
Submitted:
06 September 2023
Posted:
08 September 2023
You are already at the latest version
Abstract
Abstract: Educating healthcare workers (HCWs) to take action against monkeypox (mpox) is an important part of public health prevention efforts. The study aimed to assess the knowledge, attitudes, and willingness to vaccinate against mpox among HCWs in the Kurdistan Region of Iraq. This study utilized an online cross-sectional survey that was disseminated via Google Forms between November, 1, 2022 and January, 15, 2023, employing a convenience sampling method. The researchers utilized logistic regression to ascertain the factors associated with knowledge, attitude and willingness to vaccinate. A total of 637 HCWs were included in the analysis (ages ranged between 21 and 51 years old). The mean overall score and standard deviation of the knowledge, attitude, and willingness assessment on mpox were 8.18±3.37 out of (0–16), 3.40±1.37 out of (0–5), 2.41±1.25 out of (0–5), respectively. The multivariate logistic regression analysis showed that HCWs who heard about mpox before 2022 had a higher level of knowledge (AOR: 4.85; 95% CI: 2.81-8.36; p < 0.001). In addition, those who had less than 1 year of practice had a positive attitude about mpox (AOR: 0.35; 95% CI: 0.20-0.59; p < 0.01). Finally, none of the variable groups had the capacity to predict willingness to be vaccinated against mpox. The research revealed that HCWs exhibit a relatively low level of knowledge and attitude towards mpox, as well as a low level of willingness to receive mpox vaccinations. Further, there is an urgent need to increase their knowledge and attitude, as the success of efforts to control the global epidemic depends on them.
Keywords:
Monkeypox virus
; mpox
; knowledge
; attitude
; vaccine acceptance
; vaccine hesitancy
; healthcare workers
; doctors
; nurses
; pharmacists
1. Introduction
Beginning in early 2020, the globe was shocked by the COVID-19 pandemic, which has yet not ended, we are dealing with yet another epidemic that has the potential to decimate the humans. In 1958, researchers in Denmark discovered the first incidence of monkeypox virus (MPXV) in a group of monkeys [1]. After that, in 1970, the MPXV, an orthopox DNA virus that is zoonotic, was first discovered in humans in the Democratic Republic of the Congo (formerly Zaire) [2]. Subsequently, the disease emerged endemic throughout West and Central Africa [3,4,5]. Since then, in 2003, the first case of monkeypox (mpox) infection was recorded from endemic to non-endemic nations, caused by an imported rodent from Ghana [3,4,6,7]. Then, the confirmed of mpox cases in the United Kingdom, Israel, and Singapore in 2018 and 2019 was recorded [8,9,10]. In May, 2022, a significant number of cases were reported from nations with no known history of mpox transmission [11]. On 23 July, 2022, the World Health Organization (WHO) declared mpox infection as public health emergency of international concern (PHEIC) [12]. As of July 5, 2023, there have been 88,122 cases confirmed by laboratories, with 148 deaths reported across 112 countries [13]. The mpox outbreak that occurred in 2022 was sporadic in comparison to its prior presentations such as prolonged incubation period (up to 21 days), infection even when outside of an endemic region, prevalence in males, sexual transmission, anogenital lesions, and younger patients [1,2,14,15,16,17,18,19,20].
Humans can contract mpox by direct contact with infected animals, humans, and contaminated surfaces and raw meat [21,22,23,24]. Furthermore, it is possible that squirrels, prairie dogs, and rodents contribute to the spread of MPXV to humans [22,25]. The recent discovery of MPXV transmission from humans to dogs underscores the importance of researching the dynamics of mpox dissemination in depth [26,27]. Although everyone in close contact with infected cases is susceptible to contracting the virus, the present instances seem to be concentrated among men who engage in sexual activity with other men (MSM) [2,18,28]. Despite this, incidences have been observed in females and children [29,30,31,32]. The overwhelming majority of reported cases of mpox in recent studies conducted in the UK and Spain were found to be among MSM [14,18]. Since MSM community are disproportionately affected by mpox, we must pay close attention to the problems of stigma and discrimination, which can be just as devastating as the virus itself [33,34]. However, little is known about the potential risk factors for transmission and infection, zoonotic hosts, and vectors [17,35]. A number of circumstances, including close contact between humans and infected animals, the cessation of smallpox vaccination, and increasing international travel, will make this disease a global public health threat in the future [7,36].
The mpox is a self-limiting disease with a case fatality rate between 1% and 10% [37]. Despite this, there were only a very low number of fatalities during the ongoing outbreak [38]. Symptoms include fever, headache, back pain, myalgia, fatigue, lymphadenopathy, and a variety of skin lesions (including papules, pustules, and ulcers) on the face and body [11,39,40]. The progression of this skin eruption includes the appearance of macules, papules, pustules, vesicles, and finally scabs [41]. Lymphadenopathy appears to be one of the primary features distinguishing monkeypox from smallpox [36]. There are numerous complications associated with mpox, such as keratitis, Paraphimosis, encephalitis, pneumonitis, myocarditis, conjunctivitis and secondary bacterial infections [2,42,43,44,45,46,47,48]. Children, pregnant woman and immunosuppressed individuals, particularly HIV-positive people, are at elevated risk of severe outcomes [49,50,51,52], but whether effective HIV antiretroviral treatment (ART) reduces this risk is uncertain [53].
There is currently not an MPXV-specific vaccine and drugs available for use. Nevertheless, antiviral medications such as Cidofovir, Tecovirimat (TPOXX), Brincidofovir and Vaccinia Immune Globulin Intravenous (VIGIV) have proven to be effective [54,55,56]. The mpox infection cannot be cured with antibiotics, however they can be used to stop and control secondary bacterial infections [45]. The smallpox vaccine, however, offered cross-protection against MPXV [3]. In the fight against the smallpox virus, there have been three different generations of vaccinations used [57]. Up until 2008, the first-generation vaccination was the only one available for protection against smallpox [58,59]. This vaccination was extremely successful at preventing smallpox and played a crucial role in the worldwide elimination of the disease [59]. Some populations considered to be at high risk of contracting orthopoxvirus have benefited from the use of a live attenuated vaccination (second-generation). Third-generation vaccine modified vaccinia Ankara-Bavarian Nordic (MVA-BN) is currently licensed for use in humans in both Europe and Canada [60,61]. Despite the fact that vaccines are crucial for eradicating infectious diseases like monkeypox [62]. Recent reports have indicated that some people are hesitant to be vaccinated in response to the current mpox outbreak [63,64,65,66,67,68,69,70,71]. There are numerous reasons for vaccine hesitancy, including fear of their negative side effects, disinformation and its influence, and distrust of medical staff or the medical system [72,73]. However, healthcare workers' lack of knowledge and unsuitable attitudes might have a negative effect on HCWs' choices, infection prevention, early identification, and prompt intervention [74,75].
When a new infectious disease is discovered, it can be helpful to examine the healthcare workers' current levels of knowledge, attitude, and vaccine hesitancy. This fits with previous findings showing that misinformation about the dangers of new infectious agents can increase anxiety, worry, and even the possibility of conspiratorial thinking [64,76]. In addition, bridging knowledge gaps might be considered a crucial component of an mpox epidemic management [77]. Healthcare workers' knowledge, attitudes and willingness to mpox vaccinate are crucial to the development and implementation of an effective infection control strategy. To this day, there have been relatively few studies carried out on the degree of knowledge and attitudes towards mpox among HCWs, college students, and the general public [38,58,59,63,64,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94]. As far as we are aware, no studies have assessed the level of knowledge of HCWs regarding of mpox in Iraq. Since the mpox epidemic spread quickly, more study is required, particularly among health professionals because of their pivotal role in responding to epidemics [95,96,97].
The Kurdistan Region of Iraq has a population of around 6,000,000 and is located in the Middle East. Despite the fact that mpox has not been recorded in the Kurdistan Region of Iraq as of yet, the rapid growth of cases worldwide and the detection of mpox in other Middle Eastern nations demands for careful planning and response measures [98,99]. Taking into account the major role of healthcare workers in response to the current mpox epidemic [100,101]. The present study aimed to assess the knowledge, attitudes, and willingness to vaccinate for mpox among HCWs in the Kurdistan Region of Iraq.
2. Methods
2.1. Study Design and Setting
This was an analytical cross-sectional study conducted among healthcare workers in Kurdistan-region of Iraq between November, 1, 2022 and January, 15, 2023. This study included Iraqi Kurdistan-registered healthcare workers. These healthcare workers practices in many cities across the region and have different medical specialties.
2.2. Sample Size and Participants
We determined the appropriate size of the sample by utilizing the Raosoft calculator. We established the size of the sample based on the most recent statistics, estimating that there are 30,000 healthcare workers working in the medical field across the Kurdistan region of Iraq [102]. Considering there have been no prior studies in the KRG examining healthcare workers' knowledge of monkeypox, a 50% conservative estimate was used. A minimum of 380 samples were required to achieve a 5% margin of error in a 95% confidence interval. There were 637 total respondents whose data were used for analysis. Our target group comprised doctors, registered nurses, dentists, pharmacists, and medical technicians (MTs), aged 20 or older, willing to participate voluntarily, and residing in the Kurdistan Region of Iraq during the period of the study.
To recruit participants, convenience sampling was utilized. Google Forms were used to create the survey, and participants were recruited using various social media channels (WhatsApp, Telegram, Twitter, Instagram and Facebook). Each respondent was required to provide their informed consent by clicking on the agreement statement before starting to fill out the answers. All of the questions needed to be answered for the submission to be considered valid. For submitting the questionnaires, participants received no benefits or rewards. Moreover, participation was totally on a voluntary basis. To ensure confidentiality, participants' identities were not collected. The entire process of filling out the questionnaire required a total of ten minutes.
2.3. Study Tools
The researchers used a structured questionnaire with 34 items, including sociodemographic. The research questionnaire was developed based on the previously published studies addressing mpox knowledge, attitude, and willingness to mpox vaccinate [70,71,88,90,93,103]. The questionnaire was drafted in English and Kurdish (the local language). The questionnaire was translated to Kurdish language by different experts (Virologists, epidemiologists). A forward-backwards translation from English to Kurdish ensured precise results. There were four main parts to the questionnaire, as outlined below:
The first part included 8-items about sociodemographic data such as age, gender, marital status, highest educational level (undergraduate and postgraduate), duration of practice (in years), occupational category (Doctor, Dentist, Pharmacist, Nurse or other medical technicians), place of residence (the capital and outside the capital) and one “Yes” and “No” question about hearing mpox before 2022.
The second part included 16-items about mpox knowledge related to transmission of mpox, prevention, treatment and vaccination. The third part included 5-items about attitudes toward of mpox. The fourth part included 5-items related willingness to mpox vaccination.
On October 29, 2022, among 44 participants pilot study was conducted to assess the questionnaire's reliability (the results were excluded from final analysis). For the purpose of determining whether or not the items have a consistent internal structure, Cronbach's alpha was utilized. Cronbach's alpha was 0.77 for the knowledge scale, 0.74 for the attitude scale, and 0.75 for the willingness to mpox vaccinate scale. The overall Cronbach's alpha for the full questionnaire was 0.75, which demonstrates an appropriate level of internal consistency [104].
2.4. Study Variables
There were 16 questions on the knowledge part, and the choices were "Correct", "Incorrect," and "Don't Know". The score of 1 represented a "correct" response, and 0 represented an "Incorrect" or "Don't Know" response. Responses to inverted questions were assigned points in reverse (Correct = 0 and Incorrect = 1). Therefore, the overall score ranged from 0-16, with a higher score (12–16) indicating good knowledge and a score below 12 indicating poor knowledge about mpox disease.
The attitude part included 5-itmes, and the response of each item was measured on a 3-point Likert scale. The score 1 represented “Agree”, and 0 represented “Undecided”, or “Disagree”. The overall score ranged from 0-5, with a higher score (4-5) indicating positive attitude and score below 4 indicating a negative attitude toward of mpox disease.
The willingness to mpox vaccinate part included 5-itmes, and the response of each item was measured on a 3-point Likert scale. The score 1 represented “Agree”, and 0 represented “Undecided”, or “Disagree”. The overall score ranged from 0-5, with a higher score (4-5) represent “willing” to receive the mpox vaccine if made available, score below 4 represent “unwilling” to receive the mpox vaccine.
2.5. Ethical Consideration
The ethical approval was granted by the Research Ethics Committee at University of Raparin, College of basic education, department of kindergarten with reference number 78/2023. This research followed the principles outlined in the Declaration of Helsinki. The confidentiality and anonymity of the participants' responses were also guaranteed. The electronic inform consent was obtained from all participants involved the study.
2.6. Data Analysis
All data analysis were performed using IBM SPSS Statistics version 25 (IBM Corporation, Armonk, NY, USA). Categorical variables and sociodemographic characteristics were given as frequencies and percentages. Then, for determining the normality distribution of the data, the Shapiro-Wilk and histogram were applied, and all the variables followed the normal distribution. The standard error of the skewness coefficient and the standard error of the kurtosis coefficient were also utilized in this study to assess the normality of the data. Additionally, the chi square test was used to find out the association between baseline sociodemographic characteristics and scores of knowledge, attitude, and willingness to get vaccinated against mpox. The univariate binary logistic regression analysis was applied, and factors with a p value of <0.25 were selected for the multivariate binary logistic regression analysis. From the binary logistic regression, variables with a significance level of p-value <0.05 and an odds ratio of 95% CI were taken as statistically significant factors that were independently associated with good knowledge, a positive attitude, and willing to receive the vaccination against mpox.
3. Results
3.1. Baseline Characteristics and Demographic Data
A total of 637 participants were analyzed. All of the survey questions had to be answered for it to be submitted successfully. No one of the participants was excluded. The ages ranged between 21 and 51 years old. There were 49.9% males and 50.1% females, and 49.3% of them were single. 96.7% of the participants were undergraduates (diploma or BSc degree). Also, 42.5% of the participants had 1–5 years of experience. The majority of participants (35.6%) were nurses. Whereas 73.9% of the participants were from outside the capital (Erbil). Finally, 60% of the participants reported they heard about mpox before the 2022 outbreak (Table 1).
3.2. Knowledge, Attitude and Willingness to Mpox Vaccinate among HCWs
Table 2 showed that; 74% of the participants answered the question that mpox is a viral disease and 69.5% the question that mpox is a bacterial disease correctly. 68.3% answered the question that mpox is transmitted from one person to another and 69.4% answered the question mpox is transmitted to humans through direct contact from infected animals, correctly. About 59% of the participants reported that mpox infection is associated with typical skin lesions which is correct. Finally, 60.4% replied correctly the question that antivirals are required in the management of human mpox patients.
As shown in the Table 3 the results showed the distribution of the participants response in frequencies and percentage to the variables of attitude and willingness to get the mpox vaccination, 63.4% of the participants reported that they are confident that the world's population can control the mpox worldwide, 76% of the participants showed their interest in learning more about mpox, 66.2% of the participants reported they think that mass media coverage about mpox may have influence on its worldwide prevention, whereas 62.8% of the participants revealed they think that mass media coverage about mpox may have influence on its worldwide prevention, finally, 72.8% of the participants said they think that it is dangerous to travel to the countries epidemic with mpox. For the variables of willingness to get the vaccination for mpox, 62% of the participants reported that they were considering a smallpox vaccine to prevent mpox infection, while 52.3% of the participants said that the recommendation for the vaccination against mpox infection by doctors, the community, and other professionals has a great influence on them.
The mean scores and standard deviation for knowledge, attitude, and willingness were 8.18±3.37, 3.40±1.37, and 2.41±1.25 respectively. Consequently, 116 participants (18.2%) attained a good level of knowledge based on a 75% cutoff [105] (i.e., 12 questions answered correctly), while 319 participants (50.1%) demonstrated a positive attitude toward mpox. Nonetheless, 112 participants (17.6%) willing to receive mpox vaccine if it were provided. (Figure 1).
3.3. Relationships between Baseline Sociodemographic Characteristics and Knowledge, Attitude and Willingness Scores Toward Mpox
Table 4 shows the association between participants' sociodemographic characteristics and their knowledge, attitude toward mpox, and willingness to get the vaccine against mpox. A good knowledge of participants was associated with hearing about mpox before 2022 (p < 0.01). A positive attitude among participants was associated with age groups (p = 0.01), marital status (p < 0.01), duration of practice (p < 0.01), and place of residence (p = 0.03). High attitude scores were common among 31-41 years old participants (56.1%), more than 41 years old (66.9%), males (74%), married (58.9%) and widow/er participants (63.2%), for under graduated both level of attitude were equal (50.0%), whereas for graduated group the positive attitude was high (52.4%), also, high attitude scores were common among nurses (52.9%), physician (54.3%), capital city "Erbil" (57.2%), finally, the participants that heard about mpox before 2022 had high attitude scores (51.3%). Chi square results showed that a willingness toward getting mpox vaccination were not associated with any of the baseline sociodemographic characteristics.
3.4. Univariate Binary Logistic Regression Analysis of Knowledge, Attitude and Willingness to Mpox Vaccination
Table 5, shows the univariate binary logistic regression analysis results and revealed that the only factor which was significantly associated with good knowledge about mpox, was: participants who heard about mpox before 2022 compared with participants who didn’t hear about mpox before 2022 (OR: 4.54; 95% CI: 2.67-7.73; p < 0.01). Also, results showed that factors that were significantly associated with a positive attitude toward mpox were: 21-30 years old participants compared to the participants 31-40 years old (OR:0.51; 95% CI: 0.29-0.89; p = 0.018), participants with less than 1 year of practice compared to the participants who had 1-5 years of practice (OR:27; 95% CI: 0.17-0.42; p < 0.01), and participants who lived outside the capital compared to the participants from the capital city Erbil (OR: 0.67; 95% CI: 0.47-0.96; p = 0.033). Finally, none of the factors was significantly associated with the willingness to be vaccinated against mpox.
3.5:. Multivariate Binary Logistic Regression Analysis of Knowledge, Attitude and Willingness to Mpox Vaccination
In the Table 6 results of the multivariate binary logistic regression analysis showed that participants who heard about mpox before 2022 were more likely to have good knowledge about mpox compared to the participants who didn’t hear about Mpox before 2022 (AOR:4.85; 95% CI: 2.81-8.36; p < 0.001). Also, results showed that participants with less than 1 year of practice were more likely to have positive attitude about mpox compared to participant who had 1-5 years of practice (AOR: 0.35; 95% CI: 0.20-0.59; p < 0.01). Finally, results showed that none of the variable groups had the capacity to predict willingness to be vaccinated against mpox.
4. Discussion
This study represents the first attempt to assess the knowledge, attitudes, and willingness of healthcare workers (HCWs) in the Kurdistan Region of Iraq with respect to human mpox and the associated vaccination, as well as the factors that influence their knowledge, attitudes, and willingness to be vaccinated.
The international healthcare system has faced one of the most significant challenges in recent decades with the outbreak of COVID-19. The pandemic not only overwhelmed healthcare systems worldwide but also put immense strain on healthcare workers who had to provide care for both COVID-19 patients and non-COVID-19 patients [106]. The recovery phase of the COVID-19 pandemic brought hope as vaccination campaigns were initiated to control the spread of the virus. However, just as the healthcare system was starting to regain its footing, the re-emergence of mpox presented a new challenge. The resurgence of mpox during the resolution phase of the COVID-19 pandemic has further strained the healthcare system, especially considering that many infection prevention measures implemented during the COVID-19 pandemic were gradually relaxed or abandoned. This unexpected alert highlights the importance of maintaining a vigilant approach to infectious disease prevention and control measures in healthcare settings [107]. Investigating healthcare workers' knowledge and attitudes related to monkeypox also allows for targeted educational interventions. Identifying knowledge gaps or misconceptions can help develop tailored training programs to enhance their understanding of the disease. By addressing these gaps, healthcare workers can improve their ability to recognize mpox cases accurately, provide appropriate care, and educate patients and the community about preventive measures [108].
Our study has shown that 50.1% of HCW were female, 49.3% of them were single, and 96.7% of the participants were undergraduates (diploma or BSc degree) with 1–5 years of experience.
Also, we found that 60% of HCWs heard about mpox before the 2022 outbreak, which can be attributed to their medical education and training, engagement in professional development activities, and exposure to research and publications. These factors contribute to their overall awareness and knowledge of various infectious diseases.
In this study, gaps in mpox knowledge were most conspicuous for transmitting from one person to another, how to differentiate between mpox and smallpox clinical features, specific vaccines and treatment for mpox. Less than 40% of the HCWs correctly answered these questions. Overall, of HCWs from different categories who participated in this study, more than 80% had poor knowledge. Along the same line, recent studies that assessed HCWs’ knowledge in a Middle Eastern country [88] reported a low level of mpox knowledge among HCWs. In another hand a previous study conducted on HCWs in Saudi Arabia found that overall knowledge about mpox relatively good [109].
The significance of this result is that training HCWs on infectious diseases like mpox enables them to implement effective prevention and control measures, and HCWs trained in mpox are better equipped to recognize the signs and symptoms of the disease. Early detection is vital for initiating appropriate isolation measures and implementing supportive care promptly. Additionally, differentiate monkeypox from other similar conditions, ensuring accurate diagnosis and appropriate management.
In our data analysis, it was found that only 50% of HCWs displayed a positive attitude toward mpox, and 82.4% were not willing to be vaccinated against monkeypox. The attitude of HCWs plays a critical role in the management and control of mpox, HCWs with a positive attitude are more likely to be attentive and proactive in identifying potential cases of monkeypox and will also be an effective communicator with patients and family [108].
The finding of a mpox vaccine acceptance rate of only 17.6% in the study mentioned is significantly lower compared to the pooled estimate from a recent meta-analysis. This meta-analysis involved HCWs plotted in four different studies, which reported an acceptance rate of 63% [110]. The difference in acceptance rates between the study and the meta-analysis raises important considerations regarding mpox vaccination hesitancy among health professionals. It is worth noting that the acceptance rate reported among HCWs in the meta-analysis is higher than the rates reported among the general public worldwide. Lounis and Riad conducted a recent review that highlighted the issue of possible mpox vaccination hesitancy among health professionals despite their relatively higher rates of vaccine acceptance compared to the general public [111]. Furthermore, another recent study among medical workers in China described a majority of participants supporting the promotion of mpox vaccination, mainly among health practitioners and immune-deficient populations [112]. A study conducted on adults in the United States revealed that knowledge levels regarding mpox vaccination were low, and only 46% expressed intentions to get vaccinated if the vaccine was recommended. This suggests a lack of awareness and understanding about the importance and benefits of mpox vaccination [113].
In contrast, the recent study conducted among Pakistani university students aimed to assess their knowledge, attitudes, and willingness to vaccinate against mpox. The findings of the study revealed that there is a relatively high level of willingness among the students to receive mpox vaccination, with 68% expressing their willingness. Additionally, 35% of the participants were willing to pay for the vaccine [114]. Additional study among HCWs in China showed high willingness to get mpox vaccination at a rate of 90%.
Vaccine hesitancy refers to the delay in acceptance or refusal of vaccines, regardless of their availability. It is an intricate phenomenon influenced by various factors such as individual beliefs, attitudes, knowledge, and social influences. Thoughtful vaccine hesitancy among HCWs is crucial, as they play a dynamic role in promoting vaccination and ensuring public health. The organizational aspects within healthcare settings that can affect vaccine acceptance among HCWs, such as vaccine availability, accessibility, and convenience, can impact thier willingness to be vaccinated. Financial barriers can also be addressed by exploring options for making the vaccine more accessible and affordable. This could involve negotiating with vaccine manufacturers for reduced prices or seeking funding from the government or non-governmental organizations to subsidize the cost of vaccination.
Complacency towards mpox vaccination may arise due to a perception that the disease is not a significant threat in certain regions. Another factor contributing to vaccine reluctance could be misinformation or misconceptions about mpox and its vaccine. Misinformation can spread through various channels, including social media platforms, websites, and word-of-mouth [112].
Furthermore, cultural and religious beliefs can also play a role in vaccine reluctance. Some individuals may have concerns about the use of vaccines due to religious or cultural beliefs that discourage medical interventions. These beliefs can vary across different communities and may influence an individual's decision regarding vaccination [105].
Additionally, mistrust in healthcare systems or government authorities can contribute to vaccine hesitancy. If individuals have doubts about the transparency or effectiveness of vaccination campaigns, they may be less likely to trust and comply with recommended immunization practices. Building trust through transparent communication, providing accurate information, and addressing concerns can help mitigate vaccine hesitancy [109]. It is crucial to keep in mind that vaccine reluctance is a complex issue that depends on a variety of factors, some of which can vary across populations and regions. Understanding the specific reasons behind vaccine hesitancy in a particular context is crucial for designing targeted interventions to address these concerns effectively [115].
In this study, we found that good knowledge of HCWs was associated with hearing about mpox before 2022. This suggests that individuals who had prior awareness of mpox were more likely to possess a higher level of knowledge regarding the disease.
Additionally, a positive attitude towards mpox was linked with HCWs age groups 31-41 years old, which showed an even higher percentage (66.9%) of positive attitudes. Marital status was also found to be significantly associated with a positive attitude (p < 0.01). Furthermore, HCWs with longer durations of practice were more likely to have positive attitudes towards mpox.
When considering educational background, the study found that among under graduates, both levels of attitude (positive and negative) were equal, with 50% exhibiting high attitude scores. However, among the graduated group, a higher percentage displayed positive attitudes, at 52.4%. In terms of professional backgrounds, nurses had a relatively high prevalence of positive attitudes, with 52.9% scoring high on attitude measures. Physicians also showed a significant proportion of positive attitudes at 54.3%. Lastly, we found that geographically, the capital city (Erbil) had a relatively higher percentage of participants with positive attitudes at 57.2%.
In the current survey, a multivariate logistic regression analysis was conducted to identify additional determinants that have a significant influence on the different outcomes of interest. Specifically, the analysis revealed that the number of years of working activity in the healthcare profession and gender were predictive factors for knowledge and attitude among the sampled healthcare workers (HCWs). One possible explanation for less experienced HCWs being more active in acquiring information, reading scientific journals, and participating in recent proper training and education compared to those with more years of activity is their higher level of enthusiasm and motivation. Additionally, less experienced HCWs may have a stronger desire to establish themselves professionally and build a solid foundation of knowledge and skills. Furthermore, younger HCWs who are just starting their careers may be more comfortable with technology and digital platforms, which can facilitate access to scientific journals, online courses, webinars, and other educational resources. They may be more adept at utilizing these tools for self-directed learning compared to their more experienced counterparts, who may have been trained in a different era.
Attitudes and willingness to be vaccinated can vary based on the type of vaccine and the population of interest. This study emphasizes the need for special attention to the intricate details surrounding this topic. It acknowledges that previous evidence suggests that vaccine mandates may not always be effective due to the divided opinion among the general public and healthcare workers (HCWs), who can play a crucial role in advocating for such strategies [116,117].
5. Strengths and Limitations
A major strength of this study lies in its ability to collect data from a representative sample of different hospitals inside the Kurdistan region, to provide overview of knowledge gaps, attitudes and mpox vaccine willingness among HCWs. These gaps and attitudes can significantly impact the effectiveness of public health interventions and the overall control of the outbreak.
This study's limitations included, firstly, the cross-sectional design of the survey, which is a significant limitation. A cross-sectional study collects data at a single point in time, providing a snapshot of a population or phenomenon. While this design allows for the examination of associations between variables, it does not establish causality. Additionally, one potential limitation of using self-administered questionnaires is that participants may feel pressured to present themselves in a positive light or conform to societal norms. This can result in respondents providing answers that they believe are more socially acceptable rather than reflecting their true thoughts, feelings, or behaviors.
6. Conclusion
A gab of knowledge levels was found among HCWs toward mpox; one of the primary challenges in identifying and managing mpox cases is the lack of awareness among healthcare professionals and the general public. Without adequate knowledge about the signs, symptoms, and transmission of mpox, it becomes difficult to recognize and respond to potential cases effectively. This can lead to delays in diagnosis, treatment, and containment measures, allowing the pathogen to spread further. This can be achieved through the implementation of proper and timely awareness campaigns, educational courses, workshops, and alerts and equipping HCWs with a comprehensive understanding of mpox, and enhancing their ability to provide high-quality and safe patient care. Furthermore, it is essential to establish vigorous surveillance systems that enable early detection of mpox cases. These systems should involve close collaboration between healthcare facilities, laboratories, public health agencies, and other relevant stakeholders. By implementing real-time monitoring and reporting mechanisms, potential mpox cases can be identified promptly, allowing for timely intervention and containment measures.
One of the key actions that can be taken to combat the negative impact of endorsing vaccination hesitancy is education and awareness regarding the vaccine components, effects and, importance for both HCWs and the general population. Moreover, social media platforms should collaborate with public health organizations to ensure that accurate and up-to-date information is readily available to users, through partnerships that involve sharing verified information, promoting official health guidelines, and providing resources for users.
Author Contributions
Conceptualization, SKA; data curation, SKA, and SOA; formal analysis, SOA and SKA; funding acquisition, SKA; investigation, SKA; methodology, SKA and SOA; project administration, SKA; resources, SKA, SOA, MGM, SH, KQ,HTAB, MLF and RMO; software, SKA, SH and SOA; supervision, SKA; validation, SKA, SOA, SH, KQ, MLF, HTAB and RMO; visualization, SKA, MGM, HTAB, SH, RMO, KQ, MLF and SOA; writing—original draft, SKA, SOA, RMO and MGM; writing—review and editing, SKA, SOA, RMO, SH, KQ, HTAB, MLF and MGM. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
This study followed the Institutional Research Ethics Board and the Declaration of Helsinki guideline. The Ethical Review Committee of the University of Raparin College of basic education, department of kindergarten approved this study (Ref: 78/2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is available from the corresponding author upon reasonable request.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Parker, S.; Buller, R.M. A Review of Experimental and Natural Infections of Animals with Monkeypox Virus between 1958 and 2012. Future Virol 2013, 8, 129–157. [CrossRef]
- Thornhill, J.P.; Barkati, S.; Walmsley, S.; Rockstroh, J.; Antinori, A.; Harrison, L.B.; Palich, R.; Nori, A.; Reeves, I.; Habibi, M.S. Monkeypox Virus Infection in Humans across 16 Countries—April–June 2022. N Engl J Med 2022, 387, 679–691. [CrossRef]
- Parker, S.; Nuara, A.; Buller, R.M.L.; Schultz, D.A. Human Monkeypox: An Emerging Zoonotic Disease. Future Microbiol 2007, 2, 17–34. [CrossRef]
- Yinka-Ogunleye, A.; Aruna, O.; Dalhat, M.; Ogoina, D.; McCollum, A.; Disu, Y.; Mamadu, I.; Akinpelu, A.; Ahmad, A.; Burga, J. Outbreak of Human Monkeypox in Nigeria in 2017–18: A Clinical and Epidemiological Report. Lancet Infect Dis 2019, 19, 872–879. [CrossRef]
- Damon, I.K.; Roth, C.E.; Chowdhary, V. Discovery of Monkeypox in Sudan. N Engl J Med 2006, 355, 962–963. [CrossRef]
- Centres for Disease Control and Prevention (CDC). Monkeypox- Past U.S. Cases and Outbreaks Available online: https:%0A//www.cdc.gov/poxvirus/monkeypox/outbreak/us-outbreaks.html (accessed on 20 January 2023).
- Damon, I.K. Status of Human Monkeypox: Clinical Disease, Epidemiology and Research. Vaccine 2011, 29, D54–D59. [CrossRef]
- Vaughan, A.; Aarons, E.; Astbury, J.; Balasegaram, S.; Beadsworth, M.; Beck, C.R.; Chand, M.; O’connor, C.; Dunning, J.; Ghebrehewet, S. Two Cases of Monkeypox Imported to the United Kingdom, September 2018. Eurosurveillance 2018, 23, 1800509. [CrossRef]
- Erez, N.; Achdout, H.; Milrot, E.; Schwartz, Y.; Wiener-Well, Y.; Paran, N.; Politi, B.; Tamir, H.; Israely, T.; Weiss, S. Diagnosis of Imported Monkeypox, Israel, 2018. Emerg Infect Dis 2019, 25, 980. [CrossRef]
- Yong, S.E.F.; Ng, O.T.; Ho, Z.J.M.; Mak, T.M.; Marimuthu, K.; Vasoo, S.; Yeo, T.W.; Ng, Y.K.; Cui, L.; Ferdous, Z. Imported Monkeypox, Singapore. Emerg Infect Dis 2020, 26, 1826. [CrossRef]
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The Changing Epidemiology of Human Monkeypox—A Potential Threat? A Systematic Review. PLoS Negl Trop Dis 2022, 16, e0010141. [CrossRef]
- Nuzzo, J.B.; Borio, L.L.; Gostin, L.O. The WHO Declaration of Monkeypox as a Global Public Health Emergency. Jama 2022, 328, 615–617. [CrossRef]
- Centres for Disease Control and Prevention (CDC). 2022 Mpox Outbreak Global Map Available online: https://www.cdc.gov/poxvirus/monkeypox/response/2022/world-map.html (accessed on 20 January 2023).
- Patel, A.; Bilinska, J.; Tam, J.C.H.; Fontoura, D.D.S.; Mason, C.Y.; Daunt, A.; Snell, L.B.; Murphy, J.; Potter, J.; Tuudah, C. Clinical Features and Novel Presentations of Human Monkeypox in a Central London Centre during the 2022 Outbreak: Descriptive Case Series. bmj 2022, 378. [CrossRef]
- Mileto, D.; Riva, A.; Cutrera, M.; Moschese, D.; Mancon, A.; Meroni, L.; Giacomelli, A.; Bestetti, G.; Rizzardini, G.; Gismondo, M.R. New Challenges in Human Monkeypox Outside Africa: A Review and Case Report from Italy. Travel Med Infect Dis 2022, 102386. [CrossRef]
- Miura, F.; van Ewijk, C.E.; Backer, J.A.; Xiridou, M.; Franz, E.; de Coul, E.O.; Brandwagt, D.; van Cleef, B.; van Rijckevorsel, G.; Swaan, C. Estimated Incubation Period for Monkeypox Cases Confirmed in the Netherlands, May 2022. Eurosurveillance 2022, 27, 2200448. [CrossRef]
- Adler, H.; Gould, S.; Hine, P.; Snell, L.B.; Wong, W.; Houlihan, C.F.; Osborne, J.C.; Rampling, T.; Beadsworth, M.B.J.; Duncan, C.J.A. Clinical Features and Management of Human Monkeypox: A Retrospective Observational Study in the UK. Lancet Infect Dis 2022, 22, P1153-1162. [CrossRef]
- Tarín-Vicente, E.J.; Alemany, A.; Agud-Dios, M.; Ubals, M.; Suñer, C.; Antón, A.; Arando, M.; Arroyo-Andrés, J.; Calderón-Lozano, L.; Casañ, C. Clinical Presentation and Virological Assessment of Confirmed Human Monkeypox Virus Cases in Spain: A Prospective Observational Cohort Study. Lancet 2022, 400, 661–669. [CrossRef]
- Girometti, N.; Byrne, R.; Bracchi, M.; Heskin, J.; McOwan, A.; Tittle, V.; Gedela, K.; Scott, C.; Patel, S.; Gohil, J. Demographic and Clinical Characteristics of Confirmed Human Monkeypox Virus Cases in Individuals Attending a Sexual Health Centre in London, UK: An Observational Analysis. Lancet Infect Dis 2022, 22, 1321–1328. [CrossRef]
- Thornhill, J.P.; Palich, R.; Ghosn, J.; Walmsley, S.; Moschese, D.; Cortes, C.P.; Galliez, R.M.; Garlin, A.B.; Nozza, S.; Mitja, O. Human Monkeypox Virus Infection in Women and Non-Binary Individuals during the 2022 Outbreaks: A Global Case Series. Lancet 2022. [CrossRef]
- Heskin, J.; Belfield, A.; Milne, C.; Brown, N.; Walters, Y.; Scott, C.; Bracchi, M.; Moore, L.S.; Mughal, N.; Rampling, T. Transmission of Monkeypox Virus through Sexual Contact-A Novel Route of Infection. J Infect 2022, 83, 334–363. [CrossRef]
- Parvin, R.; Ali, A. Monkeypox Virus: A Comprehensive Review of Taxonomy, Evolution, Epidemiology, Diagnosis, Prevention, and Control Regiments so Far. Ger. [CrossRef]
- Reynolds, M.G.; Damon, I.K. Outbreaks of Human Monkeypox after Cessation of Smallpox Vaccination. Trends Microbiol 2012, 20, 80–87. [CrossRef]
- Le Pluart, D.; Ruyer-Thompson, M.; Ferré, V.M.; Mailhe, M.; Descamps, D.; Bouscarat, F.; Lescure, F.-X.; Lucet, J.-C.; Yazdanpanah, Y.; Ghosn, J. A Healthcare-Associated Infection with Monkeypox Virus of a Healthcare Worker during the 2022 Outbreak. In Proceedings of the Open Forum Infectious Diseases; Oxford University Press US, 2022; Vol. 9, p. ofac520. [CrossRef]
- Tiecco, G.; Degli Antoni, M.; Storti, S.; Tomasoni, L.R.; Castelli, F.; Quiros-Roldan, E. Monkeypox, a Literature Review: What Is New and Where Does This Concerning Virus Come From? Viruses 2022, 14, 1894. [CrossRef]
- Sah, R.; Hada, V.; Mohanty, A.; Alshahrani, N.Z.N.; Chakraborty, S.; Bhattacharya, M.; Chakraborty, C.; Dhama, K. Recent First Report of Human-to-Dog Transmission of Monkeypox Virus Emphasizes an Urgent Need of Enhancing Surveillance and Strengthen Further Explorative Research to Reveal Its Real Magnitude of Reverse Zoonosis from Other Animals Including Pets as Like. Int J Surg 2022, 106, 106949. [CrossRef]
- Seang, S.; Burrel, S.; Todesco, E.; Leducq, V.; Monsel, G.; Le Pluart, D.; Cordevant, C.; Pourcher, V.; Palich, R. Evidence of Human-to-Dog Transmission of Monkeypox Virus. Lancet 2022, 400, 658–659. [CrossRef]
- Martínez, J.I.; Montalbán, E.G.; Bueno, S.J.; Martínez, F.M.; Juliá, A.N.; Díaz, J.S.; Marín, N.G.; Deorador, E.C.; Forte, A.N.; García, M.A. Monkeypox Outbreak Predominantly Affecting Men Who Have Sex with Men, Madrid, Spain, 26 April to 16 June 2022. Eurosurveillance 2022, 27, 2200471. [CrossRef]
- Bragazzi, N.L.; Woldegerima, W.A.; Iyaniwura, S.A.; Han, Q.; Wang, X.; Shausan, A.; Badu, K.; Okwen, P.; Prescod, C.; Westin, M.; et al. Knowing the Unknown: The Underestimation of Monkeypox Cases. Insights and Implications from an Integrative Review of the Literature. Front Microbiol 2022, 13, 1011049. [CrossRef]
- Vivancos, R.; Anderson, C.; Blomquist, P.; Balasegaram, S.; Bell, A.; Bishop, L.; Brown, C.S.; Chow, Y.; Edeghere, O.; Florence, I. Community Transmission of Monkeypox in the United Kingdom, April to May 2022. Eurosurveillance 2022, 27, 2200422. [CrossRef]
- Vusirikala, A.; Charles, H.; Balasegaram, S.; Macdonald, N.; Kumar, D.; Barker-Burnside, C.; Cumiskey, K.; Dickinson, M.; Watson, M.; Olufon, O. Epidemiology of Early Monkeypox Virus Transmission in Sexual Networks of Gay and Bisexual Men, England, 2022. Emerg Infect Dis 2022, 28, 2082–2086. [CrossRef]
- van Furth, A.M.T.; van der Kuip, M.; van Els, A.L.; Fievez, L.C.R.; van Rijckevorsel, G.G.C.; van den Ouden, A.; Jonges, M.; Welkers, M.R.A. Paediatric Monkeypox Patient with Unknown Source of Infection, the Netherlands, June 2022. Eurosurveillance 2022, 27, 2200552. [CrossRef]
- Ahmed, S.K.; Abdulqadir, S.O.; Hussein, S.H.; Omar, R.M.; Ahmed, N.A.; Essa, R.A.; Dhama, K.; Lorenzo, J.M.; Abdulla, A.Q. The Impact of Monkeypox Outbreak on Mental Health and Counteracting Strategies: A Call to Action. Int J Surg 2022, 106, 106943. [CrossRef]
- Bragazzi, N.L.; Khamisy-Farah, R.; Tsigalou, C.; Mahroum, N.; Converti, M. Attaching a Stigma to the LGBTQI+ Community Should Be Avoided during the Monkeypox Epidemic. J Med Virol 2023, 95, e27913. [CrossRef]
- Peterson, B.W.; Damon, I.K. Orthopoxviruses: Vaccinia (Smallpox Vaccine), Variola (Smallpox), Monkeypox, and Cowpox. In Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. 8th ed. Philadelphia: Elsevier; 2019.
- Brown, K.; Leggat, P.A. Human Monkeypox: Current State of Knowledge and Implications for the Future. Trop Med Infect Dis 2016, 1, 8. [CrossRef]
- Ahmed, S.K.; Rashad, E.A.A.; Mohamed, M.G.; Ravi, R.K.; Essa, R.A.; Abdulqadir, S.O.; Khdir, A.A. The Global Human Monkeypox Outbreak in 2022: An Overview. Int J Surg 2022, 104, 106794. [CrossRef]
- Nath, S.D.; Majumder, K.; Rimti, F.H.; Das, J.; Tabassum, M.N.; Oishee, A.N.; Mahmood, T.; Paul, M.; Akhter, M.; Bhadra, A.B. Assessment of Knowledge on Human Monkeypox Virus among General Population in Bangladesh: A Nationwide Cross-Sectional Study. medRxiv 2022. [CrossRef]
- Vaughan, A.; Aarons, E.; Astbury, J.; Brooks, T.; Chand, M.; Flegg, P.; Hardman, A.; Harper, N.; Jarvis, R.; Mawdsley, S. Human-to-Human Transmission of Monkeypox Virus, United Kingdom, October 2018. Emerg Infect Dis 2020, 26, 782. [CrossRef]
- Gong, Q.; Wang, C.; Chuai, X.; Chiu, S. Monkeypox Virus: A Re-Emergent Threat to Humans. Virol Sin 2022, 37, 477–482. [CrossRef]
- Philpott, D. Epidemiologic and Clinical Characteristics of Monkeypox Cases—United States, May 17–July 22, 2022. MMWR Morb Mortal Wkly Rep 2022, 71, 1018–1022.
- Ly-Yang, F.; Miranda-Sánchez, A.; Burgos-Blasco, B.; Fernández-Vigo, J.I.; Gegúndez-Fernández, J.A.; Díaz-Valle, D. Conjunctivitis in an Individual with Monkeypox. JAMA Ophthalmol 2022, 140, 1022–1024. [CrossRef]
- Tan, D.H.S.; Jaeranny, S.; Li, M.; Sukhdeo, S.S.; Monge, J.C.; Callejas, M.F.; Hasso, M.; Fattouh, R.; Lalonde, S.D.; Lam, J. Atypical Clinical Presentation of Monkeypox Complicated by Myopericarditis. In Proceedings of the Open Forum Infectious Diseases; 2022; Vol. 9, p. ofac394. [CrossRef]
- Kaler, J.; Hussain, A.; Flores, G.; Kheiri, S.; Desrosiers, D. Monkeypox: A Comprehensive Review of Transmission, Pathogenesis, and Manifestation. Cureus 2022, 14. [CrossRef]
- De Sousa, D.; Frade, J.; Patrocínio, J.; Borges-Costa, J.; Filipe, P. Monkeypox Infection and Bacterial Cellulitis: A Complication to Look For. Int J Infect Dis 2022, 123, 180–182. [CrossRef]
- Milano, E.; Belati, A.; De Santis, L.; Tanese, F.; Vavallo, A.; Dachille, G.; Loconsole, D.; Bavaro, D.F.; Di Gennaro, F.; Chironna, M. First Case of Paraphimosis as a Severe Complication of Monkeypox. Vaccines 2023, 11, 63. [CrossRef]
- Billioux, B.J.; Mbaya, O.T.; Sejvar, J.; Nath, A. Potential Complications of Monkeypox. Lancet Neurol 2022, 21, 872. [CrossRef]
- Ahmed, S.K.; Dabou, E.A.; Abdelsamad, S.; Mohamed, M.G.; Chandran, D.; Chakraborty, S.; Emran, T.B.; Dhama, K. Monkeypox Virus Infection and Myocarditis: A Review of Current Evidence and Possible Pathogenesis. Narra J 2023, 3, e104. [CrossRef]
- Vouga, M.; Nielsen-Saines, K.; Dashraath, P.; Baud, D. The Monkeypox Outbreak: Risks to Children and Pregnant Women. Lancet Child Adolesc Heal 2022, 6, 751–753. [CrossRef]
- Boesecke, C.; Monin, M.B.; van Bremen, K.; Schlabe, S.; Hoffmann, C. Severe Monkeypox-Virus Infection in Undiagnosed Advanced HIV Infection. Infection 2022, 50, 1633–1634. [CrossRef]
- Menezes, Y.R.; Miranda, A.B. de Severe Disseminated Clinical Presentation of Monkeypox Virus Infection in an Immunosuppressed Patient: First Death Report in Brazil. Rev Soc Bras Med Trop 2022, 55, e0392. [CrossRef]
- Ahmed, S.K.; Mohamed, M.G.; Dabou, E.A.A.R.; Abuijlan, I.; Chandran, D.; Nahed, A.; Chopra, H.; Dhama, K. Monkeypox (Mpox) in Immunosuppressed Patients. F1000Research 2023, 12, 127. [CrossRef]
- Ogoina, D.; Iroezindu, M.; James, H.I.; Oladokun, R.; Yinka-Ogunleye, A.; Wakama, P.; Otike-Odibi, B.; Usman, L.M.; Obazee, E.; Aruna, O. Clinical Course and Outcome of Human Monkeypox in Nigeria. Clin Infect Dis 2020, 71, e210–e214. [CrossRef]
- Chakraborty, S.; Chandran, D.; Mohapatra, R.K.; Alagawany, M.; El-Shall, N.A.; Sharma, A.K.; Chakraborty, C.; Dhama, K. Clinical Management, Antiviral Drugs and Immunotherapeutics for Treating Monkeypox. An Update on Current Knowledge and Futuristic Prospects. Int J Surg 2022, 105, 106847. [CrossRef]
- De Clercq, E.; Jiang, Y.; Li, G. Therapeutic Strategies for Human Poxvirus Infections: Monkeypox (Mpox), Smallpox, Molluscipox, and Orf. Travel Med Infect Dis 2022, 52, 102528. [CrossRef]
- Ahmed, S.K.; El-Kader, R.G.A.; Abdulqadir, S.O.; Abdullah, A.J.; Nahed, A.; Chandran, D.; Dey, A.; Emran, T.B.; Dhama, K. Monkeypox Clinical Symptoms, Pathology, and Advances in Management and Treatment Options: An Update. Int J Surg 2023, 109. [CrossRef]
- Walsh, S.R.; Dolin, R. Vaccinia Viruses: Vaccines against Smallpox and Vectors against Infectious Diseases and Tumors. Expert Rev Vaccines 2011, 10, 1221–1240. [CrossRef]
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S. Knowledge of Human Monkeypox Viral Infection among General Practitioners: A Cross-Sectional Study in Indonesia. Pathog Glob Health 2020, 114, 68–75. [CrossRef]
- Meo, S.A.; Al-Khlaiwi, T.; Aljofan, Z.F.; Alanazi, A.I.; Meo, A.S. Public Perceptions of the Emerging Human Monkeypox Disease and Vaccination in Riyadh, Saudi Arabia: A Cross-Sectional Study. Vaccines 2022, 10, 1534. [CrossRef]
- Ilchmann, H.; Samy, N.; Reichhardt, D.; Schmidt, D.; Powell, J.D.; Meyer, T.P.H.; Silbernagl, G.; Nichols, R.; Weidenthaler, H.; De Moerlooze, L. Single and 2-Dose Vaccinations with Modified Vaccinia Ankara-Bavarian Nordic® Induce Durable B Cell Memory Responses Comparable to Replicating Smallpox Vaccines. J Infect Dis 2022, jiac455.
- Islam, M.R.; Hossain, M.J.; Roy, A.; Hasan, A.H.M.N.; Rahman, M.A.; Shahriar, M.; Bhuiyan, M.A. Repositioning Potentials of Smallpox Vaccines and Antiviral Agents in Monkeypox Outbreak: A Rapid Review on Comparative Benefits and Risks. Heal Sci Reports 2022, 5, e798. [CrossRef]
- Russo, A.T.; Berhanu, A.; Bigger, C.B.; Prigge, J.; Silvera, P.M.; Grosenbach, D.W.; Hruby, D. Co-Administration of Tecovirimat and ACAM2000TM in Non-Human Primates: Effect of Tecovirimat Treatment on ACAM2000 Immunogenicity and Efficacy versus Lethal Monkeypox Virus Challenge. Vaccine 2020, 38, 644–654. [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Setiawan, A.M.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P. Acceptance and Willingness to Pay for a Hypothetical Vaccine against Monkeypox Viral Infection among Frontline Physicians: A Cross-Sectional Study in Indonesia. Vaccine 2020, 38, 6800–6806. [CrossRef]
- Aljamaan, F.; Alenezi, S.; Alhasan, K.; Saddik, B.; Alhaboob, A.; Altawil, E.S.; Alshahrani, F.; Alrabiaah, A.; Alaraj, A.; Alkriadees, K. Healthcare Workers’ Worries and Monkeypox Vaccine Advocacy during the First Month of the WHO Monkeypox Alert: Cross-Sectional Survey in Saudi Arabia. Vaccines 2022, 10, 1408. [CrossRef]
- Alshahrani, N.Z.; Alzahrani, F.; Alarifi, A.M.; Algethami, M.R.; Alhumam, M.N.; Ayied, H.A.M.; Awan, A.Z.; Almutairi, A.F.; Bamakhrama, S.A.; Almushari, B.S. Assessment of Knowledge of Monkeypox Viral Infection among the General Population in Saudi Arabia. Pathogens 2022, 11, 904. [CrossRef]
- Riad, A.; Drobov, A.; Rozmarinová, J.; Drapáčová, P.; Klugarová, J.; Dušek, L.; Pokorná, A.; Klugar, M. Monkeypox Knowledge and Vaccine Hesitancy of Czech Healthcare Workers: A Health Belief Model (HBM)-Based Study. Vaccines 2022, 10. [CrossRef]
- Zucman, D.; Fourn, E.; Touche, P.; Majerholc, C.; Vallée, A. Monkeypox Vaccine Hesitancy in French Men Having Sex with Men with PrEP or Living with HIV in France. Vaccines 2022, 10, 1629. [CrossRef]
- Gagneux-Brunon, A.; Dauby, N.; Launay, O.; Botelho-Nevers, E. Attitudes towards Monkeypox Vaccination among Healthcare Workers in France and Belgium: An Element of Complacency? J Hosp Infect 2022, 130, 144–145. [CrossRef]
- Wang, B.; Peng, X.; Li, Y.; Fu, L.; Tian, T.; Liang, B.; Sun, Y.; Chen, Y.; Wu, X.; Liu, Q. Perceptions, Precautions, and Vaccine Acceptance Related to Monkeypox in the Public in China: A Cross-Sectional Survey. J Infect Public Health 2022, 16, 163–170. [CrossRef]
- Sahin, T.K.; Erul, E.; Aksun, M.S.; Sonmezer, M.C.; Unal, S.; Akova, M. Knowledge and Attitudes of Turkish Physicians towards Human Monkeypox Disease and Related Vaccination: A Cross-Sectional Study. Vaccines 2023, 11, 19. [CrossRef]
- Ahmed, S.K.; Abdulqadir, S.O.; Omar, R.M.; Abdullah, A.J.; Rahman, H.A.; Hussein, S.H.; Mohammed Amin, H.I.; Chandran, D.; Sharma, A.K.; Dhama, K. Knowledge, Attitude and Worry in the Kurdistan Region of Iraq during the Mpox (Monkeypox) Outbreak in 2022: An Online Cross-Sectional Study. Vaccines 2023, 11, 610. [CrossRef]
- Bendezu-Quispe, G.; Benites-Meza, J.K.; Urrunaga-Pastor, D.; Herrera-Añazco, P.; Uyen-Cateriano, A.; Rodriguez-Morales, A.J.; Toro-Huamanchumo, C.J.; Hernandez, A. V; Benites-Zapata, V.A. Mass Media Use to Learn About COVID-19 and the Non-Intention to Be Vaccinated Against COVID-19 in Latin America and Caribbean Countries. Front Med 2022, 9, 877764. [CrossRef]
- Rodriguez-Morales, A.J.; Franco, O.H. Public Trust, Misinformation and COVID-19 Vaccination Willingness in Latin America and the Caribbean: Today’s Key Challenges. Lancet Reg Heal 2021, 3, 100073. [CrossRef]
- Omrani, A.S.; Shalhoub, S. Middle East Respiratory Syndrome Coronavirus (MERS-CoV): What Lessons Can We Learn? J Hosp Infect 2015, 91, 188–196. [CrossRef]
- McEachan, R.; Taylor, N.; Harrison, R.; Lawton, R.; Gardner, P.; Conner, M. Meta-Analysis of the Reasoned Action Approach (RAA) to Understanding Health Behaviors. Ann Behav Med 2016, 50, 592–612. [CrossRef]
- Sallam, M.; Dababseh, D.; Yaseen, A.; Al-Haidar, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. Conspiracy Beliefs Are Associated with Lower Knowledge and Higher Anxiety Levels Regarding COVID-19 among Students at the University of Jordan. Int J Environ Res Public Health 2020, 17, 4915. [CrossRef]
- Kluge, H.; Ammon, A. Monkeypox in Europe and beyond–Tackling a Neglected Disease Together. Eurosurveillance 2022, 27, 2200482. [CrossRef]
- Bates, B.R.; Grijalva, M.J. Knowledge, Attitudes, and Practices towards Monkeypox during the 2022 Outbreak: An Online Cross-Sectional Survey among Clinicians in Ohio, USA. J Infect Public Health 2022, 15, 1459–1465. [CrossRef]
- Jairoun, A.A.; Al-Hemyari, S.S.; Abdulla, N.M.; El-Dahiyat, F.; Shahwan, M.; Hassan, N.; Alyousef, N.G.; Sharif, S.; Jaber, A.A.S. Awareness and Preparedness of Human Monkeypox Outbreak among University Student: Time to Worry or One to Ignore? J Infect Public Health 2022, 15, 1065–1071. [CrossRef]
- Lin, G.S.S.; Tan, W.W.; Chan, D.Z.K.; Ooi, K.S.; Hashim, H. Monkeypox Awareness, Knowledge, and Attitude among Undergraduate Preclinical and Clinical Students at a Malaysian Dental School: An Emerging Outbreak during the COVID-19 Era. Asian Pac J Trop Med 2022, 15, 461. [CrossRef]
- Sallam, M.; Eid, H.; Awamleh, N.; Al-Tammemi, A.B.; Barakat, M.; Athamneh, R.Y.; Hallit, S.; Harapan, H.; Mahafzah, A. Conspiratorial Attitude of the General Public in Jordan towards Emerging Virus Infections: A Cross-Sectional Study Amid the 2022 Monkeypox Outbreak. Trop Med Infect Dis 2022, 7, 411. [CrossRef]
- Temsah, M.-H.; Aljamaan, F.; Alenezi, S.; Alhasan, K.; Saddik, B.; Al-Barag, A.; Alhaboob, A.; Bahabri, N.; Alshahrani, F.; Alrabiaah, A. Monkeypox Caused Less Worry than COVID-19 among the General Population during the First Month of the WHO Monkeypox Alert: Experience from Saudi Arabia. Travel Med Infect Dis 2022, 49, 102426. [CrossRef]
- Dong, C.; Yu, Z.; Zhao, Y.; Ma, X. Knowledge and Vaccination Intention of Monkeypox in China’s General Population: A Cross-Sectional Online Survey. Travel Med Infect Dis 2022, 102533. [CrossRef]
- Gonzales-Zamora, J.; Soriano-Moreno, D.R.; Soriano-Moreno, A.N.; Ponce-Rosas, L.; Sangster-Carrasco, L.; De-Los-Rios-Pinto, A.; Benito-Vargas, R.M.; Murrieta-Ruiz, V.; Morocho-Alburqueque, N.; Caira-Chuquineyra, B. Level of Knowledge Regarding Monkeypox among Peruvian Physicians during the 2022 Outbreak: A Cross-Sectional Study. 2022. [CrossRef]
- Salim, N.A.; Septadina, I.S.; Permata, M. Knowledge, Attitude, and Perception of Anticipating 2022 Global Human Monkeypox Infection among Internal Medicine Residents at Palembang Indonesia: An Online Survey. J Kedokt dan Kesehat Publ Ilm Fak Kedokt Univ Sriwij 2022, 9, 253–262. [CrossRef]
- Al-Mustapha, A.I.; Sikiru, N.A.; Kolawole, B.; Oyewo, M.; Ahmed, H.; Odukoya, A.; Ogundijo, O.A.; Asiegbu, E.C.; Nanven, M.B.; Lawal-Atolagbe, T. A Cross-Sectional Survey of Public Knowledge of the Monkeypox Disease in Nigeria. 2022. [CrossRef]
- Ghazy, R.M.; Okeh, D.U.; Sallam, M.; Hussein, M.; Ismail, H.M.; Yazbek, S.; Mahboob, A.; Abd ElHafeez, S. Psychological Antecedents of Healthcare Workers towards Monkeypox Vaccination in Nigeria. Vaccines 2022, 10, 2151. [CrossRef]
- Sallam, M.; Al-Mahzoum, K.; Al-Tammemi, A.B.; Alkurtas, M.; Mirzaei, F.; Kareem, N.; Al-Naimat, H.; Jardaneh, L.; Al-Majali, L.; AlHadidi, A. Assessing Healthcare Workers’ Knowledge and Their Confidence in the Diagnosis and Management of Human Monkeypox: A Cross-Sectional Study in a Middle Eastern Country. In Proceedings of the Healthcare; MDPI, 2022; Vol. 10, p. 1722. [CrossRef]
- Kumar, N.; Ahmed, F.; Raza, M.S.; Rajpoot, P.L.; Rehman, W.; Khatri, S.A.; Mohammed, M.; Muhammad, S.; Ahmad, R. Monkeypox Cross-Sectional Survey of Knowledge, Attitudes, Practices, and Willingness to Vaccinate among University Students in Pakistan. Vaccines 2023, 11, 97. [CrossRef]
- Alsanafi, M.; Al-Mahzoum, K.; Sallam, M. Monkeypox Knowledge and Confidence in Diagnosis and Management with Evaluation of Emerging Virus Infection Conspiracies among Health Professionals in Kuwait. Pathogens 2022, 11, 994. [CrossRef]
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S. Physicians’ Willingness to Be Vaccinated with a Smallpox Vaccine to Prevent Monkeypox Viral Infection: A Cross-Sectional Study in Indonesia. Clin Epidemiol Glob Heal 2020, 8, 1259–1263. [CrossRef]
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S. Confidence in Managing Human Monkeypox Cases in Asia: A Cross-Sectional Survey among General Practitioners in Indonesia. Acta Trop 2020, 206, 105450. [CrossRef]
- Alshahrani, N.Z.; Algethami, M.R.; Alarifi, A.M.; Alzahrani, F.; Sheerah, H.A.; Abdelaal, A.; Sah, R.; Rodriguez-Morales, A.J. Knowledge and Attitude Regarding Monkeypox Virus among Physicians in Saudi Arabia, a Cross-Sectional Study. 2022. [CrossRef]
- Alshahrani, N.Z.; Mitra, S.; Alkuwaiti, A.A.; Alhumam, M.N.; Altmimi, S.M.B.; Alamri, M.H.M.; Albalawi, Z.A.S.; Almorgi, M.W.; Alharbi, H.K.D.; Alshahrani, S.M. Medical Students’ Perception Regarding the Re-Emerging Monkeypox Virus: An Institution-Based Cross-Sectional Study From Saudi Arabia. Cureus 2022, 14. [CrossRef]
- Ogoina, D.; Izibewule, J.H.; Ogunleye, A.; Ederiane, E.; Anebonam, U.; Neni, A.; Oyeyemi, A.; Etebu, E.N.; Ihekweazu, C. The 2017 Human Monkeypox Outbreak in Nigeria—Report of Outbreak Experience and Response in the Niger Delta University Teaching Hospital, Bayelsa State, Nigeria. PLoS ONE 2019, 14, e0214229. [CrossRef]
- Ibrahim, P.K.; Abdulrahman, D.S.; Ali, H.M.; Haji, R.M.; Ahmed, S.K.; Ahmed, N.A.; Abdulqadir, S.O.; Kareem, S.A.; Kamali, A.S.M.A. The 2022 Monkeypox Outbreak—Special Attention to Nurses’ Protection Should Be a Top Priority. Ann Med Surg 2022, 82, 104615. [CrossRef]
- Ahmed, S.K. Prevention, Vaccination, Management and Infection Control of Monkeypox Outbreak: An Update Global Recommendation for the Next Year 2023. J Pure Appl Microbiol 2022, 16, 3189–3191. [CrossRef]
- Ahmed, S.K.; Omar, R.M.; Hussein, S.H.; Ahmed, N.A.; Abdulqadir, S.O.; Essa, R.A.; Dhama, K.; Abdulla, A.Q. Middle East Countries Preparedness for Monkeypox Outbreak: A Call to Action. Int J Surg 2022, 106, 106948. [CrossRef]
- Al-Mandhari, A.; Kodama, C.; Abubakar, A.; Hajjeh, R.; Brennan, R. Monkeypox Outbreak and Response Efforts in the Eastern Mediterranean Region. East Mediterr Heal J 2022, 28, 465–468. [CrossRef]
- Shariq, A.; Rasheed, Z.; Al Abdulmonem, W. Human Monkeypox: An Update on Knowledge and Future Implications. Int J Health Sci (Qassim) 2022, 16, 1–2.
- Koenig, K.L.; Beÿ, C.K.; Marty, A.M. Monkeypox 2022: A Primer and Identify-Isolate-Inform (3I) Tool for Emergency Medical Services Professionals. Prehosp Disaster Med 2022, 1–6. [CrossRef]
- Health, M. of Health Indicators in the Kurdistan Region Available online: https://gov.krd/moh-en/publications/ (accessed on 20 January 2023).
- Riccò, M.; Ferraro, P.; Camisa, V.; Satta, E.; Zaniboni, A.; Ranzieri, S.; Baldassarre, A.; Zaffina, S.; Marchesi, F. When a Neglected Tropical Disease Goes Global: Knowledge, Attitudes and Practices of Italian Physicians towards Monkeypox, Preliminary Results. Trop Med Infect Dis 2022, 7, 135. [CrossRef]
- Taber, K.S. The Use of Cronbach’s Alpha When Developing and Reporting Research Instruments in Science Education. Res Sci Educ 2018, 48, 1273–1296. [CrossRef]
- Malaeb, D.; Sallam, M.; Salim, N.A.; Dabbous, M.; Younes, S.; Nasrallah, Y.; Iskandar, K.; Matta, M.; Obeid, S.; Hallit, S. Knowledge, Attitude and Conspiracy Beliefs of Healthcare Workers in Lebanon towards Monkeypox. Trop Med Infect Dis 2023, 8, 81. [CrossRef]
- Haldane, V.; De Foo, C.; Abdalla, S.M.; Jung, A.-S.; Tan, M.; Wu, S.; Chua, A.; Verma, M.; Shrestha, P.; Singh, S. Health Systems Resilience in Managing the COVID-19 Pandemic: Lessons from 28 Countries. Nat Med 2021, 27, 964–980. [CrossRef]
- Lai, C.-C.; Hsu, C.-K.; Yen, M.-Y.; Lee, P.-I.; Ko, W.-C.; Hsueh, P.-R. Monkeypox: An Emerging Global Threat during the COVID-19 Pandemic. J Microbiol Immunol Infect 2022, 55, 787–794. [CrossRef]
- Miraglia del Giudice, G.; Della Polla, G.; Folcarelli, L.; Napoli, A.; Angelillo, I.F.; Longanella, W.; Mensorio, M.M.; Cantore, F.; Group, C.W. Knowledge and Attitudes of Health Care Workers about Monkeypox Virus Infection in Southern Italy. Front Public Heal 2023, 11, 1091267. [CrossRef]
- Temsah, M.-H.; Aljamaan, F.; Alenezi, S.; Abouammoh, N.; Alhasan, K.; Dasuqi, S.A.; Alhaboob, A.; Hamad, M.A.; Halwani, R.; Alrabiaah, A. Monkeypox Disease (MPOX) Perceptions among Healthcare Workers versus General Population during the First Month of the WHO Alert: Cross-Sectional Survey in Saudi Arabia. Vaccines 2022, 10, 2071. [CrossRef]
- Ulloque-Badaracco, J.R.; Alarcón-Braga, E.A.; Hernandez-Bustamante, E.A.; Al-kassab-Córdova, A.; Benites-Zapata, V.A.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Acceptance towards Monkeypox Vaccination: A Systematic Review and Meta-Analysis. Pathogens 2022, 11, 1248. [CrossRef]
- Lounis, M.; Riad, A. Monkeypox (MPOX)-Related Knowledge and Vaccination Hesitancy in Non-Endemic Countries: Concise Literature Review. Vaccines 2023, 11, 229. [CrossRef]
- Mahameed, H.; Al-Mahzoum, K.; AlRaie, L.A.; Aburumman, R.; Al-Naimat, H.; Alhiary, S.; Barakat, M.; Al-Tammemi, A.B.; Salim, N.A.; Sallam, M. Previous Vaccination History and Psychological Factors as Significant Predictors of Willingness to Receive Mpox Vaccination and a Favorable Attitude towards Compulsory Vaccination. Vaccines 2023, 11, 897. [CrossRef]
- Winters, M.; Malik, A.A.; Omer, S.B. Attitudes towards Monkeypox Vaccination and Predictors of Vaccination Intentions among the US General Public. PLoS ONE 2022, 17, e0278622. [CrossRef]
- Kumar, N.; Ahmed, F.; Raza, M.S.; Rajpoot, P.L.; Rehman, W.; Khatri, S.A.; Mohammed, M.; Muhammad, S.; Ahmad, R. Monkeypox Cross-Sectional Survey of Knowledge, Attitudes, Practices, and Willingness to Vaccinate among University Students in Pakistan. Vaccines 2022, 11, 97. [CrossRef]
- Sahin, T.K.; Erul, E.; Aksun, M.S.; Sonmezer, M.C.; Unal, S.; Akova, M. Knowledge and Attitudes of Turkish Physicians towards Human Monkeypox Disease and Related Vaccination: A Cross-Sectional Study. Vaccines 2022, 11, 19. [CrossRef]
- Neufeind, J.; Schmid-Küpke, N.; Rehfuess, E.; Betsch, C.; Wichmann, O. How a Generally Well-Accepted Measles Vaccine Mandate May Lead to Inequities and Decreased Vaccine Uptake: A Preregistered Survey Study in Germany. BMC Public Health 2022, 22, 1–14. [CrossRef]
- Bardosh, K.; De Figueiredo, A.; Gur-Arie, R.; Jamrozik, E.; Doidge, J.; Lemmens, T.; Keshavjee, S.; Graham, J.E.; Baral, S. The Unintended Consequences of COVID-19 Vaccine Policy: Why Mandates, Passports and Restrictions May Cause More Harm than Good. BMJ Glob Heal 2022, 7, e008684. [CrossRef]
Figure 1.
Percentage distributions of knowledge (good and poor), attitude (positive and negative), and vaccination willingness (yes and no) for pox among health care workers in Kurdistan Region, northern Iraq.
Figure 1.
Percentage distributions of knowledge (good and poor), attitude (positive and negative), and vaccination willingness (yes and no) for pox among health care workers in Kurdistan Region, northern Iraq.
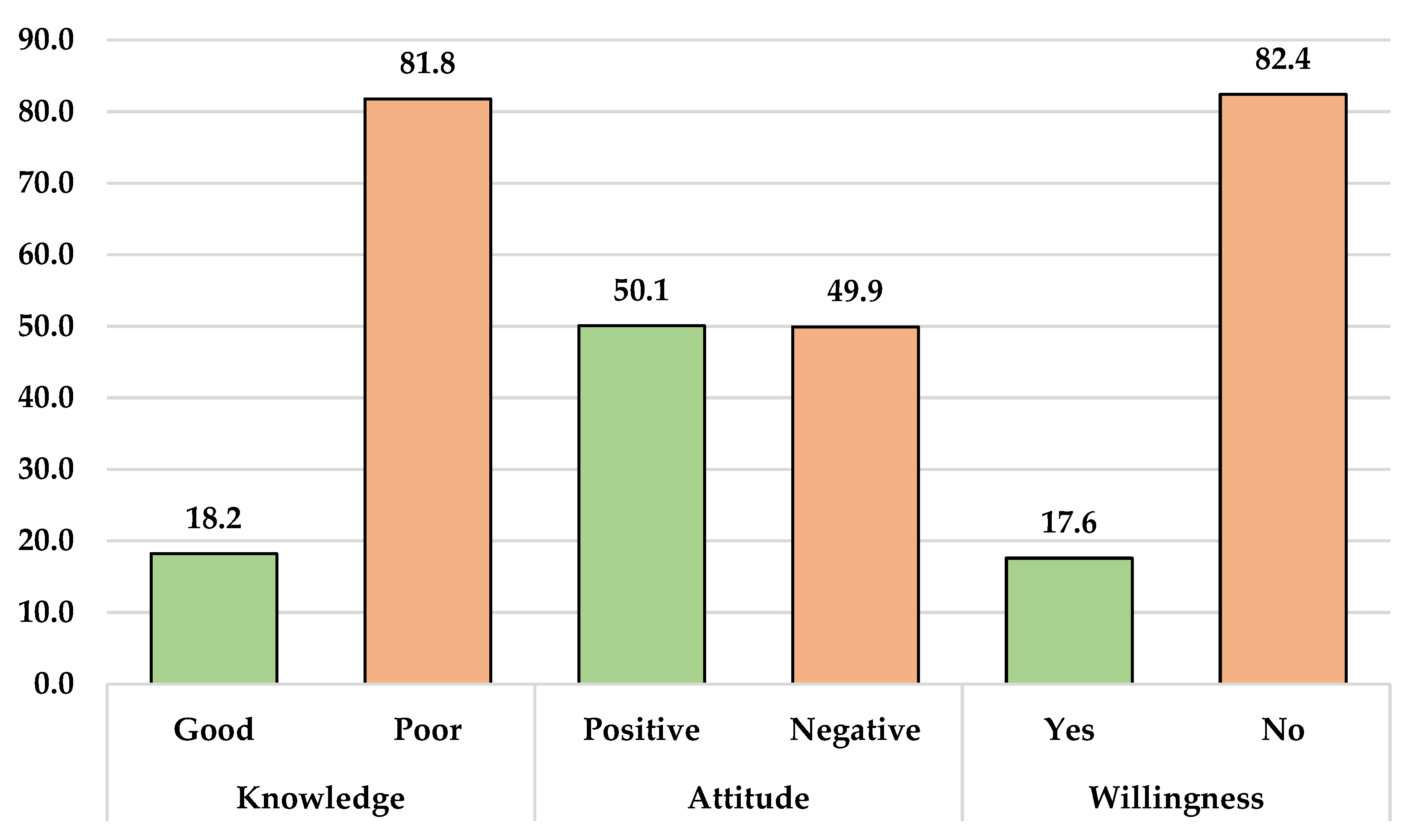

Table 1.
Sociodemographic characteristics of healthcare workers (n= 637).
| Variables | Items | Frequency | Percentage |
|---|---|---|---|
| Age | 21-30 | 401 | 63.0 |
| 31-40 | 173 | 27.2 | |
| 41+ | 63 | 9.8 | |
| Gender | Male | 318 | 49.9 |
| Female | 319 | 50.1 | |
| Marital status | Single | 314 | 49.3 |
| Married | 304 | 47.7 | |
| Widow/er | 19 | 3 | |
| Level of education | Undergraduate (diploma or BSc degree) | 616 | 96.7 |
| Postgraduate (MSc, PhD or its equivalent) | 21 | 3.3 | |
| Work experience | Less than 1 year | 168 | 26.4 |
| 1-5 years | 271 | 42.5 | |
| More than 5 years | 198 | 31.1 | |
| Occupational category | Medical technicians | 130 | 20.4 |
| Nurse | 227 | 35.6 | |
| Pharmacist | 121 | 19.0 | |
| Dentist | 65 | 10.2 | |
| Physician | 94 | 14.8 | |
| Residence area | The capital (Erbil) | 166 | 26.1 |
| Outside the capital | 471 | 73.9 | |
| Heard about human Monkeypox before 2022 | Yes | No | |
| 382 (60%) | 255 (40%) | ||
Table 2.
Knowledge of healthcare workers towards monkeypox (n = 637).
| Knowledge items | Correct answers n (%) |
Incorrect answers n (%) |
|---|---|---|
| Q1. Mpox is a new infection that appeared this year 2022. | 324 (50.9) | 313 (49.1) |
| Q2. Mpox is a viral disease infection. | 476 (74.7) | 161 (25.3) |
| Q3. Mpox is a bacterial disease infection. | 443 (69.5) | 193 (30.3) |
| Q4. Mpox is prevalent in middle eastern countries. | 283 (44.4) | 354 (55.6) |
| Q5. Mpox is prevalent in Western and Central Africa. | 334 (52.4) | 303 (47.6) |
| Q6. There are many human Mpox cases in Iraq. | 328 (51.5) | 309 (48.5) |
| Q7. Mpox is transmitted from one person to another. | 435 (68.3) | 202 (31.7) |
| Q8. Mpox is transmitted to humans through direct contact from infected animals. | 442 (69.4) | 195 (30.6) |
| Q9. Mpox is spread by droplets (coughing and sneezing). | 320 (50.2) | 317 (49.8) |
| Q10. Mpox and smallpox have similar signs and symptoms. | 176 (27.6) | 461 (72.4) |
| Q11. Mpox infection is associated with typical skin lesions. | 377 (59.2) | 260 (40.8) |
| Q12. Lymphadenopathy (swollen lymph nodes) is one clinical sign or symptom that could be used to differentiate Mpox and smallpox cases. | 275 (43.2) | 362 (56.8) |
| Q13. There is a specific vaccine for Mpox. | 195 (30.6) | 442 (69.4) |
| Q14. There is a smallpox vaccine that can be used for Mpox. | 197 (30.9) | 440 (69.1) |
| Q15. There is a specific treatment for Mpox. | 224 (35.2) | 413 (64.8) |
| Q16. Antivirals are required in the management of human Mpox patients. | 385 (60.4) | 252 (39.6) |
Table 3.
Attitude toward of mpox and willingness to vaccinate among HCWs (n = 637).
| Questions No. | Questions |
Agree No. (%) |
Disagree & Undecided No. (%) |
|
| Attitude toward of mpox | ||||
| A1 | I am confident that the world's population can control the Mpox worldwide | 404 (63.4) | 233 (36.6) | |
| A2 | I am interested in learning more about Mpox | 484 (76) | 153 (24.0) | |
| A3 | I think that Mpox can add new burden on healthcare system of the affected countries | 422 (66.2) | 215 (33.8) | |
| A4 | I think that mass media coverage about Mpox may have influence on its worldwide prevention | 400 (62.8) | 237 (37.2) | |
| A5 | I think that it is dangerous to travel to the countries epidemic with Mpox | 460 (72.2) | 177 (27.8) | |
| Willingness of HCWs to mpox vaccination | ||||
| W1 | I'm considering getting the smallpox vaccine to prevent Mpox viral infection | 395 (62) | 242 (38.0) | |
| W2 | The monkeypox infection has been alleviated, and there is no need to be vaccinated against Mpox infection. | 177 (27.8) | 460 (72.2) | |
| W3 | I am worried about the possible side effects of vaccination against Mpox infection | 307 (48.2) | 330 (58.1) | |
| W4 | The recommendation for the vaccination against Mpox infection by doctors, the community and other professionals has a great influence on me. | 333 (52.3) | 188 (29.5) | |
| W5 | If the country provides the vaccination against Mpox infection for free, I am willing to be vaccinated. | 327 (51.3) | 304 (47.7) |
Table 4.
Association between baseline sociodemographic characteristics and knowledge, attitude and willingness scores toward mpox (n = 637).
Table 4.
Association between baseline sociodemographic characteristics and knowledge, attitude and willingness scores toward mpox (n = 637).
|
Variables |
Knowledge | Attitude | Willingness | ||||||||||
| Good |
Poor |
X2 | p-value |
Positive |
Negative |
X2 | p-value |
Yes |
No |
X2 | p-value | ||
| Age (years) | 21-30 | 73 (18.2) | 328 (81.8) | 0.03 | 0.98 | 183 (45.6) | 218 (54.4) | 9.17 | 0.01 | 63 (15.7) | 338 (84.3) | 2.61 | 0.27 |
| 31-40 | 32 (18.5) | 141 (81.5) | 97 (56.1) | 76 (43.9) | 36 (20.8) | 137 (79.2) | |||||||
| 41+ | 11 (17.5) | 52 (82.5) | 39 (61.9) | 24 (38.1) | 13 (20.6) | 50 (79.4) | |||||||
| Gender | Male | 54 (16.9) | 265 (83.1) | 0.70 | 0.40 | 162 (74.0) | 157 (26.0) | 0.12 | 0.72 | 50 (15.7) | 269 (84.3) | 1.60 | 0.20 |
| Female | 62 (19.5) | 256 (80.5) | 157 (49.4) | 161 (50.6) | 62 (19.5) | 256 (80.5) | |||||||
| Marital status | Single | 55 (17.5) | 259 (82.5) | 2.71 | 0.25 | 128 (40.8) | 186 (59.2) | 21.6 | <0.01 | 57 (18.2) | 257 (81.8) | 0.16 | 0.92 |
| Married | 60 (19.7) | 244 (80.3) | 179 (58.9) | 125 (41.1) | 52 (17.1) | 252 (82.9) | |||||||
| Widow\er | 1 (5.3) | 18 (94.7) | 12 (63.2) | 7 (36.8) | 3 (15.8) | 16 (84.2) | |||||||
| Level of education | Under graduated | 115 (18.7) | 501 (81.3) | 2.63 | 0.10 | 308 (50.0) | 308 (50.0) | 0.04 | 0.83 | 109 (17.7) | 507 (82.3) | 0.16 | 0.68 |
| Graduated | 1 (4.8) | 20 (95.2) | 11 (52.4) | 10 (47.6) | 3 (14.3) | 18 (85.7) | |||||||
| Duration of practice | Less than 1 year | 31 (18.5) | 137 (81.5) | 1.54 | 0.46 | 52 (31.0) | 116 (69.0) | 37.0 | <0.01 | 31 (18.5) | 137 (81.5) | 0.31 | 0.85 |
| 1-5 years | 44 (16.2) | 227 (83.8) | 144 (53.1) | 127 (46.9) | 45 (16.6) | 226 (83.4) | |||||||
| More than 5 years | 41 (20.7) | 157 (79.3) | 123 (62.1) | 75 (37.9) | 36 (18.2) | 162 (81.8) | |||||||
| Occupation | Medical technician | 18 (13.8) | 112 (86.2) | 5.77 | 0.21 | 57 (43.8) | 73 (56.2) | 3.48 | 0.48 | 14 (10.8) | 116 (89.2) | 7.63 | 0.10 |
| Nurse | 44 (19.4) | 183 (80.6) | 120 (52.9) | 107 (47.1) | 42 (18.5) | 185 (81.5) | |||||||
| Pharmacist | 29 (24.0) | 92 (76.0) | 59 (48.8) | 62 (51.2) | 22 (18.2) | 99 (81.8) | |||||||
| Dentist | 12 (18.5) | 53 (81.5) | 32 (49.2) | 33 (50.8) | 17 (26.2) | 48 (73.8) | |||||||
| Physician | 13 (13.8) | 81 (86.2) | 51 (54.3) | 43 (45.7) | 17 (18.1) | 77 (81.9) | |||||||
| Place of residence | Outside the capital | 91 (19.3) | 380 (80.7) | 1.49 | 0.21 | 224 (47.6) | 247 (52.4) | 4.59 | 0.03 | 86 (18.3) | 385 (81.7) | 0.57 | 0.45 |
| The Capital (Erbil) | 25 (15.1) | 141 (84.9) | 95 (57.2) | 71 (42.8) | 26 (15.7) | 140 (84.3) | |||||||
| Heard about human Monkeypox before 2022 | Yes | 98 (25.7) | 284 (74.3) | 35.5 | <0.01 | 196 (51.3) | 186 (48.7) | 0.57 | 0.44 | 65 (17.0) | 317 (83.0) | 0.21 | 0.64 |
| No | 18 (7.1) | 237 (92.9) | 123 (48.2) | 132 (51.8) | 47 (18.4) | 208 (81.6) | |||||||
X2 = Chi square.
Table 5.
Univariate binary logistic regression analysis to evaluate the predictive factors associated high knowledge, attitude and willingness scores on mpox (n= 637).
Table 5.
Univariate binary logistic regression analysis to evaluate the predictive factors associated high knowledge, attitude and willingness scores on mpox (n= 637).
|
Items |
Knowledge | Attitude | Willingness | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | ||||
| Age (41+ as ref.) | ||||||||||||
| 21-30 years | 1.05 | 0.52 | 2.11 | 0.887 | 0.51 | 0.29 | 0.89 | 0.018 | 0.71 | 0.36 | 1.39 | 0.328 |
| 31-40 years | 1.07 | 0.50 | 2.28 | 0.855 | 0.78 | 0.43 | 1.41 | 0.423 | 1.01 | 0.49 | 2.06 | 0.977 |
| Gender (Female as ref.) | ||||||||||||
| Male | 0.84 | 0.56 | 1.25 | 0.401 | 1.05 | 0.77 | 1.44 | 0.721 | 0.76 | 0.50 | 1.15 | 0.206 |
| Marital status (Widow\er as ref.) | ||||||||||||
| Single | 3.82 | 0.50 | 29.23 | 0.196 | 0.40 | 0.15 | 1.04 | 0.062 | 1.18 | 0.33 | 4.19 | 0.795 |
| Married | 4.42 | 0.57 | 33.81 | 0.152 | 0.83 | 0.32 | 2.18 | 0.713 | 1.10 | 0.30 | 3.91 | 0.882 |
| Educational level (Post graduate as ref.) | ||||||||||||
| Undergraduate | 0.21 | 0.02 | 1.64 | 0.139 | 0.90 | 0.38 | 2.17 | 0.830 | 1.29 | 0.37 | 4.45 | 0.687 |
| Duration of practice (More than 5 years as ref.) | ||||||||||||
| Less than 1 year | 0.86 | 0.51 | 1.45 | 0.589 | 0.27 | 0.17 | 0.42 | < 0.01 | 1.01 | 0.59 | 1.73 | 0.947 |
| Between 1-5 years | 0.74 | 0.46 | 1.18 | 0.215 | 0.69 | 0.47 | 1.00 | 0.053 | 0.89 | 0.55 | 1.45 | 0.656 |
| Occupation (Physician as ref.) | ||||||||||||
| Medical technical | 1.00 | 0.46 | 2.16 | 0.997 | 0.65 | 0.38 | 1.12 | 0.125 | 0.54 | 0.25 | 1.17 | 0.121 |
| Nurse | 1.49 | 0.76 | 2.93 | 0.238 | 0.94 | 0.58 | 1.53 | 0.820 | 1.02 | 0.55 | 1.91 | 0.930 |
| Pharmacist | 1.96 | 0.95 | 4.03 | 0.066 | 0.80 | 0.46 | 1.37 | 0.424 | 1.00 | 0.50 | 2.02 | 0.985 |
| Dentist | 1.41 | 0.59 | 3.32 | 0.432 | 0.81 | 0.43 | 1.54 | 0.533 | 1.60 | 0.74 | 3.44 | 0.225 |
| Residence (The Capital “Erbil” as ref.) | ||||||||||||
| Outside the capital | 1.35 | 0.83 | 2.18 | 0.223 | 0.67 | 0.47 | 0.96 | 0.033 | 1.20 | 0.74 | 1.94 | 0.450 |
| Heard about mpox before 2022 (No as ref.) | ||||||||||||
| Yes | 4.54 | 2.67 | 7.73 | < 0.01 | 1.13 | 0.82 | 1.55 | 0.447 | 0.90 | 0.60 | 1.37 | 0.64 |
OR= odds ratio, CI= confidence interval, P= p-value.
Table 6.
Multivariate binary logistic regression analysis to evaluate the predictive factors associated high knowledge, attitude and willingness scores on mpox (n= 637).
Table 6.
Multivariate binary logistic regression analysis to evaluate the predictive factors associated high knowledge, attitude and willingness scores on mpox (n= 637).
|
Items |
Knowledge | Attitude | Willingness | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AOR | 95% CI | P | AOR | 95% CI | P | AOR | 95% CI | P | ||||
| Age (41+ as ref.) | ||||||||||||
| 21-30 years | - | - | - | - | 0.95 | 0.51 | 1.77 | 0.887 | - | - | - | - |
| 31-40 years | - | - | - | - | 0.91 | 0.49 | 1.68 | 0.778 | - | - | - | - |
| Gender (Female as ref.) | ||||||||||||
| Male | - | - | - | - | - | - | - | - | 0.78 | 0.51 | 1.20 | 0.268 |
| Marital status (Widow\er as ref.) | ||||||||||||
| Single | 2.99 | 0.37 | 23.90 | 0.302 | 0.48 | 0.17 | 1.32 | 0.158 | - | - | - | - |
| Married | 3.42 | 0.42 | 27.37 | 0.246 | 0.70 | 0.26 | 1.88 | 0.481 | - | - | - | - |
| Educational level (Post graduate as ref.) | ||||||||||||
| Undergraduate | 4.45 | 0.56 | 35.15 | 0.156 | - | - | - | - | - | - | - | - |
| Duration of practice (More than 5 years as ref.) | ||||||||||||
| Less than 1 year | 0.95 | 0.50 | 1.79 | 0.875 | 0.35 | 0.20 | 0.59 | < 0.01 | - | - | - | - |
| Between 1-5 years | 0.75 | 0.44 | 1.28 | 0.299 | 0.79 | 0.51 | 1.22 | 0.294 | - | - | - | - |
| Occupation (Physician as ref.) | ||||||||||||
| Medical technical | 1.19 | 0.53 | 2.68 | 0.664 | 0.74 | 0.42 | 1.31 | 0.314 | 0.56 | 0.26 | 1.20 | 0.139 |
| Nurse | 1.82 | 0.89 | 3.72 | 0.099 | 1.07 | 0.64 | 1.79 | 0.787 | 1.03 | 0.55 | 1.93 | 0.916 |
| Pharmacist | 1.81 | 0.85 | 3.86 | 0.122 | 0.83 | 0.47 | 1.46 | 0.529 | 0.96 | 0.47 | 1.94 | 0.918 |
| Dentist | 1.51 | 0.62 | 3.70 | 0.360 | 0.83 | 0.42 | 1.61 | 0.586 | 1.62 | 0.75 | 3.47 | 0.215 |
| Residence (The Capital “Erbil” as ref.) | ||||||||||||
| Outside the capital | 1.38 | 0.82 | 2.31 | 0.215 | 0.81 | 0.55 | 1.19 | 0.294 | - | - | - | - |
| Heard about mpox before 2022 (No as ref.) | ||||||||||||
| Yes | 4.85 | 2.81 | 8.36 | <0.001 | - | - | - | - | - | - | - | - |
AOR: adjusted odds ratio; ref.: reference; CI: confidence interval, P= p-value.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



