
Submitted:
28 July 2023
Posted:
31 July 2023
You are already at the latest version
Abstract
Scrub typhus (ST) is one of the most neglected tropical diseases, a leading cause of acute undifferentiated febrile illness in areas of the ‘tsutsugamushi triangle’, diagnosed frequently in South Asian countries. The bacteria Orientia tsutsugamushi is the causative agent of the disease, which enters to human body through the bite of trombiculid mite (Chigger) of the genus Leptotrombidium deliense.The diagnosis of the disease becomes challenging as its early symptoms mimic other febrile illnesses like dengue, influenza, and corona viruses. Lack of rapid, reliable, and cost-effective diagnostic methods further complicates the identification process. Northeast India, a mountainous region with a predominantly rural tribal population, has witnessed a resurgence of scrub typhus cases in recent years. Various ecological factors, including rodent population, habitat characteristics, and climatic conditions, influence its prevalence. Entomological investigations have confirmed the abundance of vector mites, highlighting the importance of understanding their distribution and the probability of transmission of scrub typhus in the region. Proper diagnosis, awareness campaigns, and behavioral interventions are essential for controlling scrub typhus outbreaks and reducing its impact on public health in Northeast India. Further research and community-based studies are necessary to accurately assess the disease burden and implement effective prevention strategies.
Keywords:
Northeast India
; scrub typhus
; Orientia tsutsugamushi
; clinical presentations
; co-infections
; diagnosis
; genetic diversity
; entomology
1. Background
Scrub typhus is a vector-borne zoonotic disease caused by Orientia tsutsugamushi, an intracellular gram negative bacteria [1]. It belongs to the order Rickettsiales within the family Rickettsiaceae [2] .The disease is transmitted to humans through the bites of infected chiggers, which are small mites of the species Leptotrombidium deliense [3]. Scrub typhus is primarily known to be endemic in the Asia-Pacific region, often referred to as the "tsutsugamushi triangle,”. However, with the passage of time, this disease has spread beyond tsutsugamushi triangle including Chile, Peru, parts of Africa, and the Arabian Peninsula [4,5]. Scrub typhus is considered a neglected tropical disease, and a significant cause of undifferentiated febrile illness [3,6]. It can be life-threatening if left untreated. It is estimated that scrub typhus intimidates more than one million infected people per year by causing substantial mortality all over the world [6].
The World Health Organization (WHO) recognizes scrub typhus as an important rickettsial infection and considers it as one of the most underreported diseases that often requires hospitalization [7]. Scrub typhus is prevalent in tropical areas throughout the year favoring the growth and reproduction of mites, while in temperate regions, the disease can occurs seasonally [8].
In the early phase, the symptoms of scrub typhus resembles those of other infections like dengue, encephalitis, influenza, and corona viruses, leading to acute febrile illness [9]. After 5-14 days of bites by an infected mite, the patient starts to exhibit an appearance of non-specific flu-like symptoms such as fever, headache, cough, myalgia, nausea, vomiting, abdominal pain, and lymphadenopathy. If not treated on time this can lead to severe complications that event in multi-organ failure including jaundice, acute renal failure, pneumonitis, acute respiratory distress syndrome (ARDS), meningoencephalitis, and disseminated intravascular coagulation. The bacteria primarily target the lungs, leading to varying degrees of pulmonary complications [10].
Eschar is a key clinical presentation of scrub typhus, a necrotic lesion on skin [11], although its absence does not rule out the infection. Laboratory-based diagnosis of scrub typhus relies on various serological assays, including the Weil-Felix test (WFT), indirect immunofluorescence assays (IFA), immunochromatographic tests (ICT), and enzyme-linked immunosorbent assay (ELISA). Although indirect IFA are considered the gold standard for diagnosing scrub typhus, they require high technical expertise. As an alternative, the IgM ELISA-based method is considered the most reliable for the diagnosis of scrub typhus [12]. ICT are particularly valuable as rapid and early diagnostic tools, especially in resource-limited areas where immediate diagnosis is essential for timely treatment [9].
A higher prevalence of this disease has been observed in rural areas of Southeast Asian countries, particularly among individuals who engage in occupational or recreational activities that expose them to mite-infested environments, such as brush and grasslands [13,14,15]. However, there has been a recent spread of scrub typhus in urban areas [16,17]. The mortality rate can vary as high as 30% or more among untreated individuals [3,9]. Imported cases of scrub typhus have also been identified in some travelers returning from the Tsutsugamushi triangle [18,19].
This disease scrub typhus was a major epidemic during the Second World War in Assam and West Bengal and in 1965 Indo-Pak war in the Jammu - Sialkot sectors among the militants [20]. After decades of rare occurrence, the re-emergence of the disease has been reported in different states of India including Tamil Nadu, Kerala, Maharashtra, Rajasthan, Himachal Pradesh, West Bengal, and in the entire North Eastern states [8].This article highlight the prevalence of scrub typhus in Northeast region and addresses the existing gaps in diagnosis and management. We also described the clinical features, laboratory investigations, risk factors, entomological investigations and treatment outcome during the studies.
2. Search Methodology
A literature search was conducted on studies documenting scrub typhus in Northeast India. All papers published between the years 2010 to 2022 from PubMed, Scopus, and Google Scholar (including non-indexed papers) were retrieved using the following search terms: ‘Scrub’, or ‘Orientia tsutsugamushi’, and ‘AND Northeast India‘. A second search included ‘Scrub typhus’ used with ‘AND’ and either ‘Mizoram’, ‘Arunachal Pradesh’, ‘Meghalaya’, ‘Nagaland’, ‘Sikkim’, ‘Assam’, ‘Tripura’, or ‘Manipur’. All the available information on the occurrence of scrub typhus in Northeast India, including exposure histories, case reports, antibiotics administered, age, sex, address, diagnosis, and laboratory test, were included. We also included the entomological investigations conducted as well as risk factors associated with the disease. Additionally, review articles were excluded to avoid duplication.
3. Geography of North-East India
Northeast India located at the easternmost part of the country, is characterized by its predominantly rural tribal population, comprising 82% of the total population whose livelihoods rely on agriculture and forest-based activities [21,22]. About two-thirds of this region is occupied by hilly and mountainous terrain ranging from 50 meters (Brahmaputra valley) to 7000 meters (Himalayan borderland) above sea level [23]. It comprises eight states and spans an area of approximately 0.26 million square kilometers. It is situated between 22°N and 29°5'N latitude and 88°E and 97°30'E longitude, sharing international borders with Bhutan (north), Tibet (north), Myanmar (east), and Bangladesh (south) (Figure 1) [24]. The forest covers around 14.2 million hectares with an approximate of 54.16% to 60% of the total geographical area [22]. Northeast India experiences a humid subtropical climate. During winter the average temperature is 16 °C and rises to approximate 30 °C during summer [25].The temperatures in the region, as anywhere else, may vary with height. No part in the Northeast receives a rainfall of less than 1,200 mm [25]. This region serves as a vital gateway to Southeast Asian countries, facilitating trade and cultural exchange.
4. Scrub Typhus in Northeast India
The Northeast India region falls within the Southeast Asia rice domain and is known for its unique practice of 'slash and burn' shifting cultivation, locally referred to as ‘jhuming’ [26]. This traditional method involves clearing the jungles, creating an environment conducive to the growth of scrub vegetation. Consequently, the region becomes an ideal habitat for the mites that are responsible for transmitting scrub typhus [10]. Northeast India is also renowned for its abundant biodiversity [26], with lush vegetation providing a suitable environment for the presence of these mites [27]. The Northeast Indian states bordering Myanmar are strategically important as they can serve as a conduit for vector-prone diseases.
In Southeast Asian countries, febrile illnesses contribute significantly to morbidity and mortality [28]. Among these, Rickettsial infections stand out as the most identifiable cause of febrile illness in the region. Prevalence rates of O. tsutsugamushi, Rickettsia typhi, and some members of Spotted fever group rickettsiae (SFGR) range from 7% to 90% of overall rickettsial infections [29]. The sub-tropical climate of Northeast India accounts for most of acute febrile illnesses such as malaria, scrub typhus, leptospirosis, chikungunya, and dengue. There has been a report of mixed infections, overlapping cases, or co-infections among febrile illnesses in India including the Northeast region [30,31]. There is widespread prevalence of rickettsial infections in the Northeast region [32]. In addition, Japanese encephalitis virus (JEV) infection, West Nile virus (WNV) infection, scrub typhus infection and leptospirosis have been identified as key contributors to acute encephalitis syndrome (AES) in the Northeastern region of India [33].
Scrub typhus, an acute febrile illness has been recognized and referred to by different names in various regions of Asia throughout history [34]. In Northeast India, the local population has long been aware of this disease and has specific names for it in different areas. In the Meghalaya region, it is referred to as "Niangsohot," which signifies an organism associated with chestnut [35]. In Manipur, it is called "Khullai-laipha” [36]. In Mizoram, there is a possible association between the disease and the flowering of bamboo, which leads to an increase in the rodent population that feeds on the nutritious bamboo fruits and flowers [37]. In the Noklak district area of Nagaland, the disease is locally known as "Hokia" meaning disease of legs. According to local people of Noklak region, the disease appears to be associated with the neighbouring region of Myanmar due to the porous border (unpublished record). It is speculated that the pathogen responsible for scrub typhus, O. tsutsugamushi, may be transported within the state through migrating rodents from various potential sources outside the state [38]. These local associations and names reflect the regional prevalence of scrub typhus in Northeast India.
The first cases of scrub typhus in Northeast India were documented along the Indo (Assam now Manipur)-Burma border during Second World War (1943-1945) [39], following which 91 cases of scrub typhus were reported among troops during the period 1965-69 [40]. Since 2001, there have been outbreaks of febrile illnesses accompanied by eschar formation reported in various parts of Northeast India [36,37,41,42], marking a resurgence after decades. Despite this, specific data regarding the occurrence of scrub typhus in many of Northeast states is still lacking. In 2004, a clinically positive scrub typhus from Sikkim was reported, which might likely be the first clinical report from Northeast India after its initial documentation [41]. Subsequently, the first outbreak in Manipur was reported in 2007 by Singh et al. [36]. Resurgence of scrub typhus was also reported in Assam, Arunachal Pradesh, and Nagaland states during 2010-2011 [43]. Since then, scrub typhus cases have been reported, indicating the continued presence of the disease in the region.
In 2020, during the COVID-19 pandemic, over 600 cases of scrub typhus were confirmed in the Noklak district of Nagaland, which borders Myanmar. Unfortunately, five people succumbed to the disease out of a total population of 24,189 (according to the 2021 Aadhar estimates). In 2022, local reports revealed that three individuals, including a three-year-old girl and an eight-year-old boy, died from scrub typhus infection, while approximately 20 people were under medical care in Manipur's Kangpokpi district [44,45]. Numerous similar outbreaks have been reported by K. Lalchhandama in different district of Mizoram [46].
Various ecological factors have the potential to influence the risk of scrub typhus such as the abundance and diversity of vector species, infection rates of Orientia chigger, the presence of small mammals, habitat characteristics including the presence of invasive plants, geographic latitude, seasonality, climate conditions, alterations in land use, as well as specific occupations and human behaviors [47,48].
4.1. Descriptive Epidemiology:
The epidemiology of scrub typhus varies geographically based on different climatic conditions, the presence of diverse etiological agents, vectors involved in transmission, various human behaviors and the susceptibility of population [49,50]. We identified 45 published papers including case reports of scrub typhus conducted between 2010- 2022 [Table 1 and Table 2]. A total of 3697 clinically diagnosed and laboratory confirmed cases of scrub typhus were reported in Northeast region (2010–2022), among whom 88 patients died. The overall case fatality was 2.4%.
The majority of patients presented with clinically suspected cases of scrub typhus, exhibiting symptoms such as prolonged fever and acute undifferentiated febrile illness. An outbreak of scrub typhus-like illness with eschar has been reported in the Northeast India since 2001 following the initial report of the disease in 1945 [36,39]. This review includes various types of studies conducted on patients attending healthcare facilities, comprising a retrospective study, a cross-sectional study, and a study carried out in a community setting. Meghalaya accounted for majority of the reported cases. The highest numbers of cases were reported during the months of July to November (monsoon or post monsoon)/autumn [Table 1]. The majority of cases and suspected cases were identified among farmers and rural inhabitants.
4.2. Age and Gender Cases
The majority of confirmed scrub typhus cases in the laboratory were among adults, with significantly higher seropositivity observed in males compared to females. This gender difference may be attributed to males engaging in more outdoor activities than females. However in some studies, positivity for scrub typhus was significantly higher among female [51,52]. In the outbreak that took place in Meghalaya, the affected individuals were primarily children, with an average age of nine years [53]. It reported a higher percentage of children being infected with scrub typhus compared to the adult population [53]. Lurshay et al. reported a higher incidence of meningoencephalitis among pediatrics patients [54]. Eschar was also observed among pediatric patients. In Mizoram, five positive cases were recorded in patients under the age of one year, unfortunately resulting in the death of a two-month-old male [55]. In addition several studies have also reported cases of scrub typhus among pediatric patients [35,41,52,55,56]. The occurrence of scrub typhus among pediatric patients could be attributed to activities like playing outdoors or being taken to fields by parents during fieldwork. It also indicates the presence of a high population of mites in an area contributing to the transmission of scrub typhus not only to adults but also to pediatric.
4.3. Diagnostic Conformation
The study's findings suggest that young adults exposed to scrub vegetation account for the majority of laboratory-confirmed cases of scrub typhus in Northeast-India. The analysis included studies that employed serological or molecular methods to confirm scrub typhus cases (excluding case report). A significant number of studies relied on ELISA (56%), an accurate and easily accessible diagnostic test, as the confirmatory measure. In a recent study comparing molecular and serologic tests for scrub typhus diagnosis, ELISA demonstrated a sensitivity of 94.2% and a specificity of 93.6%, which makes it more reliable test [57]. Additionally, ELISA is a more cost-effective alternative to polymerase chain reaction (PCR). PCR was used in combination with the WFT or ELISA to confirm 22% (7/32) of the studies (n=2 and n=6, respectively). Approximately 40% (13/32) of the studies relied on the ICT, known for its low sensitivity.
4.4. Clinical Presentations
In all the studies, fever/pyrexia was the most prevalent clinical manifestation observed among the case patients, followed by headache ranging from 25% to 100% [54,58]. The various clinical manifestations are listed in Figure 2. While the presence of an eschar is a valuable clinical clue for diagnosing scrub typhus, its absence does not rule out the possibility of the disease. According to Yoo et al., the overall prevalence rate of eschars was 58.0%, with the highest prevalence in East Asia (78.7%), followed by Oceania (52.2%), Southeast Asia (41.4%), and the lowest in South Asia (32.8%) [59]. In this review, the occurrence of eschars among the studied population ranged from 7% to 41.7% [52,53], which is similar to other states in India, where the range is between 9.5% and 55% [60,61]. Some studies did not identify any eschars in their cases. This may be attributed to unawareness of the disease in rural areas. In endemic areas, it is common for Indigenous patients to have less severe illness, often with or without rash and eschar [62].
Other clinical features observed included: nausea or vomiting (15.8% to 61.29%) [41,63], splenomegaly (5% to 45.8%) [53,64], hepatomegaly (11.1% to 41%) [34,43], lymphadenopathy (8% to 52.54%) [35,64], acute kidney injury/acute renal failure (AKI/ARF) (5% to 44.4%) [43,64], abdominal pain (13.7% to 41.6%) [58,63], myalgia (2.8% to 100%) [58,65], pneumonia (7.5% to 45.5%) [64,65], altered sensorium (5% to 56.9%) [64,66],thrombocytopenia (1.5% to 63.6%) [41,68], acute respiratory distress syndrome (ARDS) (4% to 16.6%) [54,58], multiple organ dysfunction (MOD) (14.4% to 42.6%) [54,68], meningoencephalitis (5.5% to 58.6%) [54,68], hepatitis (15.25% to 91.6%) [35,58], breathing/tachypnea (15.5% to 83.3%) [58,68],cough (23.3% to 91.6%) [58,68], rash (1.69% to 28%) [52,54], diarrhea (1.5% to 16%) [41,54], shock (2.2% to 16.6%) [58,68], icterus/jaundice (3% to 22.7%) [54,65], seizures (1.5% to 12.5%) [41,53], conjunctival redness (8.3% to 44%) [53,54], arthralgia (2.8% to 22%) [41,65], anuria/oliguria (9% to 10.17%) [35,52]. Less common manifestations included: haemoptysis (33.3%) [58], edema (25.3%) [41], epistaxis (1.69%) [35], and status epilepticus (0.5%) [65].
A publication from South India reported scrub typhus meningitis as a common central nervous system (CNS) complication. In this review, two papers presented the clinical profiles of patients with scrub typhus meningoencephalitis [69,70], where patients exhibited neurological manifestations as the main presenting feature. Various neurological manifestations include headache, meningitis, neck rigidity, seizures, and neurological deficits.
A retrospective study conducted by Khan et al. in 2017 reported O. tsutsugamushi infection as a leading cause of AES with a mortality rate of 49% [33].
4.5. Co-Infection
In tropical countries, co-infections commonly occur alongside scrub typhus infection due to the similarity in clinical features. Failing to receive treatment on time for co-infections can result in life-threatening situations [81]. A study conducted in various Indian states including Assam, Meghalaya, and Arunachal Pradesh revealed the occurrence of scrub typhus co-infections along with other febrile illnesses such as leptospirosis, dengue, chikungunya, bacteraemia, pulmonary tuberculosis, and malaria [31,35,52,68,82]. High prevalence of co-infections of about 35% between scrub typhus and malaria was observed in Thailand and low prevalence in India exclusively, according to the recent review report [83].
Scrub typhus and leptospirosis might share similar transmission routes when rodent animals are significant [84]. Borkakoty et al. observed that 25% of scrub typhus cases in Arunachal, Northeast India, had co-infection with leptospira [52]. A report however suggests that the elevated rate of co-infection could be due to cross-reactivity and the presence of background positivity in patients residing in endemic areas, rather than true co-infection [31]. Therefore, it is advisable to interpret the outcomes of a single serological test for diagnosing scrub typhus with caution.
4.6. Genetic Diversity
An extensive genetic variation has been observed across different geographical area with over 20 antigenically distinct strains including three prototypic strains—Karp, Gilliam, and Kato. In this review, we identified the circulating genotypes of O. tsutsugamushi in five different studies from Northeast India [32,33,66.73,79]. Sequences analyzed from different Northeastern states showed the presence of Karp, Kato, and Gilliam-like strains similar to those found in Southeast Asian countries [32,73,79]. Neimeng-65 strains were also reported in Shillong, Meghalaya [79]. Two studies revealed the presence of the TA763 genotype, also known as the Fan strain, which is endemic in Thailand and Taiwan [66,73].
4.7. Treatment and Outcomes
The majority of studies have documented the use of doxycycline (including pediatric cases) [85] and azithromycin as treatment option for patients with scrub typhus with better outcome. However, it is worth noting that in earlier times, traditional healers were often sought for treating illnesses that exhibited similarities to scrub typhus in some Northeast states [36,37].
Dass et al. reported the use of intravenous chloramphenicol in pediatric patients with complications such as meningoencephalitis, septic shock, or myocarditis, and azithromycin in 3 cases (12.5%) of patients below 8 years of age [53]. Furthermore, three studies have specifically reported the administration of azithromycin for the treatment of pregnant women with scrub typhus [35,41,68].
These findings highlight the commonly used antibiotics, such as doxycycline and azithromycin, for the treatment of scrub typhus, including in pediatric and pregnant populations.
4.8. Entomological Investigations
Entomological investigations were conducted in four studies (Table 3), involving the trapping of rodents in domestic and predomestic areas. Standard procedures were followed to collect and identify ectoparasites found on these rodents. Leptotrombidium deliense, known as the main vector of scrub typhus (tsutsugamushi disease) in various parts of the world [86], was abundant in three of the studies [32,87,88]. Among the trapped rodents, the infestation of vector mites was found to be the highest [87,88].
In Meghalaya and Mizoram, the chigger index exceeded the critical index of 0.69 per rodent, with values of 1.80 and 12.33 respectively. Similarly, the chigger infestation rate in Meghalaya and Mizoram were recorded as 4.8 and 18.5 respectively [87,88].
In one of the recent study conducted by Pautu et al. chigger index was 12.33 which was 27 times higher than the critical value [52].Among the two studies conducted for serological test in rodent sample; one study yielded positive results for scrub typhus pathogens [32], while the other study exhibited reactivity to one or all of PROGEN OXK, OX19, or OX2, indicating the presence of scrub typhus along with other rickettsial diseases [52].
5. Discussion
This review article highlights the continued presence of scrub typhus in the Northeast India over the past few decades. However, due to limited literatures available, the actual scenario of cases might be hidden since years. In this region scrub typhus cases are commonly reported in rural areas, as such this review attempts to highlight the scarcity of studies, underscoring the neglect of scrub typhus as a disease in terms of research and policy framing. In the course of time, different seroprevalence studies were carried out, revealing the vast variance in the prevalence rate, ranging from 0.76% to 40.3% [56,74]. This finding might be suggestive of geographical restrictions of the disease, based on varied factors.
Latest epidemiological review of scrub typhus in India reported the highest proportion of cases from South India (55.5%), while the Northeast region had the second lowest proportion (7.4%) [89].This discrepancy may be partly attributed to differences in disease awareness and the availability of diagnostic facilities. Despite scrub typhus primarily affecting rural regions, most of the studies were conducted in semi-urban or urban settings, indicating an uneven distribution of healthcare facilities and research sites, highlighting limited healthcare access for rural patients.
Scrub typhus presents diagnostic challenges, as it closely resembles other febrile illnesses such as dengue, typhoid fever, leptospirosis, murine typhus and corona virus [8,90].The presence of an eschar in patients can aid in the clinical diagnosis of scrub typhus with higher specificity, but it often goes unnoticed as it is non-itching, painless, and typically present in areas like the perineum, groin, and axilla [91]. Available studies reported the prevalence of eschar and rash ranging from 7% to 28.8% and 1.69% to 28%, respectively. The most commonly reported clinical presentations during the review included fever, followed by headache, vomiting/nausea, myalgia, cough, and breathing difficulty. Respiratory tract involvement is a frequent manifestation of scrub typhus, and clinicians need to differentiate it from community-acquired pneumonia caused by usual organisms like Streptococcus species [92]. Common complications associated with scrub typhus include acute kidney injury, hepatitis, acute respiratory distress syndrome (ARDS), meningoencephalitis, myocarditis, and septic shock.
Confirming suspected cases through appropriate laboratory tests is crucial for documenting scrub typhus infection. While the IgM-based IFA is considered the gold standard for diagnosis [93], a recent review article reported higher sensitivity and specificity for IgG and IgM ELISA compared to the IFA method [57]. In most of the studies, confirmation was primarily done using IgM ELISA, followed by ICT and WFT. Weil–Felix test has very less specificity and sensitivity due to the use of non-rickettsial antigen for agglutination. Despite its drawbacks, it is widely used in rural areas for screening scrub typhus. Further confirmation is required so as to avoid negative result during diagnosis. The use of diagnostic kits such as ICT reflects the limited resources in hospitals, as ELISA readers are not readily available in most remote care centers. Lalrinkima et al. reported a low prevalence of 6.9% using ICT [72,110,111], contrasting with Ki-Deok Lee et al. who reported higher sensitivity rates of 66.7% and 72.6% for SD Bioline ICT in Thailand and the Korean population, respectively [94].The low sensitivity of ICT kits could be attributed to the O. tsutsugamushi antigens used in their preparation. Therefore, ICT test should be followed by confirmatory tests to ensure accuracy. Relying solely on the ICT test may lead to potential false-positive or false-negative results. The time of blood sample collection also plays a significant role in determining seropositivity in scrub typhus patients. Other studies using ICT also demonstrated low sensitivity at the time of admission but showed a gradual increase in positivity over time [95,96]. Additionally, the presence of IgG antibodies in kits may lead to false positives for scrub typhus, as the patient may have had a secondary infection. Therefore, caution should be exercised when interpreting ICT results. Understanding the circulating genotype in a specific geographical area is also crucial for the development of region-specific diagnostic kits.
Although the Indian Council of Medical Research (ICMR) recommends ELISA techniques, particularly immunoglobulin M (IgM) for scrub typhus diagnosis, ICT has been found to be useful in most remote hospital settings [97,98]. Nevertheless, the findings of this review shed light on certain issues regarding the epidemiology and control of scrub typhus in India. Conducting larger studies to compare ICT results with confirmatory tests would be of tremendous value in resource-poor settings for presumptive diagnosis and management of scrub typhus.
6. Conclusions and Future Prospect
In conclusion, our review highlights the distribution of scrub typhus diseases in several parts of Northeast India, mainly hospital-based studies and only 4 community-based studies. In the majority of the papers, we observed a lack of uniform case definition, analytical studies, confirmatory laboratory tests, and entomological surveys. Most studies lacked information on the total number of participants, population patterns, and distribution, making it difficult to obtain precise epidemiological information. Thus, the actual cases of scrub typhus are likely to be substantially higher than what has been reported and summarized in this study, suggesting that our findings represent only the tip of the iceberg.
Further exploration is needed to understand the role of different vector mites and their distribution in an area. It is also crucial to examine seasonal variations of mite’s activity and their correlation with case incidence and distribution in affected areas. More research is required to assess the seroprevalence of this disease in domestic and pre-domestic areas in Northeast India, as it can provide valuable epidemiological insights.
Hospital-based studies may not accurately reflect the prevalence of scrub typhus in the community, it is important to conduct additional studies that focus on wider seroprevalence in the community and well-planned prospective evaluations of patients presenting with acute undifferentiated febrile illness (AUFI) across different states. This will enable us to understand the exact burden of the disease and implement appropriate control and prevention measures. Many studies did not provide information on the clinical presentation of the disease. As a result, the comprehensive details regarding the clinical presentation of scrub typhus may be limited in the context of this review.
It is also essential to raise awareness among doctors practicing in high-risk areas, to evaluate patients with acute febrile illness carefully. Scrub typhus is prevalence primarily among the villagers where there is the lack of adequate healthcare facilities. Health promotion programs on behavioral interventions should be prioritize, such as avoiding urination or defecation in jungle or bushy areas, protective clothing outdoors, regular bathing after field work, and using mats when lying on the floor. Implementing good sanitation practices in and around the house can effectively reduce the rodent population in the vicinity. Educating the community about the common symptoms of the disease by displaying the poster in a local dialogue, awareness campaigns and encouraging the villagers to seek early treatment from nearby health settings are vital strategies for controlling outbreaks thus reducing mortality rates.
Author Contributions
Conceptualization, M.B. and S.K.; methodology, M.B., S.K. and S.G.; data curation, S.K., M.B., S.G., K.B. and J.K.; writing—original draft preparation, S.G., S.K., J.K. and K.B.; writing—review and editing, M.B. and S.K.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing not applicable. No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Trent, B.; Fisher, J.; Soong, L. Scrub Typhus Pathogenesis: Innate Immune Response and Lung Injury During Orientia tsutsugamushi Infection. Front. Microbiol. 2019, 10, 2065. [CrossRef]
- Santos, H.A.; Massard, C.L. The Family Rickettsiaceae. In The Prokaryotes: Alphaproteobacteria and Betaproteobacteria; Rosenberg, E., DeLong, E.F., Lory, S., Stackebrandt, E., Thompson, F., Eds.; Springer: Berlin, Heidelberg, 2014; pp. 619–635 ISBN 978-3-642-30197-1.
- Bonell, A.; Lubell, Y.; Newton, P. N.; Crump, J. A.; Paris, D. H. Estimating the burden of scrub typhus: A systematic review. PLoS Neglected Trop. Dis. 2017, 11, e0005838. [CrossRef]
- Walker; David H. Scrub Typhus - Scientific Neglect, Ever-Widening Impact. New Engl. J. Med. 2016, 375, 913–15. https://pubmed.ncbi.nlm.nih.gov/27602663/.
- Jiang, J.; Richards, A.L. Scrub Typhus: No Longer Restricted to the Tsutsugamushi Triangle. Trop. Med. Infect. Dis. 2018, 3, 11. https://doi.org/10.3390/tropicalmed3010011. [CrossRef]
- Paris, D.H.; Shelite, T.R.; Day, N.P.; Walker, D.H. Unresolved Problems Related to Scrub Typhus: A Seriously Neglected Life-Threatening Disease. Am. J. Trop. Med. Hyg. 2013, 89, 301–307. https://doi.org/10.4269/ajtmh.13-0064. [CrossRef]
- World Health Organization. WHO Recommended Surveillance Standards; World Health Organization: Geneva, Switzerland, 1999.
- Chakraborty, S.; Sarma, N. Scrub typhus: an emerging threat. Indian. J. Dermatol. 2017, 62 478–485.
- Saraswati, K.; Day, N. P. J.; Mukaka, M.; Blacksell, S. D. Scrub typhus point-of-care testing: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2018, 12. https://doi.org/10.1371/journal.pntd.0006330. [CrossRef]
- Xu, G.; Walker, D.H.; Jupiter, D.; Melby, P.C.; Arcari, C.M. A Review of the Global Epidemiology of Scrub Typhus. PLoS Negl. Trop. Dis. 2017, 11, e0006062. https://doi.org/10.1371/journal.pntd.0006062. [CrossRef]
- Biswal, M.; Zaman, K.; Suri, V.; Rao, H.; Kumar, A.; Kapur, G.; Sharma, N.; Bhalla, A.; Jayashree, M. Use of Eschar for the Molecular Diagnosis and Genotypic Characterisation of Orientia Tsutsugamushi Causing Scrub Typhus. Indian. J. Med. Microbiol. 2018, 36, 422–425. https://doi.org/10.4103/ijmm.IJMM_18_8. [CrossRef]
- Phetsouvanh, R.; Thojaikong, T.; Phoumin, P.; Sibounheuang, B.; Phommasone, K.; Chansamouth, V.; Lee, S.J.; Newton, P.N.; Blacksell, S.D. Inter- and Intra-Operator Variability in the Reading of Indirect Immunofluorescence Assays for the Serological Diagnosis of Scrub Typhus and Murine Typhus. Am. J. Trop. Med. Hyg. 2013, 88, 932–936. https://doi.org/10.4269/ajtmh.12-0325. [CrossRef]
- Nadjm, B.; Thuy , P.T.; Trang, V.D.; Ha, L.D.; Kinh, N.V.; Wertheim, H.F. Scrub typhus in the northern provinces of Vietnam: An observational study of admissions to a national referral hospital. Trans. R. Soc. Trop. Med. Hyg, 2014, 108, 739–40. https://doi.org/10.1093/trstmh/tru145. [CrossRef]
- Tran, H.T.D.; Hattendorf, J.; Do, H.M.; Hoang, T.T.; Hoang, H.T.H; Lam, H.N.; Huynh, M.K.; Vu, L.T.H.; Zinsstag, J.; Paris, D.H.; Schelling, E. Ecological and behavioural risk factors of scrub typhus in central Vietnam: a case-control study. Infect. Dis. Poverty 2021, 10, 1–14. https://doi.org/10.1186/s40249-021-00893-6. [CrossRef]
- Wangrangsimakul, T.; Elliott, I.; Nedsuwan, S.; Kumlert, R.; Hinjoy, S.; Chaisiri, K.; Day, N.P.J.; Morand, S. The Estimated Burden of Scrub Typhus in Thailand from National Surveillance Data (2003-2018). PLoS Negl. Trop. Dis. 2020, 14, e0008233. https://doi.org/10.1371/journal.pntd.0008233. [CrossRef]
- Roberts, T.; Parker, D.M.; Bulterys, P.L.; Rattanavong, S.; Elliott, I.; Phommasone, K.; Mayxay, M.; Chansamouth, V.; Robinson, M.T.; Blacksell, S.D.; et al. A Spatio-Temporal Analysis of Scrub Typhus and Murine Typhus in Laos; Implications from Changing Landscapes and Climate. PLoS Negl. Trop. Dis. 2021, 15, e0009685. https://doi.org/10.1371/journal.pntd.0009685. [CrossRef]
- Trung, N.V.; Hoi, L.T.; Thuong, N.T.H.; Toan, T.K.; Huong, T.T.K.; Hoa, T.M.; Fox, A.; Kinh, N. van; van Doorn, H.R.; Wertheim, H.F.L.; et al. Seroprevalence of Scrub Typhus, Typhus, and Spotted Fever Among Rural and Urban Populations of Northern Vietnam. Am. J. Trop. Med. Hyg. 2017, 96, 1084–1087. https://doi.org/10.4269/ajtmh.16-0399. [CrossRef]
- Le Viet, N.; Laroche, M.; Thi Pham, H.L.; Viet, N.L.; Mediannikov, O.; Raoult, D.; Parola, P. Use of Eschar Swabbing for the Molecular Diagnosis and Genotyping of Orientia Tsutsugamushi Causing Scrub Typhus in Quang Nam Province, Vietnam. PLoS Negl. Trop. Dis. 2017, 11, e0005397. https://doi.org/10.1371/journal.pntd.0005397. [CrossRef]
- Costa, C.; Ferrari, A.; Binazzi, R.; Beltrame, A.; Tacconi, D.; Moro, L.; Edouard, S.; Parola, P.; Buonfrate, D.; Gobbi, F. Imported Scrub Typhus in Europe: Report of Three Cases and a Literature Review. Travel. Med. Infect. Dis. 2021, 42, 102062. https://doi.org/10.1016/j.tmaid.2021.102062. [CrossRef]
- Singh, P. Scrub typhus, a case report: Military and regional significance. Med. J. Armed Forces India 2004, 60, 89–90. [CrossRef]
- Northeast India. Available online: https://en.wikipedia.org/wiki/Northeast_India (accessed on 28 July 2023).
- Ravindranath, N.H.; Rao, S.; Sharma, N.; Nair, M.; Gopalakrishnan, R.; Rao, A.S.; Malaviya, S.; Tiwari, R.; Sagadevan, A.; Munsi, M.; et al. Climate Change Vulnerability Profiles for North East India. Curr. Sci. 2011, 101.
- Dikshit, K.R.; Dikshit, J.K. Relief Features of North-East India. In North-East India: Land, People and Economy, Dikshit, K.R.; Dikshit, J.K. Eds. Springer Netherlands: Dordrecht, 2014; pp. 91–125.
- Chakravarty, S.; Suresh, C.P.; Puri, A.; Shukla, G. North-East India, the Geographical Gateway of India. Indian. For. 2012, 138, 702–709.
- Dikshit, K.R.; Dikshit, J.K. Weather and Climate of North-East India. In North-East India: Land, People and Economy, Springer Netherlands: Dordrecht, 2014; pp. 149–173.
- Dikshit, K.R.; Dikshit, J.K. Agriculture in North-East India: Past and Present. In: North-East India: Land, People and Economy. Advances in Asian Human-Environmental Research. Springer, Dordrecht. 2013, pp 587–637 https://doi.org/10.1007/978-94-007-7055-3_16. [CrossRef]
- Richards, A.L.; Jiang, J. Scrub Typhus: Historic Perspective and Current Status of the Worldwide Presence of Orientia Species. Trop. Med. Infect. Dis. 2020, 5, 49. https://doi.org/10.3390/tropicalmed5020049. [CrossRef]
- Chandna, A.; Chew, R.; Shwe Nwe Htun, N.; Peto, T. J.; Zhang, M.; Liverani, M.; Brummaier, T.; Phommasone, K.; Perrone, C.; Pyae Phyo, A.; Sattabongkot, J.; Roobsoong, W.; Nguitragool, W.; Sen, A.; Ibna Zaman, S.; Sandar Zaw, A.; Batty, E.; Waithira, N.; Abdad, M. Y.; Blacksell, S. D.; Lubell, Y. Defining the burden of febrile illness in rural South and Southeast Asia: an open letter to announce the launch of the Rural Febrile Illness project. Wellcome Open Res. 2022, 6, 64. [CrossRef]
- Aung, A.K.; Spelman, D.W.; Murray, R.J.; Graves, S. Rickettsial Infections in Southeast Asia: Implications for Local Populace and Febrile Returned Travelers. Am. J. Trop. Med. Hyg. 2014, 91, 451–460. https://doi.org/10.4269/ajtmh.14-0191. [CrossRef]
- Mittal, G.; Ahmad, S.; Agarwal, R.K.; Dhar, M.; Mittal, M.; Sharma, S. Aetiologies of Acute Undifferentiated Febrile Illness in Adult Patients – an Experience from a Tertiary Care Hospital in Northern India. J. Clin. Diagn. Res. 2015, 9, DC22–DC24. https://doi.org/10.7860/JCDR/2015/11168.6990. [CrossRef]
- Mørch, K.; Manoharan, A.; Chandy, S.; Chacko, N.; Alvarez-Uria, G.; Patil, S.; Henry, A.; Nesaraj, J.; Kuriakose, C.; Singh, A.; Kurian, S.; Haanshuus, C.G.;, Langeland, N.; Blomberg, B.; Antony, G.V.; & Mathai, D. Acute undifferentiated fever in India: a multicentre study of aetiology and diagnostic accuracy. BMC Infect. Dis. 2017, 17, 665. [CrossRef]
- Khan, S. A.; Bora, T.; Chattopadhyay, S.; Jiang, J.; Richards, A. L.; Dutta, P. Seroepidemiology of rickettsial infections in Northeast India. Trans. R. Soc. Trop. Med. Hyg. 2016, 110, 487–494. [CrossRef]
- Khan, S. A.; Bora, T.; Laskar, B.; Khan, A. M.; Dutta, P. Scrub Typhus Leading to Acute Encephalitis Syndrome, Assam, India. Emerg. Infect. Dis. 2017, 23, 148–150.
- Richards, A.L.; Jiang, J. Scrub Typhus: Historic Perspective and Current Status of the Worldwide Presence of Orientia Species. Trop. Med. Infect. Dis. 2020, 5, 49. [CrossRef]
- Jamil, M.; Lyngrah, K. G.; Lyngdoh, M.; Hussain, M. Clinical Manifestations and Complications of Scrub Typhus : A Hospital Based Study from North Eastern India. J. Assoc. Physicians India. 2014, 62, 19–23.
- Singh, S. I.; Devi, K. P.; Tilotama, R.; Ningombam, S.; Gopalkrishna, Y.; Singh, T. B.; Murhekar, M. V. An outbreak of scrub typhus in Bishnupur district of Manipur, India, 2007. Trop Doct. 2010, 40, 169–170. [CrossRef]
- Lalmalsawma, P.; Pautu, L.; and Lalremsiama, N. Scenario of scrub typhus disease in Mizoram, Northeast India. Int. J. Curr. Adv. Res. 2017, 6, 6341–6344.
- Meerburg, B. G.; Singleton, G. R.; Kijlstra, A. Rodent-borne diseases and their risks for public health. Crit. Rev. Microbiol. 2009, 35, 221–270. https://doi.org/10.1080/10408410902989837. [CrossRef]
- Davis, G.E,; Austrian, R.C.; Bell, E.J. Observations on tsutsugamushi disease (scrub typhus) in Assam and Burma: the recovery of strains of Rickettsia orientalis. Am. J. Epidemiol. 1947, 46, 268–286.
- Kochhar, R. K. "Observations on scrub typhus in NEFA and North Assam." Armed Forces Med. J. India 1972, 28, 130–46.
- Gurung, S.; Pradhan, J.; Bhutia, P. Y. Outbreak of scrub typhus in the North East Himalayan region-Sikkim: an emerging threat. Indian. J. Med. Microbiol. 2013, 31, 72–74. [CrossRef]
- Khamo, V.; Aiko, V.; Kapfo W.; Hiese M. A report on the present scenario of Scrub typhus in Nagaland, India. Int. J. Med. Sci. Public. Health 2016, 5, 160–161.
- Khan, S. A.; Dutta, P.; Khan, A. M.; Topno, R.; Borah, J.; Chowdhury, P.; Mahanta, J. Re-emergence of scrub typhus in northeast India. Int. J. Infect. Dis. 2012, 16, e889–e890. [CrossRef]
- The Hindu: 5 killed in Nagaland scrub typhus outbreak. Available online: https://www.thehindu.com/news/national/other-states/5-killed-in-nagaland-scrub-typhus-outbreak/article32647398.ece (accessed on 28 July 2023).
- Nagaland Post Scrub typhus kills 3 in Manipur village. Available online: https://nagalandpost.com/index.php/scrub-typhus-kills-3-in-manipur-village/ (accessed on 28 July 2023).
- Lalchhandama, K. "The saga of scrub typhus with a note on the outbreaks in Mizoram". Sci. Vis. 2018, 18, 50–57. https://doi.org/10.33493/scivis.18.02.01. [CrossRef]
- Min, K.-D.; Lee, J.-Y.; So, Y.; Cho, S.-i. Deforestation Increases the Risk of Scrub Typhus in Korea. Int. J. Environ. Res. Public. Health 2019, 16, 1518. https://doi.org/10.3390/ijerph16091518. [CrossRef]
- Alkathiry, H.; Al-Rofaai, A.; Ya’cob, Z.; Cutmore, T.S.; Mohd-Azami, S.N.I.; Husin, N.A.; Lim, F.S.; Koosakulnirand, S.; Mahfodz, N.H.; Ishak, S.N.; et al. Habitat and Season Drive Chigger Mite Diversity and Abundance on Small Mammals in Peninsular Malaysia. Pathogens 2022, 11, 1087. https://doi.org/10.3390/pathogens11101087. [CrossRef]
- Chen, Y.-L.; Guo, X.-G.; Ding, F.; Lv, Y.; Yin, P.-W.; Song, W.-Y.; Zhao, C.-F.; Zhang, Z.-W.; Fan, R.; Peng, P.-Y.; et al. Infestation of Oriental House Rat (Rattus tanezumi) with Chigger Mites Varies along Environmental Gradients across Five Provincial Regions of Southwest China. Int. J. Environ. Res. Public. Health 2023, 20, 2203. https://doi.org/10.3390/ijerph20032203. [CrossRef]
- Nallan, K.; Rajan, G.; Sivathanu, L.; Devaraju, P.; Thiruppathi, B.; Kumar, A.; Rajaiah, P. Molecular Detection of Multiple Genotypes of Orientia tsutsugamushi Causing Scrub Typhus in Febrile Patients from Theni District, South India. Trop. Med. Infect. Dis. 2023, 8, 174. https://doi.org/10.3390/tropicalmed8030174. [CrossRef]
- Pautu, L.; Lalmalsawma, P.; Vanramliana ; Rosangkima, G.; Malvi, Y. SCRUB TYPHUS DISEASE OUTBREAK AT CHEURAL VILLAGE, LAWNGTLAI DISTRICT, MIZORAM, NORTH-EAST INDIA. . J. Adv. Sci. Res. 2022, 13, 12–16. [CrossRef]
- Borkakoty, B.; Jakharia, A.; Biswas, D.; Mahanta, J. Co-infection of scrub typhus and leptospirosis in patients with pyrexia of unknown origin in Longding district of Arunachal Pradesh in 2013. Indian J Med Microbiol. 2016, 34, 88–91. [CrossRef]
- Dass, R.; Deka, N. M.; Duwarah, S. G.; Barman, H.; Hoque, R.; Mili, D.; Barthakur, D. Characteristics of pediatric scrub typhus during an outbreak in the North Eastern region of India: peculiarities in clinical presentation, laboratory findings and complications. Indian. J. Pediatr. 2011 , 78, 1365–1370. [CrossRef]
- Lurshay, R.M.; Gogoi, P.R.; Deb, S. Clinico-laboratory profile of severe pediatric scrub typhus. Sch. J. App Med. Sci. 2016, 4, 3714–3720.
- Gupta, N.; Mittal, V.; Gurung, B.; Sherpa, U. Pediatric Scrub typhus in South Sikkim. Indian. Pediatr. 2012, 49, 322–324.
- Jakharia, A.; Borkakoty, B.; Biswas, D.; Yadav, K.; Mahanta, J. Seroprevalence of Scrub Typhus Infection in Arunachal Pradesh, India. Vector Borne Zoonotic Dis. 2016, 16, 659–663. [CrossRef]
- Kala, D.; Gupta, S.; Nagraik, R.; Verma, V.; Thakur, A.; Kaushal, A. Diagnosis of scrub typhus: recent advancements and challenges. 3 Biotech. 2020 ,10, 396. [CrossRef]
- Huidrom S, Singh LK. Clinical and laboratory manifestations of scrub typhus: A study from a tertiary care hospital in Manipur Indian. J. Microbiol. Res. 2017, 4, 434–436.
- Yoo, J. S.; Kim, D.; Choi, H. Y.; Yoo, S.; Hwang, J. H.; Hwang, J. H.; Choi, S. H.; Achangwa, C.; Ryu, S.; Lee, C. S. Prevalence Rate and Distribution of Eschar in Patients with Scrub Typhus. Am. J. Trop. Med. Hyg. 2022 ,106, 1358–62. [CrossRef]
- Mahajan, S. K., Rolain, J. M., Kashyap, R., Bakshi, D., Sharma, V., Prasher, B. S., Pal, L. S., & Raoult, D. Scrub typhus in Himalayas. Emerg. Infect. Dis. 2006, 12, 1590–2.
- Varghese, G. M., Janardhanan, J., Trowbridge, P., Peter, J. V., Prakash, J. A., Sathyendra, S., Thomas, K., David, T. S., Kavitha, M. L., Abraham, O. C., & Mathai, D. Scrub typhus in South India: clinical and laboratory manifestations, genetic variability, and outcome. Int. J. Infect. Dis. 2013 , 17, e981-7. [CrossRef]
- Pokhrel, A.; Rayamajhee, B.; Khadka, S.; Thapa, S.; Kapali, S.; Pun, S.B.; Banjara, M.R.; Joshi, P.; Lekhak, B.; Rijal, K.R. Seroprevalence and Clinical Features of Scrub Typhus among Febrile Patients Attending a Referral Hospital in Kathmandu, Nepal. Trop. Med. Infect. Dis. 2021, 6, 78. [CrossRef]
- Dhar, D.; Choudhury, K. A Prospective Analysis of Seroprevalence and Demographic Profile of Scrub Typhus in a Tertiary Care Hospital of South Eastern Assam. Int. J. Res. Rev. 2020, 7, 179–182.
- Debnath, P.; Debbarma, R.K.; Debbarma, D. Clinical Profile of Scrub Typhus: A Cross Sectional Study in a Tertiary Care Centre of Tripura. Inter. J. Dent. Med. Sci. Res. 2021, 3, 302–305.
- Ngulani, K.S.; Kakati, S.; Hussain, S.; Singh, M.U.; Kaguilan, K. Outbreak of scrub typhus in Manipur - experience at a tertiary care hospital. IOSR J. Dent. Med. Sci. 2019, 18, 33–8.
- Bora, T.; Khan, S. A.; Jampa, L.; Laskar, B. Genetic diversity of Orientia tsutsugamushi strains circulating in Northeast India. Trans. R. Soc. Trop. Med. Hyg. 2018, 112, 2–30. [CrossRef]
- Jamil, M.; Bhattacharya, P.; Mishra, J., Akhtar, H.; Roy, A. Eschar in Scrub Typhus: A Study from North East India. J. Assoc. Physicians India 2019, 67, 38–40.
- Sivarajan, S.; Shivalli, S.; Bhuyan, D.; Mawlong, M.; Barman, R. Clinical and paraclinical profile, and predictors of outcome in 90 cases of scrub typhus, Meghalaya, India. Infect. Dis. Poverty 2016, 5, 91. [CrossRef]
- Jamil, M. D.; Hussain, M.; Lyngdoh, M.; Sharma, S.; Barman, B.; Bhattacharya, P. K. Scrub typhus meningoencephalitis, a diagnostic challenge for clinicians: A hospital based study from North-East India. J. Neurosci. Rural. Pract. 2015, 6, 488–493. [CrossRef]
- Sharma, S. R.; Masaraf, H.; Lynrah, K. G.; Lyngdoh, M. Tsutsugamushi Disease (Scrub Typhus) Meningoencephalitis in North Eastern India: A Prospective Study. Ann. Med. Health Sci. Res. 2015, 5, 163–7.
- Palani, M.T.; Mishra, M.N.; Odyuo, B.T.S.; Mishra, P.; Abraham, S. Infection pattern and Laboratory Profile of Scrub Typhus in A Secondary Care Centre from North-East India. J. Infect. Pathol, 2022, 5, 2.
- Vanlalruati, R.S.C.; Lalhmingmawii, S.R.; Lallawmkima, I.; Lalthantluanga, B.; Renthlei, L.; Pautu, L. Serological Evidence of Scrub Typhus in Mizoram, North Eastern Region of India. Infect. Dis. Clin. Microbiol. 2022, 4, 55–61. [CrossRef]
- Khan, S.A.; Saikia, J.; Bora, T.; Khamo, V.; Rahi, M. Molecular detection of Orientiatsutsugamushi strains circulating in Nagaland. Indian. J. Med. Microbiol. 2022, 40, 443–445. [CrossRef]
- Khan, S.A.; Murhekar, M.V.; Bora, T.; Kumar, S.; Saikia, J.; Kamaraj, P.; Sabarinanthan, R. Seroprevalence of Rickettsial Infections in Northeast India: A Population-Based Cross-Sectional Survey. Asia Pac. J. Public. Health. 2021, 33, 516–522. [CrossRef]
- Durairaj, E.; Lynrah, K.; Lyngdoh, C.J.; Barman, H.; Lyngdoh, W.V.; Paul, D.Performance Analysis and Evaluation of Quantitative Real Time PCR for Diagnosis of Scrub Typhus in North-East India. IJTDH.2021, 42, 24-33. [CrossRef]
- Singh, K.R.; Singh, C.G.; Khumukcham, S.; Marak, N.D.; Kumar, P.; Parasmani, H.; Kharshiing, G.A. Scrub typhus: An unusual cause of acute abdomen. J. Med. Soc. 2019, 33, 43–46.
- Lalrinkima, H.; Lalremruata, R.; Lalchhandama, C.; Khiangte, L.; Siamthara, F. H.; Lalnunpuia, C., Borthakur, S. K., & Patra, G. (2017). Scrub typhus in Mizoram, India. J. Vector Borne Dis. 2017, 54, 369–371.
- Mohan, D.G.; Teronpi,T.; Sharma, A.; Dey, S. “Scrub typhus”: One of the leading cause of febrile illness: A report from a tertiary care centre. IJMHR. 2018, 4, 76–78.
- Varghese, G. M.; Janardhanan, J.; Mahajan, S.K.; Tariang, D.; Trowbridge, P.; Prakash, J.A.; David, T.; Sathendra, S.; Abraham, O.C. Molecular epidemiology and genetic diversity of Orientia tsutsugamushi from patients with scrub typhus in 3 regions of India. Emerg. Infect. Dis. 2015, 21, 64–69.
- Singh, S.K.; Ram, R.; Marangmei, L.; Chakma, G. Case Series on Scrub Typhus from a tertiary care hospital of North East India. IOSR J. Dent. Med. Sci. 2014, 13, 62–64. [CrossRef]
- Basheer, A.; Iqbal, N.; Mookkappan, S.; Anitha, P.; Nair, S.; Kanungo, R.; Kandasamy, R. Clinical and Laboratory Characteristics of Dengue-Orientia tsutsugamushi co-Infection from a Tertiary Care Center in South India. Mediterr. J. Hematol. Infect. Dis. 2016, 8, e2016028. https://doi.org/10.4084/MJHID.2016.028. PMID: 27413521; PMCID: PMC4928539. [CrossRef]
- Baruah, M.K.; Sharma, J. First report of scrub typhus cases in Dhemaji, Assam, India. South. Indian. J. Biol. Sci. 2015, 1, 156–157.
- Wilairatana, P.; Kuraeiad, S.; Rattaprasert, P.; Kotepui, M. Prevalence of malaria and scrub typhus co-infection in febrile patients: a systematic review and meta-analysis. Parasit. Vectors. 2021, 14, 471. [CrossRef]
- Md-Lasim, A.; Mohd-Taib, F.S.; Abdul-Halim, M.; Mohd-Ngesom, A.M.; Nathan, S.; Md-Nor, S. Leptospirosis and Coinfection: Should We Be Concerned? Int. J. Env. Res. Public. Health.2021, 18, 9411. [CrossRef]
- Gupta, N.; Mittal, V.; Gurung, B.; Sherpa, U. Pediatric Scrub typhus in South Sikkim. Indian. Pediatr. 2012, 49, 322–324.
- Lv. Y.; Guo, X.G.; Jin, D.C. Research Progress on Leptotrombidium deliense. Korean J. Parasitol. 2018, 56, 313–324. [CrossRef]
- Sharma, A.K. Entomological surveillance for rodent and their ectoparasites in Scrub typhus affected areas of Meghalaya, (India). J. Entomol. Zool.2013, 1, 27-29.
- Lalthazuali; Sharma, A.K.; Thomas, T.G.; Bhan, S.; Bhadauriya, A.S.; Ramteke, P.U.; Kumawat, R.; Singh, R. Entomological survey of vectors of Scrub typhus in Haulawng, Lunglei district, Mizoram, India. J. Commun. Dis. 2020, 52, 69–73.
- Devasagayam, E.; Dayanand, D.; Kundu, D.; Kamath, M.S.; Kirubakaran, R.; Varghese, G.M. The burden of scrub typhus in India: A systematic review. PLoS Negl. Trop. Dis. 2021,15, 9619. [CrossRef]
- Dey, R.K.; Imad, H.A.; Aung, P.L.; Faisham, M.; Moosa, M.; Hasna, M.; Afaa, A.; Ngamprasertchai, T.; Matsee, W.; Nguitragool, W.; Nakayama, E.E.; Shioda, T.Concurrent Infection with SARS-CoV-2 and Orientia tsutsugamushi during the COVID-19 Pandemic in the Maldives. Trop. Med. Infect. Dis. 2023, 8, 82. [CrossRef]
- Luce-Fedrow, A.; Lehman, M.L.; Kelly, D.J.; Mullins, K.; Maina, A.N.; Stewart, R.L.; Ge, H.; John, H.S.; Jiang, J.; Richards, A.L. A Review of Scrub Typhus (Orientia tsutsugamushi and Related Organisms): Then, Now, and Tomorrow. Trop. Med. Infect. Dis. 2018, 3, 8. [CrossRef]
- Subbalaxmi, M.V., Madisetty, M.K., Prasad, A.K., Teja, V.D., Swaroopa, K., Chandra, N., Upadhyaya, A.C., Shetty, M., Rao, M.N., Raju, Y.S.; Lakshmis, V. Outbreak of scrub typhus in Andhra Pradesh--experience at a tertiary care hospital. J. Assoc. Physicians India,2014, 62, 490-496.
- Blacksell, S.D.; Bryant, N.J.; Paris, D.H.; Doust, J.A.; Sakoda, Y.; Day, N.P.J. Scrub typhus serologic testing with the indirect immunofluorescence method as a diagnostic gold standard: a lack of consensus leads to a lot of confusion. Clin. Infect. Dis. 2007, 44, 391–401. [CrossRef]
- Lee, K.D.; Moon, C.; Oh, W.S.; Sohn, K.M.; Kim, B.N. Diagnosis of scrub typhus: introduction of the immunochromatographic test in Korea. Korean J. Intern. Med. 2014, 29, 253–255. [CrossRef]
- Blacksell, S.D.; Paris, D.H.; Chierakul, W.;Chierakul, W.;Wuthiekanun, V.; Teeratakul, A.; Kantipong, P.;Day, N.P.J.Prospective evaluation of commercial antibody-based rapid tests in combination with a loop-mediated isothermal amplification PCR assay for detection of Orientia tsutsugamushi during the acute phase of scrub typhus infection. Clin. Vaccine. Immunol.2012, 19, 391. [CrossRef]
- Blacksell, S.D.; Jenjaroen, K.; Phetsouvanh, R.; Tanganuchitcharnchai, A.; Phouminh, P.; Phongmany, S.; Day, N.P.;Newton, P.N.Accuracy of rapid IgM-based immunochromatographic and immunoblot assays for diagnosis of acute scrub typhus and murine typhus infections in Laos. Am. J. Trop. Med. Hyg. 2010, 83, 365–369. [CrossRef]
- Rahi, M.; Gupte, M.D.; Bhargava, A.; Varghese, G.M.; Arora, R. DHR-ICMR guidelines for diagnosis and management of rickettsial diseases in India. Indian. J. Med. Res. 2016, 417-422.
- Palani, M.T.; Mishra, M.N.; Odyuo, B.T.S.; Mishra, P.; Abraham, S. Infection pattern and Laboratory Profile of Scrub Typhus in A Secondary Care Centre from North-East India. J. Infect. Pathol.2022, 5, 149.
- Lallawmkima, I.; Vanlalruati, R.S.C.; Chongthu, J.L.; Renthlei, L. Scrub Typhus with Multi-Organ Dysfunction Syndrome and Immune Thrombocytopenia: A Case Report.IDCM. 2022, 4, 133–136. [CrossRef]
- Mohanty. A.; Gupta, P.; Singh, T.S; Gupta, P. Scrub typhus with a rare presentation in a child- a case report . J. Med. Sci. Clin. Res. 2017, 5, 19968–19970.
- Mohanty, A.; Kabi, A; Gupta, P.; Jha, M.K.; Rekha, U.S.; Raj, A.K. Scrub typhus - A case series from the state of Sikkim, India. Int. J. Crit. Illn. Inj. Sci. 2019, 9, 194–198.
- Mangaraj, J.; Sharma, A.; Alam, S.T. Report of sporadic cases of scrub typhus–A threat to re-emergence in Assam, India. Int. J. Curr. Microbiol. Appl. Sci.2017, 6, 1037-41. [CrossRef]
- Biradar, C.; Rama, S.K.; Nizami, A.I.; Handique, F.; Halemani, C. Soldiers from Indo Myanmar Border Presenting with Scrub Typhus.J. Dent. Med. Sci.2015, 14, 123-127.
- Tony, E.; Roy, A.; Barman, B.; Lynrah, K.; Komut, O.; Khonglah, Y. Hemophagocytic Syndrome Associated with Scrub Typhus: A Case Report from North East India. J. Clin. Case Rep.2015, 5, 10.
- Karim, H.M.R.; Bhattacharyya, P.; Yunus, M. A Case Report of an unusual presentation: Could the early use of interventional radiology have saved this patient of scrub typhus. Bangladesh Crit. Care J.2014, 2, 79-80. [CrossRef]
- Dhakal, M.; Dhakal, O.P.; Bhandari, D. Pancreatitis in scrub typhus: a rare complication. BMJ Case Rep.2014, bcr2013201849. [CrossRef]
- Sawale, V.; Upreti, S.; Singh, T.S.; Singh, N.; Singh, T.B. A rare case of Guillain-Barre syndrome following scrub typhus. Neurol. India.2014, 62, 82. [CrossRef]
- Goswami, D.; Hing, A.; Das, A.; Lyngdoh, M. Scrub typhus complicated by acute respiratory distress syndrome and acute liver failure: a case report from Northeast India. Int. J. Infect. Dis.2013, 17, e644-e645. [CrossRef]
- Dutt Y, Dhiman R, Singh T, Vibhuti A, Gupta A, Pandey RP, Raj VS, Chang CM, Priyadarshini A. The Association between Biofilm Formation and Antimicrobial Resistance with Possible Ingenious Bio-Remedial Approaches. Antibiotics (Basel). 2022 Jul 11;11(7):930. [CrossRef]
- Hardesh K. Maurya, H. K. Maurya, Ramendra Pratap, R. Pratap, Abhinav Kumar, A. Kumar, Brijesh Kumar, B. Kumar, Volker Huch, V. Huch, Vishnu K. Tandon, V. K. Tandon, & Vishnu Ji Ram, V. Ji Ram. (0000). A carbanion induced ring switching synthesis of spiranes: an unprecedented approach. RSC advances, 2, 9091-9099. [CrossRef]
- A carbanion induced ring switching synthesis of spiranes: an unprecedented approach HK Maurya, R Pratap, A Kumar, B Kumar, V Huch, VK Tandon, VJ Ram RSC advances 2 (24), 9091-9099.
- Physico-chemical properties of starch and protein and their relation to grain quality and nutritional value of rice, PK Mishra, R Pandey, Rice Breed. Pub. IRRI, Los Banos, Phillippines, 389-405.
- INFLUENCE OF FERTILITY LEVELS, VARIETIES AND TRANSPLANTING TIME ON RICE (ORYZA-SATIVA), R Pandey, MM Agarwal Indian Journal of Agronomy 36 (4), 459-463.
- Pandey RP, Mukherjee R, Priyadarshini A, Gupta A, Vibhuti A, Leal E, Sengupta U, Katoch VM, Sharma P, Moore CE, Raj VS, Lyu X. Potential of nanoparticles encapsulated drugs for possible inhibition of the antimicrobial resistance development. Biomed Pharmacother. 2021 Sep;141:111943. [CrossRef]
Figure 1.
Map locating Tsutsugamushi triangle and North-East (NE) India. Red line shows the boundaries of the eight states of NE India.
Figure 1.
Map locating Tsutsugamushi triangle and North-East (NE) India. Red line shows the boundaries of the eight states of NE India.
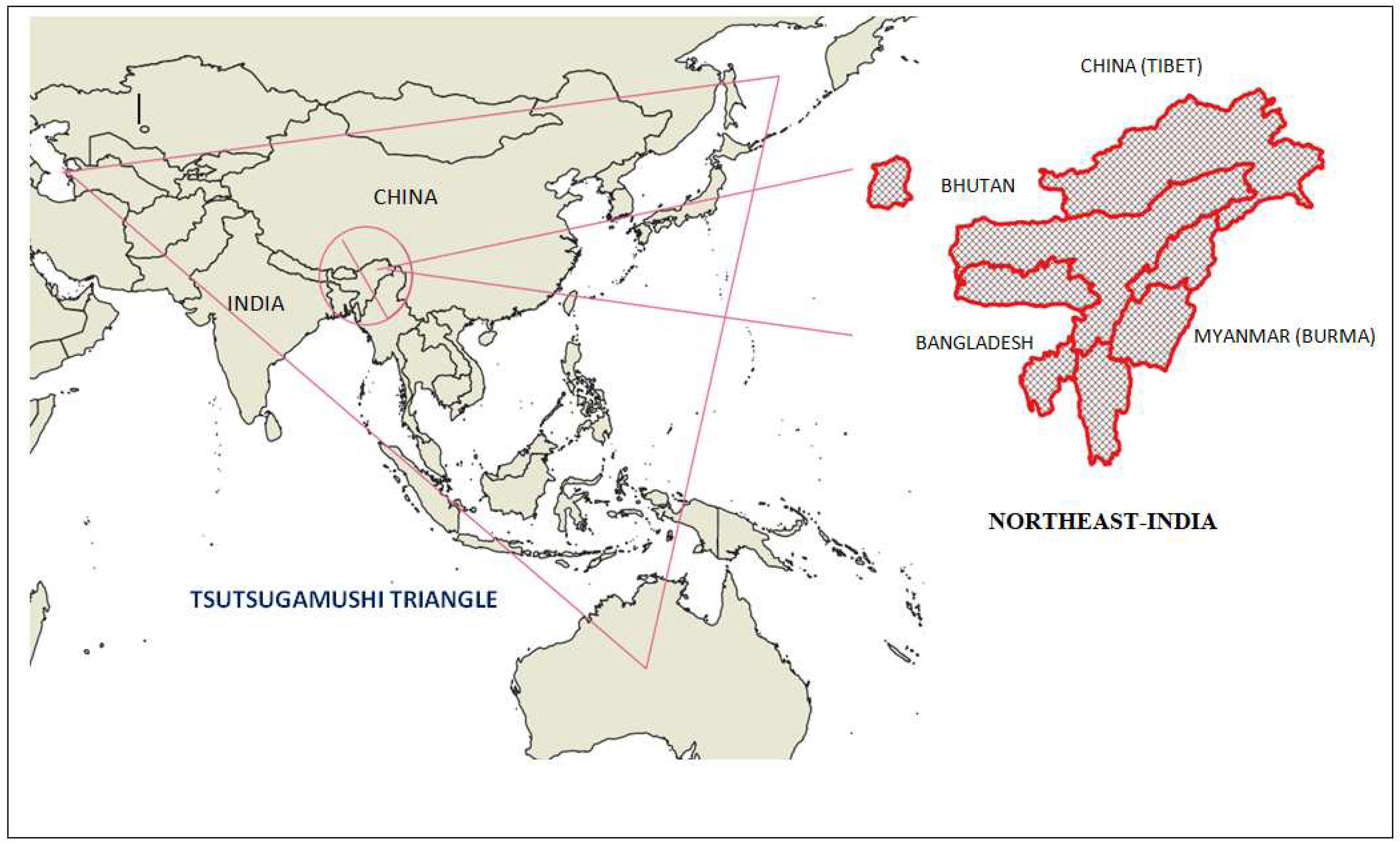
Figure 2.
Proportion (%) of clinical manifestation among scrub typhus patients.
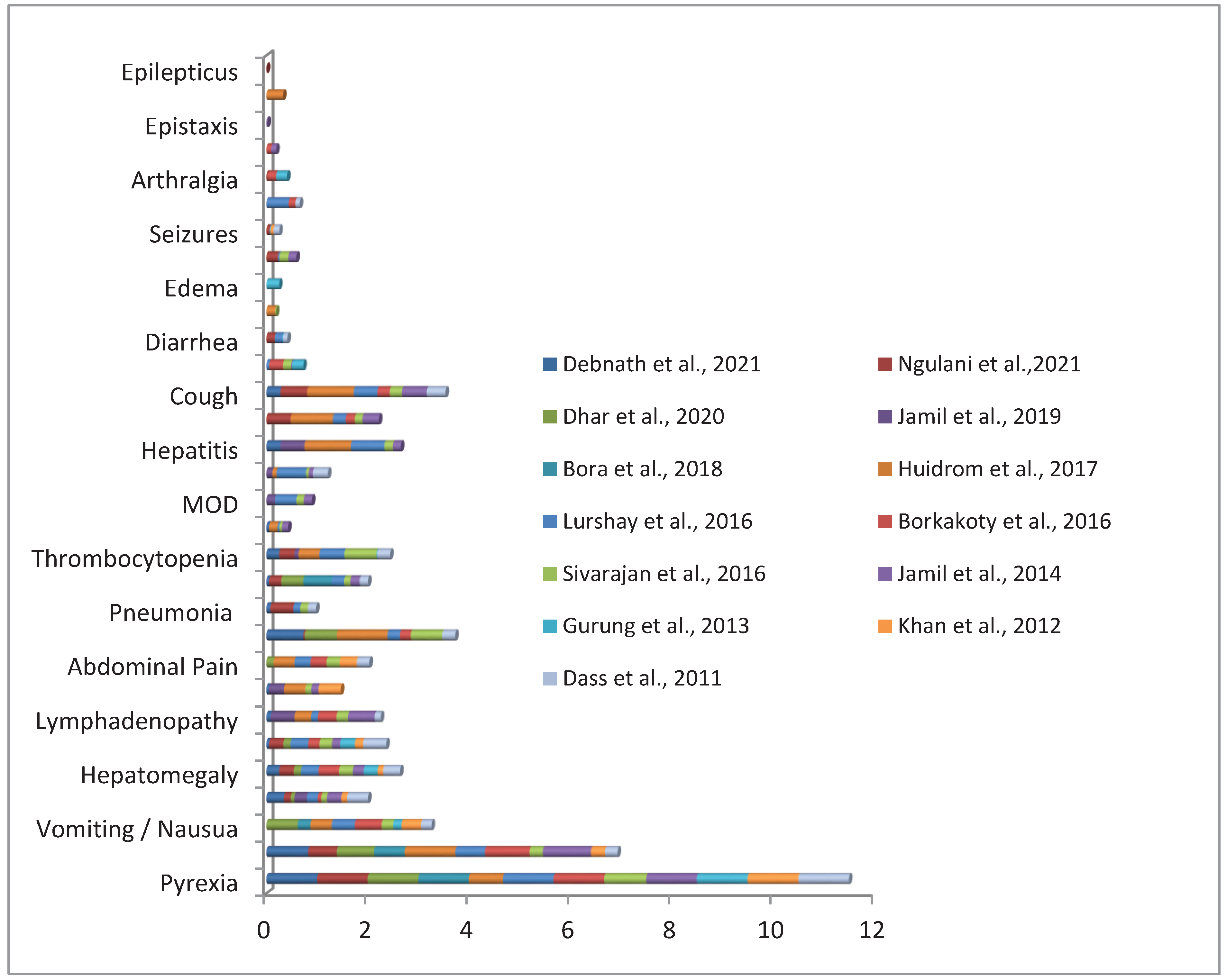

Table 1.
Prevalence of scrub typhus in North-East India.
| Region | Outbreak/ study Duration | Age in months/ Years |
Diagnostic confirm cases | Method of diagnosis | Antibody/marker gene | Fatalities | Affected groups/Outcome/Remarks | References |
|---|---|---|---|---|---|---|---|---|
| Lawngtlai District, Mizoram | December , 2019 | Mean age was 40 years | 80 | WFT | OXK | NA | Affected group: adults (31-40 age group), farmers, female, rural areas. | (Pautu et al. 2022) [51] |
| Assam | April 2017 to March 2018 | 3 to 85 yrs (mean age 39.6 yrs) | 56 | ICT | IgG, IgM, IgA | NA | Liver function evaluation and proteinuria attained statistical significance. | (Palani et al. 2022)$ [71] |
| Mizoram | October 1, 2018 to September 31, 2019 | 7 months to 94 years | 36 | ICT, ELISA |
IgG, IgM, IgA IgM |
NA | The sensitivity of IgM ELISA and Rapid test were 44.19% and 46.40% respectively. 36 positive for both ICT and ELISA. |
(Vanlalruati et al. 2022) # [72] |
| Nagaland | December 2018 | NA | 2 (pcr) 87 (WFT)= 89 |
PCRWFT | 56 kDa OXK |
NA | Closest homology with the prototype strain TA763 (endemic in Thailand and Taiwan). | (Khan et al. 2022) [73] |
| Manipur | August 2017 to December 2018 Peak season : July to November |
≥12 years Mean age: 41 years (±16) |
176 | ICT | IgG, IgM, IgA | 8 | Affected group: rural areas, farmers, and adults. | (Ngulani et al. 2021) $ [65] |
| Assam, Meghalaya, and Tripura |
September 2017 to February 2018 | 3 to 45 years | 18 | ELISA | IgG | NA | Community based studies Documented low prevalence (0.76%) of scrub typhus. |
(Khan et al. 2021)# [74] |
| Meghalaya | June 2019 to May 2020 | NA | 37 | WFT ELISA PCR |
OXK IgM 56 kDa |
NA | 14% OXK positive 34 % ELISA positive 50% PCR positive (27/54) |
(Durairaj et al. 2021) # [75] |
| Tripura | January 2018 to December 2018 Peak season: September |
Mean age 28 to 50 years. | 40 | NA | NA | 1 | Deranged liver function and thrombocytopenia significant. | (Debnath et al. 2021)# [64] |
| Assam | January 2017 to September 2017 |
≥11 yearsMean age: 20-29 years | 14 | ELISA | IgM | NA | Prevalence rate of Scrub typhus: 20%. | (Dhar et al. 2020)# [63] |
| Manipur | August 2017 to November 2018 | ≥20 years | 8 | WFT ELISA |
OXK IgM |
1 | Scrub typhus Presenting as Acute Abdomen case. | (Singh et al. 2019) # [76] |
| Meghalaya | January 2013 to December 2015 | ≥ 18 years | 129 | ICT WFT ELISA |
IgM OXK IgM |
NA | Eschar was found in 24.8% of the scrub typhus patients. | (Jamil et al. 2019) $ [67] |
| Assam and Arunachal | December 2014 to December 2016. Peak season: May to August |
3 to 80 years | 278 | ELISA PCR |
IgM, IgG, 47 KDa, 56 KDa, 16S rRNA |
NA | Pre-dominance of Karp-like strains. | (Bora et al. 2018) [66] |
| Assam | NA | 1- >60years Mean age: 25-36 yrs |
33 | ELISA | IgM | NA | Prevalence rate of scrub typhus: 22.2% | (Mohan et al. 2018) [78] |
| Mizoram | January 2012 to July 2017 Peak season: July and November |
2 months -85 years Mean age:34 years |
907 | ICT | IgM, IgG and IgA | 34 | Age group 20-30 years were affected more. The youngest patient recorded was a 2 months old male. Male affected more. |
(Lalmalsawma, et al. 2017 ) [37] |
| Manipur | January 2016 to May 2017 | 6 to 67 years | 24 | ICT | IgM, IgG and IgA | NA | Affected group: Rural background. One patient was Dengue positive |
(Huidrom et al.2017) ^* [58] |
| Tezpur, Assam | April 2011–November 2012 | ≥5 years | 75 | IFA ELISA |
IgM | NA | Affected group: Rural areas Scrub typhus co-infection observed. |
(Mørch et al. 2017)* [31] |
| Dibrugarh, Assam | 2013–2015 Peak season: July–September |
3 to 80 years | 104 | ELISA PCR |
IgM 56-kDa |
26 | 13 (12.5%) co-infected with JEV IgM. Resemblances of Karp strain. Occupation= NA High case-fatality rate of 49% (26/53 follow-up) |
(S A Khan et al. 2017) $ * [33] |
| Aizawl, Mizoram | October 2014 to December 2016. Peak season: November to February and September to October (autumn) |
1 to ≥60 years | 283 | ICT | IgM | NA | 21–30 age groups were most affected. Prevalence of ST 6.9%. |
(Lalrinkima et al. 2017) # [77] |
| Nagaland | 2014 | - | 31 | ELISA | IgM | NA | Community based studies. 7.2% samples positive by IgM ELISA. |
(Khamo et al. 2016) [42] |
| Meghalaya | January 2014 to December 2014 | Below 18 years | 75 | ICT | IgM, IgG and IgA | 1 | Inclusion: children below 18 years. Antibiotics data not available. |
(Lurshay et al. 2016) [54] |
| Arunachal Pradesh | 2009 to 2013 | 2– 80 years | 121 | ELISA | IgG | NA | Community based studies. Farmers, adults, females were affected more. Seroprevalence was 40.3%. |
(Jakharia et al. 2016) $ [56] |
| Meghalaya | September 2011 to August 2012 Peak season: September to December |
≥ 18 years Mean age: 21–30 years |
90 | ICT | IgM, IgG and IgA | 5 | Farmer, 21–30 years were more affected. 13.6 % ST positive. Malaria co-infection observed in two patients. |
(Sivarajan et al. 2016) * + [68] |
| Arunachal Pradesh | NA | 0 - ≥ 15 years | 30 | ELISA | IgM | NA | 25% cases were co-infected with leptospira. | (Borkakoty et al. 2016)* [52] |
| Assam, Arunachal, Nagaland |
2013 to 2015 | - | 390 | ELISA PCR |
IgM 56-kDa |
NA | Community based studies 30.8% positive for scrub typhus. Sequence analysis revealed Karp-like strains from Thailand, Taiwan and Vietnam. |
( Khan et al. 2016)* [32] |
| Meghalaya | October 2009 to November 2011 | 19 to 68 years | 23 (meningitis) | WFT ELISA |
OX K IgM |
NA | Scrub meningitis cases. Majority of patients were either farmers or housewives. |
(Sharma et al. 2015) # [70] |
| Meghalaya | January 1, 2013 to December 31, 2014. Peak season: October to November |
Above 12 years Mean age: 34.84 ± 16.21 years |
113 | WFT ICT |
OXK IgM |
2 | 13.2% featured with meningitis/meningoencephalitis. 0.07% had multiple eschar. |
(Jamil et al. 2015)# [69] |
| Meghalaya | September 2010 to August 2012 | Mean age 40 ± 12 years | 96 | ELISA PCR |
IgM 56-kDa |
NA | Kato (Hualien-13) closest to Cambodia and Neimang-65 strains were observed. Karp and Gilliam like strains were also observed. |
(Varghese et al. 2015) [79] |
| Meghalaya | 7th January 2013 to 6th January 2014 Peak season: September to November |
≥ 18 years | 61 | WFT ICT |
OXK IgM, IgG and IgA |
5 | 18 to 30 year’s age group was affected. 4.9% scrub typhus patients’ pregnant women were treated with azithromycin. |
(Jamil et al. 2014)# +* [35] |
| Manipur | July to October | 15-65 years | 6 | ICT | IgM, IgG and IgA | NA | Affected group: rural areas. 2 scrub typhus patients had eschar |
(Singh et al. 2014) [80] |
| Sikkim | January 2011 to December 2011 Peak season: July and October |
Above 2 years | 63 | WFT ICT ELISA |
OXK IgA, IgM, and IgG IgM |
1 | Eschar was seen in 10 pediatric patients. 55.56% had pedal edema. 30.8% scrub typhus positive for IgM ELISA. |
(Gurung et al. 2013) + [41] |
| Assam, Arunachal Pradesh, and Nagaland | 2010 to 2011 | NA | 108 | ELISA PCR |
IgM 56-kDa |
NA | 34.39% scrub typhus positive for IgM ELISA. 15.38% were PCR-positive for ST. |
(Khan et al. 2012) [43] |
| Meghalaya | October 2009 to January 2010 | Average age: 9.4 years | 24 | WFT | OXK | NA | Pediatric scrub typhus cases. | (Dass et al. 2011) [53] |
| Manipur | 2007 | 0 to ≥ 45 years | 38 | WFT | OXK | 2 | 71% received treatment from traditional healers. 55% had eschar on the perineal area. |
(Singh et al. 2010) [36] |
$ Retrospective study ; # Cross sectional study / prospective study ; ^ Antibiotics administered before confirmation of diagnosis ; + Antibiotics used in younger children or pregnant women ; * Co-infection with leptosptosis, JEV IgM, Dengue and other febrile illness. IFA: Immunofluorescence Assay, WFT: Weil Felix Test, ELISA: Enzyme-linked Immunosorbent Assay, PCR: Polymerase chain Reaction.
Table 2.
Case report of Scrub typhus from Northeast-India.
| Region | Cases | Diagnosis | Treatment | Fatalities | References |
|---|---|---|---|---|---|
| Mizoram | 1 | IgM ELISA | Ceftriaxone-sulbactam Doxycycline Azithromycin |
- | (Lallawmkima et al. 2022) [99] |
| Sikkim | 3 | WFT IgM ELISA |
Ceftriaxone^, Amiodarone^ Doxycycline + |
- | (Mohanty et al. 2019) [100] |
| Sikkim | 1 | WFT, ELISA |
Ceftriaxone^ +, Doxycycline + |
- | (Mohanty et al. 2017) [101] |
| Assam | 3 | WFT | Cefotaxime, Doxycycline Derriphylline |
- | (Mangaraj et al, 2017) [102] |
| Nagaland | 2 | ICT | Doxycycline | - | (Biradar et al. 2015) [103] |
| Assam | 3 | ELISA | NA | - | ( Baruah et al.2015) * [81] |
| Meghalaya | 1 | ICT | Ceftriaxone, Doxycycline, Azithromycin |
- | (Ete et al. 2015) [104] |
| Meghalaya | 1 | WFT | Inj. Artesunate, Inj.Acyclovir and Inj. Ceftriaxone^ Tab. Doxycycline Pantoprazole Inj. Dobutamine Inj. Azithromycin |
1 | (Karim et al. 2014) [105,112] |
| Manipur | 1( Guillain-Barre syndrome | ICT | Doxycycline | - | (Sawale et al. 2014) [107] |
| Sikkim | 1 | WFT, ICT, ELISA |
Cefotaxime, Doxycycline |
- | (Dhakal et al. 2014) [106] |
| Meghalaya | 1 | WFT | Doxycycline, Ceftriaxone Chloramphenicol. | - | (Goswami et al. 2013) [108,109] |
| Sikkim | 5 | WFT ELISA |
Doxycycline+ Ceftriaxzone+ |
1 | (Gupta et al. 2012) [85,113,114] |
$ Retrospective study ; # Cross sectional study / prospective study ; ^ Antibiotics administered before confirmation of diagnosis ; + Antibiotics used in younger children or pregnant women ; * Co-infection with leptosptosis, JEV IgM, Dengue and other febrile illness.IFA: Immunofluorescence Assay; WFT: Weil Felix Test; ELISA: Enzyme-linked Immunosorbent Assay .
Table 3.
Entomological studies on vectors.
| Region | Host | Ectoparasites | Outcome | References |
|---|---|---|---|---|
| Mizoram | Rodent Species | Mites (chigger) | Reactive with any one or all of PROGEN OXK, OX19 or OX2. Chigger (mite) index =19.2 |
[52] |
| Mizoram | Rodent Species | Mites, Lice, Fleas | Chigger (mite) index =12.33 Chigger infestation rate=18.5 |
[88] |
| Assam, Arunachal Pradesh and Nagaland | Rodents, dogs, cats, cattle, and human | Ticks, mites, fleas and lice | NA for ST(scrub typhus) Positive for spotted fever group Rickettsia species. |
[32] |
| Meghalaya | Rodent Species | Ticks, mites, fleas and lice | Chigger (mite) index =1.8 Chigger infestation rate=4.8 |
[87] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



