
Submitted:
26 July 2023
Posted:
28 July 2023
You are already at the latest version
Abstract
Background: Alzheimer's disease causes great changes, with the prefrontal cortex be-ing frequently damaged zones, affecting physical and cognitive behavioural and compromising autonomy and quality of life. Objective: To evaluate the effectiveness of feedback-based tech-nology on the improvement of physical-cognitive capacities in Alzheimer. Methods: Forty pa-tients with Alzheimer were recruited from the Santa Elena Alzheimer's Association, Seville, of which 15 ended up being pilot participants, divided randomly into controls (8) and experi-mental (7). They were evaluated with: Cognitive Mini-Examination Scale, Oddball Test and At-tention Network, Berg Scale, Tinetti, Timed up and Go and Geriatric Deterioration Scale. The experimental group was treated with feedback-based technology under the supervision of physiotherapists, during 16 thirty-minute sessions, twice a week. The control group performed their usual care. Result: A significant improvement was observed in the experimental group (Cognitive Mini-Examination and Tinetti). In the group of control, a worsening of physical and motor skills was evidenced because of the degenerative disease. Discussion/Conclusion: This treatment could be a strategy to keep the patient in early stages for longer, and improve quali-ty of life delaying dependency. It creates intergenerational bonds and use at home to promote treatment adherence.
Keywords:
Alzheimer´s disease
; balance
; gait
; cognitive decline
; exercise
; feedback-based technology
; prevention
1. Introduction
The aging rate of Western countries, including the Spanish population, continues to grow exponentially [1,2]. The aging process causes a decline at the level of different organs and systems, highlighting the prefrontal cortex, as one of the areas that is most affected by the passage of time, this structure being crucial for the effectiveness of executive skills, states attentional abilities and the capacity to be resilient[3]. Executive functions and gait are closely connected [4], so that impairment of one of them has cognitive and physical repercussions. Therefore, the ability of older people to be independent, as well as the risk of falls. The feeling of loneliness, which has also been shown due to aging [5,6], can increase the degree of dependency of these people.
On the other hand, within the elderly population, those diagnosed with Alzheimer's disease have added its manifestations. The existence of a correlation between attentional capacity and Alzheimer's disease is added [7], as well as the role of executive and frontoparietal networks [8], coinciding with previous research that has correlated physical frailty with cognitive impairment and risk of falls [9,10]. Although it has been less studied, attention as a cognitive function is affected in the disease, often being responsible for the first memory problems in patients. The main concern of the most researches testing attentional skills in Alzheimer's was the orientation of spatial attention, employing adaptations of the pre-key paradigms designed by the Posner team´s [11].
Although patients have been observed to show impairments in spatial attention orientation, the reason why is an open question. Recently there is the review developed by McDonough et al [12], which analyzes previous studies where the Attention Network Test (ANT) tool evaluated attentional networks both in healthy older people and in Alzheimer's disease. The deficiency in the executive network does not seem to be compensated in Alzheimer's disease, but it is in healthy aging.
Also, there are studies that affirm that gait disturbances may be associated with a decline in cognitive function, even that it could be guiding us to the first signs of dementia[13]. These antecedents, added to those exposed in relation to attentional networks, to the findings found in the subject of telerehabilitation [14,15,16], to the benefits found in the application of feedback-based technology on cognition, balance and avoidance of falls in elderly [17-20], determined the design of this study, whose main objective is to evaluate the effectiveness of feedback-based technology on the improvement of physical-cognitive capacities in Alzheimer.
2. Materials and Methods
A randomized pilot clinical trial, based on a previous study[20] is planned to assess the efficacy of using a technological tool with feedback (Nintendo® Wii, Video Console) on the physical-cognitive capacities of older subjects with Alzheimer's disorder. This research was based on Declaration of Helsinki[21], approved by an experimental ethics committee (University of Seville). The legal guardians proceeded to sign the informed consent. The subjects were randomized through sealed envelopes, forming them into parallel groups: control and experimental. The protocol followed the recommendations provided in the SPIRIT[22] statement.
Likewise, the Oxford[23] and Consort[24] standards have been considered for its development. The patients and the professionals who performed the assessments were blinded. Physiotherapists who delivered therapy using feedback-based technology were not blinded.
Participants: The patients were referred from the Santa Elena Alzheimer Association, Seville (Spain). The inclusion criteria were: Alzheimer diagnosed with the Diagnostic and Statistical Manual of Mental Disorder (DSM-IV criteria), reaching a value on the "Geriatric Deterioration Scale" less than or equal to 5 and walking without technical assistance. Patients excluded from the study were those with hallucinations or delusional ideation, uncompensated hearing or visual disturbances, musculoskeletal limitations, and sleep habits of less than 6 hours a day.
Outcomes measure: The study contains the following five dependent variables:
- Attention: obtained with two tests (Oddball Test and Attention Network Test- ELDERLY) [25]. The tasks require the patient´s response to an objective stimulus. In the first of them, the patient had to react by pressing the button before the appearance of red and white chessboards. This task implied 200 tries of which 50 required a response. In the second test, the patients had to click the right or left mouse button depending on the central arrow which is presented as a target stimulus. The Attention Network test was separated into two parts (72 trials / a 5-minute break to avoid fatigue / 72 trials). The features of the tool were the same as those used for the clinical trial carried out with a healthy elderly population [20].
- Memory: obtained with the Mini-mental State Examination (MMSE). At the end of the test, the patients obtain a score that determines the presence or absence of a cognitive decline. The Spanish version, called the Cognitive Mini-examination (MEC), consists of 30 items grouped into five parts: orientation, memorization, retrospective memory, concentration and calculation and language and construction. The sum of each part leads to the total score. The cut-off point for dementia is set at 24. Values closer to 30 correspond to optimal cognitive abilities.
- Balance: This outcome is measured with the application of the Berg scale [26]. The scale allows quantifying balance in different positions, obtaining a global score that guides the balance function in general which predicts on the possibility of use of wheelchair, the other technical aid or the total independence, for the development of the gait. The patients execute 14 different items, each of them being valued between 0 and 4 points. The total value is provided by the sum of the items. The balance interpretation could be good (41-56 points), compromised (21-40 points) and affected (0-20 points).
- Gait: valuated through the Timed Up and Go [27]. This measures how long it takes a subject to get up from a chair, walk three meters and go back to the starting position. A normal gait is considered if patients take less than 10 seconds to perform the test, a slight risk of falling if the test time is between 11 and 20 seconds, and a high risk of falling if it takes more than 20 seconds to perform the test.
- Functionality and risk of falls[28]: measured with the application of the Tinetti scale, an instrument that evaluates balance, gait and falls. The total items are 16 and the total score is 28 points. The scale has two dimensions: balance (9 items) with score between 0 and 16; and gait (7 items), between 0 and 12 points. The interpretation of the functionality and risk of falls is: high risk (<19 points); risk (19-23 points) and low or slight risk (24-28 points).
2.1. Treatment using feedback-based technology:
- Nintendo® Wii used with a long remote and gyroscopic technology. Movements, distances, angles, and speed are detected by wireless. This device offers acoustic feedback and visual. The main technical data are: a processor IBM Brodway 729 MHz, 512 MB Flash memory card, SD and SDHC cards, and Nintendo GameCube memory card, a Graphics ATI Hollywood 243 MHz, and Wi-Fi, Bluetooth 2.0, 2 x USB 2.0, LAN adaptor via USB 2.0.
- The Game (Wii-Fit©) requires the “Wii Balance Board”, a platform with four sensors which detects the pressure exerted on. The sensors are associated to the wireless controller and to a display with the movement bar. Later each user is registered, and its specific characteristics are evaluated, four exercise modalities are possible: yoga, toning, balance and aerobics. This research used the following game: "Penguin Slide" training balance and "Step Plus" training balance and aerobic exercises. The distance between the "Wii balance board" and the screen was one meter, and the screen was put on one meter high desk (Figure 1). "Penguin Slide" required the load transfer to both sides, the variation of the center of gravity, and the concentration of the users throughout the task in order to collect the fishes that jumped. The patients obtained points and feedback both visually and acoustic throughout the collected fish. "Step Plus" consisted of getting on and off the platform at the rhythm of the steps, simulating the gait and training balance (static, reactive and proactive). The patients obtained feedback again.
Intervention protocol: The piloting, which divided into seven phases was carried out in laboratory conditions.
-Phase I: The legal guardians read and singed the Informed Consent. Later, the users were assembled for a previous valuation and scales to identify physical-cognitive capacities by the researchers (physiotherapists and neuropsychologists).
-Phase II: It implied the collection of the initial assessments by each evaluator and later the insertion of these data in a database (ratings of each of the two observers and the average of the two).
- Phase III: Treatment using technology (games) in the intervention group. The total of the 30-minute sessions was 16, with a frequency of 2 times per week[29]. Each session consisted of 3 series of "Penguin Slide", 1 serie of "Step Plus" and 3 series more of "Penguin Slide". The sessions score was recorded on a sheet to encourage the patients and the caregivers. The infrastructure of this study made it possible to test two users at the same to improve motivation and adherence. The control group continued with their conventional treatment.
- Phase IV: Appointment of the patients for the final assessment and performance of the tests to determine the physical- cognitive capacities by the physiotherapists and the neuropsychologists.
- Phase V: The total assessments of each observer and the average scores, and to insert the data on the database.
- Phase VI: To finish the database and blinded the data to the observers, and to develop the statistical analyses.
- Phase VII: Once the data collection was finished, the control group received the same treatment than the interventional group.
2.2. Data Collection Procedures:
The physiotherapists and neuropsychologists assessing the patients had more than ten years of experience in this area. The valuations were carried out in two moments: before the intervention and seventy-two hours after the last session of the experimental group, for both groups.
The E-prime program and statistical package SPSS 18.0 were used.
The statistical analysis was as follows:
1) Shapiro-Wilk statistic was employed for the normality tests of the dependent variables. Mean and standard deviation or median and interquartile range (based on the normality of the variables) described the results of the dependent variables.
2) The homogeneity of both groups was verified before starting the treatment. In the case of those variables that have been adjusted to the normal, we use the Student's t-test for independent samples (or Welch's t-test when there is no homogeneity of the variances) and for those that do not adjust to the normal, the U from Mann-Whitney. Fisher's exact test was performed for the gender variable.
3) We proceeded to evaluate the existence of significant differences between tests and re-tests in each of the groups. The Student's t for related samples was used for the parametric variables and, the Wilcoxon Ranks for the non-parametric variables.
4) Lastly, the means of the difference variables on the MEC scale, Berg, Tinetti, "Timed up and Go test", Oddball and ANT-Elderly Tests; was calculated to compare both groups. Student's t for independent samples or Mann-Whitney U were applied by same way.
5) The effect size was calculated for the parametric variables (d=2t/√gl). Grissom criteria was applied for the non-parametric variables. The statistical analysis considered a 95% of confidence interval (p value <0.05).
2.3. Ethical considerations of the study:
The Research Ethics Committee of the University of Seville (Spain) authorized this study. The patients and the caregivers were informed about the research. Informed consent was obtained from all the legal guardian´s participants before research enrollment. The protocols followed the Declaration of Helsinki. According to Law 15/1999 on the Protection of Personal Data, the personal data that we required from the subjects were those necessary to carry out the study correctly. The study investigators did not disclose any participant information to anyone outside of the research. Participation was anonymous, however, the data of all the participants were listed and protected by the leading investigator, who would resort to it at crucial moments.
3. Results
After carrying out all the research phases reflected in the flowchart (Figure 2), the final sample consisted of 15 patients: 8 subjects for the control group (men: 37.5% ; women: 62.5%) and 7 subjects for the experimental group (men: 14.3%; women: 85.7%).
The descriptions of each of the variables valued, showing the mean with standard deviation or median with interquartile range, found differences in the experimental and control groups, as shown in the data table (Table 1).
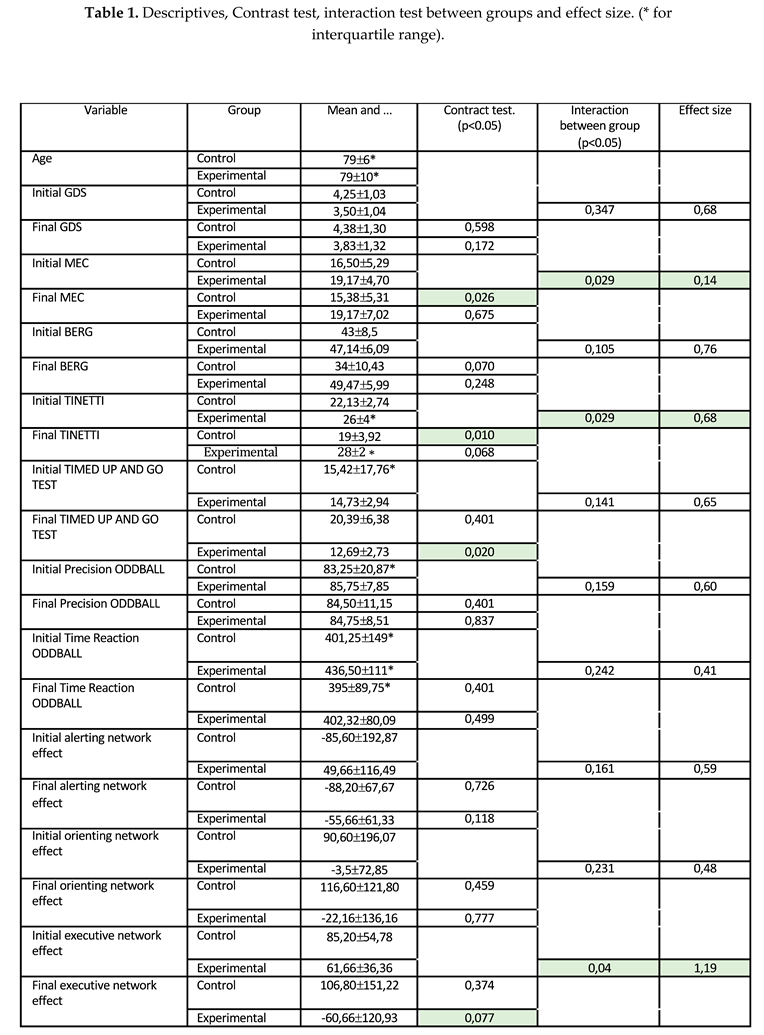
Regarding the gender of the patients in the groups, the distribution did not find statistically significant difference p(bilateral)=0.569. As regards the homogeneity tests, the analysis shows similar conditions in the respective variables for both groups. Comparing each group by isolate, a statistically significant difference was found in the Cognitive Mini-Examination (p<0.05) and Tinetti Scale (p<0.05) in the control group and a statistically significant difference in the Timed up and Go (p<0.05) in the interventional group. Figures indexed graphically expresses these differences through the marginal means (Figure 3, Figure 4 and Figure 5). The rest of the comparisons did not present statistical significance. (Table 1). Finally, the interaction between the groups showed statistically significant differences (p<0.05) in: the Cognitive Mini-Examination with a low effect size (d=0.14); the Tinetti which obtained a moderate effect size (d=0.68); and the Executive Network which found a high effect size (d=1.19). The effect sizes were calculated according to the criteria established in the methodology. The rest of the interactions do not show statistical significance. Table 1 collects all the values found in the study.
4. Discussion
The purpose of this paper was to evaluate the effectiveness of feedback-based technology on the improvement of physical-cognitive capacities in Alzheimer. After the development of the pilot using technology based on feedback, improvements in memory, balance and gait were found, as well as a decrease in the effect of the executive network. As regards physical capacities, the motor skills exercise seems to be effective for improving balance and gait (difference-Tinetti variable, p=0.029; d=0.68). The other variables that quantify balance and gait, did not observe significant differences, although the descriptive analysis points to an improvement in the results of the physical measurements applied in the experimental group with respect to the control group. Even so, the absence of worsening is considered a therapeutic achievement, as it is a degenerative disease. These findings coincide with Padala et al. [30], although to achieve a statistically significant difference, it would be necessary to expand the number of patients and design multicenter studies that would allow the sample to be increased. Agmon et al [31]also reached similar results regarding the benefits of information technologies with respect to physical abilities in these patients. With regard to cognitive abilities, the motor skills task seems to be effective in the global improvement of cognition (difference-MEC variable, p=0.029; d=0.14). This finding coincides with Maci et al [32], who determined the benefits that the development of cognitive activity, physical activity and socialization have on the course of the disease. The experimental group obtained benefits after the development of the global therapeutic program with respect to the control group, although this group of researchers focused their results more on the improvement on the main caregivers. Tools that mix cognitive, physical and social aspects seem to be effective for these patients. In this sense, the present pilot could be considered effective for the approach of these issues, being appropriate to improve the quality of life in the patients and minimize the Burnout syndrome in the caregivers.
On the other hand, the interaction between groups in the Cognitive Mini-Test agrees with the findings of Yamaguchi et al [33]. Regarding the efficacy of the motor task on attentional capacities, the results have only shown a unilateral significant difference-EXECUTIVE variable (p=0.04; d=1.19), showing a decrease in the effect of the executive network in the interventional group with respect to the control. This finding is disparate with respect to what has been found in the global cognitive assessment using the MEC. The justification for this data could be the instrument, which has shown difficulty for patients, showing an even lower precision than other investigations [34,35], as well as the complex circuits that hide the attentional networks. Global tests such as the Cognitive Mini-Examination evaluate the brain as a whole, but do not do so specifically. When we intend to specifically analyze specific neural circuits, the results may be different, and even more so if we start from the basis of a damaged brain. The routine designed in the ANT has multiple possibilities and the patient can activate different neural pathways. Regarding the Oddball Test, no statistical significance was found, but there was a clinical trend towards improvement in reaction times and accuracy percentage in the subjects of the control group compared to the experimental group. However, global cognitive abilities increase in the participants subjected to the activities with information technology. The explanation for this controversial data, even without being significant, could be that patients tend to automate the routine. A global improvement at the cognitive level can make the subject more aware of seeking an explanation for the task (for example, predicting if the target stimuli come out in a certain sequence, calculating the time between stimuli, if there is a sequence key). This fact may explain the decreased accuracy in the routine.
Based on what has been provided so far, it is understood that if physical and cognitive abilities improve after carrying out the activity using the Nintendo® Wii, autonomy will be optimized. Everyday activities imply attention, efficient motor planning processes, and useful inhibition of details that are unsuitable and irrelevant [36]. For all this, it is necessary that balance, gait, memory and attention, among other functions, be in the best conditions to achieve the greatest possible autonomy. Scherder et al [37] have already recommended the unification of physical activity and cognitive rehabilitation strategies to increase functionality. On the other hand, one of the great objectives in the gerontological sector is to prevent falls. People suffering from dementia have double risk of falling than the healthy elderly population with an annual incidence of approximately 80%[18,38]. Also, the mobility problems are considered relevant risk factors for falls [39]. The values found in this pilot study show that the experimental patients approach no risk of falls. However, in the control group, the risk increases, coinciding with other authors[9,10,30]. In this sense, although the small sample due to demanding selection criteria is proposed as a limitation, this pilot study seems to show the benefits that the use of feedback-based technology with therapeutic supervision, both in the physical capacities and in the cognitive capacities of the patients. Patients diagnosed with Alzheimer's disease, even seeing the benefit that this type of therapy could have secondarily due to its low cost, its feasibility of using it at home, as well as for creating intergenerational bonds.
5. Conclusions
This study concluded with an improvement in the physical-cognitive capacities of patients with Alzheimer's disease subjected to the use of feedback-based therapy. It should be deal with caution as it was a piloting. Likewise, the results in the control group showed a worsening in all functions. The Nintendo Wii could be an effective tool to keep patients in their initial stages, optimizing the quality of life of both them and their caregivers.
Knowledge of the state of the attentional networks by means of instruments such as the one applied in this study could be useful for selecting the ideal therapy in each case of Alzheimer's disease. Knowledge of the state of the attentional networks by means of instruments such as the one applied in this study could be useful for selecting the ideal therapy in each case of Alzheimer's disease. The use of feedback-based technology with the supervision of professionals can be an effective low-cost strategy framed in the patient's own home, as well as become an intergenerational approach.
Author Contributions
Conceptualization, MBL; methodology, GCM, MVM, MBL and CSS; formal analysis, VPC and MVM; investigation, EPP, MBL, GCM and MVM; data curation, MBL and MVM; writing—original draft preparation, MBL, GCM and CSS; writing—review and editing, MBL and GCM; supervision, MBL. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. .
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by Ethics Committee of University of Seville.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. The informed consent was signed by the patients´ legal guardians for their participation in this study. The datasets generated for this study are available on reasonable request to the corresponding author.
Acknowledgments
We would like to thank the Santa Elena Association, the main caregivers of the patients and the physiotherapist of the unit during the development of the research for their willingness and dedication. Likewise, to the patients of this disease, whom we will always remember despite their forgetfulness. In addition, the authors would like to thank the Research Group “Area of Phisiotherapy CTS-305” of the University of Seville, Spain, for their collaboration.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rodriguez-Laso A, McLaughlin SJ, Urdaneta E, Yanguas J. Defining and Estimating Healthy Aging in Spain: A Cross-sectional Study. Gerontologist. [CrossRef]
- Christensen K, Doblhammer G, Rau R, Vaupel JW. Ageing populations: the challenges ahead. The Lancet. 2009 Oct;374(9696):1196–208. [CrossRef]
- Zhao Q, Lu H, Metmer H, Li WXY, Lu J. Evaluating functional connectivity of executive control network and frontoparietal network in Alzheimer’s disease. Brain Res. 2018 Jan 1;1678:262–72. [CrossRef]
- Yogev-Seligmann G, Hausdorff JM, Giladi N. The role of executive function and attention in gait. Vol. 23, Movement Disorders. 2008. p. 329–42. [CrossRef]
- Li LZ, Wang S. Prevalence and predictors of general psychiatric disorders and loneliness during COVID-19 in the United Kingdom. Psychiatry Res. 2020 Sep 1;291. [CrossRef]
- Wu B. Social isolation and loneliness among older adults in the context of COVID-19: a global challenge. Glob Health Res Policy. 2020 Dec;5(1). [CrossRef]
- Schumacher J, Cromarty R, Gallagher P, Firbank MJ, Thomas AJ, Kaiser M, et al. Structural correlates of attention dysfunction in Lewy body dementia and Alzheimer’s disease: an ex-Gaussian analysis. J Neurol. 2019 Jul 1;266(7):1716–26. [CrossRef]
- Zhao Q, Sang X, Metmer H, Swati Z nawab NK, Lu J. Functional segregation of executive control network and frontoparietal network in Alzheimer’s disease. Cortex. 2019 Nov 1;120:36–48. [CrossRef]
- Arai H, Satake S, Kozaki K. Cognitive Frailty in Geriatrics. Clin Geriatr Med. 2018 Nov;34(4):667–75. [CrossRef]
- Walston J, Buta B, Xue QL. Frailty Screening and Interventions. Clin Geriatr Med. 2018 Feb;34(1):25–38. [CrossRef]
- Fan J, Posner M. Human Attentional Networks. Psychiatr Prax. 2004 Nov;31:210–4. [CrossRef]
- Mcdonough IM, Wood MM, Miller WS. A Review on the Trajectory of Attentional Mechanisms in Aging and the Alzheimer’s Disease Continuum through the Attention Network Test. Vol. 92, YALE JOURNAL OF BIOLOGY AND MEDICINE. 2019. PMCID: PMC6430165.
- Pieruccini-Faria F, Lord SR, Toson B, Kemmler W, Schoene D. Mental flexibility influences the association between poor balance and falls in older people - A secondary analysis. Front Aging Neurosci. 2019;11(JUN). [CrossRef]
- Cagnin A, Jelcic N, Agostini M, Meneghello F, Parise S, Galano A, et al. Feasibility and efficacy of cognitive telerehabilitation in early Alzheimer’s disease: a pilot study. Clin Interv Aging. 2014 Sep. [CrossRef]
- Burdea GC, Grampurohit N, Kim N, Polistico K, Kadaru A, Pollack S, et al. Feasibility of integrative games and novel therapeutic game controller for telerehabilitation of individuals chronic post-stroke living in the community. Top Stroke Rehabil. 2020 Jul 3;27(5). [CrossRef]
- Realdon O, Rossetto F, Nalin M, Baroni I, Cabinio M, Fioravanti R, et al. Technology-enhanced multi-domain at home continuum of care program with respect to usual care for people with cognitive impairment: the Ability-TelerehABILITation study protocol for a randomized controlled trial. BMC Psychiatry. 2016 Dec 25;16(1). [CrossRef]
- Hill NTM, Mowszowski L, Naismith SL, Chadwick VL, Valenzuela M, Lampit A. Computerized Cognitive Training in Older Adults With Mild Cognitive Impairment or Dementia: A Systematic Review and Meta-Analysis. American Journal of Psychiatry. 2017 Apr;174(4):329–40. [CrossRef]
- Choi SD, Guo L, Kang D, Xiong S. Exergame technology and interactive interventions for elderly fall prevention: A systematic literature review. Appl Ergon. 2017 Nov;65:570–81. [CrossRef]
- Chao YY, Scherer YK, Montgomery CA. Effects of Using Nintendo WiiTM Exergames in Older Adults. J Aging Health. 2015 Apr 21;27(3):379–402. [CrossRef]
- Benitez-Lugo ML, Suárez-Serrano C, Galvao-Carmona A, Vazquez-Marrufo M, Chamorro-Moriana G. Effectiveness of feedback-based technology on physical and cognitive abilities in the elderly. Front Aging Neurosci. 2022 Nov 10;14. [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013 Nov 27;310(20):2191-4. [CrossRef]
- Chan, A. W., Tetzlaff, J. M., Altman, D. G., Laupacis, A., Gøtzsche, P. C., Krleža-Jerić, K., et al. (2013). SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann. Intern. Med. 158, 200–207. [CrossRef]
- Sousa, M., Navas, Z., Laborde, M., Alfaro, B., José, J., Carrascosa, U., et al. (2017). Niveles de evidencia clínica y grados de recomendación levels of scientific evidence and degrees of recommendation. Repos Salud 29, 1–14.
- Cobos-Carbó, A., and Augustovski, F. (2011). Declaración CONSORT 2010: Actualización de la lista de comprobación para informar ensayos clínicos aleatorizados de grupos paralelos. Med. Clin. (Barc) 137, 213–21. [CrossRef]
- Vazquez-Marrufo M, Luisa Benitez M, Rodriguez-Gomez G, Galvao-Carmona A, Fernandez-Del Olmo A, Vaquero-Casares E. Attentional neural networks impairment in healthy aging. Rev. Neurol. 52, 20–26.
- Downs S. The Berg Balance Scale. J Physiother. 2015 Jan;61(1):46. [CrossRef]
- Browne W, Nair B (Kichu) R. The Timed Up and Go test. Medical Journal of Australia. 2019 Jan 28;210(1):13. [CrossRef]
- Park SH. Tools for assessing fall risk in the elderly: a systematic review and meta-analysis. Aging Clin Exp Res. 2018 Jan 3;30(1):1–16. [CrossRef]
- Lai CH, Peng CW, Chen YL, Huang CP, Hsiao YL, Chen SC. Effects of interactive video-game based system exercise on the balance of the elderly. Gait Posture. 2013 Apr;37(4):511–5. [CrossRef]
- Padala KP, Padala PR, Malloy TR, Geske JA, Dubbert PM, Dennis RA, et al. Wii-Fit for Improving Gait and Balance in an Assisted Living Facility: A Pilot Study. J Aging Res. 2012;2012:1–6. [CrossRef]
- Agmon M, Perry CK, Phelan E, Demiris G, Nguyen HQ. A Pilot Study of Wii Fit Exergames to Improve Balance in Older Adults. Journal of Geriatric Physical Therapy. 2011 Oct;34(4):161–7. [CrossRef]
- Maci T, Pira F le, Quattrocchi G, Nuovo S di, Perciavalle V, Zappia M. Physical and Cognitive Stimulation in Alzheimer Disease. The GAIA Project. American Journal of Alzheimer’s Disease & Other Dementiasr. 2012 Mar 10;27(2):107–13. [CrossRef]
- Yamaguchi H, Maki Y, Takahashi K. Rehabilitation for dementia using enjoyable video-sports games. Int Psychogeriatr. 2011 May 30;23(4):674–6. [CrossRef]
- Fernandez-Duque D, Black SE. Attentional networks in normal aging and Alzheimer’s disease. Neuropsychology. 2006;20(2):133–43. [CrossRef]
- Festa-Martino E, Ott BR, Heindel WC. Interactions Between Phasic Alerting and Spatial Orienting: Effects of Normal Aging and Alzheimer’s Disease. Neuropsychology. 2004;18(2):258–68. [CrossRef]
- Pichierri G, Wolf P, Murer K, de Bruin ED. Cognitive and cognitive-motor interventions affecting physical functioning: A systematic review. BMC Geriatr. 2011 Dec 8;11(1):29. [CrossRef]
- Scherder E, Eggermont L, Visscher C, Scheltens P, Swaab D. Understanding higher level gait disturbances in mild dementia in order to improve rehabilitation: ‘Last in–first out.’ Neurosci Biobehav Rev. 2011 Jan;35(3):699–714. [CrossRef]
- Shaw FE. Multifactorial intervention after a fall in older people with cognitive impairment and dementia presenting to the accident and emergency department: randomised controlled trial. BMJ. 2003 Jan 11;326(7380):73–73. [CrossRef]
- Speechley M. Unintentional Falls in Older Adults: A Methodological Historical Review. Can J Aging. 2011 Mar 1;30(1):21–32. [CrossRef]
Figure 1.
Task performance: devices location and patients.
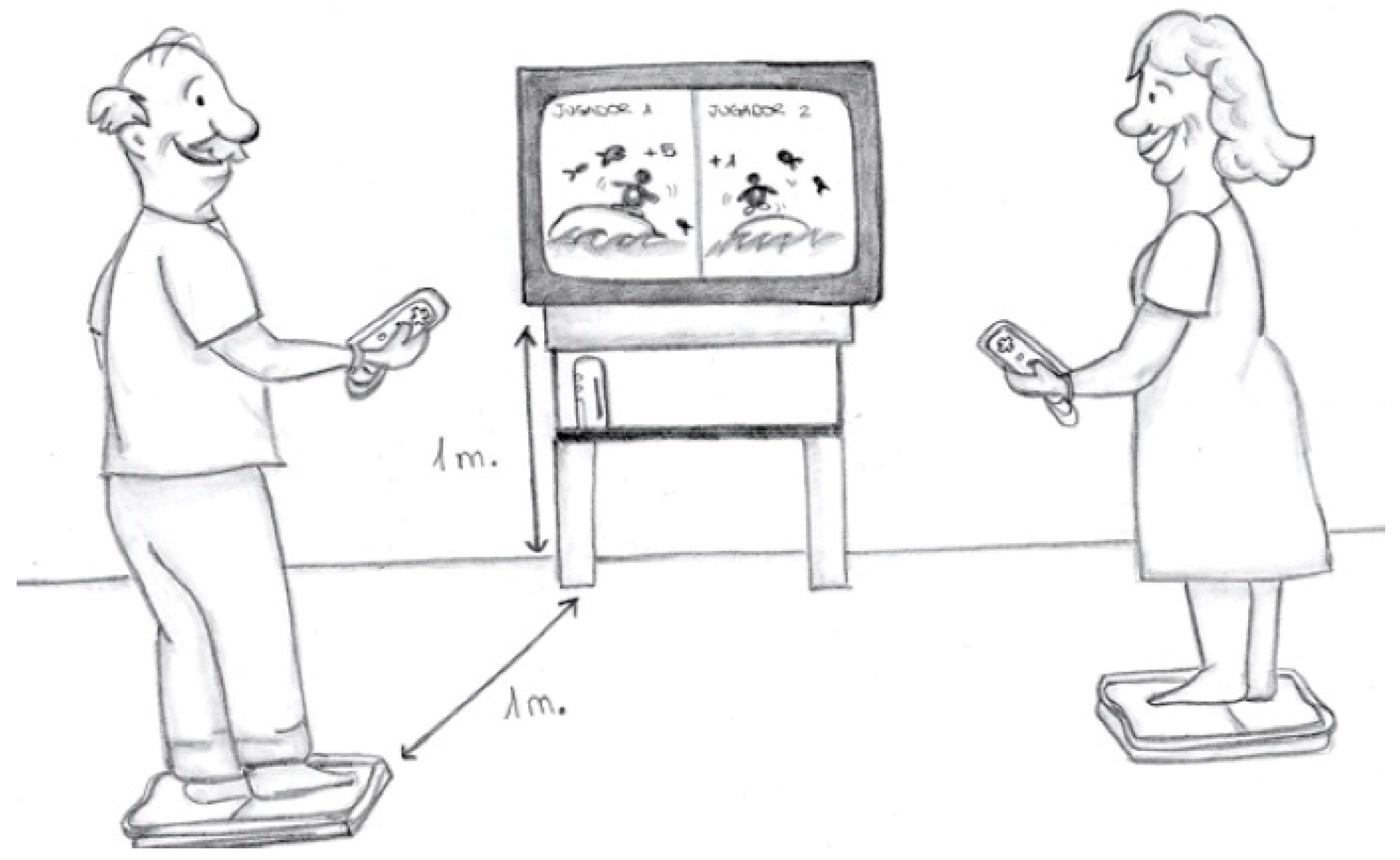
Figure 2.
Flowchart based in Consort Rules.
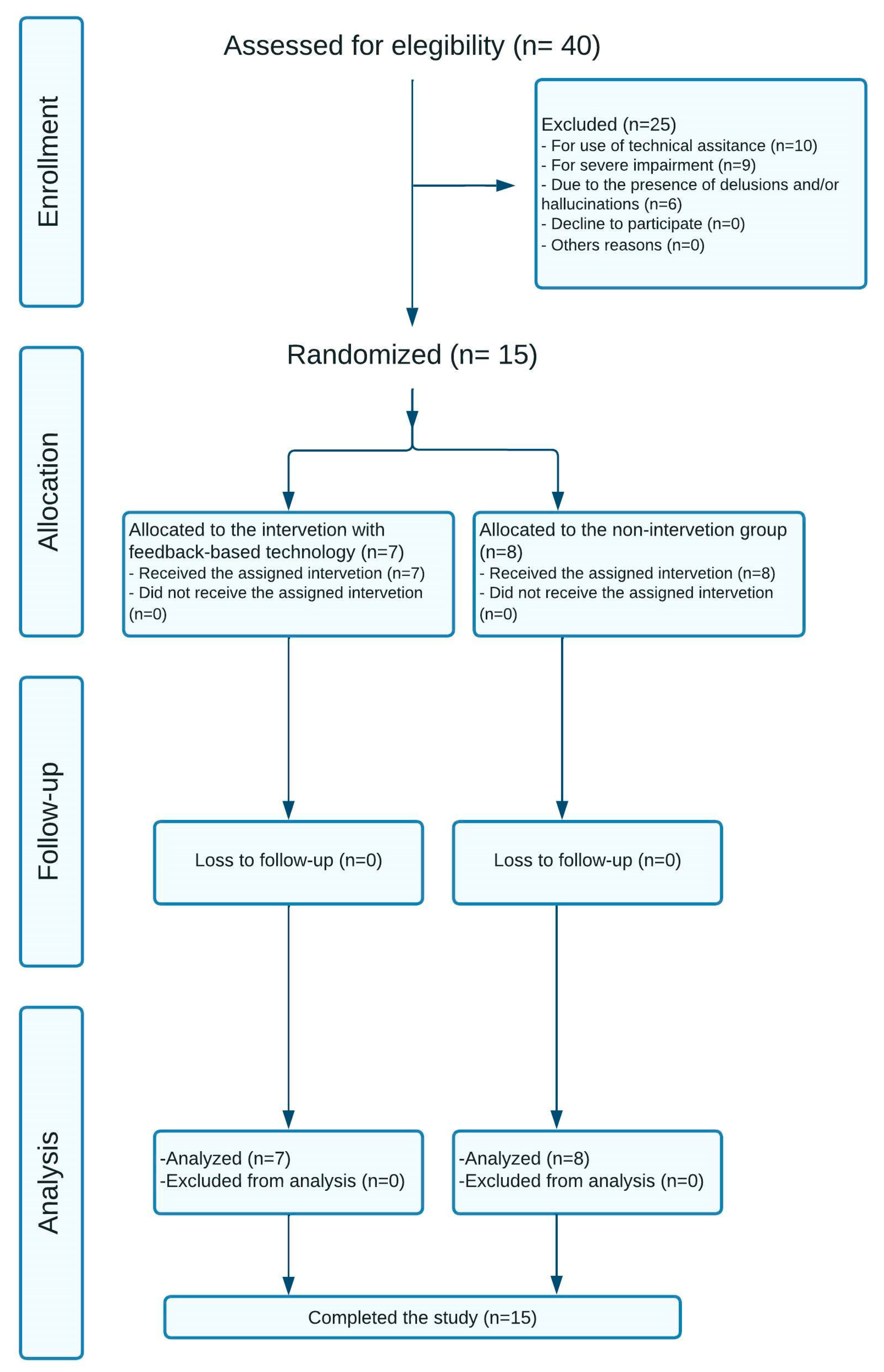
Figure 3.
MEC scale score mean.
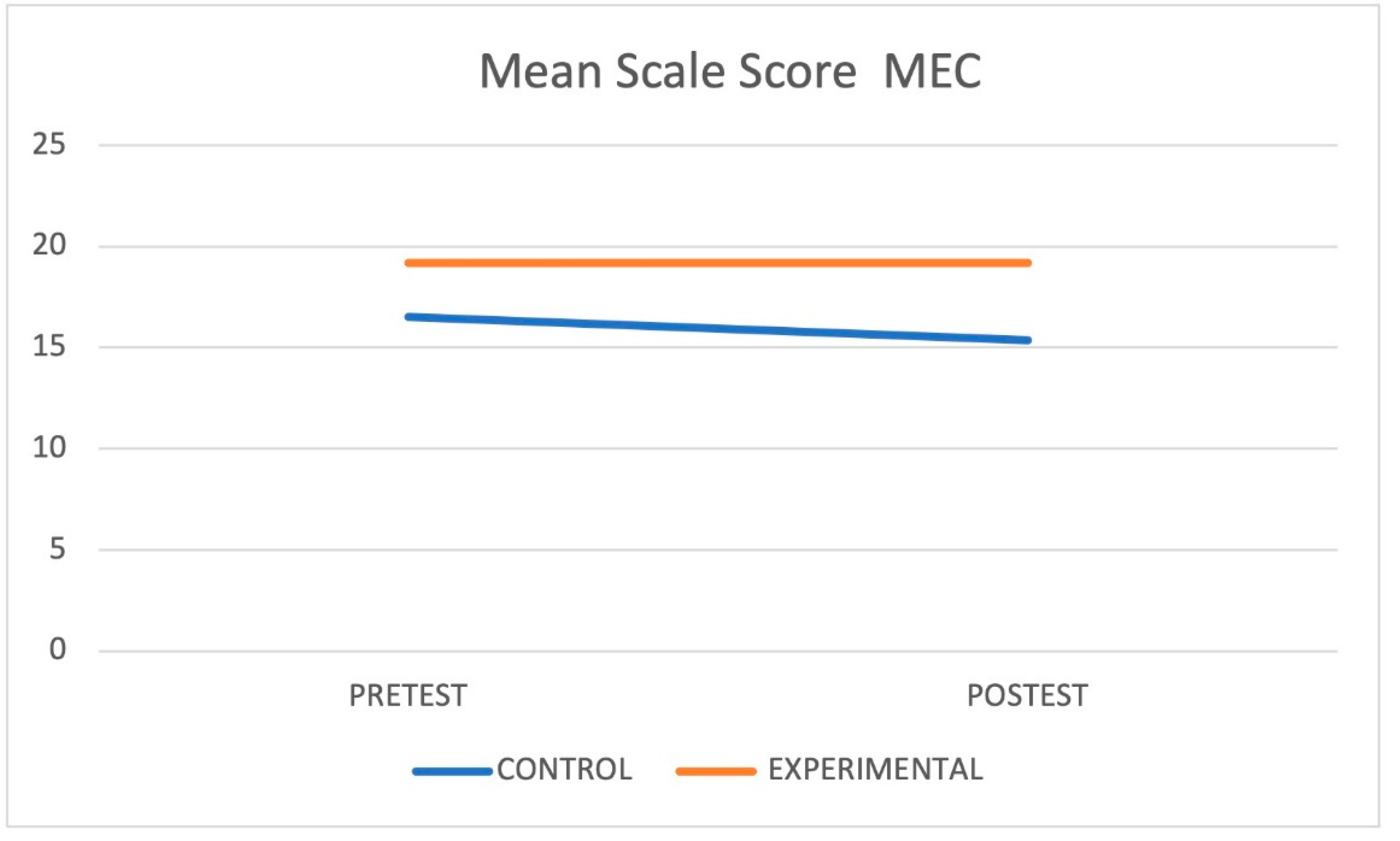
Figure 4.
TINETTI scale score mean.
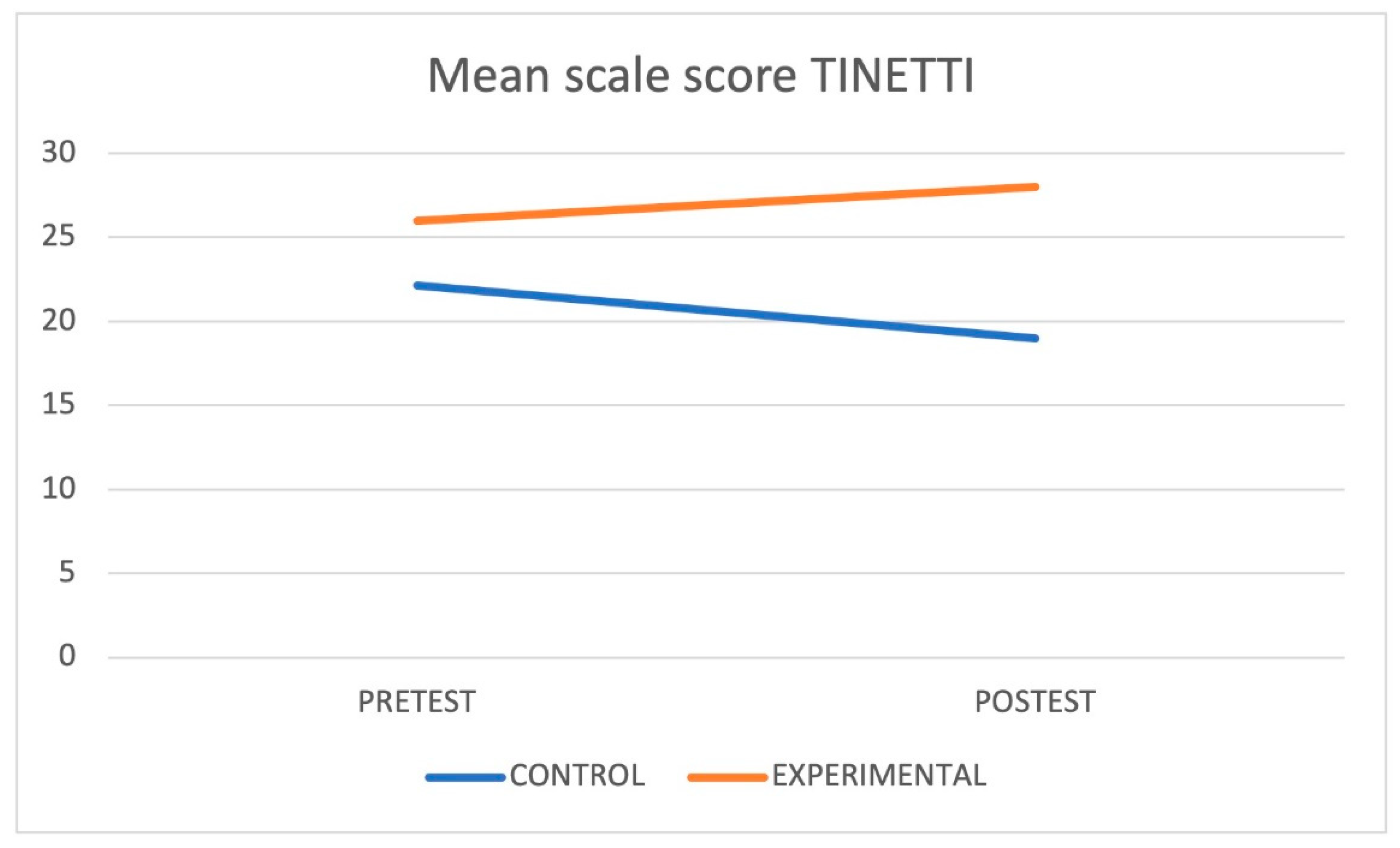
Figure 5.
TIMED UP AND GO TEST scale score mean.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



