
Submitted:
21 August 2023
Posted:
22 August 2023
You are already at the latest version
Abstract
Surgical knots are sequences of half-knots (H) or half-hitches (S), defined by their number of throws, by an opposite or similar rotation compared with the previous one and for half-hitches, whether sliding (s) or blocking (b). Opposite rotation results in (more secure) symmetric (s) knots, similar rotation in asymmetric (a) knots, and changing active and passive ends has the same effect as changing rotation. Loop security is the force to keep tissue together after a first half-knot or sliding half-hitches. With polyfilament sutures H2, H3, SSs and SSsSsSs have a loop security of 10, 18, 28 and 48 Newton (N), respectively. With monofilament sutures, they are only 7, 16, 18 and 25N. Since many knots can reorganise, the definition of knot security as the force at which the knot opens or the suture breaks should be replaced by the clinically more relevant percentage of clinically dangerous and insecure knots. Secure knots with polyfilament sutures require a minimum of 4 or 5 throws, but the risk of destabilisation is high. With monofilament sutures, only 2 symmetric+4 asymmetric blocking half-hitches are secure. In conclusion, half-hitch sequences are recommended since mandatory for monofilament sutures, adding flexibility for loop security with less risk of destabilisation.
Keywords:
knot sequences
; half-knot
; half-hitch
; knot rotation
; knot security
; loop security
; laparoscopic surgery
; gynaecology.
1. Introduction
Suturing and knot-tying are essential skills in surgery. The choice of the suture material and knots was based on common sense until the loop and knot securities were measured with a dynamometer [1].
Understanding loop and knot security is important for the laparoscopic surgeon who cannot use two-hand knot tying for loop security as done in open surgery. Knowledge of loop and knot stability permits the surgeon to choose the most appropriate suture and knot combination, and secure knots allow using thinner sutures and cutting the tails shorter with less postoperative adhesion formation. More importantly, secure knots will prevent postoperative complications by knots opening inadvertently or not being leakproof after sealing a vessel. Since still poorly documented [2,3,4], we planned to review what is known about loop and knot security in laparoscopic gynaecological suturing.
2. Materials and Methods
Pubmed was searched for ("2000/01/01"[Date - Publication]: "2023/08/01"[Date - Publication]) AND knot[Title] AND surgery AND English [Language] NOT (orthopaedic OR orthopedic) NOT video NOT Gordian. The titles of the 544 articles found were screened, and the PDFs or, if not available, the abstract of the 53 articles retained were reviewed. Finally, only 37 articles were found to be useful. A subsequent search of 'knot security'[Title/Abstract] NOT orthopaedics NOT education NOT learning found 144 articles, and after screening and checking, two more articles were included. The review was submitted to Prospero with ID 450731.
Only suture diameters between 2.0 and 1 are discussed. Only one article reported larger [5] sutures, but without changing the message.
3. Definitions and the basics of knot tying
3.1. Knots are sequences of half-knots and half-hitches
In surgery, most knots (for an overview [6]) are sequences of half-hitches (S) or half-knots (H) (Figure 1) Half-hitches result from pulling one end of the suture, called the passive end. Half-knots (H) require symmetrical pulling of both ends. Half-knots are easily converted into half-hitches and vice-versa.
Half-hitches usually consist of 1-throw and half-knots of 1 to 3 throws.
Besides the number of throws [7], rotation is essential. Compared to the previous one, alternate rotation of the same active end improves clinically§ knot security [7,8,9,10,11]. Half-knot sequences with alternate rotation result in a flat square knot, visually recognised as symmetrical [8]. Half-hitch sequences with opposite rotation stronger squeeze the passive end, and both ends stay on the same side. Similar rotation generally results in less secure knots, with the poor granny knot resulting from two 1-throw similar rotation half-knots, as an example.
3.2. Nomenclature of knots and historical perspective
The terminology or nomenclature of half-knots was described in 1976 [16] and of half-hitches in 1984 [11] (Table 1). Half-knots were indicated as 'H' and half-hitches as 'S' since sliding, followed by the number of throws. For subsequent half-knots or half-hitches, the rotation compared to the previous one was indicated by an '=' of 'x' to indicate a symmetric or asymmetric knot sequence. This terminology felt confusing since '=' is often called 'similar' without specifying that it means an alternate rotation resulting in a symmetric knot and not a similar rotation. For half-hitches, blocking was indicated by //[17].
To avoid ambiguity, we prefer to emphasise rotation since this is what the surgeon does when tying knots. [7,8,18]. It is intuitive for the surgeon who has to decide the number of throws and the sense of rotation for each half-knot or half-hitch. Therefore, the H or S is followed by the number of throws and the knot structure, which can be symmetric 's' or asymmetric 'a', when rotation of the same active thread compared to the previous one had been alternate or similar. For half-hitches, an 's' is added for sliding and a 'b' for blocking after changing active and passive ends. It should be clear that a second sliding half-hitch made with similar rotation, or SSas, can be changed into a blocking half-hitch, or SSab, by pulling the active end. However, it should be equally clear that changing the active and passive ends has the same effect as changing rotation and that SSab thus indicates a symmetric half-hitch on the new active end. However, for the surgeon, the rules are straightforward: always use alternate rotation for half-knots and sliding half-hitches. Only for blocking half-hitches similar rotation is used. This terminology can be simplified by omitting the number of throws if one and the 's' of sliding to avoid confusion with the (s) of symmetric. The surgeon also should realise the difference between mono-manual and bimanual suturing since similar rotation results in symmetric knots after changing the active and passive ends. Half-hitches remain sliding as long as the passive end remains the same. However, reorganisation might block some sequences when 6 or more half-hitch sequences are used. To summarise, SSsSsbSab indicates a second symmetrical and sliding, a third symmetrical (alternate rotation) and blocking and a fourth asymmetrical (similar rotation) and blocking half-hitch.
3.3. Testing and definitions of loop and knot security
Security of knots is mostly evaluated with a dynamometer increasing forces at a constant speed and measuring the force when a suture breaks or slides open. Dynamic testing of security will not be discussed since not yet useful in gynaecology.
Loop security or holding strength is the first aspect to consider when suturing [19]. This is the force needed to open the first loop, which can be the first half-knot, one or more sliding half-hitches, a sliding granny knot [20], or a cinch knot. Loop security keeps the tissues approximated or sutured arteries leakproof until additional half-knots or half-hitches are added, securing the knot. Loop security, thus, is essential for making tight knots. The importance of inadequate loop security is illustrated by the incidences of postoperative bleeding, which was reported as high as 4% to 10% after hysterectomy in animals [21].
The definition of knot security is variable. Knot security is mostly described as the mean force to slide open the final knot or break the suture. Another definition is the percentage of knots sliding open. A third definition is the percentage of dangerous and insecure knots. Based on clinical experience, these were defined in abdominal and gynecologic surgery as opening with less than 10N and between 10 and 30 Nexton, respectively. However, the values of insecure and dangerous knots might be much higher for knots on the abdominal fascia or when fixing a mesh to the promontory, especially during coughing. A fourth definition is the percentage of knots sliding for over 3mm before blocking and breaking the suture. This sliding reflects reorganisation when force is applied, but instead of reorganising into opening the knot, the knot 3-D structure blocks and the suture breaks. This sliding for a few mm is important for sealing vessels leakproof and in orthopaedic surgery requiring tight knots. Although not investigated in gynecologic surgery, the importance today seems to be limited to not cutting sutures shorter than 3mm. Besides these definitions, knot security after being soaked in water for some time [22] can differ slightly from dry sutures.
4. Understanding knot and loop security
4.1. Loop security
Although not measured precisely, loop security can be handled in open surgery by correct two hands knot tying, with constant tension on both suture ends [23,24]. In laparoscopic surgery, loop security only varies with the friction characteristics of the suture in the tissue and in the knot, reflecting the 3-D geometry in the knot (for mathematical models [23]).
The forces needed in abdominal surgery and gynaecology for loop security have not been documented. The only guidance is clinical experience [25], and we (the authors) estimate that the approximation of the abdominal fascia following a laparotomy or the approximation of the myometrium following a myomectomy requires loop security between 30 to 50 Newton (N). Loop security is not an issue for promontofixation since knots are secured without tension. Loop security for pulsatile arteries has not been measured. The need for much higher loop security forces in orthopaedic surgery have stimulated the development of cinch knots, or knots sliding on the passive end, that can be blocked by reorganisation by traction on the active end. These will not be discussed, being a different class of knots with unclear importance in gynaecological surgery.
Besides the friction forces of the suture in the tissue, loop security varies with the friction forces of the suture in the knot, varying with the number of throws and the 3D geometry.
For polyfilament sutures, such as polyglactin 2-0 (Vicryl), loop security of half-knots increases with the number of throws being 6, 10 and 18 Newton, for an H1, H2 or H3, respectively [7]. Loop security of symmetrical half-hitch sequences is twice as high as asymmetrical sequences [15,26] and increases with the number of half-hitches, being 24 and 48N for 2 and 4 symmetric (alternate rotation) half-hitches [13]. Although forces were not measured, the unstable granny knot (H1H1a) and H2H1a can be used to secure veins [27] or for wound closure [20].
For monofilament sutures, such as polyglecaprone 2.0 (Monocryl), loop security is lower than for Polyfilament sutures. Loop security of half-knots was 3 and 15 N for two and three throw half-knots. For half-hitch sequences, loop security was 15 N and 28 N for SSsand SSsSsSs and did not improve when 6 half-hitches were used (SSsSsSsSsSs) or 2 half-knots as H1H1s [28].
Figure 2.
Loop security of polifilament (Vicryl) and monofilament (Monocryl) sutures. Mean and SD’s are indicated. Constructed from [7].
Figure 2.
Loop security of polifilament (Vicryl) and monofilament (Monocryl) sutures. Mean and SD’s are indicated. Constructed from [7].
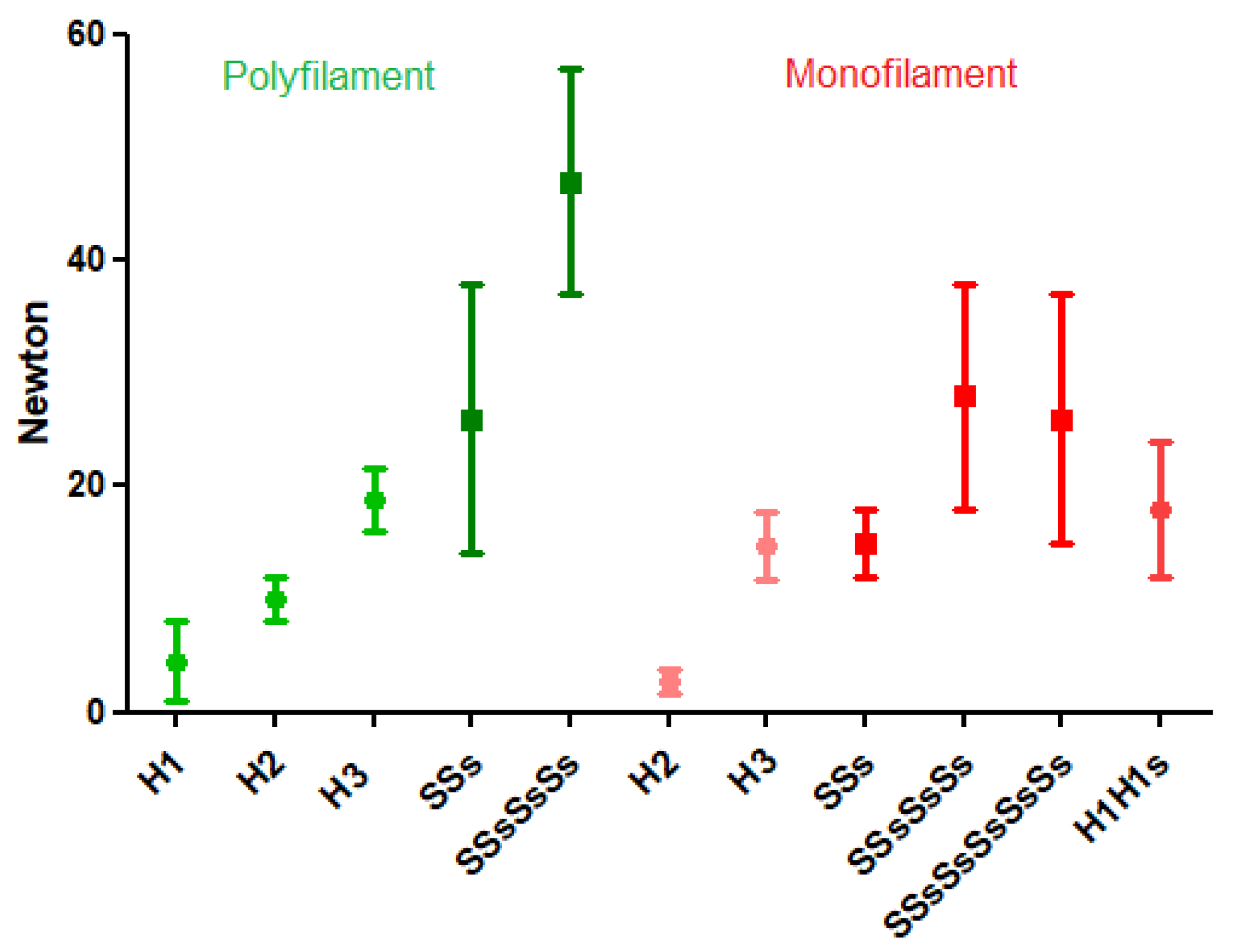
Figure 4 shows the variability of the loop security of half-hitch sequences, indicated by the large standard deviations caused by differences in forces of tying and duration of time till tested. Only recently, the surgical flexibility of half-hitch sequences was realised. If the loop security of 2 symmetrical half-hitches (SSs) is insufficient to keep tissues with stronger opening traction approximated as can occur when closing a myomectomy, a third and eventually a fourth half-hitch can be added. In addition, the last or fourth half-hitch can be transformed into a blocking half-hitch by quickly pulling the active end. If the surgeon anticipates this, the fourth half-hitch is preferably asymmetric, made by similar rotation.
The loop security of cinch knots [29,30], although overall much higher than for sliding half-knots or half-hitches, will not be discussed since rarely needed in gynaecological surgery. Cinch knots are still under active development to find the best balance between a less complicated knot, high loop security, and how to secure the knot afterwards. Also, the superiority of Millers knot [31,32] or constrictor knot [33] for sealing vessels leakproof will not be discussed.
Figure 2.
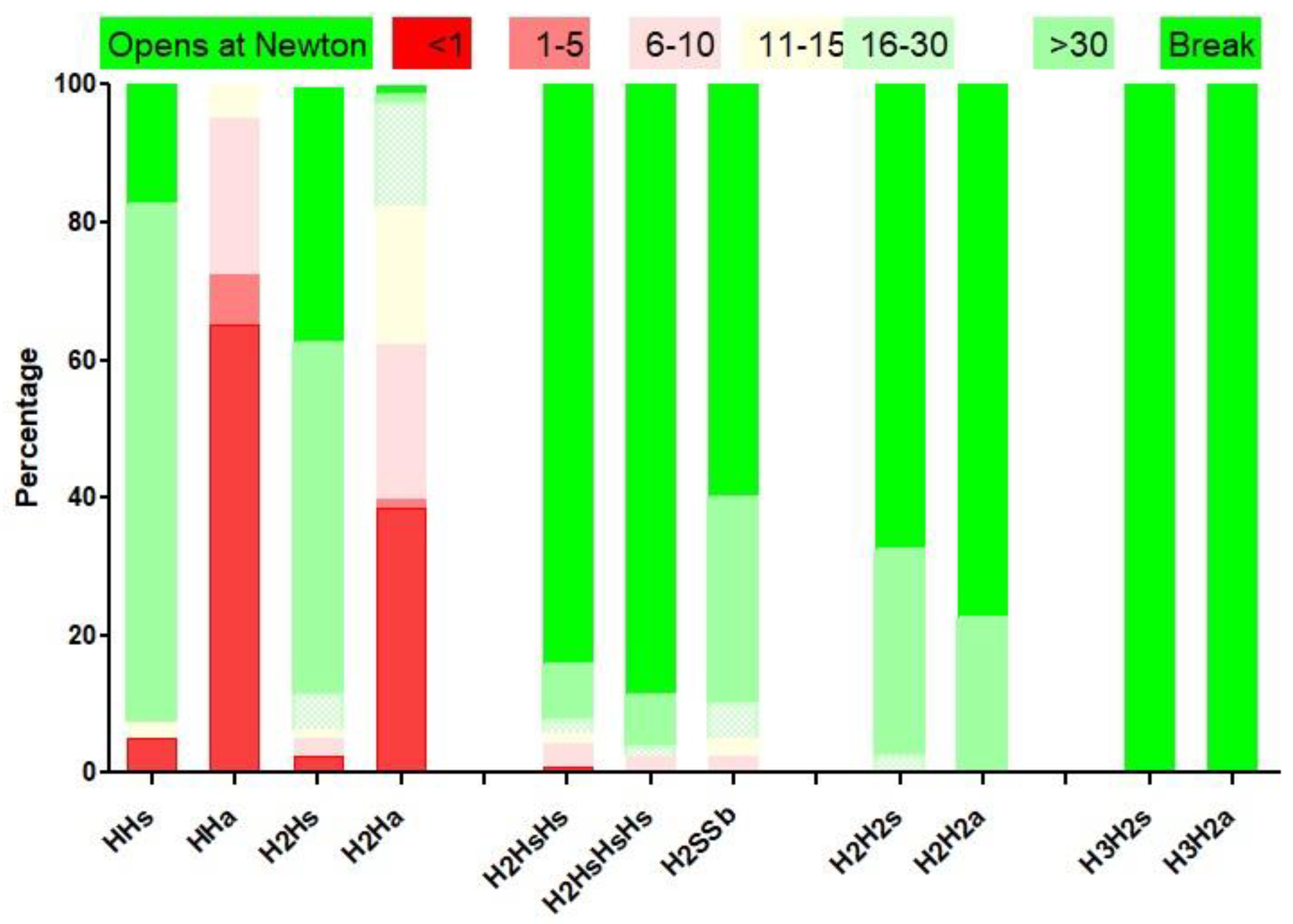
Half-knots security, defined as the percentage of dangerous knots, opening at less than 10N, and of insecure knots that open between 10 and 30N. Constructed from [7].
Figure 2.
Half-knots security, defined as the percentage of dangerous knots, opening at less than 10N, and of insecure knots that open between 10 and 30N. Constructed from [7].
4.2. Knot security
Knot security varies with the type and diameter of the suture, the knot configuration or sequences and rotation of the half-knots or half-hitches, and the number of throws [2,7,13,34]. Knot security is generally slightly lower than the breaking forces of the tread, the knot being the weakest point of a suture [4,7]. This lower breaking force is believed to be caused by angulation forces in the knot. Knot security in vivo can be slightly less because of the wet environment and resorption. Knot security is believed to decrease exponentially over time, halving every 20 days. These considerations are not clinically relevant, considering tissue repair results in 50% of its final strength within a week. Knot security is for most knots occasionally variable because of reorganisation [7,35,36]. Therefore tradional statistics using the mean and standard deviations, are not adequate to evaluate the mean forces breaking or opening the suture. For most knots some slide open with lower forces up to becoming insecure knots when opening between 10 and 30N. Occasionally, knots can open at much lower forces below 10N and are considered dangerous knots. This unpredictable behaviour is explained by the reorganisation of knots when forces are applied during tying the knot or when tissue forces try to open the knot. The consequence of reorganisation is evident when an H1H1s is transformed into a sliding SSs. The reorganisation is also illustrated by the very different reorganisation of a double-throw half-knot followed by a symmetric or asymmetric double-throw half-knot (Figure 3). Clinically reorganisation is unpredictable if the first half-knot is slightly destabilised by insufficient loop security, inadvertent traction when making the second half-knot, or asymmetric traction when tying the second half-knot. Unpredictable reorganisation resulted for the excellent surgical knot (H2H1sH1s) in more than 5% insecure knots and 5% dangerous knots [7].
Figure 3.
Rotation changes knot reorganisation. The symmetric knot remains in 1 plane. The asymmetric knot is in 2 perpendicular planes. From [7].
Figure 3.
Rotation changes knot reorganisation. The symmetric knot remains in 1 plane. The asymmetric knot is in 2 perpendicular planes. From [7].
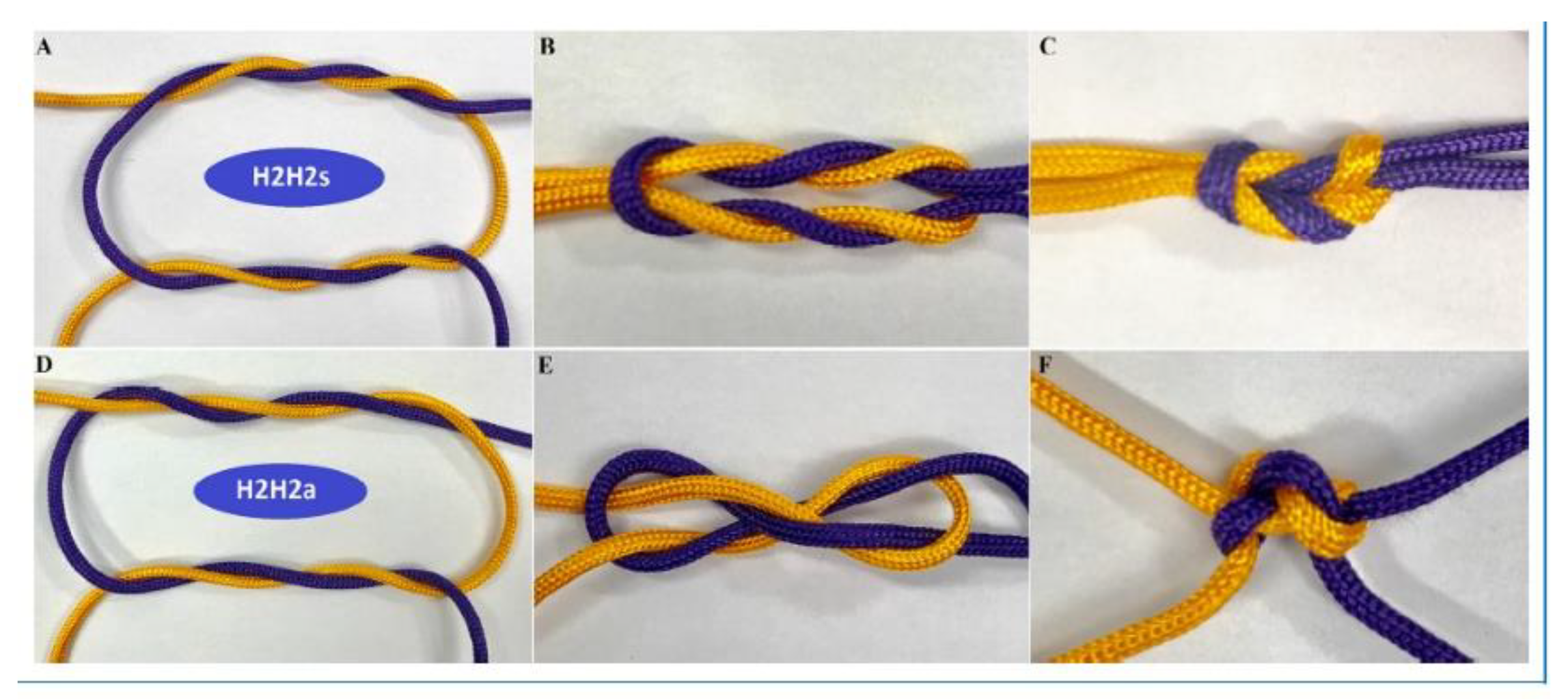
Figure 4.
Knot security and number of throws. From [7] with permission.
Figure 4.
Knot security and number of throws. From [7] with permission.
Clinically the (occasional) risk of insecure or dangerous knots is more important than the mean breaking force of a knot. This variability of knot security is caused by the reorganisation of the knot sequences when forces are applied. Equally important is the surgeon who ties the knot. He ties each half-knot or half-hitch with a specific force and maintains this force for a variable time. This introduces the poorly explored memory of the suture or knot as an additional variable. His skills are fundamental for not increasing the risk of accidentally destabilising a half-knot when making or tying the second half-knot. Also, his training and understanding of knot security are necessary since training and the mental 3-D understanding of a knot structure improve knot tying. An indirect argument is that the relatively high frequency of insecure and dangerous knots, observed in 2018 [7], disappeared progressively with the awareness of the risk of destabilisation, the importance of precision in forces used, and the duration of force and suture memory.
Unfortunately, for a risk of a few per cent insecure or dangerous knots, a high number of knots has to be tested. Using a Poisson approximation, 40 and 120 knots will detect 5% abnormality with 95% confidence intervals of 0.6% to 18.0% and 1.8% to 10.9%, respectively [37].
Knot security varies with the number of throws, the rotation and sequences of half-knots or half-hitches, the force of tying [8,38], and the type and diameter of suture used. [4,7].
For polyfilament sutures, secure knots require 5 throws, whether defined as the percentage opening [4,7,39] or as the percentage insecure and dangerous knots [7]. Knot security, defined as breaking forces, obviously increases with suture diameter. However, security also improves with rotation, with symmetric knots made by alternate rotation being more secure [15]. For example, the asymmetric granny knots (H1H1a) and even the H2H1a [20] are so unstable that they can be considered sliding knots with monofilament sutures. Secure half-knot sequences require 4 or 5 throws, and only H2H2 and H3H2 sequences are secure without insecure or dangerous knots. Rotation is clinically unimportant for these complex knots, although asymmetrical sequences have a slightly higher breaking force than symmetrical ones. Surprisingly, the surgical knot (H2H1sH1s) was published as dangerous in 5% and insecure in 15%. However, this was subsequently understood as the risk of destabilising the first loop by little involuntary traction on one of the ends when making or tying the subsequent half-knots: an H1H1 easily transforms into an S1S1, and an H2H1 into a sliding S2S1, irrespective of rotation. This risk increases with the surgeon's inexperience when threads are short and knot-tying is difficult because of location.
Secure sequences of half-hitches require at least 2 symmetrical sliding and 2 or preferably 3 asymmetrical blocking half-hitches for polyfilament sutures. Monofilament sutures require at least 6 half-hitches, 2 symmetrical sliding and 4 asymmetrical blocking [28].
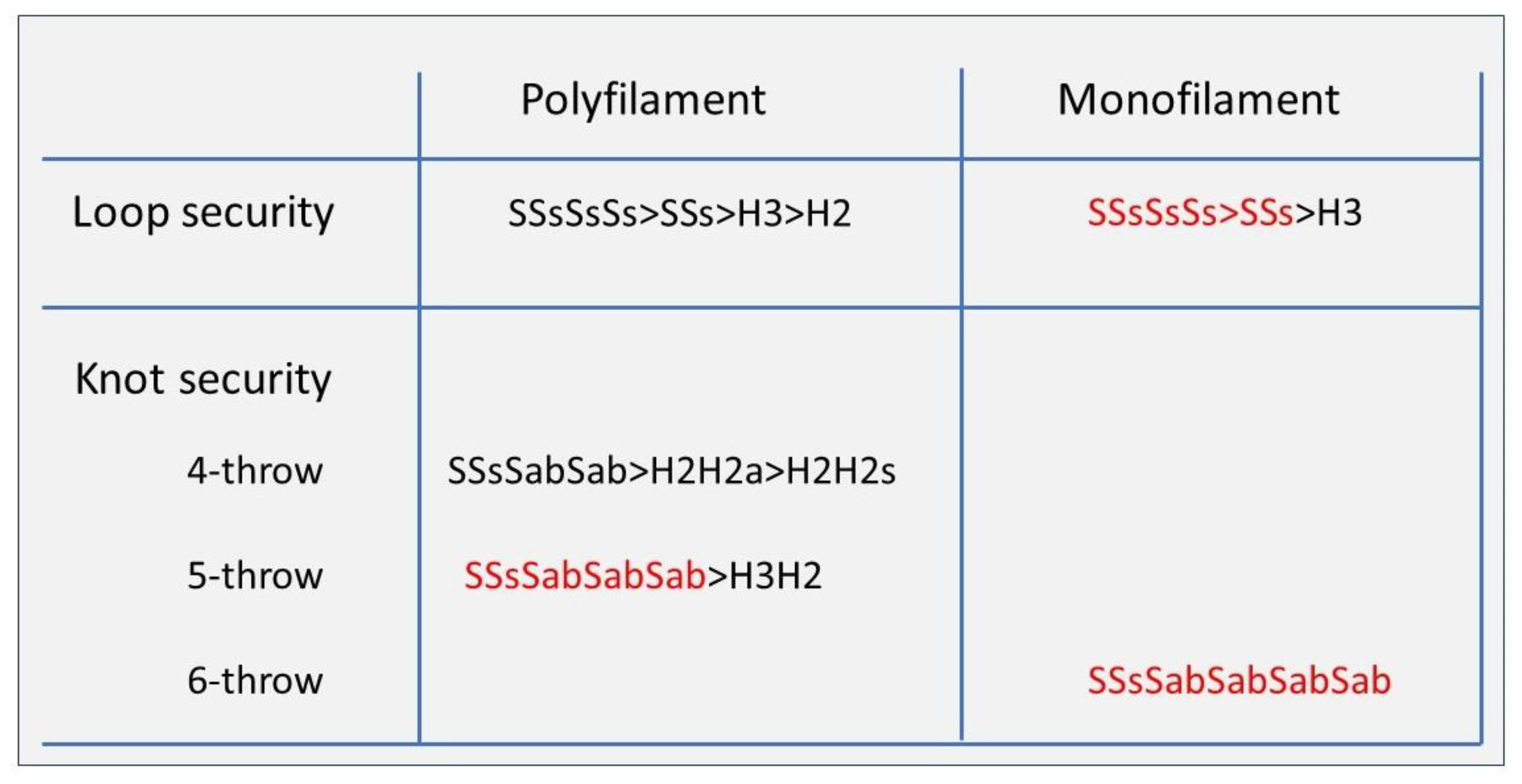
Figure 5.
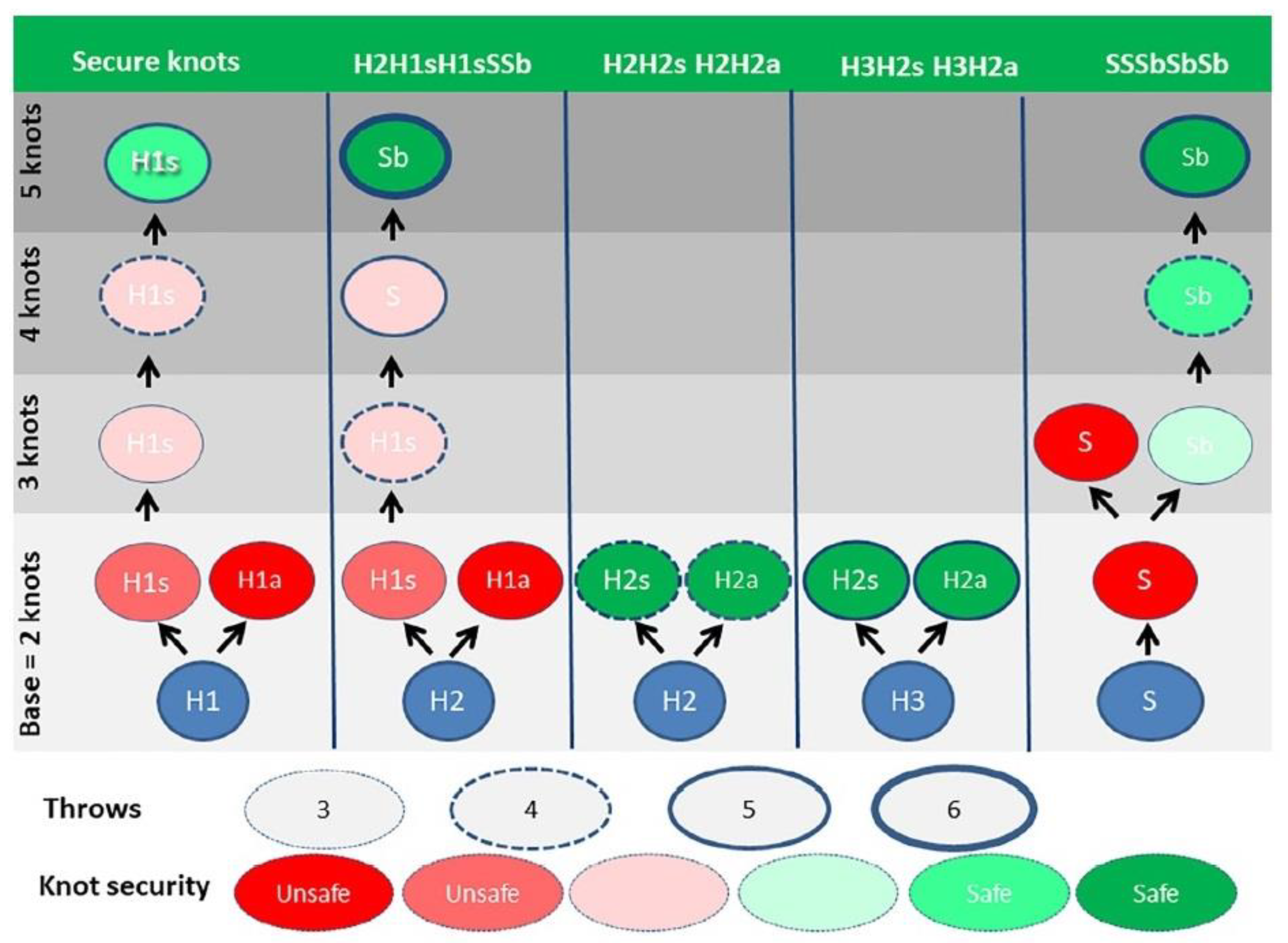
Which knos to use in laparoscopical gynaecological surgery. Secure knots are indicated in black, more secure or preferred knot sequences knots in red.
Figure 5.
Which knos to use in laparoscopical gynaecological surgery. Secure knots are indicated in black, more secure or preferred knot sequences knots in red.
5. Which knots to use in laparoscopic surgery
5.1. Considering loop security
Estimating that loop security of more than 15N is rarely required in laparoscopic gynaecological suturing, an H3, H1H1a and SSs are acceptable choices for polyfilament sutures. However, with monofilament sutures, loop security of these sliding knots and of H1H1s (which easily transforms into SSs might be insufficient. Therefore, we suggest using symmetric half-hitch sequences permitting a third and a fourth half-hitch, eventually blocking if needed. A first double throw half knot should be avoided, especially with monofilament sutures.
5.2. Considering knot security
Secure knots require a minimum of 5 throws for polyfilament and 6 throws for monofilament sutures and correct rotation, which is alternate rotation of the same active end or similar rotation if active and passive ends are changed.
Knot reorganisation during traction can result in an unpredictable, insecure or dangerous knot opening with forces of less than 10N. The risk for this unpredictable behaviour increases when the first loop is destabilised because of insufficient loop security or involuntary asymmetric traction on the first half-knot when less experienced or when sutures are short when making or tying the second half-knot. Therefore, as a general rule, we suggest avoiding starting with a double-throw half-knot, especially with monofilament sutures. Replacing half-knot sequences with half-hitch sequences is always advantageous because of higher loop security, more flexibility for loop security if needed and better or at least equal knot security. This holds for all 4, 5 and 6 throw knots. For most surgeons, this feels counter-intuitive since the surgeon’s knot (H2H1sH1s), and the H2H2 and H3H2, symmetric or asymmetric, are excellent knots.
Secure sequences of half-hitches require at least 2 symmetrical sliding and 2 or preferably 3 asymmetrical blocking half-hitches for polyfilament sutures. Monofilament sutures require at least 6 half-hitches, 2 symmetrical sliding and 4 asymmetrical blocking [28].
With our knowledge of today, knots as 5 sequential half-knots only have historical significance by demonstrating that a 2-throw half-knot followed by 3, 1-throw half-knots is slightly superior [4].
5.3. Knots and postoperative adhesion formation
Abdominal surgery is frequently associated with postoperative adhesion formation in men and women. Postoperative adhesions are a clinical burden for the patient and society since they cause 30% of postoperative pain, 30% of infertility and nearly 100% of postoperative bowel obstructions. Peritoneal repair is typically completed within three days, but adhesion formation will occur if repair is delayed by inflammation or a foreign body. Therefore suture material needing to be resorbed over more than a week is always adhesiogenic. Postoperative Adhesions thus increase with the duration of resorption, the suture characteristics, the length of the remaining tails and the volume of the knot (for review [40]), and thus with the diameter of sutures and the number of throws and half-hitches or half-knots.
Therefore, we wanted to review what is known about loop security since important in laparoscopic surgery and knot security. Knot security will permit the surgeon to choose the most appropriate knot and a thin suture with a low knot volume and to cut tails short.
6. Discussion
In open surgery, loop security was taken care of with two-hand suturing permitting constant traction of both ends. In laparoscopic surgery, the importance of loop security only became fully realised with the development of laparoscopy in orthopaedic surgery [41], requiring high loop security and tight knots. This has led to the development of a series of sliding cinch knots [42] that can be blocked when in place and subsequently secured with additional half-knots of hitches. Loop security is important for suturing vessels larger than > 5mm leakproof, introducing surgeon's throw, millers knot, and strangle knots [43], and even this year, an H3 was suggested to initiate an inverted mattress suture in dermatology [44].
In gynecologic laparoscopic surgery, loop security has received little attention since a high loop security is rarely necessary. However, when needed, such as after a large myoma resection, the surgeon should know that monofilament sutures should be avoided and that for polyfilament sutures, an H3 or better 2 symmetric half-hitches made with alternative rotation should be used. Especially for monofilament sutures, half-hitch sequences have the advantage of being flexible by permitting a third sliding and a fourth sliding half-hitch to be transformed after tying into a securing blocking Half-hitch, if needed.
Knot security should be defined by the risk of dangerous or insecure knots, not by the mean breaking forces of the knot. Therefore the clinical importance of most publications based on mean opening forces of knots can be questioned. Today's evidence can be summarised as follows: symmetric sequences are overall superior, and knot security increases with the number of throws, requiring 4 or 5 for polyfilament sutures and 6 or more throws of monofilament sutures. With polyfilament sutures, secure half-knot sequences are the 4-throw H2H2, the 5-throw H3H2 irrespective of rotation, and the surgical knot (H2H1sH1s). However, with monofilament sutures, these half-knot sequences are often insecure, and security does not improve by adding one or more half-knots. Only Half-hitch sequences are secure, provided at least 4 asymmetrical (symmetric on the new passive tread) are used. This indirectly confirms the difference in behaviour of monofilament sutures [3]. Considering the risk of reorganisation and variability of half-knots, 5 asymmetrical half-hitches seem a safer option.
This translates into a clear message for the surgeon: always use alternate rotation except for blocking half-hitches. Experienced surgeons can consider H2H2 and H3H2, irrespective of rotation, provided the first loop is not destabilised and has enough security. Half-hitch sequences are superior, especially in gynaecology, with often suturing deep in the pelvis, since the loop security is way superior to half-knots, and because of the benefit of flexibility, permitting a third and eventually a fourth half-hitch, eventually to be transformed into a blocking half-hitch, ff 2 half-hitches do not have sufficient loop security to keep the edges of the tissues approximated.
Variable knot security because of reorganisation and destabilisation is an insufficiently recognised but serious problem, requiring training, teaching and individual monitoring. Considering that more than 50 knots need to be evaluated to detect 5% unstable knots, a personal assessment of the knots made by a trainee seems mandatory. As already suggested in 1993 [45], a simple spring portable tensiometer would be welcomed to permit the trainee to check the security of their knots. Another approach is pre-training of laparoscopic psychomotor kills [46], visual force feedback [47], and the use of a knot-tying board with measurement of the vertical and lateral forces exerted [48]. Also noteworthy is the importance that a trainer cannot be replaced by a video [49], that telementoring and training on-site are equally effective [50], that video registration and artificial intelligence can help in the evaluation of trainees [51], and the importance of the mental image of knots [52] and of fatigue [53]. Ideally, a surgeon should demonstrate minimal skills and knowledge before operating on women, and a structural pre-training [38] and assessing knot security of 50 to 100 knots with a dynamometer might be a straightforward and reproducible way to evaluate this.
Understanding loop and knot security is also important for training, and expert instruction presents an advantage compared with video-based self-study [49].
Understanding suturing and knot tying are important for loop and knot security and postoperative adhesion formation. Understanding knot security permits using thinner sutures without excessive throws of half-hitches or half-knots out of prudence, and cutting threads shorter results in less adhesion formation. Since 2.0 sutures already have tensile strengths around 80 to 100 Newton, larger diameters are rarely needed in gynaecology. Although exact data of forces during coughing are not available, we only can conclude that for securing the mesh to the promontory during promontofixation, sutures with a higher tensile strength might be indicated.
These conclusions are consistent with, but change our understanding of, previous reports. Since the importance of rotation for blocking half-hitches was not clear, it is not surprising that it was concluded that six throws are needed [17,39]. We also begin to understand reports that multiplying sequences of half-knots does not lead to more secure knots, as demonstrated that 4 throw half-knots (H1H1sH1sH1s) [4] with PDS opened in 10%, and suggestions to use 5 and 6 throw half-knots such as H2H1sH1sH1s and H3H2sH1sH1s. [22].
The resorption of sutures is estimated to decrease tensile strength by half over three weeks [54,55]. This is not a concern considering that a tissue repair has 50% of its final resistance after 1 week.
A discussion of modifications and improvements of barbed sutures and of cinch knots, being too complex for intracorporeal suturing [14] is beyond this review since.
7. Conclusions
In laparoscopic gynaecological surgery, loop security is more important for holding tissues together until the knot is secured than in open surgery, permitting 2 hand knot-tying with constant traction on the sutures. Loop security of half-knots is low, resulting in many being accidentally transformed into half-hitches with the risk of changing half-knot sequences in sliding half-hitch sequences.
Knots with a very high loop and knot security, as required in ortopedic surgery, are not reviewed. These knots invariably start with a cinch knot reinforced by a series of half-knots or half-hitches, up to Double-stranded knot configurations with a loop on one side [56,57] such as the racking hitch knot [58], TSOL knots [59] and Strangler knots.
References
- Trimbos, J.B.; Klopper, P.J. Knot security of synthetic absorbable suture material; a comparison of polyglycolic acid and polyglactin-910. Eur J Obstet Gynecol Reprod Biol 1985, 19, 183–190. [Google Scholar] [PubMed]
- Wong, Y.R.; McGrouther, D.A. Biomechanics of surgical knot security: a systematic review. Int J Surg 2023, 109, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Taysi, A.E.; Taysi, N.M.; Sismanoglu, S. Does Knot Configuration Improve Tensile Characteristics of Monofilament Suture Materials? J Oral Maxillofac Surg 2023, 81, 72–79. [Google Scholar] [CrossRef]
- Wang, M.; Xiang, X.; Wang, Y.; Ren, Y.; Yang, L.; Zhang, Y. Comparison of Tensile Properties and Knot Security of Surgical Sutures: An In Vitro Mechanical Study. J Oral Maxillofac Surg 2022, 80, 1215–1222. [Google Scholar] [CrossRef] [PubMed]
- Gillen, A.M.; Munsterman, A.S.; Hanson, R.R. In Vitro Evaluation of the Size, Knot Holding Capacity, and Knot Security of the Forwarder Knot Compared to Square and Surgeon's Knots Using Large Gauge Suture. Vet Surg 2016, 45, 1034–1040. [Google Scholar] [CrossRef] [PubMed]
- Chisnall, R.C. Analysing knots and ligatures: Tying principles, knot characteristics and structural changes. Forensic Sci Int 2020, 313, 110272. [Google Scholar] [CrossRef] [PubMed]
- Romeo, A.; Rocha, C.L.; Fernandes, L.F.; Asencio, F.A.; Zomer, M.T.; Fujimoto, C.; Ussia, A.; Wattiez, A.; Koninckx, P.R.; Kondo, W. What is the Best Surgeon's Knot? Evaluation of the Security of the Different Laparoscopic Knot Combinations. J Minim Invasive Gynecol 2018, 25, 902–911. [Google Scholar] [CrossRef]
- Romeo, A.; Fernandes, L.F.; Cervantes, G.V.; Botchorishvili, R.; Benedetto, C.; Adamyan, L.; Ussia, A.; Wattiez, A.; Kondo, W.; Koninckx, P.R. Which Knots Are Recommended in Laparoscopic Surgery and How to Avoid Insecure Knots. J Minim Invasive Gynecol 2020, 27, 1395–1404. [Google Scholar] [CrossRef]
- Schubert, D.C.; Unger, J.B.; Mukherjee, D.; Perrone, J.F. Mechanical performance of knots using braided and monofilament absorbable sutures. Am J Obstet Gynecol 2002, 187, 1438–1440; discussion 1441–1432. [Google Scholar] [CrossRef]
- Van Leeuwen, N.; Trimbos, J.B. Strength of sliding knots in multifilament resorbable suture materials. Gynecological Surgery 2012, 9, 433–437. [Google Scholar] [CrossRef]
- Trimbos, J.B. Security of various knots commonly used in surgical practice. Obstet Gynecol 1984, 64, 274–280. [Google Scholar] [PubMed]
- Ishikawa, N.; Watanabe, G. Figure 4 Knot: Simple Tying Technique for Robotic and Endoscopic Sutures. Innovations (Phila) 2017, 12, 152–153. [Google Scholar] [CrossRef] [PubMed]
- Romeo, A.; Cipullo, I.; Kondo, W.; Benedetto, C.; Amro, B.; Ussia, A.; Wattiez, A.; Koninckx, P.R. The importance of rotation to teach secure half-hitch sequences in surgery. FVVOG 2023, in press. [Google Scholar]
- Mackenzie, M.W. Laparoscopic intracorporeal cinch knots: changing the square knot paradigm. J Minim Invasive Gynecol 2012, 19, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Ivy, J.J.; Unger, J.B.; Hurt, J.; Mukherjee, D. The effect of number of throws on knot security with nonidentical sliding knots. Am J Obstet Gynecol 2004, 191, 1618–1620. [Google Scholar] [CrossRef]
- Tera, H.; Aberg, C. Strength of knots in surgery in relation to type of knot, type of suture material and dimension of suture thread. Acta chirurgica Scandinavica 1977, 143, 75–83. [Google Scholar]
- Amortegui, J.D.; Restrepo, H. Knot security in laparoscopic surgery. Surgical Endoscopy 2002, 16, 1598–1602. [Google Scholar] [CrossRef]
- Kondo, W.; Zomer, M.T.; Hayashi, R.M.; Fernandes, L.F.; Fujimoto, C.; Romeo, A. Different Blocking Sequences Performed by Laparoscopy. J Minim Invasive Gynecol 2018, 25, 773. [Google Scholar] [CrossRef]
- Tremolada, G.; Hazenfield, K.M.; Smeak, D.D. In vitro holding security of four friction knots of monofilament or multifilament suture used as a first throw for vascular ligation. American Journal of Veterinary Research 2020, 81, 821–826. [Google Scholar] [CrossRef]
- Scott, J.F.; Ascha, M.; Pollard, W.; Bordeaux, J.S. A granny sliding knot for high-tension closures. J Am Acad Dermatol 2019, 80, e145–e146. [Google Scholar] [CrossRef]
- Burrow, R.; Batchelor, D.; Cripps, P. Complications observed during and after ovariohysterectomy of 142 bitches at a veterinary teaching hospital. Vet Rec 2005, 157, 829–833. [Google Scholar] [CrossRef] [PubMed]
- Sanders, R.E.; Kearney, C.M.; Buckley, C.T.; Jenner, F.; Brama, P.A. Knot Security of 5 Metric (USP 2) Sutures: Influence of Knotting Technique, Suture Material, and Incubation Time for 14 and 28 Days in Phosphate Buffered Saline and Inflamed Equine Peritoneal Fluid. Vet Surg 2015, 44, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Akiki, R.K.; Rao, V.; Borrelli, M.R.; Beqiri, D.; Liu, P.Y. To Tie or Not to Knot: How the Half Instrument Tie Technique Outdoes the Traditional Surgeon's Knot. Plast Reconstr Surg 2022, 149, 162e–164e. [Google Scholar] [CrossRef] [PubMed]
- Mohamed Rizvi, Z.; Hameed, A.; Pleass, H. Recognition of the 'Reversed 4' pattern of surgical knot tying. Clin Teach 2021, 18, 219–221. [Google Scholar] [CrossRef]
- Wattiez, A.; Schindler, L.; Ussia, A.; Campo, R.; keckstein, J.; Grimbizis, G.; Exacoustos, C.; Kondo, W.; Nezhat, C.; Canis, M.; et al. A proof of concept that experience-based management of endometriosis complements evidence-based guidelines. FVVOG 2023, in press. [Google Scholar] [CrossRef]
- Ivy, J.J.; Unger, J.B.; Mukherjee, D. Knot integrity with nonidentical and parallel sliding knots. Am J Obstet Gynecol 2004, 190, 83–86. [Google Scholar] [CrossRef]
- Al-Benna, S.; Banieghbal, B. A technique to secure a knot in a confined space. Ann R Coll Surg Engl 2020, 102, 759. [Google Scholar] [CrossRef]
- Romeo, A.; Fujimoto, C.; Cipullo, I.; Giarola, M.; Benedetto, C.; Kondo, W.; Amro, B.; Ussia, A.; Wattiez, A.; P. R., K. Effect of diameter and type of suture on knot and loop security. submitted 2023. [Google Scholar] [CrossRef]
- Shepherd, G.; Romero, R.; Grant, H. Slip-Knot-Loop Suture for Continuous Suturing in Laparoscopy. J Laparoendosc Adv Surg Tech A 2016, 26, 231–234. [Google Scholar] [CrossRef]
- Meylemans, D.; Handojo, K.; Devroe, K.; Aelvoet, C.; Vermeiren, K.; Tollens, T. A Modified Fisherman's Knot for Laparoscopic Suturing. Surg Technol Int 2016, 28, 37–39. [Google Scholar]
- Erickson, A.K.; Fox-Alvarez, W.A.; Regier, P.J.; Case, J.B. In vitro holding strength of the laparoscopic Miller's knot compared with open Miller's knot, open surgeon's throw, and laparoscopic surgeon's throw in a vascular pedicle model. Vet Surg 2020, 49, 1563–1570. [Google Scholar] [CrossRef] [PubMed]
- Ortillés, A.; Rodríguez, J.; Calvo, B. The Miller׳s knot as an alternative to the surgical knotting? Characterization of the mechanical behavior. J Mech Behav Biomed Mater 2014, 38, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Taylor, H.; Grogono, A.W. The constrictor knot is the best ligature. Ann R Coll Surg Engl 2014, 96, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Silver, E.; Wu, R.; Grady, J.; Song, L. Knot Security- How is it Affected by Suture Technique, Material, Size, and Number of Throws? J Oral Maxillofac Surg 2016, 74, 1304–1312. [Google Scholar] [CrossRef]
- Marturello, D.M.; McFadden, M.S.; Bennett, R.A.; Ragetly, G.R.; Horn, G. Knot security and tensile strength of suture materials. Vet Surg 2014, 43, 73–79. [Google Scholar] [CrossRef]
- Ching, S.S.; Mok, C.W.; Koh, Y.X.; Tan, S.M.; Tan, Y.K. Assessment of surgical trainees' quality of knot-tying. J Surg Educ 2013, 70, 48–54. [Google Scholar] [CrossRef]
- Armitage, P.; Berry, G. Factorial designs. Statistical methods in medical research. 2nd edn ed.; Publications, B.S., Ed.; Blackwell Scientific Publications: Oxford, UK, 1987. [Google Scholar]
- Takayasu, K.; Yoshida, K.; Kinoshita, H.; Yoshimoto, S.; Oshiro, O.; Matsuda, T. Analysis of the tractive force pattern on a knot by force measurement during laparoscopic knot tying. Am J Surg 2018, 216, 314–318. [Google Scholar] [CrossRef]
- Muffly, T.M.; Kow, N.; Iqbal, I.; Barber, M.D. Minimum number of throws needed for knot security. J Surg Educ 2011, 68, 130–133. [Google Scholar] [CrossRef]
- Koninckx, P.R.; Gomel, V.; Ussia, A.; Adamyan, L. Role of the peritoneal cavity in the prevention of postoperative adhesions, pain, and fatigue. Fertil Steril 2016, 106, 998–1010. [Google Scholar] [CrossRef]
- Tidwell, J.E.; Kish, V.L.; Samora, J.B.; Prud'homme, J. Knot security: how many throws does it really take? Orthopedics 2012, 35, e532–e537. [Google Scholar] [CrossRef]
- Dahl, K.A.; Patton, D.J.; Dai, Q.; Wongworawat, M.D. Biomechanical characteristics of 9 arthroscopic knots. Arthroscopy 2010, 26, 813–818. [Google Scholar] [CrossRef] [PubMed]
- Tremolada, G.; Hazenfield, K.M.; Smeak, D.D. In vitro holding security of four friction knots of monofilament or multifilament suture used as a first throw for vascular ligation. Am J Vet Res 2020, 81, 821–826. [Google Scholar] [CrossRef]
- Wuennenberg, J.; Kolli, S.S.; Powers, M.; Ozog, D. Surgeon's Knot With 3 Throws to Facilitate Wound Closure: A Video Walkthrough. Dermatol Surg 2023, 49, 309. [Google Scholar] [CrossRef] [PubMed]
- Batra, E.K.; Taylor, P.T.; Franz, D.A.; Towler, M.A.; Edlich, R.F. A portable tensiometer for assessing surgeon's knot tying technique. Gynecol Oncol 1993, 48, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Molinas, C.R.; Binda, M.M.; Sisa, C.M.; Campo, R. A randomized control trial to evaluate the importance of pre-training basic laparoscopic psychomotor skills upon the learning curve of laparoscopic intra-corporeal knot tying. Gynecol Surg 2017, 14, 29. [Google Scholar] [CrossRef]
- Horeman, T.; Blikkendaal, M.D.; Feng, D.; van Dijke, A.; Jansen, F.; Dankelman, J.; van den Dobbelsteen, J.J. Visual force feedback improves knot-tying security. J Surg Educ 2014, 71, 133–141. [Google Scholar] [CrossRef]
- Huffman, E.; Anton, N.; Martin, J.; Timsina, L.; Dearing, W.; Breece, B.; Mann, I.; Stefanidis, D. Optimizing Assessment of Surgical Knot Tying Skill. J Surg Educ 2020, 77, 1577–1582. [Google Scholar] [CrossRef]
- Romero, P.; Gerhaeuser, A.; Carstensen, L.; Kössler-Ebs, J.; Wennberg, E.; Schmidt, M.W.; Müller-Stich, B.P.; Günther, P.; Nickel, F. Learning of Intracorporal Knot Tying in Minimally Invasive Surgery by Video or Expert Instruction. Eur J Pediatr Surg 2023, 33, 228–233. [Google Scholar] [CrossRef]
- Elrod, J.; Boettcher, J.; Vincent, D.; Schwarz, D.; Trautmann, T.; Reinshagen, K.; Boettcher, M. Telementoring of Open and Laparoscopic Knot Tying and Suturing Is Possible: A Randomized Controlled Study. Eur J Pediatr Surg 2022, 32, 443–451. [Google Scholar] [CrossRef]
- Nagaraj, M.B.; Namazi, B.; Sankaranarayanan, G.; Scott, D.J. Developing artificial intelligence models for medical student suturing and knot-tying video-based assessment and coaching. Surg Endosc 2023, 37, 402–411. [Google Scholar] [CrossRef]
- De Witte, B.; Di Rienzo, F.; Martin, X.; Haixia, Y.; Collet, C.; Hoyek, N. Implementing Cognitive Training Into a Surgical Skill Course: A Pilot Study on Laparoscopic Suturing and Knot Tying. Surgical Innovation 2018, 25, 625–635. [Google Scholar] [CrossRef]
- Muffly, T.M.; Espaillat-Rijo, L.M.; Edwards, A.M.; Horton, A. Operating room fatigue: is your twentieth surgical knot as strong as your first? J Surg Educ 2012, 69, 215–217. [Google Scholar] [CrossRef] [PubMed]
- Babetty, Z.; Sumer, A.; Altintas, S. Knot properties of alternating sliding knots with different patterns in comparison to alternating and simple sliding knots. J Am Coll Surg 1998, 186, 485–489. [Google Scholar] [CrossRef] [PubMed]
- Babetty, Z. Changes in Knot-Holding Capacity of Sliding Knots In Vivo and Tissue Reaction. Archives of Surgery 1998, 133, 727. [Google Scholar] [CrossRef]
- Meyer, D.C.; Bachmann, E.; Lädermann, A.; Lajtai, G.; Jentzsch, T. The best knot and suture configurations for high-strength suture material. An in vitro biomechanical study. Orthopaedics & Traumatology: Surgery & Research 2018, 104, 1277–1282. [Google Scholar] [CrossRef]
- Corey, C.S.; Wenger, K.; Johnson, C.P.; Parada, M.S. Loop and knot security of a novel arthroscopic sliding-locking knot using high-strength sutures. Journal of Orthopaedics 2018, 15, 980–983. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.D.; Vaishnav, S.; Saunders, B.M.; Schrumpf, M.A. Optimization of the Racking Hitch Knot: How Many Half Hitches and Which Suture Material Provide the Greatest Security? Clinical Orthopaedics & Related Research 2014, 472, 1930–1935. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.; Hsu, C.-C.; Moriya, T.; Thoreson, A.R.; Cha, S.S.; Moran, S.L.; An, K.-N.; Amadio, P.C. Beyond the Square Knot: A Novel Knotting Technique for Surgical Use. Journal of Bone and Joint Surgery 2013, 95, 1020–1027. [Google Scholar] [CrossRef]
Figure 1.
Symmetric and asymmetric Half-knots are easily changed into half-hitches. Three symmetrical half-hitches remain in one plane. When the acive and passive ends are changed for a blocking half hitch, the assymmetric half hitch become symmetric on the new passive end.
Figure 1.
Symmetric and asymmetric Half-knots are easily changed into half-hitches. Three symmetrical half-hitches remain in one plane. When the acive and passive ends are changed for a blocking half hitch, the assymmetric half hitch become symmetric on the new passive end.
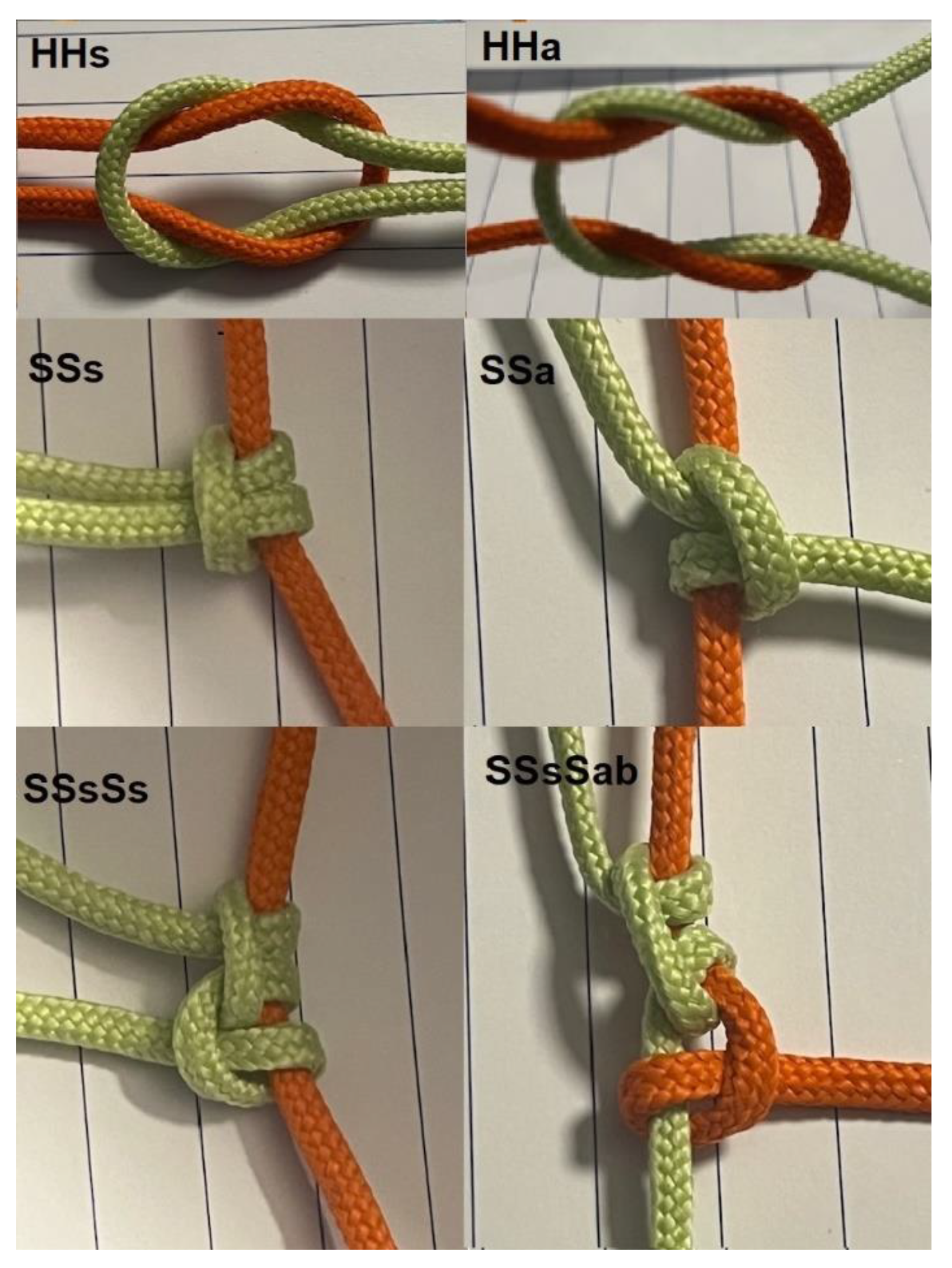

Table 1.
Knot sequences are indicated by their geometry. A flat square knot is symmetric and results from an alternate rotation of the same active end. A granny knot is asymmetric and results from a similar rotation of the same active end. Changing the active and passive ends has the same effect as changing rotation. Knot sequences used to be indicated with = for symmetric (also called identical), x for asymmetric and // for blocking. We prefer a more intuitive indication, with the type of each half-knot (H) or hitch (S), followed by the type of knot, using 's' for symmetric (alternate rotation around the passive end or mono manual suturing) and 'a' for asymmetric (similar rotation around the passive tread). For half-hitches is indicated whether they are sliding (s) or blocking (b) after changing active and passive ends. For half-hitches, the number of throws is not indicated since always one, and sliding is not indicated to avoid confusion with the s of symmetric. A 2-throw half-hitch results from the transformation of a 2-throw half-knot.
Table 1.
Knot sequences are indicated by their geometry. A flat square knot is symmetric and results from an alternate rotation of the same active end. A granny knot is asymmetric and results from a similar rotation of the same active end. Changing the active and passive ends has the same effect as changing rotation. Knot sequences used to be indicated with = for symmetric (also called identical), x for asymmetric and // for blocking. We prefer a more intuitive indication, with the type of each half-knot (H) or hitch (S), followed by the type of knot, using 's' for symmetric (alternate rotation around the passive end or mono manual suturing) and 'a' for asymmetric (similar rotation around the passive tread). For half-hitches is indicated whether they are sliding (s) or blocking (b) after changing active and passive ends. For half-hitches, the number of throws is not indicated since always one, and sliding is not indicated to avoid confusion with the s of symmetric. A 2-throw half-hitch results from the transformation of a 2-throw half-knot.
| Knots | Throws | Knot sequences | rotation | Older indication | New indication |
|---|---|---|---|---|---|
| Half knot | 1,2,3 | H1, H2, H3 | |||
| 2nd symmetric | alternate | H=H, 1=1 | H1H1s, H2H1s, H2H2s, H3H2s | ||
| 2nd asymmetric | similar | HxH, 1x1 | H1H1a, H2H1a, H2H2a, H3H2a | ||
| Secure half-knot sequences: H2H1sH1s, H2H2s or H2H2a, H3H2s or H3H2a | |||||
| Half hitch | 1,2 | S(1), (S2) | |||
| 2nd symmetric | alternate | ||||
| sliding | S=S, 1=1 | SSs(s) | |||
| blocking | S//S | SSsb | |||
| 2nd asymmetric | similar | ||||
| sliding | SxS, 1x1 | SSa(s) | |||
| blocking | S//xS | SSab | |||
| Secure Half-hitch sequences: SSsSabSab | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



