
Submitted:
19 August 2023
Posted:
23 August 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Aims: The aims of this meta-analysis were to assess: the prevalence of Post-Acute COVID-19 sequalae in HIV positive patients; average time of diagnosis; and meta-regress for possible moderators of PACS.Methods: A standard search strategy was used in PubMed, and then later modified according to each specific database to get the best relevant results. These included Medline indexed journals; PubMed Central; NCBI Bookshelf and publishers' Web sites in line with the Preferred Reporting Items for Systematic Review and Meta-Analysis statement. Search terms included “long COVID-19 or post-acute COVID-19 syndrome/sequalae”, “persons living with HIV or HIV. The criteria for inclusion were published clinical articles reporting HIV in association with long COVID-19, further, the average time to an event of post-acute COVID-19 sequelae among primary infected patients with COVID-19. Random-effects model was used. Rank Correlation and Egger's tests were used to ascertain publication bias. Sub-group, sensitivity and meta-regression analysis were conducted. A 95% confidence intervals were presented and a p-value < 0.05 was considered statistically significant. Review Manager 5.4 and comprehensive meta-analysis version 4 (CMA V4) were used for the analysis. The review/trial was PROSPERO registered (CRD42022328509).Results: A total of 43 studies reported post-acute COVID-19 syndrome. Of those, five reported post-acute COVID-19 sequalae in PLHIV. Prevalence of post-acute COVID-19 sequalae was 43.1% (95% CI 20.5% to 68.9%) in persons living with HIV (PLWH). The average time to PACS diagnosis was 4 months at 64% [0.64 (95% CI 0.230, 0.913) (P < 0.0000), I2= 93%] and at one year to PACS diagnosis was at 70 %, however with non-significant correlation (P > 0.05). On comorbidities, asthenia was associated with PACS at 17.6 % [0.176 (95% CI 0.067, 0.385) (P = 0.008), I2= 86%] while fatigue at 82%, however not related with PACS event incidence (P < 0.05). Americas, Asian and European regions showed PACS events rates of 82%, 43% and 19 % respectively (P<0.05) relative to HIV infection. Conclusion: PACS prevalence in PLWH was 43% occurring at an average time of 4 months at 64% and 70 % at 12 months however non-significant with PACS. Asthenia was significantly associated with PACS at 17.6 % while fatigue at 82%, however not related with PACS event incidence. Americas recorded the highest PACS event rates in PLWH.
Keywords:
post COVID-19 Sequelea
; HIV
; meta-analysis
; covariates
Introduction
Long COVID-19 may be defined as patients who, four weeks after the diagnosis of SARSCov-2 infection, continue to have signs and symptoms not explainable by other causes1. Recent reports have described persistent symptoms extending beyond the period of initial illness or hospitalization. Anecdotes of different signs and symptoms occurring after acute infection have also arisen in the lay press2. Long COVID encompasses multiple adverse outcomes, with common new-onset conditions including cardiovascular, thrombotic and cerebrovascular disease3, type 2 diabetes4, myalgic encephalomyelitis/chronic fatigue syndrome5. This post-acute infection represents a significant challenge for patients, physicians, and society because the causes, patient profile, and even symptom patterns remain difficult to characterize6. It may include memory loss, gastrointestinal (GI) distress, fatigue, anosmia, shortness of breath, and other symptoms. PASC has been associated with acute disease severity7, further, it is suspected to be related to autoimmune factors8, as well as unresolved viral fragments9. Post-COVID conditions are found more often in people who had severe COVID-19 illness, but anyone who has been infected with the virus that causes COVID-19 can experience post-COVID conditions, even people who had mild illness or no symptoms from COVID-1910.
The COVID-19 pandemic has substantially affected the lives of people living with HIV (PLHIV), who frequently face multiple morbidities and may be at heightened risk for COVID-19 complications, with spillover effects on other aspects as equitable access to treatment and prevention11–13. Further, PACS has been established as a common phenomenon in PLWH14.
There is a paramount importance in understanding the complexities of long COVID in general, further in immune compromising related comorbidities such as the current one on this study. The body of knowledge being developed to better understand post-COVID syndrome should be accustomed to the most vulnerable populations after mapping out the context of the phenomena among the general population. Studies of patients who have recovered from SARS-CoV-2 infection but have persistent symptoms have ranged widely in size, quality, and methodology, leading to confusion about the prevalence and types of persistent symptoms15, a peculiar issue possibly in HIV infection that requires an updated information through valid and most recent data to inform any on-going clinical, rehabilitative and public health practice. SARS-CoV- 2 can produce short/long-term sequelae and the reports describing post-acute COVID-19 syndrome (PACS) in the general population are increasing, but comprehensive data are lacking in people living with HIV (PLWH). Therefore, this review aimed at assessing the prevalence and factors associated with PACS in our cohort of PLWH.
Methods
A standard search strategy was used in PubMed, and then later modified according to each specific database to get the best relevant results. These included MEDLINE indexed journals; PubMed Central; NCBI Bookshelf and publishers' Web sites. The language was restricted to English and the search dates were for studies conducted/published between June 2021 and August 2022. The basic search strategy was built based on the research question formulation (i.e., PICO or PICOS)16. They were constructed to include free-text terms (e.g., in the title and abstract) and any appropriate subject indexing (e.g., MeSH) expected to retrieve eligible studies, with the help of an expert in the review topic field or an information specialist. The summary of search terms was; long COVID-19; long COVID-19 syndrome; post-Corona Virus syndrome; Post-acute COVID-19 sequelae; Post-acute COVID-19 syndrome; Post-acute COVID-19 condition; HIV; HIV infection; HIV disease, etc. Because the study for this topic would be limited, the outcome term (long COVID-19) in the search term was not be included initially in order to capture more studies. Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement.17 was used. All identified article titles and abstracts were screened independently by two authors (JKM, JMN), with those meeting the inclusion criteria screened further by full text review. On occasions when it was not clear from the abstract if studies were of relevance, the full text of the article was reviewed. Unanimous consensus was met on the inclusion of proposed studies for full text review among the authors. Full text studies were further evaluated against the inclusion and exclusion criteria. The reference lists of included studies were reviewed to ensure no other relevant studies were overlooked.
Search terms and criteria for inclusion
Search terms included for PubMed was as follows: (long COVID-19; long COVID-19 syndrome; post-Corona Virus syndrome; Post-acute COVID-19 sequelae; Post-acute COVID-19 syndrome; Post-acute COVID-19 condition) AND (“the study” [Publication Type] OR “study as the topic” [MeSH Terms] OR “study” AND HIV serostatus AND [All Fields]). A search limit for articles published from mid-2020 2021 applied. The criteria for inclusion were published research articles reporting: 1) the rate prevalence of post-acute COVID-19 syndrome (at admission or following admission) among PLHIV and the possible associated clinical parameters. Studies were excluded if they were case reports, review articles, conference abstracts, non-clinical studies, or were not available in the English language.
Data extraction
The included studies were evaluated for the authors, year of publication/ the study was conducted, title, where it was conducted, study design, time of diagnosis of post-acute COVID-19 sequalae (on admission or following admission with mean/ average time to diagnosis in months) and HIV infection relative to post-acute COVID-19 sequalae. A post-acute COVID-19 sequalae case was defined as the illness that occurs in people who have a history of probable or confirmed SARS-CoV-2 infection; usually within three months from the onset of COVID-19, with symptoms and effects that last for at least two months.
Outcome measures
The primary objectives were to estimate the prevalence of post-acute COVID-19 sequalae in PLWH as from mid-2020and average time of acquiring/being diagnosed with post-acute COVID-19 sequalae. Secondary objectives included meta-regressing for any possible and predetermined covariates to ascertain of any relationship with post-acute COVID-19 sequalae.
Quality assessment
Using the NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies18, all included publications were reviewed independently for potential risk of bias by two authors (JKM, JMN). The assessment tool uses 14 questions to enable allocation of a score to each article (poor, fair, or good). If there was disagreement regarding the scoring of a study, consensus was met after discussion among both assessors.
Statistical analysis
Simple descriptive analysis was performed for the five aims of the review. Heterogeneity among the studies was assessed using the chi-squared test and I², however due to suspected variation among the studies and associated heterogeneity random effects models were used for all meta analyses19. Post-acute COVID-19 events rates were estimated using random-effects model, the mortality associated with post-acute COVID-19 sequalae was statistically assessed using random effects models (DerSimonian and Laird)20, and event rates (ER) were presented. Publication bias was assessed using Begg and Mazumdar Rank Correlation Test and the Egger's Test of the Intercept and a precision funnel plot was used to ascertain this the publication bias status. To account for any possible heterogeneity (I2), sub-group and sensitivity analysis were conducted and in this, some analysis used fixed-effect model analysis, further to these, meta-regression analysis was run for specific pre-determined covariates. For each outcome variable, 95% confidence intervals (CIs) were presented. A p-value < 0.05 was considered statistically significant. This meta-analysis and meta-regression were conducted using comprehensive meta-analysis version 4 (CMA v4).
Results
A list of the five studies 14,22–25 detailing PACS in PLWH that met the inclusion criteria are illustrated below in Table 1.
Figure 1 PRISMA flow diagram showing studies identified and included in a systematic meta-analysis.
Post-acute COVID-19 sequalae event rate in PLHIV
From the analysis based on five studies detailing Post-acute COVID-19 sequalae in PLHIV (n= 320) 14,22–25, the prevalence ranged between 11% to 82% with the mean event rate at 43.1% (95% CI 20.5%, 68.9% [Heterogeneity: Tau² = 1.349; Chi² = 57.197, df = 4 (P = 0.0000); I² = 93%] (Figure 2).
The prediction interval in 95% of all the comparable populations fell between 0.013 to 0.978 demonstrating that, in some populations, the event rates of PACS is at one extreme as low as 1.3% and as high as 98%, this variation reflected differences in real proportions (Figure 3).
Begg and Mazumdar Rank Correlation Test (Kendall’s tau b = 0.10000, P-value = 0.40325) and Egger's Test of the Intercept (Intercept = 3.26596, 95% CI (-13.66376, 20.19568), with t=0.61394, df=3. P-value = 0.29134, indicated an absence of publication bias (Figure 4).
A sensitivity analysis by removing one study with the highest event rate (82%)22,the new mean event rate was 32 % (95% CI 15 %, 55%), a significant difference from the original 43.1 %. This showed that, the mean PACS event rate estimation was contributed differently by each study (p-value >.05) (Figure 5).
Sub-group and meta-regression analysis
To account for the substantial heterogeneity, it deemed applicable to better understand whether and which study-level factors drove the measures of effect. This meta-regression analysis featured as per the objectives of this meta-analysis on the prevalence of Post-Acute COVID-19 sequalae in HIV positive patients and average time of PACS diagnosis.
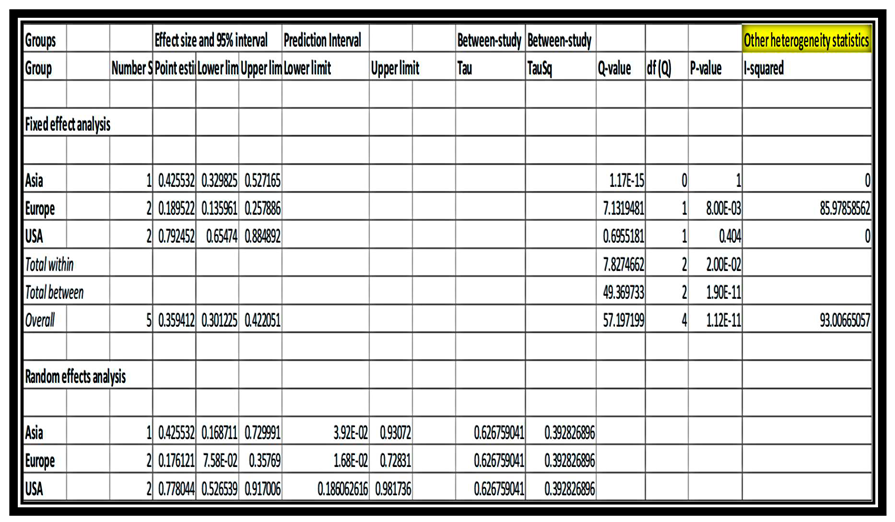
PLWH (HIV positive patients) with only the five studies detailing HIV disease 14,22–25 relative to post COVID-19 syndrome, subgroup analysis showed that, average time of four (4) months to PACS diagnosis was associated with PACS event incidence at 64% [0.64 (95% CI 0.230, 0.913) (P < 0.0000), I2= 93%], with random effects model. An average time of one year to PACS diagnosis was at 70 %, however it did not show any significance with PACS event (P > 0.05) (Fig 18). On the other hand, asthenia in PLHIV was the most associated comorbidity with PACS event at 17.6 % [0.176 (95% CI 0.067, 0.385) (P = 0.008), I2= 86%]. Fatigue was at 82% in PLWH as shown by one study22, however it was not related with PACS event incidence (P < 0.05). Sub-group analysis (fixed effect model) by region demonstrated higher PACS event rates in the United States of America relative to HIV infection, followed by Asian region and European region at 79%(P> 0.05), 43%(P>0.05) and 19 % respectively (P<0.05) (Table 2).
Discussion
This systematic review, meta-analysis and meta-regression sought to estimate the prevalence of post-acute COVID-19 sequalae in general population using the most recent data, which was done from 43 studies 7,26–70 detailing post-acute COVID-19 syndrome, of which, five reported post-acute COVID-19 sequalae in PLHIV and average time of acquiring/being diagnosed with post-acute COVID-19 sequalae. Secondary objectives included meta-regressing for any possible and predetermined covariates to ascertain of any relationship with post-acute COVID-19 sequalae.
Post-acute COVID-19 sequalae prevalence (event - rate) in PLHIV was 43.1% similar to another primary study findings that, the prevalence of long-COVID was 43.6%14 and significantly related with HIV infection as in case of a study that demonstrated that, HIV status strongly predicted the presence of PASC22. PLWH (HIV positive patients) developed signs and symptoms related to post COVID-19 syndrome at an average time of four (4) months, similar to a primary study that showed that, 4 months post COVID-19 infection, PLWH reported fatigue (42%), muscle pain (24%), concentration problems (42%), vision problems (21%) and trouble sleeping (34%)22, which are common post-acute COVID-19 sequalae signs and symptoms. Asthenia and fatigue were seen as the most persistent symptoms. This is consistent with previous findings suggestive of brain involvement which brings about similar lethargic feelings71. Seemingly, although in non-HIV population, a study72, concluded that, persistent symptoms after the first wave of COVID-19 in relation to SARS-CoV-2 serology and experience of acute symptoms: A nested survey in a population-based cohort, similar to current findings on asthenia. Similar conclusion again that,
Recent studies further report that, people with HIV are more likely to experience ‘long COVID’ symptoms and to experience serious cardiovascular and metabolic disorders and cancers after being diagnosed with COVID-1973. Two US researchers involved in long COVID research say there is an urgent need to understand why people with HIV are more vulnerable to long COVID and to include them in clinical trials of potential long COVID treatments73. The perceived prevalence of PACS in PLHIV can also be explained by recent pre-print findings where HIV plays a role as a risk predictor of long COVID-19 symptoms along side other conditions with a conclusion that, underlying HIV infection was also independently associated with neurocognitive LC (OR = 2.5)74.
A limitation of the current review was the defined inclusion criteria for a post-acute COVID-19 sequalae patient, presenting with either one or more suspected signs and symptoms depicting the syndrome. Limited number of studies (only five), seemed not sufficient enough however, these studies were retrieved from a review that consisted 43 studies categorizing PACS in general population.
Author Contributions
J.K.M: Designed the study, reviewed and analyzed the data, participated in quality assessment process, Wrote and submitted the manuscript. E.M.N: Reviewed studies and participated in quality assessment process. J.K.O: Reviewed and analyzed the data, Edited the manuscript. C.O: Reviewed the studies, participated in quality assessment process. R.M.N: Reviewed the studies, participated in quality assessment process, Proofread the manuscript.
Funding statement
No benefits in any form have been received or was received from a commercial party related directly or indirectly to the subject of this article.
Ethical review statement
No ethical approval was required for this study.
References
- Sisó-Almirall A, Brito-Zerón P, Ferrín LC, et al. Long covid-19: Proposed primary care clinical guidelines for diagnosis and disease management. Int J Environ Res Public Health. 2021;18(8). [CrossRef]
- Amenta EM, Spallone A, Rodriguez-Barradas MC, Sahly HME, Atmar RL, Kulkarni PA. Postacute covid-19: An overview and approach to classification. Open Forum Infect Dis. 2020;7(12). [CrossRef]
- Xie Y, Xu E, Bowe B, Al-Aly Z. Long-term cardiovascular outcomes of COVID-19. Nat Med. 2022;28(3). [CrossRef]
- Xie Y, Al-Aly Z. Risks and burdens of incident diabetes in long COVID: a cohort study. Lancet Diabetes Endocrinol. 2022;10(5). [CrossRef]
- Mancini DM, Brunjes DL, Lala A, Trivieri MG, Contreras JP, Natelson BH. Use of Cardiopulmonary Stress Testing for Patients With Unexplained Dyspnea Post–Coronavirus Disease. JACC Hear Fail. 2021;9(12). [CrossRef]
- Rando HM, Bennett TD, Byrd JB, et al. Challenges in defining Long COVID: Striking differences across literature, Electronic Health Records, and patient-reported information. medRxiv Prepr Serv Heal Sci. Published online 2021. [CrossRef]
- Blomberg B, Mohn KGI, Brokstad KA, et al. Long COVID in a prospective cohort of home-isolated patients. Nat Med. 2021;27(9). [CrossRef]
- Galeotti C, Bayry J. Autoimmune and inflammatory diseases following COVID-19. Nat Rev Rheumatol. 2020;16(8). [CrossRef]
- Ramakrishnan RK, Kashour T, Hamid Q, Halwani R, Tleyjeh IM. Unraveling the Mystery Surrounding Post-Acute Sequelae of COVID-19. Front Immunol. 2021;12. [CrossRef]
- Vu T, McGill SC. An Overview of Post–COVID-19 Condition (Long COVID). Can J Heal Technol. 2021;1(9). [CrossRef]
- Posada-Vergara MP, Alzate-ángel JC, Martínez-Buitrago E. Covid-19 and hiv [Covid-19 y vih]. Colomb Med. 2020;51(2).
- Lesko CR, Bengtson AM. HIV and COVID-19: Intersecting Epidemics with Many Unknowns. Am J Epidemiol. 2021;190(1). [CrossRef]
- Massarvva, T. Clinical outcomes of COVID-19 amongst HIV patients: A systematic literature review. Epidemiol Health. 2021;43. [CrossRef]
- Pujari S, Gaikwad S, Chitalikar A, Dabhade D, Joshi K, Bele V. Long-coronavirus disease among people living with HIV in western India: An observational study. Immunity, Inflamm Dis. 2021;9(3). [CrossRef]
- Garg M, Maralakunte M, Garg S, et al. The conundrum of ‘long-covid-19ʹ: A narrative review. Int J Gen Med. 2021;14. [CrossRef]
- Tawfik GM, Dila KAS, Mohamed MYF, et al. A step by step guide for conducting a systematic review and meta-analysis with simulation data. Trop Med Health. 2019;47(1). [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021;372. [CrossRef]
- Bagias C, Sukumar N, Weldeselassie Y, Oyebode O, Saravanan P. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. Int J Environ Res Public Health. 2021;18(4).
- Schreck N, Piepho HP, Schlather M. Best prediction of the additive genomic variance in random-effects models. Genetics. 2019;213(2). [CrossRef]
- Suurmond R, van Rhee H, Hak T. Introduction, comparison, and validation of Meta-Essentials: A free and simple tool for meta-analysis. Res Synth Methods. 2017;8(4). [CrossRef]
- Cochrane. Review Manager (RevMan) [Computer program]. Version 5.4. Copenhagen: The Nordic Cochrane Centre. Cochrane Collab. Published online 2020.
- Peluso MJ, Spinelli MA, Deveau TM, et al. Postacute sequelae and adaptive immune responses in people with HIV recovering from SARS-COV-2 infection. AIDS. 2022;36(12). [CrossRef]
- Mazzitelli M, Trunfio M, Sasset L, et al. Factors associated with post-acute COVID-19 syndrome in a cohort of PLWH. HIV Med. 2021;22(SUPPL 3).
- Kingery JR, Safford MM, Martin P, et al. Health Status, Persistent Symptoms, and Effort Intolerance One Year After Acute COVID-19 Infection. J Gen Intern Med. 2022;37(5). [CrossRef]
- Mazzitelli M, Trunfio M, Sasset L, et al. Factors Associated with Severe COVID-19 and Post-Acute COVID-19 Syndrome in a Cohort of People Living with HIV on Antiretroviral Treatment and with Undetectable HIV RNA. Viruses. 2022;14(3). [CrossRef]
- Goel N, Goyal N, Kumar R. Clinico-radiological evaluation of post COVID-19 at a tertiary pulmonary care centre in Delhi, India. Monaldi Arch chest Dis = Arch Monaldi per le Mal del torace. 2021;91(3). [CrossRef]
- Mahmud R, Rahman MM, Rassel MA, et al. Post-COVID-19 syndrome among symptomatic COVID-19 patients: A prospective cohort study in a tertiary care center of Bangladesh. PLoS One. 2021;16(4 April). [CrossRef]
- Khodeir MM, Shabana HA, Rasheed Z, et al. COVID-19: Post-recovery long-term symptoms among patients in Saudi Arabia. PLoS One. 2021;16(12 December). [CrossRef]
- Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223). [CrossRef]
- Kayaaslan B, Eser F, Kalem AK, et al. Post-COVID syndrome: A single-center questionnaire study on 1007 participants recovered from COVID-19. J Med Virol. 2021;93(12). [CrossRef]
- Maestre-Muñiz MM, Arias Á, Mata-Vázquez E, et al. Long-term outcomes of patients with coronavirus disease 2019 at one year after hospital discharge. J Clin Med. 2021;10(13). [CrossRef]
- Moreno-Pérez O, Merino E, Leon-Ramirez JM, et al. Post-acute COVID-19 syndrome. Incidence and risk factors: A Mediterranean cohort study. J Infect. 2021;82(3). [CrossRef]
- Venturelli S, Benatti S V., Casati M, et al. Surviving COVID-19 in Bergamo Province: A post-Acute outpatient re-evaluation. Epidemiol Infect. Published online 2021. [CrossRef]
- Hirschtick JL, Titus AR, Slocum E, et al. Population-Based Estimates of Post-acute Sequelae of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection (PASC) Prevalence and Characteristics. Clin Infect Dis. 2021;73(11). [CrossRef]
- Boscolo-Rizzo P, Guida F, Polesel J, et al. Sequelae in adults at 12 months after mild-to-moderate coronavirus disease 2019 (COVID-19). Int Forum Allergy Rhinol. 2021;11(12). [CrossRef]
- Petersen MS, Kristiansen MF, Hanusson KD, et al. Long COVID in the Faroe Islands: A Longitudinal Study among Nonhospitalized Patients. Clin Infect Dis. 2021;73(11). [CrossRef]
- Logue JK, Franko NM, McCulloch DJ, et al. Sequelae in Adults at 6 Months after COVID-19 Infection. JAMA Netw Open. 2021;4(2). [CrossRef]
- Elkan M, Dvir A, Zaidenstein R, et al. Patient-reported outcome measures after hospitalization during the covid-19 pandemic: A survey among covid-19 and non-covid-19 patients. Int J Gen Med. 2021;14. [CrossRef]
- Maamar M, Artime A, Pariente E, et al. Post-COVID-19 syndrome, low-grade inflammation and inflammatory markers: a cross-sectional study. Curr Med Res Opin. 2022;38(6). [CrossRef]
- Tleyjeh IM, Saddik B, AlSwaidan N, et al. Prevalence and predictors of Post-Acute COVID-19 Syndrome (PACS) after hospital discharge: A cohort study with 4 months median follow-up. PLoS One. 2021;16(12 December). [CrossRef]
- Wanga V, Chevinsky JR, Dimitrov L V., et al. Long-Term Symptoms Among Adults Tested for SARS-CoV-2 — United States, January 2020-April 2021. MMWR Recomm Reports. 2021;70(36). [CrossRef]
- Ogoina D, James HI, Ogoinja SZ. Post-discharge symptoms among hospitalized covid-19 patients in Nigeria: A single-center study. Am J Trop Med Hyg. 2021;105(3). [CrossRef]
- Lucas C, Wong P, Klein J, et al. Longitudinal analyses reveal immunological misfiring in severe COVID-19. Nature. 2020;584(7821). [CrossRef]
- Dryden MTG, Mudara C, Vika C, et al. Post COVID-19 Condition in South Africa: 3-Month Follow-Up after Hospitalisation with SARS-CoV-2. SSRN Electron J. Published online 2022. [CrossRef]
- Bell ML, Catalfamo CJ, Farland L V., et al. Post-acute sequelae of COVID-19 in a non-hospitalized cohort: Results from the Arizona CoVHORT. PLoS One. 2021;16(8 August). [CrossRef]
- Becker C, Beck K, Zumbrunn S, et al. Long COVID 1 year after hospitalisation for COVID-19: a prospective bicentric cohort study. Swiss Med Wkly. 2021;151(41-42). [CrossRef]
- Wang G, Cao K, Liu K, et al. Kynurenic acid, an IDO metabolite, controls TSG-6-mediated immunosuppression of human mesenchymal stem cells. Cell Death Differ. 2018;25(7). [CrossRef]
- Günster C, Busse R, Spoden M, et al. 6-month mortality and readmissions of hospitalized COVID-19 patients: A nationwide cohort study of 8,679 patients in Germany. PLoS One. 2021;16(8 August). [CrossRef]
- Arnold DT, Hamilton FW, Milne A, et al. Patient outcomes after hospitalisation with COVID-19 and implications for follow-up: Results from a prospective UK cohort. Thorax. 2021;76(4). [CrossRef]
- Huang C, Huang L, Wang Y, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. 2021;397(10270). [CrossRef]
- Ayoubkhani D, Khunti K, Nafilyan V, et al. Post-covid syndrome in individuals admitted to hospital with covid-19: Retrospective cohort study. BMJ. 2021;372. [CrossRef]
- Osikomaiya B, Erinoso O, Wright KO, et al. ‘Long COVID’: persistent COVID-19 symptoms in survivors managed in Lagos State, Nigeria. BMC Infect Dis. 2021;21(1). [CrossRef]
- Somani SS, Richter F, Fuster V, et al. Characterization of Patients Who Return to Hospital Following Discharge from Hospitalization for COVID-19. J Gen Intern Med. 2020;35(10). [CrossRef]
- Sigfrid L, Drake TM, Pauley E, et al. Long Covid in adults discharged from UK hospitals after Covid-19: A prospective, multicentre cohort study using the ISARIC WHO Clinical Characterisation Protocol. Lancet Reg Heal - Eur. 2021;8. [CrossRef]
- Taquet M, Dercon Q, Luciano S, Geddes JR, Husain M, Harrison PJ. Incidence, co-occurrence, and evolution of long-COVID features: A 6-month retrospective cohort study of 273,618 survivors of COVID-19. PLoS Med. 2021;18(9). [CrossRef]
- Wynberg E, van Willigen HDG, Dijkstra M, et al. Evolution of Coronavirus Disease 2019 (COVID-19) Symptoms During the First 12 Months After Illness Onset. Clin Infect Dis. 2022;75(1). [CrossRef]
- Osmanov IM, Spiridonova E, Bobkova P, et al. Risk factors for long covid in previously hospitalised children using the ISARIC Global follow-up protocol: A prospective cohort study. Eur Respir J. 2022;59(2). [CrossRef]
- Pereira C, Harris BHL, Di Giovannantonio M, et al. The Association Between Antibody Response to Severe Acute Respiratory Syndrome Coronavirus 2 Infection and Post-COVID-19 Syndrome in Healthcare Workers. J Infect Dis. 2021;223(10). [CrossRef]
- Fernández-de-las-Peñas C, Guijarro C, Plaza-Canteli S, Hernández-Barrera V, Torres-Macho J. Prevalence of Post-COVID-19 Cough One Year After SARS-CoV-2 Infection: A Multicenter Study. Lung. 2021;199(3). [CrossRef]
- Abdelrahman MM, Abd-Elrahman NM, Bakheet TM. Persistence of symptoms after improvement of acute COVID19 infection, a longitudinal study. J Med Virol. 2021;93(10). [CrossRef]
- Perlis RH, Green J, Santillana M, et al. Persistence of symptoms up to 10 months following acute COVID-19 illness. medRxiv Prepr Serv Heal Sci. Published online 2021. [CrossRef]
- Leijte WT, Wagemaker NMM, van Kraaij TDA, et al. [Mortality and re-admission after hospitalization with COVID-19]. Ned Tijdschr Geneeskd. 2020;164.
- Pinato DJ, Tabernero J, Bower M, et al. Prevalence and impact of COVID-19 sequelae on treatment and survival of patients with cancer who recovered from SARS-CoV-2 infection: evidence from the OnCovid retrospective, multicentre registry study. Lancet Oncol. 2021;22(12). [CrossRef]
- P. S, Madhavan S, Pandurangan V. Prevalence, Pattern and Functional Outcome of Post COVID-19 Syndrome in Older Adults. Cureus. Published online 2021. [CrossRef]
- Guarin G, Lo KB, Bhargav R, et al. Factors associated with hospital readmissions among patients with COVID-19: A single-center experience. J Med Virol. 2021;93(9). [CrossRef]
- Zayet S, Zahra H, Royer PY, et al. Post-COVID-19 syndrome: Nine months after SARS-CoV-2 infection in a cohort of 354 patients: Data from the first wave of COVID-19 in nord franche-comté hospital, France. Microorganisms. 2021;9(8). [CrossRef]
- Myall KJ, Mukherjee B, Castanheira AM, et al. Persistent post–COVID-19 interstitial lung disease: An observational study of corticosteroid treatment. Ann Am Thorac Soc. 2021;18(5). [CrossRef]
- Naik S, Haldar SN, Soneja M, et al. Post COVID-19 sequelae: A prospective observational study from Northern India. Drug Discov Ther. 2021;15(5). [CrossRef]
- Peghin M, Palese A, Venturini M, et al. Post-COVID-19 symptoms 6 months after acute infection among hospitalized and non-hospitalized patients. Clin Microbiol Infect. 2021;27(10). [CrossRef]
- Menges D, Ballouz T, Anagnostopoulos A, et al. Burden of post-COVID-19 syndrome and implications for healthcare service planning: A population-based cohort study. PLoS One. 2021;16(7 July). [CrossRef]
- Peluso MJ, Hellmuth J, Chow FC. Central Nervous System Effects of COVID-19 in People with HIV Infection. Curr HIV/AIDS Rep. 2021;18(6). [CrossRef]
- Robineau O, Wiernik E, Lemogne C, et al. Persistent symptoms after the first wave of COVID-19 in relation to SARS-CoV-2 serology and experience of acute symptoms: A nested survey in a population-based cohort. Lancet Reg Heal - Eur. 2022;17. [CrossRef]
- Yendewa G, Perez JA, Patil N, McComsey GA. HIV Infection is Associated with Higher Risk of Post-Acute Sequelae of SARS-CoV-2 (PASC) However Vaccination is Protective. SSRN Electron J. Published online 2022. [CrossRef]
- Peluso MJ, Deveau TM, Munter SE, et al. Chronic viral coinfections differentially affect the likelihood of developing long COVID. J Clin Invest. 2023;133(3). [CrossRef]
Figure 1.
Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) flow diagram for the studies identified and included in the review.
Figure 1.
Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) flow diagram for the studies identified and included in the review.
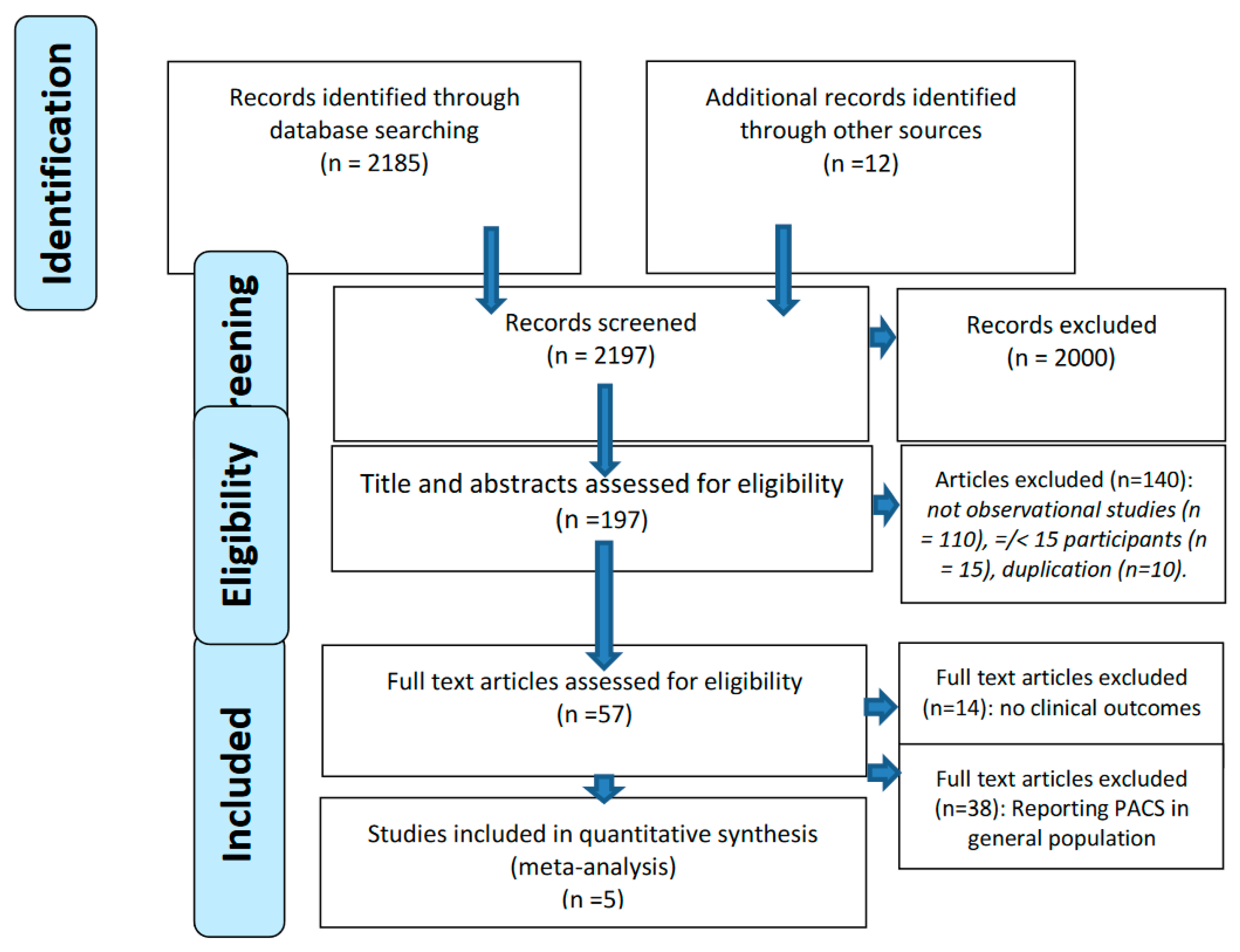
Figure 2.
Post-acute COVID-19 sequalae event rate in PLHIV.
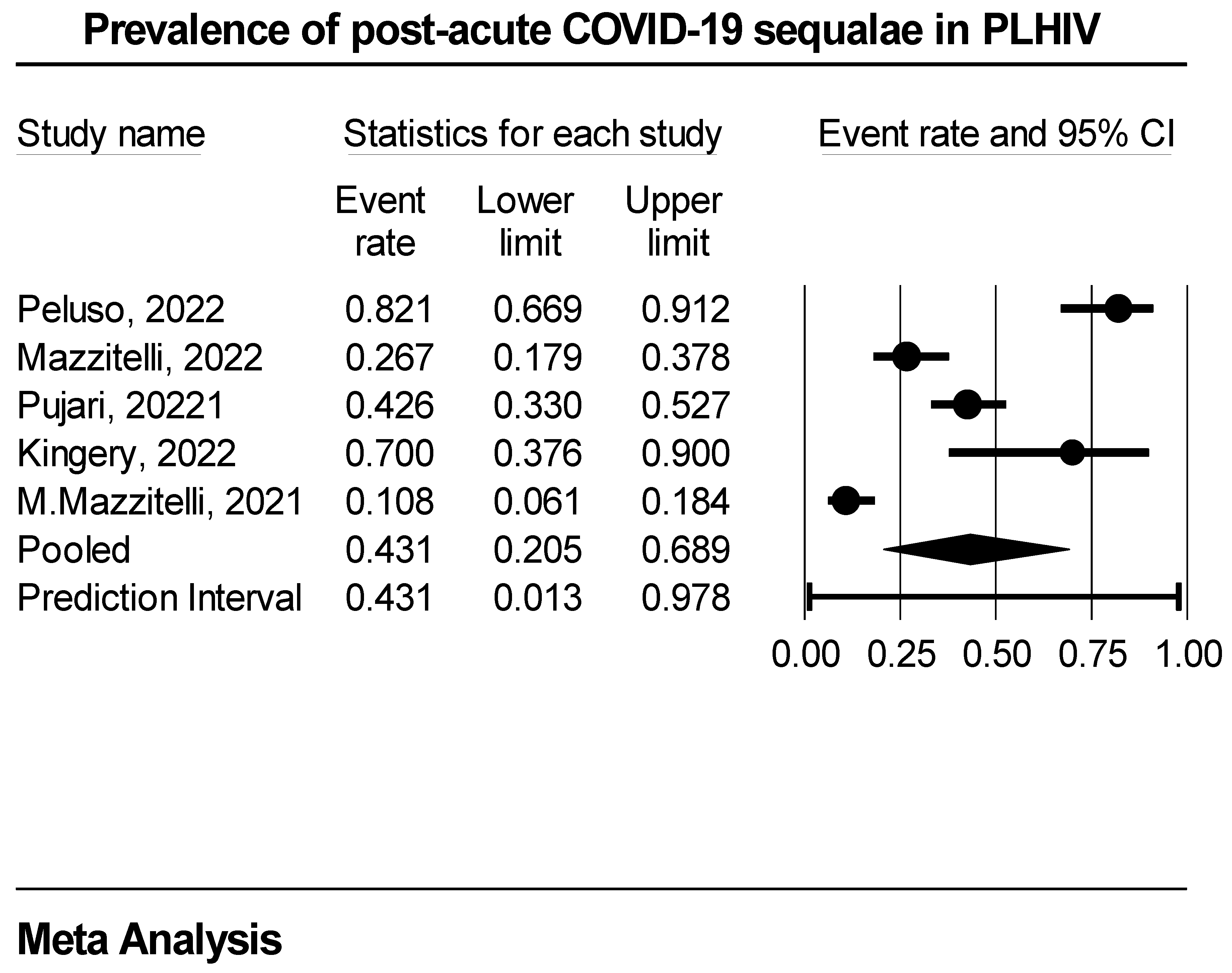
Figure 3.
Distribution of true effects on post-acute COVID-19 sequalae event rate in PLWH.
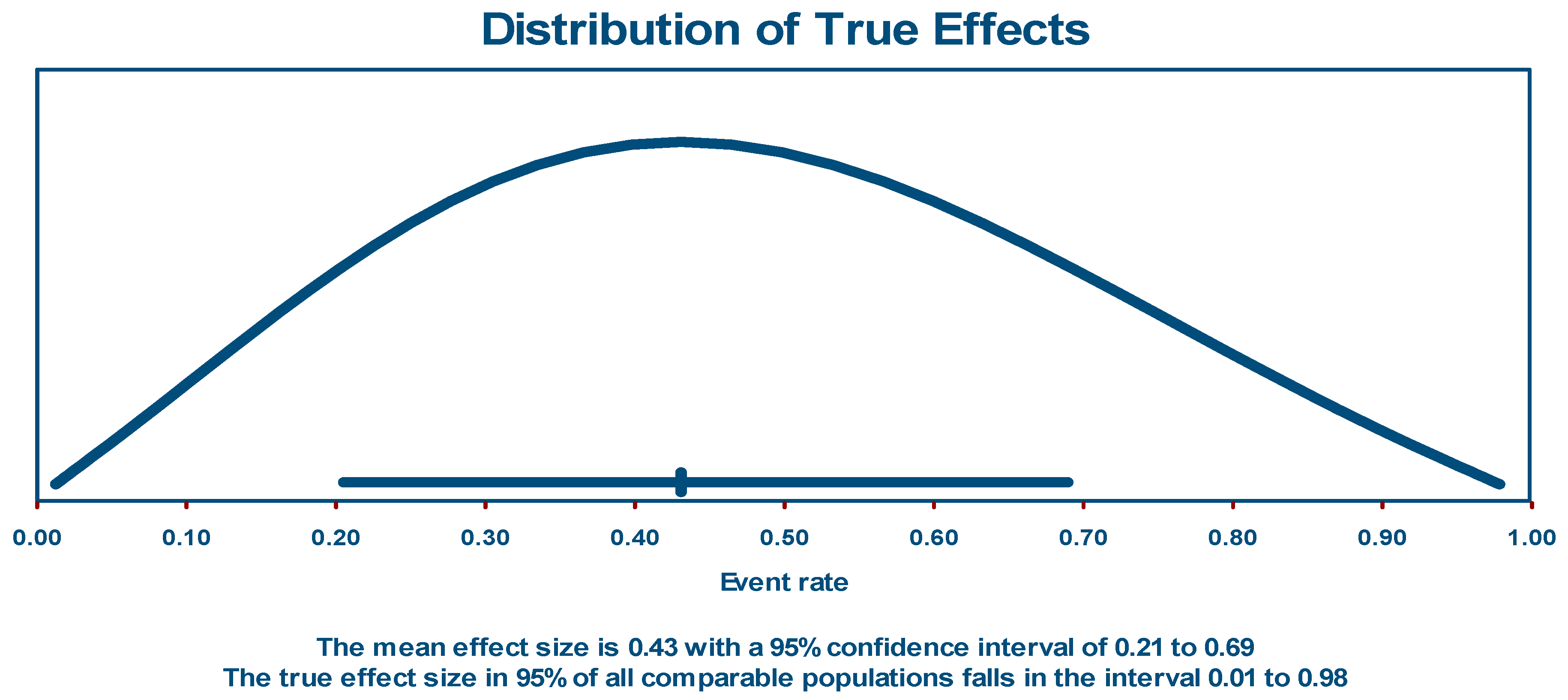
Figure 4.
Funnel plot of publication bias.
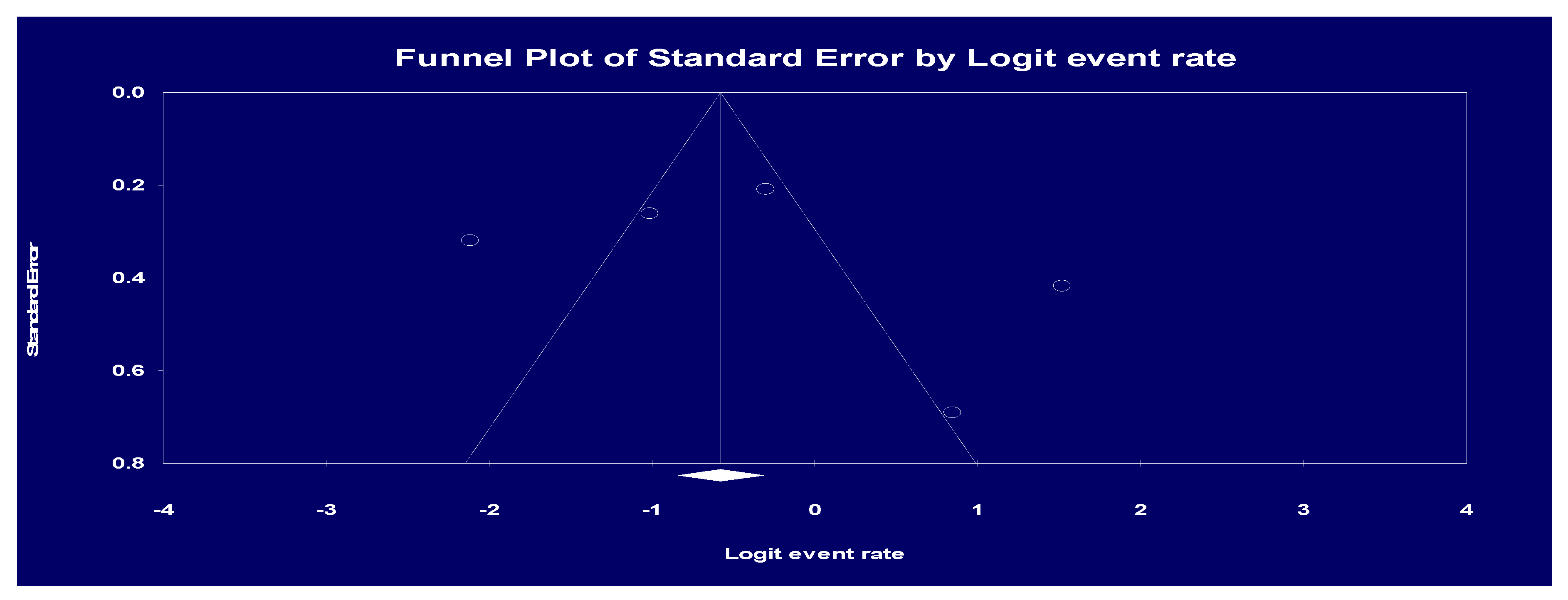
Figure 5.
A sensitivity analysis by removing one study on post-acute COVID-19 sequalae event rate in PLHIV.
Figure 5.
A sensitivity analysis by removing one study on post-acute COVID-19 sequalae event rate in PLHIV.
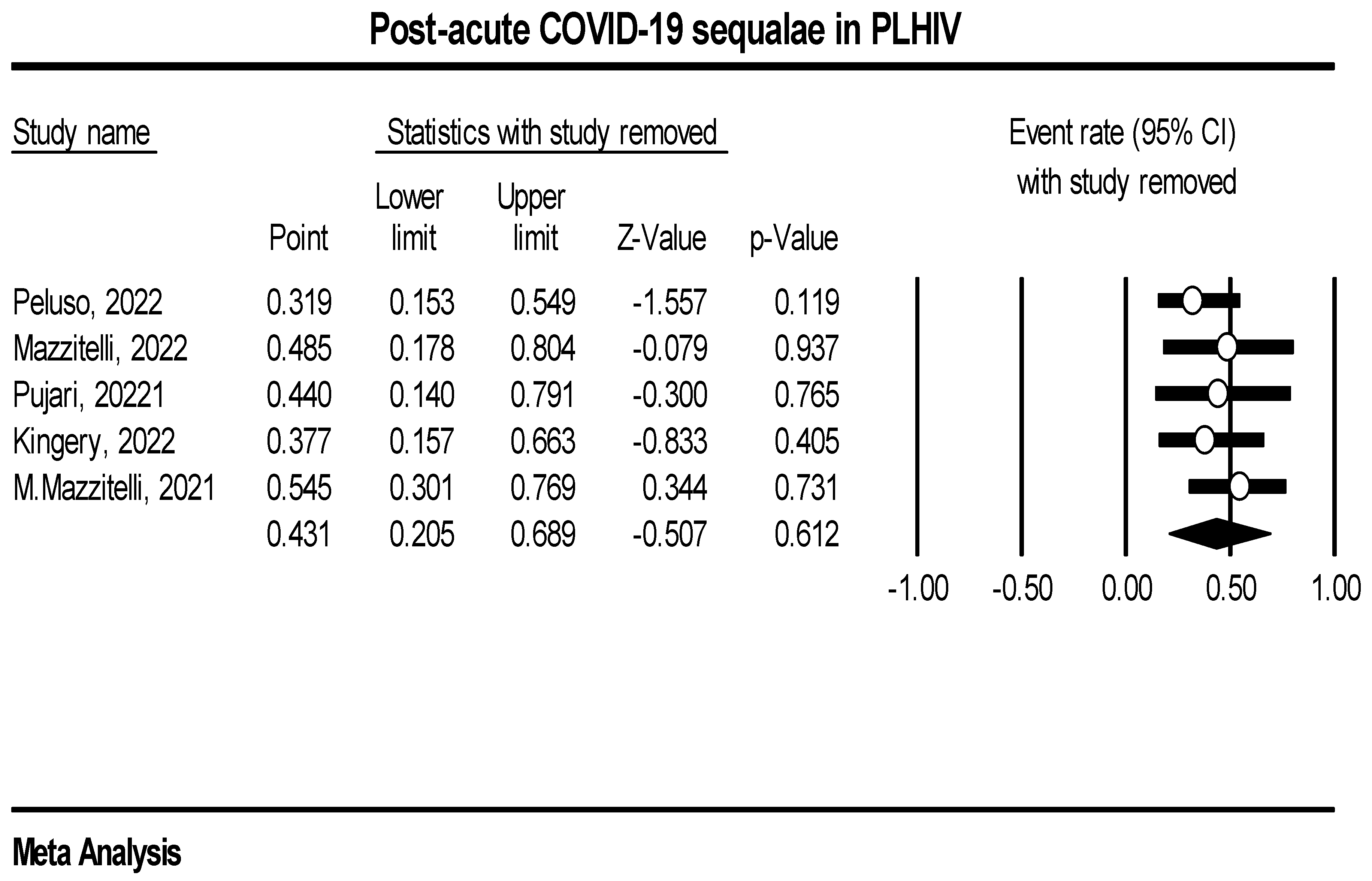

Table 1.
Summery of the studies used in the analysis.
| Study/Author | Region | Study Design | Study Setting | Average time to PACS diagnosis (in months) | |
| 1. | Peluso, 2022 | USA | Prospective | Single | 4 |
| 2. | Mazzitelli, 2022 | Europe | Prospective | Multicenter | 6 |
| 3. | Pujari, 2022 | Asia | Prospective | Single | 4 |
| 4. | Kingery, 2022 | USA | Retrospective | Single | 12 |
| 5. | Mazzitelli, 2022 | Europe | Prospective | Single | 1 |
Table 2.
Meta-analysis grid table on region of study sub-analysis.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



