Submitted:
17 July 2023
Posted:
18 July 2023
You are already at the latest version
Preprints.org 2023 Most Popular Preprints Award Winner Collection
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: COVID-19 vaccines have been linked to myocarditis which in some circumstances can be fatal. This systematic review aims to investigate potential causal links between COVID-19 vaccines and death from myocarditis using post-mortem analysis. Methods: We performed a systematic review of all published autopsy reports involving COVID-19 vaccination-related myocarditis through July 3rd, 2023. All autopsy studies that include COVID-19 vaccine-induced myocarditis as a possible cause of death were included, without imposing any additional restrictions. Causality in each case was determined by three independent reviewers with cardiac pathology experience and expertise. Results: We initially identified 1,691 studies and, after screening for our inclusion criteria, included 14 papers that contained 28 autopsy cases. The cardiovascular system was the only organ system affected in 26 cases. In 2 cases, myocarditis was characterized as a consequence from multisystem inflammatory syndrome (MIS). The mean and median number of days from last COVID-19 vaccination until death was 6.2 and 3 days, respectively. Most of the deaths occurred within a week from the last injection. We established that all 28 deaths were causally linked to COVID-19 vaccination by independent adjudication. Conclusions: The temporal relationship, internal and external consistency seen among cases in this review with known COVID-19 vaccine-induced myocarditis, its pathobiological mechanisms and related excess death, complemented with autopsy confirmation, independent adjudication, and application of the Bradford Hill criteria to the overall epidemiology of vaccine myocarditis, suggests there is a high likelihood of a causal link between COVID-19 vaccines and death from suspected myocarditis in cases where sudden, unexpected death has occurred in a vaccinated person. Urgent investigation is required for the purpose of risk stratification and mitigation in order to reduce the population occurrence of fatal COVID-19 vaccine-induced myocarditis.
Keywords:
myocarditis
; sudden death
; chest pain
; autopsy
; necropsy
; COVID-19
; COVID-19 vaccines
; mRNA
; SARS-CoV-2 vaccination
; death
; excess mortality
; spike protein
; organ system
Introduction
As of July 6th, 2023, SARS-CoV-2 has infected approximately 767,726,861 individuals around the world, causing 6,948,764 deaths1. The United States Government, in reaction to the pandemic, implemented the Operation Warp Speed (OWS) initiative. This resulted in the development and administration of the first doses of COVID-19 vaccine in less than 11 months after the identification of the SARS-CoV-2 genetic sequence2. This marked the most rapid development of a vaccine in history, however, there was insufficient time and investigation to adequately establish cardiovascular safety2. At the time of writing, about 70% of the world population have been vaccinated with at least one dose of a COVID-19 vaccine1.
The predominant COVID-19 vaccine platforms include messenger RNA (mRNA) (Pfizer-BioNTech – BNT162b2, Moderna – mRNA-1273), viral vector (AstraZeneca – ChAdOx1 nCoV-19, Johnson & Johnson – Ad26.COV2.S, Sputnik V), and protein subunit (Novavax – NVX-CoV2373, Zifivax – ZF2001)3. mRNA and viral vector vaccines involve the bodily synthesis of the SARS-CoV-2 Spike protein as the foundation of the immune response, while protein subunit vaccines utilize injection of exogenous Spike protein, bypassing the need for genetic mechanisms3. Regardless of the vaccine platform used, circulating SARS-CoV-2 Spike protein is the likely detrimental agent through which COVID-19 vaccines cause biological harm4-13. Spike protein can initiate the breakdown and internalization of ACE2 receptors, which may disrupt the renin–angiotensin system (RAS) and lead to increased inflammation, vasoconstriction, and thrombosis4. Further, Spike protein can stimulate platelets and inflict damage to the endothelium, which can lead to arterial and venous thrombosis5. Immune cells that have absorbed the lipid nanoparticles (LNPs) subsequently reintroduce them into the bloodstream with a higher number of exosomes carrying microRNAs and Spike protein, possibly resulting in drastic inflammation5. Long term immune surveillance may be compromised by mRNA COVID-19 vaccines due to IRF7, IRF9, p53, and BRCA suppression5,6. There is a high probability of a causal link between COVID-19 mRNA vaccination and myocarditis, neurodegenerative disease, immune thrombocytopenia, Bell's palsy, liver disease, impaired adaptive immunity, impeded DNA damage response and tumorigenesis5. Moreover, a recent study found that repeated COVID-19 vaccination with mRNA-based vaccines leads to the production of abnormally high concentrations of IgG4 antibodies7. These antibodies can fail to neutralize Spike protein, which has been shown to circulate for at least 28 days, cause immune suppression, and promote the development of autoimmune diseases including myocarditis7-13.
In June 2021, the United States FDA and CDC issued a joint warning on myocarditis occurring after mRNA COVID-19 vaccination14. A PUBMED search performed at the time of writing for “myocarditis” and “COVID-19 vaccination” yielded 994 results, indicating a high prevalence of COVID-19 vaccine-related myocarditis in the peer-reviewed literature. Rose and McCullough found that the peak age was 18-24 years and 90% of cases were men15. Myocarditis development most commonly occurred after the second dose, however, additional cases occurred after the third dose, adding to the cumulative risk for individuals continuing with every six-month injection schedules15. Avolio et al demonstrated the cardiac pericyte as one of several cell lines that take up mRNA, produce Spike protein and express it on the cell surface inciting autoimmune attack13. Yonker et al found that children hospitalized with myocarditis had presence of free Spike protein not neutralized by antibodies while those who were asymptomatic had appropriate neutralization of Spike protein by anti-Spike antibodies11. A biodistribution study has shown that lipid nanoparticles can travel to the heart as well as other vital organs16. Baumeier et al found that among 15 young individuals suffering from myocarditis who underwent cardiac biopsy, the myocardium stained for SARS-CoV-2 Spike protein and not nucleocapsid, effectively ruling out infection and leaving vaccination as the only possible source of Spike protein17. Furthermore, they found a range of pathologies from inflammatory cardiomyopathy to active myocarditis and severe giant cell myocarditis17. Detection of Spike protein and CD4+ T-cell-dominated inflammation within cardiac tissue suggested vaccine-triggered autoimmune processes17. Two prospective cohort studies, by Mansanguan et al18 and Le Pessec19, suggested the incidence of myocarditis or troponin elevation from COVID-19 vaccine dose number two and three could be as high as 2.3% and 2.8%, respectively. Because of the frequent occurrence of this problem in cardiovascular practice, the United Kingdom20 and Australia21 have issued clinical practice guidelines on the diagnosis and management of COVID-19 vaccine-induced myocarditis.
Up to June 16th, 2023, the Vaccine Adverse Events Reporting System (VAERS) included 1,569,668 adverse event reports associated with COVID-19 vaccines, including 35,487 deaths, 27,229 myocarditis and pericarditis, and 20,184 heart attack reports22. Before the COVID-19 pandemic, Meissner reported that 86% of VAERS entries were completed by medical personnel or vaccine manufacturers and only 14% were made by the patient or their family23. Thus, VAERS has demonstrated a very strong crude signal for myocarditis as an accepted complication of COVID-19 vaccination, however, additional information can be gleaned from autopsy in cases of death that are suspected to be caused by COVID-19 immunization. Autopsies represent one of the most powerful diagnostic methods in medicine, ascertaining causes of death and elucidating the pathophysiological mechanisms of disease24. COVID-19 vaccines exhibit multiple mechanisms of injury to the cardiovascular system and are associated with a considerable number of adverse event reports, thus representing an exposure that may be causally linked to death in some myocarditis cases. This systematic review aims to investigate potential causal links between COVID-19 vaccines and death from myocarditis using post-mortem analysis.
Methods
We performed a systematic review of all published autopsy reports involving COVID-19 vaccination-related myocarditis through July 3rd, 2023. All autopsy studies that include COVID-19 vaccine-induced myocarditis as a possible cause of death were included, without imposing any additional restrictions. We searched PubMed and ScienceDirect using the following key words: ‘COVID-19 Vaccine’, ‘SARS-CoV-2 Vaccine’, ‘COVID Vaccination’, and ‘Post-mortem’, ‘Autopsy’, or ‘myocarditis’. All included studies were examined for pertinent literature contained in their references. In the calculation of mean age, estimated age values were excluded. Causality in each case was determined in accordance with independent review by three qualified physicians with experience and expertise in cardiac pathology. A quorum of 2 out of three was required to establish a positive causal linked to COVID-19 vaccination.
Results
The database search yielded 1,691 studies that may have met our inclusion criterion. After removing 1,212 duplicate papers and screening 479 unique studies, only 12 met our inclusion criterion. A detailed screening of references found 8 additional papers, with 2 of them fulfilling our inclusion criterion. Overall, we included 14 studies that contain 28 autopsy cases of COVID-19 vaccinees diagnosed with myocarditis (Figure 1).
The included 14 reports25-38 are summarized in Table 1. Of the 28 autopsy cases, 9 (32.1%) were female. The mean age of death was 44.4 years old. 18 cases (64%) received Pfizer/BioNTech vaccines, 9 cases (32%) received Moderna vaccines, and 1 case received a Zifivax vaccine. The cardiovascular system was the only organ system affected in 26 cases. In 2 cases, myocarditis was seen as a consequence from multisystem inflammatory syndrome (MIS) (Figure 2). The number of days from vaccination to death was 6.2 (mean), 3 (median). Most (75%) of the deaths occurred within a week from last vaccination (Figure 3).
All 28 cases (100%) were found to be casually linked to COVID-19 vaccination in accordance with independent adjudication. Most cases had symptoms consistent with myocarditis prior to death (chest pain, effort intolerance) and in the case of Choi et al, a 22-year-old Korean man died in the hospital after seven hours of intensive attempts at supportive care32. The autopsy showed intense inflammation and destruction of cardiac tissue including the conduction system. Other cases had no reported symptoms before death. Gill et al reported two boys, age 16 and 17, who died a few days after mRNA injection while asleep at home30. Autopsies revealed patchy inflammation suggesting that sudden arrhythmic death had occurred. The authors in these cases concluded the cause of death was COVID-19 vaccine-induced myocarditis.
Discussion
We established that all 28 deaths are causally linked to COVID-19 vaccination by independent review of the clinical information presented in each paper. Our data are consistent with the overall epidemiological literature (PUBMED search for [COVID-19 vaccination] * [myocarditis] = 994 papers) concerning COVID-19 vaccine-induced myocarditis where the Bradford Hill Criteria39 support causality from an epidemiological perspective. This includes biological plausibility, temporal association, internal and external validity, coherence, analogy, and reproducibility with each successive report of myocarditis-related death after COVID-19 vaccination. Baumeier et al’s findings that the myocardium stained for SARS-CoV-2 Spike protein and not nucleocapsid among 15 young individuals suffering from myocarditis indicated the sole cause of cardiac injury in post-vaccine myocarditis is highly likely to be COVID-19 vaccination, confirming our results (Figure 4)17. In addition, Baumeier found Spike protein and CD4+ T-cell-dominated inflammation, suggesting the COVID-19 vaccine as the single cause of autoimmune reaction processes seen in myocardial histology (Figure 5)17. However, since the vaccines fail to stop the development of COVID-19 illness, both COVID-19 vaccination and SARS-CoV-2 infection may have contributed to cardiac Spike protein injury in cases where infection was not ruled out. The predominant mechanism of death is most likely a sudden arrhythmia such as ventricular tachycardia or ventricular fibrillation. Relatively few cases had antecedent fulminant pump failure. These data are concerning when considered in light of young individuals, particularly male athletes who have had sudden death after vaccination without an autopsy. Polykretis and McCullough have reported that, among professional and semi-professional European athletes less than 35 years old, compared to a stable period before the pandemic, the annualized rate of sudden death since the rollout of COVID-19 vaccines has increased ten-fold40. Cadegiani has postulated that a surge of catecholamines can be the trigger for COVID-19 vaccine-induced sudden death41 which could explain the occurrence during exercise and sports as well as during the early morning waking hours from sleep where there is a surge of epinephrine and norepinephrine42.
Our findings escalate concerns regarding COVID-19 vaccine-induced myocarditis and its mechanisms, particularly in cases of sudden unexpected death in younger individuals where there is no other explanation. COVID-19 vaccine Spike protein is produced in the body for an uncontrolled duration and in unknown quantity resulting in deleterious effects4-13, especially on the heart10,11,13-21, explaining the cardiovascular deaths seen in our study without evidence of other organ system involvement. Multisystem Inflammatory Syndrome (MIS) has been identified following COVID-19 vaccination in both children43 and adults44, however, we found only 2 autopsy cases with this diagnosis. MIS may be caused by the systemic distribution of the LNPs containing mRNA after vaccine administration16 and the consequent systemic Spike protein expression and circulation resulting in extensive inflammation. Considering the average time of 6.2 days between vaccination and death, a temporal link between COVID-19 vaccination and death is corroborated by the observation that SARS-CoV-2 mRNA Spike vaccine sequences can persist in the bloodstream for at least 28 days after vaccination12.
Ittiwut et al have found that genetic susceptibility to sudden death may explain some of the variation45. Polymorphisms in the SCN5A channel were associated with the highest rates of sudden death in their study45. The overwhelming predominance of men among COVID-19 vaccine-related myocarditis cases15, as well has other vaccines including smallpox and influenza46, suggests that androgen receptors or some other undiscovered interaction with male hormones may play a role in the manifestation of vaccine-induced myocarditis.
Figure 6 highlights the major steps in COVID-19 vaccine-induced myocarditis. Baseline susceptibility includes male gender, age 18-24, SCN5A polymorphisms, and athletic tendency with surges of catecholamines in routine sports activities and during sleep. Some batches/vials of mRNA may have more concentrated LNP-mRNA complexes or cDNA contaminants as suggested by Schmeling et al, who found that ~4.2% of vials are responsible for >70% of serious adverse events47. The lipid nanoparticles loaded with mRNA are known to systemically circulate for 28 days or more, thus there are many cycles of coronary flow and cardiac uptake of the LNP-mRNA complex12, 48. These data indicate that the mRNA sequences are long-lasting and durable within pericytes, cardiomyocytes, and other cell lines, providing the genetic instructions for the continuous production of Spike protein which is expressed on cell surfaces and in the interstitial space, inciting an auto-immune reaction. According to Mansanguan, 57% of cases may be asymptomatic18. Among those with symptoms, greater than 90% are hospitalized with clinical and diagnostic features including chest pain, heart failure, ECG changes, positive troponin levels, and cardiac MRI imaging demonstrating patchy late gadolinium enhancement49. If undetected, risks include sudden cardiac death during sports or sleep where approximately 65% cannot be resuscitated40 and are classified as sudden adult death syndrome (SADS). In such cases, it is important to document the brand, number of doses, inoculation dates, lot numbers and, as our data indicate, procurement of an autopsy.
Myocarditis may be a significant contributor to overall deaths observed after COVID-19 vaccination. The studies analyzed in this review are consistent with multiple studies that show excess mortality after vaccination which may have occurred due to myocarditis that was not detected before sudden death. Pantazatos and Seligmann reported that all-cause mortality increased in most age groups up to five weeks after vaccination resulting in 146,000 to 187,000 vaccine-associated deaths in the United States by August 202150. Skidmore elucidated that 278,000 Americans may have died from the COVID-19 vaccine by December 202151. These findings were corroborated by Aarstad and Kvitastein, who reported that, among European countries, a higher COVID-19 vaccine uptake in 2021 was associated with increased all-cause mortality in the first nine months of 2022 after accounting for alternative explanations52. Excess deaths not caused by COVID-19 have been identified worldwide after the mass COVID-19 vaccination programs began53-58, indicating the presence of a novel detrimental exposure among populations. Pantazatos extrapolated that VAERS reports are underreported by a factor of 2050. When this factor is applied to the June 16th, 2023, VAERS death report count of 35,48722, the number of deaths in the United States and other countries that use VAERS becomes 709,740. Should this sizeable number of fatalities be confirmed, the COVID-19 vaccines would constitute the largest biological safety disaster in human history.
Our paper has all the limitations of small sample sizes derived from assembling case reports or series. These include selection bias of cases for autopsy, publication bias against disclosing more cases from academic medical centers and medical examiners for fear of reprisal, and unknown confounders such as undetected cardiotropic pathogens, alcohol abuse, and drug abuse, which are all threats to validity.
In summary, we identified a series of myocarditis-related deaths following COVID-19 vaccination, confirmed with autopsies, to provide the medical community with a more comprehensive understanding of fatal COVID-19 vaccine-induced myocarditis. The temporal relationship, internal and external consistency seen among cases in this review with known COVID-19 vaccine-induced myocarditis, its pathobiological mechanisms and related excess death, complemented with autopsy confirmation, independent adjudication, and application of the Bradford Hill criteria to the overall epidemiology of vaccine myocarditis, suggests there is a high likelihood of a causal link between COVID-19 vaccines and death from suspected myocarditis in cases where sudden, unexpected death has occurred in a vaccinated person. If the COVID-19 vaccines remain on the market for public use, urgent investigation is required for the purpose of risk stratification and mitigation in order to reduce the population occurrence of fatal COVID-19 vaccine-induced myocarditis.
Funding
None.
Acknowledgements
None.
Disclosures
RH, WM, PM are either affiliated with or receive salary support (modest) or equity (modest) in The Wellness Company which had no role in the study.
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 25 February 2023).
- Kuter, B.J.; Offit, P.A.; Poland, G.A. The development of COVID-19 vaccines in the United States: Why and how so fast? Vaccine 2021, 39, 2491–2495. [Google Scholar] [CrossRef] [PubMed]
- Graña, C.; Ghosn, L.; Evrenoglou, T.; Jarde, A.; Minozzi, S.; Bergman, H.; Buckley, B.S.; Probyn, K.; Villanueva, G.; Henschke, N.; et al. Efficacy and safety of COVID-19 vaccines. Cochrane Database Syst. Rev. 2022, 2023, CD015477. [Google Scholar] [CrossRef]
- Trougakos, I.P.; Terpos, E.; Alexopoulos, H.; Politou, M.; Paraskevis, D.; Scorilas, A.; Kastritis, E.; Andreakos, E.; Dimopoulos, M.A. Adverse effects of COVID-19 mRNA vaccines: the spike hypothesis. Trends Mol. Med. 2022, 28, 542–554. [Google Scholar] [CrossRef] [PubMed]
- Seneff, S.; Nigh, G.; Kyriakopoulos, A.M.; McCullough, P.A. Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs. Food Chem. Toxicol. 2022, 164, 113008–113008. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Singh, A.B. S2 subunit of SARS-nCoV-2 interacts with tumor suppressor protein p53 and BRCA: an in silico study. Transl. Oncol. 2020, 13, 100814. [Google Scholar] [CrossRef]
- Uversky, V.N.; Redwan, E.M.; Makis, W.; Rubio-Casillas, A. IgG4 Antibodies Induced by Repeated Vaccination May Generate Immune Tolerance to the SARS-CoV-2 Spike Protein. Vaccines 2023, 11, 991. [Google Scholar] [CrossRef]
- Theoharides, T.C. Could SARS-CoV-2 Spike Protein Be Responsible for Long-COVID Syndrome? Mol. Neurobiol. 2022, 59, 1850–1861. [Google Scholar] [CrossRef]
- Theoharides, T.C.; Conti, P. Be aware of SARS-CoV-2 spike protein: There is more than meets the eye. J Biol Regul Homeost Agents 2021, 35, 833–838. [Google Scholar] [CrossRef]
- Bozkurt, B.; Kamat, I.; Hotez, P.J. Myocarditis With COVID-19 mRNA Vaccines. Circulation 2021, 144, 471–484. [Google Scholar] [CrossRef]
- Yonker, L.M.; Swank, Z.; Bartsch, Y.C.; Burns, M.D.; Kane, A.; Boribong, B.P.; Davis, J.P.; Loiselle, M.; Novak, T.; Senussi, Y.; et al. Circulating Spike Protein Detected in Post–COVID-19 mRNA Vaccine Myocarditis. Circulation 2023, 147, 867–876. [Google Scholar] [CrossRef]
- Castruita, J.A.S.; Vest Schneider, U.; Mollerup, S.; Leineweber, T.D.; Weis, N.; Bukh, J.; Pedersen, M.S.; Westh, H. SARS-CoV -2 spike mRNA vaccine sequences circulate in blood up to 28 days after COVID -19 vaccination. APMIS 2023, 131, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Avolio, E.; Carrabba, M.; Milligan, R.; Williamson, M.K.; Beltrami, A.P.; Gupta, K.; Elvers, K.T.; Gamez, M.; Foster, R.R.; Gillespie, K.; et al. The SARS-CoV-2 Spike protein disrupts human cardiac pericytes function through CD147 receptor-mediated signalling: a potential non-infective mechanism of COVID-19 microvascular disease. Clin. Sci. 2021, 135, 2667–2689. [Google Scholar] [CrossRef]
- Coronavirus (COVID-19) Update: June 25, 2021 [Internet]. U.S. Food and Drug Administration. 2021. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-june-25-2021.
- Rose, Jessica, McCullough, Peter. Determinants of COVID-19 Vaccine-Induced Myocarditis Requiring Hospitalization 2022. [CrossRef]
- Nonclinical Evaluation of BNT162b2 [mRNA] COVID-19 vaccine (COMIRNATY) [Internet]. Australian Government Department of Health - Therapeutic Goods Administration; 2021 [cited 2023 May 23]. Available online: https://www.tga.gov.au/sites/default/files/foi-2389-06.pdf.
- Baumeier, C.; Aleshcheva, G.; Harms, D.; Gross, U.; Hamm, C.; Assmus, B.; Westenfeld, R.; Kelm, M.; Rammos, S.; Wenzel, P.; et al. Intramyocardial Inflammation after COVID-19 Vaccination: An Endomyocardial Biopsy-Proven Case Series. Int. J. Mol. Sci. 2022, 23, 6940. [Google Scholar] [CrossRef] [PubMed]
- Mansanguan, S.; Charunwatthana, P.; Piyaphanee, W.; Dechkhajorn, W.; Poolcharoen, A.; Mansanguan, C. Cardiovascular Manifestation of the BNT162b2 mRNA COVID-19 Vaccine in Adolescents. Trop. Med. Infect. Dis. 2022, 7, 196. [Google Scholar] [CrossRef] [PubMed]
- Le Pessec G. Significant incidence of myocarditis after 3rd dose of anti-COVID 19 messenger RNA vaccine [Internet]. 2022 [cited 2023 Jul 6]. Available online: https://www.cardio-online.fr/Actualites/A-la-une/ESC-2022/Incidence-non-negligeable-myocardites-apres-3-dose-vaccin-ARN messager-anti-COVID-19.
- Myocarditis and pericarditis after COVID-19 vaccination: clinical management guidance for healthcare professionals Jan 9, 2023. Available online: https://www.gov.uk/government/publications/myocarditis-and-pericarditis-after-covid-19-vaccination/myocarditis-and-pericarditis-after-covid-19-vaccination-guidance-for-healthcare-professionals.
- Guidance on Myocarditis and Pericarditis after COVID-19 vaccines Sept 23, 2022. Available online: https://www.health.gov.au/sites/default/files/documents/2022/11/covid-19-vaccination-guidance-on-myocarditis-and-pericarditis-after-covid-19-vaccines.pdf.
- Vaccine Adverse Event Reporting System (VAERS) [online]. Available online: https://vaers.hhs.gov.
- Meissner CH. Vaccine Adverse Event Reporting System plays vital role in safety [Internet]. 2016 [cited 2023 Jul 6]. Available online: https://publications.aap.org/aapnews/news/14631.
- Scarl, R.; Parkinson, B.; Arole, V.; Hardy, T.; Allenby, P. The hospital autopsy: the importance in keeping autopsy an option. Autops. Case Rep. 2022, 12, e2021333. [Google Scholar] [CrossRef]
- Nushida, H.; Ito, A.; Kurata, H.; Umemoto, H.; Tokunaga, I.; Iseki, H.; Nishimura, A. A case of fatal multi-organ inflammation following COVID-19 vaccination. Leg. Med. 2023, 63, 102244–102244. [Google Scholar] [CrossRef] [PubMed]
- Mörz, M. A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19. Vaccines 2022, 10, 1651. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Kondo, T.; Yamasaki, G.; Sugimoto, M.; Asano, M.; Ueno, Y.; Nagasaki, Y. An autopsy case report of aortic dissection complicated with histiolymphocytic pericarditis and aortic inflammation after mRNA COVID-19 vaccination. Leg. Med. 2022, 59, 102154. [Google Scholar] [CrossRef]
- Satomi, H.; Katano, H.; Kanno, H.; Kobayashi, M.; Ohkuma, Y.; Hashidume, N.; Usui, T.; Tsukada, S.; Ito, I. An autopsy case of fulminant myocarditis after severe acute respiratory syndrome coronavirus 2 vaccine inoculation. Pathol. Int. 2022, 72, 519–524. [Google Scholar] [CrossRef]
- Suzuki, H.; Ro, A.; Takada, A.; Saito, K.; Hayashi, K. Autopsy findings of post-COVID-19 vaccination deaths in Tokyo Metropolis, Japan, 2021. Leg. Med. 2022, 59, 102134. [Google Scholar] [CrossRef]
- Gill, J.R.; Tashjian, R.; Duncanson, E. Autopsy Histopathologic Cardiac Findings in 2 Adolescents Following the Second COVID-19 Vaccine Dose. Arch. Pathol. Lab. Med. 2022, 146, 925–929. [Google Scholar] [CrossRef] [PubMed]
- Ameratunga, R.; Woon, S.-T.; Sheppard, M.N.; Garland, J.; Ondruschka, B.; Wong, C.X.; Stewart, R.A.H.; Tatley, M.; Stables, S.R.; Tse, R.D. First Identified Case of Fatal Fulminant Necrotizing Eosinophilic Myocarditis Following the Initial Dose of the Pfizer-BioNTech mRNA COVID-19 Vaccine (BNT162b2, Comirnaty): an Extremely Rare Idiosyncratic Hypersensitivity Reaction. J. Clin. Immunol. 2022, 42, 441–447. [Google Scholar] [CrossRef]
- Choi, S.; Lee, S.; Seo, J.-W.; Kim, M.-J.; Jeon, Y.H.; Park, J.H.; Lee, J.K.; Yeo, N.S. Myocarditis-induced Sudden Death after BNT162b2 mRNA COVID-19 Vaccination in Korea: Case Report Focusing on Histopathological Findings. J. Korean Med Sci. 2021, 36, e286. [Google Scholar] [CrossRef] [PubMed]
- Schneider, J.; Sottmann, L.; Greinacher, A.; Hagen, M.; Kasper, H.-U.; Kuhnen, C.; Schlepper, S.; Schmidt, S.; Schulz, R.; Thiele, T.; et al. Postmortem investigation of fatalities following vaccination with COVID-19 vaccines. Int. J. Leg. Med. 2021, 135, 2335–2345. [Google Scholar] [CrossRef] [PubMed]
- Verma, A.K.; Lavine, K.J.; Lin, C.-Y. Myocarditis after Covid-19 mRNA Vaccination. New Engl. J. Med. 2021, 385, 1332–1334. [Google Scholar] [CrossRef] [PubMed]
- Schwab, C.; Domke, L.M.; Hartmann, L.; Stenzinger, A.; Longerich, T.; Schirmacher, P. Autopsy-based histopathological characterization of myocarditis after anti-SARS-CoV-2-vaccination. Clin Res Cardiol. 2022, 112, 431–440. [Google Scholar] [CrossRef]
- Hoshino, N.; Yanase, M.; Ichiyasu, T.; Kuwahara, K.; Kawai, H.; Muramatsu, T.; Ishii, H.; Tsukamoto, T.; Morimoto, S.-I.; Izawa, H. An autopsy case report of fulminant myocarditis: Following mRNA COVID-19 vaccination. J. Cardiol. Cases 2022, 26, 391–394. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.-M.; Liu, X.; Yang, C.-T.; Qi, Q.; Shi, W.-B.; Li, Y.-M.; Zuo, M.; Wang, S.-J.; Bi, H.-T.; Ma, R.-F.; et al. Case report: Myocarditis following COVID-19 protein subunit vaccination. Front. Cardiovasc. Med. 2022, 9, 970045. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.Y.; Kim, K.H.; Lee, N.; Cho, S.H.; Kim, S.Y.; Kim, E.K.; Park, J.-H.; Choi, E.-Y.; Choi, J.-O.; Park, H.; et al. COVID-19 vaccination-related myocarditis: a Korean nationwide study. Eur. Hear. J. 2023, 44, 2234–2243. [Google Scholar] [CrossRef]
- Fedak, K.M.; Bernal, A.; Capshaw, Z.A.; Gross, S. Applying the Bradford Hill criteria in the 21st century: how data integration has changed causal inference in molecular epidemiology. Emerg. Themes Epidemiology 2015, 12, 14. [Google Scholar] [CrossRef]
- Polykretis, P.; McCullough, P.A. Rational harm-benefit assessments by age group are required for continued COVID-19 vaccination. Scand. J. Immunol. 2022, 98, e13242. [Google Scholar] [CrossRef]
- Cadegiani, F.A. Catecholamines Are the Key Trigger of COVID-19 mRNA Vaccine-Induced Myocarditis: A Compelling Hypothesis Supported by Epidemiological, Anatomopathological, Molecular, and Physiological Findings. Cureus 2022, 14, e27883. [Google Scholar] [CrossRef] [PubMed]
- Dodt, C.; Breckling, U.; Derad, I.; Fehm, H.L.; Born, J. Plasma Epinephrine and Norepinephrine Concentrations of Healthy Humans Associated With Nighttime Sleep and Morning Arousal. Hypertension 1997, 30, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Wangu, Z.; Swartz, H.; Doherty, M. Multisystem inflammatory syndrome in children (MIS-C) possibly secondary to COVID-19 mRNA vaccination. BMJ Case Rep. 2022, 15, e247176. [Google Scholar] [CrossRef] [PubMed]
- Ehikhametalor, K.; Deans-Minott, J.; Duncan, J.P. Multisystem Inflammatory Syndrome in Adults (MIS-A) After COVID-19 Infection and Recent Vaccination with Recombinant Adenoviral Vector Encoding the Spike Protein Antigen of SARS-CoV-2 (ChAdOx1 nCoV-19, Vaxzevria). J. Intensiv. Care Med. 2022, 38, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Ittiwut, C.; Mahasirimongkol, S.; Srisont, S.; Ittiwut, R.; Chockjamsai, M.; Durongkadech, P.; Sawaengdee, W.; Khunphon, A.; Larpadisorn, K.; Wattanapokayakit, S.; et al. Genetic basis of sudden death after COVID-19 vaccination in Thailand. Hear. Rhythm. 2022, 19, 1874–1879. [Google Scholar] [CrossRef] [PubMed]
- Engler, R.J.M.; Nelson, M.R.; Jr. , L.C.C.; Spooner, C.; Hemann, B.A.; Gibbs, B.T.; Atwood, J.E.; Howard, R.S.; Chang, A.S.; Cruser, D.L.; et al. A Prospective Study of the Incidence of Myocarditis/Pericarditis and New Onset Cardiac Symptoms following Smallpox and Influenza Vaccination. PLOS ONE 2015, 10, e0118283. [Google Scholar] [CrossRef]
- Schmeling, M.; Manniche, V.; Hansen, P.R. Batch-dependent safety of the BNT162b2 mRNA COVID-19 vaccine. Eur. J. Clin. Investig. 2023, 53, e13998. [Google Scholar] [CrossRef] [PubMed]
- Ogata, A.F.; Cheng, C.-A.; Desjardins, M.; Senussi, Y.; Sherman, A.C.; Powell, M.; Novack, L.; Von, S.; Li, X.; Baden, L.R.; et al. Circulating Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients. Clin. Infect. Dis. 2021, 74, 715–718. [Google Scholar] [CrossRef]
- Keshavarz, P.; Yazdanpanah, F.; Emad, M.; Hajati, A.; Nejati, S.F.; Sadabad, F.E.; Azrumelashvili, T.; Mizandari, M.; Raman, S.S. Myocarditis Following COVID-19 Vaccination: Cardiac Imaging Findings in 118 Studies. Tomography 2022, 8, 1959–1973. [Google Scholar] [CrossRef]
- Pantazatos, S.; Seligmann, H. COVID vaccination and age-stratified all-cause mortality risk. Research Gate 2021. [CrossRef]
- Skidmore, M. The role of social circle COVID-19 illness and vaccination experiences in COVID-19 vaccination decisions: an online survey of the United States population. BMC Infect. Dis. 2023, 23, 51. [Google Scholar] [CrossRef]
- Aarstad, J.; Kvitastein, O.A. Is there a Link between the 2021 COVID-19 Vaccination Uptake in Europe and 2022 Excess All-Cause Mortality? org 2023, 2023020350. [Google Scholar] [CrossRef]
- Beesoon, S.; Bakal, J.A.; Youngson, E.; Williams, K.P.; Berzins, S.A.; Brindle, M.E.; Joffe, A.M. Excess deaths during the COVID-19 pandemic in Alberta, Canada. IJID Reg. 2022, 5, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Todd, M.; Scheeres, A. Excess Mortality From Non–COVID-19 Causes During the COVID-19 Pandemic in Philadelphia, Pennsylvania, 2020–2021. Am J Public Health 2022, 112, 1800–1803. [Google Scholar] [CrossRef] [PubMed]
- Karlinsky, A.; Kobak, D. The World Mortality Dataset: Tracking excess mortality across countries during the COVID-19 pandemic. medRxiv 2021. [CrossRef]
- Wang, H.; Paulson, K.R.; A Pease, S.; Watson, S.; Comfort, H.; Zheng, P.; Aravkin, A.Y.; Bisignano, C.; Barber, R.M.; Alam, T.; et al. Estimating excess mortality due to the COVID-19 pandemic: a systematic analysis of COVID-19-related mortality, 2020–21. Lancet 2022, 399, 1513–1536. [Google Scholar] [CrossRef]
- Msemburi, W.; Karlinsky, A.; Knutson, V.; Aleshin-Guendel, S.; Chatterji, S.; Wakefield, J. The WHO estimates of excess mortality associated with the COVID-19 pandemic. Nature 2022, 613, 130–137. [Google Scholar] [CrossRef]
- Shang, W.; Wang, Y.; Yuan, J.; Guo, Z.; Liu, J.; Liu, M. Global Excess Mortality during COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 1702. [Google Scholar] [CrossRef]
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram detailing the study selection process.
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram detailing the study selection process.
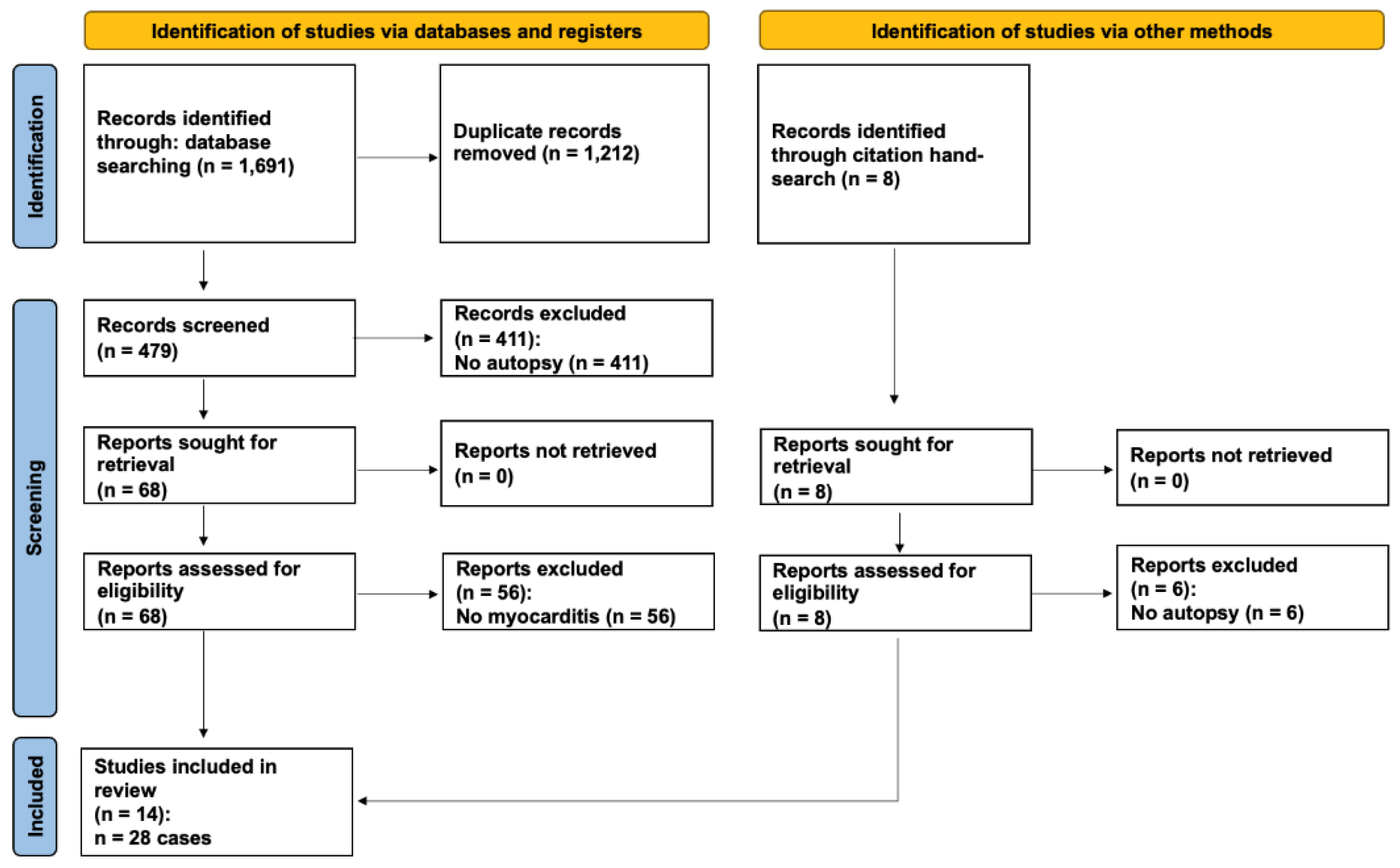
Figure 2.
Proportion of Cases by Affected Organ System.
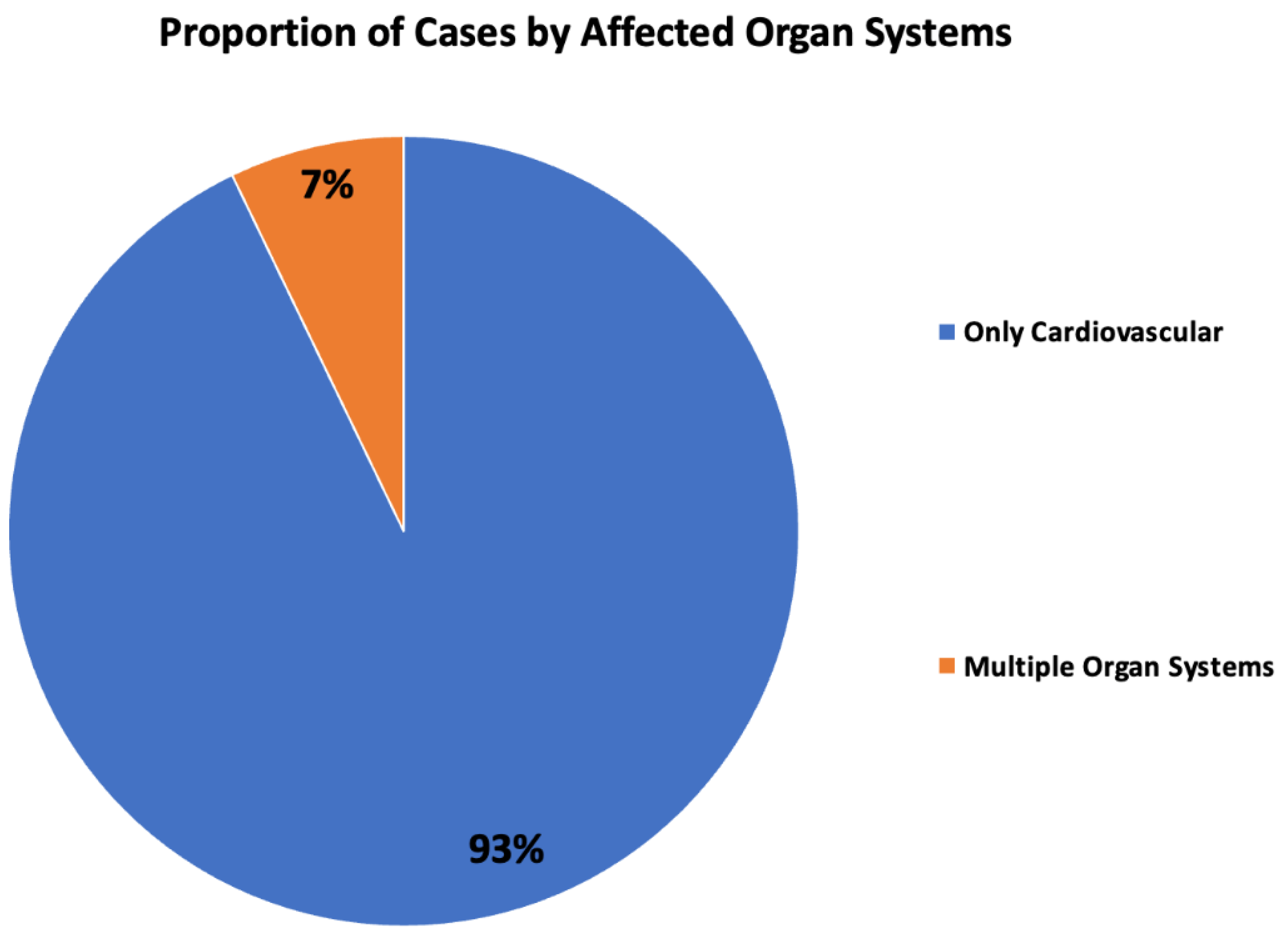
Figure 3.
Distribution of Time from Last Vaccine Administration to Death.
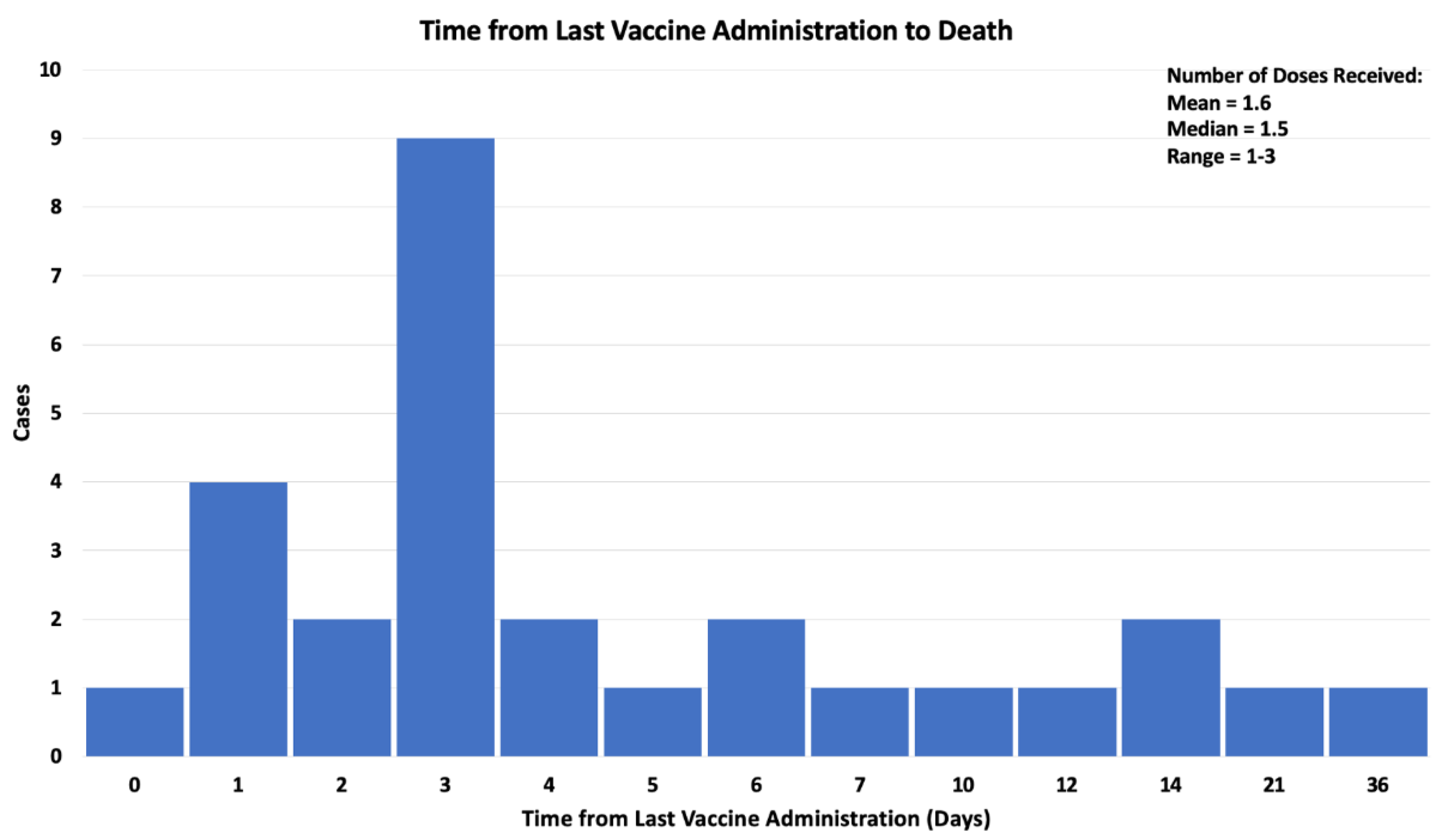
Figure 4.
Evidence of SARS-CoV-2 spike protein in cardiac tissue after COVID-19 vaccination. (A–C) Representative immunohistochemical stainings of SARS-CoV-2 spike protein in EMBs from patients diagnosed with DCMi after receiving Comirnaty® (panel A and B, patients 5 and 10) or Vaxzevria® (panel C, patient 13). (D) SARS-CoV-2-positive cardiac tissue served as positive control. Magnification 400. Scale bars 20 m. *Figure from Baumeier et al.17
Figure 4.
Evidence of SARS-CoV-2 spike protein in cardiac tissue after COVID-19 vaccination. (A–C) Representative immunohistochemical stainings of SARS-CoV-2 spike protein in EMBs from patients diagnosed with DCMi after receiving Comirnaty® (panel A and B, patients 5 and 10) or Vaxzevria® (panel C, patient 13). (D) SARS-CoV-2-positive cardiac tissue served as positive control. Magnification 400. Scale bars 20 m. *Figure from Baumeier et al.17
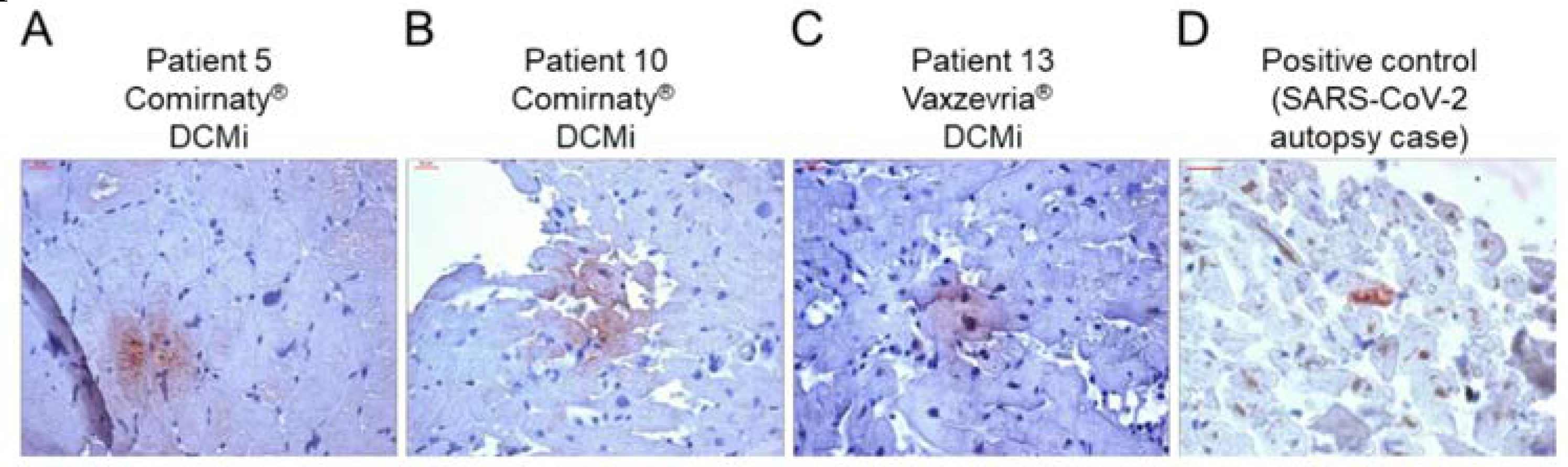
Figure 5.
Inflammatory cardiomyopathy in response to COVID-19 vaccination is dominated by CD4+ T cells. (A–C) Representative immunohistochemical stainings of CD4+ and CD8+ T cells in endomyocardial biopsies from patients diagnosed for inflammatory cardiomyopathy (DCMi) after receiving Comirnaty® (panel A and B, patients 6 and 10) or Vaxzevria® (panel C, patient 13) vaccines, respectively. Magnification 400. Scale bars 20 m. *Figure from Baumeier et al.17
Figure 5.
Inflammatory cardiomyopathy in response to COVID-19 vaccination is dominated by CD4+ T cells. (A–C) Representative immunohistochemical stainings of CD4+ and CD8+ T cells in endomyocardial biopsies from patients diagnosed for inflammatory cardiomyopathy (DCMi) after receiving Comirnaty® (panel A and B, patients 6 and 10) or Vaxzevria® (panel C, patient 13) vaccines, respectively. Magnification 400. Scale bars 20 m. *Figure from Baumeier et al.17
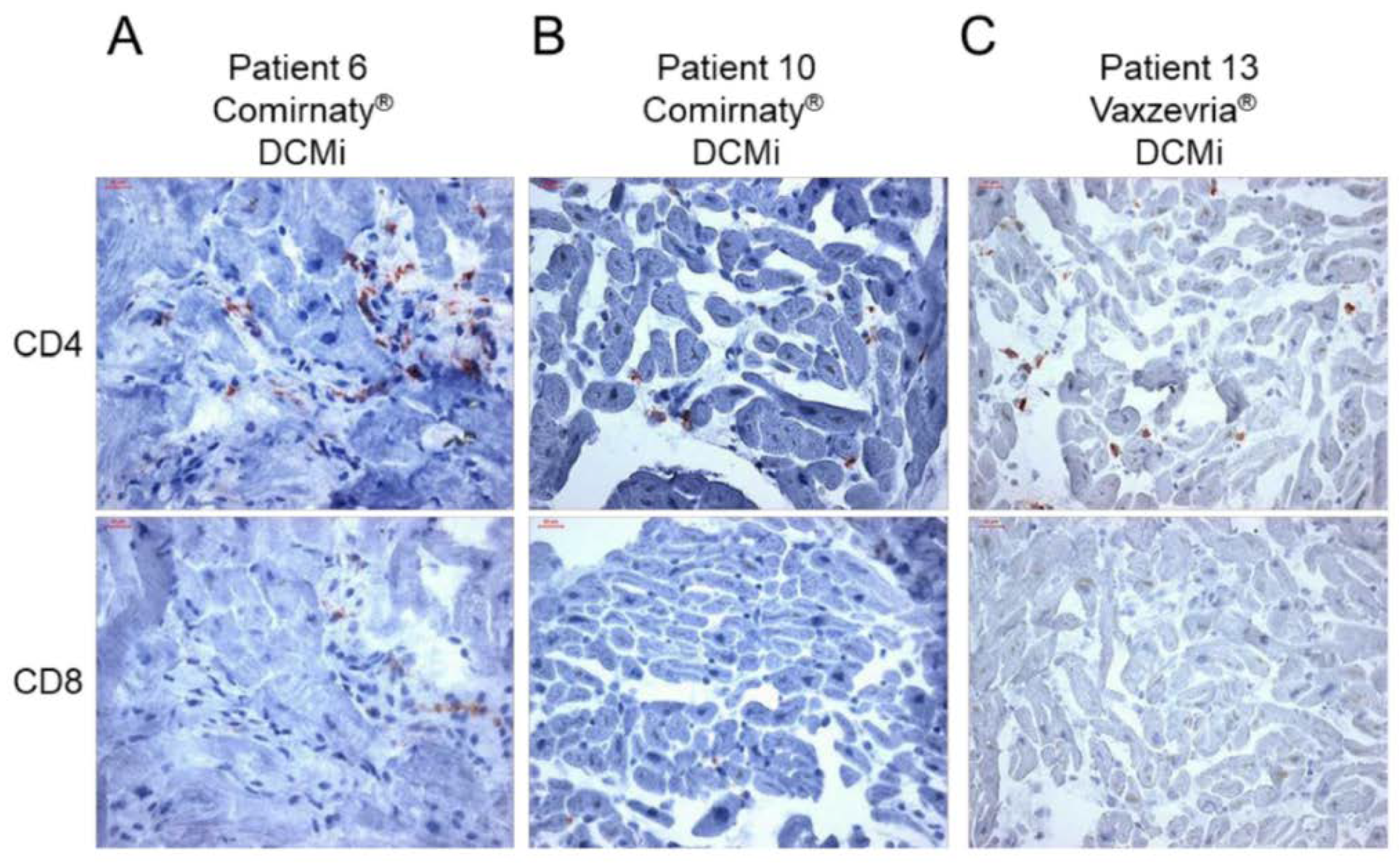
Figure 6.
COVID-19 Vaccine-induced myocarditis characteristics.
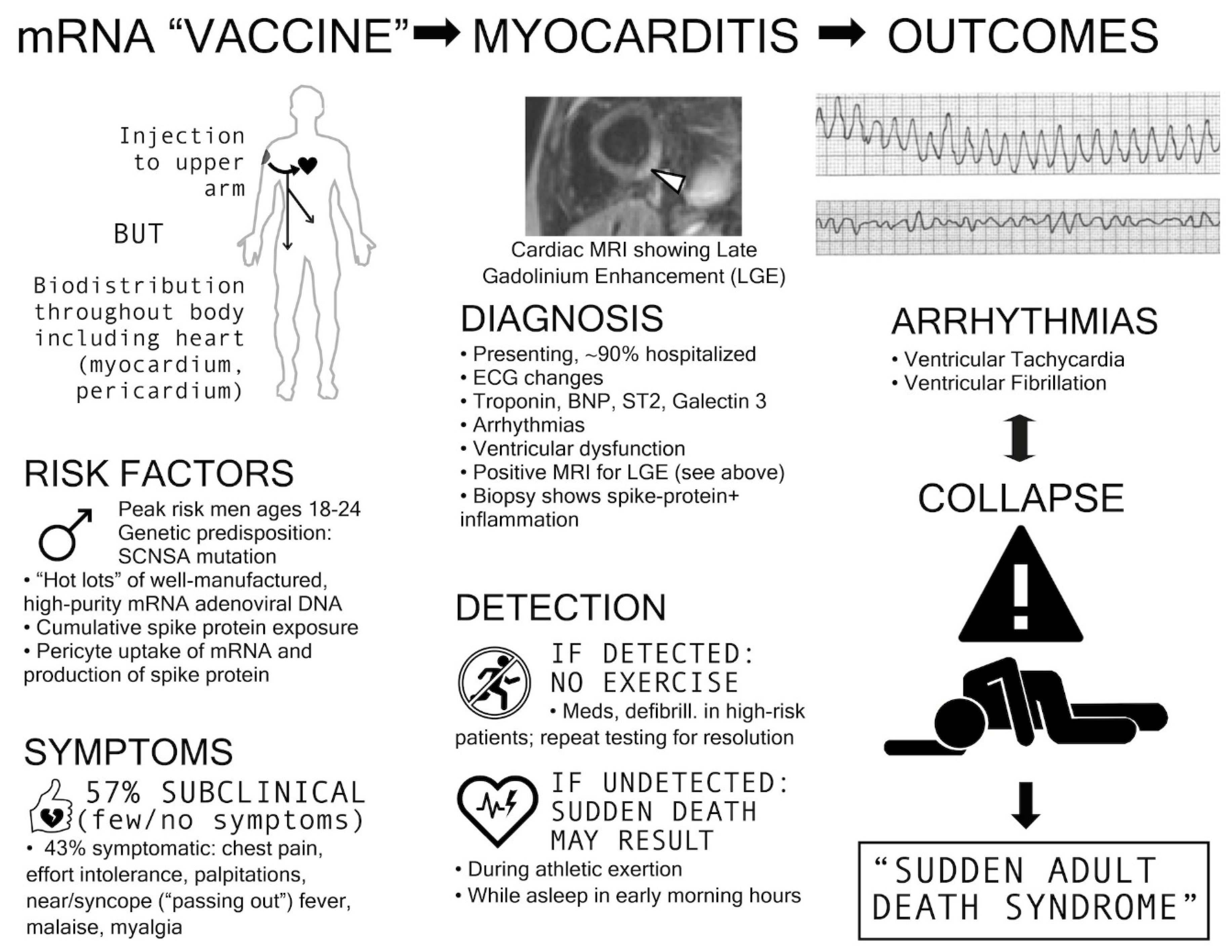

Table 1.
Case information from all included studies on autopsy-confirmed COVID-19 vaccination related myocarditis.
Table 1.
Case information from all included studies on autopsy-confirmed COVID-19 vaccination related myocarditis.
| AUthor | Case | AGE | Sex | Vaccine | Dose* | disease | period ** | Post-Mortem Findings |
|---|---|---|---|---|---|---|---|---|
| Nushida, 2023 (Japan) [25] | 1 | 14 | F | Pfizer | 3 | MIS, Myopericarditis | 2 days | Congestive edema of the lungs, T-cell lymphocytic and macrophage infiltration in the lungs, pericardium, and myocardium of the left atria and left ventricle, liver, kidneys, stomach, duodenum, bladder, and diaphragm.The presence of foci centered on the atria and breathlessness are the findings that led to the diagnosis that the cause of death was vaccine-related myopericarditis, which led to severe arrhythmias and progressive heart failure. |
| Morz, 2022 (germany) [26] | 1 | 76 | M | Pfizer | 2 | encephalitis, myocarditis | 21 days | Signs of aspiration pneumonia and systemic arteriosclerosis were evident. Brain examination uncovered acute vasculitis (predominantly lymphocytic) as well as multifocal necrotizing encephalitis of unknown etiology with pronounced inflammation including glial and lymphocytic reaction. In the heart, signs of chronic cardiomyopathy as well as mild acute lympho-histiocytic myocarditis and vasculitis were present. Only spike protein but no nucleocapsid protein could be detected within the foci of inflammation in both the brain and the heart. Also, mild acute splenitis, gastric mucosal bleeding, liver lipofuscinosis, and mild active nephritis were found. |
| Takahashi, 2022 (Japan)[27] | 1 | ‘90s’ | M | Pfizer | 3 | Pericarditis | 14 days | Dissection of the ascending aorta and pericardial hemotamponade. The heart showed a white villous surface, and the pericardium was fibrously thick. Microscopic examination revealed pericarditis with predominantly macrophage and lymphocyte infiltration. |
| Satomi, 2022 (japan) [28] | 1 | 61 | F | Pfizer | 1 | Myocarditis | 10 days | The heart showed moderate dilatation of both ventricles, and the myocardium showed an uneven color change and decreased elasticity. Histologically, severe myocarditis with extensive myocytolysis was observed. The myocarditis showed severe inflammatory cell infiltration with T-lymphocyte and macrophage predominance, and vast nuclear dust accompanying neutrophilic infiltration was observed. In the bone marrow and lymph nodes, hemophagocytosis was observed. SARS-CoV-2 nucleic acids were not detected using multivirus real-time PCR system. |
| Suzuki, 2021 (japan) [29] | 1 | 91 | M | Moderna | 1 | Ischemic heart disease, myocarditis | 6 days | Old myocardial infarction in the post lateral wall, severe coronary artery sclerosis, leukocyte and lymphocyte infiltration in the left anterior wall, diabetic nephropathy, aortic sclerosis. |
| 2 | 24 | M | Moderna | 2 | Myocarditis | 3 days | Scattered necrosis and fibrosis of cardiomyocytes with a perivascular pattern of inflammatory cell infiltration (consisting of predominantly lymphocytes). | |
| 3 | 39 | M | Moderna | 2 | Myocarditis | 3 days | Scattered inflammatory cell infiltration (consisting of predominantly monocytes) in the interstitial space of cardiomyocytes/around the coronary arteries, interstitial edema, eosinophilic and wavy change of cardiomyocytes, Lung edema, coronary sclerosis. | |
| Gill, 2022 (usa) [30] | 1 | ‘teenage’ | M | Pfizer | 2 | Myocarditis | 3 days | No molecular evidence of SARS-CoV-2 infection. Global myocardial injury with areas of coagulative myocytolysis and contractions bands, with a perivascular pattern of inflammation consisting of mainly neutrophils and histocytes, scant lymphocytes, and occasional eosinophils. No acute or organizing thrombi were detected. Pattern of injury is consistent with stress cardiomyopathy. |
| 2 | ‘teenage’ | M | Pfizer | 2 | Myocarditis | 4 days | No molecular evidence of SARS-CoV-2 infection. As with the previous case, global myocardial injury was found but with more widespread transmural ischemic changes and more interstitial inflammation. Subepicardial distribution of injury was not seen. No acute or organizing thrombi were detected. | |
| Ameratunga, 2022 (new zealand) [31] | 1 | 57 | F | Pfizer | 1 | Myocarditis | 3 days | Left pleural mass originating from the mediastinum was found. Multifocal inflammatory cell infiltration in the myocardium and areas of eosinophil-rich inflammatory aggregates with myocyte necrosis were found. An abundant eosinophilic infiltrate with myocyte necrosis was observed. Antibodies to SARS-CoV-2 were not detected. |
| Choi, 2021 (korea) [32] | 1 | 22 | M | Pfizer | 1 | Myocarditis | 5 days | Histological examination of the heart showed isolated atrial myocarditis, with neutrophil and histiocyte predominance. Immunohistochemical C4d staining showed scattered single-cell necrosis of myocytes which was not accompanied by inflammatory infiltrates. Extensive contraction band necrosis was seen in the atria and ventricles. There was no evidence of microthrombosis or infection in the heart and other organs. |
| Schneider, 2021 (germany) [33] | 1 | 65 | M | Pfizer | 1 | Myocarditis | 1 day | Severe coronary sclerosis, massive cardiac hypertrophy, myocardial infarction scars, myocarditis, anaphylaxis diagnostics negative. |
| Verma, 2021 (usa) [34] | 1 | 42 | M | Moderna | 2 | Myocarditis | ~14 days | Autopsy revealed biventricular myocarditis. An inflammatory infiltrate admixed with macrophages, T-cells, eosinophils, and B cells was also observed. |
| Schwab, 2023 (germany) [35] | 1 | 46 | M | Pfizer | 1 | Myocarditis | 0 days | Histological examination showed inflammatory infiltration of the myocardium. The infiltrate was focal and interstitial. It was predominantly detected in sections taken from the right ventricular wall and interventricular septum. The histological and immunohistochemical characterization revealed that the inflammatory infiltrate was predominantly composed of lymphocytes. Micro focal myocyte injury was demonstrable. Lacked pre-existing, clinically relevant heart disease. |
| 2 | 50 | F | Moderna | 1 | Myocarditis | 1 day | Histological examination showed inflammatory infiltration of the myocardium. The infiltrate was focal and interstitial. It was predominantly detected in sections taken from the right ventricular wall and interventricular septum. The histological and immunohistochemical characterization revealed that the inflammatory infiltrate was predominantly composed of lymphocytes. Micro focal myocyte injury was demonstrable. A n inflammatory infiltration of the epicardium and the subepicardial fat tissue was concomitantly found. L acked pre-existing, clinically relevant heart disease. | |
| 3 | 62 | F | Pfizer | 1 | Myocarditis | 7 days | Histological examination showed inflammatory infiltration of the myocardium. The infiltrate was focal and interstitial. It was predominantly detected in sections taken from the right ventricular wall and interventricular septum. The histological and immunohistochemical characterization revealed that the inflammatory infiltrate was predominantly composed of lymphocytes. Micro focal myocyte injury was demonstrable. An inflammatory infiltration of the epicardium and the subepicardial fat tissue was concomitantly found. Lacked pre-existing, clinically relevant heart disease. | |
| 4 | 55 | M | Pfizer | 2 | Myocarditis | 4 days | Histological examination showed inflammatory infiltration of the myocardium. The infiltrate was focal and interstitial. It was predominantly detected in sections taken from the right ventricular wall and interventricular septum. The histological and immunohistochemical characterization revealed that the inflammatory infiltrate was predominantly composed of lymphocytes. A n inflammatory infiltration of the epicardium and the subepicardial fat tissue was concomitantly found. L acked pre-existing, clinically relevant heart disease. | |
| 5 | 75 | F | Pfizer | 1 | Myocarditis | 1 days | Histological examination showed inflammatory infiltration of the myocardium. The infiltrate was focal and interstitial. It was predominantly detected in sections taken from the right ventricular wall and interventricular septum. The histological and immunohistochemical characterization revealed that the inflammatory infiltrate was predominantly composed of lymphocytes. An inflammatory infiltration of the epicardium and the subepicardial fat tissue was concomitantly found. Lacked pre-existing, clinically relevant heart disease. Analysis for potential infectious agents causing a myocarditis revealed low viral copy numbers of human herpes virus 6. | |
| Hoshino, 2022 (japan) [36] | 1 | 27 | M | Moderna | 1 | Myocarditis | 36 days | An autopsy revealed asymmetric left ventricular hypertrophy, thickening of the right ventricular wall (550 g; LV wall, 11–16 mm; RV wall, 5–7 mm), myxomatous degeneration of the posterior leaflet of the mitral valve, and hypertrophy of the posteromedial papillary muscle. Microscopic findings revealed that cardiac myocytolysis and widespread fibrosis were observed, and significant mixed inflammatory infiltration (T cells, macrophages, and eosinophils) was observed in the left ventricular free wall and the anterior potion of the ventricular septum. |
| DONG, 2022 (china) [37] | 1 | 34 | F | Zifivax | 1 | Myocarditis | 12 days | Autopsy showed severe interstitial myocarditis, including multiple patchy infiltrations of lymphocytes and monocytes in the myocardium of the left and right ventricular walls associated with myocyte degeneration and necrosis. |
| Cho, 2023 (korea) [38] | 1 | 22 | M | Pfizer | 1 | SCD from Myocarditis | 6 days | Diffuse inflammatory infiltration, with neutrophil and histiocyte predominance in both atria and near AV node and SA node. Free of inflammatory infiltrates in ventricular myocardium. |
| 2 | 30 | F | Pfizer | 1 | SCD from Myocarditis | 3 days | Diffuse inflammatory cell infiltration, myocardial fiber disarray, interstitial fibrosis, and localized necrosis of myocyte. | |
| 3 | 45 | M | Pfizer | 2 | SCD from Myocarditis | 3 days | Localized infiltration of neutrophils, lymphocytes, histocyte, and a few eosinophils was noted. A small number of cardiomyocyte necrosis were also seen. | |
| 4 | 25 | M | Pfizer | 2 | SCD from Myocarditis | 3 days | Autopsy revealed myocarditis. | |
| 5 | 45 | M | Pfizer | 2 | SCD from Myocarditis | 3 days | Interstitial infiltration of various inflammatory cells including lymphocyte, neutrophil, eosinophil, and focal necrosis suggesting the diagnosis of myocarditis. | |
| 6 | 36 | F | Moderna | 1 | SCD from Myocarditis | 2 days | Neutrophil, eosinophil, and histiocyte infiltration in the myocardium suggesting acute myocarditis. | |
| 7 | 33 | M | Moderna | 2 | SCD from Myocarditis | 1 day | Multiple focal infiltrations of acute inflammatory cells and chronic inflammatory cells in the myocardium. | |
| 8 | 33 | M | Moderna | 2 | SCD from Myocarditis | 3 days | Various inflammatory cells such as neutrophils, eosinophils, lymphocytes, macrophages, and cardiomyocyte necrosis in the myocardial interstitium and epicardium suggested myocarditis. |
*Dose = Total number of vaccine doses received. **Period = Days from most recent vaccine administration to death. ~ = Inferred Period (Estimated period using all available information).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



