
Submitted:
18 July 2023
Posted:
19 July 2023
You are already at the latest version
Abstract
This study aimed to evaluate the diagnostic and prognostic roles of GATA3 immunohistochemistry in urothelial carcinoma (UC) through a meta-analysis. We investigated GATA3 immunohistochemical expression rates and performed a subgroup analysis based on tumor site, study location, and histological subtypes. The overall survival rates of patients with GATA3-positive and negative UC were compared. The estimated GATA3 expression rate was 0.748 (95% confidence interval [CI]: 0.704–0.787). GATA3 expression rates in the urinary bladder and urinary tract were 0.775 (95% CI: 0.727–0.818) and 0.614 (95% CI: 0.426–0.774), respectively. The GATA expression rates of noninvasive and invasive UCs were 0.965 (95% CI: 0.938–0.980) and 0.644 (95% CI: 0.581–0.702), respectively. In invasive UCs, there was a significant difference in GATA3 expression between non-muscular invasion and muscular invasion subgroups (0.937, 95% CI: 0.883–0.967 vs. 0.753, 95% CI: 0.645–0.836). GATA3 expression was the highest in the microcytic subtype among the histologic subtypes (0.952, 95% CI: 0.724–0.993). There was a significant correlation between GATA3 expression and better prognosis (hazard ratio: 0.402, 95% CI: 0.311–0.521). Taken together, GATA3 expression significantly correlated with low-stage and better prognosis in UC. GATA3 expression is highly variable across histological subtypes and it is careful interpreting GATA3 expression.
Keywords:
urothelial carcinoma
; GATA3
; immunohistochemistry
; overall survival
; meta-analysis
1. Introduction
Urothelial carcinoma (UC) is a common malignancy of the urinary tract that affects approximately 430,000 people and 165,000 deaths worldwide annually [1]. UC is classified into non-invasive and invasive and can be sub-staged according to the presence of muscle invasion. The prognosis differs depending on the extent of UC, which in turn influences treatment decisions. Muscle-invasive UC is an aggressive and potentially life-threatening form of cancer. Thus, the identification of reliable biomarkers for invasive UC can help in the early detection and risk stratification of patients, leading to personalized treatment strategies and improved clinical outcomes [2,3]. GATA-binding protein 3 (GATA3) has emerged as a promising biomarker for UC. GATA3 is a transcription factor that regulates cell differentiation and proliferation and is commonly expressed in urothelial and breast epithelial cells [4,5]. GATA3 plays a role in regulating luminal differentiation in the breast epithelium [6,7]. In addition, GATA3 may be involved in the development or maintenance of various tissues, such as the skin, hair shafts [8,9], and endothelial cells of great vessels [10]. In breast cancer, GATA3 is associated with tumor differentiation and recurrence [11,12]. Many studies have suggested that GATA3 plays an important role as a tumor suppressor in the prevention of urothelial cancer progression and metastasis [13,14,15,16]. However, detailed GATA3 expression in the histological subtypes of UC remains poorly understood. Additionally, the prognostic value of GATA3 expression remains unclear [13,14,15,16]. It may be difficult to obtain biopsied tissues of sufficient depth, which may limit the assessment of invasiveness. If GATA3 immunohistochemical (IHC) expression differs between tumor grades, it could be useful for biopsy specimens. This study aimed to evaluate the diagnostic and prognostic roles of GATA3 IHC in UC using a meta-analysis. GATA3 IHC expression rates were investigated and a meta-analysis was performed. In addition, a subgroup analysis was performed based on the tumor site, study location, tumor stage, and histologic subtypes. The overall survival rates of patients with GATA3-positive and-negative UC were compared.
2. Materials and Methods
2.1. Literature search and selection criteria
Relevant articles were obtained by searching the PubMed and MEDLINE databases through April 15, 2023. The search was performed using ‘urothelial carcinoma,’ ‘GATA3,’ and ‘immunohistochemistry’ as search terms. The titles and abstracts of all the returned articles were screened for exclusion. Review articles were screened to identify the eligible studies. English-language studies addressing GATA3 expression in human UC were included. Case reports and review articles were excluded.
2.2. Data extraction
Thirty-nine articles were included and reviewed in this meta-analysis [15,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54]. From eligible studies, we collected the following information: first author’s name, publication date, study location, number of patients analyzed, tumor site, and expression rates of GATA3. For the quantitative aggregation of survival results, the correlation between GATA3 expression and the survival rate was analyzed according to the hazard ratio (HR). Because the survival data were in the form of graphical representations of survival distributions, survival rates were extracted at specified times to reconstruct the HR estimate and its variance under the assumption that patients were censored at a constant rate during the time intervals [55]. The published survival curves were independently evaluated by two authors to reduce variability. The HRs were then combined into an overall HR using Peto’s method [56]. Disagreements were resolved by consensus.
2.3. Statistical analyses
To perform the meta-analysis, all data were analyzed using the Comprehensive Meta-Analysis software package (Biostat, Englewood, NJ, USA). The immunohistochemical expression of GATA3 in UC was investigated in eligible studies. In addition, subgroup analyses based on tumor location, study location, tumor stage, and histological subtype were performed. Correlation between GATA3 expression and overall survival was also evaluated. As the eligible studies used various antibodies and evaluation criteria for various populations, the random-effects model was more suitable than the fixed-effects model. Heterogeneity and sensitivity analyses were conducted to assess the heterogeneity of eligible studies and the impact of each study on the combined effect. Heterogeneity between studies was checked using Q and I2 statistics, and P-values were calculated. Begg’s funnel plot and Egger’s test were used to assess publication bias. Statistical significance was set when P < 0.05.
3. Results
3.1. Selection and characteristics of studies
Database search was performed using the above-mentioned keywords. One hundred fifty-nine reports were identified in the database search. Articles were selected by screening the titles and abstracts. During the screening and full-text review, 38 articles were excluded because of insufficient information. In addition, 57 articles were excluded because they focused on other diseases. The remaining 25 articles were excluded because they were non-original (n = 22), used animals or cell lines (n = 2), or were not written in English (n = 1). Finally, 39 articles were included in the meta-analysis (Figure 1 and Table 1).
3.2. Meta-analysis for GATA3 IHC expression in urothelial carcinoma
The GATA3 IHC expression rate was 0.748 (95%: CI 0.704–0.787) in all cases (Table 2). The expression rates of UC in the urinary bladder and urinary tract were 0.775 (95% CI: 0.727–0.818) and 0.614 (95% CI: 0.426–0.774), respectively. The GATA3 expression rate in UC was significantly higher in the urinary bladder than in the urinary tract (p = 0.001 in the meta-regression test). In the subgroup analysis based on study location, GATA3 expression rates were 0.741 (95% CI: 0.627–0.829), 0.748 (95% CI: 0.590–0.859), 0.775 (95% CI: 0.723–0.819), and 0.909 (95% CI: 0.561–0.987) in the American, Asian, European, and Oceania subgroups, respectively. The GATA3 expression rates in noninvasive and invasive UC were 0.965 (95% CI: 0.938–0.980) and 0.644 (95% CI: 0.581–0.702), respectively (Table 3). The GATA3 expression rate in carcinoma in situ was 0.956 (95% CI 0.878-0.985). GATA3 expression was significantly lower in non-muscular-invasive UC than in muscular-invasive UC (0.753, 95% CI: 0.645–0.836 vs. 0.937, 95% CI: 0.883–0.967; p = 0.041 in the meta-regression test). In a subgroup analysis based on histological subtypes, subtypes with more than 90% were clear cell features and microcytic and pleomorphic adenocarcinoma subtypes. We evaluated the prognostic implications of GATA3 expression in UC. UC patients with GATA3 expression had better overall survival than those without GATA3 expression (hazard ratio 0.402, 95% CI: 0.311–0.521; Figure 2).
4. Discussion
GATA3 is expressed in various tissues and cancers [57]. GATA3 is involved in the differentiation of various cells, including the urothelium, breast epithelium, and T lymphocytes [57]. Although several studies have reported the diagnostic and prognostic roles of malignant tumors, the results vary significantly according to tumor type. Additionally, there have been several studies on GATA3 expression in UC; however, individual studies may be insufficient to assess the significance of GATA3 expression in UC. Therefore, it is necessary to obtain and analyze integrated information through systematic reviews, including meta-analyses. To the best of our knowledge, this is the first meta-analysis to elucidate the clinicopathological implications of GATA3 IHC markers in UC.
GATA3 promotes cell proliferation and differentiation in many tissues and cell types [58,59,60]. GATA3 is also involved in malignant progression [60,61]. Some cancers showed GATA3 overexpression, such as breast and colorectal carcinoma [60,61]. In breast cancer, GATA3 induces tumor differentiation in undifferentiated carcinomas [62]. Carcinomas with high GATA3 expression include basal cell carcinoma, breast cancer, germ cell tumors, and low-grade UC (> 90 percent [57]. Conversely, carcinomas with low GATA3 expression are positive in less than 10% of cases, including gastric and colorectal adenocarcinoma, endometrial adenocarcinoma, hepatocellular carcinoma, cholangiocarcinoma, prostatic adenocarcinoma, and thyroid carcinoma [57]. GATA3 is expressed in primary UC but also in metastatic UC. Naik et al. reported GATA3 expression in all metastatic UC [41]. Efforts have been made to classify UC based on GATA3 expression levels. UC can be divided into luminal and basal subtypes, with GATA3 expression in the luminal subtype and CK5/6 expression in the basal subtype. Budina reported that the luminal subtype with GATA3 expression is the predominant phenotype in T1 cancers [25]. In contrast, the basal subtype with no GATA3 expression accounts for only 5% of all T1 cancers [25]. However, there were no significant differences in sex, ethnicity, grade, recurrence, or survival between the luminal and non-luminal phenotypes [25]. Seiler et al. reported that the classification of luminal and basal tumors affects the efficacy of cisplatin-based neoadjuvant chemotherapy in muscle-invasive UC [21]. Therefore, GATA3 IHC is useful for differentiating UC phenotypes and for the differential diagnosis between UC and other malignant tumors.
We investigated the expression of GATA3 under various conditions and performed a meta-analysis. GATA3 expression was significantly lower in the urinary tract than in the urinary bladder (0.614; 95% CI: 0.426–0.774 vs. 0.775; 95% CI: 0.727–0.818). GATA3 expression in UC can differ significantly depending on the invasion status. Interestingly, even in invasive UC, GATA3 expression significantly differed depending on the presence or absence of muscle invasion. There was no significant difference between noninvasive and non-muscular-invasive UC (0.965, 95% CI: 0.938–0.980 vs. 0.937, 95% CI: 0.883–0.967). Based on this result, the presence of muscle invasion is an important factor in differentiating GATA3 expression, rather than simply the presence of invasion. Although GATA3 expression is grouped with Ta and T1 and T2 and above, the GATA3 expression rate is also significantly higher in muscle-invasive UC, with a rate of 0.753 (95% CI: 0.645–0.836). Mohammed et al. reported that high GATA3 expression is associated with significantly larger tumor size in UC [14]. In our study, the lymph node metastasis rate was not significantly different between GATA3-positive and negative UCs (0.375, 95% CI: 0.282–0.478 vs. 0.340, 95% CI: 0.239–0.459; data not shown). Our results suggest that the GATA3 expression is associated with a better prognosis, which may be related to lower staging.
Due to its location, UC may need to be differentiated from kidney or prostate cancer in some cases. There may also be high-grade UC that needs to be differentiated from metastatic squamous cell carcinoma of the uterine cervix and anal canal. As GATA3 expression may vary among histological subtypes, its use in differentiating from other tumors may have limitations. A previous report showed that among renal cell carcinomas, chromophobe had 51% GATA3 expression, and the remaining subtypes had 2% expression [57]. In addition, prostatic adenocarcinoma was positive for GATA3 in 2% of the cases. [57]. In the kidney, except for renal cell carcinoma and chromophobe, there is a low rate of GATA3 positivity, which may be helpful for differentiation.
We investigated GATA3 expression in the different histological subtypes of UC. Among various histological subtypes, conventional UC is the most common. In our meta-analysis, the subtypes of UC with GATA3 expression (0.644) in the overall invasive UCs were adenocarcinoma, adenoid differentiation, lymphoepithelioma-like, sarcomatoid, small cell neuroendocrine carcinoma, squamous cell carcinoma, squamous differentiation, signet ring cell carcinoma, and undifferentiated subtypes. Of these, adenocarcinoma, small-cell neuroendocrine carcinoma, and squamous cell carcinoma have GATA3 expression levels of less than 20%. In a subgroup analysis based on histological subtypes, subtypes with more than 90% were clear cell features and microcytic and pleomorphic adenocarcinoma subtypes. Different histological subtypes exhibited varying GATA3 expression levels. Subtypes with significant differences in GATA3 expression may be useful when differentiation is difficult in small tissues.
This study has several limitations. A total of 55 subsets were included in the invasive UC subgroup, and 19 subsets were included in the non-muscular and muscular invasive UC subgroups. As the remaining 36 subsets were not classified according to muscular invasion, the analysis was limited. In addition, there may be prognostic differences based on histological subtypes. However, a meta-analysis of the prognostic role of GATA3 within histological subgroups could not be performed because of insufficient information.
5. Conclusions
GATA3 expression is significantly higher in non-invasive and non-muscle-invasive UC than in muscle-invasive UC. In addition, GATA3 expression significantly correlated with improved overall survival in UC. GATA3 expression is highly variable across histologic subtypes. Furthermore, GATA3 IHC is useful for differentiating between UC subtypes and between low- and high-grade UCs.
Supplementary Materials
Not applicable.
Author Contributions
Conceptualization, D.Y. and J.-S.P.; methodology, J.-S.P.; software, J.-S.P.; data curation, D.Y. and N.-Y.K.; writing—original draft preparation, D.Y. and J.-S.P.; writing—review and editing, K.-W.M. and N.-Y.K.; All authors have read and agreed to the published version of the manuscript.
Funding
Not applicable.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Antoni, S.; Ferlay, J.; Soerjomataram, I.; Znaor, A.; Jemal, A.; Bray, F. Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur. Urol. 2017, 71, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.-R. Urothelial tumorigenesis: a tale of divergent pathways. Nat. Rev. Cancer 2005, 5, 713–725. [Google Scholar] [CrossRef]
- Knowles, M.A.; Hurst, C.D. Molecular biology of bladder cancer: new insights into pathogenesis and clinical diversity. Nat. Rev. Cancer 2014, 15, 25–41. [Google Scholar] [CrossRef] [PubMed]
- Labastie, M.-C.; Catala, M.; Gregoire, J.-M.; Peault, B. The GATA-3 gene is expressed during human kidney embryogenesis. Kidney Int. 1995, 47, 1597–1603. [Google Scholar] [CrossRef] [PubMed]
- Debacker, C.; Catala, M.; Labastie, M.-C. Embryonic expression of the human GATA-3 gene. Mech. Dev. 1999, 85, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Yagi, R.; Zhu, J.; Paul, W.E. An updated view on transcription factor GATA3-mediated regulation of Th1 and Th2 cell differentiation. Int. Immunol. 2011, 23, 415–420. [Google Scholar] [CrossRef]
- Oosterwegel, M.; Timmerman, J.; Leiden, J.; Clevers, H. Expression of GATA-3 During Lymphocyte Differentiation and Mouse Embryogenesis. Dev. Immunol. 1992, 3, 1–11. [Google Scholar] [CrossRef]
- Kaufman, C.K.; Zhou, P.; Pasolli, H.A.; Rendl, M.; Bolotin, D.; Lim, K.-C.; Dai, X.; Alegre, M.-L.; Fuchs, E. GATA-3: an unexpected regulator of cell lineage determination in skin. Genes Dev. 2003, 17, 2108–2122. [Google Scholar] [CrossRef]
- Sellheyer, K.; Krahl, D. Expression pattern of GATA-3 in embryonic and fetal human skin suggests a role in epidermal and follicular morphogenesis. J. Cutan. Pathol. 2010, 37, 357–361. [Google Scholar] [CrossRef]
- Song, H.; Suehiro, J.-I.; Kanki, Y.; Kawai, Y.; Inoue, K.; Daida, H.; Yano, K.; Ohhashi, T.; Oettgen, P.; Aird, W.C.; et al. Critical Role for GATA3 in Mediating Tie2 Expression and Function in Large Vessel Endothelial Cells. PEDIATRICS 2009, 284, 29109–29124. [Google Scholar] [CrossRef]
- Ordóñez, N.G. Value of GATA3 immunostaining in tumor diagnosis: a review. Adv Anat Pathol 2013, 20, 352–360. [Google Scholar] [CrossRef]
- Mehra, R.; Varambally, S.; Ding, L.; Shen, R.; Sabel, M.S.; Ghosh, D.; Chinnaiyan, A.M.; Kleer, C.G. Identification of GATA3 as a Breast Cancer Prognostic Marker by Global Gene Expression Meta-analysis. Cancer Res 2005, 65, 11259–11264. [Google Scholar] [CrossRef]
- Li, Y.; Ishiguro, H.; Kawahara, T.; Kashiwagi, E.; Izumi, K.; Miyamoto, H. Loss of GATA3 in bladder cancer promotes cell migration and invasion. Cancer Biol. Ther. 2014, 15, 428–435. [Google Scholar] [CrossRef]
- Mohammed, K.H.; Siddiqui, M.T.; Cohen, C. GATA3 immunohistochemical expression in invasive urothelial carcinoma. Urol. Oncol. Semin. Orig. Investig. 2016, 34, 432–e9. [Google Scholar] [CrossRef]
- Plage, H.; Samtleben, H.; Hofbauer, S.; Kornienko, K.; Weinberger, S.; Bruch, P.G.; Elezkurtaj, S.; Roßner, F.; Schallenberg, S.; Kluth, M.; et al. GATA3 expression loss is linked to stage progression but is unrelated to prognosis in muscle-invasive urothelial carcinoma of the bladder. Hum. Pathol. 2022, 130, 10–17. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, J.; Wang, Y.; Wang, S.; Zhang, Y.; Miao, Q.; Gao, F.; He, H. Expression status of GATA3 and mismatch repair proteins in upper tract urothelial carcinoma. Front. Med. 2019, 13, 730–740. [Google Scholar] [CrossRef]
- Agaimy, A.; Bertz, S.; Cheng, L.; Hes, O.; Junker, K.; Keck, B.; Lopez-Beltran, A.; Stöckle, M.; Wullich, B.; Hartmann, A. Loss of expression of the SWI/SNF complex is a frequent event in undifferentiated/dedifferentiated urothelial carcinoma of the urinary tract. Virchows Arch. 2016, 469, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Rana, C.; Agarwal, H.; Babu, S.; Kumar, M.; Singhai, A.; Shankhwar, S.N.; Singh, V.; Sinha, R.J. Diagnostic utility of GATA3 immunohistochemical expression in urothelial carcinoma. Indian J. Pathol. Microbiol. 2019, 62, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Barth, I.; Schneider, U.; Grimm, T.; Karl, A.; Horst, D.; Gaisa, N.T.; Knüchel, R.; Garczyk, S. Progression of urothelial carcinoma in situ of the urinary bladder: a switch from luminal to basal phenotype and related therapeutic implications. Virchows Arch. 2018, 472, 749–758. [Google Scholar] [CrossRef] [PubMed]
- Bertz, S.; Stöhr, R.; Gaisa, N.T.; Wullich, B.; Hartmann, A.; Agaimy, A. TERT promoter mutation analysis as a surrogate to morphology and immunohistochemistry in problematic spindle cell lesions of the urinary bladder. Histopathology 2020, 77, 949–962. [Google Scholar] [CrossRef]
- Bontoux, C.; Rialland, T.; Cussenot, O.; Compérat, E. A four-antibody immunohistochemical panel can distinguish clinico-pathological clusters of urothelial carcinoma and reveals high concordance between primary tumor and lymph node metastases. Virchows Arch. 2020, 478, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Borhan, W.M.; Cimino-Mathews, A.M.; Montgomery, E.A.; Epstein, J.I. Immunohistochemical Differentiation of Plasmacytoid Urothelial Carcinoma From Secondary Carcinoma Involvement of the Bladder. Am. J. Surg. Pathol. 2017, 41, 1570–1575. [Google Scholar] [CrossRef]
- Bruch, P.G.; Plage, H.; Hofbauer, S.; Kornienko, K.; Weinberger, S.; Roßner, F.; Schallenberg, S.; Kluth, M.; Lennartz, M.; Blessin, N.C.; et al. Cytokeratin 20 expression is linked to stage progression and to poor prognosis in advanced (pT4) urothelial carcinoma of the bladder. Exp. Mol. Pathol. 2023, 131, 104860. [Google Scholar] [CrossRef]
- Brunelli, M.; Tafuri, A.; Cima, L.; Cerruto, M.A.; Milella, M.; Zivi, A.; Buti, S.; Bersanelli, M.; Fornarini, G.; Vellone, V.G.; et al. MDM2 gene amplification as selection tool for innovative targeted approaches in PD-L1 positive or negative muscle-invasive urothelial bladder carcinoma. J. Clin. Pathol. 2020. [Google Scholar] [CrossRef]
- Budina, A.; Farahani, S.J.; Lal, P.; Nayak, A. Subcategorization of T1 Bladder Cancer on Biopsy and Transurethral Resection Specimens for Predicting Progression. Arch. Pathol. Lab. Med. 2021, 146, 1131–1139. [Google Scholar] [CrossRef]
- Chang, A.; Brimo, F.; Montgomery, E.A.; Epstein, J.I. Use of PAX8 and GATA3 in diagnosing sarcomatoid renal cell carcinoma and sarcomatoid urothelial carcinoma. Hum. Pathol. 2013, 44, 1563–1568. [Google Scholar] [CrossRef] [PubMed]
- Ellis, C.L.; Chang, A.G.; Cimino-Mathews, A.; Argani, P.; Youssef, R.F.; Kapur, P.; Montgomery, E.A.; Epstein, J.I. GATA-3 Immunohistochemistry in the Differential Diagnosis of Adenocarcinoma of the Urinary Bladder. Am. J. Surg. Pathol. 2013, 37, 1756–1760. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Roibon, N.; Albadine, R.; Sharma, R.; Faraj, S.F.; Illei, P.B.; Argani, P.; Ertoy, D.; Allaf, M.E.; Netto, G.J. The role of GATA binding protein 3 in the differential diagnosis of collecting duct and upper tract urothelial carcinomas. Hum. Pathol. 2013, 44, 2651–2657. [Google Scholar] [CrossRef]
- Gulmann, C.; Paner, G.P.; Parakh, R.S.; Hansel, D.E.; Shen, S.S.; Ro, J.Y.; Annaiah, C.; Lopez-Beltran, A.; Rao, P.; Arora, K.; et al. Immunohistochemical profile to distinguish urothelial from squamous differentiation in carcinomas of urothelial tract. Hum. Pathol. 2012, 44, 164–172. [Google Scholar] [CrossRef]
- Guo, C.C.; Bondaruk, J.; Yao, H.; Wang, Z.; Zhang, L.; Lee, S.; Lee, J.-G.; Cogdell, D.; Zhang, M.; Yang, G.; et al. Assessment of Luminal and Basal Phenotypes in Bladder Cancer. Sci. Rep. 2020, 10, 9743. [Google Scholar] [CrossRef]
- Haghayeghi, K.; Lu, S.; Matoso, A.; Schiff, S.F.; Mueller-Leonhard, C.; Amin, A. Association of current molecular subtypes in urothelial carcinoma with patterns of muscularis propria invasion. Virchows Arch. 2021, 479, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Inoue, S.; Mizushima, T.; Fujita, K.; Meliti, A.; Ide, H.; Yamaguchi, S.; Fushimi, H.; Netto, G.J.; Nonomura, N.; Miyamoto, H. GATA3 immunohistochemistry in urothelial carcinoma of the upper urinary tract as a urothelial marker and a prognosticator. Hum. Pathol. 2017, 64, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Jangir, H.; Nambirajan, A.; Seth, A.; Sahoo, R.K.; Dinda, A.K.; Nayak, B.; Kaushal, S. Prognostic stratification of muscle invasive urothelial carcinomas using limited immunohistochemical panel of Gata3 and cytokeratins 5/6, 14 and 20. Ann Diagn Pathol 2019, 43, 151397. [Google Scholar] [CrossRef]
- Kim, B.; Lee, C.; Kim, Y.A.; Moon, K.C. PD-L1 Expression in Muscle-Invasive Urinary Bladder Urothelial Carcinoma According to Basal/Squamous-Like Phenotype. Front. Oncol. 2020, 10, 527385. [Google Scholar] [CrossRef]
- Leite, K.R.M.; Borges, L.L.; Filho, L.R.; Chade, D.; Coelho, R.F.; Cordeiro, M.; Srougi, M.; Nahas, W.C. Histological Variants of Urothelial Carcinoma Predict No Response to Neoadjuvant Chemotherapy. Clin. Genitourin. Cancer 2021, 20, e1–e6. [Google Scholar] [CrossRef] [PubMed]
- Leivo, M.Z.; Elson, P.J.; Tacha, D.E.; Delahunt, B.; Hansel, D.E. A combination of p40, GATA-3 and uroplakin II shows utility in the diagnosis and prognosis of muscle-invasive urothelial carcinoma. Pathology 2016, 48, 543–549. [Google Scholar] [CrossRef]
- Liang, Y.; Heitzman, J.; Kamat, A.M.; Dinney, C.P.; Czerniak, B.; Guo, C.C. Differential expression of GATA-3 in urothelial carcinoma variants. Hum. Pathol. 2014, 45, 1466–1472. [Google Scholar] [CrossRef]
- Lin, X.; Zhu, B.; Villa, C.; Zhong, M.; Kundu, S.; Rohan, S.M.; Yang, X.J. The utility of p63, p40, and GATA-binding protein 3 immunohistochemistry in diagnosing micropapillary urothelial carcinoma. Hum. Pathol. 2014, 45, 1824–1829. [Google Scholar] [CrossRef]
- Liu, H.; Shi, J.; Wilkerson, M.L.; Lin, F. Immunohistochemical evaluation of GATA3 expression in tumors and normal tissues: a useful immunomarker for breast and urothelial carcinomas. Am J Clin Pathol 2012, 138, 57–64. [Google Scholar] [CrossRef]
- Beltran, A.L.; Montironi, R.; Cheng, L. Microcystic urothelial carcinoma: morphology, immunohistochemistry and clinical behaviour. Histopathology 2013, 64, 872–879. [Google Scholar] [CrossRef]
- Naik, M.; Rao, B.V.; Fonseca, D.; Murthy, S.S.; Giridhar, A.; Sharma, R.; Raju, K.; Rao, T.S.; Challa, S. GATA-3 Expression in all Grades and Different Variants of Primary and Metastatic Urothelial Carcinoma. Indian J. Surg. Oncol. 2020, 12, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Oh, W.J.; Chung, A.M.; Kim, J.S.; Han, J.H.; Hong, S.H.; Lee, J.Y.; Choi, Y.J. Differential Immunohistochemical Profiles for Distinguishing Prostate Carcinoma and Urothelial Carcinoma. J. Pathol. Transl. Med. 2016, 50, 345–354. [Google Scholar] [CrossRef]
- Olkhov-Mitsel, E.; Hodgson, A.; Liu, S.K.; Vesprini, D.; Xu, B.; Downes, M.R. Three-antibody classifier for muscle invasive urothelial carcinoma and its correlation with p53 expression. J. Clin. Pathol. 2021, 75, 766–771. [Google Scholar] [CrossRef] [PubMed]
- Paner, G.P.; Annaiah, C.; Gulmann, C.; Rao, P.; Ro, J.Y.; Hansel, D.E.; Shen, S.S.; Lopez-Beltran, A.; Aron, M.; Luthringer, D.J.; et al. Immunohistochemical evaluation of novel and traditional markers associated with urothelial differentiation in a spectrum of variants of urothelial carcinoma of the urinary bladder. Hum. Pathol. 2014, 45, 1473–1482. [Google Scholar] [CrossRef] [PubMed]
- Perrino, C.M.; Eble, J.; Kao, C.-S.; Whaley, R.D.; Cheng, L.; Idrees, M.; Hashemi-Sadraei, N.; Monn, M.F.; Kaimakliotis, H.Z.; Bandali, E.; et al. Plasmacytoid/diffuse urothelial carcinoma: a single-institution immunohistochemical and molecular study of 69 patients. Hum. Pathol. 2019, 90, 27–36. [Google Scholar] [CrossRef]
- Reiswich, V.; Schmidt, C.E.; Lennartz, M.; Höflmayer, D.; Hube-Magg, C.; Weidemann, S.; Fraune, C.; Büscheck, F.; Möller, K.; Bernreuther, C.; et al. GATA3 Expression in Human Tumors: A Tissue Microarray Study on 16,557 Tumors. Pathobiology 2023, 90, 219–232. [Google Scholar] [CrossRef]
- Samaratunga, H.; Delahunt, B.; Egevad, L.; Adamson, M.; Hussey, D.; Malone, G.; Hoyle, K.; Nathan, T.; Kerle, D.; Ferguson, P.; et al. Pleomorphic giant cell carcinoma of the urinary bladder: an extreme form of tumour de-differentiation. Histopathology 2015, 68, 533–540. [Google Scholar] [CrossRef]
- Sanfrancesco, J.; McKenney, J.K.; Leivo, M.Z.; Gupta, S.; Elson, P.; Hansel, D.E. Sarcomatoid Urothelial Carcinoma of the Bladder: Analysis of 28 Cases With Emphasis on Clinicopathologic Features and Markers of Epithelial-to-Mesenchymal Transition. Arch. Pathol. Lab. Med. 2016, 140, 543–551. [CrossRef]
- Tian, W.; Guner, G.; Miyamoto, H.; Cimino-Mathews, A.; Gonzalez-Roibon, N.; Argani, P.; Li, X.; Sharma, R.; Subhawong, A.P.; Rezaei, K.; et al. Utility of uroplakin II expression as a marker of urothelial carcinoma. Hum. Pathol. 2014, 46, 58–64. [Google Scholar] [CrossRef]
- Verduin, L.; Mentrikoski, M.J.; Heitz, C.T.; Wick, M.R. The Utility of GATA3 in the Diagnosis of Urothelial Carcinomas With Variant Morphologic Patterns. Appl. Immunohistochem. Mol. Morphol. 2016, 24, 509–513. [Google Scholar] [CrossRef]
- Wang, X.; Lopez-Beltran, A.; O Osunkoya, A.; Wang, M.; Zhang, S.; Davidson, D.D.; E Emerson, R.; Williamson, S.R.; Tan, P.-H.; Kaimakliotis, H.Z.; et al. TERT promoter mutation status in sarcomatoid urothelial carcinomas of the upper urinary tract. Futur. Oncol. 2017, 13, 705–714. [Google Scholar] [CrossRef] [PubMed]
- Weyerer, V.; Weisser, R.; A Moskalev, E.; Haller, F.; Stoehr, R.; Eckstein, M.; Zinnall, U.; Gaisa, N.T.; Compérat, E.; Perren, A.; et al. Distinct genetic alterations and luminal molecular subtype in nested variant of urothelial carcinoma. Histopathology 2019, 75, 865–875. [Google Scholar] [CrossRef]
- Zhao, L.; Antic, T.; Witten, D.; Paner, G.P.; Taxy, J.B.; Husain, A.; Gwin, K.; Mirza, M.K.; Lingen, M.W.; Tretiakova, M.S. Is GATA3 expression maintained in regional metastases? : a study of paired primary and metastatic urothelial carcinomas. Am J Surg Pathol 2013, 37, 1876–1881. [Google Scholar] [CrossRef] [PubMed]
- Zinnall, U.; Weyerer, V.; Compérat, E.; Camparo, P.; Gaisa, N.T.; Knuechel-Clarke. R.; Perren, A.; Lugli, A.; Toma, M.; Baretton, G.; Kristiansen, G.; Wirtz, R.M.; Cheng, L.; Wullich, B.; Stoehr, R.; Hartmann, A.; Bertz, S. Micropapillary urotheliall carcinoma: evaluation of HER2 status and immunohistochemical characterization of the molecular subtype. Hum Pathol 2018, 80, 55-64. [CrossRef]
- Parmar, M.K.; Torri, V.; Stewart, L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat Med 1998, 17, 2815–2834. [Google Scholar] [CrossRef]
- Peto, R. Experimental Survival Curves for Interval-Censored Data. J. R. Stat. Soc. Ser. C (Applied Stat. 1973, 22, 86. [Google Scholar] [CrossRef]
- Miettinen, M.; McCue, P.A.; Sarlomo-Rikala, M.; Rys, J.; Czapiewski, P.; Wazny, K.; Langfort, R.; Waloszczyk, P.; Biernat, W.; Lasota, J.; Wang, Z. GATA3: a multispecific but potentially useful marker in surgical pathology: a systematic analysis of 2500 epithelial and nonepithelialtumors. Am J Surg Pathol 2014, 38, 13–22. [Google Scholar] [CrossRef]
- Burch, J.B. Regulation of GATA gene expression during vertebrate development. Semin. Cell Dev. Biol. 2005, 16, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Asselin-Labat, M.-L.; Sutherland, K.D.; Barker, H.; Thomas, R.; Shackleton, M.; Forrest, N.C.; Hartley, L.; Robb, L.; Grosveld, F.G.; Van Der Wees, J.; et al. Gata-3 is an essential regulator of mammary-gland morphogenesis and luminal-cell differentiation. Nat. Cell Biol. 2007, 9, 201–209. [Google Scholar] [CrossRef]
- Davis, D.G.; Siddiqui, M.T.; Oprea-Ilies, G.; Stevens, K.; Osunkoya, A.O.; Cohen, C.; Li, X. (. GATA-3 and FOXA1 expression is useful to differentiate breast carcinoma from other carcinomas. Hum. Pathol. 2016, 47, 26–31. [Google Scholar] [CrossRef]
- Kouros-Mehr, H.; Bechis, S.K.; Slorach, E.M.; Littlepage, L.E.; Egeblad, M.; Ewald, A.J.; Pai, S.-Y.; Ho, I.-C.; Werb, Z. GATA-3 Links Tumor Differentiation and Dissemination in a Luminal Breast Cancer Model. Cancer Cell 2008, 13, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Chou, J.; Provot, S.; Werb, Z. GATA3 in development and cancer differentiation: cells GATA have it! J Cell Physiol 2010, 222, 42–49. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow chart of the searching strategy.
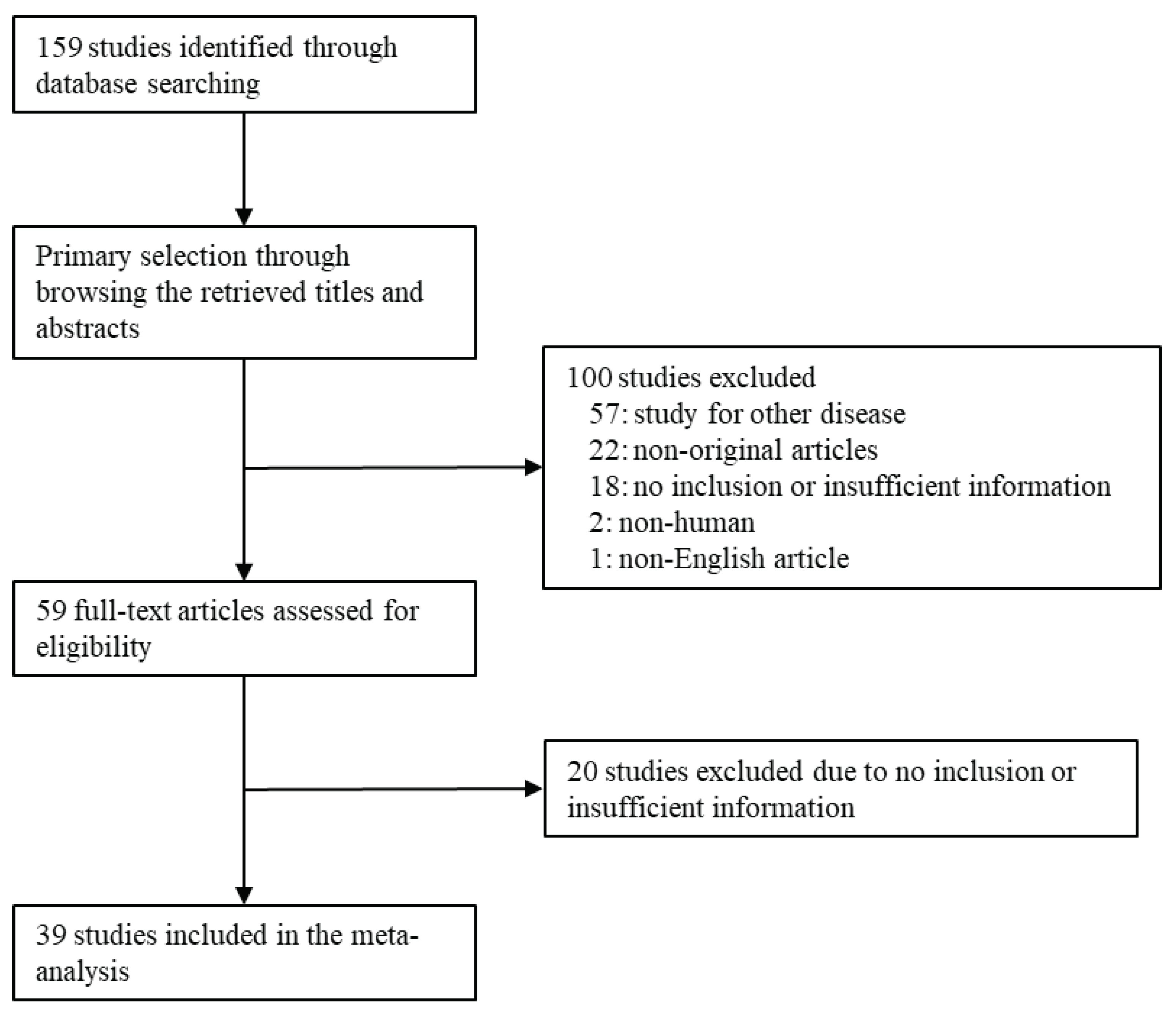
Figure 2.
Forest plot for the correlation between GATA3 expression and overall survival. ((a) Genetically unstable cases of luminal UC (b) Urothelial-like cases of luminal UC).
Figure 2.
Forest plot for the correlation between GATA3 expression and overall survival. ((a) Genetically unstable cases of luminal UC (b) Urothelial-like cases of luminal UC).
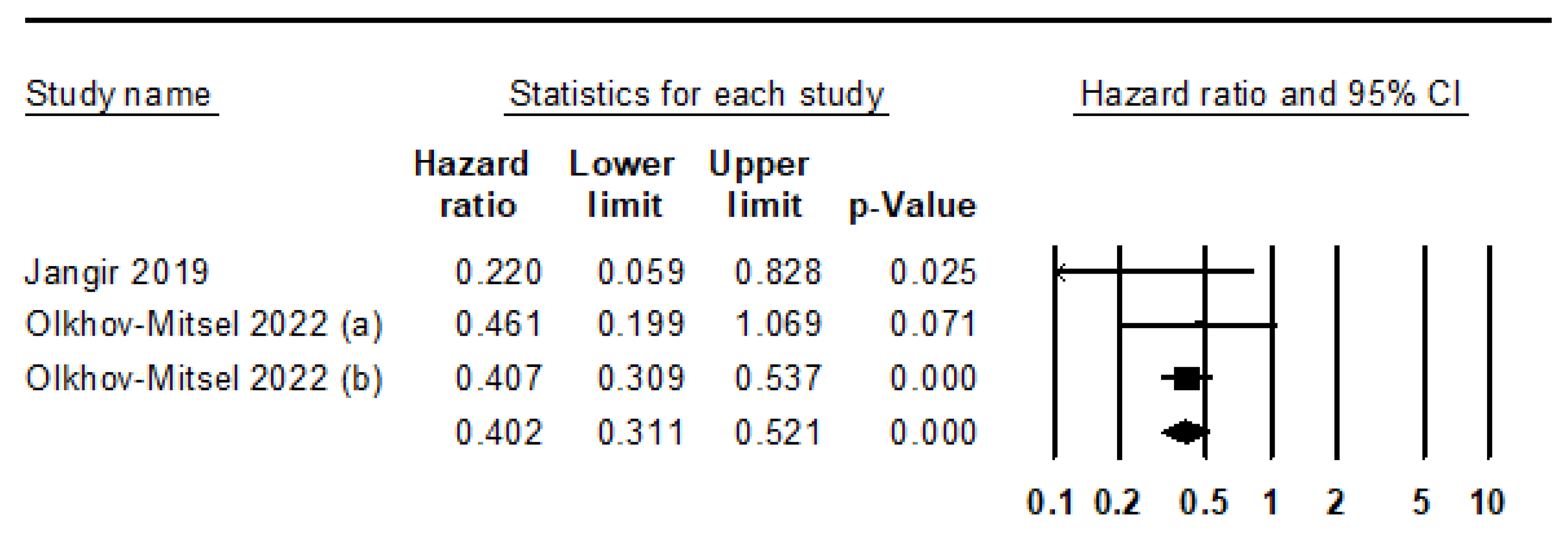

Table 1.
Main characteristics of the eligible studies.
| First Author | Location | Organ | No of patients |
First Author | Location | Organ | No of patients |
|
|---|---|---|---|---|---|---|---|---|
| Agaimy 2016 [17] | NA | UB, UT | 14 | Liang 2014 [37] | USA | UB | 127 | |
| Agarwal 2019 [18] | India | UB | 74 | Lin 2014 [38] | USA | UB | 98 | |
| Barth 2018 [19] | Germany | UB | 156 | Liu 2012 [39] | USA | UB | 72 | |
| Bertz 2020 [20] | Germany | UB | 18 | Lopez Beltran 2014 [40] | NA | UB | 20 | |
| Bontoux 2021 [21] | France | UB | 184 | Naik 2021 [41] | India | UB, UT | 122 | |
| Borhan 2017 [22] | USA | UB | 45 | Oh 2016 [42] | Korea | UB | 138 | |
| Bruch 2023 [23] | Germany | UB | 2406 | Olkhov-Mitsel 2022 [43] | Canada | UB | 243 | |
| Brunelli 2022 [24] | Italy | UB | 117 | Paner 2014 [44] | Various | UB | 111 | |
| Budina 2022 [25] | USA | UB | 67 | Perrino 2019 [45] | USA | UT | 26 | |
| Chang 2013 [26] | USA | UT | 56 | Plage 2022 [15] | Germany/Poland | UB | 2636 | |
| Ellis 2013 [27] | USA | UB | 49 | Reiswich 2023 [46] | Germany | NA | 1066 | |
| Gonzalez-Roibon 2013 [28] | USA | UT | 25 | Samaratunga 2016 [47] | New Zealand | UB | 11 | |
| Gulmann 2013 [29] | USA | UT | 85 | Sanfrancesco 2016 [48] | USA | UB | 26 | |
| Guo 2020 [30] | USA | UB | 72 | Tian 2015 [49] | USA | UB | 278 | |
| Haghayeghi 2021 [31] | USA | UB | 42 | Verduin 2016 [50] | USA | UB | 86 | |
| Inoue 2017 [32] | USA | UT | 48 | Wang 2017 [51] | USA | UT | 17 | |
| Jangir 2019 [33] | India | UB | 40 | Weyerer 2019 [52] | Germany | UB | 55 | |
| Kim 2020 [34] | Korea | UB | 166 | Zhao 2013 [53] | USA | UB | 69 | |
| Leite 2022 [35] | Brazil | UB | 25 | Zinnall 2018 [54] | Germany | UB | 91 | |
| Leivo 2016 [36] | USA | UB | 89 | |||||
| UB, urinary bladder; UT, urinary tract | ||||||||
Table 2.
Estimated GATA3 positive rates in urothelial carcinomas.
| Number of subsets |
Fixed effect [95% CI] |
Heterogeneity test [P-value] |
Random effect [95% CI] |
Egger’s test [P-value] |
|
|---|---|---|---|---|---|
| Overall | 38 | 0.726 [0.716, 0.735] | < 0.001 | 0.748 [0.704, 0.787] | 0.694 |
| Tumor site | |||||
| Urinary bladder* | 29 | 0.731 [0.720, 0.741] | < 0.001 | 0.775 [0.727, 0.818] | 0.395 |
| Urinary tract | 6 | 0.538 [0.477, 0.599] | < 0.001 | 0.614 [0.426, 0.774] | 0.391 |
| Study location | |||||
| America | 20 | 0.670 [0.641, 0.697] | < 0.001 | 0.741 [0.627, 0.829] | 0.215 |
| Asia | 4 | 0.707 [0.663, 0.747] | < 0.001 | 0.748 [0.590, 0.859] | 0.130 |
| Europe | 9 | 0.738 [0.727, 0.749] | < 0.001 | 0.775 [0.723, 0.819] | 0.416 |
| Oceania | 1 | 0.909 [0.561, 0.987] | < 0.001 | 0.909 [0.561, 0.987] | - |
| CI, Confidence interval. *, p = 0.011 in the meta-regression test between urinary bladder and urinary tract subgroups | |||||
Table 3.
Subgroup analysis of estimated GATA3 positive rates based on various subtypes of urothelial carcinomas.
Table 3.
Subgroup analysis of estimated GATA3 positive rates based on various subtypes of urothelial carcinomas.
| Number of subsets |
Fixed effect [95% CI] |
Heterogeneity test [P-value] |
Random effect [95% CI] |
Egger’s test [P-value] |
||
|---|---|---|---|---|---|---|
| Non-invasive UC* | 11 | 0.969 [0.958, 0.977] | 0.007 | 0.965 [0.938, 0.980] | 0.586 | |
| Carcinoma in situ | 2 | 0.961 [0.916, 0.982] | 0.250 | 0.956 [0.878, 0.985] | - | |
| Invasive UC | 55 | 0.626 [0.608, 0.643] | < 0.001 | 0.644 [0.581, 0.702] | 0.474 | |
| Non-muscular invasion# | 6 | 0.941 [0.902, 0.965] | 0.259 | 0.937 [0.883, 0.967] | 0.419 | |
| Muscular invasion | 13 | 0.720 [0.685, 0.752] | < 0.001 | 0.753 [0.645, 0.836] | 0.400 | |
| Histologic subtypes | ||||||
| Adenocarcinoma | 3 | 0.190 [0.093, 0.350] | 0.647 | 0.190 [0.093, 0.350] | 0.154 | |
| Clear cell | 1 | 0.929 [0.423, 0.996] | 1.000 | 0.929 [0.423, 0.996] | - | |
| Glandular differentiation | 2 | 0.474 [0.268, 0.689] | 0.809 | 0.474 [0.268, 0.689] | - | |
| Lymphoepithelioma-like | 1 | 0.300 [0.100, 0.624] | 1.000 | 0.300 [0.100, 0.624] | - | |
| Microcystic | 2 | 0.952 [0.724, 0.993] | 0.463 | 0.952 [0.724, 0.993] | - | |
| Micropapillary | 5 | 0.773 [0.697, 0.834] | < 0.001 | 0.862 [0.661, 0.952] | 0.264 | |
| Nested | 1 | 0.700 [0.376, 0.900] | 1.000 | 0.700 [0.376, 0.900] | - | |
| Plasmacytoid | 4 | 0.756 [0.637, 0.845] | 0.003 | 0.825 [0.517, 0.954] | 0.544 | |
| Pleomorphic giant cell | 1 | 0.909 [0.561, 0.987] | 1.000 | 0.909 [0.561, 0.987] | - | |
| Sarcomatoid | 8 | 0.385 [0.316, 0.459] | 0.003 | 0.407 [0.282, 0.545] | 0.370 | |
| Small cell neuroendocrine carcinoma | 4 | 0.132 [0.059, 0.267] | 0.310 | 0.125 [0.051, 0.276] | 0.231 | |
| Squamous cell carcinoma | 2 | 0.172 [0.069, 0.367] | 0.220 | 0.141 [0.031, 0.454] | - | |
| Squamous differentiation | 3 | 0.281 [0.159, 0.447] | 0.284 | 0.258 [0.122, 0.467] | 0.003 | |
| Signet ring cell carcinoma | 1 | 0.409 [0.228, 0.618] | 1.000 | 0.409 [0.228, 0.618] | - | |
| Undifferentiated | 1 | 0.643 [0.376, 0.843] | 1.000 | 0.643 [0.376, 0.843] | - | |
| CI, Confidence interval; UC, urothelial carcinoma. *, p < 0.001 in the meta-regression test between non-invasive and invasive urothelial carcinoma subgroups. #, p = 0.041 in the meta-regression test between non-muscular and muscular invasion subgroups | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



