
Submitted:
18 August 2023
Posted:
18 August 2023
You are already at the latest version
Abstract
We conducted a retrospective analysis of the immunohistochemical (IHC) staining GRP94, an ER stress protein on large B-cell lymphoma (LBCL) cells, intracellular p53, and 15 factors involved in the metabolism of CHOP regimen :AKR1C3 (HO-metabolism), CYP3A4 (CHOP-metabolism) and HO efflux pumps (MDR1, MRP1). The study subjects were 42 patients with LBCL at our hospital. IHC staining using antibodies against the 17 factors. The odds ratios by logistic regression analysis using a dichotomous variable of CR, non-CR/relapse were statistically significant: for MDR1, MRP1, and AKR1C3. The overall survival (OS) after R-CHOP was compared by the log-rank test. The four groups showed that Very good (5-year OS, 100%) consisted of 4 patients showed negative IHC staining for both GRP94 and CYP3A4. Very poor (1-year OS, 0%), consisted of 3 patients who showed positive results of IHC for both GRP94 and CYP3A4. The remaining 35 patients comprised two subgroups: Good (5-year OS 60-80%.): 15 patients who showed negative staining for both MDR1 and AKR1C3, Poor: 5-year OS, 10-20%) :20 patients who showed positive staining for either MDR, AKR1C3,,MRP1 or p53. The Histological Prognostic Index (HPI) (The four groups: Very poor, Poor, Good, and Very pood) is a breakthrough method for stratifying patients based on factors involved in the development of treatment resistance.
Keywords:
Large B-cell lymphoma (LBCL)
; Immunohistochemical (IHC) staining
; Glucoseregulated protein 94 (GRP94)
; CYP3A4
; Multidrug resistance protein 1 (MDR1)
; Aldo-keto reductase family 1 member C3 (AKR1C3)
; Multi-drug resistance-associated protein 1 (MRP1)
; P53
Introduction
R-CHOP is the standard treatment for LBCL, although about 40% of patients with this disease receiving R-CHOP develop treatment resistance1). Comprehensive analyses for numerous genes that might be potentially involved in treatment resistance have been conducted with the objective of developing strategies to overcome treatment resistance in these patients2)3). On the other hand, for many functional proteins involved in treatment resistance, the majority of studies have been published as one-off reports, and there are no reports of comprehensive analyses. In this study, we attempted a retrospective comprehensive analysis of 17 important functional proteins reported to be involved in the development of treatment resistance.
We conducted IHC analysis of specimens obtained from patients with LBCL using antibodies directed at the 17 proteins. The study included analyses for the following proteins in (1)-(4) as follows:
- (1)
- ER stress proteins: glucose-regulated protein 94 (GRP94)4)-6), GRP787)8), transforming growth factor β1 (TGFβ1)9)10), and tumor necrosis factor α1 (TNFα1)11). They act to overcome various stressful conditions in the tumor microenvironment, including hypoxia, hypoglycemia, dysregulation of homeostasis, altered cellular metabolism.
- (2)
- AS enzymes involved in anticancer drug metabolism, the following three enzymes were selected: Aldo-keto reductase family 1 member C3 (AKR1C3)12)-16), CYP3A417)18), and CYP2B619). AKR1C3 lowers the activities of hydroxyl doxorubicin (H) and oncovin (O) (HO of CHOP)14). ,The risk for disease progression and death increases in patients with LBCL carrying AKR1C312). CYP3A4 inactivates many anticancer drugs including CHOP. Therefore, intratumoral drugs, such as PTCL, may be further inactivated. Expression of CYP3A4 as a predictor of response to chemotherapy in peripheral T-cell lymphomas17). As a result, the efficacy of these drugs may be lowered, which leads to the development of drug resistance17)18). CYP62B6 activates cyclophosphamide19).
- (3)
- Anticancer drug efflux pumps : multidrug resistance protein 1 (MDR1)20)-22), multidrug resistance-associated protein 1 (MRP1)23)24), and MRP425). MDR1 and MRP1 found on cell membranes are hydroxyl doxorubicin(H) and oncovin (O) (HO of CHOP) efflux pumps. Overexpression of MDR1 and MRP1 leads to the development of drug resistance in tumors20). LBCL patients without MDR1 have a good prognosis21).
- (4)
- Other items include the revised International prognostic Index (R-IPI)-poor and high-grade B-cell lymphoma (HGBCL) , such as double-hit lymphoma (DHL),MYC translocation LBCL, follicular lymphoma transformation, lymphoplasmacytic lymphoma transformation, and HIV-related Burkitt lymphoma.. In addition, double expression (MYC and BCL2), p5326), Ki-6726), CD5, glutathione-S-transferase (GST)27), presence/absence of fibrosis, and thymidine phosphate28) were also investigated.
Herein, we report that the expression levels of GRP944)-6), CYP3A4 17), MDR120)-22), AKR1C3)12)-16), p5326), and MRP1 21) were statistically significant.
Material and methods
Patients and Sample Collection
Of patients diagnosed with LBCL who received the initial treatment at our hospital between 2012 and 2020, 42 patients were selected as the study subjects (Table 1). As shown in Table 1, the histological types were DLBCL (NOS) in 28 cases (67%) and HGBCL in 14 cases (33%). HGBCL was double hit lymphoma in 4 cases (10%) and MYC translocation only in 4 cases (10%) including HIV in 1 case. As HGBL (NOS) without MYC translocation, 4 cases (10%) of transformation from follicular lymphoma (FL) and 2 cases (5%) of transformation from lymphoplasmacytic lymphoma (LPL) were included. There were 28 cases (67%) in R-IPI poor or in advanced stage, 29 cases (69%) with serum hyper LDH level.
Results of immunohistochemistry for the 17 proteins4)-28) involved in anticancer drug metabolism were determined using an optical microscope, using the FFPE samples.
Chemotherapy was started with the R-CHOP in the 42 patients. Statistical analysis was performed, and the survivals were compared by the log-rank test (overall survival [OS] and progression-free survival [PFS]) after the initial R-CHOP therapy and expression status of factors, etc., involved in anticancer drug metabolism. In addition, logistic regression analysis (odds ratios) was performed using the dichotomous variables of CR or non-CR/relapse after R-CHOP.
Immuno-histochemical staining
Biopsy specimens from the patients were fixed in formalin and embedded in paraffin to prepare tissue blocks, which were then sectioned and stained. The primary antibodies against the major proteins involved in anticancer drug metabolism included: (1) GRP94, Proteintech, clone 1H10B7; (2) CYP3A4, Sigma-Aldrich, SAB1400064; (3) AKR1C3, Proteintech, 11194-1-AP; (4) MDR1(P-glycoprotein), Proteintech, 22336-1-AP; (5) MRP1 (CD9), Proteintech, 60232-1-IG; (5) TGF beta1, Proteintech, 21898-1-AP; (6) GRP78, Proteintech, 66574-1-IG ; (7) glutathione S-transferase kappa1 (GST), Proteintech, 14535-1-AP; (8) thymidine phosphorylase, Abcam, ab226917; (9) MRP4 (ABCC4), SANTA CRUZ BIOTECHNOLOGY, SC-376262; (10) CYP2B6, LifeSpan BioSciences, Inc., LS-C352084; (11) TNFα1, Sigma-Aldrich, SAB4502982; After the immunostaining, two pathologists determined the results of the immuno-histochemical staining and made the definitive diagnosis. Positive judgment criteria for immuno-histochemical staining are more than 50% of tumors and weakly positive abnormalities were considered.
The concordance rate for the diagnosis was about 89%. Then, in the cases with disagreement about the diagnosis between the two pathologists, the final diagnosis was reached by consensus.
Statistical Analysis
Odds ratios were calculated by univariate logistic regression analysis using the dichotomous variable of “remission” versus “non-remission or relapse” as a dependent variable, and each “poor prognostic factor” as an independent variable. Poor prognostic factors that significantly contributed to the outcomes were evaluated.
Then, to confirm the association between the “OS” and “poor prognostic factors and factors, etc., involved in anticancer drug metabolism” after initial R-CHOP, survival curves were plotted by the Kaplan-Meier method, and factors significantly associated with the “OS” were evaluated by the log-rank test. The significance level in the statistical tests was set at α = 0.05 (two-tailed), and p< 0.05 was considered as being indicative of a significant difference. Statistical analyses were performed using the EZR software (Saitama Medical Center, Jichi Medical University, Saitama, Japan)29). Multiple comparisons were not considered because of the exploratory nature of this study.
Results
Odds ratio by Logistic regression
As shown in Table 1, after R-CHOP, 22 patients showed CR, including 16 who did not develop relapse and 6 who developed relapse, and 20 patients showed non-CR. The median OS and median PFS were 64 months and 29 months, respectively.
The odds ratios for “non-remission or relapse” relative to “remission” set as the control, identified R-IPI poor (odds ratio: 5.4, p < 0.05) and HGBCL; (6.0, p < 0.05), as well as positive expressions of MDR1 (24.00, p < 0.001), MRP1 (9.37, p < 0.05), and AKR1C3 (5.56, p < 0.01) as statistically significant poor prognostic factors. For reference, the odds ratios were 5.77 (p > 0.05) for GRP94 and 2.20 (p > 0.05) for p53, and that of CYP3A4 was not evaluable, because the calculation was not applicable.
Kaplan-Meier survival curves and between-group comparisons (log-rank test).
Table 2 shows the median cumulative survival rates in 42 LBCL patients determined by the Kaplan-Meier method and the results of between-group comparisons (p-value: log-rank test). Poor prognostic factors were evaluated in relation to differences in the survival. Statistically significant (p < 0.05) poor prognostic factors were expressions of GRP94, TGFβ1, AKR1C3, CYP3A4, and HGBCL, as indicated with (♯). In addition, statistically significant combinations of poor prognostic factors were “MRP1 or p53,” “AKR1C3+ or MDR1+,” and “GRP94+ and CYP3A4+”. The “AKR1C3 or MDR1” factor.
The detail comments in Table 2 are as follows ((1)-(4)):
(1) 4 endoplasmic reticulum stress (ER) proteins; (2) 3 metabolic enzymes of anticancer drugs; (3) 3 types of anticancer drug efflux pumps; (4) other proteins (3 prognostic indexes and 7 other proteins).
(1) As ER stress proteins, the following 4 important proteins were selected: glucose-regulated protein 94 (GRP94)4)-6), glucose-regulated protein 78 (GRP78)7)8), transforming growth factor β1 (TGFβ1)9)10), and tumor necrosis factor α1 (TNFα1)11). GRP94 and GRP78 are stress-inducible molecules released into the extracellular space. They act to overcome various stressful conditions in the tumor microenvironment, including hypoxia, hypoglycemia, dysregulation of homeostasis, altered cellular metabolism, and acidosis. TGFβ1 plays an important role in promoting tumor progression. TNF inhibits tumor progression.
(2) As enzymes involved in anticancer drug metabolism, the following three enzymes were selected: aldo-keto reductase family 1 member C3 (AKR1C3)12)-16), cytochrome p450 3A4 (CYP3A4)17)18), and CYP2B619). Aldo-keto reductase (AKR1C3) is mainly found in the cytoplasm. AKR1C3 catalyzes the reduction of carbonyl groups to water-soluble alcohol groups. AKR1C3 lowers the activities of daunorubicin, hydroxyl doxorubicin (enzyme involved in the metabolism of H), idarubicin (by 2- to 5-fold), and oncovin (enzyme involved in the metabolism of O: vincristine) (enzyme involved in the metabolism of HO)14). Patients with treatment-resistant T-ALL were found to overexpress AKR1C316). The risk for disease progression and death increases in patients with diffuse large B-cell lymphoma (DLBCL) carrying the CC genotype of AKR1C312). CYP3A4 inactivates many anticancer drugs. Therefore, intratumoral drugs, such as PTCL, may be further inactivated. As a result, the efficacy of these drugs may be lowered, which leads to the development of drug resistance17)18). CYP62B6 activates cyclophosphamide19).
(3) Three types of anticancer drug efflux pumps were selected: multidrug resistance protein 1 [MDR1, P-glycoprotein, ABC subfamily B member 1 (ABCB1)]20)-22), multidrug resistance-associated protein 1 (MRP1; ABCC1)23)24), and MRP425). MDR1 and MRP1, found on cell membranes, are oncovin hydroxyl doxorubicin (OH) efflux pumps. Overexpression of MDR1 and MRP1 leads to the development of drug resistance in tumors20). DLBCL patients with relatively low expression levels of MDR1 have a good prognosis21).
(4) Other items (2 prognostic indexes and 7 other proteins) include the revised International R-IPI poor and HGBCL), such as double-hit lymphoma (DHL), follicular lymphoma transformation, lymphoplasmacytic lymphoma transformation, and HIV-related Burkitt lymphoma. In addition, double expression (expression of both MYC and BCL2), p53, Ki-6726), CD5, glutathione-S-transferase (GST)27), presence/absence of fibrosis, and thymidine phosphate28) were also investigated.
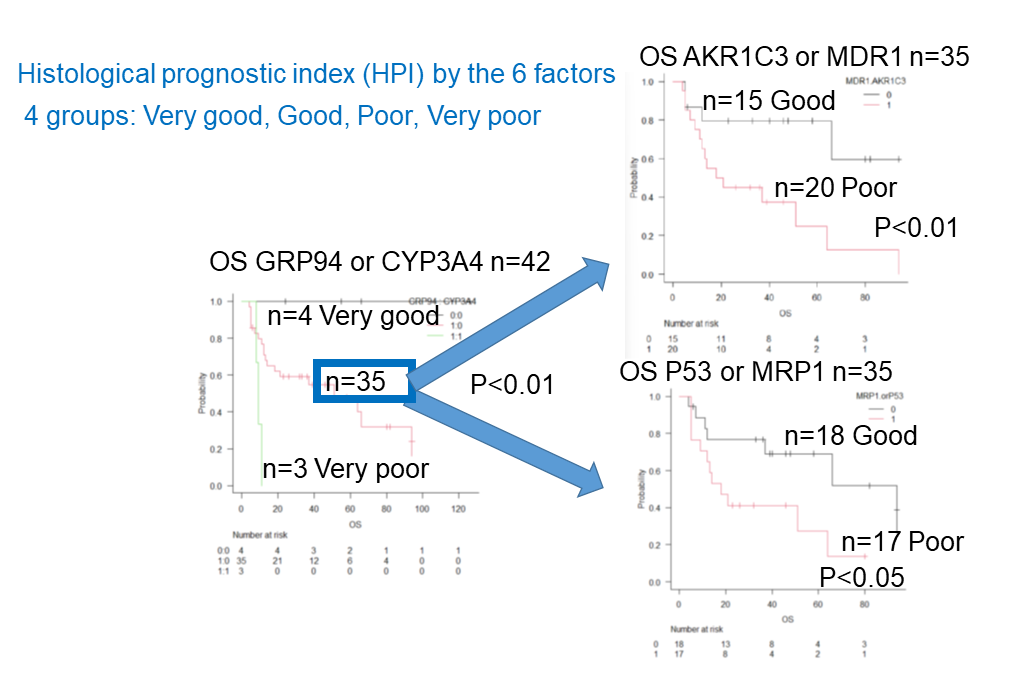
Useful results were extracted from Table 2 and are presented in Figure 1. Single prognostic factors are listed as “A” and “K” in Figure 1. The combined prognostic factors are listed from “L” to “O” in Figure 1. In particular, the three-group comparison of survival rates according to the presence or absence of GRP94 and CYP3A4 shown in Figure 1M is important.
Group 1 (n = 4), the “Very good” group, consisted of 4 patients who showed negative staining for both GRP94 and CYP3A4, including 2 patients who were censored. This group had an extremely good prognosis, and all the 4 patients survived (5-year OS: 100%). On the contrary, Group 4 (n = 3), the “very poor” group, consisted of 3 patients who showed positive staining for both GRP94 and CYP3A4. This group had a very poor prognosis and all the 3 patients died within a short period of time. The prognosis of patients in the Group 2 and 3 (n = 35) was intermediate, with the median survival of about 51 months. In Figure 1N and O, the intermediate prognosis group, that is, Group 2 (n = 35), is subdivided into “Group 2 (Good),” consisting of patients who showed negative staining for both AKR1C3 and MDR1, and “Group 2 (Good)” consisting of patients who showed negative staining for both p53 and MRP1. The remaining of Group 3 had a poor prognosis.
Taken together, we would like to propose a new concept called the Histological Prognostic Index (HPI; Urayasu classification), as a predictor of the treatment response after R-CHOP for new-onset LBCL. The HPI is classified into the following 4 groups, namely, “very good,” “good,” “poor,” and “very poor,” according to IHC for each of the 6 factors involved in LBCL: (1) Group 1 (‘Very good’ group), consisting of 4 patients who showed negative staining for both GRP94 and CYP3A4, and showed a 5-year OS of 100%; The breakdown of 4 patients: 2 DLBCL(NOS) were R-IPI poor and 1 DLBCL(NOS) was R-IPI good. 1DHL was R-IPI good. (2) Group 2 (‘Good’ group), consisting of patients showing positive staining for GRP94 and negative staining for CYP3A4, or negativity for all of AKR1C3, MDR1, MRP1, and p53, with a 5-year OS of about 60%-80% and a median survival of 66-94 months; (3) Group 3 (‘Poor’ group), consisting of patients who showed positive staining for GRP94, along with positive staining for one of the 4 factors which are AKR1C3, MDR1, p53, and MRP1, with a 5-year OS of about 10%-20% and a median survival of 16-19.5 months; (4) Group 4 (‘Very poor’ group), consisting of patients who showed positive staining for CYP3A4, with a 1-year OS of 0% and medial survival of about 9 months. The breakdown was 3 patients: 1 with DLBCL (NOS) was R-IPI good and 1 with HGBCL (only MYC translocation) was R-IPI poor. One patient with follicular lymphoma trasformation was R-IPI poor.
Of the ER stress proteins other than GRP94, patients showing positive tumor expression of TGF beta1 (Figure 1C) and GRP78 (Figure 1D) may also be expected to have a good prognosis. As seen in the combinations (Table 2). The patients showing positive staining for MDR1 or AKR1C3 showed a significantly poor prognosis (p < 0.01, Figure 1N), and even the ‘Good’ group without R-IPI poor showed a poor prognosis. Also, of the patients with HGBCL, those showing positive staining for MDR1 and AKR1C3 showed an even worse prognosis (p < 0.01). Of the patients with double-expresser lymphoma (positive staining for both MYC and BCL2), those showing positive staining for MDR1 or AKR1C3 showed an even worse prognosis (p < 0.01). Five representative cases classified according to the immune-histochemical staining pattern and HPI
Figure 2 shows cases classified by the HPI (Urayasu classification) IHC patterns: A: Case 1: A 64-year old woman. Enlargement of retroperitoneal, mesenteric, and left cervical lymph nodes. Cervical biopsy revealed HGBCL (DHL), R-IPI- good. As shown in Figure 2A and Table 3, the tumor cells showed negative staining for GRP94, and the case was classified as HPI-Group 1 (‘Very Good’ group). After 4 cycles of R-CHOP therapy, the patient was in complete remission. Thereafter, she was found to have HGBCL (double-hit lymphoma), and CR has been maintained for about 2 years after 3 additional cycles of dose-adjusted etoposide, doxorubicin, and cyclophosphamide with vincristine, prednisone and rituximab (DA-EPOCH-R). B: Case 2: A 41-year old woman. A biopsy of multiple peritoneal tumors revealed DLBCL (NOS), R-IPI- poor. As shown in Figure 2 and Table 3, the tumor cells were positive for GRP94, but were negative for the 4 factors (AKR1C3, MDR1, p53, and MRP1), and the patient was classified as HPI-Group 2 (‘Good’ group). After 6 cycles of R-CHOP therapy, she achieved the first CR. However, about one and a half years later, biopsy of an enlarged lymph node in the leg revealed the first relapse. As shown in Figure 2C and Table 3, the tumor cells were positive for GRP94 and negative for the 4 factors, and the case was classified as HPI-Group 2 (‘Good’ group). After R-ESHAP, autologous stem cell transplantation was performed, and the patient achieved a second CR. About 5 months later, cerebellar infiltration was detected and biopsy was performed, which revealed the second relapse. As shown in Figure 2D and Table 3, the tumor cells invading the cerebellum showed positive staining for GRP94 and 3 of the 4 factors, and the patient was classified as HPI-Group 3 (poor). After 4 courses of high-dose methotrexate (MTX) + cytarabine (Ara-C) therapy, the patient achieved a third CR. About 9 months later, she developed a relapse in the central nervous system (CNS) and died. C:Case 3: A 66-year old woman. She was diagnosed as having primary gastric DLBCL (not otherwise specified [NOS]), R-IPI- poor. As shown in Figure 2E and Table 3, she showed positive staining for GRP94 and 3 of the 4 factors, and the patient was classified as HPI-Group 3 (poor). After 8 cycles of R-CHOP therapy and 2 cycles of R-ESHAP therapy, the disease was found to be refractory. Autologous transplantation was performed after pretreatment with ranimustine, etoposide, cytarabine, and melphalan (MEAM). However, she developed relapse after radiotherapy, and died. D: Case 4: A 60-year old man. He had multiple enlarged lymph nodes around the abdominal aorta, mesentery, and bilateral iliac arteries, along with masses in the right lung, bilateral adrenal glands, and S7 of the liver. A lung biopsy revealed the diagnosis of HGBCL (only MYC translocation), R-IPI-poor. As shown in Figure 2F and Table 3, he showed positive staining for both GRP94 and CYP3A4, and was classified as HPI- Group 4 (‘very poor’ group). He underwent 6 cycles of R-CHOP therapy, 2 cycles of R-ESHAP therapy, IVAM (ifosfamide, etoposide, cytarabine, and methotrexate), and DeVIC (dexamethasone, etoposide, ifosfamide, and carboplatin). However, the disease was proved refractory, and the patient died 1 year later. D. Case 5: A 40-year old man. He was hospitalized for treatment of extramural obstruction of the common bile duct caused by mediastinal and hilar to para-aortic lymph node enlargement. Biopsy revealed the diagnosis of human immunodeficiency virus (HIV)-related BL (only MYC traslocation), R-IPI-poor. As shown in Figure 2G and Table 3, he showed positive staining for GRP94 and 2 of the 4 factors, and was classified as HPI-Group 3 (‘poor’ group). He did not respond to 2 cycles of CHOP, 2 cycles of DA-EPOCH-R, R-HDAC/MA (rituximab, high-dose cytarabine, with methotrexate and cytarabine), and ICE (ifosfamide, carboplatin, and etoposide). He died early, about 5 months after the start of treatment due to CNS invasion and leukemic transformation. Table 3 summarizes the outcomes of the 5 cases.
Discussion
In general, under an optical microscope, LBCL cells can be seen infiltrating diffusely into adjacent tissues. It is relatively easy to identify LBCL with anti-CD20 antibodies. Immunohistochemistry is considered as being very useful, because it allows assessment of positive and negative staining while confirming tumor cells. In this study, we conducted a retrospective IHC for 17 proteins4)-28) that have been reported in the literature as being potentially important. Our results revealed that of the 17 proteins, 6 (GRP94, CYP3A4, AKR1C3, MDR1, MRP1, and p53) were found clinically significant.
ER stress proteins (GRP94, GRP78 and TGFbeta1) enable LBCL tumor cells to survive in harsh microenvironments. In the absence of ER stress proteins, the survival of LBCL tumor cells in harsh microenvironments becomes difficult, and the patients may be expected to survive for prolonged periods of time. Among the patients with LBCL, particularly all those who showed negative staining for GRP94 all survived (Figure 1B). Thus, patients showing negative results of IHC for GRP94 were found to show an extremely good prognosis and GRP94 could be a selective target for the treatment of cancer5)6).
Factors involved in the metabolism of the anticancer drugs in CHOP promote the acquisition of resistance to anti-tumor drugs. The mechanisms include: 1) decrease in drug uptake; 2) promotion of drug efflux; 3) improved DNA damage repair; 4) resistance to aging of cells (apoptosis); 5) changes in drug metabolism; 6) alterations in drug targets; 7) epigenetic modifications; and 8) amplification of the target genes. These mechanisms, individually or in combination, lead to the development of resistance of cancer cells to single or multiple drugs22).
“1) Decrease in drug uptake” is unlikely to occur, because the intake of CHOP into cells is driven by a concentration gradient. However, equilibrative nucleoside transporter 1 (ENT1) is involved in the uptake of cytarabine and bendamastine30). For “2. Promotion of drug efflux,” particularly MDR1, MRP1 is important, (Figure 1N and O)21). Regarding “3. Improvement in DNA damage repair” and “4. Resistance to aging of cells (apoptosis),” In malignant tumors, p53 mutations, which result in its increased expression, cause loss of p53 function (Figure 1N and O)26). Regarding “5. Changes in drug metabolism,”AKR1B1C3 is an enzyme involved in the metabolism of doxorubicin and vincristine19). In addition, CYP3A417) is an enzyme involved in the metabolism of CHOP (Figure 1E, F, M, and N). For “6. Alterations in drug targets,” “7. Epigenetic modifications,” and “8. Amplification of target genes,” please refer to other reports2)3). However, NOTCH12), which is a marker for poor prognosis, regulates the expression of MRP131).
Of the ER stress proteins other than GRP94, patients showing positive results of IHC for TGF-beta1 (Figure 1C) and GRP78-(Figure 1D) may also be expected to show a good prognosis. GST is a useful defense against reactive oxygen species induced by H-enzyme (reactive oxygen species induced by hydroxyl doxorubicin). GST inactivates the H-enzyme in cooperation with the efflux pumps (MDR1 and MRP1) and AKR1C3, which inhibits the H enzyme21). Therefore, it is the expression of GST in patients showing positive results of IHC for MDR1 or MRP1 or AKR1C3 that is considered to confer the poor prognosis (p < 0.05). On the other hand, since GST also inactivates bendamustine, it can be a reference for the selection of Pola BR (polatuzumab vedotin combined with bendamustine and rituximab) therapy in patients with relapsed/refractory LBCL.
As seen from the combinations shown in Table 2, even the ‘Good’ group not classified as ‘poor’ according to the R-IPI could have a poor prognosis. Also, among HGBCL patients, those showing positive results of IHC for MDR1 or AKR1C3 showed a worse prognosis (p < 0.01). Of the patients with double-expresser lymphoma (positive results of IHC for both MYC and BCL2), those with positivity for MDR1 or AKR1C3 showed a worse prognosis (p < 0.01).
The results shown in Figure 2 are summarized in Table 3. HPI is more useful than R-IPI, because it takes into account tumor resistance mechanisms and offers greater potential for the development of treatments stratified by the risk for treatment resistance.
In the future, the HPI (Urayasu classification) is expected to serve as a useful reference in clinical practice, along with HGBCL (Figure 1K), R-IPI, etc. Addition of IHC for 6 proteins at the time of the initial examination would allow classification by the HPI and treatment stratified according to the pattern of tumor resistance treatment. For example, treatment selection can be made as follows: (1) For the ‘very good’ group, select R-CHOP; (2) For the ‘good’ group, select R-CHOP after administration of a GRP94 inhibitor or anti-GRP94 antibody4)-6); (3) For the ‘poor’ group, select R-CHOP after combination therapy using a GRP94 inhibitor, anti-GRP94 antibody4)-6), AKR1C3 inhibitor (epalrestat, a non-steroidal anti-inflammatory drug [NSAID], etc.), or MDR1 and MRP1 inhibitor (cyclosporine A32), etc.)12)-16); (4) For the ‘very poor’ group, select R-CHOP after administration of a CYP3A4 inhibitor17)18) or CYP3A4 inhibitor conjugated anti-CD 20 antibody using a GRP94 inhibitor, anti-GRP94 antibody4)-6),. When the therapy includes cytarabine, bendamustine, or gemcitabine, use of equilibrative nucleoside transporter 1 (ENT1), which regulates drug uptake, although not investigated in the present study, should be considered. If bendamustine is included in the therapy, the use of glutathione-S-transferase (GST)27), a rate-limiting metabolic enzyme, may also be considered. In addition, it has been reported that NOTCH1, a marker of poor prognosis, regulates the expression of MRP131). In the future, it is expected that the recent findings2)3) on LBCL genes will be integrated with the concept of HPI.
It is, of course, acceptable to select Pola-R-CHP (polatuzumab with rituximab, cyclophosphamide, doxorubicin, and prednisone) therapy, instead of R-CHOP, for patients with new-onset advanced LBCL. Pola-R-CHP, is considered as being essentially similar to R-CHOP in terms of metabolism, because Pola-R-CHP contains polatuzumab conjugated with monomethyl auristatin E (MMAE), instead of vincristine. In the case of HGBCL, intensive treatment regimens [DA-EPOCH, Hyper CVAD (hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone), etc.) with pretreatment can be selected instead of R-CHOP or Pola-R-CHP.
In summary, in patients diagnosed as having LBCL, IHC of the expressions of at least 6 proteins (GRP94, CYP3A4, AKR1C3, p53, MDR1, and MRP1) should be performed at diagnosis, for evaluation of the prognosis using the new HPI (Urayasu classification). If possible, testing should also be conducted for 5 additional molecules (TGF-beta1, GRP78, GST, MYC, and BCL2) should be performed. Thus, testing for a total of 11 molecules, in addition to the conventional measurements, including for the identification of HGBCL (MYC and BCL2 translocations by FISH), R-IPI, and HIV antibody assay, would be desirable. Further studies are needed for patients with new-onset or relapsed LBCL using inhibitors and antibodies after evaluation of the HPI, including development of strategies to improve the outcomes of treatment. In the future, it is necessary to accumulate more cases and analyze them.
Patents
This section is not mandatory but may be added if there are patents resulting from the work reported in this manuscript.
Author Contributions
Specific contributions of the authors in the paper were as follows: The planning authors: HT, MN, YA; The conduct authors: HT, YA, MF; The reporting authors: HT, MN; The conception authors: HT, MN; The design authors: HT, MN; The acquisition of data authors: YA, MF, ST, SK, HA, MO, TS; The analysis and interpretation of data authors: HT, MN, MA, TN, HN, HIH.
Acknowledgments
We greatly appreciate the assistance we received from Kotobiken Medical Laboratories Inc. (Tokyo, Japan) for the immunohistochemical analysis. We are also grateful to Dr. Konishi (Funabashi Natsumi Forest Clinic in Chiba, Japan) for his support.
Conflicts of Interest
A Conflict of Interest statement is not included for each of the authors. All authors have no conflicts of interest.
Ethics statement
Approval of the research protocol by an Institutional Reviewer Board in Juntendo University Ethics Committee. https://www.juntendo.ac.jp/hospital/clinic_c/gcp/file/rinsho/iinkai/proceedings/2022-08.pdf.
Patient and Public Involvement
None of the patients was involved in the design of this study. The results will be made known to the study participants on the homepage of our website.
References
- Bertrand Coiffier, Cle´mentine Sarkozy. Diffuse large B-cell lymphoma: R-CHOP failure—what to do? Hematology Am Soc Hematol Educ Program. 2016, Dec 2 (1):366-378. [CrossRef]
- R. Schmitz, G.W. Wright, D.W. Huang, C.A. et al. Genetics and Pathogenesis of Diffuse Large B-Cell Lymphoma. N Engl J Med. 2018, April 12;378(15): 1396-1407.
- Bjoern Chapuy, Jaegil Kim, Atanas Kamburov et al. Molecular subtypes of diffuse large B cell lymphoma are associated with distinct pathogenic mechanisms and outcomes. Nat Med. 2018, May 24(5): 679–690. [CrossRef]
- Jerina Boelens, Jean, Philippe Jais, Barbara Vanhoecke et al. ER stress in diffuse large B cell lymphoma: GRP94 is a possible biomarker in germinal center versus activated B-cell type. Leukemia Research 2013,37:3-8. [CrossRef]
- JiWoong Kim, Yea Bin Cho, Sukmook Lee. Cell Surface GRP94 as a Novel Emerging Therapeutic Target for Monoclonal Antibody Cancer Therapy. Cells, 2021 Mar17, 10(3), 670. https://doi.org/10.3390/cells10030670. [CrossRef]
- Xiaofeng Duan, Stephen Iwanowycz, Soo Ngoi, Megan Hill, Qiang Zhao, Bei Liu. Molecular Chaperone GRP94/GP96 in Cancers. Oncogenesis and Therapeutic Target. Front. Oncol., 09 2021, 09 April. Volume 11, Article 629846.. https://doi.org/10.3389/fonc.2021.62984. [CrossRef]
- Ana Mozos , Gaël Roué, Armando López-Guillermo et sl. The expression of the endoplasmic reticulum stress sensor BiP/GRP78 predicts response to chemotherapy and determines the efficacy of proteasome inhibitors in diffuse large b-cell Lymphoma. Am J Pathol, 2011. 179(5): 2601–2610, https://doi.org/10.1016/j.ajpath.2011.07.031. Epub 2011 Sep 9. [CrossRef]
- 8. Hua-chuan Zheng, Hiroyuki Takahashi, Xiao-han Li et al. . Overexpression of GRP78 and GRP94 are markers for aggressive behavior and poor prognosis in gastric carcinomas. Human Pathology 2008,39,1042–1049. [CrossRef]
- Ashraf M. El-Hefnia, Nashwa M. et al. Prognostic Utility of Transforming Growth Factor Beta-1 in Diffuse Large Cell Non-Hodgkin Lymphoma. J Hematol. 4(1):131-136. 2015. [CrossRef]
- Sulsal Haque and John C. Morris. Transforming growth factor-b: A therapeutic target for cancer. HUMAN VACCINES & IMMUNOTHERAPEUTICS, VOL. 13, NO. 8, 1741–1750, 2017. [CrossRef]
- Shoko Nakayama, Taiji Yokote, Motomu Tsuji, et al. TNF-a Receptor 1 Expression Predicts Poor Prognosis of Diffuse Large B-cell Lymphoma, Not Otherwise Specified. Am J Surg Pathol, 2014, Aug;38(8):1138-46. [CrossRef]
- Heather L, Gustafson. Song Yao et al.. Genetic polymorphisms in oxidative stress related genes are associated with outcomes following treatment for aggressive B cell non-Hodgkin lymphoma. Am J Hematol.2014 89(6): 639–645. [CrossRef]
- Yang Liu, Siyu He, Ying Chen et al. Overview of AKR1C3: Inhibitor Achievements and Disease Insights. J. Med. Chem., 2020. 63, 11305−11329. [CrossRef]
- Trevor M. Penning, Sravan Jonnalagadda, Paul C. Trippier, Tea Lanišnik Rižner... Aldo-Keto Reductases and Cancer Drug Resistance. Pharmacol Rev 2021 Jul y 73(3)1150–1171. [CrossRef]
- Wei Xiong, Jing Zhao, Hongliang Yu. Elevated Expression of AKR1C3 Increases Resistance of Cancer Cells to Ionizing Radiation via Modulation of Oxidative Stress. November 24, 2014. https://doi.org/10.1371/journal.pone.0111911. [CrossRef]
- Donya Moradi Manesh, Jad El-Hoss, Kathryn Evans, Jennifer Richmond et al. AKR1C3 is a biomarker of sensitivity to PR-104 in preclinical models of T-cell acute lymphoblastic leukemia. Blood.;126(10):1193-1202, 2015. [CrossRef]
- Cristina Rodríguez-Antona, Susanna Leskelä, Magdalena Zajac et al. Expression of CYP3A4 as a predictor of response to chemotherapy in peripheral T-cell lymphomas. Blood. 2007,110:3345-3351. [CrossRef]
- 18. Laura Molenaar-Kuijsten, Dorieke E M Van Balen , Jos H Beijnen, Neeltje Steeghs, Alwin D R Huitema. A Review of CYP3A Drug-Drug Interaction Studies: Practical Guidelines for Patients Using Targeted Oral Anticancer Drugs. Front Pharmacol . 2021 Aug 30;12:670862. https://doi.org/10.3389/fphar.2021.670862. [CrossRef]
- Ibrahim El-Serafi, Parvaneh Afsharian, Ali Moshfegh, Moustapha Hassan, Ylva Terelius. Cytochrome P450 Oxidoreductase Influences CYP2B6 Activity in Cyclophosphamide Bioactivation. PLOS ONE, November 6, 2015. https://doi.org/10.1371/journal.pone.0141979. [CrossRef]
- Robert W. Robey, Kristen M. Pluchino, Matthew D. Hall et al. Revisiting the role of ABC transporters in multidrug- resistant cancer. Nature Reviews Cancer 2018, 18: 452–464. [CrossRef]
- Charalambos Andreadis, Phyllis A. Gimotty, Peter Wahl et al. Members of the glutathione and ABC-transporter families are associated with clinical outcome in patients with diffuse large B-cell lymphoma. Blood. 2007,109:3409-341. [CrossRef]
- Ilaria Genovesea, Andrea Ilarib, Yehuda G. Assarafaf, Francesco Fazi, Gianni Colotti. Not only P-glycoprotein: Amplification of the ABCB1-containing chromosome region 7q21 confers multidrug resistance upon cancer cells by coordinated overexpression of an assortment of resistance-related proteins. Drug Resistance Updates Volume 32, May 2017, Pages 23-46. [CrossRef]
- Éva Bakos, László Homolya. Portrait of multifaceted transporter, the multidrug resistance-associated protein 1 (MRP1/ABCC1). Eur J Physiol 2017, 453:621–641. https://doi.org/10.1007/s00424-006-0160-8, 2007. [CrossRef]
- Jamie F. Lu, Deep Pokharel, Mary Bebawy. MRP1 and its role in anticancer drug resistance. Drug Metabolism Reviews, 2015, 47:4, 406-419. [CrossRef]
- Tony Huynh, Murray D. Norris, Michelle Haber, Michelle J. Henderson. ABCC4/MRP4: a MYCN regulated transporter and potential therapeutic target in neuroblastoma. Front Oncol. 2012, Dec 19;2:178. https://doi.org/10.3389/fonc. 2012.00178. [CrossRef]
- Tarek N El-Bolkainy, Mohamed N El-Bolkainy, Hussein M Khaled et al. Evaluation of MIB-1 and p53 Overexpression as Risk Factors in Large Cell Non-Hodgkin Lymphoma in Adults. Journal of the Egyptian Nat. Cancer Inst., Vol. 19, No. 4, 2007, December: 231-238.
- Danyelle M Townsend, Kenneth D Tew. The role of glutathione-S-transferase in anti-cancer drug resistance. Oncogene 2003, 22, 7369–7375. [CrossRef]
- Xingcao Nie, Peter M Clifford, Rekha Bhat, Rebecca Heintzelman, Mini Abraham, J Steve Hou. Thymidine phosphorylase expression in B-cell lymphomas and its significance: a new prognostic marker? Anal Quant Cytopathol Histpathol. 2013 Dec;35(6):301-5. 2013.
- Y Kanda TECHNICAL REPORT Investigation of the freely available easy-to-use software‘EZR’ for medical statistics. Bone Marrow Transplantation 48, 452–458. 2013. [CrossRef]
- Nobuya Hiraoka, Jiro Kikuchi, Takahiro Yamauchi et al.. Purine Analog-Like Properties of Bendamustine Underlie. Rapid Activation of DNA Damage Response and Synergistic Effects with Pyrimidine Analogues in Lymphoid Malignancies. PLoS One.; 2014, 9(3): e90675. [CrossRef]
- Sungpil Cho, Meiling Lu, Xiaolong He et al. .Notch1 regulates the expression of the multidrug resistance gene ABCC1/MRP1 in cultured cancer cells. PNAS vol. 108 no. 51:20778–20783, 2011. [CrossRef]
- Hisham Qosa,, David S. Miller, Piera Pasinelli, Davide Trotti. Regulation of ABC Efflux Transporters at Blood-Brain Barrier in Health and Neurological Disorders. Brain Res. 2015, Dec. 2, 1628(Pt B): 298–316. https://doi.org/10.1016/j.brainres.2015.07.005. [CrossRef]
Figure 1.
Overall survival of patients with and without the prognostic factors. Kaplan-Meier survival curves and between-group comparisons (log-rank test). (A) Overall survival (n=42); (B) GRP94 negative n=4, positive n=38, p<0.05; (C) TGF1 negative n=8, positive n=34, p<0.05; (D) GRP78 negative n=2, positive n=40, p>0.05; (E) AKR1C3 negative n=16 positive n=26, p<0.05; (F); CYP3A4 negative n=39 positive n=3, p<0.05. G. MDR1 negative n=25, positive n=17, p>0.05; H. MRP1 negative n=31, positive n=11, p>0.05; I. P53 negative n=27, positive n=15, p>0.05; J. R-IPI poor negative n=28, positive n=14, p>0.05; K.HGBCL negative n=28, positive n=14, p>0.05; L. MYC+BCL2+ negative n=17, positive n=25, p>0.05. M. GRP94- CYP3A4- n=4 Group1 Very good(5-year OS 100%). GRP94+ CYP3A4- n=35; In the Group 4 (Very poor, n = 3) consisting of 3 patients with positivity for both GRP94 and CYP3A4. All the 3 patients died within a short period. p<0.01; N .AKR1C3 or MDR1 negative n=15 positive n=20 p<0.01; O..P53 or MRP1 negative n=18 positive n=17 p<0.05.
Figure 1.
Overall survival of patients with and without the prognostic factors. Kaplan-Meier survival curves and between-group comparisons (log-rank test). (A) Overall survival (n=42); (B) GRP94 negative n=4, positive n=38, p<0.05; (C) TGF1 negative n=8, positive n=34, p<0.05; (D) GRP78 negative n=2, positive n=40, p>0.05; (E) AKR1C3 negative n=16 positive n=26, p<0.05; (F); CYP3A4 negative n=39 positive n=3, p<0.05. G. MDR1 negative n=25, positive n=17, p>0.05; H. MRP1 negative n=31, positive n=11, p>0.05; I. P53 negative n=27, positive n=15, p>0.05; J. R-IPI poor negative n=28, positive n=14, p>0.05; K.HGBCL negative n=28, positive n=14, p>0.05; L. MYC+BCL2+ negative n=17, positive n=25, p>0.05. M. GRP94- CYP3A4- n=4 Group1 Very good(5-year OS 100%). GRP94+ CYP3A4- n=35; In the Group 4 (Very poor, n = 3) consisting of 3 patients with positivity for both GRP94 and CYP3A4. All the 3 patients died within a short period. p<0.01; N .AKR1C3 or MDR1 negative n=15 positive n=20 p<0.01; O..P53 or MRP1 negative n=18 positive n=17 p<0.05.
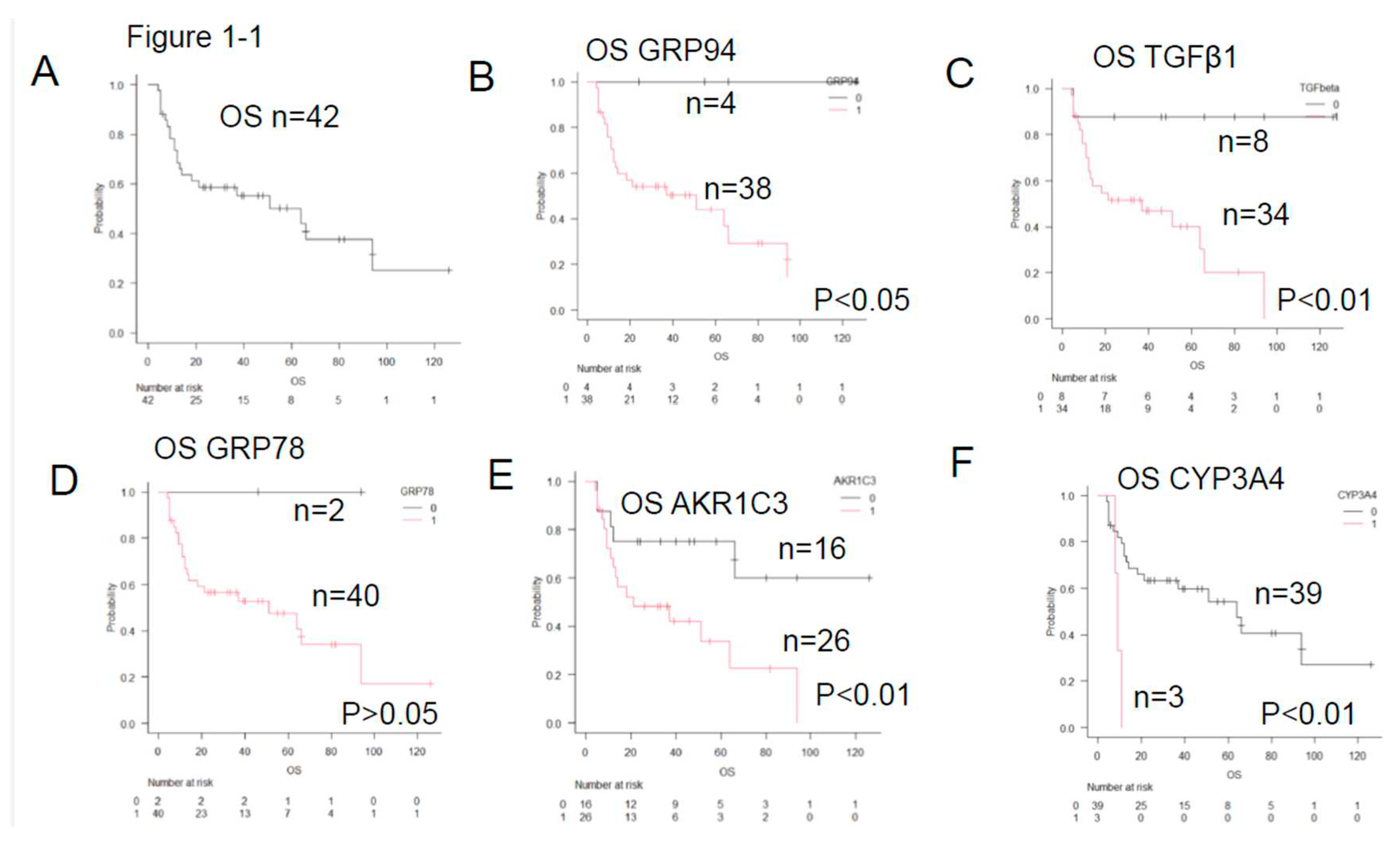
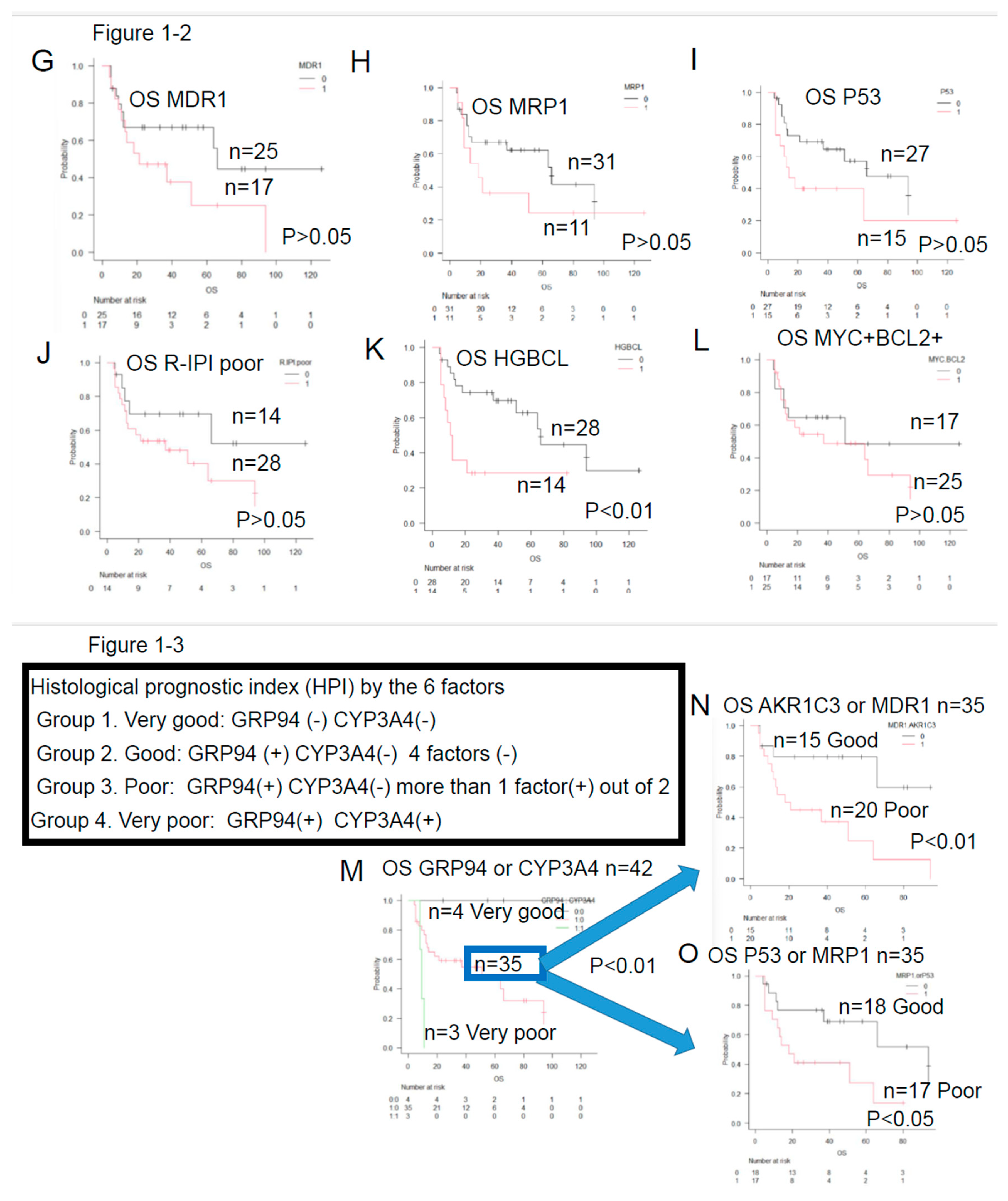
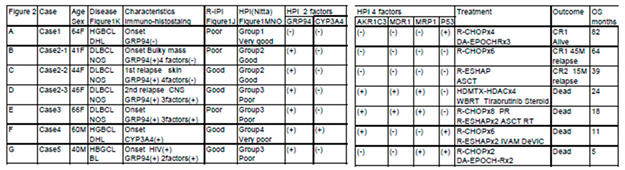
Figure 2.
Five representative cases of immune-histochemical staining methods and HPI; Red indicates positivity, and black indicates negativity. CR1 indicates first complete remission. HE indicates hematoxylin-eosin staining. A. HPI Group1: Very good group. Case1 .64yo female HGBCL(DHL) in the lymph node. R-IPI poor 2 years CR1 GRP94(-) CYP3A4(-)AKR1C3(-)MDR1(-) MRP1(-)P53(+). B. HPI Group2: Good Case2 41yo female DLBCL in the LN CR1 before relapse GRP94(+) CYP3A4(-)AKR1C3(-)MDR1(-). C. HPI Group 2: Good Case2 41yo female DLBCL 1st relapse in the skin GRP94(+) CYP3A4(-)AKR1C3(-)MDR1(-). D. HPI Group3: Poor Case2 41yo female DLBCL 2nd relapse in the brain GRP94(+) CYP3A4(-)AKR1C3(+)MDR1(+). E. HPI Group 3 Poor : Case3 66yo female the gastric DLBCL PD. GRP94(+) CYP3A4(-)AKR1C3(+)MDR1(+). F. HPI Group 4. Very poor . Case4 60yo male DHL refractory GRP94(+) CYP3A4(+)AKR1C3(+)MDR1(-). G. HPI Group3 Poor Case5 40yo male HIV+BL GRP94(+) CYP3A4(-). AKR1C3(- )MRP1(+) P53(+).
Figure 2.
Five representative cases of immune-histochemical staining methods and HPI; Red indicates positivity, and black indicates negativity. CR1 indicates first complete remission. HE indicates hematoxylin-eosin staining. A. HPI Group1: Very good group. Case1 .64yo female HGBCL(DHL) in the lymph node. R-IPI poor 2 years CR1 GRP94(-) CYP3A4(-)AKR1C3(-)MDR1(-) MRP1(-)P53(+). B. HPI Group2: Good Case2 41yo female DLBCL in the LN CR1 before relapse GRP94(+) CYP3A4(-)AKR1C3(-)MDR1(-). C. HPI Group 2: Good Case2 41yo female DLBCL 1st relapse in the skin GRP94(+) CYP3A4(-)AKR1C3(-)MDR1(-). D. HPI Group3: Poor Case2 41yo female DLBCL 2nd relapse in the brain GRP94(+) CYP3A4(-)AKR1C3(+)MDR1(+). E. HPI Group 3 Poor : Case3 66yo female the gastric DLBCL PD. GRP94(+) CYP3A4(-)AKR1C3(+)MDR1(+). F. HPI Group 4. Very poor . Case4 60yo male DHL refractory GRP94(+) CYP3A4(+)AKR1C3(+)MDR1(-). G. HPI Group3 Poor Case5 40yo male HIV+BL GRP94(+) CYP3A4(-). AKR1C3(- )MRP1(+) P53(+).
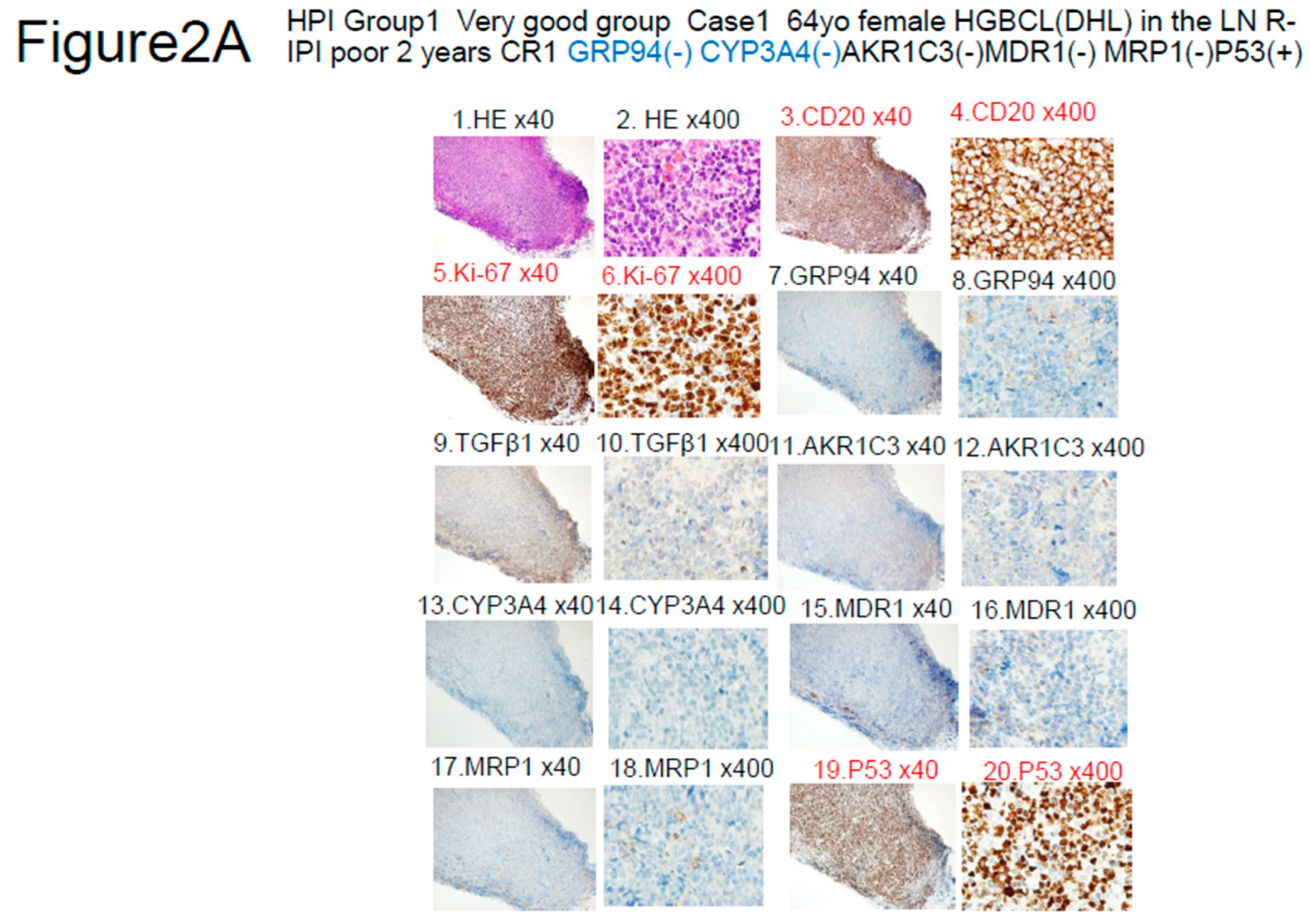
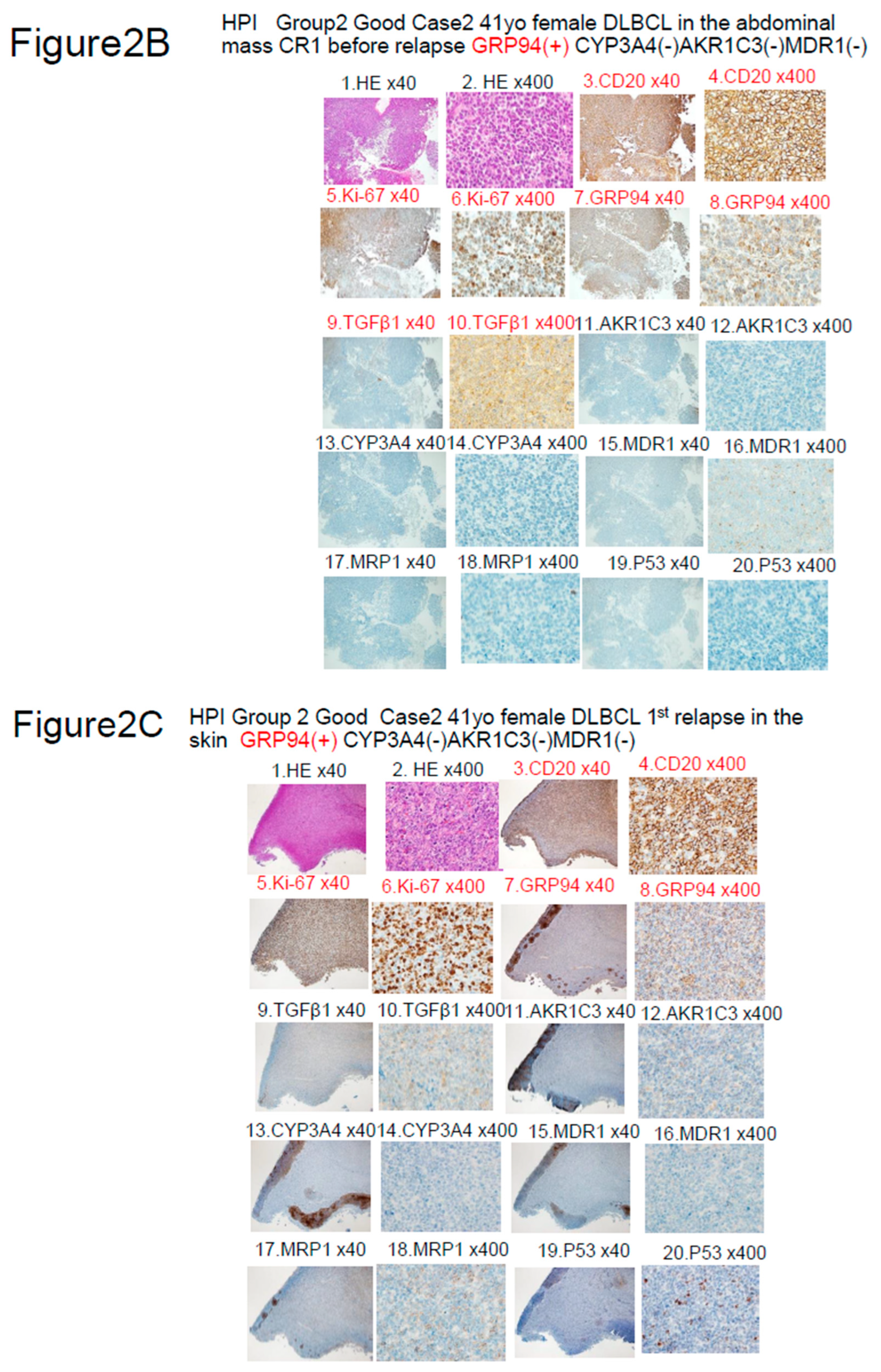
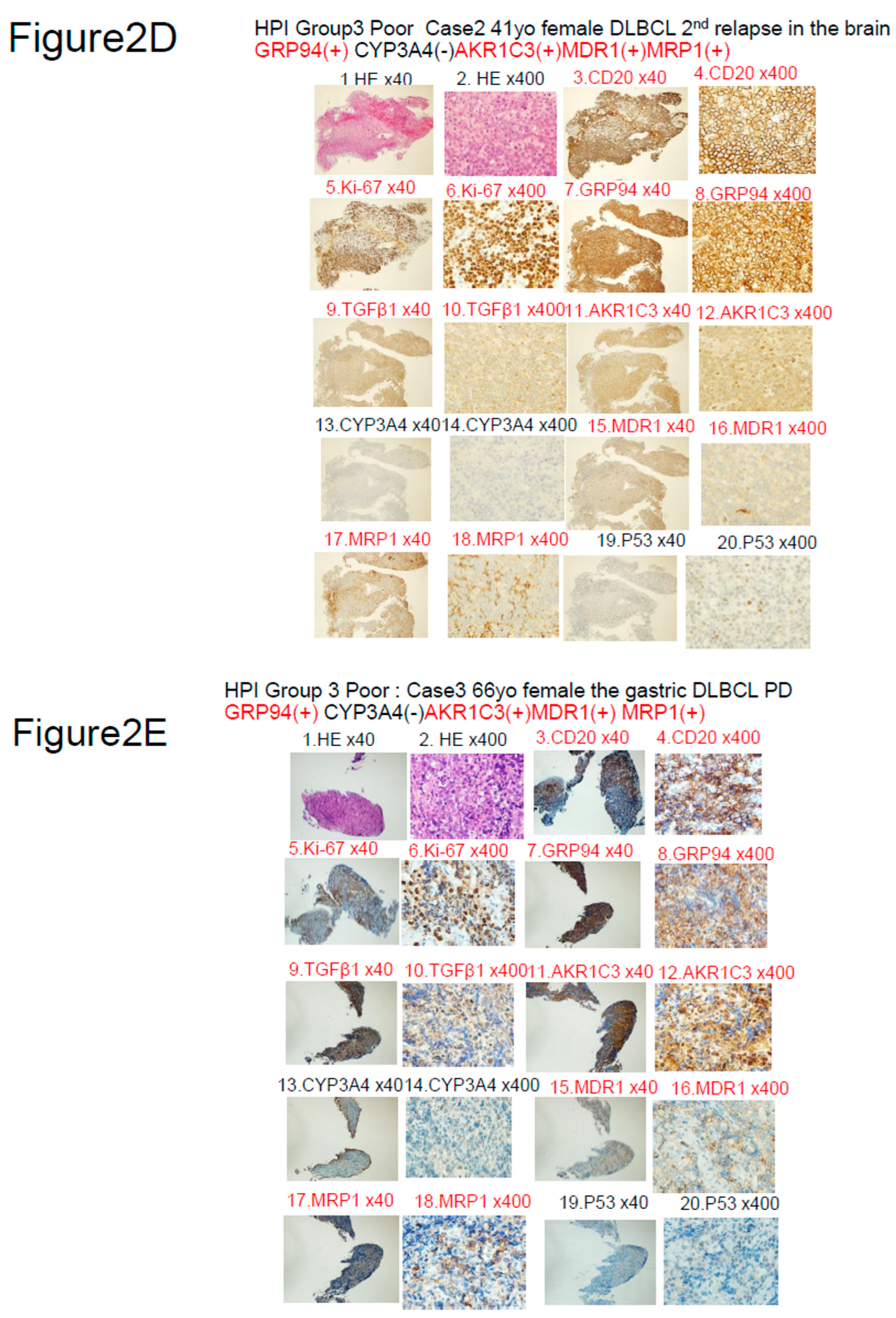
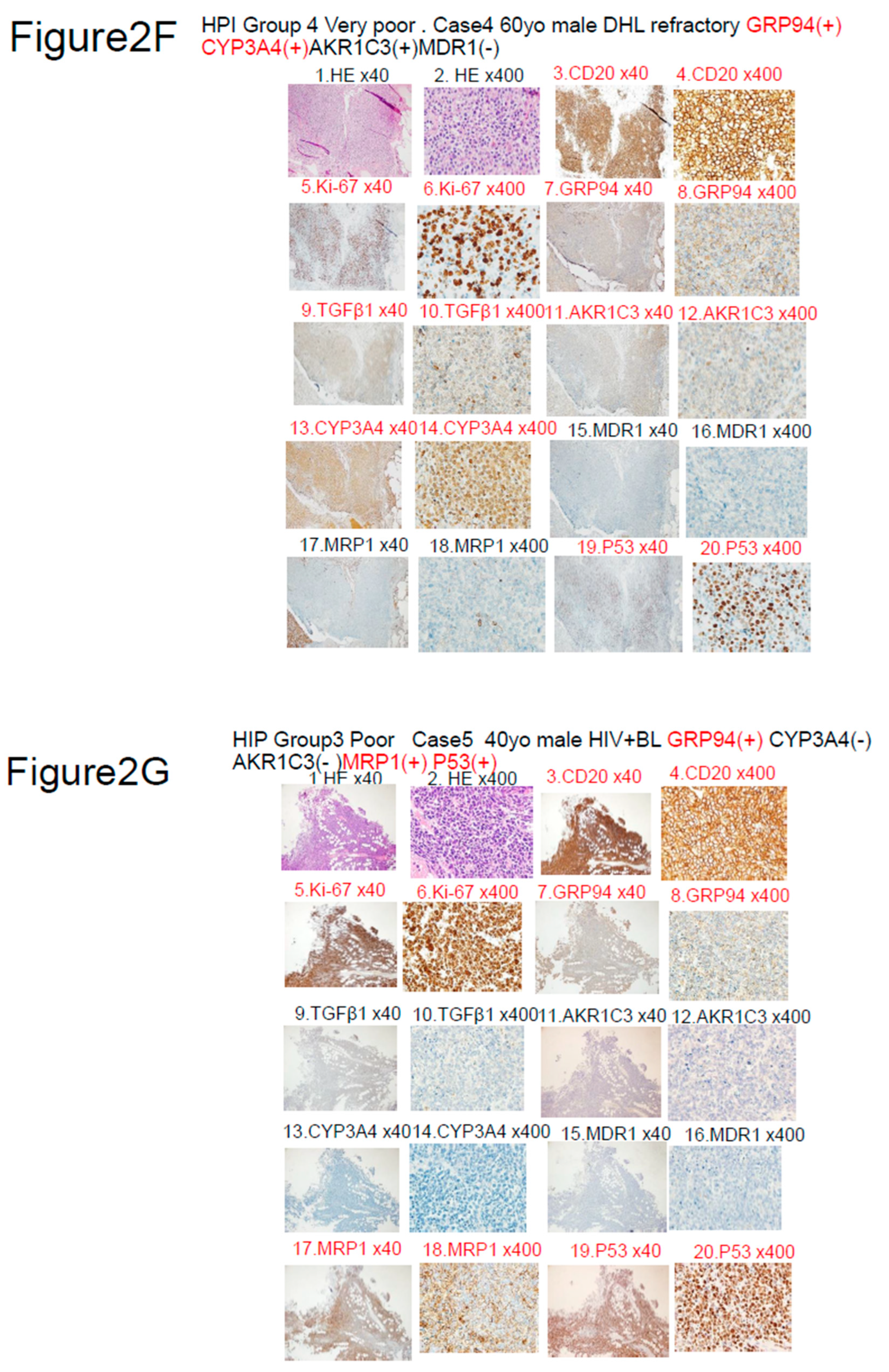

Table 1.
Characteristics of LBCL patients in this analysis (n=42).
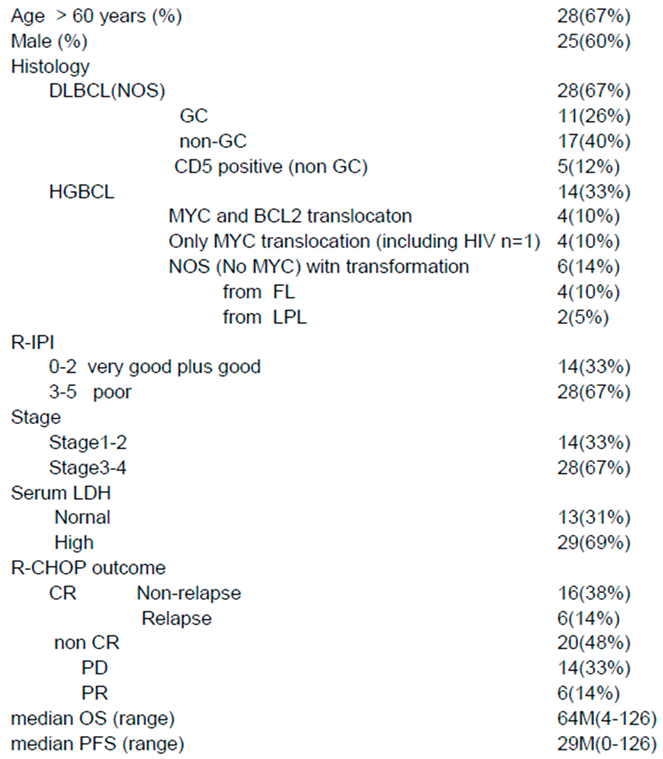 |
Notes: Abbreviations: DLBCL, diffuse large B-cell lymphoma; NOS, not otherwise specified; HGBCL, High grade B-cell lymphoma; R-IPI, Revised International Prognostic Index; CR, complete remission; PD, progressive disease; PR, partial remission; OS, overall survival; PFS, progression free survival.
Table 2.
Summary of the Immuno-histochemical findings in LBCL (n=42). Notes: Among the many proteins found in the literature, we selected 17 proteins that we considered as being potentially important, along with 3 prognostic indexes. Using antibodies against these proteins, a comprehensive retrospective analysis of LBCL was performed by immunohistochemistry. The analysis was performed for: (1) 4 endoplasmic reticulum stress (ER) proteins; (2) 3 metabolic enzymes of anticancer drugs; (3) 3 types of anticancer drug efflux pumps; (4) others (3 prognostic indexes and 7 other proteins). Abbreviations: OH, oncovin + hydroxyl doxorubicin. MTX, methotrexate sodium. DHL, double hit lymphoma.
Table 2.
Summary of the Immuno-histochemical findings in LBCL (n=42). Notes: Among the many proteins found in the literature, we selected 17 proteins that we considered as being potentially important, along with 3 prognostic indexes. Using antibodies against these proteins, a comprehensive retrospective analysis of LBCL was performed by immunohistochemistry. The analysis was performed for: (1) 4 endoplasmic reticulum stress (ER) proteins; (2) 3 metabolic enzymes of anticancer drugs; (3) 3 types of anticancer drug efflux pumps; (4) others (3 prognostic indexes and 7 other proteins). Abbreviations: OH, oncovin + hydroxyl doxorubicin. MTX, methotrexate sodium. DHL, double hit lymphoma.
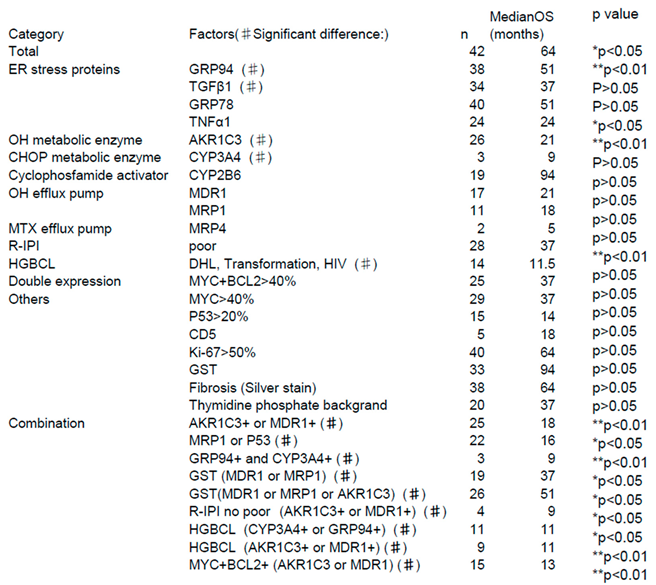 |
Table 3.
Summary of the outcomes of the five cases in Figure 2. Notes: Abbreviations: F: female, M: male, HPI: histological prognostic index, R-IPI: revised international prognostic index. GRP94: glucose-regulated protein 94, CYP3A4: cytochrome p450 3A4, AKR1C3: aldo-keto reductase family 1 member C3, MDR1: multidrug resistance protein 1, MRP1: multidrug resistance-associated protein 1, OS: overall survival, HGBCL: high-grade B-cell lymphoma, DHL: double-hit lymphoma, DA: dose adjust, CR1: the first complete remission, CR2: the second complete, ASCT: autologous stem cell transplantation, CNS: central nervous system, HDAC: High dose arabinoside , HDMTX: High dose methotrexate, WBRT: Whole brain radiotherapy, PR: partial remission, RT: radiotherapy.
Table 3.
Summary of the outcomes of the five cases in Figure 2. Notes: Abbreviations: F: female, M: male, HPI: histological prognostic index, R-IPI: revised international prognostic index. GRP94: glucose-regulated protein 94, CYP3A4: cytochrome p450 3A4, AKR1C3: aldo-keto reductase family 1 member C3, MDR1: multidrug resistance protein 1, MRP1: multidrug resistance-associated protein 1, OS: overall survival, HGBCL: high-grade B-cell lymphoma, DHL: double-hit lymphoma, DA: dose adjust, CR1: the first complete remission, CR2: the second complete, ASCT: autologous stem cell transplantation, CNS: central nervous system, HDAC: High dose arabinoside , HDMTX: High dose methotrexate, WBRT: Whole brain radiotherapy, PR: partial remission, RT: radiotherapy.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



