Submitted:
21 August 2023
Posted:
22 August 2023
You are already at the latest version
Abstract
This study investigated the effects of whole-body circuit training using a weighted vest on plasma resistin, cardiovascular disease risk factors, and cardiorespiratory fitness for normal-weight obese women. In this study, thirty- six normal-weight obese women were divided into three groups: Weighted Vest Circuit Training (WVCT) (n = 12), Body Weight Circuit Training (BWCT) (n = 12), and Control (CON) (n = 12). Whole-body circuit training was conducted three times a week for eight weeks to compare and analyze plasma resistin, cardiovascular disease risk factors, and cardiorespiratory fitness before and after training. Although there was no significant baseline difference between the groups regarding skeletal muscle mass, it significantly increased for the WVCT group after eight weeks. percent body fat significantly decreased for the WVCT and BWCT groups, and there was a significant difference when the percent body fat of these two groups were compared to that of the control group. Moreover, the WVCT and BWCT groups displayed a significant decrease in plasma resistin, showing a significant difference from the CON group. The WVCT and BWCT group showed a significant decrease in plasma IL-6, whereas the CON group showed a significant increase. VO2max significantly increased post-training compared to before in the BWCT group and the WVCT group, and the WVCT group showed differences between groups compared to the BWCT group and the CON group. None of the three groups displayed significant changes in plasma hs-CRP, yet there was a significant difference between the hs-CRPs of the WVCT and BWCT group and that of the CON group. In conclusion, whole-body circuit training using a weighted vest efficiently improves body composition, plasma resistin, and cardiopulmonary fitness, reducing cardiovascular disease risk factors in normal-weight obese women.
Keywords:
circuit training
; resistin
; weighted vest
; normal weight obesity
; cardiopulmonary fitness
; Vo2max
; IL-6
; hs-CRP
; cardiovascular
; cardiovascular disease risk factors
1. Introduction
Obesity is the storage of excess fat in the body, and the obese population is increasing exponentially worldwide [1]. Obesity increases the size and number of adipocytes, causing metabolic disorders [2,3]. A previous study has reported that approximately 29 % of normal-weight women were actually normal-weight obese [4]. Normal-weight obese individuals have a standard Body Mass Index (BMI) yet a percent body fat of more than 30% and low skeletal muscle mass [5,6]. Furthermore, normal-weight obesity has been reported to occur more frequently in women and damage the body due to the high percent body fat [7,8].
Low skeletal muscle mass in normal-weight obesity reduces fatty acid oxidation and basal metabolic rate, increasing visceral and abdominal fat [9]. Thus, it increases the percent body fat in the body and inflammation, increasing the risk of developing cardiovascular disease [10,11]. It has also been reported that normal-weight obesity is associated with a 2.2-fold higher incidence of cardiovascular disease than in the general population[2,12]. high body fat increases resistin, one of the adipocytokines secreted by adipocytes. In turn, this in-creased resistin increases the cardiovascular disease risk factors IL-6 (Interleukin-6) and hs-CRP (high-sensitivity C-reactive protein), causing inflammation in the body [13]. The increased risk factors for cardiovascular disease inhibit the insulin pathway and increase insulin resistance [14,15,16]. Therefore, normal-weight obese individuals should reduce cardiovascular disease factors through improving body composition.
Circuit training is a training method that can simultaneously achieve body fat reduction and skeletal muscle increase by stimulating the whole body through a sequence of regularly circulating exercise forms (stations) [17,18]. Whole-body circuit training using body weight can achieve aerobic and anaerobic training in a short time [19], so the effects of training can be obtained more efficiently and in a shorter time than for complex training [20]. However, in some studies, circuit training using body weight alone did not increase skeletal muscle mass. A previous study related to the above reported that, for obese older women, while weight and body fat mass decreased, skeletal muscle mass did not increase with 50-minute whole-body circuit training at 70 % HRmax three times a week for 12 weeks [21]. In the case of normal-weight obese women, it is essential to reduce body fat. However, since an increase in skeletal muscle mass increases energy consumption [22], it is essential to improve the low resting metabolic rate by increasing the skeletal mass in normal-weight obese women.
Recently, training has been conducted by wearing a weighted vest to increase skeletal muscle mass and improve exercise performance. Training using a weighted vest develops nerve roots through an increase in motor units compared to conventional training due to an increase in load. Moreover, the, increase in mechanical stress activates mTOR (mammalian Target Of Rapamycin), a muscle protein synthesis factor, and promotes muscle protein synthesis. The result is a significant increase in both muscle strength and skeletal muscle mass [23,24]. In addition, in postmenopausal women with osteoporosis, after treadmill aerobic training for 20 minutes at 50-60 % HRR(Heart Rate Reserve) intensity three times a week for six weeks, the group wearing a Weighted Vest (8 % of body weight) had lower body fat mass than the group not wearing a Weighted Vest. Moreover, wearing a weighted vest was also found to be more effective for increasing skeletal muscle mass. Moreover, more effective in increasing skeletal muscle mass [25]. Given these results, for normal-weight obese women, whole-body circuit training performed wearing the Weighted Vest is expected to not only reduce body fat but also increase skeletal muscle mass.
The research findings above allow predictions to be made about the positive results of whole-body circuit training using a Weighted Vest. Circuit training using a weighted vest is expected to be more effective for increasing skeletal muscle mass. The approach is also expected to reduce plasma resistin concentration and cardiovascular disease risk factors as the percent body fat decreases and increases skeletal muscle mass. In addition, the resulting changes in body composition are expected to positively affect cardiovascular disease risk factors. This study aims to confirm the expected effects of whole-body circuit training using a weighted vest on plasma resistin, cardiovascular disease risk factors, and cardiopulmonary fitness.
2. Materials and Methods
2.1. Subjects
This study recruited as subjects normal-weight obese women in their 20s and 30s living in Seoul. Through a pre-survey, normal-weight obese women who had no particular medical disease and had not participated in a regular exercise program for the past six months were selected. In addition, only normal-weight obese women who had not taken oral contraceptives within the last six months and had regular menstrual cycles were recruited. This study was conducted with the approval of the Korea University Bioethics Committee (KUIRB-2020-0279-01). Following the Declaration of Helsinki, the purpose and procedures of this study were fully explained to the participants, and for participation in the study the consent form and questionnaire were voluntarily filled out before proceeding. The number of study participants was set to achieve an effect size η2 = 0.095, significance level 0.05, statistical power 0.85 in Repeated measures ANOVA within-between interaction using G*Power (gpower.software.informer.com/3.1). As a result of G*Power calculation, the number of participants was calculated as thirty people. Therefore, thirty-six participants were recruited, considering dropouts due to injury or illness. Moreover, the participants were randomly placed into the Weighted Vest Circuit Training (WVCT) group, Body Weighted Circuit Training group (BWCT), and Control (CON) group. The body composition of the study participants is shown in <Table 1>, and the criteria for determining normal-weight obesity were established based on the criteria applied in previous studies [7]
BMI: 18–25 kg / m²
Percent Body Fat: more than 30 %
2.2. Experimental Design
This experiment was a randomized control experiment, and participants were tested before (PRE) and after (POST) an eight-week treatment. Pre- and post-tests measured body composition, grade exercise test, and blood pressure. The measurement procedure is shown in <Figure 1>.
2.3. Measurement
(1) Body Composition
The body composition of the study subjects was measured twice, before (0 weeks) and after (8 weeks). After fasting for 12 hours, the percent body fat, skeletal muscle mass, height, weight, and body mass index of all participants was measured using a bioelectrical resistance meter (Inbody 570, Biospace, Korea) and an automatic height weight meter (BSM 330, Biospace, Korea). The participants were measured while wearing simple clothes (pants, short sleeves, shorts).
(2) Graded Exercise Test(Cardiorespiratory Fitness)
Excessive physical activity was prohibited 24 hours before the test, and the participants arrived in the laboratory 1 hour before the graded exercise test measurement and were stabilized. After the participants had lightly stretched as a warm-up, rested until reaching a stable heart rate and worn a gas mask, the test began. Following the Modified Bruce Protocol, a treadmill was used for the graded exercise test. During the test, VO2max was measured using a respiratory gas analyzer (Quark b2, Cosmed, Italy), and the internal temperature and humidity of the laboratory were maintained at 22 ℃ and 50 %, respectively. Heart rate was monitored throughout the exercise using a wireless heart rate monitor (RS400, Polar, Finland). Following the Modified Bruce Protocol, the load started at 1.7 mph, and the speed and gradient were increased every 3 minutes until the participants were exhausted. The criteria for discontinuation of the test were the respiratory exchange rate being 1.15 or higher, the oxygen intake remaining at a plateau despite increased exercise intensity, or the participant voluntarily expressing her intention to give up [26].
(3) Blood Sampling and Blood Pressure Measurement
The participants’ menstrual cycles were noted, and blood was collected in the follicular phase when the hormone cycle was most stable for the blood. Participants visited the laboratory to give blood samples after fasting for 12 hours. After resting for 30 minutes, the blood pressure of the brachial artery was measured using a blood pressure monitor (HEM-7121-E, Omron, Japan). Afterward, samples were collected from the central forearm vein once before and after. All blood samples were separated into plasma and serum by centrifugation at 3000 rpm for 15 minutes immediately after blood collection and stored at -80 C°. The collected blood samples were used to analyze plasma resistin, IL-6, hs-CRP, total cholesterol (TC), HDL-C (High Density Lipoprotein Cholesterol), LDL-C (Low Density Lipoprotein Cholesterol).
2.4. Training Protocol
Whole-body circuit training was performed three times a week for eight weeks. Before and after training, a 5-minute stretching routine was performed as warm-up and cool-down. Modifying and supplementing the whole-body circuit training protocol of the previous study[20], the training protocol included nine exercise stations that used the large muscle groups of the whole body (Figure 2). The calorie consumption during training was adjusted to 200 kcal before the program was carried out. In addition, the weight of the weighted vest was 10% of the body weight, and the load was set by rounding to one decimal place. During exercise, the training intensity and amount of exercise was monitored using a wireless heart rate monitor and a momentum meter (A370, Polar, Finland). The target heart rate was set according to the Karvonen formula [(resting heart rate x 60–70 %) + resting heart rate], and 2–3 SETs were performed according to the amount of exercise required. 1 minute break time was given between sets. Before the experiment, to adapt to the equipment and injury prevention, all participants wore a weighted vest of 5 % of their body weight twice a week for two weeks. They then proceeded with just 1 SET of the Whole-body circuit training protocol.
2.5. Data Analysis
All the data collected in this study was statistically processed using SPSS ver. 25.0 (SPSS Inc, Chicago, USA). All parameters are presented as mean and standard deviations. Repeated measures ANOVA was conducted to determine the difference between the measured values of the three groups, and the Bonferroni method was used as post hoc test. If no interaction was apparent, the main effect of the independent variable was confirmed, and the statistical significance level was set at p < .05.
3. Results
The results of this study were derived by analyzing the differences in the data before and after eight weeks of training by normal-weight obese women.
3.1. Changes in Body Composition
<Table 2> shows the results of analyzing changes in body composition.
Body Weight (kg), after eight weeks of training, showed no interaction between time and group (df = 2, F = .892, p = .419). There was a significant difference when comparing time points by group (p = .028), but no significant difference occurred when comparing the main effects (p = .080; p = .051; p = .609).
BMI (kg/m2) did not show any change.
An interaction between the time point and group in Skeletal Muscle Mass(kg) was found (df = 2, F = 3.193, p = .042). In the WVCT group, Skeletal Muscle Mass increased significantly post- compared to pre-training (p = .000). There was no significant change between the BWCT group and the CON group post and pre (p = .448; p = .477).
Interaction between the time point and group was apparent regarding Percent Body Fat (%) (df = 2, F = 10.721, p = .000). For the WVCT group and the BWCT group, Percent Body Fat decreased significantly between pre- and post-training (p =.002; p =.002), whereas for the CON group it did not (p = .740). Furthermore, considering Percent Body Fat, post-training, the WBCT group and the BWCT group showed significant difference to the CON group (p =.003; p =019).
3.2. Changes in Cardiorespiratory Fitness
<Figure 3> shows the result of analyzing changes in VO2max(ml/kg/min).
After eight weeks of training, there was an interaction between time and group in VO2max (ml/kg/min) (df=2, F=4.899, p=.014). In the WVCT and BWCT groups, VO2max significantly increased post-training compared to before (p =.000; p =.040). In contrast, the CON group showed no significant change (p = .743). The WVCT group showed a significant increase in VO2max compared to the BWCT and CON groups (p = .004; p = .001).
3.3. Changes in Plasma Resistin.
Resistin (ng/ml) showed an interaction between the time point and group (df = 2, F = 8.528, p = .001). For the WVCT group and the BWCT group, there was a significant decrease post-training compared to pre-training (p =.000, p = .006), whereas the CON group had no significant difference (p = .306). After training, the WVCT and BWCT groups showed significant differences compared to the CON group (p = .001; p = .007) (Figure 4).
3.4. Changes in Cardiovascular Disease Risk Factors
<Table 3> shows the results of analyzing changes in Cardiovascular Disease Risk Factors.
After eight weeks of training, IL-6 (pg/ml) showed no interaction between time and group (df = 2, F = 20.698, p = .082). With the WVCT and BWCT groups, there was a significant decrease post-training compared to before (p = .000, p = .003). There was no change for the control group (p = .557). After training, the WVCT and BWCT groups significantly decreased in IL-6 compared to the CON group (p = .022; p = .038).
For hs-CRP (mg/L), an interaction between the time point and group was found (df = 2, F = 13.206, p = .000). There was a significant increase in the CON group post-training compared to the pre-group (p = .003), but no change was observed with the WVCT and BWCT groups (p = .075; p = .135). After training, the WVCT and BWCT groups showed intergroup difference compared to the CON group (p = .035; p = .013).
For TC (mg/dL), an interaction between the time point and group was found (df = 2, F = 3.303, p = .049). With the WVCT group, there was a significant decrease in post-training compared to pre-training (p = .016), but no change was observed with the WVCT and CON groups (p = .569; p = .784).
For LDL-C (mg/dL, an interaction between the time point and group ) was observed (df = 2, F = 6.292, p = .005). The WBCT group showed a significant decrease post-training compared to the pre-training (p = .011), but no change was found in the BWCT and CON groups (p = .562; p = .668).
With HDL-C (mg/dL), there was no interaction between the time point and group (df = 2, F = 1.930, p = .161). There was a significant decrease in the CON group post-training compared to the pre-training (p = .000), whereas no change was observed in the WVCT and BWCT groups (p = .479; p = .342). After training, the WVCT group showed a group difference compared to the CON group (p = .014).
With SBP (mmHg), there was no interaction between the time point and group (df = 2, F = .187, p = .831). After training, the WVCT group exhibited an intergroup difference compared to both the BWCT and CON groups (p = .039; p = .032).
For DBP (mmHg, there was no change, either between time points or groups.
3.5. Changes in Rate of Improvement in Normal-Weight Obesity
The improvement rate (%) of normal-weight obesity was 58.33% for the WVCT group and 25% for the BWCT group, improving only in the two groups, and no change was observed in the CON group.
4. Discussion
This study confirmed the effects for normal obese women of whole-body circuit training using a weighted vest for eight weeks to improve body composition in terms of plasma resistin, cardiovascular disease risk factors, and Cardiorespiratory Fitness. Comparative groups were compared and analyzed.
Regarding body composition, this study showed that skeletal muscle mass increased significantly in the WVCT group, and percent body fat decreased significantly in both the WVCT and BWCT groups. Circuit training is a method in which short breaks are set during resistance training, and these short breaks during exercise stimulate growth hormone secretion [27]. In addition, circuit training using the whole body has the effect of simultaneously reducing body fat through aerobic training and maintaining Skeletal muscle mass through resistance training [28]. According to previous studies, aerobic training performed by postmenopausal women with osteoporosis using a treadmill for 20 minutes at an HRR of 50-60% intensity wearing a weighted vest 4-8% of body weight three times a week for six weeks causes skeletal muscle mass to significantly increase [25]. The increased mechanical load promotes the secretion of growth hormone, IGF-1(Insulin Like Growth Factor-1) and anabolic hormones and activates mTOR [29,30,31]. The current study concluded that, using a weighted vest for whole-body circuit training rather than conventional whole-body circuit training, body composition was improved due to the increased mechanical stress.
Conducting whole-body circuit training for eight weeks with normal-weight obese women caused VO2max to significantly increase in both the WVCT group using a Weighted Vest and the BWCT groups without. The effect was significantly higher in the WVCT group post-training. Simultaneous training, involving both aerobic and resistance training, reduces muscle oxygen saturation and increases active oxygen in the body, stimulating hypoxia-inducible factor HIF-1α(Hypoxia-inducible factors-1-alpha). When HIF-1α is stimulated, PGC-1α (Peroxisome proliferator-activated receptor gamma coactivator 1-alpha) is activated to increase cardiorespiratory fitness [32]. In addition, increased mechanical stress due to exercise has been reported to increase reactive oxygen species[33,34]. In this study, after training VO2max was found to be higher in the WVCT group than in the BWCT group. This extra improvement was thought to be caused by the increase in mechanical stress due to the weighted vest leading to increased active oxygen in the body, thereby further increasing VO2max.
Resistin is one of the adipocytokines secreted by adipocytes and promotes cardiovascular disease by increasing inducing inflammation [35]. Plasma resistin concentration has also been reported to correlate positively with body fat mass [36,37]. In this study, the plasma resistin concentration was significantly decreased in both the WVCT and BWCT groups. In previous studies, plasma resistin concentration decreased mainly though aerobic and combined training [38,39] Aerobic exercise training by women in their 20s using a treadmill at 70 to 80 % HRmax, for eight weeks four times a week, was found to cause plasma resistin concentration to decrease [40]. Similarly, plasma resistin concentration was found to significantly decrease in a study of overweight adolescents undergoing aerobic training using a treadmill, rowing machine, and cycle ergometer at an intensity of 60 to 85% VO2max 3 times a week for eight weeks [41]. Previous studies reported that the decrease in plasma resistin concentration resulted from a decrease in body fat, and it is thought that the reduction of plasma resistin concentration in this study is also due to the decrease in the percent body fat.
Normal-weight obese people have a body weight and BMI within the normal range, but their percent body fat is the same as that of obese people. A high percent body fat increases cytokine IL-6, an inflammatory substance, and promotes hs-CRP production in the liver [42]. The increase in IL-6 and hs-CRP deteriorates vascular function and promotes cardiovascular disease. The results of this study show that the concentration of plasma IL-6 is significantly decreased in both the WVCT and BWCT groups. While there was no significant difference in hs-CRP, there was a decreasing trend in the WVCT and BWCT groups. In a previous study conducting combined training five times a week for eight weeks, plasma IL-6 and CRP concentrations were found to be significantly reduced[43]. In the current study, the concentration of plasma IL-6 decreased, and the concentration of hs-CRP in blood tended to decrease. The level of resistin in the blood affects the level of IL-6 because it activates NF-kβ and AP-1 [15]. Therefore, the decrease in plasma IL-6 concentration in this study results from the decrease in resistin concentration. It has also been reported that hs-CRP is a protein affected by diet, age, training intensity, and training duration [44]. The lack of change in plasma hs-CRP concentration is thought to be due to the participants’ lack of control over daily life and low initial fitness levels.
Total cholesterol and LDL-C cause hypercholesterolemia and increase the prevalence of cardiovascular disease. In addition, total cholesterol and LDL-C positively correlate with the percent body fat [45,46]. In the current study, serum total cholesterol and LDL-C levels were found to significantly decrease only in the WVCT group. In a previous study in which circuit training was undertaken for 30 minutes twice a week for 12 weeks by middle-aged women, serum total cholesterol and LDL-C levels decreased. LDL-C concentration in obese men decreased due to 60-minute Whole-body circuit training at 60% HRmax intensity three times a week for 12 weeks [28]. Previous studies have reported that this results from a decrease in body fat. In the current study, the reduction in LDL-C and total cholesterol in the WVCT group is thought to result from improved body composition.
HDL-C prevents cardiovascular disease and plays a role in protecting blood vessels. This study showed no significant change in serum HDL-C concentration after training. In another study, complex training, aerobic training, and resistance training conducted five times a week for 12 weeks with obese people led to no significant change in HDL-C concentration in all groups [47]. Another study, in which circuit training was conducted three times a week for 12 weeks with obese female college students, showed no change in blood HDL-C concentration [48]. Previous studies reported that blood HDL-C did not increase because it was affected by diet, training intensity, type, and time. Therefore, the result of this study is considered to be the result of the same reason as the previous study, and it is considered that the HDL-C concentration in the blood of the research subjects did not increase further because it was within the normal range.
Blood pressure is closely related to cardiovascular and stroke diseases. Blood pressure has been found to be directly related to cardiovascular disease and cause various complications [49]. The results in the current study show that systolic blood pressure was significantly reduced in the WVCT group compared to the BWCT group, and no significant change occurred in diastolic blood pressure. It has been reported that blood pressure decreases when aerobic training is performed at an intensity of 70 % VO2max or higher [50]. In this study, it is considered that the participants’ blood pressure was within the normal range and at a relatively normal level; therefore, no change was seen.
In this study, normal weight obesity was improved only in the WVCT and BWCT groups, with the WVCT group showing a higher improvement rate of 58.33 % compared to that 25% for the BWCT group. These results show the effect of training using the Weighted Vest, and it is thought that the percent body fat decreased further as the skeletal muscle mass increased.
5. Conclusions
In conclusion, 8-week weighted vest circuit training conducted on normal-weight obese women is more effective in improving plasma resistin, cardiovascular disease risk factors, and Cardiorespiratory Fitness than body-weighted circuit training, despite the same intensity and amount of exercise. Although the body weight and body mass index did not show significant differences, the percent body fat decreased, and skeletal muscle mass increased. positively affects plasma resistin, cardiovascular disease risk factors, and Cardiorespiratory Fitness. Whole-body circuit training using a weighted vest effectively improves plasma resistin, cardiovascular disease risk factors, Cardiorespiratory Fitness, and body composition for normal-weight obese people with high percent body fat and low skeletal muscle mass. It will also be an effective exercise method for normal-weight obese people with low physical fitness.
This study conducted whole-body circuit training using a weighted vest for eight weeks on normal-weight obese women, and the percent body fat decreased. Furthermore, the skeletal muscle mass increased. In future studies, it would be helpful to check anabolic hormones such as growth hormones to confirm the effect of the Weighted Vest on normal-weight obese people more closely. Also, Insulin resistance and fasting blood glucose associated with type 2 diabetes should be checked. It would also be helpful to check changes in body composition, resistin, cardiovascular disease risk factors, and cardiorespiratory fitness by diversifying the load and exercise method (station motion, intensity).
Author Contributions
Conceptualization, J.-W.K. ; methodology: J.-W.K. and S.-J.Y.; validation of data: J.-W.K. and D.-H.K.; formal analysis: J.-W.K. and E.-S.K; investigation: J.-W.K; writing original draft: J.-W.K.; visualization: J.-W.K.; writing—review and editing, J.-W.K, D.-H.K and E.-S.K.; supervision: S.-J.Y.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the Institutional Review Board of Korea University (KUIRB-2020-0279-01) before the experiment and was conducted by their guidelines and the Declaration of Helsinki (1964).
Informed Consent Statement
After explaining the purpose, method, and potential risks of the study to all participants, the consent form was signed, and participants who were willing to participate voluntarily were recruited. Moreover, written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
The data in this study are appropriately provided by the corresponding author via email.
Acknowledgments
We thank all the participants and researchers who participated in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Organization, W.H. Obesity and overweight. 2017.
- Oliveros, E.; Somers, V.K.; Sochor, O.; Goel, K.; Lopez-Jimenez, F. The concept of normal weight obesity. Progress in cardiovascular diseases 2014, 56, 426–433. [Google Scholar] [CrossRef]
- Wang, Q.A.; Tao, C.; Gupta, R.K.; Scherer, P.E. Tracking adipogenesis during white adipose tissue development, expansion and regeneration. Nature medicine 2013, 19, 1338–1344. [Google Scholar]
- Kim, J. Risk stratification of metabolic syndrome according to obesity, abdominal obesity and gender in Korean adults [dissertation]. Seoul: Korea University. 2014. [Google Scholar]
- Flegal, K.M.; Shepherd, J.A.; Looker, A.C.; Graubard, B.I.; Borrud, L.G.; Ogden, C.L.; Harris, T.B.; Everhart, J.E.; Schenker, N. Comparisons of percentage body fat, body mass index, waist circumference, and waist-stature ratio in adults. The American journal of clinical nutrition 2009, 89, 500–508. [Google Scholar] [CrossRef]
- Romero-Corral, A.; Somers, V.K.; Sierra-Johnson, J.; Thomas, R.J.; Collazo-Clavell, M.; Korinek, J.; Allison, T.G.; Batsis, J.; Sert-Kuniyoshi, F.; Lopez-Jimenez, F. Accuracy of body mass index in diagnosing obesity in the adult general population. International journal of obesity 2008, 32, 959–966. [Google Scholar] [CrossRef]
- De Lorenzo, A.; Martinoli, R.; Vaia, F.; Di Renzo, L. Normal weight obese (NWO) women: an evaluation of a candidate new syndrome. Nutrition, Metabolism and Cardiovascular Diseases 2006, 16, 513–523. [Google Scholar] [CrossRef]
- De Lorenzo, A.; Del Gobbo, V.; Premrov, M.G.; Bigioni, M.; Galvano, F.; Di Renzo, L. Normal-weight obese syndrome: early inflammation? The American journal of clinical nutrition 2007, 85, 40–45. [Google Scholar]
- Lim, K.; Yang, S.; Kim, T.; Yoo, H.; Kang, H.; Song, W.; Baik, S.-H.; Choi, D.; Choi, K.M. The association between the ratio of visceral fat to thigh muscle area and metabolic syndrome: the Korean Sarcopenic Obesity Study (KSOS). Clinical endocrinology 2010, 73, 588–594. [Google Scholar] [CrossRef]
- You, T.; Ryan, A.S.; Nicklas, B.J. The metabolic syndrome in obese postmenopausal women: relationship to body composition, visceral fat, and inflammation. The Journal of Clinical Endocrinology & Metabolism 2004, 89, 5517–5522. [Google Scholar] [CrossRef]
- Valdez, R.; Seidell, J.; Ahn, Y.I.; Weiss, K.M. A new index of abdominal adiposity as an indicator of risk for cardiovascular disease. A cross-population study. International journal of obesity and related metabolic disorders: journal of the International Association for the Study of Obesity 1993, 17, 77–82. [Google Scholar]
- Romero-Corral, A.; Somers, V.K.; Sierra-Johnson, J.; Korenfeld, Y.; Boarin, S.; Korinek, J.; Jensen, M.D.; Parati, G.; Lopez-Jimenez, F. Normal weight obesity: a risk factor for cardiometabolic dysregulation and cardiovascular mortality. European heart journal 2010, 31, 737–746. [Google Scholar] [CrossRef]
- Banerjee, R.R.; Rangwala, S.M.; Shapiro, J.S.; Rich, A.S.; Rhoades, B.; Qi, Y.; Wang, J.; Rajala, M.W.; Pocai, A.; Scherer, P.E. Regulation of fasted blood glucose by resistin. Science 2004, 303, 1195–1198. [Google Scholar] [CrossRef]
- Benomar, Y.; Gertler, A.; De Lacy, P.; Crépin, D.; Ould Hamouda, H.; Riffault, L.; Taouis, M. Central resistin overexposure induces insulin resistance through Toll-like receptor 4. Diabetes 2013, 62, 102–114. [Google Scholar] [CrossRef]
- Dasari, R.; Raghunath, V. Obesity and Type II diabetes mellitus: Is resistin the link? Journal of Diabetes and Endocrine Practice 2018, 1, 1–8. [Google Scholar]
- Luo, Z.; Zhang, Y.; Li, F.; He, J.; Ding, H.; Yan, L.; Cheng, H. Resistin induces insulin resistance by both AMPK-dependent and AMPK-independent mechanisms in HepG2 cells. Endocrine 2009, 36, 60–69. [Google Scholar] [CrossRef]
- Adamson, G.T.; Morgan, R. Circuit training. Journal of the Physical Education Association 1954, 46. [Google Scholar] [CrossRef]
- Haennel, R.; Teo, K.-K.; Quinney, A.; Kappagoda, T. Effects of hydraulic circuit training on cardiovascular function. Medicine and science in sports and exercise 1989, 21, 605–612. [Google Scholar] [CrossRef]
- Solanki, R.; Bhise, A.; Shukla, Y.; Prabhakar, M. Effects of high intensity circuit training using body weight on aerobic fitness and muscular endurance in college students. Physiotherapy 2015, 101, e1418–e1419. [Google Scholar] [CrossRef]
- Klika, B.; Jordan, C. High-intensity circuit training using body weight: Maximum results with minimal investment. ACSM’s Health & Fitness Journal 2013, 17, 8–13. [Google Scholar]
- Bocalini, D.S.; Lima, L.S.; de Andrade, S.; Madureira, A.; Rica, R.L.; Dos Santos, R.N.; Serra, A.J.; Silva Jr, J.A.; Rodriguez, D.; Figueira Jr, A. Effects of circuit-based exercise programs on the body composition of elderly obese women. Clinical interventions in aging 2012, 551–556. [Google Scholar] [CrossRef]
- Potteiger, J.A.; Kirk, E.P.; Jacobsen, D.J.; Donnelly, J.E. Changes in resting metabolic rate and substrate oxidation after 16 months of exercise training in overweight adults. International journal of sport nutrition and exercise metabolism 2008, 18, 79–95. [Google Scholar] [CrossRef]
- Galvao, D.A.; Taaffe, D.R. Resistance exercise dosage in older adults: single-versus multiset effects on physical performance and body composition. Journal of the American Geriatrics Society 2005, 53, 2090–2097. [Google Scholar] [CrossRef] [PubMed]
- Macadam, P.; Cronin, J.B.; Feser, E.H. Acute and longitudinal effects of weighted vest training on sprint-running performance: A systematic review. Sports Biomechanics 2022, 21, 239–254. [Google Scholar] [CrossRef] [PubMed]
- Roghani, T.; Torkaman, G.; Movasseghe, S.; Hedayati, M.; Goosheh, B.; Bayat, N. Effects of short-term aerobic exercise with and without external loading on bone metabolism and balance in postmenopausal women with osteoporosis. Rheumatology international 2013, 33, 291–298. [Google Scholar] [CrossRef] [PubMed]
- McInnis, K.; Balady, G.J. Comparison of submaximal exercise responses using the Bruce vs modified Bruce protocols. Medicine and science in sports and exercise 1994, 26, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Murphy, E.; Schwarzkopf, R. Effects of Standard Set and Circuit Weight Training on Excess Post-exercise Oxygen. Journal of Applied Sport Science Research 1992, 6, 88–91. [Google Scholar]
- Contrò, V.; Bianco, A.; Cooper, J.; Sacco, A.; Macchiarella, A.; Traina, M.; Proia, P. Effects of different circuit training protocols on body mass, fat mass and blood parameters in overweight adults. Journal of Biological Research-Bollettino della Società Italiana di Biologia Sperimentale 2017, 90. [Google Scholar] [CrossRef]
- Juffer, P.; Jaspers, R.T.; Lips, P.; Bakker, A.D.; Klein-Nulend, J. Expression of muscle anabolic and metabolic factors in mechanically loaded MLO-Y4 osteocytes. American Journal of Physiology-Endocrinology and Metabolism 2012, 302, E389–E395. [Google Scholar] [CrossRef]
- Juffer, P.; Bakker, A.D.; Klein-Nulend, J.; Jaspers, R.T. Mechanical loading by fluid shear stress of myotube glycocalyx stimulates growth factor expression and nitric oxide production. Cell biochemistry and biophysics 2014, 69, 411–419. [Google Scholar] [CrossRef]
- Zanchi, N.E.; Lancha, A.H. Mechanical stimuli of skeletal muscle: implications on mTOR/p70s6k and protein synthesis. European journal of applied physiology 2008, 102, 253–263. [Google Scholar] [CrossRef]
- Fyfe, J.J.; Bishop, D.J.; Stepto, N.K. Interference between concurrent resistance and endurance exercise: molecular bases and the role of individual training variables. Sports medicine 2014, 44, 743–762. [Google Scholar] [CrossRef]
- Close, G.L.; Ashton, T.; Cable, T.; Doran, D.; MacLaren, D.P. Eccentric exercise, isokinetic muscle torque and delayed onset muscle soreness: the role of reactive oxygen species. European journal of applied physiology 2004, 91, 615–621. [Google Scholar] [CrossRef]
- Ozaki, H.; Loenneke, J.P.; Buckner, S.L.; Abe, T. Muscle growth across a variety of exercise modalities and intensities: contributions of mechanical and metabolic stimuli. Medical hypotheses 2016, 88, 22–26. [Google Scholar] [CrossRef]
- Holcomb, I.N.; Kabakoff, R.C.; Chan, B.; Baker, T.W.; Gurney, A.; Henzel, W.; Nelson, C.; Lowman, H.B.; Wright, B.D.; Skelton, N.J. FIZZ1, a novel cysteine-rich secreted protein associated with pulmonary inflammation, defines a new gene family. The EMBO journal 2000, 19, 4046–4055. [Google Scholar] [CrossRef]
- Azuma, K.; Katsukawa, F.; Oguchi, S.; Murata, M.; Yamazaki, H.; Shimada, A.; Saruta, T. Correlation between serum resistin level and adiposity in obese individuals. Obesity research 2003, 11, 997–1001. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Qin, Y.; Zheng, X.; Qiu, J.; Gong, L.; Mao, H.; Jia, W.; Guo, J. The relationship between human serum resistin level and body fat content, plasma glucose as well as blood pressure. Zhonghua yi xue za zhi 2002, 82, 1609–1612. [Google Scholar] [PubMed]
- Afshounpour, M.T.; Habibi, A.; Ranjbar, R. Impact of combined exercise training on plasma concentration of Apelin, resistin and insulin resistance in patients with type 2 diabetics’ male. Hormozgan Medical Journal 2016, 20. [Google Scholar]
- Hejazi, K.; Hosseini, S.R.A.; Fathi, M.; Ziaaldini, M.M. Responses of Visfatin and Resistin Concentration to Different Aerobic Training Intensities Protocols. Annals of Military and Health Sciences Research 2020, 18. [Google Scholar] [CrossRef]
- Rashidlamir, A.; Gholamian, S.; Ebrahimi Atri, A.; Seyyedalhoseyni, M.; Hesar Kooshki, M. Effect of regular aerobic exercise on plasma levels of resistin and adiponectin in active young females. Journal of Mazandaran University of Medical Sciences 2013, 23, 67–76. [Google Scholar]
- Jones, T.E.; Basilio, J.; Brophy, P.; McCammon, M.; Hickner, R. Long-term exercise training in overweight adolescents improves plasma peptide YY and resistin. Obesity 2009, 17, 1189–1195. [Google Scholar] [CrossRef]
- Shah, A.; Mehta, N.; Reilly, M.P. Adipose inflammation, insulin resistance, and cardiovascular disease. Journal of Parenteral and Enteral Nutrition 2008, 32, 638–644. [Google Scholar] [CrossRef]
- Lee, J.S.; Kim, C.G.; Seo, T.B.; Kim, H.G.; Yoon, S.J. Effects of 8-week combined training on body composition, isokinetic strength, and cardiovascular disease risk factors in older women. Aging clinical and experimental research 2015, 27, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Rifai, N.; Pfeffer, M.A.; Sacks, F.; Braunwald, E. Long-term effects of pravastatin on plasma concentration of C-reactive protein. Circulation 1999, 100, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, J.; Murano, S.; Kawamura, I.; Nakamura, F.; Murase, Y.; Kawashiri, M.-a.; Nohara, A.; Asano, A.; Inazu, A.; Mabuchi, H. The relationship of percent body fat by bioelectrical impedance analysis with blood pressure, and glucose and lipid parameters. Journal of atherosclerosis and thrombosis 2006, 13, 221–226. [Google Scholar] [CrossRef]
- Oda, E. LDL cholesterol was more strongly associated with percent body fat than body mass index and waist circumference in a health screening population. Obesity research & clinical practice 2018, 12, 195–203. [Google Scholar] [CrossRef]
- Ho, S.S.; Dhaliwal, S.S.; Hills, A.P.; Pal, S. The effect of 12 weeks of aerobic, resistance or combination exercise training on cardiovascular risk factors in the overweight and obese in a randomized trial. BMC public health 2012, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-W.; Ko, Y.-C.; Seo, T.-B.; Kim, Y.-P. Effect of circuit training on body composition, physical fitness, and metabolic syndrome risk factors in obese female college students. Journal of exercise rehabilitation 2018, 14, 460. [Google Scholar] [CrossRef] [PubMed]
- Burt, V.L.; Cutler, J.A.; Higgins, M.; Horan, M.J.; Labarthe, D.; Whelton, P.; Brown, C.; Roccella, E.J. Trends in the prevalence, awareness, treatment, and control of hypertension in the adult US population: data from the health examination surveys, 1960 to 1991. Hypertension 1995, 26, 60–69. [Google Scholar] [CrossRef]
- Halbert, J.A.; Silagy, C.A.; Finucane, P.; Withers, R.; Hamdorf, P.; Andrews, G. The effectiveness of exercise training in lowering blood pressure: a meta-analysis of randomised controlled trials of 4 weeks or longer. Journal of human hypertension 1997, 11, 641–649. [Google Scholar] [CrossRef]
Figure 1.
Research Procedure.
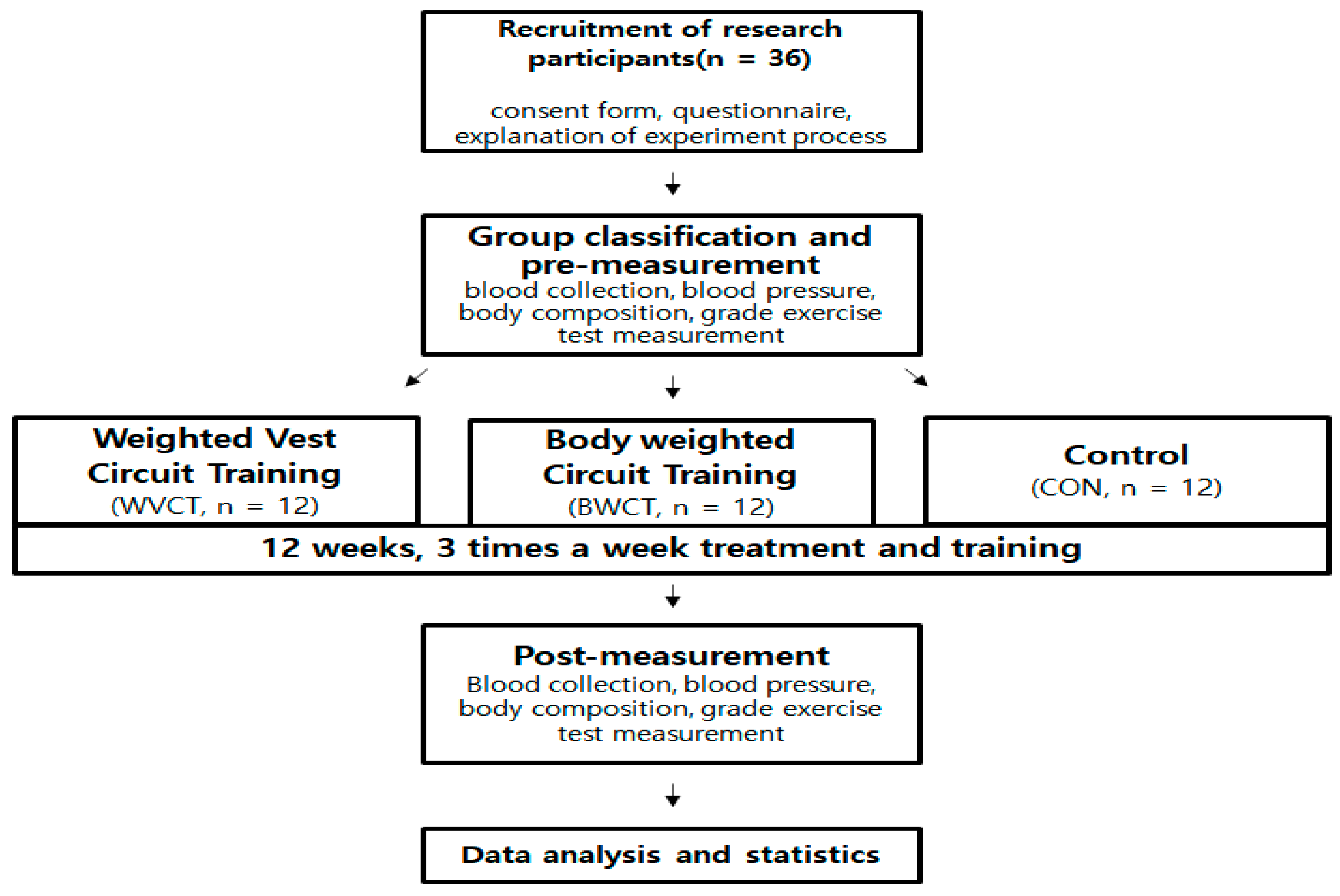
Figure 2.
Training Protocol.
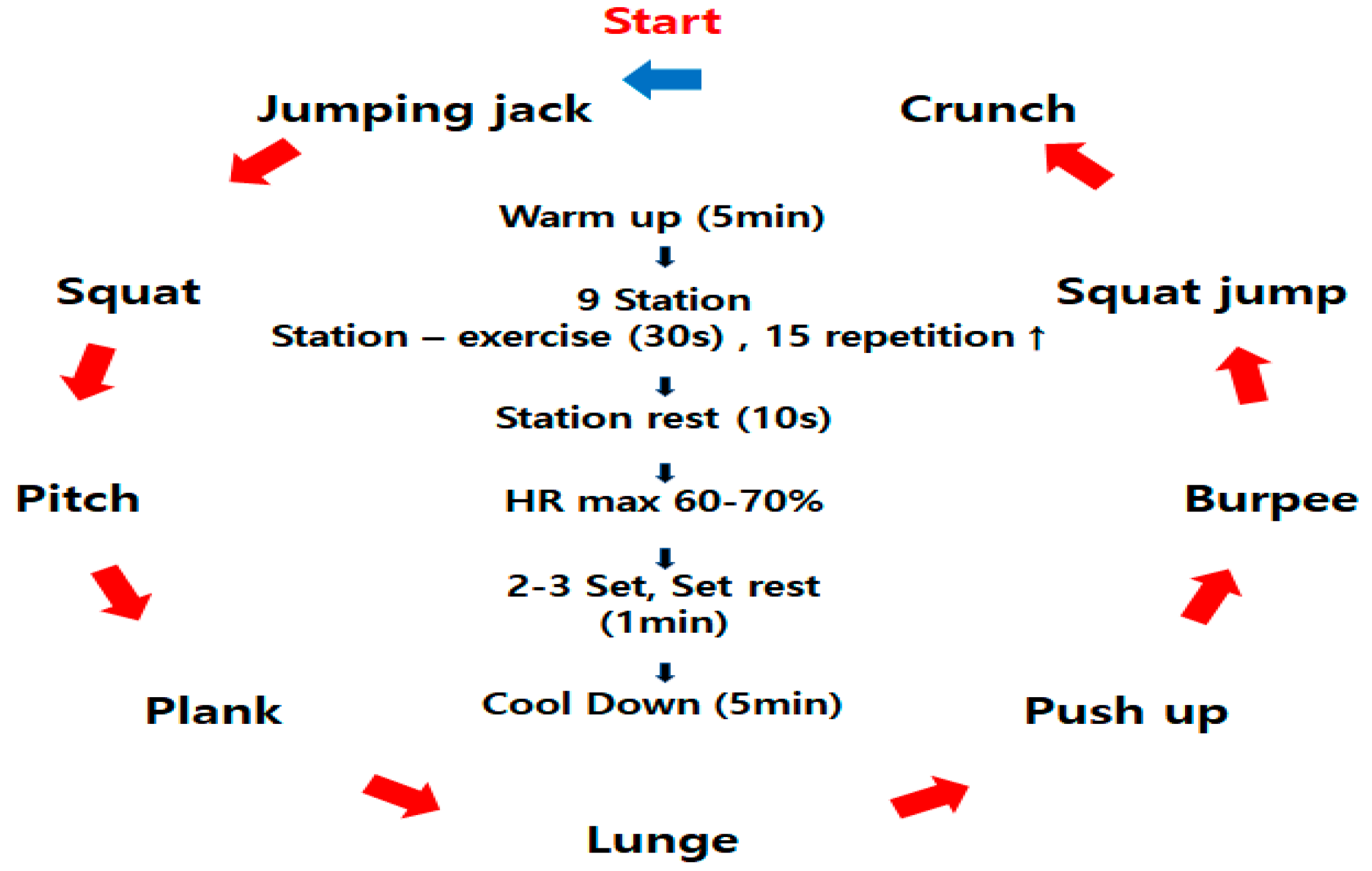
Figure 3.
Changes in Cardiorespiratory Fitness.
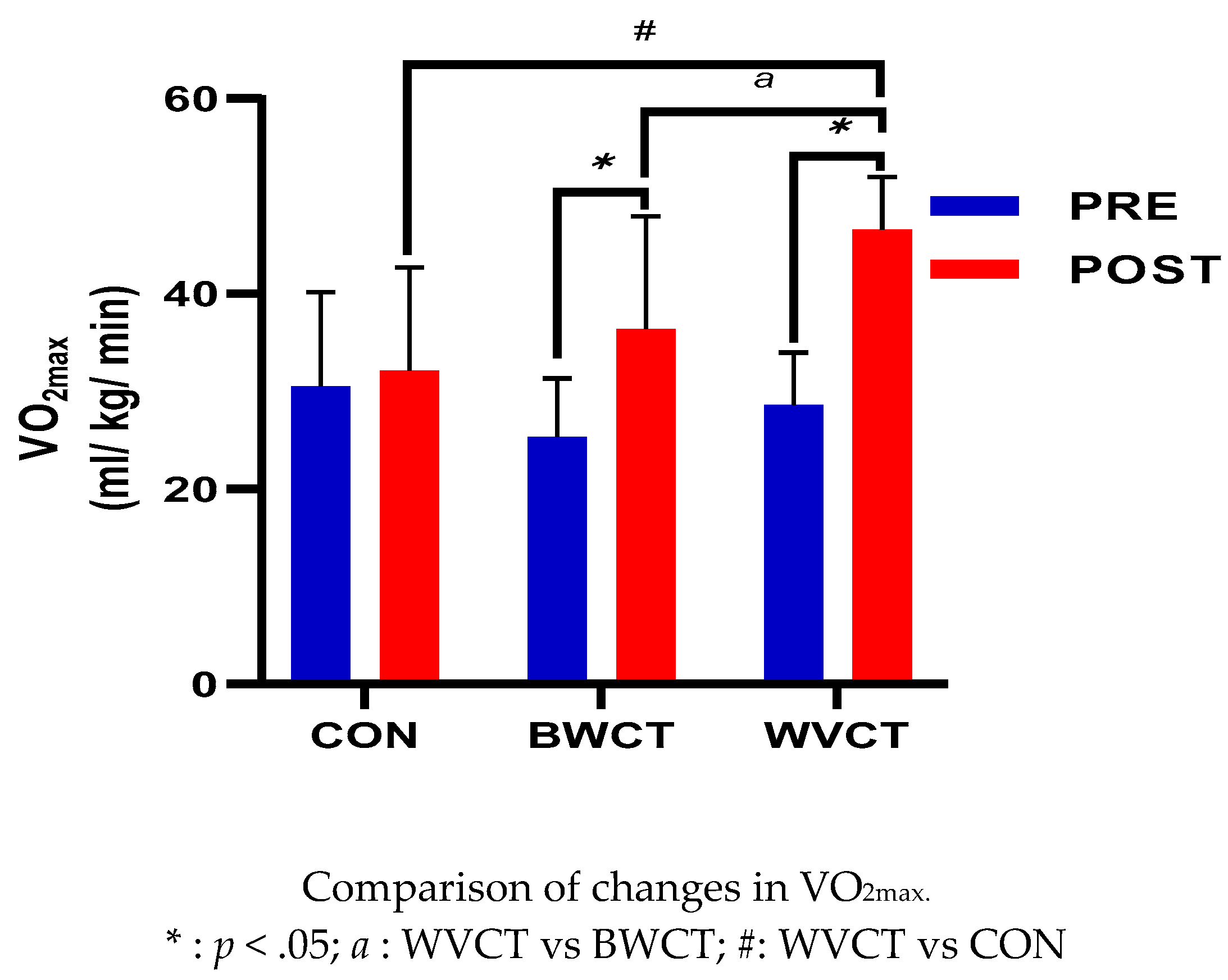
Figure 4.
Changes in Plasma Resistin.
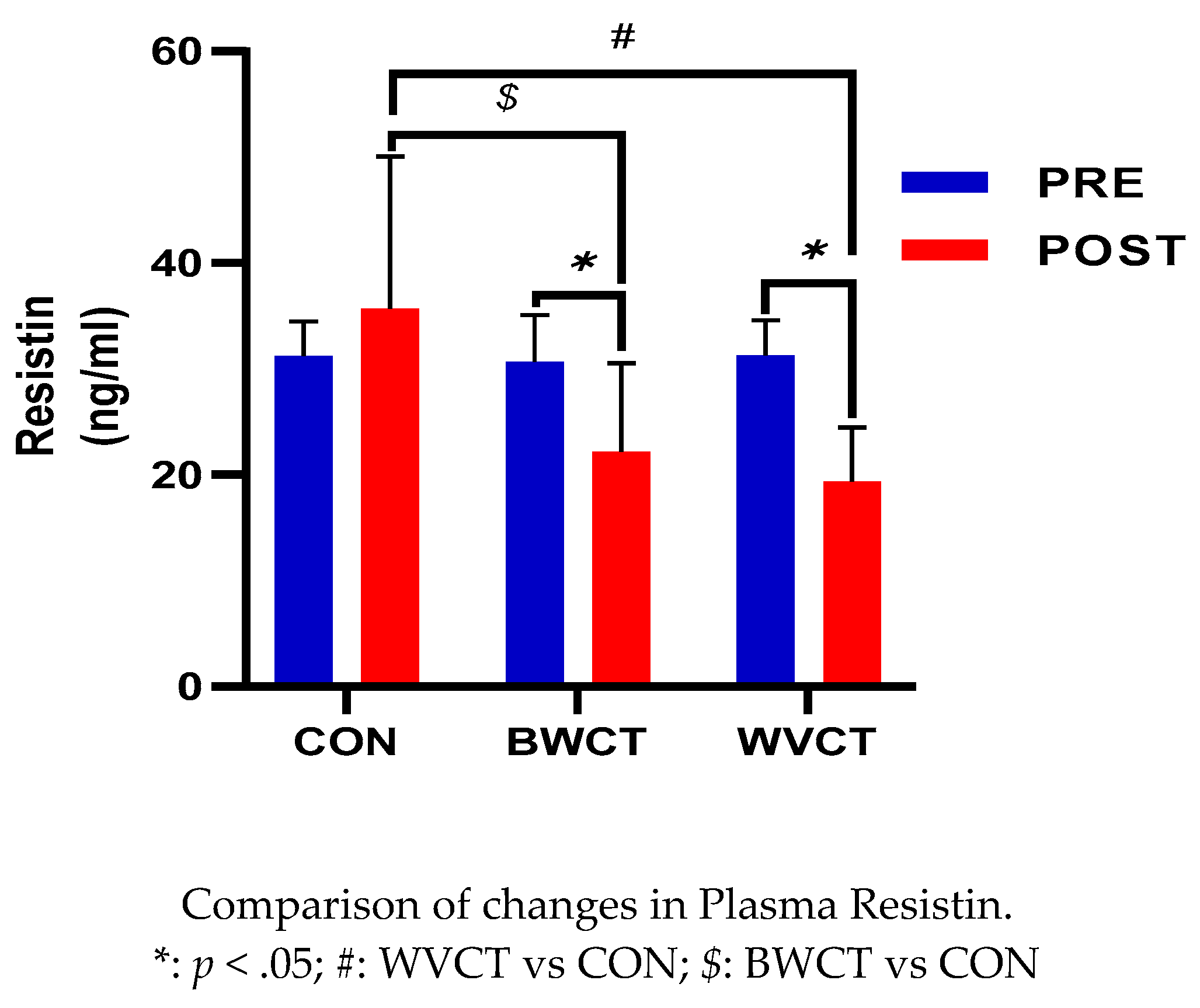

Table 1.
Research participant characteristics.
| Group | CON (n = 12) | BWCT (n = 12) | WVCT (n = 12) | p-value |
|---|---|---|---|---|
| Age (yrs) |
27.00 ± 5.38 | 23.00 ± 2.26 | 24.25 ± 4.27 | ns |
| Height (cm) |
161.10 ± 3.56 | 162.3 ± 6.19 | 162.50 ± 5.85 | ns |
| Body Weight (kg) |
55.18 ± 5.93 | 57.56 ± 6.94 | 57.54 ± 8.41 | ns |
| BMI (kg/m2) |
21.20 ± 1.64 | 21.81 ± 1.76 | 21.73 ± 2.10 | ns |
| Skeletal Muscle Mass (kg) |
20.58 ± 2.07 | 21.15 ± 3.04 | 20.99 ± 2.98 | ns |
| Percent Body Fat (%) |
32.19 ± 1.93 | 32.82 ± 2.25 | 32.53 ± 2.40 | ns |
WVCT : Weighted Vest Circuit Training; BWCT : Body Weighted Circuit Training; CON : Control; Values are mean ± SD; ns: non-significant difference.
Table 2.
Descriptive statistics of Body Composition.
| Variable | CON (n = 12) |
BWCT (n = 12) |
WVCT (n = 12) |
F | p | ||||
|---|---|---|---|---|---|---|---|---|---|
| PRE | POST | PRE | POST | PRE | POST | ||||
| Body Weight (kg) |
56.76 ± 5.93 | 54.55 ± 3.80 | 57.56 ± 6.94 | 56.50 ± 6.26 | 57.54 ± 8.41 | 55.00 ± 7.19 | Time | 9.567 | .028* |
| Group | .361 | .700 | |||||||
| Time × Group | .892 | .419 | |||||||
| BMI (kg/m2) |
21.58 ± 1.64 | 21.02 ± 1.17 | 21.80 ± 1.76 | 21.42 ± 1.58 | 21.73 ± 2.10 | 21.66 ± 2.59 | Time | 1.192 | .283 |
| Group | .379 | .687 | |||||||
| Time × Group | .238 | .789 | |||||||
| Skeletal Muscle Mass(kg) |
20.58 ± 2.07 | 20.25 ± 1.30 | 21.15 ± 3.04 | 21.52 ± 2.42 | 20.99 ± 2.98 | 22.13 ± 2.99 | Time | 3.012 | .092 |
| Group | .733 | 488 | |||||||
| Time × Group | 3.483 | .042* | |||||||
| Percent Body Fat(%) | 32.19 ± 1.93 | 32.29 ± 1.98 | 32.82 ± 2.25 | 30.21 ± 2.08 | 32.53 ± 2.40 | 29.63 ± 2.11 | Time | 38.194 | .000** |
| Group | .377 | .689 | |||||||
| Time × Group | 10.721 | .000** | |||||||
Mean ± SD; * p < .05; ** p < .001.
Table 3.
Descriptive statistics of quantity of Cardiovascular Disease Risk Factors.
| Variable | CON (n=12) |
BWCT (n=12) |
WVCT (n=12) |
F | p | ||||
|---|---|---|---|---|---|---|---|---|---|
| PRE | POST | PRE | POST | PRE | POST | ||||
| IL-6 (pg/ml) |
21.20 ± 3.36 | 19.84 ± 5.95 | 20.03 ± 4.04 | 15.14 ± 4.70 | 19.95 ± 3.98 | 13.30 ± 3.72 | Time | 20.649 | .000** |
| Group | 4.458 | .019* | |||||||
| Time × Group | 2.698 | .082 | |||||||
| TC (mg/dL) |
170.75 ± 31.10 | 172.08 ± 28.60 | 183.08 ± 28.05 | 179.42 ± 30.31 | 189.33 ± 32.96 | 169.75 ± 21.41 | Time | 4.433 | .043* |
| Group | .453 | .639 | |||||||
| Time × Group | 3.303 | .049* | |||||||
| LDL-C (mg/dL) |
99.92 ± 28.15 | 101.92 ± 27.93 | 111.33 ± 17.41 | 109.33 ± 13.12 | 109.67 ± 30.69 | 87.75 ± 22.66 | Time | 5.816 | .022* |
| Group | .913 | .411 | |||||||
| Time × Group | 5.962 | .006* | |||||||
| HDL-C (mg/dL) |
61.92 ± 5.92 | 57.33 ± 5.12 | 62.75 ± 16.81 | 59.50 ± 11.55 | 66.25 ± 10.23 | 68.25 ± 8.58 | Time | 1.807 | .188 |
| Group | 2.166 | .131 | |||||||
| Time × Group | 1.930 | .161 | |||||||
| SBP (mmHg) |
112.17 ± 9.73 | 111.33 ± 10.82 | 113.42 ± 9.69 | 111 ± 8.28 | 104.92 ± 11.97 | 101.42 ± 7.42 | Time | 1.577 | .218 |
| Group | 4.679 | .016* | |||||||
| Time × Group | .187 | .831 | |||||||
| DBP (mmHg) |
72.58 ± 3.68 | 76.14 ± 6.63 | 71.75 ± 6.87 | 73.50 ± 5.84 | 70.75 ± 6.40 | 72.58 ± 5.98 | Time | 2.393 | .131 |
| Group | 1.565 | .224 | |||||||
| Time × Group | .150 | .861 | |||||||
Mean ± SD; * p < .05; ** p < .001; TC: Total Cholesterol; SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



