
Submitted:
17 August 2023
Posted:
21 August 2023
You are already at the latest version
Abstract
Pain is a complex multidimensional feeling combined with sensorial and emotional features. The majority of patients undergoing orthodontic treatment reported various degrees of pain, which is perceived as widely variable between individuals, even when the stimulus is the same. Orthodontic pain is considered the main cause of poor-quality outcomes, patients' dissatisfaction, and lack of collaboration up to the interruption of the therapy. A deep understanding of pain and how it influences the patient’s daily life is fundamental to establishing proper therapeutic procedures and obtaining the correct collaboration. Because of its multifaced and subjective nature, pain is a difficult dimension to measure. The use of questionnaires and their relative rating scales is actually considered the gold standard for pain assessment. Depending on the patient’s age and cognitive abilities is possible to choose the most appropriate instrument for self-reported pain records. Although several scales have been proposed and a lot of them are applied, it remains uncertain which of these tools represents the standard and performs the most precise, universal, and predictable task. This review aims to give an overview of the aspects which describe pain, specifically the pain experienced during orthodontic treatment, the main tool to assess self-perceived pain in a better and more efficient way, the different indications for each of them, and their correlated advantages or disadvantages.
Keywords:
pain perception
; discomfort
; orthodontic appliances
; visual analogue scale (VAS)
1. Introduction
During orthodontic treatment, the feeling of discomfort and the experience of some degree of pain are commonly reported [1]. Orthodontic patients may go through feelings of tension, pressure, and soreness of teeth as far as the perception of pain [2].
Pain is the main concern of people undergoing orthodontic treatment. It has been reported that the fear of pain is one of the primary factors that negatively influence the patient’s willingness to treatment uptake and discourage it, together with the appearance of braces and the fear of being teased [3].
This may conditionate also their collaboration during all treatment time, the outcome, the patient satisfaction, and even their quality of life [4]. Patients' unsatisfaction may lead to longer treatment times and poor-quality therapy results [5]. A significant proportion of patients (8%) decide to interrupt the therapy because of the pain suffered in the initial stages of the treatment [6].
For these reasons, orthodontic pain, its management, and assessment are fundamental for patients and clinicians who had to handle the situation in the best possible way [5].
Applying an assessment tool is necessary to evaluate some specific features. Every tool must have characteristics of validity and sensitivity [7].
Validity is the ability of an assessment to measure what it was supposed to measure. In the case of a questionnaire, the validity permits to collect high-quality data with increasing credibility. To be sure that the questionnaire is valid and it provides the information for which it is developed, it must undergo a validation process [8]. A valid questionnaire must have the following aspects: 1) simplicity and viability, 2) reliability and precision, 3) adequate for the problem intended to measure, 4) reflect underlying theory or concept to be measured, 5) capable of measuring change [9].
Reliability indicates low sensitivity to random error. Reliability is linked to reproducibility: the test provides the same results even if repeated. The third fundamental feature of an assessment tool and questionnaire is sensitivity, especially if it is used for evaluative purposes. This could permit underline changes in the same patient, during the therapy [7].
2. Materials and Methods
2.1. Focused Questions
What are the most relevant aspects when assessing pain, especially chronic pain? What are the main tools used to evaluate it?
2.2. Eligibility Criteria
The following inclusion criteria guided the analysis of the studies: (I) study design—narrative reviews, systematic reviews, clinical trials, case-control studies, case-reports (II) participants—patients with painful conditions and/or psychological implications, (III) interventions—pain assessment (IV) outcome—pain intensity, pain assessment tools, psychological assessment tools. We considered including only studies with free full text available. Only studies that met all the inclusion criteria were included. It was also considered to exclude (I) abstracts of articles published in non-English languages, (II) duplicate studies, (III) in vitro or animal clinical studies, (IV), not pertinent studies, and (V) the absence of free full-texts available.
2.3. Search Strategy
The PICO model (Population, Intervention, Comparison, Outcome) was used to perform this review, through a literature search of the PubMed (MEDLINE) and Scopus electronic databases. Abstracts of studies that evaluated the assessment of pain and/or psychological implications were reviewed.
2.4. Research
The medical subject heading (MeSH) terms are pain, pain assessment, questionnaire, visual analogue scale, and orthodontic. An electronic search was carried out with the PubMed (MEDLINE) and Scopus databases. The articles published in the years 1962–2022 were targeted. The duration of data extraction was about 8 weeks. The last search was performed on 29 July 2023. All the titles and abstracts were read thoroughly from the articles searched primarily, and nonrelevant studies were excluded. The relevant articles were enlisted and scrutinized for any similar studies that matched our inclusion criteria. For the extraction of pertinent results, we read the full texts of the included studies, and the findings were recorded.
3. Results
The primary search identified 883 articles based on MeSH terms, published from 1983 to 2021. Following those, the research has been restricted to narrative reviews, systematic reviews, case reports, and meta-analyses concerning human studies and the English language, so 96 results were found. As a result, it was decided that only articles with full text or free full text should be used, so 38 articles were screened and evaluated for eligibility (Figure 1).
4. Discussion
4.1. Features of pain
In 2020 the IASP (International Association for the Study of Pain) updated the last definition of pain: “An unpleasant sensory and emotional experience associated with or resembling that associated with actual or potential tissue damage”. The association adds six features that better characterize pain: 1) Pain is a personal experience, influenced by biological, psychological, and social factors, 2) Pain and nociception are different concepts, with the first being much more complex than the second, 3) Individuals learn what pain means during their life, 4) When a patient says to be feeling pain, his statement must always be respected, 5) Despite his protective and adaptive functions, pain can have adverse effects on psychological and social functioning, 6) Verbal description is only one of the methods for depicting pain [10].
Based on this definition, pain is a multidimensional feeling that can be described as a union of two components: sensorial and emotional. The sensorial one is derived from anatomical features of the nervous system: stimuli are received and transported to the central nervous system (CNS) through a tri-neuronal network that originates from the periphery and reaches the cerebral cortex. The emotional component is related to the limbic system, a group of structures located in the deep telencephalon, which is liable for the subjective part of the painful stimulus [11].
4.2. Features of orthodontic pain
Tooth movement is only possible through a process of inflammation as an outcome of the forces applied during the course of orthodontic therapy [12].
The feeling of dental pain is a consequence of stretch and compression forces applied to the periodontal ligament and the alveolar bone. This causes a change in the blood flow of the periodontal apparatus up to induce the release of the tissue biochemical moderators and determine the inflammatory reaction which leads to the sensation of pain [8].
Orthodontic patients experience pain during the treatment in a range of 70%-95% and they reported the highest intensity of pain during the first 24 hours [13,14,15].
According to the literature, 39%-49% experience pain all over the time of treatment or after the removal of the appliance [16,17].
The intensity of pain depends on several factors both subjective and objective: gender, age, sex, the magnitude of force applied, state of emotion and stress, personal pain threshold, individual culture, and previous pain experience [1,14,18,19].
Furthermore, the type and intensity of suffering can change depending on the appliances used and the type of force applied [20].
Although the quantity and quality of pain may depend on the typology of appliances, it has been stated that 70% of orthodontic patients experienced some type of suffering or pain, regardless of the type of appliance [21].
In the case of fixed appliance-based treatment, within two hours from the insertion of the first arch-wire, the patients report a feeling of pain that increases progressively. After 24 hours, almost the totality of patients (95%) reported pain that reaches its peak and starts to decrease [16,22].
Burstone classified pain into three degrees: 1) pain is produced by heavy pressure on the tooth with an instrument in the same direction as the force of the fixed appliance, 2) pain evocates by clenching or heavy biting, 3) the patient suffers by a spontaneous pain or is unable to masticate food [12].
Bergus et al described two different types of pain experienced during the active orthodontic phase of the treatment: constant pain and chewing-related pain. 82% of orthodontic patients report pain during chewing/biting, while 24% declare constant pain on the first day after activation. The suffering is decreasing gradually from the second day till the seventh when the spontaneous pain reported is null. However, 30% still reported pain during chewing/biting [1].
A large number of unidimensional and multidimensional assessment tools have been suggested to measure the patient’s pain. One-dimensional tools focus on and consider only one characteristic aspect of pain (such as pain intensity) simplifying the pain experience. These instruments are rapid to administer and require less intellectual ability rather than the multidimensional ones [23].
4.3. Pain intensity assessment
The European Palliative Care Research Collaborative, agree the most clinically relevant dimension to pain assessment, regardless of disease or condition, is pain intensity (PI) [24].
The extent of pain intensity is conventionally assessed subjectively using different types of pain scales and unidimensional tools [25].
Over the years several subjective methods which include pain scales like NRS, VAS, and VRS were proposed to assess the experience of pain more accurately [26]. Currently, these scales are the best instruments for measuring individual pain, and pain assessment tools based on self-reported perception using questionnaires and their relative scales are the gold standard [24].
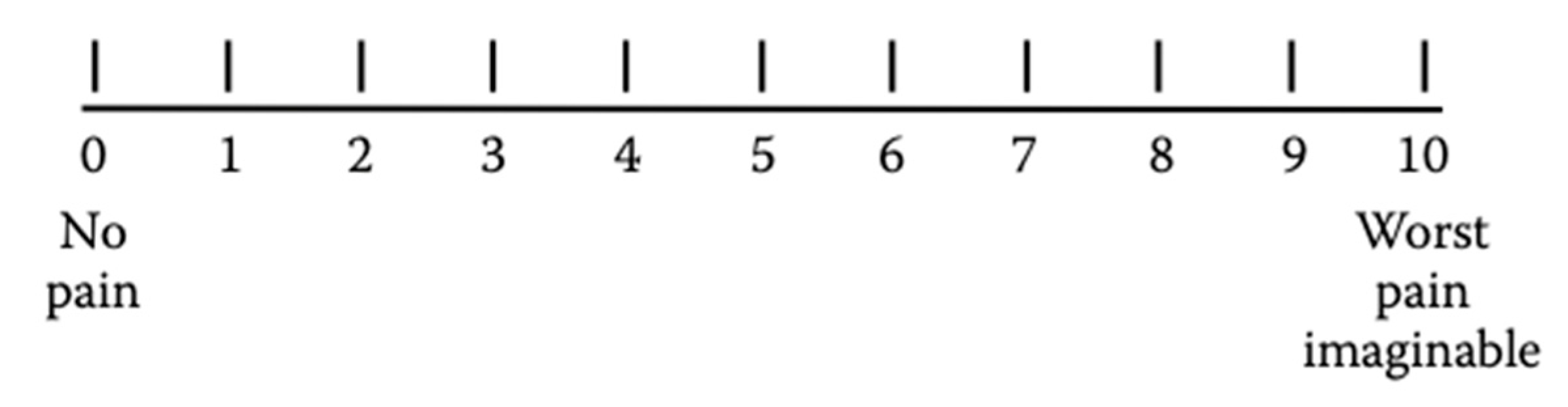
A preponderance of evidence demonstrates that the 100 mm Visual Analog Scale (VAS) is the by far the most frequently used assessment pain tool [24].
This scale is composed of a line of a fixed length with defined endpoints. One extremity of the line was labeled “no pain” and the other end as “worst pain imaginable” (Figure 2). Patients are required to indicate the place on the line corresponding to their self-perceived state [27].
Patients mark on the 10cm line the point which represents their self-perception to quantify and record the pain intensity in a range from 0 to 100 mm. The obtained value provides a quantitative variable of pain [25].
The VAS is a popular tool in a clinical setting because of its rapidity of administration and simplicity. It can be used by anyone cognitively capable to respond to clinician instructions [28] however someone can find the tool too difficult or too abstract to be understood, especially ones with a physical disability or cognitive dysfunction [23]. One of the main limitations of the VAS is that it must be administered on paper or electronically, it cannot be administered orally [29].
The VAS showed good reliability and sensitivity, being able to detect PI variation over time [30,31].
The VAS scale is frequently used to assess pain intensity during treatment in the orthodontic field.
A clinical trial performed on 64 patients was aimed to compare the pain intensity between subjects treated with passive self-ligating fixed appliances and those treated with Invisalign aligners. The subjective perception of pain is recorded using a questionnaire based on VAS [32].
The same results were obtained in a prospective longitudinal study which is performed to make a comparison between Invisalign and fixed appliances during the first week of therapy. It was shown that patients treated with fixed appliances reported a higher level of pain intensity, according to VAS, rather than those treated with Invisalign therapy [33].
Another study is carried out to make a comparison of patients treated by 3 different orthodontic appliances in terms of pain level: clear aligners, self-ligating and conventional. During the first week of therapy, the VAS scale demonstrates that the lowest level of pain is reported by the clear aligner group. Furthermore, the self-ligating group reported a significantly low level of pain rather than the conventional one [34].
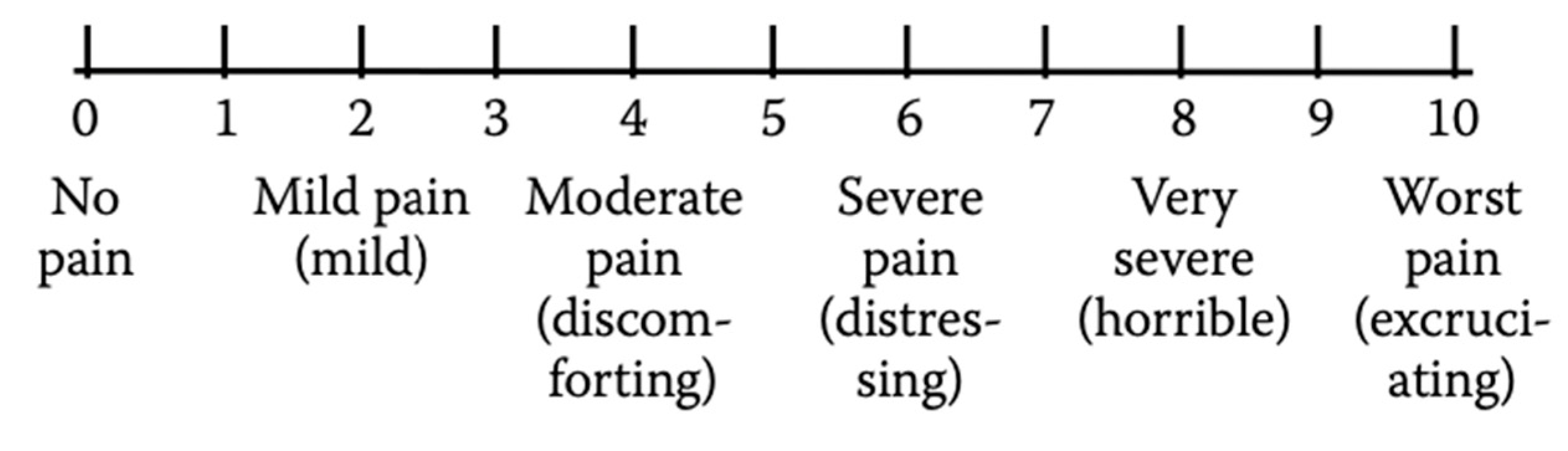
For the intensity pain assessment during adulthood or childhood, the Numerical Rating Scale (NRS) can be used. The NRS is a segmented numerical version of the VAS which consists of a numerical scale ranging from 0 to 100 where the extreme 0 corresponds to “no pain” and the other extreme represents “pain as bad as it could be” (Figure 3). Patients are required to mark the number corresponding to their perceived level of pain intensity [35].
The intensity of pain using the NRS is assessed as follows: no pain = 0, mild pain = 1–3, moderate pain = 4–6, and severe pain ≥7 [36].
Using NRS, a study performed on 165 patients who agreed to have miniscrew insertion during their orthodontic treatment to facilitate tooth movement, was aimed to evaluate their experience of pain during the post-operatory time [37].
Although the NRS and the VAS are the most widely used self-report pain scales they have the disadvantage correlated to a request of a notable level of abstract thinking to correlate pain experience with a number or a point on the line [38].
The VRS is more appropriate for patients with cognitive impairment thanks to its simplicity. It has been shown that VRS provides high response rather than NRS e VAS [39].
The VRS is made up of a list of adjectives corresponding to different levels of pain. The first adjective is related to lower pain intensity, while the others correspond to a gradually higher pain level. An example of adjectives that can be used is “none”, “mild”, “moderate”, and “severe” [40].
Among the various advantages of the VRS, it can be underlined its rapidity and simplicity to use. It is easy to teach the patients its correct compilation and it is easy to score and document the results. Furthermore, the tool is well-validated and can be used to detect treatment effects. The verbal rating scale can overcome some limits concerning the VAS: it can be administered verbally thereby permitting its use by those who have physical or visual difficulty [23].
In literature, among the orthodontic studies which take advantage of VRS, a prospective randomized trial is performed to compare pain experience during orthodontic treatment with self-ligating brackets and conventional ones [41].
4.4. Pain assessment in children
Pain assessment in children is a challenge linked to the complex nature of pain, language limitation and difficulty in comprehension and self-reporting, and the social feature of pain (different pain experiences depending on age, sex, and race) [42].
The level of cognitive development, language comprehension, and vocabulary may influence children’s capacity to provide a self-report of pain intensity and the ability their ability to use a pain scale accurately [43,44].
Children understand and express pain differently depending on their age stage. Thus, the pain assessment must be age dependent [45].
Pawar and Garten have described the difference in the expression of pain in various pediatric age groups:
Preschoolers: may verbalize the intensity of pain, see pain as punishment, exhibit thrashing of arms and legs, attempt to push a stimulus away before it is applied, be uncooperative, need physical restraint, request emotional support, understand that there can be secondary gains associated with pain, or be unable to sleep.
School-age children: may verbalize pain, use an objective measurement of pain, be influenced by cultural beliefs, experience nightmares related to pain, exhibit stalling behaviors, have muscular rigidity, e.g. clenched fists, white knuckles, gritted teeth, contracted limbs; exhibit body stiffness, closed eyes, wrinkled forehead, engage in the same behaviors listed for pre-schoolers/young children, or be unable to sleep.
Adolescents: may localize and verbalize pain, deny pain in the presence of peers, have changes in sleep patterns or appetite, be influenced by cultural beliefs, exhibit muscle tension and body control, display regressive behavior in the presence of the family, or be unable to sleep [23].
Nevertheless, children aged ≤7 are able to report the pain severity and from age 3 to 7 they increase progressively their capacity to describe, analyze and localize it [36].
In the pediatric field facial scales are a widespread tool for severity pain assessment. They consist of a sequence of facial expressions that correspond to a spectrum of increasing pain intensity. Although various face scales have been developed, the Wong-Baker Faces Pain Rating Scale (WBS) has been demonstrated as appropriate in various pediatric settings it is the most widely applied [36,46].
The Wong-Baker Faces Pain Scale is composed of six faces where the first one is a happy smiling face while the last one is sad and tearful. The faces in the middle represent varying and increasing degrees of pain. The patient is asked to choose the face most like his/her during pain [47].
This tool is simple and quick to administer, is easy to score, requires no reading or verbal skills, is unaffected by issues of gender or ethnicity, and provides three scales in one (i.e., facial expressions, numbers, and words). For these reasons, the most widely used scales for children’s pain intensity records are the Wong-Baker Faces Pain Rating Scale, various visual analog scales, and verbal numeric scales [43].
The leading disadvantage of this tool is the possibility of measuring mood instead of pain, and the interpretation of sad or crying faces is dependent on different cultures [23].
Nowadays one of the most widely instruments used in school-age patients and adolescents to obtain self-reports of pain intensity is the Verbal Numerical Rating Scale (NRS or VNRS). This scale is made up of a list of adjectives that correspond to an increase in pain intensity. The patient has to choose one of six descriptors (“No pain,” “Mild pain,” “Moderate pain,” “Severe pain,” “Very severe pain,” and “Worst pain possible”) that best represents the level of self-perceived pain intensity. The numbers may be used to ease the recording of the results. The VNRS has a marked validity and reliability in little patients aged ≥8 years [48,49].
Figure 4.
Verbal Numerical Rating Scale (VNRS).
Because of lower developmental skills, children aged ≤7 years lack the developmental skills, necessary for accurate use of this pain tool [50,51].
In a recent prospective study performed in 2020, a questionnaire composed of NRS and Wong-Backer faces pain scale was used to assess and compare the intensity of pain following the maxillary expansion with two different types of expanders (Hyrax and Haas type). The conclusions suggest that the pain was reported in both types of expansion and the highest pain is shown on the first day of activation in the Hyrax group [52].
Another recent study based on VAS and the Wong-Baker Faces Pain Rating Scale was carried out (Figure 4). The study records the self-pain perception experienced by patients after the mini-implant placement concluding that the maximum pain was recorded in the case of palatal miniscrew [53].
Figure 4.
Visual Analogue Scale and Faces Pain Rating Scale.
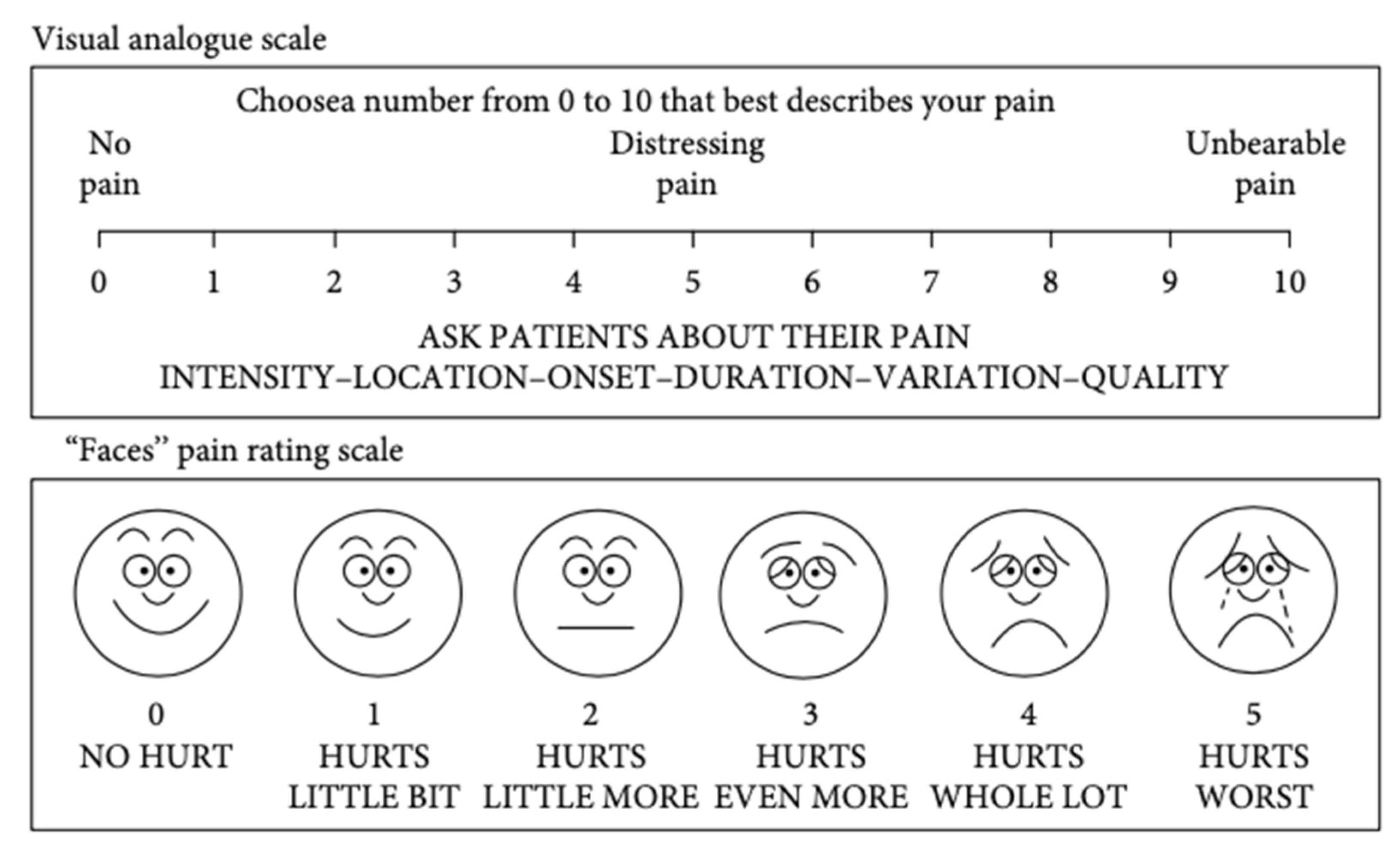
[Sreenivasagan et al., 2021]
Since pain is defined as a multidimensional emotion, a multidimensional tool permits a much more comprehensive and exhaustive pain assessment. In this way, not only PI but all the pain features including the psychological, emotional, and behavioral ones are examined [54].
The main disadvantage of the traditional methods of pain measurement (visual analogue scale, numerical rating scale, verbal rating scale) treat pain as if it were a single dimension experience that can be described using the only dimension of the intensity measured with a single unique scale. Although intensity is one of the main features of pain, the word "pain" refers to several qualities categorized under a single linguistic term, not to a specific, single feeling that varies only in intensity [55].
McGill Pain Questionnaire (MPQ) is a multidimensional tool developed by Melzack and Torgerson for a self-reporting measure of pain assessing both the quality and the quantity. This questionnaire permits the evaluation of sensorial aspects such as intensity, localization, temporality, quality, and affective aspects of pain. The original MPQ comprised 78 pain descriptors categorized into three major classes. The classes included terms that describe the sensory, affective, and evaluative quality of the pain experience [56].
The MPQ is also employed to assess pain intensity. The Pain Rating Index (PRI) is based on a 1-5 intensity scale and it is built thanks to a numerical grading of words describing sensory, affective and evaluative features of pain. The rank values of the word chosen by the patient are summed to obtain a separate score for the three major classes [57]. In addition to PRI, the Present pain intensity (PPI) score ranges from 1 (mild) to 5 (excruciating) is considered. It can be obtained by scoring the response to the question, "Which word describes your pain right now?" [58].
Over the years, the MPQ has become one of the most commonly widespread clinical and research tool. This instrument is not perfect and numerous variants have been proposed [59,60].
The MPQ takes 5-10 minutes to administer which is too long time for some research that requires more rapid collection of data. For this aim an alternative and shortened form of the standard MPQ has been provided. The short-form MPQ (SF-MPQ) which permits obtaining the needed data in a limited time was proposed in 1987 by Melzack and Ronald. SF-MPQ is based on selected and most representative words from the three categories of the original questionnaire. The magnitude of the pain intensity is assessed by the present pain intensity (PPI) and the visual analogue scale [61].
A study carried out on a sample of 189 orthodontic patients in a range of 12-30 years, took advantage of the submission of the modified McGill Pain Questionnaire with VAS to assess the quality and intensity of pain after insertion of initial six different NiTi orthodontic wire as a part of fixed appliances. Each patient received one of the six different superelastic or heat-activated NiTi archwires to solve the crowding and level the teeth in the first phase of the therapy. The research concluded that no correlation is shown between the patient's pain perception and the different types of NiTi arch or the gravity of crowding even though most of the patients reported pain starting 12 hours after the application and lasting for the first 3-4 days [62].
A short version of MPQ was applied to study the effect of orthodontic pain on the Quality of Life (QoL) in patients undergoing orthodontic therapy. 200 patients aged from 13 to 18 are enrolled and underwent the McGill-short form questionnaire with VAS and PPI to evaluate the intensity and severity of pain and if it influenced their quality of life during the first month after the insertion of the appliance. The results support that the orthodontic fixed appliances have a considerable impact on patients’ daily life, especially during the first days when 85% of them think that their QoL is reduced as a consequence of the beginning of the therapy [63].
5. Conclusions
The multidimensional subjective nature of pain makes its objective measurement difficult. Pain assessment is a complex process that tries to describe in an objective way pain as a multifaced phenomenon consisting of different aspects: sensorial, psychological, and experiential. Various assessment tools have been developed and used in the orthodontic field for sensorial aspects assessment based on rating scales and questionnaires: VAS, NRS, VRS, FPS, MPQ.
The use of these instruments makes possible the comparison between the pain experienced during different orthodontic therapy or different appliances, the assessment of the quality and quantity of pain, and the monitoring of pain.
Author Contributions
Conceptualization, D.P. and S.A.; methodology, D.P and S.A..; software, F.C.; validation, D.P., A.S.; formal analysis, A.S. and D.P.; investigation, C.M.V. and A.S.; resources, A.S.; data curation, S.F., A.S. and D.P.; writing—original draft preparation, C.M.V., F.C. and S.F.; writing—review and editing, F.C., S.F., and S.A..; visualization, D.P. and A.S..; supervision, D.P., S.A..; project administration, S.A..; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data supporting reported results are available on request from the corresponding authors.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bergius, M.; Kiliaridis, S.; Berggren, U. Pain in orthodontics. A review and discussion of the literature. J Orofac Orthop. 2000, 61, 125–137. [Google Scholar] [CrossRef]
- Ngan, P.; Kess, B.; Wilson, S. Perception of discomfort by patients undergoing orthodontic treatment. Am J Orthod Dentofacial Orthop. 1989, 96, 47–53. [Google Scholar] [CrossRef]
- Kazancı, F.; Aydoğan, C.; Alkan, Ö. Patients' and parents' concerns and decisions about orthodontic treatment. Korean J Orthod. 2016, 46, 20–26. [Google Scholar] [CrossRef]
- Haynes, S. Discontinuation of orthodontic treatment relative to patient age. J Dent. 1974, 2, 138–142. [Google Scholar] [CrossRef]
- Krishnan, V. Orthodontic pain: from causes to management--a review. Eur J Orthod. 2007, 29, 170–179. [Google Scholar] [CrossRef]
- Patel, V. Non-completion of Active Orthodontic Treatment. British Journal of Orthodontics. 1992, 19, 47–54. [Google Scholar] [CrossRef]
- Oxman, A.D.; Guyatt, G.H. Validation of an index of the quality of review articles. J Clin Epidemiol. 1991, 44, 1271–1278. [Google Scholar] [CrossRef]
- Kazi, A.M.; Khalid, W. Questionnaire designing and validation. J Pak Med Assoc. 2012, 62, 514–516. [Google Scholar]
- Garcia de Yebenes Prous, M.A.; Rodriguez Salvanes, F.; Carmona Ortells, L. [Validation of questionnaires]. Reumatol Clin 2009, 5, 171–177. [Google Scholar]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; Song, X.J.; Stevens, B.; Sullivan, M.D.; Tutelman, P.R.; Ushida, T.; Vader, K. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020, 161, 1976–1982. [Google Scholar] [CrossRef]
- Mercer Lindsay, N.; Chen, C.; Gilam, G.; Mackey, S.; Scherrer, G. Brain circuits for pain and its treatment. Sci Transl Med. 2021, 13, eabj7360. [Google Scholar] [CrossRef]
- Burstone, C. The Biomechanics of Tooth Movement. In Vistas in Orthodontics; Kraus, B.S., Riedel, R.A., Eds.; Lea & Febiger: Philadelphia, 1962; pp. 197–213. [Google Scholar]
- Erdinç, A.M.; Dinçer, B. Perception of pain during orthodontic treatment with fixed appliances. Eur J Orthod 2004, 26, 79–85. [Google Scholar] [CrossRef]
- Firestone, A.R.; Scheurer, P.A.; Bürgin, W.B. Patients' anticipation of pain and pain-related side effects, and their perception of pain as a result of orthodontic treatment with fixed appliances. Eur J Orthod 1999, 21, 387–396. [Google Scholar] [CrossRef]
- Zhang, M.; McGrath, C.; Hägg, U. Changes in oral health-related quality of life during fixed orthodontic appliance therapy. Am J Orthod Dentofacial Orthop 2008, 133, 25–29. [Google Scholar] [CrossRef]
- Jones, M.; Chan, C. The pain and discomfort experienced during orthodontic treatment: A randomized controlled clinical trial of two initial aligning arch wires. Am J Orthod Dentofacial Orthop 1992, 102, 373–381. [Google Scholar] [CrossRef]
- Chen, Y.M.; Mai, L.X.; Li, Y.R. Oral health-related quality of life of fixed orthodontic appliance therapy in adult patients. Chin J Stomal Res 2012, 4, 49–53. [Google Scholar]
- Scheurer, P.A; Firestone, A.R.; Bürgin, W.B. Perception of pain as a result of orthodontic treatment with fixed appliances. Eur J Orthod 1996, 18, 349–357. [Google Scholar] [CrossRef]
- Brown, D.F.; Moerenhout, R.G. The pain experience and psychological adjustment to orthodontic treatment of preadolescents, adolescents, and adults. Am J Orthod Dentofacial Orthop. 1991, 100, 349–356. [Google Scholar] [CrossRef]
- Cardoso, P.C.; Espinosa, D.G.; Mecenas, P.; Flores-Mir, C.; Normando, D. Pain level between clear aligners and fixed appliances: a systematic review. Prog Orthod. 2020, 21, 3. [Google Scholar] [CrossRef]
- Oliver, R.G.; Knapman, Y.M. Attitudes to orthodontic treatment. Br J Orthod. 1985, 12, 179–188. [Google Scholar] [CrossRef]
- Jones, M.L. An investigation into the initial discomfort caused by placement of an archwire. Eur J Orthod 1984, 6, 48–54. [Google Scholar] [CrossRef]
- Pawar, D.; Garten, L.; Kopf, A.; Pathel, N.B. Pain management in children. In Guide to Pain Management in Low-Resource Settings; Int Assoc Study Pain, 2010; pp. 255–267. [Google Scholar]
- Breivik, H. Assessment of pain. BJA: British Journal of Anaesthesia 2008, 101, 17–24. [Google Scholar] [CrossRef]
- Reed, M.D.; Van Nostran, W. Assessing pain intensity with the visual analog scale: a plea for uniformity. J Clin Pharmacol. 2014, 54, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res (Hoboken). 2011, 63 (Suppl 11), S240–52. [Google Scholar] [PubMed]
- Huskisson, E.C. Visual analogue scales. In Pain measurement and assessment; Melzack, R., Ed.; New York Raven Press, 1983; pp. 33–37. [Google Scholar]
- Younger, J.; McCue, R.; Mackey, S. Pain outcomes: a brief review of instruments and techniques. Curr Pain Headache Rep. 2009, 13, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Townsend, M.; Berman, L.B.; Keller, J.L. A comparison of Likert and visual analogue scales for measuring change in function. J Chronic Dis. 1987, 40, 1129–1133. [Google Scholar] [CrossRef]
- Taddio, A.; O'Brien, L.; Ipp, M.; Stephens, D.; Goldbach, M.; Koren, G. Reliability and validity of observer ratings of pain using the visual analog scale (VAS) in infants undergoing immunization injections. Pain. 2009, 147, 141–146. [Google Scholar] [CrossRef]
- Kendrick, D.B.; Strout, T.D. The minimum clinically significant difference in patient-assigned numeric scores for pain. Am J Emerg Med. 2005, 23, 828–832. [Google Scholar] [CrossRef]
- Almasoud, N.N. Pain perception among patients treated with passive self-ligating fixed appliances and Invisalign® aligners during the first week of orthodontic treatment. Korean J Orthod. 2018, 48, 326–332. [Google Scholar] [CrossRef]
- Miller, K.B.; McGorray, S.P.; Womack, R.; Quintero, J.C.; Perelmuter, M.; Gibson, J.; Dolan, T.A.; Wheeler, T.T. A comparison of treatment impacts between Invisalign aligner and fixed appliance therapy during the first week of treatment. Am J Orthod Dentofacial Orthop. 2007, 131, 302–e1. [Google Scholar] [CrossRef]
- Diddige, R.; Negi, G.; Kiran, K.V.S.; Chitra, P. Comparison of pain levels in patients treated with 3 different orthodontic appliances - a randomized trial. Med Pharm Rep. 2020, 93, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.P.; Karoly, P.; Braver, S. The measurement of clinical pain intensity: a comparison of six methods. Pain. 1986, 27, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Zieliński, J.; Morawska-Kochman, M.; Zatoński, T. Pain assessment and management in children in the postoperative period: A review of the most commonly used postoperative pain assessment tools, new diagnostic methods and the latest guidelines for postoperative pain therapy in children. Adv Clin Exp Med. 2020, 29, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Zawawi, K.H. Acceptance of orthodontic miniscrews as temporary anchorage devices. Patient Prefer Adherence. 2014, 8, 933–937. [Google Scholar] [CrossRef]
- Pathak, A.; Sharma, S.; Jensen, M.P. The utility and validity of pain intensity rating scales for use in developing countries. Pain Rep 2018, 3, e672. [Google Scholar] [CrossRef] [PubMed]
- Closs, S.J.; Barr, B.; Briggs, M. et al. A comparison of five pain assessment scales for nursing home residents with varying degrees of cognitive impairment. J Pain Symptom Manage 2004, 27, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Alghadir, A.H.; Anwer, S.; Iqbal, A.; Iqbal, Z.A. Test-retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. J Pain Res. 2018, 11, 851–856. [Google Scholar] [CrossRef]
- Rahman, S.; Spencer, R.J.; Littlewood, S.J.; O'Dywer, L.; Barber, S.K.; Russell, J.S. A multicenter randomized controlled trial to compare a self-ligating bracket with a conventional bracket in a UK population: Part 2: Pain perception. Angle Orthod. 2016, 86, 149–156. [Google Scholar] [CrossRef]
- Manworren, R.C.; Stinson, J. Pediatric Pain Measurement, Assessment, and Evaluation. Semin Pediatr Neurol. 2016, 23, 189–200. [Google Scholar] [CrossRef]
- Huguet, A.; Stinson, J.N.; McGrath, P.J. Measurement of self-reported pain intensity in children and adolescents. J Psychosom Res. 2010, 68, 329–336. [Google Scholar] [CrossRef]
- Stinson, J.N.; Kavanagh, T.; Yamada, J.; Gill, N.; Stevens, B. Systematic review of the psychometric properties, interpretability and feasibility of self-report pain intensity measures for use in clinical trials in children and adolescents. Pain. 2006, 125, 143–157. [Google Scholar] [CrossRef] [PubMed]
- Andersson, V.; Bergman, S.; Henoch, I. et al. Pain and pain management in children and adolescents receiving hospital care: a cross-sectional study from Sweden. BMC Pediatr. 2002, 252. [Google Scholar] [CrossRef] [PubMed]
- Garra, G.; Singer, A.J.; Taira, B.R.; Chohan, J.; Cardoz, H.; Chisena, E.; Thode, H.C. Jr. Validation of the Wong-Baker FACES Pain Rating Scale in pediatric emergency department patients. Acad Emerg Med. 2010, 17, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.L.; Baker, C.M. Pain in children: comparison of assessment scales. Pediatr Nurs. 1988, 14, 9–17. [Google Scholar]
- Williamson, A.; Hoggart, B. Pain: a review of three commonly used pain rating scales. J Clin Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef]
- Bailey, B.; Daoust, R.; Doyon-Trottier, E.; Dauphin-Pierre, S.; Gravel, J. Validation and properties of the verbal numeric scale in children with acute pain. Pain. 2010, 149, 216–221. [Google Scholar] [CrossRef]
- Sánchez-Rodríguez, E.; Miró, J.; Castarlenas, E. A comparison of four self-report scales of pain intensity in 6- to 8-year-old children. Pain. 2012, 153, 1715–1719. [Google Scholar] [CrossRef]
- Castarlenas, E.; Miró, J.; Sánchez-Rodríguez, E. Is the verbal numerical rating scale a valid tool for assessing pain intensity in children below 8 years of age? J Pain. 2013, 14, 297–304. [Google Scholar] [CrossRef]
- De Araújo, M.C.; Bocato, J.R.; Berger, S.B.; Oltramari, P.V.P.; de Castro Ferreira Conti, A.C.; de Almeida, M.R.; Freire Fernandes, T.M. Perceived pain during rapid maxillary expansion in children with different expanders. Angle Orthod. 2021, 91, 484–489. [Google Scholar] [CrossRef]
- Sreenivasagan, S.; Subramanian, A.K.; Selvaraj, A.; Marya, A. Pain Perception Associated with Mini-Implants and Interventions for Pain Management: A Cross-Sectional Questionnaire-Based Survey. Biomed Res Int. 2021, 2021, 4842865. [Google Scholar] [CrossRef]
- Duncan, G.H.; Bushnell, C.M.; Lavigne, G.J. Comparison of verbal and visual analogue scales for measuring the intensity and unpleasantness of experimental pain. Pain. 1989, 37, 295–303. [Google Scholar] [CrossRef] [PubMed]
- Beecher, H.K. Measurement of subjective responses: quantitative effects of drugs; Oxford University Press, 1959. [Google Scholar]
- Katz, J.; Melzack, R. The McGill Pain Questionnaire: Development, psychometric properties, and usefulness of the long form, short form, and short form-2. In Handbook of pain assessment; Turk, D.C., Melzack, R., Eds.; The Guilford Press, 2011; pp. 45–66. [Google Scholar]
- Melzack, R.; Katz, J. The McGill Pain Questionnaire: appraisal and cur- rent status. In Handbook of pain assessment; Turk, D.C., Melzack, R., Eds.; Guilford Press: New York, 1990; pp. 152–168. [Google Scholar]
- Shroff, R.; Dabholakar, T. . Mc Gill Pain Questionnaire: A Cross-Cultural Adaptation Study in Chronic Neck Pain. Int J Physio 2023, 10, 19–23. [Google Scholar] [CrossRef]
- Wilkie, D.J.; Savedra, M.C.; Holzemer, W.L.; Tesler, M.D.; Paul, S.M. Use of the McGill Pain Questionnaire to measure pain: a meta-analysis. Nurs Res. 1990, 39, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Melzack, R.; Katz, J.; Jeans, M.E. The role of compensation in chronic pain: analysis using a new method of scoring the McGill Pain Questionnaire. Pain. 1985, 23, 101–112. [Google Scholar] [CrossRef]
- Melzack, R. The short-form McGill Pain Questionnaire. Pain. 1987, 30, 191–197. [Google Scholar] [CrossRef]
- Marković, E.; Fercec, J.; Šćepan, I.; Glišić, B.; Nedeljković, N.; Juloski, J.; RudolF, R. The correlation between pain perception among patients with six different orthodontic archwires and the degree of dental crowding. Srp Arh Celok Lek. 2015, 143, 134–140. [Google Scholar] [CrossRef]
- Banerjee, S.; Banerjee, R.; Shenoy, U.; Agarkar, S.; Bhattacharya, S. Effect of orthodontic pain on quality of life of patients undergoing orthodontic treatment. Indian J Dent Res. 2018, 29, 4–9. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of the review process.
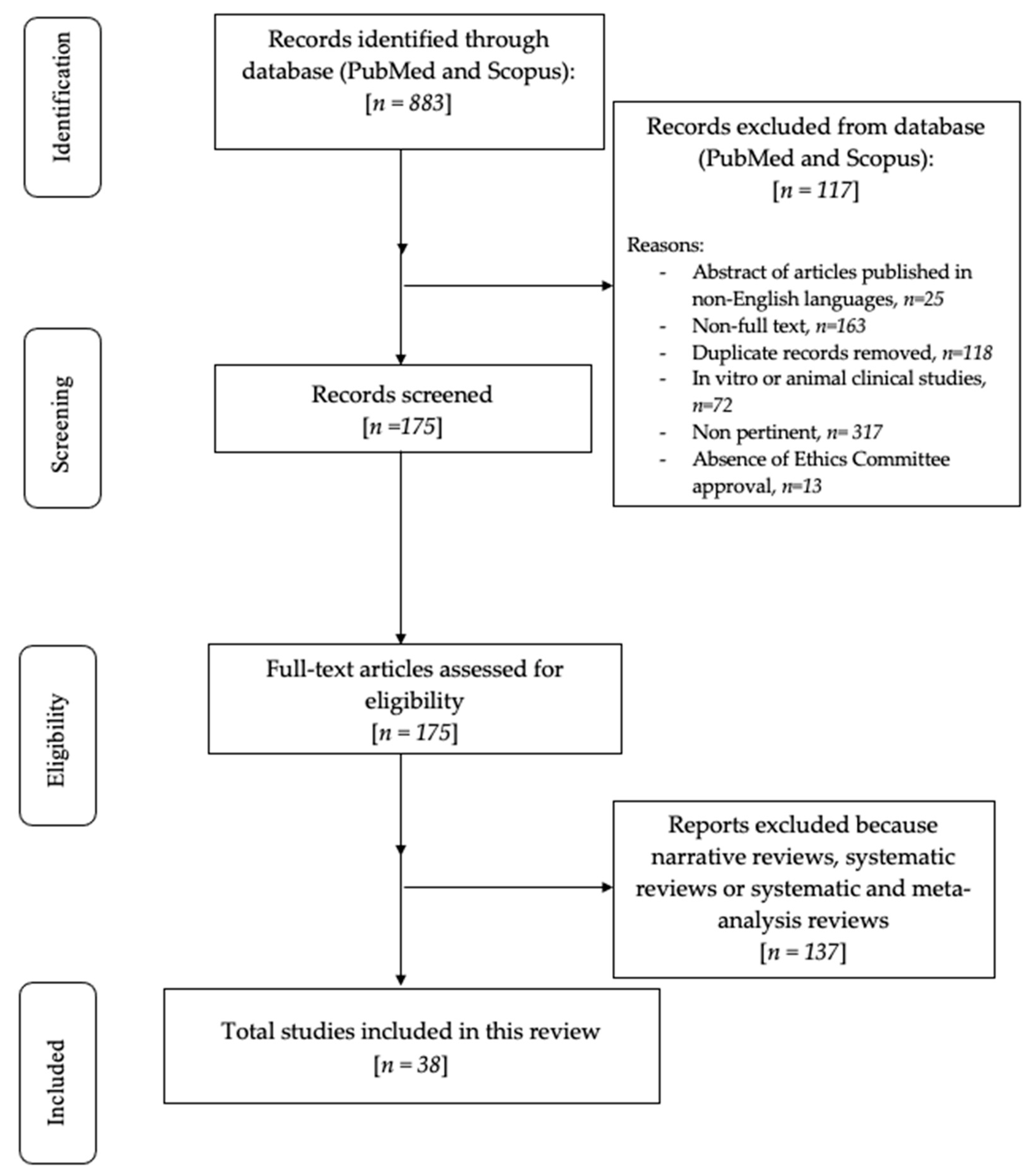
Figure 2.
The visual analog scale.
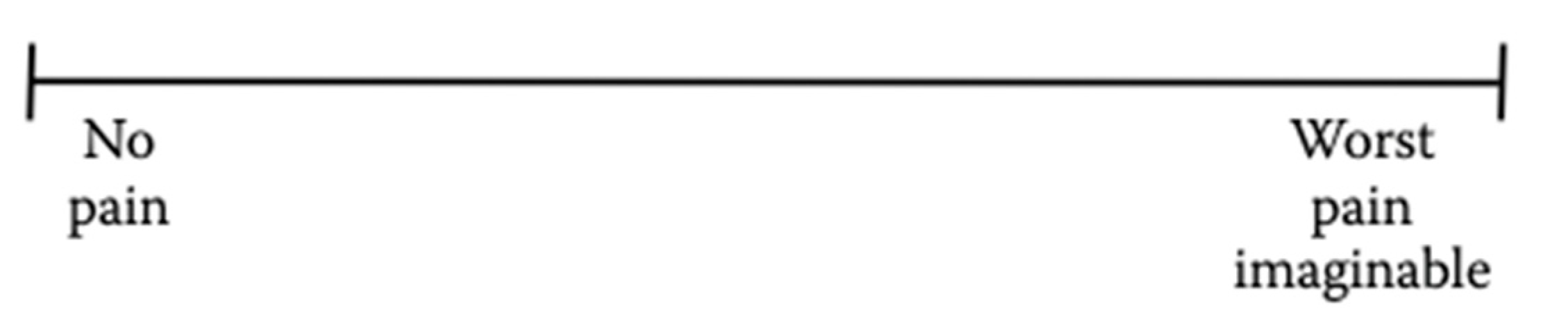
Figure 3.
Numerical Rating Scale (NRS).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



