
Submitted:
23 July 2023
Posted:
24 July 2023
You are already at the latest version
Abstract
Background: Community acquired Acinetobacter pneumonia (CAAP) typically presents with rapid progression to fulminant disease, and is complicated by high mortality. Australian epidemiological studies are few. Methods: We conducted a retrospective study on bacteraemic cases of CAAP over twenty years, (2000-2019) in North Queensland. Cases were selected on microbiologic, clinical, and radiographic parameters. Data on patient demographics were obtained, along with microbial, antibiotic, mortality, and climatic data. Results: 28 cases of CAAP were included. Nineteen (67.9%) were male, twenty-three (82.1%) were Indigenous Australians, and mean age was 45.9 years. Most presentations were of moderate to severe pneumonia, 25/28 (89.3%). 90% of cases had two or more risk factors. The strongest risk factors for CAAP were alcohol excess and tobacco use. No statistically significant difference in presenting severity, ICU admission or mortality was seen between dry and wet season disease. Dry season disease accounted for 35.7% of cases. Overall mortality was 28.6%. Early use of meropenem or gentamicin reduced mortality irrespective of presenting severity (mortality 17.6%) Non-targeted antibiotic therapy was associated with a non-significant difference in mortality of 44.4%. Conclusions: Early administration of targeted antibiotics can mitigate a high mortality rate. Choice of antibiotic therapy for community acquired pneumonia should be based upon severity, risk factors and clinical suspicion of CAAP rather than seasonality.
Keywords:
Acinetobacter
; pneumonia
; community-acquired
; tropical
; infection
; bacteramic
1. Introduction
Acinetobacter baumannii is an ubiquitous environmental bacterium [1,2,3,4]. Unlike nosocomial strains, community-acquired strains of A.baumannii manifest with a more fulminant course [1,5,6]. Consequently, the mortality rate can exceed 60% [1,2,7,8,9]. Community-acquired strains exhibit less anti-microbial resistance compared to nosocomial strains [10,11]. The Australian Therapeutic Guidelines, is the main reference for evidence-based antibiotic prescribing in Australia. The most recent revision of the Therapeutic Guidelines recommends the use of carbapenems, or single-dose gentamicin in moderate-to-severe pneumonia, where CAAP is suspected [12]. Where suspicion for CAAP is reliant on presentation in the tropical wet season in patients with typical risk factors [10,12,13,14]. Adherence to an earlier version of these antibiotic guidelines has shown to significantly reduce mortality rate, to as low as 11% [7].
2. Methods
2.1. Aims
- To evaluate risk factors associated with community-acquired Acinetobacter Pneumonia in a North Queensland cohort;
- To assess the efficacy of antibiotic therapy in community-acquired Acinetobacter pneumonia;
- To evaluate how antibiotic prescribing practices in CAAP influence mortality;
- To investigate mortality rate and factors associated with mortality.
2.2. Study Design
This study was conducted at Cairns Hospital, a main referral centre servicing the Far North Queensland region, encompassing 380,748 km2 and servicing a population of approximately 280, 000 people, 9% of whom identify as being of Aboriginal or Torres Strait Islander heritage [15].
We present a retrospective cohort study on bacteraemic cases of CAAP presenting to Cairns Hospital between January 2000 and December 2019 inclusive.
2.3. Participant recruitment and sample collection
Inclusion required clinical, radiologic and microbiologic evidence of Acinetobacter pneumonia. Isolation of Acinetobacter baumannii complex from blood was required for diagnosis, as sputum cultures alone may be insufficient to diagnose CAAP [16]. Criteria for community-acquired infection required patients to be free of hospital presentation within the preceding 72 hours.
Acinetobacter baumannii bacteraemic pneumonia was diagnosed with the following criteria:
- Blood culture positive for Acinetobacter baumannii complex;
- Clinical features consistent with pneumonia;
- Radiographic evidence of pneumonia on chest radiograph or computed tomography scan.
Mortality was defined as death attributable to Acinetobacter pneumonia within 30 days of hospital admission. Pneumonia severity was characterized using SMART-COP score [17], based on information at the time of admission. Data were collected for potential risk factors for CAAP as defined by literature [1,2,18,19,20,21,22], which included presence of renal failure, diabetes mellitus, chronic pulmonary disease, current tobacco use, hazardous alcohol intake, malignancy, immunosuppression, and heart failure. Wet season disease was determined by a high average monthly rainfall between the months of October and April at the patient’s town of residence, available from the Australian Bureau of Meteorology [23].
2.4. Definitions
Unless otherwise stated, A. baumannii refers to Acinetobacter baumannii complex. Hypoxaemia was defined by SMART-COP score parameters with either SpO2 of <94% or pO2 of <70mmHg. Shock was considered if the systolic blood pressure was recorded as <90mmHg at time of presentation. Immunosuppression was based on either chronic glucocorticoid use (>10mg/day of prednisolone or equivalent), maintenance immunosuppressive therapy, or a known immunodeficiency syndrome. Targeted antibiotic therapy refers to the first line antibiotics given at commencement treatment. This does not refer to antibiotics that may have efficacy but are given as part of an ‘oral-tail’ i.e., ciprofloxacin or trimethoprim-sulfamethoxazole. First line targeted antibiotic therapy included intravenous antibiotics with established efficacy for CAAP, either gentamicin or carbapenem.
2.5. Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics package version 27. Chi-square test for independence or Fisher exact tests were used for comparison of two categorical variables. Mann-Whitney U-test was used for comparison of categorical with continuous variables where continuous variables were non-parametric.
2.6. Ethics
This project was granted ethics approval by the Far North Queensland Human Research Ethics Committee, Cairns Hospital (HREC/16/QCH/106-1080QA).
3. Results
There were 135 identified encounters of Acinetobacter spp. bacteraemia, of which 37 met inclusion criteria for community-acquired Acinetobacter baumannii pneumonia. One case of Acinetobacter haemolyticus pneumonia was excluded and a further nine cases were unavailable. Twenty-eight cases were available for final inclusion (Figure 1). The overall mortality was 28.6% (8/28). Greater mortality was seen in patients who did not receive targeted antibiotic therapy from day one (45.5%), compared with those who received gentamicin or carbapenem on day one (17.6%).
The mean age of patients presenting with CAAP was 43 (36.8-51.3) (Table 1). Patients were more likely to be male (67.9%), Indigenous Australians (82.1%), and to present in the Wet Season (64.3%).
Clinically, patients presented with sputum production (47.8%), pleuritic chest pain (64.3%), and were observed to be pyrexical (57.1%) and hypoxaemic (71.4%). 89.3% of patients had moderate or severe pneumonia (SMART-COP) and often required admission to ICU (57.1%).
Biochemical abnormalities included neutrophilia (57.1%) and elevated C-reactive protein (95.5%) (Table 2). The median time to blood culture positivity for Acinetobacter baumannii was 10.7 hours. Radiographically, 9 (32.1%) patients had disease limited to the left hemithorax, 12 (42.9%) had disease limited to the right hemithorax, and 6 (21.4%) had bilateral infiltrates. In total, 16 (57.1%) had multi-lobar disease. Pleural effusions were uncommon, 7/28 (25%). No pleural aspirates were performed.
Current tobacco use and hazardous ethanol consumption were the risk factors most frequently associated with CAAP (Table 1). Tobacco smoking was not associated with increased mortality (Table 3). 89.3% of individuals had two or more recognized risk factors for disease. Disease severity was not associated with the presence of multiple risk factors, nor the length of hospital stay. Non-targeted antibiotics for the treatment of CAAP on day one were found to confer the greatest risk for mortality amongst CAAP patients (50%) (Table 3). While a greater proportion of patients with mild-to-moderate CAAP on presentation died (4/10) than those with severe CAAP (4/18), there was no statistically significant difference in mortality between the two groups (χ2 = 0.742, df = 1, p = 0.320).
There was no statistically significant difference between the season of presentation (wet vs dry) and effect on presenting severity, (Table 1) (F = 0.395, df = 26, p = 0.535) or mortality (χ2 = 0.16, df = 1, p = 0.901). Although there were more presentations to ICU during wet season, 10/16 (62.5%), this did not reach statistical significance (χ2 = 0.052, df = 1, p = 0.820). Of three patients who died from fulminant sepsis within 24 hours, one occurred in the dry season and two occurred in the wet season. An equal number of patients received gentamicin on day one in both wet and dry season respectively, and 5 cases received meropenem on day one in both wet and dry seasons.
A greater proportion of patients received CAAP targeted antibiotic therapy on day one if they had severe SMART-COP score, (z = 1.854, df =26, p =0.064). There was no significant difference between day 1 antibiotic choice and requirement for ICU (χ2 = 3.194, df = 26, p = 0.535). Additionally, there was a non-statistically significant difference in day 1 targeted antibiotic choice and mortality, (χ2 = 2.530, df = 1, p = 0.200). 45.5% (5/11) of patients who did not receive targeted antibiotics died, whereas only 17.6% (3/17) receiving targeted antibiotics on day 1 died. Of total deaths, 50% (4/8) did not receive gentamicin or meropenem on day 1 (Table 4).
4. Discussion
The demographics of our cohort mirror previous Australian studies with an over-representation of Indigenous Australians, males, and the middle aged [1,7]. The laboratory investigations represented in Table 2 are consistent with infection, and are not discriminatory alone for the diagnosis of CAAP. Most patients had multi-lobar infection, and no tendency to a single hemithorax.
Hazardous alcohol intake and current smoking status were the most common risk factors. Although supported by other Australian studies [1,7], this contrasts with studies from South East Asia where excess alcohol consumption is less common [6,8,18,24]. Cases of diabetes mellitus (DM) and chronic renal failure (CRF) were underrepresented in distinction to other studies [1,6,8,10,19,20]. As few patients had pre-morbid renal function, or assessment for DM it is possible these comorbidities are under reported. Our cohort had similar presenting severity to a large Australian cohort from Darwin with median SMART-COP scores of 6.0 and 5.5 respectively [7]. Despite similar severity, we had fewer ICU admissions (57% vs 80%) [7].
An earlier pilot study during the wet season in tropical Australia demonstrated throat carriage of Acinetobacter in 10% of residents consuming excessive alcohol [18]. Ethanol impairs host immunity by adversely affecting phagocytosis, intracellular killing, cytokine production, antigen presentation, and B-cell function [2,25]. Additionally, ethanol may hinder surfactant production, reducing anti-bacterial activity [25]. Secondly, ethanol may promote micro-aspiration of colonised pharyngeal bacteria leading to nascent pulmonary infection [16]. We propose that ethanol may contribute to; upper airway colonisation with Acinetobacter, risk of aspiration, and impaired immune response to infection.
A recent study from the Northern Territory has shown community-acquired strains of A.baumannii harbour fewer virulence factors than nosocomial strains [26]. Additionally, no correlation was seen between strains harbouring more virulence factors and disease severity, ICU admission or mortality [26]. Therefore, host factors such as alcohol and tobacco consumption are likely more important in promoting disease transmission and impairing host response to infection [2,26,27]. Alcohol intoxication in itself may influence bacterial gene expression [26], and promote growth of Acinetobacter [2], adding to the complex interplay between host and bacterial factors affecting virulence.
It is important to recognise the role of risk factors in disease acquisition, host response and clinical outcomes, although they have less discriminatory value in distinguishing CAAP from other causes of severe pneumonia or gram-negative sepsis. A consideration, given that Australian antibiotic guidelines lean on risk factor identification for the purpose of rationalising antibiotic therapy.
Community-acquired Acinetobacter baumannii pneumonia, is considered a tropical or sub-tropical wet season disease [2,7,21,27,28,29,30]. We observed over one third of patients presenting with CAAP in the dry season. This observation is supported by a case control series in Japan, which found no difference in season in respect to the number of CAAP presentations [22]. Other case series have reported a wet season ‘peak’ but, found no significant difference between season [9], or acknowledged there were reasonable case numbers in the dry season [1,8]. Prior studies suggest the seasonal predominance is due to promotion of bacterial growth in warm, humid environments [27,28,30], although this does not explain the mechanism leading to initial nasopharyngeal colonisation. Presumably, and similar to Burkholderia pseudomallei [31,32,33], Acinetobacter is liberated from soil in aerosols during severe wet weather. We therefore propose that the initial nasopharyngeal colonisation may occur during the wet season, although subsequent infection may occur later with aspiration [2,16], or during a relative immunocompromised state.
We found no significant difference in disease severity at presentation as defined by SMART-COP score between wet and dry season disease (p = 0.535). Furthermore, there was no significant difference in ICU presentations between wet and dry seasons (p = 0.82). This is an important consideration, as a determinant for considering empiric treatment of CAAP is if it occurs during the wet season [12,13,14]. In the authors’ experience, CAAP is not typically considered, nor is it deliberately treated empirically in the drier months. Surprisingly, there was an equal proportion of gentamicin and meropenem use on day one in both dry and wet season disease. This potentially reflects coverage for severe CAP or gram-negative sepsis, rather than empirical treatment for suspected CAAP.
We suggest that the relatively improved mortality rate of 28.6% in our cohort, compared to previous studies [1,2,9,18,19], is a reflection of a higher proportion of moderate-to-severe CAP treated with targeted antibiotics for CAAP. If subjects were given gentamicin or meropenem on day one, they were less likely to die (17.6%) compared to those who did not receive targeted antibiotics on day 1 (44.4%). This is despite lower acuity illness, as measured by median SMART-COP score in those who did not receive targeted antibiotic therapy (4 vs 7). Although this rate did not reach statistical significance, the trend may be clinically significant. Furthermore, presenting severity of CAAP did not influence mortality (p = 0.320). Our mortality rate of 28.6% exceeded that of the Darwin cohort at 11% [7]. However, all patients in the Darwin cohort received timely antibiotics targeted to CAAP [7], compared to 61% of patients in our cohort. Evaluating patients who received targeted antibiotics on Day 1, only 3 died (17.6%) with a much-improved mortality rate. Furthermore, 2 of these 3 patients died within hours of arrival. This more likely reflects decompensated sepsis than failure of antibiotic therapy per se. This highlights the importance of timely targeted antibiotic therapy in mitigating mortality associated with CAAP including in initially mild to moderate illness, and further supports the conclusions drawn from the Darwin study that mortality rates can be significantly improved with gentamicin or carbapenems [7].
We compared outcomes between the two frontline antibiotics, meropenem and gentamicin to determine efficiency and patient outcomes. Unfortunately, we had insufficient data to make definitive statistical conclusions. Table 4 compares the patient groups who received either gentamicin or meropenem upfront, or who received it later in the course of disease, presumably either due to deterioration in disease severity or following identification of Acinetobacter baumannii on culture. Mortality, hospital length of stay, and disease severity on presentation are similar between both meropenem on day one and gentamicin on day one. The higher proportion of patients who received meropenem that required ICU (8/10 meropenem, 2/4 gentamicin) may reflect the prescribing practices amongst ICU clinicians or difference in disease severity.
Furthermore, there was greater mortality with delayed access to meropenem compared with a delay to gentamicin (3/5 vs 0/3). Limited data may diminish the strength of our conclusions, but importantly, a single dose of administered gentamicin may provide efficacy whilst awaiting confirmatory culture. This finding supports recent revisions of the Therapeutic Guidelines, which suggest an initial single dose gentamicin as part of ‘triple therapy’ for moderate disease where CAAP is suspected [12].
4.1. Limitations
Given the retrospective nature of this study, some data was limited, including data for SMART-COP scores where blood gas analysis was unavailable for some patients. This may have underestimated disease severity. It was presumed the presenting severity guided antibiotic decision making on day one. Although this does not appreciate the rapidity with which patients may deteriorate. This may explain some discordance with antibiotic choice, patient outcomes, and the defined severity of illness. Strict definitions on hazardous ethanol intake could not be adhered to and were reliant on clinician discretion and documentation. We defined cases of community-acquired disease to be free of hospital presentation within the preceding 72 hours. Given the retrospective nature of cases, there may be instances of community-onset disease that is not strictly community-acquired. However, antibiotic susceptibility profiling of cases suggests that all cases were community-acquired. Cases excluded due to the inaccessibility of patient records were over-represented by peripheral hospitals, possibly contributing to selection bias. Furthermore, as this is a single centre study, overall results may be less generalisable. Although we believe this still adds to the growing literature on CAAP given previous Australian studies have been limited to a single centre in the Northern Territory of Australia.
5. Conclusions
We report retrospectively on twenty-eight cases of community-acquired bacteraemic Acinetobacter baumannii pneumonia from North Queensland. Risk factors identified are similar to prior Australian studies, with middle age, male, and Indigenous Australians over-represented. The most commonly reported modifiable risk factors included hazardous alcohol intake, and current smoking, with 89% having two or more risk factors. First line antibiotics for A.baumannii are gentamicin or carbapenems. We propose that risk factors confer the greatest likelihood of sepsis arising from CAAP, and therefore irrespective of initial severity early use of first line antibiotic therapy can reduce mortality. We advocate for the use of targeted antibiotics in suspected cases of CAAP where clinical suspicion should be one based on risk factors, disease severity and clinical acumen, irrespective of season at presentation. Unfortunately, these risk factors are not unique for CAAP and thus do not discriminate from other infectious aetiologies.
The authors agree with current antibiotic guidelines for wet season CAP in tropical Australia. Although our study consists of relatively few numbers, we have demonstrated dry season CAAP in a third of overall cases. Supported by the data from our cohort, we would contend the use of single dose gentamicin be considered in future guidelines for empirical cover of dry season CAAP in suspected cases whilst awaiting culture confirmation. Single dose gentamicin may also be considered in cases of mild pneumonia where the patient later deteriorates. Particularly as the time to blood culture positivity in most instances is brief. In our experience, single dose gentamicin is safe to prescribe even in renal impairment or sepsis. This change in clinic practice may help improve mortality in dry-season disease. Furthermore, it may help diminish the over-reliance on carbapenems, and the development of subsequent antibiotic resistance this entails. Overall, mortality rates remain poor even in well-managed cases and thus ongoing vigilance by clinical caregivers in Australia is paramount.
Author Contributions
Timothy Riddles contributed to data curation, data analysis, writing original draft preparation, and editing. Daniel Judge contributed to conceptualization, methodology, review and editing, as well as supervision.
Funding
This research received no external funding.
Institutional Review Board Statement
This project was granted ethics approval by the Far North Queensland Human Research Ethics Committee, Cairns Hospital (HREC/16/QCH/106-1080QA).
Informed Consent Statement
Patient consent was waived, as the project fell under the category of a quality audit project.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to containing information that may compromise the privacy of participants.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Anstey, N.M.; Currie, B.J.; Withnall, K.M. Community-Acquired Acinetobacter Pneumonia in the Northern Territory of Australia. Clin. Infect. Dis. 1992, 14, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Dexter, C.; Murray, G.L.; Paulsen, I.T.; Peleg, A.Y. Community-acquiredAcinetobacter baumannii: clinical characteristics, epidemiology and pathogenesis. Expert Rev. Anti-infective Ther. 2015, 13, 567–573. [Google Scholar] [CrossRef]
- Yang, C.-H.; Chen, K.-J.; Wang, C.-K. Community-acquired Acinetobacter pneumonia: A case report. J. Infect. 1997, 35, 316–318. [Google Scholar] [CrossRef] [PubMed]
- Antunes, L.C.; Visca, P.; Towner, K.J. Acinetobacter baumannii: evolution of a global pathogen. Pathog. Dis. 2014, 71, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, T.; Barnes, D.J. COMMUNITY-ACQUIRED ACINETOBACTER PNEUMONIA. Aust. New Zealand J. Med. 1989, 19, 259–260. [Google Scholar] [CrossRef]
- Chen, M.-Z.; Hsueh, P.-R.; Lee, L.-N.; Yu, C.-J.; Yang, P.-C.; Luh, K.-T. Severe Community-Acquired Pneumonia due to Acinetobacter baumannii. Chest 2001, 120, 1072–1077. [Google Scholar] [CrossRef]
- Davis, J.S.; McMillan, M.; Swaminathan, A.; Kelly, J.A.; Piera, K.E.; Baird, R.W.; Currie, B.J.; Anstey, N.M. A 16-Year Prospective Study of Community-Onset Bacteremic Acinetobacter Pneumonia. Chest 2014, 146, 1038–1045. [Google Scholar] [CrossRef]
- Ong CWM, Lye DCB, et al. Severe community acquired Acinetobacter baumannii pneumonia: an emerging highly lethal infectious disease in the Asia-Pacific. Respirology. 2009, 14, 1200–1205. [CrossRef]
- Patamatamkul, S.; Klungboonkrong, V.; Praisarnti, P.; Jirakiat, K. A case-control study of community-acquired Acinetobacter baumannii pneumonia and melioidosis pneumonia in northeast Thailand: an emerging fatal disease with unique clinical features. Diagn. Microbiol. Infect. Dis. 2017, 87, 79–86. [Google Scholar] [CrossRef]
- Chusri, S.; Chongsuvivatwong, V.; Silpapojakul, K.; Singkhamanan, K.; Hortiwakul, T.; Charernmak, B.; Doi, Y. Clinical characteristics and outcomes of community and hospital-acquired Acinetobacter baumannii bacteremia. J. Microbiol. Immunol. Infect. 2019, 52, 796–806. [Google Scholar] [CrossRef]
- Lee YL, Lu MC, et al. Nationwide surveillance of antimicrobial resistance among clinically important Gram-negative bacteria, with an emphasis on carbapenems and colistin: Results from the surveillance of multicentre antimicrobial resistance in Taiwan (SMART) in 2018. Int. J. Antimicrob. Agents. 2019, 54, 318–328. [CrossRef]
- Kelly H, Buising K, et al. Electronic Therapeutic Guidelines Antibiotic [on-line]. 16th Edition. Melbourne: Therapeutic Guidelines Limited; 2019. Respiratory tract infections: community-acquired pneumonia.
- Christiansen K, Currie B, et al. Therapeutic Guidelines Antibiotic. 11th Edition. Melbourne: Therapeutic Guidelines Limited; 2000. Respiratory tract infections: lower; p. 141-149.
- Moulds R, Boutlis C, et al. Therapeutic Guidelines Antibiotic. 15th Edition. Melbourne: Therapeutic Guidelines Limited; 2014. Respiratory tract infections: community-acquired pneumonia; p. 153-180.
- Lee, A.; Hanson, J.; Fox, P.; Spice, G.; Russell, D.; Boyd, P. A decentralised, multidisciplinary model of care facilitates treatment of hepatitis C in regional Australia. J. Virus Erad. 2018, 4, 160–164. [Google Scholar] [CrossRef]
- Anstey, N.M.; Currie, B.J.; Hassell, M.; Palmer, D.; Dwyer, B.; Seifert, H. Community-Acquired Bacteremic Acinetobacter Pneumonia in Tropical Australia Is Caused by Diverse Strains of Acinetobacter baumannii, with Carriage in the Throat in At-Risk Groups. J. Clin. Microbiol. 2002, 40, 685–686. [Google Scholar] [CrossRef] [PubMed]
- Charles, P.G.P.; Wolfe, R.; Whitby, M.; Fine, M.J.; Fuller, A.J.; Stirling, R.; Wright, A.A.; Ramirez, J.A.; Christiansen, K.J.; Waterer, G.W.; et al. SMART-COP: A Tool for Predicting the Need for Intensive Respiratory or Vasopressor Support in Community-Acquired Pneumonia. Clin. Infect. Dis. 2008, 47, 375–384. [Google Scholar] [CrossRef]
- Wang, J.-T.; McDonald, L.C.; Chang, S.-C.; Ho, M. Community-Acquired Acinetobacter baumannii Bacteremia in Adult Patients in Taiwan. J. Clin. Microbiol. 2002, 40, 1526–1529. [Google Scholar] [CrossRef]
- Leung, W.-S.; Chu, C.-M.; Tsang, K.-Y.; Lo, F.-H.; Lo, K.-F.; Ho, P.-L. Fulminant Community-Acquired Acinetobacter baumannii Pneumonia as a Distinct Clinical Syndrome. Chest 2006, 129, 102–109. [Google Scholar] [CrossRef]
- Falagas, M.E.; Karveli, E.A.; Kelesidis, I.; Kelesidis, T. Community-acquired Acinetobacter infections. Eur. J. Clin. Microbiol. Infect. Dis. 2007, 26, 857–868. [Google Scholar] [CrossRef]
- Sia TLL, Chua H. Case series: Fulminant community-acquired Acinetobacter pneumonia. Med J Malaysia. 2020, 75, 186–188.
- Asai, N.; Sakanashi, D.; Suematsu, H.; Kato, H.; Watanabe, H.; Shiota, A.; Hagihara, M.; Koizumi, Y.; Yamagishi, Y.; Mikamo, H. Clinical manifestations and risk factors of community-onset Acinetobacter species pneumonia in Japan; case control study in a single institute in Japan. J. Infect. Chemother. 2019, 25, 639–642. [Google Scholar] [CrossRef]
- Australian Bureau of Meteorology. Climate statistics for Australian sites: Queensland [Internet]. Australian Government. 2019. Available from: http://www.bom.gov.au/climate/averages/tables/ca_qld_names.
- Wu, C.-L.; Ku, S.-C.; Yang, K.-Y.; Fang, W.-F.; Tu, C.-Y.; Chen, C.-W.; Hsu, K.-H.; Fan, W.-C.; Lin, M.-C.; Chen, W.; et al. Antimicrobial drug-resistant microbes associated with hospitalized community-acquired and healthcare-associated pneumonia: A multi-center study in Taiwan. J. Formos. Med Assoc. 2013, 112, 31–40. [Google Scholar] [CrossRef]
- Gandhi, J.A.; Ekhar, V.V.; Asplund, M.B.; Abdulkareem, A.F.; Ahmadi, M.; Coelho, C.; Martinez, L.R. Alcohol Enhances Acinetobacter baumannii-Associated Pneumonia and Systemic Dissemination by Impairing Neutrophil Antimicrobial Activity in a Murine Model of Infection. PLOS ONE 2014, 9, e95707. [Google Scholar] [CrossRef] [PubMed]
- Meumann, E.M.; Anstey, N.M.; Currie, B.J.; Piera, K.A.; Kenyon, J.J.; Hall, R.M.; Davis, J.S.; Sarovich, D.S. Genomic epidemiology of severe community-onset Acinetobacter baumannii infection. Microb. Genom. 2019, 5. [Google Scholar] [CrossRef]
- Wong, D.; Nielsen, T.B.; Bonomo, R.A.; Pantapalangkoor, P.; Luna, B.; Spellberg, B. Clinical and Pathophysiological Overview of Acinetobacter Infections: a Century of Challenges. Clin. Microbiol. Rev. 2017, 30, 409–447. [Google Scholar] [CrossRef]
- Munoz-Price, L.S.; Weinstein, R.A. Acinetobacter Infection. New Engl. J. Med. 2008, 358, 1271–1281. [Google Scholar] [CrossRef] [PubMed]
- Eveillard, M.; Kempf, M.; Belmonte, O.; Pailhoriès, H.; Joly-Guillou, M.-L. Reservoirs of Acinetobacter baumannii outside the hospital and potential involvement in emerging human community-acquired infections. Int. J. Infect. Dis. 2013, 17, e802–e805. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.A.; Kim, J.J.; Won, D.J.; Lee, K. Seasonal and Temperature-Associated Increase in Community-Onset Acinetobacter baumannii Complex Colonization or Infection. Ann. Lab. Med. 2018, 38, 266–270. [Google Scholar] [CrossRef]
- Cheng, A.C.; Currie, B.J.; Dance, D.A.B.; Funnell, S.G.P.; Limmathurotsakul, D.; Simpson, A.J.H.; Peacock, S.J. Clinical Definitions of Melioidosis. Am. J. Trop. Med. Hyg. 2013, 88, 411–413. [Google Scholar] [CrossRef]
- Mu, J.-J.; Cheng, P.-Y.; Chen, P.-S.; Chen, Y.-L. The occurrence of melioidosis is related to different climatic conditions in distinct topographical areas of Taiwan. Epidemiology Infect. 2013, 142, 415–423. [Google Scholar] [CrossRef]
- Currie, B.J.; Jacups, S.P. Intensity of Rainfall and Severity of Melioidosis, Australia. Emerg. Infect. Dis. 2003, 9, 1538–1542. [Google Scholar] [CrossRef]
Figure 1.
Case Selection.
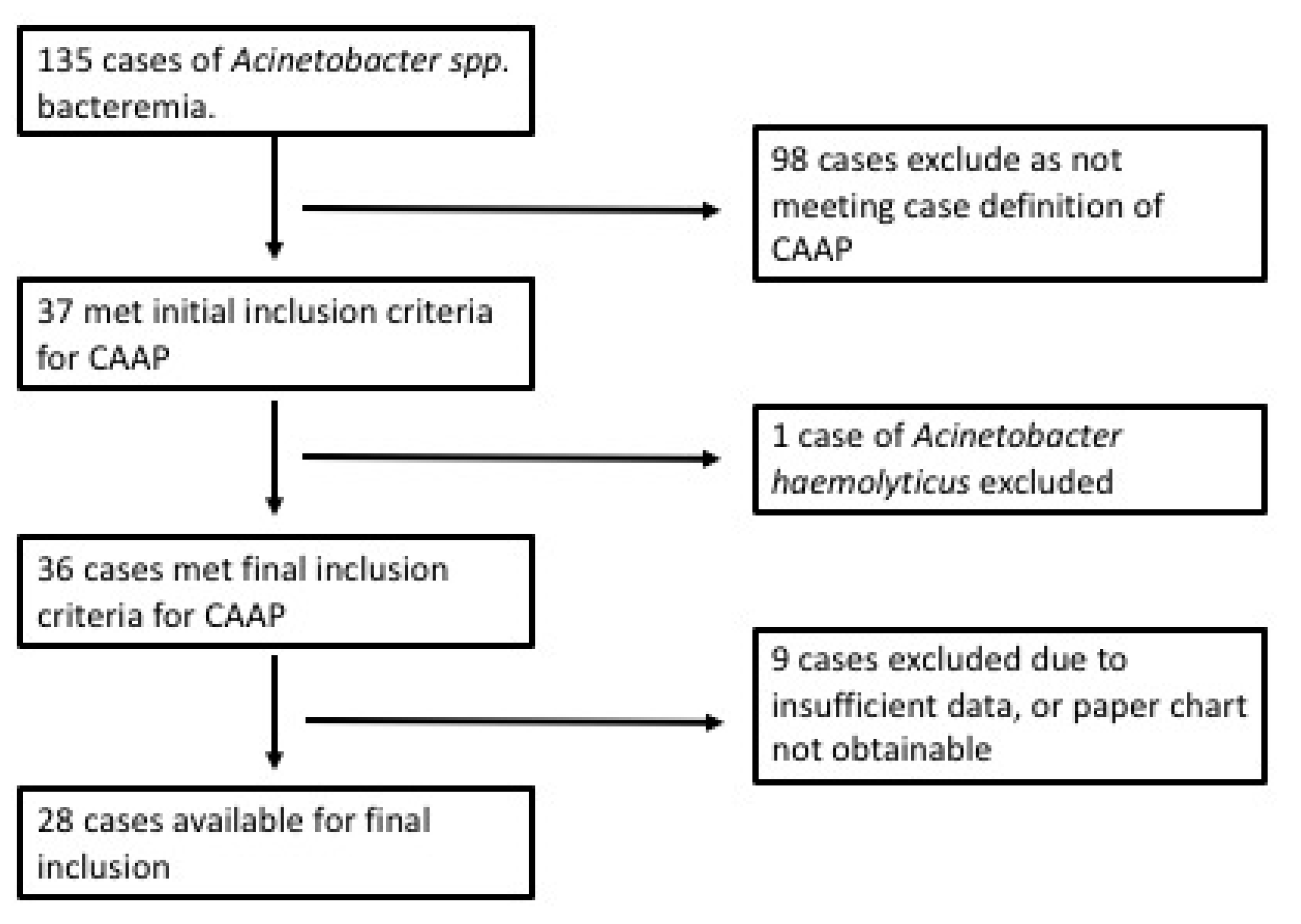

Table 1.
Demographics, Presenting Features, and Presenting Severity of CAAP.
| Patient Characteristic | Proportion of patients, n = 28 (%), [IQR] |
|---|---|
| Age in years, median, [IQR] | 43, [36.8-51.3] |
| Male | 19 (67.9) |
| Indigenous Australian | 23 (82.1) |
| Resident of Cairns | 9 (32.1) |
| Wet Season Disease | 18 (64.3) |
| Dry Season Disease | 10 (35.7) |
| Clinical features | |
| Pleurisy | 18 (64.3) |
| Pyrexia (>38 degrees) | 16 (57.1) |
| Muco-Purulent or Purulent Sputum | 11 (47.8) |
| Blood-stained Sputum | 11 (47.8) |
| Severity | |
| ICU admission | 16 (57.1) |
| SMART-COP (moderate to severe) | 25 (89.3) |
| SMART-COP, median and [IQR] | 6, [4-8] |
| Hypoxaemia | 20 (71.4) |
| Shock | 10 (35.7) |
| Death | 8 (28.6) |
| Risk Factors for CAAP | |
| Current tobacco Use | 23 (82.1) |
| Hazardous Alcohol Consumption | 20 (71.4) |
| Hazardous Alcohol & Tobacco Use | 17 (60.7) |
| Chronic Lung disease | 7 (25) |
| Heart Failure | 4 (14.3) |
| Diabetes Mellitus | 3 (10.7) |
| Chronic Kidney Disease | 4 (14.3) |
| Immunosuppression | 1 (3.6) |
| Malignancy | 1 (3.6) |
| ≥ 2 Risk Factors | 25 (89.3) |
IQR = Interquartile Range, ICU = Intensive Care Unit,.
Table 2.
Biochemical Results on Presentation.
| Test | Median [IQR] | Above Normal (%) | Below Normal (%) | Normal Reference Range |
|---|---|---|---|---|
| White Cell Count | 11.8 [7.8-17.4] | 14/28 (50) | 5/28 (17.9) | 4-11 × 109/L |
| Haemoglobin | 136 [121-146] | 0 (0) | 7/28 (25) | 135-175/120-155 (M/F) g/L |
| Neutrophils | 9.37 [5.46-15.5] | 16/28 (57.1) | 5/28 (17.9) | 2-7.5 × 109/L |
| Lymphocytes | 0.53 [0.41-0.93] | 0 (0) | 21/28 (75) | 1.5-4 × 109/L |
| Platelets | 177 [91.3-221] | 1/28 (3.57) | 12/28 (42.9) | 150-400 × 109/L |
| Albumin | 29.5 [25-33.5] | 0 (0) | 21/28 (75) | 35-50 g/L |
| C-Reactive Protein | 154 [63-231] | 21/22 (95.5) | 0 (0) | <5 mg/L |
IQR = Interquartile Range, M = Male, F= Female.
Table 3.
Risk Factors Related to Mortality.
| Risk Factor (RF) | Number (%) of those with RF who died | p-value |
|---|---|---|
| Shock | 3/10 (30) | 0.615 |
| Chronic Lung Disease | 3/7 (42.9) | 0.411 |
| Multi-Lobar Pneumonia | 3/16 (18.8) | 0.183 |
| Non-targeted ABs D1 | 4/8 (50) | 0.123 |
| Hazardous Alcohol Consumption | 6/20 (30) | 0.589 |
| Hazardous Alcohol & Tobacco Consumption | 4/17 (23.5) | 0.376 |
| Tobacco Consumption | 4/23 (17.4) | 0.015* |
| SMART-COP >/= 5 (Severe) | 4/18 (22.2) | 0.284 |
| Multiple Risk Factors >2 | 7/25 (28) | 0.652 |
| Overall mortality | 8/28 {28.6%} |
Non-targeted Antibiotics = antibiotics other than gentamicin or carbapenem, D1 = Day 1, defined as date of admission to hospital, RF = Risk Factor, *Significantly more patients lived who were current smokers. Test statistic from Fisher exact test.
Table 4.
Risk Factors Related to Mortality.
| Antibiotic Practice | No. | Died: Number (% sample/% total deaths) |
Died < 24 hours | Mean LOS | ICU | Median SMART-COP on Admission |
|---|---|---|---|---|---|---|
| Meropenem D1 | 10 | 2 (7.1/25) | 1 | 17.8 | 8 | 8 |
| Gentamicin D1 | 4 | 1 (3.6/12.5) | 1 | 16.5 | 2 | 6.5 |
| Both D1 | 3 | 0 | 0 | 22.7 | 2 | 6 |
| Total Mero/Gent D1 | 17 | 3 (10.7/37.5) | 2 | 18.3 | 12 | 7 |
| Delay to either | 9 | 4 (14.3/50) | 1 | 10 | 3 | 4 |
| Delay Gentamicin | 3 | 0 | 0 | 10.3 | 0 | 3 |
| Delay Meropenem | 5 | 3 (10.7/37.5) | 0 | 10.6 | 3 | 4 |
| Delay Both | 1 | 1 (3.6/12.5) | 0 | 6 | 0 | 2 |
| Mero D1 delay gent | 1 | 1 (3.6/12.5) | 0 | 25 | 1 | 8 |
| Gent D1 delay mero | 3 | 0 | 0 | 21.7 | 2 | 6 |
LOS = Length of Stay, D1 = Day 1, Mero = Meropenem, Gent = Gentamicin, ICU = Intensive Care Unit.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



