
Submitted:
25 July 2023
Posted:
26 July 2023
You are already at the latest version
Abstract
(1) Introduction: Every two hours, a Romanian woman is diagnosed with cervical cancer [1] as the country ranks second in Europe in terms of mortality and incidence rate [2]. This paper aims to identify the main reasons that have led to this situation, focusing on the measures taken by the Romanian Ministry of Health for the prevention of this type of cancer national - programs for cervical cancer screening and HPV vaccination. (2) Materials and methods: We performed a study based on available secondary data from the National Statistics Institute, World Health Organization and Bucharest Institute of Oncology in order to assess the burden associated with cervical cancer and placing it in the context of known global and European incidence and mortality rates, thus evaluating the importance of this health issue in Romania. The second component of our study was a cross-sectional study, using a 14 questions questionnaire, applied to the women participating in the National Screening Program for Cervical Cancer, aimed to evaluate the women’s level of knowledge about screening and HPV vaccination and their access cervical cancer specific health-care services. (3) Results: The results of the research shows that a high percentage of women postpone the routine checks due to lack of time and financial resources and indicate that low level of knowledge about the disease and the specific preventive methods determines low participation screening and HPV vaccination programs implemented in Romania contributing to the country’s situation of cervical cancer. (4) Conclusions: The national programs have complicated procedures, are underfunded, and do not motivate enough health care workers. This combined with the lack of information adds up to an extremely low number of women screened and vaccinated. Our conclusion is that the Romanian Ministry of Health must take immediate action by conducting major awareness campaigns, implementing measures to make the programs functional and ensuring coherent funding.
Keywords:
social and global inequities
; access to health programs
; cervical cancer screening program
; HPV vaccination programs
; knowledge
; believes
; acceptance of vaccines/ screening
; participation in screening programs
; incidence and mortality rates for cervical cancer
; pelvectomies
1. Introduction
In Romania, neoplastic disease represents the 2nd cause of death, after cardiovascular disease [3] and cervical cancer remains by far one of the most severe problems faced by the health system. If, when it comes to other cancers, Romania follows the European trend, in the case of cervical cancer we rank in a not very honorable place, namely the second (being outranked only by Montenegro) both in terms of incidence and specific mortality [2]. In Romania, the incidence rate of cervical cancer is more than double the average of European countries (34.2 vs. 15.0), and the mortality rate is triple (18.3 vs. 6.7). These incidence values situate the country among countries like Somalia, Indonesia, Suriname, Myanmar, Republic of Congo, Venezuela, Peru, Central African Republic, Jamaica, Ethiopia, Nicaragua, or Sierra Leone, ranking 43rd worldwide [2]. 52-60% of the deaths by cervical cancer occur in low- and middle-income counties due to failure in implementing population-based screening programs [4,5,6] and Romania stands out in a negative way being an upper middle-income country [7].
Obviously, the question arises as to how Romania ended up in this situation, especially when we are talking about a disease with a very well documented infectious etiology, with an extremely effective vaccine against the main etiological factor of the disease and for which we have countless screening methods adapted to any healthcare budget with proven effectiveness over the years in various other countries. The main reasons are the extreme health-illiteracy of most citizens and how much Romania, as a country, allocates for disease-prevention from the total health-care expenses. Only in 2015, Romania allocated a little over 2% of the health budget to the prevention of diseases (this representing the total budget allocated for all preventive measures for all diseases and not just for specific methods for the prevention of cervical cancer). Except for 2015, the allocated percentage varied between 1.18 and 1.76%. This is data freely available on the National Statistical Institute site. The data is available until 2019 [8].
2. Materials and Methods
Our study has two components. One is based on descriptive statistic of information from the internal electronic database of Bucharest Institute of Oncology “Prof. Dr. Alexandru Trestioreanu”, the largest center for cancer care in Romania. We tried to assess the burden associated with cervical cancer among the pathology treated in our hospital and placing it in the context of known global and European incidence and mortality rates, thus evaluating the importance of this health issue in Romania. Permission for retrieving data from the internal electronic database and statistical analysis was obtained from the leadership of the Institute. For this study, we screened the electronic database of our Institution using as filtering criteria ICM 10 code C53 – Malignant tumor of cervix and we extracted data concerning the number of patients treated each year for cervical cancer between 2012 and 2022, the number of distinct hospitalization episodes that were necessary for cervical cancer, number of surgical procedures performed for this pathology and the total number of surgical procedures performed.
The second component was a cross-sectional study, using a questionnaire as a research tool, applied to the women participating in the National Screening Program for Cervical Cancer during Pap smear testing campaigns with the mobile screening unit, organized in disadvantaged parts of Romania (known for lower income and accessibility to education and healthcare). All participants signed an informed consent form. The questionnaire contained 14 questions presented in Table 1 and aimed to evaluate the women’s level of knowledge about screening and HPV vaccination and their access cervical cancer specific health-care services.
Statistical Analysis
Data was collected and analyzed in Excel. Data were labelled as nominal or quantitative variables. Nominal variables were characterized by means of frequencies.
3. Results
3.1. Burden of Cervical Cancer in Bucharest Oncology Institute
Cervical cancer (CC) causes a huge burden on the health system in Romania, both as number of cases and as severity of disease. Over the last decade, cervical cancer accounted for 17.97 to 29.56 percents of the total of cases treated in Bucharest Oncology Institute. 15 to 30 percentage of all surgical procedures performed in a year were addressed to malignant tumors of the cervix. Also, most cases were diagnosed in advanced stages that require more than local treatment. For some of those cases extreme surgical procedures (like pelvic exenterations) are required to ensure optimal treatment for the patient. This combined with the severity of the associated pathology of our patients (many being elderly or having cardiac, pulmonary, renal, or other chronic illnesses) led to the increase of the medium duration of hospital stay for each episode and of the cost of treating the case. The medium duration of hospital stay was 7.62 days in 2022, 10.12 days in 2021 and 10.25 days in 2020, with extremes varying from 1 to 56 days. The cost per CC case treated increased constantly in the last years, thus further burdening a health-care system already underfunded, more than doubling in the past 3 years, reaching a value of 12.000 Romanian lei/case treated. This, however, needs to be interpreted in the context of the amount refunded to the hospital by the state which currently is less than 7.000 Romanian lei/case treated. So, as a result of the current refunding system each case treated for cervical cancer determines a significant financial deficit in the budget of the hospital, thus endangering the future care of these patients.
During the pandemic years (2020-2022) we saw a reduction of cervical cancer cases, in parallel with the overall reduction of all cancer cases treated. This was caused by the restrictions imposed during the COVID 19 pandemic and the patients’ fear of contracting the SARS-COV2 virus while being treated for other pathologies, which severely limited the access of patients to treatment, resulting in a huge impact on treatment and oncologic outcomes for cancer patients [9]. However, the percentage of hospitalization episodes and number of surgical procedures caused by CC out of total remained the same as the pre-pandemic years. The restrictions were only lifted in 2022. The general characteristics of this pathology in our Institute are summarized in Table 2.
3.2. Knowledge about Cervical Cancer Prevention, Early Detection Methods and Health-Care Access among Targeted Population
The second component of our study consisting in a cross-sectional study of the women participating in the National Screening Program for Cervical Cancer during Pap smear testing campaigns with the mobile screening unit, organized in the counties of Tulcea, Buzau and Ilfov. 528 women answered a 14 questions questionnaire evaluating demographic data, the women’s level of knowledge about screening and HPV vaccination and their access cervical cancer specific health-care services.
3.2.1. Demographic Data of Responders
General demographic characteristics of responders are presented in Figure 1, Figure 2 and Figure 3. Medium age of responders was 47.86 years, with extremes ranging from 19 to 69 years old. 28% (149 women) are residents of urban area and 71% (379 women) are residents of underprivileged rural areas of Romania (known for lower income and accessibility to education and healthcare). As for access to education we need to first say that in Romania school is mandatory and free for both primary and medium levels (for a total of 12 or 13 years) since 2020. Even before 2020, school was mandatory and free for 8 grades which meant finishing the primary gymnasia cycle. Parents can be fined for not sending their children to school and many non-profit and charitable organizations are helping children to be able to go to school. Yet 2% of our responders (12 women) did not go to school ever and 14% only finished primary level education (71 women). Most of our responders (63%) had finished high-school or at least went to 2 out of 4 years of high-school (260 finished high-school, 68 had 10 grade education). Only 21% had post-high school education (48 had professional short term superior degrees and 62 bachelor’s or master’s degrees). 521 out of 528 responders told us about their education.
3.2.2. Access to Cervical Cancer Specific Preventive/Diagnostic Methods
As a measure of access to specific preventive methods, we asked the responders if they previously had a Pap-smear. All participants answered the question. More than a fifth of our responders never had a Pap-smear in their life (112 women – 21% of responders). Of the 416 responders (79% of responders) that previously had a Pap-smear, only 384 recalled when they had it. Only 77 women had been tested in the previous year, 137 women had a Pap-smear 2 to 4 years before and 170 women had 5 years or more since the test. Even worse, most women on this last category only got tested once in their life (usually the test was performed before childbirth and not by choice), 73 of them had more than 10 years since the test and 26 more than 20 years (Figure 4).
We also asked our responders if they would have gotten screened for cervical cancer by choice if the mobile screening unit wouldn’t have come to their city and 526 women answered the question. Only 44% (233 women) answered yes. 293 had no intention of getting tested by choice/demand. 13 women gave no reason for this and 15 gave multiple reasons. Each multiple reason was split into component reasons for statistical analysis.
Figure 5.
Probability of going for additional tests and reasons for non-attending.
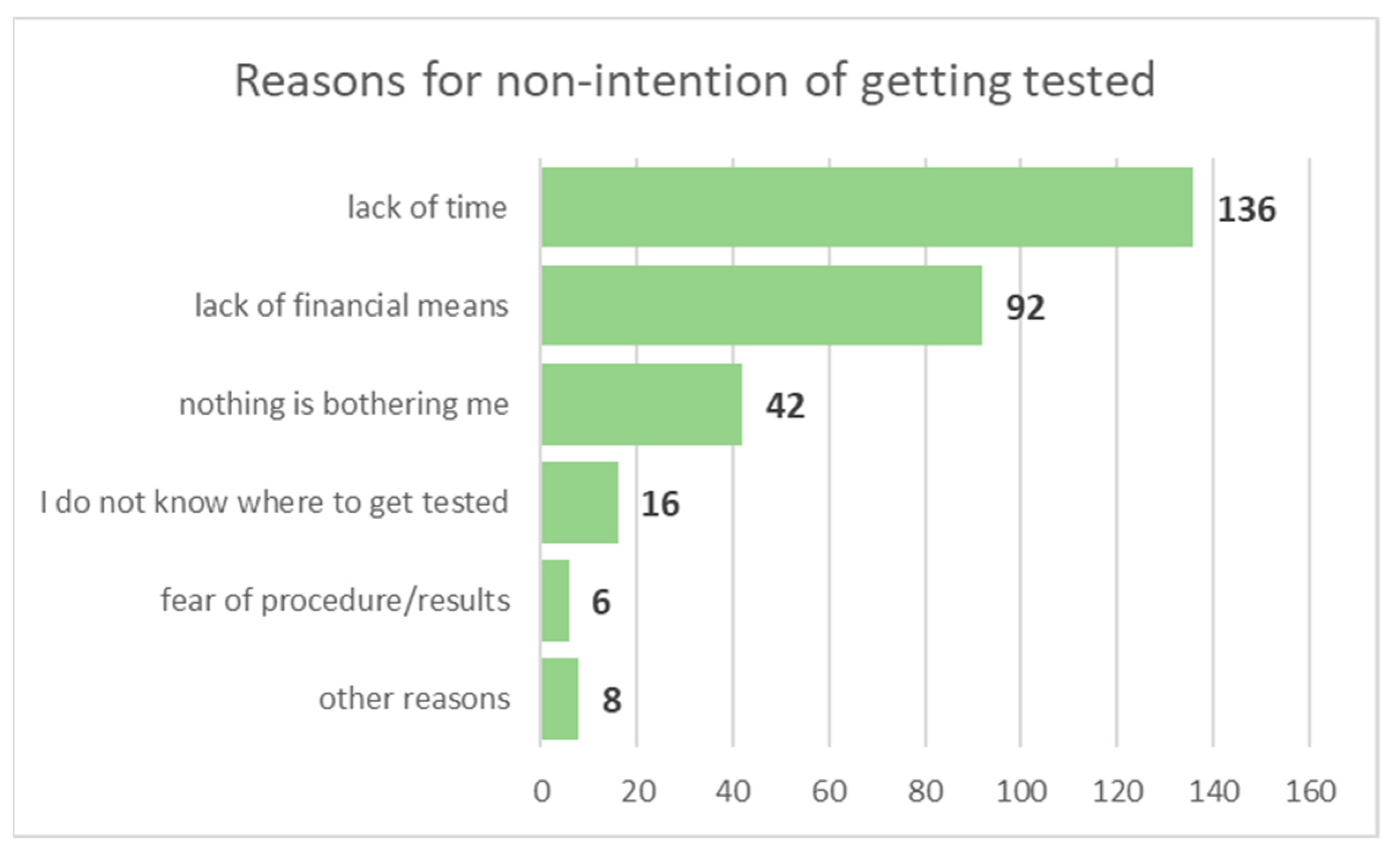
The most frequent reasons given for the lack of intention of getting a Pap-smear in the absence of the immediate opportunity presented by the mobile screening unit were, in order of frequency, lack of time (45.33%), lack of financial means (30.66%) and the absence of any symptomatology (14%). Among other reasons given we identify the lack of information about where/how to get tested, fear of procedure/test results and the need to travel to another city in order to get tested.
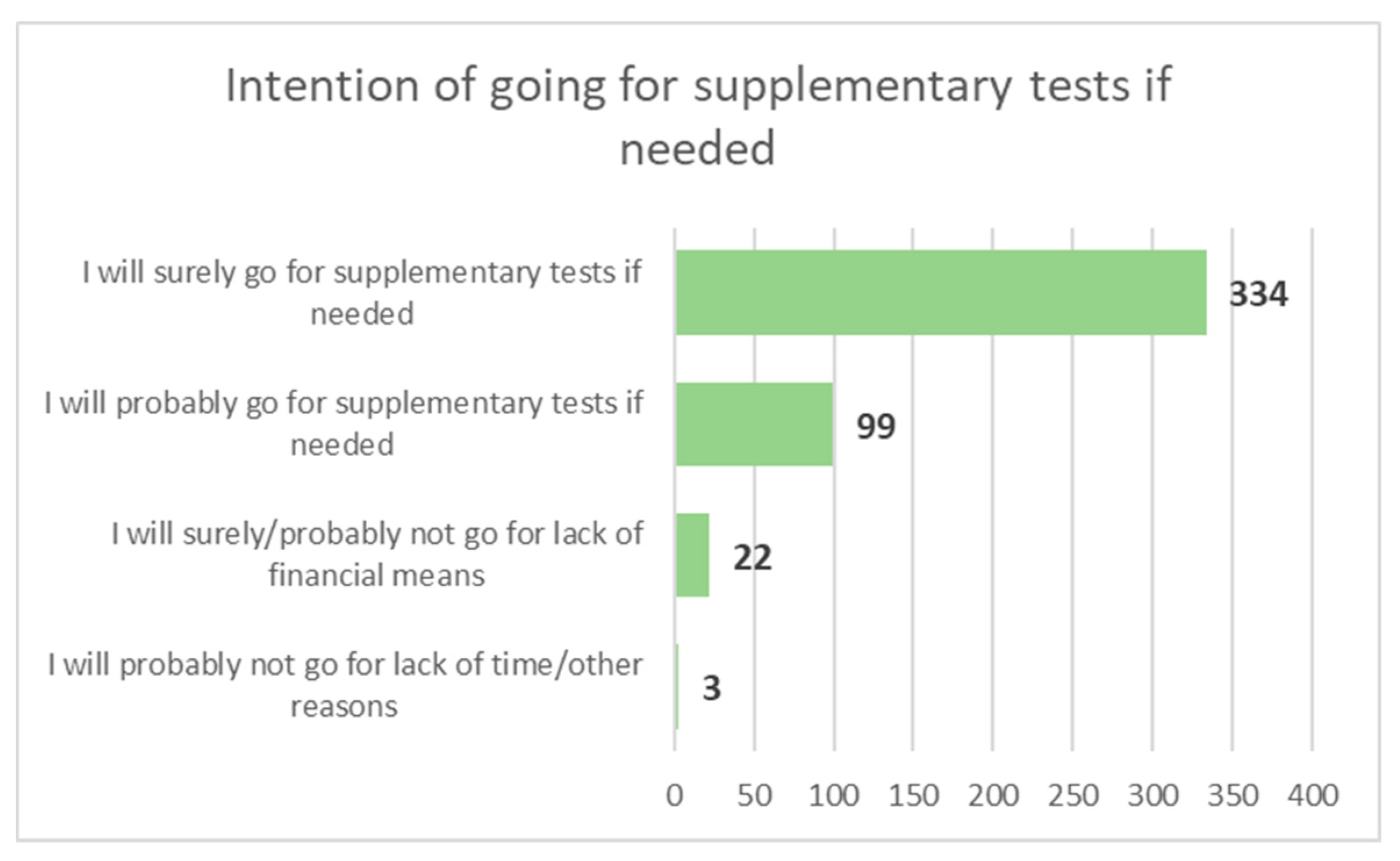
Another question was aimed at evaluating the access of responders to supplementary diagnostic test specific for cervical cancer. We asked about the probability of undergoing supplementary tests if needed and the reasons for not attending those tests. 458 women responded this question (86.74%). Most responders (94.54%) responded they will surely/probably go to supplementary diagnostic tests if the Pap-smear results would indicate the need. But 4.8% responded they would surely/probably won’t go due to lack of financial means, indicating an acute lack of knowledge about the possibility of having those tests free of charge in state hospitals.
Figure 6.
Access to supplementary diagnostic tests.
3.2.3. Knowledge about HPV and HPV-Vaccination, Access to Vaccine
Regarding the HPV infection, most of the respondents have heard of this infection and are aware of the link between HPV and cervical cancer. 524 women answered this question and only 11% did not know of HPV and its link to cervical malignant tumors (Figure 7). During our analysis we saw that, even though, most women that do not know about the connection between HPV infection and cervical cancer have no or primary education, they are not the only ones - women with superior education accounted for 5% of the “No” responses).
However, although most respondents (79% - 416 out of 528 responders) are aware there is an effective vaccine against HPV (Figure 8), most (96% - 503 out of 524 responders) are not vaccinated (Figure 9). Only 22 women out of 524 responders declare they are HPV-vaccinated. Vaccinated women have a maximum age of 54, almost half live in urban areas and all have high-school or higher education. All women with higher education know there is an effective HPV vaccine.
As a final analysis we tried to evaluate the knowledge of our respondents about the existence of the national HPV-vaccination program that offers free vaccination for girls aged 11 to 18, and their intent in letting their daughters participate. Only 57% of the women knew about this possibility (295 of 521 responders) – Figure 10. And even after being told about this possibility of free HPV-vaccination only 57% of the women would vaccinate their daughters (271 out of 471 responders) – Figure 11. Main reasons for refusing to vaccinate their daughters are summarized in Figure 12.
4. Discussion
4.1. Cervical Cancer in Romania Vs. Europe/World – Current Situation, Trends, Incidence, and Mortality
Romania is a country located in South-Eastern part of Europe, member of the European Union (EU) since 2007, with a population of 19.04 million resident citizens in 2022 according to the National Statistics Institute, 9.80 million being women [8]. Romania has the highest proportion of rural population among EU member states with a value of 46% [10]. Life expectancy for women in Romania is 79.3 years at birth, below the EU average [11]. Cervical cancer represents the 5th cancer-related cause of death in Romania after lung, breast, colon, and prostate [8].
For most cancers Romania follows the European trends, but for cervical cancer the country’s situation is extremely alarming with high rates of incidence and mortality – in Figure 13 we present the country’s situation by comparison to the European average for top 5 female cancers using data from GLOBOCAN 2020 and Human Papillomavirus and related Disease report World [2,12]. Even so the data for Romania may be underestimated since the country does not have a functional cancer registry for the accurate monitoring of incidence or mortality rates, nor does Romania have a registry for recording a woman’s individual screening history [13] that would be helpful in evaluating potential preventative measures. Also, testing laboratories, hospitals and doctors are not obliged to report screening results and there is no possible way of correctly evaluating the screening coverage among the targeted age group.
Romania, like other European Union member states, has several serious public health issues that still need to be addressed. However, significant contrasts are observed between older and newer member states, when it comes to incidence and mortality rates for cervical cancer. These inequities between states might be explained by differences in preventive strategies adopted by each country during time [14] and the duration for which those strategies were in effect.
Previous studies [14] that proved the positive impact of functional screening programs had in various EU states, also showed that Romania is in a situation similar that of other EU states in 1960s-1970s, before the implementation of national screening programs. In those countries the cervical cancer specific mortality rates decreased significantly after the initiation of the screening program [15].
A functional national screening program is essential for early diagnosis and the potential for curable therapeutic intervention [16]. Studies showed that even a single lifetime screening can significantly decrease mortality and incidence of advanced cervical cancer compared to no screening [17]. Some studies have shown that women attending screening programs benefit of a 41 to 92% reduction in cervical cancer mortality [18].
Even though both Romania and the EU have shown decreasing trends in cervical cancer specific mortality (56% vs. 58% reduction in mortality rates in 2016 compared to 2002), Romania still has a huge difference in mortality. In 2002 the mortality difference compared to the European Union was extreme (276%). In 2016 the gap remained the same situated at 277% [19]. Among Romania’s regions we see that a huge gap between mortality rates in rural vs urban area persists despite an impressive 44% reduction of mortality over the past two decades in some rural areas situated in North-Western and Western parts of the country. The rural–urban mortality gap was 24% in 2019 [19].
Since December 2003, there is an EU Council recommendation addressed to member states to implement population-based systematic screening programs for cervical, breast and colo-rectal cancer [20]. In 2017, 22 out of 28 member states had implemented a form of cervical cancer screening program (national or regional), ensuring an average coverage of 59,2% of women between 30 to 59 years, with a participation rate of 50.7% [21]. The screening programs developed by member states varied widely in both targeted age-range, methods used for screening, form of screening (voluntary/ compulsory/ invitation based) and coverage of certain regions (discrepancies between rural and urban areas or covering only some regions as pilot programs) [14,22]. Given the heterogeneity between various national programs it is hard to compare the quality of testing, the monitoring and evaluation methods or the cost effectiveness of each program [21,23,24]. However, there is a clear connection between access to organized screening programs and cervical cancer specific incidence and mortality rates [21,25,26,27].
4.2. Cervical Cancer Screening Program in Romania
The screening for cervical cancer in Romania started with a population-based pilot-program conducted in Cluj County between 2002 and 2008. The coverage of this regional pilot program was 21% by the end of 2008 [28]. In 2012 the state started a 5-years nationwide pilot screening program for cervical cancer [29]. As a design, the program consisted of establishing a network of medical healthcare workers that has as target the testing by Pap-smear once every 5 years all eligible women, aged 25 to 64 years old, regardless of ensured/ non-ensured, with no symptomatology and no previous cervical cancer diagnosis or total hysterectomy. The eligible population was evaluated at over 6 million women in all country. The general practitioners and the obstetrics-gynecology specialists were forced to participate by law. At the end of the pilot program 730.000 women were tested (13.6% of eligible women) [30]. However, the program had limited success (at its peak in 2014, the national coverage of eligible women was 8%). The reason for this failure was a weak participation of doctors with only 48% of them actively recommended testing through the program. The main reason cited was the complicated procedures and documents [1]. At the same time, the funds allocated to the program were very few and very sparce, which meant that many times a woman went to the gynecologist to be tested with the screening form filled out by the general practitioner, and not being tested due to lack of funds. This, as well as the delay in providing the results, seriously affected the credibility of the program. Another reason for the failure of the pilot program was an almost non-existent coverage of rural areas [1].
After the experience gained through this pilot program, several measures were implemented to remedy the identified shortcomings, namely: (1) regional monitoring and management units of the program were established that reduced the problems related to the delay of results, bureaucracy and procedures, ensuring at the same time the external control of the quality of the testing procedures and the issued results; (2) the possibility of covering rural regions was created through the operationalization of mobile screening units.
However, even in the years 2018-2023, the program does not register the expected success for the following reasons: (1) most doctors believe that the program no longer works; (2) most eligible women do not know about the possibility of free Babes-Papanicolaou testing through the program; (3) very few medical personnel are qualified according to the methodological norms to collect the tests (only gynecologists and general practitioners [31]) which makes it very difficult to find doctors willing to go in screening campaigns; (4) the lack of coherent funding causing a delay of 5-6 months in the payment of the services performed, causes the discouragement of the staff and ultimately the abandonment of the program.
In 2020 the number of eligible women in Romania was, according to the National Statistics Institute, 5.104.624. The same Institute provides us with data about the coverage of the eligible women by the national screening program. The percentage of eligible women covered by testing in the last 5 years is 2.6% in 2018, 3.1% in 2019 and 3.4% in 2020 (2020 is the last year for which there is data available, but the data is partial, still being compiled by the Institute) [32]. This translates into roughly 175.000 women being tested in the last 5 years. However, according to Romania’s cervical cancer country profile [33], 38% of women of eligible age report they have been screened in the last 5 years. This demonstrates that most of the cervical cancer screening is opportunistic rather than systematic, contradicting the EU [20] and WHO (World Health Organization) recommendations on this matter.
Proportion of women with high level of education screened is almost 5 times higher than that of women with a low level of education. In terms of income categories, the proportion of women with high incomes who benefited from a screening test is 3 times higher, compared to that of women with low incomes (43.3% vs. 12.8%) [25]. In Romania more than 10% of population consists of various minorities [32], and 3,3% belong to the Roma community although this number may be underestimated [34]. It is a well-established fact that non-ethnic Romanians, especially Roma women, participate less frequently in screening programs compared to the main ethnic group [35,36]. This aspect is linked to a lower level of knowledge about the existence of screening programs, mistrust about the free of charge policy of the screening programs and about the benefits screening could bring [13,36]. Anterior cross-sectional studies using questionnaires, addressed to both Romanian and ethnic-minority population in Romania showed that the low attendance in screening procedures is caused by lack of awareness about the existence of the screening program [1] and a perceived lack of financial means to get screened and to follow-up positive test results [1,37]. Although Romanian women have a positive attitude towards preventive medicine [38] this does not necessarily correlate with actual participation in screening programs mostly because the perceived subjective “costs” of having a test is significantly higher than the perceived benefits, this being true especially for women who had never had a Pap smear [39]. This comes as a surprise since in Romania access to health care is guaranteed by the Constitution, the Health System is based on equality of accessibility to medical services regardless of financial contribution of each citizen and many underprivileged citizens are freely ensured for health care. The state funded system provides free access to preventive medical services, to diagnostic procedures and investigations (including complex imaging that can help in differentiating between metastatic lesions and primary/other lesions [40,41] or diagnostic synchronous lesions [42]), to all treatment options for both precursors lesions and for invasive cancer and simultaneous treatment of primary and metastatic lesions [43] through national treatment programs [44] (surgery - including novel techniques such as laparoscopy for both oncologic diagnosis and staging, radical or palliative treatment [45], robotic surgery, novel surgical techniques for cancer [46], sentinel lymph node identification with radioactive material which has become standard of care for some cancers [47] or Indocyanine-green [48], reconstructive surgery, identification of occult cancer lesions using radioactive colloids [49], radiotherapy, chemotherapy, immunotherapy [50], personalized oncological treatments and so on) and also for follow-up procedures and investigations. All being said, it becomes apparent that focused information campaigns are of paramount importance for resolving the problems cervical cancer is facing in Romania, health-illiteracy being the primary reason for the current situation.
4.3. HPV Vaccination Program in Romania
In Romania there is also a national program that provides free anti-HPV vaccine through the family doctor. HPV vaccination is an extremely controversial subject in Romania and is not mandatory nor covered by the National Vaccination Program[51]. The HPV vaccination program was introduced for the first time in 2008 when the vaccine was offered for 10–11-year-old girls (only 2.57% of the total eligible population was vaccinated then). In 2009, the eligibility age was extended to 14 years, but in 2010 the program was discontinued due to lack of participation. Starting from January 2021, the program was resumed for girls aged 11-14 in a modified form, and from September 2021 the eligible age was extended to 18 years, so that currently the HPV vaccination in Romania is free upon request at the family doctor for girls aged 11-18. The rest of the female population and male adolescents are not eligible for free vaccination through the program, these categories only being able to get vaccinated by supporting he full cost. The full cost of 3 doses of HPV-vaccine Gardasil-9 is the equivalent of the current in-pay minimum wage. The Ministry of Health although recommending the vaccination for boys does not provide gender-neutral accessibility to vaccine.
Like the national screening program, the national HPV vaccination program is also a failure (Romania having an extremely low rate of HPV vaccination – 12-13% of eligible population [52]), but in this case the main causes are related more to an acute lack of information of the parents and eligible girls [53,54] or to the parents' information from dubious sources (social media, internet, mass-media, etc.) [55] as well as for reasons related to parents' beliefs, attitudes, and social prejudices. Poor participation in all vaccination campaigns was generated by deficient public health strategies – there were enough vaccine doses to ensure coverage of targeted population, there was adequate diffusion in all areas and in locations that facilitated access (the vaccination campaigns were implemented in schools), and there were enough doctors to administer the vaccine [56]. The only reason for the failure of the vaccination programs remains the lack of adequate information campaigns addressing the lack of knowledge about the connection HPV-cancer and the general lack of acknowledgement of the importance and benefits of HPV vaccination.
Given the fact that in Romania, parents’ consent and active request of the HPV vaccine is required for children under 18 years to be vaccinated, it is paramount to understand parents’ profiles, beliefs and general acceptance of the vaccine, in order to optimize vaccination and improving participation rates. Among the facilitators of parents being willing to HPV vaccinate their children are obtaining information from medical sources [56], female gender [56,57], urban settings [58,59], higher income status and higher educational level [60,61]. As with other vaccines, the physician’s recommendation favored parents’ consent [62]. Hesitance about vaccination is generated by a preconceived notion of the parents that HPV vaccination may adversely influence the sexual behavior of their children [63] or conspiracy beliefs stimulated by mass-media or social platforms [55]. Other most common reasons for unwillingness to vaccinate are doubts about efficacy of vaccine, cost, and fear of side effects [64,65].
Human papilloma virus is the most common sexually transmitted viral infection in the world [66], most sexually active persons coming across at least one strain of the virus during their life span [54]. HPV chronic infection can lead to head and neck [67,68,69,70], skin [71,72,73,74] or anogenital [75] cancers determining enormous medical costs [74] and can severely affect fertility in both men and women [76,77] and alter the efficacy of assisted-reproductive techniques [78,79]. We can see that HPV infection seriously affects both genders and it becomes apparent that, in order to meet the World Health Organization’s goal of eradicating cervical cancer, a gender-neutral HPV vaccination strategy needs to be applied, this being, even at a moderate coverage, the most effective way of achieving this goal [80,81,82]. A gender-neutral campaign also favors the development of a herd immunization effect among adolescents with beneficial results [83].
In conclusion, all future HPV vaccination programs in Romania need to consider the lack of information and confusion regarding adverse effects, which can be solved through education by intense information campaigns. The HPV vaccination programs need to be gender-neutral in order to achieve optimum herd-immunization effect and need to be fully state funded in order to address the accessibility issues real or perceived.
5. Limitations
The main limitation of our study is the fact that mobile unit screening campaigns for cervical cancer are usually addressed to women in rural areas with low access to healthcare and lower education levels. Our results are surely influenced by this factor, and we believe that the results may change if the questionnaire would be answered by a population consisting of both women in underprivileged areas and women in high-density urban areas. Another limitation of our study is the fact that the level of functional illiteracy among Romanian population is extremely high (at around 60% according to some statistics) which means that even if our respondents declare they went to school and they can read, some of them do not understand the questions and prefer not to answer or answer by guess, thus affecting our results. As proof of this we encountered respondents that, even though they said they did not know about the existence of the HPV vaccine, they answered “YES” to the question “Are you HPV vaccinated?”.
6. Conclusions
The responses of our patients indicate the marked need for sustained population information campaigns (like those for conducted in Romania for breast cancer) pointing out the impact, symptomatology, and preventive and diagnostic methods of cervical cancer as the subject, the association of HPV infection with cervical cancer and the existence of the national screening and vaccination programs which offer free screening and access to vaccination.
For the success of the national programs aiming to reduce the impact of cervical cancer, the Ministry of Health should organize coherent and sustained information campaigns, addressed to both patients and doctors, should ensure the continuity of the funds intended for the programs thus avoiding delays in the payment of services, simplify the bureaucratic procedures and modify the functioning of the screening program by allowing the participation of other medical categories, thus avoiding staff shortages. Another important of mitigating the impact of cervical cancer in Romania is the gender-neutrality of HPV vaccination campaigns.
Author Contributions
Conceptualization, Laurentiu Simion, Vlad Rotaru and Elena Chitoran; Data curation, Daniela-Cristina Stefan, Horia Doran and Elena Chitoran; Formal analysis, Ciprian Cirimbei, Laurentia Gales, Daniela-Cristina Stefan, Horia Doran and Elena Chitoran; Investigation, Dan Luca; Methodology, Vlad Rotaru, Sinziana Ionescu and Elena Chitoran; Project administration, Laurentiu Simion and Elena Chitoran; Resources, Vlad Rotaru, Sinziana Ionescu and Dan Luca; Software, Sinziana Ionescu and Dan Luca; Supervision, Laurentiu Simion; Validation, Laurentiu Simion, Ciprian Cirimbei, Laurentia Gales and Daniela-Cristina Stefan; Visualization, Ciprian Cirimbei and Laurentia Gales; Writing – original draft, Vlad Rotaru and Elena Chitoran; Writing – review & editing, Laurentiu Simion. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of Bucharest Oncological Institute “Prof. Dr. Alexandru Trestioreanu”.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study that answered the questionnaire. Permission for statistical analysis and data extraction from the internal database of the Institution was obtained prior to study.
Data Availability Statement
Since it involves personal data, due to privacy issues, data will be available upon request by e-mail to E.C.
Conflicts of Interest
V.R. and E.C. are the coordinators of the National Cervical Cancer Screening Program for the South-Eastern part of Romania and Bucharest-Ilfov region respectively since 2023. The authors declare no other conflict of interest.
References
- Todor, R.D.; Bratucu, G.; Moga, M.A.; Candrea, A.N.; Marceanu, L.G.; Anastasiu, C.V. Challenges in the Prevention of Cervical Cancer in Romania. Int J Environ Res Public Health 2021, 18, 1–14. [Google Scholar] [CrossRef]
- World Health Organization Cancer Today. Available online: https://gco.iarc.fr/today/home (accessed on 5 June 2023).
- Agache, A.; Mustãåea, P.; Mihalache, O.; Bobîrca, F.T.; Georgescu, D.E.; Jauca, C.M.; Bîrligea, A.; Doran, H.; Pãtraaecu, T. Diabetes Mellitus as a Risk-Factor for Colorectal Cancer Literature Review-Current Situation and Future Perspectives. Chirurgia (Bucur) 2018, 113. [Google Scholar] [CrossRef] [PubMed]
- Organization, W.H. WHO Guidance Note: Comprehensive Cervical Cancer Prevention and Control: A Healthier Future for Girls and Women. 2013.
- Gaffney, D.K.; Hashibe, M.; Kepka, D.; Maurer, K.A.; Werner, T.L. Too Many Women Are Dying from Cervix Cancer: Problems and Solutions. Gynecol Oncol 2018, 151, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Simms, K.T.; Steinberg, J.; Caruana, M.; Smith, M.A.; Lew, J. Bin; Soerjomataram, I.; Castle, P.E.; Bray, F.; Canfell, K. Impact of Scaled up Human Papillomavirus Vaccination and Cervical Screening and the Potential for Global Elimination of Cervical Cancer in 181 Countries, 2020–2099: A Modelling Study. Lancet Oncol 2019, 20, 394–407. [Google Scholar] [CrossRef] [PubMed]
- World Bank Romania’s Income Level. Available online: https://data.worldbank.org/?locations=RO-XT (accessed on 16 July 2023).
- Institutul national de statistica Statistici Isnne. Available online: http://statistici.insse.ro:8077/tempo-online (accessed on 5 June 2023).
- Trifanescu, O.G.; Gales, L.; Bacinschi, X.; Serbanescu, L.; Georgescu, M.; Sandu, A.; Michire, A.; Anghel, R. Impact of the COVID-19 Pandemic on Treatment and Oncologic Outcomes for Cancer Patients in Romania. In Vivo (Brooklyn) 2022, 36, 934–941. [Google Scholar] [CrossRef]
- Rural Population (% of Total Population) | Data. Available online: https://data.worldbank.org/indicator/SP.RUR.TOTL.ZS?view=chart (accessed on 16 July 2023).
- European Commission Health Europa. Available online: https://health.ec.europa.eu/system/files/2022-12/2022_healthatglance_rep_en_0.pdf (accessed on 5 June 2023).
- Human Papillomavirus and Related Diseases Report WORLD. Available online: www.hpvcentre.net/statistics/report/XWX.pdf (accessed on 13 June 2023).
- Ilisiu, M.B.; Hashim, D.; Andreassen, T.; Støer, N.C.; Nicula, F.; Weiderpass, E. HPV Testing for Cervical Cancer in Romania: High-Risk HPV Prevalence among Ethnic Subpopulations and Regions. Ann Glob Health 2019, 85. [Google Scholar] [CrossRef]
- Anttila, A.; Ronco, G. Description of the National Situation of Cervical Cancer Screening in the Member States of the European Union. Eur J Cancer 2009, 45, 2685–2708. [Google Scholar] [CrossRef]
- Todorova, I.L.G.; Baban, A.; Balabanova, D.; Panayotova, Y.; Bradley, J. Providers’ Constructions of the Role of Women in Cervical Cancer Screening in Bulgaria and Romania. Soc Sci Med 2006, 63, 776–787. [Google Scholar] [CrossRef]
- Arbyn, M.; Raifu, A.O.; Weiderpass, E.; Bray, F.; Anttila, A. Trends of Cervical Cancer Mortality in the Member States of the European Union. Eur J Cancer 2009, 45, 2640–2648. [Google Scholar] [CrossRef]
- Peirson, L.; Fitzpatrick-Lewis, D.; Ciliska, D.; Warren, R. Screening for Cervical Cancer: A Systematic Review and Meta-Analysis. Syst Rev 2013, 2. [Google Scholar] [CrossRef]
- Jansen, E.E.L.; Zielonke, N.; Gini, A.; Anttila, A.; Segnan, N.; Vokó, Z.; Ska Ivanu, U.; Mckee, M.; De Koning, H.J.; De Kok, I.M.C.M. Effect of Organised Cervical Cancer Screening on Cervical Cancer Mortality in Europe: A Systematic Review. Eur J Cancer 2020, 127, 207–223. [Google Scholar] [CrossRef] [PubMed]
- Furtunescu, F.; Bohiltea, R.E.; Neacsu, A.; Grigoriu, C.; Pop, C.S.; Bacalbasa, N.; Ducu, I.; Iordache, A.M.; Costea, R.V. Cervical Cancer Mortality in Romania: Trends, Regional and Rural–Urban Inequalities, and Policy Implications. Medicina (B Aires) 2022, 58, 18. [CrossRef]
- EU Commission: Council Recommendation of 2 December... - Google Academic. Available online: https://scholar.google.com/scholar_lookup?journal=Off.+J.+Eur.+Union&title=Council+recommendation+of+2+December+2003+on+cancer+screening+(2003/878/EC)&volume=327&publication_year=2003&pages=34-38& (accessed on 16 July 2023).
- Ponti, A.; Anttila, A.; Ronco, G.; Senore, C. Cancer Screening in the European Union (2017). Report on the Implementation of the Council Recommendation on Cancer Screening. Cancer screening in the European Union (2017). Report on the implementation of the council recommendation on cancer screening. 2017.
- Nicula, F. Al; Anttila, A.; Neamtiu, L.; Žakelj, M.P.; Tachezy, R.; Chil, A.; Grce, M.; Kesić, V. Challenges in Starting Organised Screening Programmes for Cervical Cancer in the New Member States of the European Union. Eur J Cancer 2009, 45, 2679–2684. [Google Scholar] [CrossRef] [PubMed]
- Furtunescu, F.; Bohiltea, R.E.; Voinea, S.; Georgescu, T.A.; Munteanu, O.; Neacsu, A.; Pop, C.S. Breast Cancer Mortality Gaps in Romanian Women Compared to the EU after 10 Years of Accession: Is Breast Cancer Screening a Priority for Action in Romania? (Review of the Statistics). Exp Ther Med 2021, 21. [Google Scholar] [CrossRef] [PubMed]
- Elfström, K.M.; Arnheim-Dahlström, L.; Von Karsa, L.; Dillner, J. Cervical Cancer Screening in Europe: Quality Assurance and Organisation of Programmes. Eur J Cancer 2015, 51, 950–968. [Google Scholar] [CrossRef]
- Wojtyla, C.; Janik-Koncewicz, K.; La Vecchia, C. Cervical Cancer Mortality in Young Adult European Women. Eur J Cancer 2020, 126, 56–64. [Google Scholar] [CrossRef]
- Altobelli, E.; Lattanzi, A. Cervical Carcinoma in the European Union: An Update on Disease Burden, Screening Program State of Activation, and Coverage as of March 2014. Int. J. Gynecol. Cancer 2015, 25, 474–483. [Google Scholar] [CrossRef]
- Kesic, V. Prevention of Cervical Cancer in Central and Eastern Europe and Central Asia: A Challenge for the Future. Vaccine 2013, 31, vii–ix. [Google Scholar] [CrossRef]
- Nicula, F. Al; Anttila, A.; Neamtiu, L.; Žakelj, M.P.; Tachezy, R.; Chil, A.; Grce, M.; Kesić, V. Challenges in Starting Organised Screening Programmes for Cervical Cancer in the New Member States of the European Union. Eur J Cancer 2009, 45, 2679–2684. [Google Scholar] [CrossRef]
- Eniu, A.; Dumitraşcu, D.; Geanta, M. Romania, Attempting to Catch up the European Standards of Care for Cancer Patients. Cancer Care Ctries. Soc. Transit. Individ. Care Focus 2016, 361–374. [Google Scholar] [CrossRef]
- Romania’s National Cancer Plan. Available online: https://www.ms.ro/media/documents/Planul_Na%C8%9Bional_de_Combatere_%C8%99i_Control_al_Cancerului_RIQiTXG.pdf (accessed on 16 July 2023).
- Sănătății, M. ACTE ALE ORGANELOR DE SPECIALITATE ALE ADMINISTRAȚIEI PUBLICE CENTRALE O R D I N Privind Aprobarea Normelor Tehnice de Realizare a Programelor Naționale de Sănătate Publică*) – order given by the Romanian Ministry of Health.
- Official Statistics in Romania | National Institute of Statistics. Available online: https://insse.ro/cms/en/content/official-statistics-romania (accessed on 17 July 2023).
- Romania’s Cervical Cancer Country Profile. Available online: https://www.iccp-portal.org/system/files/plans/cervical-cancer-rou-2021-country-profile-en.pdf (accessed on 16 July 2023).
- Hajioff, S.; McKee, M. The Health of the Roma People: A Review of the Published Literature. J Epidemiol Community Health (1978) 2000, 54, 864–869. [Google Scholar] [CrossRef]
- Andreassen, T.; Melnic, A.; Figueiredo, R.; Moen, K.; Şuteu, O.; Nicula, F.; Ursin, G.; Weiderpass, E. Attendance to Cervical Cancer Screening among Roma and Non-Roma Women Living in North-Western Region of Romania. Int J Public Health 2018, 63, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Andreassen, T.; Weiderpass, E.; Nicula, F.; Suteu, O.; Itu, A.; Bumbu, M.; Tincu, A.; Ursin, G.; Moen, K. Controversies about Cervical Cancer Screening: A Qualitative Study of Roma Women’s (Non) Participation in Cervical Cancer Screening in Romania. Soc Sci Med 2017, 183, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Rada, C. Sexual Behavior and Sexual and Reproductive Health Education: A Cross-Sectional Study in Romania. Reprod Health 2014, 11, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Balazsi, R.; Bradley, J.; Szentagotai-Tatar, A. Psychosocial and Health System Dimensions of Cervical Screening in Romania OPEN RES View Project a Computational Distributed System to Support the Treatment of Patients with Major Depression (Help4Mood). View Project; 2000.
- Todorova, I.; Baban, A.; Alexandrova-Karamanova, A.; Bradley, J. Inequalities in Cervical Cancer Screening in Eastern Europe: Perspectives from Bulgaria and Romania. Int J Public Health 2009, 54, 222–232. [Google Scholar] [CrossRef]
- Gherghe, M.; Mutuleanu, M.D.; Stanciu, A.E.; Irimescu, I.; Lazar, A.; Bacinschi, X.; Anghel, R.M. Quantitative Analysis of SPECT-CT Data in Metastatic Breast Cancer Patients—The Clinical Significance. Cancers (Basel) 2022, 14. [Google Scholar] [CrossRef]
- Pãtrascu, Tr.; Doran, H.; Catrina, E.; Mihalache, O.; Degeratu, D.; Predescu, G. Tumori Sincrone Ale Tractului Digestiv. Chirurgia (Bucur) 2010, 0. [Google Scholar]
- Cirimbei, C.; Rotaru, V.; Radu, M.; Cirimbei, S.E. Association of Colorectal Cancer and GIST Tumors - A Diagnostic and Therapeutic Challenge: A Case Report. Int. Res. J. Med. Med. Sci. 2020, 8, 25–29. [Google Scholar] [CrossRef]
- Simion, L.; Rotaru, V.; Cirimbei, S.; Chitoran, E.; Gales, L.; Luca, D.C.; Ionescu, S.; Tanase, B.; Ginghina, O.; Alecu, M.; et al. Simultaneous Approach of Colo-Rectal and Hepatic Lesions in Colo-Rectal Cancers with Liver Metastasis - A Single Oncological Center Overview. Chirurgia (Bucur) 2023, 118. [Google Scholar] [CrossRef]
- Programul National de Oncologie. Available online: http://www.casan.ro/page/programul-national-de-oncologie.html (accessed on 17 July 2023).
- Cirimbei, C.; Rotaru, V.; Chitoran, E.; Cirimbei, S. Laparoscopic Approach in Abdominal Oncologic Pathology, Proceedings of the 35th Balkan Medical Week, Athens, Greece, 25-27 September 2018. Available online: https://www.webofscience.com/wos/woscc/full-record/WOS:000471903700043 (accessed on 20 July 2023).
- Rotaru, V.; Chitoran, E.; Cirimbei, C.; Cirimbei, S.; Simion, L. Preservation of Sensory Nerves During Axillary Lymphadenectomy, Proceedings of the 35th Balkan Medical Week, Athens, Greece, 25-27 September 2018. Available online: https://www.webofscience.com/wos/woscc/full-record/WOS:000471903700045 (accessed on 20 July 2023).
- Gheghe, M.; Bordea, C.; Blidaru, Al. Clinical Significance of the Lymphoscintigraphy in the Evaluation of Non-Axillary Sentinel Lymph Node Localization in Breast Cancer. Chirurgia (Bucur) 2015, 110, 26–32. [Google Scholar]
- Simion, L.; Ionescu, S.; Chitoran, E.; Rotaru, V.; Cirimbei, C.; Madge, O.L.; Nicolescu, A.C.; Gherghe, M.; Tanase, B.; Andreescu, I.G.D.; et al. Indocyanine Green (Icg) And Colorectal Surgery: A Literature Review on Qualitative and Quantitative Methods of Usage. 2023. [CrossRef]
- Bordea, C.; Plesca, M.; Condrea, I.; Gherghe, M.; Gociman, A.; Blidaru, A. Occult Breast Lesion Localization and Concomitant Sentinel Lymph Node Biopsy in Early Breast Cancer (SNOLL). Chirurgia (Bucur) 2012, 107, 722–729. [Google Scholar] [CrossRef]
- Simion, L.; Rotaru, V.; Cirimbei, C.; Stefan, D.C.; Gherghe, M.; Ionescu, S.; Tanase, B.C.; Luca, D.C.; Gales, L.N.; Chitoran, E. Analysis of Efficacy-To-Safety Ratio of Angiogenesis-Inhibitors Based Therapies in Ovarian Cancer: A Systematic Review and Meta-Analysis. Diagnostics 2023, 13. [Google Scholar] [CrossRef] [PubMed]
- Romanian Ministry of Health Vaccinarea Populației La Vârstele Prevăzute În Calendarul Național de Vaccinare.
- Simion, L.; Chitoran, E.; Cirimbei, C.; Stefan, D.-C.; Neicu, A.; Tanase, B.; Ionescu, S.O.; Luca, D.C.; Gales, L.; Gheorghe, A.S.; et al. A Decade of Therapeutic Challenges in Synchronous Gynecological Cancers from the Bucharest Oncological Institute. Diagnostics 2023, 13, 2069. [Google Scholar] [CrossRef] [PubMed]
- Maier, C.; Maier, T.; Neagu, C.E.; Vlədəreanu, R. Romanian Adolescents’ Knowledge and Attitudes towards Human Papillomavirus Infection and Prophylactic Vaccination. European Journal of Obstetrics and Gynecology and Reproductive Biology 2015, 195, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Sabina Cornelia Manolescu, L.; Iulia Mitran, C.; Irina Mitran, M.; Roxana Georgescu, S.; Tampa, M.; Suciu, I.; Suciu, G.; Preda, M.; Cerasella Dragomirescu, C.; Loredana Popa, G.; et al. Knowledge, attitude and perception towards the hpv infection and immunization among romanian medical students. ROMANIAN ARCHIVES OF MICROBIOLOGY AND IMMUNOLOGY 80, 22–34.
- Pent¸a, M.A.P.; Ba, A. Mass Media Coverage of HPV Vaccination in Romania: A Content Analysis. [CrossRef]
- Manolescu, L.S.C.; Zugravu, C.; Zaharia, C.N.; Dumitrescu, A.I.; Prasacu, I.; Radu, M.C.; Letiția, G.D.; Nita, I.; Cristache, C.M.; Gales, L.N. Barriers and Facilitators of Romanian HPV (Human Papillomavirus) Vaccination. Vaccines (Basel) 2022, 10. [Google Scholar] [CrossRef]
- Chen, G.; Wu, B.; Dai, X.; Zhang, M.; Liu, Y.; Huang, H.; Mei, K.; Wu, Z. Gender Differences in Knowledge and Attitude towards HPV and HPV Vaccine among College Students in Wenzhou, China. Vaccines (Basel) 2021, 10. [Google Scholar] [CrossRef]
- Goessl, C.L.; Christianson, B.; Hanson, K.E.; Polter, E.J.; Olson, S.C.; Boyce, T.G.; Dunn, D.; Williams, C.L.; Belongia, E.A.; McLean, H.Q.; et al. Human Papillomavirus Vaccine Beliefs and Practice Characteristics in Rural and Urban Adolescent Care Providers. BMC Public Health 2022, 22. [Google Scholar] [CrossRef]
- Degarege, A.; Krupp, K.; Fennie, K.; Li, T.; Stephens, D.P.; Marlow, L.A.V.; Srinivas, V.; Arun, A.; Madhivanan, P. Urban-Rural Inequities in the Parental Attitudes and Beliefs Towards Human Papillomavirus Infection, Cervical Cancer, and Human Papillomavirus Vaccine in Mysore, India. J Pediatr Adolesc Gynecol 2018, 31, 494–502. [Google Scholar] [CrossRef]
- Lu, P. jun; O’Halloran, A.; Kennedy, E.D.; Williams, W.W.; Kim, D.; Fiebelkorn, A.P.; Donahue, S.; Bridges, C.B. Awareness among Adults of Vaccine-Preventable Diseases and Recommended Vaccinations, United States, 2015. Vaccine 2017, 35, 3104. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Mahzoum, K.; Eid, H.; Assaf, A.M.; Abdaljaleel, M.; Al-Abbadi, M.; Mahafzah, A. Attitude towards HPV Vaccination and the Intention to Get Vaccinated among Female University Students in Health Schools in Jordan. Vaccines (Basel) 2021, 9. [Google Scholar] [CrossRef]
- Popa, G.L.; Muntean, A.A.; Muntean, M.M.; Popa, M.I. Knowledge and Attitudes on Vaccination in Southern Romanians: A Cross-Sectional Questionnaire. Vaccines (Basel) 2020, 8, 1–7. [Google Scholar] [CrossRef]
- Lin, C.; Mullen, J.; Smith, D.; Kotarba, M.; Kaplan, S.J.; Tu, P. Healthcare Providers’ Vaccine Perceptions, Hesitancy, and Recommendation to Patients: A Systematic Review. Vaccines (Basel) 2021, 9. [Google Scholar] [CrossRef]
- Paul, P.; Fabio, A. Literature Review of HPV Vaccine Delivery Strategies: Considerations for School- and Non-School Based Immunization Program. Vaccine 2014, 32, 320–326. [Google Scholar] [CrossRef]
- Lin, C.; Mullen, J.; Smith, D.; Kotarba, M.; Kaplan, S.J.; Tu, P. Healthcare Providers’ Vaccine Perceptions, Hesitancy, and Recommendation to Patients: A Systematic Review. Vaccines (Basel) 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Pagliusi, S.R.; Aguado, M.T. Efficacy and Other Milestones for Human Papillomavirus Vaccine Introduction. Vaccine 2004, 23, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Syrjänen, K.J.; Pyrhönen, S.; Syrjänen, S.M.; Lamberg, M.A. Immunohistochemical Demonstration of Human Papilloma Virus (HPV) Antigens in Oral Squamous Cell Lesions. British Journal of Oral Surgery 1983, 21, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Pytynia, K.B.; Dahlstrom, K.R.; Sturgis, E.M. Epidemiology of HPV-Associated Oropharyngeal Cancer. Oral Oncol 2014, 50, 380–386. [Google Scholar] [CrossRef]
- Spence, T.; Bruce, J.; Yip, K.W.; Liu, F.F. HPV Associated Head and Neck Cancer. Cancers 2016, 8, 75. [Google Scholar] [CrossRef] [PubMed]
- Bratman, S. V.; Bruce, J.P.; O’Sullivan, B.; Pugh, T.J.; Xu, W.; Yip, K.W.; Liu, F.F. Human Papillomavirus Genotype Association with Survival in Head and Neck Squamous Cell Carcinoma. JAMA Oncol 2016, 2, 823–826. [Google Scholar] [CrossRef]
- Chahoud, J.; Semaan, A.; Chen, Y.; Cao, M.; Rieber, A.G.; Rady, P.; Tyring, S.K. Association between β-Genus Human Papillomavirus and Cutaneous Squamous Cell Carcinoma in Immunocompetent Individuals-a Meta-Analysis. JAMA Dermatol 2016, 152, 1354–1364. [Google Scholar] [CrossRef]
- Connolly, K.; Manders, P.; Earls, P.; Epstein, R.J. Papillomavirus-Associated Squamous Skin Cancers Following Transplant Immunosuppression: One Notch Closer to Control. Cancer Treat Rev 2014, 40, 205–214. [Google Scholar] [CrossRef]
- Bandolin, L.; Borsetto, D.; Fussey, J.; Da Mosto, M.C.; Nicolai, P.; Menegaldo, A.; Calabrese, L.; Tommasino, M.; Boscolo-Rizzo, P. Beta Human Papillomaviruses Infection and Skin Carcinogenesis. Rev Med Virol 2020, 30. [Google Scholar] [CrossRef]
- Tampa, M.; Mitran, C.I.; Mitran, M.I.; Nicolae, I.; Dumitru, A.; Matei, C.; Manolescu, L.; Popa, G.L.; Caruntu, C.; Georgescu, S.R. The Role of Beta HPV Types and HPV-Associated Inflammatory Processes in Cutaneous Squamous Cell Carcinoma. J Immunol Res 2020, 2020. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.A.; O’Rorke, M.A.; Wilson, R.; Jamison, J.; Gavin, A.T. HPV Prevalence and Type-Distribution in Cervical Cancer and Premalignant Lesions of the Cervix: A Population-Based Study from Northern Ireland. J Med Virol 2016, 88, 1262–1270. [Google Scholar] [CrossRef] [PubMed]
- Condrat, C.E.; Filip, L.; Gherghe, M.; Cretoiu, D.; Suciu, N. Maternal HPV Infection: Effects on Pregnancy Outcome. Viruses 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Souho, T.; Benlemlih, M.; Bennani, B. Human Papillomavirus Infection and Fertility Alteration: A Systematic Review. PLoS One 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Zullo, F.; Fiano, V.; Gillio-Tos, A.; Leoncini, S.; Nesi, G.; Macrì, L.; Preti, M.; Rolfo, A.; Benedetto, C.; Revelli, A.; et al. Human Papillomavirus Infection in Women Undergoing In-Vitro Fertilization: Effects on Embryo Development Kinetics and Live Birth Rate. Reprod. Biol. Endocrinol. 2023, 21. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, M.; Sar-Shalom Nahshon, C.; Feferkorn, I.; Bornstein, J. Evaluation of Human Papilloma Virus in Semen as a Risk Factor for Low Sperm Quality and Poor in Vitro Fertilization Outcomes: A Systematic Review and Meta-Analysis. Fertil Steril 2020, 113, 955-969.e4. [CrossRef]
- Lehtinen, M.; Söderlund-Strand, A.; Vänskä, S.; Luostarinen, T.; Eriksson, T.; Natunen, K.; Apter, D.; Baussano, I.; Harjula, K.; Hokkanen, M.; et al. Impact of Gender-Neutral or Girls-Only Vaccination against Human Papillomavirus—Results of a Community-Randomized Clinical Trial (I). Int J Cancer 2018, 142, 949–958. [Google Scholar] [CrossRef]
- Vänskä, S.; Luostarinen, T.; Baussano, I.; Apter, D.; Eriksson, T.; Natunen, K.; Nieminen, P.; Paavonen, J.; Pimenoff, V.N.; Pukkala, E.; et al. Vaccination with Moderate Coverage Eradicates Oncogenic Human Papillomaviruses If a Gender-Neutral Strategy Is Applied. J Infect Dis 2020, 222, 948–956. [Google Scholar] [CrossRef]
- de Sanjose, S.; Bruni, L. Is It Now the Time to Plan for Global Gender-Neutral HPV Vaccination? Journal of Infectious Diseases 2020, 222, 888–889. [Google Scholar] [CrossRef]
- Cameron, R.L.; Kavanagh, K.; Pan, J.; Love, J.; Cuschieri, K.; Robertson, C.; Ahmed, S.; Palmer, T.; Pollock, K.G.J. Human Papillomavirus Prevalence and Herd Immunity after Introduction of Vaccination Program, Scotland, 2009–2013. Emerg Infect Dis 2016, 22, 56–64. [Google Scholar] [CrossRef]
Figure 1.
Distribution of responders by age (years).
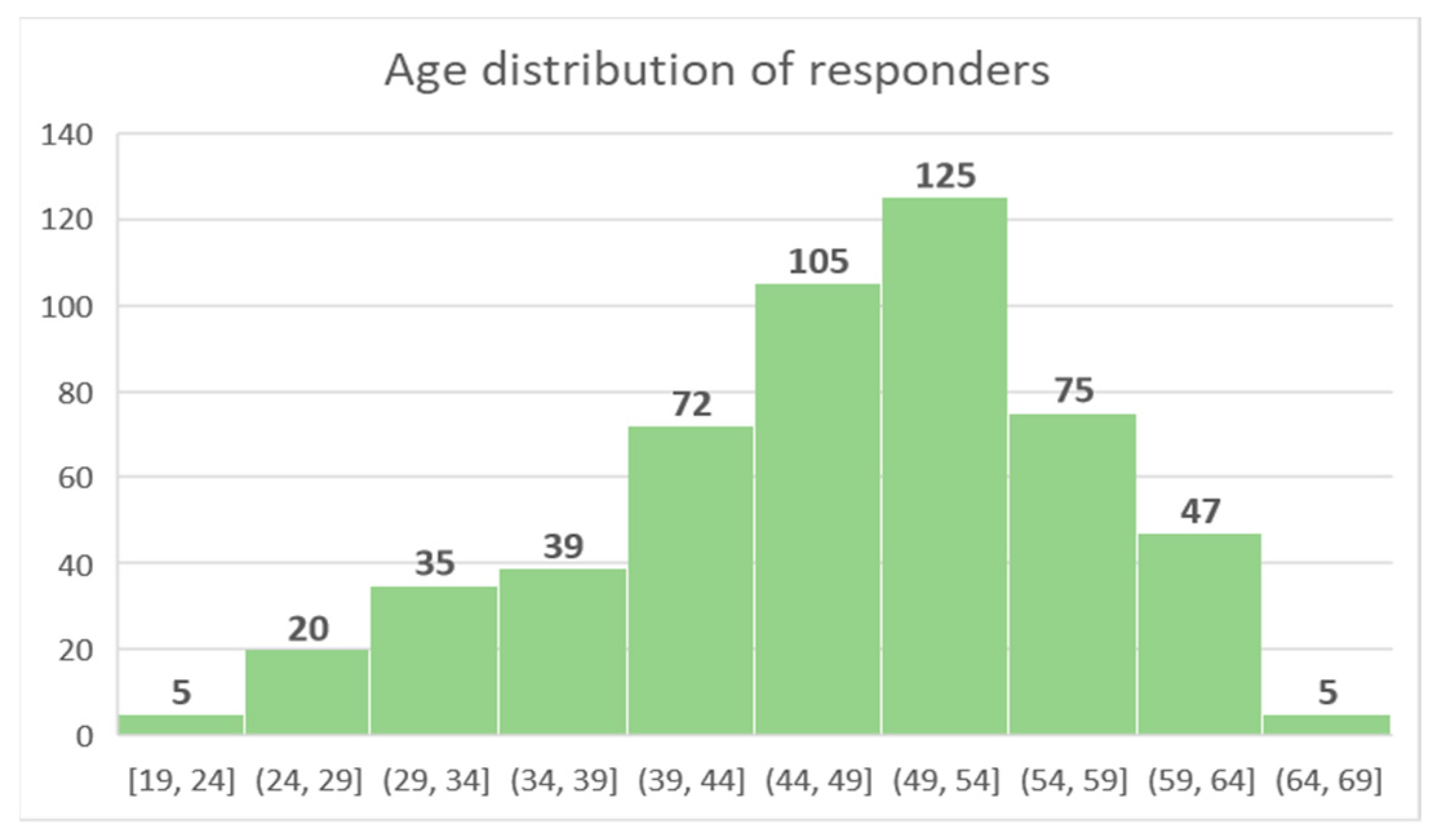
Figure 2.
Distribution of responders by living conditions.
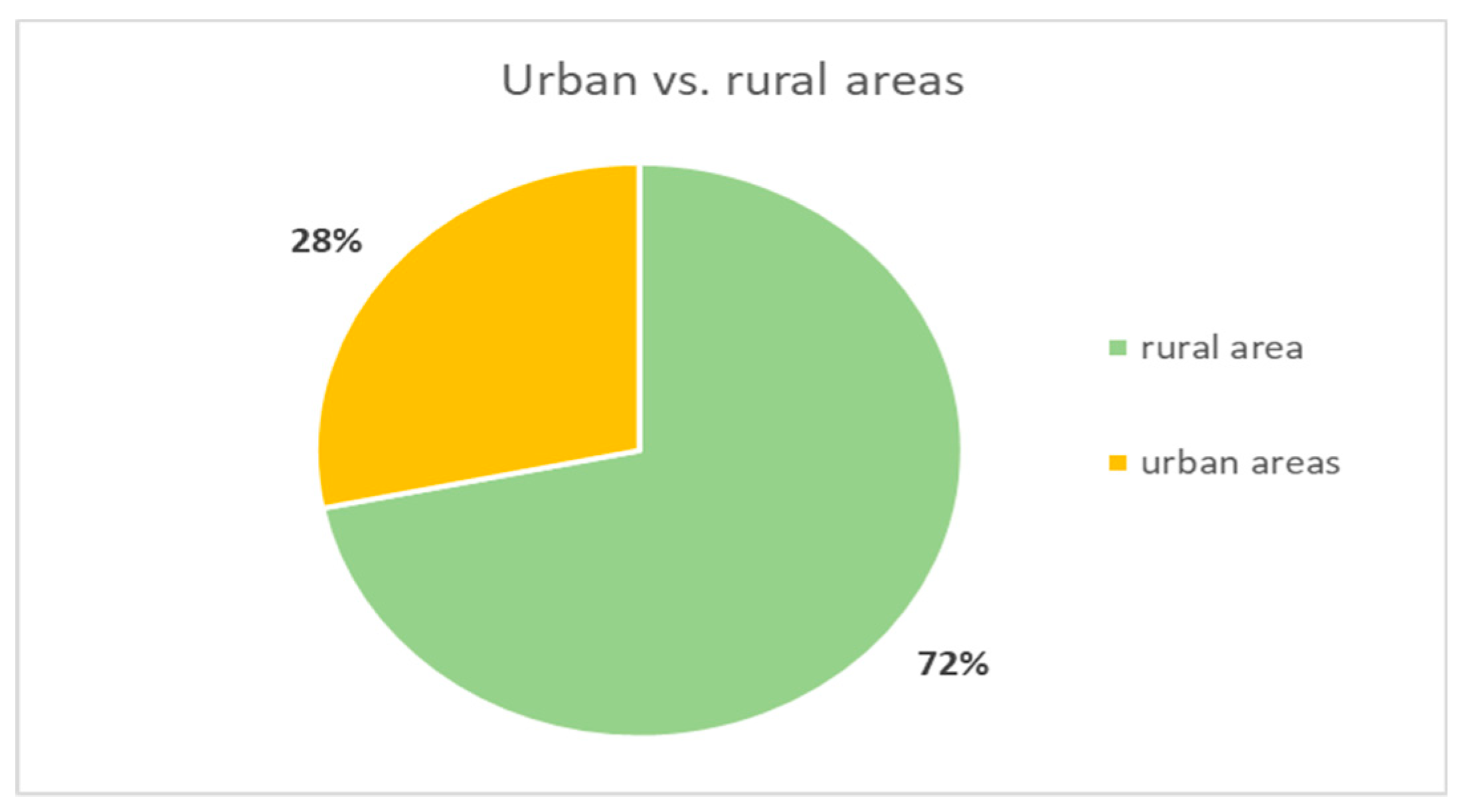
Figure 3.
Distribution of responders by level of education.
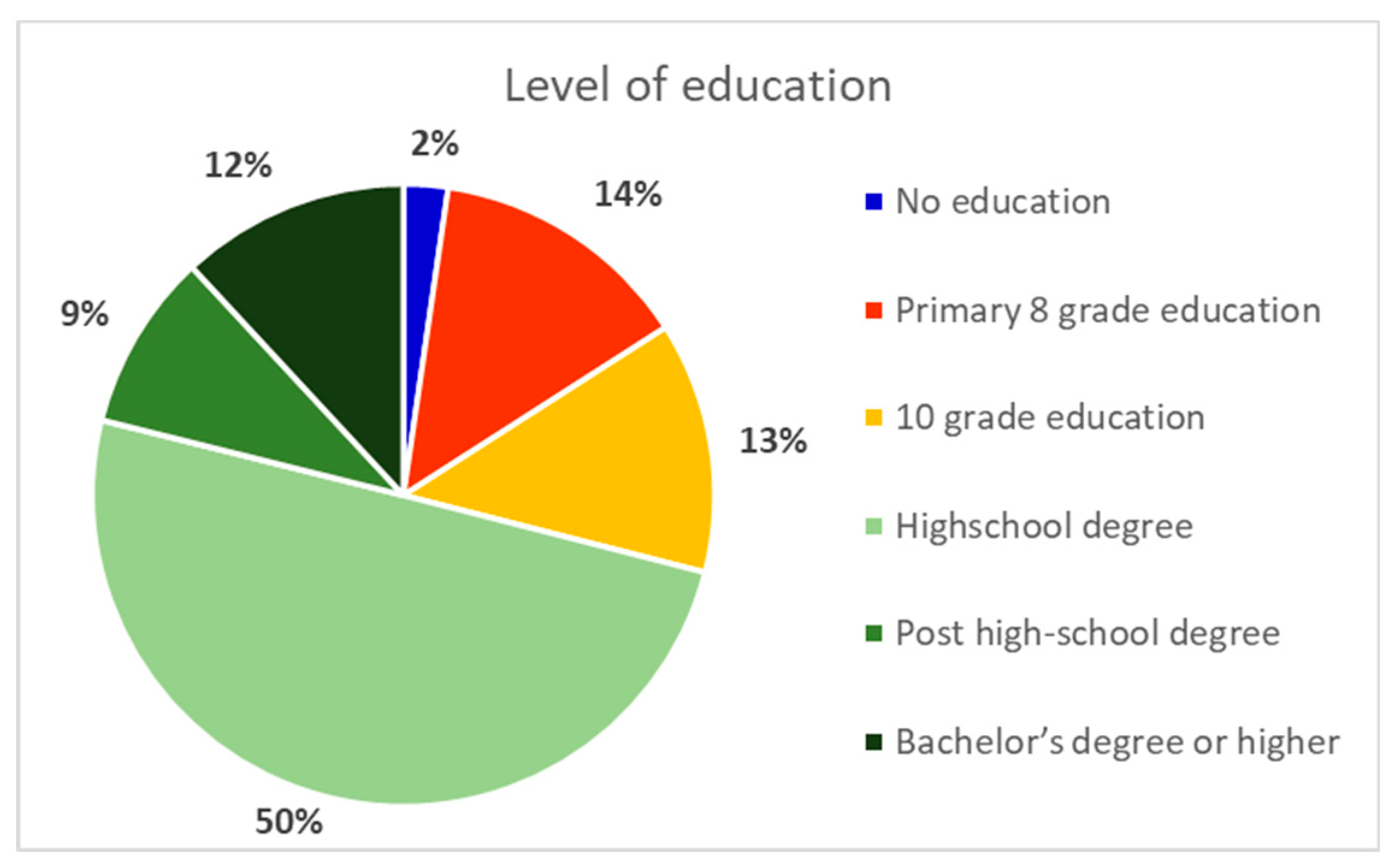
Figure 4.
Time since last Pap-smear.
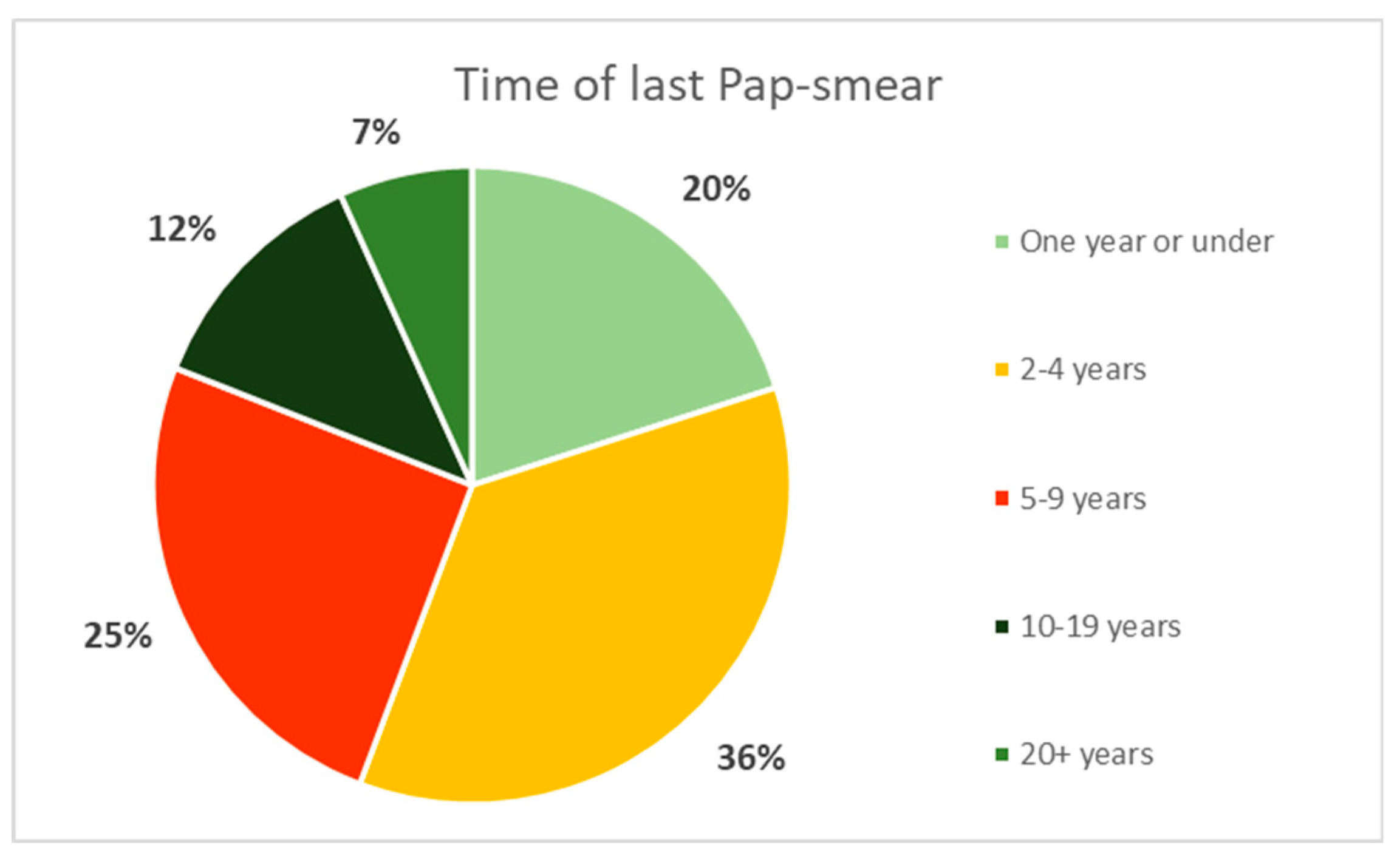
Figure 7.
Knowledge about the connection between HPV and cervical cancer.
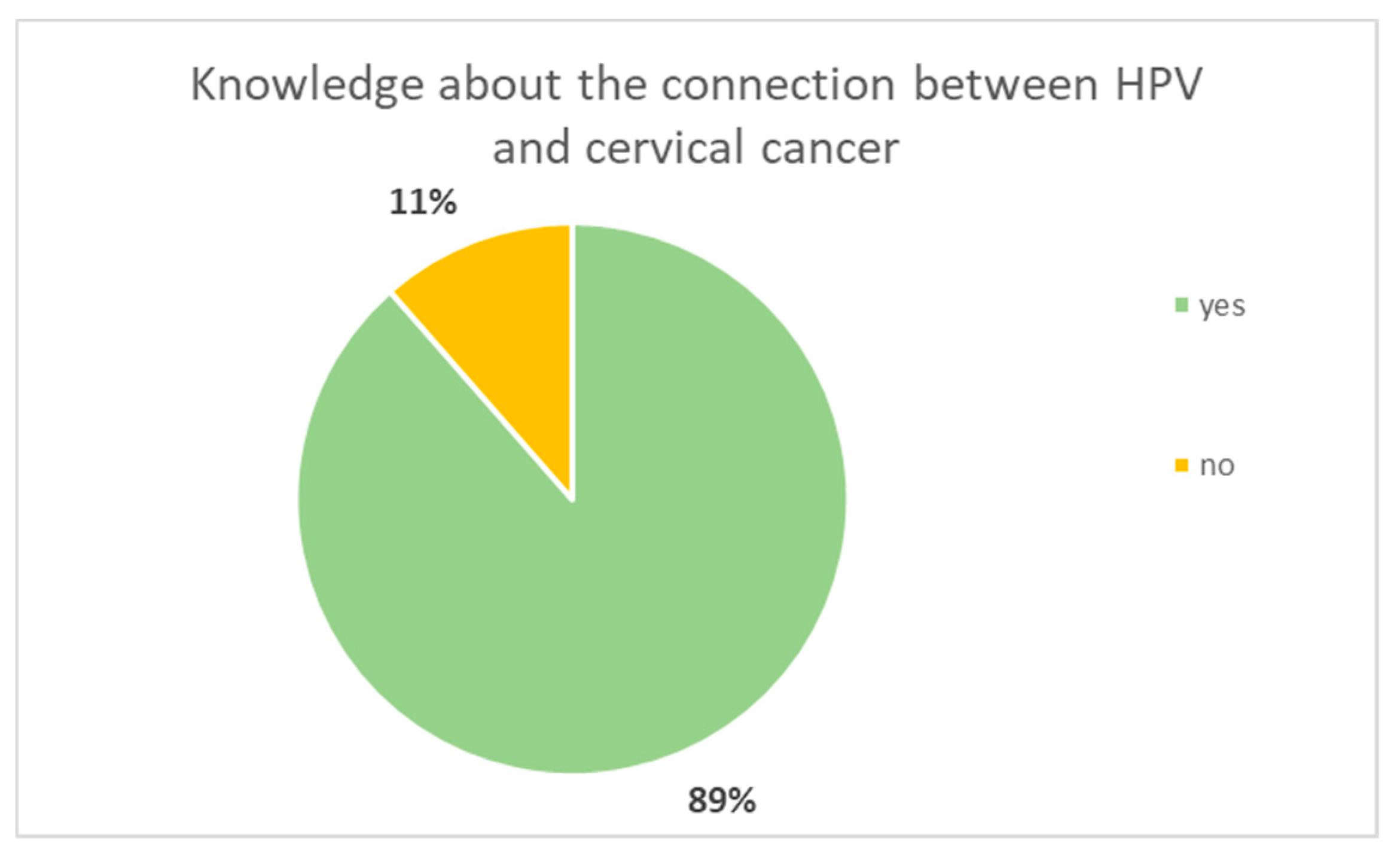
Figure 8.
Knowledge about the existence of a HPV vaccine.
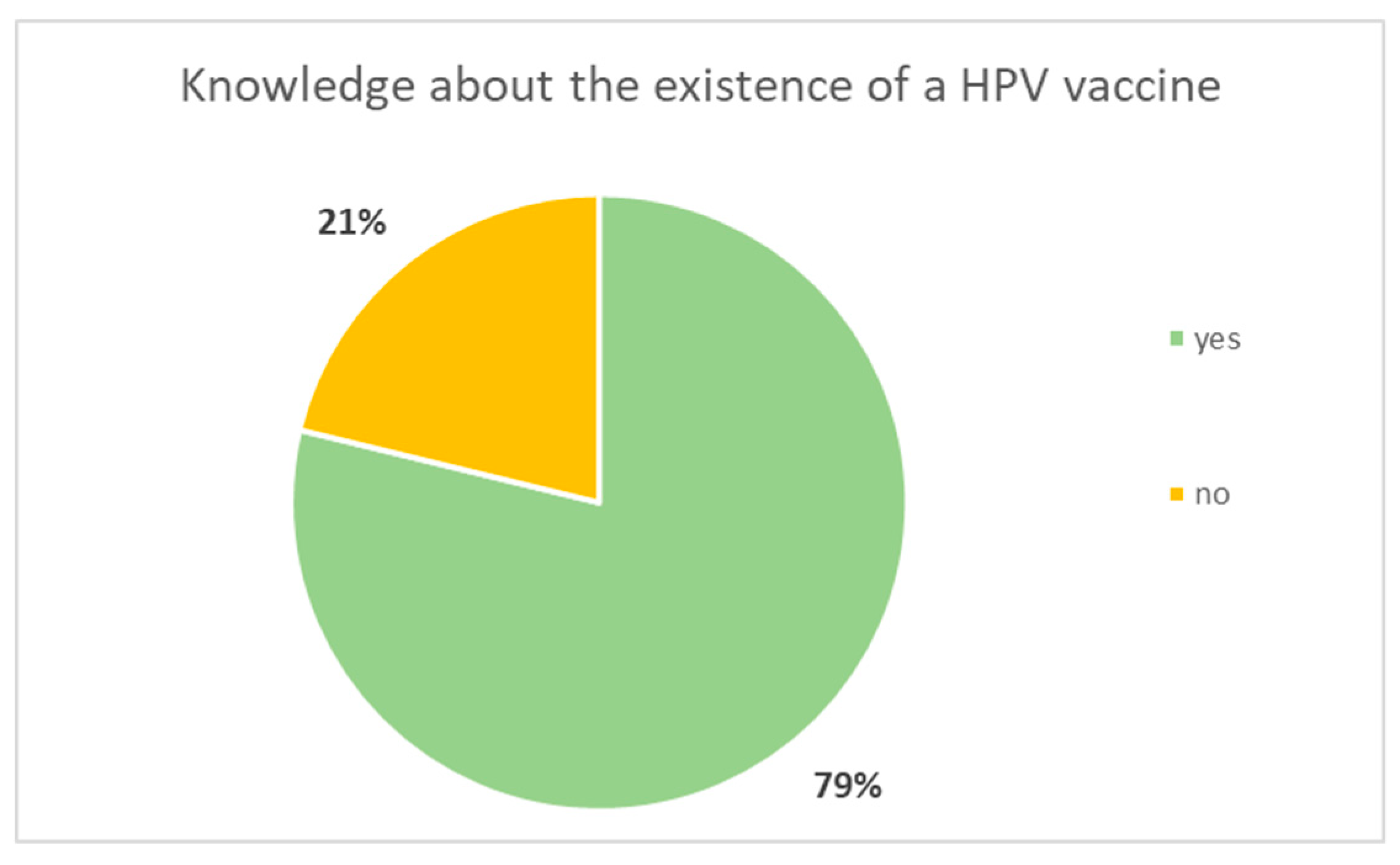
Figure 9.
Status of HPV vaccination.
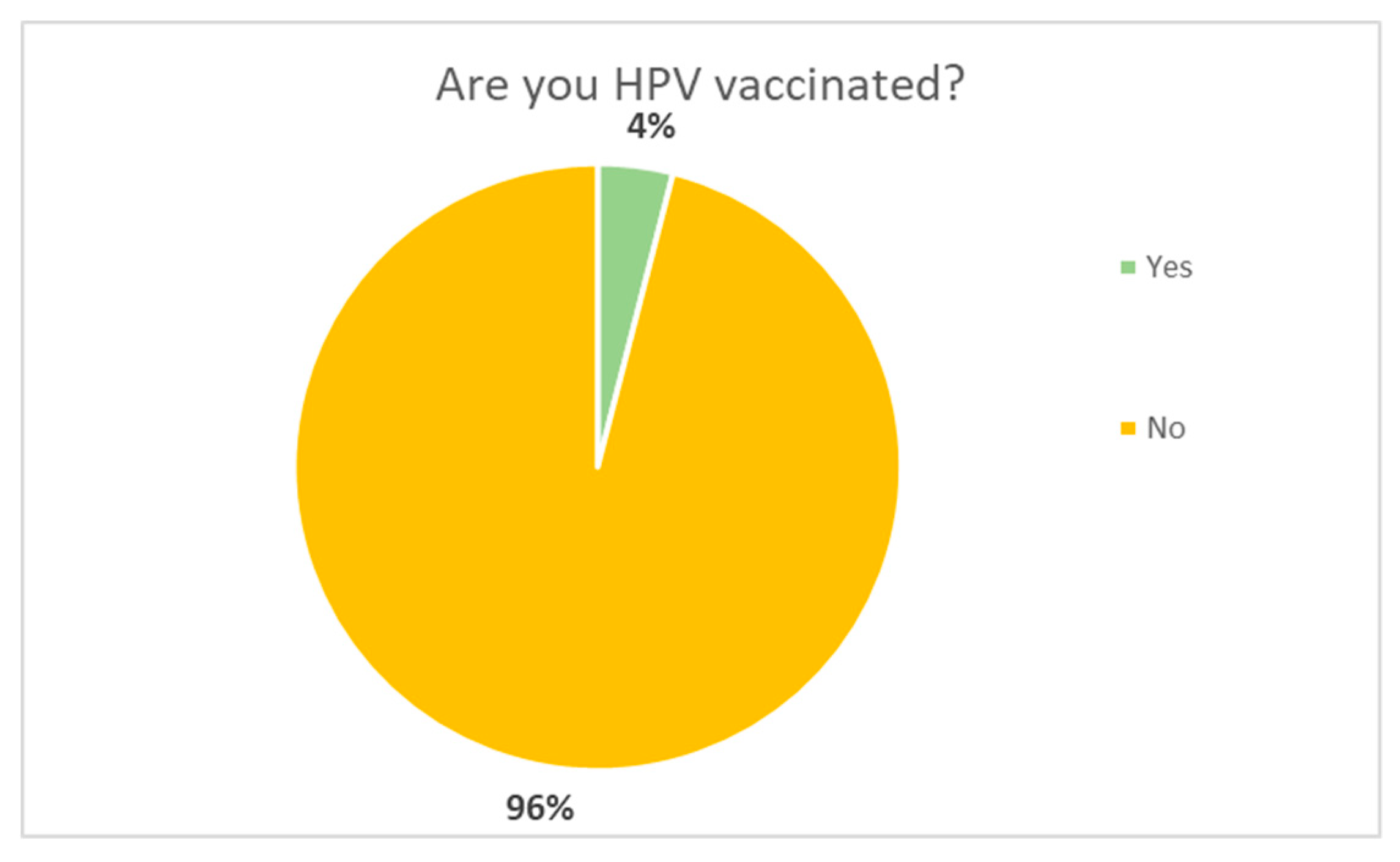
Figure 10.
Knowledge about the free HPV vaccination national program.
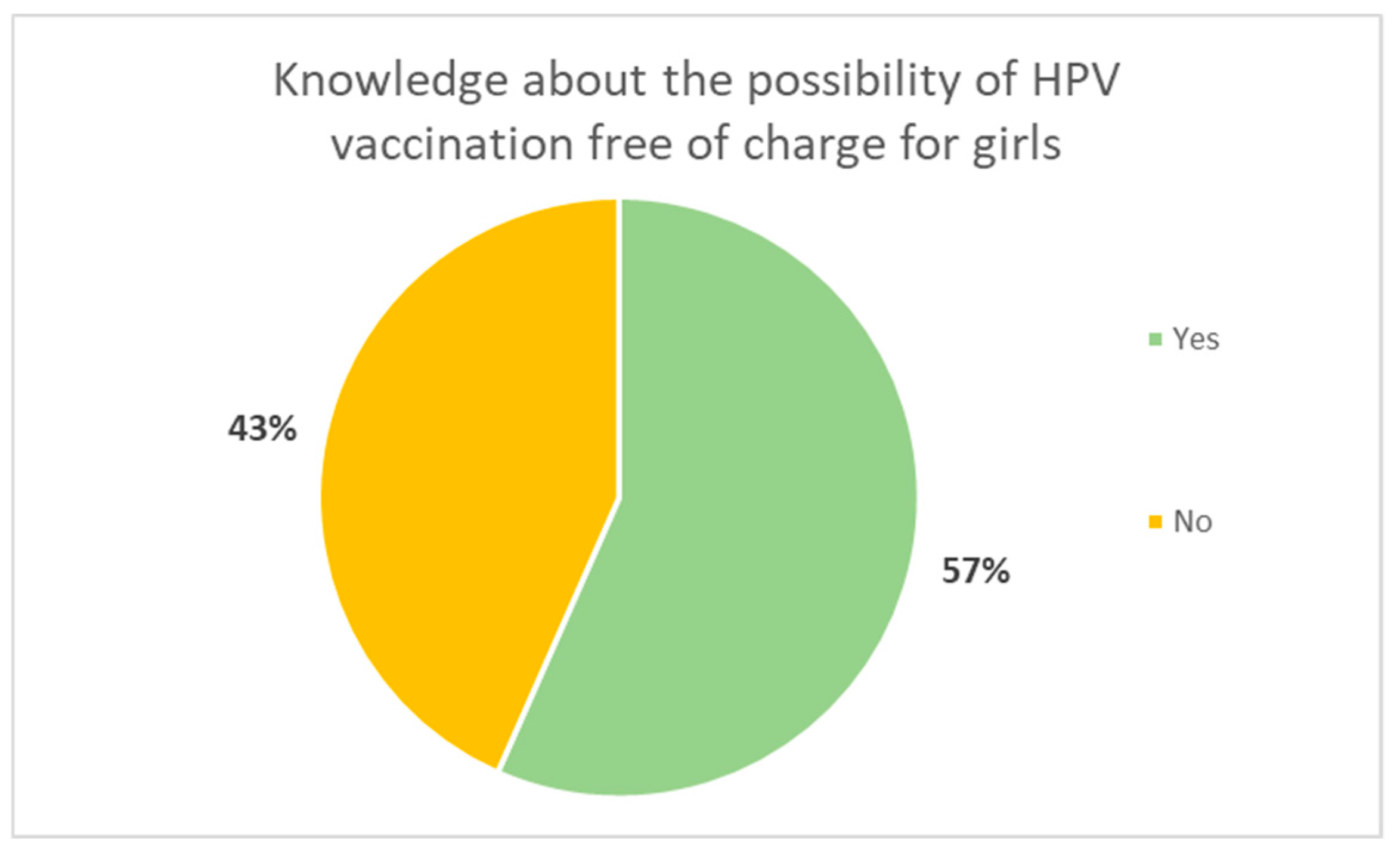
Figure 11.
Responders’ intention of HPV vaccination of their daughters.
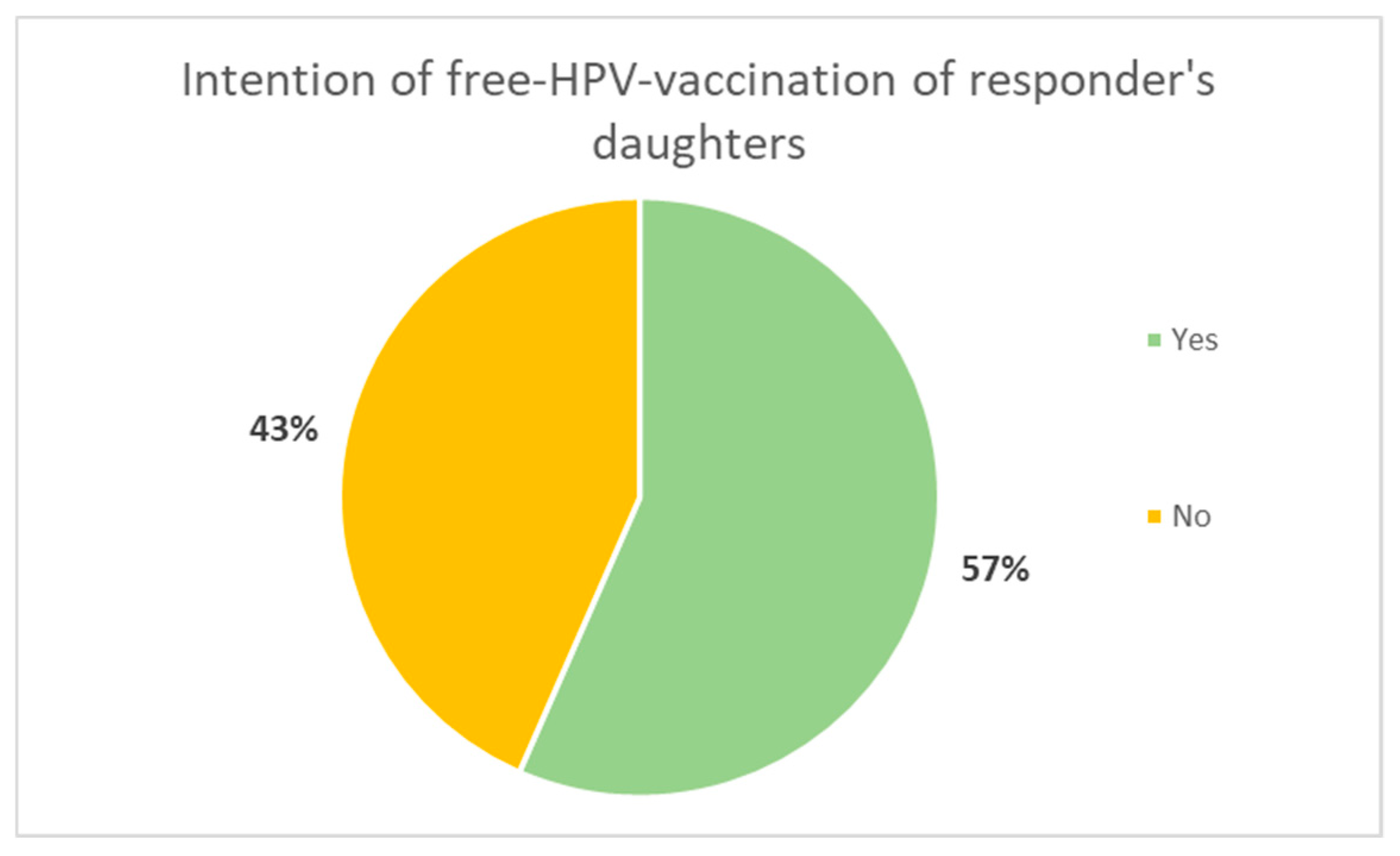
Figure 12.
Reasons given for not wanting to vaccinate children.
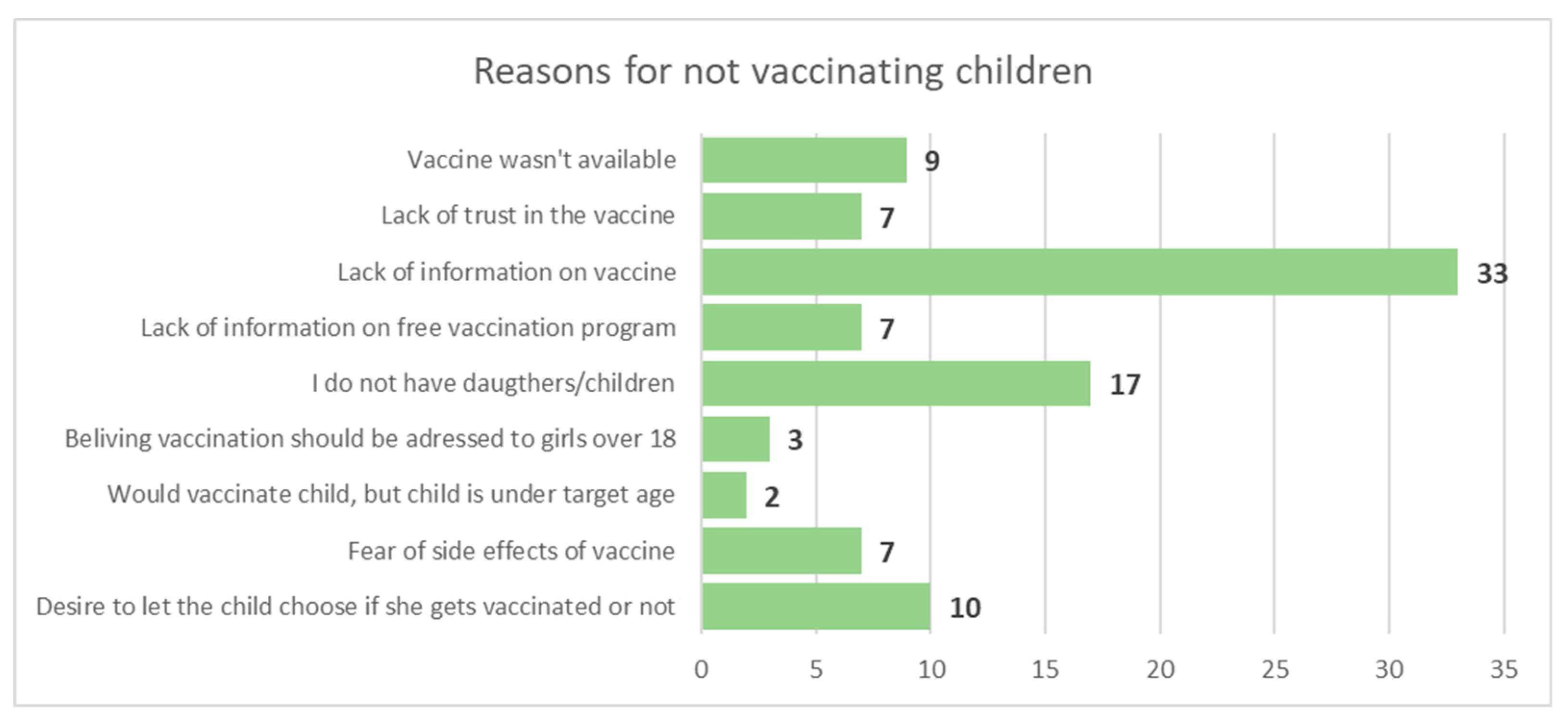
Figure 13.
Comparison between Romanian and European incidence and mortality rates for neoplastic disease in women.
Figure 13.
Comparison between Romanian and European incidence and mortality rates for neoplastic disease in women.
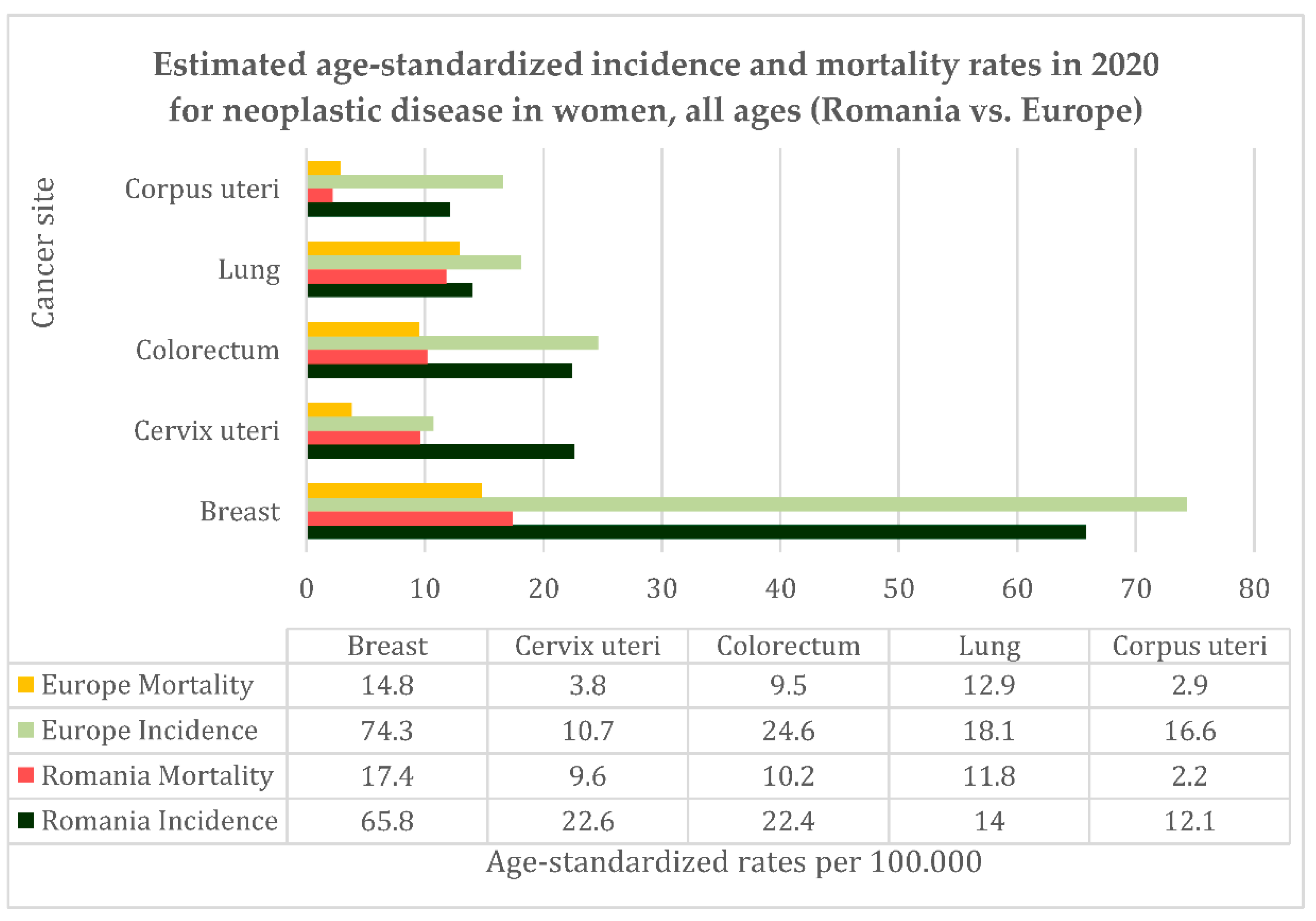

Table 1.
characteristics of questionnaire applied to the women participating in the National Screening Program for Cervical Cancer during testing campaigns in disadvantaged parts of Romania.
Table 1.
characteristics of questionnaire applied to the women participating in the National Screening Program for Cervical Cancer during testing campaigns in disadvantaged parts of Romania.
| Question | Possible responses | |
|---|---|---|
| 1 | Level of education | No education 8 grade education 10 grade education High school degree/ Professional degree Bachelor’s degree or higher |
| 2 | Age | Numerical |
| 3 | Place of residence | Name of town/village |
| 4 | Have you ever been tested before by Pap smear? | YES NO |
| 5 | When have you been tested by Pap smear? | Free form answer |
| 6 | Would you have gone to be tested if the mobile screening unit wouldn’t have come to your town/village? | YES NO |
| 7 | If the answer to the previous question is NO then answer why not? | Lack of financial means Lack of time I do not know where to get tested Nothing is bothering me Other reasons |
| 8 | If you will get a test result that requires other investigations, will you do them? | Definitely yes Probably yes Probably no due to the lack of financial means Probably no due to other reasons Definitely no |
| 9 | Have you ever heard that HPV infection can lead to cervical cancer? | YES NO |
| 10 | Do you know there is an HPV vaccine available? | YES NO |
| 11 | Are you HPV vaccinated? | YES NO |
| 12 | Are you aware that HPV vaccine is freely available for girls at the general practitioner? | YES NO |
| 13 | Knowing this would you vaccinate your daughters? | YES NO |
| 14 | If the answer to the previous question is NO then answer why not? | Free form answer |
Some answers were recorded in order to be statistically analyzed.
Table 2.
Disease burden associated with cervical cancer (CC) in Bucharest Oncology Institute 2012-2022: General overview.
Table 2.
Disease burden associated with cervical cancer (CC) in Bucharest Oncology Institute 2012-2022: General overview.
| 2022 | 2021 | 2020 | 2019 | 2018 | 2017 | 2016 | 2015 | 2014 | 2013 | 2012 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Nr. of hospitalization episodes for CC | 3726 | 3028 | 2460 | 3775 | 4590 | 4679 | 4585 | 4315 | 5648 | 5734 | 4906 |
| Total nr. of hospitalization episodes | 12603 | 10962 | 11637 | 21008 | 21326 | 21153 | 22059 | 22393 | 22665 | 22029 | 21701 |
| Percentage | 29.56 | 27.62 | 21.14 | 17.97 | 21.52 | 22.12 | 20.79 | 19.27 | 24.92 | 26.03 | 22.61 |
| Nr. of unique patients treated for CC | 967 | 827 | 805 | 1290 | 1456 | 1543 | 1620 | 1585 | 1918 | 1994 | 1817 |
| Surgical procedures for CC | 668 | 651 | 642 | 1204 | 1251 | 1180 | 1274 | 1155 | 1911 | 1925 | 1868 |
| Total nr of surgical procedures | 4425 | 3947 | 3512 | 6338 | 6330 | 6392 | 6531 | 6611 | 6547 | 6612 | 6484 |
| Percentage | 15.09 | 16.49 | 18.28 | 18.99 | 19.28 | 18.46 | 19.5 | 17.47 | 29.18 | 29.11 | 28.8 |
| Percentage of ≥stage Ib CC | 92.15 | 94.61 | 87.32 | 89.14 | 91.57 | 90.86 | 91.79 | 89.99 | 93.63 | 92.47 | 91.52 |
| Medium hospital stay (days) | 7.62 | 10.12 | 10.25 | - | - | - | - | - | - | - | - |
| Medium cost of hospitalization episode for CC (Romanian Lei) | 12149 | 9833 | 5146 | - | - | - | - | - | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



