 | 4 | 21.05 | 10 | 52.62 | |
| Cholesterol |
normal | 7 | 36.84 | 5 | 26.31 | 12 | 63.15 |
| Abnormal | 2 | 10.52 | 5 | 26.05 | 6 | 36.57 | |
| HDL-COL |
normal | 7 | 36.84 | 5 | 26.31 | 12 | 63.15 |
| abnormal | 2 | 10.52 | 5 | 26.05 | 6 | 36.57 | |
| LDL-COL |
normal | 5 | 26.31 | 3 | 15.78 | 8 | 42.09 |
| abnormal | 4 | 21.05 | 7 | 36.84 | 11 | 57.89 | |
| Triglycerides |
normal | 5 | 26.31 | 3 | 15.78 | 8 | 42.09 |
| abnormal | 4 | 21.05 | 7 | 36.84 | 11 | 57.89 | |
Table 6.
ARV treatment before admission of the patients that were already in our evidence.
| ARV therapy regimens | Number of patients | % |
|---|---|---|
| Protease inhibitors | 7 | 46.15 |
| Integrase inhibitors | 5 | 38.46 |
| 2 INNRT+ INRT | 1 | 7.69 |
Table 7.
Distribution by CD4+ T-lymphocytes level and sex, one month after ART.
| CD4 levels (p=0.053) |
male | female | Total | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| 0-200 cells/μl | 1 | 7.69 | 0 | 0 | 1 | 7.69 |
| 200-499 cells/μl | 1 | 7.69 | 3 | 23.07 | 4 | 30.76 |
| >500 cells/μl | 3 | 23.07 | 5 | 38.46 | 8 | 61.53 |
Table 8.
Distribution by HIV viral load level, at first presentation and one month after ART.
| HIV Viral Load (p=0,5) |
First presentation | One month after ART | ||
|---|---|---|---|---|
| n | % | n | % | |
| <40 copies/ml | 0 | 0 | 11 | 84.61 |
| >40 copies/ml | 19 | 100 | 2 | 15.38 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



