
Submitted:
24 July 2023
Posted:
25 July 2023
You are already at the latest version
Abstract
Background: Post-delivery period could be characterized by psychological distress (e.g., anxiety, sadness, and irritability), leading to post-partum depression (PPD). Objective: The present clinical study assess the effect of probiotic supplementation containing Limosilactobacillus reuteri PBS072 and Bifidobacterium breve BB077 (4x109 CFU/day) on mother’s mood and breastfeeding quality during the first trimester after delivery. Methods: A Randomized Double Blind Controlled (RDBPC) trial has been carried out in 200 healthy new mothers divided into an active group taking a supplement containing Limosilactobacillus reuteri PBS072 and Bifidobacterium breve BB077 (4x109 CFU/day) plus multivitamins, and a control group (multivitamin complex only) for 90 days. Symptoms related to maternal depression and breastfeeding quality were evaluated at days 45 and 90 by Edinburgh Postnatal Depression Scale (EPDS) and Breastfeeding Self-Efficacy Scale Short-Form (BSES-SF). Results: At days 45 and 90, probiotic treatment significantly ameliorated the mothers’ mood compared to the control treatment (p<0.001). Likewise, breastfeeding quality and baby’s cries significantly improved in the probiotic group (p<0.001). Conclusions: Microbiota alterations could influence post-delivery woman’s mental state. According to our results, L. reuteri PBS072 and B. breve BB077 are potential candidates able to improve stress resilience in the post-partum period.
Keywords:
gut-brain axis
; post-partum
; depression
; Limosilactobacillus reuteri PBS072
; Bifidobacterium breve BB077
; delivery
; breastfeeding
; probiotics
1. Introduction
Postpartum depression (PPD) is a subtype of depressive disorder affecting a large number of women immediately after childbirth which could seriously compromise both mother and newborn’s health [1,2].
Around 60-80% of new mothers experience “baby blues” few days after delivery, a condition characterized by feelings of sadness, loneliness, worthlessness, restlessness, and anxiety which usually resolve within the first two weeks [3,4]. This temporary discomfort, characterized by unstable mood and crying crisis, is caused by the rapid hormonal and psychic adaptation processes happening the first weeks after childbirth. Sometimes these feelings persist for a longer period, leading to psychic fragility, stress and anxiety [5]. PPD is a long-lasting depressive disorder that occurs 4-6 weeks after childbirth in which women experience depressed mood, loss of interest and pleasure, loss of confidence and self-esteem, excessive guilt, difficulty concentrating, sleep and appetite disturbances [6]. The prevalence of PPD is around 10-20%, even if it varies according to different cultures and income levels of studied countries [7].
Generally, women are subjected to many biological variations after delivery, such as altered levels of sexual hormones (oestrogen and progesterone), lactogenic hormones (oxytocin and prolactin) and increased amount of stress hormones (e.g., cortisol), correlated with a dysregulation in the hypothalamic–pituitary–adrenal (HPA) axis [8]. However, these hormonal imbalances lead to the depression onset only for women with a predisposition for mood disorders [9]. Other factors playing a role in physiological changes after childbirth are neurotransmission dysfunction (i.e., γ-aminobutyric acid or GABA and glutamate) and monoamine (i.e., serotonin and dopamine) [10]. Common changes in the mother’s normal daily routine, such as sleep disturbances and alteration of appetite, could lead to diurnal variations in mood, loss of concentration, and irritability, which altogether are possible cause of PPD development [7].
Another recurrent feeling that women might experience in the first trimester after delivery is the sense of guilt, arising from the difficulty to look after their baby. Even though this emotion has a serious impact on both mother and child’s lives, it is very often underestimated and it is not reported by women because of the fear to be labelled as "bad mothers” [11].
The first six months after birth have a pivotal role in child’s physical and psychological development. For this reason, PPD can have serious consequences on the baby. Uncertain affection, reduced psychomotor and cognitive development are just some of the possible effects, which can globally affect the infant’s development, especially in terms of intelligence and language learning ability [1,12]. One of the most important leading consequence of women’s depressive mood after delivery is the difficulty in lactation [13]. Breastfeeding is of paramount importance both for the newborn’s optimal immune system development, and for the mother’s health, since it reduces type 2 diabetes, cardiovascular risk, and breast and ovarian cancer development [14,15]. Sometimes lactation could cause mastitis, an inflammation of breast tissue, usually followed by infection. It is a common and debilitating disease which often comes with the cessation of exclusive breastfeeding. Mastitis and breast abscesses are usually associated with the pathogens Staphylococcus aureus, Staphylococcus epidermidis and some members of Corynebacteria that are known to produce biofilms and show multidrug resistance. For these reasons, antibiotic treatment is frequently ineffective, causing in many cases breastfeeding cessation [16,17,18].
Nowadays, PPD current best practices involve pharmacological interventions, cognitive therapy, psychological support and, in worst cases, hospitalization [19]. Thus, the development of non-invasive and non-harmful treatments to support new-mothers’ health is eagerly required.
In this scenario, probiotics have been extensively studied due to their ability to improve gut microbiota (GM) and eubiosis. Indeed, such microorganisms affect host’s health, influencing both the gastro-intestinal and the immune system [20,21]. Bacteria living in the gut are also able to modulate the brain functions through a bi-directional communication pathway, named “gut-brain axis” [22]. Such pathway includes neuroendocrine secretions, short-chain fatty acid production and autonomic nervous system stimulation [23]. Consequently, intestinal dysbiosis can be associated to a wide range of psychological problems, including neuropsychiatric disorders, depression, and anxiety, that are characterized by increased levels of pro-inflammatory cytokines and oxidative stress [24,25]. Thus, an alteration of the intestinal microbial composition can affect the gut-brain communication, leading to the onset of depressive disorders [26].
In vitro studies suggest that Limosilactobacillus reuteri PBS072 and Bifidobacterium breve BB077 can influence the endogenous production of GABA and serotonin and improve stress-related parameters. Following these promising results, two clinical trials have been carried-out in different target population, such as stressed students during exam session and employees in the early pandemic, showing an improvement in cognitive functions, mood and sleep quality [27,28].
The primary aim of the present study was to determine if a probiotic supplement containing Limosilactobacillus reuteri PBS072 and Bifidobacterium breve BB077 could improve new mothers’ psychological and physical well-being by reducing the risk of developing PPD, through the modulation of the gut-brain-axis. As a secondary outcome, self-confidence and breastfeeding ease were evaluated as a marker of mothers’ mental state in the post-partum period. Indeed, these two outcomes are related to lactation performance, decreasing excessive baby crying and reducing the production of intestinal gas (i.e. infant colic), due to a relaxed attitude of the new mothers.
2. Materials and Methods
2.1. Study design, population and products
A multicentre randomized double-blind controlled clinical study was carried out in compliance with the Helsinki Declaration (1964) and its amendment. The study protocol was approved by the “Independent Ethical Committee for Non-Pharmacological Clinical Studies” (Genova, Italy). Written informed consent was obtained from all subjects before enrolment. The study was registered at ISRCTN registry (registration number: ISRCTN99047904). Subject enrolment was carried out between July 2020 and July 2021.
Two-hundred healthy pregnant women, aged between 18 and 50-year-old, were enrolled according to the inclusion and exclusion criteria reported in Table 1. Ten subjects drop out, thus a total of 190 subjects completed the treatment (95 for the active treatment and 95 for the control one). The average age of women was 32,54 ± 4,16 years. The study starts the day of first intake of the product (T0), within 3 (±1) days maximum after delivery. No adverse events were reported and both products used in this clinical study were well tolerated. The level of compliance to the treatment was high. Figure 1 shows a visual overview of the study design (flowchart).
Subjects were randomly assigned to 2 groups according to a randomization list previously generated using the statistic algorithm “Wey’s urn”. The two groups (95 subjects each) were provided with two different products as follows: one group used the probiotic plus multivitamin food supplement (active treatment), while the other group used the multivitamins food supplement only (control treatment). The active product contained: two probiotic strains, named Limosilactobacillus reuteri PBS072 and Bifidobacterium breve BB077, for a final dosage of 4*109 CFU/day (2*109 CFU for each strain); a multivitamin mix (vitamins B1, B2, B3, B5, B6, B9, B12, D, and E); dried corn starch, magnesium stearate, and silicon dioxide. The control treatment was composed by the same multivitamin mix as the active product plus maltodextrin, magnesium stearate, and silicon dioxide. Products were administered in form of capsules and subjects were instructed to take 1 capsule a day of the active/control product with a glass water (not sparkling water) away from meals. Participants were encouraged to maintain the habitual daily routine. If antibiotics were prescribed, women were encouraged to continue with their treatment regime, but advised to take the treatment at least 2 h after taking the antibiotic. Clinical visits were scheduled as follow: initial visit-recruitment (T-1), start of the study – first product intake (T0), intermediate visit (i.e., 45 days after the beginning of the treatment T1), final visit (i.e., 90 days after the beginning of the treatment T2). The study schedule is reported in Table 2. During the initial visit, the gynaecologist invited the subjects to communicate the date of delivery (corresponding to the beginning of products intake), in order to plan the date for the intermediate and final visits. The study timeline is illustrated in Figure 2.
2.2. Outcome measures
Evaluation of depression-related symptoms was carried out by using the Edinburgh Postnatal Depression Scale (EPDS) [29]. EPDS is a 10-item self-reporting questionnaire developed by Cox et al. to identify women who may suffer from post-partum depression [30]. The 10 questions of the scale correspond to various clinical depression symptoms, such as feeling guilty, sleep disturbance, low energy, anhedonia, and suicidal ideation. Each answer is given a score ranging from 0 to 3, with a maximum score of 30 points; a score of 10 or above suggests an intensification of the depressive state [31]. A score of 12 is interpreted as “fairly high possibility of depression”.
Evaluation of breastfeeding quality was performed using the Breastfeeding Self-Efficacy Scale-Short Form (BSES-SF) reported by Rashid et al. [32]. The BSES-SF is a 14-item instrument developed to measure breastfeeding confidence, based on a 5-point Likert-type scale, ranging from 1 (not at all confident) to 5 (always confident), with a maximum score of 70. The higher is the score, the better is the quality of breastfeeding. In addition to the 14 items of the BSES-SF, three more questions were added regarding the crying/fussing and possible mastitis events. Mothers were asked to report, with yes or no, if they noted improvement. Furthermore, subjects were invited to quantify the average daily number of baby crying episodes during the treatment.
Questionnaires were completed at T1 and T2. At T0 no questionnaire was filled since generally depression symptoms appear within 30-40 days from delivery [3].
2.3. Statistical analysis
Statistical analysis was performed using NCSS 10 Statistical Software (version 10.0.7 for Windows; NCSS, Kaysville, UT, USA) running on Windows Server 2008 R2 Standard SP1 64-bit edition (Microsoft, USA). Data normality was checked using Shapiro-Wilk W normality test and data shape. Intergroup (active vs control) comparisons were carried out using Mann-Whitney U test. Data were expressed as mean ± standard deviation (SD). A p-value <0.05 was considered statistically significant. Statistical analysis was carried out on raw data.
3. Results
3.1. Depression symptoms evaluation
The evaluation of depression symptoms was assessed by the Edinburgh Postnatal Depression Scale, after 45 and 90 days of active/control treatment (T1 and T2, respectively). At T1, the active treatment group reach a total score underneath the limit of minor depression (i.e., 10 points) with an average score of 9.0±4.8, while the control group reached a mean value of 12.1±5.9 points. The result obtained for the active treatment was significantly lower than the control (p<0.001; Figure 3). This difference was even more evident at T2. At this time point, the use of the probiotic treatment produced a significantly lower average score of 7.0±3.3 if compared to control group which scored a mean value of 10.8±6.2 (p<0.001; Figure 3).
3.2. Breastfeeding quality assessment
The breastfeeding quality was determined using the BSES-SF questionnaire filled by subjects after 45 and 90 days of treatment. The active product showed a spoignificant improvement in the average score obtained with respect to control already at T1 (51.46±9.1 vs. 42.80±10.7, respectively, with p<0.001; Figure 2). After 90 days of treatment, probiotics seemed to still exert a positive significant effect on the breastfeeding quality (p<0.001), reaching an average value of 56,37±7,9, while at the same time the control average score was 45,48±11,9 (Figure 4).
3.4. Baby’s crying/fussing events
Regarding the daily improvement of crying/fussing events, a positive effect was observed in the group treated with probiotics. At T1, considering the positive answer to item 15 the of the BSES-SF questionnaire (assessing the crying/fussing events during the treatment), 81% of active group reported an improvement in comparison to the 42% obtained in the control group (Table 3). The difference in the percentage of positive answers was confirmed also at T2, where active and control group reached 78% and 43%, respectively. In addition, the average number of crying/fussing events was significantly lower (p<0.001) in the probiotic treated group with respect to the multivitamin product, both at T1 and T2 (Figure 5).
4. Discussion
According to the World Health Organization, stress has been defined as the “Health Epidemic of the 21st Century”. Indeed, the physical and psychological burden caused by long stress period is increasing [33]. Stressful situation can affect quality of sleep, provoking fatigue, irritability, and concentration difficulties. Moreover, stress may lead to intestinal dysbiosis and modify the GM, and consequently the gut-brain communication. Therefore, keeping a balanced gut-microbiota through probiotic supplementation could be a valid solution to achieve an effective gut-brain crosstalk, resulting in an improvement of mental conditions, as reported by previous studies [22,34,35]. Studies on animal models of depression reveal that GM in depressed mice changes significantly from healthy subjects. Indeed, GM modulates neuro-inflammatory activity in the hippocampus through a dysfunctional microbiota-gut-brain axis, leading to anxiety- and depression-like phenotypes [36]. Similarly, a study revealed that fecal microbiota transplantation (FMT) from human patients with major depressive disorder (MDD) into rats could induce a depressive-like phenotype in the recipient animals [37]. Rats receiving the FMT from depressed humans showed significantly higher immobility and less struggling in the forced swim test than rats receiving FMT from healthy human donors, a behavior interpreted as depressive phenotype. Furthermore, the former group showed an altered intestinal tight junction gene expression compared to animals receiving FTM from healthy donors [37]. These data highlight the key role of microbiota in modulating depression.
Nowadays, it is well-known that probiotics supplementation in women at the last trimester of gestation and breastfeeding shape newborns’ immune system. According to the 2015 World Allergy Organization guidelines, pregnant women whose infants are at high risk for allergy should assume probiotics as a preventive treatment. Indeed, probiotic integration positively stimulates the children’s immune system, decreasing in the onset of allergic diseases [38].
The majority of scientific studies available in literature evaluating the immune system response and the GM composition of new-born babies involve women taking probiotic supplements, especially during the perinatal period [39]. Thus, the effect of probiotic supplementation both during pregnancy and in the puerperium have been rarely assessed. Indeed, in the puerperium, mothers experience several physiological changes that could lead to stress and anxiety. Progesterone and estrogen, two hormones increasing tenfold during pregnancy, dramatically drop after the delivery. This condition could persist for 3-4 weeks and it is related to many changes in the mother’s life, such as diurnal variations in mood, poor concentration, and irritability [7]. Usually this condition self-resolves without any intervention, but sometimes these mental states could last longer, leading to more serious discomforts, such as PPD [5].
The aim of our study was to assess if a supplement containing Limosilactobacillus reuteri PBS072 and Bifidobacterium breve BB077 plus multivitamins may provide a safe support to new mothers after delivery, especially improving their mental state. Indeed, we observed the effect on mood of two probiotic strains administered to mothers immediately after delivery, in order to prevent the onset of depressive and anxious symptoms linked to PPD development, together with the indirect influence of the probiotic intake on new-born during the first trimester.
The evidence that women supplemented with probiotics had fewer symptoms of postnatal anxiety and depression caused by stress is consistent with two previous clinical studies evaluating the effect of probiotics on stress-related parameters in different target populations. The first study is a proof-of-concept trial of 30 students enrolled during exam session and treated with a probiotic supplement containing the same strains L. reuteri PBS072 and B. breve BB077. Results show an improvement in their cognitive function and sleep quality [27]. In the second study, Nobile et al. reported the improvement of the general mood state, anger, and tension feelings, as well as sleep quality, in employees administered with the same probiotic blend during pandemic lockdown, suggesting their potential role in the management of work-related stress [28].
According to these preliminary evidence, our study was designed to assess the effect of probiotics on mood and mental state in the period in which first PPD symptoms emerge. It is worth to notice that the clinical protocol could not include evaluation questionnaires at T0 since they are not relevant before the occurring of different and opposite emotional events (e.g., excitement and joy up to weakness and frightening due to motherhood). However, this study demonstrated a significant improvement of mothers’ mood in the first trimester when supplemented with Limosilactobacillus reuteri PBS072, Bifidobacterium breve BB077, and vitamins compared to the control group in accordance to the EPDS questionnaire (26% at T1 and 35% at T2, respectively). In addition, the probiotic group at T1 resulted in a total score underneath the threshold of minor depression, while the control group reached a mean value of 12, which is interpreted as “fairly high possibility of depression” on the EPDS [30]. On the same way, this study demonstrated a significant improvement in breastfeeding quality in the probiotic group in accordance to the BSES-SF (20% at T1 and 24% at T2, respectively). This questionnaire is associated with the self-confidence during breastfeeding, assessed as lactation performance in new-mothers.
Remarkably, this study showed a significant daily improvement in baby crying/fussing events (p<0.001), according to the BSES-SF questionnaire at both T1 and T2 for the probiotic group. A possible explanation could be that probiotics may ameliorate mother’s mood, who being less stressed and happier, may differently perceive the crying episodes of their children in terms of episodes’ number and severity. Also, it could be speculated that more self-confident and calm mothers positively influence baby’s behavior. A further potential explanation of this outcome is that crying events could be possibly linked to reduction of infant colic mediated by the indirect probiotic intake through breastfeeding [40]. Scientific evidence correlates changes in the GM with colicky infants, thus the use of probiotics to counteract this disorder has rapidly increased in recent years, focusing on the reduction of crying time as a primary outcome [41,42,43]. It is well known that bacteria present in the breast milk are transferred from the mother’s intestine to the mammary gland, and consequently from the mother milk to the infant gut [39]. In this context, a balanced microbiota in the mother’s gut could influence the growth of the child’s resident bacterial population, preventing intestinal gases production. Therefore, probiotic assumption might reduce infant colic episodes, decreasing crying events and improving mother’s mood [44].
To the best of our knowledge, only another published study assessed PPD neurological parameters as a result of the effect that probiotics in new mothers. This study investigated the effect of Lactobacillus rhamnosus HN001 on postpartum depression and anxiety symptoms using EPDS and State Trait Anxiety Inventory (STAI) questionnaires [34]. Slykerman and colleagues studied the oral intake of a probiotic supplement throughout the entire perinatal period, up to 6 months from delivery. The data of this study were collected retrospectively the occurring of the events (up to 6 months later). Due to the latency between the effective occurring event and its registration, this design could be a limitation of the study since mothers could have not remembered correctly the events throughout the long administration/ observational period.
In our study, the questionnaires used for the assessment of mothers’ mood state and breastfeeding confidence lack of the basal score, as selected questionnaires only refer to post-natal period; indeed, they could not be properly filled at T0 since mothers have just undergone delivery, without experiencing the wide range of emotional events linked to motherhood yet. For this reason, no evaluation was performed at T0 in order to avoid any alteration of the EPDS and BSES-EF questionnaires.
As secondary outcome, mastitis incidence was taken into consideration to further characterize the lactation performance. However, since the two items of BSES-SF questionnaire related to mastitis did not record any episodes, this outcome was not considered.
5. Conclusions
The mechanism by which probiotics modulate the mood is still to be clarified; however, growing evidences suggest their influence on the gut-brain axis.
The aim of the present study was to further investigate the efficacy of the two probiotics strains in a transitory stress condition as the post-partum. For this reason, early PPD could be considered as a novel condition to explore, considering its high prevalence in developed countries.
Our study provides evidence that the administration of a probiotic supplement containing L. reuteri PBS072 and B. breve BB077 could reduce the possibility to develop anxiety and stress in mothers after delivery, and prevent from the onset of PPD. To support these promising results, further studies are required to define the specific mechanism of action.
Author Contributions
Conceptualization, F.V. and V.D.L.; investigation, M.T. and V.D.L.; data curation, M.T. and V.D.L.; writing—original draft preparation, F.V., P.M., M.T. and V.D.L.; writing—review and editing, F.V., P.M., M.T., G.C, L.L, and V.D.L.; supervision, F.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. The APC was funded by Synbalance srl.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Indipendent Ethical Committee for Non-Pharmacological Clinical Studies, Genova, Italy (protocol code K.E.HU.NN.NGN00.000.00.00_2019/FV, approved on 13/11/2019). The study was registered at ISRCTN registry with the following registration number: ISRCTN99047904.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors would like to express their gratitude to dr. Vincenzo Nobile for its professionalism and support on the statistical analysis of data, and Roelmi HPC for providing probiotic and multivitamin products.
Conflicts of Interest
Patrizia Malfa is a Synbalance srl employee. She had no role in the design of the study, the collection, analyses or interpretation of data; she contributed to the writing of the manuscript.
References
- Abdollahi, F.; Rezai Abhari, F.; Zarghami, M. Post-Partum Depression Effect on Child Health and Development. Acta Med Iran. 2017, 55, 109–114. [Google Scholar] [PubMed]
- Guintivano, J.; Sullivan, P.F.; Stuebe, A.M.; Penders, T.; Thorp, J.; Rubinow, D.R.; Meltzer-Brody, S. Adverse life events, psychiatric history, and biological predictors of postpartum depression in an ethnically diverse sample of postpartum women. Psychol Med. 2018, 48, 1190–1200. [Google Scholar] [CrossRef] [PubMed]
- Mughal, S.; Azhar, Y.; Siddiqui, W. Postpartum Depression. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022; Volume 7. [Google Scholar]
- Manjunath, N.G.; Venkatesh, G.; Rajanna, *!!! REPLACE !!!*. Postpartum Blue is Common in Socially and Economically Insecure Mothers. Indian J Community Med. 2011, 36, 231–233. [Google Scholar] [CrossRef] [PubMed]
- Kołomańska-Bogucka, D.; Mazur-Bialy, A.I. Physical Activity and the Occurrence of Postnatal Depression-A Systematic Review. Medicina. 2019, 55, 560. [Google Scholar] [CrossRef] [PubMed]
- Falana, S.D.; Carrington, J.M. Postpartum Depression: Are You Listening? Nurs Clin North Am. 2019, 54, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Anokye, R.; Acheampong, E.; Budu-Ainooson, A.; Obeng, E.I.; Akwasi, A.G. Prevalence of postpartum depression and interventions utilized for its management. Ann Gen Psychiatry. 2018, 17, 18. [Google Scholar] [CrossRef]
- Schiller, C.E.; Meltzer-Brody, S.; Rubinow, D.R. The role of reproductive hormones in postpartum depression. CNS Spectr. 2015, 20, 48–59. [Google Scholar] [CrossRef]
- Bloch, M.; Rotenberg, N.; Koren, D.; Klein, E. Risk factors associated with the development of postpartum mood disorders. J Affect Disord. 2005, 88, 9–18. [Google Scholar] [CrossRef]
- Payne, J.L.; Maguire, J. Pathophysiological mechanisms implicated in postpartum depression. Front Neuroendocrinol. 2019, 52, 165–180. [Google Scholar] [CrossRef]
- Çapik, A.; Durmaz, H. Fear of Childbirth, Postpartum Depression, and Birth-Related Variables as Predictors of Posttraumatic Stress Disorder After Childbirth. Worldviews Evid Based Nurs. 2018, 15, 455–463. [Google Scholar] [CrossRef]
- Slomian, J.; Honvo, G.; Emonts, P.; Reginster, J.Y.; Bruyère, O. Consequences of maternal postpartum depression: A systematic review of maternal and infant outcomes. Womens Health (Lond). 2019, 15, 1745506519844044. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, B.; Dias, C.C.; Brandão, S.; Canário, C.; Nunes-Costa, R. Breastfeeding and postpartum depression: state of the art review. J Pediatr (Rio J). 2013, 89, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Andreas, N.J.; Kampmann, B.; Mehring Le-Doare, K. Human breast milk: A review on its composition and bioactivity. Early Hum Dev. 2015, 91, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Dieterich, C.M.; Felice, J.P.; O'Sullivan, E.; Rasmussen, K.M. Breastfeeding and health outcomes for the mother-infant dyad. Pediatr Clin North Am. 2013, 60, 31–48. [Google Scholar] [CrossRef] [PubMed]
- Angelopoulou, A.; Field, D.; Ryan, C.A.; Stanton, C.; Hill, C.; Ross, R.P. The microbiology and treatment of human mastitis. Med Microbiol Immunol. 2018, 207, 83–94. [Google Scholar] [CrossRef]
- Arroyo, R.; Martín, V.; Maldonado, A.; Jiménez, E.; Fernández, L.; Rodríguez, J.M. Treatment of infectious mastitis during lactation: antibiotics versus oral administration of Lactobacilli isolated from breast milk. Clin Infect Dis. 2010, 50, 1551–1558. [Google Scholar] [CrossRef]
- Delgado, S.; Arroyo, R.; Jiménez, E.; Marín, M. L.; del Campo, R.; Fernández, L.; Rodríguez, J. M. Staphylococcus epidermidis strains isolated from breast milk of women suffering infectious mastitis: potential virulence traits and resistance to antibiotics. BMC Microbiol. 2009, 9, 82. [Google Scholar] [CrossRef]
- Fitelson, E.; Kim, S.; Baker, A.S.; Leight, K. Treatment of postpartum depression: clinical, psychological and pharmacological options. International journal of women's health. 2010, 3, 1–14. [Google Scholar]
- Valdes, A.M.; Walter, J.; Segal, E.; Spector, T.D. Role of the gut microbiota in nutrition and health. BMJ. 2018, 361, k2179. [Google Scholar] [CrossRef]
- Zheng, D.; Liwinski, T.; Elinav, E. Interaction between microbiota and immunity in health and disease. Cell Res. 2020, 30, 492–506. [Google Scholar] [CrossRef]
- Carabotti, M.; Scirocco, A.; Maselli, M.A.; Severi, C. The gut-brain axis: interactions between enteric microbiota, central and enteric nervous systems. Ann Gastroenterol. 2015, 28, 203–209. [Google Scholar] [PubMed]
- Dalile, B.; Van Oudenhove, L.; Vervliet, B.; Verbeke, K. The role of short-chain fatty acids in microbiota-gut-brain communication. Nat Rev Gastroenterol Hepatol. 2019, 16, 461–478. [Google Scholar] [CrossRef] [PubMed]
- Cenit, M.C.; Sanz, Y.; Codoñer-Franch, P. Influence of gut microbiota on neuropsychiatric disorders. World J Gastroenterol. 2017, 23, 5486–5498. [Google Scholar] [CrossRef]
- Capuco, A.; Urits, I.; Hasoon, J.; Chun, R.; Gerald, B.; Wang, J. K.; Kassem, H.; Ngo, A.L.; Abd-Elsayed, A.; Simopoulos, T.; Kaye, A.D.; Viswanath, O. Current Perspectives on Gut Microbiome Dysbiosis and Depression. Adv Ther. 2020, 37, 1328–1346. [Google Scholar] [CrossRef] [PubMed]
- Simpson, C.A.; Diaz-Arteche, C.; Eliby, D.; Schwartz, O.S.; Simmons, J.G.; Cowan, C.S.M. The gut microbiota in anxiety and depression - A systematic review. Clin Psychol Rev. 2021, 83, 101943. [Google Scholar] [CrossRef] [PubMed]
- Nobile, V.; Giardina, S.; Puoci, F. The Effect of a Probiotic Complex on the Gut-Brain Axis: A Translational Study. Neuropsychobiology. 2021, 30, 1–11. [Google Scholar]
- 28. Nobile V, Puoci F. Effect of a Multi-Strain Probiotic Supplementation to Manage Stress during the COVID-19 Pandemic: A Randomized, Double-Blind, Placebo-Controlled, Cross-Over Clinical. Neuropsychobiology 2023, 1–11. [CrossRef]
- Benvenuti, P.; Ferrara, M.; Niccolai, C.; Valoriani, V.; Cox, J.L. The Edinburgh Postnatal Depression Scale: validation for an Italian sample. J Affect Disord. 1999, 53, 137–141. [Google Scholar] [CrossRef]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry. 1987, 150, 782–786. [Google Scholar] [CrossRef]
- Pham, D.; Cormick, G.; Amyx, M.M.; Gibbons, L.; Doty, M. , Brown, A.; Norwood, A.; Daray, F. M.; Althabe, F.; Belizán, J. M. Factors associated with postpartum depression in women from low socioeconomic level in Argentina: A hierarchical model approach. J Affect Disord. 2018, 227, 731–738. [Google Scholar] [CrossRef]
- Rashid, A.A.; Shamsuddin, N.H.; Ridhuan, R.D.A.R.M.; Amalina, N.; Sallahuddin, N.K.D. Breastfeeding practice, support, and self-efficacy among working mothers in a rural health clinic in Selangor. J Malaysian Journal of Medicine Health Sciences. 2018, 14, 39–49. [Google Scholar]
- Fink, G. Stress: Concepts, Definition and History. Reference Module in Neuroscience and Biobehavioral Psychology. 2017. [Google Scholar]
- Slykerman, R. F.; Hood, F.; Wickens, K.; Thompson, J.M.D.; Barthow, C.; Murphy, R.; Kang, J.; Rowden, J.; Stone, P.; Crane, J.; Stanley, T.; Abels, P.; Purdie, G.; Maude, R.; Mitchell, E.A. Effect of Lactobacillus rhamnosus HN001 in Pregnancy on Postpartum Symptoms of Depression and Anxiety: A Randomised Double-blind Placebo-controlled Trial. EBioMedicine. 2017, 24, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Barthow, C.; Wickens, K.; Stanley, T.; Mitchell, E.A.; Maude, R.; Abels, P.; Purdie, G.; Murphy, R.; Stone, P.; Kang, J.; Hood, F.; Rowden, J.; Barnes, P.; Fitzharris, P.; Craig, J.; Slykerman, R.F.; Crane, J. The Probiotics in Pregnancy Study (PiP Study): rationale and design of a double-blind randomised controlled trial to improve maternal health during pregnancy and prevent infant eczema and allergy. BMC Pregnancy Childbirth. 2016, 16, 133. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Wang, Q.; Wang, Y.; Sun, A.; Lin, Y.; Jin, Y.; Li, X. Fecal microbiota transplantation from chronic unpredictable mild stress mice donors affects anxiety-like and depression-like behavior in recipient mice via the gut microbiota- inflammation-brain axis. Stress(Amsterdam,Netherlands). 2019, 22, 592–602. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, J. K.; Michaelsen, T. Y.; Bundgaard-Nielsen, C.; Nielsen, R. E.; Hjerrild, S.; Leutscher, P.; Wegener, G.; Sørensen, S. Faecal microbiota transplantation from patients with depression or healthy individuals into rats modulates mood-related behaviour. Scientific reports. 2021, 11, 21869. [Google Scholar] [CrossRef]
- Fiocchi, A.; Pawankar, R.; Cuello-Garcia, C.; Ahn, K.; Al-Hammadi, S.; Agarwal, A.; Beyer, K.; Burks, W.; Canonica, G.W.; Ebisawa, M.; Gandhi, S.; Kamenwa, R.; Lee, B.W.; Li, H.; Prescott, S.; Riva, J.J.; Rosenwasser, L.; Sampson, H.; Spigler, M.; Terracciano, L.; … Schünemann, H.J. World Allergy Organization-McMaster University Guidelines for Allergic Disease Prevention (GLAD-P): Probiotics. The World Allergy Organization journal. 2015, 8, 4. [Google Scholar] [CrossRef]
- Baldassarre, M.E.; Palladino, V.; Amoruso, A.; Pindinelli, S.; Mastromarino, P.; Fanelli, M.; Di Mauro, A.; Laforgia, N. Rationale of Probiotic Supplementation during Pregnancy and Neonatal Period. Nutrients 2018, 10, 1693. [Google Scholar] [CrossRef]
- Gelfand, A.A. Infant Colic. Seminars in pediatric neurology, 2016, 23, 79–82. [Google Scholar] [CrossRef]
- de Weerth, C.; Fuentes, S.; Puylaert, P.; de Vos, W.M. Intestinal microbiota of infants with colic: development and specific signatures. Pediatrics. 2013, 131, e550–e558. [Google Scholar] [CrossRef]
- Dryl, R.; Szajewska, H. Probiotics for management of infantile colic: a systematic review of randomized controlled trials. Archives of medical science: AMS. 2018, 14, 1137. [Google Scholar] [CrossRef] [PubMed]
- Chau, K.; Lau, E.; Greenberg, S.; Jacobson, S.; Yazdani-Brojeni, P.; Verma, N.; Koren, G. Probiotics for infantile colic: a randomized, double-blind, placebo-controlled trial investigating Lactobacillus reuteri DSM 17938. J Pediatr. 2015, 166, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Sung, V.; Collett, S.; de Gooyer, T.; Hiscock, H.; Tang, M.; Wake, M. Probiotics to prevent or treat excessive infant crying: systematic review and meta-analysis. JAMA pediatrics. 2013, 167, 1150–1157. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart of the study.
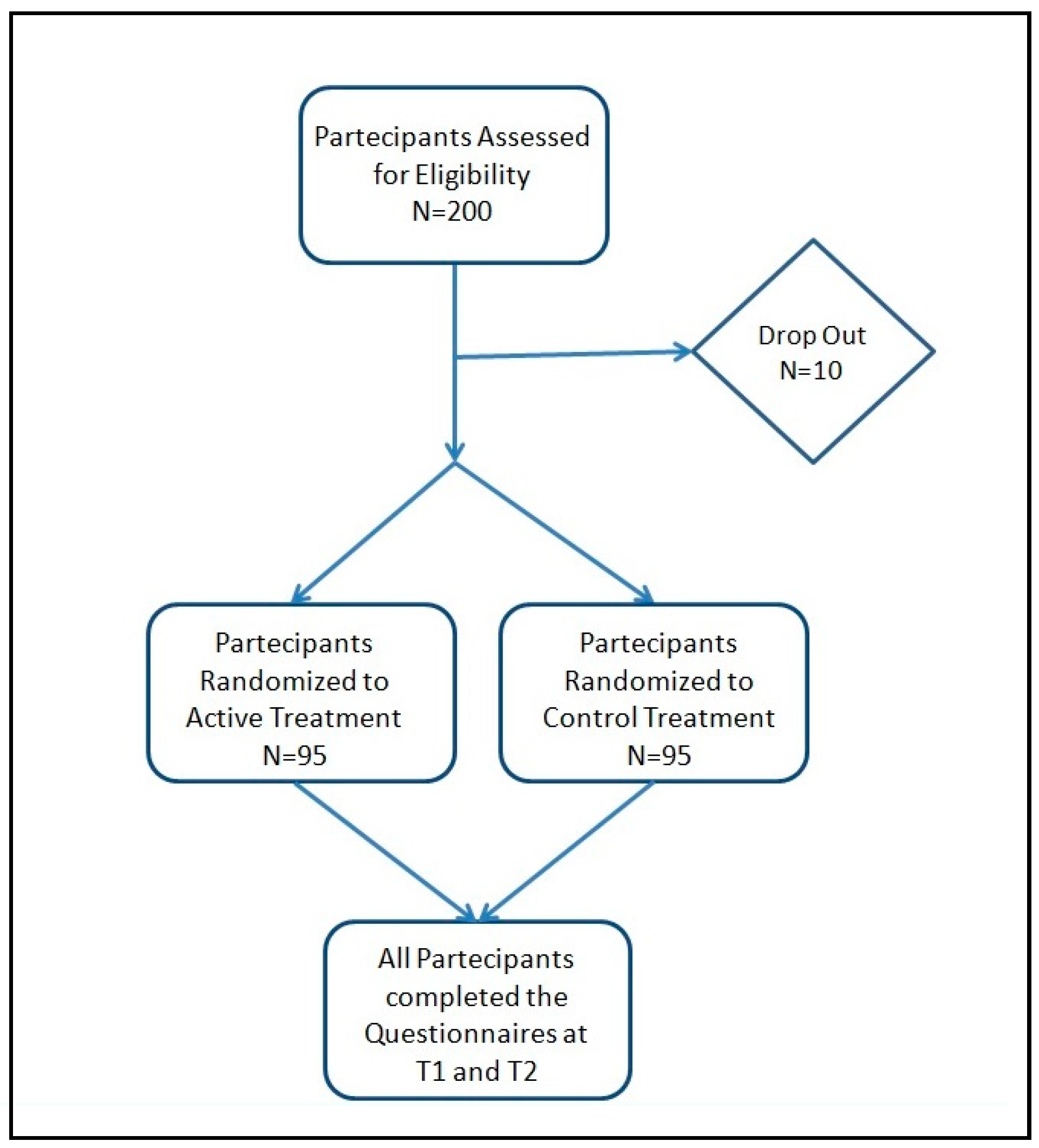
Figure 2.
Study timeline.
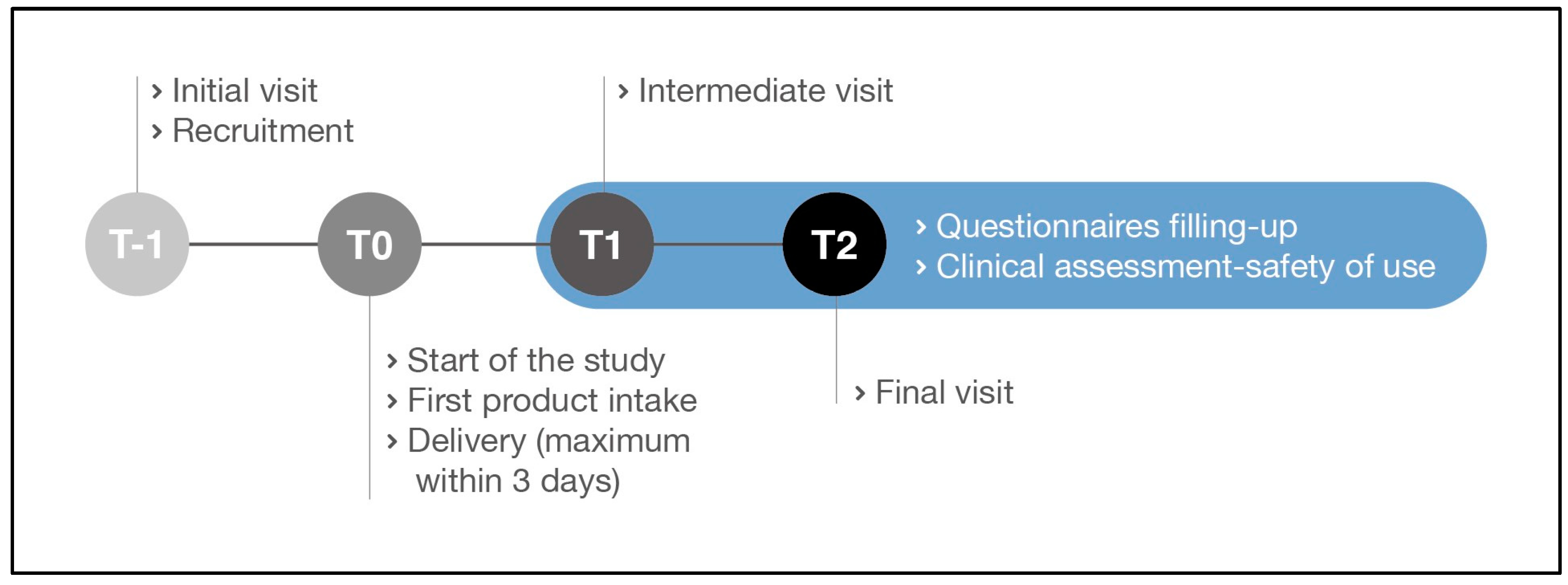
Figure 3.
Score obtained from the Edinburgh Postnatal Depression Scale questionnaire. Comparison between the active and control products at T1 (a) and T2 (b). The boxplots show the minimum, the median, and the maximum of the values collected. Statistical differences were calculated using Mann Whitney U test: * p-value <0.001.
Figure 3.
Score obtained from the Edinburgh Postnatal Depression Scale questionnaire. Comparison between the active and control products at T1 (a) and T2 (b). The boxplots show the minimum, the median, and the maximum of the values collected. Statistical differences were calculated using Mann Whitney U test: * p-value <0.001.
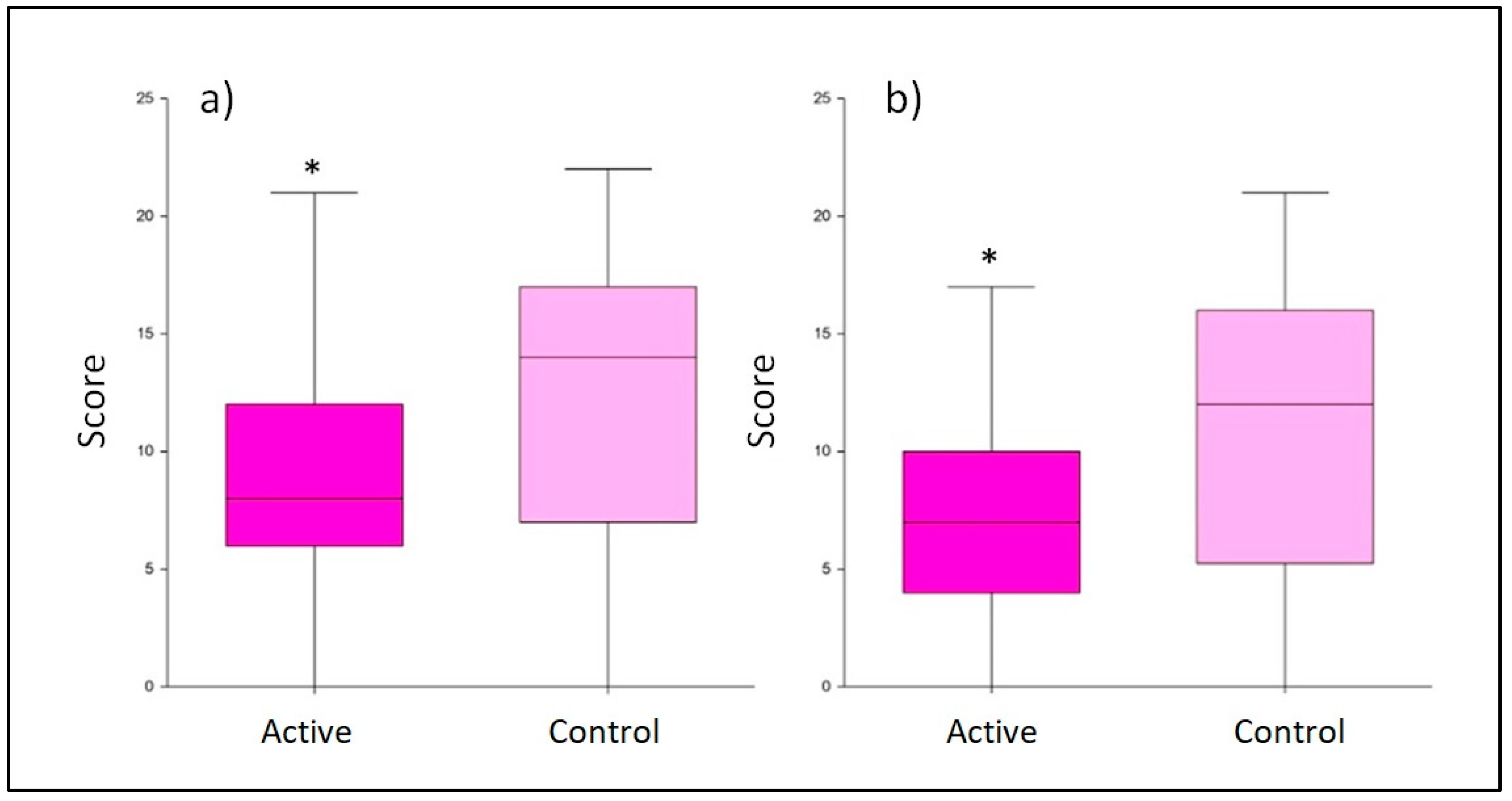
Figure 4.
Score obtained from the Breastfeeding Self-Efficacy Scale-Short Form (BSES-SF) questionnaire. Comparison between active and control at (a) T1 and (b) T2. The boxplots show the minimum, the median, and the maximum of the values collected. Statistical differences were calculated using Mann Whitney U test: * p-value <0.001.
Figure 4.
Score obtained from the Breastfeeding Self-Efficacy Scale-Short Form (BSES-SF) questionnaire. Comparison between active and control at (a) T1 and (b) T2. The boxplots show the minimum, the median, and the maximum of the values collected. Statistical differences were calculated using Mann Whitney U test: * p-value <0.001.
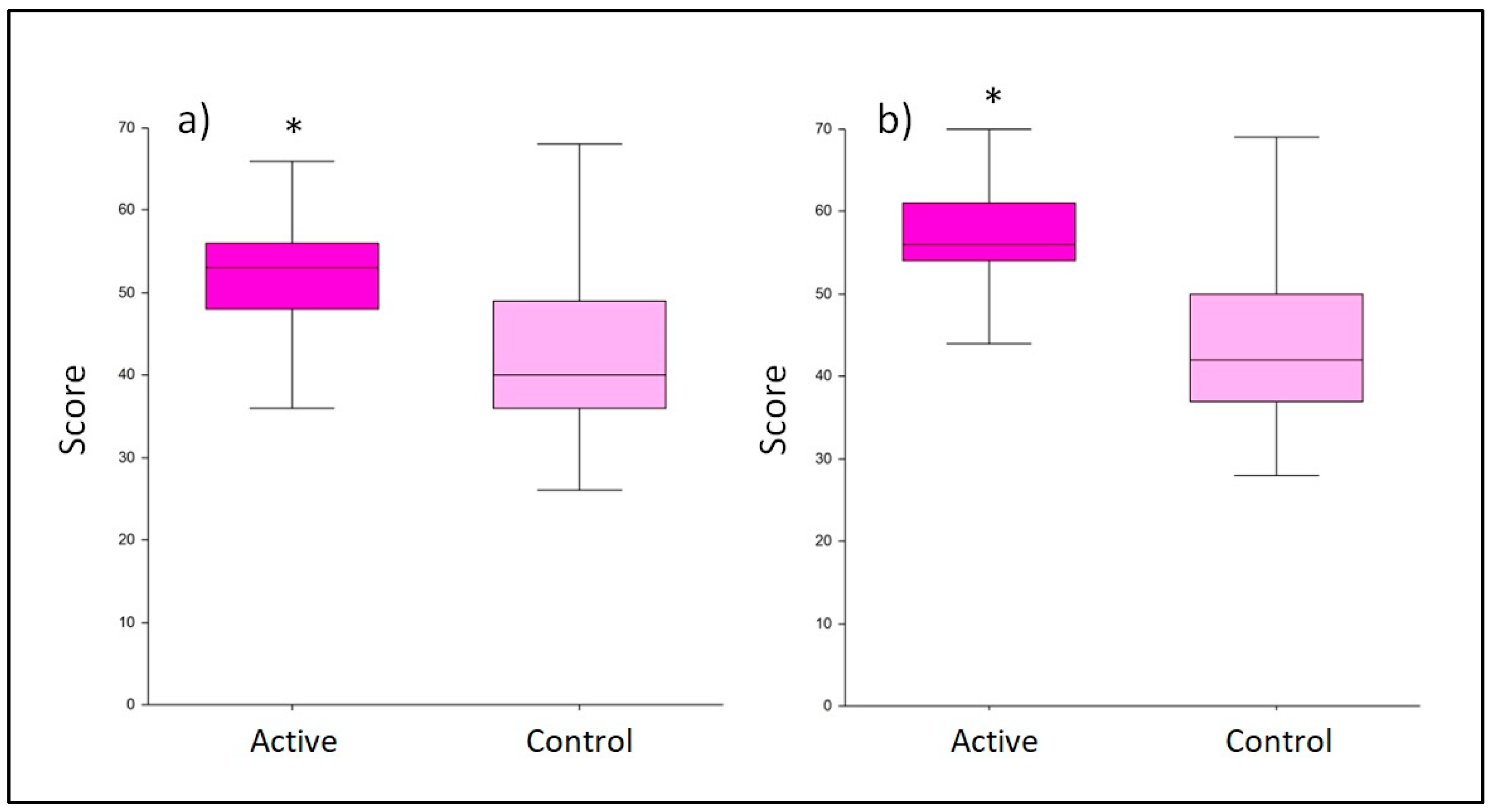
Figure 5.
Average number of crying/fussing events. Comparison between the active and control product at T1 (a) and T2 (b). The boxplots show the minimum, the median, and the maximum of the collected values. Statistical differences were calculated using Mann Whitney U test: * p-value <0.001.
Figure 5.
Average number of crying/fussing events. Comparison between the active and control product at T1 (a) and T2 (b). The boxplots show the minimum, the median, and the maximum of the collected values. Statistical differences were calculated using Mann Whitney U test: * p-value <0.001.
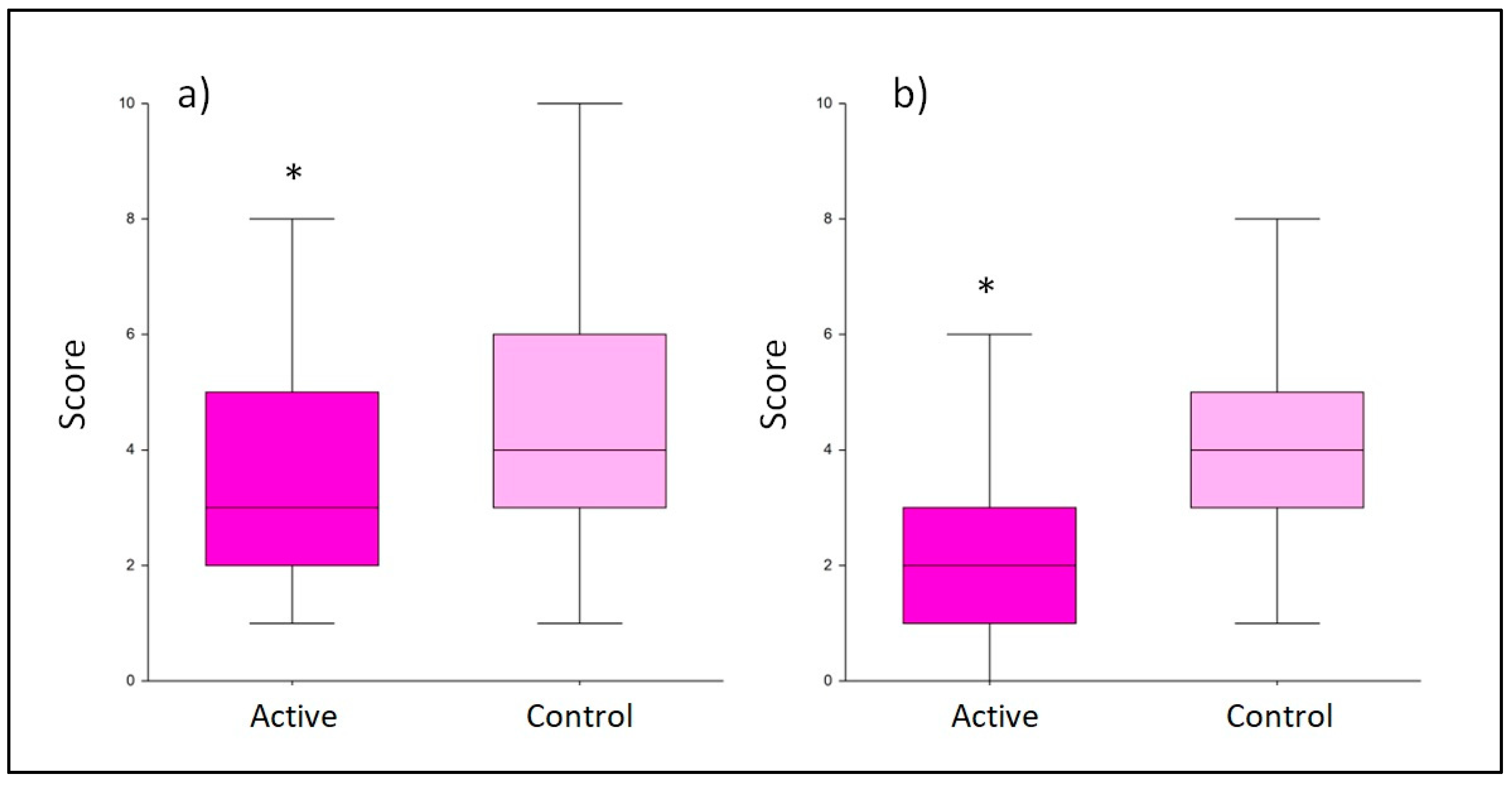

Table 1.
Inclusion and exclusion criteria of the study.
| Inclusion criteria | Exclusion criteria |
|---|---|
| Good general health condition | Subjects who do not meet the inclusion criteria |
| Women in the first trimester post-partum | Subjects considered as not adequate to participate to the study by the investigator |
| Aged between 18 and 50-year-old (extremes included) | Subjects with known or suspected sensitization to one or more test formulation ingredients |
| Willingness to breastfeed* | Adult protected by law (under control or hospitalized in public or private institutions for reasons other than research, or incarcerated) |
| Willingness to use probiotics and multivitamin food supplements that will be consigned at the last visit before delivery | Subjects not able to communicate or cooperate with the investigator for problems related to language, mental retardation or impaired brain function |
| Willingness to fill-up questionnaire | Subjects suffering from other psychiatric disorders such as schizophrenia, other psychotic disorders, bipolar disorder or substance use disorder |
| Willingness to use only the products to be tested during all the study period | Subjects with serious physical illnesses or mental disorders due to a general medical condition which are judged by the investigator to render unsafe |
| Willingness not to use similar products that could interfere with the product to be tested | Subjects with significant risk of infanticide according to the investigator assessment |
| Willingness not to vary the normal daily routine (i.e. lifestyle, physical activity, etc.) | Subjects taking herbal remedies or psychotropic drugs that are intended for depression are taken within the last 2 weeks prior to baseline or during the study |
| Subjects aware of the study procedures and having signed an informed consent form | Subjects receiving counselling or psychological therapies at baseline or during the study |
| Subjects who do not meet the inclusion criteria |
1 *If the woman after delivery will not be able to breastfeed, she can still remain in the panel since maternal breastfeeding is a secondary outcome.
Table 2.
Study schedule.
| Study phases | Initial visit Recruitment (T-1) |
Start of the study Product intake (T0) |
Intermediate visit (T1) |
Final visit (T2) |
|---|---|---|---|---|
| Signed Informed consent | X | - | - | - |
| Subject eligibility | X | - | X | X |
| Clinical assessment-safety of use | - | - | X | X |
| Questionnaires filling-up supported by the gynecologist | - | - | X | X |
| Products distribution | X | - | - | - |
| Unused product collection | - | - | - | X |
Table 3.
Positive and negative answers to question number 15 of the Breastfeeding Self-Efficacy Scale-Short Form (BSES-SF). The question was related to the improvement recorded in the crying/fussing events during the treatment.
Table 3.
Positive and negative answers to question number 15 of the Breastfeeding Self-Efficacy Scale-Short Form (BSES-SF). The question was related to the improvement recorded in the crying/fussing events during the treatment.
| Treatment | Answer at T1 | Answer at T2 | ||
|---|---|---|---|---|
| Yes | No | Yes | No | |
|
Active product (probiotics plus multivitamins) |
77 | 18 | 74 | 21 |
|
Control (multivitamins only) |
40 | 55 | 41 | 54 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



