
Submitted:
14 August 2023
Posted:
16 August 2023
You are already at the latest version
Abstract
Background: To analyze long-term outcomes in patients undergoing thoracic endovascular aortic repair (TEVAR).
Methods: All consecutive 97 patients undergoing TEVAR between September 2014 and September 2022 were included in the study. Primary outcome was long-term incidence of overall death and major adverse cardiovascular and cerebrovascular events (MACCE).
Results: Mean age was 70.4 years, and 22(23.2%) had cerebrovascular disease (CBVD). A total of 49(51.6%) of patients had prior cardiac surgery intervention and 8(8.5%) had prior aortic valve replacement. Twenty-eight patients(28.8%) presented with aortic dissection, 60(61.8%) had aortic aneurysm, 4(4.1%) had intramural hematoma, and 5(5.1%) had other presentations. An emergent procedure was performed in 6(6.2%) patients, an urgent procedure in 37(38.1%) patients and 54(55.7%) patients had an elective procedure. Intraoperatively, 78.3% had percutaneous TEVAR, 5.1% had ministernotomy TEVAR, while 10.3% had concomitant full sternotomy TEVAR repair. Hospital mortality was 7 patients(7.2%). At 8-years follow-up, 76% were alive, 25.8% had MACCE, 21.6% were diagnosed with endoleaks(13 patients type II and 2 patients type 1) while 10.3% un-derwent repeat intervention.
Conclusions: This single center experience in patients undergoing TEVAR evidenced good short and long-term survival and MACCE. Nonetheless, almost half of the patients underwent an ur-gent/emergent procedure, clinical results were favourable for TEVAR.
Keywords:
TEVAR
; long-term outcome
; MACCE
1. Introduction
Thoracic endovascular aortic repair (TEVAR) has gained popularity among cardiac surgeons and numbers of procedures worldwide have shown an upward trend [1,2]. Several series have reported encouraging results with TEVAR [3,4,5,6,7]. In addition, multicenter studies reported good long-term outcomes in patients undergoing TEVAR versus thoracoabdominal cardiovascular surgery [8,9]. However, long-term outcome complications, including aortic rupture and endoleaks, have an overall negative impact on long-term survival and repeat intervention [10]. Encouraging results of TEVAR have prompted many surgeons to use stent-grafts in more challenging anatomical regions, therefore using a hybrid approach and increasing the risk of procedural failure. In this context, periprocedural risk predictors that impact long-term prognosis after TEVAR remain hindered. In addition, long-term outcomes from TEVAR have prompted ambiguous outcomes in patients with aortic disease. Therefore, we aimed to analyze our single center experience in patients undergoing TEVAR. In addition, we aimed to find and analyze periprocedural risk predictors that impact long-term prognosis after TEVAR.
2. Materials and Methods
2.1. Patient’s Identification and Inclusion Criteria
We identified all consecutive patients who underwent TEVAR between September 2014 and September 2022 at Lankenau Heart Institute (Lankenau Medical Center, PA, USA). The study protocol was approved by the Main Line Health Hospitals Institutional Review Board (IRB 45CFR164.512). Inclusion criteria was all patients who underwent TEVAR. All patients baseline demographics and pre-operative characteristics were described in the analysis.
Patients were identified via operation codes in a digital operation registry, as well as from a centralized cardiac surgery database for all TEVAR operations. Clinical data was derived from medical records that were populated prospectively. Underlying in-hospital outcomes were recorded from the charts and death certificate made out by the responsible physician.
2.2. Patients’ follow-up
Follow-up was done at our outpatient’s clinic and from the hospital registry. During the study period, four surgeons performed TEVAR procedures in our institution. All patients had at least one follow-up time point available. In case the patient did not show up at a follow-up visit, we called the referring cardiologist to acquire the information for this study.
2.3. Clinical Assessment of the Patients
Pre-operative assessment included evaluation of patient’s risk factors, imaging, and sizing (CT-scan calibrated aortography) of the aorta and iliac arteries, and a consensual final decision was taken following a multidisciplinary active heart staff meeting involving a cardiac and a vascular surgeon, an anaesthetist, a cardiologist, a radiologist, and a respiratory physician.
2.4. Primary and Secondary Objectives and Definitions
Primary outcome was analysis of all-cause death and MACCE in patients undergoing TEVAR. Secondary goals were non-fatal stroke, non-fatal myocardial infarction (MI), reintervention and presence of endoleaks as discrete events on the composite. Other clinical definitions are included in Supplemental Document S1.
2.5. Interventional Procedure
For pathologies involving the aortic arch, successful stent-graft placement required supra-aortic vessel (SAV) debranching before stent graft deployment, to achieve a suitable proximal landing zone. In case of staged procedure, 1 week interval was kept between debranching and TEVAR procedures. Prophylactic use of cerebrospinal fluid drainage to prevent spinal cord ischemia was used. In cases where over-stenting of the origin of the left subclavian artery was necessary, revascularization was performed in elective cases and in emergent patients without unstable hemodynamic status at the time of treatment. In a few cases, over-stenting of the celiac aorta was deemed necessary. Visceral debranching was performed via a prosthetic bypass from the aorta or iliac artery to the celiac trunk, superior mesenteric artery, and/or renal arteries. After achieving suitable landing zones, endograft deployment was performed. After deployment, stent-graft modeling with a low-pressure balloon was performed, except in dissection cases. Outcome criteria were defined according to the Reporting Standards for Thoracic Endovascular Aortic Repair [11]. Technical success required successful introduction and successful deployment of the device in absence of surgical conversion to open repair, death within 24 hours, type I or II endoleaks as evidenced by procedural angiography, or graft obstruction. Follow-up included clinical examination and computed tomography scans during hospital stay, and at 1 month, 6 months, and yearly after the procedure.
2.6. Covariates included in the study
Covariate included in the study were age, gender, race, STS-PROM risk score, body mass index (BMI), obesity, creatinine level, comorbidities such as preoperative dialysis, smoking, hypertension, dyslipidemia, cerebrovascular disease (CBVD), peripheral vascular disease (PVD), liver disease, diabetes, mediastinal radiation, prior percutaneous coronary intervention (PCI), prior CABG, prior MI, prior valve surgery, atrial fibrillation (Afib), ejection fraction (EF).
2.7. Statistical Analysis
Creatinine clearance was calculated according to the Cockcroft-Gault equation. Estimated weights were incorporated into Cox-proportional hazards regression models for primary and secondary end points. To illustrate the effect of TEVAR intervention on long-term survival, Kaplan–Meier cumulative survival curves were constructed and compared by the log-rank test. A sensitivity analysis was done in a series of covariate adjusted. Pre-operative variables were incorporated into a Cox-proportional hazards regression model to find predictors impacting all-cause death, cardiac death, MACCE (all-cause death, stroke, MI, repeat intervention), stroke, MI, repeat intervention, and incidence of endoleak.
All analyses were performed in Stata 17.0 (StataCorp, LLC. College Station, TX). 95% confidence intervals and p-values are reported with a p-value < 0.05 considered significant.
3. Results
3.1. Pre-operative Characteristics
A total of 97 consecutive endografts were deployed (Table 1). Patients’ characteristics included a mean age of 70.4 years. 50.5% were females, 23.2% had cerebrovascular disease (CBVD), 27.1% had chronic obstructive pulmonary disease (COPD), mean EF was 61%, 62.9% had aortic aneurysm, 27.8% had aortic dissection, 51.6% had previous cardiac surgery, 25.8% had non-surgical aortic valve disease, and 69.5% had mild/moderate mitral valve regurgitation. Twenty-eight patients (28.8%) presented with aortic dissection, 60 patients (61.8%) had aortic aneurysm, 4 (4.1%) had intramural hematoma, and 5 (5.1%) had other presentations. An emergent procedure was performed in 6 (6.2%) patients, an urgent procedure in 37 (38.1%) patients and 54 (55.7%) patients had an elective procedure (Table 2).
3.2. Intra-operative and post-operative characteristics
Intraoperatively, mean time in the operating room (OR) was 4.3 hours, 16.5% had blood products use, 72.2% of patients were extubated in the OR (Table 2). In addition, 78.3% of patients had percutaneous TEVAR procedure, 5.1% had partial sternotomy and 10.3% had combined procedures including zone II debranching. There was no intraprocedural death. Postoperatively, mean intensive care unit (ICU) stay was 56.2 hours, mean hospital length of stay (LOS) was 6 days, 32% of patients had blood products use. Mean creatinine level was 1.1 µmol/L, mean creatinine clearance was 71.6, while 18.6% of patients needed prolonged ventilation (>24 hours). In-hospital complications included 7 cases (7.2%) of hospital mortality of whom 4 (4.12%) were due to cardiac arrest and 3 (3.1%) to cerebrovascular events, while there were no transient ischemic attack (TIA) events.
3.3. Patients Follow-up
At 8-year follow-up, overall survival was 76.3%. Incidence of MACCE was 25.8%, and 21.6% of patients had endoleaks (13 patients type II and 2 patients type 1) (Table 3, Figure 1 and Figure 2). Overall hospital readmission incidence was 60.8% while cardiac readmission was 26.8%. A time-sensitivity analysis showed that all-cause mortality, cardiac death, MACCE, stroke, MI, repeat intervention, and endoleaks incidence tend to increase at 1-, 2-, and 5-years follow-up (Table 4).
3.4. Emergent TEVAR procedure
Emergent TEVAR procedures (6 patients) had 1 (16.6%) in-hospital death, 1 (16.6%) CVA, 2 (33.3%) renal failures, and 2 (33.3%) 30-day cardiac readmissions (Supplemental Table S1). At 8-year follow-up, 4 (80%) of patients were alive, 2 (40%) had MACCE and 2 (40%) new endoleak not requiring reintervention (Supplemental Table S2). There were no reoperations, MI, or cardiac deaths events.
3.5. Urgent TEVAR procedure
Post-operative results of 37 (38.1%) patients included 5 (13.5%) in-hospital deaths, 1 (2.7%) (three due to cardiac arrests), 1 (2.7%) CVA episode, 1 (2.7%) deep sternal wound infection, and 4 (10.8%) renal failures of whom 3 (8.1%) requiring dialysis. Cardiac readmission rate was 29.7% (11 patients) (Supplemental Table S3). At 8-years follow-up, 28 (87.5%) of patients were alive, 13 (40%) had MACCE, 3 (9.3%) had a stroke episode, 2 (6.2%) experienced MI, and 4 (12.5%) had a cardiac related death. Repeat intervention occurred in 6 patients (18.7%) (Supplemental Table S4).
3.6. Aortic Dissection Presentation
Twenty-eight patients presented with an aortic dissection and underwent TEVAR procedure. Post-operatively, there were 2 (7.1%) CVA events, 2 (7.1%) in-hospital deaths, 1 (3.6%) ICU readmission, and 6 (21.4%) renal failures of whom 3 (10.7%) requiring dialysis. Hospital cardiac readmission rate was 25% (7 patients) (Supplemental Table S5). At 8-year follow-up, 21 (80.7%) of patients were alive, 5 (19.3%) experienced a MACCE episode, 1 (3.8%) had cardiac death, and 4 (15.4%) patients were diagnosed with a new endoleak of whom 1 (3.8%) had reoperation (Supplemental Table S6).
3.7. Aortic Aneurysm Presentation
Sixty patients presented with an aortic aneurysm and underwent TEVAR procedure. Postoperatively, there were 5 (8.3%) hospital deaths, 3 (5%) had renal failure of whom 2 (3.3%) necessitated dialysis. In addition, 4 (6.7%) had a cardiac arrest episode, 8 (13.3%) necessitated a prolonged ventilation period (>24 hours), and 9 (15%) had a new episode of post-operative atrial fibrillation (Supplemental Table S7). At 8-years follow-up, 45 (81.8%) patients were alive, 12 (21.8%) experienced a MACCE, 5 (9.1%) had a stroke episode, 7 (12.7%) had reoperation and 1 (1.8%) had a cardiac death (Supplemental Table S8).
3.8. Cox-regression analysis for analyses of periprocedural risk predictors that impact long-term prognosis
The Cox-regression analysis evidenced that risk predictors that impacted all-cause mortality included the presence of aortic valve regurgitation (HR 4.01 [1.56, 10.3], p = 0.004), COPD (HR 9.42 [3.47, 25.6], p < 0.001), presence of aortic valve stenosis (AVS) (HR 4.32 [1.27, 14.72], p = 0.019), and CBVD (HR 2.88 [1.09, 7.57], p = 0.032) (Table 5). Risk predictors that impact cardiac death are AVS (HR 7.95 [1.15, 54.89], p = 0.035) and COPD (HR 7.29 [1.37, 38.78], p = 0.02). Risk predictors that impact MACCE are AVS (HR 6.20 [1.98, 19.49], p=0.002), COPD (HR 3.27 [1.41, 7.57], p = 0.006), and CBVD (HR 2.73 [1.13, 6.62], p = 0.026). Risk predictors that impact MI are syncope (HR 38.57 [4.22, 352.11], p = 0.001) and cardiogenic shock (HR 22.42 [1.78, 282.64], p = 0.016). Risk predictor that impacts repeat intervention is prior mediastinal radiation (HR 8.88 [1.76, 44.7], p = 0.008). Risk predictor that impacts the presence of endoleaks is aortic valve disease (HR 3.29 [1.39, 7.79], p = 0.007).
4. Discussion
The main findings of the study are: (1) at follow-up, overall survival was 76.3% while incidence of MACCE was 25.8%; (2) a total of 21.6% of patients had endoleaks (13 patients type II and 2 patients type I); (3) periprocedural risk predictors impacting long-term all-cause death included COPD, aortic valve disease, and CBVD; (4) the risk of all-cause death and other long-term complications progressively increases at 1-, 2-, and 5-years follow-up.
This 8-year follow-up analysis provided several novel insights in the fragile TEVAR population. Firstly, overall death and MACCE in patients undergoing TEVAR is high and remains high at 1-, 2-, and 5-years follow-up. Secondly, new risk predictors, including COPD and aortic valve disease, appears associated with long-term prognosis after TEVAR.
4.1. All-cause mortality
In our experience of patients undergoing TEVAR, post-operative incidence of all-cause mortality shows that nonetheless being minimally invasive, TEVAR remain a major procedure a bearing significant all-cause mortality. In this context, mortality is influenced by patient selection, as almost 54% of patients present as emergent procedures according to the American Society of Anesthesiologists [11]. In our study, incidence of urgent procedures was 38% and that of emergent procedures was 6%, which can partially explain the high mortality observed. However, given the small numbers of patients included in our study its definitive conclusions cannot be asserted.
4.2. Neurological Outcomes
Neurologic morbidity in our study is similar to previously reported outcomes [12]. CBVD occurred during the perioperative period for 3% of patients. Literature showed similar results (2.0% to 9.3%) [12,13,14,15,16,17,18,19,20,21,22]. Moreover, international medical literature shows an overall incidence of TIA between 11.5-13% on the long-term follow-up. These results are similar to our single center TEVAR experience with an overall incidence of 12/97 (12%) [22].
4.3. Predictors Impacting Long-term Prognosis
Predictors of long-term prognosis in patients undergoing TEVAR included COPD and aortic valve disease. In this context, we hypothesize that pre-operative medical optimization of COPD patients undergoing TEVAR procedure may improve long-term prognosis. A recent single center retrospective study showed similar incidence of stroke and COPD and diabetes were shown to be risk predictors for stroke [22,23]. Interestingly, the study reported that left subclavian procedural access is a risk predictor for stroke. Unfortunately, this variable was absent in our analysis as we performed the procedure only through femoral access.
4.4. Incidence of Endoleaks
The incidence of endoleaks at follow-up after TEVAR remains a major hurdle often requiring repeats intervention [24]. A recent single center German study reported an incidence of type II endoleak of 8.7% while indications for repeat intervention were diameter expansion and extensive leakage [25]. Our study found a higher incidence (6.5%) of endoleak type II at follow-up. The presence of aortic valve disease was found to increase the incidence of endoleaks at follow-up. Other studies reported that stent-graft diameter ≥40 mm and excessively oversized (≥14%) stent-grafts increase the probability of observing endoleaks at follow-up [26,27,28,29,30].
Given the apparent adequacy of our study analysis (with minimal standardized mean differences) based on elements available in claims data, it is likely that patients undergoing TEVAR may benefit from these outcomes.
This retrospective study was subject to all limitations inherent to a non-randomized study, including potential selection bias regarding which patients underwent TEVAR procedure. In addition, the study includes a large timeframe (2014-2022) and many advanced techniques and changes in medical treatments have occurred in this period. Another limitation is the single-center data therefore, our analysis requires further validation from multicenter studies.
5. Conclusions
Patients undergoing TEVAR have a survival rate of almost 80% at 8-year follow-up. Nonetheless almost half of the patients underwent an urgent/emergent procedure, clinical results were favourable for TEVAR.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, A.D. and G.T.; analysis, R.M.; investigation, S.S. and R.R.; data curation, D.V.; writing—original draft preparation, B.B. and F.C.; writing—review and editing, A.U. and H.H.; supervision, R.B. and M.B. All authors have read and agreed to the published version of the manuscript.
Funding
This manuscript received funding from Sharpe-Strumia Research Foundation of Bryn Mawr Hospital, Wynnewood, Pennsylvania, USA. Grant Number (SSRF2022-10).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the by the Main Line Health Hospitals Institutional Review Board (IRB 45CFR164.512).
Informed Consent Statement
Informed consent was collected according to IRB.
Data Availability Statement
The data that support the findings of this study are available upon reasonable request to Dr. Sicouri pending institutional approval.
Acknowledgments
none.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Weissler, E.H.; Osazuwa-Peters, O.L.; Greiner, M.A.; Hardy, N.C.; Kougias, P.; O’brien, S.M.; Mark, D.B.; Jones, W.S.; Secemsky, E.A.; Vekstein, A.M.; et al. Initial Thoracic Endovascular Aortic Repair vs Medical Therapy for Acute Uncomplicated Type B Aortic Dissection. JAMA Cardiol. 2023, 8, 44–53. [Google Scholar] [CrossRef]
- Patel, R.; Sweeting, M.J.; Powell, J.T.; Greenhalgh, R.M. Endovascular versus open repair of abdominal aortic aneurysm in 15-years’ follow-up of the UK endovascular aneurysm repair trial 1 (EVAR trial 1): a randomised controlled trial. Lancet 2016, 388, 2366–2374. [Google Scholar] [CrossRef] [PubMed]
- Anaya-Ayala, J.E.; Cheema, Z.F.; Davies, M.G.; et al. Hybrid thoracic endovascular aortic repair via right anterior minithoracotomy. J Thorac Cardiovasc Surg. 2011, 142, 314–8. [Google Scholar] [CrossRef] [PubMed]
- El-Sayed, H.; Ramlawi, B. The current status of endovascular repair of thoracic aortic aneurysms (TEVAR). Methodist Debakey Cardiovasc J. 2011, 7, 15–9. [Google Scholar] [CrossRef] [PubMed]
- Ramlawi, B.; Reardon, M.J. Aortic arch debranching: advanced and hybrid techniques. Methodist Debakey Cardiovasc J. 2011, 7, 43–7. [Google Scholar] [CrossRef]
- Leurs, L.J.; Bell, R.; Degrieck, Y.; Thomas, S.; Hobo, R.; Lundbom, J. Endovascular treatment of thoracic aortic diseases: Combined experience from the EUROSTAR and United Kingdom Thoracic Endograft registries. J. Vasc. Surg. 2004, 40, 670–679. [Google Scholar] [CrossRef]
- Bonacchi, M.; Cabrucci, F.; Bacchi, B.; Haranal, M.; Gelsomino, S.; Ramlawi, B.; Dokollari, A. Editorial: Novel insights into aortic arch repair. Front. Cardiovasc. Med. 2022, 9, 1087952. [Google Scholar] [CrossRef]
- Dokollari, A.; Bisleri, G. Watchful waiting during visceral malperfusion in DeBakey type I aortic dissection: A possible paradigm shift? JTCVS Tech. 2020, 4, 81–82. [Google Scholar] [CrossRef]
- Coselli, J.S.; Rosu, C.; Amarasekara, H.S.; Green, S.Y.; Zhang, Q.; Price, M.D.; LeMaire, S.A. Reoperative surgery on the thoracoabdominal aorta. J. Thorac. Cardiovasc. Surg. 2018, 155, 474–485. [Google Scholar] [CrossRef]
- Augoustides, J.; Mz, T.; Mj, E.; Ee, R.; Eh, B.; F, X.; M, I. ; Johnston; Eg, S. ; Fg, B.; et al. Faculty Opinions recommendation of Outcomes of open versus endovascular repair of descending thoracic and thoracoabdominal aortic aneurysms. 2021. [Google Scholar] [CrossRef]
- Braconi, L.; Cabrucci, F.; Bacchi, B.; Bonacchi, M. A threatening meteor for cardiac surgeons: anomalous left main coronary origin in type A aortic dissection. Eur. J. Cardio-Thoracic Surg. 2022, 62. [Google Scholar] [CrossRef] [PubMed]
- Isselbacher, E.M.; Preventza, O.; Hamilton Black, J., 3rd; et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022, 146, e334–e482. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, J.S.; Cambria, R.P.; Dake, M.D.; Moore, R.D.; Svensson, L.G.; Snyder, S. International controlled clinical trial of thoracic endovascular aneurysm repair with the Zenith TX2 endovascular graft: 1-year results. J. Vasc. Surg. 2008, 47, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.A.; Daniels, M.J.; Beaver, T.M.; Klodell, C.T.; Raghinaru, D.E.; Hess, P.J. Late Outcomes of a Single-Center Experience of 400 Consecutive Thoracic Endovascular Aortic Repairs. Circulation 2011, 123, 2938–2945. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, J.A.; Olsen, D.M.; Shtutman, A.; Lucas, L.A.; Wheatley, G.; Alpern, J.; Ramaiah, V.; Diethrich, E.B. Application of endograft to treat thoracic aortic pathologies: A single center experience. J. Vasc. Surg. 2007, 46, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Riambau, V.; Zipfel, B.; Coppi, G.; Czerny, M.; Tealdi, D.G.; Ferro, C.; Chiesa, R.; Sassi, C.; Rousseau, H.; Berti, S. Final operative and midterm results of the European experience in the RELAY Endovascular Registry for Thoracic Disease (RESTORE) study. J. Vasc. Surg. 2011, 53, 565–573. [Google Scholar] [CrossRef]
- Fillinger, M.F.; Greenberg, R.K.; McKinsey, J.F.; Chaikof, E.L. Reporting standards for thoracic endovascular aortic repair (TEVAR). J. Vasc. Surg. 2010, 52, 1022–1033. [Google Scholar] [CrossRef]
- Alric, P.; Canaud, L.; Branchereau, P.; Marty-Anne, C. Traitement endovasculaire des anevrysmes de l’aorte thoracique descendante. EMC Techniques chirurgicales – Chirurgie vasculaire. 2012, 7, 1–20. [Google Scholar] [CrossRef]
- Dokollari, A.; Cameli, M.; Wang, L.; Bisleri, G. Aortic intimo-intimal intussusception in Stanford type A acute aortic dissection. Eur. Hear. J. 2020, 42, 3410–3410. [Google Scholar] [CrossRef]
- Bonacchi, M.; Dokollari, A.; Parise, O.; Sani, G.; Prifti, E.; Bisleri, G.; Gelsomino, S. Ministernotomy compared with right anterior minithoracotomy for aortic valve surgery. J. Thorac. Cardiovasc. Surg. 2021, 165, 1022–1032. [Google Scholar] [CrossRef]
- Dokollari, A.; Cameli, M.; Mandoli, G.E.; Kalra, D.-K.S.; Poston, R.; Coku, L.; Pernoci, M.; Miri, M.; Bonacchi, M.; Gelsomino, S. Early and Midterm Clinical Outcomes of Transcatheter Valve-in-Valve Implantation Versus Redo Surgical Aortic Valve Replacement for Aortic Bioprosthetic Valve Degeneration: Two Faces of the Same Medal. J. Cardiothorac. Vasc. Anesthesia 2021, 35, 3223–3231. [Google Scholar] [CrossRef]
- Tsilimparis, N.; Stana, J.; Konstantinou, N.; Chen, M.; Zhou, Q.; Kölbel, T. Identifying risk factors for early neurological outcomes following thoracic endovascular aortic repair using the SUMMIT database. Eur. J. Cardio-Thoracic Surg. 2021, 62. [Google Scholar] [CrossRef]
- Zha, Z.; Pan, Y.; Zheng, Z.; Wei, X. Prognosis and Risk Factors of Stroke After Thoracic Endovascular Aortic Repair for Stanford Type B Aortic Dissection. Front. Cardiovasc. Med. 2022, 8, 787038. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.; Corriere, M.A.; Veeraswamy, R.K.; Kasirajan, K.; Milner, R.; Dodson, T.F.; Salam, A.A.; Chaikof, E.L. Risk factors for late mortality after endovascular repair of the thoracic aorta. J. Vasc. Surg. 2010, 52, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Morales, J.P.; Greenberg, R.K.; Lu, Q.; Cury, M.; Hernandez, A.V.; Mohabbat, W.; Moon, M.C.; Morales, C.A.; Bathurst, S.; Schoenhagen, P. Endoleaks Following Endovascular Repair of Thoracic Aortic Aneurysm: Etiology and Outcomes. J. Endovasc. Ther. 2008, 15, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, M.S.; Geisbüsch, P.; Kotelis, D.; Müller-Eschner, M.; Hyhlik-Dürr, A.; Böckler, D. Clinical significance of type II endoleaks after thoracic endovascular aortic repair. J. Vasc. Surg. 2013, 58, 643–650. [Google Scholar] [CrossRef]
- Kanaoka, Y.; Ohki, T.; Maeda, K.; Baba, T. Analysis of Risk Factors for Early Type I Endoleaks After Thoracic Endovascular Aneurysm Repair. J. Endovasc. Ther. 2016, 24, 89–96. [Google Scholar] [CrossRef]
- Bonacchi, M.; Prifti, E.; Giunti, G.; Frati, G.; Sani, G. Does ministernotomy improve postoperative outcome in aortic valve operation? A prospective randomized study. Ann. Thorac. Surg. 2002, 73, 460–465. [Google Scholar] [CrossRef]
- Prifti E, Bonacchi M, Frati G, et al. Early and long-term outcome in patients undergoing aortic root replacement with composite graft according to the Bentall’s technique. Eur J Cardiothorac Surg. 2002, 21, 15–21. [Google Scholar] [CrossRef]
- De Jong, M.M.; Lorusso, R.; Al Awami, F.; Matteuci, F.; Parise, O.; Lozekoot, P.; Bonacchi, M.; Maessen, J.G.; Johnson, D.M.; Gelsomino, S. Vascular complications following intra-aortic balloon pump implantation: an updated review. Perfusion 2017, 33, 96–104. [Google Scholar] [CrossRef]
- Seike, Y.; Matsuda, H.; Shimizu, H.; Ishimaru, S.; Hoshina, K.; Michihata, N.; Yasunaga, H.; Komori, K. ; on behalf of the Japanese Committee for Stentgraft Management (JACSM)* Nationwide Analysis of Persistent Type II Endoleak and Late Outcomes of Endovascular Abdominal Aortic Aneurysm Repair in Japan: A Propensity-Matched Analysis. Circulation 2022, 145, 1056–1066. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Kaplan–Meier Survival Curves. (A)—Survival; (B)—MACCE; (C)—Stroke; (D)—MI; (E)—Stroke; (F)—Endoleaks.
Figure 1.
Kaplan–Meier Survival Curves. (A)—Survival; (B)—MACCE; (C)—Stroke; (D)—MI; (E)—Stroke; (F)—Endoleaks.
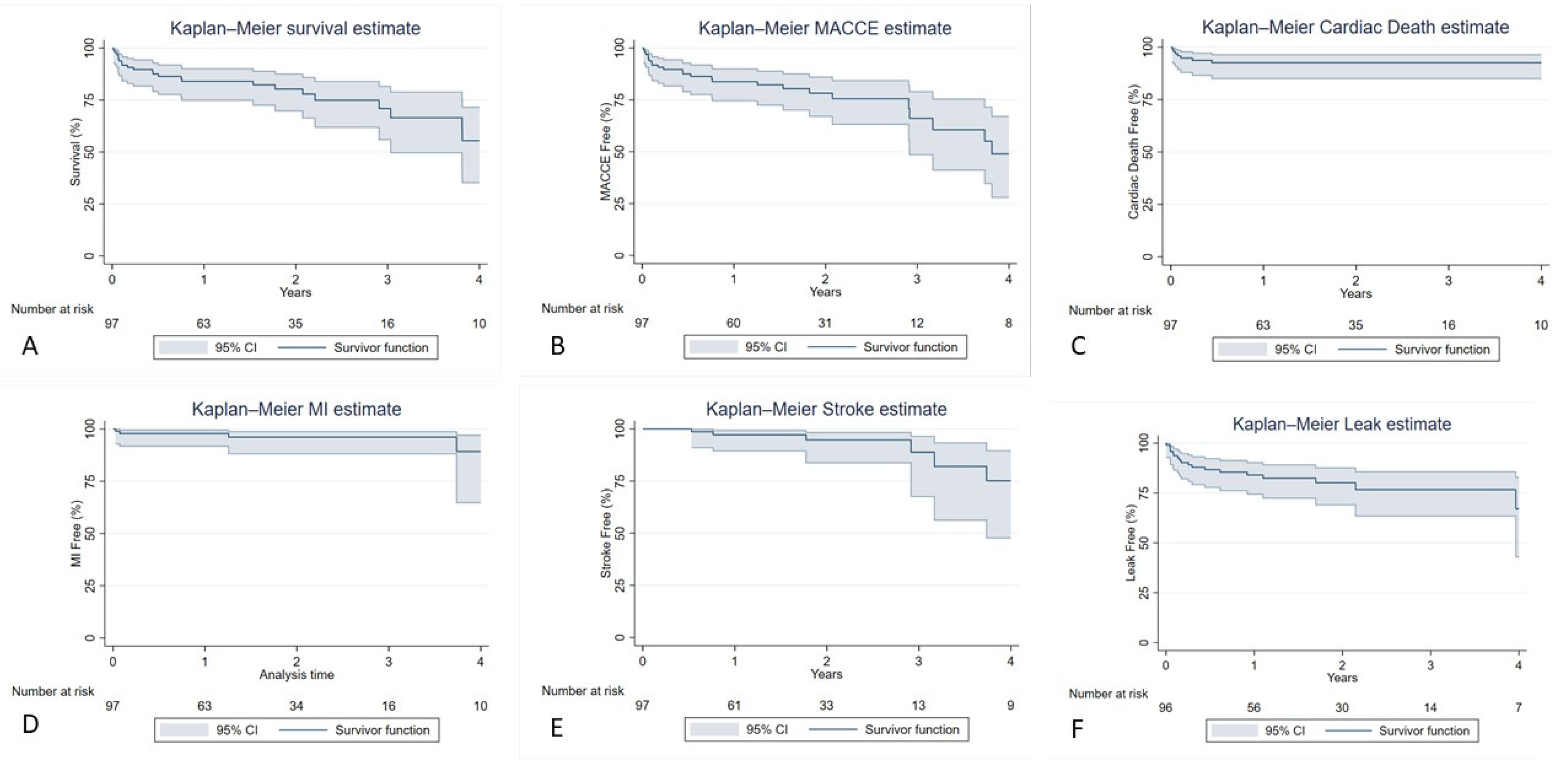
Figure 2.
Kaplan–Meier Survival Curve. A-Repeat Intervention.
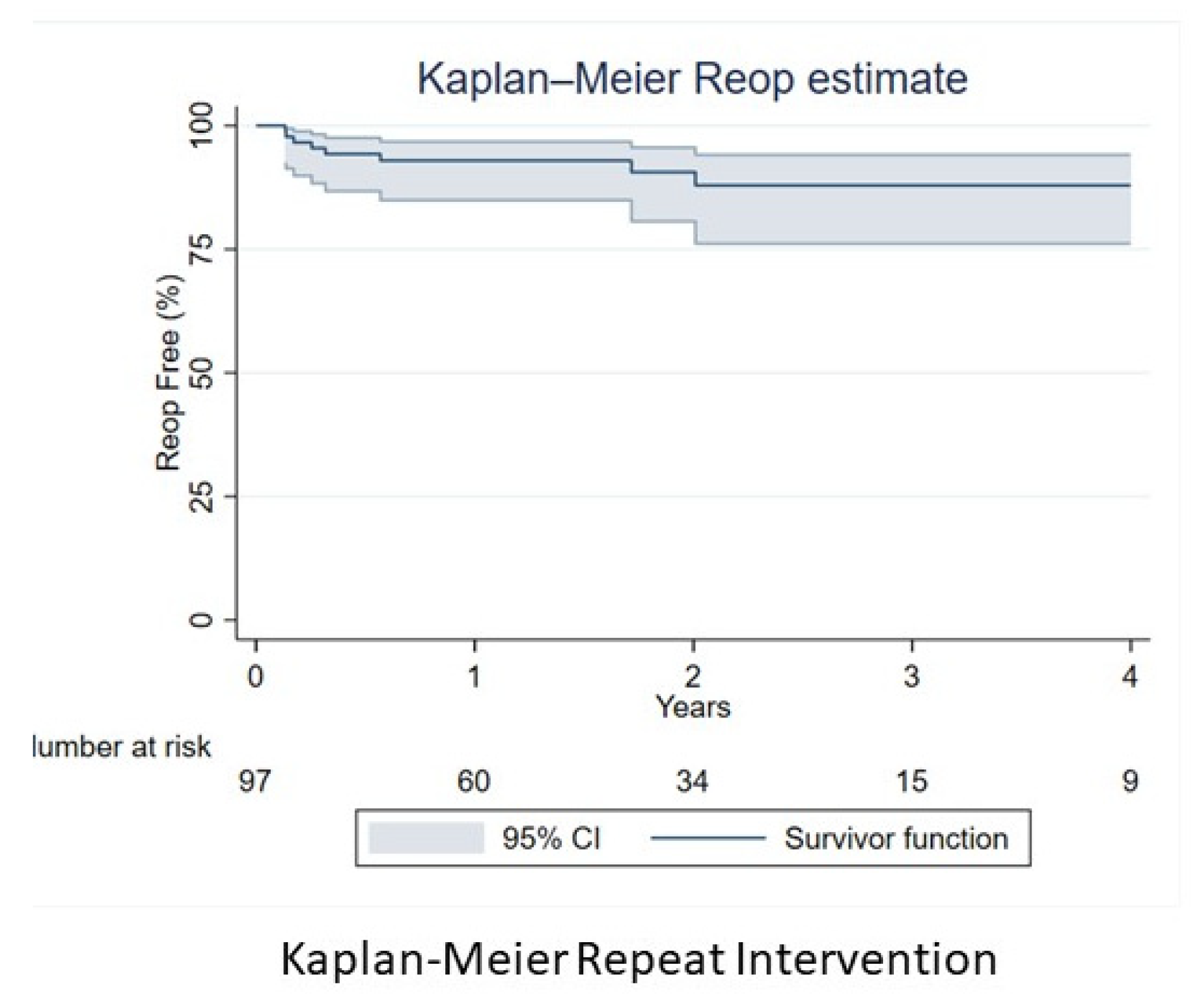

Table 1.
Pre-operative Patients Characteristics. EF—ejection fraction; BMI—body mass index; INR—international rationalized ration; COPD—chronic obstructive pulmonary disease; PVD—peripheral vascular disease; PCI—percutaneous coronary disease; CABG—coronary artery bypass grafting; AICD—automatic implantable cardioverter defibrillator; MI—myocardial infarction; TIA—transient ischemic attack.
Table 1.
Pre-operative Patients Characteristics. EF—ejection fraction; BMI—body mass index; INR—international rationalized ration; COPD—chronic obstructive pulmonary disease; PVD—peripheral vascular disease; PCI—percutaneous coronary disease; CABG—coronary artery bypass grafting; AICD—automatic implantable cardioverter defibrillator; MI—myocardial infarction; TIA—transient ischemic attack.
| Pre-operative Patients Characteristics | Patients n = 97 |
|---|---|
| Male n (%) | 48 (49.5%) |
| Female n (%) | 49 (50.5%) |
| White n (%) | 57 (59.4%) |
| Non-White n (%) | 39 (40.6%) |
| Age Years (Mean/SD) | 70.4 (13.5) |
| BMI kg/m² (Mean/SD) | 28.6 (5.5) |
| Obese ≥25 kg/m² n (%) | 30 (30.9%) |
| EF (Mean/SD) | 61.1 (9.9) |
| EF<50% n (%) | 8 (8.2%) |
| Creatinine level (Median/IQR) | 1.1 (0.9-1.3) |
| Creatinine Clearance (Mean/SD) | 71.6 (34.2) |
| Creatinine Clearance <60 (Yes) n (%) | 36 (37.1%) |
| INR (Median/IQR) | 1.1 (1-1.2) |
| Hemoglobin level (Median/IQR) | 11.7 (10.1-12.9) |
| Dialysis n (%) | 4 (4.2%) |
| Diabetes n (%) | 17 (17.1%) |
| Smoking n (%) | 65 (67.7%) |
| COPD n (%) | 26 (27.1%) |
| Hypertension n (%) | 84 (87.5%) |
| Dyslipidemia n (%) | 24 (24.7%) |
| Pneumonia n (%) | 4 (4.3%) |
| Cerebrovascular Disease n (%) | 22 (23.2%) |
| PVD n (%) | 39 (40.6%) |
| Endocarditis n (%) | 1 (1.0%) |
| Immunocompromise n (%) | 5 (5.2%) |
| Home O2 therapy n (%) | 4 (4.2%) |
| Cancer (within 5 years) n (%) | 8 (8.6%) |
| Aortic Aneurysm n (%) | 61 (62.9%) |
| Aortic Dissection n (%) | 27 (27.8%) |
| Aortic Other n (%) | 7 (7.22%) |
| Previous Mediastinal Radiation n (%) | 2 (2.1%) |
| Prior PCI n (%) | 11 (11.3%) |
| Syncope n (%) | 3 (3.1%) |
| Previous Cardiac Surgery n (%) | 49 (51.6%) |
| Prior CABG n (%) | 7 (7.2%) |
| Prior Valve Surgery n (%) | 18 (18.6%) |
| Prior Aortic Valve replacement n (%) | 8 (8.5%) |
| Prior Aortic Valve repair n (%) | 12 (12.8%) |
| Prior AICD Implantation n (%) | 3 (3.2%) |
| Preoperative Arrhythmia n (%) | 18 (18.6%) |
| Atrial Fibrillation n (%) | 12 (12.8%) |
| Paced Rhythm n (%) | 4 (4.3%) |
| MI n (%) | 11 (11.6%) |
| TIA n (%) | 9 (9.3%) |
| Cardiogenic Shock n (%) | 2 (2.1%) |
| Heart Failure n (%) | 21 (21.9%) |
| Coronary Artery Disease n (%) | 22 (22.7%) |
| Internal Mammary Artery use n (%) | 4 (4.3%) |
| Aortic Valve Disease n (%) | 25 (25.8%) |
| Aortic Valve Regurgitation n (%) | 35 (36.1%) |
| Aortic Valve Stenosis n (%) | 6 (6.2%) |
| Mitral Valve Stenosis n (%) | 3 (3.1%) |
| Mitral Valve Regurgitation n (%) | 66 (69.5%) |
| Tricuspid Valve Regurgitation n (%) | 76 (80.0%) |
| Aortic Aneurysm Etiology n (%) | 60 (61.8%) |
| Aortic Dissection Etiology n (%) | 28 (28.8%) |
| Intramural Hematoma Etiology n (%) | 4 (4.1%) |
| Other Etiology n (%) | 5 (5.1%) |
Table 2.
Intra-operative characteristics and post-operative outcomes. RBC—red blood cells; CPB—cardiopulmonary bypass; FFP—fresh frozen plasma; ICU—intensive care unit; LOS-length of stay.
Table 2.
Intra-operative characteristics and post-operative outcomes. RBC—red blood cells; CPB—cardiopulmonary bypass; FFP—fresh frozen plasma; ICU—intensive care unit; LOS-length of stay.
| Variables | Patients n = 97 |
|---|---|
| Intra-operative | |
| Time in OR (Hours) Mean/SD | 4.3 (2.8) |
| Blood Products Used n (%) | 16 (16.5%) |
| RBC Units n (%) | 16 (16.5%) |
| Cryoprecipitate Units n (%) | 6 (6.2%) |
| Platelet Units n (%) | 8 (8.3%) |
| FFP Units n (%) | 6 (6.2%) |
| Cross Clamp Time (Median/IQR) | 87 (76-145) |
| CBP utilization n (%) | 8 (8.2%) |
| CBP time (Median/IQR) | 172 (119-178) |
| Extubated in OR n (%) | 70 (72.2%) |
| Elective n (%) | 54 (55.7%) |
| Emergent n (%) | 6 (6.2%) |
| Urgent n (%) | 37 (38.1%) |
| Percutaneous n (%) | 76 (78.3%) |
| Partial Sternotomy n (%) | 5 (5.1%) |
| Combined Procedure | 10 (10.3%) |
| Other | 6 (6.2%) |
| Post-operative | |
| Total ICU (Hours) (Median/IQR) | 56.2 (28.3-114.5) |
| Total LOS (Days) (Median/IQR) | 6 (4-10) |
| Blood Products Used n (%) | 31 (32.0%) |
| RBC Units n (%) | 28 (29.2%) |
| Cryoprecipitate Units n (%) | 2 (2.1%) |
| Platelet Units n (%) | 7 (7.2%) |
| FFP Units n (%) | 5 (5.2%) |
| Creatine level (Median/IQR) | 1.1 (0.9-1.7) |
| Creatinine Clearance (mean/SD) | 63.1 (32.8) |
| Creatinine Clearance < 60 ml/min n (%) | 46 (47.4%) |
| Reoperation for Bleeding n (%) | 3 (3.1%) |
| Prolonged Ventilation >24 hours n (%) | 18 (18.6%) |
| Superficial Infection n (%) | 2 (2.1%) |
| Deep Sternal Infection n (%) | 3 (3.1%) |
| Cerebrovascular Accident n (%) | 3 (3.1%) |
| TIA n (%) | 0 (0.0%) |
| Cardiac Arrest n (%) | 4 (4.12%) |
| Renal Failure n (%) | 9 (9.3%) |
| Dialysis n (%) | 6 (6.2%) |
| New Atrial Fibrillation n (%) | 12 (12.4%) |
| ICU Readmission n (%) | 4 (4.1%) |
| Operative Mortality n (%) | 6 (6.2%) |
| In-hospital Mortality n (%) | 7 (7.2%) |
| Readmission n (%) | 59 (60.8%) |
| Cardiac Readmission n (%) | 26 (26.8%) |
Table 3.
Long-term Outcomes. MI—myocardial infarction.
| Follow-up Outcomes | Patients n = 97 |
|---|---|
| Survival (all cause) | |
| Yes n (%) | 74 (76.3%) |
| No n (%) | 23 (23.7%) |
| MACCE n (%) | 25 (25.8%) |
| Stroke n (%) | 6 (6.2%) |
| MI n (%) | 4 (4.1%) |
| Reoperation n (%) | 10 (10.3%) |
| Cardiac Death n (%) | 7 (7.2%) |
| Presence of endoleak n (%) | 21 (21.6%) |
Table 4.
Time-sensitivity analysis of follow-up outcomes. MI- myocardial infarction.
| Variables | Patients n = 97 |
|---|---|
| All-Cause Mortality | |
| 1 year | 15 (15.5%) |
| 2 years | 17 (17.5%) |
| 5 years | 23 (23.7%) |
| MACCE | |
| 1 year | 15 (15.5%) |
| 2 years | 18 (18.6%) |
| 5 years | 24 (24.7%) |
| Stroke | |
| 1 year | 2 (2.1%) |
| 2 years | 3 (3.1%) |
| 5 years | 6 (6.2%) |
| MI | |
| 1 year | 2 (2.1%) |
| 2 years | 3 (3.1%) |
| 5 years | 4 (4.1%) |
| Reoperation | |
| 1 year | 6 (6.2%) |
| 2 years | 7 (7.2%) |
| 5 years | 8 (8.2%) |
| Cardiac Death | |
| 1 year | 7 (7.2%) |
| 2 years | 7 (7.2%) |
| 5 years | 7 (7.2%) |
| All-type Endoleak | |
| 1 year | 15 (15.5%) |
| 2 years | 17 (17.5%) |
| 5 years | 19 (19.6%) |
Table 5.
Risk factors impacting long-term prognosis. COPD-chronic obstructive pulmonary disease; CBVD-cerebrovascular disease; MI-myocardial infarction; EF- ejection fraction.
Table 5.
Risk factors impacting long-term prognosis. COPD-chronic obstructive pulmonary disease; CBVD-cerebrovascular disease; MI-myocardial infarction; EF- ejection fraction.
| All-Cause Mortality | HR (95% CI) | p-value |
|---|---|---|
| Aortic valve regurgitation | 4.01 (1.56, 10.3) | 0.004 |
| COPD | 9.42 (3.47, 25.6) | <0.001 |
| Aortic valve stenosis | 4.32 (1.27, 14.72) | 0.019 |
| CBVD | 2.88 (1.09, 7.57) | 0.032 |
| Cardiac Death | HR (95% CI) | p-value |
| Aortic valve stenosis | 7.95 (1.15, 54.89) | 0.035 |
| COPD | 7.29 (1.37, 38.78) | 0.02 |
| MACCE | HR (95% CI) | p-value |
| Aortic valve stenosis | 6.20 (1.98, 19.49) | 0.002 |
| COPD | 3.27 (1.41,7.57) | 0.006 |
| CBVD | 2.73 (1.13, 6.62) | 0.026 |
| STROKE | HR (95% CI) | p-value |
| EF | 0.95 (0.91, 0.99) | 0.043 |
| MI | HR (95% CI) | p-value |
| Syncope | 38.57 (4.22, 352.11) | 0.001 |
| Cardiogenic Shock | 22.42 (1.78, 282.64) | 0.016 |
| Reoperation | HR (95% CI) | p-value |
| Prior Mediastinal Radiation | 8.88 (1.76, 44.7) | 0.008 |
| Endoleak Leak | HR (95% CI) | p-value |
| Aortic valve disease | 3.29 (1.39, 7.79) | 0.007 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



