
Submitted:
17 August 2023
Posted:
18 August 2023
You are already at the latest version
Abstract
Introduction: Prostate cancer (PCa) is one of the deadliest and most common causes of malignancy and death in men worldwide, more specifically with higher prevalence and mortality in developing countries. Factors such as age, family history, race and certain genetic mutations are some of the factors contributing to the occurrence of PCa in men. The recent advances in technology and algorithms gave rise to the computer-aided diagnosis (CAD) of PCa. With the availability of medical image datasets and emerging trends in state-of-the-art machine and deep learning techniques, there is a growth in recent related publications.
Materials and Methods: In this study, we present a systematic review of PCa diagnosis with medical images using machine learning and deep learning techniques. We conducted a thorough review through relevant studies indexed in four databases (IEEE, PubMed, Springer and ScienceDirect) using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. With well-defined search terms, a total of 608 articles were identified and 77 met the final inclusion criteria. Key elements in the included papers were presented and conclusions were drawn from them.
Results: Findings showed that the United States has the most research in PCa diagnosis with machine learning, Magnetic Resonance Images are the most used datasets and transfer learning is the most used method of diagnosing PCa in recent times. In addition, some available PCa datasets and some key considerations for choice of loss function in the deep learning models were presented. The limitations and lessons learnt were discussed and some key recommendations were made.
Conclusion: The discoveries and the conclusions of this work have been organized so as to enable researchers in the same domain to use this work and make crucial implementation decisions.
Keywords:
machine learning
; deep learning
; prostate cancer
; review
; PRISMA
; CNN
1. Introduction
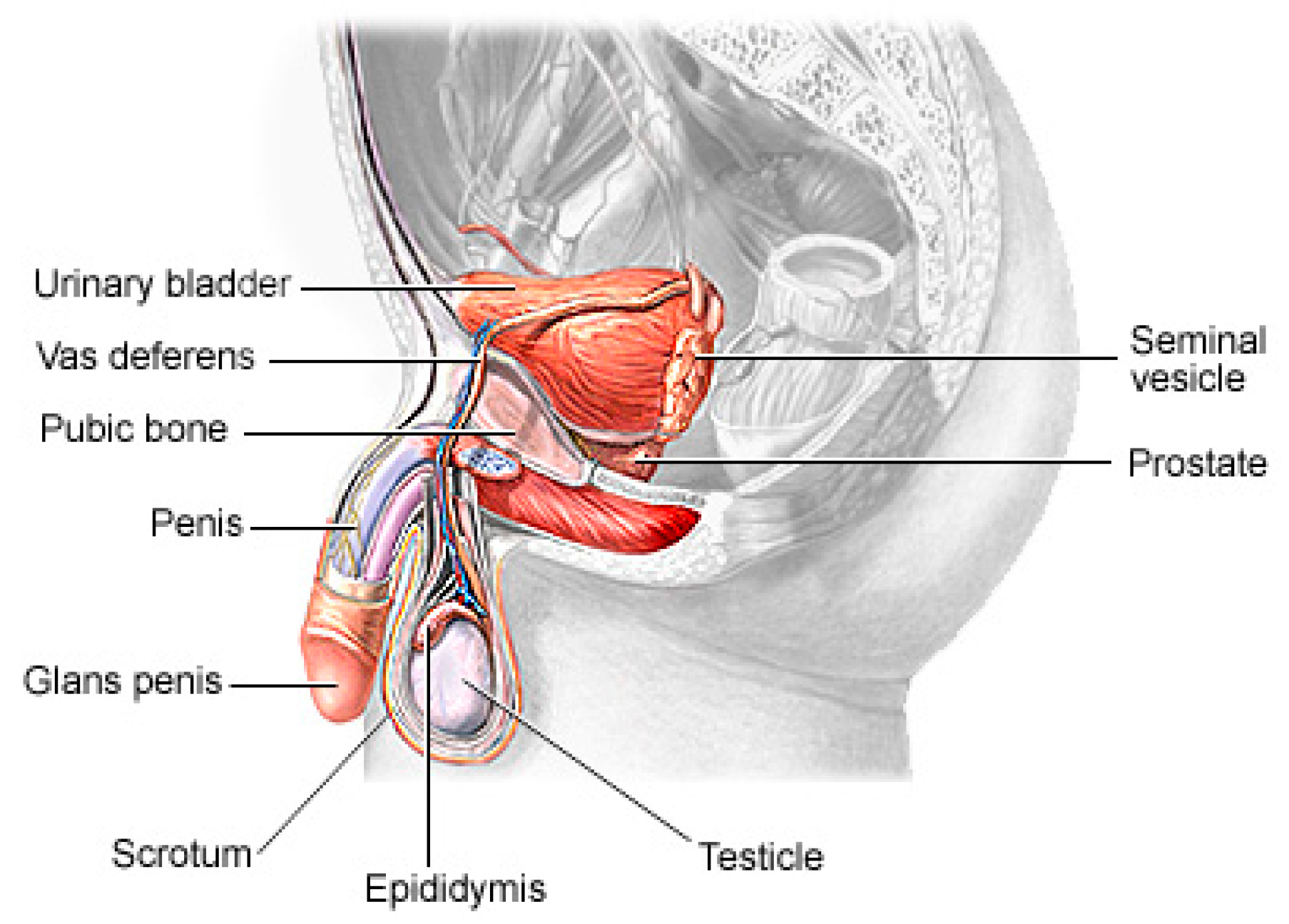
Prostate cancer (PCa) is the second most lethal and prevalent noncutaneous tumor in males globally [1]. Global Cancer statistics show that in 2018, there were more than 1.2 million new instances of PCa, which resulted in more than 350,000 fatalities[2]. By 2030, it is anticipated that there would be 11 million cancer deaths, a record high[3]. Worldwide, this type of cancer affects many males, with developing and underdeveloped countries having higher prevalence and mortality rates[4]. PCa is a type of cancer that develops in the prostate gland, a small walnut-shaped gland located below the bladder in men[5]. The male reproductive system contains the prostate, a small gland that is located under the bladder and in front of the rectum. It surrounds the urethra, the tube that carries urine from the bladder out of the body. The primary function of the prostate is to produce and secrete a fluid that makes up a part of semen, the fluid that carries sperm during ejaculation[6]. The development of PCa in an individual can be caused by a variety of circumstances including age (older men are more likely to develop prostate cancer), family history (having a close relative who has prostate cancer increases the risk), race (African-American males are more likely to develop prostate cancer), and specific genetic mutations[7,8].
Figure 1.
The Physiology of a Human Prostate.
PCa, in its early stages, is a confusable disease which makes it relatively more difficult to diagnose. Its early symptoms include, among others, urinary issues (difficulty urinating, weak urine flow, frequent urination, especially at night, and the sensation that the bladder is not empty), bloody urine, bloody semen, erectile dysfunction, pelvic pain, lower back pain, hip pain, or thigh pain, and fatigue brought on by an insufficient level of erythrocytes. Over 33,000 deaths and almost 200,000 new cases were reported in the United States in 2020[9]. Several studies have also identified older men as the susceptible group. Older men have been reported as the vulnerable group in many research works. According to statistics, one in ten men will develop PCa at some point in their lives. According to studies from the American Cancer Society from 2022, PCa is extremely uncommon in men under the age of 40 and is found in men 65 years of age and above in 60% of verified PCa cases. Therefore, all data point to PCa being one of the worst diseases affecting men[10,11] thereby making all scientific and medical research works to reduce its fatality justifiable.
The recent advances in sophisticated computers and algorithms recent decades have paved the way for improved PCa diagnosis and treatment[12]. Computer-aided diagnosis (CAD) refers to the use of computer algorithms and technology to assist healthcare professionals in the prognosis and diagnosis of patients[13]. CAD systems are designed to serve as Decision Support (or Expert) Systems which analyze medical data, such as images or test results, and provide experts with additional information or suggestions to aid in the interpretation and diagnosis of various medical conditions. They are commonly used in medical imaging fields to detect anomalies or assist in the interpretation and analysis of medical images such as X-rays, Computed Tomography (CT) scans, Magnetic Resonance Imaging (MRI) scans and mammograms[14]. These systems use pattern recognition, machine learning, and deep learning algorithms to identify specific features or patterns that may indicate the presence or absence of a disease or condition[15]. It can also help radiologists by highlighting regions of interest (ROIs) or by providing quantitative measurements for further analysis. Soft computing techniques play a major role in decision making across several sectors of the field of medical image analysis[16,17]. Deep learning, a branch of Artificial Intelligence, has shown promising performance in the identification of patterns and classification of medical images[18,19].
Several studies have investigated some CAD solutions to identify PCa by analyzing medical images as a decision support tool for an effective and efficient diagnosis process, easing these tasks as well as reducing human errors and effort. Also, there are avalanche of review and survey papers published in this area which summarized and organized recent works and aid understanding of the state-of-the-art in this field, discussing the trends and recommending future directions.
This study presents a guided systematic review of the application of these ML and DL techniques for the diagnosis of PCa, especially in their applications in the process of segmentation, cancer detection, assessment of lesion aggressiveness, local staging, and pre-treatment assessment among others. We present, evaluate and summarize various studies from our selected databases, give insights into the use of different datasets and different imaging modalities, explore the trends in this area, analyze the state-of-the-art deep learning architectures, provide derivations, taxonomies and summaries based on these observations and some limitations, open challenges and possible future directions. Machine learning specialists, medics and decision makers can benefit from this study vis-a-vis what machine learning model is appropriate for what characteristics of dataset as well as gain insights into future directions for research and development. Figure 2 shows the trend of publications on the subject matter since the previous ten years till date which is obtained from a tailored search on Google Scholar (https://scholar.google.com) with the query: ‘machine learning deep learning "prostate cancer" -review’ and filtered by year.
Figure 3 shows the trend of review papers publication on the subject matter over the previous ten years till date. This is obtained from a tailored search on Google Scholar (https://scholar.google.com) with the query: ‘machine learning deep learning intitle:"prostate cancer" intitle:"review"’ and filtered by year.
These two figures show that although there is an increasing wave of research in this subject matter, there are not enough systematic review studies done to match up with this ever-rising trend. This justifies that this study is highly relevant given the experiment to review study ratio in the last decade.
1.1. Related Works
Many review and survey papers have investigated the application of machine learning and deep learning models to support the diagnosis and decision-making process of PCa. These papers have addressed the use of several deep learning models on various datasets and image modalities and presented the findings of authors in those respective papers. Table 1 summarizes the review papers identified as relevant to our aim in this study as well as their findings so far.
Review articles have done tremendous work in the investigation of the role of ML and DL models for clinically significant prostate cancer (csPCa). However, some limitations are identified. First, review articles which met most authors’ final inclusion criteria are very small compared to the hundreds of articles released on a weekly basis. Second, most studies focused on a single image modality whereas there are other imaging modalities that should be included. Some studies also used a single database as reference search, which we know cannot provide a representative study of the subject matter. Also, some studies did not discuss major considerations such as choice of dataset, choice of image modalities, choice of ML/DL models, hyperparameter tuning and optimization among others. These are some of the lapses our work seeks to address.
1.2. Scope of Review
This study aims to address the following research questions in the context of diagnosing PCa with ML and DL techniques. This can be utilized by researchers and medics to obtain a comprehensive view of the evolution of these techniques, datasets, imaging modalities and the effectiveness of these techniques in the effective PCa diagnosis. The following research questions (RQs) are considered in this study:
| RQ1: | What are the trends and evolutions of this study? |
| RQ2: | What ML and DL models are used for this study? |
| RQ3: | What datasets are publicly available? |
| RQ4: | What are the necessary considerations for application of these artificial intelligence (AI) techniques in PCa diagnosis? |
| RQ5: | What are the limitations so far identified by authors? |
| RQ6: | What are the future directions for this research? |
We also investigated the verifiability of these studies by checking whether a medic or radiologist was one of the contributors or the results of the model was stated to have been verified by one. We also included citation metric and impact index in our work to measure the impact of the reviewed articles.
1.3. High-Level Structure of this Study
This study is organized as indicated in Figure 4. The first section presents a general overview of this study, related review works and the scope of the study. Section 2 discusses the method of review employed in this paper. Section 3 engages in preliminary discussions concerning imaging modalities, risks of PCa and general deep learning architecture for PCa diagnosis. Section 4 presents a summary table of papers that meet the inclusion criteria in this study with comparative analysis of trends, datasets, methods, techniques and journals.
Section 5 discusses some popular deep learning approaches and gives guidelines for the choice of individual techniques and optimization considerations as well as the choice of loss function. Section 6 presents discussion of findings We also discussed the identified limitations, lessons learned and recommendations. The final section concludes this study.
2. Methods
This review paper explores, investigates, evaluates and summarizes findings in literature which discussed PCa diagnosis with ML and DL techniques and image datasets; thereby equipping readers with a wholistic view of the subject matter, summaries of different techniques, datasets and models as well as various optimization techniques available for model training. Authors will conduct various possible comparisons and discuss challenges, limitations and suggest future work directions and areas of improvement. The Preferred Reporting Items for Systematic Reviews and Meta Analysis (PRISMA)[27] guideline was used for conducting this review.
2.1. Database Search and Eligibility Criteria
In this systematic review, we constructed a search strategy and used it to scout four major databases (ScienceDirect, PubMed, Springer and IEEE) in search of up-to-date, relevant research publications on the research study of using ML and DL models to clinically diagnose csPCa. Google Scholar (https://scholar.google.com) was used as the secondary resource used in the preliminary and expository discussions. The timeframe for the investigation is year 2015–2023. These sources were selected because of their extensive publications of research in this area of study.
2.2. Review Strategy
The review process involves study selection, research design, search strategy, information sources, and data collection techniques. The evaluation of papers that complied with the initial inclusion and exclusion criteria. Editorials, comments, letters, preprints, databases not included in the four categories, and other types of manuscripts were not accepted. The search strategy is composed as follows: (a) construct search terms by identifying major keywords, required action, and expected results; (b) determine the synonyms or alternative words for the major keywords; (c) establish exclusion criteria to make exclusions in the course of search; and (d) apply Boolean operators to construct the required search term.
- Results for (a): Deep Learning Machine Learning Significant Prostate Cancer Artificial Intelligence Prediction Diagnosis
- Results of (b): Prediction/Diagnosis/Classification Machine/Deep Prostate Cancer/PCa/csPCa
- Results for (c): review, systematic review, preprint, risk factor, treatment, biopsy, gleason grading, DRE
- Result (d): a, b, c combined using AND OR.
In this review, publications were chosen from the peer-reviewed literature by conducting a search using the generated search phrase on Science Direct, Springer, IEEE, and PubMed. Conference proceedings, journals, book chapters, and whole books are all examples of vetted resources. The initial number of results returned was 608; of those, 543 fulfilled the initial selection criterion and 77 fulfilled the final requirements. The studies were appropriately grouped. Figure 5 shows the preferred reporting items for systematic reviews and meta-analyses for scoping review (PRISMA-ScR) flowchart for study selection.
Our exclusion requirements include duplicates, preprints, review articles, opinions and commentaries, editorials, non-English paper, irrelevant title, irrelevant content, irrelevant techniques and date of publication.
2.3. Characteristics of Studies
The characteristics of the 77 reviewed articles is given in Figure 6. The outer later is the distribution of the image modalities, followed by the article type, database and total number of article reviewed.
2.4. Quality Assessment
Most studies failed to satisfy standards in at least one of the six quality criteria examined. Limited sample size, an inadequate scientific strategy and failure to disclose results for computational techniques were the most frequently observed issues regarding lack of quality throughout the investigations.
2.5. Data Sources and Search Strategy
We searched the four selected databases for studies published before July 2023 but not earlier than 2015. Keywords from subject headings or titles or abstracts of the studies were searched for with the help of Boolean operators (and, or) with language restricted to English. In addition, we reviewed the reference lists of primary studies and review articles.
2.6. Inclusion and Exclusion Criteria
Research papers in which ML and DL approaches were applied to predict and characterize PCa were reported. The included publications must document the AI technique(s) used and PCa image analysis problem addressed in the article. Articles dealing with PCa key datasets and associated analysis techniques were also included in the study selection. Articles in preprints, not published in our selected databases, opinions, commentaries and non-English papers were all excluded. Editorials, narrative review articles, case studies, conference abstracts, and duplicate publications were all discarded from the analysis. Articles which discuss similar techniques and results were ignored.
2.7. Data Extraction
The full texts of the qualified papers chosen for review were acquired, and the reviewers independently collected all study data, resolving disagreements by consensus. The references, year of publication, study setting, ML approach, the imaging modality used or recommended, performance measures used, and accuracy attained were all extracted for every included paper and comparative analyses were done on the extracted dataset were necessary.
3. Preliminary Discussions
3.1. Imaging Modalities
Prostate imaging refers to various techniques and procedures used to visualize the prostate gland for diagnostic and treatment purposes. These imaging methods help in evaluating the size, shape, and structure of the prostate, as well as detecting any abnormalities or diseases, such as prostate cancer[28,29] and they include Transrectal Ultrasound (TRUS)[30], Magnetic Resonance Imaging (MRI)[31], Computed Tomography (CT)[32], Prostate-Specific Antigen (PSA)[33], Prostate-Specific Membrane Antigen (PET/CT)[34] and bone scans[35]. The TRUS involves inserting a small probe into the rectum, which emits high-frequency sound waves to create real-time images of the prostate gland. TRUS is commonly used to guide prostate biopsies and assess the size of the prostate[30,36]. MRI, one of the most common prostate imaging methods, uses a powerful magnetic field and radio waves to generate detailed images of the prostate gland. It can provide information about the size, location, and extent of tumors or other abnormalities. Multiparametric MRI (mpMRI) combines different imaging sequences to improve the accuracy of prostate cancer detection[37,38]. CT scan uses X-ray technology to produce cross-sectional images of the prostate gland. It may be utilized to evaluate the spread of prostate cancer to nearby lymph nodes or other structures. PSMA PET/CT imaging is a relatively new technique that uses a radioactive tracer targeting PSMA, a protein highly expressed in prostate cancer cells[39]. It provides detailed information about the location and extent of prostate cancer, including metastases. Bone scans are often performed in cases where prostate cancer has spread to the bones. A small amount of radioactive material is injected into the bloodstream, which is then detected by a scanner[35]. The scan can help identify areas of bone affected by cancer. PSA (density mapping) combines the results of PSA blood tests with transrectal ultrasound measurements to estimate the risk of prostate cancer. It helps assess the likelihood of cancer based on the size of the prostate and the PSA level[40]. The choice of imaging technique depends on various factors, including the specific clinical scenario, availability of resources, and the goals of the evaluation[41,42].
3.2. Risks of PCa
The risk of PCa varies in men depending on several factors and identifying these factors can aid in the prevention and early detection, personalized healthcare, research and public health policies, genetic counseling and testing and lifestyle modifications. The most common clinically and scientifically verified risk factors include age, obesity and family history[43,44]. In low-risk vulnerable populations, risk factors such as benign prostatic hyperplasia (BPH), smoking, diet and alcohol consumption[45]. Although PCa is found to be rare in population below 40 years of age, an autopsy study on China, Israel, Germany, Jamaica, Sweden and Uganda showed that 30% of men in their fifties and 80% of men in their seventies had PCa[46]. Studies also found that genetic factors, lack of exercise, sedentary lifestyles are cogent risk factors of PCa, including obesity, elevated blood testosterone level[47–50]. Consumption of fruits and vegetables, frequency of high-fat meat consumption, level of Vitamin D in blood streams, cholesterol level, infections and other environmental factors are deemed to contribute to PCa occurrence in men[51,52].
3.3. Generic Overview of Deep Learning Architecture for PCa Diagnosis
Deep learning (DL) architectures have shown promising effectiveness and relative efficiency in PCa diagnosis due to their ability to analyze complex patterns and extract features from medical imaging data[17]. One commonly used deep learning architecture for cancer diagnosis is Convolutional Neural Networks (CNNs). CNNs are particularly effective in image analysis tasks, including medical image classification, segmentation, prognosis and detection[53]. Deep learning, given its ever-advancing variations, has recorded significant advancements in the analysis of cancer images including histopathology slides, mammograms, CT scans, and other medical imaging modalities. DL models can automatically learn hierarchical representations of images, enabling them to detect patterns and features indicative of cancer. They are also trained to classify PCa images into different categories or subtypes. By learning from labeled training data, these models can accurately classify new images, aiding in cancer diagnosis and subtyping[54].
Transfer learning is often employed in PCa image analysis. Pre-trained models, such as CNNs trained on large-scale datasets like ImageNet, are fine-tuned or used as feature extractors for PCa-related tasks. This approach leverages the learned features from pre-training, improving performance even with limited annotated medical image data. One image dataset augmentation framework is the Generative Adversarial Networks (GANs). They can generate realistic synthetic images, which can be used to supplement training data, enhance model generalization, and improve the performance of cancer image analysis models. The performance and effectiveness of deep learning models for PCa image analysis, however, depend on various factors, including the quantity and quality of labeled data, choice of architecture, training methodology, and careful validation on diverse datasets.
The key compartments in a typical deep CNN model for a PCa diagnosis as shown in Figure 7 include the convolutional layers, the pooling layers, the fully connected layers, the activation functions, the data augmentation and the attention mechanisms[55,56]. The convolutional layers are the fundamental building blocks of CNNs. They apply filters or kernels to input images to extract relevant features. These filters detect patterns at different scales and orientations, allowing the network to learn meaningful representations from the input data. The pooling layers downsample feature maps, reducing the spatial dimensions while retaining important features. Max pooling is a commonly used pooling technique, where the maximum value in each pooling window is selected as the representative value[57]. The fully connected layers are used at the end of CNN architectures to make predictions based on the extracted features. These layers connect all the neurons from the previous layer to the subsequent layer, allowing the network to learn complex relationships and make accurate classifications. Activation functions introduce non-linearity into the CNN architecture, enabling the network to model more complex relationships. Common activation functions include ReLU (Rectified Linear Unit), sigmoid, and tanh[58,59]. The transfer learning involves leveraging pre-trained CNN models on large datasets (such as ImageNet, ResNet, VGG-16, VGG-19, Inception-v3, ShuffleNet, EfficientNet, GoogleNet, ResNet-50, SqueezeNet etc.) and adapting them to specific medical imaging tasks. By using pre-trained models, which have learned general features from extensive data, the model construction time can be saved as well as computational resources and achieve good performance even on smaller medical datasets. Data augmentation techniques, such as rotation, scaling, and flipping, can be employed to artificially increase the diversity of the training data. Data augmentation helps improve the generalization of the CNN model by exposing it to variations and reducing overfitting. Attention mechanisms allow the network to focus on relevant regions or features within the image. These mechanisms assign weights or importance to different parts of the input, enabling the network to selectively attend to salient information[60,61].
4. Results
4.1. Review Summary of Relevant Papers
In this section, we present a table summarizing the core contents of papers which met our final inclusion criteria. The overall search captured 77 papers. The distribution of these publications among the four databases consulted is indicated in Table 2. PubMed serves as a mop-up database for the other three because some papers published elsewhere are also indexed in PubMed which form a part of removed duplicates explained on our PRISMA-ScR in Figure 5. The figure indicates that ScienceDirect has the most papers on the subject matter.
Table 3, Table 4, Table 5 and Table 6 highlight, for each database considered, the year in which the study was conducted, imaging modalities, the ML/DL models employed in the study, the problem addressed, the reported performance metrics and scores, the reported hyperparameter tuning, the country in which the study was conducted, the citations received for each paper as at the time of the study, whether the study was verified by a medical personnel or a radiologist, the number of observations or images considered for the study and the machine learning type whether supervised or unsupervised. The distribution of the included publications by the year in which the study was conducted as given in Figure 8 shows this study paid more attention to recent publications in the application of ML/DLs for PCa diagnosis.
Figure 9 shows the word cloud of topics of reviewed papers as generated by the word frequency. It gives a diagrammatic distribution of words as contained in the titles of included papers. It also shows that this study focuses on image-based detection of prostate cancer using deep learning techniques. Figure 10 shows the image modalities used in the diagnosis of PCa. Two papers used Computed Tomography (CT), 51 papers used Magnetic Resonance Images (MRI), 10 papers used UltraSound (US) while 14 papers used other imaging methods such as Whole Slide Images (WSI), histopathological images and biopsy images.
We also discovered from the review that the deep CNN is the most used ML/DL model spanning about 49 studies out of the 77 reviewed papers. It is also snoteworthy that transfer-learning-based DL architecture dominated the studies reviewed in this work with UNet, ResNet, GoogleNet and DenseNet being the topmost frameworks used in the analysis of PCa images. This is understandable because transfer learning offers a range of advantages, including reduced training time, improved generalization, effective feature extraction, addressing data imbalance, and facilitating domain adaptation. In the aspect of the performance of the models reported in the reviewed papers, the area under curve (AUC) is the most used metric, followed by accuracy and sensitivity. Most studies also used supervised learning (classification) methods. Images were manually annotated by medical professionals and radiologists for adequate performance evaluation of the models. However, absence of sufficient data for model training forced most authors into using secondary data and pretrained (transfer learning) models. In terms of countries where the reviewed studies were conducted, Figure 11 shows that USA has the highest number of studies. Table 7 shows the topmost impactful papers in our included papers. The impact index is calculated as in Equation 1 below:
This gives readers an overview of where to publish related research. It is evident from this table that Nature, Elsevier and Springer are top publishers to consider.
5. Discussion
5.1. Considerations for Choice of Deep Learning for PCa Image Data Analysis
The choice of what deep learning models to use for PCa detection in clinical images must be guided by the thorough exploration of their context of usages and associated strengths and weaknesses. Table 8 gives a summary of some specialties of each of the deep learning models to guide researchers’ choice of experimenting with PCa image datasets.
5.2. Considerations for Choice of Loss Functions for PCa Image Data Analysis
One specific and very important concept in the training of deep learning models for PCa diagnosis is the choice of loss functions which plays a significant role in training and optimizing the performance of the models[145,146]. Loss functions guide the optimization process by quantifying the discrepancy between the predicted output of the model and the ground truth labels or targets. The choice of loss function affects how the model learns and updates its parameters during training. A carefully selected loss function helps the model converge to an optimal solution efficiently[147]. Loss functions are also helpful in handling imbalance datasets – a common challenge where certain classes or abnormalities are rare compared to others. In such cases, loss functions need to address the imbalance to prevent the model from being biased towards the majority class. It also helps handling noise and outliers, in model interpretability as well as in gradient stability[148]. Although the choice of loss function depends largely on the specific task, the nature of the problem and the characteristics of the dataset, Table 9 summarizes some of the most used loss functions in deep learning and their best-suited context of usage. This does not replace the need for necessary experimentation and evaluation while choosing the applicable and appropriate loss function.
5.3. Prostate Cancer Datasets
Prostate cancer datasets consist of clinical and pathological information collected from patients diagnosed with prostate cancer and may include various types of data, such as patient demographics, clinical features, laboratory test results, imaging data (e.g., MRI, US or CT scans), histopathology slides (WSI), and treatment outcomes. They are useful for developing and evaluating machine learning and deep learning models for prostate cancer detection, diagnosis, prognosis, and treatment prediction. Table 10 presents some publicly available databases of PCa datasets.
5.4. Some Important Limitations Discussed in Literature
In this section, we harvest some crucial limitations identified by authors in the reviewed literature. This will aid readers on understanding the challenges encountered by researchers in conducting experiments in the application of deep learning to PCa diagnosis. Authors[89,96] identified limitations which included small and highly unbalanced dataset[98] with unavoidable undersampling. They also noted that in an ultrasound-guided biopsy’s registration, similar to other manual pathological-radiological strategies, personal bias of the regions of interest (ROIs) selection cannot be avoided. Study has also shown that when explainability and interpretability are taken into account in PCa prediction model construction, runtime becomes a critical issue and a conscious trade-off decision must be made[98]. CNN engines have also been reported to have poor interpretability. This is because the last convolutional layer of a classical CNN model contains the richest spatial and semantic information through multiple convolutions and pooling, and the next layer is the fully connected with SoftMax layers, which contain information that is difficult for humans to understand and difficult to visualize[104]. Some authors noted that models that behave like feed-forward, Long Short-Term Memory (LSTM) for instance, have a bit parity issue if not augmented with deep and transfer learning methods to classify PCa and non-PCa subjects[115]. In the summary tables, studies identified that multi-modal and multi-center study are said to deflect the performance of a model adjudged to be good enough in a unimodal and single-center study[124].
5.5. Lessons Learned and Recommendations
Deep learning application for prostate cancer detection has made significant advancements in recent years, and this study will expose reader to the trends in the techniques, models, datasets and some other critical considerations when venturing into similar studies. Data quality and availability has been a major limitation of existing studies. Data for PCa are scanty, often small and imbalanced leading to model’s generalizability and performance. Interpretability is of great concern in deep learning models especially because models reviewed in this study are meant to be utilized by medics and radiologists as a decision-support system (DSS). Deep learning models are often referred to as "black boxes" because they lack explainability. While they can accurately make predictions, understanding the underlying factors or features that contribute to those predictions can be difficult. This lack of interpretability is a significant limitation when it comes to clinical decision-making and explaining the rationale behind a model's predictions. Clinical validation, as seen in the summary tables, should be given attention in CAD-related studies. Many deep learning studies for prostate cancer focus on retrospective analyses using archival data. While these studies can provide valuable insights, there is a need for robust clinical validation to assess the real-world performance and impact of these models. Clinical validation requires multi-modal and multi-Centre applicability. Also, PCa datasets are often limited, and the complex nature of the disease makes it challenging to build models that can generalize effectively. Regularization techniques and careful validation are required to mitigate the risk of overfitting and improve generalization. Finally, for deep learning models to have a real impact on prostate cancer diagnosis, prognosis, or treatment, they need to be seamlessly integrated into the clinical workflow. This requires addressing practical challenges such as compatibility with existing electronic health record systems, establishing trust among healthcare professionals, and addressing regulatory and ethical considerations.
6. Conclusion
This study investigated wholistically the application of machine and deep learning models to prostate cancer detection and diagnosis. We presented also conducted a publisher-based comparison to give readers a view of some possible tendencies such as potential impact. Considerations regarding ML/DL models, PCa datasets and loss functions were also discussed. We found out that although the trend curves of systematic review (Figure 3) and actual experimental study (Figure 2) look similar, there is need for a thorough systematic study to investigate the trend, challenges and future directions in the application of ML/DL models to the ravaging disease. Although one of the advantages of deep learning models for segmentation is that they are fully automatic, requiring no intervention, studies showed that performance can be improved by having some method to improve initial organ localization which will allow for a relatively smaller, higher-resolution sub-volume to be extracted instead of using the entire image which contains noise. We conclude that transfer learning models are recommended for PCa diagnosis. This is because transfer learning offers significant advantages for prostate cancer diagnosis by leveraging pre-trained models, reducing data requirements, improving model performance, enabling faster training, capturing complex features, enhancing generalization, and expediting deployment in clinical practice. Clinical verification is also required in these studies to ensure the usability and responsibility of these studies. This will ensure that CAD-related studies do not end up just as papers but integrable into existing clinical systems.
References
- Litwin, M.S. and H.-J. Tan, The diagnosis and treatment of prostate cancer: a review. Jama, 2017. 317(24): p. 2532-2542.
- Rawla, P., Epidemiology of prostate cancer. World journal of oncology, 2019. 10(2): p. 63.
- Akinnuwesi, B.A.; Olayanju, K.A.; Aribisala, B.S.; Fashoto, S.G.; Mbunge, E.; Okpeku, M.; Owate, P. Application of support vector machine algorithm for early differential diagnosis of prostate cancer. J. Inf. Technol. Data Manag. 2023, 6, 1–12. [Google Scholar] [CrossRef]
- Ayenigbara, I.O. Risk-Reducing Measures for Cancer Prevention. Korean J. Fam. Med. 2023, 44, 76–86. [Google Scholar] [CrossRef]
- Musekiwa, A.; Moyo, M.; Mohammed, M.; Matsena-Zingoni, Z.; Twabi, H.S.; Batidzirai, J.M.; Singini, G.C.; Kgarosi, K.; Mchunu, N.; Nevhungoni, P.; et al. Mapping Evidence on the Burden of Breast, Cervical, and Prostate Cancers in Sub-Saharan Africa: A Scoping Review. Front. Public Heal. 2022, 10, 908302. [Google Scholar] [CrossRef]
- Walsh, P.C. and J.F. Worthington, Dr. Patrick Walsh's guide to surviving prostate cancer. 2010: Grand Central Life & Style.
- Hayes, R.B.; Pottern, L.M.; Strickler, H.; Rabkin, C.; Pope, V.; Swanson, G.M.; Greenberg, R.S.; Schoenberg, J.B.; Liff, J.; Schwartz, A.G.; et al. Sexual behaviour, STDs and risks for prostate cancer. Br. J. Cancer 2000, 82, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Plym, A.; Zhang, Y.; Stopsack, K.H.; Delcoigne, B.; Wiklund, F.; Haiman, C.; Kenfield, S.A.; Kibel, A.S.; Giovannucci, E.; Penney, K.L.; et al. A Healthy Lifestyle in Men at Increased Genetic Risk for Prostate Cancer. Eur. Urol. 2023, 83, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L.; Thomson, C.A.; Sullivan, K.R.; Howe, C.L.; Kushi, L.H.; Caan, B.J.; Neuhouser, M.L.; Bandera, E.V.; Wang, Y.; Robien, K.; et al. American Cancer Society nutrition and physical activity guideline for cancer survivors. CA: A Cancer J. Clin. 2022, 72, 230–262. [Google Scholar] [CrossRef] [PubMed]
- Wender, R.; Fontham, E.T.H.; Ermilo Barrera, E.B., Jr; Colditz, G.; Church, T.R.; Ettinger, D.S.; Etzioni, R.; Flowers, C.R.; Gazelle, G.S.; Kelsey, D.K.; et al. American Cancer Society lung cancer screening guidelines. CA: A Cancer J. Clin. 2013, 63, 106–117. [Google Scholar] [CrossRef]
- Wolf, A.M.D.; Wender, R.C.; Etzioni, R.B.; Thompson, I.M.; D'Amico, A.V.; Volk, R.J.; Brooks, D.D.; Dash, C.; Guessous, I.; Andrews, K.; et al. American Cancer Society Guideline for the Early Detection of Prostate Cancer: Update 2010. CA: A Cancer J. Clin. 2010, 60, 70–98. [Google Scholar] [CrossRef]
- Alkadi, R.; Taher, F.; El-Baz, A.; Werghi, N. A Deep Learning-Based Approach for the Detection and Localization of Prostate Cancer in T2 Magnetic Resonance Images. J. Digit. Imaging 2018, 32, 793–807. [Google Scholar] [CrossRef]
- Ishioka, J.; Matsuoka, Y.; Uehara, S.; Yasuda, Y.; Kijima, T.; Yoshida, S.; Yokoyama, M.; Saito, K.; Kihara, K.; Numao, N.; et al. Computer-aided diagnosis of prostate cancer on magnetic resonance imaging using a convolutional neural network algorithm. BJU Int. 2018, 122, 411–417. [Google Scholar] [CrossRef]
- Reda, I.; Shalaby, A.; El-Ghar, M.A.; Khalifa, F.; Elmogy, M.; Aboulfotouh, A.; Hosseini-Asl, E.; El-Baz, A.; Keynton, R. A new NMF-autoencoder based CAD system for early diagnosis of prostate cancer. 2016, 1237–1240. [CrossRef]
- Wildeboer, R.R.; van Sloun, R.J.; Wijkstra, H.; Mischi, M. Artificial intelligence in multiparametric prostate cancer imaging with focus on deep-learning methods. Comput. Methods Programs Biomed. 2020, 189, 105316. [Google Scholar] [CrossRef] [PubMed]
- Aribisala, B. and O. Olabanjo, Medical image processor and repository–mipar. Informatics in Medicine Unlocked, 2018. 12: p. 75-80.
- Shen, D.; Wu, G.; Suk, H.-I. Deep Learning in Medical Image Analysis. Annu. Rev. Biomed. Eng. 2017, 19, 221–248. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; An, X. A classification model for the prostate cancer based on deep learning. 2017, 1–6. [CrossRef]
- Wang, X.; Yang, W.; Weinreb, J.; Han, J.; Li, Q.; Kong, X.; Yan, Y.; Ke, Z.; Luo, B.; Liu, T.; et al. Searching for prostate cancer by fully automated magnetic resonance imaging classification: deep learning versus non-deep learning. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef]
- Suarez-Ibarrola, R.; Hein, S.; Reis, G.; Gratzke, C.; Miernik, A. Current and future applications of machine and deep learning in urology: a review of the literature on urolithiasis, renal cell carcinoma, and bladder and prostate cancer. World J. Urol. 2019, 38, 2329–2347. [Google Scholar] [CrossRef] [PubMed]
- Almeida, G.; Tavares, J.M.R. Deep Learning in Radiation Oncology Treatment Planning for Prostate Cancer: A Systematic Review. J. Med Syst. 2020, 44, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Khan, Z.; Yahya, N.; Alsaih, K.; Al-Hiyali, M.I.; Meriaudeau, F. Recent Automatic Segmentation Algorithms of MRI Prostate Regions: A Review. IEEE Access 2021, 9, 97878–97905. [Google Scholar] [CrossRef]
- Roest, C.; Fransen, S.J.; Kwee, T.C.; Yakar, D. Comparative Performance of Deep Learning and Radiologists for the Diagnosis and Localization of Clinically Significant Prostate Cancer at MRI: A Systematic Review. Life 2022, 12, 1490. [Google Scholar] [CrossRef]
- Castillo T, J.M., et al., Automated classification of significant prostate cancer on MRI: a systematic review on the performance of machine learning applications. Cancers, 2020. 12(6): p. 1606.
- Michaely, H.J.; Aringhieri, G.; Cioni, D.; Neri, E. Current Value of Biparametric Prostate MRI with Machine-Learning or Deep-Learning in the Detection, Grading, and Characterization of Prostate Cancer: A Systematic Review. Diagnostics 2022, 12, 799. [Google Scholar] [CrossRef]
- Naik, N.; Tokas, T.; Shetty, D.K.; Hameed, B.Z.; Shastri, S.; Shah, M.J.; Ibrahim, S.; Rai, B.P.; Chłosta, P.; Somani, B.K. Role of Deep Learning in Prostate Cancer Management: Past, Present and Future Based on a Comprehensive Literature Review. J. Clin. Med. 2022, 11, 3575. [Google Scholar] [CrossRef]
- Sarkis-Onofre, R.; Catalá-López, F.; Aromataris, E.; Lockwood, C. How to properly use the PRISMA Statement. Syst. Rev. 2021, 10, 1–3. [Google Scholar] [CrossRef]
- Hricak, H.; Choyke, P.L.; Eberhardt, S.C.; Leibel, S.A.; Scardino, P.T. Imaging Prostate Cancer: A Multidisciplinary Perspective. Radiology 2007, 243, 28–53. [Google Scholar] [CrossRef] [PubMed]
- Kyle, K.Y. and H. Hricak, Imaging prostate cancer. Radiologic Clinics of North America, 2000. 38(1): p. 59-85.
- Cornud, F.; Brolis, L.; Delongchamps, N.B.; Portalez, D.; Malavaud, B.; Renard-Penna, R.; Mozer, P. TRUS–MRI image registration: a paradigm shift in the diagnosis of significant prostate cancer. Abdom. Imaging 2013, 38, 1447–1463. [Google Scholar] [CrossRef] [PubMed]
- Reynier, C.; Troccaz, J.; Fourneret, P.; Dusserre, A.; Gay-Jeune, C.; Descotes, J.; Bolla, M.; Giraud, J. MRI/TRUS data fusion for prostate brachytherapy. Preliminary results. Med Phys. 2004, 31, 1568–1575. [Google Scholar] [CrossRef] [PubMed]
- Rasch, C.; Barillot, I.; Remeijer, P.; Touw, A.; van Herk, M.; Lebesque, J.V. Definition of the prostate in CT and MRI: a multi-observer study. Int. J. Radiat. Oncol. 1999, 43, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Pezaro, C.; Woo, H.H.; Davis, I.D. Prostate cancer: measuring PSA. Intern. Med. J. 2014, 44, 433–440. [Google Scholar] [CrossRef]
- Takahashi, N.; Inoue, T.; Lee, J.; Yamaguchi, T.; Shizukuishi, K. The Roles of PET and PET/CT in the Diagnosis and Management of Prostate Cancer. Oncology 2007, 72, 226–233. [Google Scholar] [CrossRef]
- Sturge, J., M.P. Caley, and J. Waxman, Bone metastasis in prostate cancer: emerging therapeutic strategies. Nature reviews Clinical oncology, 2011. 8(6): p. 357.
- Raja, J.; Ramachandran, N.; Munneke, G.; Patel, U. Current status of transrectal ultrasound-guided prostate biopsy in the diagnosis of prostate cancer. Clin. Radiol. 2006, 61, 142–153. [Google Scholar] [CrossRef]
- Bai, H.; Xia, W.; Ji, X.; He, D.; Zhao, X.; Bao, J.; Zhou, J.; Wei, X.; Huang, Y.; Li, Q.; et al. Multiparametric Magnetic Resonance Imaging-Based Peritumoral Radiomics for Preoperative Prediction of the Presence of Extracapsular Extension With Prostate Cancer. J. Magn. Reson. Imaging 2021, 54, 1222–1230. [Google Scholar] [CrossRef]
- Jansen, B.H., et al. Adding multiparametric MRI to the MSKCC and Partin nomograms for primary prostate cancer: Improving local tumor staging? in Urologic Oncology: Seminars and Original Investigations. 2019. Elsevier.
- Maurer, T.; Eiber, M.; Schwaiger, M.; Gschwend, J.E. Current use of PSMA–PET in prostate cancer management. Nat. Rev. Urol. 2016, 13, 226–235. [Google Scholar] [CrossRef]
- Stavrinides, V.; Papageorgiou, G.; Danks, D.; Giganti, F.; Pashayan, N.; Trock, B.; Freeman, A.; Hu, Y.; Whitaker, H.; Allen, C.; et al. Mapping PSA density to outcome of MRI-based active surveillance for prostate cancer through joint longitudinal-survival models. Prostate Cancer Prostatic Dis. 2021, 24, 1028–1031. [Google Scholar] [CrossRef]
- Fuchsjäger, M., et al., Prostate cancer imaging. Acta Radiologica, 2008. 49(1): p. 107-120.
- Ghafoor, S.; Burger, I.A.; Vargas, A.H. Multimodality Imaging of Prostate Cancer. J. Nucl. Med. 2019, 60, 1350–1358. [Google Scholar] [CrossRef]
- Rohrmann, S.; Roberts, W.W.; Walsh, P.C.; Platz, E.A. Family history of prostate cancer and obesity in relation to high-grade disease and extraprostatic extension in young men with prostate cancer. Prostate 2003, 55, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Porter, M.P.; Stanford, J.L. Obesity and the risk of prostate cancer. Prostate 2004, 62, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Gann, P.H., Risk factors for prostate cancer. Reviews in urology, 2002. 4(Suppl 5): p. S3.
- Tian, W. and M. Osawa, Prevalent latent adenocarcinoma of the prostate in forensic autopsies. Journal of Clinical Pathology and Forensic Medicine, 2015. 6(3): p. 11-13.
- Marley, A.R. and H. Nan, Epidemiology of colorectal cancer. International journal of molecular epidemiology and genetics, 2016. 7(3): p. 105.
- Kumagai, H.; Zempo-Miyaki, A.; Yoshikawa, T.; Tsujimoto, T.; Tanaka, K.; Maeda, S. Lifestyle modification increases serum testosterone level and decrease central blood pressure in overweight and obese men. Endocr. J. 2015, 62, 423–430. [Google Scholar] [CrossRef] [PubMed]
- A Moyad, M. Is obesity a risk factor for prostate cancer, and does it even matter? A hypothesis and different perspective. Urology 2002, 59, 41–50. [Google Scholar] [CrossRef]
- Parikesit, D., et al., The impact of obesity towards prostate diseases. Prostate international, 2016. 4(1): p. 1-6.
- Tse, L.A.; Lee, P.M.Y.; Ho, W.M.; Lam, A.T.; Lee, M.K.; Ng, S.S.M.; He, Y.; Leung, K.-S.; Hartle, J.C.; Hu, H.; et al. Bisphenol A and other environmental risk factors for prostate cancer in Hong Kong. Environ. Int. 2017, 107, 1–7. [Google Scholar] [CrossRef]
- Vaidyanathan, V.; Naidu, V.; Kao, C.H.-J.; Karunasinghe, N.; Bishop, K.S.; Wang, A.; Pallati, R.; Shepherd, P.; Masters, J.; Zhu, S.; et al. Environmental factors and risk of aggressive prostate cancer among a population of New Zealand men – a genotypic approach. Mol. Biosyst. 2017, 13, 681–698. [Google Scholar] [CrossRef]
- Minaee, S., et al., Image segmentation using deep learning: A survey. IEEE transactions on pattern analysis and machine intelligence, 2021. 44(7): p. 3523-3542.
- Zhang, X.; Li, H.; Wang, C.; Cheng, W.; Zhu, Y.; Li, D.; Jing, H.; Li, S.; Hou, J.; Li, J.; et al. Evaluating the Accuracy of Breast Cancer and Molecular Subtype Diagnosis by Ultrasound Image Deep Learning Model. Front. Oncol. 2021, 11. [Google Scholar] [CrossRef]
- Tammina, S. Transfer learning using VGG-16 with Deep Convolutional Neural Network for Classifying Images. Int. J. Sci. Res. Publ. (IJSRP) 2019, 9, 143–150. [Google Scholar] [CrossRef]
- Abbas, A.; Abdelsamea, M.M.; Gaber, M.M. Classification of COVID-19 in chest X-ray images using DeTraC deep convolutional neural network. Appl. Intell. 2020, 51, 854–864. [Google Scholar] [CrossRef]
- Christlein, V., et al. Deep generalized max pooling. in 2019 International conference on document analysis and recognition (ICDAR). 2019. IEEE.
- Sharma, S., S. Sharma, and A. Athaiya, Activation functions in neural networks. Towards Data Sci, 2017. 6(12): p. 310-316.
- Sibi, P., S.A. Jones, and P. Siddarth, Analysis of different activation functions using back propagation neural networks. Journal of theoretical and applied information technology, 2013. 47(3): p. 1264-1268.
- Fu, J.; Zheng, H.; Mei, T. Look Closer to See Better: Recurrent Attention Convolutional Neural Network for Fine-Grained Image Recognition. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 4476–4484. [Google Scholar]
- Yin, W.; Schütze, H.; Xiang, B.; Zhou, B. ABCNN: Attention-Based Convolutional Neural Network for Modeling Sentence Pairs. Trans. Assoc. Comput. Linguistics 2016, 4, 259–272. [Google Scholar] [CrossRef]
- Otálora, S.; Marini, N.; Müller, H.; Atzori, M. Semi-weakly Supervised Learning for Prostate Cancer Image Classification with Teacher-Student Deep Convolutional Networks. 2020, 193–203. 2020. [CrossRef]
- Zhao, L.; Bao, J.; Qiao, X.; Jin, P.; Ji, Y.; Li, Z.; Zhang, J.; Su, Y.; Ji, L.; Shen, J.; et al. Predicting clinically significant prostate cancer with a deep learning approach: a multicentre retrospective study. Eur. J. Nucl. Med. 2022, 50, 727–741. [Google Scholar] [CrossRef] [PubMed]
- Papp, L.; Spielvogel, C.P.; Grubmüller, B.; Grahovac, M.; Krajnc, D.; Ecsedi, B.; Sareshgi, R.A.; Mohamad, D.; Hamboeck, M.; Rausch, I.; et al. Supervised machine learning enables non-invasive lesion characterization in primary prostate cancer with [68Ga]Ga-PSMA-11 PET/MRI. Eur. J. Nucl. Med. 2020, 48, 1795–1805. [Google Scholar] [CrossRef] [PubMed]
- Wildeboer, R.R.; Mannaerts, C.K.; van Sloun, R.J.G.; Budäus, L.; Tilki, D.; Wijkstra, H.; Salomon, G.; Mischi, M. Automated multiparametric localization of prostate cancer based on B-mode, shear-wave elastography, and contrast-enhanced ultrasound radiomics. Eur. Radiol. 2019, 30, 806–815. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.; Gujrathi, I.; Haider, M.A.; Khalvati, F. Prostate Cancer Detection using Deep Convolutional Neural Networks. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef]
- Hou, Y.; Bao, M.-L.; Wu, C.-J.; Zhang, J.; Zhang, Y.-D.; Shi, H.-B. A radiomics machine learning-based redefining score robustly identifies clinically significant prostate cancer in equivocal PI-RADS score 3 lesions. Abdom. Imaging 2020, 45, 4223–4234. [Google Scholar] [CrossRef]
- Perera, M.; Mirchandani, R.; Papa, N.; Breemer, G.; Effeindzourou, A.; Smith, L.; Swindle, P.; Smith, E. PSA-based machine learning model improves prostate cancer risk stratification in a screening population. World J. Urol. 2020, 39, 1897–1902. [Google Scholar] [CrossRef]
- Swiderska-Chadaj, Z.; de Bel, T.; Blanchet, L.; Baidoshvili, A.; Vossen, D.; van der Laak, J.; Litjens, G. Impact of rescanning and normalization on convolutional neural network performance in multi-center, whole-slide classification of prostate cancer. Sci. Rep. 2020, 10, 1–14. [Google Scholar] [CrossRef]
- Khan, U.A.H.; Stürenberg, C.; Gencoglu, O.; Sandeman, K.; Heikkinen, T.; Rannikko, A.; Mirtti, T. Improving Prostate Cancer Detection with Breast Histopathology Images. 2019, 91–99. [CrossRef]
- Azizi, S.; Imani, F.; Zhuang, B.; Tahmasebi, A.; Kwak, J.T.; Xu, S.; Uniyal, N.; Turkbey, B.; Choyke, P.; Pinto, P.; et al. Ultrasound-Based Detection of Prostate Cancer Using Automatic Feature Selection with Deep Belief Networks. 2015, 70–77. 2015; 77. [CrossRef]
- Sedghi, A.; Mehrtash, A.; Jamzad, A.; Amalou, A.; Wells, W.M.; Kapur, T.; Kwak, J.T.; Turkbey, B.; Choyke, P.; Pinto, P.; et al. Improving detection of prostate cancer foci via information fusion of MRI and temporal enhanced ultrasound. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 1215–1223. [Google Scholar] [CrossRef]
- Capobianco, N.; Sibille, L.; Chantadisai, M.; Gafita, A.; Langbein, T.; Platsch, G.; Solari, E.L.; Shah, V.; Spottiswoode, B.; Eiber, M.; et al. Whole-body uptake classification and prostate cancer staging in 68Ga-PSMA-11 PET/CT using dual-tracer learning. Eur. J. Nucl. Med. 2021, 49, 517–526. [Google Scholar] [CrossRef]
- Deniffel, D.; Abraham, N.; Namdar, K.; Dong, X.; Salinas, E.; Milot, L.; Khalvati, F.; Haider, M.A. Using decision curve analysis to benchmark performance of a magnetic resonance imaging–based deep learning model for prostate cancer risk assessment. Eur. Radiol. 2020, 30, 6867–6876. [Google Scholar] [CrossRef] [PubMed]
- Bleker, J.; Kwee, T.C.; Rouw, D.; Roest, C.; Borstlap, J.; de Jong, I.J.; Dierckx, R.A.J.O.; Huisman, H.; Yakar, D. A deep learning masked segmentation alternative to manual segmentation in biparametric MRI prostate cancer radiomics. Eur. Radiol. 2022, 32, 6526–6535. [Google Scholar] [CrossRef] [PubMed]
- Yu, X., et al. Deep attentive panoptic model for prostate cancer detection using biparametric MRI scans. in Medical Image Computing and Computer Assisted Intervention–MICCAI 2020: 23rd International Conference, Lima, Peru, October 4–8, 2020, Proceedings, Part IV 23. 2020. Springer. 4 October.
- Korevaar, S.; Tennakoon, R.; Page, M.; Brotchie, P.; Thangarajah, J.; Florescu, C.; Sutherland, T.; Kam, N.M.; Bab-Hadiashar, A. Incidental detection of prostate cancer with computed tomography scans. Sci. Rep. 2021, 11, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Nagpal, K., et al., Development and validation of a deep learning algorithm for improving Gleason scoring of prostate cancer. NPJ digital medicine, 2019. 2(1): p. 48.
- Tolkach, Y.; Dohmgörgen, T.; Toma, M.; Kristiansen, G. High-accuracy prostate cancer pathology using deep learning. Nat. Mach. Intell. 2020, 2, 411–418. [Google Scholar] [CrossRef]
- Singhal, N.; Soni, S.; Bonthu, S.; Chattopadhyay, N.; Samanta, P.; Joshi, U.; Jojera, A.; Chharchhodawala, T.; Agarwal, A.; Desai, M.; et al. A deep learning system for prostate cancer diagnosis and grading in whole slide images of core needle biopsies. Sci. Rep. 2022, 12, 1–11. [Google Scholar] [CrossRef]
- Del Rio, M.; Lianas, L.; Aspegren, O.; Busonera, G.; Versaci, F.; Zelic, R.; Vincent, P.H.; Leo, S.; Pettersson, A.; Akre, O.; et al. AI Support for Accelerating Histopathological Slide Examinations of Prostate Cancer in Clinical Studies. 2022, 545–556. [CrossRef]
- Gour, M.; Jain, S.; Shankar, U. Application of Deep Learning Techniques for Prostate Cancer Grading Using Histopathological Images. 2022, 83–94. [CrossRef]
- Bhattacharya, I.; Lim, D.S.; Aung, H.L.; Liu, X.; Seetharaman, A.; Kunder, C.A.; Shao, W.; Soerensen, S.J.C.; Fan, R.E.; Ghanouni, P.; et al. Bridging the gap between prostate radiology and pathology through machine learning. Med Phys. 2022, 49, 5160–5181. [Google Scholar] [CrossRef]
- Hassan, R.; Islam, F.; Uddin, Z.; Ghoshal, G.; Hassan, M.M.; Huda, S.; Fortino, G. Prostate cancer classification from ultrasound and MRI images using deep learning based Explainable Artificial Intelligence. Futur. Gener. Comput. Syst. 2021, 127, 462–472. [Google Scholar] [CrossRef]
- Liu, B.; Cheng, J.; Guo, D.; He, X.; Luo, Y.; Zeng, Y.; Li, C. Prediction of prostate cancer aggressiveness with a combination of radiomics and machine learning-based analysis of dynamic contrast-enhanced MRI. Clin. Radiol. 2019, 74, 896–e1. [Google Scholar] [CrossRef]
- Salvi, M.; Bosco, M.; Molinaro, L.; Gambella, A.; Papotti, M.; Acharya, U.R.; Molinari, F. A hybrid deep learning approach for gland segmentation in prostate histopathological images. Artif. Intell. Med. 2021, 115, 102076. [Google Scholar] [CrossRef]
- Salman, M.E.; Çakar, G. .; Azimjonov, J.; Kösem, M.; Cedi̇moğlu,.H. Automated prostate cancer grading and diagnosis system using deep learning-based Yolo object detection algorithm. Expert Syst. Appl. 2022, 201. [Google Scholar] [CrossRef]
- Stanzione, A.; Cuocolo, R.; Cocozza, S.; Romeo, V.; Persico, F.; Fusco, F.; Longo, N.; Brunetti, A.; Imbriaco, M. Detection of Extraprostatic Extension of Cancer on Biparametric MRI Combining Texture Analysis and Machine Learning: Preliminary Results. Acad. Radiol. 2019, 26, 1338–1344. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Yang, C.; Huang, J.; Liu, S.; Zhuo, Y.; Lu, X. Deep learning framework based on integration of S-Mask R-CNN and Inception-v3 for ultrasound image-aided diagnosis of prostate cancer. Futur. Gener. Comput. Syst. 2020, 114, 358–367. [Google Scholar] [CrossRef]
- Zhang, L.; Li, L.; Tang, M.; Huan, Y.; Zhang, X.; Zhe, X. A new approach to diagnosing prostate cancer through magnetic resonance imaging. Alex. Eng. J. 2020, 60, 897–904. [Google Scholar] [CrossRef]
- Stojadinovic, M.; Milicevic, B.; Jankovic, S. Improved predictive performance of prostate biopsy collaborative group risk calculator when based on automated machine learning. Comput. Biol. Med. 2021, 138, 104903. [Google Scholar] [CrossRef] [PubMed]
- ElKarami, B.; Deebajah, M.; Polk, S.; Peabody, J.; Shahrrava, B.; Menon, M.; Alkhateeb, A.; Alanee, S. Machine learning-based prediction of upgrading on magnetic resonance imaging targeted biopsy in patients eligible for active surveillance. Urol. Oncol. Semin. Orig. Investig. 2022, 40, 191–e15. [Google Scholar] [CrossRef]
- Lu, X.; Zhang, S.; Liu, Z.; Liu, S.; Huang, J.; Kong, G.; Li, M.; Liang, Y.; Cui, Y.; Yang, C.; et al. Ultrasonographic pathological grading of prostate cancer using automatic region-based Gleason grading network. Comput. Med Imaging Graph. 2022, 102, 102125. [Google Scholar] [CrossRef]
- Hambarde, P.; Talbar, S.; Mahajan, A.; Chavan, S.; Thakur, M.; Sable, N. Prostate lesion segmentation in MR images using radiomics based deeply supervised U-Net. Biocybern. Biomed. Eng. 2020, 40, 1421–1435. [Google Scholar] [CrossRef]
- Isaksson, L.J.; Repetto, M.; Summers, P.E.; Pepa, M.; Zaffaroni, M.; Vincini, M.G.; Corrao, G.; Mazzola, G.C.; Rotondi, M.; Bellerba, F.; et al. High-performance prediction models for prostate cancer radiomics. Informatics Med. Unlocked 2023, 37. [Google Scholar] [CrossRef]
- Li, J.; Weng, Z.; Xu, H.; Zhang, Z.; Miao, H.; Chen, W.; Liu, Z.; Zhang, X.; Wang, M.; Xu, X.; et al. Support Vector Machines (SVM) classification of prostate cancer Gleason score in central gland using multiparametric magnetic resonance images: A cross-validated study. Eur. J. Radiol. 2017, 98, 61–67. [Google Scholar] [CrossRef]
- Shao, W.; Banh, L.; Kunder, C.A.; Fan, R.E.; Soerensen, S.J.; Wang, J.B.; Teslovich, N.C.; Madhuripan, N.; Jawahar, A.; Ghanouni, P.; et al. ProsRegNet: A deep learning framework for registration of MRI and histopathology images of the prostate. Med Image Anal. 2020, 68, 101919. [Google Scholar] [CrossRef]
- Wang, Y., et al., Stacking-based ensemble learning of decision trees for interpretable prostate cancer detection. Applied Soft Computing, 2019. 77: p. 188-204.
- Bhattacharya, I.; Seetharaman, A.; Kunder, C.; Shao, W.; Chen, L.C.; Soerensen, S.J.; Wang, J.B.; Teslovich, N.C.; Fan, R.E.; Ghanouni, P.; et al. Selective identification and localization of indolent and aggressive prostate cancers via CorrSigNIA: an MRI-pathology correlation and deep learning framework. Med Image Anal. 2021, 75, 102288–102288. [Google Scholar] [CrossRef] [PubMed]
- Saha, A.; Hosseinzadeh, M.; Huisman, H. End-to-end prostate cancer detection in bpMRI via 3D CNNs: Effects of attention mechanisms, clinical priori and decoupled false positive reduction. Med Image Anal. 2021, 73, 102155. [Google Scholar] [CrossRef] [PubMed]
- Trigui, R.; Mitéran, J.; Walker, P.; Sellami, L.; Ben Hamida, A. Automatic classification and localization of prostate cancer using multi-parametric MRI/MRS. Biomed. Signal Process. Control. 2017, 31, 189–198. [Google Scholar] [CrossRef]
- Chen, J.; Wan, Z.; Zhang, J.; Li, W.; Chen, Y.; Li, Y.; Duan, Y. Medical image segmentation and reconstruction of prostate tumor based on 3D AlexNet. Comput. Methods Programs Biomed. 2020, 200, 105878. [Google Scholar] [CrossRef]
- Jia, H.; Xia, Y.; Song, Y.; Cai, W.; Fulham, M.; Feng, D.D. Atlas registration and ensemble deep convolutional neural network-based prostate segmentation using magnetic resonance imaging. Neurocomputing 2018, 275, 1358–1369. [Google Scholar] [CrossRef]
- Li, B.; Oka, R.; Xuan, P.; Yoshimura, Y.; Nakaguchi, T. Robust multi-modal prostate cancer classification via feature autoencoder and dual attention. Informatics Med. Unlocked 2022, 30, 100923. [Google Scholar] [CrossRef]
- Patsanis, A.; Sunoqrot, M.R.; Langørgen, S.; Wang, H.; Selnæs, K.M.; Bertilsson, H.; Bathen, T.F.; Elschot, M. A comparison of Generative Adversarial Networks for automated prostate cancer detection on T2-weighted MRI. Informatics Med. Unlocked 2023, 39. [Google Scholar] [CrossRef]
- Abraham, B.; Nair, M.S. Automated grading of prostate cancer using convolutional neural network and ordinal class classifier. Informatics Med. Unlocked 2019, 17, 100256. [Google Scholar] [CrossRef]
- Akamine, Y.; Ueda, Y.; Ueno, Y.; Sofue, K.; Murakami, T.; Yoneyama, M.; Obara, M.; Van Cauteren, M. Application of hierarchical clustering to multi-parametric MR in prostate: Differentiation of tumor and normal tissue with high accuracy. Magn. Reson. Imaging 2020, 74, 90–95. [Google Scholar] [CrossRef]
- Yang, X.; Liu, C.; Wang, Z.; Yang, J.; Le Min, H.; Wang, L.; Cheng, K.-T. (. Co-trained convolutional neural networks for automated detection of prostate cancer in multi-parametric MRI. Med Image Anal. 2017, 42, 212–227. [Google Scholar] [CrossRef]
- Gentile, F.; La Civita, E.; Della Ventura, B.; Ferro, M.; Cennamo, M.; Bruzzese, D.; Crocetto, F.; Velotta, R.; Terracciano, D. A Combinatorial Neural Network Analysis Reveals a Synergistic Behaviour of Multiparametric Magnetic Resonance and Prostate Health Index in the Identification of Clinically Significant Prostate Cancer. Clin. Genitourin. Cancer 2022, 20, e406–e410. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.A.; Mercaldo, S.; Chung, R.; Ulrich, E.; Jones, R.W.; Harisinghani, M. Improving Prostate Cancer Detection With MRI: A Multi-Reader, Multi-Case Study Using Computer-Aided Detection (CAD). Acad. Radiol. 2022, 30, 1340–1349. [Google Scholar] [CrossRef] [PubMed]
- Otálora, S.; Atzori, M.; Khan, A.; Jimenez-Del-Toro, O.; Andrearczyk, V.; Müller, H. A systematic comparison of deep learning strategies for weakly supervised Gleason grading. 2020, 11320, 113200L. [CrossRef]
- Alam, M., et al. A machine learning classification technique for predicting prostate cancer. in 2020 IEEE International Conference on Electro Information Technology (EIT). 2020. IEEE.
- Feng, Y.; Yang, F.; Zhou, X.; Guo, Y.; Tang, F.; Ren, F.; Guo, J.; Ji, S. A Deep Learning Approach for Targeted Contrast-Enhanced Ultrasound Based Prostate Cancer Detection. IEEE/ACM Trans. Comput. Biol. Bioinform. 2018, 16, 1794–1801. [Google Scholar] [CrossRef] [PubMed]
- de Vente, C.; Vos, P.; Hosseinzadeh, M.; Pluim, J.; Veta, M. Deep Learning Regression for Prostate Cancer Detection and Grading in Bi-Parametric MRI. IEEE Trans. Biomed. Eng. 2020, 68, 374–383. [Google Scholar] [CrossRef]
- Iqbal, S.; Siddiqui, G.F.; Rehman, A.; Hussain, L.; Saba, T.; Tariq, U.; Abbasi, A.A. Prostate Cancer Detection Using Deep Learning and Traditional Techniques. IEEE Access 2021, 9, 27085–27100. [Google Scholar] [CrossRef]
- Duran-Lopez, L.; Dominguez-Morales, J.P.; Conde-Martin, A.F.; Vicente-Diaz, S.; Linares-Barranco, A. PROMETEO: A CNN-Based Computer-Aided Diagnosis System for WSI Prostate Cancer Detection. IEEE Access 2020, 8, 128613–128628. [Google Scholar] [CrossRef]
- Chaddad, A.; Kucharczyk, M.J.; Desrosiers, C.; Okuwobi, I.P.; Katib, Y.; Zhang, M.; Rathore, S.; Sargos, P.; Niazi, T. Deep Radiomic Analysis to Predict Gleason Score in Prostate Cancer. IEEE Access 2020, 8, 167767–167778. [Google Scholar] [CrossRef]
- Wang, Z.; Liu, C.; Cheng, D.; Wanga, L.; Yang, X.; Cheng, K.-T. Automated Detection of Clinically Significant Prostate Cancer in mp-MRI Images Based on an End-to-End Deep Neural Network. IEEE Trans. Med Imaging 2018, 37, 1127–1139. [Google Scholar] [CrossRef]
- Li, W.; Li, J.; Sarma, K.V.; Ho, K.C.; Shen, S.; Knudsen, B.S.; Gertych, A.; Arnold, C.W. Path R-CNN for Prostate Cancer Diagnosis and Gleason Grading of Histological Images. IEEE Trans. Med Imaging 2018, 38, 945–954. [Google Scholar] [CrossRef]
- Wiratchawa, K., et al. Training Deep CNN's to Detect Prostate Cancer Lesion with Small Training Data. in 2022 37th International Technical Conference on Circuits/Systems, Computers and Communications (ITC-CSCC). 2022. IEEE.
- Reda, I., et al. A new CNN-based system for early diagnosis of prostate cancer. in 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018). 2018. IEEE.
- Cao, R.; Bajgiran, A.M.; Mirak, S.A.; Shakeri, S.; Zhong, X.; Enzmann, D.; Raman, S.; Sung, K. Joint Prostate Cancer Detection and Gleason Score Prediction in mp-MRI via FocalNet. IEEE Trans. Med Imaging 2019, 38, 2496–2506. [Google Scholar] [CrossRef]
- Mosleh, M.A., M.H. Hamoud, and A.A. Alsabri. Detection of Prostate Cancer Using MRI Images Classification with Deep Learning Techniques. in 2022 2nd International Conference on Emerging Smart Technologies and Applications (eSmarTA). 2022. IEEE.
- Castillo, J.; Starmans, M.P.A.; Niessen, W.J.; Schoots, I.; Klein, S.; Veenland, J.F. Classification Of Prostate Cancer: High Grade Versus Low Grade Using A Radiomics Approach. 2019 IEEE 16th International Symposium on Biomedical Imaging (ISBI 2019) Venice, Italy, 8–11 April 2019, 1319–1322. 8–11 April. [CrossRef]
- Hassanzadeh, T.; Hamey, L.G.C.; Ho-Shon, K. Convolutional Neural Networks for Prostate Magnetic Resonance Image Segmentation. IEEE Access 2019, 7, 36748–36760. [Google Scholar] [CrossRef]
- Morris, D.C.; Chan, D.Y.; Chen, H.; Palmeri, M.L.; Polascik, T.J.; Foo, W.-C.; Huang, J.; Mamou, J.; Nightingale, K.R. Multiparametric Ultrasound for the Targeting of Prostate Cancer using ARFI, SWEI, B-mode, and QUS. 2019, 880–883. [CrossRef]
- Bertelli, E.; Mercatelli, L.; Marzi, C.; Pachetti, E.; Baccini, M.; Barucci, A.; Colantonio, S.; Gherardini, L.; Lattavo, L.; Pascali, M.A.; et al. Machine and Deep Learning Prediction Of Prostate Cancer Aggressiveness Using Multiparametric MRI. Front. Oncol. 2022, 11, 802964. [Google Scholar] [CrossRef] [PubMed]
- Dai, X.; Park, J.H.; Yoo, S.; D’imperio, N.; McMahon, B.H.; Rentsch, C.T.; Tate, J.P.; Justice, A.C. Survival analysis of localized prostate cancer with deep learning. Sci. Rep. 2022, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, A.A.; Hussain, L.; Awan, I.A.; Abbasi, I.; Majid, A.; Nadeem, M.S.A.; Chaudhary, Q.-A. Detecting prostate cancer using deep learning convolution neural network with transfer learning approach. Cogn. Neurodynamics 2020, 14, 523–533. [Google Scholar] [CrossRef]
- Hiremath, A.; Shiradkar, R.; Fu, P.; Mahran, A.; Rastinehad, A.R.; Tewari, A.; Tirumani, S.H.; Purysko, A.; Ponsky, L.; Madabhushi, A. An integrated nomogram combining deep learning, Prostate Imaging–Reporting and Data System (PI-RADS) scoring, and clinical variables for identification of clinically significant prostate cancer on biparametric MRI: a retrospective multicentre study. Lancet Digit. Heal. 2021, 3, e445–e454. [Google Scholar] [CrossRef]
- Mehralivand, S.; Yang, D.; Harmon, S.A.; Xu, D.; Xu, Z.; Roth, H.; Masoudi, S.; Kesani, D.; Lay, N.; Merino, M.J.; et al. Deep learning-based artificial intelligence for prostate cancer detection at biparametric MRI. Abdom. Imaging 2022, 47, 1425–1434. [Google Scholar] [CrossRef]
- Hosseinzadeh, M.; Saha, A.; Brand, P.; Slootweg, I.; de Rooij, M.; Huisman, H. Deep learning–assisted prostate cancer detection on bi-parametric MRI: minimum training data size requirements and effect of prior knowledge. Eur. Radiol. 2021, 32, 2224–2234. [Google Scholar] [CrossRef]
- Khosravi, P.; Lysandrou, M.; Eljalby, M.; Li, Q.; Kazemi, E.; Zisimopoulos, P.; Sigaras, A.; Brendel, M.; Barnes, J.; Ricketts, C.; et al. A Deep Learning Approach to Diagnostic Classification of Prostate Cancer Using Pathology–Radiology Fusion. J. Magn. Reson. Imaging 2021, 54, 462–471. [Google Scholar] [CrossRef]
- Takeuchi, T.; Hattori-Kato, M.; Okuno, Y.; Iwai, S.; Mikami, K. Prediction of prostate cancer by deep learning with multilayer artificial neural network. Can. Urol. Assoc. J. 2018, 13, E145–E150. [Google Scholar] [CrossRef]
- Soni, M.; Khan, I.R.; Babu, K.S.; Nasrullah, S.; Madduri, A.; Rahin, S.A. Light Weighted Healthcare CNN Model to Detect Prostate Cancer on Multiparametric MRI. Comput. Intell. Neurosci. 2022, 2022, 1–11. [Google Scholar] [CrossRef]
- Azizi, S.; Bayat, S.; Yan, P.; Tahmasebi, A.; Kwak, J.T.; Xu, S.; Turkbey, B.; Choyke, P.; Pinto, P.; Wood, B.; et al. Deep Recurrent Neural Networks for Prostate Cancer Detection: Analysis of Temporal Enhanced Ultrasound. IEEE Trans. Med Imaging 2018, 37, 2695–2703. [Google Scholar] [CrossRef]
- Laabidi, A.; Aissaoui, M. Performance analysis of Machine learning classifiers for predicting diabetes and prostate cancer. 2020, 1–6. [CrossRef]
- Murakami, Y.; Magome, T.; Matsumoto, K.; Sato, T.; Yoshioka, Y.; Oguchi, M. Fully automated dose prediction using generative adversarial networks in prostate cancer patients. PLOS ONE 2020, 15, e0232697. [Google Scholar] [CrossRef]
- Kohl, S., et al., Adversarial networks for the detection of aggressive prostate cancer. arXiv preprint arXiv:1702.08014, 2017. arXiv:1702.08014, 2017.
- Yu, H.; Zhang, X. Synthesis of Prostate MR Images for Classification Using Capsule Network-Based GAN Model. Sensors 2020, 20, 5736. [Google Scholar] [CrossRef]
- Li, Y.; Wang, J.; Hu, M.; Patel, P.; Mao, H.; Liu, T.; Yang, X. Prostate gleason score prediction via MRI using capsule network. 2023, 12465, 507–512. [CrossRef]
- Ding, M.; Lin, Z.; Lee, C.H.; Tan, C.H.; Huang, W. A Multi-Scale Channel Attention Network for Prostate Segmentation. IEEE Trans. Circuits Syst. II: Express Briefs 2023, 70, 1754–1758. [Google Scholar] [CrossRef]
- Xu, X.; Lian, C.; Wang, S.; Zhu, T.; Chen, R.C.; Wang, A.Z.; Royce, T.J.; Yap, P.-T.; Shen, D.; Lian, J. Asymmetric multi-task attention network for prostate bed segmentation in computed tomography images. Med Image Anal. 2021, 72, 102116–102116. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Qin, W.; Buyyounouski, M.; Ibragimov, B.; Hancock, S.; Han, B.; Xing, L. Prostate cancer classification with multiparametric MRI transfer learning model. Med Phys. 2018, 46, 756–765. [Google Scholar] [CrossRef] [PubMed]
- Janocha, K.; Czarnecki, W.M. On Loss Functions for Deep Neural Networks in Classification. Schedae Informaticae 2017, 1/2016, 4959. [Google Scholar] [CrossRef]
- Zhao, H., et al., Loss functions for neural networks for image processing. arXiv preprint arXiv:1511.08861, 2015. arXiv:1511.08861, 2015.
- Ghosh, A.; Kumar, H.; Sastry, P.S. Robust Loss Functions under Label Noise for Deep Neural Networks. Proc Conf AAAI Artif Intell 2017, 31. [Google Scholar] [CrossRef]
- Xu, C., et al., Multi-loss regularized deep neural network. IEEE Transactions on Circuits and Systems for Video Technology, 2015. 26(12): p. 2273-2283.
- Kim, T.; Oh, J.; Kim, N.Y.; Cho, S.; Yun, S.-Y. Comparing Kullback-Leibler Divergence and Mean Squared Error Loss in Knowledge Distillation. 2021, 3, 2628–2635. [CrossRef]
- Qi, J.; Du, J.; Siniscalchi, S.M.; Ma, X.; Lee, C.-H. On Mean Absolute Error for Deep Neural Network Based Vector-to-Vector Regression. IEEE Signal Process. Lett. 2020, 27, 1485–1489. [Google Scholar] [CrossRef]
- Ruby, U. and V. Yendapalli, Binary cross entropy with deep learning technique for image classification. Int. J. Adv. Trends Comput. Sci. Eng, 2020. 9(10).
- Ho, Y.; Wookey, S. The Real-World-Weight Cross-Entropy Loss Function: Modeling the Costs of Mislabeling. IEEE Access 2020, 8, 4806–4813. [Google Scholar] [CrossRef]
- Gordon-Rodriguez, E., et al., Uses and abuses of the cross-entropy loss: Case studies in modern deep learning. 2020.
- Sudre, C.H., et al. Generalised dice overlap as a deep learning loss function for highly unbalanced segmentations. in Deep Learning in Medical Image Analysis and Multimodal Learning for Clinical Decision Support: Third International Workshop, DLMIA 2017, and 7th International Workshop, ML-CDS 2017, Held in Conjunction with MICCAI 2017, Québec City, QC, Canada, September 14, Proceedings 3. 2017. Springer. 14 September.
- Zhang, Y.; Liu, S.; Li, C.; Wang, J. Rethinking the Dice Loss for Deep Learning Lesion Segmentation in Medical Images. J. Shanghai Jiaotong Univ. (Science) 2021, 26, 93–102. [Google Scholar] [CrossRef]
- Mukhoti, J., et al., Calibrating deep neural networks using focal loss. Advances in Neural Information Processing Systems, 2020. 33: p. 15288-15299.
- Lin, T.-Y., et al. Focal loss for dense object detection. in Proceedings of the IEEE international conference on computer vision. 2017.
- Asperti, A.; Trentin, M. Balancing Reconstruction Error and Kullback-Leibler Divergence in Variational Autoencoders. IEEE Access 2020, 8, 199440–199448. [Google Scholar] [CrossRef]
- Phan, H.; Mikkelsen, K.; Chén, O.Y.; Koch, P.; Mertins, A.; Kidmose, P.; De Vos, M. Personalized automatic sleep staging with single-night data: a pilot study with Kullback–Leibler divergence regularization. Physiol. Meas. 2020, 41, 064004. [Google Scholar] [CrossRef] [PubMed]
- Tomczak, K.; Czerwińska, P.; Wiznerowicz, M. Review The Cancer Genome Atlas (TCGA): an immeasurable source of knowledge. Contemp. Oncol. 2015, 2015, 68–77. [Google Scholar] [CrossRef]
- Wang, Z.; Jensen, M.A.; Zenklusen, J.C. A.; Zenklusen, J.C. A Practical Guide to The Cancer Genome Atlas (TCGA). In Statistical Genomics; Humana Press: New York, NY, USA, 2016; Volume 1418, pp. 111–141. [Google Scholar] [CrossRef]
- Hutter, C.; Zenklusen, J.C. The Cancer Genome Atlas: Creating Lasting Value beyond Its Data. Cell 2018, 173, 283–285. [Google Scholar] [CrossRef]
- Vaske, C.J.; Benz, S.C.; Sanborn, J.Z.; Earl, D.; Szeto, C.; Zhu, J.; Haussler, D.; Stuart, J.M. Inference of patient-specific pathway activities from multi-dimensional cancer genomics data using PARADIGM. Bioinformatics 2010, 26, i237–i245. [Google Scholar] [CrossRef]
- Ganini, C.; Amelio, I.; Bertolo, R.; Bove, P.; Buonomo, O.C.; Candi, E.; Cipriani, C.; Di Daniele, N.; Juhl, H.; Mauriello, A.; et al. Global mapping of cancers: The Cancer Genome Atlas and beyond. Mol. Oncol. 2021, 15, 2823–2840. [Google Scholar] [CrossRef]
- Rosenkrantz, A.B.; Oto, A.; Turkbey, B.; Westphalen, A.C. Prostate Imaging Reporting and Data System (PI-RADS), Version 2: A Critical Look. Am. J. Roentgenol. 2016, 206, 1179–1183. [Google Scholar] [CrossRef]
- Westphalen, A.C.; Rosenkrantz, A.B. Prostate Imaging Reporting and Data System (PI-RADS): Reflections on Early Experience With a Standardized Interpretation Scheme for Multiparametric Prostate MRI. Am. J. Roentgenol. 2014, 202, 121–123. [Google Scholar] [CrossRef]
- Deng, K.; Li, H.; Guan, Y. Treatment Stratification of Patients with Metastatic Castration-Resistant Prostate Cancer by Machine Learning. iScience 2020, 23, 100804. [Google Scholar] [CrossRef]
- Abdallah, K.; Hugh-Jones, C.; Norman, T.; Friend, S.; Stolovitzky, G. The Prostate Cancer DREAM Challenge: A Community-Wide Effort to Use Open Clinical Trial Data for the Quantitative Prediction of Outcomes in Metastatic Prostate Cancer. Oncol. 2015, 20, 459–460. [Google Scholar] [CrossRef] [PubMed]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M.; et al. The Cancer Imaging Archive (TCIA): Maintaining and Operating a Public Information Repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef] [PubMed]
- Prior, F.; Smith, K.; Sharma, A.; Kirby, J.; Tarbox, L.; Clark, K.; Bennett, W.; Nolan, T.; Freymann, J. The public cancer radiology imaging collections of The Cancer Imaging Archive. Sci. Data 2017, 4, 170124. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Yang, G.; Mirak, S.A.; Hosseiny, M.; Azadikhah, A.; Zhong, X.; Reiter, R.E.; Lee, Y.; Raman, S.S.; Sung, K. Automatic Prostate Zonal Segmentation Using Fully Convolutional Network With Feature Pyramid Attention. IEEE Access 2019, 7, 163626–163632. [Google Scholar] [CrossRef]
- Mehrtash, A.; Sedghi, A.; Ghafoorian, M.; Taghipour, M.; Tempany, C.M.; Wells, W.M.; Kapur, T.; Mousavi, P.; Abolmaesumi, P.; Fedorov, A. Classification of clinical significance of MRI prostate findings using 3D convolutional neural networks. In Proceedings of the Medical Imaging 2017: Computer-Aided Diagnosis, Orlando, FL, USA, 3 March 2017. [Google Scholar] [CrossRef]
Figure 2.
Trend of research in ML/DL models for PCa diagnosis (actual experimental study).
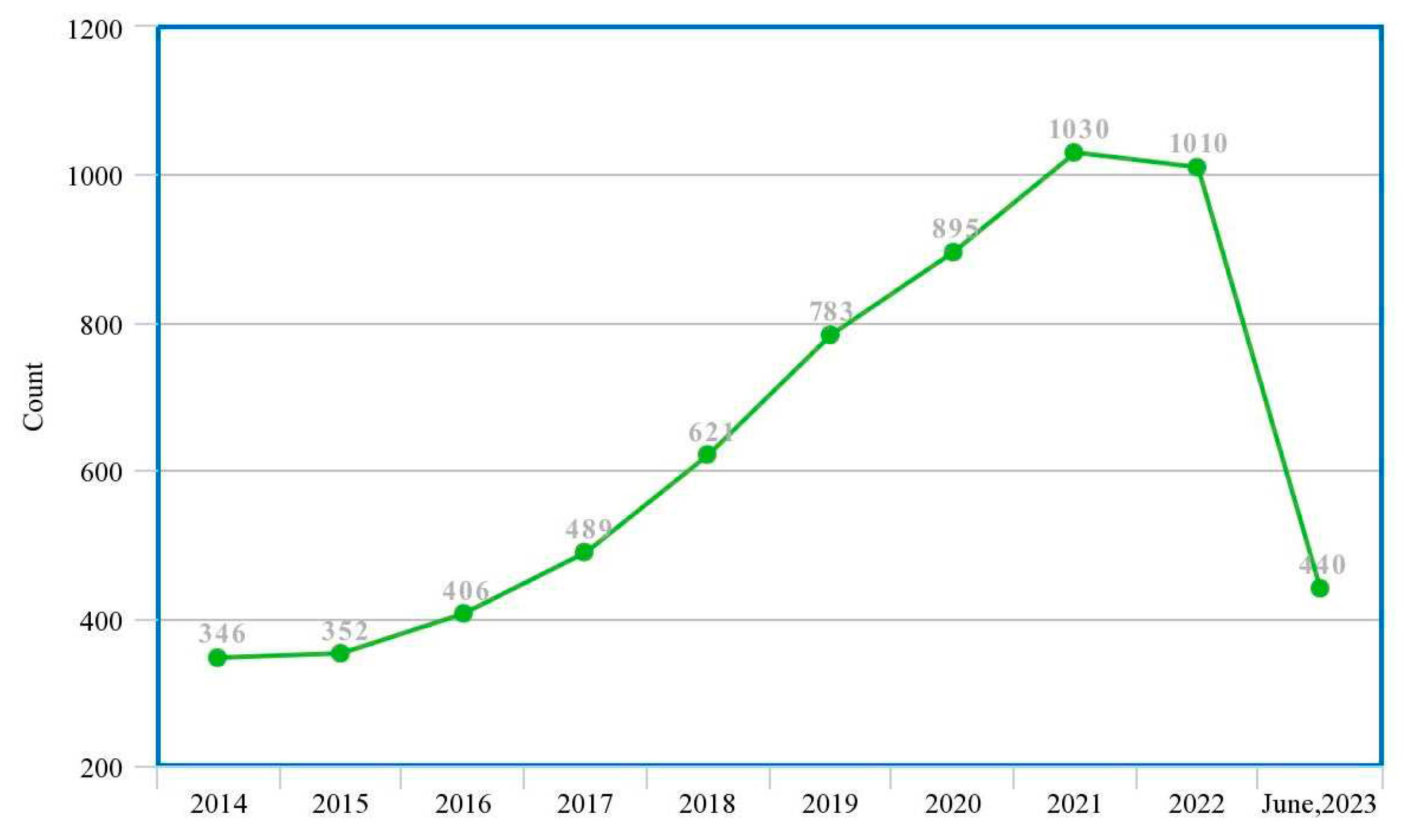
Figure 3.
Trend of research in ML/DL models for PCa diagnosis (systematic review study).
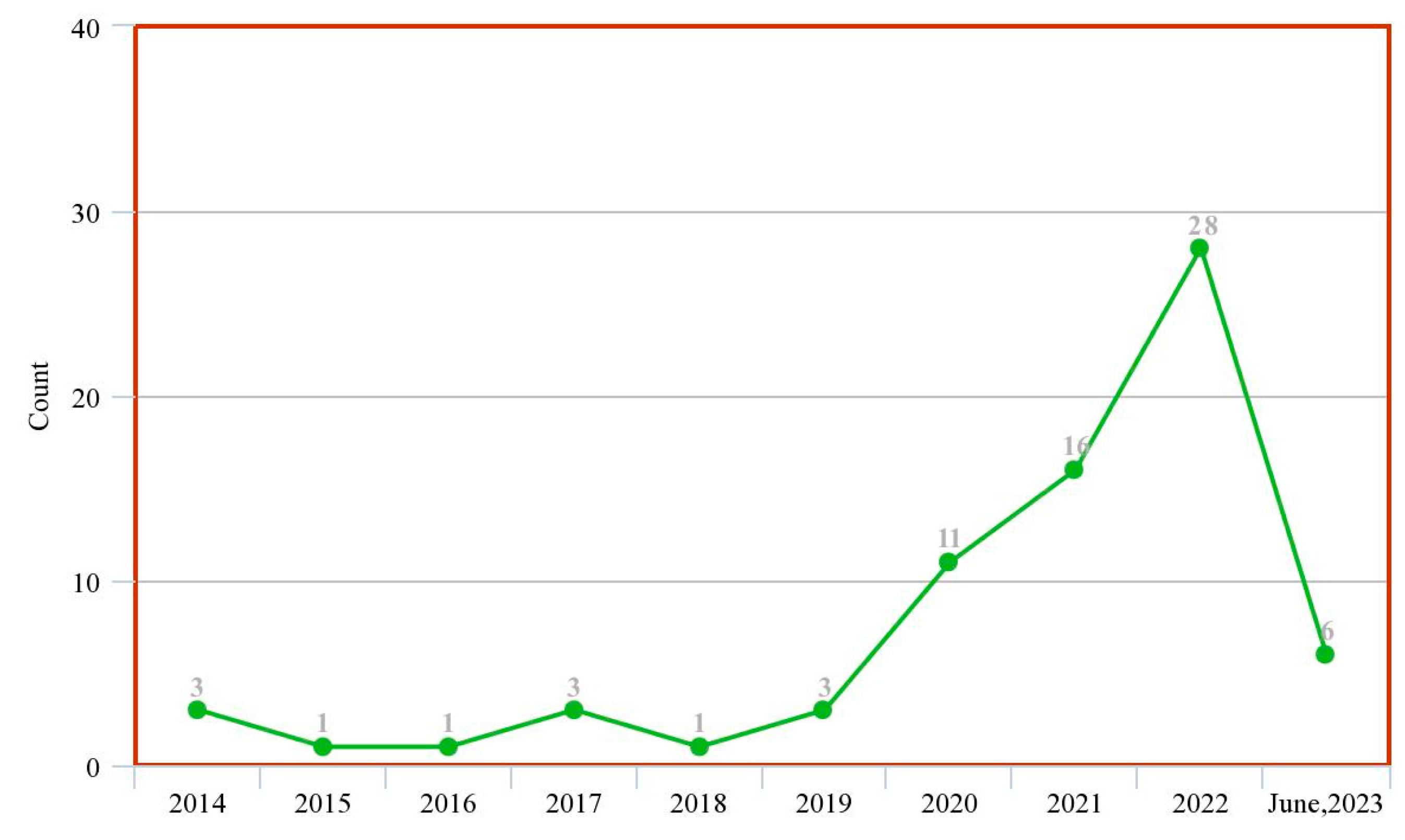
Figure 4.
High-level structure of this research.
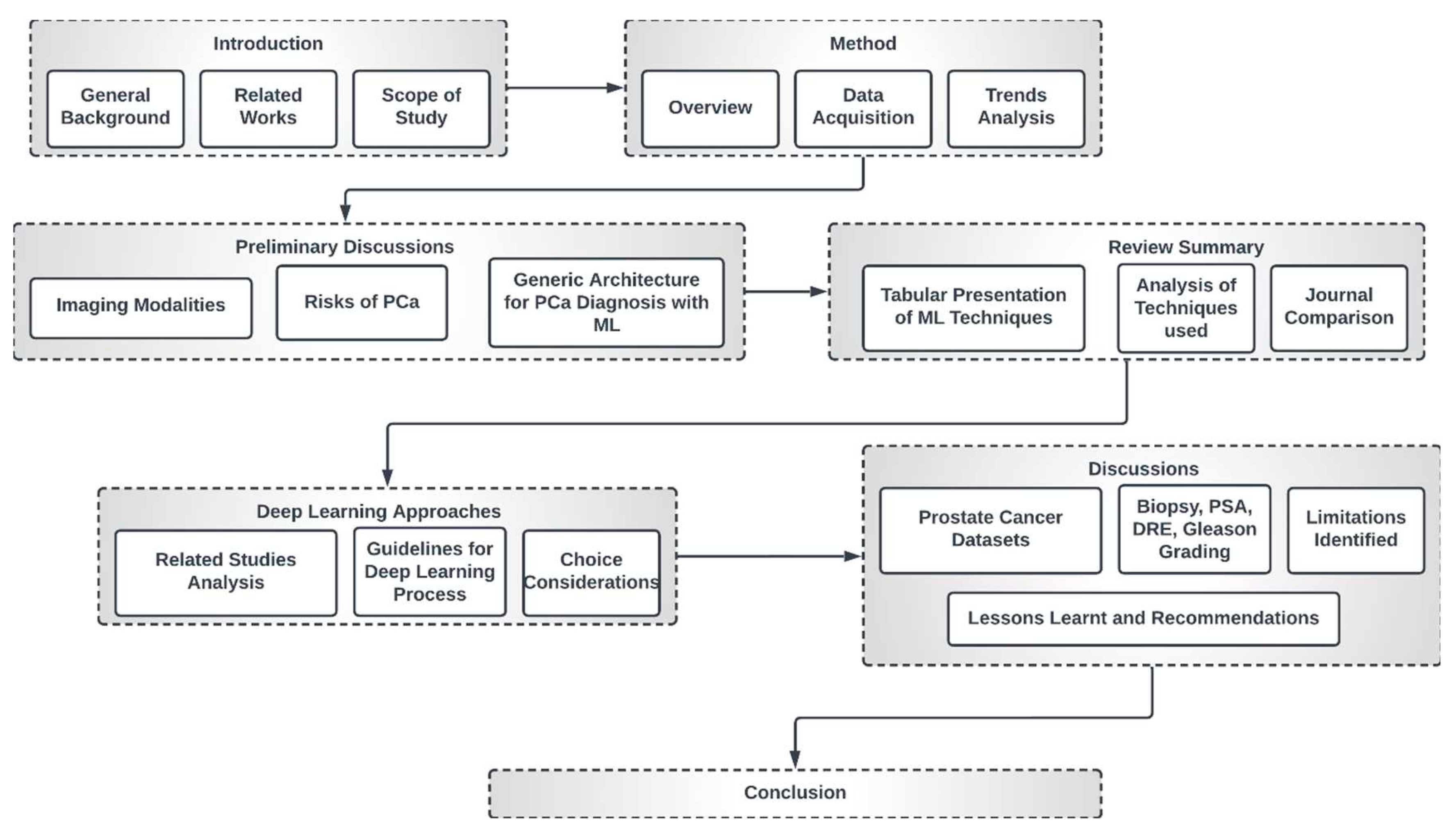
Figure 5.
PRISMA-Scr numerical flow guideline for systematic review employed in this study.
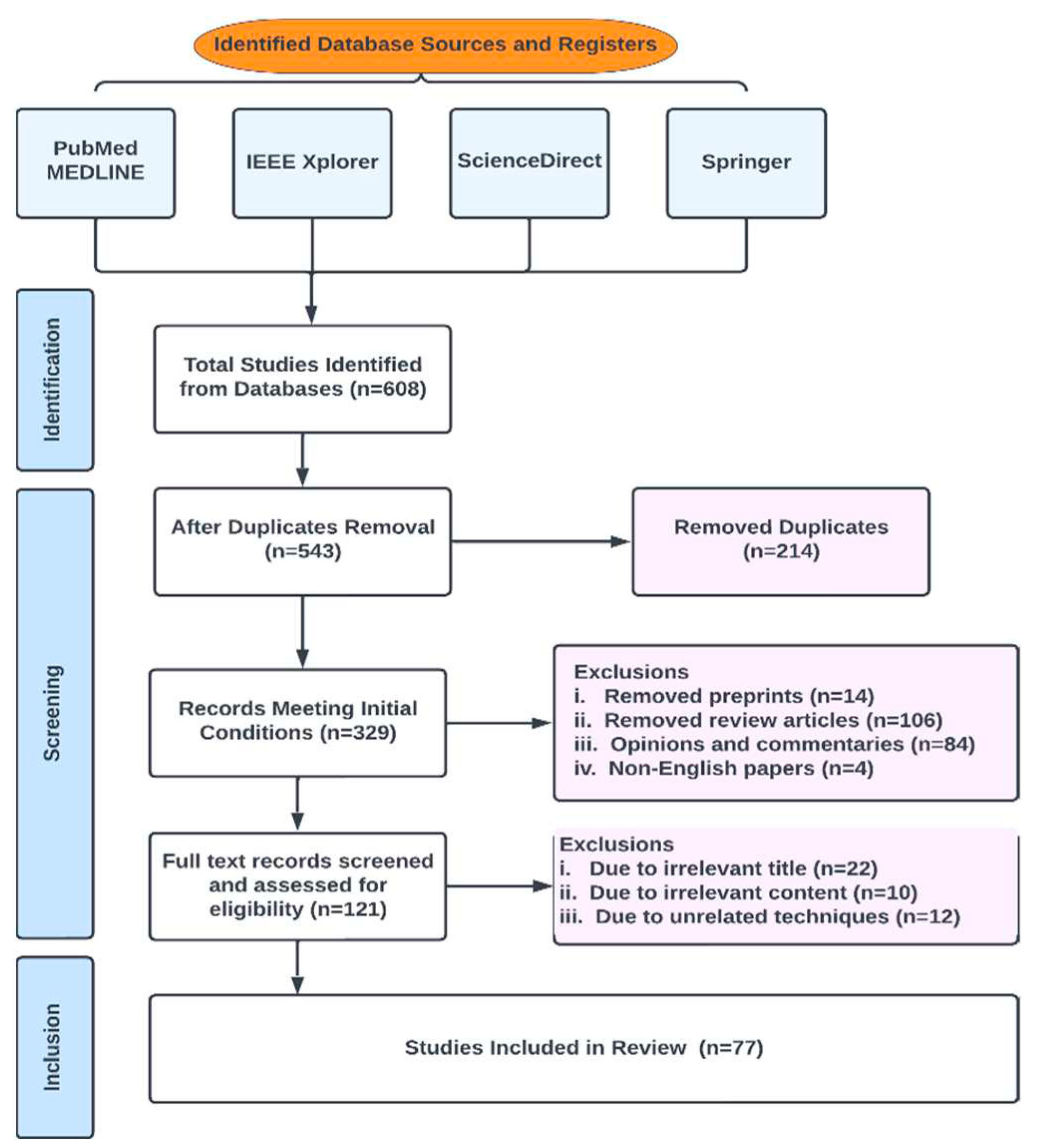
Figure 6.
Characteristics of reviewed literature.
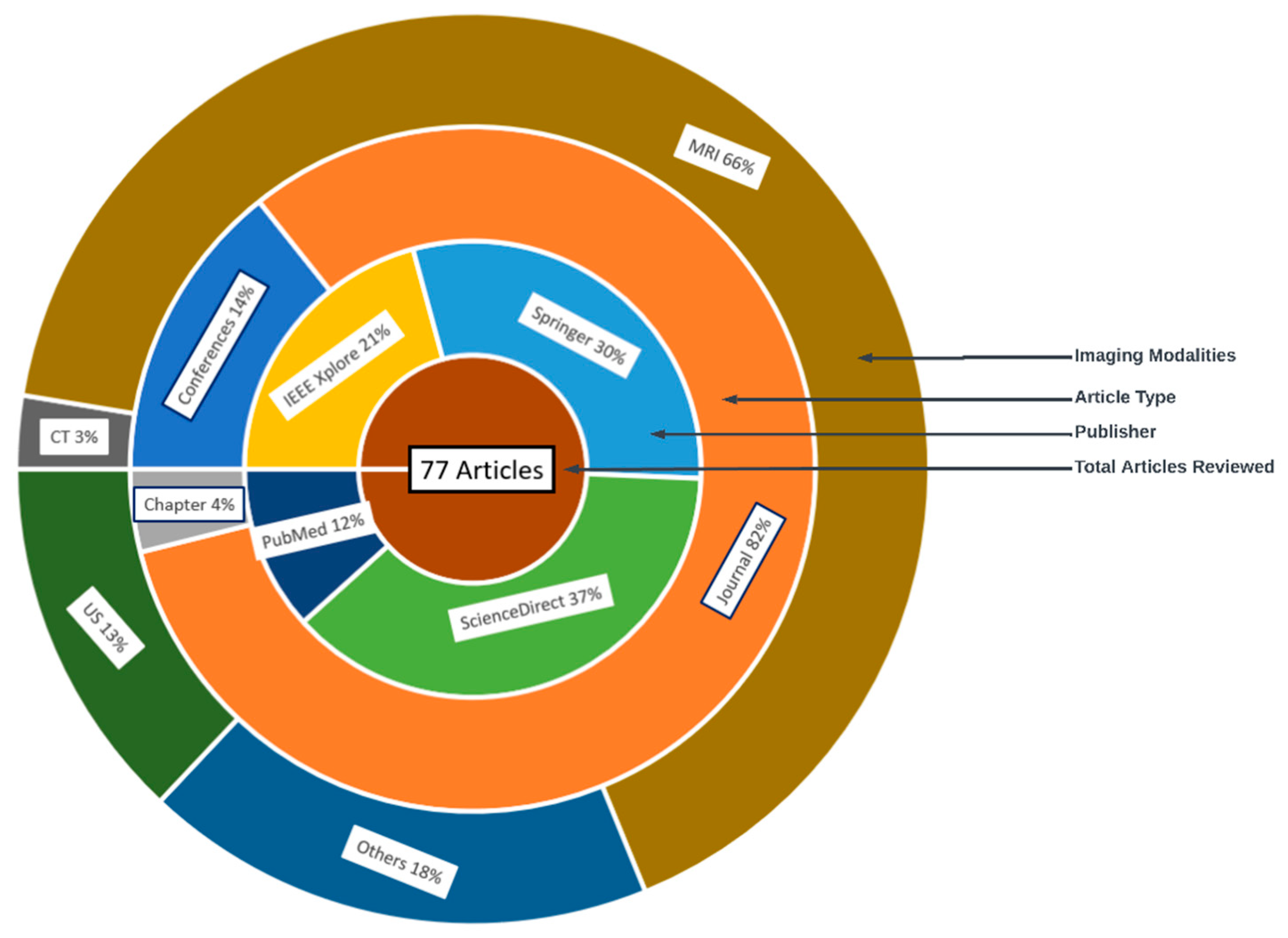
Figure 7.
Generic Deep learning architecture for PCa image analysis.
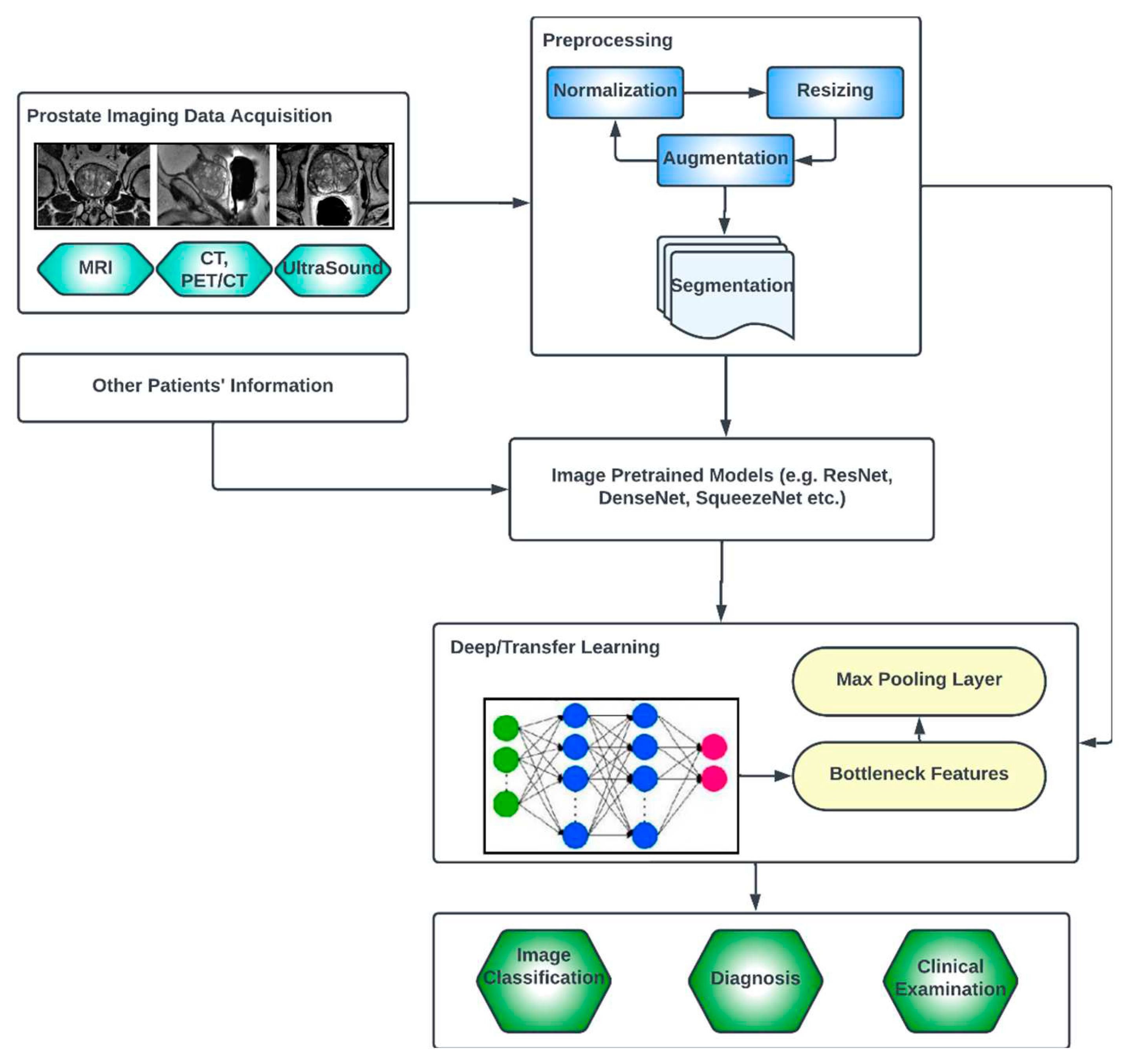
Figure 8.
Year distribution of included papers.
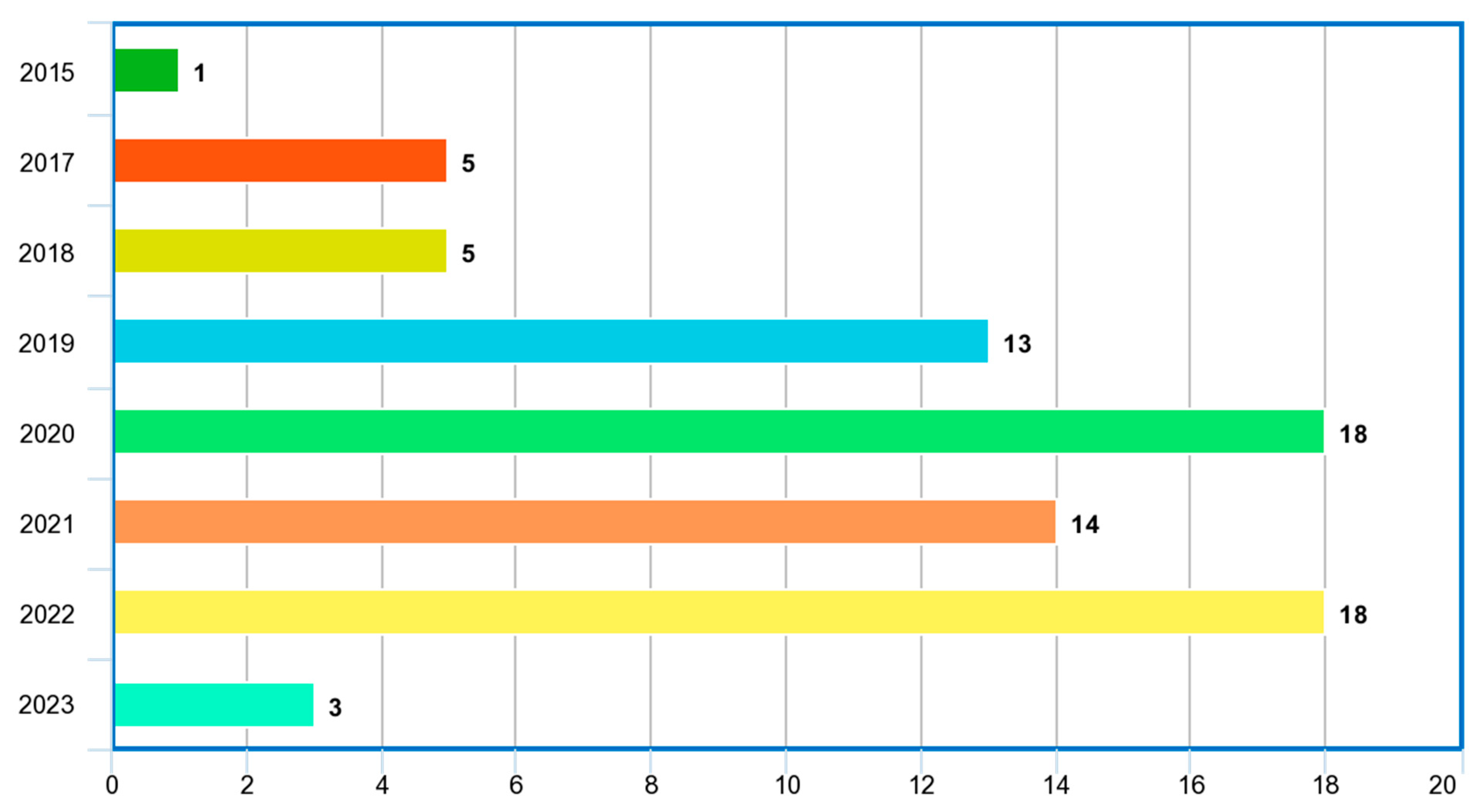
Figure 9.
Word cloud of topics of reviewed papers.
Figure 10.
Image modalities used in reviewed papers.
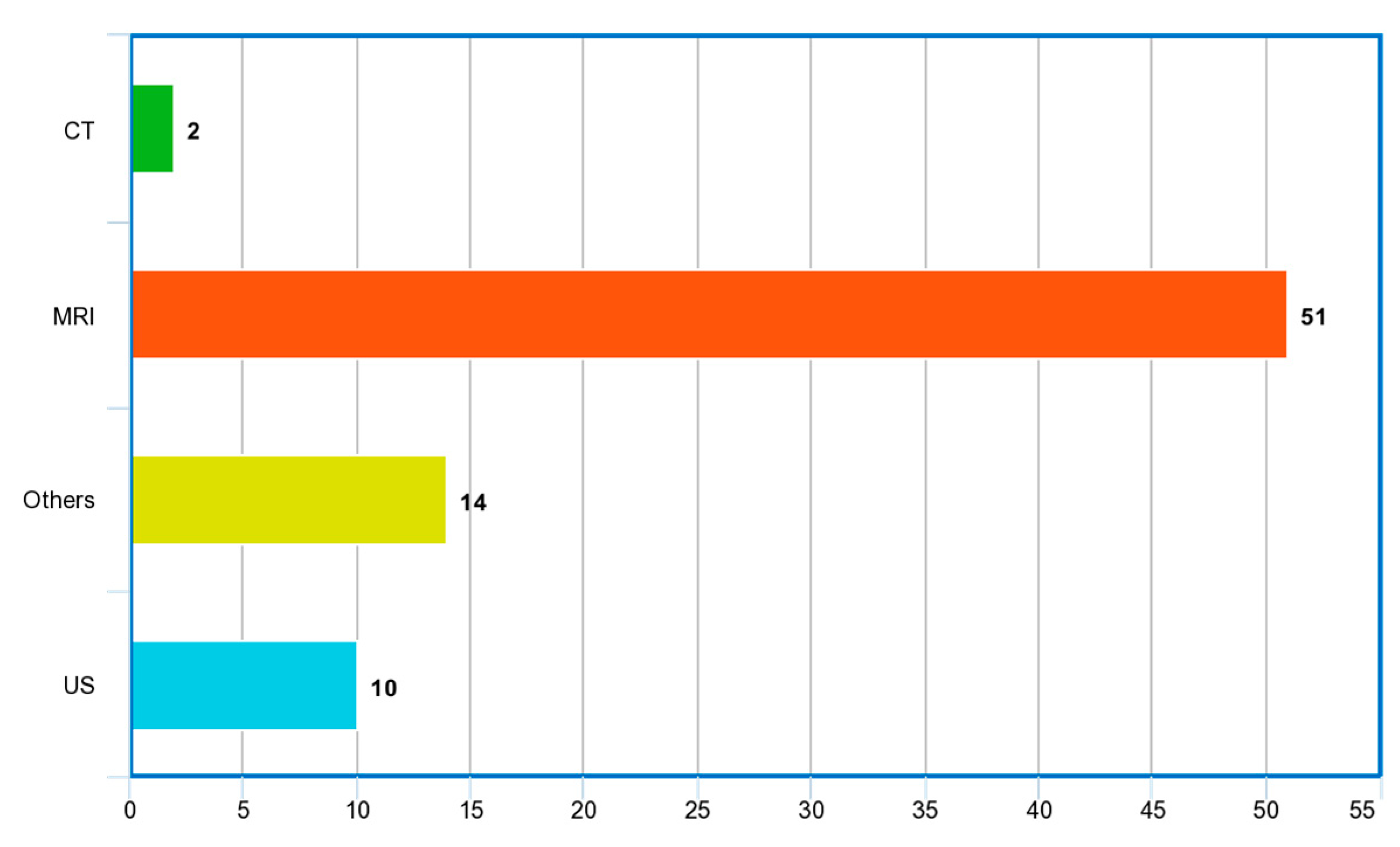
Figure 11.
Country distribution of reviewed studies.
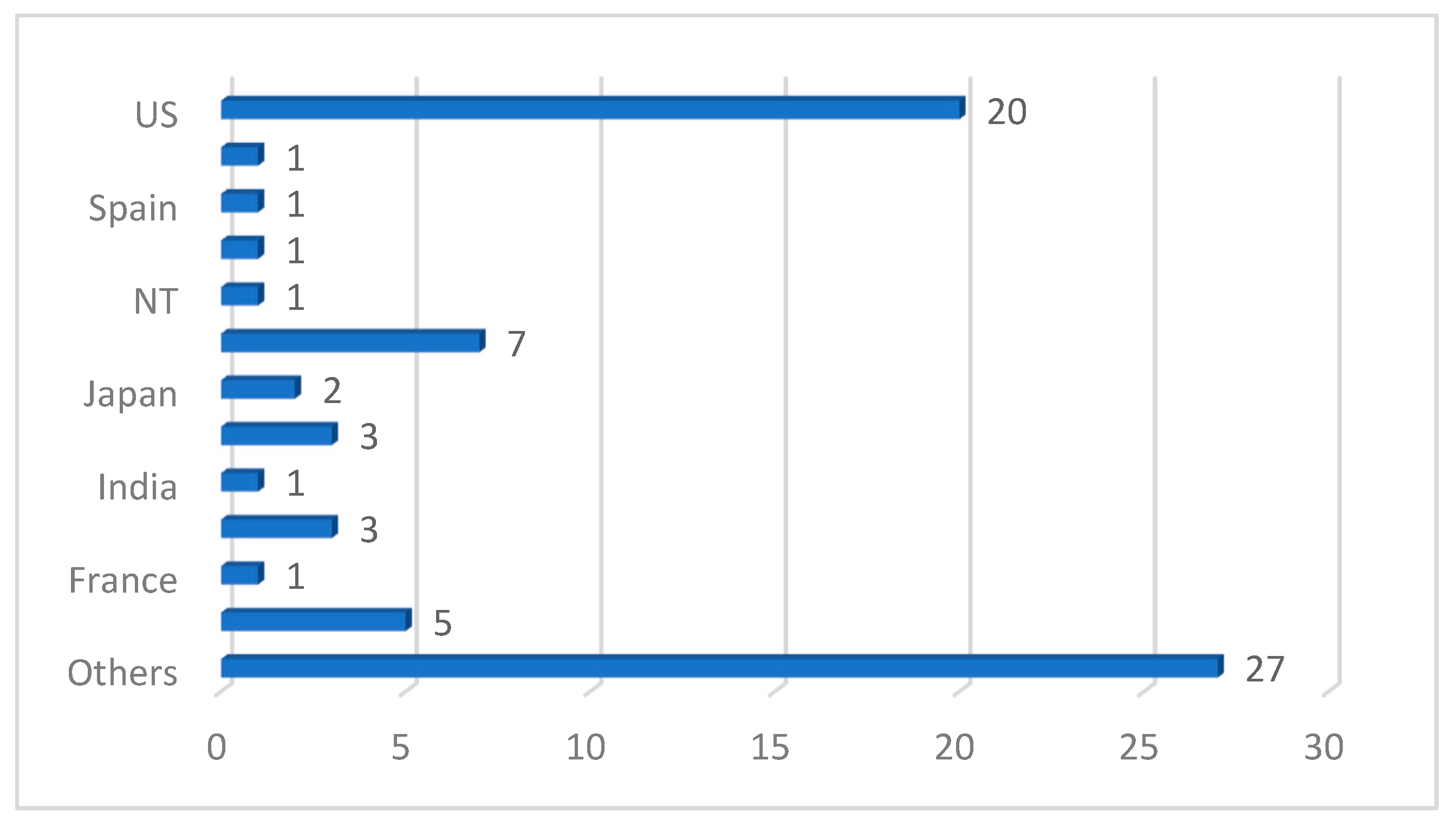

Table 1.
Some selected related systematic review and survey articles for deep learning diagnosis of PCa in Clinical Patients.
Table 1.
Some selected related systematic review and survey articles for deep learning diagnosis of PCa in Clinical Patients.
| Ref. | Year | Articles Included | Work Done |
|---|---|---|---|
| [20] | 2019 | 43 | Authors investigated current and future applications of ML and DL urolithiasis, renal cell carcinoma, and bladder and prostate cancer. Only PubMed database was used. It was concluded in study that machine learning techniques outperform classical statistical methods. |
| [21] | 2020 | 28 | Study investigated deep learning methods for CT and MRI images for PCa diagnosis and analysis. It was concluded that most deep learning models are limited by the size of the dataset used in model training. |
| [22] | 2021 | 100 | Study investigated 22 machine learning and 88 deep learning-based segmentation of only MRI images. Authors also presented popular loss functions for the training of these models and discussed public PCa-related datasets. |
| [23] | 2022 | 8 | Authors reviewed eight papers on the use of bi-parametric MRI (bpMRI) for deep learning diagnosis of clinically significant PCa. It was discovered that although deep learning proves highly performing in terms of accuracy, there is lower sensitivity when compared to human radiologists. Dataset size has also been identified as a major limitation in these deep learning experiments |
| [24] | 2020 | 27 | Embase and Ovid MEDLINE databases were searched for application of ML and DL for differential diagnosis of PCa using multi-parametric MRI. |
| [25] | 2022 | 29 | Authors investigated the current value of bpMRI using ML and DL in the grading, detection and characterization of PCa. |
| [26] | 2022 | 24 | Authors reviewed the role of deep learning in PCa management. Study also recommended that focus should be on model improvement in order to make these models verifiable as well as clinically acceptable. |
Table 2.
Distribution of publications included in the study according to databases consulted after screening.
Table 2.
Distribution of publications included in the study according to databases consulted after screening.
| SN | Databases | URL | Count | % Count |
|---|---|---|---|---|
| 1 | IEEE Xplorer | https://ieeexplore.ieee.org | 16 | 20.78 |
| 2 | Springer | https://link.springer.com | 23 | 29.87 |
| 3 | ScienceDirect | https://sciencedirect.com | 29 | 37.66 |
| 4 | PubMed | https://pubmed.ncbi.nlm.nih.gov/ | 9 | 11.69 |
Table 3.
Springer Papers on Prostate Cancer Detection using Machine Learning, Deep Learning or Artificial Intelligence Methods.
Table 3.
Springer Papers on Prostate Cancer Detection using Machine Learning, Deep Learning or Artificial Intelligence Methods.
| Ref. | Year | Imaging Modality | ML/DL Model | Problem Addressed | Metrics Reported | Hyperparameter Reported | Country | Citations | MV | Dataset | ML Type |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [19] | 2017 | MRI | DCNN, SIFT-BoW, Linear-SVM | Comparison between deep learning and non-deep classifier for performance evaluation of classification of PCa. | AUC=0.84, Sensitivity = 69.6%, Specificity = 83.9%, PPV=78.6%, NPV=76.5% | Gamma= 0.1, momentum= 0.9, weight decay = 0.1, Max Training iteration = 1000, 10-fold CV | China | 175 | Y | 172 Samples | SL/PD |
| [62] | 2020 | WSI | CNN, DenseNet121 | Classifying PCa tissue with weakly semi-supervised technique | - | Batch-size =128,32, learning rate = , decay -rate = , Adam optimizer | - | 11 | N | 1368 Whole Slides Images | Semi-SL/SD |
| [63] | 2023 | bpMRI | PI-RADS, CNN (ResNet3D, DenseNet3D, ShfeNet3D, and MobileNet3D) | Predicting clinically significant prostate cancer with a deep learning approach in a multi-centre study. | Sensitivity = 98.6%, p-value>0.99, Specificity = 35.0% | cross-entropy loss, Adam optimizer, learning rate = 0.01, epochs =30, batch size=32 | China | 1 | Y | 1861 patients | SL |
| [64] | 2021 | MRI | Ga-PSMA-11 SUV (Ensemble ML), RH | Classification of patient overall risk with ML on high or low lesion in PCa | AUC =0.86 | 1000-fold CV, | - | 58 | Y | 52 Patients | - |
| [65] | 2020 | US | RF | Localization of PCa lesion using multiparametric ML on transrectal US. | ROC-AUC for PCa and Gleason>3+4 = 0.75, 0.90 | Depth = 50 nodes, | NT | 62 | Y | 50 Patients | SL/PD |
| [66] | 2019 | MRI | CNN, ResNet | Clinically significant PCa detection using CNN | AUC= 0.87 | ReLU, learning rate = 0.001, batch size = 8, dropout rate = 0.90, weight decay = 0.000001 and momentum = 0.90 | - | 134 | Y | 427 Patients | SL/SD |
| [67] | 2020 | mpMRI | Radiomics ML (RML), SVM | ML model capable of predicting PI-RADS score 3 lesions differentiating between non-csPCa from csPCa. | AUC =0.89 | misclassification penalty = (0.1- 10, 0.1), Regressionloss epsilon = (0.1- 10, 0.1) and numerical tolerance | - | 22 | Y | 263 Patients | - |
| [68] | 2021 | MRI | Dense NN, | PCa risk classification using ML techniques | AUC=0.72, Sensitivity = 80%, Specificity = 45.3% | Epochs =2500, stochastic gradient descent, learning rate = 0.001, drop-out layers = 50% | - | 15 | Y | 4548 Patients | SL |
| [12] | 2019 | MRI | Deep convolutional encoder-decoder, CNN | Prostate detection, segmentation and localization in MRI. | AUC=0.995, Accuracy=0.894, recall =0.928 | Epochs= 100, learning rate = 0.001, batch-size = 2 | - | 78 | N | 19 Patients | SL/SD |
| [69] | 2020 | WSI | DenseNetFCN, U-Net, EfcientNet | Impact of Scanning systems and cycle-GAN-based normalization on performance of DL algorithms in detecting PCa | AUC =0.98, Sensitivity = 1, Specificity = 0.5-0.75 | CV = 3, batch size = 3, learning rate = 0.0005, Stochastic gradient descent, categorical cross entropy lossfunction | - | 37 | N | 582 slides | SL/SD |
| [70] | 2019 | Histopathological images | Transfer learning, deep CNN | Transfer learning approach from breast histopathological images for detection of PCa | AUC = 0.936 | Epochs = 50 | US | 14 | Y | ImageNet, BrCa | SL/SD |
| [71] | 2015 | US | DBN, SVM, | Developed a feature extraction framework from US Prostate tissue. | AUC = 0.91, Accuracy = 93%, Sensitivity = 98%,and Specificity =90% | Radial basis function, leave-one-core-out CV | - | 35 | N | 31 Patients with 35 biopsy cores | SL/NG |
| [72] | 2020 | US, bpMRI | FCN, U-Net | Multimodality to improve detection of PCa in cancer foci during biopsy | AUC for PCa foci= 0.76, of all PCa with larger foci = 0.89 | Mini-batch stochastic gradient descent with Adam update rule, learning rate = , Exponentially decayed = 0.75 epochs = 10 | - | 21 | N | 107 patients with 145 biopsy cores | SL |
| [73] | 2022 | CT | CNN | Image-based PCa staging support system | AP = 80.4%, (CI: 71.1–87.8), Acc = 77% (CI: 70.0–83.4) | 4-fold CV = 121 | - | 19 | Y | 173 subjects (F-FDG data) | SL |
| [74] | 2020 | mpMRI | 3D-CNN | Risk assessment of csPCa using mpMRI | Hosmer-Lemeshow calibration test p = 0.41 and good discrimination (C = 0.85) | Cross-entropy loss function, Adam optimizer with learning rate = and weight decay = , epochs =100 | - | 16 | Y | 499 Patients | - |
| [75] | 2022 | bpMRI | deep learning masked (DLM) | Proposed a better segmentation technique of csPCa. | AUC = 0.76 | CV = 10, Optuna objective function, cross-entropy, Adam optimizer | - | 4 | N | 930 patients with 524 PCa lesions | - |
| [76] | 2020 | mpMRI | ResNet50, FPN, UNet, Mask R-CNN | Lesion detection and novel segmentation method for both local and global image features | Sensitivity =89%, 85% False Positive= 0.94 and 0.62 per patient,ROC curve (AUC) = 0.897 | binary cross entropy, Adam optimizer, learning rate = , epochs = 100 | - | 18 | Y | 243 patients | SL/PD |
| [77] | 2021 | CT | CNN | Incident detection of csPCa on CT scan | ROC-AUC = 0.88 (95%CI 0.86–0.90) per patient csPCa detection on CT, Sensitivity = 0.56, Specificity = 0.99 | cross entropy loss function, CV =5, AdamW optimizer (weight decay) | - | 7 | N | 571 scans | SL |
| [78] | 2019 | WSI | DLS, CNN, InceptionV3 | Gleason grading of whole-slide images of prostatectomies | Accuracy = 0.70 | - | United States | 320 | Y | 1226 slides | SL |
| [79] | 2020 | WSI | NASNetLarge, CNN | Detection of PCa tissue in whole-slide images | Accuracy = 97.3% | - | - | 81 | Y | 600 slides | SL |
| [80] | 2022 | WSI | CNN | Segmentation and grading of epithelial tissue for PCa region detection | Accuracy = 89.4%, κquad = 0.92 | - | India | 15 | Y | 3741 biopsies | SL |
| [81] | 2022 | WSI | DeepHealth-based DL | Image analysis AI support for PCa and tissue region detection | AUC = 0.986, F1-score = 0.969, Accuracy = 0.96 | CV = 5, Epochs = 30, | - | 2 | Y | 533 slides | SL |
| [82] | 2022 | Histopathological images | CNN, MobileNet-V2, ResNet50, DenseNet121, DenseNet169, VGG16, VGG19, Xception, InceptionV3, InceptionResNet-V2, and EfficientNet-B7 | Gleason grading for PCa in biopsy tissues. | Accuracy = 90.90% | - | - | 2 | N | PANDA | SL |
Table 4.
ScienceDirect Papers on Prostate Cancer Detection using Machine Learning, Deep Learning or Artificial Intelligence Methods.
Table 4.
ScienceDirect Papers on Prostate Cancer Detection using Machine Learning, Deep Learning or Artificial Intelligence Methods.
| Ref. | Year | Imaging Modality | ML/DL Model | Problem Addressed | Metrics Reported | Hyperparameter Reported | Country | Citations | MV | Dataset | ML Type |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [83] | 2022 | MRI | SPCNet, U-Net, branched UNet and DeepLabv3+ | Effect of labelling strategies on performance of PCa detection | ROC-AUC = 0.91-0.94 | loss fn, Adam optimizer, batch size = 22, epochs =30, Cross-entropy | USA | 3 | Y | 390 Patients | SL/PD |
| [84] | 2022 | MRI, US | CNN, SVM, Adaboost, K-NN, and RF | Detection of PCa with an explainable early detection classification model. | Acc = 97%. | ReLU fn | USA | 31 | N | 61,1119 images from 1151 patients | SL/SD |
| [85] | 2019 | MRI | LR, SVM on linear kernel, RF, DT and KNN | Radiomics and machine learning techniques to detect PCa aggressiveness biopsy. | AUC=0.93 | fold cross validation (K=5) | USA | 33 | Y | 40 Patients | SL/SD |
| [86] | 2021 | Histopathological images | RINGS, CNN | Segmentation of prostate glands with an ensemble deep and classical learning method | DICE = 90.16% | Batch-size =128, learning rate = , epochs=30 | - | 26 | Y | 18851 glands | SL/SD |
| [87] | 2022 | Digital camera | YOLO, CNN | A grading automated prostate cancer detection model with YOLO | Acc=97% | AF= Sigmoid, Tanh, batch size=24, max_batches=500,200,LR = 0.001, filters =27 | Turkey | 13 | Y | 500 tissue biopsy images | SL |
| [88] | 2019 | MRI | C4.5, DT, RT, RF, SVM, kNN, locally weighted learning,BN and NB | Textual Analysis and Machine Learning models to detect extraprostatic cancer. | Acc = 82%, AUC=88%, TP rate= 82%, TN =80% | fold cross validation (K=10) | Italy | 60 | Y | 39 patients | SL |
| [89] | 2021 | US | S-Mask, R-CNN and Inception-v3. | Diagnosis of PCa with integration of multiple deep leaning approaches. | Map=88%, DICE=87%, IOU=79%, AP=92% | Vector =0.001, weight decay rate=0.0001, number of iterations =3000 | China | 68 | Y | 704 images | SL |
| [90] | 2021 | MRI | GrowCut and Zernik feature extraction, Voting (KNN, SVM and MLP) | Detection of PCa with an Improved feature extraction methods with ensemble machine learning. | Acc=80.97%, Preci =76.69%, recall=77.32%, Error rate =19.02% | - | - | 9 | Y | 271 Samples | SL |
| [91] | 2021 | US | Ensemble Machine learning techniques | Prostate biopsy calculator using an automated machine learning technique. | high-grade PCa AUC=0.990, detection of PCa AUC= 0.703 | - | Serbia | 5 | Y | 832 patients | SL |
| [92] | 2022 | MRI, US | AdaBoost, RF | Upgrading a patient from MRI targeted biopsy to active surveillance with machine learning model. | Acc= 94.3%, 88.1%, Pre=94.6%, 88.0%, Recall = 94.3%, 88.1% for Adaboost and RF. | - | USA | 3 | Y | 592 patients | SL/PD |
| [93] | 2022 | US | Region labeling object detection (RLOD), Gleason grading network (GNet) | A pathological grading of PCa on single US image. | Pre= 0.830, mean Dice=0.815 | - | - | 0 | Y | ||
| [94] | 2020 | MRI | U-Net | A radiomics deeply supervised Segmentation method for prostate gland and lesion | mean Dice Similarity Coefficient (DSC) = 0.8958 and 0.9176 | - | - | 35 | Y | 50 Patients | SL/SD |
| [95] | 2023 | MRI | GBDTs, Multilayer perceptions, CNN, and Transformers. | Performance comparison of promising machine learning models on a typical PCa radiomics. | MCC=4.47, AUC Rank = 4, Acc =4.0 | - | Italy | 1 | Y | 949 PCa patients | SL/PD |
| [96] | 2018 | MRI | SVM | SVM on Gleason grading of PCa based image features (mpMRI) | AUC=0.99 | 10-fold cross-validation | - | 67 | 48 PCa patients | SL | |
| [97] | 2021 | MRI | ProsRegNet | Deep learning model to simplify PCa image registration in order to map regions of interest. | Dice-Co=0.96-0.98, H dis=1.7-2.0mm, UD =2.4-2.9mm and landmark error =2.7mm | 50 epochs | USA | 34 | Y | 152 Patients | |
| [98] | 2019 | US | RF Classifier | An interpretable PCa ensemble deep learning model to enhance decision making for clinicians. | Acc= 0.8602, Sensitivity= 0.8571, specificity= 0.8923 | Tree no =50, depth of tree =5 | China | 114 | N | 1402 cases | SL/SD |
| [99] | 2022 | MRI | CorrSigNIA, CNN | Ensemble feature extraction methods for PCa aggressiveness and indolent detection. | Acc =80%, ROC-AUC= 0.81±0.31 | Epochs=100, batch size =8, Adam optimizer, learning rate = , weight decay = 0.1 | USA | 14 | Y | 98 Men | SL |
| [100] | 2021 | MRI | CNN | Detection of PCa using 3D-CAD in bpMR images | Sen = 75.31± 3.64%, Spec = 85.83 ±2.22%, kappa =76.69%,81.08% | - | Netherlands | 58 | Y | 1950 scans, 2317 patients | SL/PD |
| [101] | 2017 | MRI | SVM, RF | PCa localization and classification with ML. | Global ER=1%, Sens=99.1% and Speci= 98.4% | - | Germany | 35 | Y | 34 patients | SL/SD |
| [102] | 2021 | MRI | CNN, 3D AlexNet | Segmentation of MR images tested on DL methods. | Acc =0.921, Speci = 0.896, Sens = 0.902, AUC= 0.964, MAD= 0.356 mm, HD= 1.024 mm, Dice= 0.9768. | - | - | 53 | Y | 500 PCa patients | SL/PD |
| [103] | 2018 | MRI | DNN | Segmenting MR images of PCa using deep learning separation techniques | Dice=0.910 ± 0.036, ABD = 1.583 ± 0, Hausdorff Dis = 441,4.579 ± 1.791 | - | Norway, US, UK, Netherlands | 85 | N | 304 Samples (PROMIS12, PROSTATEx17) | SP/SD |
| [104] | 2022 | MRI | CNN, RMANet | Detection of PCa leveraging on the strength of multi-modality of MR images. | AUC = 0.84, Sens = 0.84, Speci = 0.78 | cross-entropy loss, batch size = 2, trained epochs = 200, Adam optimization method, learning rate= 1e-5 | Japan | 1 | Y | 379 Samples | SL, UL (for features extraction), SD |
| [105] | 2023 | MRI | GANs | GANs were investigated for detection of PCa with MRI. | AUC=0.73, Average AUCs SD = 0.71 ± 0.01 and 0.71 ± 0.04. | GANs parameters were maintained. | Norway, US, UK, Netherlands | 0 | Y | 1160 Samples | SL/SD |
| [106] | 2019 | MR guided biopsy | VGG-16 CNN, J48 | Gleason grading for PCa detection with deep learning techniques. | Quadratic weighted kappa score = 0.4727, Positive predictive = 0.9079 | - | Norway, US, UK, Netherlands | 39 | N | PROSTATEx-2 dataset () | SL/SD |
| [107] | 2020 | MRI | Hierarchical clustering (HC) | HC for early diagnosis of PCa | Acc =96.3% in and TZ=97.8% | - | Netherlands | 10 | N | 50 subjects | US/PD |
| [108] | 2017 | MRI | CNN, SVM | Detection of PCa in an image and lesion simultaneously with deep learning feature and a classifier. | Sens=0.46, 0.92 0.97 at FP = 0.1,1,10 | SoftMax function | - | 126 | Y | 160 Patients | SL/SD |
| [109] | 2022 | mpMRI | ANN | Ensemble method of mpMRI and PHI for diagnosis of early PCa | Sensi = 80%, Speci=68% | - | - | 7 | Y | 177 patients | |
| [110] | 2022 | MRI | RF, CAD | An improved CAD MRI for significantly PCa detection. | AUC = 0.72 | - | - | 1 | Y | 150 samples | SL/PD |
| [111] | 2020 | WSI | DLN, CNN | Compared deep learning models for classification of PCa with GG | kappa score = 0:44 | Layer = 121, LR = 0.0001, Adam optimizer | - | 17 | 341 Sliding Images | SL/SD |
Table 5.
Elsevier Papers on Prostate Cancer Detection using Machine Learning, Deep Learning or Artificial Intelligence Methods.
Table 5.
Elsevier Papers on Prostate Cancer Detection using Machine Learning, Deep Learning or Artificial Intelligence Methods.
| Ref. | Year | Imaging Modality | ML/DL Model | Problem Addressed | Metrics Reported | Hyperparameter Reported | Country | Citations | MV | Dataset | ML Type |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [18] | 2017 | MRI | CNN, DL | Classification of MRI images for easy diagnosis of PCa. | Accuracy for training = 0.80, Accuracy for testing = 0.78 | ReLU | China | 33 | N | Patients = 200, diffusion weighted images (DWI) = 13,408 (LSVRC Dataset) | SL/SD |
| [112] | 2020 | MRI | MLR, DT, ANN, KNN, SVM,RF, LR. | Classification of prostate cancer using ML techniques. | Accuracy = 0.97, Specificity = 98%.Sensitivity= 96% | LeastAbsolute Shrinkage and Selection Operator (LASSO), log loss function | 17 | N | 387 samples with 188 PCa and 190 not PCa images. | SL/ | |
| [113] | 2018 | US | 3D-CNN | Detection of PCa in sequential CEUS images. | Specificity =91%, Average accuracy =0.90 | Layers = 6, kernels = 2-12 | Netherlands | 49 | Y | 21844 samples and non-targeted 25738 samples for (contrast-enhanced ultrasound (CEUS) imaging | SL/SD |
| [114] | 2020 | MRI | They adapted U-Net network. | A neural network that detects and grade a prostate cancer tissue. | voxel-wise weighted kappa=0:446± 0:082, Dice similarity=0:37±0 0:046 | Cross-validation =5 | Netherlands | 73 | Y | For training 99 patients and 112 lesions while 63 patients and 70 Lesions for testing. | SL/SD |
| [115] | 2021 | MRI | Long short-term memory (LSTM) and Residual Net (ResNet−101), SVM, Gaussian Kernel, (KNN − Cosine), Kernel-NB, DT, RUSBoost tree | They compared the performance of deep learning models to classical models in detection of PCa. | Accuracy =1.00, AUC = 1 | 10-fold cross-validation | USA | 40 | N | 230 patients | SL/SD |
| [116] | 2020 | WSI | CNN, | CNN based WSI for PCa detection. | Accuracy = 0.99, F1 score = 0.99, AUC = 0.99 | Cross-validation =3 | Spain | 41 | N | 97 WSI | SL/PD |
| [117] | 2020 | mpMRI | DEF, CNN, RF, NASNet-mobile | Deep entropy features (DEFs)from CNNs applied to MRI images of PCa to predict Gleason score (GS) of PCa lesions | AUC = 0.80, 0.86, 0.97, 0.98, and 0.86 | Number of trees = 500, maximum tree depth= 15 and minimum number of samples in a node = 4 | USA | 16 | Y | Patient = 99, with 112 lesions | SL/SD |
| [118] | 2018 | mpMRI | Tissue DeformationNetwork (TDN), CNN | An automated csPCa detection using deep neural network. | Sensitivity= 0.6374, 0.8978 at 0.1 and1 false positive/ patient | Cross-validation = 5, loss function (classification loss, inconsistency loss and overlap loss), | Germany | 124 | N | 360 patients | SL/SD |
| [119] | 2017 | WSI | R-CNN | Epithelial cells detection and Gleason grading in histological images | Accuracy = 0.99,AUC = 0.998, | Cross validation = 5 | USA | 97 | N | 513 images from 20 patients | SL/SD |
| [120] | 2020 | MRI | Deep-CNN, EfficientDet, YOLOv4, YOLOv5 | Detecting PCa lesions in MRI with minimal dataset | Accuracy = 52.63% | 0 | |||||
| [121] | 2018 | Diffusion weighted MRI | CNN | Early diagnosis of PCa using CNN-CAD system | Accuracy = 0.96, Sensitivity = 100%, Specificity = 91.67% | ReLU, layers = 6 | 48 | Y | 23 Patients | SL/PD | |
| [122] | 2019 | mpMRI | FocalNet (Multi-class CNN) | Detection of PCa and Gleason grading for PCa aggressiveness | Sensitivity= 89.7%, 87.9%, e AUC = 0.81, 0.79(PCa for GS≥3+4 and PCa GS≥4+3) | Cross validation = 5 | Germany | 131 | Y | 417 patients | SL/PD |
| [123] | 2022 | MRI | CNN, Inception-v3, Inception-v4, Inception-Resent-v2=, Xception, PolyNet | Detection of PCa with CNN | Accuracy = 0.99 | 0 | N | 1524 samples | SL/SD | ||
| [124] | 2019 | MRI | SVM | Classify PCa lesions into high-grade and low-grade | AUC= 77[0.66-0.87], Sensitivity 0.74[0.57-0.91], Specificity = 0.66[0.50-0.82 | Cross validation = 100 | Netherlands | 13 | Y | 40 Patients with 72 lesions | SL/SD |
| [125] | 2019 | MRI | FCNN | Improved MRI segmentation for PCa | Average mean Dice Coefficient (DSC) of EndorectalCoil (ERC) = 0.8576,Average DSC of non-ERC = 0.8727 | Cross validation = 50, ADAM optimizer, learning rate = 0.001, batch size = 32, epoch = 25, dropout = 0.2 | France | 35 | Y | PROMISE12 dataset (50 Volume of MRI) | SL/SD |
| [126] | 2019 | TRUS | Linear SVM, KNN, RF, Multilayer perceptron, DT, LDA | Improved TRUS for detection of csPCa | Accuracy =0.79, PPV = 95% | Cross validation =11 | USA | 2 | Y | 30 Patients | SL/PD |
Table 6.
PubMed Papers on Prostate Cancer Detection using Machine Learning, Deep Learning or Artificial Intelligence Methods.
Table 6.
PubMed Papers on Prostate Cancer Detection using Machine Learning, Deep Learning or Artificial Intelligence Methods.
| Ref. | Year | Imaging Modality | ML/DL Model | Problem Addressed | Metrics Reported | Hyperparameter Reported | Country | Citations | MV | Dataset | ML Type |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [127] | 2022 | mpMRI | CNN | The aggressiveness of PCa was predicted using ML/DL frameworks | AUROC – 0.75Specificity –78%Sensitivity –60% | 5-fold CV, 87-13 train-test splitting | Italy | 20 | Y | 112 patients | SL/SD |
| [128] | 2022 | PSA, Biopsy | RNN | Survival analysis of localized prostate cancer was conducted | - | 80/20 splitting | USA | 1 | Y | 112,276 samples | SL/PD |
| [129] | 2020 | MRI | CNN (GoogleNet) | Transfer learning approach with CNN framework for detecting PCa | AUC-1.00Accuracy-100% | ReLU activationMax pooling | USA | 71 | N | 230 Images | SL/SD |
| [130] | 2021 | bpMRI | Logistic Regression | Construction of integrated nomogram combining deep-learning-based imaging predictions, PI-RADS scoring and clinical variables to identify csPCa on bpMRI | AUC – 0.81 | - | USA | 31 | Y | 592 patients | SL/SD |
| [131] | 2022 | bpMRI | CNN-UNet | UNet-based PCa detection system using MRI. | Sensitivity – 72.8%PPV – 35.5% | 70/30 splitting, Dice Coefficient used | USA | 7 | Y | 525 patients | SL/PD |
| [114] | 2020 | bpMRI | CNN-UNet | DL regression analysis for PCa detection and gleason sscoring | Weighted kappa of 0.446 ± 0.082, Dice similarity coefficient of 0.370 ± 0.046, | Dice Coefficient used, 5 fold CV | Netherlands | 75 | Y | - | SL/SD |
| [132] | 2021 | mpMRI | CNN-UNet | Development of a UNet architecture for PCa detection with minimum training data size with effect of prior knowledge | Sensitivity – 87%AUC – 0.88 | -- | Netherlands | 36 | Y | 1952 patients | SL/SD |
| [133] | 2021 | MRI + histological data | CNN-GoogleNet | Bi-modal deep learning model fusion of Pathology-Radiology data for PCa diagnostic classification | AUC – 0.89 | - | USA | 33 | Y | 1484 images | SL/PD |
| [134] | 2019 | mpMRI | Multi-layer ANN | ANN was used to accurately predicted PCa withoutbiopsy marginally better than LR | - | 5 fold CV,Cross-entropyLearning rate 0.0001L2 regularization penalty of 0.0005 | Japan | 37 | Y | 334 patients | SL/PD |
Abbreviations: MRI—Magnetic Resonance Imaging, SVM—Support Vector Machine, LDA—Linear discriminant analysis, QDA—Quadratic discriminant analysis, RINGS Rapid—Identification of Glandular Structures, YOLO—You only look once, BN—Bayesian Network, ROC—Receiver operating characteristic, NB—Naïve Bayes, TP—True Positive, TN—True Negative, R-CNN—Region-based Convolutional Neural Networks, AUC—Area under the ROC Curve, SL—Supervised Learning, UL —Unsupervised Learning, PD—Primary Data, SD—Secondary Data, SVM-RBF— SVM-Radial basis function kernel classifier, PPV—Positive Predictive Value , NPV—Negative Predictive Value , Y—Yes, N—No, ML—Machine learning , DL—Deep learning , MV—Medic Verification, CNN—Convolutional Neural Network , PCa—Prostate Cancer, mpMRI—Multiparametric Magnetic Resonance Imaging, bpMRI—Biparametric Magnetic Resonance Imaging, USA—United State of America, WSIs—Whole Slides Images, PI-RADS—Prostate Imaging Reporting & Data System, TeUS—Temporal Enhanced Ultrasound , US—Ultrasound, RF—Random Forest Classifier, PSA—Prostate-specific antigen, ANN—Artificial Neural network, AUC-ROC—Area under the Receiver operating characteristic Curve, ResNet—Residual Network, ReLU—Rectified linear unit, csPCa—Clinically significant Prostate Cancer, PLCO—Prostate, Lung, Colorectal and Ovarian, Densenet—Densely-connected-convolutional networks, GAN—Generative Adversarial Networks, BRCA—Breast Cancer gene, DPN—Deep Believe Network, FCN—Fully Convolutional Network, CT—Computerized Tomography , Cl—Confidence level, RNA-Seg—RNA sequencing, CLSTM—bi-directional convolutional long short-term memory, BPH—benign prostatic hyperplasia , RFE—Recursive Feature Elimination, LR—Logistic Regression, DLS—Deep Learning System, k—kappa coefficient, KN—K-neighbors , DT—Decision tree , MLPC—Multi-layer perceptron classifier, MLP—Multilayer perceptron, ADA—Adaptive boosting, QWK—Quadratic Weighted Kappa, IoU—Intersection over union, AP— Average precision, NN—Neural Network, GBDTs—Gradient-boosted decision trees (GBDTs), CACN—Channel attention classification network, DSC — Dice Similarity Coefficient, MCCM— Matthew's correlation coefficient, SVM-PCa-EDD—Support vector machine for early differential diagnosis of PCa, CAD — Computer Aided Design, RMANet— Multi-modal Feature Autoencoder Attention net.
Table 7.
Top 10 most impactful papers.
| Ref | Title | Journal | Publisher | Year | Citation | Impact Index |
|---|---|---|---|---|---|---|
| [78] | Development and validation of a deep learning algorithm for improving Gleason scoring of prostate cancer. | NPJ digital medicine | Nature | 2019 | 320 | 80 |
| [89] | Deep learning framework based on integration of S-Mask R-CNN and Inception-v3 for ultrasound image-aided diagnosis of prostate cancer. | Future Generation Computer Systems | Elsevier | 2021 | 68 | 34 |
| [66] | Prostate cancer detection using deep convolutional neural networks. | Scientific reports | Springer | 2019 | 134 | 33.5 |
| [122] | Joint prostate cancer detection and Gleason score prediction in mp-MRI via FocalNet. | IEEE transactions on medical imaging | IEEE | 2019 | 131 | 32.75 |
| [84] | Prostate cancer classification from ultrasound and MRI images using deep learning based Explainable Artificial Intelligence. | Future Generation Computer Systems | Elsevier | 2022 | 31 | 31 |
| [19] | Searching for prostate cancer by fully automated magnetic resonance imaging classification: deep learning versus non-deep learning. | Scientific reports | Springer | 2017 | 175 | 29.16667 |
| [64] | Supervised machine learning enables non-invasive lesion characterization in primary prostate cancer with [68 Ga] Ga-PSMA-11 PET/MRI. | European journal of nuclear medicine and molecular imaging | Springer | 2021 | 58 | 29 |
| [100] | End-to-end prostate cancer detection in bpMRI via 3D CNNs: effects of attention mechanisms, clinical priori and decoupled false positive reduction. | Medical image analysis | Elsevier | 2021 | 58 | 29 |
| [98] | Stacking-based ensemble learning of decision trees for interpretable prostate cancer detection. | Applied Soft Computing | Elsevier | 2019 | 114 | 28.5 |
| [79] | High-accuracy prostate cancer pathology using deep learning. | Nature Machine Intelligence | Nature | 2020 | 81 | 27 |
Table 8.
Summary of considerations for choice of deep learning models for PCa diagnosis using medical images.
Table 8.
Summary of considerations for choice of deep learning models for PCa diagnosis using medical images.
| Model | Considerations |
|---|---|
| Convolutional Neural Networks (CNN)[116,121,135] | CNNs are the most used deep learning method for PCa image analysis tasks. They are effective in capturing spatial patterns and features from images. CNN architectures, such as VGG, ResNet, and Inception, have achieved remarkable success in various cancer image analysis applications, including detection, classification, and segmentation. |
| Recurrent Neural Networks (RNN)[136,137] | RNNs are suited for sequential data, such as time-series or sequential medical data. In cancer image analysis, RNNs are often used for tasks like analyzing electronic health records or genomic data to predict cancer outcomes or identify potential biomarkers. |
| Generative Adversarial Networks (GAN) [138,139] | GANs are used for generating synthetic data or enhancing existing data. In cancer image analysis, it can be employed to generate realistic synthetic images for data augmentation or to address data imbalance issues. GANs can also be used for image-to-image translation tasks, such as converting MRI images to PET images for multi-modal analysis. |
| Capsule Networks[140,141] | Capsule Networks are an alternative to CNNs that aim to capture hierarchical relationships between features. They have shown promise in tasks such as lung cancer detection in CT scans. Capsule Networks offer the advantage of better handling spatial relationships and viewpoint variations within images. |
| Attention Models[142,143] | Attention mechanisms have been integrated into deep learning models for cancer image analysis to focus on relevant regions or features. They help to identify important areas in the image and improve the interpretability and performance of the model. Attention mechanisms can be applied in CNNs, RNNs, or other architectures. |
| Transfer Learning[129,144] | Transfer learning involves utilizing pre-trained models trained on large-scale datasets and adapting them to cancer image analysis tasks. By leveraging the learned features from pre-training, transfer learning enables effective learning even with limited labeled medical data. |
Table 9.
Considerations for choice of loss functions in deep learning.
| Loss Functions | Considerations |
|---|---|
| Mean Squared Error (MSE) loss[149,150] | MSE loss measures the average squared difference between predicted and target values. It is commonly used for regression tasks. It penalizes large errors heavily, which can be useful when the magnitude of errors is important. However, it is sensitive to outliers and can result in slow convergence. |
| Binary Cross-Entropy Loss[151,152] | Binary cross-entropy loss is used for binary classification tasks. It measures the dissimilarity between the predicted probability and the true label for each binary class separately. It encourages the model to assign high probabilities to the correct class and low probabilities to the incorrect class. It is robust to class imbalance and is widely used in tasks like cancer classification. |
| Categorical Cross-Entropy Loss[152,153] | Categorical cross-entropy loss is used for multi-class classification tasks. It extends binary cross-entropy loss to handle multiple classes. It measures the average dissimilarity between the predicted class probabilities and the true one-hot encoded labels. It encourages the model to assign high probabilities to the correct class and low probabilities to other classes. |
| Dice Loss[154,155] | Dice loss is commonly used in segmentation tasks, where the goal is to segment regions of interest (ROI) in images. It measures the overlap between predicted and target segmentation masks. It is especially useful when dealing with class imbalance, as it focuses on the intersection between predicted and target masks. It can handle partial matches and is robust to the background class. |
| Focal Loss[156,157] | Focal loss is designed to address class imbalance in classification tasks, especially when dealing with rare classes. It introduces a balancing factor to downweight easy examples and focus on hard examples. It emphasizes learning from the difficult samples, helps mitigate the impact of class imbalance and improves model performance on rare classes by assigning higher weights to misclassified examples |
| Kullback-Leibler Divergence (KL Divergence) Loss [158,159] | KL divergence loss is used in tasks involving probability distributions. It measures the dissimilarity between the predicted probability distribution and the target distribution. It is commonly used in tasks such as generative modeling or when training variational autoencoders. |
Table 10.
Some publicly available databases for PCa datasets.
| Databases | Description |
|---|---|
| The Cancer Genome Atlas (TCGA)[160–164] | TCGA provides comprehensive molecular characterization of various cancer types, including prostate cancer. It includes genomic data, gene expression profiles, DNA methylation data, and clinical information of patients. |
| The Prostate Imaging-Reporting and Data System (PI-RADS)[165,166] | PI-RADS is a standardized reporting system for prostate cancer imaging. Datasets based on PI-RADS provide radiological imaging data, such as MRI scans, annotated with regions of interest and corresponding clinical outcomes. |
| The Prostate Imaging Database (PRID) | PRID is a database that contains MRI data of prostate cancer patients, along with associated clinical information. It can be used for developing and evaluating machine learning algorithms for prostate cancer detection and segmentation. |
| The Prostate Cancer DREAM Challenge dataset[167,168] | This dataset was part of a crowdsourced competition aimed at developing predictive models for prostate cancer prognosis. It includes clinical data, gene expression profiles, and survival outcomes of prostate cancer patients. |
| The Cancer Imaging Archive (TCIA)[169,170] | TCIA (https://www.cancerimagingarchive.net/) provides a collection of publicly available medical imaging data, including some datasets related to prostate cancer. While not exclusively focused on prostate cancer, it contains various imaging modalities, such as MRI and CT scans, from patients with prostate cancer. |
| SPIE-AAPM-NCI PROSTATEx Challenge[171,172] | The SPIE-AAPM-NCI PROSTATEx Challenge dataset for prostate cancer (https://wiki.cancerimagingarchive.net/display/ProstateChallenge/PROSTATEx+Challenges) was released as part of a challenge aimed at developing computer-aided detection and diagnosis algorithms for prostate cancer. It includes multi-parametric MRI images, pathology data, and ground truth annotations. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



