Submitted:
31 July 2023
Posted:
02 August 2023
You are already at the latest version
Abstract
Considering the controversial benefits of video-assisted thoracoscopic surgery (VATS), we intended to evaluate the impact of surgical approach on cardiac function after lung resection using myocardial work analysis. Echocardiographic data of 45 patients (25 thoracotomy vs. 20 VATS) were retrospectively analyzed. All patients underwent transthoracic echocardiography (TTE) 2 weeks before and after surgery, including two-dimensional speckle tracking and tissue doppler imaging. No notable changes in left ventricular (LV) function, assessed mainly using the LV global longitudinal strain (GLS), global myocardial work index (GMWI), and global work efficiency (GWE), were observed. Right ventricular (RV) TTE values, including tricuspid annular plane systolic excursion (TAPSE), tricuspid annular systolic velocity (TASV), and RV free-wall GLS (RVFWGLS), indicated greater RV function impairment in the thoracotomy group than in the VATS group [TAPSE (mm): 17.90 ± 3.80 vs. 20.60 ± 3.50, p < 0.018; TASV (cm/s): 12.40 ± 2.90 vs. 14.60 ± 2.50, p < 0.010; RVFWGLS (%): −11.50 ± 8.50 vs. −17.50 ± 9.70, p < 0.033), respectively]. Unlike RV function, LV function remained preserved after lung resection. The thoracotomy group exhibited greater RV function impairment than did the VATS group. Further studies should evaluate the long-term impact of surgical approach on cardiac function.
Keywords:
echocardiography
; non-invasive
; global myocardial work
; thoracotomy
; video-assisted thoracoscopic surgery
; VATS
; lung resection
; lung surgery
; right ventricle
; left ventricle
1. Introduction
Cancer is among the most common causes of death globally, with lung cancer being the foremost cause of cancer-associated death [1,2]. Surgical treatment remains the most common and preferred therapeutic option for early-stage lung cancer [3,4]. Evidence has shown that patients undergoing lung resection through the minimally invasive Video-Assisted Thoracoscopic Surgery (VATS) technique have significantly shorter drainage time and hospital stay and better long-term survival than do patients undergoing conventional lateral thoracotomy [5,6]. There are various levels involved in the complex interdependence between cardiac and respiratory function [7,8]. Lung resections have been associated with long-term cardiorespiratory morbidity, primarily caused by cardiovascular changes resulting from right and LV dysfunction [9,10]. Transthoracic echocardiography (TTE) has remained the leading method for the routine clinical assessment of cardiac changes after lung resection due to ease of accessibility in standard care hospitals, as well as cost and time effectiveness [11].
The complexity of the right ventricular (RV) anatomy and physiology, especially the marked load dependency of RV function, demands multiparametric echocardiographic assessment, including longitudinal strain, tissue doppler imaging, and myocardial work analysis.[12,13]
The effects of lung resection and surgical approach (i.e., VATS vs. open thoracotomy) on myocardial function have not been adequately studied. Hence, the current study aimed to identify changes in myocardial function after lung resection using myocardial work (MW) analysis, a novel non-invasive method based on echocardiography [14,15,16].
2. Methods
2.1. Patient collection and study protocol
Our study was conducted at the cardiothoracic surgery department of the university hospital of RWTH Aachen in Germany. Patients who underwent surgery from January 2015 to December 2021 were enrolled (Figure 1). We screened 187 patients but only included 45 (25 thoracotomy vs. 20 VATS) owing to exclusion criteria: (1) prior cardiac surgery, (2) prior lung resection, (3) pneumonectomy, (4) severe heart failure, (5) moderate or severe valvular disease, (6) moderate or severe pulmonary hypertension (PAH), (7) inappropriate ultrasound windows, (8) pregnancy, and (9) arrhythmias. Cardio pulmonary bypass and pericardiotomy during cardiac surgery can cause serious changes in right ventricle (RV) and left ventricle (LV) function, consequently we excluded all patients with prior cardiac surgery procedures. [17,18] The patients were then divided into the following two groups: VATS (n = 20) and thoracotomy (n = 25). Our study was based on retrospective patient data collection from our institutional database. Ethical approval was obtained from the Research Ethics Committee of RWTH-University Aachen, Germany (EK 151/09). The ethical board waived the need for informed consent due to the retrospective nature of the study.
2.2. Echocardiographic measurements
All patients underwent standardized transthoracic echocardiography before and after surgery as part of our routine perioperative clinical care. TTE was performed within 2 weeks before and 2 weeks after the surgery. All echocardiographic measurements were performed in accordance with the European Association of Cardiovascular Imaging and American Society of Echocardiography (ASE) [19,20,21].
Biplane apical four-chamber (4CH) and two-chamber (2CH) views were used for measuring the left ventricular ejection fraction (LVEF). Peak systolic global longitudinal strain average (GLS avg) from left ventricle (LV) was measured in all three standard apical views, using two-dimensional speckle tracking (2D-STE).
RV diameter and area measurements were made in a modified 4CH view. Right ventricular fractional area change (RVFAC) was calculated using the following formula: (end-diastolic area − end-systolic area) / end-diastolic area × 100%. Additional parameters of the RV like RV free-wall GLS (RVFWGLS) were measured in a modified 4CH view.
Tricuspid annular plane systolic excursion (TAPSE) was measured using M-mode in the apical modified 4CH view from minimum to maximum excursion. Tricuspid annular systolic velocity (TASV) was measured using pulsed-wave tissue doppler imaging of the free tricuspid annulus in the 4CH view.
MW measurements and calculations, including global work index (GWI) and global work efficiency, were performed with a specific commercially available processing software (GE Vivid E90 with the EchoPAC workstation) as described by Russell et al. [16]. Blood pressure was determined using a brachial cuff immediately before each TTE.
All echocardiography studies were performed using Vivid E9 (GE Vingmed Ultrasound AS, Horton, Norway), and measurements were performed using EchoPAC version BT 202 (GE Vingmed Ultrasound AS) (Figure 2).
2.3. Surgical procedures
In accordance with our hospital’s surgical standards, all thoracic procedures were performed under general anesthesia using single-lung ventilation and a double-lumen tube. All patients were placed in right or left lateral decubitus position. For postoperative pain management, epidural or serratus plane nerve catheters were used.
Muscle-sparing antero-lateral thoracotomy in the fifth or sixth intercostal space (ICS) was performed as the conventional surgical approach. In contrast, VATS was the was performed as the minimally invasive surgical approach, which involved placing one or two 1–2 cm ports at the 7th or 8th ICS following the midaxillary line and a 3rd port at the same ICS level following the posterior axillary line. In cases requiring the use of the uniportal technique, the incision was made at 6th or 7th ICS following the midaxillary line.
2.4. Laboratory tests
Standard perioperative blood tests, including creatinine, hemoglobin, leucocyte, thrombocyte, lactate dehydrogenase (LDH), aspartate transaminase (AST), and alanine transaminase (ALT) levels, were conducted 1 day before and after surgery.
2.5. Statistical analysis
Categorical variables were expressed as absolute numbers and percentages, whereas continuous variables were expressed as means and standard deviations. All analyses were conducted using R statistics inside the R Studio interface version 4.0.3 (RStudio Team, Boston, MA) in conjunction with the jamovi project (2020) (jamovi computer software, version 2.3.9; JAMovi.org), which may be accessed at https://www.jamovi.org/. Comparisons between groups were conducted using two-tailed Student's t-tests for normally distributed, non-repeated continuous variables. These tests were run with the assumption that the variables were not identical. Two-way analysis of variance was used to examine continuous repeating variables for intra- and intergroup comparisons. We used either the chi square test or Fisher's exact test, where suitable, for the analysis of categorical variables. Moreover, p values were rounded off to three decimal places or presented as numbers with at least one non-zero digit. A p value of <0.05 indicated statistical significance. A post-hoc power analysis was conducted using G * Power3 and tested the difference between two independent group means using a two-tailed test for the result TASV, a medium effect size (d = 0.50) and an alpha of 0.05. [22] The result showed that our study achieves a power of 0.78 with our sample size (thoracotomy n = 25 vs. VATS n = 20).
3. Results
All procedures were performed uneventfully. No significant adverse events or in-hospital mortality occurred. No vasoactive or inotrope drugs were required postoperatively. After screening a total of 187 patients, 142 were subsequently excluded (Figure 1) The final group consisted of 45 patients, among whom 20 (44.4%) underwent VATS and 25 (55.6%) underwent thoracotomy. Lobectomy, anatomical segment resection, and atypical resection were performed in 6 (30%), 4 (20%), and 10 (50%) patients in the VATS group and 15 (60%), 4 (16%), and 6 (24%) patients in the thoracotomy group, respectively (Figure 1). Table 1 summarize the detailed demographic data for the VATS and thoracotomy groups. The two groups were quite similar in age, body mass index (BMI), sex distribution, preoperative comorbidities, laboratory parameters, and predicted in-hospital death rate (Thoracoscore) [23]. The thoracotomy and VATS groups had a mean age of 63 ± 14 and 70 ± 11 years and included 10 and 9 females, respectively.
3.1. Laboratory blood tests
Hemoglobin levels significantly decreased in both groups after surgery (Thoracotomy: 13.20 ± 1.91 vs. 11.30 ± 1.82 mg/dL; p < 0.001; VATS: 13.40 ± 1.36 vs. 12.00 ± 1.74 mg/dL; p < 0.001). However, only the thoracotomy group showed a significant increase in leukocytes (8.04 ± 2.82 vs. 9.98 ± 2.74 103/µL; p < 0.007). No discernible difference in any blood test was observed between the groups (Table 2).
3.2. Echocardiographic findings within the groups
Table 3 shows the echocardiographic parameters within the groups. No significant changes in all measured echocardiographic parameters, except for TAPSE, were observed within the groups after the surgery. Accordingly, the thoracotomy group (n = 25) showed a significant decrease in TAPSE after the surgery (20.80 ± 3.25 vs. 17.90 ± 3.83 mm; p < 0.005; Table 3).
3.3. Echocardiographic findings between groups
On the other hand, significant changes in postoperative RV echocardiography parameters indicating impairment in RV function were found between thoracotomy and VATS groups (TAPSE 17.90 ± 3.80 vs. 20.60 ± 3.50 mm: p < 0.018; TASV: 12.40 ± 2.90 vs. 14.60 ± 2.50 cm/s: p < 0.010; RVFWGLS: −11.50% ± 8.50% vs. −17.50% ± 9.70%; p < 0.033; Table 4).
4. Discussion
The main findings of the present study suggest that RV function deteriorated more significantly after thoracotomy than after VATS. This is shown by the significant decrease in TAPSE, TASV, and RVFWGLS in the thoracotomy group (Table 4). Modifications in RV function were noted despite preservation of LV function, suggesting that the RV/pulmonary vascular unit was the primary target of modifications after lung resection. We showed that pulmonary resection during thoracic surgery (either open or minimally invasive surgery) had no major effect on RV or LV diastolic or systolic function. However, VATS promoted better preservation of RV function than did thoracotomy. In both thoracotomy and VATS groups, no major RV dysfunction following pulmonary resection was observed. Conversely, Reed et al. [24], who did observe major RV dysfunction, concluded that this dysfunction was multifactorial and may solely be attributed to a contractile impairment of the RV. The discrepancy between our results and those shown by Reed et al. [24] may be explained by the fact that we analyzed the postoperative echocardiogram data 2 weeks after the surgery, whereas Reed et al. [24] analyzed the data during the very early postoperative period (postoperative days 1 and 2). A lung resection can cause a reduction in the pulmonary vascular system [25]. This, in turn, can lead to a reduction in the pulmonary vascular cross-sections, which consequently results in pulmonary arterial hypertension and then right heart failure. During thoracotomy and anesthesia, alterations occur in the pulmonary vascular system. Additionally, evidence has shown a rise in intrathoracic pressures [26], which is detrimental to the filling pressure of the RV [25,27]. On the other hand, neither the systolic RV parameters nor RV inflow showed any signs of an identifiable alteration. We hypothesize that the RV afterload would greatly increase in the acute phase after lung resection and that the RV function would deteriorate in the very early postoperative period as the heart struggles to adjust to the increasing afterload. However, after comparing the postoperative RV echocardiographic parameters between the VATS and thoracotomy groups, we found that the VATS group had better RV function preservation than did the thoracotomy group. One possible explanation for this finding could be the sudden establishment of a negative intrathoracic pressure, which has the potential to severely compromise ventricular mechanics [28]. This phenomenon occurs more frequently during abnormal breathing in patients undergoing thoracotomy than in those undergoing VATS due to more severe postoperative pain [29,30].
Our study has been the first to use the novel, non-invasive MW assessment of the LV function after lung resection. MW is a new method for measuring LV performance that has lesser reliance on load than does GLS [31,32]. An increase in preload or afterload may decrease strain while maintaining MW under various physiologic and pathologic situations. MW enables the measurement of global function after adjusting for systolic blood pressure. Despite the independency of the MW from pre- to afterload, we detected no significant changes in the LVMWI or MWE after lung resection in either the thoracotomy or VATS group. However, non-invasive measurements of the RVMW have still not been available, and we were not able to perform RVMW analysis. Examination of RV pressure–volume loops before and after surgery following lobar pulmonary artery clamping convincingly showed an impairment in patients after lung resection under experimental settings [25,33]. Despite this drastic redistribution of pulmonary blood flow during lung resection, one study showed that systemic arterial blood pressure and cardiac output were maintained in the great majority of patients undergoing thoracic surgery even with lobectomy [27]. In a few of individuals, however, pulmonary vascular or RV comorbidity may hinder their ability to adjust appropriately [25,27].
5. Conclusions
Our results showed that LV function was preserved after lung surgery. In contrast, thoracotomy promoted a significantly greater deterioration in RV function than did VATS. Pain associated with abnormal breathing mechanics may have a negative impact on ventricular filling and contractility. This should be investigated prospectively in larger cohorts with longer follow-up durations.
6. Limitations
This study suffers from the typical shortcomings associate with a single-center study. Our study included a small number of patients, which, along with the retrospective analysis, limits the interpretation of our results. Given that none of the TTE measurements were particularly taken for the intended study but rather for clinical examinations as part regular perioperative care protocols, the echocardiography examination time frames were not similar. Given the retrospective nature of our study, patient selection and data collection were susceptible to potential bias. The limited number of patients in our study did not allow us to conduct a sub group analysis to explore the impact of the resected lung volume on the RV and LV function changes.
The complexity of the RV anatomy and physiology, particularly the marked load dependence of RV function, also contributes to measurement variation. However, we excluded individuals with any cardiac structural or valvular disease given that inaccurate LV pressure calculation based on brachial-cuff blood pressure measurements may arise owing to individual anatomical or pathological variations in the artery system.
Given that our study had a maximum follow-up duration of 2 weeks, more research with larger cohorts and longer-term follow-up would be required to make any long-term conclusions. However, due to the fact that all of our patients are oncology patients, and the majority of them required chemotherapy and / or radiation after surgery, and due to the cardiotoxicity of chemotherapy, we were unable to conduct long-term echocardiography studies because it will be impossible to distinguish the cause of the further changes in LV and RV (cardiotoxicity or surgery) in long-term follow-up.
Author Contributions
A.K. and S.L. contributed equally as first authors; R.Z. and M.A.K. contributed equally as last authors; A.K. wrote the first version of the manuscript and drafted it; R.Z. J.S., and M.A.K. concept and design; R.Z., M.F.A., N.H. and A.F.M. resources and administration; A.K., S.L., M.S. data collection; A.K., S.L., N.H., M.A.K. and R.Z. performed echocardiography; A.K., M.A.K. and S.L. conducting the study; A.K., S.L., N.H. and R.Z. echocardiography analysis; A.K., S.L., R.Z. and M.A.K. interpretation of data; A.K., S.L., R.Z., M.S. and A.F.M.; visualization; A.K.. and S.L. statistical analysis; J.S., R.Z. and M.A.K. supervision; A.K., S.L., R.Z. and M.A.K. methodology; all authors critically reviewed the manuscript for intellectual content. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of RWTH-University Aachen, Germany (EK 151/09).
Informed Consent Statement
Patient consent was waived by the ethical board due to the retrospective nature of the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors thank Payam Akhyari, Department of Cardiac Surgery, University Hospital of RWTH Aachen, Germany, for critical review of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rana, J.S.; Khan, S.S.; Lloyd-Jones, D.M.; Sidney, S. Changes in mortality in top 10 causes of death from 2011 to 2018. J Gen Intern Med 2021, 36, 2517–2518. [Google Scholar] [CrossRef]
- Siegel, R.; Ma, J.; Zou, Z.; Jemal, A. Cancer statistics, 2014. CA Cancer J Clin 2014, 64, 9–29. [Google Scholar] [CrossRef] [PubMed]
- Howington, J.A.; Blum, M.G.; Chang, A.C.; Balekian, A.A.; Murthy, S.C. Treatment of stage I and II non-small cell lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143, e278S–e313S. [Google Scholar] [CrossRef]
- Sangha, R.; Price, J.; Butts, C.A. Adjuvant therapy in non-small cell lung cancer: current and future directions. Oncologist 2010, 15, 862–872. [Google Scholar] [CrossRef] [PubMed]
- Al-Ameri, M.; Bergman, P.; Franco-Cereceda, A.; Sartipy, U. Video-assisted thoracoscopic versus open thoracotomy lobectomy: a Swedish nationwide cohort study. J Thorac Dis 2018, 10, 3499–3506. [Google Scholar] [CrossRef]
- Batihan, G.; Ceylan, K.C.; Usluer, O.; Kaya, Ş.Ö. Video-assisted thoracoscopic surgery vs thoracotomy for non-small cell lung cancer greater than 5 cm: is VATS a feasible approach for large tumors? J Cardiothorac Surg 2020, 15, 261–261. [Google Scholar] [CrossRef]
- Pinsky, M.R. Cardiopulmonary interactions: physiologic basis and clinical applications. Ann Am Thorac Soc 2018, 15, S45–S48. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, S.S. Heart-lung interactions in health and disease. Am J Med Sci 1987, 294, 451–461. [Google Scholar] [CrossRef] [PubMed]
- Vainshelboim, B.; Fox, B.D.; Saute, M.; Sagie, A.; Yehoshua, L.; Fuks, L.; Schneer, S.; Kramer, M.R. Limitations in exercise and functional capacity in long-term postpneumonectomy patients. J Cardiopulm Rehabil Prev 2015, 35, 56–64. [Google Scholar] [CrossRef]
- Wang, Z.; Yuan, J.; Chu, W.; Kou, Y.; Zhang, X. Evaluation of left and right ventricular myocardial function after lung resection using speckle tracking echocardiography. Medicine (Baltimore) 2016, 95, e4290–e4290. [Google Scholar] [CrossRef]
- Pedoto, A.; Amar, D. Right heart function in thoracic surgery: role of echocardiography. Curr Opin Anaesthesiol 2009, 22, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Haddad, F.; Hunt, S.A.; Rosenthal, D.N.; Murphy, D.J. Right ventricular function in cardiovascular disease, part I: Anatomy, physiology, aging, and functional assessment of the right ventricle. Circulation 2008, 117, 1436–1448. [Google Scholar] [CrossRef]
- Peyrou, J.; Parsaï, C.; Chauvel, C.; Simon, M.; Dehant, P.; Abergel, E. Echocardiographic assessment of right ventricular systolic function in a population of unselected patients before cardiac surgery: a multiparametric approach is necessary. Arch Cardiovasc Dis 2014, 107, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Urheim, S.; Edvardsen, T.; Torp, H.; Angelsen, B.; Smiseth, O.A. Myocardial strain by Doppler echocardiography. Validation of a new method to quantify regional myocardial function. Circulation 2000, 102, 1158–1164. [Google Scholar] [CrossRef] [PubMed]
- Boe, E.; Skulstad, H.; Smiseth, O.A. Myocardial work by echocardiography: a novel method ready for clinical testing. Eur Heart J Cardiovasc Imaging 2019, 20, 18–20. [Google Scholar] [CrossRef]
- Russell, K.; Eriksen, M.; Aaberge, L.; Wilhelmsen, N.; Skulstad, H.; Remme, E.W.; Haugaa, K.H.; Opdahl, A.; Fjeld, J.G.; Gjesdal, O.; et al. A novel clinical method for quantification of regional left ventricular pressure-strain loop area: a non-invasive index of myocardial work. Eur Heart J 2012, 33, 724–733. [Google Scholar] [CrossRef]
- Singh A, Huang X, Dai L, et al. Right ventricular function is reduced during cardiac surgery independent of procedural characteristics, reoperative status, or pericardiotomy. J Thorac Cardiovasc Surg. 2020;159(4):1430-1438.e4. 1: Surg. 2020;159(4). [CrossRef]
- Steffen HJ, Kalverkamp S, Zayat R, et al. Is Systolic Right Ventricular Function Reduced after Thoracic Non-Cardiac Surgery? A Propensity Matched Echocardiographic Analysis. Ann Thorac Cardiovasc Surg. 2018;24(5):238-246. [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 2015, 28, 1–39.e14. [Google Scholar] [CrossRef]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for performing a comprehensive transthoracic echocardiographic examination in adults: recommendations from the American Society of Echocardiography. J Am Soc Echocardiogr 2019, 32, 1–64. [Google Scholar] [CrossRef]
- Galderisi, M.; Cosyns, B.; Edvardsen, T.; Cardim, N.; Delgado, V.; Di Salvo, G.; Donal, E.; Sade, L.E.; Ernande, L.; Garbi, M.; et al. Standardization of adult transthoracic echocardiography reporting in agreement with recent chamber quantification, diastolic function, and heart valve disease recommendations: an expert consensus document of the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 2017, 18, 1301–1310. [Google Scholar] [CrossRef]
- Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175-191. [CrossRef]
- Falcoz, P.E.; Conti, M.; Brouchet, L.; Chocron, S.; Puyraveau, M.; Mercier, M.; Etievent, J.P.; Dahan, M. The Thoracic Surgery Scoring System (Thoracoscore): risk model for in-hospital death in 15,183 patients requiring thoracic surgery. J Thorac Cardiovasc Surg 2007, 133, 325–332. [Google Scholar] [CrossRef]
- Reed, C.E.; Spinale, F.G.; Crawford, F.A., Jr. Effect of pulmonary resection on right ventricular function. Ann Thorac Surg 1992, 53, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Shelley, B.; Glass, A.; Keast, T.; McErlane, J.; Hughes, C.; Lafferty, B.; Marczin, N.; McCall, P. Perioperative cardiovascular pathophysiology in patients undergoing lung resection surgery: a narrative review. Br J Anaesth 2023, 130, e66–e79. [Google Scholar] [CrossRef] [PubMed]
- Lansdorp, B.; Hofhuizen, C.; van Lavieren, M.; van Swieten, H.; Lemson, J.; van Putten, M.J.; van der Hoeven, J.G.; Pickkers, P. Mechanical ventilation-induced intrathoracic pressure distribution and heart-lung interactions*. Crit. Care Med. 2014, 42, 1983–1990. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.F.; Ueda, K. Pulmonary hypertension in thoracic surgical patients. Curr Opin Anaesthesiol 2010, 23, 25–33. [Google Scholar] [CrossRef]
- Koshino, Y.; Villarraga, H.R.; Orban, M.; Bruce, C.J.; Pressman, G.S.; Leinveber, P.; Saleh, H.K.; Konecny, T.; Kara, T.; Somers, V.K.; et al. Changes in left and right ventricular mechanics during the Mueller maneuver in healthy adults. Circ Cardiovasc Imaging 2010, 3, 282–289. [Google Scholar] [CrossRef]
- Wei, X.; Yu, H.; Dai, W.; Mu, Y.; Wang, Y.; Liao, J.; Peng, L.; Han, Y.; Li, Q.; Shi, Q. Patient-reported outcomes of video-assisted thoracoscopic surgery versus thoracotomy for locally advanced lung cancer: a longitudinal cohort study. Ann Surg Oncol 2021, 28, 8358–8371. [Google Scholar] [CrossRef]
- Homma, T.; Shimada, Y.; Tanabe, K. Decreased postoperative complications, neuropathic pain and epidural anesthesia-free effect of uniportal video-assisted thoracoscopic anatomical lung resection: a single-center initial experience of 100 cases. J Thorac Dis 2022, 14, 3154–3166. [Google Scholar] [CrossRef]
- D'Andrea, A.; Sperlongano, S.; Formisano, T.; Tocci, G.; Cameli, M.; Tusa, M.; Novo, G.; Corrado, G.; Ciampi, Q.; Citro, R.; et al. Stress echocardiography and strain in aortic regurgitation (SESAR protocol): left ventricular contractile reserve and myocardial work in asymptomatic patients with severe aortic regurgitation. Echocardiography (Mount Kisco, N.Y.) 2020, 37, 1213–1221. [Google Scholar] [CrossRef]
- D'Andrea, A.; Radmilovic, J.; Carbone, A.; Mandoli, G.E.; Santoro, C.; Evola, V.; Bandera, F.; D'Ascenzi, F.; Bossone, E.; Galderisi, M.; et al. Speckle tracking evaluation in endurance athletes: the "optimal" myocardial work. Int J Cardiovasc Imaging 2020, 36, 1679–1688. [Google Scholar] [CrossRef]
- Yerebakan, C.; Klopsch, C.; Niefeldt, S.; Zeisig, V.; Vollmar, B.; Liebold, A.; Sandica, E.; Steinhoff, G. Acute and chronic response of the right ventricle to surgically induced pressure and volume overload--an analysis of pressure-volume relations. Interact. Cardiovasc Thorac Surg 2010, 10, 519–525. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of the study: patient collection.
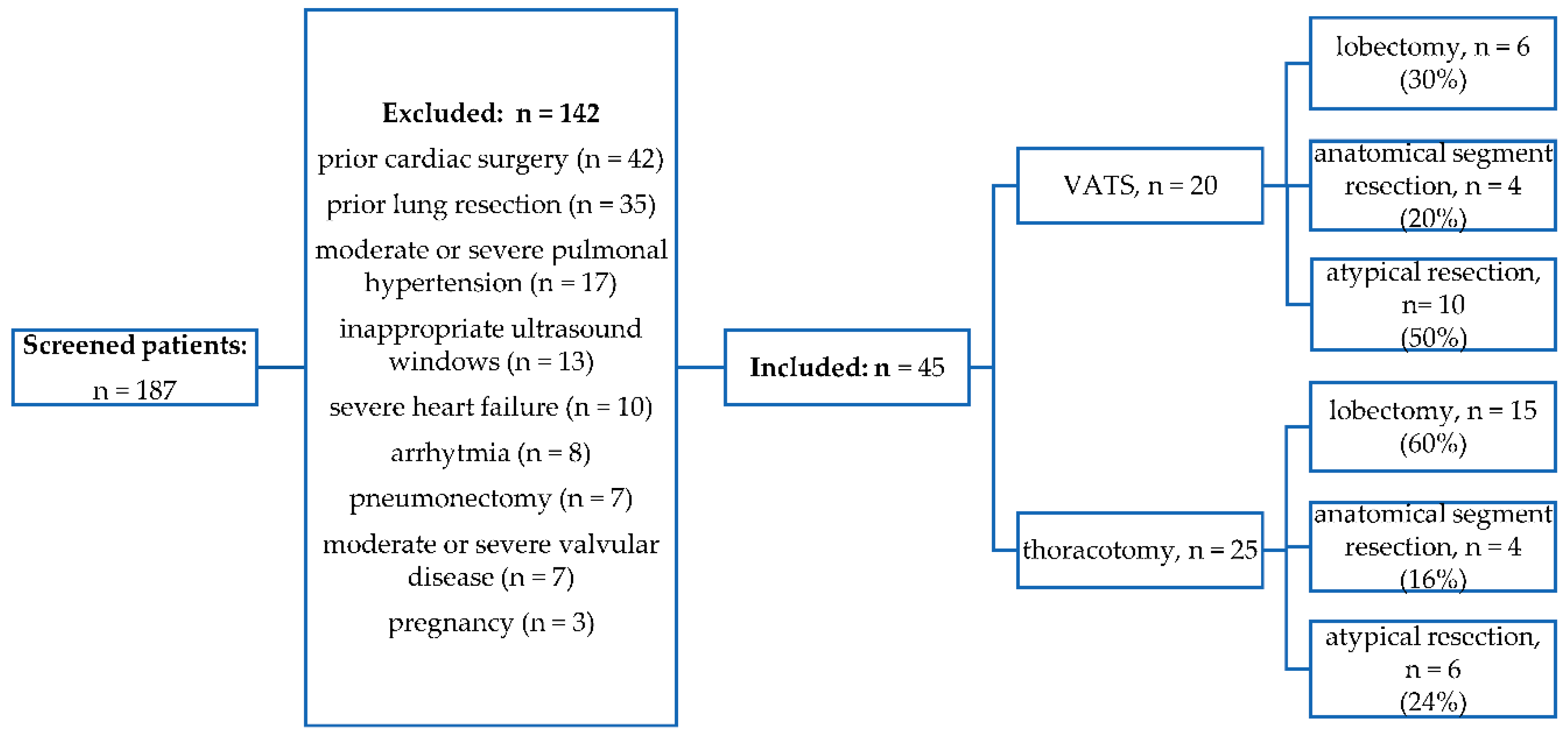
Figure 2.
Exemplary demonstration of selected echocardiography studies. (A) GLS of the LV, measured in all three standard apical views; (B) peak systolic strain and GMWI (bull’s eye) estimation; (C) TASV estimated from TDI; and (D) GLS of the RV measured in the 4CH view. GLS, global longitudinal strain; LV, left ventricle; GMWI, global myocardial work index; TASV, tricuspid annular systolic velocity; TDI, tissue doppler imaging; RV, right ventricle; 4CH, four-chamber.
Figure 2.
Exemplary demonstration of selected echocardiography studies. (A) GLS of the LV, measured in all three standard apical views; (B) peak systolic strain and GMWI (bull’s eye) estimation; (C) TASV estimated from TDI; and (D) GLS of the RV measured in the 4CH view. GLS, global longitudinal strain; LV, left ventricle; GMWI, global myocardial work index; TASV, tricuspid annular systolic velocity; TDI, tissue doppler imaging; RV, right ventricle; 4CH, four-chamber.
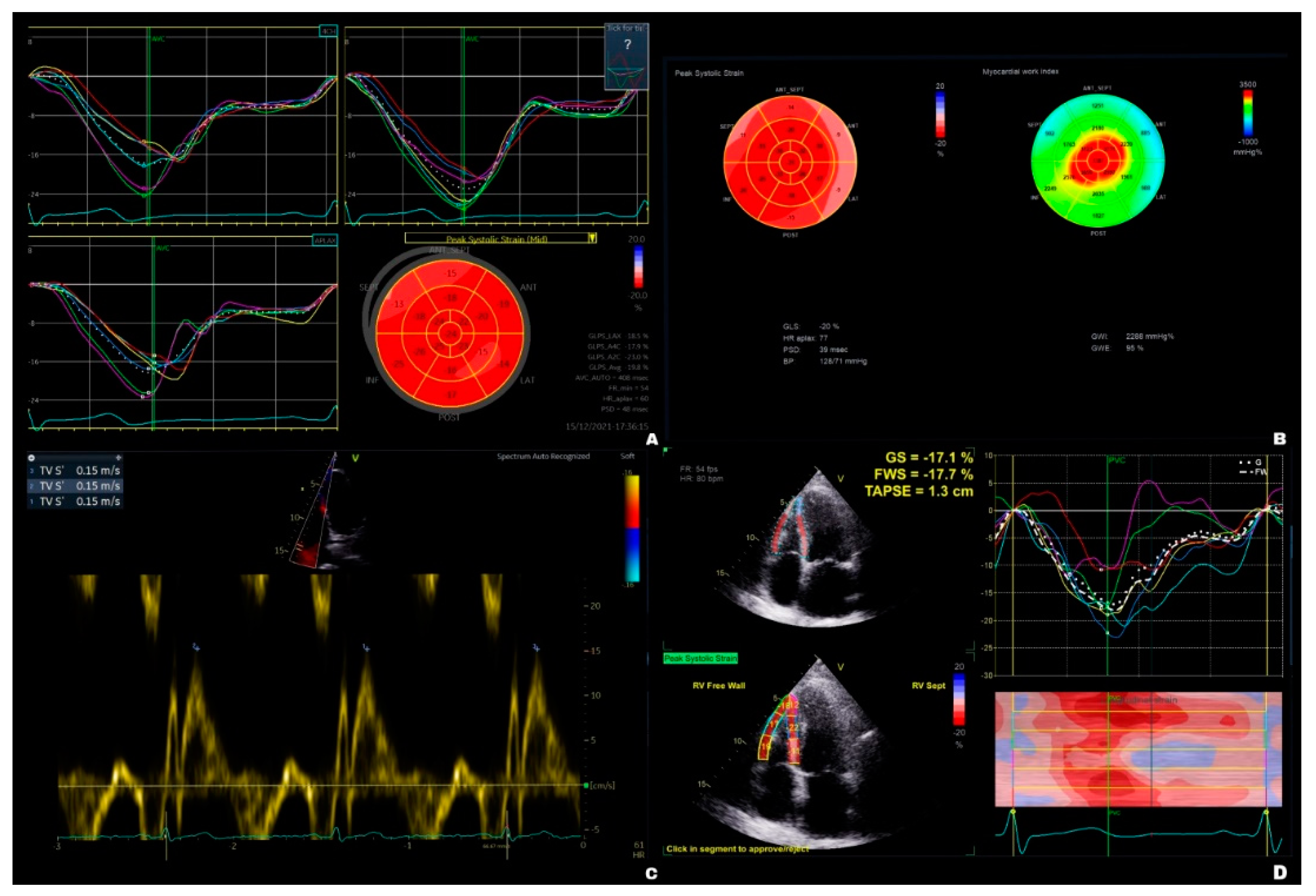

Table 1.
Patient demographics.
| Thoracotomy (n = 25) | VATS (n = 20) | p values | |
|---|---|---|---|
| Mean age, years | 63 ± 14 | 70 ± 11 | 0.10 |
| Female, n (%) | 10 (40) | 9 (45) | 0.74 |
| COPD ≥ GOLD III, n (%) | 2 (8) | 0 (0) | 0.06 |
| PAD, n (%) | 3 (12) | 1 (5) | 0.62 |
| Diabetes mellitus, n (%) | 3 (12) | 6 (20) | 0.16 |
| Hypertension, n (%) | 17 (68) | 15 (75) | 0.61 |
| Smoking, n (%) | 15 (60) | 8 (40) | 0.18 |
| KDIGO ≥ G3, n (%) | 3 (12) | 3 (15) | 0.37 |
| NYHA ≥ III, n (%) | 3 (12) | 1 (5) | 0.59 |
| Non-cardiopulmonary prior thoracic surgery, n (%) | 3 (12) | 0 (0) | 0.49 |
| BMI (kg/m2) | 26.9 ± 4.12 | 25.2 ± 4.36 | 0.13 |
| Thoracoscore PPD, (%) | 2.67 ± 2.75 | 2.67 ± 2.52 | 0.87 |
| Creatinine (mg/dL) | 0.96 ± 0.41 | 0.88 ± 0.2 | 0.85 |
| Hemoglobin (mg/dL) | 13.00 ± 1.91 | 13.70 ± 1.36 | 0.59 |
| Leukocytes (103/µL) | 7.30 ± 2.82 | 8.05 ± 3.28 | 0.27 |
| Thrombocytes (103/µL) | 246 ± 47.2 | 276 ± 92.1 | 0.13 |
| LDH (U/L) | 198 ± 30.9 | 210 ± 64.7 | 0.74 |
| AST (U/L) | 23 ± 14.7 | 24 ± 5.39 | 0.88 |
| ALT (U/L) | 19 ± 16.4 | 18 ± 7.29 | 0.57 |
VATS, video-assisted thoracoscopic surgery; COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; PAD, peripheral arterial disease; Diabetes mellitus included patients with oral antidiabetic drugs or insulin therapy; KDIGO, Kidney Disease Improving Global Outcomes; NYHA, New York Heart Association; BMI, body mass index; PPD, Predicted perioperative death rate; LDH, lactate dehydrogenase; AST, aspartate transaminase; ALT, alanine transaminase. Bold entries indicate significance.
Table 2.
Comparison of laboratory blood tests between the groups.
| Thoracotomy (n = 25) | VATS (n = 20) | VATS vs. thoracotomy postoperative |
|||||
| Preoperative | Postoperative | p values | Preoperative | Postoperative | p values | p values | |
| Creatinine (mg/dL) | 1.00 ± 0.41 | 1.02 ± 0.76 | 0.989 | 0.92 ± 0.20 | 0.84 ± 0.23 | 0.076 | 0.328 |
| Hemoglobin (mg/dL) | 13.20 ± 1.91 | 11.30 ± 1.82 | < 0.001 | 13.40 ± 1.36 | 12.00 ± 1.74 | < 0.001 | 0.631 |
| Leukocytes (103/µL) | 8.04 ± 2.82 | 9.98 ± 2.74 | 0.007 | 8.89 ± 3.28 | 9.51 ± 4.42 | 0.766 | 0.668 |
| Thrombocytes (103/µL) | 249.00 ± 47.20 | 224.00 ± 82.10 | 0.236 | 297.00 ± 92.00 | 224.00 ± 98.90 | 0.087 | 0.175 |
| LDH (U/L) | 206.00 ± 30.90 | 209.00 ± 50.60 | 0.992 | 220.00 ± 64.70 | 210.00 ± 41.80 | 0.871 | 0.944 |
| AST (U/L) | 26.40 ± 14.70 | 26.30 ± 13.00 | 1.000 | 23.50 ± 5.39 | 31.90 ± 8.40 | 0.663 | 0.576 |
| ALT (U/L) | 24.90 ± 16.40 | 24.30 ± 13.60 | 0.992 | 20.10 ± 7.29 | 19.50 ± 11.20 | 0.994 | 0.214 |
VATS, video-assisted thoracoscopic surgery; LDH, lactate dehydrogenase; AST, aspartate transaminase; ALT, alanine transaminase. Bold entries indicate significance.
Table 3.
Comparison of echocardiographic changes within the groups.
| Thoracotomy (n = 25) | VATS (n = 20) | |||||
| Preoperative | Postoperative | p values | Preoperative | Postoperative | p values | |
| LVIDd (cm) | 4.44 ± 0.55 | 4.84 ± 0.74 | 0.101 | 4.43 ± 0.82 | 4.53 ± 0.90 | 0.961 |
| LVIDs (cm) | 3.20 ± 0.74 | 3.50 ± 0.84 | 0.343 | 3.18 ± 0.92 | 3.31 ± 0.93 | 0.883 |
| LVEDV (mL) | 103.00 ± 17.90 | 106.00 ± 15.20 | 0.991 | 101.00 ± 20.30 | 100.00 ± 22.20 | 0.992 |
| LVESV (mL) | 41.80 ± 11.10 | 45.20 ± 11.30 | 0.832 | 45.00 ± 13.70 | 45.10 ± 12.90 | 1.000 |
| LVEF (%) | 59.40 ± 6.26 | 59.2 ± 7.43 | 0.997 | 56.3 ± 7.04 | 56.50 ± 7.70 | 0.994 |
| CO (L/min) | 5.31 ± 1.19 | 5.66 ± 1.30 | 0.606 | 4.90 ± 1.23 | 4.97 ± 1.09 | 0.963 |
| GLSLV avg. (%) | -17.40 ± 4.14 | -16.7 ± 4.13 | 0.813 | -17.5 ± 2.78 | -16.10 ± 4.46 | 0.532 |
| GWILV | 1617 ± 529 | 1637 ± 462 | 0.997 | 1778 ± 580 | 1505 ± 636 | 0.074 |
| GWELV (%) | 90.90 ± 9.05 | 90.60 ± 7.56 | 0.991 | 93.20 ± 5.72 | 89.30 ± 10.70 | 0.068 |
| RVIDd (cm) | 3.13 ± 0.63 | 3.02 ± 0.67 | 0.674 | 2.90 ± 0.45 | 2.81 ± 0.65 | 0.926 |
| RVIDs (cm) | 1.85 ± 0.46 | 1.90 ± 0.51 | 0.968 | 1.64 ± 0.40 | 1.71 ± 0.41 | 0.441 |
| RVD1basal (cm) | 3.89 ± 0.79 | 3.69 ± 0.73 | 0.714 | 3.79 ± 0.63 | 3.81 ± 0.72 | 0.992 |
| RVD3long (cm) | 6.92 ± 0.79 | 7.20 ± 0.59 | 0.356 | 6.87 ± 0.97 | 6.81 ± 0.86 | 0.923 |
| RVFAC (%) | 51.2 ± 9.62 | 51.40 ± 7.55 | 0.997 | 47.90 ± 10.60 | 48.20 ± 7.33 | 0.994 |
| PASP (mm Hg) | 21.00 ± 8.42 | 21.00 ± 9.01 | 0.992 | 16.90 ± 6.59 | 19.70 ± 9.38 | 0.482 |
| TAPSE (mm) | 20.80 ± 3.25 | 17.90 ± 3.83 | 0.005 | 20.60 ± 3.79 | 20.60 ± 3.51 | 1.000 |
| TASV (cm/s) | 13.90 ± 3.45 | 12.40 ± 2.86 | 0.184 | 14.10 ± 2.25 | 14.60 ± 2.54 | 0.874 |
| RV4CHGLS (%) | -16.80 ± 3.28 | -16.00 ± 4.46 | 0.911 | -16.70 ± 6.46 | -16.40 ± 4.91 | 0.992 |
| RVFWGLS (%) | -17.20 ± 9.07 | -11.50 ± 8.50 | 0.133 | -18.60 ± 10.30 | -17.50 ± 9.71 | 0.983 |
VATS, video-assisted thoracoscopic surgery; LVIDd, Left ventricular internal diameter end diastole; LVIDs, Left ventricular internal diameter end systole; LVEDV, Left ventricular end-diastolic volume; LVESV, Left ventricular end-systolic volume; LVEF, left ventricular ejection fraction; CO, cardiac output; GLSLVavg., global longitudinal strain left ventricular average; GWI LV, global work index left ventricle; GWELV, global work efficiency left ventricle; RVIDd, right ventricular internal diameter at end diastole; RVIDs, right ventricular internal diameter at end systole; RVD1 basal, right ventricular basal diameter at end-diastole; RVD3 long, right ventricular longitudinal diameter at end-diastole; RVFAC, right ventricular fractional area change; PASP, pulmonary arterial systolic pressure; TAPSE, tricuspid annular plane systolic excursion; TASV, tricuspid annular systolic velocity; RV4CHGLS, right ventricular four-chamber global longitudinal strain; RVFWGLS, right ventricular free-wall global longitudinal strain. Bold entries indicate significance.
Table 4.
Comparison of echocardiographic changes between the groups.
| Thoracotomy | VATS | p values | |
|---|---|---|---|
| preoperative | |||
| LVIDd (cm) | 4.40 ± 0.60 | 4.40 ± 0.80 | 0.975 |
| LVIDs (cm) | 3.20 ± 0.70 | 3.20 ± 0.90 | 0.921 |
| LVEDV (mL) | 102.70 ± 17.90 | 100.60 ± 20.30 | 0.712 |
| LVESV (mL) | 41.80 ± 11.10 | 45.00 ± 13.70 | 0.391 |
| LVEF (%) | 59.40 ± 6.30 | 56.30 ± 7.00 | 0.130 |
| CO (L/min) | 5.30 ± 1.20 | 4.90 ± 1.20 | 0.264 |
| LVGLS (%) | -17.40 ± 4.10 | -17.50 ± 2.80 | 0.922 |
| LVGWI | 1616.80 ± 529.50 | 1778.00 ± 580.00 | 0.347 |
| LVGWE (%) | 90.90 ± 9.10 | 93.20 ± 5.70 | 0.344 |
| RVIDd (cm) | 3.10 ± 0.60 | 2.90 ± 0.40 | 0.178 |
| RVIDs (cm) | 1.80 ± 0.50 | 1.60 ± 0.40 | 0.135 |
| RVD1basal (cm) | 3.90 ± 0.80 | 3.80 ± 0.60 | 0.625 |
| RVD3basal (cm) | 6.90 ± 0.80 | 6.90 ± 1.00 | 0.823 |
| RVFAC (%) | 51.20 ± 9.60 | 47.90 ± 10.60 | 0.283 |
| PASP (mm Hg) | 21.00 ± 8.40 | 16.90 ± 6.60 | 0.095 |
| TAPSE (mm) | 20.80 ± 3.20 | 20.60 ± 3.80 | 0.857 |
| TASV (cm/s) | 13.90 ± 3.50 | 14.10 ± 2.20 | 0.835 |
| RV4CHGLS (%) | -16.80 ± 3.30 | -16.70 ± 6.50 | 0.957 |
| RVFWGLS (%) | -17.20 ± 9.10 | -18.60 ± 10.30 | 0.647 |
| postoperative | |||
| LVIDd (cm) | 4.80 ± 0.70 | 4.50 ± 0.90 | 0.228 |
| LVIDs (cm) | 3.50 ± 0.80 | 3.30 ± 0.90 | 0.481 |
| LVEDV (mL) | 105.90 ± 15.20 | 100.00 ± 22.20 | 0.313 |
| LVESV (mL) | 45.20 ± 11.30 | 45.10 ± 12.90 | 0.993 |
| LVEF (%) | 59.20 ± 7.40 | 56.50 ± 7.70 | 0.249 |
| CO (L/min) | 5.70 ± 1.30 | 5.00± 1.10 | 0.072 |
| LVGLS (%) | -16.70 ± 4.10 | -16.10 ± 4.50 | 0.670 |
| LVGWI | 1636.80 ± 462.00 | 1504.90 ± 636.40 | 0.448 |
| LVGWE (%) | 90.60 ± 7.60 | 86.30 ± 10.60 | 0.141 |
| RVIDd (cm) | 3.00 ± 0.70 | 2.80 ± 0.60 | 0.329 |
| RVIDs (cm) | 1.90 ± 0.50 | 1.70 ± 0.40 | 0.212 |
| RVD1basal (cm) | 3.70 ± 0.70 | 3.80 ± 0.70 | 0.597 |
| RVD3basal (cm) | 7.20 ± 0.60 | 6.80 ± 0.90 | 0.093 |
| RVFAC (%) | 51.40 ± 7.50 | 48.20 ± 7.30 | 0.174 |
| PASP (mm Hg) | 21.00 ± 9.00 | 19.70 ± 9.40 | 0.664 |
| TAPSE (mm) | 17.90 ± 3.80 | 20.60 ± 3.50 | 0.018 |
| TASV (cm/s) | 12.40 ± 2.90 | 14.60 ± 2.50 | 0.010 |
| RV4CHGLS (%) | -16.00 ± 4.50 | -16.40 ± 4.90 | 0.787 |
| RVFWGLS (%) | -11.50 ± 8.50 | -17.50 ± 9.70 | 0.033 |
VATS, video-assisted thoracoscopic surgery; LVIDd, Left ventricular internal diameter end diastole; LVIDs, Left ventricular internal diameter end systole; LVEDV, Left ventricular end-diastolic volume; LVESV, Left ventricular end-systolic volume; LVEF, left ventricular ejection fraction; CO, cardiac output; GLSLVavg., global longitudinal strain left ventricular average; GWILV, global work index left ventricle; GWELV, global work efficiency left ventricle; RVIDd, right ventricular internal diameter at end diastole; RVIDs, right ventricular internal diameter at end systole; RVD1 basal, right ventricular basal diameter at end-diastole; RVD3 long, right ventricular longitudinal diameter at end-diastole; RVFAC, right ventricular fractional area change; PASP, pulmonary arterial systolic pressure; TAPSE, tricuspid annular plane systolic excursion; TASV, tricuspid annular systolic velocity; RV4CHGLS, right ventricular four-chamber global longitudinal strain; RVFWGLS, right ventricular free-wall global longitudinal strain. Bold entries indicate significance.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



