
Submitted:
24 July 2023
Posted:
25 July 2023
You are already at the latest version
Abstract
Background/Aims: Conflicting results have been reported regarding the interaction between proton pump inhibitors (PPIs) and clopidogrel. We investigated whether concomitant PPI use influenced the risk of recurrence in patients with stroke and myocardial infarction (MI).
Methods: This study used two databases for different designs, the Korean National Health Insurance Service (NHIS) database for a self-controlled case series design, and the national sample cohort of the NHIS database converted to the Observational Medical Outcomes Partnership-Common Data Model version for a cohort study.
Results: In the PPI co-prescription group, recurrent hospitalization with stroke occurred in 17.6% of the 8,201 patients with history of stroke, and recurrent MI occurred in 17.1% of the 1,216 patients with history of MI during 1 year. According to the self-controlled case series, the overall relative risk (RR) of recurrent stroke was 2.09 [95% confidence interval (CI); 1.83-2.38], and the RR showed an increasing trend with PPI duration. In the cohort study, there was a higher incidence of recurrent stroke in the PPI co-prescription group [Hazard ratio (HR): 1.34, 95% CI: 1.01-1.76, P=0.04]. The overall RR of recurrent MI was 1.47 (95% CI; 1.02-2.11) in the self-controlled case series; however, there was no statistically significant difference in recurrent MI in the cohort study (HR:1.42, 95% CI:0.79-2.49, P=0.23). The impact of individual PPIs on stroke and MI showed different patterns.
Conclusions: PPI co-prescription with clopidogrel was associated with recurrent stroke; however, its association with recurrent MI remains inconclusive. The influence of individual PPIs should be clarified in the future.
Keywords:
Proton pump inhibitors
; Clopidogrel
; Stroke
; Myocardial infarction
Introduction
Proton pump inhibitors (PPIs) promote peptic ulcer recovery by suppressing gastric acid secretion and reduce the incidence of complications from ulcers such as perforation or bleeding [1]. PPIs improve reflux symptoms and prevent complications from reflux esophagitis [2,3,4] and are fuzndamental in treating gastroesophageal reflux disease. PPIs also prevent gastrointestinal bleeding in patients using antithrombotic agents or non-steroidal anti-inflammatory drugs [5] and have, therefore, been the basis for the treatment of various gastrointestinal diseases.
As PPI use increases worldwide, growing concerns about PPI complications have been raised [6,7,8]. Specifically, drug interaction with clopidogrel, which is an antiplatelet agent classified as thienopyridines, has been postulated in many recent studies [9,10,11,12,13,14,15,16,17,18]. Both PPIs and clopidogrel are metabolized by hepatic cytochrome P450 (CYP) enzymes, and in the presence of CYP2C19 inhibition, PPIs could reduce the efficacy of clopidogrel's protective roles in cardiovascular events [19]. Moreover, when clopidogrel and PPIs were co-administered, the ability of platelet aggregation increased, and the results supporting the hypothesis that the concentration of the metabolite of clopidogrel would be lowered [20,21]. Hence, The US Food and Drug Administration (FDA) issued safety announcements between January 2009 and October 2010 warning against concomitant use of clopidogrel and PPIs, especially omeprazole and esomeprazole, due to a potential drug interaction that may attenuate clopidogrel’s antiplatelet activity [22]. However, despite the FDA warnings, the real-world evidence of clopidogrel and individual PPI interaction has not been fully evaluated, especially in Asian populations, which are known with a high frequency of poor metabolizer CYP2C19 enzymes. In addition, previous observational studies were limited by multiple confounding factors and small sample sizes.
To overcome these limitations, we conducted a nationwide population-based study using two different designs: a large-scale propensity score (PS) matching cohort and a self-controlled case series. We aimed to identify the risk of recurrent events in patients diagnosed with stroke and myocardial infarction (MI) and concomitant use of PPIs and clopidogrel. We also evaluated the impact of the concomitant use of individual PPIs and clopidogrel on recurrent stroke and MI.
Methods
Data sources
This study utilized two databases: we converted the large-scale cohort from the Korean National Health Insurance Service (NHIS) database from 2009 to 2014 and the National Sample Cohort (NSC) of the NHIS database from 2002 to 2013 to the Observational Medical Outcomes Partnership-Common Data Model (OMOP-CDM) version. The Korean NHIS database is a large dataset of 1.3 trillion records, including diagnoses, procedures, surgeries, and prescriptions. It also contains medical data, including sociodemographic status, body height and weight, comorbidities, and health-related behaviors such as alcohol consumption and smoking habits [23,24]. In the OMOP-CDM version of the Korean NHIS-NSC (NHIS-CDM), the data of 1.13 million patients was converted to the OMOP-CDM, resulting in a 99.1% conversion rate [25]. The OMOP-CDM represents healthcare data from a diverse source in a consistent and standardized manner [26]. Furthermore, the NHIS-CDM database has been applied in multiple studies [27,28,29]. The study protocol was approved by the Institutional Review Board of Kangdong Sacred Heart Hospital (IRB number: 2021-07-011), and National Health Insurance Service Ilsan Hospital (IRB number: 2020-06-037).
Study design and population
Self-controlled case series study
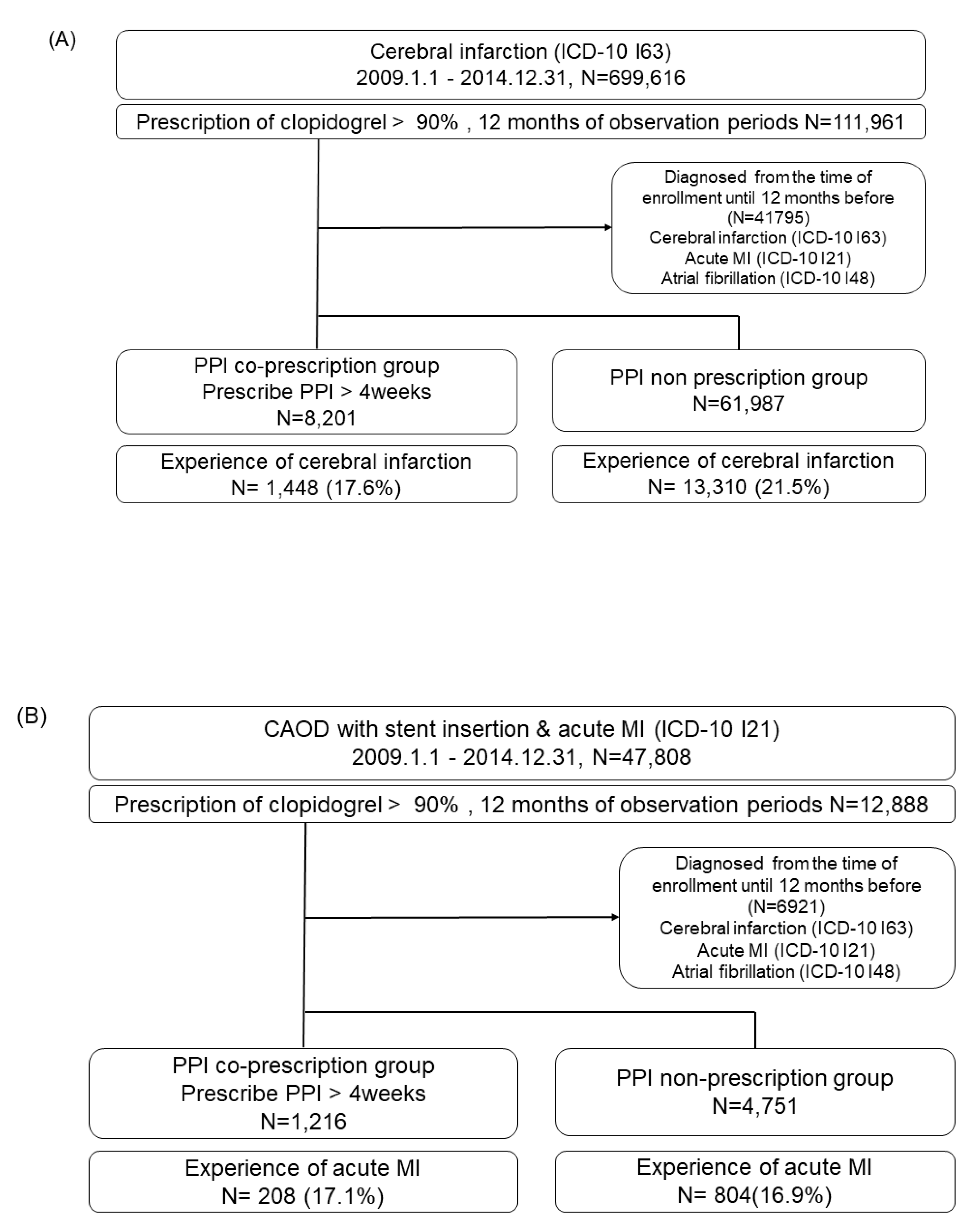
We included adult patients from the Korean NHIS database who were newly diagnosed with cerebral infarction (ICD-10 I63) and acute MI (ICD-10 I21) or percutaneous coronary intervention from January 1, 2009, to December 31, 2014, and prescribed clopidogrel during > 90% of the observation period. The PPI co-prescription group was defined as PPI prescription > 4 weeks. The exclusion criteria were as follows: (1) observation period < 1 year before cohort entry, (2) atrial fibrillation, and (3) PPI exposure < 4 weeks. The flow of the study is presented in Figure 1. In the PPI co-prescription group, recurrent hospitalization due to stroke occurred in 17.6% of the 8,201 patients with a history of stroke (Figure 1A), and recurrent MI occurred in 17.1% of the 1,216 patients with a history of MI within 1 year after the initial diagnosis (Figure 1B).
Figure 1.
Study flow chart in the analysis of stroke (A) and myocardial infarction (B). Abbreviations: PPI, proton pump inhibitor; MI, myocardial infarction; ICD, International Classification of Diseases; CAOD, coronary artery obstructive disease.
Figure 1.
Study flow chart in the analysis of stroke (A) and myocardial infarction (B). Abbreviations: PPI, proton pump inhibitor; MI, myocardial infarction; ICD, International Classification of Diseases; CAOD, coronary artery obstructive disease.
Self-controlled case series analysis is a type of cohort study in which relative risk is based on within-person comparisons between exposed and unexposed observation times, meaning that only exposed patients with events can be included [30]. We included only patients with recurrent stroke and MI in the PPI co-prescription group for the self-controlled case series analysis. We considered PPI exposure to begin on the date of PPI prescription and end after its calculated duration, including any consecutive prescriptions, plus an additional 30-day washout period. PPI duration was divided as follows: 0–2, 2–4, 4–6, 6–8, and > 8 weeks. We also analyzed the overall relative risk for each PPI type.
Cohort Study
The cohort study was conducted using the NHIS-CDM database, which could be analyzed with large-scale PS matching to improve comparability between PPI and non-PPI groups. The target cohort was defined as new clopidogrel use over 4 weeks with a co-prescription of PPI over 4 weeks in patients diagnosed with stroke or acute MI. The target cohort was censored if patients were diagnosed with any of the outcomes or if the observation ended. The comparator cohort was defined as new clopidogrel use over 4 weeks with no PPI exposure within 4 weeks of clopidogrel exposure in patients with stroke or acute MI. The censoring rule was PPI exposure, outcome ascertainment, or end of observation. The observation period before cohort entry was at least 1 year for both cohorts. The primary outcome was the incidence rates of recurrent stroke or MI with hospitalization in patients with a history of stroke or MI, respectively.
Statistical analyses
We used SAS version 9.4 (SAS Institute, Cary, NC, USA) and Stata version 15.1 (Stata Corporation, College Station, TX, USA) for all statistical analyses in the self-controlled case series. Categorical variables were analyzed using the chi-squared test, and continuous variables were analyzed using t-tests. We calculated the incidence rate ratio, which is the ratio of the incidence rate of an event during the exposure period to the non-exposure period, and described the relative risk and 95% confidence interval (CI).
The cohort study was performed using ATLAS ver. 2.7 and R statistical software (version 3.6.1 for Windows; R Foundation for Statistical Computing). We analyzed Cox proportional hazard models to calculate the hazard ratios (HRs) with 95% CI for outcomes between the target and comparator cohorts using the CohortMethod package in R. The Kaplan–Meier method was used to estimate the cumulative incidence rates, and the cumulative incidence between the two groups was compared using the log-rank test.
The OMOP-CDM research provides large-scale PS models with regularized logistic regression [31]. The following covariates were used for PS matching: age, sex, all previous comorbidities, all drugs in the 365 days prior to the index date, and the Charlson comorbidity index score. We considered the main analysis to be 1:4 propensity score matching, and sensitivity analyses were performed with differing matching ratios, observation periods, and PS stratifications. Statistical significance was set at P < 0.05.
Results
Self-controlled case series design
The comparison of the baseline characteristics between the PPI co-prescription and non-prescription groups for stroke and MI is presented in Table 1. The PPI co-prescription group was significantly older than the PPI non-prescription group. There was a significant difference in the proportion of comorbidities between the two groups (Table 1). We included 1,448 patients with recurrent stroke and 208 patients with recurrent MI in the PPI co-prescription group.

Table 1.
Comparison of baseline characteristics between PPI co-prescription and non-prescription groups (self-controlled case series analysis).
Table 1.
Comparison of baseline characteristics between PPI co-prescription and non-prescription groups (self-controlled case series analysis).
| Stroke | Myocardial infarction | |||||
|---|---|---|---|---|---|---|
| Variables | PPI co-prescription groups (n=8,201) |
PPI non-prescription group (n=61,987) |
P-value | PPI co-prescription group (n=1,216) |
PPI non-prescription group (n=4,751) |
P-value |
| Sex | ||||||
| Women, n (%) | 3,742 (45.8) | 25,662 (41.4) | <0.001 | 670 (55.1) | 3,043 (64.0) | <0.001 |
| Age | 67.28 ± 10.99 | 66.14 ± 11.86 | <0.001 | 69.64 ± 10.26 | 68.06 ± 11.51 | <0.001 |
| Aspirin co-prescription | 3,094 (37.8) | 22,810 (36.8) | 0.069 | 982 (80.8) | 3,608 (75.9) | <0.001 |
| Comorbidity | ||||||
| Hypertension | 6,357 (77.7) | 46,388 (74.8) | <0.001 | 1,080 (58.1) | 4,103 (86.4) | 0.023 |
| Diabetes mellitus | 4,041 (49.4) | 32,432 (52.3) | <0.001 | 707 (58.1) | 2,662 (56.0) | 0.185 |
| Dyslipidemia | 5,499 (67.3) | 38,245 (61.7) | <0.001 | 917 (75.4) | 3,534 (74.4) | 0.463 |
| Smoking history | ||||||
| Never smoker | 2,610 (31.9) | 16,837 (27.1) | <0.001 | 341(28.0) | 1,146 (24.1) | 0.020 |
| Ex-smoker | 728 (8.9) | 4,643 (7.5) | 106 (8.7) | 389 (8.2) | ||
| Current smoker | 1,137 (13.9) | 8,531 (13.8) | 159 (13.1) | 625 (13.2) | ||
| BMI (kg/m2) | 24.43± 3.09 | 24.39 ± 3.05 | 0.479 | 24.11±3.1 | 24.41±3.08 | 0.032 |
| Total cholesterol level (mg/dL) | 202.52 ± 42.01 | 204.96 ± 45.07 | <0.001 | 205.94 ±44.95 | 207.52± 53.37 | 0.460 |
PPI, proton pump inhibitor; BMI, body mass index.
Relative risk of recurrent stroke in the PPI co-prescription group
Of the 1,448 hospitalizations with stroke as the primary diagnosis, 653 events occurred while patients were co-prescribed PPIs, and 795 events occurred while patients were prescribed clopidogrel alone. The overall relative risk of recurrent stroke was 2.09 (95% CI; 1.83-2.38) (Table 2). According to PPI co-prescription duration, the RR showed an increasing trend [0~2 weeks; 1.76 (95% CI; 1.50-2.07), 2~4 weeks; 2.02 (95% CI; 1.68-2.43), 4~6 weeks; 3.02 (95% CI; 2.36-3.86), 6~8 weeks; 2.81 (95% CI; 2.02-3.92), >8 weeks; 5.57 (95% CI; 4.06-7.64)] (Table 2). We also conducted an analysis including PPI washout periods. During the remaining 4 weeks after the end of the PPI prescription, 201 events occurred. The RR including the 4-week washout periods was 2.47 (95% CI 2.16-2.80) (Table 2).
To identify the impact of individual PPIs on clopidogrel, we repeated the analysis according to PPI type. The most commonly prescribed drug was rabeprazole (n=492), followed by esomeprazole (n=373), pantoprazole (n=364), lansoprazole (n=170), omeprazole (n=137) and dexlansoprazole (n=12). Table 3 shows the RR of risk periods during PPI co-prescription periods only, including the 4-week PPI washout periods. Esomeprazole showed the highest RR (2.75. 95% CI; 2.12-3.57), and the risk was more significant, including during the washout period (Table 3).
Relative risk of recurrent MI in the PPI co-prescription group
Of 208 hospitalizations with MI as the primary diagnosis, 95 events occurred while patients were co-prescribed PPIs, and 113 events occurred while patients were prescribed clopidogrel alone. The overall relative risk of recurrent MI was 1.47 (95% CI; 1.02-2.11) (Table 2). According to PPI co-prescription duration, the RR showed an increasing trend [0~2 weeks; 1.30 (95% CI; 0.83-2.04), 2~4 weeks; 0.95 (95% CI; 0.54-1.69), 4~6 weeks; 2.33 (95% CI; 1.32-4.13), 6~8 weeks; 1.99 (95% CI; 0.98-4.03), >8 weeks; 3.80 (95% CI; 1.93-7.45)] (Table 2). We also conducted an analysis including the PPI washout periods, and the RR including the 4-week washout periods was 1.87 (95% CI:1.31-2.65) (Table 2).
The most commonly prescribed drug was pantoprazole (n=82), followed by rabeprazole (n=58), esomeprazole (n=50), lansoprazole (n=32), omeprazole (n=9) and dexlansoprazole (n=2). Only pantoprazole showed a significant RR for MI (2.56, 95% CI; 1.46-4.50) (Table 3).
Cohort study
The flow chart of the cohort study is shown in Figure S1. Initially, 442 patients in the PPI co-prescription group and 11,078 patients in the non-prescription group were included in the analysis of stroke, and 245 patients in the PPI co-prescription group and 3,933 patients in the non-prescription groups were included in the analysis of MI. A total of 9,947 and 7,979 covariates were used for large-scale PS matching in the analysis of stroke and MI, respectively (Figure S2). The baseline characteristics of stroke and MI before and after 1:4 PS matching are presented in Supplementary Table S1 and Table S2, respectively. After PS matching, 373 patients were included in the PPI co-prescription group, 1,051 in the non-prescription group, 179 in the PPI co-prescription group, and 439 in the non-prescription groups in the final analysis of stroke and MI, respectively. The most standardized mean difference was less than 0.1, which suggests that the PPI co-prescription and non-prescription groups were well balanced after large-scale PS matching.
Incidence of recurrent stroke in the PPI co-prescription group
The results of Cox regression analysis with 1:4 PS matching are shown in Table 4. There was a higher incidence of recurrent stroke in the PPI co-prescription group [PPI co-prescription group (n=373) vs. non-prescription group (n=1,051); 81/240 person-years vs. 189/740 person-years, HR: 1.34, 95% CI; 1.01-1.76, P=0.04]. Sensitivity analysis was performed using 1:1 matching, PS stratification, and different observation periods. In the analysis of stroke, the sensitivity analysis showed results consistent with those of the main analysis (Table 5).
Incidence of recurrent MI in the PPI co-prescription group
There was no statistically significant difference in the incidence rate of recurrent MI between the PPI co-prescription and non-prescription groups [PPI co-prescription group (n=179) vs. non-prescription group (n=439); 23/133 person-years vs. 43/336 person-years, HR:1.42, 95% CI:0.79-2.49, P=0.23) (Table 4). Sensitivity analysis also showed inconsistent results (Table 5). Only the results with 1:4 PS matching until 6 months showed a significantly higher incidence of recurrent MI in the PPI co-prescription group (HR,2.15; 95% CI:1.10-4.13).
Discussion
In the present study, the risk of recurrent stroke was higher in the PPI co-prescription group with clopidogrel in patients with stroke in both the self-controlled case series analysis and the large-scale PS-matched cohort study. However, the risk of recurrent MI showed different results among various analyses, suggesting that the interaction between PPI and clopidogrel on MI should be elucidated. In addition, we evaluated the impact of the concomitant use of individual PPIs and clopidogrel on cardiovascular event rates. To date, there have been few large-scale Asian studies on the interaction of PPI and clopidogrel on cardiovascular outcomes, by using various study designs, including the analysis of individual PPIs at the population level.
Our study results are consistent with a recent meta-analysis including 22 studies [14]. The study revealed that concomitant use of PPI with thienopyridines was associated with increased risk of stroke (hazard ratios adjusted, 1.30; 95% CI, 1.04-1.61; P=0.02), composite stroke/MI/cardiovascular death (hazard ratios adjusted, 1.23; 95% CI, 1.03-1.47; P=0.02), but not with MI (hazard ratios adjusted, 1.19; 95% CI, 0.93-1.52; P=0.16) [14]. In the UK General Practice Research Database cohort study, the hazard ratio for the association between PPI use and death or MI incidence was 1.37 (95% CI, 1.27-1.48), but there was a lack of specific association in the self-controlled case series analysis [17]. On the contrary, meta-analyses of studies published in 2012–2016 showed that combined use of clopidogrel with PPI is associated with significantly higher adverse cardiovascular events, such as major adverse cardiac events (MACE), stent thrombosis, and MI following PCI [32]. However, most of these studies were Western observational studies, and the types of PPI were distributed heterogeneously [32].
Notably, CYP2C19 is subject to genotypic variation, with some individuals and ethnicities having naturally poor 2C19 metabolic activity. CYP2C19 poor metabolic phenotypes are found in 13–23% of healthy East Asian populations but in only 2–5% of Caucasians [12]. A recent meta-analysis evaluated the effect of concomitant use of dual antiplatelet therapy and PPI and assessed the effect of ethnic variance on clinical outcomes [33]. The PPI co-medication was associated with increased risk for all endpoints among Caucasian population; however, there was no association with increased risk for MACE, all-cause death, and cardiac death among Asian populations [33]. In another 12,440 multi-ethnic Asian population study, the risk of subsequent MI was higher in the Malay and Chinese populations than in the Indian population [9]. Our study was the first, large-scale, observational study of the interaction between PPI and clopidogrel on cardiovascular outcomes in the Korean population.
After the FDA’s warnings against the use of clopidogrel with inhibiting PPIs (omeprazole and esomeprazole), treatment with inhibiting PPIs and clopidogrel has continued to decrease since 2010 [22]. To date, however, there have been few studies comparing the impact of individual PPIs with clopidogrel on cardiovascular outcomes, and conflicting results have been reported [34]. In our study, the impact of individual PPIs on stroke and MI showed different patterns. Esomeprazole had the highest RR, followed by rabeprazole, omeprazole, and pantoprazole in recurrent stroke. Lansoprazole and dexlansoprazole were not significantly associated with recurrent strokes. In contrast, only pantoprazole showed a significant risk of recurrent MI. However, our results should be interpreted with caution because the sample size of individual PPIs was relatively small in the analysis of recurrent MI. Therefore, it may be necessary to directly compare the impact of individual PPIs on clopidogrel in the future.
The main advantage of this study was the use of two different designs. The primary study design was a self-controlled case series, which removes all fixed confounding between individuals as the comparisons are made within an individual, relying on patients who have both exposed and unexposed periods for the main comparison [17]. We also performed self-controlled case series analysis according to PPI duration to show the dose-response relationship, while including PPI washout periods. The secondary study design was a large-scale PS-matching-based cohort study using the OMOP-CDM-based database. In the traditional cohort study, at baseline, PPI users tended to be older and have more comorbidities than non-users, despite adjusting for known confounding factors. The large-scale PS matching included all previously recorded comorbidities, all drugs, and Charlson comorbidity index scores before cohort entry as covariates, which enabled adjustment of unmeasured confounding factors [35]. In addition, multiple sensitivity analyses with different matching ratios and methods showed consistent results in the analysis of stroke; however, inconsistent results were obtained in the analysis of MI. The OMOP-CDM-based research also has the strength to be applied to other ethnic groups through the common analytic R code [36,37].
The present study had several limitations. First, we defined the recurrence of stroke or MI as hospitalization with a primary diagnostic code, which might have been overestimated. Moreover, the recurrence rates of stroke and MI in this study were higher than those reported in previous studies. Second, in the self-controlled case series, the event should not condition the probability of subsequent exposure [38]. To ensure this assumption, a “pre-exposure” time risk window can be created to examine whether or not the exposure depends on the occurrence of the outcome [38]. We could not establish a pre-exposure time period, therefore, there could be potential bias in the self-controlled case series design. Third, large-scale PS matching leads to inevitable case loss; thus, it might have influenced the statistically insignificant result in the analysis of MI. We also could not separate individual PPIs in the cohort study due to the small sample size. Finally, despite efforts to reduce confounding factors, the current study was an observational study. The possibility of misclassification or residual biases exists because of the limitations of the claim database.
In conclusion, PPI co-prescription for > 4 weeks with clopidogrel was associated with recurrent stroke in patients with stroke history. The risk showed an increasing trend parallel to the duration of PPI use and differed according to individual PPI types. However, the association with recurrent MI in the PPI co-prescription group did not show consistent results in the multiple analyses. Further comprehensive large-scale studies, including multiple races and ethnicities, are required.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
This work was partly supported by the Korean College of Helicobacter and Upper Gastrointestinal Research Foundation Grant (Grant Number, KCHUGR 202102003) and the National Health Insurance Service Ilsan Hospital Grant (NHIMC 2020-20-020).
Conflicts of Interest
None.
References
- Scally, B.; Emberson, J.R.; Spata, E.; Reith, C.; Davies, K.; Halls, H.; Holland, L.; Wilson, K.; Bhala, N.; Hawkey, C.; et al. Effects of gastroprotectant drugs for the prevention and treatment of peptic ulcer disease and its complications: a meta-analysis of randomised trials. Lancet Gastroenterol Hepatol 2018, 3, 231–241. [Google Scholar] [CrossRef]
- Katz, P.O.; Dunbar, K.B.; Schnoll-Sussman, F.H.; Greer, K.B.; Yadlapati, R.; Spechler, S.J. ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease. The American journal of gastroenterology 2022, 117, 27–56. [Google Scholar] [CrossRef]
- Iwakiri, K.; Fujiwara, Y.; Manabe, N.; Ihara, E.; Kuribayashi, S.; Akiyama, J.; Kondo, T.; Yamashita, H.; Ishimura, N.; Kitasako, Y.; et al. Evidence-based clinical practice guidelines for gastroesophageal reflux disease 2021. J Gastroenterol 2022, 57, 267–285. [Google Scholar] [CrossRef]
- Jung, H.K.; Tae, C.H.; Song, K.H.; Kang, S.J.; Park, J.K.; Gong, E.J.; Shin, J.E.; Lim, H.C.; Lee, S.K.; Jung, D.H.; et al. 2020 Seoul Consensus on the Diagnosis and Management of Gastroesophageal Reflux Disease. J Neurogastroenterol Motil 2021, 27, 453–481. [Google Scholar] [CrossRef]
- Abraham, N.S.; Hlatky, M.A.; Antman, E.M.; Bhatt, D.L.; Bjorkman, D.J.; Clark, C.B.; Furberg, C.D.; Johnson, D.A.; Kahi, C.J.; Laine, L.; et al. ACCF/ACG/AHA 2010 expert consensus document on the concomitant use of proton pump inhibitors and thienopyridines: a focused update of the ACCF/ACG/AHA 2008 expert consensus document on reducing the gastrointestinal risks of antiplatelet therapy and NSAID use. A Report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. J Am Coll Cardiol 2010, 56, 2051–2066. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Kandulski, A.; Venerito, M. Proton-pump inhibitors: understanding the complications and risks. Nat Rev Gastroenterol Hepatol 2017, 14, 697–710. [Google Scholar] [CrossRef]
- Vaezi, M.F.; Yang, Y.X.; Howden, C.W. Complications of Proton Pump Inhibitor Therapy. Gastroenterology 2017, 153, 35–48. [Google Scholar] [CrossRef]
- Savarino, V.; Marabotto, E.; Zentilin, P.; Furnari, M.; Bodini, G.; De Maria, C.; Pellegatta, G.; Coppo, C.; Savarino, E. Proton pump inhibitors: use and misuse in the clinical setting. Expert Rev Clin Pharmacol 2018, 11, 1123–1134. [Google Scholar] [CrossRef]
- Muthiah, M.D.; Zheng, H.L.; Chew, N.W.S.; Xiao, J.L.; Lim, L.G.; Tan, H.C.; Lee, C.H.; Low, A.F.; Foo, L.L.; Richards, A.M.; et al. Outcomes of a multi-ethnic Asian population on combined treatment with clopidogrel and omeprazole in 12,440 patients. J Thromb Thrombolys 2021. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Cryer, B.L.; Contant, C.F.; Cohen, M.; Lanas, A.; Schnitzer, T.J.; Shook, T.L.; Lapuerta, P.; Goldsmith, M.A.; Laine, L.; et al. Clopidogrel with or without omeprazole in coronary artery disease. The New England journal of medicine 2010, 363, 1909–1917. [Google Scholar] [CrossRef]
- Vaduganathan, M.; Cannon, C.P.; Cryer, B.L.; Liu, Y.; Hsieh, W.H.; Doros, G.; Cohen, M.; Lanas, A.; Schnitzer, T.J.; Shook, T.L.; et al. Efficacy and Safety of Proton-Pump Inhibitors in High-Risk Cardiovascular Subsets of the COGENT Trial. The American journal of medicine 2016, 129, 1002–1005. [Google Scholar] [CrossRef]
- Zou, D.; Goh, K.L. East Asian perspective on the interaction between proton pump inhibitors and clopidogrel. Journal of gastroenterology and hepatology 2017, 32, 1152–1159. [Google Scholar] [CrossRef]
- Goodman, S.G.; Clare, R.; Pieper, K.S.; Nicolau, J.C.; Storey, R.F.; Cantor, W.J.; Mahaffey, K.W.; Angiolillo, D.J.; Husted, S.; Cannon, C.P.; et al. Association of proton pump inhibitor use on cardiovascular outcomes with clopidogrel and ticagrelor: insights from the platelet inhibition and patient outcomes trial. Circulation 2012, 125, 978–986. [Google Scholar] [CrossRef]
- Malhotra, K.; Katsanos, A.H.; Bilal, M.; Ishfaq, M.F.; Goyal, N.; Tsivgoulis, G. Cerebrovascular Outcomes With Proton Pump Inhibitors and Thienopyridines: A Systematic Review and Meta-Analysis. Stroke 2018, 49, 312–318. [Google Scholar] [CrossRef]
- Ho, P.M.; Maddox, T.M.; Wang, L.; Fihn, S.D.; Jesse, R.L.; Peterson, E.D.; Rumsfeld, J.S. Risk of adverse outcomes associated with concomitant use of clopidogrel and proton pump inhibitors following acute coronary syndrome. Jama 2009, 301, 937–944. [Google Scholar] [CrossRef]
- Rassen, J.A.; Choudhry, N.K.; Avorn, J.; Schneeweiss, S. Cardiovascular outcomes and mortality in patients using clopidogrel with proton pump inhibitors after percutaneous coronary intervention or acute coronary syndrome. Circulation 2009, 120, 2322–2329. [Google Scholar] [CrossRef]
- Douglas, I.J.; Evans, S.J.; Hingorani, A.D.; Grosso, A.M.; Timmis, A.; Hemingway, H.; Smeeth, L. Clopidogrel and interaction with proton pump inhibitors: comparison between cohort and within person study designs. BMJ 2012, 345, e4388. [Google Scholar] [CrossRef]
- Pang, J.; Wu, Q.; Zhang, Z.; Zheng, T.Z.; Xiang, Q.; Zhang, P.; Liu, X.; Zhang, C.; Tan, H.; Huang, J.; et al. Efficacy and safety of clopidogrel only vs. clopidogrel added proton pump inhibitors in the treatment of patients with coronary heart disease after percutaneous coronary intervention: A systematic review and meta-analysis. Int J Cardiol Heart Vasc 2019, 23, 100317. [Google Scholar] [CrossRef]
- Lima, J.J.; Thomas, C.D.; Barbarino, J.; Desta, Z.; Van Driest, S.L.; El Rouby, N.; Johnson, J.A.; Cavallari, L.H.; Shakhnovich, V.; Thacker, D.L.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2C19 and Proton Pump Inhibitor Dosing. Clin Pharmacol Ther 2021, 109, 1417–1423. [Google Scholar] [CrossRef]
- Sibbing, D.; Morath, T.; Stegherr, J.; Braun, S.; Vogt, W.; Hadamitzky, M.; Schömig, A.; Kastrati, A.; von Beckerath, N. Impact of proton pump inhibitors on the antiplatelet effects of clopidogrel. Thromb Haemost 2009, 101, 714–719. [Google Scholar]
- Siller-Matula, J.M.; Spiel, A.O.; Lang, I.M.; Kreiner, G.; Christ, G.; Jilma, B. Effects of pantoprazole and esomeprazole on platelet inhibition by clopidogrel. Am Heart J 2009, 157, 148–e141. [Google Scholar] [CrossRef]
- Farhat, N.; Haddad, N.; Crispo, J.; Birkett, N.; McNair, D.; Momoli, F.; Wen, S.W.; Mattison, D.R.; Krewski, D. Trends in concomitant clopidogrel and proton pump inhibitor treatment among ACS inpatients, 2000-2016. Eur J Clin Pharmacol 2019, 75, 227–235. [Google Scholar] [CrossRef]
- Song, S.O.; Jung, C.H.; Song, Y.D.; Park, C.Y.; Kwon, H.S.; Cha, B.S.; Park, J.Y.; Lee, K.U.; Ko, K.S.; Lee, B.W. Background and data configuration process of a nationwide population-based study using the korean national health insurance system. Diabetes Metab J 2014, 38, 395–403. [Google Scholar] [CrossRef]
- Lee, Y.H.; Han, K.; Ko, S.H.; Ko, K.S.; Lee, K.U. Data Analytic Process of a Nationwide Population-Based Study Using National Health Information Database Established by National Health Insurance Service. Diabetes Metab J 2016, 40, 79–82. [Google Scholar] [CrossRef]
- You, S.C.; Lee, S.; Cho, S.Y.; Park, H.; Jung, S.; Cho, J.; Yoon, D.; Park, R.W. Conversion of National Health Insurance Service-National Sample Cohort (NHIS-NSC) Database into Observational Medical Outcomes Partnership-Common Data Model (OMOP-CDM). Studies in health technology and informatics 2017, 245, 467–470. [Google Scholar]
- Hripcsak, G.; Duke, J.D.; Shah, N.H.; Reich, C.G.; Huser, V.; Schuemie, M.J.; Suchard, M.A.; Park, R.W.; Wong, I.C.; Rijnbeek, P.R.; et al. Observational Health Data Sciences and Informatics (OHDSI): Opportunities for Observational Researchers. Studies in health technology and informatics 2015, 216, 574–578. [Google Scholar]
- Seo, S.I.; Park, C.H.; You, S.C.; Kim, J.Y.; Lee, K.J.; Kim, J.; Kim, Y.; Yoo, J.J.; Seo, W.W.; Lee, H.S.; et al. Association between proton pump inhibitor use and gastric cancer: a population-based cohort study using two different types of nationwide databases in Korea. Gut 2021. [Google Scholar] [CrossRef]
- Park, D.H.; Seo, S.I.; Lee, K.J.; Kim, J.; Kim, Y.; Seo, W.W.; Lee, H.S.; Shin, W.G.; Yoo, J.J. Long-term proton pump inhibitor use and risk of osteoporosis and hip fractures: A nationwide population-based and multicenter cohort study using a common data model. J Gastroenterol Hepatol 2022, 37, 1534–1543. [Google Scholar] [CrossRef]
- Seo, S.I.; Park, C.H.; Kim, T.J.; Bang, C.S.; Kim, J.Y.; Lee, K.J.; Kim, J.; Kim, H.H.; You, S.C.; Shin, W.G. Aspirin, metformin, and statin use on the risk of gastric cancer: A nationwide population-based cohort study in Korea with systematic review and meta-analysis. Cancer Med 2022, 11, 1217–1231. [Google Scholar] [CrossRef]
- Whitaker, H.J.; Hocine, M.N.; Farrington, C.P. The methodology of self-controlled case series studies. Stat Methods Med Res 2009, 18, 7–26. [Google Scholar] [CrossRef]
- Tian, Y.; Schuemie, M.J.; Suchard, M.A. Evaluating large-scale propensity score performance through real-world and synthetic data experiments. International journal of epidemiology 2018, 47, 2005–2014. [Google Scholar] [CrossRef]
- Bundhun, P.K.; Teeluck, A.R.; Bhurtu, A.; Huang, W.Q. Is the concomitant use of clopidogrel and Proton Pump Inhibitors still associated with increased adverse cardiovascular outcomes following coronary angioplasty?: a systematic review and meta-analysis of recently published studies (2012 - 2016). BMC Cardiovasc Disord 2017, 17, 3. [Google Scholar] [CrossRef]
- Shi, W.C.; Yan, L.; Yang, J.G.; Yu, M.Y. Ethnic variance on long term clinical outcomes of concomitant use of proton pump inhibitors and clopidogrel in patients with stent implantation A PRISMA-complaint systematic review with meta-analysis. Medicine 2021, 100. [Google Scholar] [CrossRef]
- Lee, D.; Kim, J.S.; Kim, B.J.; Shin, S.Y.; Kim, D.B.; Ahn, H.S. Influence of individual proton pump inhibitors on clinical outcomes in patients receiving clopidogrel following percutaneous coronary intervention. Medicine (Baltimore) 2021, 100, e27411. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, Y.; Schuemie, M.J.; Blei, D.M.; Hripcsak, G. Adjusting for indirectly measured confounding using large-scale propensity score. Journal of biomedical informatics 2022, 134, 104204. [Google Scholar] [CrossRef]
- You, S.C.; Rho, Y.; Bikdeli, B.; Kim, J.; Siapos, A.; Weaver, J.; Londhe, A.; Cho, J.; Park, J.; Schuemie, M.; et al. Association of Ticagrelor vs Clopidogrel With Net Adverse Clinical Events in Patients With Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention. Jama 2020, 324, 1640–1650. [Google Scholar] [CrossRef]
- Suchard, M.A.; Schuemie, M.J.; Krumholz, H.M.; You, S.C.; Chen, R.; Pratt, N.; Reich, C.G.; Duke, J.; Madigan, D.; Hripcsak, G.; et al. Comprehensive comparative effectiveness and safety of first-line antihypertensive drug classes: a systematic, multinational, large-scale analysis. Lancet (London, England). [CrossRef]
- Requena, G.; Douglas, I.J.; Huerta, C.; de Abajo, F. Impact of pre-exposure time bias in self-controlled case series when the event conditions the exposure: Hip/femur fracture and use of benzodiazepines as a case study. Pharmacoepidemiol Drug Saf 2020, 29, 388–395. [Google Scholar] [CrossRef]
Table 2.
Relative risk for hospitalization with stroke or myocardial infarction during PPI exposure according to PPI duration (self-controlled case series analysis).
Table 2.
Relative risk for hospitalization with stroke or myocardial infarction during PPI exposure according to PPI duration (self-controlled case series analysis).
| Stroke | Myocardial infarction | |||
|---|---|---|---|---|
| Number of events | Relative risk (95% CI) | Number of events | Relative risk (95% CI) | |
| Total events | 1448 | 208 | ||
| RR of PPIs exposed periods (PPIs co-prescribed periods only) | ||||
| PPIs unexposed | 795 | 1 (reference) | 113 | 1 (reference) |
| Overall | 653 | 2.09 (1.83-2.38) | 95 | 1.47 (1.02-2.11) |
| 0~2 weeks | 254 | 1.76 (1.50-2.07) | 32 | 1.30 (0.83-2.04) |
| 2~4 weeks | 187 | 2.02 (1.68-2.43) | 16 | 0.95 (0.54-1.69) |
| 4~6 weeks | 90 | 3.02 (2.36-3.86) | 19 | 2.33 (1.32-4.13) |
| 6~8 weeks | 47 | 2.81 (2.02- 3.92) | 11 | 1.99 (0.98-4.03) |
| >8 weeks | 75 | 5.57 (4.06-7.64) | 17 | 3.80 (1.93-7.45) |
| RR of PPIs exposed periods (included PPIs washout periods) | ||||
| Non-risk periods | 594 | 1 (reference) | 85 | 1 (reference) |
| Risk-periods | 854 | 2.47 (2.16-2.81) | 123 | 1.87 (1.31-2.65) |
Table 3.
Relative risk for hospitalization with stroke or myocardial infarction during PPI exposure according to PPI type (self-controlled case series analysis).
Table 3.
Relative risk for hospitalization with stroke or myocardial infarction during PPI exposure according to PPI type (self-controlled case series analysis).
| Type of PPIs | Stroke | Myocardial infarction | |||
|---|---|---|---|---|---|
| Number of events | Relative risk (95% CI) | Number of events | Relative risk (95% CI) | ||
| Omeprazole | PPIs unexposed | 83 | 1 (reference) | 7 | 1 (reference) |
| Overall | 54 | 1.84 (1.18-2.86) | 2 | 0.33 (0.47-2.34) | |
| Non-risk periods | 64 | 1 (reference) | 5 | 1 (reference) | |
| Risk periods including washout periods | 73 | 2.03 (1.34-3.08) | 4 | 1.04 (0.13-8.40) | |
| Esomeprazole | PPIs unexposed | 181 | 1 (reference) | 29 | 1 (reference) |
| Overall | 192 | 2.75 (2.12-3.57) | 21 | 0.89 (0.36-2.18) | |
| Non-risk periods | 128 | 1 (reference) | 23 | 1 (reference) | |
| Risk periods including washout periods | 245 | 3.18 (2.45-4.11) | 27 | 1.18 (0.52-2.65) | |
| Pantoprazole | PPIs unexposed | 213 | 1 (reference) | 42 | 1 (reference) |
| Overall | 151 | 1.61 (1.21-2.13) | 40 | 2.56 (1.46-4.50) | |
| Non-risk periods | 175 | 1 (reference) | 35 | 1 (reference) | |
| Risk periods including washout periods | 189 | 1.80 (1.37-2.35) | 47 | 2.53 (1.47-4.36) | |
| Rabeprazole | PPIs unexposed | 295 | 1 (reference) | 39 | 1 (reference) |
| Overall | 197 | 1.88 (1.49-2.36) | 19 | 1.11(0.54–2.24) | |
| Non-risk periods | 232 | 1 (reference) | 32 | 1 (reference) | |
| Risk periods including washout periods | 260 | 2.02 (1.62-2.52) | 24 | 1.14 (0.54-1.98) | |
| Lansoprazole | PPIs unexposed | 121 | 1 (reference) | 21 | 1 (reference) |
| Overall | 49 | 1.32 (0.87-2.01) | 11 | 0.58 (0.22-1.52) | |
| Non-risk periods | 99 | 1 (reference) | 16 | 1 (reference) | |
| Risk periods including washout periods | 71 | 1.63 (1.12-2.38) | 16 | 0.87 (0.33-2.24) | |
| Dexlansoprazole | PPIs unexposed | 9 | 1 (reference) | 0 | 1 (reference) |
| Overall | 3 | 1.08 (0.18-6.49) | 2 | NA | |
| Non-risk periods | 6 | 1 (reference) | 0 | 1 (reference) | |
| Risk periods including washout periods | 6 | 3.65 (0.71-8.78) | 2 | NA | |
PPI, proton pump inhibitors; NA, not applicable.
Table 4.
Cox regression analysis for recurrent stroke and myocardial infarction during 1 year after PPI co-prescription (cohort study).
Table 4.
Cox regression analysis for recurrent stroke and myocardial infarction during 1 year after PPI co-prescription (cohort study).
| Outcome | Cohort | Patients, n | Observation, person-years | Events | Incidence ratea | HR (95% CI) | P-value |
|---|---|---|---|---|---|---|---|
| Stroke | PPI | 373 | 240 | 81 | 337.5 | 1.34 (1.01-1.76) | 0.04 |
| Non-PPI | 1,051 | 740 | 189 | 255.2 | Reference | ||
| Myocardial infarction | PPI | 179 | 133 | 23 | 171.7 | 1.42 (0.79-2.49) | 0.23 |
| Non-PPI | 439 | 336 | 43 | 127.8 | Reference |
a Incidence rate expressed per 1,000 person-years. PPI, proton pump inhibitor; HR, hazard ratio.
Table 5.
Sensitivity analysis with different matching ratios, observation periods, and stratifications (cohort study).
Table 5.
Sensitivity analysis with different matching ratios, observation periods, and stratifications (cohort study).
| Analysis | Observation period | Stroke HR (95% CI) |
Myocardial infarction HR (95% CI) |
|---|---|---|---|
| PS matching 1:4(main analysis) | 12 months | 1.34 (1.01-1.76) | 1.42 (0.79-2.49) |
| 1:4 | 6 months | 1.42 (1.05-1.90) | 2.15 (1.10-4.13) |
| 1:1 | 12 months | 1.52 (1.06-2.20) | 1.33 (0.69-2.65) |
| 1:1 | 6 months | 1.56 (1.07-2.30) | 2.12 (0.95-5.21) |
| PS stratification | 12 months | 1.37 (1.08-1.73) | 1.15 (0.71-1.81) |
| 6 months | 1.43 (1.10-1.84) | 1.69 (0.96-2.92) |
PS, propensity score; HR, hazard ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



