
Submitted:
04 August 2023
Posted:
09 August 2023
You are already at the latest version
Abstract
Per- and polyfluoroalkyl substances (PFASs) are a group of fluorinated, organic, man-made chemicals; they do not occur naturally in the environment. This study aimed to determine the profile and content of PFASs in volunteers’ blood plasma and urine after fermented red beetroot juice consumption and correlated it with the blood parameters. During 42 days, 24 healthy volunteers intake 200 mL/60 kg of body weight fermented red beetroot juice. PFASs were analyzed using micro-HPLC-MS/MS method. Five perfluoroalkyl substances were found in human body fluids. After juice consumption, PFASs, due to the consumption of food contaminated with them, was discovered that for perfluorocarboxylic acids, a downward trend was observed, while for perfluoroalkane sulfonates, their plasma content showed a statistically significant upward trend. Analysis of the hematology parameters indicated that the intake the fermented red beetroot juice showed a significant decrease in mean corpuscular volume (MCV), platelets concentration, mean platelet volume (MPV), platelet large cell ratio (P-LCR) at the significance level p < 0.01, and he-matocrit (p < 0.05). On the other hand, the dietary intervention also indicated a significant (p < 0.01) increase corpuscular/ cellular hemoglobin concentration (MCHC). In the case of blood biochemi-stry, no significant change in blood samples after intake the fermented beetroot juice was observed. However, a decreasing tendency of total cholesterol and low-density lipoprotein concentration (LDL-C) were observed. Based on the presented results, there is a need to analyze and monitor health-promoting food regarding undesirable substances and their impact on consumer health.
Keywords:
perfluoroalkyl substances
; fermented red beetroot juice
; human body fluids
; blood parameters
1. Introduction
Nowadays, it is believed that the vegetables and food obtained from them are a crucial part of the daily human diet [1]. These products are considered one of the best sources of essential nutrients and bioactive compounds [2]. In addition, many studies suggest that the intake of vegetables positively affects consumer health. Regular consumption of vegetables can positively affect the prevention of many diseases, such as cancer (colorectal and breast cancer [3,4]) and cardiovascular diseases [5].
Red beetroot (Beta vulgaris L. subsp. vulgaris) is one of the most popular vegetables with a valuable source of vitamins, minerals, and bioactive compounds [6]. Due to the high contents of phytochemicals, intake of this vegetable may indicate positive, beneficial effects for consumers. Red beetroot shows anti-neurodegenerative, antitumor, anti-inflammatory, antibacterial, antiviral, cardioprotective, and lipid peroxidation inhibitory activities [7]. Moreover, this vegetable is trendy in the food industry. It produces many red beetroot products or additives (drinking and concentrated juices, yoghurts, and frozen foods) and prepares natural red dyes [6]. On the other hand, red beetroot may contain other compounds, such as perfluoroalkyl substances (PFASs) [2].
These molecules are a wide range of synthetic organofluorine compounds which have been based used in the industry [8]. They are a group of organofluorine compounds, aliphatic hydrocarbons, in which all or almost all hydrogen atoms are replaced with fluorine. They consist of a hydrophobic alkyl chain of varying lengths (typically C4 to C16) and a hydrophilic end group, which may be fully or partially fluorinated. PFASs are classified as persistent and bioaccumulative substances [9]. They are a diverse group of compounds with high thermal, chemical, and biological inertness [10,11]. PFASs remain stable in the presence of acids, bases, oxidants, and reductants. Furthermore, they exhibit high resistance to degradation by photolytic or metabolic processes and microbial decomposition. Nevertheless, their widespread use led to contamination of the environment, which, as a consequence, led to the exposure of these compounds in humans and animals [8,12]. PFAAs are ubiquitous in various environmental media and are distributed globally. Due to their ability to migrate, they can be transferred from water to soils, taken up by plants, and thus enter the food chain. These substances enter the human body through the digestive, respiratory systems, and skin. Moreover, they are not metabolized and accumulate in the body [13]. Furthermore, direct and indirect contact with PFAS-containing materials such as oil and water-resistant materials, detergents, paints, and fabrics causes high exposure of humans to their toxic properties [11]. In living organisms, high absorption levels and low elimination rates of PFASs have been observed [14].
Researchers confirmed that PFASs exist in human and animal tissues and blood (serum or plasma). Studies indicated that anionic PFASs were detected primarily in the human plasma/serum [15]. Biomonitoring of PFASs in the human body started in 2000. Many PFASs have been detected in human matrices, most commonly in blood samples [16,17]. In recent years, a number of papers have confirmed the occurrence of these compounds in breast milk [18], seminal plasma [19], umbilical cord blood [20], and liver [21]. However, in contrast to most other persistent organic pollutants (POPs), they do not tend to accumulate in fat tissues but bind to serum albumin and other cytosolic proteins and accumulate mainly in the liver, the kidneys, and bile secretion [22,23]. In addition, positive associations were observed between levels of PFOS and PFOA detected in serum, and total cholesterol, low-density lipoprotein cholesterol, thyroxine and thyroid hormone concentrations [24,25].
PFASs are extensively applied in various industrial and consumer goods. Fluorosurfactants are more effective and efficient in surface activity than their hydrogenated analogues. These and other properties, such as high thermal, chemical, and biological stabilities, make PFASs perfect material for industrial and domestic applications [26,27]. Typical applications encompass the automotive and aviation industries (hydraulic fluids, low-friction bearings and seals, and materials for car interiors), construction technology (paints and coating additives and glues), biocides (herbicides and pesticides), electronics (flame retardants, weather resistant coatings, and insulators), household products (wetting and cleaning agents, nonstick coatings, and components of cosmetic formulations), medical articles (stain and water repellents in surgical equipment, raw materials for implants), and packaging materials (oil and grease repellent materials) and textiles (impregnating agents for fabrics, leather, and breathable membranes) [11,28,29].
Due to the presence of PFAAs in ambient air, various consumer products, drinking water, and food, it has become necessary to assess their potential impact on human health accurately. Researchers have reviewed the occurrence of highly fluorinated compounds in human matrices in recent years, and there is indisputable evidence that their bioaccumulation potential in tissues is high [30,31]. However, there is uncertainty regarding the accumulation processes themselves and the acute or chronic toxicity effects due to variation of observed toxic response to PFAAs between species and genders within tested species. Varieties of PFASs have been detected in human blood (both in serum and plasma) [8,17,32,33] as well as in the umbilical cord [34,35] and maternal [36,37] blood. Besides blood, some PFASs have also been found in other human tissues. PFASs were predominantly found in the liver [38,39]. Furthermore, studies show some accumulation potential in the lungs, kidneys, bones, and the brain [40]. Numerous recent studies have confirmed their presence in seminal plasma [19], breast milk [41] of lactating mothers, and umbilical cord blood, all drawing attention to their influence on the human reproductive system. In conjunction with the bioaccumulation and biomagnification potential of PFASs, these long half-lives can give rise to various processes within the living cell and lead to concern over their potential hazard to human health. Because of their capacity to modify surface properties, even on the molecular level, it is essential to elucidate their toxicity and toxicokinetic activity [42].
Both PFOA and PFOS have shown moderate acute toxicity via ingestion. The oral LD50 levels assessed for PFOS were 230 and 270 mg kg−g bw for male and female rats, respectively [43]. In contrast to PFOS, PFOA is moderately toxic. The LD50 value in rats ranged from 430 to 680 mg kg−g bw [44]. The suspected toxic effects of PFASs include the following: liver toxicity, including liver hypertrophy [45,46]; liver cancer [47]; disruption of lipid metabolism due to their effect on serum cholesterol and triglyceride levels [16,48]; function of the immune system, causing atrophy of the thymus and spleen or suppressed antibody responses [49,50,51]; function of the endocrine system due to their effects on thyroid hormone levels (triiodothyronine (T3) and thyroxine (T4)) [52,53]; induction of adverse neurobehavioral reactions [54]; tumor formation [55]; prenatal and neonatal toxicity [16]; decreased birth weight and size [56]; and even obesity [57]. Several studies cover the putative modes of action of PFASs on a cellular level, but these mechanisms still need to be fully defined. Nevertheless, due to the structural similarities of PFASs to endogenous fatty acids, these reactions can be partly attributed to their morphology, more precisely to activity resulting from their chemical structure. PFASs are characterized by the high tendency to noncovalent, intracellular binding to β-lipoproteins, albumin, and other plasma proteins, such as fatty acid-binding protein (L-FABP) [22]. The proliferation of peroxisomes is one of the main reasons for liver toxicity observed in laboratory animal studies.
Considering all the aspects, this study aimed to determine the perfluoroalkyl substances' content in fermented red beetroot juice and human body fluids (blood plasma and urine) before and after intake of this product. The novelty of the work lies in linking dietary exposure to PFASs and blood parameters, bringing a new perspective to our understanding of these compounds. To our best knowledge, this paper is the first detailed and cross-sectional investigation of selected perfluoroalkyl substances in human body fluids after exposure to fermented red beetroot juice.
2. Results and discussion
2.1. Perfluoroalkyl substances content
The content of perfluoroalkyl substances was tested in fermented red beetroot juice and human body fluids (blood plasma and urine) of volunteers before and after intake of these products (Table 1). In urine samples, PFOA was the only perfluoroalkyl substance found in trace amounts (<LOQ). This confirms the information found in the literature that these compounds metabolize very poorly; thus they are excreted from the human body very poorly; they only accumulate in it, which makes them even more dangerous [13]. For PFAS, a high absorption level is observed with a low elimination rate of the substance [14]. Available epidemiological studies support an association between exposure to certain PFASs and various health outcomes, including altered immune and thyroid function, liver disease, lipid and insulin dysregulation, kidney disease, adverse reproductive and developmental effects, and cancer [58].
In the tested fermented red beetroot juice, among the analyzed PFAS, only the most common perfluoroalkyl substance apart from PFOS, i.e. PFOA, was identified, the content of which was 0.099±0.07 ng/mL. There are many scientific articles about fermented red beetroot juice. They concern the range of volatile or bioactive compounds of the polyphenols and red and yellow betalains. Still, none relate to the contained contaminants, in particular perfluoroalkyl substances. To our best knowledge, this paper is the first detailed and cross-sectional investigation of selected perfluoroalkyl substances in human body fluids after exposure to fermented red beetroot juice. Same with red beetroot, recent modern studies have shown a variety of health benefits for it and its active compounds, betalains (also betanin) as antioxidative, anti-inflammation, anticancer, blood pressure and lipid lowering, also antidiabetic and anti-obesity effects. Still, it's hard to find information about its contamination, especially with PFASs. In their study, Sznajder-Karatzyńska et al. [2] investigated 55 samples of locally – grown and imported fruit and vegetable. Among other, they determined the content of 10 PFASs in red beetroot. In this case, the only identified PFASs was PFOA, and its content ranged from 0.050 to 0.090 (ng g-1 ww). For beetroot, the frequency of its occurrence was 100%. There is no possibility to compare these data with the limits provided by the relevant agencies because they have not been established and do not exist. On August 26, 2022,only Recommendation (EU) 2022/1431 on monitoring the presence of perfluoroalkyl substances in food was issued. Also, Herzke et al. [59] studied the contamination of vegetables by PFASs and reported that perfluorocarboxylic acids were the most frequently detected substances, with PFOA as the most abundant group. Its concentration was found between 0.008 and 0.121 ng g−1 of fresh weight. These findings are in good agreement with our study.
In the case of volunteers' blood plasma collected before and after fermented red beetroot juice intake, no statistical difference was observed in the median value of the content of perfluoroalkyl acids (Table 2). Among the 24 volunteers tested, an upward trend in PFOA content was observed for 5 people. A downward trend in the median value was observed for the other identified perfluorocarboxylic acids, PFDA and PFNA (Table 2). And for individual results, in the case of PFNA and 10 volunteers, there was a statistically significant decrease in the analyte content in the tested blood plasma samples, while PFDA in as many as 14. The sum of the determined acids also showed a statistically significant downward trend (Table 2), which can be explained by the fact that excluding the consumption of certain products (which was required by the assumptions of the experiment), the supply of perfluoroalkyl acids was limited. These compounds are in significant amounts in packaging dedicated to food storage [25], thus getting into the human body. Reducing the consumption of processed food thus resulted in a decrease in the supply of these specific compounds in the diet.
In the case of the determined perfluoroalkane sulfonates, a statistically significant upward trend was observed (p<0.01). Such a situation took place both for individually identified compounds, i.e. PFOS (14 volunteers) and PFHS (22 volunteers) and for their sum (Table 2). This slight but statistically significant increase could have been caused by the supply of other food products consumed by the volunteers.
2.2. Blood parameters
To the best of the authors’ knowledge, this study is the first to show the effect of a six-week intake of fermented beetroot juice on the twelve hematology and five blood biochemistry parameters.
The blood parameter values before and after the intervention are presented in Table 3. Analysis of the hematology parameters indicated that the intake of the fermented beetroot juice showed a significant decrease of MCV, platelets concentration, MPV, and P-LCR at the significance level p < 0.01 and hematocrit (p < 0.05). On the other hand, the dietary intervention also indicated a significant (p < 0.01) increase in corpuscular/ cellular hemoglobin concentration (MCHC). In the case of blood biochemistry, no significant change in blood samples after intake of the fermented beetroot juice was observed (Table 3). However, a decreasing tendency of total cholesterol and LDL-C concentration were observed. Previously published data showed an ambiguous influence of red beet products on blood parameters.
Nevertheless, the previous studies investigated only the three blood parameters: total cholesterol, LDL-C and HDL-C [60,61]. The study by de Castro et al. [60] conducted on volunteers with overweight/obesity and dyslipidemia who consumed freeze-dried red beet leaves (2.5 g/ day) for four weeks showed a significant reduction of LDL. However, in our study, as mentioned above, the concentration of LDL shows only a decrease tendency. Also, no statistical difference in the total cholesterol concentration before and after the intervention was observed in the cited study. In turn, the study by Asgary et al. [61] showed a significant reduction of total cholesterol and LDL-C after consumption of raw beetroot juice (250 mL/day) by two weeks.
On the other hand, Asgary et al. [61] noticed no significant changes in the case of these same parameters (total cholesterol and LDL-C) after intake of cooked beetroots (250 mg/ day). The blood parameters may affect the red beet product (food matrix) type, dose and intervention time. It should be mentioned that beetroot is rich in several bioactive compounds, i.e. betalains, phenolics, carotenoids, minerals and vitamins [62], which may affect the blood parameters tested.
Changes in blood parameters may signal adverse health effects caused by, e.g. nutritional intervention. One of the blood parameters that showed a decrease after consuming fermented beetroot juice was MCV. MCV is routinely measured in blood tests and is generally used to help classify the cause of anaemia [63]. We observed that platelet-related parameters, such as platelet count, MPV, and P-LCR, decreased in blood samples analyzed after nutritional intervention. Generally, platelet count determines bleeding risk and monitors thrombopoiesis [64]. Moreover, increasing evidence describes the important role of platelets in physiological processes such as immune response, angiogenesis and fibrosis formation [64,65]. This suggests that platelets independently influence morbidity and mortality rather than merely reflecting underlying disease. An abnormal platelet count indicates poor prognosis in some patient groups, including in cancer and in critically ill patients [64,66,67].
The correlation between the individual PFAS compounds, total perfluorocarboxilic acids, perfluoroalkane sulfonates and PFASs and blood parameters were presented in Figure 1. Before intervention, moderate positive correlations (0.3 ≤ r < 0.5) were observed between PFHS and erythrocytes, hemoglobin and hematocrit. Also, a moderate positive correlation was calculated between total perfluoroalkane sulfonates and erythrocytes. A good negative correlation (0.5 to < 0.7) was observed between RDW-CV and PFOA, while moderate negative correlations were determined between RDW-CV and PFNA, total perfluorocarboxilic acids and total PFASs. Additionally, moderate positive correlations were observed between glycated hemoglobin, PFOS, PFHS and total perfluoroalkane sulfonates. Moreover, before the intervention, a positive tendency was observed between PFOS and erythrocytes and LDL-C and between total perfluoroalkane sulfonates and hemoglobin, hematocrit and LDL-C. A negative trend was found between total perfluoroalkane sulfonates and HDL-C. On the other hand, after diet intervention moderate negative correlation was only observed between cholesterol HDL and PFHS (Figure 1). A negative tendency was observed between PFOS, total perfluoroalkane sulfonates and HDL-C. Moreover, a positive tendency was noticed after intake of the fermented beetroot juice between PFOS, total perfluoroalkane sulfonates and erythrocytes and total PFAs and hemoglobin.
However, some limitations of the study should be taken into account. First, the lack of control over food intake and potential sources of PFASs. Second, we assessed blood parameters on two points that may not account for intra-individual variability in blood parameters. Also, the number of participants participating in the study was relatively small, which could not show unambiguous statistical differences between individual parameters.
3. Materials and Methods
3.1. The Chemicals, reagents, and study material
Gradient reagents, including methanol, acetonitrile, formic acid, and water, were purchased from Sigma Chemical Co. (St. Louis, MO, USA). A native standard mixture of PFASs containing seven perfluorocarboxylic acids (PFCAs) such as perfluorobutanoic acid (PFBA), perfluoropentanoic acid (PFPeA), perfluorohexanoic acid (PFHxA), perfluoroheptanoic acid (PFHpA), perfluorooctanoic acid (PFOA), perfluorononanoic acid (PFNA) and perfluorodecanoic acid (PFDA) and three perfluoroalkane sulfonates (PFSAs), namely perfluorobutane sulfonate (PFBS), perfluorohexane sulfonate (PFHxS) and perfluorooctane sulfonate (PFOS) prepared in methanol, with chemical purity of >98% each, purchased from Wellington Laboratories, Inc., (Guelph, ON, Canada). The isotopically labelled internal standards (ISs): perfluoro-n-[13C8] octanoic acid (13C8-PFOA) in methanol, with chemical purity of >98%, and sodium perfluoro-1-[13C8] octane sulfonate (13C8-PFOS) in methanol, with chemical purity of >98%, were obtained from Wellington Laboratories, Inc., (Guelph, ON, Canada). Auxiliary equipment such as MPW-351R Centrifuge (MPW Med. Instruments, Warsaw, Poland), Vacuum Concentrator Plus (Eppendorf AG, Hamburg, Germany) and ultrasonicator were used for sample preparation.
Stock, intermediate and working standard solutions of native PFASs and internal standards (13C8-PFOA and 13C8-PFOS named IS1 and IS2, respectively) were prepared in MeCN. Intermediate and working standard solutions of native PFASs with concentrations of 100 ng/mL and 1 ng/mL, respectively, were prepared by diluting the standards with the mixture of 20% MeOH in water (v/v) with the addition of 1% (v/v) of FA. Internal standard solutions were prepared according to the above procedure.
Fermented red beetroot juice was specially prepared for this study by the fruit and vegetable processing company s headquartered in Poland.
3.2. Characteristic of participants and study design
The subjects who met the inclusion criteria (body mass index (BMI) under 30; without gastrointestinal disturbances, including gastric and duodenal ulcers; they could not participate in other clinical trials within 90 days before the survey, take drugs, abuse alcohol, be pregnant and breast-feeding, or take any medications or vitamin supplements), and they had to be certified healthy at a medical interview were accepted to the study. Ultimately, 24 healthy subjects, 5 males and 19 females, aged between 24 and 40, participated in the experiment (Table 4).
The study was conducted for six weeks (42 days). For 42 days, once a day, volunteers consumed a dose of the fermented beetroot juice (200 mL/60 kg of body weight) directly after breakfast. Every 7 days, the health status of all volunteers was assessed by the doctor, and they received the fermented beetroot juice for the next week. Under fasting conditions, before consumption (sample zero), and at the end of the experiment, the blood samples were taken into heparinized vacutainers and then centrifuged (500 × g, 15 min, 1000 × g, 10 min, 4°C). According to the above sampling scheme (0 and 42 days), urine samples were collected from the volunteers. After that, the separated plasma and collected urine were frozen and stored at 80°C until analysis. The study design is presented in Figure 2.
3.3. Ethical aspects
The experimental design and procedure were accepted by the Bioethical Committee at the Faculty of Medical Science of the University of Warmia and Mazury in Olsztyn (Poland, No. 7/2015). All volunteers were fully informed about the potential benefits and risks and signed an informed consent form. Moreover, the study was conducted under medical supervision in the NZOZ Atarax Clinic in Olsztyn, Poland.
3.4. Plasma and urine samples preparation
The content of perfluoroalkyl substances was determined in the plasma and urine samples. The plasma samples were prepared according to Rotander et al. [68]. Briefly: 200 µL of plasma with 4 µL of ISs solution (2.5 µg mL-1) was extracted with 1.5 mL 100% acetonitrile (MeCN) using ultrasonication followed by vortex extraction, centrifugation and evaporation to dryness in a vacuum concentrator. The residue was reconstituted with 100 µL of MeOH. Before the micro-HPLC-MS/MS analysis, samples were diluted fivefold in deionised water with 1% (v/v) of FA addition to the final volume of 500 µL. The same analytical procedure was applied to blank samples. Each sample for the assay was prepared in triplicate.
The urine samples were prepared according to Perez et al. [69]. Briefly: 500 µL of urine with 3.2 µL of ISs solution (2.5 µg mL-1) was mixed. Precipitation of traces of protein was induced by mixing the samples with acetonitrile (1:1). After centrifugation at 4000 rpm for 10 min, 400 µL of the supernatant was transferred to a PP tube and evaporation to dryness in a vacuum concentrator. The residue was reconstituted with 80 µL of MeOH. Before the micro-HPLC-MS/MS analysis, samples were diluted fivefold in deionised water with 1% (v/v) of FA addition to the final volume of 400 µL. The same analytical procedure was applied to blank samples. Each sample for the assay was prepared in triplicate.
3.5. Instrumental analysis
The investigated substances were analyzed by micro-HPLC/MS/MS with negative ion electrospray ionization (ESI) and Multiple Reaction Monitoring (MRM) mode. Chromatographic separation was carried out using an Eksigent LC200 System (AB SCIEX, Concord, Canada). The column used was HALO C18 column 50 mm x 0.5 mm x 2.7 µm (Eksigent, Concord, Canada), and it was termostated at the temperature of 45 °C with the mobile phase flow rate of 20 µL/min. A binary gradient consisting of water (A) and MeCN (B) (both with 0.1 % FA) was applied. The gradient was set as follows: 40% B (0-0.5 min), 40-90% B (0.5-3.0 min), 90% B (3.0-4.0 min), 90-40% B (4.0-4.2 min) and 40% B (4.2-5.0 min). The injection volume was 5 µL. The autosampler temperature was set at 40 °C. The mass spectrometer used was QTRAP 5500 with ESI (AB SCIEX, Concord, Canada). The optimal sensitivity for the investigated PFASs was obtained under the following settings: curtain gas flow: 25 L/min, collision gas flow: 9 L/min, ion spray voltage: -4500 V, temperature: 350 °C, 1 ion source gas flow: 30 L/min, 2 ion source gas flow: 35 L/min, declustering potential range: -30 to -85 V, entrance potential: -10 V, collision energy range: -10 to -65 eV and collision cell exit potential range: -10 to -38 V [70]. Quantitative analyses were performed using the multiple reaction monitoring (MRM) mode. Data analysis was done with Analyst Software (AB SCIEX, Concord, Canada) (version 1.5.2).
3.6. Analysis of blood parameters
The analysis of blood samples was conducted by the Medical Diagnostic Laboratory of the Provincial Specialist Hospital in Olsztyn, Poland. The blood hematology parameters included leukocytes, erythrocytes, hemoglobin, hematocrit, mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular/cellular hemoglobin concentration (MCHC), platelets, red cell distribution width (RDW-CV), platelet distribution width (PDW), mean platelet volume (MPV), and platelet large cell ratio (P-LCR), also was measured blood biochemistry parameters which included lipid profile (total cholesterol, triglycerides, high-density lipoprotein (HDL), low-density lipoprotein (LDL) and glycated hemoglobin.
3.7. Statistical analysis
Statistical analysis were performed using Statistica software (v. 13, StatSoft, Tulsa, Ok, USA). The normal distribution of the data was evaluated using a Shapiro-Wilk W test. The tested groups showed a non-normal distribution, therefore, quantitative variables are expressed as median (P25-P75). Comparisons within the groups, between the baseline and after the exposure to the fermented red beetroot juice, were performed using Wilcoxon signed-rank tests. Correlations between the concentration of individual PFASs, total acids, total sulfonates, total PFASs and blood parameters (leukocytes, erythrocytes, hemoglobin, hematocrit, MCV, MCH, MCHC, platelets, RDW-CV, PDW, MPV, P-LCR, total cholesterol, cholesterol HDL, cholesterol LDL, triglycerides, glycated hemoglobin) were analyzed using a Pearson correlation coefficient test. Statistical significance thresholds were set at p < 0.05 (*) and p < 0.01 (**). The strength of the correlation was described as fair (<0.3), moderate (0.3 to <0.5), good (0.5 to <0.7), or very good (≥0.7) [71].
4. Conclusions
This type of experiment was carried out for the first time, and although we cannot draw clear conclusions regarding the increase in the content of perfluoroalkyl substances in human body fluids due to the consumption of food contaminated with them, it proves that such research is necessary and should be continued. In the case of perfluorocarboxylic acids, a downward trend was observed, while perfluoroalkane sulfonates' plasma content showed a statistically significant upward trend. This confirms previous scientific data that these compounds metabolize very poorly; therefore, they are very poorly excreted from the human body; they only accumulate in it, which makes them even more dangerous for the consumer. On the other hand, it has been observed that fermented red beetroot juice can affect blood parameters. The effect of beetroot products depends on the type of food matrix, dose and time of intervention. It is worth mentioning that beetroot is rich in several bioactive compounds (betalains, phenols, carotenoids, minerals and vitamins) that can have a synergistic effect on the blood parameters tested.
More research is needed to determine the sources and impact of PFASs on consumer health. Ongoing research is critical to developing future strategies to control consumer exposure to PFASs and points to areas for further improvement of multidisciplinary collaboration.
Author Contributions
Conceptualization, M.S. and W.W.; methodology, M.S. and W.W.; formal analysis, M.S., T.S.; investigation, M.S., W.W., T.S.; resources, M.P., W.W; data curation, M.S.; writing—original draft preparation, M.S., T.S.; writing—review and editing, M.P., W.W.; visualization, T.S.; supervision, M.P.; project administration, W.W, M.P.; funding acquisition, M.P., W.W. All authors have read and agreed to the published version of the manuscript.
Funding
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
This work was supported by Institute of Animal Reproduction and Food Research Polish Academy of Science in Olsztyn project grants under the statutory subsidy - GW3, The impact of the consumption of food phytochemicals on the metabolomic profile of consumers.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ellegrad, L.H.; Andersson, S.W.; Normen, A.L.; Andersson, H.A. Dietary plants sterols and cholesterol metabolism. Nutr. Rev. 2007, 65, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Sznajder-Katarzyńska, K.; Surma, M.; Cieślik, E.; Wiczkowski, W. The perfluoroalkyl substances (PFASs) contamination of fruits and vegetables. Food Addit. Contam. Part A 2018, 35, 1776–1786. [Google Scholar] [CrossRef]
- Bradbury, K.E.; Appleby, P.N.; Key, T.J. Fruit, vegetable, and fiber intake in relation to cancer risk: findings from the European Prospective Investigation into Cancer and Nutrition. Am. J. Clin. Nutr. 2014, 100, 394S–398S. [Google Scholar] [CrossRef] [PubMed]
- Farvid, M.S.; Chen, W.Y.; Rosner, B.A.; Rulla, M.T.; Willett, W.C.; Eliassen, A.H. Fruit and vegetable consumption and breast cancer incidence: Repeated measures over 30 years of follow-up. Int. J. Cancr 2018, 144, 1496–1510. [Google Scholar] [CrossRef]
- Zhan, J.; Liu, Y.J.; Cai, L.B.; Xu, F.-R.; Xie. T.; He, Q.-Q. Fruit and vegetable consumption and risk of cardiovascular disease: A meta-analysis of prospective cohort studies. Crit. Revi. Food Sci. Nutr. 2017, 57, 1650–1663. [Google Scholar] [CrossRef] [PubMed]
- Płatosz, N.; Sawicki. T.; Wiczkowski, W. Profle of phenolic acids and flavonoids of red beet and its fermentation products. Does long-term consumption of fermented beetroot juice affect phenolics profle in human blood plasma and urine? Polish J. Food Nutr. Sci. 2020, 70, 55–65. [Google Scholar] [CrossRef]
- Crawford, N.M.; Fenton, S.E.; Strynar, M.; Hines, E.P.; Pritchard, D.A.; Steiner, A.Z. Effects of perfluorinated chemicals on thyroid function, markers ofovarian reserve, and natural fertility. Reprod. Toxicol. 2017, 69, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Poothong, S.; Thomsec, C.; Padilla-Sanchez, J.A.; Papadopoulou, E.; Haug, L.S. Distribution of novel and well-know poly-and perfluoroalkyl substances (PFASs) in human serum, plasma, and whole blood. Environ. Sci. Technol. 2017, 51, 13388–13396. [Google Scholar] [CrossRef]
- JOGSTEN I.E., PERELLO G., LLEBARIA X., BIGAS E., MARTI-CID R., KARRMAN A., DOMINGO J.L., Exposure to perfluorinated compounds in Catalonia, Spain, through consumption of various raw and cooked foodstuffs, including packaged food. Food Chem. Toxicol., 47, (7), 1577, 2009. 1577; 47.
- A. B. Lindstrom, M. J. Strynar, and E. L. Libelo, “Polyfluorinated compounds: past, present, and future,” Environmental Science & Technology, vol. 45, no. 19, pp. 7954–7961, 2011.
- M. P. Krafft and J. G. Riess, “Per- and polyfluorinated substances (PFASs): environmental challenges,” Current Opinion in Colloid & Interface Science, vol. 20, no. 3, pp. 192–212, 2015.
- Sznajder-Katarzyńska, K.; Surma, M.; Cieślik, I. A review of perfluoroalkyl AIDS (PFAAs) in terms of sources, applications, human exposure, dietary intake, toxicity, legal regulation, and methods of determination. J. Chem. 2019, 2717528. [Google Scholar]
- Giesy, J.P.; Kannan, K. Peer Reviewed: Perfluorochemical Surfactants in the Environment. Environ. Sci. Technol. 2008, 36, 146A–152A. [Google Scholar] [CrossRef]
- Geueke, B. Dossier – Per- and polyfluoroalkyl substances (PFASs). Food Packag. Forum 2016, 1–13. [Google Scholar] [CrossRef]
- Ehresman, D.J.; Froehlich, J.W.; Olsen, G.W.; Chang, S.C.; Butenhoff, J.L. Comparison of human whole blood, plasma, and serum matrices for the determination of perfluorooctanesulfonate (PFOS), perfluorooctanoate (PFOA), and other fluorochemicals. Environ. Res. 2007, 103, 176–184. [Google Scholar] [CrossRef] [PubMed]
- C. Lau, K. Anitole, C. Hodes, D. Lai, A. Pfahles-Hutchens, and J. Seed, “Perfluoroalkyl acids: a review of monitoring and toxicological findings,” Toxicological Sciences, vol. 99, no. 2, pp. 366–394, 2007.
- K. G´oralczyk, K. A. Pachocki, A. Hernik et al., “Perfluorinated chemicals in blood serum of inhabitants in central Poland in relation to gender and age,” Science of the Total Environment, vol. 532, pp. 548–555, 2015.
- A. K¨arrman, I. Ericson, B. van Bavel et al., “Exposure of perfluorinated chemicals through lactation: levels of matched human milk and serum and a temporal trend, 1996–2004, in Sweden,” Environmental Health Perspectives, vol. 115, no. 2, pp. 226–230, 2007.
- K. S. Guruge, S. Taniyasu, N. Yamashita et al., “Perfluorinated organic compounds in human blood serum and seminal plasma: a study of urban and rural tea worker populations in Sri Lanka,” Journal of Environmental Monitoring, vol. 7, no. 4, pp. 371–377, 2005.
- K. Inoue, F. Okada, R. Ito et al., “Perfluorooctane sulfonate (PFOS) and related perfluorinated compounds in human maternal and cord blood samples: assessment of PFOS exposure in a susceptible population during pregnancy,” Environmental Health Perspectives, vol. 112, no. 11, pp. 1204–1207, 2004.
- L. Domingo, I. E. Jogsten, U. Eriksson et al., “Human dietary exposure to perfluoroalkyl substances in Catalonia, Spain. Temporal trend,” Food Chemistry, vol. 135, no. 3, pp. 1575–1582, 2012.
- P. D. Jones, W. Hu, W. De Coen, J. L. Newsted, and J. P. Giesy, “Binding of perfluorinated fatty acids to serum proteins,” Environmental Toxicology and Chemistry, vol. 22, no. 11, pp. 2639–2649, 2003.
- F. P´erez, M. Nadal, A. Navarro-Ortega et al., “Accumulation of perfluoroalkyl substances in human tissues,” Environment International, vol. 59, pp. 354–362, 2013.
- Frisbee, S.J.; Shankar, A.; Knox, S.; Steenland, K.; Savitz, D.A.; Fletcher, T.; Ducatman, A.M. Perfluorooctanoic acid, perfluorooctanesulfonate, and serum lipids in children and adolescents. Arch. Pediatr. Adolesc. Med. 2010, 164, 860–869. [Google Scholar] [CrossRef] [PubMed]
- Clifford, T.; Howatson, G.; West, D.J.; Stevenson, E.J. The potential benefits of red beetroot supplementation in health and disease. Nutrients 2015, 7, 2801–2822. [Google Scholar] [CrossRef]
- G. Webster, Potential Human Health Effects of Perfluorinated Chemicals (PFCs), National Collaborating Centre for Environmental Health-NCCEH, Vancouver, Canada, 2010.
- Z. Wang, I. T. Cousins, M. Scheringer, and K. Hungerbuehler, “Hazard assessment of fluorinated alternatives to long-chain perfluoroalkyl acids (PFAAs) and their precursors: status quo, ongoing challenges and possible solutions,” Environment International, vol. 75, pp. 172–179, 2015.
- Organisation for Economic Co-operation and Development (OECD), “Results of the 2006 survey on production and use of PFOS, PFAS, PFOA, PFCA, their related substances and products/mixtures containing these substances,” in Proceedings of the ENVIRONMENT DIRECTORATE ?e Joint Meeting of the Chemicals Committee and Working Party on Chemicals, Pesticides and Biotechnology, ENV/JM/MONO(2006), p. 36, Paris, France, February 2006.
- M. P. Krafft and J. G. Riess, “Highly fluorinated amphiphiles and colloidal systems, and their applications in the biomedical field. A contribution,” Biochimie, vol. 80, no. 5-6, pp. 489–514, 1998.
- S. Ganesan and N. Vasudevan, “Impacts of perfluorinated compounds on human health,” Bulletin of Environment, Pharmacology and Life Sciences, vol. 4, no. 7, pp. 183–191, 2015.
- L. Maestri, S. Negri, M. Ferrari et al., “Determination of perfluorooctanoic acid and perfluorooctanesulfonate in human tissues by liquid chromatography/single quadrupole mass spectrometry,” Rapid Communications in Mass Spectrometry, vol. 20, no. 18, pp. 2728–2734, 2006.
- K. Kannan, S. Corsolini, J. Falandysz et al., “Perfluorooctanesulfonate and related fluorochemicals in human blood from several countries,” Environmental Science & Technology, vol. 38, no. 17, pp. 4489–4495, 2004.
- X. Wu, D. H. Bennett, A. M. Calafat et al., “Serum concentrations of perfluorinated compounds (PFC) among selected populations of children and adults in California,” Environmental Research, vol. 136, pp. 264–273, 2015.
- G.-W. Lien, T.-W. Wen, W.-S. Hsieh, K.-Y. Wu, C.-Y. Chen, and P.-C. Chen, “Analysis of perfluorinated chemicals in umbilical cord blood by ultra-high performance liquid chromatography/tandem mass spectrometry,” Journal of Chromatography B, vol. 879, no. 9-10, pp. 641–646, 2011.
- B. J. Apelberg, F. R. Witter, J. B. Herbstman et al., “Cord serum concentrations of perfluorooctane sulfonate (PFOS) and perfluorooctanoate (PFOA) in relation to weight and size at birth,” Environmental Health Perspectives, vol. 115, no. 11, pp. 1670–1676, 2007.
- R. Monroy, K. Morrison, K. Teo et al., “Serum levels of perfluoroalkyl compounds in human maternal and umbilical cord blood samples,” Environmental Research, vol. 108, no. 1, pp. 56–62, 2008.
- L. Hanssen, A. A. Dudarev, S. Huber, J. Ř. Odland, E. Nieboer, and T. M. Sandanger, “Partition of perfluoroalkyl substances (PFASs) in whole blood and plasma, assessed in maternal and umbilical cord samples from inhabitants of arctic Russia and Uzbekistan,” Science of the Total Environment, vol. 447, pp. 430–437, 2013.
- A. Karrman, J. L. Domingo, X. Llebaria et al., “Biomonitoring perfluorinated compounds in Catalonia, Spain: concentrations and trends in human liver and milk samples,” Environmental Science and Pollution Research, vol. 17, no. 3, pp. 750–758, 2010.
- J.-L. He, T. Peng, J. Xie et al., “Determination of 20 perfluorinated compounds in animal liver by HPLC-MS/MS,” Chinese Journal of Analytical Chemistry, vol. 43, no. 1, pp. 40–48, 2015.
- F. P´erez, M. Nadal, A. Navarro-Ortega et al., “Accumulation of perfluoroalkyl substances in human tissues,” Environment International, vol. 59, pp. 354–362, 2013.
- W. Volkel, O. Genzel-Borovicz´eny, H. Demmelmair et al., “Perfluorooctane sulphonate (PFOS) and perfluorooctanoic acid (PFOA) in human breast milk: results of a pilot study,” International Journal of Hygiene and Environmental Health, vol. 211, no. 3-4, pp. 440–446, 2008.
- S. Rainieri, N. Conlledo, T. Langerholc, E. Madorran, M. Sala, and A. Barranco, “Toxic effects of perfluorinated compounds at human cellular level and on a model vertebrate,” Food and Chemical Toxicology, vol. 104, pp. 14–25, 2017.
- Committee on Toxicity of Chemicals in Food, Consumer Products and the Environment (COT) (2006) COT Statement on the Tolerable Daily Intake for Perfluorooctane Sulfonate. COT Statement 2006/09, Committee on Toxicity of Chemicals in Food, London, UK, 2006, https://cot.food.gov.uk/sites/default/files/cot/cotstatementpfos200609.pdf.
- G. L. Kennedy, J. L. Butenhoff, G. W. Olsen et al., “-etoxicology of perfluorooctanoate,” Critical Reviews in Toxicology, vol. 34, no. 4, pp. 351–384, 2004.
- A. M. Seacat, P. J. -omford, K. J. Hansen, G. W. Olsen, M. T. Case, and J. L. Butenhoff, “Subchronic toxicity studies on perfluorooctanesulfonate potassium salt in cynomolgus monkeys,” Toxicological Sciences, vol. 68, no. 1, pp. 249–264, 2002.
- L. Zheng, G.-H. Dong, Y.-H. Jin, and Q.-C. He, “Immunotoxic changes associated with a 7-day oral exposure to perfluorooctanesulfonate (PFOS) in adult male C57BL/6 mice,” Archives of Toxicology, vol. 83, no. 7, pp. 679 689, 2009.
- A. D. Benninghoff, G. A. Orner, C. H. Buchner, J. D. Hendricks, A. M. Duffy, and D. E. Williams, “Promotion of hepatocarcinogenesis by perfluoroalkyl acids in rainbow trout,” Toxicological Sciences, vol. 125, no. 1, pp. 69–78, 2012.
- J. W. Nelson, E. E. Hatch, and T. F. Webster, “Exposure to polyfluoroalkyl chemicals and cholesterol, body weight, and insulin resistance in the general U.S. population,” Environmental Health Perspectives, vol. 118, no. 2, pp. 197–202, 2010.
- J. C. DeWitt, M. M. Peden-Adams, J. M. Keller, and D. R. Germolec, “Immunotoxicity of perfluorinated compounds: recent developments,” Toxicologic Pathology, vol. 40, no. 2, pp. 300–311, 2012.
- M. R. Qazi, Z. Xia, J. Bogdanska et al., “-e atrophy and changes in the cellular compositions of the thymus and spleen observed in mice subjected to short-term exposure to perfluorooctanesulfonate are high-dose phenomena mediated in part by peroxisome proliferator-activated receptoralpha (PPARα),” Toxicology, vol. 260, no. 1–3, pp. 68–76, 2009.
- P. Grandjean, E. W. Andersen, E. Budtz-Jørgensen et al., “Serum vaccine antibody concentrations in children exposed to perfluorinated compounds,” JAMA, vol. 307, no. 4, pp. 391–397, 2012.
- N. M. Crawford, S. E. Fenton, M. Strynar, E. P. Hines, D. A. Pritchard, and A. Z. Steiner, “Effects of perfluorinated chemicals on thyroid function, markers of ovarian reserve, and natural fertility,” Reproductive Toxicology, vol. 69, pp. 53–59, 2017.
- M.-J. Lopez-Espinosa, D. Mondal, B. Armstrong, M. S. Bloom, and T. Fletcher, “-yroid function and 18 Journal of Chemistry perfluoroalkyl acids in children living near a chemical plant,” Environmental Health Perspectives, vol. 120, no. 7, pp. 1036–1041, 2012.
- N. Johansson, A. Fredriksson, and P. Eriksson, “Neonatal exposure to perfluorooctane sulfonate (PFOS) and perfluorooctanoic acid (PFOA) causes neurobehavioural defects in adult mice,” Neurotoxicology, vol. 29, no. 1, pp. 160–169, 2008.
- A. J. Filgo, E. M. Quist, M. J. Hoenerhoff, A. E. Brix, G. E. Kissling, and S. E. Fenton, “Perfluorooctanoic acid (PFOA)-induced liver lesions in two strains of mice following developmental exposures,” Toxicologic Pathology, vol. 43, no. 4, pp. 558–568, 2015.
- C. Fei, J. K. McLaughlin, R. E. Tarone, and J. Olsen, “Perfluorinated chemicals and fetal growth: a study within the Danish National Birth Cohort,” Environmental Health Perspectives, vol. 115, no. 11, pp. 1677–1682, 2007.
- T. I. Halldorsson, D. Rytter, L. S. Haug et al., “Prenatal exposure to perfluorooctanoate and risk of overweight at 20 years of age: a prospective cohort study,” Environmental Health Perspectives, vol. 120, no. 5, pp. 668–673, 2012.
- Fenton, S.E.; Ducatman, A.; Boobis, A. Per- and polyfluoroalhyl substances toxicity and human health review: current state of knowledge and strategies for informing future research. Environ. Toxicol Chem. 2021, 40, 606–630. [Google Scholar] [CrossRef]
- Herzke D, Huber S, Bervoets L, D’Hollander W, Hajslova J, Pulkrabova J, Brambilla G, De Filippis SP, Klenow S, Heinemeyer G, et al. 2013. Perfluorinated alkylated substances in vegetables collected in four European countries; occurrence and human exposure estimations. Environ Sci Pollut Res. 20:7930–7939.
- de Castro, A.P.R.B.; da Cunha, D.T.; Antunes, A.E.C.; Corona, L.P.; Bezerra, R.M.N. Effect of freeze-dried red beet (beta vulgaris l.) leaf supplementation on biochemical and anthropometrical parameters in overweight and obese individuals: a pilot study. Plant Foods Hum. Nutr. 2017, 74, 232–234. [Google Scholar] [CrossRef]
- Asgary, S.; Afshani, M.R.; Sahebkar, A.; Keshvari, M.; Taheri, M.; Jahanian, E.; Rafieian-Kopaei, M.; Malekian, F.; Sarrafzadegan, N. Improvement of hypertension, endothelial function and systemic inflammation following short-term supplementation with red beet (Beta vulgaris L.) juice: a randomized crossover pilot study. J. Hum. Hypertens. 2016, 30, 627–632. [Google Scholar] [CrossRef]
- Nowacka, M.; Tappi, S.; Wiktor, A. The impact of pulsed electric field on the extraction of bioactive compounds from beetroot. Foods 2019, 8, 244. [Google Scholar] [CrossRef]
- Nakamura, K.; seishima, R.; Matsui, S.; Shiggeta, K.; Okabayashi, K.; Kitagawa, Y. The prognostic impact of preoperative mean corpuscular volume in colorectal cancer. Jpn. J. Clin. Oncol. 2022, 52, 562–570. [Google Scholar] [CrossRef]
- Vinholt, P.J.; Hvas, A.M. , Frederiksen, H.; Bathum, L.; Jorgensen, M.K.; Nybo, M. Platelet count is associated with cardiovascular disease, cancer and mortality: A population-based cohort study. Thromb. Res. 2016, 148, 136–142. [Google Scholar] [CrossRef]
- Semple, J.M.; Italiano Jr., J. E.; Freedman, J. Platelets and the immune continuum. Nat. Rev, Immunol. 2011, 11, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Golebiewska, E.M.; Poole, A.W. Platelet secretion: from haemostasis to wound healing and beyond. Blood Rev. 2015, 29, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Gay, L.J.; Felding-Habermann, B. Contribution of platelets to tumour metastasis. Nat. Rev. Cancer 2011, 11, 123–134. [Google Scholar] [CrossRef] [PubMed]
- Rotander, A.; Toms, L.-M.L.; Aylward, L.; Kay, M.; Mueller, J.F. Elevated levels of PFOS and PFHxS in firefighters exposed to aqueous film forming foam (AFFF). Environ. Int. 2015, 82, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Peraz, F.; Llorca, M.; Farré, M.; Barcelo, D. Automated analysis of perfluorinated compounds In human hair and urine samples by turbulent flow chromatography coupled to tandem mass spectrometry. Anal. Bioanal. Chem. 2012, 402, 2369–2378. [Google Scholar] [CrossRef]
- Surma, M.; Wiczkowski, W.; Zieliński, H.; Cieślik, E. Determination of selected perfluorinated acids (PFCAs) and perfluorinated sulfonates (PFASs) in food contact materials using LC-MS/MS. Packag. Technol. Sci. 2015, 28, 789–799. [Google Scholar] [CrossRef]
- Niedzwiedzka, E.; Wadolowska, L.; Kowalkowska, J. Reproducibility of a non-quantitative food frequency questionnaire (62-Item FFQ-6) and PCA-driven dietary pattern identification in 13-21-year-old females. Nutrients 2019, 1, 2183. [Google Scholar] [CrossRef]
Figure 1.
Correlation heat map between individual compounds, total acids, sulfates and PFASs and blood parameters before (A) and after (B) intake of fermented red beetroot juice. (*) – significant correlation, (p < 0.05).
Figure 1.
Correlation heat map between individual compounds, total acids, sulfates and PFASs and blood parameters before (A) and after (B) intake of fermented red beetroot juice. (*) – significant correlation, (p < 0.05).
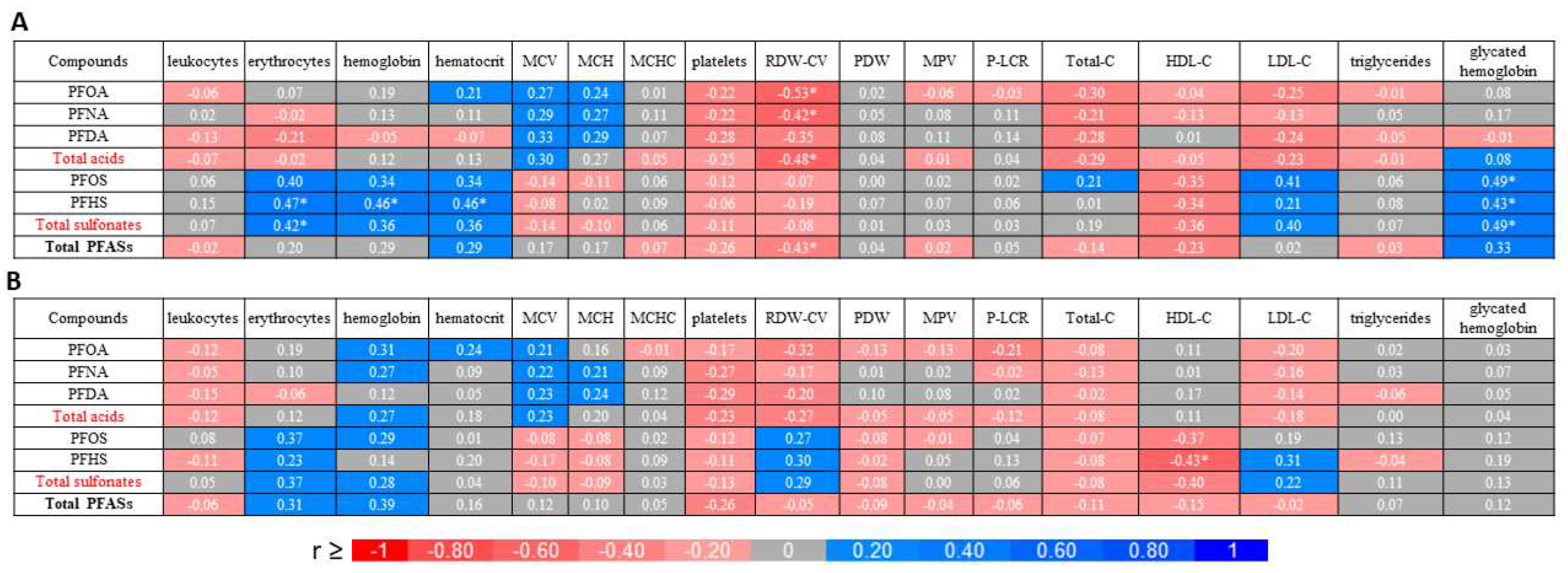
Figure 2.
Flow diagram of participant recruitment during the study.
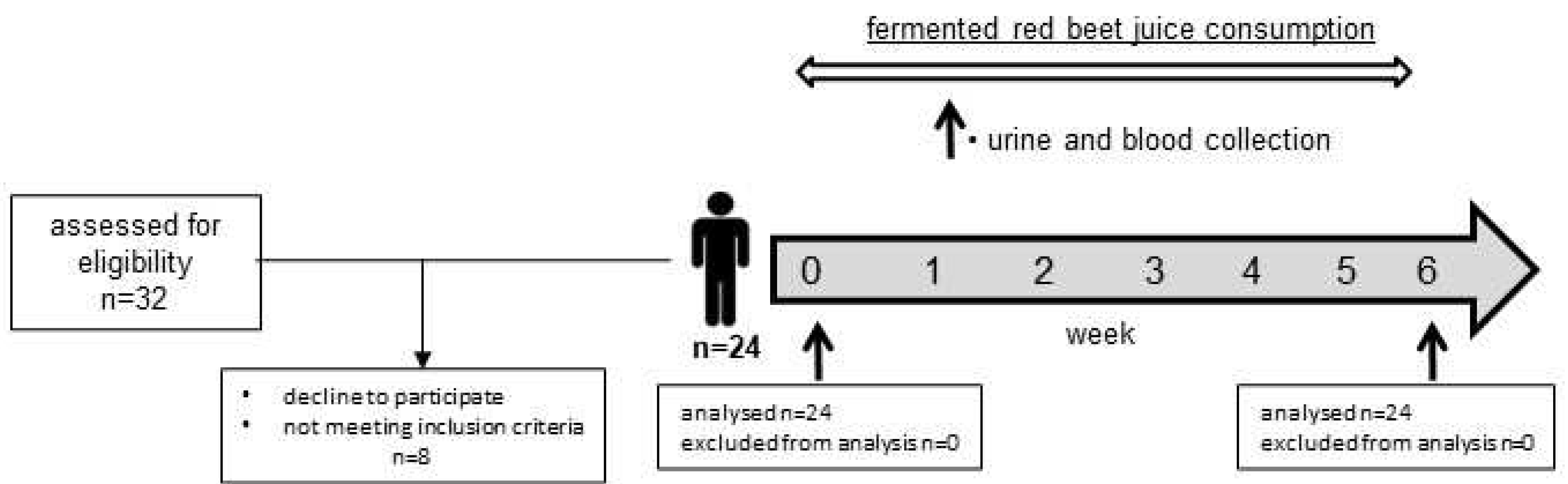

Table 1.
PFASs detected in the fermented red beetroot juice, urine and blood plasma of volunteers.
| No | Compounds | Rt (min) |
[M]- (m/z) |
MS/MS (m/z) |
Sample |
|---|---|---|---|---|---|
| Perfluorocarboxilic acids | |||||
| 1 | PFOA | 2.02 | 413 | 369 | J, B, U |
| 2 | PFNA | 2.43 | 463 | 419 | B |
| 3 | PFDA | 2.86 | 513 | 469 | B |
| Perfluoroalkane sulfonates | |||||
| 4 | PFOS | 2.97 | 499 | 80 | B |
| 5 | PFHS | 2.11 | 399 | 80 | B |
Rt—retention time; J—red beetroot juice; B—blood plasma; U—urine.
Table 2.
Blood plasma profile of PFASs in volunteers before (T0) and after (T1) intake of fermented red beetroot juice. Values are expressed in ng/mL and are presented as median (P25-P75).
Table 2.
Blood plasma profile of PFASs in volunteers before (T0) and after (T1) intake of fermented red beetroot juice. Values are expressed in ng/mL and are presented as median (P25-P75).
| No | Compounds | Blood plasma samples |
p T0 vs T1 |
|
|---|---|---|---|---|
| T0 | T1 | |||
| Acids | ||||
| 1 | PFOA | 0.94 (0.76-1.56) | 0.93 (0.77-1.52) | 0.627 |
| 2 | PFNA | 0.39 (0.26-0.58) | 0.34 (0.23-0.58) | < 0.001** |
| 3 | PFDA | 0.30 (0.20-0.46) | 0.23 (0.17-0.38) | < 0.001** |
| Total acids | 1.65 (1.29-2.94) | 1.49 (1.19-2.64) | 0.009** | |
| Sulfonates | ||||
| 4 | PFOS | 0.59 (0.44-0.80) | 0.71 (0.53-0.96) | < 0.001** |
| 5 | PFHS | 0.11 (0.09-0.17) | 0.25 (0.15-0.37) | < 0.001** |
| Total sulfonates | 0.67 (0.53-0.92) | 0.96 (0.68-1.37) | < 0.001** | |
| Total of PFASs | 2.66 (1.90-4.47) | 2.62 (2.08-4.17) | 0.031* | |
* p < 0.05; ** p < 0.01
Table 3.
Descriptive statistics for blood parameters before (T0) and after (T1) consumed fermented red beet juice, expressed as median (P25-P75).
Table 3.
Descriptive statistics for blood parameters before (T0) and after (T1) consumed fermented red beet juice, expressed as median (P25-P75).
| Blood parameters | Samples |
p T0 vs T1 |
|
|---|---|---|---|
| T0 | T1 | ||
| Hematology | |||
| Leukocytes [k/μL] | 5.2 (4.9-6.0) | 5.1 (4.6-5.8) | 0.961 |
| Erythrocytes [mln/μL] | 4.6 (4.3-5.1) | 4.7 (4.3-4.9) | 0.246 |
| Hemoglobin [g/dL] | 13.2 (12.9-14.7) | 13.6 (12.7-14.1) | 0.721 |
| Hematocrit [%] | 41.0 (39.0-45.0) | 40.0 (37.0-42.0) | 0.013* |
| MCV [fl] | 88.0 (85.0-92.0) | 87.0 (84.0-90.0) | 0.001** |
| MCH [pg] | 29.0 (28.0-30.0) | 29.0 (28.0-31.0) | 0.686 |
| MCHC [g/dL] | 32.9 (32.3-33.5) | 33.4 (33.1-34.2) | < 0.001** |
| RDW-CV [%] | 13.0 (12.0-14.0) | 13.0 (12.0-13.0) | 0.208 |
| Platelets [k/μL] | 273.0 (215.0-318.0) | 262.0 (202.0-299.0) | 0.002** |
| PDW [fl] | 14.0 (13.0-15.0) | 14.0 (12.0-15.0) | 0.083 |
| MPV [fl] | 11.2 (10.7-11.9) | 10.9 (10.4-11.7) | < 0.001** |
| P-LCR [%] | 34.0 (29.0-38.0) | 32.0 (28.0-38.0) | < 0.001** |
| Blood biochemistry | |||
| Total-C [mg/dL] | 184.0 (165.0-197.0) | 168.0 (155.0-194.0) | 0.074 |
| HDL-C [mg/dL] | 69.0 (64.0-86.0) | 73.0 (57.0-88.0) | 0.897 |
| LDL-C [mg/dL] | 80.6 (64.8-109.8) | 76.4 (66.4-98.4) | 0.128 |
| Triglycerides [mg/dL] | 80.0 (48.0-102.0) | 71.0 (58.0-81.0) | 0.412 |
| Glycated hemoglobin [%] | 5.2 (5.0-5.3) | 5.2 (5.1-5.3) | 0.877 |
MCV—mean corpuscular volume; MCH—mean corpuscular hemoglobin; MCHC—mean corpuscular/cellular hemoglobin concentration; RDW-CV—red cell distribution width; PDW—platelet distribution width; MPV—mean platelet volume; P-LCR—platelet large cell ratio; Total-C—total cholesterol; HDL—high density lipoprotein; LDL—low density lipoprotein; * p < 0.05; ** p < 0.01
Table 4.
Anthropometric parameters and demographic characteristics of the sample (% or mean and standard deviation, SD).
Table 4.
Anthropometric parameters and demographic characteristics of the sample (% or mean and standard deviation, SD).
| Characteristics | Total |
|---|---|
| Sample size | 24 |
| Sample percentage | 100.0 |
| Age (years), mean (SD) | 29.5 (3.6) |
| Gender, n (%) | |
| women | 19 (79.2) |
| men | 5 (20.8) |
| BMI (kg/m2), mean (SD) | 24.9 (1.8) |
| Residence, n (%) | |
| Urban | 17 (70.8) |
| Rural | 7 (29.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



