
Submitted:
27 July 2023
Posted:
28 July 2023
You are already at the latest version
Abstract
This study aimed to compare the efficacies and safety of enhanced and standard monofocal intraocular lenses (IOLs) in eyes with early glaucoma. Patients with concurrent cataracts and open-angle glaucoma (OAG) were enrolled. They underwent cataract surgery with IOL implantation. Manifest refraction; monocular uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), uncorrected intermediate visual acuity (UIVA), and uncorrected near visual acuity (UNVA); visual field (VF); contrast sensitivity (CS); defocus curves and questionnaires were assessed three months postoperatively. Thirty-four and 38 patients had enhanced and standard monofocal IOLs, respectively. The enhanced monofocal IOL provided better UIVA than the standard monofocal IOL (p = 0.003) but similar UDVA, CDVA and UNVA. The enhanced monofocal IOL had more consistent defocus curves than the standard monofocal IOL, especially at -1 (p = 0.042) and -1.5 (p = 0.026) diopters. The enhanced monofocal IOL provided better satisfaction (p = 0.019) and lower spectacle dependence (p = 0.004) than the standard monofocal IOL for intermediate vision, with similar VF and CS. In conclusion, the enhanced monofocal IOL is recommended for patients with OAG because they provide better intermediate vision, higher satisfaction, and lower dependence on spectacles than standard monofocal IOL, without worsening other visual outcomes.
Keywords:
enhanced monofocal intraocular lens
; open-angle glaucoma
; cataract surgery
; visual outcomes
1. Introduction
Glaucoma and cataract are intrinsically age-related, and their comorbidity rate is high [1]. In a previous study, the most common ocular comorbidity in cataract patients was glaucoma [2]. As patients with glaucoma get older, the development of cataracts is inevitable and has also been associated with glaucoma medication [3,4]. Cataract surgery can significantly improve vision and quality of life for glaucoma patients, just as it does for nonglaucoma patients [5,6]. When choosing an intraocular lens (IOL) for glaucoma patients, it is essential to consider its potential impact on visual acuity (VA), contrast sensitivity (CS), and visual field (VF) [7]. Previously, patients with glaucoma were not considered suitable candidates for multifocal IOL because there was a fear that this would further reduce CS and lead to other visual symptoms, such as photic phenomena [8,9,10]. Previous studies have shown that patients with glaucoma may experience decreased CS after bifocal IOL implantation [7,9,11]. However, in a previous study, a non-diffractive, wavefront-shaping extended depth of focus (EDOF) IOL provides good visual acuity and high patient satisfaction in eyes with mild, pre-perimetric open-angle glaucoma (OAG) [12]. In addition, EDOF IOL has been reported to provide similar CS and VF outcomes to those of standard monofocal IOL in cataract patients without ocular comorbidities [13,14,15].
The enhanced monofocal IOL is a new refractive IOL with enhanced intermediate function. It uses the geometric, material, and corneal spherical aberration correction features of the standard monofocal IOL, as well as a higher-order aspheric profile on the anterior optic surface. The design of the enhanced monofocal IOL allows it to provide improved intermediate vision while maintaining the benefits of a standard monofocal IOL, such as clear distance vision. Previous studies have shown no significant difference between the enhanced and standard monofocal IOLs in terms of CS, photic phenomena and the incidence of side effects in eyes without ocular comorbidities [16,17]. Innovation in IOL technology have helped to overcome the limitations of earlier presbyopia-correcting IOLs [10,18,19]. Based on previous reports, we hypothesized that enhanced monofocal IOL are viable for patients with concomitant cataracts and glaucoma. To the best of our knowledge, this study is the first in the literature to report the clinical results of enhanced monofocal IOL in patients with glaucoma. This study aimed to compare the efficacies and safety of enhanced and standard monofocal IOLs in eyes with early OAG.
2. Materials and Methods
2.1. Study design
This prospective, nonrandomized, observational, comparative study included patients with concurrent visually significant cataracts and OAG. As part of preoperative counseling, all patients were educated on the inherent risks of surgery, the characteristics of IOLs, and some characteristics of their eyes. The patients selected IOLs after considering their lifestyles, personalities, professions, hobbies, and the characteristics of their eyes. All patients were informed of the study and provided informed consent for participation. This study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of Chonnam National University Hospital (CNUH-2023-174). All study participants signed an informed consent form before enrollment.
2.2. Participants
This study included patients who were 50 years of age or older, had visually significant cataracts, and had medically controlled early OAG without central VF defects. The following inclusion criteria were used; (1) early OAG as defined by the presence of glaucomatous optic disc changes (vertical cup-to-disc ratio above 0.7 or an inter-eye asymmetry of more than 0.2 or neuroretinal rim notching) with corresponding VF defects, open angle observed via gonioscopic examination, and reliable 30-2 VF test results(false-positive errors < 15%, false-negative errors < 15%, and fixation loss < 20%) with a mean deviation (MD) score of -6 dB or better; (2) medically controlled glaucoma defined as no changes in the glaucoma medication regimen within the last 1 year with intraocular pressure (IOP) at the target level (defined as IOP < 21 mmHg and at the individual IOP level at which ophthalmologist believe that further optic nerve progression is unlikely to occur) and reliable 30-2 VF test results for three consecutive tests [20]; and (3) eyes without a central VF defect, which is defined as the 4 most central points among the 76 testing points of the 30-2 VF test [21]. The exclusion criteria included amblyopia; axial length above 26.0 mm; corneal astigmatism above 0.75 D; previous ocular surgery; previous ocular inflammation; acute ocular infection; diabetes mellitus with retinal changes; pseudoexfoliation syndrome; pathological miosis; possibility of floppy-iris syndrome; presence of corneal dystrophy; and any other ocular pathology that may limit visual function. Only one eye per patient was included in this study. If both eyes were included, the eye that underwent initial cataract surgery was included.
2.3. Preoperative examination
Within 30 days of the surgery, all patients underwent a comprehensive preoperative ophthalmic examination including manifest refraction; monocular uncorrected distance visual acuity (UDVA at 4m), corrected distance visual acuity (CDVA at 4m), uncorrected intermediated visual acuity (UIVA at 66 cm), and uncorrected near visual acuity (UNVA at 33 cm) under photopic conditions (85 cd/㎡) with the Early Treatment Diabetic Retinopathy Study charts; IOP measurement (Haag-Streit USA, Mason, Ohio, USA); topography (Pentacam; Oculus Optikgeräte GmbH Inc., Wetzlar, Germany); optical biometry (IOL master 700; Carl Zeiss Meditec, Dublin, California, USA); global peripapillary retinal nerve fiber layer (pRNFL) thickness measurement by swept-source optical coherence tomography (OCT) (DRI OCT Triton; Topcon Corporation, Tokyo, Japan); VF test (Humphrey Field Analyzer; Carl Zeiss Meditec, Dublin, California, USA); slit lamp examination; gonioscopy; fundocopy; and mesopic (3 cd/㎡) pupillometry.
2.4. Surgical technique
All the surgeries were performed by a single expert surgeon (PSW). Under topical anesthesia, a 2.8-mm corneal incision was made and a 5.0-mm sized capsulorrhexis was performed manually. Phacoemulsification was performed using the stop-and-chop technique with a phacoemulsification device (Centurion; Alcon Laboratories Inc., Fort Worth, TX, USA). All IOLs were implanted into bags. The incisions were sealed with hydrosutures. The postoperative target refraction was determined as the lowest myopic value after emmetropia using the Barrett Universal II formula. Each patient received topical antibiotic and anti-inflammatory prophylaxis and postoperative treatment with topical nonsteroidal anti-inflammatory, steroid, and antibiotic eye drops.
2.5. Intraocular lenses
The standard monofocal IOL (Tecnis model ZCB00; Johnson and Johnson Vision Care Inc., Santa Ana, CA) is a single-piece, hydrophobic acrylic monofocal IOL with an aspheric anterior surface. The aspheric surface has a spherical aberration of -0.27 μm, which helps to reduce spherical aberration to zero. The enhanced monofocal IOL (Tecnis Eyhance model ICB00; Johnson and Johnson Vision Care Inc.) was made of the same hydrophobic acrylic material and had the same overall geometry and dimensions as the standard monofocal IOL. Additionally, the enhanced monofocal IOL has a unique refractive optical design with a higher-order aspheric anterior surface, which produces a continuous increase in power. This design is intended to improve intermediate vision while maintaining distance vision comparable to that of a standard monofocal IOL. This is why it is called an enhanced monofocal. It is based on refractive technology without diffractive rings and zones and is visually indistinguishable from standard monofocal IOL.
2.6. Postoperative examination
The UDVA, CDVA, UIVA, and UNVA under photopic conditions and postoperative manifest refraction were measured 3 months postoperatively. The corrected defocus curves were measured monocularly using defocusing lenses with a power range of 1.00 D to -4.00 D at 0.5 D intervals and a distance of 4 m. The lenses were inserted into a test frame to account for the manifest error in the refraction at distance [22]. The corrected CS was measured using the functional acuity contrast test of the Optec 6500 view-in test system (Stereo Optical Co., Inc., Chicago, Illinois, USA) with stimulus spatial frequencies between 1.5 and 18 cycles/degree under photopic (85 cd/㎡) and mesopic (3 cd/㎡) conditions with and without glare. Twelve white light-emitting diodes were used as the source of glare: 10 lx under photopic conditions and 1 lx under mesopic conditions. The VF test was performed using a Humphrey field analyzer with the Swedish Interactive Threshold Algorithm. The test was conducted under a 30-2 grid, with a white stimulus color, stimulus size III, and a background luminance of 31.5 apostilbs. Refractive corrections were performed for all eyes at a testing distance of 33 cm. Testing was repeated if the test results were unreliable. VF parameters, such as MD, pattern standard deviation (PSD), and visual field index (VFI), were assessed. The dB values of the four central test points of the VF 30-2 test program were anti-logged to obtain sensitivity on a linear scale. Subsequently, the mean of the four central test points was logged again to transform them back to a dB scale [23]. This value is defined as the central VF total deviation. Finally, patients completed questionnaires to assess the experience of photic phenomena (glare, starbursts, and halos); their satisfaction with their overall, near, intermediate, and distance vision; and their dependence on spectacles for near, intermediate, and distance vision. The questionnaires included illustrations to help patients identify photic phenomena. Patient satisfaction was rated on a scale of 1 to 5: 1, very dissatisfied; 2, dissatisfied; 3, neutral; 4, satisfied; and 5, very satisfied. Spectacle dependence was rated on a scale of 1 to 5: 1, never; 2, seldom; 3, about half the time; 4, usually; and 5, always [24,25].
2.7. Statistical analysis
All statistical analyses were performed using SPSS version 26.0 (SPSS Inc., Chicago, IL, USA). Data are presented as means ± standard deviation. All VA measurements were converted to the logarithm of the minimum angle of resolution (logMAR) for data analysis. Student’s t-test, Pearson’s chi-square test, and Fisher’s exact test were used to verify the differences between the two groups. A paired t-test was used to compare the VF parameters before and after surgery in both groups. Statistical significance was set at p < 0.05.
3. Results
In this study, 72 eyes of 72 patients were evaluated. Thirty-four patients chose enhanced monofocal IOLs, and 38 patients chose standard monofocal IOLs. The demographic and preoperative clinical characteristics of all patients are shown in Table 1. There were no significant differences between the two groups based on age, sex, laterality, preoperative spherical equivalent (SE), axial length, mesopic pupil size, UDVA, CDVA, UIVA, UNVA, IOP, global pRNFL thickness, number of glaucoma medications and VF parameters. All surgeries proceeded smoothly, and all IOLs were successfully implanted in the capsular bag. There were no postoperative adverse events such as cystoid macular edema, uncontrolled IOP, or endophthalmitis. All of the patients were able to complete the follow-up period. No patient showed clinically significant posterior capsular opacification at the 3-month follow-up.
Table 2 presents 3 months of postoperative visual outcomes for both groups. There were no significant differences in UDVA, CDVA, and UNVA between the two groups. However, there were statistically significant differences in UIVA; compared with the standard monofocal IOL group, the enhanced monofocal IOL group showed a significantly better UIVA (p = 0.003). The UIVA was 0.34 ± 0.10 logMAR for the enhanced monofocal IOL group and 0.41 ± 0.10 logMAR for the standard monofocal IOL group.
Figure 1 shows the changes in VF parameters after surgery in both groups. The MD (p < 0.001 in both groups) and central VF total deviation (p = 0.017 for the enhanced monofocal IOL group and p = 0.010 for the standard monofocal IOL group) significantly improved at three months postoperatively, compared with the baseline values for each group. The PSD and VFI showed no significant changes after surgery in either group. There were no statistically significant differences in any VF parameters between the enhanced and standard monofocal IOL groups at baseline and 3 months postoperatively (p > 0.05).
Figure 2 shows the corrected monocular defocus curves for the two groups at 3 months postoperatively. Both curves peaked at a defocus of 0.00 D. VA decreased with increasing negative defocus. The enhanced monofocal IOL group had a smoother and wider defocus curve, especially within the intermediate defocus range (up to -1.50 D, corresponding to 66 cm). The enhanced monofocal IOL group showed significantly better defocus at -1.0 D (0.16 ± 0.08 logMAR for the enhanced monofocal IOL group vs. 0.21 ± 0.10 logMAR for the standard monofocal IOL group, p = 0.042) and -1.5 D (0.21 ± 0.10 logMAR in the enhanced monofocal IOL group vs. 0.25 ± 0.08 logMAR in the standard monofocal IOL group, p = 0.026) than the standard monofocal IOL group. This means that the enhanced monofocal IOL group had better intermediate vision than the standard monofocal IOL group.
The monocular and corrected distance CS test results at 3 months under mesopic and photopic conditions with and without glare for eyes in the subgroup of patients are presented in Figure 3. The CS results showed no significant differences under any light condition between the enhanced and standard monofocal IOL groups for any spatial frequency (p > 0.05).
Questionnaires on the perception of photic phenomena, visual satisfaction, and spectacle dependence were administered. No statistically significant differences were observed between the enhanced and standard monofocal IOL groups in terms of glare, starburst, and halo perception (Table 3). In both groups, > 90% of patients did not experience glare, halo, or starburst phenomena. Overall visual satisfaction was observed in both groups. There was no statistically significant difference between the enhanced and standard monofocal IOL groups based on satisfaction and spectacle dependence for near and distance vision. However, for intermediate vision, the enhanced monofocal IOL group showed higher satisfaction (p = 0.019) and lower spectacle dependence (p = 0.004) than the standard monofocal IOL group (Figure 4).
4. Discussion
Cataract surgery is one of the most common surgical procedures globally. In recent years, it has evolved from simply removing clouded lenses to refractive surgery. Presbyopia-correcting IOLs such as accommodative, bifocal, trifocal, and EDOF IOLs have been introduced. These IOLs provide greater spectacle independence and improved visual performance compared to standard monofocal IOLs [26]. However, some patients with multifocal IOLs may experience photic phenomena, such as glare and halo, or perceive reduced CS [27,28]. Patients with glaucoma have the same high desires as their friends and family members who do not have glaucoma for a wide range of vision and reduced dependence on spectacles after cataract surgery. However, previous presbyopia-correcting IOL options, such as trifocal and bifocal IOLs, were considered unsuitable for patients with glaucoma because these IOLs can reduce CS and cause photic phenomena. Recently, enhanced monofocal IOL has been introduced to provide excellent VA for distance while improving intermediate vision without the side effects that are typically associated with multifocal IOLs [29]. The study was designed to compare the efficacies and safety of enhanced and standard monofocal IOLs to provide improved vision for glaucoma patients.
The enhanced monofocal IOL has a unique refractive optical design with a higher-order aspheric anterior surface, which produces a continuous increase in power. The unique optical design of the enhanced monofocal IOL resulted in a more consistent defocus curve and a larger range of acceptable defocus values than those of the standard monofocal IOL. This is consistent with previous studies involving patients without ocular comorbidities [16,30]. As a result, the enhanced monofocal IOL can improve vision at intermediate distances, which is helpful for several modern daily life activities, such as using a computer screen, tablet display, car dashboard, or playing sports [31]. This study shows that enhanced monofocal IOL improve intermediate vision with increased depth of focus in glaucoma patients, as observed in patients without ocular comorbidities [16,32,33].
CS is closely associated with the ability to perform daily activities and provide valuable insights into quality-of-life assessments. Glaucoma first affects CS more than visual acuity [34]. CS, especially at mesopic levels, decreases early during the disease and is correlated with the severity of VF loss in patients with glaucoma [35]. Therefore, additional CS loss is a main concern for patient with glaucoma. It is well known that CS decreases at higher spatial frequencies in eyes with multifocal IOLs [9,10]. Multifocal IOLs can reduce CS more than monofocal IOLs because one image is always blurred, and defocused light energy can create disturbances [36,37]. Therefore, multifocal IOLs are not recommended for glaucoma patients because they can further reduce CS. To overcome these limitations, advancements have been made in IOL technology. A previous study found that eyes with EDOF IOL have similar CS to eyes with monofocal IOL [10,13]. In this study, the monocular corrected distance CS under mesopic and photopic conditions with or without glare were similar for the eyes with enhanced and standard monofocal IOLs, as reported by previous studies on patients without ocular comorbidities [16,30,32]. The enhanced monofocal IOL uses the same optical platform as the standard monofocal IOL, except for its unique anterior surface and a thickness difference of 1.5 microns with a diameter of nearly 2 mm in the optical center [38,39]. This subtle difference in optical design is not expected to have a significant impact on CS in patients with glaucoma. The results of this study show that an enhanced monofocal IOL may be an appropriate choice for glaucoma patients who are concerned about reduced CS.
Patients with glaucoma who already have decreased VF sensitivity are at risk of further reductions due to cataract development. The deterioration of VF sensitivity by cataract can be significantly improved by cataract removal and IOL implantation [40]. Several studies have reported improved MD and unchanged VFI after cataract surgery in glaucoma patients; however, the postoperative changes in PSD, which vary from patient to patient, are still controversial [41,42]. In this study, MD and central VF total deviation significantly improved after surgery using any of both IOLs. However, PSD and VFI remained unchanged for both IOLs. As the type of IOL can affect the results of the VF test, it is important to carefully select the IOL for patients with glaucoma. Previous studies found that patients with multifocal IOL had significantly lower MD values than those with monofocal IOL [43,44]. However, a different study found that EDOF IOL were comparable to monofocal IOL based on both MD and foveal threshold values [15]. In this study, there were no significant differences in MD, PSD, and VFI between the two groups at 3 months postoperatively. Additionally, there was no significant difference in the central VF total deviation value, which was strongly associated with the best-corrected VA and quality of life of the patients with enhanced and standard monofocal IOLs [45]. This suggests that enhanced monofocal IOL may be appropriate for patients with glaucoma who are concerned about the deterioration of VF.
The enhanced monofocal IOL has an additional design in its central optics for intermediate vision. This design may increase the risk of positive dysphotopsia or photic phenomena, such as glare, halos, and starbursts. However, there was no significant difference in patient-reported visual symptoms between the two IOL groups. This subtle difference in optical design is not expected to have a significant impact on the photic phenomena. The majority of patients did not experience any significant problems or were not significantly bothered by photic phenomena. The enhanced monofocal IOL resulted in significantly better satisfaction with intermediate vision and lower spectacle dependence than the standard monofocal IOL. These results suggest that enhanced monofocal IOL can provide satisfactory vision at both far and intermediate distances, with minimal photic phenomena.
To date, patients and surgeons have been reluctant to use multifocal IOLs not only because of concerns about the disadvantages of multifocal IOLs but also because of the potential risk of glaucoma progression. Therefore, it is important to choose an IOL that is less affected by glaucoma progression. Especially in younger patients with a longer duration of disease progression, increased emphasis on presbyopia correction is associated with a greater risk of visual impairment in future if glaucoma progresses. It would be ideal if an IOL could perfectly correct presbyopia and its efficacy was not affected by glaucoma severity. However, such IOL have not yet been developed. It is necessary to make a balanced choice between the correction of presbyopia and the risk of glaucoma progression. In this regard, enhanced monofocal IOL may be an appropriate balanced option for glaucoma patients who will undergo cataract surgery. The enhanced monofocal IOL share more similar optical features to standard monofocal IOLs than other presbyopic-correcting IOLs. Although the presbyopia correction is less than other presbyopic-correcting IOLs, it provides improved intermediate vision that is satisfactory to patients, and it minimizes the disadvantages of presbyopia-correcting IOLs. Our study did not find any other negative effects of the enhanced monofocal IOL in glaucoma patients, but there is a potential risk. The risks and benefits of using enhanced monofocal IOL in glaucoma patients should be carefully considered.
The present study had several limitations. The main limitation was the lack of randomization as the patients were divided according to their personal preferences. Patients already knew the properties of the IOL, which was intended to enhance intermediate vision. This may have affected the patients’ responses to the questionnaire. Second, even though central VF was evaluated using the central portion of the 30-2 visual field test, a more precise evaluation, such as the 10-2 VF test, is needed for a more appropriate central VF function. Third, although an uncorrected defocus curve may be representative of real-life visual function as perceived by patients, a corrected defocus curve was obtained to better represent the inherent characteristics of IOLs. Additional studies that use uncorrected defocus curves may yield more practical outcomes. Fourth, medically controlled OAG may slowly progress to disease; however, the 3 months was too short for follow-up. Analysis after long-term follow-up may yield different results. Fifth, only the unilateral eyes of the patients were evaluated. Finally, this study involved patients with early OAG, preserved central VF, and a low risk of glaucoma progression. Therefore, it may be difficult to apply our results to all glaucoma patients. Based on the current results, future studies on the long-term visual outcomes of enhanced monofocal IOL in patients with varied glaucoma severities may be needed.
In conclusion, we suggest enhanced monofocal IOL for patients with OAG because they provide better intermediate vision, higher satisfaction, and lower dependence on spectacles than standard monofocal IOL, without worsening other visual outcomes.
Author Contributions
Conceptualization, S.W.P.; methodology, J.W.N., J.H.L., M.S.S. and S.W.P.; validation, J.W.N., H.Z., M.S.S. and S.W.P.; formal analysis, J.W.N., J.H.L., H.Z. and M.S.S.; investigation, J.W.N., J.H.L., H.Z. and M.S.S.; resources, J.W.N. and M.S.S.; data curation, J.W.N. and M.S.S.; writing—original draft preparation, J.W.N., J.H.L and M.S.S.; writing—review and editing, J.W.N. and S.W.P.; visualization, J.W.N., M.S.S. and S.W.P.; supervision, M.S.S. and S.W.P.; funding acquisition, M.S.S. and S.W.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by a Patient-Centered Clinical Research Coordinating Center grant funded by the Ministry of Health & Welfare, Republic of Korea (HI19C0481, HC19C0276). Funding organizations had no role in the design or conduct of this study.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Chonnam National University Hospital (CNUH-2023-174).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Resnikoff, S.; Pascolini, D.; Etya'Ale, D.; Kocur, I.; Pararajasegaram, R.; Pokharel, G.P.; Mariotti, S.P. Global data on visual impairment in the year 2002. Bull. World Health Organ. 2004, 82, 844–851. [Google Scholar]
- Tseng, V.L.; Yu, F.; Lum, F.; Coleman, A.L. Risk of Fractures Following Cataract Surgery in Medicare Beneficiaries. JAMA 2012, 308, 493–501. [Google Scholar] [CrossRef]
- Leske, M.; Wu, S.-Y.; Nemesure, B.; Hennis, A.; Barbados Eye Studies Group. Risk factors for incident nuclear opacities. Ophthalmology 2002, 109, 1303–1308. [Google Scholar] [CrossRef] [PubMed]
- Herman, D.C.; Gordon, M.O.; Beiser, J.A.; Chylack, L.T.; Lamping, K.A.; Schein, O.D.; Soltau, J.B.; Kass, M.A.; Ocular Hypertension Treatment Study (OHTS) Group. Topical Ocular Hypotensive Medication and Lens Opacification: Evidence From the Ocular Hypertension Treatment Study. Am. J. Ophthalmol. 2006, 142, 800–810. [Google Scholar] [CrossRef] [PubMed]
- Cataract Surgery Outcomes in Glaucomatous Eyes: Results From the Veterans Affairs Ophthalmic Surgery Outcomes Data Project - ClinicalKey. https://www.clinicalkey.com/#!/content/playContent/1-s2.0-S0002939415004444?returnurl=https:%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS0002939415004444%3Fshowall%3Dtrue&referrer=https:%2F%2Fwww.ajo.com%2F (accessed 2023-07-02).
- Musch, D.C.; Gillespie, B.W.; Niziol, L.M.; Janz, N.K.; Wren, P.A.; Rockwood, E.J.; Lichter, P. R; Collaborative Initial Glaucoma Treatment Study Group. Cataract Extraction in the Collaborative Initial Glaucoma Treatment Study: Incidence, Risk Factors, and the Effect of Cataract Progression and Extraction on Clinical and Quality-of-Life Outcomes. Arch. Ophthalmol. 2006, 124, 1694–1700. [Google Scholar] [CrossRef]
- Bhartiya, S.; Sharma, A.; Ichhpujani, P. Premium IOLs in Glaucoma. J. Curr. Glaucoma Pr. 2013, 7, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Ichhpujani, P.; Thakur, S.; Spaeth, G.L. Contrast Sensitivity and Glaucoma. Eur. J. Gastroenterol. Hepatol. 2020, 29, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Braga-Mele, R.; Chang, D.; Dewey, S.; Foster, G.; Henderson, B.A.; Hill, W.; Hoffman, R.; Little, B.; Mamalis, N.; Oetting, T.; et al. Multifocal intraocular lenses: Relative indications and contraindications for implantation. J. Cataract. Refract. Surg. 2014, 40, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Schallhorn, J.M.; Pantanelli, S.M.; Lin, C.C.; Al-Mohtaseb, Z.N.; Steigleman, W.A.; Santhiago, M.R.; Olsen, T.W.; Kim, S.J.; Waite, A.M.; Rose-Nussbaumer, J.R. Multifocal and Accommodating Intraocular Lenses for the Treatment of Presbyopia: A Report by the American Academy of Ophthalmology. Ophthalmology 2021, 128, 1469–1482. [Google Scholar] [CrossRef] [PubMed]
- Teichman, J.C.; Ahmed, I.I.K. Intraocular lens choices for patients with glaucoma. Curr. Opin. Ophthalmol. 2010, 21, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, T.J.; Wilson, C.W.; Shafer, B.M.; Berdahl, J.P.; Terveen, D.C. Clinical Outcomes of a Non-Diffractive Extended Depth-of-Focus IOL in Eyes with Mild Glaucoma. Clin. Ophthalmol. 2023, ume 17, 861–868. [Google Scholar] [CrossRef]
- Pedrotti, E.; Bruni, E.; Bonacci, E.; Badalamenti, R.; Mastropasqua, R.; Marchini, G. Comparative Analysis of the Clinical Outcomes With a Monofocal and an Extended Range of Vision Intraocular Lens. J. Refract. Surg. 2016, 32, 436–442. [Google Scholar] [CrossRef]
- Lee, J.; Mori, Y.; Nejima, R.; Minami, K.; Miyata, K. Influence of implantations of extended depth-of-focus on standard automated perimetry. Sci. Rep. 2020, 10, 20153. [Google Scholar] [CrossRef]
- Takahashi, M.; Yamashiro, C.; Yoshimoto, T.; Kobayashi, Y.; Higashijima, F.; Kobayashi, M.; Hatano, M.; Ohta, M.; Nagai, T.; Teranishi, S.; et al. Influence of extended depth of focus intraocular lenses on visual field sensitivity. PLOS ONE 2020, 15, e0237728. [Google Scholar] [CrossRef] [PubMed]
- Auffarth, G.U.; Gerl, M.; Tsai, L.; Janakiraman, D.P.; Jackson, B.; Alarcon, A.; Dick, H.B. ; Quantum Study Group Clinical evaluation of a new monofocal IOL with enhanced intermediate function in patients with cataract. J. Cataract. Refract. Surg. 2020, 47, 184–191. [Google Scholar] [CrossRef]
- Wan, K.H.; Au, A.C.; Kua, W.N.; Ng, A.L.; Cheng, G.P.; Lam, N.M.; Chow, V.W. Enhanced Monofocal Versus Conventional Monofocal Intraocular Lens in Cataract Surgery: A Meta-analysis. J. Refract. Surg. 2022, 38, 538–546. [Google Scholar] [CrossRef]
- Rampat, R.; Gatinel, D. Multifocal and Extended Depth-of-Focus Intraocular Lenses in 2020. Ophthalmology 2021, 128, e164–e185. [Google Scholar] [CrossRef] [PubMed]
- Bala, C.; Poyales, F.; Guarro, M.; Mesa, R.R.; Mearza, A.M.; Varma, D.K.B.; Jasti, S.; Lemp-Hull, J.D. Multicountry clinical outcomes of a new nondiffractive presbyopia-correcting IOL. J. Cataract. Refract. Surg. 2022, 48, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Majstruk, L.; Leray, B.; Bouillot, A.; Michée, S.; Sultan, G.; Baudouin, C.; Labbé, A. Long term effect of phacoemulsification on intraocular pressure in patients with medically controlled primary open-angle glaucoma. BMC Ophthalmol. 2019, 19, 149. [Google Scholar] [CrossRef] [PubMed]
- Park, K.; Kim, J.; Lee, J. Measurement of macular structure-function relationships using spectral domain-optical coherence tomography (SD-OCT) and pattern electroretinograms (PERG). PLOS ONE 2017, 12, e0178004. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Eom, Y.; Park, S.Y.; Choi, S.Y.; Hwang, H.S.; Kim, J.-H.; Song, J.S.; Kim, H.M. Rainbow halos occur less following implantation of extended range of vision one-piece intraocular lenses vs diffractive bifocal intraocular lenses. Int. J. Ophthalmol. 2020, 13, 913–919. [Google Scholar] [CrossRef]
- Hood, D.C.; Kardon, R.H. A framework for comparing structural and functional measures of glaucomatous damage. Prog. Retin. Eye Res. 2007, 26, 688–710. [Google Scholar] [CrossRef]
- Huh, J.; Eom, Y.; Yang, S.K.; Choi, Y.; Kim, H.M.; Song, J.S. A comparison of clinical outcomes and optical performance between monofocal and new monofocal with enhanced intermediate function intraocular lenses: a case-control study. BMC Ophthalmol. 2021, 21, 365. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Jung, J.W.; Lee, J.M.; Seo, K.Y.; Kim, E.K.; Kim, T.-I. Clinical Outcomes Following Implantation of Diffractive Multifocal Intraocular Lenses With Varying Add Powers. Arch. Ophthalmol. 2015, 160, 702–709. [Google Scholar] [CrossRef] [PubMed]
- de Vries, N.E.; Nuijts, R.M. Multifocal intraocular lenses in cataract surgery: Literature review of benefits and side effects. J. Cataract. Refract. Surg. 2013, 39, 268–278. [Google Scholar] [CrossRef] [PubMed]
- Black, S. A clinical assessment of visual performance of combining the TECNIS® Symfony Extended Range of Vision IOL (ZXR00) with the +3.25 D TECNIS Multifocal 1-piece IOL (ZLB00) in subjects undergoing bilateral cataract extraction. Clin. Ophthalmol. 2018, ume 12, 2129–2136. [CrossRef]
- Rosen, E.; Alió, J.L.; Dick, B.H.; Dell, S.; Slade, S. Efficacy and safety of multifocal intraocular lenses following cataract and refractive lens exchange: Metaanalysis of peer-reviewed publications. J. Cataract. Refract. Surg. 2016, 42, 310–328. [Google Scholar] [CrossRef]
- Fernández, J.; Rocha-De-Lossada, C.; Zamorano-Martín, F.; Rodríguez-Calvo-De-Mora, M.; Rodríguez-Vallejo, M. Positioning of enhanced monofocal intraocular lenses between conventional monofocal and extended depth of focus lenses: a scoping review. BMC Ophthalmol. 2023, 23, 101. [Google Scholar] [CrossRef]
- Choi, W.K.; Han, H.J.; Son, H.-S.; Khoramnia, R.; Auffarth, G.U.; Choi, C.Y. Clinical outcomes of bilateral implantation of new generation monofocal IOL enhanced for intermediate distance and conventional monofocal IOL in a Korean population. BMC Ophthalmol. 2023, 23, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Elliott, D.B.; Hotchkiss, J.; Scally, A.J.; Foster, R.; Buckley, J.G. Intermediate addition multifocals provide safe stair ambulation with adequate ‘short-term’ reading. Ophthalmic Physiol. Opt. 2016, 36, 60–68. [Google Scholar] [CrossRef]
- Mencucci, R.; Cennamo, M.; Venturi, D.; Vignapiano, R.; Favuzza, E. Visual outcome, optical quality, and patient satisfaction with a new monofocal IOL, enhanced for intermediate vision: preliminary results. J. Cataract. Refract. Surg. 2020, 46, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Cinar, E.; Bolu, H.; Erbakan, G.; Yuce, B.; Aslan, F.; Fece, M.; Emre, S. Vision outcomes with a new monofocal IOL. Int. Ophthalmol. 2021, 41, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, A.S.; Szlyk, J.P.; Ardickas, Z.; Alexander, K.R.; Wilensky, J.T. Comparison of Contrast Sensitivity, Visual Acuity, and Humphrey Visual Field Testing in Patients with Glaucoma. Eur. J. Gastroenterol. Hepatol. 2003, 12, 134–138. [Google Scholar] [CrossRef]
- Korth, M.J.; Jünemann, A.M.G.; Horn, F.K.; Bergua, A.; Cursiefen, C.; Velten, I.; Budde, W.M.; Wisse, M.; Martus, P. Synopsis of various electrophysiological tests in early glaucoma diagnosis--temporal and spatiotemporal contrast sensitivity, light- and color-contrast pattern-reversal electroretinogram, blue-yellow VEP. Klin. Monatsbl. Augenheilkd. 2000, 216, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Cillino, S.; Casuccio, A.; Di Pace, F.; Morreale, R.; Pillitteri, F.; Cillino, G.; Lodato, G. One-Year Outcomes with New-Generation Multifocal Intraocular Lenses. Ophthalmology 2008, 115, 1508–1516. [Google Scholar] [CrossRef] [PubMed]
- Barisić, A.; Dekaris, I.; Gabrić, N.; Bohac, M.; Romac, I.; Mravicić, I.; Lazić, R. Comparison of Diffractive and Refractive Multifocal Intraocular Lenses in Presbyopia Treatment. Coll. Antropol. 2008, 32 Suppl 2, 27–31. [Google Scholar]
- Mesci, C.; Erbil, H.H.; Olgun, A.; Aydin, N.; Candemir, B.; A Akçakaya, A. Differences in contrast sensitivity between monofocal, multifocal and accommodating intraocular lenses: long-term results. Clin. Exp. Ophthalmol. 2010, 38, 768–777. [Google Scholar] [CrossRef] [PubMed]
- Alarcon, A.; Cánovas, C.; Koopman, B.; Weeber, H.; Auffarth, G.U.; Piers, P.A. Enhancing the Intermediate Vision of Monofocal Intraocular Lenses Using a Higher Order Aspheric Optic. J. Refract. Surg. 2020, 36, 520–527. [Google Scholar] [CrossRef]
- Hayashi, K.; Hayashi, H.; Nakao, F.; Hayashi, F. Influence of cataract surgery on automated perimetry in patients with glaucoma. Arch. Ophthalmol. 2001, 132, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Seol, B.R.; Jeoung, J.W.; Park, K.H. Changes of visual-field global indices after cataract surgery in primary open-angle glaucoma patients. Jpn. J. Ophthalmol. 2016, 60, 439–445. [Google Scholar] [CrossRef]
- Rao, H.L.; Jonnadula, G.B.; Addepalli, U.K.; Senthil, S.; Garudadri, C.S. Effect of Cataract Extraction on Visual Field Index in Glaucoma. Eur. J. Gastroenterol. Hepatol. 2013, 22, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Farid, M.; Chak, G.; Garg, S.; Steinert, R.F. Reduction in Mean Deviation Values in Automated Perimetry in Eyes with Multifocal Compared to Monofocal Intraocular Lens Implants. Arch. Ophthalmol. 2014, 158, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Aychoua, N.; Montolio, F.G.J.; Jansonius, N.M. Influence of Multifocal Intraocular Lenses on Standard Automated Perimetry Test Results. JAMA Ophthalmol 2013, 131, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Flaxel, C.J.; Samples, J.R.; Dustin, L. Relationship Between Foveal Threshold and Visual Acuity Using the Humphrey Visual Field Analyzer. Arch. Ophthalmol. 2007, 143, 875–877. [Google Scholar] [CrossRef]
Figure 1.
Visual field parameters of the two IOL groups at baseline and 3 months postoperatively. (a) mean deviation; (b) pattern standard deviation; (c) central visual field total deviation; (d) visual field index. (* = p < 0.05).
Figure 1.
Visual field parameters of the two IOL groups at baseline and 3 months postoperatively. (a) mean deviation; (b) pattern standard deviation; (c) central visual field total deviation; (d) visual field index. (* = p < 0.05).
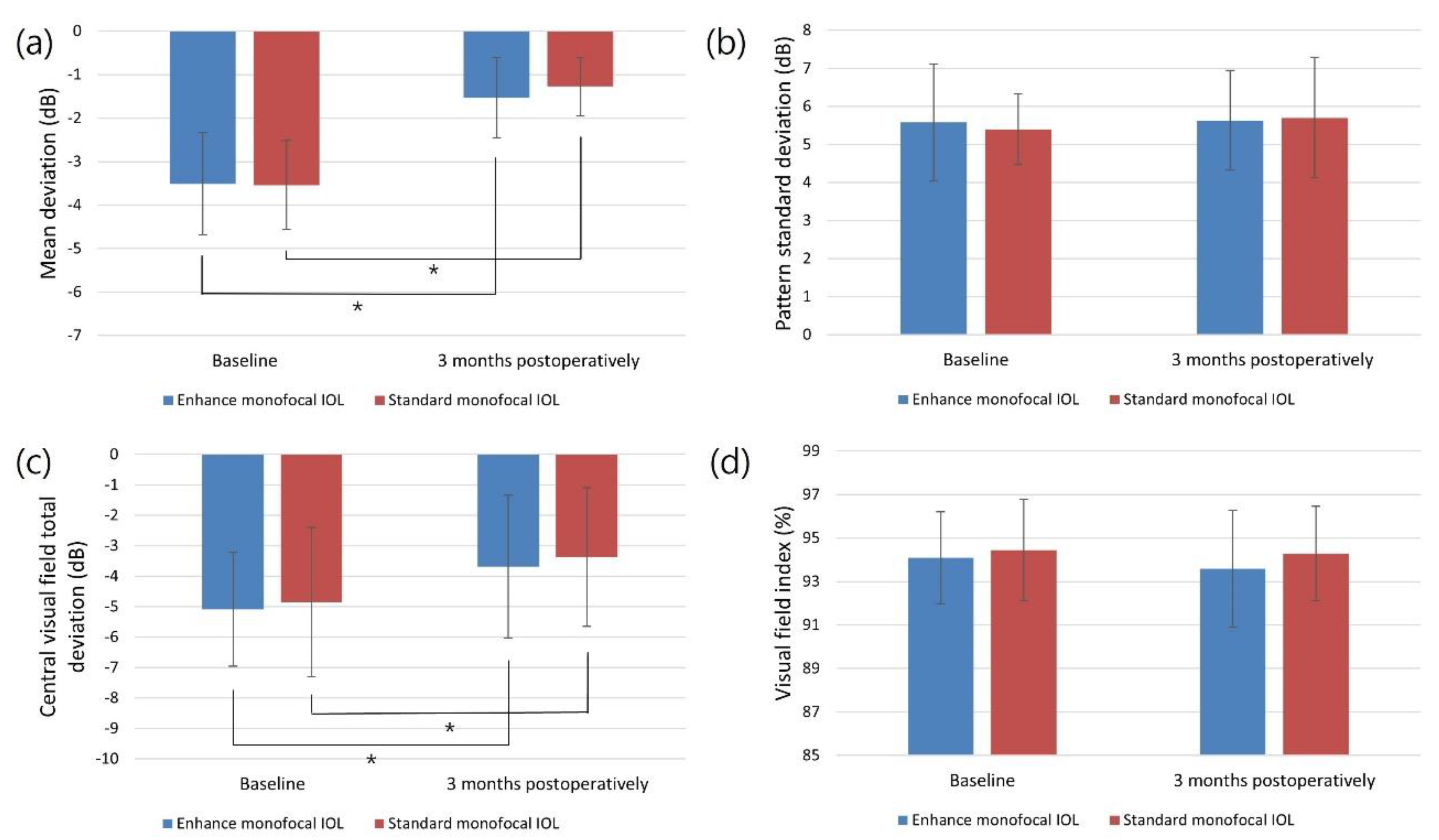
Figure 2.
Corrected monocular defocus curve of the two IOL groups at 3 months postoperatively. (* = p < 0.05).
Figure 2.
Corrected monocular defocus curve of the two IOL groups at 3 months postoperatively. (* = p < 0.05).
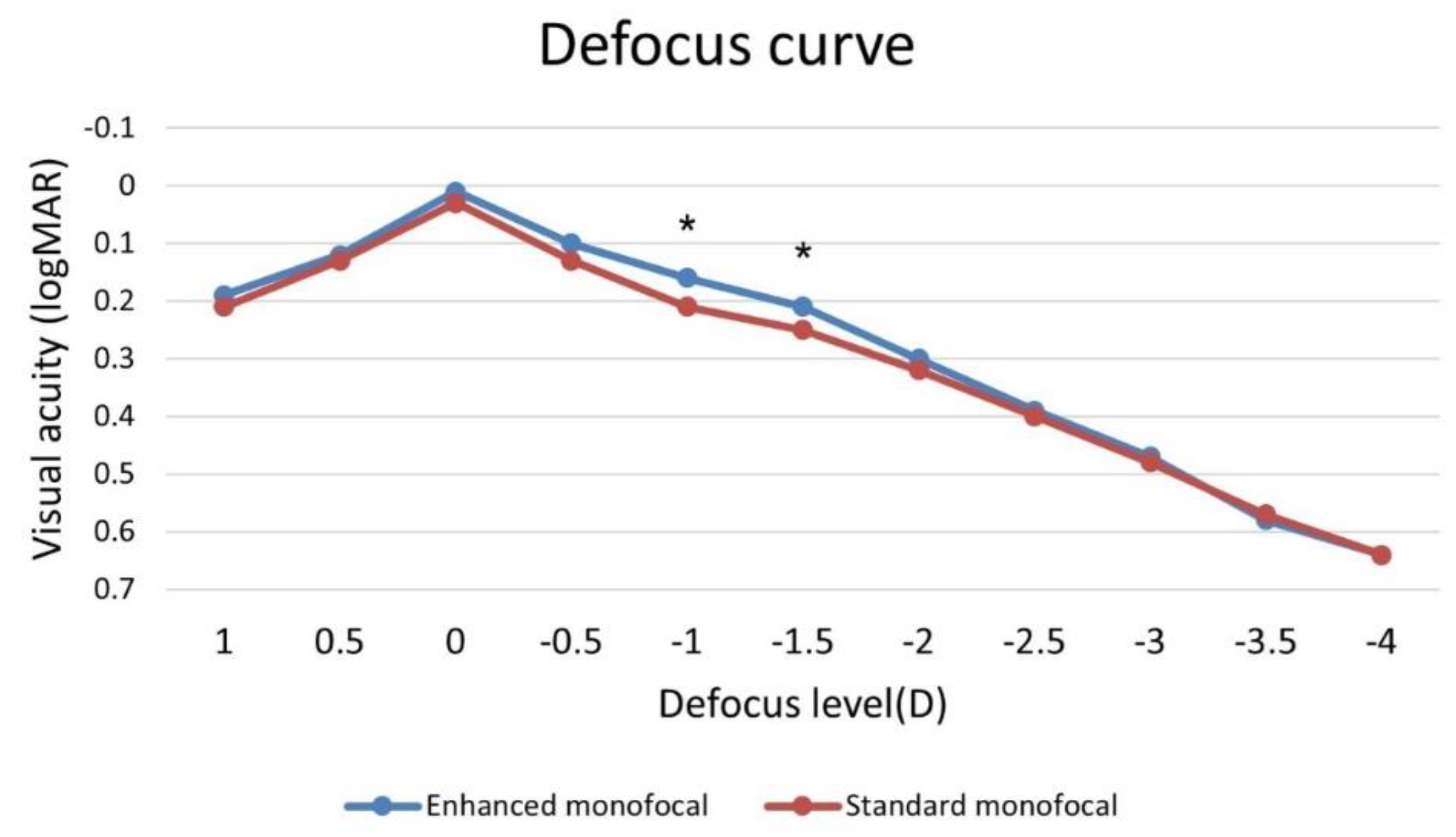
Figure 3.
Corrected monocular contrast sensitivity of the two IOL groups at 3 months postoperatively. (a) photopic condition without glare; (b) photopic condition with glare; (c) mesopic condition without glare; (d) mesopic condition with glare. (* = p < 0.05).
Figure 3.
Corrected monocular contrast sensitivity of the two IOL groups at 3 months postoperatively. (a) photopic condition without glare; (b) photopic condition with glare; (c) mesopic condition without glare; (d) mesopic condition with glare. (* = p < 0.05).
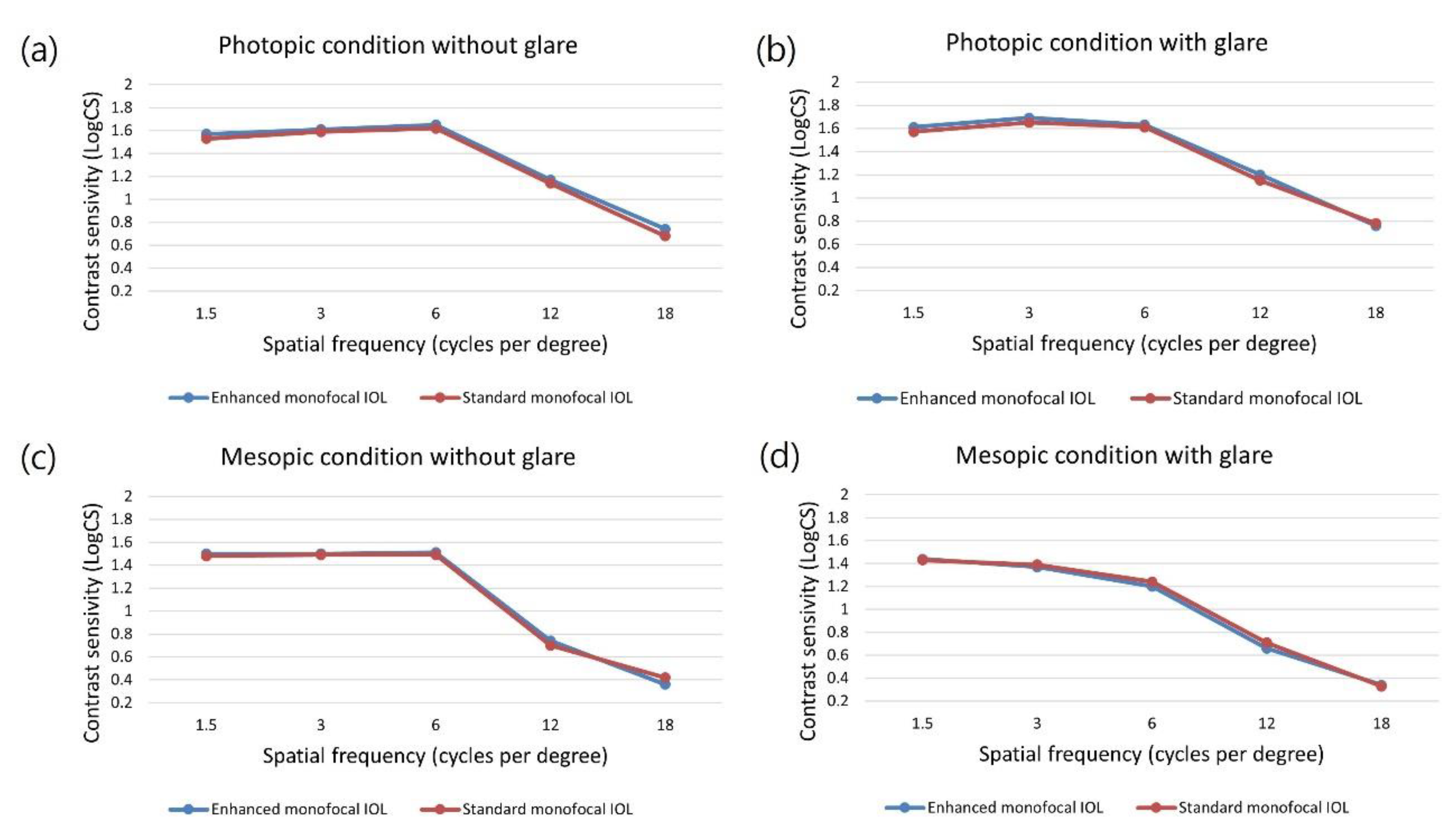
Figure 4.
Questionnaire results for vision satisfaction and spectacle dependence of the two IOL groups at 3 months postoperatively. (a) satisfaction score: 1, very dissatisfied; 2, dissatisfied; 3, neutral; 4, satisfied; and 5, very satisfied; (b) spectacle dependence score: 1, never; 2, seldom; 3, about half the time; 4, usually; and 5, always. (* = p < 0.05).
Figure 4.
Questionnaire results for vision satisfaction and spectacle dependence of the two IOL groups at 3 months postoperatively. (a) satisfaction score: 1, very dissatisfied; 2, dissatisfied; 3, neutral; 4, satisfied; and 5, very satisfied; (b) spectacle dependence score: 1, never; 2, seldom; 3, about half the time; 4, usually; and 5, always. (* = p < 0.05).
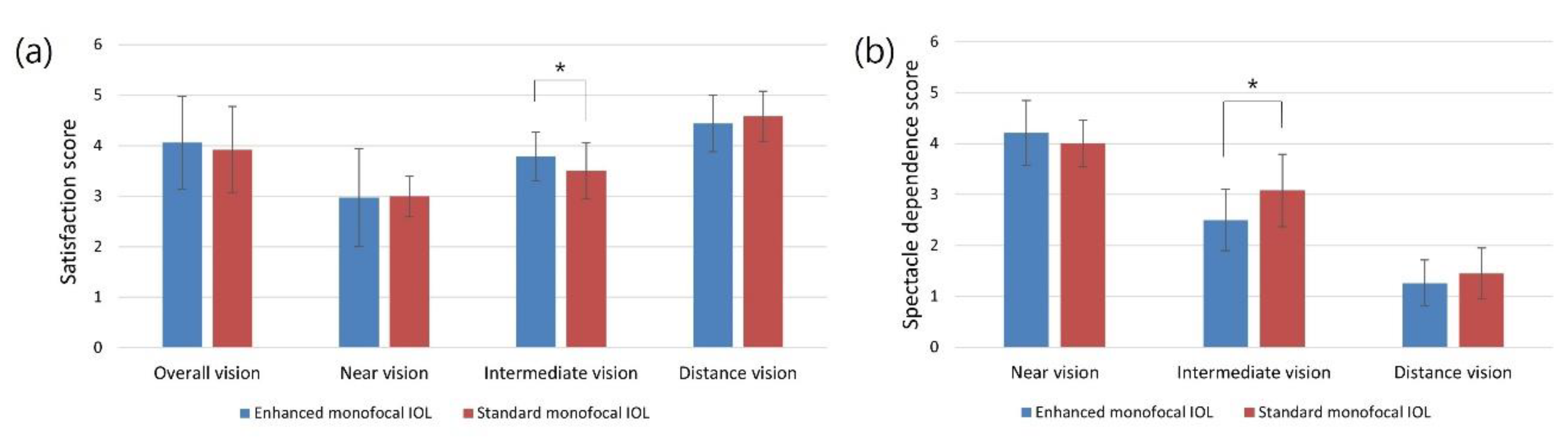

Table 1.
Demographic and preoperative characteristics of the two IOL groups.
| Variable | Enhanced monofoal IOL (n = 34) | Standard monofocal IOL (n = 38) | p-Value* |
|---|---|---|---|
| Age (years) | 68.76 ± 6.96 | 66.00 ± 7.59 | 0.113 |
| Sex (male/female) | 18/16 | 18/20 | 0.979 |
| Laterality (right/left) | 19/15 | 18/20 | 0.471 |
| SE (diopter) | 0.46 ± 1.67 | 0.75 ± 1.80 | 0.488 |
| Axial length (mm) | 24.74 ± 0.77 | 24.57 ± 0.84 | 0.370 |
| Mesopic pupil size (mm) | 3.76 ± 0.82 | 3.90 ± 0.83 | 0.478 |
| UDVA (logMAR) | 0.39 ± 0.17 | 0.36 ± 0.20 | 0.612 |
| CDVA (logMAR) | 0.22 ± 0.16 | 0.23 ± 0.14 | 0.698 |
| UIVA (logMAR) | 0.42 ± 0.14 | 0.43 ± 0.17 | 0.880 |
| UNVA (logMAR) | 0.56 ± 0.14 | 0.52 ± 0.14 | 0.183 |
| IOP (mmHg) | 12.76 ± 1.94 | 12.97 ± 1.81 | 0.638 |
| Global pRNFL thickness (μm) | 86.29 ± 10.67 | 84.53 ± 10.44 | 0.480 |
| Number of glaucoma medications | 1.47 ± 0.51 | 1.45 ± 0.50 | 0.846 |
| 30-2 VF parameters | |||
| MD (dB) | -3.51 ± 1.18 | -3.54 ± 1.02 | 0.903 |
| PSD (dB) | 5.58 ± 1.53 | 5.40 ± 0.93 | 0.562 |
| VFI (%) | 94.09 ± 2.11 | 94.45 ± 2.34 | 0.499 |
| Central VF total deviation (dB) | -5.09 ± 1.87 | -4.85 ± 2.45 | 0.645 |
SE = spherical equivalent; UDVA = uncorrected distance visual acuity; CDVA = corrected distance visual acuity; UIVA = uncorrected intermediate visual acuity; UNVA = uncorrected near visual acuity; logMAR = logarithm of the minimal angle of resolution; IOP = intraocular pressure; pRNFL = peripapillary retinal nerve fiber layer; VF = visual field; MD = mean deviation; PSD = pattern standard deviation; VFI = visual field index. Factors with statistical significance are shown in bold.
Table 2.
Visual acuity outcomes of the two IOL groups at 3 months postoperatively.
| Variable | Enhanced monofoal IOL (n = 34) | Standard monofocal IOL (n = 38) | p-Value* |
|---|---|---|---|
| UDVA (logMAR) | 0.05 ± 0.07 | 0.05 ± 0.06 | 0.983 |
| CDVA (logMAR) | 0.01 ± 0.04 | 0.02 ± 0.04 | 0.678 |
| UIVA (logMAR) | 0.34 ± 0.10 | 0.41 ± 0.10 | 0.003 |
| UNVA (logMAR) | 0.50 ± 0.10 | 0.53 ± 0.08 | 0.168 |
| SE (diopter) | -0.25 ± 0.22 | -0.21 ± 0.36 | 0.605 |
UDVA = uncorrected distance visual acuity, CDVA = corrected distance visual acuity, UIVA = uncorrected intermediate visual acuity, UNVA = uncorrected near visual acuity, logMAR logarithm of the minimal angle of resolution, SE = spherical equivalent. Factors with statistical significance are shown in bold.
Table 3.
Questionnaire results for photic phenomena of the two IOL groups at 3 months postoperatively.
Table 3.
Questionnaire results for photic phenomena of the two IOL groups at 3 months postoperatively.
| Variable | Enhanced monofoal IOL (n = 34) | Standard monofocal IOL (n = 38) | p-Value* |
|---|---|---|---|
| Glare (yes/no) | 2/32 | 3/35 | >0.999 |
| Starbursts (yes/no) | 1/33 | 2/36 | >0.999 |
| Halos (yes/no) | 2/32 | 1/37 | 0.599 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



