
Submitted:
16 August 2023
Posted:
18 August 2023
You are already at the latest version
Abstract
Enamel erosion is a process which happens every time we eat and it may be accelerated by some particular acid foods, drinks or other agents. Dental enamel when damaged by low pH substances becomes chalky, rough, opaque, yellowed and it can be related to dentinal hypersensitivity. To the present day, several possible solutions are available, therefore the aim of this study was to evaluate the effect of a biocompatible minerals serum based on calcium silicate, sodium phosphate and fluoride (Regenerate™) on the damaged enamel by four different acid liquids. 135 ovine teeth were equally divided into 5 groups and submerged for one week into lemon juice, energy drink, coffee, tea and physiologic solution for the negative control. The first 4 groups were evaluated for their color with an analogical color scale (Vita® Scale) and for their surface assigning a qualitative aspect among opaque, rough, chalky or smooth. Then they were treated with hydroxyapatite gels and re-evaluated for the same parameters. Data were checked for the normal distribution with Shapiro-Wilk test and analyzed with dependent t-test or Wilcoxon Signed Rank test, every test with a p≤0.05. Both color and surface aspect showed a strongly significant improvement after the treatment. Biocompatible minerals serum based on hydroxyapatite is able to reverse teeth erosion, improve the color and restore the smoothness of the dental enamel.
Keywords:
biocompatible minerals
; calcium silicate sodium phosphate
; enamel
; Erosion
; hydroxyapatite
; remineralization
1. Introduction
Dental hard tissues erosion is characterized by an irretrievable gradual decline of mineral components in tooth enamel, dentin and cementum according to the severity of the process, caused by non-bacterial acids [1]. The burden of this problem is significant especially considering the fact that tooth demineralization happens several times a day after eating, drinking or when pathological habits occur e.g. gastroesophageal reflux, chronic gastritis, hiatal hernia, esophageal atresia, bulimia and more [2,3,4]. The modern society often experimented erosive tooth wear, since it has been described as the second most prevalent oral disease after dental caries [5]. While dental caries has been characterized by a critical pH limit of 5.5-5.7 for enamel, dental erosion has no critical pH value which varies according to the acid solution in contact to the hard tissues [6]. The reason why dental erosion has no critical pH limit is because the rate of erosion is also affected by other factors, such as the concentration of the acid, the duration of exposure to the acid, and the individual's susceptibility to erosion. In general, acids with a lower pH will cause erosion more quickly than acids with a higher pH. However, even acids with a relatively high pH, such as orange juice (pH 3.5), can cause erosion if they are in contact with the teeth for a long period of time.
From a histopathological point of view, erosive demineralization begins with a surface softening following a centripetal process conferring a typical “rough irregular etched pattern” to the enamel. This process progresses through narrow pores and reaches crystals in the enamel subsurface causing their demineralization (near-surface demineralization). This resulting softening layer is more susceptible to further progressive wear originating both from mechanical and chemical causes [7]. Enamel includes less soluble mineral compounds than dentin, hence its erosive deconstruction develops more slowly.
Solubility is the ability of a substance to dissolve in a solvent. The less soluble a substance is, the more difficult it is for it to dissolve. Enamel is made up of hydroxyapatite, which is a very insoluble mineral. Dentin, on the other hand, is made up of collagen, which is a protein that is more soluble than hydroxyapatite. This difference in solubility means that acids are less likely to dissolve enamel than dentin. As a result, erosive destruction of enamel develops more slowly than erosive destruction of dentin. In addition to the difference in solubility, there are other factors that contribute to the slower rate of erosive destruction of enamel. Enamel also has a higher fluoride content than dentin, which makes it more resistant to acid attack [8].
Dental erosion shows a multifactorial etiology, and it may be caused by extrinsic acids (beverages or acidic foods, or drugs) or intrinsic factors (such as gastroesophageal re-flux or regurgitation due to bulimic or anorexic disorders) [9].
The entire process of dental erosion begins at the surface of dental, with the destruction of the dental pellicle due to chelating agents/decalcifying acids, then tooth’s organic substrate is dissolved, and the enamel undergoes demineralization. The mechanical friction, associated with swallowing, chewing or brushing, may damage the exposed dental surface and affect hard tissues of the tooth (both enamel and dentin). These lesions are usually found in specifical areas of the teeth (cervical, vestibular or oral regions) and show a concave and smooth appearance [10]. When the process has begun and the demineralization affects superficial layers of dental enamel, erosion goes forward and worse if other minor mechanical stress set in (lips or cheeks muscles contraction, food impact) [11]. Dental erosion may be diagnosed using several criteria: non-carious etiology loss of tooth structure, outside the point of contact or occlusal guidance, and a smooth, polished, curved shape. In addition, negative gap areas at the edges of amalgam or composite fillings can also be observed [12]. Identifying intrinsic or extrinsic etiological factors is a very important step towards best and customized treatment, and taking patient’s oral medical history is a crucial part of the process. Each etiological factor shows a preferential erosive zone location: for intrinsic factors, lesions are most frequently searched out on the palatal side of the maxillary anterior elements first, then extending to the palatal areas of maxillary lateral teeth and finally to the lingual and occlusal surfaces of the mandibular elements; vestibular areas of the teeth are most frequently in-volved when extrinsic factors are involved. By taking a careful history and examining the location of the lesions, dentists can often identify the underlying cause of tooth erosion and recommend the best course of treatment.Changes in dietary habits of population in developed countries in the last ten years, with a massive raise of consumption of acidic beverages, may be related to the increased incidence of dental erosion [13]. The consumption of energy drinks (carbonated soft drinks with low pH, refined carbohydrates and additives, such caffeine) has gone through an incredible expansion in many countries all over the world, exceeding 5.8 billion liters [14]; the intensification of consumption of this kind of beverages was due to energy’s augmentation, related to their content in sugar, caffeine and taurine [15], making them very popular among young populations, especially students (pleasant taste and stimulating action). Several studies have reported that chemical characteristics of acidic beverages, such as energy drinks, are the main factors to determine the erosive potential: pH, buffering capacity, acid titration, type of acid (phosphoric, citric, etc.), total acid content, presence of calcium, phosphate and fluorine are the most relevant [16]. Although lots of in vitro study have been published about the effects of carbonated soft drinks on dental enamel, limited data has been made available on the linking between intake of other type of beverages (sports and high-energy drinks, processed fruit-based beverages, coffee beverages, bottled water) and enamel erosion [17]. In order to protect teeth from dental erosion, one important step is to limit the intake of acidic beverages. If people do drink acidic beverages, they should rinse their mouths with water afterwards and avoid chewing acidic gum or candy.
Treatment of dental erosion provides the elimination of the causes that accelerate the process (reducing consumption of sweet or acidic food and drinks, regularly brushing teeth after meals, chewing sugar-free gums to remove food residues), in addition to the use of products containing fluoride and other minerals (toothpaste based on fluoride and remineralizing elements, in office topical and professional treatments), which may fortify the damaged enamel surface. Recently, a new product has been developed to regenerate the enamel loss caused by erosive acids; this toothpaste works as a topical source of calcium and phosphate in order to raise the level of these two ions in saliva and to promote remineralization by forming hydroxyapatite (HAP) [18]. This dentifrice is composed of 1450 ppm sodium monofluorophosphate (MFP), calcium silicate, and sodium phosphate salts (monosodium phosphate and trisodium phosphate) and shows its protective effect by depositing calcium silicate on enamel surface and form HAP [19]. To promote additional remineralization, a dual-phase gel was also developed and has two parts (one part contains calcium silicate and sodium phosphate salts, and the other part contains sodium fluoride). Previous studies demonstrate that the use of sodium phosphate and calcium silicate dentifrice pastes produced a greater gain in surface hardness and a lower enamel loss after an erosive cycling model [20].
The present study aimed to investigate the appearance of the enamel of ovine teeth subjected to various acidic solutions and treated with calcium silicate and sodium phosphate serum.
2. Materials and Methods
A sample of 135 ovine teeth were collected by 5 sheep head retrieved by the butcher shop. One surface of each dental element underwent ultrasonic scaling (Piezo Mectron Dental s.p.a. Italy) and then they were equally dived and immersed into 5 different solutions as lemon juice, energy drink (Redbull®), coffee without sugar, tea without sugar and physiologic solution as a control group. Each solution was previously tested for the pH using a digital professional pHmeter (Figure 1, pH7Vio, XS Instrument®, Italy) as shown in Table 1.
Teeth were left in their liquid for one week, then the surface previously subjected to scaling was evaluated according to its color with analogical Vita Color Scale (Vita®, Italy) and for its aspect with a probe by assign a qualitative parameter as opaque, rough, chalky or smooth (Figure 2). Both the examination was provided by a calibrated operator. After the evaluation, the first 4 groups were treated with a serum based on biocompatible and biomimetic minerals (Figure 3, Regenerate™ Serum, Unilever). The dual-phase serum is composed of calcium phosphate and sodium silicate, which in the oral cavity forms hydroxyapatite (Table 2). Additionally, it contains fluoride 1450 parts per million (ppm). Following the producer protocol, teeth were left into the serum for 3 minutes, then they were gently rinsed and immersed into the original acid fluid. This protocol was repeated for 3 days, after which a new colorimetric and qualitative assessments were registered.
Statistical analysis
Data were tested for normal distribution using Shapiro-Wilk analysis, if passed the dependent t-test was performed. If data were not normally distributed, a Wilcoxon signed-rank test was performed. For each test a significance of p≤0.05 was chosen. The statistical software employed was the Statistical Package for the Social Sciences (IBM SPSS version 29.0; SPSS Inc. Chicago, IL).
3. Results
3.1. Color analysis
3.1.1. Lemon
Shapiro Wilk’s test significance value was found to be 0.075, so the distribution of the differences was not significant from a normal distribution. Therefore, a dependent t-test was carried out to perform the analysis. The results from the pre-treatment (M=8.85, SD=5.45) and post-test (M=4.93, SD=4.66) indicate that the treatment resulted in a significant change in color for ovine teeth put in lemon solution, t(26)=7.8, p=0.000.
3.1.2. Energy drink
Shapiro Wilk’s test p-value observed was 0.000, therefore it was concluded that the data deviated from normality, so the Wilcoxon signed-rank test was performed. For the ovine teeth submersed in an energy drink, the color change was significantly different during pre-treatment (Mdn=9) than post-treatment (Mdn=8), z=4.204, p<0.05.
3.1.3. Coffee
The Shapiro Wilk’s test p-value observed was 0.003, therefore it was concluded that the data is not normally distributed, so Wilcoxon signed-rank test was performed. For the ovine teeth submersed in coffee, the color change was significantly different during pre-treatment (Mdn= 13) than post-treatment (Mdn= 13), z= 4.159, p<0.05.
3.1.4. Tea
The Shapiro Wilk’s test p-value observed was 0.006, therefore it was concluded that the data is not normally distributed and Wilcoxon signed rank test should be performed. For the ovine teeth put in tea, the color change was significantly different during pre-treatment (Mdn= 10) than post-treatment (Mdn= 8), z= 3.886, p<0.05.
Color results are provided by Table 3.
3.2. Qualitative surface aspect
In the second part of the analysis, a chi-square test was performed in order to check if there is an association between the treatment and the aspects of the enamel. As observed by the frequencies cross-tabulated in the Table 4, there is a strong significant relationship between the two variables, χ2 (8,N= 375)= 105.066, p<0.05.
4. Discussion
A description of erosive consequences on enamel by different acid solutions, and an overview of the effects after the remineralizing treatment with a biocompatible minerals serum were carried out.
The remineralization of dental hard tissues provided by the saliva is well known in literature [21], due to the delivery of bioavailable forms of Ca2+ and PO43– which can diffuse into enamel, dentine and cementum when the saliva has a physiological pH. This means that these ions are in a form that can be easily absorbed by the teeth. The bioavailable forms of calcium and phosphate are also in a ratio that is optimal for remineralization. [22,23]. Thus, the salivary remineralization of dental hard tissues is a complex process that involves a number of factors. However, the transfer of bioavailable forms of calcium and phosphate is essential for the process to be effective. When the saliva has a physiological pH and contains the right balance of minerals, the teeth are better able to resist demineralization and maintain their health. Studies by Mattousch et al. [24] and van der Veen et al. [25] following the natural progression of white spot lesions showed that they were steady even after 2 years without treatment. However, salivary remineralization is a slow process, because the mineral gain is limited to the surface of the enamel due to the low ion concentration gradient from saliva into the enamel [26,27]. Additional extrinsic sources of stabilized calcium phosphate ions could augment the natural remineralization potential of saliva by increasing diffusion gradients favouring faster and deeper subsurface remineralization [28]. Sun et al. [19] stated that calcium silicate toothpaste was able to form HAP onto enamel surface, becoming increasingly crystalline over 3 hours. As evidence of this, Li et al. [29] demonstrated how calcium silicate and sodium phosphate toothpaste completely occluded dentine tubules and formed HAP. According to the authors, the deposited material on and within dentine tubules was resilient to acid erosive challenges. The sealing of dentinal tubules is clinically of help in the management of dental hypersensitivity, thus Seong et al. [30] proved how a toothpaste based on calcium silicate and sodium phosphate was more effective than a control fluoride toothpaste in reducing dentine hypersensitivity pain, with a relief lasting for 12 hours. A particular point of view is given by the work of Wood et al. [31], studying what happens into interproximal areas treated with a toothpaste consisting of the same molecules: enamel specimens treated with the calcium silicate phosphate toothpastes softened less than those treated with control fluoridated or non-fluoride toothpastes.
If a lot is known about calcium silicate, sodium phosphate and fluoride based toothpaste, the same can not be assessed for gel serum with the aforementioned compounds. Most of the studies concern the system composed by toothpaste and gel serum. Actually, as claimed by Hornby et al. [32], the system made up of toothpaste and serum based on these minerals was able to improve the enamel microhardness after 3 days of use. In line with these results, Joiner et al. [33] found out that the same system of toothpaste and serum was able to re-harden previously acid-challenged enamel to a greater extent than other toothpastes. Similar results are provided by the work of Jones et al. [34], the combination of these toothpaste and serum increased the remineralization in the interproximal surfaces more than other control toothpaste with or without fluoride. However, Zanatta et al. [35] assessed that the calcium silicate/sodium phosphate toothpaste and serum increased microhardness of eroded dentin, but they did not significantly reduce enamel and dentin loss compared to the non-fluoride control toothpaste.
Considering the previous background, the effectiveness of a calcium silicate, sodium phosphate and fluoride gel alone was investigated for the first time in the current study. Our results demonstrate that the present serum had the capacity to improve the shade variation of worn enamel for all the acid solutions tested. In addition, the studied gel proved to reestablish a smooth regular surface in every groups. This dual-phase product is based on NR-5™ technology, which increase the natural mineralization of human saliva by supplying additional calcium through the release of calcium silicate and phosphate from sodium phosphate salts. This phenomenon helps the nucleation of HAP [18] by establishing a biomimetic remineralization. In other words, calcium silicate, sodium phosphate and fluoride gel is able to mimic the natural aggregation of the HAP on the enamel surface. The study was conducted in a laboratory setting, therefore further studies are needed to quantify the effectiveness of the serum and gel in a clinical setting. The present in vitro results on erosion with acid or carbonated drinks could be translated to the application of this remineralizing agents on patients with systemic disorders as GERD, bulimia, bariatric surgery, in order to prevent or treat erosive damage of the enamel [36]. The results suggested that remineralizing agents containing calcium silicate, sodium phosphate and fluoride could be a promising new treatment for patients with systemic disorders that are associated with erosive tooth wear. Ulterior in vivo studies have to be conducted to evaluate the long-term protective effects of remineralizing biocompatible and biomimetic substances.
5. Conclusions
Enamel erosion is a continuous phenomenon presenting every time we eat and it can be enhanced by markedly acid food and beverages. Acidic tooth wear leads to enamel discoloration and softening, visible as a yellowish, chalky and rough surface, up to the exposition of the underlying dentin. With the limitations of the study, biocompatible and biomimetic minerals serum based on calcium silicate, sodium phosphate and fluoride is able to reverse teeth erosion, improve the color and restore the smoothness of dental enamel after 3 times of use. By conducting further in vivo studies, a better understanding can be gained about the lasting benefits of remineralizing biocompatible and biomimetic compounds.
Author Contributions
Conceptualization, S.D.; methodology, S.D.; software, J.R.; validation, J.R., M.D. and S.D.; investigation, S.D.; resources, G.V.; data curation, S.D. and J.R.; writing—original draft preparation, S.D. and G.V.; writing—review and editing, S.D., G.V. and M.D.; supervision, M.D., S.D.; project administration, M.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Imfeld T. Dental erosion. Definition, classification and links. Eur J Oral Sci. 1996 Apr;104(2 ( Pt 2)):151-5. [CrossRef]
- D’Agostino S, Bissoli A, Caporaso L, Iarussi F, Pulcini R, et al. Gastroesophageal reflux disease and dental erosion: A modern review. Japanese J Gastroenterol Res 2021, 1, 1003.
- Couselo M, Ibáñez V, Ortolá P, Carazo E, Valdés E, Vila JJ. Adequate timing of diagnostic tests for gastroesophageal reflux in children with esophageal atresia. Cir Pediatr. 2023 Jan 1;36(1):5-11. English, Spanish. [CrossRef]
- Monda M, Costacurta M, Maffei L, Docimo R. Oral manifestations of eating disorders in adolescent patients. A review. Eur J Paediatr Dent. 2021 Jun;22(2):155-158. [CrossRef]
- Jaeggi T, Lussi A. Prevalence, incidence and distribution of erosion. Monogr Oral Sci. 2014;25:55-73. [CrossRef]
- Lussi A, Carvalho TS. Erosive tooth wear: a multifactorial condition of growing concern and increasing knowledge. Monogr Oral Sci. 2014;25:1-15. [CrossRef]
- Devadiga D, Shetty P, Hegde MN. Characterization of dynamic process of carious and erosive demineralization - an overview. J Conserv Dent. 2022 Sep-Oct;25(5):454-462. [CrossRef]
- Lussi A, Schlueter N, Rakhmatullina E, Ganss C. Dental erosion--an overview with emphasis on chemical and histopathological aspects. Caries Res. 2011;45 Suppl 1:2-12. [CrossRef]
- Bartlett DW, Evans DF, Smith BGN: The relationship between gastrooesophageal reflux disease and dental erosion. J Oral Rehabil 1996, 23, 289–297. [CrossRef] [PubMed]
- Laserre JF: Recherches sur l’usure dentaire et evaluation «in vitro» de biomateriaux restaurateurs avec le simulateur d’usure UVSB2, thése pour le doctorat en Sciences Odontologiques Université de Bordeaux 2, 2003.
- Larsen MJ: Dissolution of enamel. Scand J Dental Res 1973, 81, 518–522.
- Lussi A, Jaeggi T, Scharer S: The influence of different factors on in vitro enamel erosion. Caries Res 1993, 27, 387–393. [CrossRef] [PubMed]
- Gambon DL, Brand HS, Veerman EC. Dental erosion in the 21st century: what is happening to nutritional habits and lifestyle in our society? Br Dent J. 2012, 213, 55–57. [CrossRef] [PubMed]
- Alsunni, AA. Energy Drink Consumption: Beneficial and Adverse Health Effects. Int J Health Sci. 2015, 9, 468–474. [Google Scholar] [CrossRef]
- Ghozayel M, Ghaddar A, Farhat G, Nasreddine L, Kara J, Jomaa L. Energy drinks consumption and perceptions among University Students in Beirut, Lebanon: A mixed methods approach. PLoS One 2020, 15, e0232199. [CrossRef] [PubMed]
- Saads Carvalho T, Lussi A. Chapter 9: Acidic Beverages and Foods Associated with Dental Erosion and Erosive Tooth Wear. Monogr Oral Sci 2020, 28, 91–98.
- Kitchens M, Owens BM. Effect of carbonated beverages, coffee, sports and high energy drinks, and bottled water on the in vitro erosion characteristics of dental enamel. J Clin Pediatr Dent. 2007 Spring;31(3):153-9. [CrossRef]
- Parker, A. S., Patel, A. N., Al Botros, R., Snowden, M. E., McKelvey, K., Unwin, P. R., et al. (2014). Measurement of the efficacy of calcium silicate for the protection and repair of dental enamel. Journal of Dentistry, 42, S21–9. [CrossRef]
- Sun, Y., Li, X., Deng, Y., Sun, J. N., Tao, D., Chen, H., et al. (2014). Mode of action studies on the formation of enamel minerals from a novel toothpaste containing calcium silicate and sodium phosphate salts. Journal of Dentistry, 42, S30–S38. [CrossRef]
- Ionta, F. Q., dos Santos, N. M., Mesquita, I. M., Dionísio, E. J., Cruvinel, T., Honório, H. M., et al. (2019). Is the dentifrice containing calcium silicate, sodium phosphate, and fluoride able to protect enamel against chemical mechanical wear? An in situ/ex vivo study. Clinical Oral Investigations, 1–8. [CrossRef]
- Stookey GK. The effect of saliva on dental caries. J Am Dent Assoc. 2008 May;139 Suppl:11S-17S. [CrossRef]
- Cochrane NJ, Reynolds EC: Calcium phosphopeptides – mechanisms of action and evidence for clinical efficacy. Adv Dent Res 2012, 24, 41–47. [CrossRef] [PubMed]
- Cochrane NJ, Cai F, Huq NL, Burrow MF, Reynolds EC: New approaches to enhanced remineralization of tooth enamel. J Dent Res 2010, 89, 1187–1197. [CrossRef] [PubMed]
- Mattousch TJ, van der Veen MH, Zentner A. Caries lesions after orthodontic treatment followed by quantitative light-induced fluorescence: a 2-year follow-up. Eur J Orthod. 2007 Jun;29(3):294-8. [CrossRef]
- van der Veen MH, Mattousch T, Boersma JG. Longitudinal development of caries lesions after orthodontic treatment evaluated by quantitative light-induced fluorescence. Am J Orthod Dentofacial Orthop. 2007 Feb;131(2):223-8. [CrossRef]
- Dowd, F.J. Saliva and dental caries. Dent Clin North Am 1999, 43, 579–597. [Google Scholar] [CrossRef] [PubMed]
- Silverstone LM: Remineralization of human enamel in vitro. Proc R Soc Med 1972, 65, 906–908.
- Philip N. State of the Art Enamel Remineralization Systems: The Next Frontier in Caries Management. Caries Res. 2019;53(3):284-295. [CrossRef] [PubMed]
- Li H, Liu W, Zhou HJ, Sun Y, Zhang M, Wang J, Limer A, Owens G, Joiner A. In vitro dentine tubule occlusion by a novel toothpaste containing calcium silicate and sodium phosphate. J Dent. 2020;103S:100024. [CrossRef] [PubMed]
- Seong J, Newcombe RG, Matheson JR, Weddell L, Edwards M, West NX. A randomised controlled trial investigating efficacy of a novel toothpaste containing calcium silicate and sodium phosphate in dentine hypersensitivity pain reduction compared to a fluoride control toothpaste. J Dent. 2020 Jul;98:103320. [CrossRef] [PubMed]
- Wood NJ, Jones SB, Chapman N, Joiner A, Philpotts CJ, West NX. An interproximal model to determine the erosion-protective effect of calcium silicate, sodium phosphate, fluoride formulations. Dent Mater. 2018 Feb;34(2):355-362. [CrossRef] [PubMed]
- Hornby K, Ricketts SR, Philpotts CJ, Joiner A, Schemehorn B, Willson R. Enhanced enamel benefits from a novel toothpaste and dual phase gel containing calcium silicate and sodium phosphate salts. J Dent. 2014 Jun;42 Suppl 1:S39-45. [CrossRef] [PubMed]
- Joiner A, Schäfer F, Naeeni MM, Gupta AK, Zero DT. Remineralisation effect of a dual-phase calcium silicate/phosphate gel combined with calcium silicate/phosphate toothpaste on acid-challenged enamel in situ. J Dent. 2014, 42 (Suppl. 1), S53–S59. [CrossRef] [PubMed]
- Jones SB, Davies M, Chapman N, Willson R, Hornby K, Joiner A, West NX. Introduction of an interproximal mineralisation model to measure remineralisation caused by novel formulations containing calcium silicate, sodium phosphate salts and fluoride. J Dent. 2014, 42 (Suppl. 1), S46–S52. [CrossRef] [PubMed]
- Zanatta RF, Ávila DMDS, Maia MM, Viana ÍEL, Scaramucci T, Torres CRG, Borges AB. Protection of calcium silicate/sodium phosphate/fluoride toothpaste with serum on enamel and dentin erosive wear. J Appl Oral Sci. 2021 Oct 1;29:e20210081. [CrossRef]
- Moras CG, Acharya SR, Adarsh UK, Unnikrishnan VK. Regenerative biomineralization potential of commercially available remineralizing agents as a preventive treatment approach for tooth erosion - An in vitro laser-induced breakdown spectroscopy analysis. J Conserv Dent. 2023 Mar-Apr;26(2):165-169. [PubMed]
Figure 1.
Portable pHmeter.
Figure 2.
Ovine teeth immersed in different fluids. A, lemon juice. B, energy drink. C, coffee. D, tea. E, control group in physiologic.
Figure 2.
Ovine teeth immersed in different fluids. A, lemon juice. B, energy drink. C, coffee. D, tea. E, control group in physiologic.
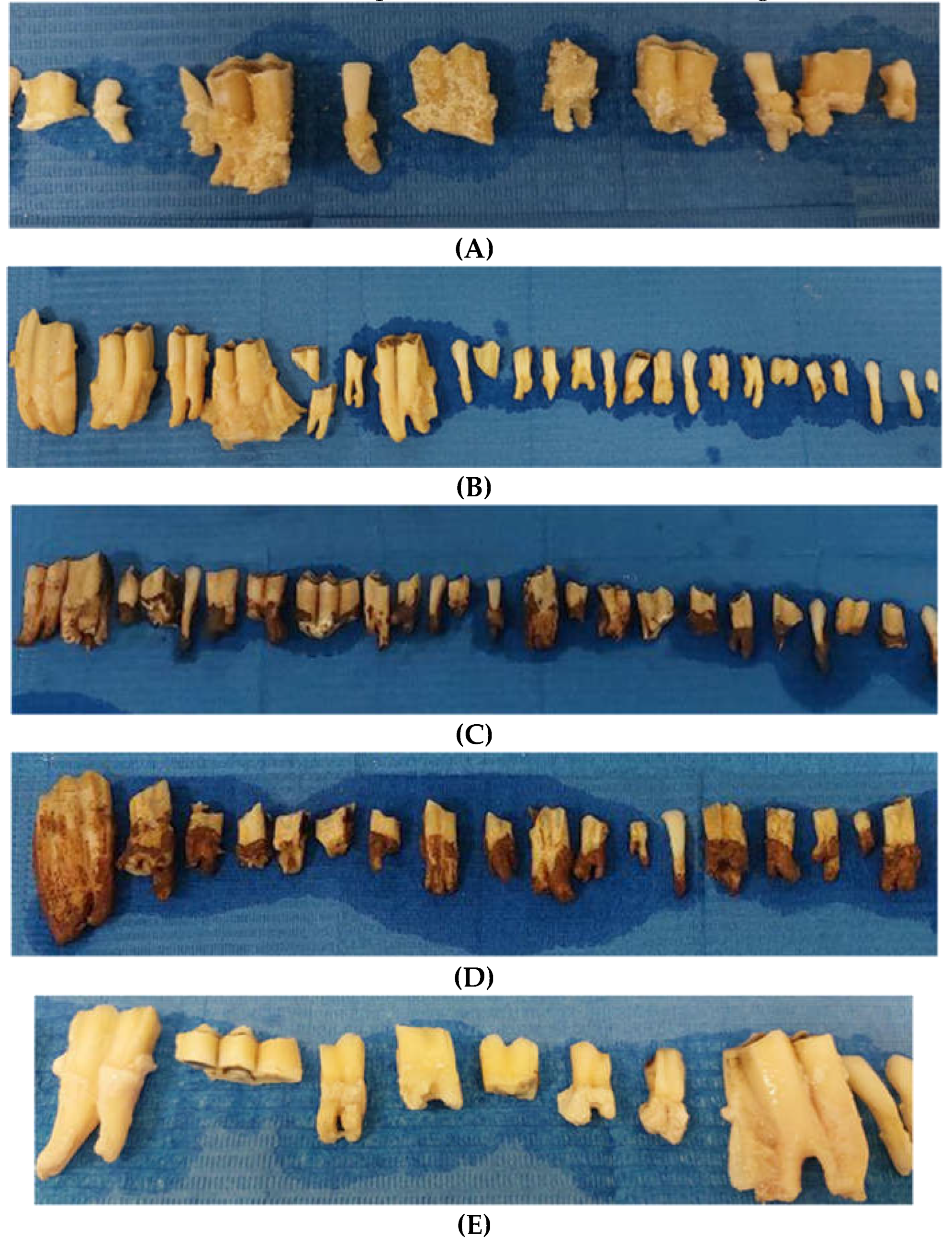
Figure 3.
A, Biocompatible minerals serum, external pack. B, Tubes. On the left, tube with NR-5™ serum based on calcium phosphate, sodium silicate and fluoride 1450 ppm. On the right, tube with activator gel.
Figure 3.
A, Biocompatible minerals serum, external pack. B, Tubes. On the left, tube with NR-5™ serum based on calcium phosphate, sodium silicate and fluoride 1450 ppm. On the right, tube with activator gel.
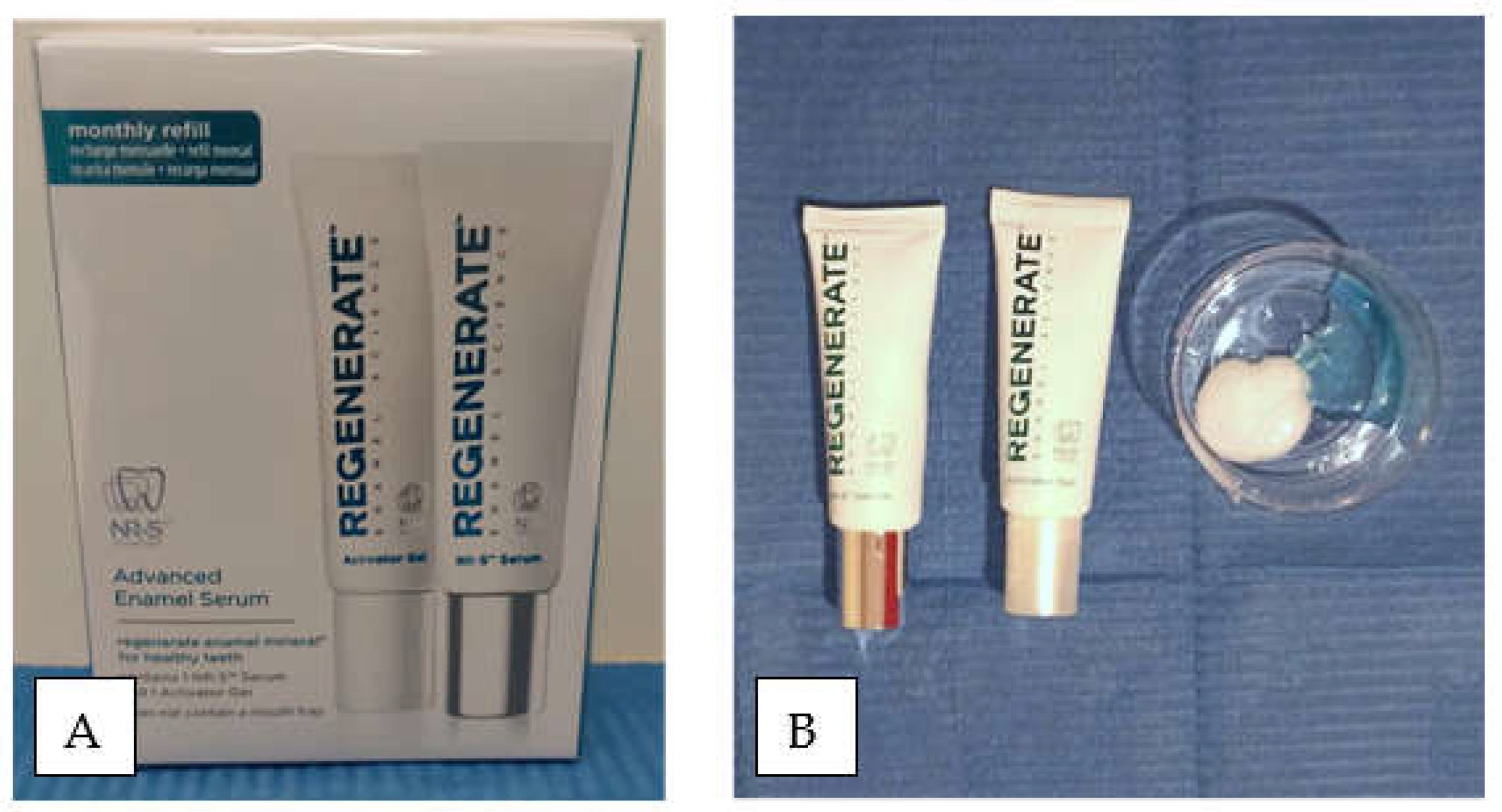

Table 1.
pH of the five solutions used.
| Solution | pH |
|---|---|
| Lemon juice | 3.1 |
| Energy drink | 3.3 |
| Coffee | 5 |
| Tea | 4.9 |
| Physiologic solution | 5.8 |
Table 2.
Composition of the two tubes. A, tube with NR-5. B, tube with activator gel.
| Tube | Composition |
|---|---|
| Tube A | Water, Glycerin, Calcium Silicate, PEG 8, Hydrated Silica, Trisodium, Phosphate, Sodium Phosphate, PEG-60, Sodium Laury Sulfate, Sodium Monofluorophosphate (1450 ppm), flavour, Sythetic Fluorphlogopite, Sodium Saccharin, Polyacrylic Acid, Tin Oxide, Limonene |
| Tube B | Water, Glycerin, Cellulose Gum, Sodium Fluoride, Benzyl Alcohol, Ethylhexylglycerin, Phenoxyethanol, Sodium Fluoride (1450 ppm) |
Table 3.
Main results for color. SD: standard deviation.
| Solution | Mean(SD)/Median* | t/Z* | p-value | |
|---|---|---|---|---|
| Lemon juice | Pre | 8.85(4.45) | 7.8 | 0.000 a |
| Post | 4.93(6.66) | |||
| Energy drink | Pre | 9* | 4.204* | 0.000 a |
| Post | 8* | |||
| Coffee | Pre | 13* | 4.159* | 0.000 a |
| Post | 13* | |||
| Tea | Pre | 10* | 3.886* | 0.000 a |
| Post | 8* |
a: The results are significant at 0.05 level, therefore they were strongly relevant. *: Wilcoxon Signed Rank test results.
Table 4.
Chi-square contingency table test for independence. OP, opaque. CHA, chalky. RO, rough. SM, smooth. ZWE, zones without enamel. OZ, opaque zones. CZ, chalky zones. RZ, rough zones. SZ, smooth zones.
Table 4.
Chi-square contingency table test for independence. OP, opaque. CHA, chalky. RO, rough. SM, smooth. ZWE, zones without enamel. OZ, opaque zones. CZ, chalky zones. RZ, rough zones. SZ, smooth zones.
| OP | CHA | RO | SM | ZWE | OZ | CZ | RZ | SZ | Total | |
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | 89 | 20 | 50 | 0 | 5 | 15 | 11 | 23 | 1 | 214 |
| Post | 52 | 6 | 12 | 28 | 0 | 28 | 3 | 8 | 24 | 161 |
| Total | 141 | 26 | 62 | 28 | 5 | 43 | 14 | 31 | 25 | 375 |
| Chi Square | 105.066 | |||||||||
| df | 8 | |||||||||
| p-value | 3.92*10-19 a | |||||||||
a) Results are significant at 0.05 level, therefore they were strongly relevant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



