
Submitted:
02 August 2023
Posted:
03 August 2023
You are already at the latest version
Abstract
This study aimed to evaluate the diagnostic roles of various immunohistochemical markers in urothelial carcinoma in situ (uCIS) through a meta-analysis and review of diagnostic test accuracy. Immunohistochemical markers CK20, CD44, AMACR, and p53 were evaluated in the present study. We analyzed the expression rates of immunohistochemical markers and compared their diagnostic accuracies. The estimated expression rates were 0.803 (95% confidence interval [CI]: 0.726–0.862), 0.142 (95% CI: 0.033–0.449), 0.824 (95% CI: 0.720–0.895), and 0.600 (95% CI: 0.510–0.683) for CK20, CD44, AMACR, and p53, respectively. In the comparison between uCIS and reactive/normal urothelium, the expression of CK20, AMACR, and p53 in uCIS was significantly higher than in reactive/normal urothelium. CD44 showed significantly lower expression in uCIS than in the reactive/normal urothelium. Among the markers, AMACR had the highest sensitivity, specificity, and diagnostic odds ratio. The AUC on SROC was the highest for CK20. In conclusion, immunohistochemical markers, such as CK20, CD44, AMACR, and p53, can be useful in differentiating uCIS from reactive/normal urothelium.
Keywords:
urothelial carcinoma in situ
; immunohistochemistry
; meta-analysis
; diagnostic test accuracy review
1. Introduction
Urothelial carcinoma in situ (uCIS) is defined as the flat proliferation of high-grade malignant cells without papillar formation. Although uCIS is most common in the urinary bladder, it can occur throughout the urinary tract. Among urothelial malignancies, the incidence of uCIS is estimated at 1–3% [1]. The clinical implications of uCIS are well understood. uCIS is a non-muscle-invasive UC that has the potential to progress to an invasive lesion. uCIS is associated with an increased risk of recurrence [2]. In addition, the finding of uCIS indicates that there may be high-grade papillary or invasive urothelial carcinoma in the remaining tissue. It has been reported that 50–60% of patients with T1 or higher bladder cancer have co-occurring CIS [1]. Bacillus Calmette-Guerin (BCG) therapy is the mainstay of uCIS treatment [3]. In this case, residual urothelial lesions or changes in the urothelium may affect the diagnosis, for example, subsequent recurrence. Differential lesions may include reactive urothelium. Histological and cytological differentiation can be challenging; therefore, ancillary tests can be helpful. Immunohistochemical (IHC) staining, which is performed in many pathology laboratories, may be useful. Common IHC markers used in daily practice include cytokeratin CK20 and CD44. In addition, some studies have suggested that p53 and Ki-67 may be helpful [4,5,6,7,8]. In uCIS, CK20 expression may appear to diffuse to full thickness, and CD44 may be expressed in the basal layer [4,5,6,7,8,9]. However, this expression pattern is inconsistent across all cases, which can present diagnostic challenges. This study aimed to investigate the usefulness of IHC markers through meta-analysis and diagnostic test accuracy review of published articles. In this study, IHC markers, including CK20, CD44, AMACR, and p53, were evaluated. The expression rates of IHC markers were estimated and compared between uCIS and reactive/normal urothelium.
2. Materials and Methods
2.1. Literature search and selection criteria
Relevant articles were obtained by searching the PubMed and MEDLINE databases on April 15, 2023. The search terms used were ‘urothelial carcinoma in situ,’ ‘immunohistochemistry or immunohistochemical,’ and ‘CK20 or CD44 or AMACR or p53.’ The titles and abstracts of all returned articles were screened for exclusion. Review articles were screened to identify additional eligible studies. English-language studies regarding CK20, CD44, AMACR, and p53 IHC expression in human uCIS were included. Case reports and review articles were excluded.
2.2. Data extraction
Twenty-five articles were included and reviewed in this meta-analysis [4,6,7,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30]. From eligible studies, we collected the following information: first author’s name, publication date, study location, number of patients and immunohistochemical markers analyzed, and expression rates of lesions. Disagreements were resolved by consensus.
2.3. Statistical analyses
To perform the meta-analysis, all data were analyzed using the Comprehensive Meta-Analysis software package (Biostat, Englewood, NJ, USA). The immunohistochemical expressions of CK20, CD44, AMACR, and p53 in uCIS and reactive/normal urothelium were investigated in eligible studies. Because the eligible studies used various antibodies and evaluation criteria for various populations, a random-effects model was more suitable than a fixed-effects model. Heterogeneous and sensitivity analyses were conducted to assess the heterogeneity of eligible studies and the impact of each study on the combined effect, respectively. Heterogeneity between studies was checked using the Q and I2 statistics and demonstrated p-values. To assess publication bias, Begg’s funnel plot and Egger’s test were performed. Statistical significance was set at p < 0.05.
Moreover, a diagnostic test accuracy review was performed using the Meta-Disc program (version 1.4) (Unit of Clinical Biostatics, Ramon y Cajal Hospital, Madrid, Spain) [31]. Pooled sensitivity and specificity were gathered sensitivity and specificity from each eligible study, and forest plots were obtained. The summary receiver operating characteristic (SROC) curve was initially constructed by plotting the ‘sensitivity’ and ‘1-specificity’ of each study, and curve fitting was performed through linear regression using the Littenberg and Moses linear model [32]. Because heterogeneity by evaluation criteria was present, the accuracy data were pooled by fitting the SROC curve and measuring the area under the curve (AUC). An AUC close to 1 is considered a perfect test, and an AUC close to 0.5 is considered a poor test. In addition, the diagnostic odds ratio (OR) was calculated using Meta-Disc software.
3. Results
3.1. Selection and characteristics of studies
A total of 107 studies were found in the database search. In the review, 115 reports were excluded due to insufficient information. The remaining reports were excluded because they studied other diseases (n = 20), were non-original articles (n = 18), used animals or cell lines (n = 7), or were non-English (n = 2). Twenty-five articles were included in this meta-analysis and DTA review (Figure 1 and Table 1).
3.2. Immunohistochemical expression rates in urothelial carcinoma in situ
Immunohistochemical expression rates of CK20, CD44, AMACR, and p53 were 0.803 (95% CI: 0.726–0.862), 0.142 (95% CI: 0.033–0.449), 0.824 (95% CI: 0.720–0.895), and 0.600 (95% CI: 0.510–0.683) in uCIS, respectively (Table 2). Next, the immunohistochemical expression rates were compared between uCIS and the reactive/normal urothelium. The expressions of CK20, AMACR, and p53 were significantly higher in uCIS than in reactive/normal urothelium (OR: 71.313, 95% CI: 30.176–168.530; OR 142.931, 95% CI: 31.109–656.697; and OR 16.774, 95% CI: 6.713–41.916, respectively; Table 3). The odds ratio of CD44 expression between uCIS and reactive/normal urothelium was 0.016 (95% CI: 0.006–0.043).
3.3. Diagnostic test accuracy review of immunohistochemical markers in urothelial carcinoma in situ
The evaluated parameters of the DTA review were sensitivity, specificity, diagnostic OR, and AUC on the SROC. The pooled sensitivities of CK20, CD44, AMACR, and p53 were 0.937 (95% CI: 0.910–0.957), 0.865 (95% CI: 0.803–0.913), 0.984 (95% CI: 0.915–1.000), and 0.843 (95% CI: 0.794–0.884), respectively (Table 4). The pooled specificities of CK20, CD44, AMACR, and p53 were 0.773 (95% CI: 0.735–0.809), 0.767 (95% CI: 0.698–0.827), 0.829 (95% CI: 0.725–0.906), and 0.657 (95% CI: 0.607–0.705), respectively. The diagnostic OR of CK20, CD44, AMACR, and p53 were 77.22 (95% CI: 30.17–172.85), 61.11 (95% CI: 23.08–161.81), 142.93 (95% CI: 31.11–656.70), and 17.17 (95% CI: 6.72–43.87), respectively. The AUC on the SROC of CK20, CD44, AMACR, and p53 were 0.942, 0.940, 0.770, and 0.711, respectively.
4. Discussion
Flat urothelial lesions include uCIS and reactive urothelium [7]. Cases that are difficult to differentiate can be aided by IHC staining. In daily practice, CK20 and CD44 are useful IHC markers [11]. In uCIS, CK20 was used as a positive marker and CD44 as a negative marker. The reactive urothelium shows the opposite IHC pattern. However, there are cases where differentiation is difficult, even with IHC staining. To the best of our knowledge, the present study is the first DTA review to compare immunohistochemical markers between uCIS and reactive/normal urothelium.
Urothelial carcinoma can be divided into non-muscle-invasive urothelial carcinoma (pathologic stages Ta, T1, and Tis) and muscle-invasive urothelial carcinoma (pathologic stage T2 or higher). Among non-muscle-invasive UCs, those with a flat growth pattern and no subepithelial invasion will be diagnosed with uCIS. The incidence of uCIS is extremely low compared to that of papillary urothelial carcinoma [30]. There are important differences in the treatment of urothelial carcinoma based on muscle invasion. Non-muscle-invasive urothelial carcinoma, including Ta urothelial carcinoma, is diagnosed and treated by transurethral resection of bladder tumors [3]. uCIS has high-grade malignant urothelial cells. In cases with high-grade malignant urothelial cells, IHC may characteristically show CK20-positive and CD44-negative findings. Because some cases are CK20 negative, IHC staining may not be helpful in cases where histological differentiation is difficult. Various IHC markers have been used in real-world diagnostics and have been studied for their usefulness. However, comparative studies on diagnostic accuracy are lacking, and a comprehensive comparison through a DTA review would provide useful information.
In this study, we analyzed the expression of CK20, CD44, AMACR, and p53. The estimated expression rates of CK20, AMACR, and p53 were 0.803 (95% CI: 0.726–0.862), 0.824 (95% CI: 0.720–0.895), and 0.600 (95% CI: 0.510–0.683), respectively. However, CD44 had a low positive rate in uCIS (0.142, 95% CI: 0.033–0.449). We identified differences in the expression of the four markers in uCIS and reactive/normal urothelium. Of the four types of markers, the one with the critical difference between uCIS and reactive/normal urothelium was AMACR (OR, 142.931, 95% CI: 31.109–656.697). Furthermore, the expression comparison of uCIS with reactive/normal urothelium showed an odds ratio of 0.016 (95% CI: 0.006–0.043). As shown in our results, CD44 is highly expressed in the reactive and normal urothelium. Therefore, CD44 may be a useful negative marker for uCIS. In daily practice, CK20 and CD44 are used as a combination of positive and negative markers. The significance of this study is that additional staining of AMACR may improve the differentiation between uCIS and reactive/normal urothelium.
To evaluate the accuracy of the diagnostic test, we performed a DTA review of the four markers. The sensitivity and specificity of the four markers ranged from 0.843–0.984 and 0.657–0.829, respectively. These markers can be evaluated as highly sensitive. However, p53 was less specific than the other markers. Based on the AUC of SROC, we can see that the two markers, CK20 and CD44, were higher than the other AMACRs and p53. As mentioned earlier, the widely used CK20 and CD44 markers have relatively high sensitivity and specificity. In daily practice, using only positive markers may not be helpful for diagnosing CK20-negative uCIS. Therefore, it can be helpful to check for negative markers as well, and our results can be used as evidence for this. In the DTA review, this protein was evaluated as a negative marker of CD44. The sensitivity and specificity were 0.865 (95% CI: 0.803–0.913) and 0.767 (95% CI: 0.698–0.827), respectively. The results showed a slightly lower sensitivity and similar specificity compared with CK20.
In our study, a DTA review of the AMACR was conducted. To our knowledge, our study is the first DTA review of AMACR in uCIS. Based on our results, it has higher sensitivity and specificity than CK20. CK20-negative uCIS has been identified in up to 55.1% of cases [4,6,7,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30]. Since we did not use a 0% threshold for evaluating CK20, there could be different distributions based on that threshold. Because some reactive/normal urothelium can show positivity in umbrella cells, there can be variations in the CK20 negative rate. However, given the large number of CK20-negative cases, it is likely that positive markers other than CK20 could be helpful in differentiating flat lesions. The thresholds used in the studies included in our meta-analysis varied slightly between studies, with one-third of the urothelium or more, or 5% or more. In the literature, based on 1/3 of the urothelium, it was 100% negative in the reactive urothelium [22]. Eighty percent of uCIS were positive for CK20 [22]. Among positive cases, 58.3% to 2/3 of urothelium were positive [22]. Alston (2019) reported a 73% AMACR positivity rate in uCIS, with two-thirds of the urothelium positive in all positive cases [10]. Aron (2013) reported that although the threshold was set at 5%, positive cases showed a diffuse and strong pattern [4].
Straccia’s meta-analysis is recently published in 2022 [33]. CK20, CD44, and p53 were analyzed using the same markers as in our study. Unlike our study, they evaluated the KI-67. While the original meta-analysis included 15 articles, our study included 25 articles, which is a much larger number. In addition, a previous meta-analysis was performed on the expression rates of each marker. Compared to our results, they showed lower CK20 expression and higher CD44 expression. In addition, a comparison of expression in the reactive/normal urothelium was performed in our meta-analysis. In contrast to the previous meta-analysis, only AMACR was present in our results. In a comparison between uCIS and reactive/normal urothelium, AMACR was highly expressed in uCIS (OR: 142.931, 95% CI: 31.109–656.697). Although the results are taken from three papers, our results are significant. Compared to the positive marker CK20, AMACR has higher sensitivity and specificity. Although more detailed studies may be needed, it is useful for CK20-negative uCIS.
This study has limitations. First, the reactive and normal urothelium were analyzed in the same category. As there were fewer studies in both subgroups, reactive and normal urothelium were combined. Second, the use of Ki-67 immunohistochemistry in the evaluation of flat urothelial lesions may lead to misclassification [23]. Finally, the labeling index was excluded from this study because of its significance and confusion with positive and negative evaluations based on the baseline.
5. Conclusions
IHC markers CK20, CD44, AMACR, and p53 are significantly different in terms of uCIS and reactive/normal urothelium. Moreover, AMACR is a useful positive marker for uCIS.
Author Contributions
Conceptualization, D.Y. and J.-S.P.; methodology, J.-S.P.; software, J.-S.P.; data curation, D.Y. and N.-Y.K.; writing—original draft preparation, D.Y. and J.-S.P.; writing—review and editing, K.-W.M. and N.-Y.K.; All authors have read and agreed to the published version of the manuscript.
Funding
Not applicable.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Casey, R.G.; Catto, J.W.F.; Cheng, L.; Cookson, M.S.; Herr, H.; Shariat, S.; Alfred Witjes, J.; Black, P.C. Diagnosis and management of urothelial carcinoma in situ of the lower urinary tract: A systematic review. Eur Urol 2015, 67, 876–888. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Cheville, J.C.; Neumann, R.M.; Leibovich, B.C.; Egan, K.S.; Spotts, B.E.; Bostwick, D.G. Survival of patients with carcinoma in situ of the urinary bladder. Cancer 1999, 85, 2469–2474. [Google Scholar] [CrossRef]
- Flaig, T.W.; Spiess, P.E.; Agarwal, N.; Bangs, R.; Boorjian, S.A.; Buyyounouski, M.K.; Chang, S.; Downs, T.M.; Efstathiou, J.A.; Friedlander, T.; et al. Bladder cancer, version 3.2020, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 2020, 18, 329–354. [Google Scholar] [CrossRef]
- Aron, M.; Luthringer, D.J.; McKenney, J.K.; Hansel, D.E.; Westfall, D.E.; Parakh, R.; Mohanty, S.K.; Balzer, B.; Amin, M.B. Utility of a triple antibody cocktail intraurothelial neoplasm-3 (IUN-3-CK20/CD44s/p53) and a-methylacyl-CoA racemase (AMACR) in the distinction of urothelial carcinoma in situ (CIS) and reactive urothelial atypia. Am J Surg Pathol 2013, 37, 1815–1823. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Trpkov, K.; Lopez-Beltran, A.; Grignon, D.; Members of the ISUP Immunohistochemistry in Diagnostic Urologic Pathology Group. Best practices recommendations in the application of immunohistochemistry in the bladder lesions: Report from the International Society of Urologic Pathology consensus conference. Am J Surg Pathol 2014, 38, e20–e34. [Google Scholar] [CrossRef] [PubMed]
- Mallofré, C.; Castillo, M.; Morente, V.; Solé, M. Immunohistochemical expression of CK20, p53, and Ki-67 as objective markers of urothelial dysplasia. Mod Pathol 2003, 16, 187–191. [Google Scholar] [CrossRef] [PubMed]
- McKenney, J.K.; Desai, S.; Cohen, C.; Amin, M.B. Discriminatory immunohistochemical staining of urothelial carcinoma in situ and non-neoplastic urothelium: An analysis of cytokeratin 20, p53, and CD44 antigens. Am J Surg Pathol 2001, 25, 1074–1078. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Zhang, P.L.; Herrera, G.A. p53 protein and Ki-67 overexpression in urothelial dysplasia of bladder. Appl Immunohistochem Mol Morphol 2002, 10, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Alston, E.L.J.; Zynger, D.L. Does the addition of AMACR to CK20 help to diagnose challenging cases of urothelial carcinoma in situ? Diagn Pathol 2019, 14, 91. [Google Scholar] [CrossRef] [PubMed]
- Arias-Stella, J.A., 3rd; Shah, A.B.; Gupta, N.S.; Williamson, S.R. CK20 and p53 Immunohistochemical Staining Patterns in Urinary Bladder Specimens With Equivocal Atypia. Arch Pathol Lab Med 2018, 142, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Asgari, M.; Nabi Maybodi, M.; Abolhasani, M. Differential diagnosis of urothelial carcinoma in situ from non-neoplastic urothelia: Analysis of CK20, CD44, P53 and Ki67. Med J Islam Repub Iran 2016, 30, 400. [Google Scholar] [PubMed]
- Barth, I.; Schneider, U.; Grimm, T.; Karl, A.; Horst, D.; Gaisa, N.T.; Knüchel, R.; Garczyk, S. Progression of urothelial carcinoma in situ of the urinary bladder: A switch from luminal to basal phenotype and related therapeutic implications. Virchows Arch 2018, 472, 749–758. [Google Scholar] [CrossRef] [PubMed]
- Dhawan, D.; Hamdy, F.C.; Rehman, I.; Patterson, J.; Cross, S.S.; Feeley, K.M.; Stephenson, Y.; Meuth, M.; Catto, J.W. Evidence for the early onset of aberrant promoter methylation in urothelial carcinoma. J Pathol 2006, 209, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Edgecombe, A.; Nguyen, B.N.; Djordjevic, B.; Belanger, E.C.; Mai, K.T. Utility of cytokeratin 5/6, cytokeratin 20, and p16 in the diagnosis of reactive urothelial atypia and noninvasive component of urothelial neoplasia. Appl Immunohistochem Mol Morphol 2012, 20, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Garczyk, S.; Bischoff, F.; Schneider, U.; Golz, R.; von Rundstedt, F.C.; Knüchel, R.; Degener, S. Intratumoral heterogeneity of surrogate molecular subtypes in urothelial carcinoma in situ of the urinary bladder: Implications for prognostic stratification of high-risk non-muscle-invasive bladder cancer. Virchows Arch 2021, 479, 325–335. [Google Scholar] [CrossRef]
- Hacek, J.; Brisuda, A.; Babjuk, M.; Zamecnik, J. Expression of cancer stem cells markers in urinary bladder urothelial carcinoma and its precursor lesions. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 2021, 165, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Ick, K.; Schultz, M.; Stout, P.; Fan, K. Significance of p53 overexpression in urinary bladder transitional cell carcinoma in situ before and after bacillus Calmette-Guérin treatment. Urology 1997, 49, 541–546; discussion 546–547. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Wu, C.; Eslami, Z.; Tanguay, S.; Aprikian, A.; Kassouf, W.; Brimo, F. The role of immunohistochemistry in the diagnosis of flat urothelial lesions: A study using CK20, CK5/6, P53, Cd138, and Her2/Neu. Ann. Diagn. Pathol. 2014, 18, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Kunju, L.P.; Lee, C.T.; Montie, J.; Shah, R.B. Utility of cytokeratin 20 and Ki-67 as markers of urothelial dysplasia. Pathol Int 2005, 55, 248–254. [Google Scholar] [CrossRef]
- Lombardo, K.A.; Murati Amador, B.; Parimi, V.; Hoffman-Censits, J.; Choi, W.; Hahn, N.M.; Kates, M.; Bivalacqua, T.J.; McConkey, D.; Hoque, M.O.; et al. Urothelial Carcinoma In Situ of the Bladder: Correlation of CK20 Expression With Adaptive Immune Resistance, Response to BCG Therapy, and Clinical Outcome. Appl Immunohistochem Mol Morphol 2021, 29, 127–135. [Google Scholar] [CrossRef]
- Lopez-Beltran, A.; Jimenez, R.E.; Montironi, R.; Patriarca, C.; Blanca, A.; Menendez, C.L.; Algaba, F.; Cheng, L. Flat urothelial carcinoma in situ of the bladder with glandular differentiation. Hum Pathol 2011, 42, 1653–1659. [Google Scholar] [CrossRef] [PubMed]
- Neal, D.J.; Amin, M.B.; Smith, S.C. CK20 versus AMACR and p53 immunostains in evaluation of Urothelial Carcinoma in Situ and Reactive Atypia. Diagn Pathol 2020, 15, 61. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, J.K.; Przybycin, C.G.; McKenney, J.K.; Magi-Galluzzi, C. Immunohistochemical staining patterns of Ki-67 and p53 in florid reactive urothelial atypia and urothelial carcinoma in situ demonstrate significant overlap. Hum Pathol 2020, 98, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Oliva, E.; Pinheiro, N.F.; Heney, N.M.; Kaufman, D.S.; Shipley, W.U.; Gurski, C.; Spicer, B.; Paner, G.P.; Gown, A.M.; Amin, M.B. Immunohistochemistry as an adjunct in the differential diagnosis of radiation-induced atypia versus urothelial carcinoma in situ of the bladder: A study of 45 cases. Hum Pathol 2013, 44, 860–866. [Google Scholar] [CrossRef]
- Ozdemir, E.; Kakehi, Y.; Okuno, H.; Habuchi, T.; Okada, Y.; Yoshida, O. Strong correlation of basement membrane degradation with p53 inactivation and/or MDM2 overexpression in superficial urothelial carcinomas. J Urol 1997, 158, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Sangoi, A.R.; Falzarano, S.M.; Nicolas, M.; McKenney, J.K. Carcinoma In Situ With Plasmacytoid Features: A Clinicopathologic Study of 23 Cases. Am J Surg Pathol 2019, 43, 1638–1643. [Google Scholar] [CrossRef] [PubMed]
- Sato, M.; Yanai, H.; Morito, T.; Oda, W.; Shin-no, Y.; Yamadori, I.; Tshushima, T.; Yoshino, T. Association between the expression pattern of p16, pRb and p53 and the response to intravesical bacillus Calmette-Guerin therapy in patients with urothelial carcinoma in situ of the urinary bladder. Pathol Int 2011, 61, 456–460. [Google Scholar] [CrossRef] [PubMed]
- Schmitz-Dräger, B.J.; van Roeyen, C.R.; Grimm, M.O.; Gerharz, C.D.; Decken, K.; Schulz, W.A.; Bültel, H.; Makri, D.; Ebert, T.; Ackermann, R. P53 accumulation in precursor lesions and early stages of bladder cancer. World J Urol 1994, 12, 79–83. [Google Scholar] [CrossRef]
- Shariat, S.F.; Kim, J.H.; Ayala, G.E.; Kho, K.; Wheeler, T.M.; Lerner, S.P. Cyclooxygenase-2 is highly expressed in carcinoma in situ and T1 transitional cell carcinoma of the bladder. J Urol 2003, 169, 938–942. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Tokuhara, Y.; Hosokawa, S.; Ohsaki, H.; Morinishi, T.; Yamamoto, T.; Teramoto, N.; Hirakawa, E. Overexpression of the PPAR-γ protein in primary Ta/T1 non-muscle-invasive urothelial carcinoma. Mol Clin Oncol 2022, 16, 36. [Google Scholar] [CrossRef]
- Zamora, J.; Abraira, V.; Muriel, A.; Khan, K.; Coomarasamy, A. Meta-DiSc: A software for meta-analysis of test accuracy data. BMC Med Res Methodol 2006, 6, 31. [Google Scholar] [CrossRef] [PubMed]
- Moses, L.E.; Shapiro, D.; Littenberg, B. Combining independent studies of a diagnostic test into a summary ROC curve: Data-analytic approaches and some additional considerations. Stat Med 1993, 12, 1293–1316. [Google Scholar] [CrossRef] [PubMed]
- Straccia, P.; Fiorentino, V.; Martini, M.; Pierconti, F. A systematic review and meta-analysis of CK20, CD44, Ki67 and p53 as im-munohistochemical markers in bladder carcinoma in situ. Actas Urol Esp (Engl Ed) 2022, 46, 521–530. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of the searching strategy.
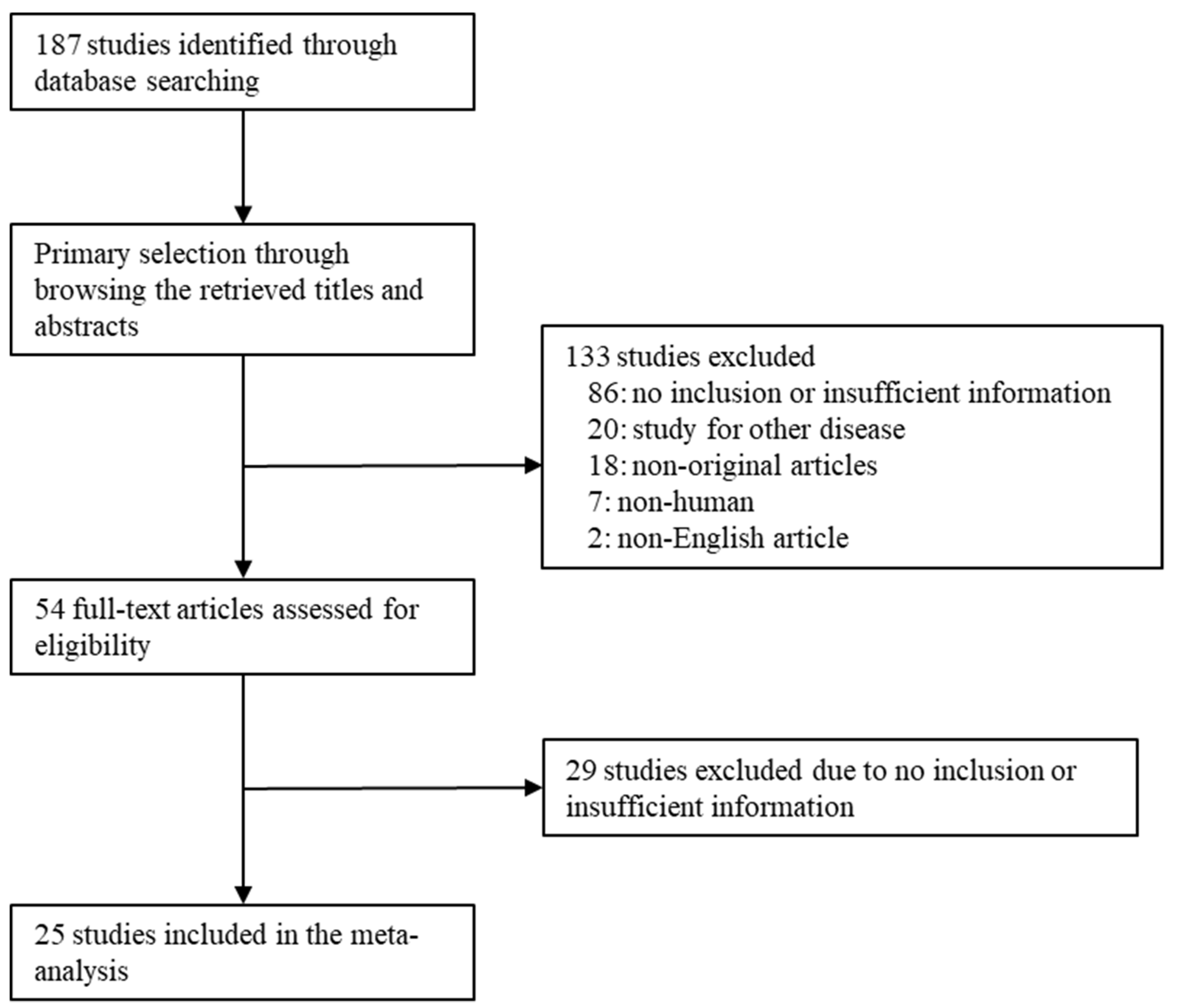

Table 1.
Main characteristics of the eligible studies.
| First Author | Location | Organ | No of patients | Interpreted markers | |
|---|---|---|---|---|---|
| CIS | RA/Non-neoplatic/ Normal urothelium |
||||
| Alston 2019 [9] | USA | UB | 42 | 30 | CK20, AMACR |
| Arias-Stella 2018 [10] | USA | UB | 69 | CK20 | |
| Aron 2013 [4] | Canada | UB | 43 | 35 | CK20, CD44, AMACR |
| Asgari 2016 [11] | Iran | UB | 20 | 40 | CK20, CD44, p53 |
| Barth 2018 [12] | Germany | UB | 156 | CK20 | |
| Dhawan 2006 [13] | UK | UB | 65 | 56 | CK20, p53 |
| Edgecombe A [14] | Canada | UB | 20 | 10 | CK20 |
| Garczyk 2021 [15] | Germany | UB | 99 | CK20 | |
| Hacek 2021 [16] | Czech Republic | UB | 32 | CD44 | |
| Ick 1997 [17] | USA | UB | 12 | p53 | |
| Jung 2014 [18] | Canada | UB | 41 | 52 | CK20, p53 |
| Kunju 2005 [19] | USA | UB | 50 | 50 | CK20 |
| Lombardo 2021 [20] | USA | UB | 43 | CK20, p53 | |
| Lopez-Beltran 2010 [21] | Spain | UB | 39 | CK20, p53 | |
| Mallofré 2003 [6] | USA | UB/UT | 50 | 50 | CK20, p53 |
| McKenney 2001 [7] | UB | 21 | 25 | CK20, CD44, p53 | |
| Neal 2020 [22] | USA | UB | 15 | 15 | CK20, AMACR, p53 |
| Nguyen 2020 [23] | USA | UB | 40 | 40 | CK20, CD44, p53 |
| Oliva 2013 [24] | USA | UB | 17 | 28 | CK20, CD44, p53 |
| Ozdemir 1997 [25] | Japan | UB/UT | 18 | p53 | |
| Sangoi 2019 [26] | USA | UB | 25 | CK20, CD44, p53 | |
| Sato 2011 [27] | Japan | UB | 27 | p53 | |
| Schmitz-Dräger 1994 [28] | Germany | UB | 24 | p53 | |
| Shariat 2003 [19] | USA | UB | 39 | p53 | |
| Tanaka 2022 [30] | Japan | UB | 19 | p53 | |
CIS, carcinoma in situ; RA, reactive atypia; UB, urinary bladder; UT, urinary tract.
Table 2.
Estimated expression rates of various immunohistochemical markers in urothelial carcinoma in situ.
Table 2.
Estimated expression rates of various immunohistochemical markers in urothelial carcinoma in situ.
| Number of subsets |
Fixed effect [95% CI] |
Heterogeneity test [p-value] |
Random effect [95% CI] |
Egger’s Test [p-value] |
|
|---|---|---|---|---|---|
| CK20 | 19 | 0.722 [0.686, 0.755] | < 0.001 | 0.803 [0.726, 0.862] | 0.002 |
| CD44 | 7 | 0.364 [0.265, 0.476] | < 0.001 | 0.142 [0.033, 0.449] | 0.037 |
| AMACR | 3 | 0.824 [0.720, 0.895] | 0.726 | 0.824 [0.720, 0.895] | 0.339 |
| p53 | 18 | 0.585 [0.537, 0.631] | < 0.001 | 0.600 [0.510, 0.683] | 0.143 |
CI, Confidence interval.
Table 3.
Expression ratio of various immunohistochemical markers between urothelial carcinoma in situ and reactive/normal urothelium.
Table 3.
Expression ratio of various immunohistochemical markers between urothelial carcinoma in situ and reactive/normal urothelium.
| Number of subsets |
Fixed effect [95% CI] |
Heterogeneity test [p-value] |
Random effect [95% CI] |
Egger’s Test [p-value] |
|
|---|---|---|---|---|---|
| CK20 | 16 | 28.848 [17.968, 46.318] | 0.001 | 71.313 [30.176, 168.530] | < 0.001 |
| CD44 | 7 | 0.017 [0.007, 0.043] | 0.370 | 0.016 [0.006, 0.043] | 0.110 |
| AMACR | 3 | 142.931 [31.109, 656.697] | 0.968 | 142.931 [31.109, 656.697] | 0.116 |
| p53 | 11 | 8.955 [5.413, 14.814] | 0.011 | 16.774 [6.713, 41.916] | 0.008 |
CI, Confidence interval.
Table 4.
Sensitivity, specificity, diagnostic odds ratio and area under curve of summary receiver operation characteristics curve of various immunohistochemical markers in urothelial carcinoma in situ.
Table 4.
Sensitivity, specificity, diagnostic odds ratio and area under curve of summary receiver operation characteristics curve of various immunohistochemical markers in urothelial carcinoma in situ.
| Included studies |
Sensitivity (%) [95% CI] |
Specificity (%) [95% CI] |
Diagnostic OR [95% CI] |
AUC on SROC |
|
|---|---|---|---|---|---|
| CK20 | 16 | 0.937 [0.910, 0.957] | 0.773 [0.735, 0.809] | 77.22 [30.17, 172.85] | 0.942 |
| CD44 * | 7 | 0.865 [0.803, 0.913] | 0.767 [0.698, 0.827] | 61.11 [23.08, 161.81] | 0.940 |
| AMACR | 3 | 0.984 [0.915, 1.000] | 0.829 [0.725, 0.906] | 142.93 [31.11, 656.70] | 0.770 |
| p53 | 11 | 0.843 [0.794, 0.884] | 0.657 [0.607, 0.705] | 17.17 [6.72, 43.87] | 0.711 |
CI, Confidence interval; OR, Odds ratio; AUC, Area under curve; SROC, summary receiver operating characteristic. *, negative marker.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



