
Submitted:
06 August 2023
Posted:
08 August 2023
You are already at the latest version
Abstract
In recent years, the number of open preservation surgeries for treatment of laryngeal Cancer has increased. The purpose of this surgery is to avoid the highly mutilating intervention of a total laryngectomy (TL) and to maintain laryngeal function while ensuring oncological radicality. The aim of this study was to assess the oncologic results of OPHL I and II and to identify prognostic factors that could impact patient survival and local failure rates. This study was conducted on 182 patients with laryngeal squamous cell carcinoma treated with OPHLs between 2005 and 2015. The survival rates of a group of patients treated with TL between 2004 and 2014 were taken into con-sideration to compare survival outcomes. The DSS in pT2 and pT3 tumors in relation to the type of surgery showed no statistically significant difference between OPHLs and TL (p=0.54 and p=0.63 respectively). The 5-years T-recurrence free survival showed that pT4 tumors, perineural/vascular positive invasion and OPHL IIb + ARY treated tumors were associated with a higher risk of tumor recurrence (p<0.0001, p=0.0005 and p=0.016 respectively). OPHLs represent an excellent alterna-tive to TL considering the characteristics of the tumor and the general conditions of the patient.
Keywords:
open partial horizontal laryngectomy
; laryngeal cancer
; laryngeal preservation
; laryngectomy free survival
; disease specific survival
; total laryngectomy
1. Introduction
Laryngeal cancer is one of the most common malignancies in the upper aerodigestive tract, accounting for 4.5% of all cancers [1]. Treatment options are determined by the disease stage at diagnosis and may include transoral laser microsurgery, partial horizontal laryngectomy, and radiotherapy, all of which have shown good oncological and functional outcomes. In recent years, there has been a rise in open preservation surgeries, aiming to avoid the highly mutilating total laryngectomy procedure [2] while ensuring both laryngeal function preservation and oncological radicality [3,4,5]. Recently, Succo et al. [6] proposed a new classification of open partial horizontal laryngectomy (OPHL) based on the cranio-caudal extent of resected laryngeal structures. This classification includes three types of OPHL: Type I - supraglottic, Type II - supracricoid, and Type III - supratracheal. Maintaining at least one cricoarytenoid unit remains crucial for overall functional recovery of the neolarynx, even after the removal of the entire thyroid shield. Over time, indications [7,8] and surgical techniques have evolved, resulting in improved oncological and functional outcomes [12,13,14,15,16,17,18]. However, limited literature exists on the long-term oncological outcomes of OPHLs compared to total laryngectomy, specifically regarding local extensions [19], which could provide valuable insights to clarify appropriate indications for each type of OPHL. Thus, identifying clinical and pathological prognostic factors is essential to establish clear therapeutic indications and to predict the risk of local failure, as the primary objective of OPHL is to preserve the larynx while ensuring oncological effectiveness.
Therefore, the aim of this multi-institutional retrospective case series study was to assess the oncological outcomes of OPHL I and II in previously untreated patients and to evaluate the prognostic factors that may influence patient survival and the occurrence of local failure.
2. Materials and Methods
2.1. Population
This multicenter retrospective study was conducted on 182 patients with laryngeal squamous cell carcinoma who were treated with open partial horizontal laryngectomies OPHLs (OPHLI, OPHLIIa,OPHL IIa+ARY, IIb, IIb+ARY) between 2005 and 2015 at the Otolaryngology Unit of the Department of Health Sciences, University of Catanzaro, Italy, Otolaryngology Unit, Cannizzaro Hospital, Catania, Italy, and Villa Sofia-Cervello Hospital, Palermo. The previously published survival rates [20] of a group of patients treated with total laryngectomy between 2004 and 2014 at the Otolaryngology Unit of the Department of Health Sciences, University of Catanzaro, Italy, were considered for comparison of survival outcomes. All patients were informed of the benefits, risks, possible complications, and alternatives to OPHLs before providing their informed consent. This study was approved by the Institutional Review Boards at the University of Catanzaro, and the requirement to obtain written informed consent from patients was waived due to the retrospective nature of the investigation. To protect patient privacy, their personal information was appropriately anonymized prior to analysis. All included patients had a minimum follow-up time of 60 months. Previously treated patients, those lost to follow-up, patients with incomplete medical or clinical data, and patients eligible for transoral laser surgery were excluded from this study. Prior to surgery, patients underwent videolaryngoscopy with a flexible endoscope and videolaryngostroboscopy. The neck was examined through palpation, while ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI) were included for staging. The stage was determined according to the 8th edition of the TNM classification established by the American Joint Committee for Cancer. All patients were followed up within 1 month of surgery, every 3 months for 3 years, and every 6 months thereafter. Follow-up visits included clinical examination, laryngoscopy, and radiological examinations, such as neck ultrasound and chest X-ray every six months, and CT or MRI every year or according to clinical evidence. Clinical and anamnestic data were collected and organized in a database for each patient.
2.2. Statistical analysis
The study assessed the five-year overall survival time, five-year disease-free survival rate, and five-year disease-specific survival rate. Statistical analysis was performed using MedCalc Software (v 9.0; MedCalc Software bvba, Ghent, Belgium). The collected data included the mean, median, and standard deviation. Pearson's chi-squared and/or Fisher's exact tests were used to identify differences in demographic and clinicopathologic data between the cohorts. The D'Agostino-Pearson test was used for normally distributed data. The variables considered in the survival analysis included age, subsite, grading, cT and cN status, pT and pN status, T recurrence, N recurrence, second tumor, and type of OPHLs. The Kaplan-Meier method was used to analyze survival, and the log-rank test was utilized to compare survival curves between groups. Cox proportional hazards regression was performed to determine independent prognostic factors. OS was defined as the time interval from surgery ± adjuvant treatment until death (from any cause). DFS and DSS were defined as the time intervals from treatment until loco-regional recurrence and death due to the disease, respectively. All deaths due to other causes were considered censored. A p-value of <0.05 was considered statistically significant.
3. Results
3.1. Pateints (forse meglio Population)
A total of 182 patients (16 females and 166 males) were included in the study. The mean age at diagnosis was 61.3 ± 8.6 SD years. The average follow-up time was 98.6 ± 34.6 SD months. Among the patients, 148 (81.3%) had tumors located in the glottic region, while 34 (18.7%) had supraglottic tumors. The histological grading showed that 39 (21.4%) patients had G1 tumors, 120 (65.9%) had G2 tumors, and 23 (12.6%) had G3 tumors. In terms of staging, 88 (48.3%) patients were classified as Stage I, 45 (24.7%) as Stage II, 42 (23%) as Stage III, and 7 (4.0%) as Stage IV. According to the cTNM classification, 105 lesions (57.7%) were classified as T1-T1b, 56 (30.7%) as T2, and 21 (11.6%) as T3. Resection margins were positive in 7 out of 182 patients (3.8%), while cartilage invasion was present in 8 patients (4.3%), and perineural/vascular invasion was observed in 11 patients (6.04%). Regarding post-operative pT classification,102 cases (56%) were classified as pT1, 43 (23.6%) as pT2, 33 (18.2%) as pT3, and 4 (2.2%) as pT4. Lymph node clinical status was classified as N0 in 131 patients and N+ in 51 patients. Among the 182 patients, 52 underwent neck dissection, with 43 of them having metastatic lymph nodes. Additionally, a total of 36 patients received either surgery plus radiotherapy or radiotherapy plus chemotherapy (Table 1).
In the study, a total of 77 patients treated with total laryngectomy were included; among them, 2 were female and 75 were male. The mean age at diagnosis was 66 ± 9.7 SD years. The average follow-up time was 76.0 ± 43.3 SD months. Of the patients, 31 (40.2%) had glottic tumors, 23 (29.9%) had supraglottic tumors, and the remaining 23 (29.9%) had transglottic tumors. Histological evaluation revealed that 5 patients (6.5%) had G1 tumors, 42 (54.5%) had G2 tumors, and 30 (39.0%) had G3 tumors. According to the cTNM classification, 21 lesions (27.3%) were staged as T2, 35 (45.4%) as T3, and 21 (27.3%) as T4. Post-operative pT classification was as follows: pT2 in 21 cases (27.3%), pT3 in 35 cases (45.4%), and pT4 in 21 cases (27.3%). Lymph node clinical status was classified as N0 in 39 patients, N1 in 12 patients, N2 in 23 patients, and N3 in 3 patients. Out of the total of 77 patients, 63 received neck dissection, and among them, 38 had metastatic lymph nodes. Furthermore, 34 patients underwent surgery plus radiotherapy, whereas 8 patients underwent radiotherapy plus chemotherapy.
3.2. Survival rates and correlation between OPHLs and Total laryngectomy
The study reported a five-year overall survival rate of 87.91% with 22 out of 182 patients deceased. Specifically, 7 patients died due to distant metastasis or a second tumor, 5 died after locoregional recurrence, and 10 died of non-cancer-related diseases. Considering the clinical variables, only perineural/vascular invasion (p = 0.001) was found to be statistically significant for five-year overall survival (Table 2).
The five-year disease-free survival rate was 81.87%. Notably, variables such as cT stage (p = 0.0030), pT stage (p= 0.0001), cN stage (p=0.041), pN stage (p = 0.0083), perineural/vascular invasion (p=0.006), and the type of OPHLs (p = 0.041) showed significant statistical differences (Table 2). Additionally, the five-year DSS rate was 92.31%, with statistically significant differences observed for grading (p=0.029), subsite (p =0.046), cT stage (p=0.037), cN stage (p=0.008), and perineural/vascular invasion (p<0.0001) (Table 2). The five-year laryngectomy-free survival (LFS) rate was 92.86%, and significant differences were noted for the variables pT stage (p = 0.0001) and pN stage (p=0.008 ) (Table 2). A Cox proportional hazards regression model was used in the study to analyze the role of clinical variables as risk factors for OS, DFS, DSS and LFS. The results showed that perineural/vascular invasion was an independent prognostic factor associated with worse overall survival (OS) (p=0.019), and both grading (p=0.032) and perineural/vascular invasion (p=0.007) were identified as independent prognostic factors associated with worse disease-specific survival (DSS). Additionally, the pT variable (p=0.047) was found to be an independent prognostic factor for worse LFS.
When comparing OS and DSS between OPHLs and TLs, a statistically significant difference was observed (OS 87.91% and 62.34% for OPHL and TL, respectively, p=0.043; DSS 92.31% and 68.42% for OPHL and TL, respectively, p=0.0002). Patients treated with TL exhibited worse OS (Figure 1) and DSS (Figure 2).
As the group treated with total laryngectomy did not include any pT1 tumors, and the OPHLs group had only a few pT4 tumors, we conducted an analysis of the DSS in the pT2 and pT3 tumors. The aim was to understand the impact of the type of surgery on DSS in relation to pT status. The results showed that the 5-years DSS in pT2 (Figure 3) and pT3 tumors (Figure 4) in relation to the type of surgery showed no statistically significant difference between OPHLs and total laryngectomy (p=0.54 and p=0.63 respectively) (Table 3).
3.3. Oncological Outcomes and Pattern of local failure of the OPHLs
Out of the 182 patients, 24 (13.1%) presented loco-regional recurrence during the follow-up period after a mean time of 23.5 ± 14.8 SD months. Among these patients, nine (37.5%) developed lymph node metastasis, and fifteen (62.5%) developed local recurrence (13 of them were treated with TL, and 2 underwent chemo-radiation). A total of 13 (7.14%) of the 182 patients developed a second tumor or distant metastasis after a mean time of 32.9 ± 14.8 SD months (range: 8–60 months). Among these, 9 of the patients (69.4%) developed pulmonary metastasis, 1 (7.65%) had esophagus cancer, 2 (15.3%) had oropharyngeal carcinoma, and 1 (7.65%) had prostate cancer. The 5-year T-recurrence-free survival (TRFS) rate was 91.76%. According to the type of OPHL, a statistically significant correlation has been shown between OPHL IIb+ARY and T recurrence (p=0.004) (Table 4).
Table 5 presents the correlation between clinical variables and T recurrence.
A statistically significant difference was noted in T recurrence for the variables cT stage (p=0.014), pT stage (p=0.0002), perineural/vascular invasion (p=0.018), and type of OPHL (p=0.0049). The 5-year TRFS survival according to pT status, perineural/vascular invasion, and type of OPHLs showed that pT4 tumors, positive perineural/vascular invasion, and OPHL IIb+ARY treated tumors were associated with worse TRFS (p<0.0001, p=0.0005, and p=0.016, respectively; Figure 5, Figure 6 and Figure 7).
Finally, in Table 6, we report the correlation between clinical variables and larynx preservation, where advanced pT status (p=0.0009) and a more demolitive type of OPHL (p=0.046) were significant prognostic factors for the loss of laryngeal preservation.
4. Discussion
The main purpose of open organ preservation surgery for the treatment of laryngeal cancer is to preserve the larynx and its functions while ensuring oncological radicality. It is therefore assumed that the survival rates of partial laryngectomies (OPHLs) should not be inferior to total laryngectomies. In our study, the overall survival, disease-free survival (DFS), and disease-specific survival (DSS) at 5 years were found to be 87.91%, 81.87%, and 92.31% respectively, which is similar to the results reported by Saraniti et al. [21] in a recent review [21]. The patients died laryngeal cancer related cause were 12 out of 22 (54.5%), with the majority of deaths attributed to the development of secondary tumors or distant metastases. Clinical variables such as cT and cN status, as well as the type of OPHLs, were found to influence disease-free survival, with more advanced stage tumors (higher T and N stages) and patients treated with more aggressive OPHL procedures showing a higher risk of disease recurrence. Clinical variables such as tumor location, grading (cT and N status) and perineural/vascular invasion were identified as prognostic factors for disease-specific survival (DSS). Most of our patients had early-stage tumors, such as supraglottic cT1 and glottic T1b tumors, which were not amenable to transoral laser microsurgery, or were in an intermediate stage. Taking into consideration the data obtained from patients classified as pT1, we observed a 5-year disease-free survival (DFS) and disease-specific survival (DSS) rates of 88.24% and 95.10%, respectively, along with an organ preservation rate of 95.10%. In a study conducted by Laccourraye et al. [22], involving 62 patients with T1b glottic carcinoma treated with SCL-CHEP, a 5-year local control rate of 98.2% was reported. Similarly, Atallah et al. [23] observed a 5-year DFS and DSS of 87% and 95.6%, respectively, in 53 patients with T1b glottic carcinoma who underwent SCL-CHEP. When comparing these alternative treatment approaches for T1 laryngeal tumors to OPHL, a study by Alkan et al. [24] found that on 54 patients with T1 laryngeal cancer, the local control rates were 75% and 97% for those treated with transoral laser microsurgery (TLM) and radiotherapy, respectively. A review from Baird et al. [25] report a local control of 82.8% and 73.2% in patients treated by Radiotherapy or Transoral laser microsurgery (TLM), respectively. Campo et al. 2021 [26], in a study conducted on T2 glottic tumors, found that patients treated with OPHL showed better long-term local control and laryngeal preservation compared to patients treated with TLM or RT. When considering only staged cT2-cT3 tumors, the DSS and DFS results observed in our study were similar to those reported in the literature. Specifically, in pT3 classified tumors, we observed a lower DSS (90.91%) compared to pT4 classified tumors (100%). This could potentially be explained by recent findings from Succo et al. [27] regarding the behavior of cT3 tumors in relation to their extent of spread. The authors have emphasized the importance of the posterior laryngeal compartment. Lesions are classified as anterior or posterior to a plane passing through the arytenoid vocal process perpendicular to the ipsilateral thyroid lamina, known as the “magic plane”. They demonstrate that posterior T3 tumors may be more similar to T4 tumors. In particular, survival analysis showed that posterior T3 lesions have worse survival outcomes compared to anterior T4 lesions. These findings have been confirmed by other studies [28,29,30]. To assess the oncological radicality of OPHL compared to total laryngectomy, we compared the 5-year overall survival (OS) and disease-specific survival (DSS). Patients treated with total laryngectomy showed worse survival outcomes (OS 87.91% and 62.34% for OPHL and TL, respectively, p=0.043; DSS 92.31% and 68.42% for OPHL and TL, respectively, p=0.0002). This is likely due to the fact that patients treated with total laryngectomy had a more advanced stage of the disease. Therefore, we compared the survival outcomes in patients with tumor classification of pT2 and pT3, and no statistically significant difference was found, confirming the excellent oncological results achieved with OPHL. There are few studies that directly compare the survival rates between patients treated with OPHL and those treated with TL. In a review, by Campo et al. [31], only three studies [29,32,33] on T3 patients were identified that compared survival outcomes in patients treated with OPHL versus TL. These studies confirmed that OPHL achieves excellent oncological results that are not inferior to TL. One of the main objectives of OPHLs is laryngeal preservation. For this reason, we examined the risk factors for tumor recurrence and the correlation between clinical variables and organ preservation. In evaluating the recurrence-free survival (RFS) of T, we found that patients with pT4 tumors (50% vs. 91.76% of the total) and those with perineural/vascular invasion showed the worst RFS. The type of OPHLs also emerged as a risk factor for T recurrence, particularly in patients undergoing OPHLIIb+ARY, who showed a higher risk of T recurrence (79.31% vs. 91.76%). Regarding the correlation between clinical variables and larynx preservation, we found that advanced pT status (p=0.0009) and more extensive types of OPHL (p=0.046) were significant prognostic factors for the loss of laryngeal preservation. Our data confirm the effectiveness of OPHLs in terms of 5-year disease-specific survival (DSS) and organ preservation in early and intermediate stage tumors. The scientific evidence is limited regarding the analysis of risk factors for local recurrence in OPHLs [34,35]. In our study, the failure of organ preservation due to T recurrence appears to correlate with advanced clinical variables, such as advanced T stage, perineural invasion, and more aggressive types of OPHLs. These results are similar to those reported by Crosetto et al. [35] in their study, which focused on patients treated with OPHLII and OPHLIII. Therefore, it is evident that patient selection criteria for OPHL are crucial in achieving laryngeal preservation, especially in advanced cases, although there is currently no unanimous consensus on how to select patients. De Vincentiis et al. [28] suggest limiting the indication for tumors with the following characteristics: tumor limited to the anterior 2/3 of the larynx; no extensive invasion of the pre-epiglottic space with involvement of the hyoid bone; minimal erosion or invasion of the thyroid cartilage without extracartilaginous involvement; N0 lymph nodes, anterior subglottic extension, and <5mm of extension [28]. The results of our study confirm excellent oncological radicality of OPHLs with a high rate of organ preservation for early and intermediate-stage tumors, and caution is needed in patient selection criteria for advanced-stage cases. The limitations of our study include its retrospective multicenter design and the predominance of T1 cases.
5. Conclusions
Partial laryngectomies (OPHL) represent an excellent alternative to TL, with remarkable results in terms of DSS, DFS and organ preservation. In advanced tumors, OPHL remains a valid alternative to total laryngectomy, taking into consideration the tumor characteristics as well as the overall condition of the patient.
Author Contributions
Conceptualization, E.A.; Methodology and data curation, M.R.B.; Resourcers, A.A., D.M.M., D.L., F.O, and E.P.; supervision, M.G. and V.S..
Funding
This research received no external funding.
Conflicts of Interest
The authors declare that they have no competing interests.
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global Cancer Statistics. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Allegra, E.; La Mantia, I.; Bianco, M.R.; Drago, G.D.; Le Fosse, M.C.; Azzolina, A.; Grillo, C.; Saita, V. Verbal performance of total laryngectomized patients rehabilitated with esophageal speech and tracheoesophageal speech: impacts on patient quality of life. Psychol Res Behav Manag. 2019, 12, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Garozzo, A.; Allegra, E.; La Boria, A.; Lombardo, N. Modified Supracricoid Laryngectomy. Otolaryngol. Head Neck Surg. 2010, 142, 137–139. [Google Scholar] [CrossRef] [PubMed]
- de Vincentiis, M.; De Virgilio, A.; Bussu, F.; Gallus, R.; Gallo, A.; Bastanza, G.; Parrilla, C.; Greco, A.; Galli, J.; Turchetta, R.; Almadori, G.; Pagliuca, G.; Valentini, V.; Paludetti, G. Oncologic results of the surgical salvage of recurrent laryngeal squamous cell carcinoma in a multicentric retrospective series: emerging role of supracricoid partial laryngectomy. Head Neck. 2015, 37, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Allegra, E.; Saita,V. ; Azzolina, A.; De Natale, M.; Bianco, M.R.; Modica, DM.; Garozzo, A. Impact of the anterior commissure involvement on the survival of early glottic cancer treated with cricohyoidoepiglottopexy: a retrospective study. Cancer Manag Res. 2018, 8, 5553–5558. [Google Scholar] [CrossRef]
- Succo, G.; Peretti, G.; Piazza, C.; Remacle, M.; Eckel, HE.; Chevalier, D.; Simo, R.; Hantzakos, AG.; Rizzotto, G.; Lucioni, M.; Crosetti, E.; Antonelli, AR. Open partial horizontal laryngectomies: a proposal for classification by the working committee on nomenclature of the European Laryngological Society. Eur Arch Otorhinolaryngol. 2014, 271, 2489–96. [Google Scholar] [CrossRef]
- Pellini, R.; Pichi, B.; Ruscito, P.; Ceroni, AR.; Caliceti, U.; Rizzotto, G.; Pazzaia, A.; Laudadio, P.; Piazza, C.; Peretti, G.; Giannarelli, D.; Spriano, G. Supracricoid partial laryngectomies after radiation failure: a multi-institutional series. Head Neck. 2008, 30, 372–9. [Google Scholar] [CrossRef]
- Mercante, G.; Grammatica, A.; Battaglia, P.; Cristalli, G.; Pellini, R.; Spriano, G. Supracricoid partial laryngectomy in the management of t3 laryngeal cancer. Otolaryngol Head Neck Surg 2013, 149, 714–720. [Google Scholar] [CrossRef]
- Piquet, JJ.; Desaulty, A.; Decroix, G. Crico-hyoido-epiglotto-pexy. Surgical technic and functional results. Ann Otolaryngol Chir Cervicofac. 1974, 91, 681–6. [Google Scholar]
- Guerrier, B.; Lallemant, JG.; Balmigere, G.; Bonnet, P.; Arnoux, B. Our experience in reconstructive surgery in glottic cancer. Ann Otolaryngol Chir Cervicofac. 1987, 104, 175–179. [Google Scholar]
- Garozzo. A.; Allegra, E.; La Boria, A.; Lombardo, N. Modified supracricoid laryngectomy. Otolaryngol Head Neck Surg. 2010, 142, 137–139. [Google Scholar] [CrossRef]
- de Vincentiis, M.; Minni, A.; Gallo, A.; Di Nardo, A. Supracricoid partial laryngectomies: oncologic and functional results. Head Neck. 1998, 20, 504–9. [Google Scholar] [CrossRef]
- Allegra, E.; Lombardo, N.; La Boria, A.; Rotundo, G.; Bianco, MR.; Barrera, T.; Cuccunato, M.; Garozzo, A. Quality of voice evaluation in patients treated by supracricoid laryngectomy and modified supracricoid laryngectomy. Otolaryngol Head Neck Surg. 2011, 145, 789–95. [Google Scholar] [CrossRef] [PubMed]
- Allegra, E.; Franco, T. , Trapasso, S., Domanico, R.; La Boria, A.; Garozzo, A. Modified supracricoid laryngectomy: oncological and functional outcomes in the elderly. Clin Interv Aging. 2012, 7, 475–80. [Google Scholar] [CrossRef] [PubMed]
- Saito, K.; Araki, K.; Ogawa, K.; Shiotani, A. Laryngeal function after supracricoid laryngectomy. Otolaryngol Head Neck Surg. 2009, 140, 487–492. [Google Scholar] [CrossRef]
- Schindler, A.; Favero, E.; Nudo, S.; Albera, R.; Schindler, O.; Cavalot, AL. Long-term voice and swallowing modifications after supracricoid laryngectomy: objective, subjective and self-assessment data. Am J Otolaryngol. 2006, 27, 378–383. [Google Scholar] [CrossRef]
- Schindler, A.; Pizzorni, N.; Mozzanica, F.; Fantini, M.; Ginocchio, D.; Bertolin, A.; Crosetti, E.; Succo, G. Functional outcomes after supracricoid laryngectomy: what do we not know and what do we need to know? Eur Arch Otorhinolaryngol. 2016, 273, 3459–3475. [Google Scholar] [CrossRef]
- Lips, M.; Speyer, R.; Zumach, A.; Kross, KW.; Kremer, B. Supracricoid laryngectomy and dysphagia: A systematic literature review. Laryngoscope. 2015, 125, 2143–56. [Google Scholar] [CrossRef]
- Campo, F.; Mazzola, F. : Bianchi, G.; Manciocco, V.; Ralli, M.; Greco, A.; Sperduti, I.; de Vincentiis, M.; Pellini, R. Partial laryngectomy for naïve pT3N0 laryngeal cancer: Systematic review on oncological outcomes. Head & Neck. 2023, 45, 243–250. [Google Scholar]
- Allegra, E.; Bianco, MR.; Ralli, M.; Greco, A.; Angeletti, D.; de Vincentiis, M. Role of Clinical-Demographic Data in Survival Rates of Advanced Laryngeal Cancer. Medicina. 2021, 57, 267. [Google Scholar] [CrossRef]
- Saraniti, C.; Verro, B.; Ciodaro, F.; Galletti, F. Oncological Outcomes of Primary vs. Salvage OPHL Type II: A Systematic Review. Int J Environ Res Public Health. 2022, 19, 1837. [Google Scholar] [CrossRef] [PubMed]
- Laccourreye, O.; Muscatello, L.; Laccourreye, L.; Naudo, P.; Brasnu, D.; Weinstein, G. Supracricoid partial laryngectomy with cricohyoidoepiglottopexy for "early" glottic carcinoma classified as T1-T2N0 invading the anterior commissure. Am J Otolaryngol. 1997, 18, 385–90. [Google Scholar] [CrossRef] [PubMed]
- Atallah, I.; Berta, E.; Coffre, A.; Villa, J.; Reyt, E.; Righini, CA. Supracricoid partial laryngectomy with crico-hyoido-epiglottopexy for glottic carcinoma with anterior commissure involvement. Acta Otorhinolaryngol Ital. 2017, 37, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Alkan, U.; Nachalon, Y.; Shkedy, Y.; Yaniv, D.; Shvero, J.; Popovtzer, A. T1 squamous cell carcinoma of the glottis with anterior commissure involvement: Radiotherapy versus transoral laser microsurgery. Head Neck. 2017, 39, 1101–1105. [Google Scholar] [CrossRef]
- Baird, BJ.; Sung, CK.; Beadle, BM.; Divi, V. Treatment of early-stage laryngeal cancer: A comparison of treatment options. Oral Oncology. 2018, 87, 8–16. [Google Scholar] [CrossRef]
- Campo, F.; Zocchi, J.; Ralli, M.; De Seta, D.; Russo, FY.; Angeletti, D.; Minni, A.; Greco, A.; Pellini, R.; de Vincentiis, M. Laser Microsurgery Versus Radiotherapy Versus Open Partial Laryngectomy for T2 Laryngeal Carcinoma: A Systematic Review of Oncological Outcomes. Ear Nose Throat J. 2021, 100 1_suppl, 51S–58S. [Google Scholar] [CrossRef]
- Succo, G.; Crosetti, E.; Bertolin, A.; Piazza, C.; Molteni, G.; Cirillo, S.; Petracchini, M.; Tascone, M.; Sprio, AE.; Berta, GN.; Peretti, G.; Presutti, L.; Rizzotto, G. Treatment for T3 to T4a laryngeal cancer by open partial horizontal laryngectomies: Prognostic impact of different pathologic tumor subcategories. Head Neck. 2018, 40, 1897–1908. [Google Scholar] [CrossRef]
- de Vincentiis, M.; Greco, A.; Campo, F.; Candelori, F.; Ralli, M.; Di Traglia, M.; Colizza, A.; Cambria, F.; Zocchi, J.; Manciocco, V.; Spriano, G.; Pellini, R. Open partial horizontal laryngectomy for T2-T3-T4a laryngeal cancer: oncological outcomes and prognostic factors of two Italian hospitals. Eur Arch Otorhinolaryngol. 2022, 279, 2997–3004. [Google Scholar] [CrossRef]
- Mattioli, F.; Fermi, M.; Molinari, G.; Capriotti, V.; Melegari, G.; Bertolini, F.; D'Angelo, E.; Tirelli, G.; Presutti, L. pT3 N0 Laryngeal Squamous Cell Carcinoma: Oncologic Outcomes and Prognostic Factors of Surgically Treated Patients. Laryngoscope. 2021, 131, 2262–2268. [Google Scholar] [CrossRef]
- Del Bon, F.; Piazza, C.; Lancini, D.; Paderno, A.; Bosio, P.; Taboni, S.; Morello, R.; Montalto, N.; Missale, F.; Incandela, F.; Marchi, F.; Filauro, M.; Deganello, A.; Peretti, G.; Nicolai, P. Open Partial Horizontal Laryngectomies for T3⁻T4 Laryngeal Cancer: Prognostic Impact of Anterior vs. Posterior Laryngeal Compartmentalization. Cancers (Basel) 2019, 1, 289. [Google Scholar] [CrossRef]
- Campo, F.; Mazzola, F.; Bianchi, G.; Manciocco, V.; Ralli, M.; Greco, A.; Sperduti, I.; de Vincentiis, M.; Pellini, R. Partial laryngectomy for naïve pT3N0 laryngeal cancer: Systematic review on oncological outcomes. Head Neck. 2023, 45, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Zhou, L.; Tao, L.; Zhang, M.; Wu, H.; Chen, X.; Li, X.; Li, C.; Gong, H. Oncologic outcomes of surgical treatment for T3 glottic laryngeal squamous cell carcinoma. Head Neck. 2018, 40, 1734–1742. [Google Scholar] [CrossRef] [PubMed]
- Xia, X.; Zhu, YY.; Diao, WW.; Zhu, XL.; Shi, XH.; Li, WY.; Gao, ZQ.; Li, GJ.; Chen, XM. Matched-pair analysis of survival in the patients with T3 laryngeal squamous cell carcinoma treated with supracricoid partial laryngectomy or total laryngectomy. Onco Targets Ther. 2018, 11, 7947–7953. [Google Scholar] [CrossRef] [PubMed]
- Gallo, A.; Manciocco, V.; Simonelli, M.; Pagliuca, G.; D’Arcangelo, E.; & De Vincentiis, M.; & De Vincentiis, M. . Supracricoid partial laryngectomy in the treatment of laryngeal cancer: univariate and multivariate analysis of prognostic factors. Arch Otolaryngol Head Neck Surg. 2005, 131, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Crosetti, E.; Bertolin, A.; Molteni, G.; Bertotto, I.; Balmativola, D.; Carraro, M.; Sprio, AE.; Berta, GN.; Presutti, L.; Rizzotto, G.; Succo, G. Patterns of recurrence after open partial horizontal laryngectomy types II and III: univariate and logistic regression analysis of risk factors. Acta Otorhinolaryngol Ital. 2019, 39, 235–243. [Google Scholar] [CrossRef]
Figure 1.
5-years overall survival.
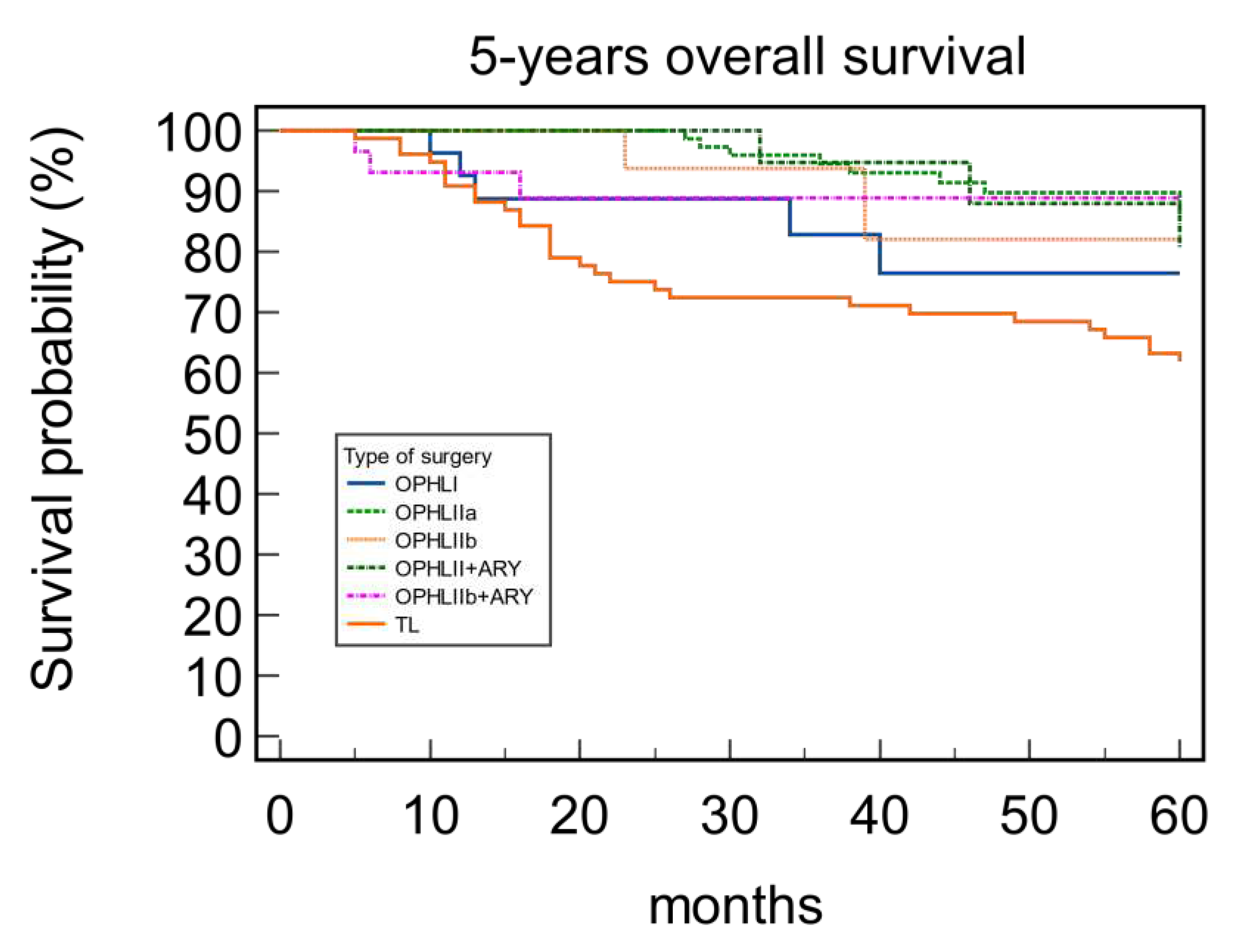
Figure 2.
5-years disease specific survival
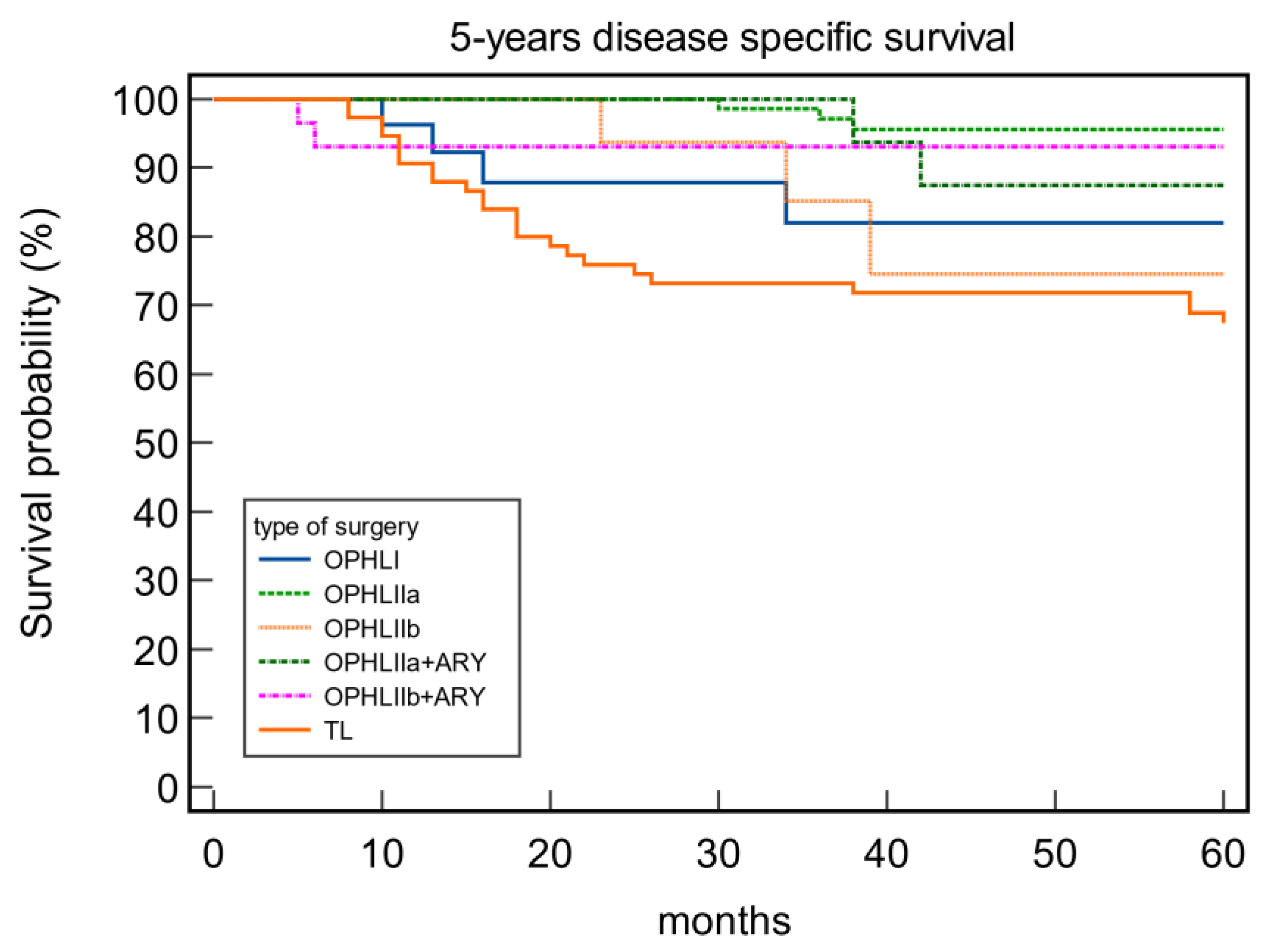
Figure 3.
5-years disease specific survival in pT2 tumors.
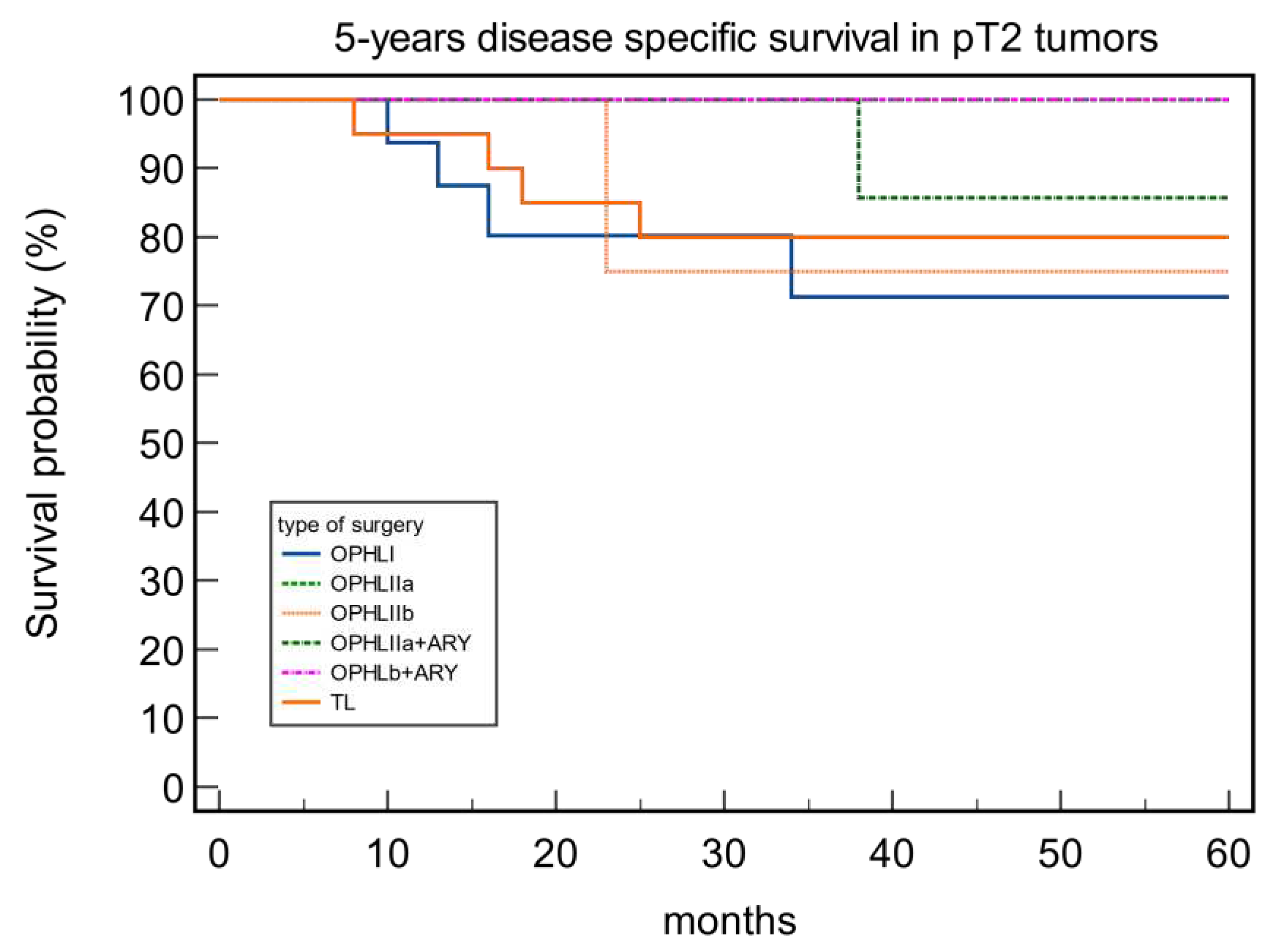
Figure 4.
Figure 4. 5-years disease specific survival in pT3 tumors
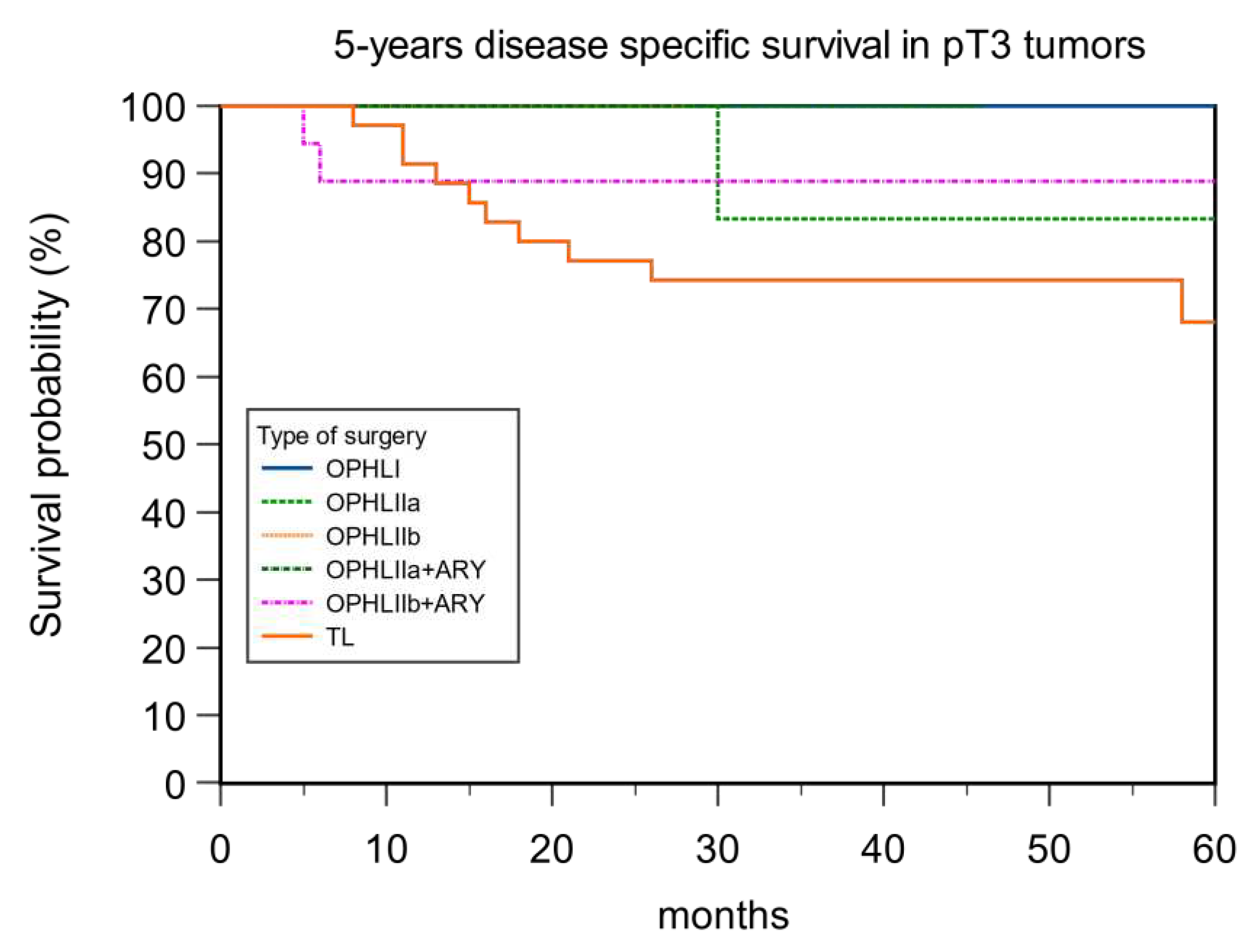
Figure 5.
5-years T recurrence free survival.
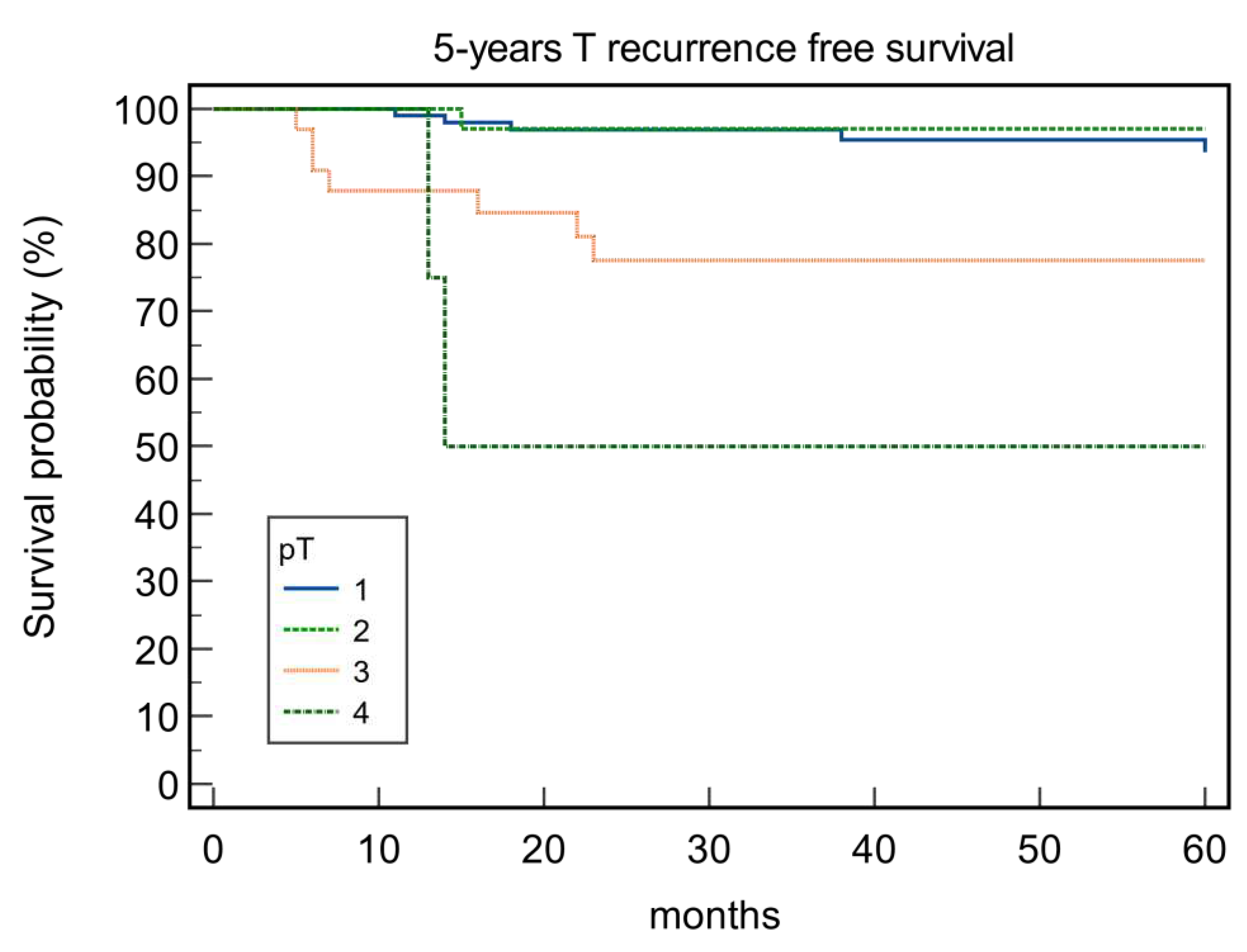
Figure 6.
5-years T recurrence free survival.
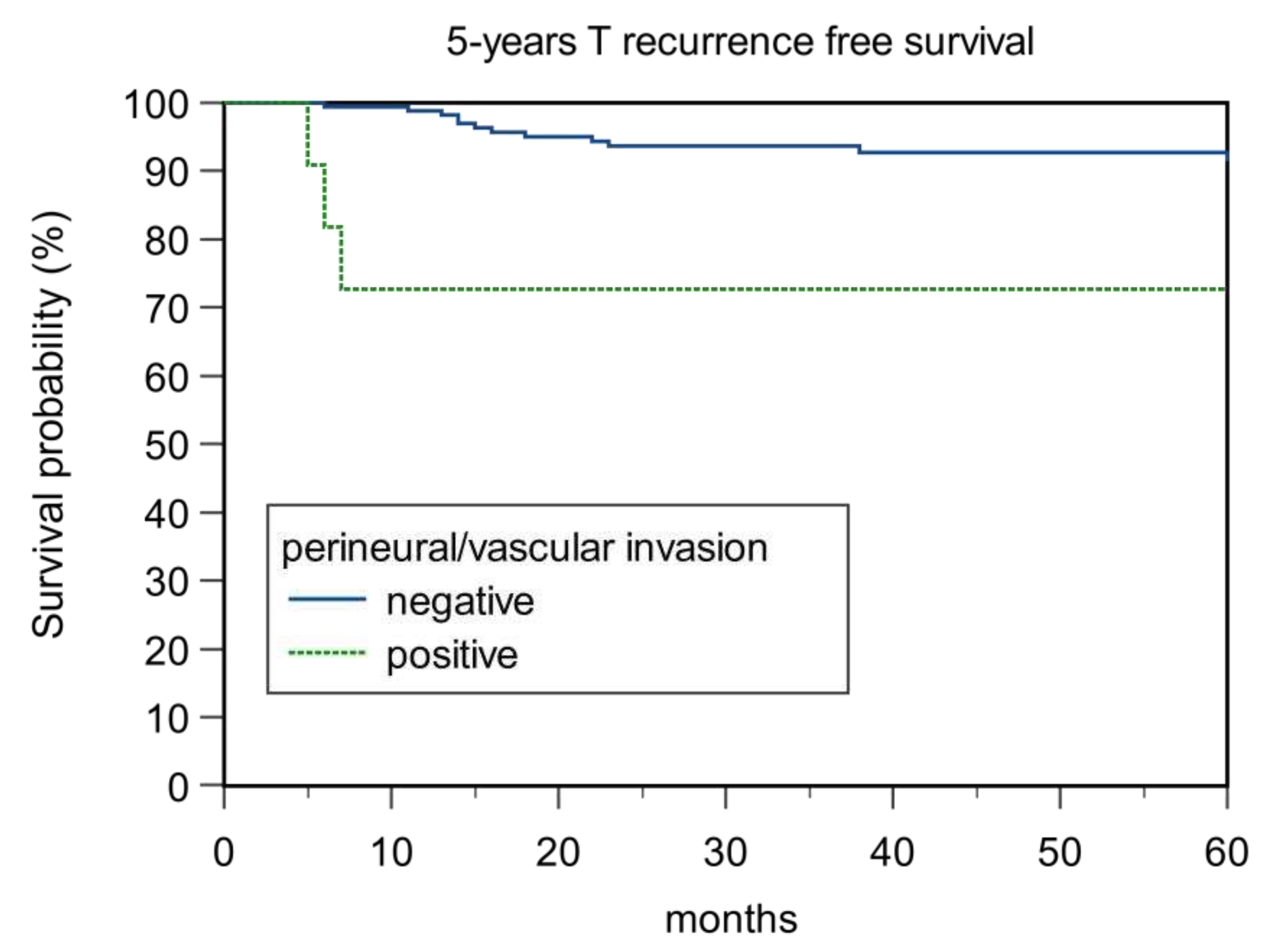
Figure 7.
5-years T recurrence free survival.
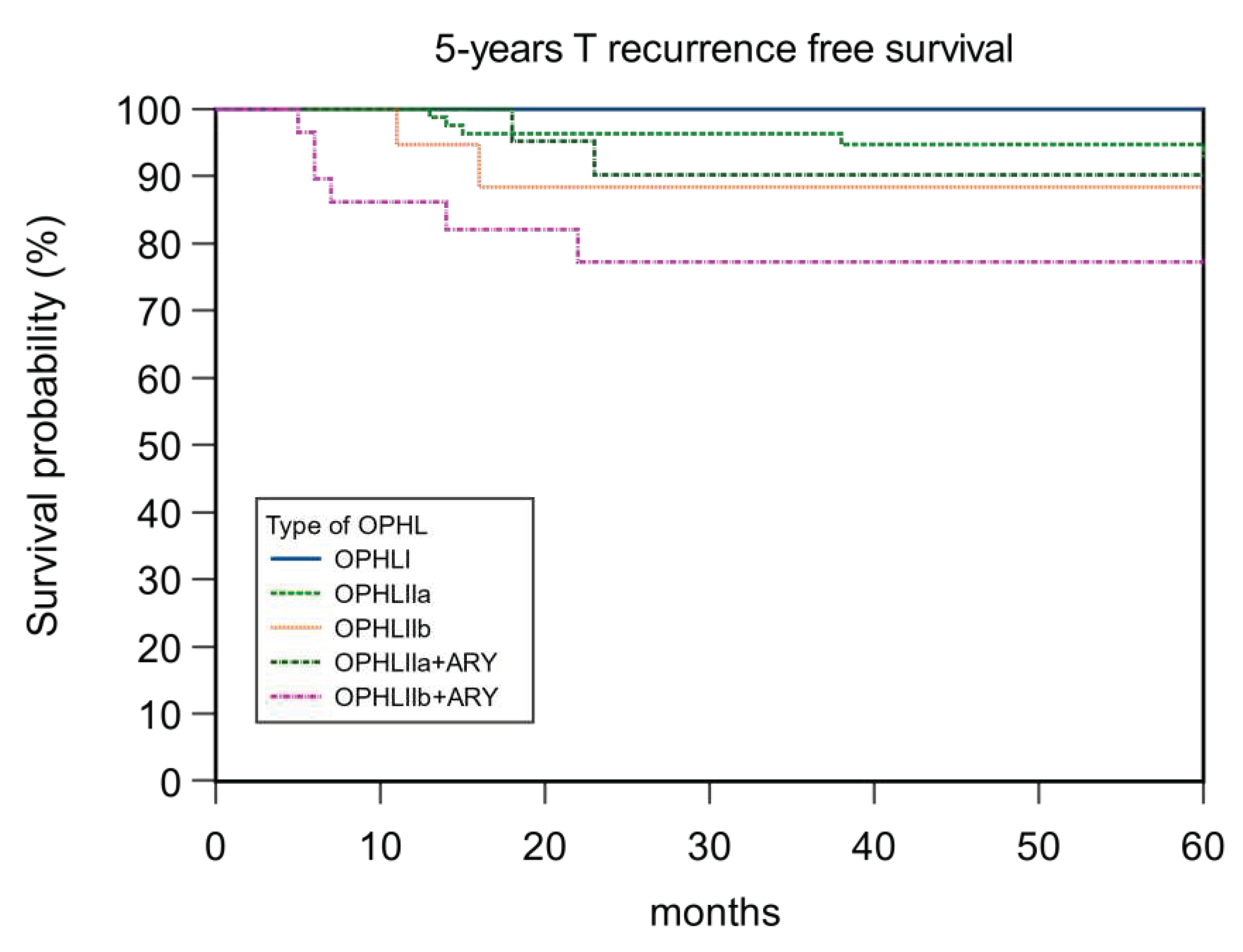

Table 1.
Patients clinical-demographic data.
| Variables | Patients n.182 |
|---|---|
| Age | |
| Mean±SD (years) | 61.3±8.6SD |
| Follow-up | |
| mean±SD(months) | 98.6 ± 34.6SD |
| Sex | |
| M | 166 |
| F | 16 |
| Grading | |
| 1 | 39 |
| 2 | 120 |
| 3 | 23 |
| Subsite | |
| Supraglottic | 34 |
| Glottic | 148 |
| cT STAGE | |
| 1 | 105 |
| 2 | 56 |
| 3 | 21 |
| pT STAGE | |
| 1 | 102 |
| 2 | 43 |
| 3 | 33 |
| 4 | 4 |
| cN STAGE | |
| N0 | 131 |
| N+ | 51 |
| pN STAGE | |
| N0 | 9 |
| N+ | 43 |
| Resection Margins | |
| Negative | 175 |
| Positive | 7 |
| Cartilage Invasion | |
| Negative | 174 |
| Positive | 8 |
| Perineural/Vascular Invasion | |
| Negative | 171 |
| Positive | 11 |
| OPHLs | |
| I | 27 |
| IIa | 84 |
| IIb | 19 |
| IIa+ARY | 23 |
| IIb+ARY | 29 |
Table 2.
Survival rates and clinical variables.
| Variables | OS % | p | DFS% | p | DSS% | p | LFS% | p |
|---|---|---|---|---|---|---|---|---|
| Grading | 0.34 | 0.08 | 0.02 | 0.89 | ||||
| 1 | 92.31 | 84.62 | 94.87 | 92.31 | ||||
| 2 | 88.33 | 84.17 | 94.17 | 92.50 | ||||
| 3 | 78.26 | 65.22 | 78.26 | 95.65 | ||||
| Subsite | 0.12 | 0.82 | 0.04 | 0.10 | ||||
| Glottic | 89.19 | 81.76 | 93.92 | 91.22 | ||||
| Supraglottic | 82.35 | 82.35 | 85.29 | 100 | ||||
| cT Status | 0.29 | 0.003 | 0.037 | 0.10 | ||||
| 1 | 89.52 | 87.62 | 95.24 | 95.24 | ||||
| 2 | 85.71 | 76.79 | 89.29 | 91.07 | ||||
| 3 | 85.71 | 66.67 | 85.71 | 85.71 | ||||
| pT Status | 0.53 | 0.001 | 0.17 | 0.0001 | ||||
| 1 | 89.22 | 88.24 | 95.10 | 95.10 | ||||
| 2 | 83.72 | 76.74 | 86.05 | 97.67 | ||||
| 3 | 87.88 | 75.76 | 90.91 | 84.85 | ||||
| 4 | 100 | 25.00 | 100 | 50.00 | ||||
| cN Status | 0.19 | 0.041 | 0.008 | 0.50 | ||||
| N0 | 88.50 | 83.97 | 94.66 | 93.13 | ||||
| N+ | 86.27 | 76.47 | 86.26 | 92.16 | ||||
| pN Status | 0.08 | 0.008 | 0.06 | 0.008 | ||||
| N0 | 89.21 | 84.89 | 95.53 | 84.89 | ||||
| N+ | 83.72 | 72.09 | 88.37 | 72.09 | ||||
| Resection Margins | 0.35 | 0.86 | 0.47 | 0.41 | ||||
| Negative | 87.36 | 81.61 | 91.95 | 93.10 | ||||
| Positive | 100 | 85.71 | 100 | 85.71 | ||||
| Cartilage invasion | 0.76 | 0.41 | 0.42 | 0.45 | ||||
| Negative | 87.93 | 82.18 | 92.53 | 93.10 | ||||
| Positive | 87.50 | 75.00 | 87.50 | 87.50 | ||||
| Perineural/Vascular Invasion | 0.001 | 0.0006 | <0.0001 | 0.35 | ||||
| Negative | 88.89 | 87.04 | 93.57 | 92.98 | ||||
| Positive | 72.73 | 63.64 | 72.73 | 90.91 | ||||
| OPHL | 0.58 | 0.041 | 0.80 | 0.16 | ||||
| I | 81.48 | 81.48 | 85.19 | 100 | ||||
| IIa | 89.29 | 88.10 | 96.43 | 94.05 | ||||
| IIb | 89.47 | 73.68 | 84.21 | 89.46 | ||||
| IIa+ARY | 86.96 | 78.26 | 93.30 | 91.30 | ||||
| IIb+ARY | 89.66 | 72.41 | 93.10 | 86.21 |
Table 3.
5-years disease specific survival according type of OPHLa on pT2-3 tumors compared to total laryngectomy.
Table 3.
5-years disease specific survival according type of OPHLa on pT2-3 tumors compared to total laryngectomy.
| Type of Surgery | DSS pT2 | DSS pT3 |
|---|---|---|
| OPHL I | 75% | 100% |
| OPHL IIa | 100% | 85.71% |
| OPHL IIb | 75% | 100% |
| OPHLIIa+ARY | 88% | 100% |
| OPHLIIb+ARY | 100% | 88.89% |
| Total Laryngectomy | 80% | 68.57% |
| p value | 0.54 | 0.63 |
Table 4.
Pattern of failure according to the type of OPHLs.
| OPHL I | OPHL IIa | OPHL IIb | OPHL IIa + ARY | OPHL IIb + ARY | Total | p | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N. | % | N. | % | N. | % | N. | % | N. | % | N. | % | ||
| T recurrence | 0 | 0 | 5 | 5.9 | 2 | 10.5 | 2 | 8.6 | 6 | 20.5 | 15 | 8.2 | 0.004 |
| N recurrence | 3 | 11.1 | 4 | 4.7 | 1 | 5.2 | 0 | 0 | 1 | 3.4 | 9 | 4.94 | 0.17 |
| Second/Distant metastasis | 4 | 14.8 | 3 | 3.5 | 0 | 0 | 4 | 17.3 | 2 | 1.8 | 13 | 7.14 | 0.058 |
Table 5.
5-years T recurrence free survival and clinical variables.
| Variables | No Recurrence N.167 |
Recurrence N.15 |
P value |
|---|---|---|---|
|
Grading 1 2 3 |
36 109 22 |
3 11 1 |
0.73 |
|
Subsite Glottic Supraglottic |
133 34 |
15 0 |
0.053 |
|
cT 1 2 3 |
100 51 16 |
5 5 5 |
0.014 |
|
pT 1 2 3 4 |
97 42 26 2 |
5 1 7 2 |
0.0002 |
|
cN N0 N+ |
122 45 |
9 6 |
0.28 |
|
pN N0 N+ |
129 38 |
10 5 |
0.35 |
|
Resection Margin negative positive |
161 6 |
14 1 |
0.55 |
|
Perineural Invasion Negative positive |
159 8 |
12 3 |
0.018 |
|
Cartilage Invasion Negative positive |
160 7 |
14 1 |
0.65 |
|
Type of OPHL I IIa IIb IIa+ARY IIb+ARY |
27 79 17 21 23 |
0 5 2 2 6 |
0.0049 |
Table 6.
Correlation between clinical variables and laryngectomy free.
| Variables | Laryngectomy Free Yes Not N.% N.% |
p |
|---|---|---|
|
Grading 1 2 3 |
36 3 111 9 22 1 |
0.89 |
|
Subsite Glottic Supraglottic |
135 13 34 0 |
0.13 |
|
cT status 1 2 3 |
100 5 51 5 18 3 |
0.09 |
|
pT status 1 2 3 4 |
97 5 42 1 28 5 2 2 |
0.0009 |
|
cN status N0 N+ |
122 9 47 4 |
0.81 |
|
pN status N0 N+ |
129 10 40 3 |
0.96 |
|
Resection margins Negative Positive |
163 12 6 1 |
0.45 |
|
Cartilage invasion Negative Positive |
162 12 7 1 |
0.45 |
|
Periveural/Vascular Invasion Negative Positive |
159 12 10 1 |
0.79 |
|
OPHL I IIa IIb IIa+ARY IIb+ARY |
27 0 79 5 17 2 21 2 25 4 |
0.046 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



