
Submitted:
27 July 2023
Posted:
31 July 2023
You are already at the latest version
Abstract
Patient safety is a top priority for all healthcare systems globally. Promoting the adoption of policies for reporting and learning from errors is an important strategy for improving care safety. Therefore, the aim of our study was to detect how much patient safety culture influences the reporting of adverse events and the use of the incident reporting tool. The study protocol was developed according to PRISMA guidelines. Articles were searched electronically in PubMed/MEDLINE, the COCHRANE library, and Google Scholar by two independent reviewers, and those that met the eligibility criteria were included. Synthesis of qualitative data from included studies was performed by graphical descriptive statistical analysis. The results of the systematic review showed that health care organizations' increasing focus on staff development of a safety culture has led to a significant increase in incident reporting rates over the years. Moreover, in situations where safety culture is placed at the top of the nations, there is a higher frequency of incident reporting. An efficient incident reporting system should be an essential foundation for healthcare organizations, as it allows them to collect experiences and data and provide feedback to healthcare providers and staff involved in care.
Keywords:
healthcare workers
; health personnel
; risk management
; medical error
; incident reporting
; patient safety
; patient security
; professional education
; safety management
1. Introduction
The World Health Organization (WHO) has pronounced the development of a culture of safety as the basis for improving the quality of health care [1]. Globally, patient safety is a top priority for all healthcare systems. It has become particularly important since WHO established guidelines in 2005 to promote the adoption of policies on reporting and learning from errors to improve the safety of care.
Patient safety is understood as “the absence of accidental injury during the course of medical treatment; activities to avoid, prevent, or correct adverse events that may result from the delivery of health care” [2]. Problems are the adverse events that may happen. An adverse event is defined as “any unintentional harm resulting in temporary or permanent disability and/or prolongation of hospitalization time or death of a patient, as a result of healthcare provided by any member of the healthcare institution” [3].
Such unintentional harms can be patient falls in the hospital; in fact, according to epidemiological data collected from hospitals in the United Kingdom, 250,000 falls occurred between 2015 and 2016, resulting in femur fractures, significant lengthening of hospital stays, loss of patients' self-confidence, stress for families and healthcare staff, as well as increased medical-legal litigation against healthcare institutions [4]. Another most frequent adverse event, accounting for 70 percent of reported incidents, is “improper blood component transfusion” (IBCT), in which a patient receives a blood component that does not meet the correct specifications or is intended for another patient [5]. Unintentional harm can also result from peripheral intravenous catheters (PVCs), medication errors or especially vulnerable for patient’s safety is the process of triage.
WHO estimates have shown that 1 in 10 patients in high-income countries suffer an injury during hospital treatment each year, while in low-income countries 1 in 4 patients suffer an injury during hospitalizations [6,7]. Adverse events can be distinguished into nonpreventable and preventable adverse events. The former are complications that cannot be prevented [8], while the latter are attributable to errors, either in planning or execution of an action [9].
In addition, errors can be divided into human, violation, and organizational errors.
According to a field study conducted in Switzerland [10] half of all documented accidents are human errors, followed by organizational settings, infrastructure and environment, and technical problems, etc. The study conducted in Milan, Italy, found that most of the incidents involved nursing staff injuries, medication regulation, and errors in diagnostic procedures. In agreement with another study conducted in Genoa, Italy, patient falls, nursing staff accidents and errors in diagnostic procedures were reported [11]. While the study conducted in Japan, covered medication errors, followed by complications and errors with medical supplies and errors with patient falls [12].
Globally, there are an estimated 421 million hospitalizations each year and approximately 42.7 million are due to medical incidents related to diagnosis, documentation, medication, prescribing, dispensing, drug administration, surgery, procedures, and decision-making [13,14]. In a study conducted in Latin America, an incidence of adverse events of 19.8% was recorded and, specifically, in Colombia, the prevalence of which was 13.1% [15]. In another study, 34% of patients included in the research were found to have experienced an adverse event during their care [16], while in Spain up to 57.8% of healthcare workers were exposed to such events [17]. Patient safety events in healthcare in terms of accidents, near misses or unsafe conditions have been discussed in recent decades, following the Institute of Medicine report To Err is Human [18]. Adverse event reporting is not only a tool to make a diagnosis, but also to implement preventive measures, aimed at reducing events affecting patient safety [19].
Error can be contained with risk management initiatives, a systematic process aimed at identifying, assessing and dealing with current and potential risks [20,21].
In order to ensure safe care, it is important to have systemic thinking, both on the part of health policy makers and health care managers and clinical staff, in the area of Clinical Governance. Clinical Governance is “a system whereby organizations in the National Health System are responsible for continuously improving the quality of their services, ensuring high standards of care [22] and promoting integration and self-regulation of professionals [23]. Clinical Governance makes use of tools such as Evidence-Based Medicine, Quality Systems, Performance Assessment, Clinical Risk, Audit, and Health Technology Assessment, which enable the planning and evaluation of health care interventions [24].
So, a health care system, can reduce the occurrence of human error, minimize its impact on patients when it occurs, and learn so that it knows how to implement actions to protect future patients.
Patient safety monitoring can be approached with the reactive strategy (on a retrospective basis to identify the causes that led to the incident by employing Incident Reporting, Review, Root Cause Analysis, etc.); and proactive analysis (on a preventive basis, analyzing the causes that could lead to the incident, organizational processes, and their criticality, using Failure Mode Effects and Criticality Analysis).
As highlighted patient safety monitoring can be addressed through several strategies; one of the many is the reporting of adverse events through the Incident Reporting System.
Incident Reporting (IR) is one of the reactive analysis approaches for the management of clinical care risk and provides for a subsequent study of accidents, aimed at identifying the causes that led to the occurrence of an event [25]. The main purpose of this tool is to identify safety risks and implement interventions to mitigate these risks, in order to reduce harm in clinical practice. Typically, the Incident Reporting Record Sheet contains information about context, patient data and investigation type, factors that may have contributed to the event, the consequences of the event, the outcome of the event, and finally information on how the event could have been prevented [25].
This tool is used in the risk identification phase and covers other areas of the clinical risk management process, such as risk analysis and monitoring. The purpose of the tool is, therefore, to collect reports of events or near misses for the purpose of providing a database to prepare strategies, corrective actions and improvements to prevent their recurrence in the future. Appropriate use of the tool also provides a basis for analysis and improvement actions, such as identification of critical processes and business level.
IR is also used to detect preventable events, but many of them go unreported or simply unrecognized because healthcare professionals don't feel free, for fear of punitive action, blame or shame.
Thus, to ensure an approach that promotes continuous improvement, healthcare organizations must have continuous access to essential information to learn from experience in order to effectively identify and implement measures to prevent errors [26]. Incident reporting is an ideal tool to promote this strategy because, in addition to meeting the requirements of validity and reliability, it also indirectly provides data on the diffusion of safety culture among healthcare professionals and the full implementation of no-blame culture by healthcare organizations [27,28].
Therefore, the objective of the present study was to detect how much patient safety culture affects the reporting of adverse events and the use of the incident reporting tool.
2. Materials and Methods
The literature review was conducted using PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis) [29] guidelines.
The research question that guided this review was “How important is safety culture in adverse event reporting?” and the clinical question was developed following the P.I.C.O. format below:
P (Population): Healthcare workers and Health personnel.
I (Intervention): Risk management, medical error and Incident reporting.
C (Comparison): Patients safety culture and use of incident reporting.
O (Outcome): Patient safety, Security, Professional education.
2.1. Serarch Strategy and Study Selection
In May 2022, a bibliographic search was carried out on the Medline database (Pubmed), Google Scholar, and COCHRANE library databases, using the following MeSH terms: “healthcare workers”, “health personnel”, “risk management”, “medical error”, “incident reporting”, “patient safety”, “patient security”, “professional education”, “safety management”.
The following inclusion criteria were used:
- culture of safety within healthcare facilities;
- event reporting through incident reporting;
- culture of safety and reporting of adverse events.
In addition, the following exclusion criteria were used: tools for evaluating adverse events other than IR.
2.2. Data collection, extraction, synthesis and quality assessment
The following filters were applied: publications from the last 5 years. Screening, selection, exclusion, and data extraction of studies were performed by two independent reviewers. Any disagreements were discussed and a consensus was reached. The following information was extracted from each article: first author, year of publication, type of study and key points.
With focus on the study population, intervention, comparison and outcome, a narrative synthesis was performed. Synthesis of qualitative data from included studies was performed by graphical descriptive statistical analysis using Microsoft Excel 2023 software, version 16.72 (Microsoft Corporation, Redmond, WA, USA).
The methodological quality of the studies included in the systematic review was assessed through the Joanna Briggs Institute (JBI) Critical Appraisal Tool, which is recommended for the “risk of bias” of case reports, qualitative studies, mixed-method studies, and cross-sectional studies, used in our study [30].
3. Results
The initial search yielded 4,305 relevant studies. 4,256 articles were excluded after selecting titles and abstracts, according to the eligibility criteria; finally, 41 potential articles were screened for full text, reported in the following flowchart (Figure 1). After reading the full text, 33 articles were eliminated from the selection, as they did not meet the eligibility criteria, for a total of 8 articles included in the present systematic review [31,32,33,34,35,36,37,38].
The studies were conducted in Oman, Sweden, the Netherlands, the United Kingdom, Malaysia, Austria and Iran. All are considered to be of high quality, as they are described in detail and answer the research question and the key points are represented in the table below (Table 1).
A case study from the United Kingdom showed that the health care organization's special and increasing focus on staff in developing a culture of safety led to a significant increase in incident reporting rates over the years (t = 4.40, d.f. = 22, p < 0.01), with a mean value of monthly adverse event reporting rates in 2016 of 44.38 ± 3.21; and in 2017, 49.52 ± 2.96(Figure 2) [34].
In situations where safety culture is placed at the top of the nations, there was a greater influence in the frequency of event reporting: in the period prior to the implementation of a national program, it was 37.4%, while, in the period after, it was 62.7% (Figure 3) [38], fueled by healthcare organizations whose mission is continuous improvement [37].
Conversely, a qualitative survey from Oman showed that less attention to reporting incidents leads to a low perception of patient safety: the frequency of reported events has reached 40%, with a non-punitive response to error of 27% [31]. Perceptions of patient safety were limited, with 64% of study participants agreeing that their procedures and systems were effective in preventing errors.
Incident reporting is configured as a means to evaluate quality [36]: indeed, in a qualitative study, incident reporting provided information about problem areas of healthcare organizations that can lead to error and a less prevalence of fear of guilt, which is replaced by a greater focus on learning [32]. Incident reporting also enables attitudes towards patient safety to be changed by helping to generate “safety thinking”, which goes beyond learning to prevent adverse events and refers to a way in which professionals approach their work, aware of the risks to which they are exposed [33].
4. Discussion
This systematic review aimed to assess how much patient safety culture influences the reporting of adverse events and the use of the incident reporting tool.
The result of the systematic review showed that safety culture is the basis for continuous improvement in the care provided, and adverse event reporting is the tool for improvement. In agreement with Petschnig and Haslinger-Baumann, who showed that the increasing focus of healthcare organizations on developing a safety culture has led to a significant increase in incident reporting rates over the years (Figure 2) [36]. On the other hand, in safety-conscious healthcare organizations, incident reporting is a key tool for the continuous promotion of the reporting culture, without the healthcare professional having to feel guilty as a result of reporting the error [32,39,40]. It should be noted that even the most reputable healthcare organizations are not immune to adverse events, and several factors contribute to the frailty of health care services, the most common of which are patients falls, AB0 incompatible transfusions, catheter complications, medication errors, and patient assessment and classification at triage, which can have potentially disastrous outcomes.
In agreement with the results of our review, Verbeek-van Noord et al. highlight several issues related to patient harm, but also point out that nationwide patient safety programs (PSPs) can make patient harm highly predictable [38].
It has been observed that in the United States, 30-50% of falls that occur in the hospital result in injuries and an average increase of 6.3 days of hospitalization, with an average cost per fall estimated at about $14,000 [41]. The situation in Italy is no more comforting. The Ministry of Health [42] has defined serious injury or death due to falls in the hospital as a “sentinel event”, i.e., an “adverse event of particular severity, which may result in death or serious harm to the patient, and which determines a loss of public confidence in the health service”. Specifically, falls with injury was the most reported sentinel event: 471 events, or 24.6% of the total during the monitoring period from September 2005 to December 2012. As a result, the report affirms the need to support the use of fall risk assessment tools to identify patients at risk in order to develop interventions aimed at prevention [42].
Another most frequently occurring adverse event, in 70% of reported incidents, is “incorrect blood component transfusion” (IBCT) to the patient [43]. The Serious Hazards of Transfusion (SHOT) [44] scheme reported that IBCT events result in 50% of the cases being errors in the process, while 70% of the errors occur in the clinical areas and are due to failure to perform a final pre-transfusion check at the patient's bedside. On the other hand, acute intravascular hemolysis due to ABO incompatibility with catastrophic outcome can be due to incorrect patient identification, sample mislabeling, and incorrect component collection and administration.
Unintentional harm can also result from peripheral intravenous catheters (PVCs), which are the most widely used invasive medical devices in hospitals [45]. In the United States alone, about 330 million are sold annually [46]. Unfortunately, PVCs can fail before the end of treatment due to complications, which can be mechanical, such as occlusion, infiltration, and accidental removal; vascular, such as venous thrombotic occlusion and phlebitis; or infectious, which can be bacterial or fungal and local or systemic bloodstream infections. In the United States, estimating the overall hospital population, an estimated 250,000 cases of catheter-related bloodstream infections (CRBSIs) occur annually [47].
A central issue in patient safety is medical errors, which have recently been listed as the third leading cause of death in the United States [48,49]. Among adverse events in medical practice, therapeutic errors are the most common cause. Several studies estimate that medication-related incidents account for 6-12% of hospital admissions and 2 out of every 1,000 hospital deaths, making them a serious public health problem [50,51,52].
It should be remembered that therapeutic errors result in annual costs to European health care systems of between 4.5 and 21.8 billion euros [53,54]. They can occur at any stage of the therapeutic process and can affect different groups of health care providers. In the United States of America, medication errors cause at least one death per day and injure about 1.3 million people each year [55,56].
In addition to therapeutic errors, surgical errors can also have serious consequences, including preventable deaths [57]. In 1991, the Harvard Medical Practice study found that 53% of adverse events were associated with surgery. Of these, 26% were technical adverse events and 10% were due to failure to achieve surgical goals [58].
Another particularly vulnerable point in patient safety is triage. Triage is the first process of assessing and classifying patients arriving in emergency departments; at this stage, triage registered nurses are critical in assessing patients' acuity levels, mortality risks posed by their conditions, and anticipated resource needs. Under- or over-triage errors can lead to adverse outcomes or patient deaths [59].
The important point is to translate all these negative events into moments of professional growth to promote a robust and resilient system that can respond promptly to any other event.
One instance is the Led Outdoor Activities (LOA) [60] held annually in Australia and attended by thousands of people. The main characteristic of LOAs is to conduct outdoor activities [61] within school camps with a higher level of risk to achieve learning and developmental outcomes [62,63,64,65]. LOAs in Australia are conducted with low levels of negative incidents, despite the increased risk. This is because safety controls are in place in most cases to prevent accidents [66,67] and the accident rate for people participating in LOAs is 2 per 1000 participants with minor severity [67]. This example suggests that formal incident reporting prevents future events [68,69,70].
According to data extracted by Ghasemi et al. [35], errors can be influenced by personal, professional, and organizational factors. In the personal factor category, nurse fatigue and physical health had the greatest and least weight, respectively. Compared with the work category, workload has the highest weight; at the same time, work environment has the lowest weight. In the organization category, the highest and lowest weights were associated with patient safety climate and communication among staff, respectively. A more positive safety culture has been shown to be associated with higher reporting rates [71,72,73]. In order to improve patient safety, it is essential not only to obtain detailed information about the event, but also to standardize the safety management system in hospitals, creating openness on the topic to patients and users [74].
In agreement with the results of our review, a study conducted in Ethiopia, showed that those who had received adequate training on adverse event reporting were 3.6 times more likely to report events than providers who received no training on the subject. Furthermore, health care workers who did not receive feedback following the reporting of adverse events were 69.3% more likely to report them than those who do not [75]. In agreement with Naome et al. [76] whose survey results showed that 93% of respondents believe that knowledge of what, how and to whom to report incidents is crucial.
Another key factor in promoting safety culture is teamwork, which reduces the occurrence of adverse events and, at the same time, improves their reporting [77,78,79]. Indeed, effective leadership is able to create and promote a culture of patient safety. Even opinion leaders, through their authority and charisma, can increase the culture of safety and reporting in healthcare organizations, motivating colleagues to change their performance and their behavior, through an audit-and-feedback system [80].
In addition, the implementation of a safety culture system at the individual country level appears to have a positive effect on error reporting [38,79,81]. The IR system, if implemented appropriately, enables the development of a culture of continuous learning and improvement [34,82]. According to De Kam et al. [33], as reporting decreased, the perceived absence of punishment with respect to need to report errors has increased in health care staff. Indeed, the key elements of a well-functioning reporting system are feedback, involvement of all staff in an organization, leadership [31], including top management commitment, and integration of 'IR into both risk management and quality management. In this regard, in the research of Carlfjord et al. [32], it was shown how IR increases the pursuit of quality in the management of care delivered and places the management of safety of care for both physicians and staff at the 1st place on the nursing agenda. A well-planned and implemented incident reporting system can improve organizational culture of error reporting, learning processes, and safety of care [64]. Staff training on the topic is also critical to increase awareness of reporting. In a study conducted in Taiwan, it was found that nurses who are in a managerial role and hold advanced degrees play a crucial role in promoting event reporting and the development of a culture of patient safety [82,83]. It is important for managers to ensure that staff consider patient safety as a top priority, motivating and empowering staff to prevent adverse events and promote patient safety [84]. To this end, a qualified corporate risk manager should be established to encourage the recognition and implementation of the adverse event reporting system [85]. Only through the information provided with the report card is it possible to analyze the reported events to identify the factors that contributed to the occurrence of the reported event or risk situation and to share with the facilities involved possible corrections to prevent recurrence or contain the possible harm caused. Within healthcare organizations, for the culture of safety to improve, communication based on mutual trust and openness must be established [86]. Patient safety must always remain the priority in health care, and contributions from health care providers must be ongoing to enable continuous organizational improvements [87]. In accordance with the precursor of clinical risk management, the well-known Florence Nightingale who, more than a century ago, indicated the need to ensure that patients did not also suffer from the unintended consequences of the care provided to them, in addition to those due to their illness [80].
It is important for healthcare systems need to invest in staff training and a non-punitive error culture [34,88], through the adoption of incident reporting (IR) systems that can stimulate social and participatory learning [33]. Learning, in fact, represents a shared understanding among group members of a new course of action to minimize or prevent the recurrence of adverse events [89,90,91,92,93,94,95,96,97,98,99]. Learning also occurs through the study and investigation of near misses. Missed incidents go unexamined because of professionals' fear of consequences, the attribution of an exclusively negative valence to error, the belief that the highly skilled professional cannot make errors, the belief that errors are causal and highly variable, the belief that training and practice improve, and the belief that it is more effective to replace people than contexts [100].
Effective communication among healthcare professionals is critical to ensuring safe care, especially in multidisciplinary settings of complex medical services [101]. In this perspective, the World Health Organization (WHO) has promoted “World Patient Safety Day” [102] to urge all countries to sustain attention and information on the issue of safety of care and the person being cared for by organizing national events and initiatives.
According to our analysis, therefore, improving ongoing communication must be a challenge, especially with regard to incident reporting and actions to promote safe care, with the aim of building a virtuous circle that contributes to the improvement of organizational culture.
Our study has some limitations, one of which is the total number of 8 articles included in this systematic review, which may seem small, but considering our inclusion and exclusion criteria, only a few articles in the literature have considered Incident Reporting (IR) as a tool for evaluating adverse events. In addition, we excluded some databases (Scopus, LILACS, and EMBASE) from the electronic search.
5. Conclusions
In summary, we can say that a culture of safety can only be achieved in an environment that is open, transparent, and involves all levels of the organization. These principles are the fundamental basis for being able to work in an organization that can reduce the risk of adverse events as much as possible. An efficient incident reporting system should be an essential foundation for health care organizations [76], as it allows them to collect experiences and data (such as, for example, adverse events and near misses) and provide feedback to health care providers and staff involved in care. In addition, ensuring support for professionals involved in events is critical; professionals involved in the event most often remain emotionally traumatized by it and can therefore be considered “second victims.” Without adequate support, the event experience can damage the emotional and physical health of the professional involved, generate doubts about his or her skills and knowledge, reduce job satisfaction, and even lead, in extreme cases, to a desire to leave the health care profession. Achieving a culture of safety requires understanding the values, attitudes, beliefs, and norms that are important to health care organizations and the appropriate and expected attitudes and behaviors for patient safety [19]. Differences between contexts (e.g., policies, culture, and health care organization characteristics) may explain differences in the effects of implementing patient safety solutions. There is a need to implement a system of continuing education for staff in healthcare organizations so that they understand that corrective actions can result from an error, aimed at continuous improvement and ensuring safe care. In addition, safety management must be conceived at all levels of decision-making and intervention in health care, since at the central level (ministerial or regional) it can be a tool of authority and territorial weight of interventions; and at the peripheral level (companies or individual operating units), an effective tool, thanks to the direct involvement and motivation of operators [103].
Author Contributions
Conceptualization, V.C., A.P. and B.I.; methodology, V.C., A.P. and S.M.A.; software, S.M.A.; validation, V.C., A.P. and B.I.; investigation, V.C., V.A. and S.M.A.; data curation, V.C. and V.A.; writing—original draft preparation, V.C., V.A. and S.M.A.; writing—review and editing, S.M.A.; visualization, B.I. and R.H.W.F.; supervision, R.H.W.F. and M.C.; project administration, V.A. and M.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Medline/PubMed, Cochrane databases and Google Scholar.
Acknowledgments
Thanks to Giosuè Bacchin for precious assistance in translating the paper.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO. Patient safety in developing and transitional countries: new insights from Africa and the Eastern Mediterranean. Geneva, Switzerland, World Health Organization, 2011.
- Kohn, L.T.; Corrigan, J.M.; Donaldson, M.S. Errors in Health Care: A Leading Cause of Death and Injury. In: To Err Is Human: Building a Sager Health System, National Academy Press, Washington DC, 2000, 26-48.
- Mira, J.J.; Cho, M.; Montserrat, D.; Rodríguez, J.; Santacruz, J. Elementos clave en la implantación de siste- mas de notificación de eventos adversos hospitalarios en América Latina. Rev Panam Salud Publica. 2013, 33(1), 1–7.
- Royal College of Physicians. National Audit of Inpatients Falls: Audit report 2017. London, Royal College of Phsysicians, 2017.
- Stainsby D. ABO incompatible transfusions--experience from the UK Serious Hazards of Transfusion (SHOT) scheme Transfusions ABO incompatible. Transfus Clin Biol. 2005, 12(5), 385-8. [CrossRef]
- WHO. Patient safety: making health care safer. Geneva, Switzerland: World Health Organization 2017.
- WHO. Patient Safety – Making Health Care Safe. Switzerland, World Health Organization, 2019.
- Leape, L. L.; Lawthers, A. G.; Brennan, T. A.; Johnson, W. G. Preventing medical injury. QRB. Quality review bulletin, 1993, 19(5), 144–149. [CrossRef]
- Reason, J. Human Error. Cambridge, Cambridge University Press, 1990.
- Rose, N.; Germann, D. Resultate eines krankenhausweiten Critical Incident Reporting System (CIRS). Gesundheitsökonomie Qualitätsmanagement. 2005,10(2), 83–9. [CrossRef]
- Tereanu, C.; Minca, D.G.; Costea, R; Grego, S; Ravera, L; Pezzano, D.; Vigano, P. ExpIR-RO: a collaborative international project for experimenting voluntary incident reporting in the public healthcare sector in Romania. Iran J Public Health. 2011, 40(1), 22–31.
- Nakajima, K.; Kurata, Y.; Takeda, H. A web-based incident reporting system and multidisciplinary collaborative projects for patient safety in a Japanese hospital. Qual Saf Health Care. 2005, 14(2), 123–9. [CrossRef]
- World Alliance for Patient Safety. WHO draft guidelines for adverse event reporting and learning systems. 2005. Available from: https://apps.who.int/iris/bitstream/handle/10665/69797/WHO-EIP-SPO-QPS-05.3-eng.pdf (accessed on July 7, 2023).
- Institute of Medicine (US) Committee on Optimizing Graduate Medical Trainee (Resident) Hours and Work Schedule to Improve Patient Safety. In: Ulmer C, Miller Wolman D, Johns MME, editors. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. Washington (DC): National Academies Press (US); 2009. p. 8. System Strategies to Improve Patient Safety and Error Prevention. Available from: https://www.ncbi.nlm.nih.gov/books/NBK214937/ (accessed on July 7, 2023).
- Ministerio de Sanidad y Politica Social de Espana/OMS. Estudio IBEAS: Prevalencia de efectos adversos en hospitales de Latinoamerica, 2019.
- Parra, C.V.; Lopez, J.S.; Bejarano, C.H.; Puerto, A.H.; Galeano, M.L. Eventos adversos en un hospital pediatrico de tercer nivel de Bogota. Rev Fac Nac Salud Publica. 2017, Vol. 35, N.2.
- Mira JJ, Carrillo I, Lorenzo S, Ferrús L, Silvestre C, Pérez-Pérez P, Olivera G, Iglesias F, Zavala E, Maderuelo-Fernández JÁ, Vitaller J, Nuño-Solinís R, Astier P; Research Group on Second and Third Victims. The aftermath of adverse events in Spanish primary care and hospital health professionals. BMC Health Serv Res. 2015, 9(15), 151. [CrossRef]
- Khon, L.; Corrigan, J.; Donaldson, M. Errare è umano: costruire un sistema sanitario più sicuro. Comitato per la qualità della salute in America, Institute of Medicine. Washington, DC: National Academy Press, 1999.
- Miasso, A.; Grou, C.; Cassiani, S.; Silva, A.; Fakih, F. Erros de medicacno: Tipos, fatores causais e providencias em quatro hospitais brasileiros. Rev Esc Enferm USP. 2006, 40(4).
- Del Vecchio, M.; Cosmi, L. Il Risk management nelle aziende sanitarie. Milano, McGraw-Hill, 2003.
- Damiani, G.; Specchia, M.; Ricciardi, W. Manuale di Programmazione e organizzazione sanitaria. Napoli, Idelson-Gnocchi, 2018.
- Secretary of State for Health. The New NHS: modern, dependable. London, Stationery Office, 1997.
- Ricciardi, W.; Boccia, S. Igiene, Medicina Preventiva e Sanità Pubblica. Napoli: Idelson-Gnocchi, 2021.
- Buscemi, A.; Limone, D.; Bugiolacchi, L.; Turco, A. Il Risk management in sanità (2nd ed.). Milano: Franco Angeli, 2015.
- Bizzarri, G.; Canciani, M.; Farina, M. Strategia e gestione del rischio clinico nelle organizzazioni sanitarie: approcci, modalità, strumenti e risultati. Milano, Franco Angeli, 2018.
- Cascini, F., La Regina, M., Ricciardi, W., & Tartaglia, R. Manuale di sicurezza del paziente e gestione del rischio clinico. Perugia, Cultura e Salute Editore, 2022.
- Joint Commission International. JCI Accreditation Standards for Hospitals, 7th ed.; Joint Commission Resources: Oakbrook Terrace, IL, USA, 2020.
- Vetrugno, G.; Foti, F.; Grassi, V.M.; De-Giorgio, F.; Cambieri, A.; Ghisellini, R.; Clemente, F.; Marchese, L.; Sabatelli, G.; Delogu, G.; et al. Malpractice Claims and Incident Reporting: Two Faces of the Same Coin? Int. J. Environ. Res. Public Health 2022, 19, 16253. [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [CrossRef]
- Ma, LL.; Wang, YY.; Yang, ZH. et al. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: what are they and which is better?. Military Med Res 2020, 7, 7. [CrossRef]
- Al Lawati, M. H.; Short, S. D.; Abdulhadi, N. N.; Panchatcharam, S. M.; Dennis, S. Assessment of patient safety culture in primary health care in Muscat, Oman: A questionnaire -based survey. BMC Family Practice, 2019, 20(1), 50. [CrossRef]
- Carlfjord, S.; Öhrn, A.; Gunnarsson, A. Experiences from ten years of incident reporting in health care: A qualitative study among department managers and coordinators. BMC Health Services Research, 2018, 18(1), 113. [CrossRef]
- De Kam, D.; Kok, J.; Grit, K.; Leistikow, I.; Vlemminx, M.; Bal, R. How incident reporting systems can stimulate social and participative learning: A mixed-methods study. Health Policy (Amsterdam, Netherlands), 2020, 124(8), 834–841. [CrossRef]
- Flott, K.; Nelson, D.; Moorcroft, T.; Mayer, E. K.; Gage, W.; Redhead, J.; Darzi, A. W. Enhancing Safety Culture Through Improved Incident Reporting: A Case Study in Translational Research. Health Affairs (Project Hope), 2018, 37(11), 1797–1804. [CrossRef]
- Ghasemi, F.; Babamiri, M.; Pashootan, Z. A comprehensive method for the quantification of medication error probability based on fuzzy SLIM. PloS One, 2022, 17(2), e0264303. [CrossRef]
- Petschnig, W.; Haslinger-Baumann, E. Critical Incident Reporting System (CIRS): A fundamental component of risk management in health care systems to enhance patient safety. Safety in Health, 2017, 3(1), 9. [CrossRef]
- Raeissi, P.; Reisi, N.; Nasiripour, A. A. Assessment of Patient Safety Culture in Iranian Academic Hospitals: Strengths and Weaknesses. Journal of Patient Safety, 2018, 14(4), 213–226. [CrossRef]
- Verbeek-van Noord, I.; Smits, M.; Zwijnenberg, N. C.; Spreeuwenberg, P.; Wagner, C. A nation-wide transition in patient safety culture: A multilevel analysis on two cross-sectional surveys. International Journal for Quality in Health Care: Journal of the International Society for Quality in Health Care, 2019, 31(8), 627–632. [CrossRef]
- Aaron, M.; Webb, A.; Luhanga, U. A Narrative Review of Strategies to Increase Patient Safety Event Reporting by Residents. Journal of Graduate Medical Education, 2020, 12(4), 415–424. [CrossRef]
- Chiang, H.-Y.; Lee, H.-F.; Lin, S.-Y.; Ma, S.-C. Factors contributing to voluntariness of incident reporting among hospital nurses. Journal of Nursing Management, 2019, 27(4), 806–814. [CrossRef]
- Commission J. Preventing falls and fall-related injuries in health care facilities. Sentinel Event Alert 2015, 55, 1-5.
- Ministero della Salute. Protocollo di monitoraggio degli eventi sentinella: 5° rapporto Settembre 2005-Dicembre 2012. Roma, 2013.
- Stainsby, D. ABO incompatible transfusions—experience from the UK Serious Hazards of Transfusion (SHOT) scheme Transfusions ABO incompatible. Transfusion clinique et biologique 2005, 12, 385–388. [CrossRef]
- Serious Hazards of Transfusion. Available from www.shotuk.org. (Accessed on July 23, 2023).
- Keogh, S.; Flynn, J.; Marsh, N.; et al. Varied flushing frequency and volume to prevent peripheral intravenous catheter failure: a pilot, factorial randomised controlled trial in adult medical-surgical hospital patients. Trials 2016, 17, 348. [CrossRef]
- Hadaway L. Short peripheral intravenous catheters and infections. J Infus Nurs 2012, 35, 230–40. [CrossRef]
- Guenezan, J.; Drugeon, B.; O'Neill, R. et al. Skin antisepsis with chlorhexidine–alcohol versus povidone iodine–alcohol, combined or not with use of a bundle of new devices, for prevention of short-term peripheral venous catheter- related infectious complications and catheter failure: an open- label, single-centre, randomised, four-parallel group, two-by-two factorial trial: CLEAN 3 protocol study. BMJ Open 2019, 9, e028549. [CrossRef]
- Makary, M.A.; Daniel, M. Medical error: The third leading cause of death in the US. BMJ. 2016, 353, i2139. [CrossRef]
- Mackenzie, C.F.; Shackelford, S.A.; Tisherman, S.A.; Yang, S.; Puche, A.; Elster, E.A.; Bowyer, M.W. Retention and Assessment of Surgical Performance Group of Investigators. Critical errors in infrequently performed trauma procedures after training. Surgery. 2019, 166(5), 835-843. [CrossRef]
- Hartel, M.J.; Staub, L.P.; Röder, C.; Eggli, S. High incidence of medication documentation errors in a Swiss university hospital due to the handwritten prescription process. BMC Health Serv Res 2011, 11, 199. [CrossRef]
- Jolivot, P-A.; Pichereau, C.; Hindlet, P.; Hejblum, G.; Bigé, N.; Maury, E. et al. An observational study of adult admissions to a medical ICU due to adverse drug events. Ann Intensive Care 2016, 6(1), 9. [CrossRef]
- Morimoto, T.; Sakuma, M.; Matsui, K.; Kuramoto, N.; Toshiro, J.; Murakami, J.; Fukui, T.; Saito, M.; Hiraide ,A.; Bates, D.W. Incidence of Adverse Drug Events and Medication Errors in Japan: the JADE Study. Journal of General Internal Medicine. 2010, 26(2), 148–153. [CrossRef]
- World Health Organization. Reporting and learning systems for medication errors: the role of pharmacovigilance centres. 2014. Available from: http://www.who.int/medicines/areas/quality_safety/safety_efficacy/emp_mes/en (Accessed on July 12, 2023).
- Goedecke, T.; Ord, K.; Newbould, V. et al. Medication Errors: New EU Good Practice Guide on Risk Minimisation and Error Prevention. Drug Saf 2016, 39, 491–500. [CrossRef]
- World Health Organization (2017b). WHO launches global effort to halve medication-related errors in 5 years. Available from https://www.who.int/news-room/detail/29-03-2017-who-launches-global-effort-to-halve-medication-related-errors-in-5-years (Accessed on July 12, 2023).
- Suclupe, S.; Martinez-Zapata, M.J.; Mancebo, J. et al. Medication errors in prescription and administration in critically ill patients. JAN Loading Global Nursing Research 2020, 76(5), 1192-1200. [CrossRef]
- Mackenzie, C.F.; Shackelford, S.A.; Tisherman, S.A.; Yang, S.; Puche, A.; Elster, E.A.; Bowyer, M.W. Retention and Assessment of Surgical Performance Group of Investigators. Critical errors in infrequently performed trauma procedures after training. Surgery. 2019, 166(5), 835-843. [CrossRef]
- Leape, L.L.; Brennan, T.A.; Laird, N.; et al. The nature of adverse events in hospi- talized patients: Results of the Harvard Medical Practice Study II. N Engl J Med. 1991, 324, 377e384. [CrossRef]
- Ausserhofer,D.; Zaboli, A.; Pfeifer, N.; Solazzo, P.; Magnarelli, G.; Marsoner, T.; Siller, M.; Turcato, G. Errors in nurse-led triage: An observational study. International Journal of Nursing Studies, 2021, 113, 103788. [CrossRef]
- McLean, S.; Finch, C.; Coventon, L.; Salmon, P.M. Incidents in the Great Outdoors: A systems approach to understanding and preventing led outdoor accidents. Proceedings of the Human Factors and Ergonomics Society Annual Meeting, 2020, 64(1), 1740–1744. [CrossRef]
- Salmon, P.; Williamson, A.; Lenné, M.; Mitsopoulos-Rubens, E.; Rudin-Brown, C. M.Systems-based accident analysis in the led outdoor activity domain: application and evaluation of a risk management framework. 2010, 53(8), 927-939. [CrossRef]
- Carden, T.; Goode, N.; Salomon P.M. Simplifying safety standard: Using work domain analysis to guide regulatory restructure. Safety Science 2021, 138, 105096. [CrossRef]
- Carden, T.; Goode, N.; Read, G.J.M.; Salmon, P.M. Sociotechnical systems as a framework for regulatory system design and evaluation: Using Work Domain Analysis to examine a new regulatory system. [CrossRef]
- Carden, T.; Goode, N.; Salomon, P.M. Not as simply as it look: led outdoor activities are complex sociotechnical systems. Theoretical Issues in Ergonomics Science 2017, 18(4), 318-337. [CrossRef]
- Dallat, C.; Salomon, P.M.; Goode, N. All about the Teacher, the Rain and the Backpack: The Lack of a Systems Approach to Risk Assessment in School Outdoor Education Programs. Procedia Manufacturing 2015, 3, 1157-1164. [CrossRef]
- McLean, E.V.; Whang, T. Do sanctions spell disaster? Economic sanctions, political institutions, and technological safety. European Journal of International Relations 2020, 26(3), 767-792. [CrossRef]
- McLean, S.; Coventon, L.; Finch, C.F.; Dallat, C.; Carden, T.; Salmon, P.M. Evaluation of a systems ergonomics-based incident reporting system. Appl. Ergon. 2022, 100, 103651.
- Goode, N.; Salmon, P.M.; Lenne, M.; Finch, C. Translating Systems Thinking into Practice. A Guide to Developing Incident Reporting Systems. CRC Press 2018, 26, 308.
- Jacobsson, A.; Ek, A.; Akselsson, R. Method for evaluating learning from incidents using the idea of “level of learning”. Journal of Loss Prevention in Process Industries 2011, 24(4), 333-343. [CrossRef]
- Nielsen, K.; Carstensen, O.; Rasmussen, K. The prevention of occupational injuries in two industrial plants using an incident reporting scheme. Journal of Safety Research 2006, 37(5), 479-486. [CrossRef]
- Hutchinson, A.; Young, T. A.; Cooper, K. L.; McIntosh, A.; Karnon, J. D.; Scobie, S.; Thomson, R. G. Trends in healthcare incident reporting and relationship to safety and quality data in acute hospitals: Results from the National Reporting and Learning System. Quality and Safety in Health Care 2009, 18(1), 5. [CrossRef]
- Ferorelli, D.; Solarino, B.; Trotta, S.; Mandarelli, G.; Tattoli, L.; Stefanizzi, P.; Bianchi, F. P.; Tafuri, S.; Zotti, F.; Dell’Erba, A. Incident Reporting System in an Italian University Hospital: A New Tool for Improving Patient Safety. International Journal of Environmental Research and Public Health,2020, 17(17). [CrossRef]
- Jiang, K.; Tian, L.; Yan, C.; Li, Y.; Fang, H.; Peihang, S.; Li, P.; Jia, H.; Wang, Y.; Kang, Z.; Cui, Y.; Liu, H.; Zhao, S.; Anastasia, G.; Jiao, M.; Wu, Q.; Liu, M. A cross-sectional survey on patient safety culture in secondary hospitals of Northeast China. PloS One, 2019, 14(3), e0213055. [CrossRef]
- Plsek, P. E.; Wilson, T. Complexity, leadership, and management in healthcare organisations. BMJ, 2001, 323(7315), 746–749. [CrossRef]
- Yalew, Z. M.; Yitayew, Y. A. Clinical incident reporting behaviors and associated factors among health professionals in Dessie comprehensive specialized hospital, Amhara Region, Ethiopia: A mixed method study. BMC Health Services Research, 2021, 21(1), 1331. [CrossRef]
- Naome, T.; James, M.; Christine, A. et al. Practice, perceived barriers and motivating factors to medical-incident reporting: a cross-section survey of health care providers at Mbarara regional referral hospital, southwestern Uganda. BMC Health Serv Res 2020, 20, 276. [CrossRef]
- Jiang, K., Tian, L., Yan, C., Li, Y., Fang, H., Peihang, S., Li, P., Jia, H., Wang, Y., Kang, Z., Cui, Y., Liu, H., Zhao, S., Anastasia, G., Jiao, M., Wu, Q., & Liu, M. A cross-sectional survey on patient safety culture in secondary hospitals of Northeast China. PloS One, 2019, 14(3), e0213055. [CrossRef]
- Kakemam, E., Hajizadeh, A., Azarmi, M., Zahedi, H., Gholizadeh, M., & Roh, Y. S. Nurses’ perception of teamwork and its relationship with the occurrence and reporting of adverse events: A questionnaire survey in teaching hospitals. Journal of Nursing Management, 2021, 29(5), 1189–1198. [CrossRef]
- Lurvey, L. D.; Fassett, M. J.; & Kanter, M. H. Self-Reported Learning (SRL), a Voluntary Incident Reporting System Experience Within a Large Health Care Organization. Joint Commission Journal on Quality and Patient Safety, 2021, 47(5), 288–295. [CrossRef]
- Grilli, R.; Taroni, F. Governo delle Organizzazioni Sanitarie e qualità della sicurezza. Roma, Il Pensiero Scientifico Editore, 2004.
- Müller, B. S.; Beyer, M.; Blazejewski, T.; Gruber, D.; Müller, H.; Gerlach, F. M. Improving critical incident reporting in primary care through education and involvement. BMJ Open Quality,2019, 8(3), e000556. [CrossRef]
- Chen, L.-C., Wang, L.-H., Redley, B., Hsieh, Y.-H., Chu, T.-L., & Han, C.-Y. A Study on the Reporting Intention of Medical Incidents: A Nursing Perspective. Clinical Nursing Research, 2018, 27(5), 560–578. [CrossRef]
- Tlili, M. A.; Aouicha, W.; Sahli, J.; Zedini, C.; Ben Dhiab, M.; Chelbi, S.; Mtiraoui, A.; Said Latiri; H., Ajmi, T.; Ben Rejeb, M.; Mallouli, M. A baseline assessment of patient safety culture and its associated factors from the perspective of critical care nurses: Results from 10 hospitals. Australian Critical Care: Official Journal of the Confederation of Australian Critical Care Nurses, 2021, 34(4), 363–369. [CrossRef]
- Liukka, M., Hupli, M., & Turunen, H. How transformational leadership appears in action with adverse events? A study for Finnish nurse manager. Journal of Nursing Management, 2018, 26(6), 639–646. [CrossRef]
- Gunkel, C.; Rohe, J.; Heinrich, A.S.; Hahnenkamp, C.; Thomeczek, C. CIRS – Gemeinsames Lernen durch Berichts- und Lernsysteme. In: Herbig N, Poppelreuter S, Thomann H, editors. Qualitätsmanagement im Gesundheitswesen. 31. Aktualisierung. Köln: TÜV Media; 2013. p. 1–46, Anhang. Berlin: ÄZQ; 2013. (äzq Schriftenreihe; 42).
- Yoo, M. S., & Kim, K. J. Exploring the Influence of Nurse Work Environment and Patient Safety Culture on Attitudes Toward Incident Reporting. The Journal of Nursing Administration, 2017, 47(9), 434–440. [CrossRef]
- Pauletti, G., Girotto, C., De Luca, G., & Saieva, A. M. Incident reporting reduction during the COVID-19 pandemic in a tertiary Italian hospital: A retrospective analysis. International Journal for Quality in Health Care: Journal of the International Society for Quality in Health Care, 2022, 34(2), mzab161. [CrossRef]
- McFarland, D. M., & Doucette, J. N. Impact of High-Reliability Education on Adverse Event Reporting by Registered Nurses. Journal of Nursing Care Quality, 2018, 33(3), 285–290. [CrossRef]
- Ramanujam, R.; Goodman, P. S. The challenge of collective learning from event analysis. Safety Science 2011, 49(1), 83–89. [CrossRef]
- Yoo, M. S.; Kim, K. J. Exploring the Influence of Nurse Work Environment and Patient Safety Culture on Attitudes Toward Incident Reporting. The Journal of Nursing Administration, 2017, 47(9), 434–440. [CrossRef]
- Birkeli, G. H.; Jacobsen, H. K.; Ballangrud, R.Nurses’ experience of incident reporting culture before and after implementing the Green Cross method: A quality improvement project. Intensive & Critical Care Nursing, 2022, 69, 103166. [CrossRef]
- Nuckols, T.K.; Bell, D.S.; Liu, H.; Paddock, S.M.; Hilborne, L.H. Rates and types of events reported to establish incident reporting systems in two US hospitals. Qual Saf Health Care. 2007, 16, 164–8. [CrossRef]
- Panzica, M.; Krettek, C.; Cartes, M. Clinical Incident Reporting System als Instrument des Risikomanagements für mehr Patientensicherheit. Unfallchirurg. 2011, 114, 758–67. [CrossRef]
- Heideveld-Chevalking, A.J.; Calsbeek, H.; Damen, J.; Gooszen, H.; Wolff, A.P. The Impact of a standardized incident reporting system in the perioperative setting. A single center experience on 2.563 ‘near-misses’ and adverse events. Patient Saf Surg. 2014, 8(46), 1–10. [CrossRef]
- Cousins, D.H.; Gerrett, D.; Warner, B. A review of medication incidents reported to the National Reporting and Learning System in England and Wales over 6 years (2005–2010). Br J Clin Pharmacol. 2012, 74(4), 597–604. [CrossRef]
- Levtzion-Korach, O.; Frankel, A.; Alcalai, H.; Keohane, C.; Orav, J.; Graydon-Baker, E.; Barnes, J.; Gordon, K, Puopulo AL, Tomov EI, Sato L, Bates DW. Integrating incident data from five reporting systems to assess patient safety: making sense of the elephant. Jt Comm J Qual Patient Saf. 2010, 36(9), 402–10. [CrossRef]
- Steyrer, J.; Schiffinger, M.; Huber, C.; Valentin, A.; Strunk, G. Attitude is everything? The Impact of workload, safety climate, and safety tools on medical errors: a study of intensive care units. Health Care Manag Rev. 2013, 38(4), 306–16. [CrossRef]
- Hoffinger, G.; Horstmann, R.; Waleczek, H. Das Lernen aus Zwischenfällen lernen: Incident Reporting im Krankenhaus, Hochleistungsmanagement. München: Gabler; 2008, 207–24. [CrossRef]
- Benn, J.; Koutantji, M.; Wallace, L.; Spurgeon, P.; Rejman, M.; Healey, A.; Vincent, C. Feedback from incident reporting: information and action to improve patient safety. Qual Saf Health Care. 2009, 18(1), 11–21. [CrossRef]
- Buscemi, A. Il risk management in sanità. Gestione del rischio, errori, responsabilità professionale, aspetti assicurativi e risoluzione stragiudiziale delle controversie. Milano, Franco Angeli, 2017.
- Clanton, J.; Clark, M.; Loggins ,W.; Herron, R. Effective handoff communication. In: Firstenberg MS, Stawicki S, editors. Vignettes in patient safety. London: Inte- chOpen 2018, 2, 25-44. [CrossRef]
- World Health Organization (WHO). World Patient Safety Day. Available from https://www.who.int/campaigns/world-patient-safety-day/2022 (Accessed on July 22, 2023).
- Ministero della Salute. Risk Management in Sanità. Il problema degli errori. Roma, 2003.
Figure 1.
Flowchart of the item selection process.
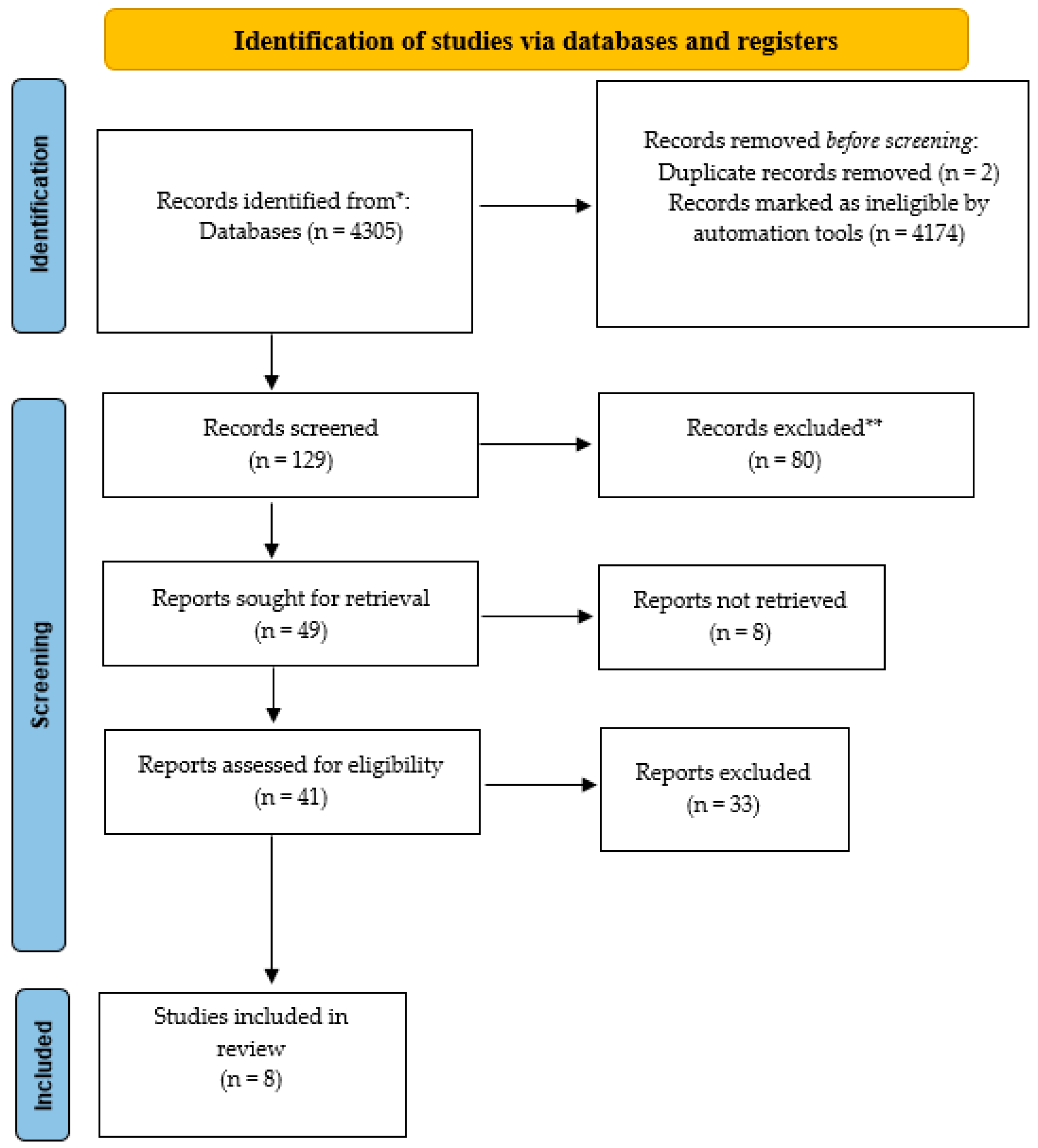
Figure 2.
Increase in monthly reporting rates of adverse events between 2016 and 2017.
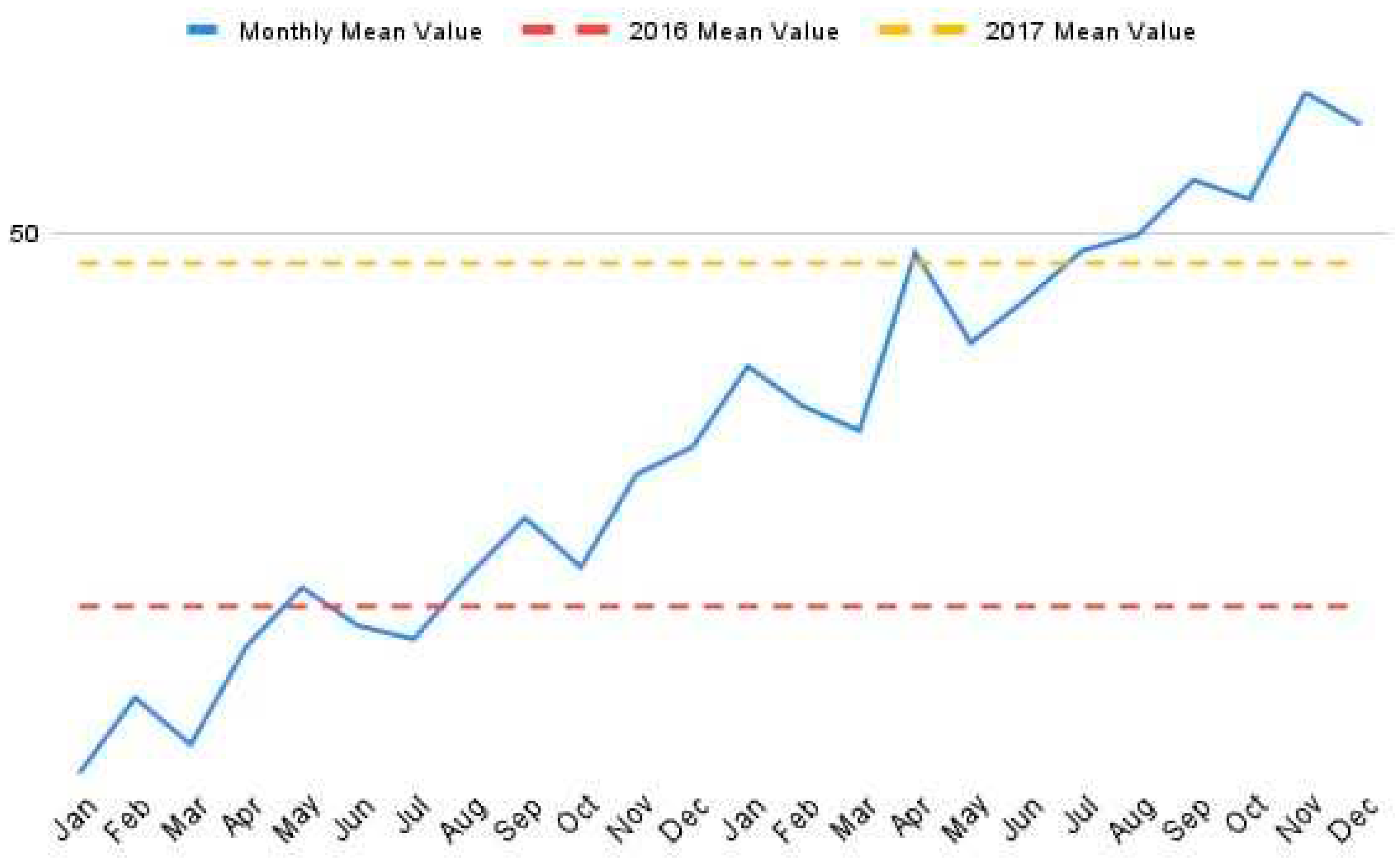
Figure 3.
Implementation of Incident Reporting with the National program.
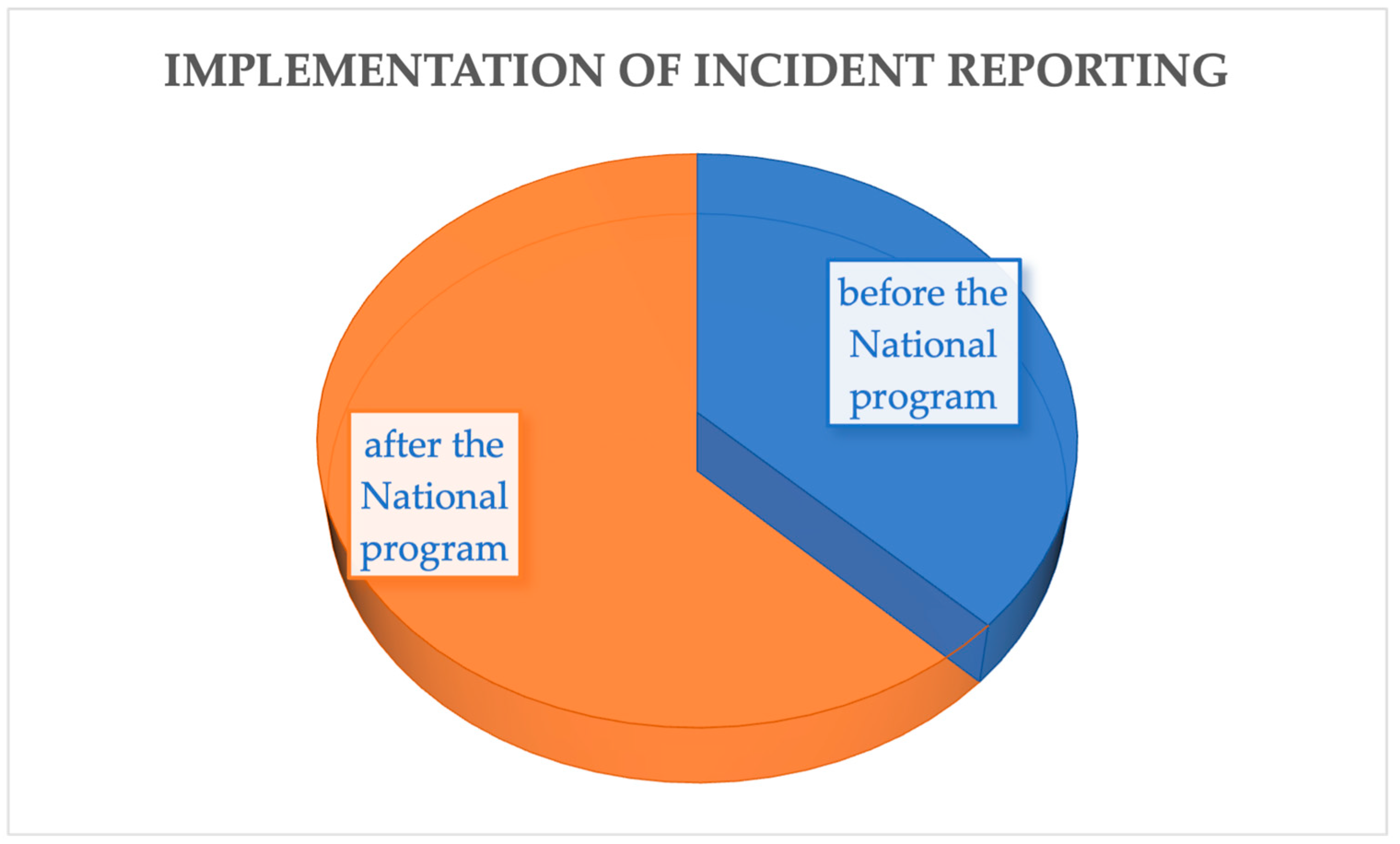

Table 1.
Characteristics of included studies.
| Studies | Location | Type of study | Keyword |
|---|---|---|---|
| Al Lawati, 2019 [31] | Oman | Qualitative study | Low safety culture, lower error reporting |
| Carlfjord, 2018 [32] | Sweden | Qualitative study | Improved safety culture, increased IR use |
| De Kam, 2020 [33] | Netherlands | Mixed method study | Event reporting system (IRS) increased knowledge of patient safety |
| Flott, 2018 [34] | United Kingdom | Case report | Improved event reporting process, developed basis for safety culture |
| Ghasemi, 2022 [35] | Malaysia | Case report | Positive safety culture associated with fewer verified errors |
| Petschnig & Haslinger-Baumann, 2017 [36] | Austria | Qualitative study | Incident reporting takes the form of a quality assessment tool |
| Raeissi, 2018 [37] | Iran | Qualitative study | Perception of safety culture greater than event reporting |
| Verbeek-van Noord, 2019 [38] | Netherlands | Cross-sectional study | Establishment of a national patient safety program, increased number of adverse event reports |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



