
Submitted:
21 August 2023
Posted:
25 August 2023
You are already at the latest version
Abstract
Chronic Limb Threatening Ischemia (CLTI) represents the end stage form of peripheral arterial disease (PAD) and is associated to very poor prognosis with high risk of limb loss and mortality. It can be considered very similar to a terminal cancer disease reflecting a large impact on quality of life and healthcare costs. The aim of this study is to offer an overview of the relationship between CLTI, limb salvage and mortality with a focus on the need of a fast-track team-based management, that’s a driver to achieve better survival results. This review can be useful to improve management of this growing impact disease, and promote standardisation of care and communication between specialist and non-specialist health care professionals.
Keywords:
peripheral arterial disease
; critical limb ischemia
; chronic limb-threatening ischemia
; survival
; mortality
; limb salvage
1. Introduction
Peripheral arterial disease (PAD) is a global pandemic of growing proportions and increasing health care costs around the globe [1]. The Global Burden of Disease study reported that 202 million adults worldwide have PAD, a higher prevalence than ischemic heart disease (154 million), heart failure (64 million), Alzheimer’s disease/dementia (44 million), cancer (43 million) [2]. Alarmingly, the prevalence of PAD will probably grow due to population aging and growing prevalence of risk factors, in particular diabetes mellitus (DM). Between 2017 and 2045 the prevalence of DM is expected to rise from 451 to 693 million people worldwide (in 2040, one in 10 adults will have diabetes), and is well known that DM increases the risk and severity of PAD [3].
According to the 2019 Global Vascular Guidelines (GVG) from the European Society for Vascular Surgery, advanced PAD is described as Chronic Limb Threatening Ischemia (CLTI) that represents the end stage form of the disease [4]. This new definition overcome the previous concept of critical limb ischemia (CLI) requiring for diagnosis an objectively documented atherosclerotic PAD in association with ischemic rest pain > 2 weeks duration or tissue loss. GVG recommend to use objective hemodynamic tests such as ankle-brachial index (ABI) < 0.4, absolute ankle pressure (AP) < 50 mmHg, absolute toe pressure (TP) < 30 mmHg, transcutaneous pressure of oxygen (TcPO2) < 30 mmHg and flat or minimal pulsatile volume recording (PVR) waveforms to determine the presence and to quantify severity of ischemia in all patients with suspected CLTI (Recommendation 1.1). In addition, GVG stresses the use of threatened limb classification based on the presence and degree of tissue loss, ischemia, and infection (eg, WIfI classification) that grades wound extent, degree of ischemia, and severity of infection to guide clinical management (Recommendation 1.2). CLTI definition, being accompanied by objective evidence of significant PAD (eg, WIfI ischemia grade > 1), excludes purely neuropathic, traumatic, or venous ulcers lacking any ischemic component.
CLTI affects up to 10% of patients with PAD and is associated with significant mortality, pain, amputation rate, and impaired quality of life. Up to 50% of all patients with CLTI are diagnosed with DM, which co-prevalence is associated with lower revascularisation success rates, decreased wound healing, and higher amputation and mortality rates compared with those without diabetes [5].
CLTI generally results from involvement of at least two arterial segments (aorto-iliac, femoro-popliteal, tibio-pedal) or severe tibio-pedal disease alone. The latter is particularly involved in patients with DM, end-stage renal disease (ESRD), or very elderly. CLTI is a strong indication to endovascular, surgical or hybrid revascularization, in order to prevent major (above the ankle) amputation with the aim of preserving foot plantar support despite the need for minor (below the ankle) amputations, so obtaining limb salvage (LS).
2. CTLI mortality and amputation rate
General and limb prognosis of these frail patients is adverse: they are at continuous risk of a major cardiovascular event, sudden death and major amputation. When an individual first receives a diagnosis of CLTI, mortality risk is around 20-25% over 1 year, and around 60% over 5 years [6,7]. Reported 5 year all cause and cardiovascular mortality rates twice as high (57% and 29%) compared with patients with intermittent claudication (IC) (31% and 15%), respectively, according to a Dutch national registry study [8].
CLTI can be considered very similar to a terminal cancer disease. Few diseases connote a higher mortality rate. Data collected from American Cancer Statistics Center show that among 22 different types of malignancy, only six have a 5-year mortality rate higher than that of CLTI. Yet CLTI is even more deadly than this statistic suggests. Many cancers with high mortality rates are relatively rare, so the overall mortality burden to the population is modest; conversely, the mortality burden associated with some of the most common cancers is blunted due to relatively low mortality rates. Consequently, several deadly cancers, such as melanoma or ovarian cancer, are actually less common and less deadly than CLTI. Because CLTI is both common and deadly, more incident cases die over 5 years after a CLTI diagnosis than with any type of cancer, except for lung cancer [9].
If left untreated, the overall risk of limb loss in CLTI is estimated at approximately 20-25% at 1 year reflecting a large impact on quality of life and healthcare costs. More than half of people with a major amputation will be dead in 5 years [10,11].
A meta-analysis of 13 studies with 1527 patients on the natural history of untreated CLTI reported that at a median follow-up of 12 months both the mortality and the amputation rates were 22%, although there was a marked heterogeneity between the studies [7].
In a study of 574 patients with CLTI who did not undergo revascularization after 2 years, 31.6% had died, primarily of cardiovascular disease, and 23% required major amputation [12].
A recent study [13] investigated long term survival and amputation free survival at 5-year in a cohort of 150 patients with not-revascularizable or so called “no option” CLTI. Amputation free survival was 43% five years after inclusion. This outcome was driven by an equal rate of all-cause mortality (35%) and amputation (33%). Amputation occurred predominantly in the first year. Furthermore, 33% of those with amputation subsequently died within the investigated period, with a median interval of 291 days. Meloni et al. reported a 30% amputation rate and 50% mortality rate for no option-CLTI diabetic patients at 1 year follow-up in a retrospective cohort study [14].
3. Limb Salvage and mortality
Major amputation is an established risk factor for death. Perioperative mortality rate after below the knee amputation (BKA) is around 5-10% and raises to 15-20% after above the knee amputation (AKA). Five-year mortality rate up to 85% have been reported in elderly CLI amputees, and seven-year rates after below and above the knee amputations in a veteran cohort published in 2003 were 72% and 80%, respectively [15,16].
Other studies showed a 3-year death rate of 33.3% after BKA, and 71.4% after AKA. At 5 years these rates raised at 63.3% for BKA and 85.7% for AKA [17].
Despite the guidelines generally recommend to revascularize CLTI patients, the underlying evidence for such a recommendation is limited. However, if we consider the group of patients that undergo some kind of revascularization in order to prevent major amputation outcomes are more favourable [18].
A German Study on a retrospective real-world cohort [19] comparing outcome of CLTI patients with and without revascularization in a period between 2009 and 2011 showed that revascularization is associated with significantly better short and long-term outcomes in term of limb amputation (40,4% vs. 46,5%) and overall mortality (42,6% vs. 48,2%), respectively.
The Italian CLIMATE registry on 2,399 patients treated for CLTI [20] documented an overall mortality of 3,1% at 30-day, and 13,5% at 1-year. Mortality did not statistically differ between genders even if females, who have less comorbidities but are significantly older (over-75), died more than males. Age seems to be a key determinant factor in the outcome of patients treated for CLTI. Age > 75 yrs, coronary-artery disease (CAD), cerebrovascular disease (CVD), and major amputation at the first operation are independent negative prognostic factors for survival at short and mid-term, as well as hemodialysis treatment and tissue loss for 1-year survival. These findings support the effort to attempt revascularization in patients with CLTI, avoiding primary major amputation if possible. Approach to this fragile population should therefore be directed towards aggressive risk factors control by best medical therapy in the long term, and strategies to decrease the amputation risk by means of timely evidence-based revascularization in the short term, as pointed out from the GVG.
4. Medical management improving survival in CLTI and limb salvage
CLTI is a terminal manifestation of systemic atherosclerosis: therefore, it is often accompanied by clinically significant CAD and CVD, resulting in exceedingly high mortality from stroke and myocardial infarction. CAD and CVD are independent predictive factors for mortality at 1 year. The goal of treating patients with CLTI is not only to save a still functional limb, but to reduce major adverse cardiac events (MACE) through aggressive risk factor modification and best medical therapy. Whereas certain risk factors cannot be modified (such as age and sex), others can (DM, hyperlipidemia, hypertension, diabetes, smoking, and sedentary lifestyle). In the absence of aggressive identification and treatment of risk factors and associated comorbidities, the prognosis of CLTI is usually poor [21,22]. However, less than one-third of patients with CLTI are prescribed optimal medical therapy [23].
The GVG strongly recommend best medical therapy including the use of moderate or high-intensity statin, antihypertensive, glycemic control and antiplatelet agents, to reduce all-cause and cardiovascular mortality in patients with CLTI as well as counselling on smoking cessation, healthy diet and weight loss, regular physical exercise, and preventive foot care [4].
Novel oral anticoagulants (NOACs) are assuming increasing role in reducing MACE and major adverse limb events (MALE) in PAD patients. According to the COMPASS study a low dose rivaroxaban (2.5 mg twice a day) plus 100 mg ASA determine a 28% reduction in MACE, a 46% reduction in MALE, and a 31% reduction in the composite endpoint occurrence rates compared to ASA, with no excess in fatal or critical bleedings [24]. The VOYAGER PAD trial demonstrated that dual therapy with low dose rivaroxaban and aspirin reduces significantly MACE and MALE occurrence also in patients with symptomatic PAD undergoing revascularization vs aspirin alone (HR 0.85, 95% CI 0.76–0.96) [25].
5. The need for Fast Track team-based management for optimal CLTI care
CLTI patients represent an extremely high-risk subset and deserve a proven clinical pathway. Limiting limb tissue loss in CLTI patients is of paramount importance in preventing major amputations that is one of the major drivers to mortality in these patients, therefore CLTI is a strong indication to revascularization (endovascular, surgical, or hybrid) with two main targets:
- (1)
- Clinical: prevent major amputation (above the ankle) and obtain LS keeping plantar standing despite the need for minor (below the ankle) amputations
- (2)
- Technical: obtain direct flow at least on one tibial artery
As stressed from GVG [4], treatment should be achieved within 2 weeks from diagnosis. Despite the availability of different treatments and specific guidelines, patients with CLTI are often undertreated. Long-standing concern exists regarding late presentation and delayed management contributing to increased amputation rates. Multiple health care specialists are involved in the management of CLTI, yet lack of public awareness and the frequent failure to make an early diagnosis continue to be major obstacles to effective treatment. Time delays in CLTI identification, referral and management have a direct and detrimental impact on the outcome for the patient [26]. Societal guidelines recommend that all individuals diagnosed with CLTI undergo an imaging study to assess the viability of endovascular or surgical revascularization but variability in practice patterns is high, contributing to a broad disparity in the use of treatments and clinical outcomes. For example, a study from the United States suggested that many patients do not even receive angiography in the year before major limb amputation [27]. In the last two decades, improved awareness of the need for limb preservation has given rise to the idea of integrated amputation prevention programs in which specialized multidisciplinary teams cooperate in the medical/surgical management of these patients [28]. In the new GVG the importance of multidisciplinary teams (MDT) and centers of excellence for amputation prevention is stressed as a key health system initiative [4]. Evaluation of peripheral vasculature and prompt revascularization are therefore key components in managing CLTI.
In our institution in Arezzo, since the first decade of this century, we strived to achieve excellence in the management of diabetic foot and CLTI developing a fast-track team-based approach [29]. That was assured by the presence of a high-volume diabetic foot clinic with dedicated personnel and surgical competencies, an aggressive endovascular interventionalist attitude, and a daily collaborative interaction between different specialists: diabetologist with special expertise in diabetic foot, vascular specialist with special expertise in peripheral procedures (either vascular surgeon and interventional cardiologist both in charge for endovascular revascularization, and vascular surgeon responsible for open surgical approach), infectious disease specialists, and orthopedic surgeons. A podologist and two specially trained nurses are also essential members of the team. In addition to this the foot clinic works closely together with nurses of the community wound-service that provide home wound care. Of note, the cardiovascular laboratory interventional team (including nurses and radiology technicians) and two cath-labs are shared between the vascular surgeons and interventional cardiologists.
The implementation of a team approach has led to a systematic process for screening, evaluation, treatment, and follow-up of CLTI patient (with or without diabetes mellitus). These results have been certified by a national evaluation, becoming a benchmark in Italy. The number of major amputations in Italy ranges between 34 to 43 per million inhabitants, whereas in the Arezzo province (350,000 residents and more than 14,000 diabetics), major amputations occur in between 6 to 12 per million inhabitants. Performance data from Mes Sant’Anna-Pisa, referring to 2022, reported 10.3 major amputations per million inhabitants. The core strategy leading to these results has been the implementation of a fast-track approach centering on the proactive role of the foot specialist, and on the direct involvement in the diagnostic phase of the vascular specialist (either an interventional cardiologist or a vascular surgeon) that will take in charge the patient for the eventual endovascular treatment.
Patient can be referred to foot clinic (mainly diabetic patients) or directly to vascular surgeon (mainly non-diabetic patients) that will ask foot clinical evaluation in case of ulcerations/tissue loss.
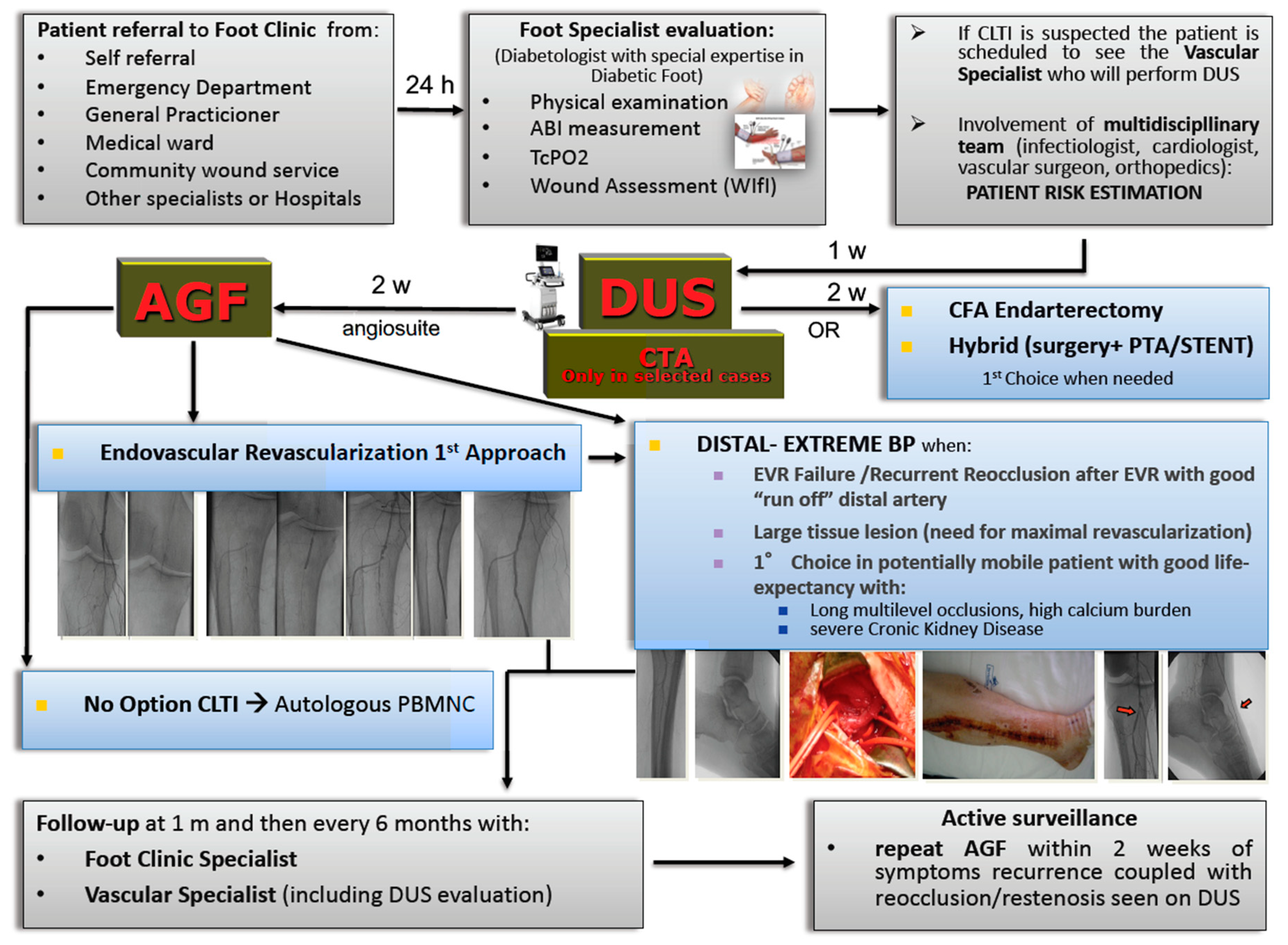
Our treatment algorithm in case of CLTI patient with tissue loss referred to the “Foot Clinic” is summarized in Figure 1.
Foot Clinic evaluation provides complete physical examination and non-invasive hemodynamic tests (including ABI, TcPo2, and continuous-wave Doppler) in order to collect objective parameters to define the degree of ischemia and establish correct WIfI score. If CLTI is suspected by the foot specialist, the patient is scheduled to see the vascular specialist that will perform rapid-access intervention oriented duplex ultrasound (DUS) in maximum of 1 week time. The vascular specialist is the same who will eventually execute the possible angiography and eventual consensual endovascular revascularization. DUS is a first line imaging technique, and is the only preoperative imaging technique we use in the majority of cases. It allows to detect associated vascular diseases (such as abdominal aortic aneurysm, or internal carotid artery stenosis), the location and extension of the lesions, the availability of autologous veins for eventual distal bypass, and helps in planning the surgical or endovascular intervention. Only few cases need computed tomography angiography (CTA) to get essential information for planning. If a definitive diagnosis of CLTI is established, according to the recent GVG, LS is attempted within 2 weeks in all cases, after a careful planning of the interventional solutions, including the decision of whether the strategy can be completed in one or multiple sessions [4].
LS is associated with endovascular or open surgery revascularization. The complex clinical scenario of CLTI patients, especially with diabetes or ERSD, requires integration between the vascular anatomy, the interventional possibilities, and the comorbidities of the patient in order to select the appropriate revascularization strategy that has to be tailored on the single patient.
We follow an “endovascular-first” approach unless the vascular anatomy suggests surgical or hybrid procedure (such as common femoral artery endarterectomy, with or without PTA/stenting of the iliac-femoral-popliteal-tibial arteries). Distal bypass to the foot is preferred as first approach only for average-risk patients with advanced limb threat and high complexity disease in presence of a suitable great saphenous vein.
Notably, as underlined from GVG, the first step that control all the treatment algorithm is the patient risk estimation [4]. Team evaluation of patient frailty, periprocedural risk, quality of life and life expectancy leads to LS candidacy decision. To define a strategy, it’s paramount to consider the patient first, and not the lesion. That’s the cornerstone of the patient-centered approach in a multidisciplinary team. Primary amputation or palliation should be offered to patients with limited life expectancy, poor functional status (eg, non-ambulatory), or unsalvageable limb after shared decision-making. Revascularization as a palliative treatment should only be considered to improve inflow for a subsequent major amputation at the more distal level, or to relieve intractable pain.
“No option” CLTI patients, that are not eligible for revascularization as a result of the inability to overcome vessel obstruction, no visible arterial circulation in the foot (“desert foot”) and/or for critical general conditions [14,30] can be candidates for autologous cell therapy with peripheral blood mononuclear cells (PBMNC), that has arisen as a possible strategy to relieve ischemic pain and promote ulcer healing before eventually taking into consideration a major amputation [31,32].
Once discharged, all patients are asked to return at specified follow-up intervals (at 1 month, then every 6 months) to a dedicated clinic run by vascular specialists for DUS control. The foot specialist reviews the patients during the same appointment.
The dedicated foot/cardiovascular clinic also forms the backbone of our clinical research activity, which has so far produced several randomized, industry-independent trials published in high-impact journals [32-38].
Outside this scheduled follow-up scheme, the foot specialist plays a crucial role in dictating the indication to repeat revascularization, alerting the vascular specialist regarding the reoccurrence of rest pain and negative outcome of the ulcer. The foot specialist receives also continuous feedback from nurses of the community wound service that provide home wound-care. No healing, onset of new lesion, worsening of the wound (increase, necrotic margin, fibrin deposition, regression of granulation tissue) detected during wound medication sessions prompt DUS evaluation of the treated or contralateral limb. If reocclusion or restenosis are detected, revascularization is scheduled within 2 weeks.
6. The impact of Paclitaxel-Eluting Devices (PED) on Mortality
The advent of drug-eluting technology with PED significantly reduced restenosis rate, and the need for target lesion redo endovascular treatment of CLTI patients [32-39]
A meta-analysis of randomized trials of PED for femoropopliteal interventions published in 2019 reported a safety issue related to a two-fold increase in 5-year mortality in patients treated with PED, compared to non-eluting devices (NED) [40]. The mechanism responsible for late mortality remained unknown. Reasonable doubts has been raised on methodical issues (such as lack of information on the original patient data, cross-over, relevant loss of follow-up in the RCTs, incomplete RCT data reporting), and alimented a world-wide scientific debate. The FDA reccomended the use of treatments other than paclitaxel-coated balloons and stents for most PAD patients. In response to this safety signal, several studies on large health-care databases and patient-level data of the single RCTs included in the meta-analysis were published, and in none of them PED were associated to a significant increased mortality risk [41-44].
An insight from the Voyager PAD RCT has clearly demonstrated no different impact on long term mortality according to the use of PED or NED, with all-cause mortality of 12,9% in NED group vs. 12,1% in PED group at 42 months from randomisation [45].
We recently published the 10-year experience from our interventional center focused on limb salvage, investigating mortality in PED treated patients [46]. Results suggested a clear reduced mortality for PED compared to NED treatment in a real-worl CLTI scenario at 2 years (12% vs. 18%) and 5 years (30% vs. 36%). This advantage tends to disappear at 7-year follow-up due to the reduced life expectancy of >75 yo patients. Moreover, 7-year major amputations rate was very low in our study (2,3% in NED, 1,6% in PED), though without reaching statistical significance. The reason for this low major amputation rate is probably correlated with the foot-healing program, and the continuous monitoring of healing and patency as a fast-track strategy for reintervention in case of need, as previously mentioned.
7. Conclusions
The impact of CLTI on the affected patient is comparable to that of cancer, and the costs involved in the management of this widespread disease are enormous. Despite the availability of different treatments and specific guidelines, patients with CLTI are often undertreated. Limiting limb tissue loss is paramount in preventing major amputation, that is one of the major drivers to mortality in this subset of patients. The key to preventing limb loss is aggressive risk factors management and best medical therapy, together with timely revascularization that should be attempted whenever possible. A fast-track strategy with less than 2-week interval between diagnosis and treatment offer the chance to rapid restore of direct flow to the foot in order to prevent larger extent of tissue loss. The combination of a wise, although aggressive, interventional strategy together with continued ulceration debridement, healing process evaluation, appropriate medical therapy, and immediate ultrasound evaluation in case of possible CLTI recurrence are the keys to success.
Only spreading awareness and appropriate pathways can control the growing impact of this deadly disease. Foot clinic service providing rapid access to collaborative multidisciplinary specialist assessment and management of CLTI patient focusing on fast-track approach is crucial. It is hoped that the publication of the Global Vascular Guidelines will lead to the adoption of a common language providing greater standardization in care.
Experience of single members of the team is also a cornerstone of management success.
Notably, this field of action is a great challenge for vascular surgeons that need to acquire advanced DUS performing skills, high expertise in both endovascular and open surgery lower limb revascularization, aggressive but also versatile planning attitude in order to tailor interventional strategy on the single patient, and an open mind oriented with an eye on cost/effectiveness evaluations. Vascular surgeon’s societies should have active role in promoting this educational top-goal.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Fowkes, F.G.R.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.; Williams, L.J.; Mensah, G.A.; et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef]
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef]
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract 2018, 138, 271–81. [Google Scholar] [CrossRef]
- Conte, M.S.; Bradbury, A.W.; Kolh, P.; White, J.V.; Dick, F.; Fitridge, R.; Mills, J.L.; Ricco, J.B.; Suresh, K.R.; Murad, M.H.; et al. Global vascular guidelines on the management of chronic limb-threatening ischemia. J Vasc Surg 2019, 69, 3S–125S. [Google Scholar] [CrossRef]
- Mohammedi, K.; Woodward, M.; Hirakawa, Y.; Zoungas, S.; Colagiuri, S.; Hamet, P.; Harrap, S.; Poulter, N.; Matthews, D.R.; Marre, M.; et al. Presentations of major peripheral arterial disease and risk of major outcomes in patients with type 2 diabetes: Results from the ADVANCE-ON study. Cardiovasc Diabetol 2016, 15, 129. [Google Scholar] [CrossRef]
- Mustapha, J.A.; Katzen, B.T.; Neville, R.F.; Lookstein, R.A.; Zeller, T.; Miller, L.E.; Jaff, M.R. Disease burden and clinical outcomes following initial diagnosis of critical limb ischemia in the Medicare population. JACC Cardiovasc Interv 2018, 11, 1011–1012. [Google Scholar] [CrossRef]
- Abu Dabrh, A.M.; Steffen, M.W.; Undavalli, C.; Asi, N.; Wang, Z.; Elamin, M.B.; Conte, M.S.; Murad, M.H. The natural history of untreated severe or critical limb ischemia. J Vasc Surg 2015, 62, 1642–51. [Google Scholar] [CrossRef]
- Van Haelst, S.T.W.; Koopman, C.; Den Ruijter, H.M.; Moll, F.L.; Visseren, F.L.; Vaartjes, I.; de Borst, G.J. Cardiovascular and all-cause mortality in patients with intermittent claudication and critical limb ischaemia. Br J Surg.
- Mustapha, J.A.; Katzen, B.T.; Neville, R.F.; Lookstein, R.A; Zeller, T.; Miller, L.E.; Driver, V.R.; and JAFF, M.R. Critical Limb Ischemia: a threat to life and limb. Endovascular Today, 20 May.
- Ward, R.; Dunn, J.; Clavijo, L.; Shavelle, D.; Rowe, V.; Woo, K. Outcomes of critical limb ischemia in an urban, safety net hospital population with high WIfI amputation scores. Ann Vasc Surg 2017, 38, 84–9. [Google Scholar] [CrossRef]
- Duff, S.; Mafilios, M.S.; Bhounsule, P.; Hasegawa, J.T. The burden of critical limb ischemia: a review of recent literature. Vasc Health Risk Manag 2019, 15, 187–208. [Google Scholar] [CrossRef]
- Marston, W.A.; Davies, S.W.; Armstrong, B.; Farber, M.A.; Mendes, R.C.; Fulton, J.J.; Keagy, B.A. Natural history of limbs with arterial insufficiency and chronic ulceration treated without revascularization. J Vasc Surg 2006, 44, 108–14. [Google Scholar] [CrossRef]
- Verwer, M.C.; Wijnand, J.G.J.; Teraa, M.; Verhaar, M.C.; de Borst, G.J. Long Term Survival and Limb Salvage in Patients With Non-Revascularisable Chronic Limb Threatening Ischaemia. Eur J Vasc Endovasc Surg 2021, 62, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Meloni, M.; Izzo, V.; Da Ros, V.; Morosetti, D.; Stefanini, M.; Brocco, E.; Giurato, L.; Gandini, R.; Uccioli, L. Characteristics and Outcome for Persons with Diabetic Foot Ulcer and No-Option Critical Limb Ischemia. J Clin Med 2020, 9, 3745. [Google Scholar] [CrossRef]
- Klaphake, S.; de Leur, K.; Mulder, P.G.; Ho, G.H.; de Groot, H.G.; Veen, E.J.; Verhagen, H.J.; van der Laan, L. Mortality after major amputation in elderly patients with critical limb ischemia. Clin Interv Aging 2017, 12, 1985–92. [Google Scholar] [CrossRef] [PubMed]
- Cruz, C.P.; Eidt, J.F.; Capps, C.; Kirtley, L.; Moursi, M.M. Major lower extremity amputations at a Veterans Affairs hospital. Am J Surg 2003, 186, 449–54. [Google Scholar] [CrossRef]
- Ferraresi, R.; Mauri, G.; Losurdo, F.; Troisi, N.; Brancaccio, D.; Caravaggi, C.; Neri, L. BAD transmission and SAD distribution: A new scenario for critical limb ischemia. J Cardiovasc Surg 2018, 59, 655–664. [Google Scholar] [CrossRef] [PubMed]
- Almasri, J.; Adusumalli, J.; Asi, N.; Lakis, S.; Alsawas, M.; Prokop, L.J.; Bradbury, A.; Kolh, P.; Conte, M.S.; Murad, M.H. A systematic review and meta-analysis of revascularization outcomes of infrainguinal chronic limb-threatening ischemia. J Vasc Surg 2018, 68, 624–633. [Google Scholar] [CrossRef] [PubMed]
- Stella, J.; Engelbertz, C.; Gebauer, K.; Hassu, J.; Meyborg, M.; Freisinger, E.; Malyar, N.M. Outcome of patients with chronic limb-threatening ischemia with and without revascularization. Vasa 2020, 49, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Martelli, E.; Zamboni, M.; Sotgiu, G.; Saderi, L.; Federici, M.; Sangiorgi, G.M.; Puci, M.V.; Martelli, A.R.; Messina, T.; Frigatti, P.; et al. Sex-Related Differences and Factors Associated with Peri-Procedural and 1 Year Mortality in Chronic Limb-Threatening Ischemia Patients from the CLIMATE Italian Registry. J Pers Med 2023, 13, 316. [Google Scholar] [CrossRef]
- Armstrong, E.J.; Wu, J.; Singh, J.D.; Dawson, D.L.; Pevec, W.C.; Amsterdam, E.A.; Laird, J.R. Smoking cessation is associated with decreased mortality and improved amputation-free survival among patients with symptomatic peripheral artery disease. J Vasc Surg 2014, 60, 1565–1571. [Google Scholar] [CrossRef]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.P.; Czerny, M.; Carlo, M.D.; Debus, S.; et al. 2017 ESC guidelines on the diagnosis and treatment of Peripheral Arterial Diseases in collaboration with the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–821. [Google Scholar] [CrossRef]
- Hung, J.; Timaran, D.A.; Modrall, J.G.; Ahn, C.; Timaran, C.H; Kirkwood, M.L.; Baig, M.S.; Valentine, R.J. Optimal medical therapy predicts amputation-free survival in chronic critical limb ischemia. J Vasc Surg 2013, 58, 972–980. [Google Scholar]
- Anand, S.S.; Bosch, J.; Eikelboom, J.W.; Connolly, S.J.; Diaz, R.; Widimsky, P.; Aboyans, V.; Alings, M.; Kakkar, A.K.; Keltai, K.; et al. Rivaroxaban with or without aspirin in patients with stable peripheral or carotid artery disease: An international, randomised, double-blind, placebo-controlled trial. Lancet 2018, 391, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Bonaca, M.P.; Bauersachs, R.M.; Anand, S.S.; Debus, E.S.; Nehler, M.R.; Patel, M.R.; Fanelli, F.; Capell, W.H.; Diao, L.; Jaeger, N.; et al. Rivaroxaban in peripheral artery disease after revascularization. N. Engl. J. Med. 2020, 382, 1994–2004. [Google Scholar] [CrossRef] [PubMed]
- Nickinson, A.T.O.; Bridgwood, B.; Houghton, J.S.M.; Nduwayo, S.; Pepper, C.; Payne, T.; Bown, M.J.; Davies, R.S.M.; Sayers, R.D. A systematic review investigating the identification, causes, and outcomes of delays in the management of chronic limb-threatening ischemia and diabetic foot ulceration. J Vasc Surg 2020, 71, 669–681. [Google Scholar] [CrossRef] [PubMed]
- Goodney, P.P.; Holman, K.; Henke, P.K.; Travis, L.L.; Dimick, J.B.; Stukel, T.A.; Fisher, E.S.; Birkmeyer, J.D. Regional intensity of vascular care and lower extremity amputation rates. J Vasc Surg, 1471; -9. [Google Scholar]
- Alexandrescu, V.; Hubermont, G.; Coessens, V.; Philips, Y.; Guillaumie, B.; Ngongang, C.; Vincent, G.; Azdad, K.; Ledent, G.; De Marre, C.; Macoir, C. Why a multidisciplinary team may represent a key factor for lowering the inferior limb loss rate in diabetic neuro-ischaemic wounds: application in a departmental institution. Acta Chir Belg 2009, 109, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Liistro, F.; Porto, I.; Angioli, P.; Ducci, K.; Falsini, G.; Grotti, S.; Ricci, L.; Ventoruzzo, G.; Turini, F.; Bellandi, G.; et al. A Team-Based Strategy for Optimal CLI Care. Endovascular Today 2014, 5, 35–40. [Google Scholar]
- Caetano, A.P.; Conde Vasco, I.; Veloso Gomes, F.; Costa, N.V.; Luz, J.H.; Spaepen, E.; Formiga, A.; Coimbra, É. ; Neves, J.; Bilhim, T. Successful Revascularization has a Significant Impact on Limb Salvage Rate and Wound Healing for Patients with Diabetic Foot Ulcers: Single-Centre Retrospective Analysis with a Multidisciplinary Approach. Cardiovasc Intervent Radiol 2020, 43, 1449–1459. [Google Scholar] [CrossRef]
- Rigato, M.; Monami, M.; Fadini, G.P. Autologous Cell Therapy for Peripheral Arterial Disease: Systematic Review and Meta- Analysis of Randomized, Nonrandomized, and Noncontrolled Studies. Circ Res 2017, 120, 1326–1340. [Google Scholar] [CrossRef]
- Scatena, A.; Petruzzi, P.; Maioli, F.; Lucaroni, F.; Ambrosone, C.; Ventoruzzo, G.; Liistro, F.; Tacconi, D.; Di Filippi, M.; Attempati, N.; et al. Autologous Peripheral Blood Mononuclear Cells for Limb Salvage in Diabetic Foot Patients with No-Option Critical Limb Ischemia. J Clin Med 2021, 10(10), 2213. [Google Scholar] [CrossRef]
- Liistro, F.; Porto, I.; Angioli, P.; Grotti, S.; Ricci, L.; Ducci, K.; Falsini, G.; Ventoruzzo, G.; Turini, F.; Bellandi, G.; et al. Drug-eluting balloon in peripheral intervention for below the knee angioplasty evaluation (DEBATE-BTK): a randomized trial in diabetic patients with critical limb ischemia. Circulation 2013, 128, 615–621. [Google Scholar] [CrossRef]
- Liistro, F.; Grotti, S.; Porto, I.; Angioli, P.; Ricci, L.; Ducci, K.; Falsini, G.; Ventoruzzo, G.; Turini, F.; Bellandi, G.; et al. Drug-eluting balloon in peripheral intervention for the superficial femoral artery: the DEBATE-SFA randomized trial (drug eluting balloon in peripheral intervention for the superficial femoral artery). JACC Cardiovasc Interv 2013, 6, 1295–1302. [Google Scholar] [CrossRef] [PubMed]
- Liistro, F.; Angioli, P.; Porto, I.; Ricci, L.; Ducci, K.; Grotti, S.; Falsini, G.; Ventoruzzo, G.; Turini, F.; Bellandi, G.; et al. Paclitaxel-eluting balloon vs. standard angioplasty to reduce recurrent restenosis in diabetic patients with in-stent restenosis of the superficial femoral and proximal popliteal arteries: the DEBATE- ISR study. J Endovasc Ther 2014, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Liistro, F.; Angioli, P.; Porto, I.; Ducci, K.; Falsini, G.; Ventoruzzo, G.; Ricci, L.; Scatena, A.; Grotti, S.; Bolognese, L. Drug-eluting balloon versus drug-eluting stent for complex femoropopliteal arterial lesions: The drastico study. J Am Coll Cardiol 2019, 74, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Liistro, F.; Angioli, P.; Ventoruzzo, G.; Ducci, K.; Reccia, M.R.; Ricci, L.; Falsini, G.; Scatena, A.; Pieroni, M.; Bolognese, L. Randomized Controlled Trial of Acotec Drug-Eluting Balloon Versus Plain Balloon for Below-the-Knee Angioplasty. JACC Cardiovasc Interv, 2277; 13. [Google Scholar]
- Liistro, F.; Angioli, P.; Reccia, M.R.; Ducci, K.; Falsini, G.; Pieroni, M.; Ventoruzzo, G.; Scatena, A.; Bolognese, L. Long-term mortality in patients undergoing lower-limb revascularization with Paclitaxel eluting devices. Int J Cardiol 2021, 339, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Feldman, D.N.; Armstrong, E.J.; Aronow, H.D.; Gigliotti, O.S.; Jaff, M.R.; Klein, A.J.; Parikh, S.A.; Prasad, A.; Rosenfield, K.; Shishehbor, M.H.; et al. SCAI consensus guidelines for device selection in femoral-popliteal arterial interventions. Catheter Cardiovasc Interv 2018, 92, 124–140. [Google Scholar] [CrossRef]
- Katsanos, K.; Spiliopoulos, S.; Kitrou, P.; Krokidis, M.; Karnabatidis, D. Risk of death following application of paclitaxel-coated balloons and stents in the femoropopliteal artery of the leg: A systematic review and meta-analysis of randomized controlled trials. J Am Heart Assoc 2018, 7, e011245. [Google Scholar] [CrossRef]
- Schneider, P.A.; Laird, J.R.; Doros, G.; Gao, Q.; Ansel, G.; Brodmann, M.; Micari, A.; Shishehbor, M.H.; Tepe, G.; Zeller, T. Mortality Not Correlated With Paclitaxel Exposure: An Independent Patient-Level Meta-Analysis of a Drug-Coated Balloon. J Am Coll Cardiol 2019, 73, 2550–2563. [Google Scholar] [CrossRef]
- Freisinger, E.; Koeppe, J.; Gerss, J.; Goerlich, D.; Malyar, N.M.; Marschall, U.; Faldum, A.; Reinecke, H. Mortality after use of paclitaxel-based devices in peripheral arteries: a real-world safety analysis. Eur Heart J, 3732. [Google Scholar]
- Dake, M.D.; Ansel, G.M.; Bosiers, M.; Holden, A.; Iida, O.; Jaff, M.R.; Lottes, A.E.; O'Leary, E.E.; Saunders, A.T.; Schermerhorn, M.; et al. Paclitaxel-Coated Zilver PTX Drug-Eluting Stent Treatment Does Not Result in Increased Long-Term All-Cause Mortality Compared to Uncoated Devices. Cardiovasc Intervent Radiol 2020, 43, 8–19. [Google Scholar] [CrossRef]
- Secemsky, E.A.; Kundi, H.; Weinberg, I.; Jaff, M.R.; Krawisz, A.; Parikh, S.A.; Beckman, J.A.; Mustapha, J.; Rosenfield, K.; Yeh, R.W. Association of Survival With Femoropopliteal Artery Revascularization With Drug-Coated Devices. JAMA Cardiol 2019, 4, 332–340. [Google Scholar] [CrossRef]
- Hess, C.N.; Patel, M.R.; Bauersachs, R.M.; Anand, S.S.; Debus, E.S.; Nehler, M.R.; Fanelli, F.; Yeh, R.W.; Secemsky, E.A.; Beckman, J.A.; et al. Safety and Effectiveness of Paclitaxel Drug-Coated Devices in Peripheral Artery Revascularization: Insights From VOYAGER PAD. J Am Coll Cardiol 2021, 78(18), 1768–1778. [Google Scholar] [CrossRef]
- Liistro, F.; Angioli, P.; Reccia, M.R.; Ducci, K.; Falsini, G.; Pieroni, M.; Ventoruzzo, G.; Scatena, A.; Bolognese, L. Long-term mortality in patients undergoing lower-limb revascularization with Paclitaxel eluting devices. Int J Cardiol 2021, 339, 150–157. [Google Scholar] [CrossRef]
Figure 1.
Algorithm of the Arezzo fast-track team-based management of CLTI patients with tissue loss. ABI, ankle-brachial index; TcPO2, trancutaneous oxygen pressure; WIfi, Wound-Ischemia-foot Infection classification; CLTI, chronic limb-threatening ischemia; DUS, duplex ultrasound; AGF, angiography; CTA, computerized tomography angiography; CFA, common femoral artery; PTA, percutaneous transluminal angioplasty; BP, bypass; EVR, endovascular revascularization; PBMNC, peripheral bood mononuclear cells.
Figure 1.
Algorithm of the Arezzo fast-track team-based management of CLTI patients with tissue loss. ABI, ankle-brachial index; TcPO2, trancutaneous oxygen pressure; WIfi, Wound-Ischemia-foot Infection classification; CLTI, chronic limb-threatening ischemia; DUS, duplex ultrasound; AGF, angiography; CTA, computerized tomography angiography; CFA, common femoral artery; PTA, percutaneous transluminal angioplasty; BP, bypass; EVR, endovascular revascularization; PBMNC, peripheral bood mononuclear cells.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



