
Submitted:
07 August 2023
Posted:
09 August 2023
You are already at the latest version
Abstract
Aim
The use of prophylactic antibiotics prior to colorectal surgery reduces surgical site infections. Cefazolin and metronidazole is a standard regimen. Ampicillin-sulbactam may be an alternative, but the data are limited. We compared the efficacy of ampicillin-sulbactam with cefazolin and metronidazole as prophylactic antibiotics.
Methods
Patients who underwent colorectal surgery at Inha University Hospital between 2010 and 2020 were treated prophylactically with cefazolin and metronidazole or ampicillin-sulbactam, and observed for 30 days following surgery. The primary outcome was surgical site infections. Secondary outcomes were deep/organ infections and the need for drainage.
Results
SSIs occurred in 2.6% (17/646) of the ampicillin-sulbactam group and was not inferior to the occurrence in the cefazolin and metronidazole group (3.8%, 21/556). There was no significant difference between the two groups in the secondary outcomes.
Conclusion
Compared with the cefazolin and metronidazole combination, the ampicillin-sulbactam group is non-inferior as a preoperative prophylactic antibiotic regimen for colorectal surgery.
Keywords:
Ampicillin
; Antibiotics prophylaxis
; cefazolin
; Colorectal surgery
1. Introduction
Surgical site infections (SSIs) are one of the main causes of nosocomial infections, which lower the quality of life, lengthen hospital stay, and increase the economic burden [1]. SSIs also increase the chances of hospital readmission by five times and death by two times [2]. Many studies have sought to reduce SSIs. Antibiotics administered prophylactically before surgery significantly lower this risk [3]. In particular, because colorectal surgery resects the intestine, the risk of infection is higher than in other clean surgeries [4]. SSIs occur in approximately 4%–10% of patients undergoing colon surgery and in 3%–27% of patients after rectal surgery [5]. In colorectal surgery, the pathogen mainly originates in the intestine [6]. Therefore, antibiotics that act on Enterobacteriaceae and anaerobes have been selected as preoperative antibiotics [7].
Several preoperative antibiotic options may be available. Antibiotics such as carbapenem have been used in institutions reporting severely resistant strains [7]. The most commonly used prophylactic antibiotic regimen is a combination of first-generation cephalosporin and metronidazole [8,9]. Ampicillin-sulbactam is easily administered and is active against Enterococcus. Therefore, the combination may be an alternative to the first-generation cephalosporin and metronidazole combination. However, studies on the effectiveness of ampicillin-sulbactam as a prophylactic antibiotic is relatively old and involved a small number of patients [10]. It is possible that antibiotic susceptibility and gut flora have changed. Thus, more recent data are needed. Therefore, we planned a study to compare the effectiveness of cefazolin/metronidazole and ampicillin/sulbactam as prophylactic antibiotics before surgery.
2. Results
2.1. General characteristics
A total of 556 patients were assigned to the CFZ/MTZ group and 646 to the AMP/SUL group. The mean age of the patients was 64.3 years and 56% were male. There was no statistically significant difference in most variables between the two groups. However, rectal surgery and obesity were more common in the CFZ/MTZ group. (Table 1).
2.2. Risk analysis of SSI using logistic regression analysis
Smoking was the most significant risk factor with an odds ratio (OR) of 3.489 [95% confidence interval (CI): 1.784 – 6.8222]. Long operation time and Male sex appeared to be a risk factors in the univariate analysis, but there was no statistically significant difference in multivariate analysis. Compared to the AMP/SUL group, SSI was more frequent in the CFZ/MTZ group, but the difference was not statistically significant in either univariate or multivariate analysis (Table 2)
2.3. Comparison of outcomes of two groups (t-test, non-inferiority)
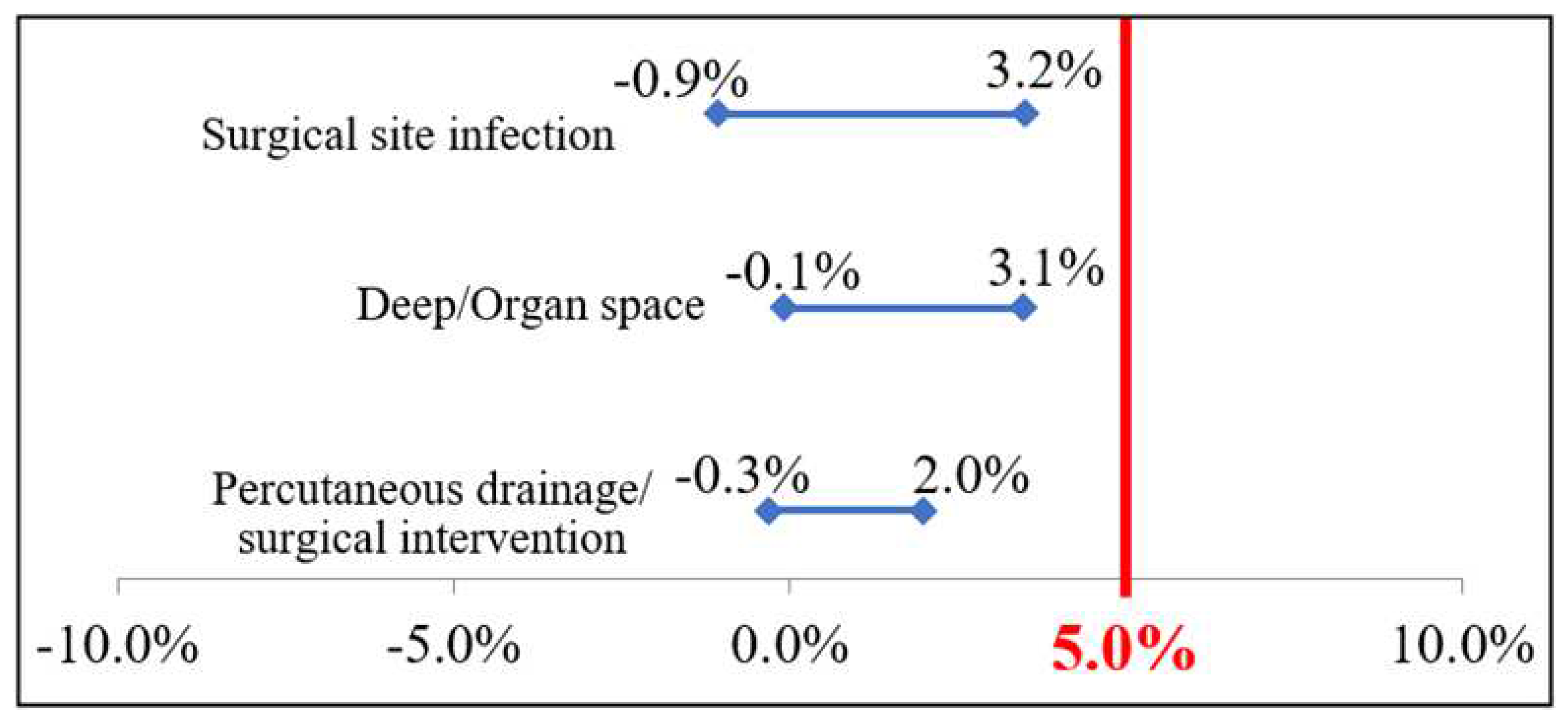
SSI occurred in 2.6% (17/646) of the AMP/SUL group and was not inferior to 3.8% (21/556) of the CFZ/MTZ group (p=0.264, CI= - 0.009 – 0.032). Deep/organ space infections occurred in 1.24% (8/646) of the AMP/SUL group, which was non-inferior to 2.7% (15/556) of the CFZ/MTZ (p=0.073, CI= - 0.001 – 0.031). The need for drainage was also non-inferior, with values of 0.6% (4/646) in the AMP/SUL group and 1.6% (9/556) in the CFZ/MTZ group (p=0.167, CI= - 0.003 – 0.020) (Table 3). In the CFZ/MTZ group, SSIs involved Enterococcus spp. (n=3), Escherichia coli (n=5), Klebsiella pneumoniae (n=1), Pseudomonas (n=1), Morganella morganii (n=1), and methicillin-resistant Staphylococcus aureus (MRSA, n=2). SSIs in the AMP/SUL group included Enterococcus spp. (n=2), Escherichia coli (n=2), and Enterobacter (n=1). Extended-spectrum β-lactamase (ESBL)-producing pathogens were isolated from one case in the AMP/SUL group and three cases in the CFA/MTZ group.
Figure 1.
3. Discussion
There have been few studies on the effects of ampicillin/sulbactam as a preoperative antibiotic in colorectal surgery. In a previous study conducted in the 1990s, a comparison of patients treated using the combination of ampicillin/sulbactam (n=63) and gentamicin and metronidazole (n=65) did not show a significant difference in the incidence of SSIs (9.5% vs. 10.7%) [10]. Another paper in the 1990s compared amoxycillin/clavulanate to cefotaxime + metronidazole as prophylactic antibiotic regimens in colorectal surgery. No difference in the effectiveness of preventing SSIs was evident between the two regimens, with SSIs in 8 of 76 patients treated with amoxycillin/clavulanate and 9 of 88 patients treated with cefotaxime + metronidazole [12]. Based on these studies, ampicillin/sulbactam has been suggested as an alternative to preoperative antibiotics in colorectal surgery. However, this has not been established definitively.
A 2013 study analyzed the effects of prophylactic antibiotics in patients who underwent colorectal surgery at 112 hospitals. A study subgroup included ampicillin/sulbactam and cefazolin + metronidazole [13]. In that study, SSIs occurred in 11.3% of the 363 patients treated with ampicillin/sulbactam. This rate was inferior to the rate of 6.2% in the 899 patients treated with cefazolin/metronidazole. In the above-mentioned study, the possibility of selecting antibiotics according to the preoperative wound class could not be excluded. In addition, there was a strong correlation between SSI and the skill of the surgeon, which could not be controlled. Furthermore, the number of patients in the ampicillin/sulbactam group was relatively small. In contrast, our study involved only specialists, excluding those with < 10 years of experience. Moreover, in our study, antibiotic selection was distributed by period. Thus, the possibility of bias in the selection of preoperative antibiotics according to the surgeon’s propensity or preoperative wound class was low.
As the rationale for the inferior prophylactic effect of ampicillin/sulbactam compared to cefazolin + metronidazole in the aforementioned study [13], the authors suggested an increasing antibiotic resistance of Bacteroides fragilis. Increasing resistance of B. fragilis to ampicillin/sulbactam has been evident, since 2010. However, the most recently reported nosocomial intra-abdominal infections are Escherichia coli, Pseudomonas spp., and Enterococcus spp. [14,15]. Similarly, in our study, anaerobes were not isolated in the ampicillin/sulbactam group. Therefore, there is no evidence that ampicillin-sulbactam is vulnerable to anaerobe-induced SSIs than cefazolin and metronidazole.
The increase in the viable count of Enterococcus should be considered in the selection of prophylactic antibiotics for colorectal surgery. Enterococcus infection is a major complication of colorectal surgery [16] and can cause anastomotic leakage [17]. Ampicillin is the preferred therapeutic agent for susceptibility to Enterococcus species [18]. In contrast, cefazolin is intrinsically resistant to cephlosporins in Enterococcus species (18). Changes in antibiotic susceptibility should also be considered. The increasing number of ESBL-producing pathogens is emerging as a major problem in nosocomial infections. One study reported that 38% of SSIs after colorectal surgery were ESBL-producing pathogens [19]. Sulbactam is a β-lactamase inhibitor that is beneficial for ESBL-producing strains [20]. Considering this pattern of resistance, changes may be necessary in the selection of prophylactic antibiotics. In our study, deep/organ infections tended to be lower in the AMP/SUL group than in the CFZ/MTZ group, although the difference was not statistically significant. In cultured bacteria, Enterobacteriaceae, including Escherichia coli, were less abundant in the AMP/SUL group. ESBL production was also not statistically significant, but it was lower in the AMP/SUL group than in the CFZ/MTZ group. Considering the increasing resistance of Enterobacteriaceae to antibiotics, the AMP/SUM group appears suitable as a preoperative antibiotic regimen for colorectal surgery.
This study has several limitations. First, it was a retrospective study with a small number of patients. Second, it is not possible to control variables, such as the handwashing performance rate and environmental disinfection. Third, differences in side effects, such as gastrointestinal trouble or Clostridium difficile-associated disease, were not investigated. Fourth, there may be differences in the susceptibility of pathogens to antibiotics by region.
In conclusion, ampicillin-sulbactam was not inferior to cefazoline/metronidazole as a prophylactic antibiotic regimen for colorectal surgery. It is necessary to consider the susceptibility to antibiotics by region and institution. Large-scale studies controlling for various variables are needed.
4. Materials and Methods
4.1. Study population
Patients who underwent colorectal surgery at Inha University Hospital between July 2010 and December 2020 were enrolled. Patients treated by emergency surgery and combined surgery with other organs were excluded from this study. Specialists with < 10 years of experience in colorectal surgery were excluded. Only patients who underwent surgery from three specialists were analyzed. Patients were divided into two groups according to preoperative antibiotics: i) cefazolin (intravenous, 2 g) and metronidazole (intravenous or oral, 500 mg) combination (CFZ/MTZ group) and ii) ampicillin/sulbactam (intravenous, 3 g; AMP/SUL group).
4.2. Characteristics of patients
The following indicators were used to compare characteristics in patients undergoing surgery: age, sex, operation time, wound class, American Society of Anesthesiologists (ASA) score, endoscopic operation, diabetes, obesity, and smoking. The preoperative wound class was divided into four levels: clean, clean-contaminated, contaminated, and dirty. ASA score was divided into six stages: healthy, with mild systemic diseases, severe systemic diseases, diseases that are a constant threat to life, moribund patients who are not expected to survive without the operation, declared brain death. Obesity was defined as a body mass index ≥ 30 kg/m2.
4.3. Outcomes
SSI in the 30 days following surgery was the primary outcome. SSI was defined according to the criteria of the Centers for Disease Control and Prevention [11]. The secondary outcomes were the grade of SSI and treatment method. The SSI grade was i) none, ii) superficial incisional, iii) deep incisional, and iv) organ/space. Treatment methods comprised were divided into (i) only antibiotics and (ii) antibiotics and percutaneous or surgical drainage.
4.4. Ethics statement
This study was approved by the Institutional Review Board of Inha University Hospital, Incheon, Korea. All patient records were anonymized.
4.5. Statistical analyses
Chi-square test or Fisher’s exact test was used to compare the general characteristics of the CFZ/MTZ and AMP/SUL groups. A non-inferiority test was performed on the incidence of SSI between the CFZ/MTZ and AMP/SUL groups. The margin was set at 5%. Logistic regression analysis was used to analyze the risk of SSI. For logistic analysis, wound classes were divided into clean-clean/contamination and contaminated/dirty. The ASA score was divided into 1–2 points and 3–6 points. The operation time was divided based on 75% of the total colorectal surgeries. A two-sided test was used, and a P-value ≤ 0.05 was considered statistically significant. The analyses were performed using SPSS version 21.0.
Author Contributions
Conceptualization: Im JH, Jung ST. Data curation: Im JH, Kang DY, Lee SJ, Baek JH, Lee JS, Kim EJ. Formal analysis: Lee DY, Kang DY. Writing - original draft: Im JH, Lee DY. Writing - review & editing: Lee JS, Kang DY. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
References
- Martone, W.J.; Nichols, R.L. Recognition, prevention, surveillance, and management of surgical site infections: introduction to the problem and symposium overview. Clinical Infectious Diseases 2001, 33, S67–S68. [Google Scholar] [CrossRef] [PubMed]
- Kirkland, K.B.; Briggs, J.P.; Trivette, S.L.; Wilkinson, W.E.; Sexton, D.J. The impact of surgical-site infections in the 1990s: attributable mortality, excess length of hospitalization, and extra costs. Infection Control & Hospital Epidemiology 1999, 20, 725–730. [Google Scholar]
- Gorbach, S.L.; Condon, R.E.; Conte Jr, J.E.; Kaiser, A.B.; Ledger, W.J.; Nichols, R.L. Evaluation of new anti-infective drugs for surgical prophylaxis. Clinical infectious diseases 1992, 15, S313–S338. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, S.P.; Burton, R.C. Effects of prophylactic antibiotics on wound infection after elective colon and rectal surgery: 1960 to 1980. The American Journal of Surgery 1983, 145, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.R.; Peterson, K.D.; Mu, Y.; Banerjee, S.; Allen-Bridson, K.; Morrell, G.; Dudeck, M.A.; Pollock, D.A.; Horan, T.C. National Healthcare Safety Network (NHSN) report: data summary for 2006 through 2008, issued December 2009. Am J Infect Control 2009, 37, 783–805. [Google Scholar] [CrossRef] [PubMed]
- Nichols, R.L. Prophylaxis for intraabdominal surgery. Reviews of infectious diseases 1984, 6, S276–S282. [Google Scholar] [CrossRef] [PubMed]
- Bratzler, D.W.; Dellinger, E.P.; Olsen, K.M.; Perl, T.M.; Auwaerter, P.G.; Bolon, M.K.; Fish, D.N.; Napolitano, L.M.; Sawyer, R.G.; Slain, D. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Surgical infections 2013, 14, 73–156. [Google Scholar] [CrossRef] [PubMed]
- Shatney, C.H. Antibiotic prophylaxis in elective gastro-intestinal tract surgery: a comparison of single-dose pre-operative cefotaxime and multiple-dose cefoxitin. Journal of Antimicrobial Chemotherapy 1984, 14, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Lumley, J.; Siu, S.; Rllay, S.; Stitz, R.; Kemp, R.; Faoagali, J.; Nathanson, L.; White, S. Single dose ceftriaxone as prophylaxis for sepsis in colorectal surgery. Australian and New Zealand Journal of Surgery 1992, 62, 292–296. [Google Scholar] [CrossRef] [PubMed]
- AhChong, K.; Yip, A.; Lee, F.; Chiu, K. Comparison of prophylactic ampicillin/sulbactam with gentamicin and metronidazole in elective colorectal surgery: a randomized clinical study. Journal of Hospital Infection 1994, 27, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Control, C.f.D.; Prevention. Surgical site infection event SSI. National Healthcare Safety Network (NHSN) 2021. [Google Scholar]
- Kwok, S.; Lau, W.; Leung, K.; Ku, K.; Ho, W.; Li, A. Amoxycillin and clavulanic acid versus cefotaxime and metronidazole as antibiotic prophylaxis in elective colorectal resectional surgery. Chemotherapy 1993, 39, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Deierhoi, R.J.; Dawes, L.G.; Vick, C.; Itani, K.M.; Hawn, M.T. Choice of intravenous antibiotic prophylaxis for colorectal surgery does matter. Journal of the American College of Surgeons 2013, 217, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Pochhammer, J.; Köhler, J.; Schäffer, M. Colorectal surgical site infections and their causative pathogens: differences between left-and right-side resections. Surgical infections 2019, 20, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Du, M.; Liu, B.; Li, M.; Cao, J.; Liu, D.; Wang, Z.; Wang, Q.; Xiao, P.; Zhang, X.; Gao, Y. Multicenter surveillance study of surgical site infection and its risk factors in radical resection of colon or rectal carcinoma. BMC infectious diseases 2019, 19, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.I.; Keskey, R.; Ackerman, M.T.; Zaborina, O.; Hyman, N.; Alverdy, J.C.; Shogan, B.D. Enterococcus faecalis Is Associated with Anastomotic Leak in Patients Undergoing Colorectal Surgery. Surgical Infections 2021. [Google Scholar] [CrossRef] [PubMed]
- Shogan, B.D.; Belogortseva, N.; Luong, P.M.; Zaborin, A.; Lax, S.; Bethel, C.; Ward, M.; Muldoon, J.P.; Singer, M.; An, G. Collagen degradation and MMP9 activation by Enterococcus faecalis contribute to intestinal anastomotic leak. Science translational medicine 2015, 7, 286ra268–286ra268. [Google Scholar] [CrossRef] [PubMed]
- Kristich, C.J.; Rice, L.B.; Arias, C.A. Enterococcal infection—treatment and antibiotic resistance. Enterococci: from commensals to leading causes of drug resistant infection [Internet], 2014. [Google Scholar]
- Kalakouti, E.; Simillis, C.; Pellino, G.; Mughal, N.; Warren, O.; Mills, S.; Tan, E.; Kontovounisios, C.; Tekkis, P.P. Characteristics of Surgical Site Infection Following Colorectal Surgery in a Tertiary Center: Extended-spectrum β-Lactamase-producing Bacteria Culprits in Disease. Wounds: a compendium of clinical research and practice 2017, 30, 108–113. [Google Scholar] [PubMed]
- Bhattacharjee, A.; Sen, M.R.; Prakash, P.; Anupurba, S. Role of β-lactamase inhibitors in enterobacterial isolates producing extended-spectrum β-lactamases. Journal of antimicrobial chemotherapy 2008, 61, 309–314. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Comparison of general characteristics of the two groups.
| Variables | CFZ/MTZ N=556 |
AMP/SUL N=646 |
P-value |
|---|---|---|---|
| Age in years, mean ± standard deviation | 64.2 ± 12.0 | 64.4 ± 12.8 | 0.831 |
| Sex | |||
| Male | 318 (47.3) | 355 (52.7) | 0.449 |
| Female | 291 (45.0) | 291 (55.0) | |
| Surgical site | |||
| Colon | 267 (43.1) | 353 (56.9) | 0.021 |
| Rectum | 289 (49.8) | 291 (50.2) | |
| Operation time | |||
| <75% | 394 (46.3) | 457 (53.7) | 0.294 |
| ≥75% | 114 (50.4) | 112 (49.6) | |
| ASA score | |||
| I–II | 269 (50.9) | 260 (49.1) | 0.244 |
| III–IV | 253 (47.2) | 283 (52.8) | |
| Diabetes mellitus | |||
| No | 425 (49.5) | 433 (50.5) | 0.227 |
| Yes | 99 (44.8) | 122 (55.2) | |
| Current Smoking | |||
| No | 425 (48.5) | 451 (51.5) | 1.000 |
| Yes | 99 (48.8) | 104 (51.2) | |
| Obesity | |||
| No | 320 (44.0) | 407 (56.0) | <0.001 |
| Yes | 204 (58.0) | 148 (42.0) | |
| Wound class | |||
| Clean or clean/contaminated | 515 (49.0) | 535 (51.0) | 1.000 |
| Contaminated/dirty | 8 (50.0) | 8 (50.0) | |
| Surgical approach | |||
| Minimally invasive | 416 (47.3) | 463 (52.7) | 0.240 |
| Open | 140 (43.3) | 183 (56.7) | |
| Improper timing of administration | |||
| No | 534 (46.4) | 617 (53.6) | 1.000 |
| Yes | 22 (46.8) | 25 (53.2) | |
| Oral kanamycin | |||
| No | 218 (44.0) | 278 (56.0) | 0.196 |
| Yes | 338 (47.9) | 368 (52.1) |
CFZ/MTZ = cefazolin/metronidazole group; AMP/SUL = ampicillin/sulbactam group; ASA = American Society of Anesthesiologists; Inappropriate timing of administration = administration cannot be done within 1 hour before surgery.
Table 2.
Risk factors for surgical site infections based on common characteristics of both groups.
| Variables | Surgical site infection | Univariate | Multivariate | |
|---|---|---|---|---|
| Antibiotics group | 0.940 (0.843–1.047) | - | ||
| CFZ/MTZ (n=556) | 21 (55.3) | |||
| AMP/SUL (n=646) | 17 (44.7) | |||
| Age, years | 1.256 (0.617–2.558) | - | ||
| 18–59 (n=405) | 11 (28.9) | |||
| 60–99 (n=797) | 27 (71.1) | |||
| Sex | 0.444* (0.214–0.922) | - | ||
| Male (n=673) | 28 (73.7) | |||
| Female (n=529) | 10 (26.3) | |||
| Site | 1.868 (0.957–3.648) | - | ||
| Colon (n=620) | 14 (36.8) | |||
| Rectum (n=580) | 24 (63.2) | |||
| Operation time | 2.103* (1.053–4.199) | - | ||
| <75% (n=851) | 24 (64.9) | |||
| ≥75% (n=226) | 13 (35.1) | |||
| ASA score | 0.663 (0.340–1.293) | - | ||
| I–II (n=529) | 22 (59.5) | |||
| III–IV (n=536) | 15 (40.5) | |||
| Diabetes mellitus | 1.258 (0.585–2.707) | - | ||
| No (n=858) | 28 (75.7) | |||
| Yes (n=221) | 9 (24.3) | |||
| Current smoking | 3.484*** (1.784–6.803) | 3.489*** (1.784-6.822) | ||
| No (n=876) | 21 (56.8) | |||
| Yes (n=203) | 16 (43.2) | |||
| Obesity | 0.560 (0.253–1.237) | - | ||
| No (n=727) | 29 (78.4) | |||
| Yes (n=352) | 8 (21.6) | |||
| Wound class | 1.878 (0.241–14.606) | - | ||
| Clean or clean/contaminated (n=1,050) | 36 (97.3) | |||
| Contaminated/dirty (n=16) | 1 (2.7) | |||
| Surgical approach | 1.433 (0.724–2.835) | - | ||
| Minimally invasive (n=879) | 25 (65.8) | |||
| Open (n=323) | 13 (34.2) | |||
| Improper timing of administration | 0.654 (0.326-1.314) | - | ||
| No (n=47) | 3 (7.9) | |||
| Yes (n=1,151) | 35 (92.1) | |||
| Oral kanamycin | 1.212 (0.620-2.366) | - | ||
| No (n=496) | 14 (36.8) | |||
| Yes (n=706) | 24 (63.2) | |||
CFZ/MTZ = cefazolin/metronidazole group; AMP/SUL = ampicillin/sulbactam group; ASA = American Society of Anesthesiologists; Inappropriate timing of administration = administration cannot be done within 1 hour before surgery; *: p-value<0.05; ***: p-value<0.001.
Table 3.
Comparison of non-inferiority between the two groups.
| CFZ/MTZ | AMP/SUL | RD | 95% confidence interval of the difference | P-value | |||
|---|---|---|---|---|---|---|---|
| M ± SD | M ± SD | ||||||
| Primary endpoint |
Surgical site infection | 0.04 ± 0.191 | 0.03 ± 0.160 | 0.05 | -0.009 | 0.032 | 0.264 |
| Secondary endpoint |
Deep/Organ space | 0.03 ± 0.162 | 0.01 ± 0.111 | 0.05 | -0.001 | 0.031 | 0.073 |
| Percutaneous drainage/surgical intervention | 0.01 ± 0.119 | 0.01 ± 0.079 | 0.05 | -0.003 | 0.020 | 0.167 | |
CFZ/MTZ = cefazolin/metronidazole group; AMP/SUL = ampicillin/sulbactam group; M = mean, SD = standard deviation, RD = risk difference.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



