
Submitted:
13 August 2023
Posted:
14 August 2023
You are already at the latest version
Abstract
(1) Background: Respiratory infections are a major public health problem worldwide, with potentially serious consequences. Indeed, these infections remain one of the main causes of morbidity and mortality in children under 5 years old in developing countries. Etiological information on respiratory infections is crucial for prevention and case management strategies. This systematic review aims to describe the etiology of respiratory infections reported in studies carried out in sub-Saharan African countries; (2) Methods: Using PubMed, HINARI and Google scholar search engines, a systematic search was carried out to identify published articles on the etiology of viral and/or bacterial respiratory infections in sub-Saharan Africa in patients of all ages. We have only considered data from sub-Saharan Africa. Papers published from 2010 to 2021, in English or French have been included in this review; (3) Results: After reviewing 115 articles reporting studies carried out in the African continent, only 32 articles were selected of which, studies were conducted in 15 sub-Saharan African countries, including 6/32 (18.75%) in Cameroon. Twenty (62.5%) were cross-sectional studies, and twenty-four (75%) were hospital-based investigations. In these studies, RT-PCR and culture methods were respectively used for viruses and bacteria investigations. Respiratory syncytial virus was the most frequently identified, with prevalence ranging from 0.6% to 59%, followed by rhinovirus (9.3% -73%), influenza virus (flu) A/B (0.9%-69.1%), and human adenovirus (0.9% - 30.8%). Streptococcus pneumoniae (14.2% - 96%), followed by Haemophilus influenzae type b (2.5% - 54%), and Klebsiella pneumoniae (1.4% - 49.9%) were the most frequently detected bacteria; (4) Conclusions: This review has reported that many pathogens, mainly viruses, are associated with acute respiratory infections in sub-Saharan Africa in both children and adults. Unfortunately, the limited geographical distribution of data across sub-Saharan Africa does not allow most of countries to develop an effective strategy for the prevention and treatment of respiratory infections.
Keywords:
Respiratory infection
; etiology
; viruses
; bacteria
; sub-Saharan Africa
1. Introduction
Respiratory viral infections are increasingly recognized as major contributors to hospitalization and mortality in all age groups of populations worldwide [1]. Most epidemiological knowledge is based on data from developed countries. In contrast, the burden of acute respiratory infections (ARI) is particularly heavy among children in developing countries, with high rates of hospital admissions and mortality [2,3]. Indeed, it is estimated that about 126 to 156 million cases of acute lower respiratory tract infections (ALRI) such as pneumonia and bronchiolitis occur in children worldwide each year, causing around 1.4 million deaths, with over 95% of which occur in Africa and Southeast Asia [4].
Upper respiratory tract infections are commonly caused by viruses or bacteria. Respiratory viruses are more often responsible for upper tract ARIs than bacteria in children under 5 years of age [3]. Common symptoms include nasal congestion, cough, sore throat, and fever. However, bacteria are less identified because of low sensitivity of bacterial culture in patients with community-acquired pneumonia [5]. Respiratory viruses such as respiratory syncytial virus, influenza viruses (A and B), parainfluenza viruses, human adenovirus, human coronaviruses OC43 and 229E, rhinovirus and metapneumovirus are currently recognized as common etiologies of ARI in young children in developed countries [2].
Recent use of molecular diagnostic techniques has identified other respiratory viruses associated with ARI, including human metapneumovirus, human Boca virus, human coronavirus NL63 and human coronavirus HKU1. In addition, human rhinovirus is implicated in the majority of cold cases and often induces lower respiratory tract infections [3].
A better understanding of the range of pathogens responsible for ARI is therefore essential for clinical cases management and the design of preventive strategies aimed at reducing childhood morbidity and mortality.
Lower respiratory tract infection (LRTI) is common in the elderly, children under five years of age and people who are immunocompromised or suffering from comorbidity [6]. People with symptoms suggestive of LRTIs can contract tuberculosis (TB) and/or other bacterial and viral infections [7]. Over the years, the most severe cases of pneumonia have been associated with Mycobacterium tuberculosis, with little information on other relevant bacterial pathogens [8]. Some common pathogens causing LRTIs other than Mycobacterium tuberculosis include: Streptococcus pneumoniae, Haemophilus influenzae, Klebsiella pneumoniae and Staphylococcus aureus [8].
The viral and bacterial etiologies of ARIs have been well documented in Northern Hemisphere countries. However, few studies are available in Africa [9]. Thus, the present study aimed at summarizing the literature related to the etiology of respiratory infections, in sub-Saharan African countries and to identify information gaps in order to improve essential knowledge on the subject.
We focused our research on sub-Saharan Africa, as epidemiological, socioeconomic and vaccine policy factors in North Africa would probably be very different [10].
2. Methods
The Materials and Methods should be described with sufficient details to allow others to replicate and build on the published results. Please note that the publication of your manuscript implicates that you must make all materials, data, computer code, and protocols associated with the publication available to readers. Please disclose at the submission stage any restrictions on the availability of materials or information. New methods and protocols should be described in detail while well-established methods can be briefly described and appropriately cited.
2.1. Search strategy
This review considers data from documents published online (articles, review, report, etc...) that reported information on both viral and bacterial etiology of ARIs in Africa, by searching the online bibliographic databases PubMed, HINARI and Google Scholar using the following key terms: “Acute respiratory infections”, “Upper respiratory infections”, “Lower respiratory infections”, “Viruses”, “Bacteria”, “Respiratory syndrome”, “Influenza syndrome”, “Africa”, “Prevalence”, and “etiology”. The reference list of selected articles was used as a lead for identifying further studies. The Boolean operators “AND” and “OR” were used to combine two or more terms. The search was limited to studies published in English or French, involving patients of any age in sub-Saharan Africa, in which pathogens were identified using immunofluorescence assays (IFA), Polymerase Chain Reactions (PCR), viral cultures, bacterial cultures or a combination of these methods.
2.2. Study selection
This review compiles studies focused on ARIs caused by viruses and/or bacteria. We only considered data from sub-Saharan Africa reported in papers published between 2010 and 2021, in English or French.
2.3. Inclusion criteria
Studies included were cohort, case-control, prospective, retrospective, and cross-sectional investigations reporting the prevalence of respiratory viruses in hospital and/or community settings. In the case of repeated studies, where the same population was recruited and examined over the same period, only the most recent or most complete study was included.
2.4. Exclusion criteria
There were no age or gender restrictions (Figure 1). Exclusion criteria were mainly: i) respiratory infections of non-human infections; ii) comparison of PCR kits for identification of respiratory pathogens and iii) studies on respiratory infection management policy.
2.5. Data extraction
Full versions of selected articles were downloaded and reviewed by two study authors. Data were extracted using a predefined form with the following information: i) references; ii) sample collection period; iii) year of publication; iv) study country; v) target population (age); vi) study area; vii) sample size; viii) sampling type; ix) prevalence of identified pathogens and; x) study type.
2.6. Data summary
We synthesized the data by summarizing the main findings of each study. Given the variety of study types included in the review, ranging from simple descriptive to analytical studies, we have considered a synthesis more appropriate rather than a formal meta-analysis. A table was created to list all the pathogens found in each study, together with relevant study information as mentioned above on data extraction.
2.7. Ethics and distribution
This work is based on published data and therefore does not require ethical approval. This systematic review should serve as a basis for developing strategies to prevent and control respiratory infections in sub-Saharan Africa, and as a foundation for future research that can focus on identifying the gaps found. We also plan to update the study in the future to track changes and guide solutions for health services and policies.
3. Results
3.1. Literature review
The published articles included in this review were those from studies with samples collected from 2010 to 2021. In order to filter articles for this review, we initially identified a total of 115 articles from PubMed, HINARI and Google Scholar that fit with our initial search strategy. Of these, 32 articles were included and 83 were excluded, after screening each article (Figure 1).
Of the 32 articles included, 5 (three for bronchiolitis and two for influenza) focused on viral and/or bacterial strains responsible for pneumonia in children and the elderly [11,12,13,14,15] and 27 focused on the surveillance and epidemiology of viral and/or bacterial strains responsible for respiratory infections (Table 1).
Many of these studies were carried out among children under 5 years of age. Articles excluded were related to comparisons of amplification kits, respiratory infection management policy, data from countries other than Africa, and those concerning non-human respiratory infections.
3.2. Features of included items
The 32 articles involved a total of 41,164 patients. Sample size ranged from 51 to 6,381 ARI patients per study. The included studies were obviously conducted in 15 sub-Saharan African countries (Figure 2).
A total of 6 published studies were conducted in Cameroon, 3 in the Democratic Republic of Congo (DRC), Ghana, and Gabon; two studies in Burkina Faso, South Africa, Côte d'Ivoire, Kenya, Niger and Nigeria respectively, and one study in each of the following countries: Senegal, Tanzania, Mali, Central African Republic (CAR) and Madagascar.
We identified 20 (62.5%) cross-sectional studies, 9 (28.12%) prospective studies, 4 (12.5%) retrospective studies and 4 (12.5%) cohort studies. We also noted case-control, analytical, longitudinal, and descriptive studies (Table 1).
Considering settings in which these published studies were focused, there were 24 (75%) hospital-based studies and 8 (25%) community-based studies. The study setting was urban in 27 (84.37%) studies, and mixed (rural, semi-rural and pre-urban) in 5 (15.62%) studies.
Pathogens were identified in a variety of respiratory samples, including nasal swabs, oropharyngeal swabs, nasopharyngeal aspirates, induced sputum, tracheal aspirates, bronchoalveolar lavage swabs and pulmonary aspirates.
Respiratory viruses were detected using immunofluorescence tests, multiplex RT-PCR, conventional PCR and viral cultures. RT-PCR was the most frequently used diagnostic method. For the detection of individual bacteria, only bacterial cultures were performed.
3.3. Etiology of pathogens detected
All the respiratory pathogens identified in these studies were viral and bacterial (Table 1). Among 32 articles reviewed, human respiratory syncytial virus was the most frequently identified, with a prevalence ranging from 0.6% - 59%, followed by human rhinovirus (9.3% - 73%), influenza A/B virus (0.9% - 69.1%), human adenovirus (0.9% - 30.8%), human parainfluenzavirus 1-4 (3.8% - 24%), enterovirus (2.9% - 25.5%), human coronaviruses (1.4% - 13.9%), human metapneumovirus (1.7% - 13.7%), and human bocavirus (1.4% - 10.6%) (Table 2).
Among the bacteria detected (Table 1), the most prevalent were Streptococcus pneumoniae (14.2% - 96%), followed by Haemophilus influenzae type b (2.5% - 54%), and Klebsiella pneumoniae (1.4% - 49.9%). Other bacterial species, notably Staphylococcus aureus (7.1% - 12.2%), Pnseudomonas aeruginosa (1.4% - 15.2%), and Mycobacterium tuberculosis (6.5%) were the least identified (Table 2).
4. Discussion
This review updates known information on respiratory infections of viral and/or bacterial etiology, in sub-Saharan Africa over the last twelve years. The overall aim of this systematic review was to inform public health actors and researchers on the etiology of respiratory infections (viral and bacterial) in Africa, and to provide information that can support actions to optimize decision-making by health authorities for the control of these infections.
A wide variety of detection techniques have been found in this review, including molecular viral detection, bacterial culture which are universal and reference methods for the characterization of respiratory infection pathogens. The results highlight a predominance of human respiratory syncytial virus and a strong association between human rhinovirus and influenza A/B virus in children aged under 5 years old presenting with influenza-like illness. The other most frequently detected viruses were adenovirus and all four types of human Parainfluenzae virus. This study also showed respiratory infections of bacterial origin, with the most frequently identified species being Streptococcus pneumoniae and Haemophilus influenzae in bacterial culture mainly as well as on sputum and Branco-alveolar lavage (BAL) samples in adults.
Little or no data were found on the etiology of respiratory infections in many sub-Saharan African countries. Of the 48 countries in sub-Saharan Africa (wikipedia.org/wiki/Afique_sub-saharienne), the 32 articles included in this review were carried out in only 15 countries, the majority of which were in Central and West Africa (Figure 2). No published studies were carried out in the Republic of Congo, although it borders with two (Cameroon and DRC) of the five countries where the number of deaths from childhood pneumonia is or was highest [39]. This lack of data could probably be due to the poor implementation of respiratory infection surveillance activities.
The pattern of predominance of human respiratory syncytial virus in this study is consistent with that reported by several previous narrative reviews [3,40]. Regardless of various factors, including screening test, type of sample tested, age of children, type of education and severity of infection, most studies indicated that human respiratory syncytial virus is the predominant causative agent of cases of respiratory diseases such as bronchiolitis, asthma, and wheezing with an incidence of between 50 and 80% [41]. Rhinovirus and influenzae A/B, the second most common viruses observed, have long been considered a cause of benign respiratory tract infections such as the common cold [9].
We found five studies that presented cases of viral and bacterial co-infections at rates of around 14% in our review [9,12,13,14,15]. Although Streptococcus pneumoniae is known to be more prevalent in superinfection in some respiratory syndromes, such as influenza [42,43], Haemophilus influenzae, and Klebsiella spp were also identified mostly in co-infection. This observation correlates with the review by Lansbury et al. who also showed that Klebsiella pneumoniae and Haemophilus influenzae were among the most frequent co-infecting bacterial pathogens [44]. Staphylococcus aureus was one of the least present, as expected [11]. Irrespective of testing issues, co-infection with other respiratory pathogens has important implications for diagnosis and prognosis.
Seasonality and study duration could clearly also lead to variability in the prevalence of viruses/bacteria responsible of respiratory infections.
5. Conclusion
This review shows that a number of viruses are associated with ARIs in children and adults in sub-Saharan Africa. The WHO’s global strategy for the control of ARI in children under 5 years of age must rigorously consider the importance of both viral and bacterial cases. Moreover, the results highlight the lack of data for several sub-Saharan African countries. Further high-quality studies are needed to determine the role of viruses and bacteria in ARI.
6. Study limits
This study has several limitations. Firstly, only publications in English or French were taken into account, excluding data published in Portuguese, which is the official language of five African countries (Angola, Cape Verde, Guinea-Bissau, Mozambique and Sao Tome and Principe), and in Spanish, the official language of Equatorial Guinea. Secondly, unpublished literature also constitutes an information bias in this systematic review. Finally, we did not assess the statistical quality of the studies by meta-analysis, but included all articles that met the inclusion criteria.
Author Contributions
DJE and PIM conceived, designed the study, and initiated the manuscript, KKF, BP, LE and NFR supervised the study. All authors read and approved the manuscript.
Acknowledgments
This review is a prelude to the activities of the COPANFLU project funded by IRD as part of the “Jeunes Equipes Associées à l'IRD” program. Many thanks to Donatien MOUKASSA, Grace FILA-FILA, Hosanna LEGUIYA, Henri OBA, aldi MANDIANGOU, Novy BOBOUAKA, Dachel EYENET, Yann MAVOUNGOU, Georcil AHOUET, Isaac ONYANKWANG, Reiche ELENGA, Durel BABISSAT, Valchy MIEGAKANDA, Jordy DONIAMA, Stéphane VEMBE, George TSOUMOU, Ines BAKOUMA, Laureate MADINGOU, Amour MOUANDA for their assistance with documentary research and reading of the manuscript.
Conflicts of Interest
The authors declare no competing interests.
References
- Zhang, S.; Zhang, W.; Tang, Y.W. Molecular diagnosis of viral respiratory infections. Current Infectious Disease Reports 2011, 13, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Ouédraogo, S.; Traoré, B.; Nene Bi, Z.A.B.; Yonli, F.T.; Kima, D.; Bonané, P.; Gueudin, M. Viral etiology of respiratory tract infections in children at the pediatric hospital in Ouagadougou (Burkina Faso). PloS one 2014, 9, e110435. [Google Scholar] [CrossRef] [PubMed]
- Sanou, A.M.; Cissé, A.; Millogo, T.; Sagna, T.; Tialla, D.; Williams, T. Systematic review of articles on etiologies of acute respiratory infections in children aged less than five years in sub-Saharan Africa, 2000-2015. EC Microbiology 2016, 6, 556–71. [Google Scholar]
- Sonego, M.; Pellegrin, M.C.; Becker, G.; Lazzerini, M. Risk factors for mortality from acute lower respiratory infections (ALRI) in children under five years of age in low and middle-income countries: a systematic review and meta-analysis of observational studies. PloS one 2015, 10, e0116380. [Google Scholar] [CrossRef]
- Gadsby, N.J.; McHugh, M.P.; Russell, C.D.; Mark, H.; Morris, A.C.; Laurenson, I.F.; Templeton, K.E. Development of two real-time multiplex PCR assays for the detection and quantification of eight key bacterial pathogens in lower respiratory tract infections. Clinical microbiology and infection 2015, 21, 788–e1. [Google Scholar] [CrossRef]
- Ayar, G.; Sahin, S.; Yazici, M.U.; Parlakay A, Ö.; Tezer, H. RSV pneumonia in the pediatric intensive care unit. J Pediatr Inf 2014, 8, 12–7. [Google Scholar] [CrossRef]
- Dube, F.S.; Kaba, M.; Robberts, F.J.; Ah Tow, L.; Lubbe, S.; Zar, H.J.; Nicol, M.P. Respiratory microbes present in the nasopharynx of children hospitalized with suspected pulmonary tuberculosis in Cape Town, South Africa. BMC infectious diseases 2016, 16, 597. [Google Scholar] [CrossRef]
- Deberu, O.; Nkrumah, B.; Sylverken, A.A.; Sambian, D.; Acheampong, G.; Amuasi, J.; Owusu, M. Common bacteria in sputum or gastric lavage of patients presenting with signs and symptoms of lower respiratory tract infections. The Pan African Medical Journal 2021, 38. [Google Scholar] [CrossRef]
- Lagare, A.; Maïnassara, H.B.; Issaka, B.; Sidiki, A.; Tempia, S. Viral and bacterial etiology of severe acute respiratory illness among children< 5 years of age without influenza in Niger. BMC infectious diseases 2015, 15, 1–7. [Google Scholar]
- Gessner, B.D.; Shindo, N.; Briand, S. Seasonal influenza epidemiology in sub-Saharan Africa: a systematic review. The Lancet infectious diseases 2011, 11, 223–235. [Google Scholar] [CrossRef]
- Tchatchouang, S.; Nzouankeu, A.; Kenmoe, S.; Ngando, L.; Penlap, V.; Fonkoua, M.C.; Njouom, R. Bacterial aetiologies of lower respiratory tract infections among adults in Yaoundé, Cameroon. BioMed research international 2019, 2019. [Google Scholar] [CrossRef] [PubMed]
- Lagare, A.; Ousmane, S.; Dano, I.D.; Issaka, B.; Issa, I.; Mainassara, H.B.; Mamadou, S. Molecular detection of respiratory pathogens among children aged younger than 5 years hospitalized with febrile acute respiratory infections: A prospective hospital-based observational study in Niamey, Niger. Health Science Reports 2019, 2, e137. [Google Scholar] [CrossRef] [PubMed]
- Birindwa, A.M.; Kasereka, J.K.; Gonzales-Siles, L.; Geravandi, S.; Mwilo, M.; Tudiakwile, L.K.; Skovbjerg, S. Bacteria and viruses in the upper respiratory tract of Congolese children with radiologically confirmed pneumonia. BMC Infectious Diseases 2021, 21, 1–11. [Google Scholar] [CrossRef]
- Mhimbira, F.; Hiza, H.; Mbuba, E.; Hella, J.; Kamwela, L.; Sasamalo, M.; Fenner, L. Prevalence and clinical significance of respiratory viruses and bacteria detected in tuberculosis patients compared to household contact controls in Tanzania: a cohort study. Clinical microbiology and infection 2018, 25, 107–e1. [Google Scholar] [CrossRef]
- Razanajatovo, N.H.; Guillebaud, J.; Harimanana, A.; Rajatonirina, S.; Ratsima, E.H.; Andrianirina, Z.Z.; Heraud, J.M. Epidemiology of severe acute respiratory infections from hospital-based surveillance in Madagascar, November 2010 to July 2013. PLoS One 2018, 13, e0205124. [Google Scholar] [CrossRef]
- Lekana-Douki, S.E.; Mouinga-Ondémé, A.; Nkoghe, D.; Drosten, C.; Drexler, J.F.; Kazanji, M.; Leroy, E.M. Early introduction and delayed dissemination of pandemic influenza, Gabon. Emerging Infectious Diseases 2013, 19, 644. [Google Scholar] [CrossRef] [PubMed]
- Lekana-Douki, S.E.; Nkoghe, D.; Drosten, C.; Ngoungou, E.B.; Drexler, J.F.; Leroy, E.M. Viral etiology and seasonality of influenza-like illness in Gabon, March 2010 to June 2011. BMC infectious diseases 2014, 14, 1–11. [Google Scholar] [CrossRef]
- Breiman, R.F.; Cosmas, L.; Njenga, M.K.; Williamson, J.; Mott, J.A.; Katz, M.A.; Feikin, D.R. Severe acute respiratory infection in children in a densely populated urban slum in Kenya, 2007-2011. BMC infectious diseases 2015, 15, 1–11. [Google Scholar] [CrossRef]
- Serengbe, G.B.; Gody, J.C.; Fioboy, R.; Nakoune, E. Viral etiology of acute respiratory infections in children in Bangui. Archives de Pediatrie 2014, 22, 324. [Google Scholar] [CrossRef]
- Kenmoe, S.; Tchendjou, P.; Vernet, M.A.; Moyo-Tetang, S.; Mossus, T.; Njankouo-Ripa, M.; Njouom, R. Viral etiology of severe acute respiratory infections in hospitalized children in Cameroon, 2011-2013. Influenza and other respiratory viruses 2016, 10, 386–393. [Google Scholar] [CrossRef]
- Uzoamaka, M.; Ngozi, O.; Johnbull, O.S.; Martin, O. Bacterial etiology of lower respiratory tract infections and their antimicrobial susceptibility. The American Journal of the Medical Sciences 2017, 354, 471–475. [Google Scholar] [CrossRef]
- Niang, M.N.; Diop, N.S.; Fall, A.; Kiori, D.E.; Sarr, F.D.; Sy, S.; Dia, N. Respiratory viruses in patients with influenza-like illness in Senegal: focus on human respiratory adenoviruses. PLoS One 2017, 12, e0174287. [Google Scholar] [CrossRef] [PubMed]
- Famoroti, T.; Sibanda, W.; Ndung'u, T. Prevalence and seasonality of common viral respiratory pathogens, including Cytomegalovirus in children, between 0-5 years of age in KwaZulu-Natal, an HIV endemic province in South Africa. BMC pediatrics 2018, 18, 1–10. [Google Scholar] [CrossRef]
- Kadjo, H.A.; Adjogoua, E.; Dia, N.; Adagba, M.; Abdoulaye, O.; Daniel, S.; Dosso, M. Detection of non-influenza viruses in acute respiratory infections in children under five-year-old in Cote d'Ivoire (January-December 2013). African Journal of Infectious Diseases 2018, 12, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Sanou, A.M.; Wandaogo SC, M.; Poda, A.; Tamini, L.; Kyere, A.E.; Sagna, T.; Snoeck, C.J. Epidemiology and molecular characterization of influenza viruses in Burkina Faso, sub-Saharan Africa. Influenza and other respiratory viruses 2018, 12, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Obodai, E.; Odoom, J.K.; Adiku, T.; Goka, B.; Wolff, T.; Biere, B.; Reiche, J. The significance of human respiratory syncytial virus (HRSV) in children from Ghana with acute lower respiratory tract infection: a molecular epidemiological analysis, 2006 and 2013-2014. PLoS One 2018, 13, e0203788. [Google Scholar] [CrossRef] [PubMed]
- Lekana-Douki, S.E.; Behillil, S.; Enouf, V.; Leroy, E.M.; Berthet, N. Detection of human bocavirus-1 in both nasal and stool specimens from children under 5 years old with influenza-like illnesses or diarrhea in Gabon. BMC research notes 2018, 11, 1–7. [Google Scholar] [CrossRef]
- Kabego, L.; Balol'Ebwami, S.; Kasengi, J.B.; Miyanga, S.; Bahati, Y.L.; Kambale, R.; de Beer, C. Human respiratory syncytial virus: prevalence, viral co-infections and risk factors for lower respiratory tract infections in children under 5 years of age at a general hospital in the Democratic Republic of Congo. Journal of Medical Microbiology 2018, 67, 514–522. [Google Scholar] [CrossRef]
- Kenmoe, S.; Vernet, M.A.; Le Goff, J.; Penlap, V.B.; Vabret, A.; Njouom, R. Molecular characterization of human adenovirus associated with acute respiratory infections in Cameroon from 2011 to 2014. Virology journal 2018, 15, 1–7. [Google Scholar] [CrossRef]
- Adema, I.W.; Kamau, E.; Uchi Nyiro, J.; Otieno, G.P.; Lewa, C.; Munywoki, P.K.; Nokes, D.J. Surveillance of respiratory viruses among children attending a primary school in rural coastal Kenya. Wellcome Open Research 2020, 5, 63. [Google Scholar] [CrossRef]
- Kengne-Nde, C.; Kenmoe, S.; Modiyinji, A.F.; Njouom, R. Prevalence of respiratory viruses using polymerase chain reaction in children with wheezing, a systematic review and meta-analysis. Plos one 2020, 15, e0243735. [Google Scholar] [CrossRef]
- Buchwald, A.G.; Tamboura, B.; Tennant, S.M.; Haidara, F.C.; Coulibaly, F.; Doumbia, M.; Tapia, M.D. Epidemiology, risk factors, and outcomes of respiratory syncytial virus infections in newborns in Bamako, Mali. Clinical Infectious Diseases 2020, 70, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Obe, O.A.; Mutiu, B.W.; Amoo, A. Respiratory Syncytial Virus Infection among Children in Lagos, Nigeria. J Clin Immunol Microbiol 2021, 2, 1–11. [Google Scholar] [CrossRef]
- Kouakou, V.; Kadjo, H.; N'nan Alla Oulo, F.D.; N'guessan AN, D. Surveillance of Respiratory Syncytial Virus in Children Aged 0-5 years in Côte d'Ivoire. American Journal of BioScience 2021, 9, 185. [Google Scholar] [CrossRef]
- Kenmoe, S.; Sadeuh-Mba, S.A.; Vernet, M.A.; Penlap Beng, V.; Vabret, A.; Njouom, R. Molecular epidemiology of Enteroviruses and Rhinoviruses in patients with acute respiratory infections in Yaounde, Cameroon. Influenza and other respiratory viruses 2021, 15, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Baillie, V.L.; Moore, D.P.; Mathunjwa, A.; Baggett, H.C.; Brooks, A.; Feikin, D.R.; Madhi, S.A. Epidemiology of the rhinovirus (RV) in African and Southeast Asian children: a case-control pneumonia etiology study. Viruses 2021, 13, 1249. [Google Scholar] [CrossRef]
- Ntagereka, P.B.; Basengere, R.A.; Baharanyi, T.C.; Kashosi, T.M.; Buhendwa JP, C.; Bisimwa, P.B.; Mukwege, D. Molecular evidence of coinfection with acute respiratory viruses and high prevalence of SARS-CoV-2 among patients presenting flu-like illness in Bukavu city, Democratic Republic of Congo. Canadian Journal of Infectious Diseases and Medical Microbiology 2022, 2022. [Google Scholar] [CrossRef]
- Kafintu-Kwashie, A.A.; Nii-Trebi, N.I.; Obodai, E.; Neizer, M.; Adiku, T.K.; Odoom, J.K. Molecular epidemiological surveillance of viral agents of acute lower respiratory tract infections in children in Accra, Ghana. BMC pediatrics 2022, 22, 364. [Google Scholar] [CrossRef]
- Nair, H.; Simões, E.A.; Rudan, I.; Gessner, B.D.; Azziz-Baumgartner, E.; Zhang JS, F.; Campbell, H. Global and regional burden of hospital admissions for severe acute lower respiratory infections in young children in 2010: a systematic analysis. The Lancet 2013, 381, 1380–1390. [Google Scholar] [CrossRef]
- Kenmoe, S.; Kengne-Nde, C.; Ebogo-Belobo, J.T.; Mbaga, D.S.; Fatawou Modiyinji, A.; Njouom, R. Systematic review and meta-analysis of the prevalence of common respiratory viruses in children< 2 years with bronchiolitis in the pre-COVID-19 pandemic era. PLoS One 2020, 15, e0242302. [Google Scholar]
- Van der Zalm, M.M.; Uiterwaal, C.S.; Wilbrink, B.; Koopman, M.; Verheij, T.J.; van der Ent, C.K. The influence of neonatal lung function on rhinovirus-associated wheeze. American journal of respiratory and critical care medicine 2011, 183, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Ge, Y.; Wu, T.; Zhao, K.; Chen, Y.; Wu, B.; Cui, L. Co-infection with respiratory pathogens among COVID-2019 cases. Virus research 2020, 285, 198005. [Google Scholar] [CrossRef] [PubMed]
- Musuuza, J.S.; Watson, L.; Parmasad, V.; Putman-Buehler, N.; Christensen, L.; Safdar, N. Prevalence and outcomes of co-infection and superinfection with SARS-CoV-2 and other pathogens: a systematic review and meta-analysis. PloS one 2021, 16, e0251170. [Google Scholar] [CrossRef] [PubMed]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID-19: a systematic review and meta-analysis. Journal of Infection 2020, 81, 266–275. [Google Scholar] [CrossRef]
Figure 1.
Summary of search strategy.
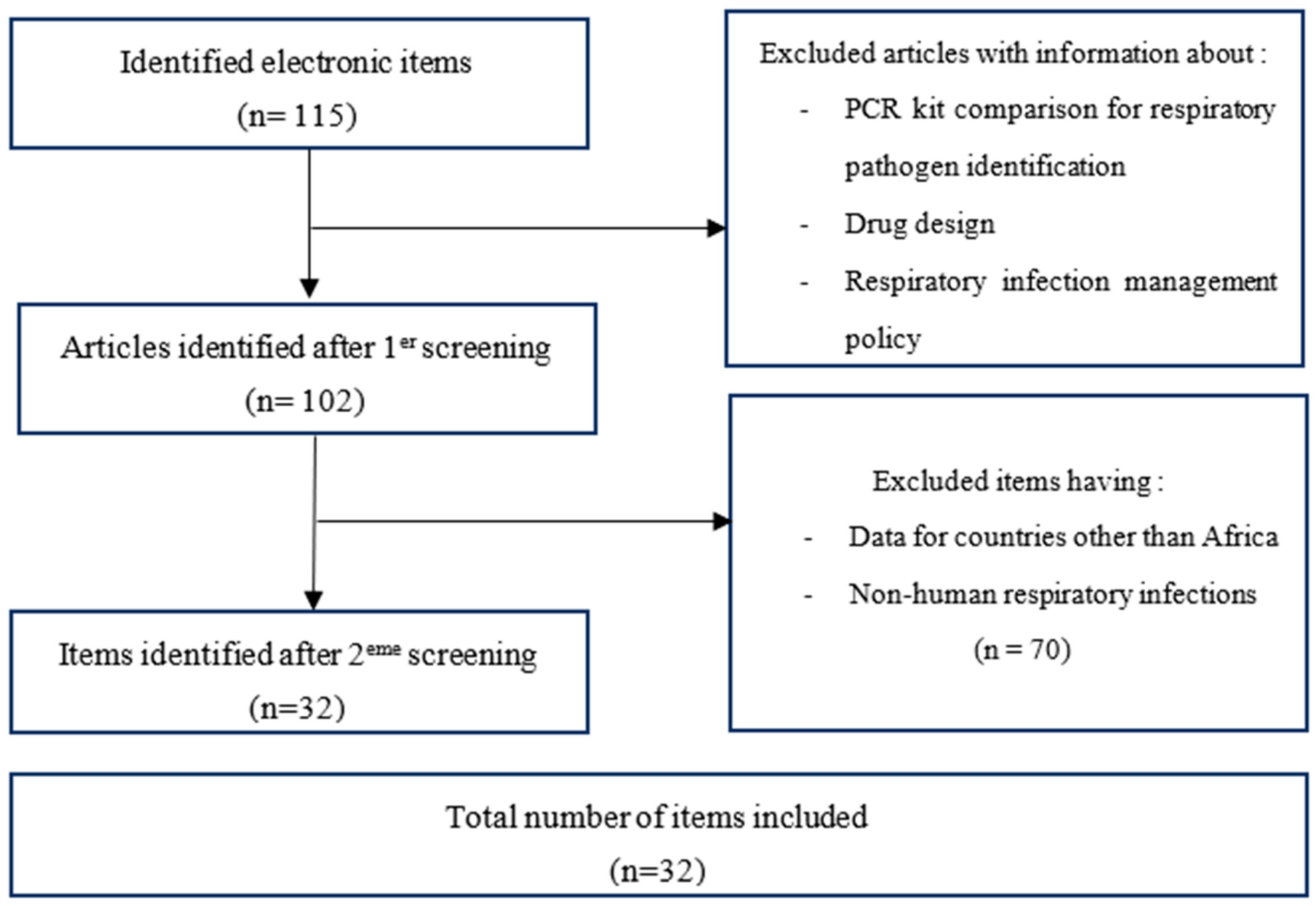
Figure 2.
Geographical identification of the 32 included studies (map generating with QGIS 3.16.0).
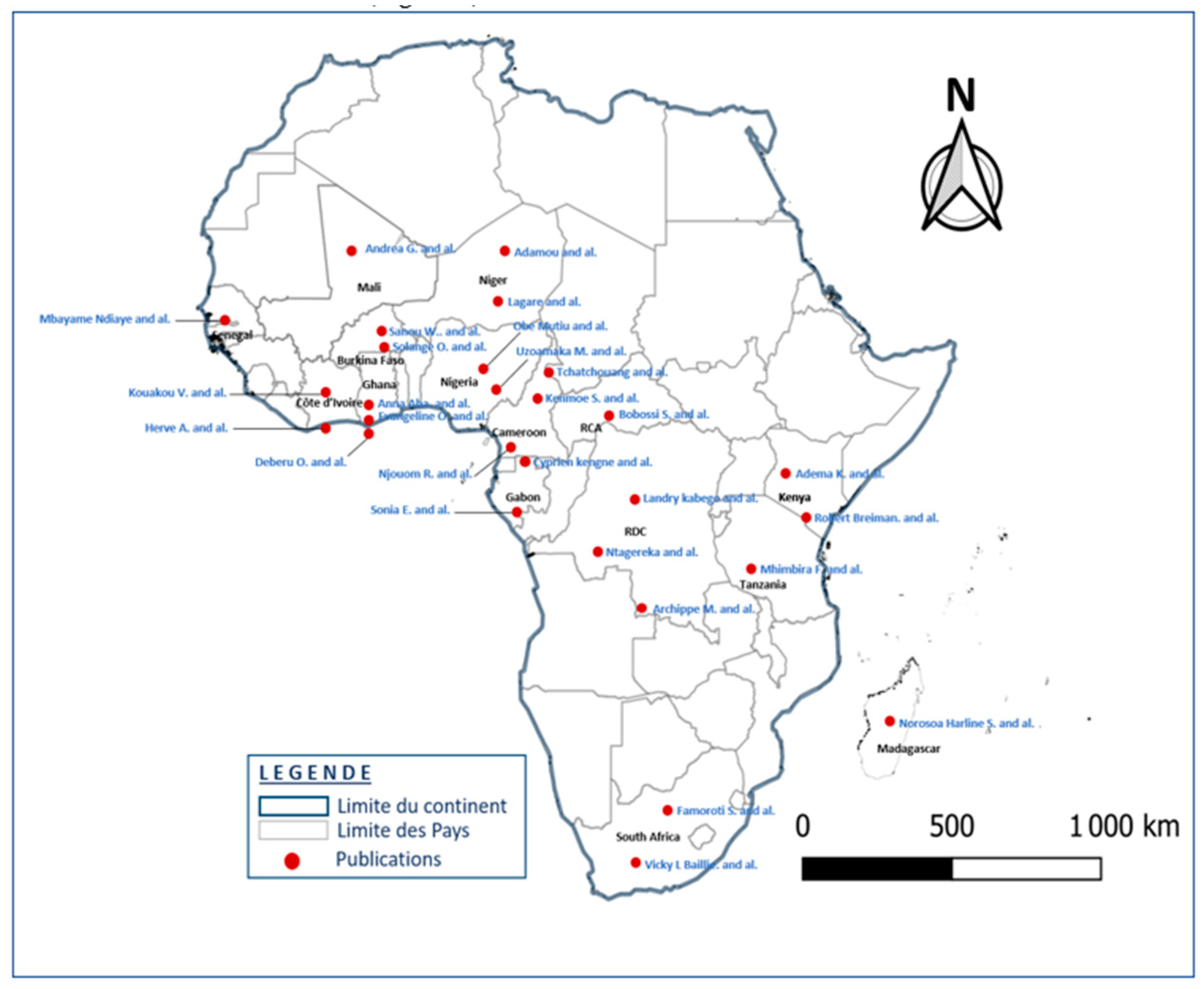

Table 1.
Summary of published articles included in the review.
| References | Collection period | Year of publication | Study country | Age range | Zone / Sample size | Type of sampling | Prevalence of pathogens | Type of study |
|---|---|---|---|---|---|---|---|---|
| [16] Lekana-Douki et al. | 2009 - 2011 | 2013 | Gabon | No limit | Urban/966 | Nasal | Flu A (61%); Flu B (39%) | Cross-sectional/ Prospective |
| [17] Lekana-Douki et al. | 2010 - 2011 | 2014 | Gabon | No limit | (Urban) /1041 | Nasopharyngeal | HAdV (17.5%), HPIV 1-4 (16.8%), EV (14.7%), HRSV (13.5%), and Flu A (11.9%). | Cross-sectional |
| [2] Ouédraogo et al. | 2010 - 2011 | 2014 | Burkina Faso | < 3 years | (Urban) /209 | Nasopharyngeal | HRV (59.1%); EV (25.5%); HRSV (16.1%); HMPV (9.4%) | Prospective |
| [9] Lagare et al. | 2010 -2012 | 2015 | Niger | < 5 years | (Urban) /160 | Nasopharyngeal | HRSV (35%); HRV (29%); HPIV (24%); S. pneumoniae (56%); H. inflenzae (12%) | Retrospective |
| [18] Breiman et al. | 2007 - 2011 | 2015 | Kenya | < 5 years | 2592 | Naso/ Oro -pharyngeal | HRV/EV ( 42% ); HRSV ( 25% ); HAdV ( 20% ); HMPV ( 13,7% ), Flu A ( 10,8% ) | Cross-sectional |
| [19] Serengbe et al. | 2013 | 2015 | CAR | < 5 years | 361 | Nasopharyngeal | HRV(47,5%);FluA/B (26,6%);HPIV-3(9,3%);HRSV(5,8% ); EV(4,3%); HAdV (2,9%); HBoV (1,4%); HCoV (1,4%) | Cross-sectional |
| [20] Kenmoe et al. | 2011 - 2013 | 2016 | Cameroon | ≤15 | (Urban) /347 | Nasopharyngeal | HRSV ( 13.2% ), HAdV ( 27.3% ), HboV ( 10.6% ), Flu A/B ( 9.8% ); HPIV ( 6.6% ); HCoV ( 5.7% ); HMPV ( 2.3% ); HRV/EV (11.5%) | Prospective |
| [21] Uzoamaka et al. | 2014 - 2016 | 2017 | Nigeria | No limit | (Peri-urban) / 954 |
Expectoration | Klebsiella pneumonia ( 49,9% ); Klebsiella spp/ Pseudomonas aeruginosa, ( 1.4% ) | Cross-sectional |
| [22] Niang et al. | 2012 - 2015 | 2017 | Senegal | No limit | (Urban) /6381 | Naso/ Oro -pharyngeal | HAdV ( 30,8% ); FluA/B ( 53,1% ); HRV ( 30% ); Ev ( 18,5% ); HRSV ( 13,5% ) | Cross-sectional, Prospective |
| [23] Famoroti et al. | 2011 - 2015 | 2018 | South Africa | 0 - 5 years | (Urban) /2172 | Expectoration /Nasopharyngeal |
HRSV (32.1%), HAdV (21.8%), HRV (15.4%), FluA swl (5.1%) | Retrospective |
| [24] Kadjo et al. | 2013 | 2018 | Ivory Coast | < 5 years | (Urban) /1340 | Nasopharyngeal | HRV (31.92%), HRSV (24.4%), HPIV (20.5%), HCoV 229E ( 12.05% ) | Cross-sectional |
| [25] Sanou et al. | 2014 - 2015 | 2018 | Burkina Faso | < 5 years | (Urban) / 924 | Nasopharyngeal | Flu A/B (15.1%), A(H3N2) (69.1%) A(H1N1) pdm09 (30.9%) | Cross-sectional |
| [26] Obodai et al. | 2006, 2013-2014 | 2018 | Ghana | < 5 years | (Urban) /552 | Nasopharyngeal | HRSV ( 23% ) | Cross-sectional |
| [27] Lekana-Douki et al. | 2018 | 2018 | Gabon | < 5 years | (Urban) / 810 | Nasopharyngeal | HBoV ( 4,4% ) | Retrospective |
| [28] Kabego et al. | 2016 | 2018 | DRC | < 5 years | (Urban) / 146 | Nasopharyngeal | HRSV ( 21.2 % ); HRV ( 16.4 % ); HPIV-3 ( 13.7% ) and HAdV ( 4.79 % ). | Cross-secctional, analytical/ Prospective |
| [14] Mhimbira et al. | 2013 - 2015 | 2018 | Tanzania | No limit | (Urban) /972 | Nasopharyngeal | HRV ( 9.3% ); Influenza A ( 3.1% ); HRSV A/B ( 1.9% ); H. influenzae ( 26.1% ); S. pneumoniae ( 21.5% ) | Prospective cohort |
| [29] Kenmoe et al. | 2011 - 2014 | 2018 | Cameroon | < 15 years | (Urban) / 811 | Nasopharyngeal | HAdV( 27.12% ) | Cross-sectional |
| [15] Razanajatovo et al. | 2010 - 2013 | 2018 | Madagascar | No limit | (Urban) / 876 | Nasopharyngeal, Expectorations Blood |
HRSV ( 37,7% ) ; FluA ( 18,4% ) ; HRV ( 13,5% ) ; HAdV ( 8,3% ) ; S. Pneumoniae ( 50,3% ) ; H. Influenzae b ( 21,4% ) ; Klebsiella ( 4,6% ) | Prospective |
| [12] Lagare, et al. | 2015 | 2019 | Niger | < 5 years | (Urban) / 638 | Expectoration /Nasopharyngeal |
HRSV ( 23,3 % ), HPIV ( 12,2% ), HRV ( 9,4 % ), HAdV ( 9,4 % ), Flu A ( 8,1 %) / S. pneumoniae ( 39%) , Staph. aureus ( 12,2% ), H. influenzae B ( 2,5% ) | Prospective |
| [11] Tchatchouang et al. | 2019 | 2019 | Cameroon | No limit | (Urban) /141 | Branco-alveolar lavage (BAV) | S. pneumoniae/ H. infuenzae (14.2%); K. pneumoniae (9.2%); Staph. aureus, (7.1%) | Foresight |
| [30] Adema et al. | 2017 - 2018 | 2020 | Kenya | < 20 years | (Urban) /781 | Nasopharyngeal | HRV (16.7%); HPIV (2.7%) ; HCoV (229E,NL63, OC43 ) (2.0%) ; HAdV (0.9%) ; HRSV (0.6%) | Longitudinal/ Cohort |
| [31] Kengne-Nde et al. | 2019 | 2020 | Cameroon | No limit | 1426 | Naso/ Oro -pharyngeal | HRV ( 35,6% ); HRSV ( 31,0% ); HBoV ( 8,1% ); HAdV ( 7,7% ); Flu A/B ( 6,5% ); HMPV ( 5,8% ); EV ( 4,3% ); HPIV 1-4 ( 3,8% ); HCoV ( 2,2% ) | Cohort, Case-control, Cross-sectional |
| [49] Kenmoe et al. | 2019 - 2020 | 2020 | Cameroon | < 2 years | 51 | Naso/ Oro -pharyngeal | HRSV ( 59% ); HRV ( 19,3% ); HBoV ( 8,2% ); HAdV ( 6,1% ); HMPV ( 5,4% ); HPIV ( 5,4% ); Flu A/B ( 3,2% ); HCoV ( 2,9% ); Ev ( 2,9% ) | Cross-sectional |
| [32] Buchwald et al. | 2011 - 2013 | 2020 | Mali | < 2 years | (Urban) /1333 | Naso/ Oro -pharyngeal | HRSV ( 37% ) | Cohort |
| [33] Obe et al. | 2021 | 2021 | Nigeria | < 5 years | (Urban) /200 | Nasopharyngeal | HRSV ( 22.5% ) | Cross-sectional |
| [8] Deberu et al. | 2018 - 2019 | 2021 | Ghana | No limit | (Urban) /264 | Expectoration | Klebsiella spp. (28%); M. tuberculosis (6.5%); Pseudomonas spp.( 15.2% ) | Retrospective |
| [34] Kouakou et al. | 2021 | 2021 | Ivory Coast | ≤ 5 years | (Urban/rural) / 5648 | Nasopharyngeal | HRSV ( 10% ) | Cross-sectional/ descriptive |
| [35] Kenmoe et al. | 2011 - 2014 | 2021 | Cameroon | No limit | (Urban) / 974 | Nasopharyngeal | HRV/EV ( 16.4% ) | Cross-sectional |
| [13] Birindwa et al. | 2015 - 2017 | 2021 | DRC | ≤ 5 years | (Urban) /2322 | Nasopharyngeal | H. influenzae ( 54% ); S. pneumoniae ( 96% ); HRV ( 73% ); EV ( 17% ); HRSV ( 7% ); | Cross-sectional |
| [36] Baillie et al. | 2011 - 2014 | 2021 | South Africa | ≤ 5 years | (Urban) /4232 | Naso/ Oro -pharyngeal | HRV ( 21% ) ; | Cross-sectional |
| [37] Ntagereka, et al. | 2021 | 2022 | DRC | No limit | (Urban) /1352 | Oro-pharyngeal | SARS-CoV-2 ( 13.9% ), Flu A ( 5.6% ), Flu B (0.9%) | Cross-sectional |
| [38] Kafintu-Kwashie et al. | 2015 - 2016 | 2022 | Ghana | < 5 years | (Urban) /188 | Nasopharyngeal | HRSV (11.4); HMPV ( 1.7 %); | Cross-sectional |
ABBREVIATIONS: HRSV: Human Respiratory Syncytial Virus; HRV: Human Rhinovirus; HAdV: Human Adenovirus; Flu A/B: Influenza viruses A/B type; HPIV 1-4: Human Parainfluenza viruses 1-4 types; EV: Enterovirus; hCoV: Human Coronavirus ; hMPV: Human Metapnemovirus; hBoV: Human Bocavirus; SARS-CoV-2: Severe acute respiratory syndrome coronavirus 2 ; S. pneumoniae: Streptococcus pneumoniae; S. aureus: Staphylococcus aureus; H. influenza b: Haemophilus influenzae b type; K. pneumoniae: Klebsiella pneumoniae; P. aeruginosa: Pnseudomonas aeruginosa; M. tuberculosis: Mycobacterium tuberculosis.
Table 2.
Proportion of pathogens identified in the 32 articles studied, conducted in several countries.
Table 2.
Proportion of pathogens identified in the 32 articles studied, conducted in several countries.
| Prevalence (%) | Number of studies | Number of countries | |
|---|---|---|---|
| VIRUS | |||
| Human Respiratory Syncytial Virus | 0,6 - 59 | 23 | 15 |
| Human rhinovirus | 9,3 - 73 | 17 | 11 |
| Influenza virus A/B | 0,9 - 69 | 18 | 11 |
| Human adenovirus | 0,9 - 30,8 | 14 | 9 |
| Para Human Influenza virus | 3,8 - 24 | 10 | 7 |
| Human Enterovirus | 2,9 - 25,5 | 9 | 7 |
| HCoV NL63 | 1,4 - 5,7 | 7 | 3 |
| HCoV OC43 | 1,4 - 5,7 | 7 | 3 |
| HCoV 229E | 2,0 - 12,05 | 7 | 4 |
| HCoV HKU-1 | 1,4 - 5,7 | 6 | 2 |
| Human metapneumovirus | 1,7 - 13,7 | 6 | 4 |
| Human bocavirus | 1,4 - 10,6 | 5 | 3 |
| BACTERIA | |||
| Streptococcuspneumoniae | 14,2 - 96 | 6 | 5 |
| Haemophilus influenzaetype b | 2,5 - 54 | 6 | 5 |
| Klebsiella pneumoniae | 1,4 - 49,9 | 5 | 4 |
| Staphylococcus aureus | 7,1 - 12,2 | 2 | 2 |
| Pnseudomonas aeruginosa | 1,4 - 15,2 | 2 | 2 |
| Mycobacterium tuberculosis | 0 - 6,5 | 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



