
Submitted:
16 August 2023
Posted:
17 August 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Bacteremia and fungemia are significant causes of morbidity and mortality which frequently occur as co-infections with viral respiratory infections including SARS-CoV-2. It was aimed to evaluate the microorganisms isolated from blood cultures of SARS-CoV-2 positive and negative patients and investigate their antimicrobial resistance patterns. A retrospective analysis was performed with the total number of 22,944 blood cultures sent to the laboratory between November 2020 and December 2021. Blood cultures were performed on the BD Bactec automated system. Identification was performed using conventional methods, VITEK-2 and MALDI-TOF MS. Antibacterial/antifungal susceptibility tests were performed according to EUCAST/CLSI recommendations. SARS-CoV-2 tests were performed with RT-PCR. It was detected 1,630 culture positivity belonging to 652 patients. Totally 633 of 652 patients were tested for SARS-CoV-2; 118 (18.6%) were positive and 515 (81.3%) were negative. The bacteria and fungi isolated at the high-est rate in SARS-CoV-2 positive patients were methicillin-resistant coagulase negative staphylococci (MR-CoNS) (21.5%), Escherichia coli (12.4%), Klebsiella pneumoniae (12.4%), Candida albicans (1.65%) and Candida glabrata complex (1.65%); while in negative patients, E. coli (21.3%), MR-CoNS (13.5%), K. pneumoniae (12.05%), C. albicans (2.1%), Candida parapsilosis (1.1%) and Candida tropicalis (0.9%). The fact that the most common isolate was MR-CoNS in SARS-CoV-2 positive patients (p = 0.028); the detection of Acinetobacter baumannii was more frequent (p = 0.001) and the isolation of carbapenem-resistant K. pneumoniae was at a higher rate than in SARS-CoV-2 negative patients; also, the increase in multidrug-resistant strains indicate that healthcare-associated infec-tions should not be disregarded while focusing on the outbreak.
Keywords:
blood culture
; SARS-CoV-2
; COVID-19
; co-infection
; antimicrobial resistance
1. Introduction
Bacteremia and fungemia, which frequently occur as co-infections during viral respiratory tract infections including SARS-CoV-2, are significant causes of morbidity and mortality. These co-infections may be healthcare-associated due to prolonged hospitalization and intensive care requirements [1]. Data show that these culture-proven infections occur in 4-15% of hospitalized COVID-19 patients and are significantly associated with mortality [2]. Pathogens often display a multidrug-resistant phenotype such as carbapenem-resistant Enterobacterales (CRE) and this can cause problems in the antimicrobial treatment processes [2].
SARS-CoV-2 infection can also occur as a co-infection secondary to bacterial infection or bacterial super-infection may develop secondary to SARS-CoV-2 infection, depending on the host, virus, and bacterial factors. Bloodstream infections (BSIs) in COVID-19 patients may be associated with systemic dissemination of co-pathogens caused by SARS-CoV-2- induced tissue destruction [3].
In patients with severe febrile illness, blood cultures are still essential for ruling out bacterial/fungal infections. However, there are a few data on the prevalence of bacterial and fungal agents causing BSI in patients infected with SARS-CoV-2 [4,5]. Also, it is important to evaluate these infections to guide appropriate empirical antimicrobial treatment at the time of presentation [4]. In these patients, despite little evidence of a bacterial cause of infection, there is overwhelmingly prescribed empirical antimicrobial treatments. So, determination of the prevalence of bacterial co-infections and the susceptibility results are likely to provide important information regarding the need for and choice of antibiotics.
The aim of the study is to evaluate the microorganisms isolated from blood cultures of SARS-CoV-2 positive and negative patients, investigate their antimicrobial resistance patterns and to compare the findings of these two patient groups by determining the rates of bacteremia and fungemia.
2. Materials and Methods
2.1. Study population
A retrospective analysis was performed with a total of 22,944 blood cultures sent to the laboratory between November 2020 and December 2021. When defining BSI, if a species belonging to the skin flora was found among the isolated microorganisms, it was considered that the same species should be recovered in at least two blood cultures collected from the same patient within 24 hours, according to Centers for Disease Control and Prevention (CDC) criteria [6]. The growth of these microorganisms in a single blood culture within 24 hours was considered as contamination except in the neonatal period [7].
2.2. Blood culture
Blood cultures were performed on the BD Bactec FX (Becton Dickinson, USA) automated system and cultures were incubated for up to five days. Under special circumstances (for Brucella spp., etc.) cultures were incubated longer than standard procedure. All positive blood cultures were subcultured to 5% Columbia sheep blood agar (Becton Dickinson, USA) and incubated at 35-37 0C under 5-10% CO2 atmosphere for 48 h. Anaerobic positive blood cultures were subcultured additionally to anaerobic media and incubated at 35-37 0C under anaerobic atmosphere for 48 h. If there was no growth on initial media, the blood cultures were subcultured onto chocolate agar (incubated at 35-37 0C under 5-10% CO2 atmosphere for 48 h) for the isolation of fastidious microorganisms and blood agar (incubated microaerobically at 35-37 0C for 48 h) for Campylobacter species.
2.2.1. Identification of bacterial and fungal isolates
Bacterial identification was performed using conventional methods and/or VITEK-2 Compact system (bioMérieux, France). Fungi isolated from Myco F or aerobic bottles were identified by morphological examination on cornmeal agar with Tween 80 and API ID 32C (bioMérieux, France). Additionally, MALDI-TOF MS (bioMérieux, France) was used to confirm the rare bacterial isolates and/or fungi that could not be identified by other methods.
2.2.2. Antimicrobial Susceptibility Testing
Antibacterial susceptibilities of the isolates were investigated by standard Kirby-Bauer disk diffusion method and VITEK-2 Compact system (bioMérieux, France) when necessary. Antifungal susceptibility was tested with the gradient test method using Roswell Park Memorial Institute medium (RPMI-1640) (Sigma-Aldrich, USA) in order to detect minimum inhibitory concentrations (MICs). Antibacterial and antifungal susceptibility tests were carried out and evaluated in accordance with EUCAST/CLSI criteria [8-11]. ‘’Intermediate (I): susceptible, increased exposure’’ strains of bacteria were considered as susceptible. Since there are no clinical breakpoints for Candida auris, the MICs were evaluated according to the tentative breakpoints determined by CDC [12].
2.3. Patients' COVID-19 diagnoses
COVID-19 status was confirmed by SARS-CoV-2 real-time polymerase chain reaction (RT-PCR) test positivity in nasopharyngeal and oral swabs.
2.4. Statistical Analysis
SPSS 15.0 for Windows was used for statistical analysis. Descriptive statistics were given as numbers and percentages for categorical variables. Proportions were compared with the chi-square (χ²) test in independent groups. The statistical alpha significance level was considered as p < 0.05.
2.5. Ethical Approval
The research was approved by University of Health Sciences İstanbul Training and Research Hospital Ethics Committee (protocol code: 63 and date of approval:11.02.2022).
3. Results
In a total of 22,944 blood cultures, 1,630 culture positivity belonging to 652 patients were detected. Of the 652 patients (321 outpatients and 331 inpatients), 633 were tested for SARS-CoV-2; 118 were positive (18.6%; 45 females, 73 males; mean age: 62.7 years) and 515 were negative (81.3%; 247 females, 268 males; mean age: 61.7 years).
SARS-CoV-2 positive (38 of 118 patients) and SARS-CoV-2 negative (243 of 515 patients) patients were most frequently internal medicine outpatients. The distribution of clinics and intensive care units (ICU) where the blood samples were collected is given in the Table 1.
A total of 671 pathogens were isolated from the patients. Of these, 252 were fermentative Gram-negative rods, 66 were non-fermentative Gram-negative rods, 300 were Gram-positive cocci, three were Gram-positive rods, seven were anaerobic bacteria, and five were other bacterial species [Listeria monocytogenes (n:2), Campylobacter coli (n:1), Campylobacter jejuni (n:1), and Moraxella nonliquefaciens (n:1)], totaling 633 bacteria (94.3%). Fungi were isolated from the blood cultures of 38 (5.7%) patients. The isolated microorganisms and their antimicrobial resistance patterns are shown in Table 2 and Table 3 and Figure 1.
The microorganisms isolated at the highest rate in SARS-CoV-2 positive patients were methicillin-resistant coagulase negative staphylococci (MR-CoNS) (21.5%), Escherichia coli (12.4%), Klebsiella pneumoniae (12.4%), Candida albicans (1.65%) and Candida glabrata complex (1.65%); while in negative patients E. coli (21.3%), MR-CoNS (13.5%), K. pneumoniae (12.05%), C. albicans (2.1%), Candida parapsilosis (1.1%) and Candida tropicalis (0.9%). Cultures from 15 patients had polymicrobial growth, and five of them were SARS-CoV-2 positive (Table 4). E. coli was more common (p = 0.026) in the PCR negative group, whereas MR-CoNS were found to be higher (p = 0.028) in the PCR positive group. The rate of carbapenem-resistant isolates among K. pneumoniae strains was 60% and 43.75% in SARS-CoV-2 positive and negative patients, respectively (p > 0.05). Acinetobacter baumannii was detected at the rate of 5.8% in SARS-CoV-2 positive patients and 1.1% in SARS-CoV-2 negative patients (p = 0.004) (Table 2). Imipenem and meropenem resistance in A. baumannii isolates were detected in six of seven SARS-CoV-2 positive and all of (n=6) the SARS-CoV-2 negative patients.
Three species that were isolated at the highest rate among fungi were C. albicans (39.47%; n:15), C. parapsilosis (18.42%; n:7), and C. tropicalis (15.78%; n:6). Moreover, C. auris was isolated from a COVID-19 patient at intensive care unit. Susceptibility tests were performed for 15 of the isolated fungi against antifungals requested by the clinician (Table 3). Among seven C. parapsilosis complex isolates, three isolates tested for antifungal susceptibilities and in two of them resistance to fluconazole was detected. Posaconazole and voriconazole susceptibilities were determined in three C. albicans isolates. One isolate was detected resistant to voriconazole and three of them had MIC values above the ECVs for posaconazole. The C. auris isolate was resistant to fluconazole, and amphotericin B.
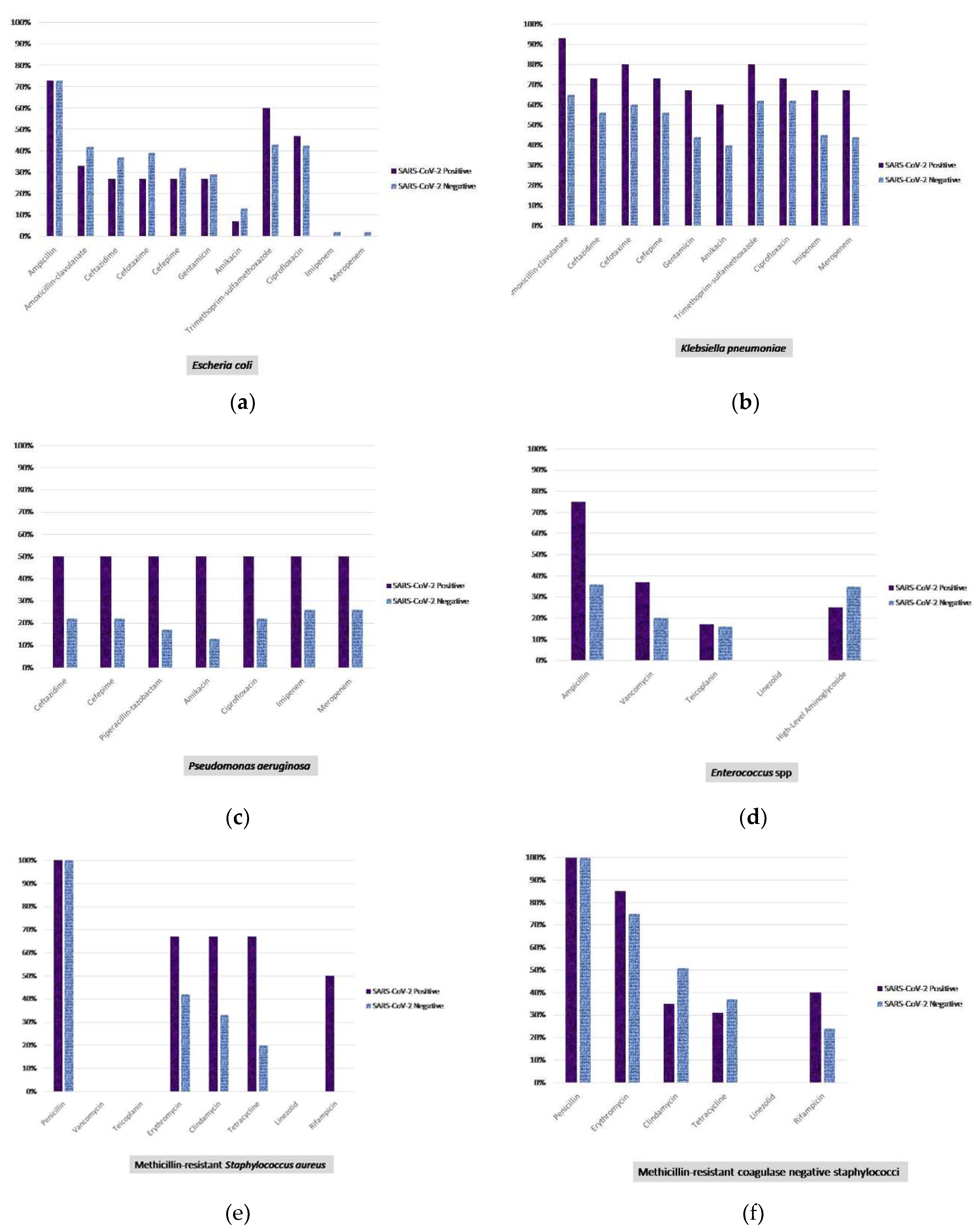
Figure 2.
Antibiotic resistance profiles of the most frequently isolated bacteria. (a) Escherichia coli; (b) Klebsiella pneumoniae; (c) Pseudomonas aeruginosa; (d) Enterococcus spp.; (e) Methicillin resistant Staphylococcus aureus; (f) Methicillin resistant coagulase negative staphylococcus.
Figure 2.
Antibiotic resistance profiles of the most frequently isolated bacteria. (a) Escherichia coli; (b) Klebsiella pneumoniae; (c) Pseudomonas aeruginosa; (d) Enterococcus spp.; (e) Methicillin resistant Staphylococcus aureus; (f) Methicillin resistant coagulase negative staphylococcus.
4. Discussion
COVID-19 pandemic has posed a devastating burden on healthcare system [14]. By affecting the epidemiology of other infections, the pandemic may have been reflected in health services as altered courses of bacteremia and fungemia. There are ongoing studies examining the distribution of bacterial and fungal agents as well as their resistance profiles in BSIs among COVID-19 patients. In these studies, it was stated that the agents isolated from COVID-19 patients were organisms that reflected the commensal skin microbiota at a high rate [15,16]. Moreover, increased and prolonged hospitalizations during the pandemic period have increased healthcare-associated infections together with the isolation of multi-drug-resistant microorganisms, leading to an increase in antibiotic consumption by the patients [17,18].
Taking into account the importance of antimicrobial management in preventing the emergence of antimicrobial resistance, assessment of the prevalence and epidemiological characteristics of bacterial co-infection is crucial in the guidance of the appropriate empirical antibiotic therapy in the presence of an infection. Antimicrobial drugs can be prescribed either prophylactically or preemptively especially in ICU patients. In a study involving patients hospitalized in ICUs from 88 different countries, despite the suspicion or the presence of bacterial co-infection among only 54% of the patients, treatment or prophylaxis with at least one antibiotic was implemented for 70% of them [19]. In another study that was carried out on COVID-19 patients, antibiotics were prescribed for 72% of the patients although only 8% of them had confirmed bacterial or fungal co-infection [19]. Improper use of antibiotics may also lead to the emergence of resistance in bacteria and side effects among patients.
In the present study, the number of patients hospitalized in the ICU was 120, of whom 37 were SARS-CoV-2 positive. In a study performed during the pandemic period, although Enterococcus spp., Staphylococcus aureus, K. pneumoniae and C. albicans were found at higher rates compared to pre-pandemic era, community acquired BSIs were reported to be higher in individuals who were SARS-CoV-2-negative (15.8 per 1000 admissions) than those who were positive (9.6 per 1000 admissions) [20]. In the present study, microorganisms were detected in 79.1% and 18% of the blood cultures of SARS-CoV-2 negative individuals and positive patients, respectively. In addition, lower rates of fermentative Gram-negative bacilli and E. coli (p = 0.012, p=0.026, respectively), and higher rates of A. baumannii, MR-CoNS, Rhizobium radiobacter and C. glabrata complex (p = 0.001, p = 0.028, p = 0.034, p = 0.034, respectively) were found in SARS-CoV-2 positive patients compared to SARS-CoV-2 negative patients in all clinics. In parallel to the other studies, MR-CoNS (21.5%) was isolated at the highest rate from the blood samples of SARS-CoV-2 patients. For example, in the study of Michailides et al. [21] in patients with Covid-19; CoNS, and K. pneumoniae together with A. baumannii, were the most frequently isolated bacteria in early and late (>5 days) nosocomial bacterial infections, respectively. Bahceci et al. [22] isolated CoNS (31%) and A. baumannii (27.5%) at higher rates. In the present study, A. baumannii strains were isolated at higher frequencies in COVID-19 positive patients than in those who were negative.
Segala et al. [23] reported higher incidence rates of nosocomial BSIs related to S. aureus and Acinetobacter spp. in pre-pandemic era among COVID-19 negative patients in wards compared to COVID-19 positive patients who were hospitalized in ICUs during the pandemic period (0.3 [%95 CI 0.21–0.32] and 0.11 [0.08–0.16] new infection per 100 patient/day, respectively) but 48% lower incident risk of E. coli infections in COVID-positive wards. E. coli isolation rate was found to be higher in patients who were SARS-CoV-2 negative (p = 0.026) in this study.
The presence of bacterial and fungal co-infections has been reported to increase the mortality of the patients with severe COVID-19 [21,24]. CoNS (OR: 25.39), non-albicans Candida species (OR: 11.12), S. aureus (OR: 10.72), Acinetobacter spp. (OR: 6.88), Pseudomonas spp. (OR: 4.77), and C. albicans (OR: 3.97) were isolated from the cases [24].
According to the COVID-19 special report published by the CDC in 2022, which investigated the impact of COVID-19 on antimicrobial resistance, there was a 35% increase in carbapenem-resistant Acinetobacter infections compared to 2019 and 2020, and a 78% increase in nosocomial infections, while a 35% increase in carbapenem-resistant Enterobacterales infections was reported [18].
The situation shows that the isolation rates of carbapenem-resistant K. pneumonia and A. baumannii strains should not be overlooked in healthcare-associated infections among SARS-CoV-2 positive patients [25,26]. Following up the antibiotic resistance rates has been of great importance due to the increase in the isolation of multi-drug resistant strains. In a study carried out on COVID-19 positive patients, 48% (n=38/79) of S. aureus and 40% (n=10/25) of K. pneumoniae isolates were found to be resistant to methicillin and carbapenems, respectively [23]. On the other hand, in our study MR-CoNS was isolated from SARS-CoV-2 positive patients at a significantly higher rate (21.5%) but statistically significant difference was not detected in the isolation rate of S. aureus and methicillin resistance rate of the isolates between COVID-19 positive patients and SARS-CoV-2 negative individuals. In another study, meropenem resistance in K. pneumoniae strains isolated from the patients in ICU was reported to increase from 79.8% in 2019 to 92.4% in 2022. Moreover, meropenem resistance rates of A. baumannii was determined to increase from 92.6% in 2018 to 97.9% in 2022 in ICU and from 82.3% to 91.6% in wards (p < 0.001) [25]. In our study, imipenem resistance of K. pneumoniae isolates was found to be 66.7% and 45.3% (p = 0.137) whereas meropenem resistance was 66.7% and 43.8% (p = 0.110) in SARS-CoV-2 positive and negative individuals, respectively. A great majority of A. baumannii isolates were resistant to imipenem and meropenem in both SARS-CoV-2 positive and negative patients.
Since fastidious bacteria cannot grow on standard media, the isolation of such microorganisms from blood cultures is closely associated with the media used for subculture and incubation conditions [7]. Fastidious bacteria isolated in our study shows the importance of using additional enriched media and various incubation conditions.
Species level identification of not only bacteria but also fungi isolated from blood cultures is important in predicting the antifungal resistance of the isolates. As found in the present study, it is noteworthy that C. auris, a species that is resistant to numerous antifungal drugs which can cause fatal outbreaks in the ICU, has been reported during the COVID-19 pandemic [13,27-30]. Moreover, in a study that investigated fungal colonization in different body parts of COVID-19 patients hospitalized in the ICU, it was reported that the presence of colonization with non-albicans Candida species which can be associated with treatment failures due to the antifungal resistance, was significantly higher and more common in ICU patients compared to non-COVID-19 patients [31].
5. Conclusions
The results of the study imply the importance of not ignoring nosocomial infections while focusing on COVID-19 during the pandemic, paying attention to isolation procedures and the major impact of measures on reduction in mortality via reducing the risk of infection.
Author Contributions
Conceptualization, Bahar Akgün Karapınar and Betigül Öngen; Data curation, Bahar Akgün Karapınar, Zayre Erturan and Betigül Öngen; Formal analysis, Bahar Akgün Karapınar, Zayre Erturan, Ali Ağaçfidan and Betigül Öngen; Investigation, Bahar Akgün Karapınar, İlvana Çaklovica Küçükkaya, Yasemin Bölükbaşı and Sertaç Küçükkaya; Methodology, Bahar Akgün Karapınar, İlvana Çaklovica Küçükkaya, Yasemin Bölükbaşı, Sertaç Küçükkaya, Gonca Erköse Genç, Zayre Erturan, Ali Ağaçfidan and Betigül Öngen; Writing – original draft, Bahar Akgün Karapınar, İlvana Çaklovica Küçükkaya, Yasemin Bölükbaşı, Sertaç Küçükkaya, Gonca Erköse Genç, Zayre Erturan, Ali Ağaçfidan and Betigül Öngen; Writing – review & editing, Bahar Akgün Karapınar, Gonca Erköse Genç, Zayre Erturan and Betigül Öngen.
Funding
This research received no external funding.
Institutional Review Board Statement
The research was approved by University of Health Sciences İstanbul Training and Research Hospital Ethics Committee (protocol code: 63 and date of approval:11.02.2022).
Acknowledgments
The study was presented at the “32nd European Congress of Clinical Microbiology & Infectious Diseases, Lisbon, Portugal,” held on 23-26 April 2022. Poster number: 4568.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Manohar, P.; Loh, B.; Nachimuthu, R.; Hua, X.; Welburn, S.C.; Leptihn, S. Secondary bacterial infections in patients with viral pneumonia. Front. Med. 2020, 7, 420. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Simmonds, A.; Annavajhala, M.K.; McConville, T.H.; Dietz, D.E.; Shoucri, S.M.; Laracy, J.C.; Rozenberg, F.D.; Nelson, B.; Greendyke, W.G.; Furuya, E.Y.; Whittier, S.; Uhlemann, A.C. Carbapenemase-producing Enterobacterales causing secondary infections during the COVID-19 crisis at a New York City hospital. J. Antimicrob. Chemother. 2021, 76, 380–384. [Google Scholar] [CrossRef]
- Bengoechea, J.A.; Bamford, C.G. SARS-CoV-2 bacterial co-infections and AMR: the deadly trio in COVID-19. EMBO. Mol. Med. 2020, 12, e12560. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Amin, A.K.; Khanna, P.; Aali, A.; McGregor, A.; Bassett, P.; Gopal Rao, G. An observational cohort study of bacterial coinfection and implications for empirical antibiotic therapy in patients presenting with COVID-19 to hospitals in North West London. J. Antimicrob. Chemother. 2021, 76, 796–803. [Google Scholar] [CrossRef]
- Yu, D.; Ininbergs, K.; Hedman, K.; Giske, C.G.; Stralin, K.; Özenci, V. Low prevalence of bloodstream infection and high blood culture contamination rates in patients with COVID-19. Plos One. 2020, 15, e0242533. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Bloodstream infection event (central line-associated bloodstream infection and non-central line-associated bloodstream infection). 2021. Available online: https://www.cdc.gov/nhsn/pdfs/pscmanual/4psc_clabscurrent.pdf (accessed on 12 December 2022).
- Gilligan, P.H.; Alby, K.; York, M.K. Blood cultures. In Clinical Microbiology Procedures Handbook, , Leber, A.L. Ed. in chief., 4th ed.; ASM Press: Washington, USA, 2016. [Google Scholar]
- CLSI. Epidemiological cutoff values for antifungal susceptibility testing. 3rd ed. CLSI supplement M59. Wayne, PA: Clinical and Laboratory Standards Institute; 2020.
- Clinical and Laboratory Standards Institute. Reference method for broth dilution antifungal susceptibility testing of yeasts; 4th informational supplement M27-S4. CLSI, Wayne, PA, 2012.
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 10.0, 2020. http://www.eucast.org.
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 11.0, 2021. http://www.eucast.org.
- Centers for Disease Control and Prevention (CDC). Candida auris. Available online: https://www.cdc.gov/fungal/candida-auris/index.html (accessed on 16 February 2021).
- Bölükbaşı, Y.; Erköse, G.G.; Orhun, G.; Kuşkucu, M.A.; Çağatay, A.; Önel, M.; Öngen, B.; Ağaçfidan, A.; Esen, F.; Erturan, Z. First case of COVID-19 positive Candida auris fungemia in Turkey. Mikrobiyol. Bul. 2021, 55, 648–655. [Google Scholar] [CrossRef]
- Willan, J.; King, A.J.; Jeffery, K.; Bienz, N. Challenges for NHS hospitals during Covid-19 epidemic. BMJ. 2020, 368, m1117. [Google Scholar] [CrossRef]
- Sepulveda, J.; Westblade, L.F.; Whittier, S.; Satlin, M.J.; Greendyke, W.G.; Aaron, J.G.; Zucker, J.; Dietz, D.; Sobieszczyk, M.; Choi, J.J.; Liu, D.; Russell, S.; Connelly, C.; Green, D.A. Bacteremia and blood culture utilization during COVID-19 surge in New York City. J. Clin. Microbiol. 2020, 58, e00875–20. [Google Scholar] [CrossRef]
- Hughes, S.; Troise, O.; Donaldson, H.; Mughal, N.; Moore, L.S.P. Bacterial and fungal coinfection among hospitalized patients with COVID-19: a retrospective cohort study in a UK secondary-care setting. Clin. Microbiol. Infect. 2020, 26, 1395–1399. [Google Scholar] [CrossRef]
- Mahmoudi, H. Bacterial co-infections and antibiotic resistance in patients with COVID-19. GMS. Hyg. Infect. Control. 2020, 15, Doc35. [Google Scholar]
- Center for Disease Control and Prevention. COVID-19: US Impact on Antimicrobial Resistance, Special Report 2022; US Department of Health and Human Services, CDC: Atlanta, GA, USA, 2022. [Google Scholar]
- Getahun, H.; Smith, I.; Trivedi, K.; Paulin, S.; Balkhy, H.H. Tackling antimicrobial resistance in the COVID-19 pandemic. Bull. World Health Organ. 2020, 98, 442–442A. [Google Scholar] [CrossRef]
- Bauer, K.A.; Puzniak, L.A.; Yu, K.C.; Finelli, L.; Moise, P.; Ai, C.; Watts, J.A.; Gupta, V. Epidemiology and outcomes of culture-positive bloodstream pathogens prior to and during the SARS-CoV-2 pandemic: a multicenter evaluation. BMC. Infect. Dis. 2022, 22, 841. [Google Scholar] [CrossRef] [PubMed]
- Michailides, C.; Paraskevas, T.; Karalis, I.; Koniari, I.; Pierrakos, C.; Karamouzos, V.; Marangos, M.; Velissaris, D. Impact of bacterial infections on COVID-19 patients: is timing important? Antibiotics (Basel). 2023, 12, 379. [Google Scholar] [CrossRef] [PubMed]
- Bahceci, I.; Yildiz, I.E.; Duran, O.F.; Soztanaci, U.S.; Kirdi Harbawi, Z.; Senol, F.F.; Demiral, G. Secondary bacterial infection rates among patients with COVID-19. Cureus. 2022, 14, e22363. [Google Scholar] [CrossRef] [PubMed]
- Segala, F.V.; Pafundi, P.C.; Masciocchi, C.; Fiori, B.; Taddei, E.; Antenucci, L.; De Angelis, G.; Guerriero, S.; Pastorino, R.; Damiani, A.; Posteraro, B.; Sanguinetti, M.; De Pascale, G.; Fantoni, M.; Murri, R. Incidence of bloodstream infections due to multidrug-resistant pathogens in ordinary wards and intensive care units before and during the COVID-19 pandemic: a real-life, retrospective observational study. Infection. 2023, 51, 1061–1069. [Google Scholar] [CrossRef]
- Silva, D.L.; Lima, C.M.; Magalhães, V.C.R.; Baltazar, L.M.; Peres, N.T.A.; Caligiorne, R.B.; Moura, A.S.; Fereguetti, T.; Martins, J.C.; Rabelo, L.F.; Abrahão, J.S.; Lyon, A.C.; Johann, S.; Santos, DA. Fungal and bacterial coinfections increase mortality of severely ill COVID-19 patients. J. Hosp. Infect. 2021, 113, 145–154. [Google Scholar] [CrossRef]
- Petrakis, V.; Panopoulou, M.; Rafailidis, P.; Lemonakis, N.; Lazaridis, G.; Terzi, I.; Papazoglou, D.; Panagopoulos, P. The impact of the Covıd-19 pandemic on antimicrobial resistance and management of bloodstream infections. Pathogens. 2023, 12, 780. [Google Scholar] [CrossRef]
- Sinto, R.; Lie, K.C.; Setiati, S.; Suwarto, S.; Nelwan, E.J.; Djumaryo, D.H.; Karyanti, M.R.; Prayitno, A.; Sumariyono, S.; Moore, C.E.; Hamers, R.L.; Day, N.P.J.; Limmathurotsakul, D. Blood culture utilization and epidemiology of antimicrobial-resistant bloodstream infections before and during the COVID-19 pandemic in the Indonesian national referral hospital. Antimicrob. Resist. Infect. Control. 2022, 11, 73. [Google Scholar] [CrossRef]
- Chowdhary, A.; Tarai, B.; Singh, A.; Sharma, A. Multidrug-resistant Candida auris infections in critically ill coronavirus disease patients, India, April-July 2020. Emerg. Infect. Dis. 2020, 26, 2694–2696. [Google Scholar] [CrossRef]
- Arastehfar, A.; Carvalho, A.; Nguyen, M.H.; Hedayati, M.T.; Netea, M.G.; Perlin, D.S.; Hoenigl, M. COVID-19-associated candidiasis (CAC): an underestimated complication in the absence of immunological predispositions? J. Fungi (Basel). 2020, 6, 211. [Google Scholar] [CrossRef]
- Rodriguez, J.Y.; Le Pape, P.; Lopez, O.; Esquea, K.; Labiosa, A.L.; Alvarez-Moreno, C. Candida auris: a latent threat to critically ill patients with Coronavirus disease 2019. Clin. Infect. Dis. 2020, 73, e2836–7. [Google Scholar] [CrossRef] [PubMed]
- Magnasco, L.; Mikulska, M.; Giacobbe, D.R.; Taramasso, L.; Vena, A.; Dentone, C.; Dettori, S.; Tutino, S.; Labate, L.; Di Pilato, V.; Crea, F.; Coppo, E.; Codda, G.; Robba, C.; Ball, L.; Patroniti, N.; Marchese, A.; Pelosi, P.; Bassetti, M. Spread of carbapenem-resistant gram-negatives and Candida auris during the COVID-19 pandemic in critically ill patients: one step back in antimicrobial stewardship? Microorganisms. 2021, 9, 95. [Google Scholar] [CrossRef] [PubMed]
- Çaklovica-Küçükkaya, İ.; Orhun, G.; Çağatay, A.A.; Kalaycı, S.; Esen, F.; Şahin, F.; Ağaçfidan, A.; Erturan, Z. P494 Comparison of Candida colonization in intensive care unit patients with and without COVID-19: first prospective cohort study from Turkey, Medical Mycology, Volume 60, Issue Supplement_1, September 2022, myac072P494. 20 September. [CrossRef]

Table 1.
Distribution of SARS-CoV-2 (+) and SARS-CoV-2 (-) patients according to clinics.
| Clinics | Unit | SARS CoV-2 (+) | SARS CoV-2 (-) | Not tested |
|---|---|---|---|---|
| Inpatient | Surgical | 24 | 96 | - |
| Internal | 19 | 69 | 3 | |
| Outpatient | Surgical | - | 26 | - |
| Internal | 38 | 243 | 14 | |
| Intensive Care Unit | Surgical | 5 | 43 | 1 |
| Internal | 32 | 38 | 1 |
Table 2.
Distribution of bacteria and fungi isolated from blood cultures.
| Microorganisms | TotalWYXWYX[n(%)] | SARS-CoV-2WYXWYXPositive [n (%)] | SARS-CoV-2WYXWYXNegative [n (%)] | SARS-CoV-2WYXWYXNon tested [n (%)] | Positive vs. Negative |
|---|---|---|---|---|---|
| All microorganisms | 671 (100) | 121 (18) | 531 (79.1) | 19 (2.8) | p value |
| FermentativeGram-negative rods | 252 (37.5) | 34 (28) | 214 (40.3) | 4 (21) | 0.012 |
| Escherichia coli | 131 (19.5) | 15 (12.4) | 113 (21.3) | 3 (15.8) | 0.026 |
| Klebsiella pneumoniae1/ Carbapenem-resistant K. pneumoniae2 | 80/38 (11.9/5.6) | 15/9 (12.4/7.4) | 64 / 28 (12.05 /5.3) | 1/1 (5.3/5.3) | 0.9171WYXWYX0.3532 |
| Klebsiella oxytoca | 5 (0.7) | 0 (0.0) | 5 (0.9) | - | 0.590 |
| Enterobacter spp. | 7 (1.05) | 1 (0.8) | 6 (1.1) | - | 0.770 |
| Serratia marcescens | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Serratia spp. | 2 (0.3) | 0 (0.0) | 2 (0.4) | - | 1.000 |
| Citrobacter spp. | 3 (0.45) | 0 (0.0) | 3 (0.6) | - | 1.000 |
| Citrobacter koseri | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Proteus mirabilis | 13 (1.9) | 1 (0.8) | 12 (2.3) | - | 0.309 |
| Morganella morganii | 3 (0.45) | 0 (0.0) | 3 (0.6) | - | 1.000 |
| Raoultella planticola | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Aeromonas spp. | 1 (0.15) | 0 (0.0) | 1 (0.2) | 1.000 | |
| Salmonella Enteritidis | 4 (0.6) | 2 (1.65) | 2 (0.4) | - | 0.105 |
| Non-FermentativeGram-negative rods | 66 (9.8) | 16 (13.2) | 48 ( 9 ) | 2 (10.5) | 0.163 |
| Pseudomonas aeruginosa | 25 (3.7) | 2 (1.65) | 23 (4.3) | - | 0.166 |
| Pseudomonas stutzeri | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Pseudomonas spp. | 5 (0.7) | 2 (1.65) | 3 (0.6) | - | 0.216 |
| Acinetobacter baumannii | 14 (2.1) | 7 (5.8) | 6 (1.1) | 1 (5.3) | 0.001 |
| Acinetobacter lwoffii | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Acinetobacter spp. | 4 (0.6) | 2 (1.65) | 2 (0.4) | - | 0.105 |
| Rhizobium radiobacter | 2 (0.3) | 2 (1.65) | 0 (0.0) | - | 0.034 |
| Achromobacter xylosoxidans | 1 (0.15) | - | - | 1 (5.3) | - |
| Ochrobactrum anthropi | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Sphingomonas paucimobilis | 2 (0.3) | 0 (0.0) | 2 (0.4) | - | 1.000 |
| Stenotrophomonas maltophilia | 7 (1.05) | 1 (0.8) | 6 (1.1) | - | 0.770 |
| Burkholderia cepacia | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Pandoraea spp. | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Non-Fermentative Gram-negative rod | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Gram-positive cocci | 300 (44.7) | 59 (48.8) | 231 (40.1) | 10 (52.6) | 0.294 |
| Methicillin resistant Staphylococcus aureus | 27 (4.0) | 3 (2.5) | 24 (4.5) | - | 0.309 |
| Methicillin sensitive Staphylococcus aureus | 53 (7.9) | 7 (5.8) | 43 (8.1) | 3 (15.8) | 0.388 |
| Methicillin resistant coagulase negative staphylococcus | 102 (15.2) | 26 (21.5) | 72 (13.5) | 4 (21.05) | 0.028 |
| Methicillin sensitive coagulase negative staphylococcus | 49 (7.3) | 12 (9.9) | 35 (6.6) | 2 (10.5) | 0.202 |
| Enterococcus faecalis | 12 (1.8) | 2 (1.65) | 10 (1.9) | - | 0.865 |
| Enterococcus faecium | 12 (1.8) | 3 (2.5) | 9 (1.7) | - | 0.562 |
| Enterococcus avium | 4 (0.6) | 0 (0.0) | 4 (0.75) | - | 1.000 |
| Enterococcus gallinarum | 3 (0.45) | 1 (0.8) | 2 (0.4) | - | 0.509 |
| Enterococcus spp. | 16 (2.4) | 2 (1.65) | 14 (2.6) | - | 0.528 |
| Streptococcus pneumoniae | 4 (0.6) | 2 (1.65) | 2 (0.4) | - | 0.105 |
| Streptococcus agalactiae | 3 (0.45) | 0 (0.0) | 3 (0.6) | - | 1.000 |
| Streptococcus gallolyticus | 2 (0.3) | 0 (0.0) | 2 (0.4) | - | 1.000 |
| Streptococcus equi | 1 (0.15) | 1 (0.8) | 0 (0.0) | - | 0.186 |
| Leuconostoc pseudomesenteroides | 2 (0.3) | 0 (0.0) | 1 (0.2) | 1 (5.3) | 1.000 |
| Alpha hemolytic streptococcus | 7 (1.05) | 0 (0.0) | 7 (1.3) | - | 0.359 |
| Beta hemolytic streptococcus | 2 (0.3) | 0 (0.0) | 2 (0.4) | - | 1.000 |
| Non-hemolytic streptococcus | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Gram-positive rods | 3 (0.45) | 1 (0.8) | 2 (0.4) | 0 (0) | 0.509 |
| Corynebacterium jeikeium | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Corynebacterium striatum | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Lactobacillus casei | 1 (0.15) | 1 (0.8) | 0 (0.0) | - | 0.186 |
| Other bacteria | 5 (0.7) | 2 (1.65) | 3 (0.6) | 0 (0) | 0.216 |
| Listeria monocytogenes | 2 (0.3) | 1 (0.8) | 1 (0.2) | - | 0.251 |
| Campylobacter coli | 1 (0.15) | 1 (0.8) | 0 (0.0) | - | 0.186 |
| Campylobacter jejuni | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Moraxella nonliquefaciens | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Anaerobic bacteria | 7 (1.05) | 1 (0.8) | 6 (1.13) | 0 (0) | 0.770 |
| Bacteroides fragilis | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Bacteroides spp. | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Prevotella spp. | 2 (0.3) | 0 (0.0) | 2 (0.4) | - | 1.000 |
| Clostridium clostridioforme | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Fusobacterium nucleatum | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Anaerobic Gram-positive rod | 1 (0.15) | 1 (0.8) | 0 (0.0) | - | 0.186 |
| Fungi | 38 (5.7) | 8 (6.6) | 27 (5.1) | 3 (15.8) | 0.501 |
| Candida albicans | 15 (2.2) | 2 (1.65) | 11 (2.1) | 2 (10.5) | 0.766 |
| Candida parapsilosis complex | 7 (1.05) | 1 (0.8) | 6 (1.1) | - | 0.770 |
| Candida tropicalis | 6 (0.9) | 0 (0.0) | 5 (0.9) | 1 (5.3) | 0.590 |
| Candida kefyr | 2 (0.3) | 1 (0.8) | 1 (0.2) | - | 0.252 |
| Candida glabrata complex | 2 (0.3) | 2 (1.65) | 0 (0.0) | - | 0.034 |
| Candida metapsilosis | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Candida krusei | 1 (0.15) | 1 (0.8) | 0 (0.0) | - | 0.186 |
| Candida auris | 1 (0.15) | 1 (0.8) | 0 (0.0) | - | 0.186 |
| Kodamaea ohmeri | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Cryptococcus neoformans | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
| Rhodotorula spp. | 1 (0.15) | 0 (0.0) | 1 (0.2) | - | 1.000 |
Table 3.
Antifungal resistance profiles of fungal isolates.
| Fungi | Antifungal MIC, µg/ml | |||||||
|---|---|---|---|---|---|---|---|---|
| Species (tested/total n) | Strain No | Fluconazole | Posaconazole | Voriconazole | İtraconazole | Amphotericin B | Caspofungin | Anidulafungin |
| Candida albicans(7/15) | 1 | 2 (S) | 0.064ᵃ (NWT) | 0.25 (I) | - | 0.5ᵃ (WT) | 0.016 (S) | 0.012 (S) |
| 2 | 2 (S) | 0.064ᵃ (NWT) | 0.047 (S) | - | - | - | - | |
| 3 | 0.75 (S) | - | - | - | - | 0.5 (I) | - | |
| 4 | 2 (S) | - | - | - | 0.25ᵃ (WT) | 0.5 (I) | 0.012 (S) | |
| 5 | 1,5 (S) | - | - | - | - | - | - | |
| 6 | - | 0.25ᵃ (NWT) | 1 (R) | - | - | 0.065 (S) | - | |
| 7 | 0.125 (S) | - | - | - | 0.047ᵃ (WT) | 0.096 (S) | 0.003 (S) | |
| Candida parapsilosiscomplex (3/7) | 1 | 0.75 (S) | - | - | - | 0.25ᵃ (WT) | 0.75 (S) | - |
| 2 | >256 (R) | 0.19ᵃ (WT) | 0.5 (I) | 2c | 0.75ᵃ (WT) | 0.38 (S) | 0.75 (S) | |
| 3 | 24 (R) | 0.25ᵃ (WT) | 0.75 (S) | |||||
| Candida tropicalis(2/6) | 1 | 0.5 (S) | - | 0.008 (S) | - | 0.25ᵃ (WT) | 0.094 (S) | 0.008 (S) |
| 2 | 0.5 (S) | - | - | - | 0.25ᵃ (WT) | - | 0.008 (S) | |
| Candida glabratacomplex (1/2) | 1.5 (SDD) | - | 0.032ᵃ (WT) | - | - | 0.25 (I) | - | |
| Candida auris(1/1)b | >256 (R) | 0.016c | 0.19c | 0,19 c | 3 (R) | 1 (S) | 0.094 (S) | |
| Cryptococcus neoformans(1/1) | 8ᵃ (WT) | - | - | - | 0.5ᵃ (WT) | - | - | |
MIC: Minimal inhibitory concentration; n: Number of isolates; a: Epidemiological cut-off values (ECVs); b: MICs were evaluated according to te tentative breakpoinst determined by CDC; c: There are no clinical breakpoints or ECVs; S: Susceptible; I: Intermediate; R: Resistant; SDD: Susceptible-dose dependent; WT: Wild type; NWT: Non-wild type.
Table 4.
Distribution of polymicrobial growths detected in patients.
| Unit | Microorganism | ||
|---|---|---|---|
| SARS-CoV-2 (+) [n=8] | Inpatient (n=3) | Surgical (n=1) | Candida krusei, Kodamea ohmeri |
| Internal (n=2) | Proteus mirabilis, Escherichia coli | ||
| Klebsiella pneumoniae, Candida glabrata complex | |||
| Outpatient (n=4) | Surgical (n=1) | Candida glabrata complex, Candida albicans | |
| Internal (n=3) | Streptococcus pneumoniae, Escherichia coli | ||
| Candida kefyr, Enterococcus gallinarum, Enterococcus faecium | |||
| Escherichia coli, Enterobacter spp. | |||
| Intensive Care Unit (n=1) | Surgical (n=0) | - | |
| Internal (n=1) | Enterococcus spp., Candida albicans | ||
| SARS-CoV-2 (-) [n=7] | Inpatient (n=1) | Surgical (n=2) | Candida albicans, Candida parapsilosis |
| Escherichia coli, Candida parapsilosis | |||
| Internal (n=1) | Pseudomonas aeruginosa, Acinetobacter spp. | ||
| Outpatient (n=5) | Surgical (n=1) | Citrobacter spp., Klebsiella oxytoca | |
| Internal (n=4) | Raoultella planticola, Escherichia coli | ||
| Klebsiella pneumoniae, Enterococcus spp. | |||
| Enterococcus spp., Escherichia coli, MSSA* | |||
| Enterococcus spp., Escherichia coli | |||
| Intensive Care Unit (n=1) | Surgical (n=0) | - | |
| Internal (n=1) | Proteus mirabilis, Klebsiella pneumoniae | ||
*Methicillin sensitive Staphylococcus aureus.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



