
Submitted:
23 August 2023
Posted:
24 August 2023
You are already at the latest version
Abstract
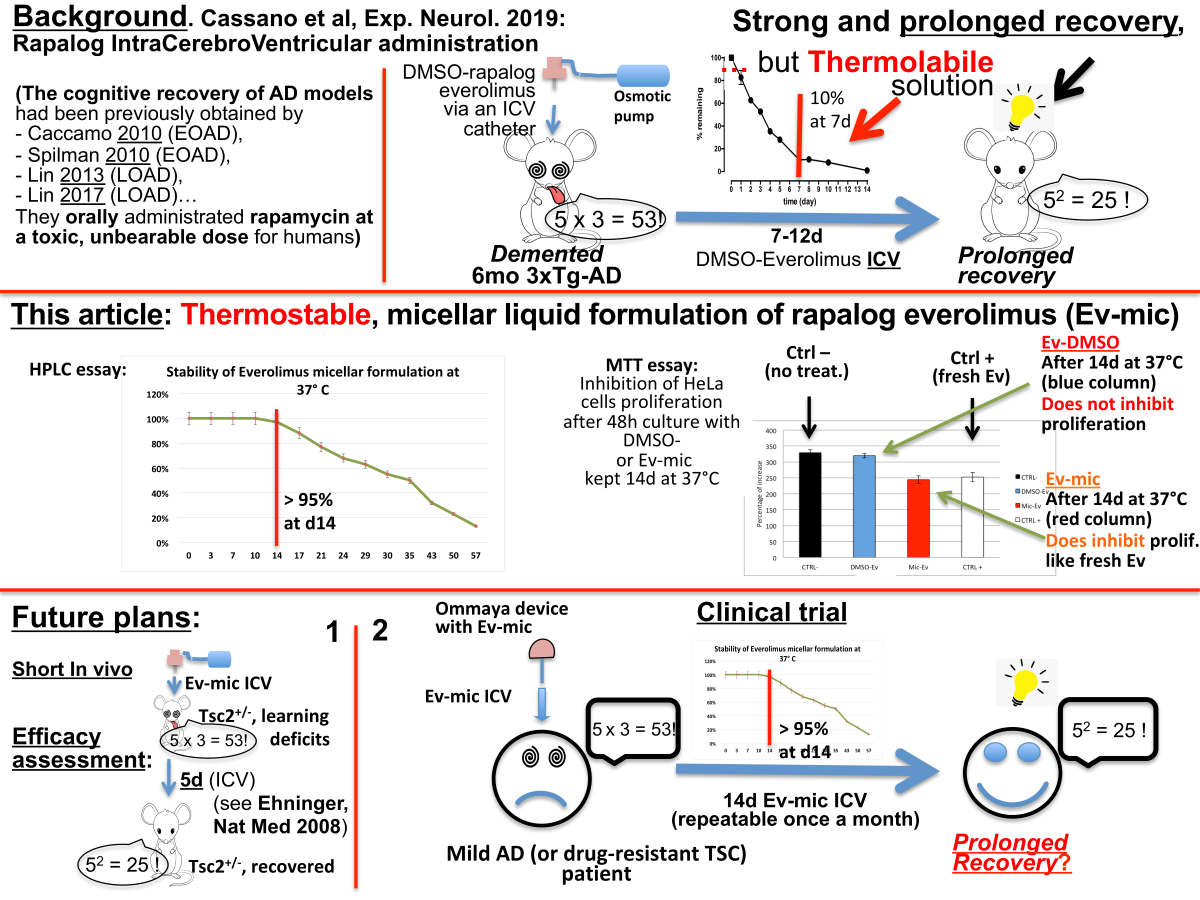
A large body of evidence, replicated in many mouse models of Alzheimer Disease (AD), demonstrated the therapeutic efficacy of oral rapamycin. Administration of m-TOR inhibitors (mTOR-Is), early after the clinical onset, greatly diminished cognitive impairment, amyloid angiopathy, intracellular beta Amyloid and neurofibrillary tangles load. The daily intake of rapamycin has always been 2.24g/Kg/24h. In humans the maximal tolerated oral dose is a few milligrams/day, and at this dosage patients are severely immunosuppressed. Thanks to rapalogs’ scarce CNS-related side effects, we administered intracerebroventricularly (ICV) high doses of the mTOR-I everolimus in a mouse model of AD (3xTg-AD) without significant systemic effects. The instability of the liquid formulation at body temperature (BT) made the treatment very short. Nevertheless, the efficacy of the treatment was high and much longer lasting than expected. In order to set up a thermostable, translational liquid formulation of mTOR-Is, we loaded everolimus in distearoylphosphatidylethanolamine-polyethylene glycol 2000 (DSPE-PEG2000) micelles by the thin layer method. The formulation we obtained maintained over 95% of activity after 14 days at BT. We can envision short, potentially periodic ICV treatments in AD patients which replicate results obtained on animal models. The treatment could benefit also Tuberous Sclerosis and Multiple Sclerosis patients.
Keywords:
Intracerebroventricular
; ICV
; mTOR
; mTOR-I
; rapalog
; Tuberous Sclerosis
; TSC
; Multiple Sclerosis
; MS
; Experimental Autoimmune Encephalitis
; EAE
; Alzheimer’s Disease
; AD
; Thermostable Micelles
; Micellar Liquid Formulation
; Ommaya device
1. Introduction
Taken orally, mTOR inhibitors (mTOR-Is, rapamycin and synthetic analogues, rapalogs) are powerful immunosuppressant drugs widely used in the control of organ transplant rejection [1]. They exert their effect on every cell in the body, without distinction, heavily influencing its metabolism and blocking the cell cycle in G1 phase, thus inhibiting proliferation [2]. The latter action prevents the lymphocytes’ clonal expansion, which causes Immune System (IS) suppression.
Tuberous Sclerosis Complex, TSC [3] is a rare inborn disorder due to mutation of either TSC1 or TSC2 genes (both mTOR inhibitors). It is characterized by hyperactivation of mTOR and benign tumors in almost every organ, therefore also by cerebral SubEpendymal Nodules (SENs) and by fast-growing, life-threatening neurinomas [4], called SEGAs (SubEpendymal Giant Cell Astrocytomas). Despite its heavy immunosuppressive effect, but exploiting the antiproliferative one, the oral administration of the rapalog everolimus has been the first choice for treatment of TSC patients since the second decade of this century [5]. However, due to the low therapeutic index of mTOR-Is, the maximal tolerated dose of everolimus (blood concentration 9-15 ng/ml) can benefit only 40% of patients, reducing the size of their SEGAs [6] and allowing seizures to become manageable [7]. In the same study, a lower dose (3-7ng/ml), was more tolerable, but resulted completely ineffective.
In different conditions rapalogs display an immunomodulatory effect. Administered in vitro to dendritic cell (DC) cultures together with an alloantigen, once injected back into the bloodstream, so “rapaolog-conditioned” DCs reach the regional lymph nodes (LNs) and there they induce the production of regulatory T lymphocytes’ clones (Tregs), inducing tolerance towards said alloantigen [8,9,10,11,12,13] (Figure 1). However, until now this tolerizing effect has never been exploited with oral administration.
In preclinical experiments on the mouse model of Multiple Sclerosis (MS), the Experimental Autoimmune Encephalomyelitis (EAE) [14,15,16,17,18,19], in clinical trial on MS [20], as well as on type 1 diabetes [21] the immunosuppressant antiproliferative effect has so far prevailed, and symptoms reappeared shortly after the drug’s withdrawal.
The Alzheimer Disease (AD) mouse model created in the LaFerla laboratory [22], the 3xTg-AD mouse, displays clear cognitive impairment at 6 months of age, presenting only sporadic beta amyloid (βA) plaques, but significant intracellular βA load. Nonetheless, severe synaptic dysfunction can be assessed. Since 2010 [23] we know that high-dose oral administration of rapamycin leads to memory recovery of cognitively impaired AD mice. It was demonstrated that a major role was played by autophagy activation. It provokes reduction of βA and tau intracellular load, and restored synaptic function. However, the severe immunosuppression caused by the drug [1] may have helped to control the inflammatory aspects of the disease, which are only recently emerging [24]. The same effect of severe mTOR inhibition was demonstrated in other Early Onset (EOAD) and Late Onset Alzheimer Disease (LOAD) mouse models, if treated promptly after clinical onset [23,25]. Amyloid angiopathy is also reduced [26,27]. All models treated with oral rapamycin took a dose of 2,24g/Kg/24h for months [28]. Surprisingly, the role of the immunosuppressive effect of mTOR-Is on disease recovery was poorly studied, likely because it was difficult to distinguish from the contribution of autophagy. Again, as in TSC, the low therapeutic index of rapalogs represented the main obstacle and impeded the treatment from being immediately transferable to humans, where a few mg/day is sufficient to induce severe immunosuppression and heavy metabolic Side Effects (SEs) [1]. After more than a decade from the first publications demonstrating its efficacy in mice, a trial based on the oral administration of rapamycin on already symptomatic patients has finally arrived at clinical verification. The initial phase 1 study (NCT04200911, CARPE DIEM https://classic.clinicaltrials.gov/ct2/show/NCT04200911) has been concluded. Phase 2 study (NCT04629495, REACH https://classic.clinicaltrials.gov/ct2/show/NCT04629495) is now in progress. Just like all treated AD mouse models [23,25,26,27], in both studies rapamycin is the given drug. However, the daily oral dose to patients is not 2.24g/Kg, but 1mg/patient. The results are expected by mid 2024.
Thanks to the scarce CNS-related SEs (e.g., cephalea and nausea, rarely severe enough to compromise administration), we thought that the only way to bring these results rapidly to the bedside was the local, intracerebroventricular (ICV) administration [29], despite the obvious invasiveness. In our opinion our study [30] gave good and prolonged results on cognitive functions and even on mood (Figure 2).
At the same time a serious limit of our method was highlighted: the solution of the mTOR inhibitor in DMSO (dimethylsulfoxide, the most common organic solvent) was extremely thermolabile at body temperature. Even Everolimus, slightly more resistant than rapamycin, decayed (Figure 3), becoming undetectable within 12 days, but reduced by over 90% within a week.
It was necessary and urgent to develop a thermostable solution, which would allow therapeutic cycles of at least 10-15 days. The most common ICV delivery apparatus is the Ommaya device [31] (Figure 4). We think that the micellar liquid formulation that we have developed and present here meets these requirements.
2. Results
Every m-TOR-inhibitor can be encapsulated in micellar formulation. However, we preferred to start with everolimus.
2.1. Evaluation of Ev-Sol and Ev-Mic Stability by HPLC Analysis
To measure the stability of the DMSO-Everolimus solution (Ev-sol) and the Everolimus-micelles (Ev-mic), incubated at 4°, 25° and 37°C, solution and diluted micellar suspension samples (15 μL) were injected, at the programmed time, for HPLC-UV analysis (Figure 5). At 37°C, the Ev-mic showed higher stability than Ev-sol, as reported in Figure 3A: while Ev-sol dropped to zero at day 14, Ev-mic resulted undetectable by day 98. As shown in Figures 3B and 3C, Ev-mic was more stable at 25° and 4°C as compared to Ev-sol with around 100% of drug concentration after 98 days of incubation, while Ev-sol decayed completely on the 35th day in the samples incubated at 25°C, and on the 50th day in those incubated at 4°C.
2.2. Evaluation of Ev-sol and Ev-mic Stability by Cell Cultures
To verify the greater stability of Ev-mic as resulted from the HPLC analysis, the Ev-sol and Ev-mic activity was assessed on HeLa (Figure 6A) and SH-SY5Y cells. Ev-sol and Ev-mic, prepared as in the stability experiment, were used, at final concentration of 5 nM in medium, fresh or after incubation at 37°, 25° and 4°C for 7, 14, 35, 50 and 77 days. The inhibition of cell proliferation was evaluated by an MTT assay. Untreated, DMSO-treated (Veh) and empty micelles-treated (Empty mic) cells were used as negative controls. Fresh DMSO-everolimus solution was used as positive control. The day after the MTT treatment, the cell proliferation was measured by spectrophotometric readings at 589 nm and 650 nm. As reported in Figure 6A, at 37°C the Ev-mic activity was no longer detectable after 77 days, while at 25° and 4°C it remained substantially unvaried. It lasted a bit longer at 25° and 4°C. Ev-sol activity ceased to be detectable at 35 and 50 days, respectively. As reported in Figure 6B, at 37°C the Ev-sol activity was not detectable on the 14th day. Therefore, the data demonstrate a longer pharmacological activity of Ev-mic than Ev-sol on HeLa cell proliferation. Results obtained on the HeLa cell line were confirmed by analysis conducted on SH-SY5Y cells in the same experimental conditions (data not shown).
2.3. Empty Micelles Toxicity was Evaluated by MTT Analysis
The assay was conducted on HeLa cells (3000 cells/well) for 24 and 48 h of treatment. Empty micelles, suspended in PBS or in physiological solution, were used at final concentration of 0.2, 1, 2, 4, 8, 16 and 32X in reference to Ev-micelles concentration of 5 nM considered as 1X.
The cell proliferation underwent an insignificant reduction after the empty mic treatment. The results obtained from empty micelles in PBS corresponded to the ones in physiological solution (data not shown).
3. Discussion
3.1. Our Attempt to Make the mTOR Inhibition in AD Translational
In this article we demonstrate the thermostability of a new liquid formulation of mTOR inhibitors.
Its advantages are also its ease of production, storage and preparation for use. It is because of these characteristics that the micellar preparations have already reached the clinic in phase 3 trials. No particular criticalities have emerged and therefore they will soon reach the patient’s bedside [32,33].
A sound body of evidence demonstrates the efficacy of oral administration of rapamycin in the recovery from cognitive decline of many AD mouse models. The benefit is shown in all aspects of both EOAD and LOAD [23,25,26,27,30]. This effect was obtained by administering the drug orally at a dosage of 2.24 g/Kg every day [28]. Considering on one hand the invasiveness and difficult scalability of the ICV route of administration, and, on the other, the advantages of easily replicating cognitive recovery bypassing SEs, the latter weighed more and we took the risk [29]. We injected intracerebroventricularly, via an osmotic pump, the maximum tolerated dose of everolimus in DMSO: 44ng/g of brain on day 1. In the following days the solution degraded rapidly (see Figure 2 and Figure 3), reducing both the toxicity and efficacy of the treatment, and becoming undetectable by day 12. The treatment was performed in the same experimental conditions utilized by Caccamo et al. [23]: 3xTg-AD mice of 6 months of age, therefore already cognitively impaired. The high dose but short administration was sufficient to obtain the cognitive recovery of treated mice. We were surprised to observe that it also lasted for a much longer time than expected, more than 1.5 months from the beginning of the therapy (see Figure 2 and Cassano [30]).
The 3xTg-AD mouse [22] carries three transgenes, PS1M146V, APPSwe, and tauP301L. The first two cause Early-Onset AD in humans, the third is involved in causing frontotemporal dementia. Thirty days after the ICV treatment onset (and more than 15 from its end), the βA level was significantly reduced, but not eliminated. Therefore, we would have expected to observe, test after test, a gradual reduction in the effectiveness of that single week-12 days of administration. This did not occur (see Figure 2).
A safe liquid drug formulation maintaining over 95% activity after 14 days in the ICV delivery device at BT is now available. This allows us to envision a rapid clinical translation to AD and other mTOR-linked CNS diseases. We intend to study the suitable time, between one refill and another of the delivery device (if more than one is required).
A brief in vivo validation is still required. Ehninger et al. [34] demonstrated a reversal of learning deficits in a Tsc2+/- mouse model of tuberous sclerosis after oral administration of rapamycin for only 5 days, assessed by the Morris Water Maze test. We planned a 5-day ICV administration of our micellar rapalog formulation, which is expected to provoke the same results.
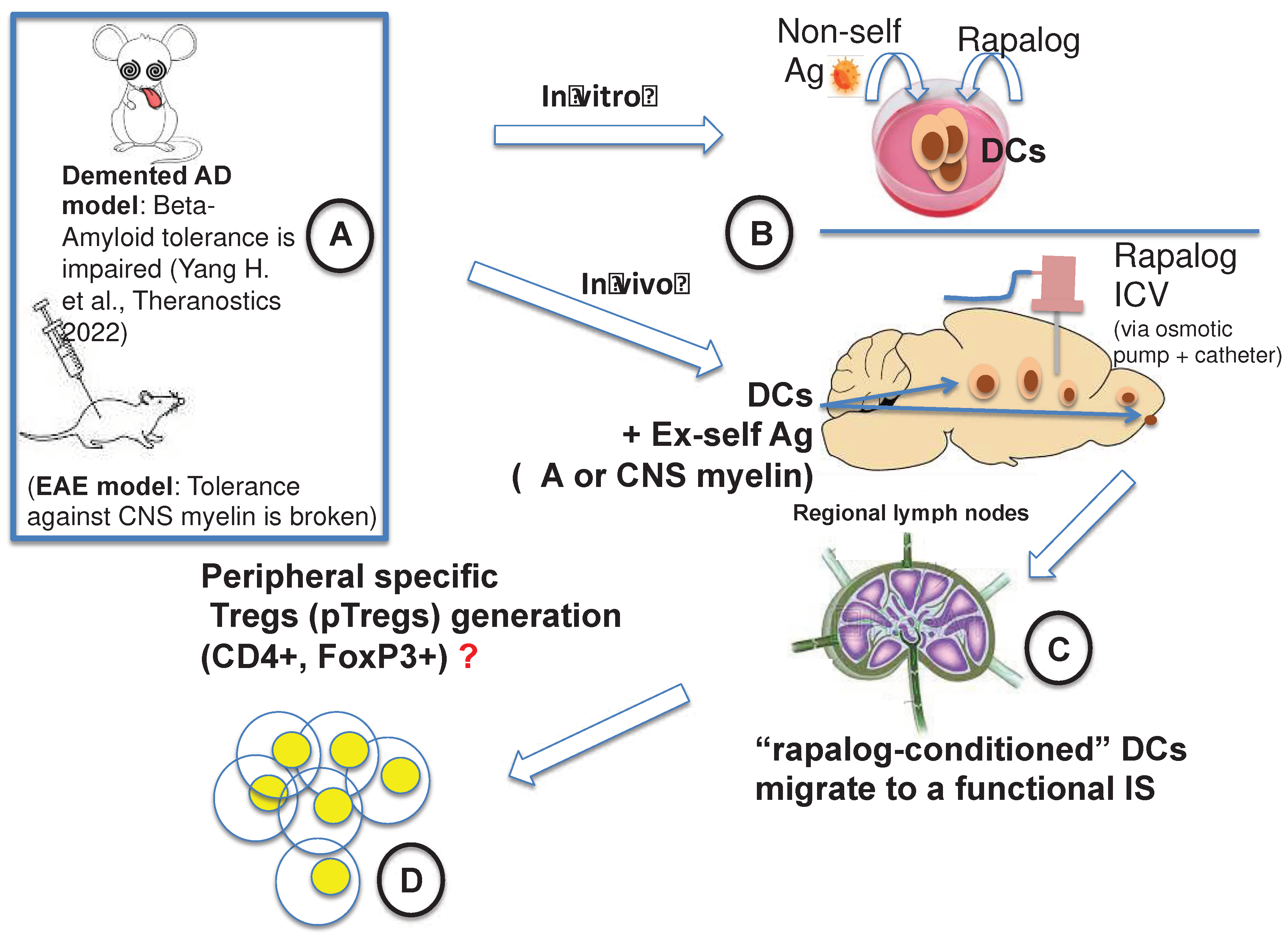
Speculating about the prolonged efficacy of our short treatment in 3xTg-AD mouse, an elegant paper by Mohammad et al. [35], about the mechanism of action of fingolimod, a widely used drug for MS control, offered a possible explanation. They demonstrated in the mouse a continuous flow of DCs patrolling the brain: they enter the brain through choroid plexuses, then cross the ependymal layer, proceed along the rostral migratory stream and exit the brain through the lamina cribrosa, reach the lymphatic vessels, then the cervical LNs. According to Mohammad et al., fingolimod exerts its therapeutic effect (both in the mouse and in humans) blocking the DCs’ egression from the brain, impeding them from reaching the cervical LNs carrying inflammatory signals and promoting relapse, resulting in DCs gathering in olfactory bulbs. In the case of our ICV administration it is certain that the DCs patrolling the CNS were strongly “rapalog-conditioned” (mTOR-inhibited) and, after gathering and processing self-antigens, they migrated to the regional LNs. Here, however, they found an active immune system, able to expand lymphocyte clones. Unlike oral administration, in which cells are all blocked in phase G1 of the cell cycle [2], we may have replicated in vivo and locally - in the CNS - the “conditioning” of DCs with a rapalog which has often been done by others in vitro (see Figure 1 and ref [8,9,10,11,12,13]). This might have helped control the inflammatory side of AD [36,37,38,39], and might have restored the impaired tolerance to beta-amyloid. It has been recently demonstrated that administration of βA specific Tregs obtained in vitro ameliorates cognitive impairment in AD mouse models [36] (Figure 7).
In the mouse model of the Experimental Autoimmune Encephalomyelitis (EAE), Esposito et al. [14] obtained interesting results regarding the treatment of Multiple Sclerosis (MS): stable symptoms remission as long as rapamycin was administered. Considering this and Mohammad paper [35], we think that the same results might be obtained administering (cyclically if necessary) our liquid formulation of rapalogs to EAE mice, avoiding systemic immunosuppression and metabolic SEs.
Beside AD, other neurological conditions might benefit from an ICV administration of a thermostable mTOR-Is liquid formulation: other neuroproteinopathies [40], and mentioned Multiple Sclerosis [20]. Everolimus in TSC already revolutionized the clinical course and life expectancy of over 40% of patients [6,7]. Part of the remaining 60% would likely take advantage from the ICV administration.
3.2. ICV Administration: Safety and Invasiveness
The ICV route of administration requires minor surgical intervention and periodic refill (Figure 3), and, fortunately, is compulsory in rather rare clinical conditions, recently reviewed in several publications [31,41,42,43]. Bacterial meningoencephalitis sensitive to antibiotics unable to pass through the blood-brain barrier (BBB) and primary cerebral lymphomas that need a high-dose drug with a low therapeutic index are just two examples of the pathologies that actually require ICV therapy.
The devices available are very effective but still “niche”, resulting from research investments appropriate to the size of the population that uses them and not developed with the aim of facilitating use on large numbers of patients. The surgical procedure takes little time, is considered a “minor” neurosurgical operation and, in expert hands, safe [31,41,42,43]. The most frequent complications, local infection and intracerebral hemorrhage, in the aforementioned study [42] never caused the patient’s death or serious long-term complications, but only a temporary interruption of therapy.
3.3. Scalability
While the oral or intravenous routes of administration are easily accessible to the entire population involved, limited only by the side effects of the treatment, the ICV route requires a real neurosurgical operation. Although minor, given the incidence of the disease in the general population, it could cause an unsustainable overload for local health facilities.
We were aware of this at the beginning of our project, and before embracing it we studied the alternatives. As we found no other possibilities, we calculated the impact that the application of a temporary or permanent administration device (e.g., Ommaya device) to newly diagnosed AD cases would have on the Healthcare System, given the current state of available technologies (which we consider completely inadequate for the new task and which require up-to-date improvement). Our opinion is that, using the neurosurgeries of the hospitals in an average western health district, this effort could be sustained, while remaining economically absolutely convenient.
The incidence of dementia in Europe as a whole has been estimated at 8.6 per 1,000 people/year [44], which in a district such as Vicenza - Italy (about 865,000 inhabitants) means about 7,440 new patients/year. Utilizing the 7 operating rooms in the entire province every working day in a year (250 or more), it would be a question of performing 30 surgeries per day in the whole district, or 4 operations a day in each operating room.
The greatest current limitation is therefore not the number of operations needed, but the number of neurosurgeons available. In our vision, the greatest commitment, which we have been thinking about for years, will be to make this operation highly robotic, minimal-risk, and performable by a general surgeon. We believe that this is possible, and that the time is ripe for modernizing quickly both the Ommaya device and the other ICV infusion devices that have remained substantially unchanged since the past century.
3.4. A clinical Trial Worth Performing
Our opinion is that preclinical science should matter, and that the efficacy of rapalogs in the treatment of AD is unquestionable. When we consider the huge body of data supporting the therapeutic efficacy of mTOR inhibition in many models of AD [23,25,26,27], the narrow therapeutic index of mTOR-Is, and our article [30], which successfully widened that therapeutic window, achieving rapid recovery, then we can believe that our approach, based on the ICV infusion of a thermostable, micellar liquid formulation of mTOR-Is (see Figure 5), represents an immediately viable strategy for facing AD and the 60% of “drug-resistant” TSC patients [6,7].
3.5. Brain-Restricted mTOR Inhibition: A Breakthrough
An article published by Shokat’s group [45] has recently appeared. In Parkinson’s disease (PD) “Carbidopa+Levodopa” are administered in association. Carbidopa blocks the peripheral conversion of L-DOPA in dopamine. Thus, this conversion happens entirely in the CNS. The research group has developed an effective and selective peripheral rapamycin inhibitor called Rapablock, which is not able to cross the BBB, exactly like carbidopa in Parkinson’s disease therapy. The group has also developed a third-generation mTOR-I that is particularly effective in crossing the BBB (called Rapalink-1). This association, which we might call the “Shokat combination” (“Central Rapamycin”/“Peripheral Rapamycin Inhibitor”, namely Rapablock + Rapalink-1), replicates in AD what the association “Carbidopa+Levodopa” represents in PD, and promises excellent results in all situations in which the BBB is intact (therefore impermeable to the contrast medium gadolinium). If it is not, the inhibitory Rapablock will cross it and inhibit Rapalink-1 within the brain. The inflammatory component of AD does not always spare the BBB integrity [44].
4. Materials and Methods
4.1. Preparation of Everolimus Solution
Everolimus (Selleck Chemicals) was dissolved in DMSO (VWR, Milan, Italy) at a concentration of 1 mg/mL. The solution was subsequently diluted in 10% v/v DMSO/physiological solution to obtain a 10 μg/mL concentration (Ev-sol) to be incubated at 4°C, 25°C (room temperature, RT) and 37°C (body temperature, BT).
4.2. Preparation of Everolimus Loaded Micelles
Carefully weighed amounts of everolimus and distearoylphosphatidyl-ethanolamine -polyethyleneglycole 2000 (DSPE-PEG2000, Lipoid, Switzerland) were dissolved in 3 mL of chloroform (Sigma-aldrich, Milan, Italy) in a 50 mL round flask. The solvent was removed by gentle evaporation at Room Temperature (RT) under nitrogen stream and vacuum dried for 1 hour to eliminate residual solvent traces. The thin film obtained was reconstituted in an exact volume (3 mL) of physiologic solution by slow solvent addition and vortexing. After complete reconstitution a clear micellar dispersion (Ev-mic) was obtained. The dispersion was then incubated at 4°, 25° and 37 °C.
4.3. Everolimus Quantification
The drug was quantified using a HPLC method. Briefly, the instrument used was a Portlab STAYER HPLC system equipped with UV detection, a parallel pump and Triathlon autosampler (Portlab, Rome, Italy). The conditions were the following: isocratic mode with acetonitrile:water (60:40, v/v) eluted at 0.8 mL/min and a Zorbax C8, 4.6 mm ID x 250 mm (5 μm) column (Agilent, Milan, Italy) equilibrated at 55°C. UV detection was performed at 278 nm. A calibration curve was built in the concentration range 0.62-10 μg/mL (r2=0.9992).
Solution samples were directly injected (15 mL injection volume), while the micellar suspension was first diluted 200 times in DMSO prior to being submitted to analysis. To reduce carry over effects and excessive accumulation of lipids in the column, solution and micellar samples were injected alternately. Periodic washing of the column with chloroform and methanol was performed to avoid accumulation of the lipid and performance loss. All measurements were taken in triplicate and results expressed as mean ± S.D..
4.4. Cell Cultures
Both HeLa cells (uterine cervix carcinoma cell line) and SH-SY5Y cells (neuroblastoma cell line) were obtained from American Type Culture Collection (Manassas, VA, USA) and were cultured in Dulbecco’s modified Eagle’s medium (DMEM with L-glutamine) supplemented with 10% (v/v) heat-inactivated fetal bovine serum (FBS), 100 U penicillin, 100 U streptomycin in a humidified incubator under 5% CO2 at 37°C.
4.5. MTT Analysis
Everolimus solution (Ev-sol) and Everolimus-micelles (Ev-mic) stability was determined by evaluating cell proliferation after treatments. Briefly, HeLa and SH-SY5Y cells were seeded in a 96-well plate at the concentration of 3000 cells/well and 6000 cells/well, respectively and were maintained in culture medium (100 µl) 24 h before the treatment. Every condition was tested in 3 wells. Ev-sol and Ev-mic were suspended in cell culture medium at a final concentration of 5nM and were used fresh or maintained at 37°, 25° and 4°C for 7, 14, 35, 50 and 77 days. As controls, untreated, DMSO-treated (Veh) and empty micelle-treated (Empty mic) cells were assayed. Cell proliferation was evaluated by using 3-[4,5-dimethylthiazol-2-yl]-2,5-diphenyltetrazolium bromide (MTT; Sigma-Aldrich) assay according to the manufacturer’s manual. Cells were mixed with 10 µL MTT (0.5 mg/ml) and maintained for 4 h in a humidified incubator at 37°C. Successively, 100 µl of solubilisation solution (10% SDS with 0.01 N HCl) were added in each well. The solubilisation of formazan crystals was performed overnight in an incubator at 37°C. The following day, cell proliferation was evaluated by spectrophotometry. Readings were performed on Beckman Coulter DTX 880 Multimode Detector (Beckman Coulter Inc., Brea, CA, USA) using a 589 nm line and 650 nm reference.
4.6. Cytotoxicity
Empty micelles’ (Empty mic) toxicity was evaluated on HeLa cells by MTT assay. HeLa cells were seeded in a 96-well plate at the concentration of 3000 cells/well and maintained in 100 µL of medium. The assay was performed at 24 and 48 h after treatment. Empty micelles, suspended in PBS or in physiological solution, were used at final concentration of 0.2, 1, 2, 4, 8, 16 and 32X in reference to Ev-micelles concentration of 5 nM considered as 1X.
5. Conclusion
Despite the limitation of the difficult scalability, the important advantage of the proposed therapeutic approach for AD is that it is “immediately” available. It utilizes widely used delivery devices and drugs, bypassing well-known SEs, and relies on logical and sound preclinical results.
Until gene correction of subependymal Neural Stem Cells (NSCs) in affected neonates is performed, in TSC patients too the only way to control neurological manifestations, today, is ICV infusion of thermostable micellar solution as soon as possible after birth. In drug-resistant adult patients, this might improve SEGAs and epilepsy control. If the “Shokat Combination” (Rapabolck + Rapalink) confirms its safety and efficacy in appropriate clinical trials, it will soon replace the ICV route of administration.
Until the “Shokat Combination’’ is clinically validated, the ICV administration of a thermostable mTOR-I solution likely represents an immediately available treatment also for other forms of dementia and neuroproteinopathies (e.g., [46]).
The case is different for all situations in which the gadolinium contrast medium permanently crosses the barrier, demonstrating its alteration: in this case the “Shokat combination” will never be fully effective. Progressive autoimmune diseases, some forms of AD [47] and brain tumours are known to alter the BBB [48], as confirmed in Shokat’s data themselves [45].
Author Contributions
Laura Gianessi, supervised by Stefano Giovagnoli and Alessandro Magini, performed both the in vitro and in vivo experiments. Diego Dolcetta (DD) acquired the funding for research and personally paid the patent expenses, administered the project, wrote and prepared the original draft. DD conceptualized the thermostable formulation together with Stefano Giovagnoli (SG). SG followed and analyzed data of the in vitro experiments. Alessandro Magini (AM) followed and analysed data of experiments on cell cultures. Roberto Dominici contributed to editing the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received funding by Associazione Sclerosi Tuberosa (https://www.sclerosituberosa.org) and Smuovilavita Foundation (http://www.smuovilavita.it). The APC was funded by the “Istituto di Neuroscienze di Rosà” (Director Dr. MD. Piergiorgio Miottello).
Acknowledgments
We thank Carol Metz De Maria for the careful and patient language revision.
Conflicts of Interest
DD, SG and AM are co-authors of the patent WO2021205297 (A1).
References
- Nguyen, L.S.; Vautier, M.; Allenbach, Y.; Zahr, N.; Benveniste, O.; Funck-Brentano, C.; Salem, J.-E. Sirolimus and MTOR Inhibitors: A Review of Side Effects and Specific Management in Solid Organ Transplantation. Drug Saf. 2019, 42, 813–825. [Google Scholar] [CrossRef] [PubMed]
- Dumont, F.J.; Su, Q. Mechanism of Action of the Immunosuppressant Rapamycin. Life Sci. 1995, 58, 373–395. [Google Scholar] [CrossRef] [PubMed]
- Curatolo, P.; Bombardieri, R.; Jozwiak, S. Tuberous Sclerosis. Lancet Lond. Engl. 2008, 372, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Shrikhande, G.; Xu, J.; McKay, R.M.; Burns, D.K.; Johnson, J.E.; Parada, L.F. Tsc1 Mutant Neural Stem/Progenitor Cells Exhibit Migration Deficits and Give Rise to Subependymal Lesions in the Lateral Ventricle. Genes Dev. 2011, 25, 1595–1600. [Google Scholar] [CrossRef]
- Franz, D.N.; Leonard, J.; Tudor, C.; Chuck, G.; Care, M.; Sethuraman, G.; Dinopoulos, A.; Thomas, G.; Crone, K.R. Rapamycin Causes Regression of Astrocytomas in Tuberous Sclerosis Complex. Ann. Neurol. 2006, 59, 490–498. [Google Scholar] [CrossRef]
- Franz, D.N.; Belousova, E.; Sparagana, S.; Bebin, E.M.; Frost, M.; Kuperman, R.; Witt, O.; Kohrman, M.H.; Flamini, J.R.; Wu, J.Y.; et al. Efficacy and Safety of Everolimus for Subependymal Giant Cell Astrocytomas Associated with Tuberous Sclerosis Complex (EXIST-1): A Multicentre, Randomised, Placebo-Controlled Phase 3 Trial. Lancet Lond. Engl. 2013, 381, 125–132. [Google Scholar] [CrossRef]
- French, J.A.; Lawson, J.A.; Yapici, Z.; Ikeda, H.; Polster, T.; Nabbout, R.; Curatolo, P.; de Vries, P.J.; Dlugos, D.J.; Berkowitz, N.; et al. Adjunctive Everolimus Therapy for Treatment-Resistant Focal-Onset Seizures Associated with Tuberous Sclerosis (EXIST-3): A Phase 3, Randomised, Double-Blind, Placebo-Controlled Study. Lancet Lond. Engl. 2016, 388, 2153–2163. [Google Scholar] [CrossRef]
- Chapman, N.M.; Chi, H. MTOR Signaling, Tregs and Immune Modulation. Immunotherapy 2014, 6, 1295–1311. [Google Scholar] [CrossRef]
- Silk, K.M.; Leishman, A.J.; Nishimoto, K.P.; Reddy, A.; Fairchild, P.J. Rapamycin Conditioning of Dendritic Cells Differentiated from Human ES Cells Promotes a Tolerogenic Phenotype. J. Biomed. Biotechnol. 2012, 2012, 172420. [Google Scholar] [CrossRef]
- Stallone, G.; Infante, B.; Di Lorenzo, A.; Rascio, F.; Zaza, G.; Grandaliano, G. MTOR Inhibitors Effects on Regulatory T Cells and on Dendritic Cells. J. Transl. Med. 2016, 14, 152. [Google Scholar] [CrossRef]
- Turnquist, H.R.; Raimondi, G.; Zahorchak, A.F.; Fischer, R.T.; Wang, Z.; Thomson, A.W. Rapamycin-Conditioned Dendritic Cells Are Poor Stimulators of Allogeneic CD4+ T Cells, but Enrich for Antigen-Specific Foxp3+ T Regulatory Cells and Promote Organ Transplant Tolerance. J. Immunol. Baltim. Md 1950 2007, 178, 7018–7031. [Google Scholar] [CrossRef] [PubMed]
- Fischer, R.; Turnquist, H.R.; Taner, T.; Thomson, A.W. Use of Rapamycin in the Induction of Tolerogenic Dendritic Cells. Handb. Exp. Pharmacol. 2009, 215–232. [Google Scholar] [CrossRef]
- Macedo, C.; Turquist, H.; Metes, D.; Thomson, A.W. Immunoregulatory Properties of Rapamycin-Conditioned Monocyte-Derived Dendritic Cells and Their Role in Transplantation. Transplant. Res. 2012, 1, 16. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Ruffini, F.; Bellone, M.; Gagliani, N.; Battaglia, M.; Martino, G.; Furlan, R. Rapamycin Inhibits Relapsing Experimental Autoimmune Encephalomyelitis by Both Effector and Regulatory T Cells Modulation. J. Neuroimmunol. 2010, 220, 52–63. [Google Scholar] [CrossRef]
- Hou, H.; Miao, J.; Cao, R.; Han, M.; Sun, Y.; Liu, X.; Guo, L. Rapamycin Ameliorates Experimental Autoimmune Encephalomyelitis by Suppressing the MTOR-STAT3 Pathway. Neurochem. Res. 2017, 42, 2831–2840. [Google Scholar] [CrossRef] [PubMed]
- Dello Russo, C.; Lisi, L.; Feinstein, D.L.; Navarra, P. MTOR Kinase, a Key Player in the Regulation of Glial Functions: Relevance for the Therapy of Multiple Sclerosis. Glia 2013, 61, 301–311. [Google Scholar] [CrossRef]
- Li, X.-L.; Zhang, B.; Liu, W.; Sun, M.-J.; Zhang, Y.-L.; Liu, H.; Wang, M.-X. Rapamycin Alleviates the Symptoms of Multiple Sclerosis in Experimental Autoimmune Encephalomyelitis (EAE) Through Mediating the TAM-TLRs-SOCS Pathway. Front. Neurol. 2020, 11, 590884. [Google Scholar] [CrossRef]
- Li, Z.; Nie, L.; Chen, L.; Sun, Y.; Li, G. Rapamycin Relieves Inflammation of Experimental Autoimmune Encephalomyelitis by Altering the Balance of Treg/Th17 in a Mouse Model. Neurosci. Lett. 2019, 705, 39–45. [Google Scholar] [CrossRef]
- Vakrakou, A.G.; Alexaki, A.; Brinia, M.-E.; Anagnostouli, M.; Stefanis, L.; Stathopoulos, P. The MTOR Signaling Pathway in Multiple Sclerosis; from Animal Models to Human Data. Int. J. Mol. Sci. 2022, 23, 8077. [Google Scholar] [CrossRef]
- Bagherpour, B.; Salehi, M.; Jafari, R.; Bagheri, A.; Kiani-Esfahani, A.; Edalati, M.; Kardi, M.T.; Shaygannejad, V. Promising Effect of Rapamycin on Multiple Sclerosis. Mult. Scler. Relat. Disord. 2018, 26, 40–45. [Google Scholar] [CrossRef]
- Monti, P.; Scirpoli, M.; Maffi, P.; Piemonti, L.; Secchi, A.; Bonifacio, E.; Roncarolo, M.-G.; Battaglia, M. Rapamycin Monotherapy in Patients with Type 1 Diabetes Modifies CD4+CD25+FOXP3+ Regulatory T-Cells. Diabetes 2008, 57, 2341–2347. [Google Scholar] [CrossRef] [PubMed]
- Oddo, S.; Caccamo, A.; Shepherd, J.D.; Murphy, M.P.; Golde, T.E.; Kayed, R.; Metherate, R.; Mattson, M.P.; Akbari, Y.; LaFerla, F.M. Triple-Transgenic Model of Alzheimer’s Disease with Plaques and Tangles: Intracellular Abeta and Synaptic Dysfunction. Neuron 2003, 39, 409–421. [Google Scholar] [CrossRef] [PubMed]
- Caccamo, A.; Majumder, S.; Richardson, A.; Strong, R.; Oddo, S. Molecular Interplay between Mammalian Target of Rapamycin (MTOR), Amyloid-Beta, and Tau: Effects on Cognitive Impairments. J. Biol. Chem. 2010, 285, 13107–13120. [Google Scholar] [CrossRef] [PubMed]
- Haage, V.; De Jager, P.L. Neuroimmune Contributions to Alzheimer’s Disease: A Focus on Human Data. Mol. Psychiatry 2022, 27, 3164–3181. [Google Scholar] [CrossRef]
- Spilman, P.; Podlutskaya, N.; Hart, M.J.; Debnath, J.; Gorostiza, O.; Bredesen, D.; Richardson, A.; Strong, R.; Galvan, V. Inhibition of MTOR by Rapamycin Abolishes Cognitive Deficits and Reduces Amyloid-Beta Levels in a Mouse Model of Alzheimer’s Disease. PloS One 2010, 5, e9979. [Google Scholar] [CrossRef]
- Lin, A.-L.; Zheng, W.; Halloran, J.J.; Burbank, R.R.; Hussong, S.A.; Hart, M.J.; Javors, M.; Shih, Y.-Y.I.; Muir, E.; Fonseca, R.S.; et al. Chronic Rapamycin Restores Brain Vascular Integrity and Function Through NO Synthase Activation and Improves Memory in Symptomatic Mice Modeling Alzheimer’s Disease. J. Cereb. Blood Flow Metab. 2013, 33, 1412–1421. [Google Scholar] [CrossRef]
- Lin, A.-L.; Jahrling, J.B.; Zhang, W.; DeRosa, N.; Bakshi, V.; Romero, P.; Galvan, V.; Richardson, A. Rapamycin Rescues Vascular, Metabolic and Learning Deficits in Apolipoprotein E4 Transgenic Mice with Pre-Symptomatic Alzheimer’s Disease. J. Cereb. Blood Flow Metab. Off. J. Int. Soc. Cereb. Blood Flow Metab. 2017, 37, 217–226. [Google Scholar] [CrossRef]
- Harrison, D.E.; Strong, R.; Sharp, Z.D.; Nelson, J.F.; Astle, C.M.; Flurkey, K.; Nadon, N.L.; Wilkinson, J.E.; Frenkel, K.; Carter, C.S.; et al. Rapamycin Fed Late in Life Extends Lifespan in Genetically Heterogeneous Mice. Nature 2009, 460, 392–395. [Google Scholar] [CrossRef]
- Dolcetta, D.; Dominici, R. The Local Mammalian Target of Rapamycin (MTOR) Modulation: A Promising Strategy to Counteract Neurodegeneration. Neural Regen. Res. 2019, 14, 1711–1712. [Google Scholar] [CrossRef]
- Cassano, T.; Magini, A.; Giovagnoli, S.; Polchi, A.; Calcagnini, S.; Pace, L.; Lavecchia, M.A.; Scuderi, C.; Bronzuoli, M.R.; Ruggeri, L.; et al. Early Intrathecal Infusion of Everolimus Restores Cognitive Function and Mood in a Murine Model of Alzheimer’s Disease. Exp. Neurol. 2019, 311, 88–105. [Google Scholar] [CrossRef]
- Atkinson, A.J. Intracerebroventricular Drug Administration. Transl. Clin. Pharmacol. 2017, 25, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Figueiras, A.; Domingues, C.; Jarak, I.; Santos, A.I.; Parra, A.; Pais, A.; Alvarez-Lorenzo, C.; Concheiro, A.; Kabanov, A.; Cabral, H.; et al. New Advances in Biomedical Application of Polymeric Micelles. Pharmaceutics 2022, 14, 1700. [Google Scholar] [CrossRef] [PubMed]
- Negut, I.; Bita, B. Polymeric Micellar Systems-A Special Emphasis on “Smart” Drug Delivery. Pharmaceutics 2023, 15, 976. [Google Scholar] [CrossRef] [PubMed]
- Ehninger, D.; Han, S.; Shilyansky, C.; Zhou, Y.; Li, W.; Kwiatkowski, D.J.; Ramesh, V.; Silva, A.J. Reversal of Learning Deficits in a Tsc2+/- Mouse Model of Tuberous Sclerosis. Nat. Med. 2008, 14, 843–848. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, M.G.; Tsai, V.W.W.; Ruitenberg, M.J.; Hassanpour, M.; Li, H.; Hart, P.H.; Breit, S.N.; Sawchenko, P.E.; Brown, D.A. Immune Cell Trafficking from the Brain Maintains CNS Immune Tolerance. J. Clin. Invest. 2014, 124, 1228–1241. [Google Scholar] [CrossRef]
- Yang, H.; Park, S.-Y.; Baek, H.; Lee, C.; Chung, G.; Liu, X.; Lee, J.H.; Kim, B.; Kwon, M.; Choi, H.; et al. Adoptive Therapy with Amyloid-β Specific Regulatory T Cells Alleviates Alzheimer’s Disease. Theranostics 2022, 12, 7668–7680. [Google Scholar] [CrossRef] [PubMed]
- Faridar, A.; Thome, A.D.; Zhao, W.; Thonhoff, J.R.; Beers, D.R.; Pascual, B.; Masdeu, J.C.; Appel, S.H. Restoring Regulatory T-Cell Dysfunction in Alzheimer’s Disease through Ex Vivo Expansion. Brain Commun. 2020, 2, fcaa112. [Google Scholar] [CrossRef]
- Weaver, D.F. Alzheimer’s Disease as an Innate Autoimmune Disease (AD2 ): A New Molecular Paradigm. Alzheimers Dement. J. Alzheimers Assoc. 2022. [Google Scholar] [CrossRef]
- Liston, A.; Dooley, J.; Yshii, L. Brain-Resident Regulatory T Cells and Their Role in Health and Disease. Immunol. Lett. 2022, 248, 26–30. [Google Scholar] [CrossRef]
- Xu, Y.; Li, Y.; Wang, C.; Han, T.; Liu, H.; Sun, L.; Hong, J.; Hashimoto, M.; Wei, J. The Reciprocal Interactions between Microglia and T Cells in Parkinson’s Disease: A Double-Edged Sword. J. Neuroinflammation 2023, 20, 33. [Google Scholar] [CrossRef]
- Chaichana, K.L.; Pinheiro, L.; Brem, H. Delivery of Local Therapeutics to the Brain: Working toward Advancing Treatment for Malignant Gliomas. Ther. Deliv. 2015, 6, 353–369. [Google Scholar] [CrossRef] [PubMed]
- Peyrl, A.; Chocholous, M.; Azizi, A.A.; Czech, T.; Dorfer, C.; Mitteregger, D.; Gojo, J.; Minichmayr, E.; Slavc, I. Safety of Ommaya Reservoirs in Children with Brain Tumors: A 20-Year Experience with 5472 Intraventricular Drug Administrations in 98 Patients. J. Neurooncol. 2014, 120, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Giordan, E.; Palandri, G.; Lanzino, G.; Murad, M.H.; Elder, B.D. Outcomes and Complications of Different Surgical Treatments for Idiopathic Normal Pressure Hydrocephalus: A Systematic Review and Meta-Analysis. J. Neurosurg. 2018, 1–13. [Google Scholar] [CrossRef]
- Ponjoan, A.; Garre-Olmo, J.; Blanch, J.; Fages, E.; Alves-Cabratosa, L.; Martí-Lluch, R.; Comas-Cufí, M.; Parramon, D.; Garcia-Gil, M.; Ramos, R. Epidemiology of Dementia: Prevalence and Incidence Estimates Using Validated Electronic Health Records from Primary Care. Clin. Epidemiol. 2019, 11, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Fan, Q.; Luo, X.; Lou, K.; Weiss, W.A.; Shokat, K.M. Brain-Restricted MTOR Inhibition with Binary Pharmacology. Nature 2022, 609, 822–828. [Google Scholar] [CrossRef]
- Kocak, M.; Ezazi Erdi, S.; Jorba, G.; Maestro, I.; Farrés, J.; Kirkin, V.; Martinez, A.; Pless, O. Targeting Autophagy in Disease: Established and New Strategies. Autophagy 2022, 18, 473–495. [Google Scholar] [CrossRef] [PubMed]
- Alruwais, N.M.; Rusted, J.M.; Tabet, N.; Dowell, N.G. Evidence of Emerging BBB Changes in Mid-Age Apolipoprotein E Epsilon-4 Carriers. Brain Behav. 2022, 12, e2806. [Google Scholar] [CrossRef] [PubMed]
- Patil, R.; Galstyan, A.; Grodzinski, Z.B.; Shatalova, E.S.; Wagner, S.; Israel, L.L.; Ding, H.; Black, K.L.; Ljubimova, J.Y.; Holler, E. Single- and Multi-Arm Gadolinium MRI Contrast Agents for Targeted Imaging of Glioblastoma. Int. J. Nanomedicine 2020, 15, 3057–3070. [Google Scholar] [CrossRef]
Figure 1.
“Rapalog-conditioned” DCs are obtained by co-cultivating Dendritic Cells with an alloantigen in the presence of rapalog (A). After injection in the bloodstream (B), “conditioned” DCs migrate to the regional lymph nodes (C), where they give rise to Treg clones specific for the alloantigen (D). This allows specific peripheral tolerance to be obtained (according to Macedo et al., Transplantation Research, 2012 and ref [8,9,10,11,12,13]).
Figure 1.
“Rapalog-conditioned” DCs are obtained by co-cultivating Dendritic Cells with an alloantigen in the presence of rapalog (A). After injection in the bloodstream (B), “conditioned” DCs migrate to the regional lymph nodes (C), where they give rise to Treg clones specific for the alloantigen (D). This allows specific peripheral tolerance to be obtained (according to Macedo et al., Transplantation Research, 2012 and ref [8,9,10,11,12,13]).
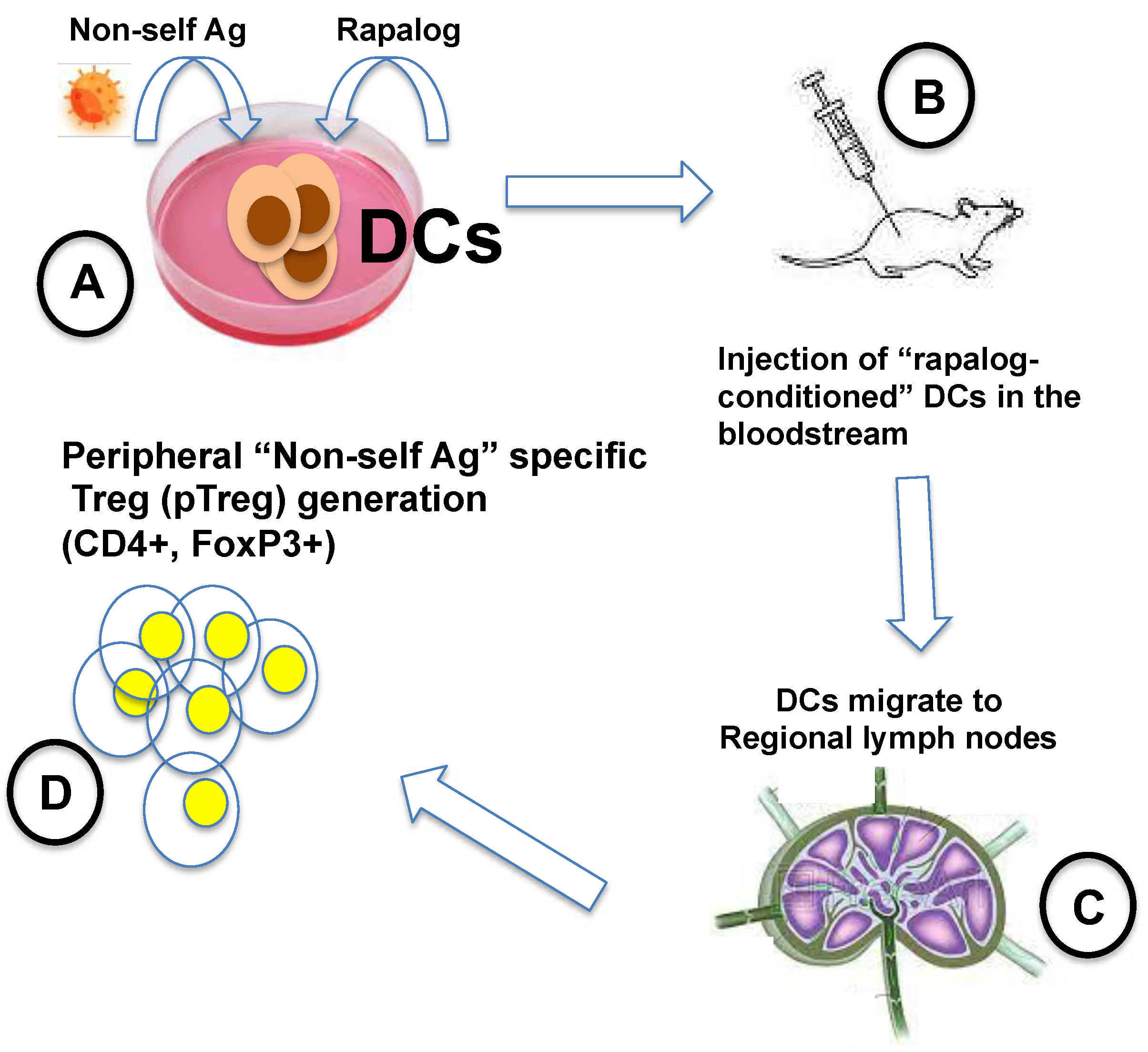
Figure 2.
The scheme of our experimental plan is shown. With a short ICV administration of the highest tolerated dose of everolimus, which rapidly decayed at Body Temperature, we obtained good results on mood (assessed by the sucrose preference test, SPT) and on memory performance (assessed by the Morris Water Maze, MWM); surprisingly the benefit lasted many weeks after the treatment. (from Cassano et al., Experimental Neurology, 2019 Jan;311:88-105 [30], Copyright Elsevier, 2019, with permission).
Figure 2.
The scheme of our experimental plan is shown. With a short ICV administration of the highest tolerated dose of everolimus, which rapidly decayed at Body Temperature, we obtained good results on mood (assessed by the sucrose preference test, SPT) and on memory performance (assessed by the Morris Water Maze, MWM); surprisingly the benefit lasted many weeks after the treatment. (from Cassano et al., Experimental Neurology, 2019 Jan;311:88-105 [30], Copyright Elsevier, 2019, with permission).
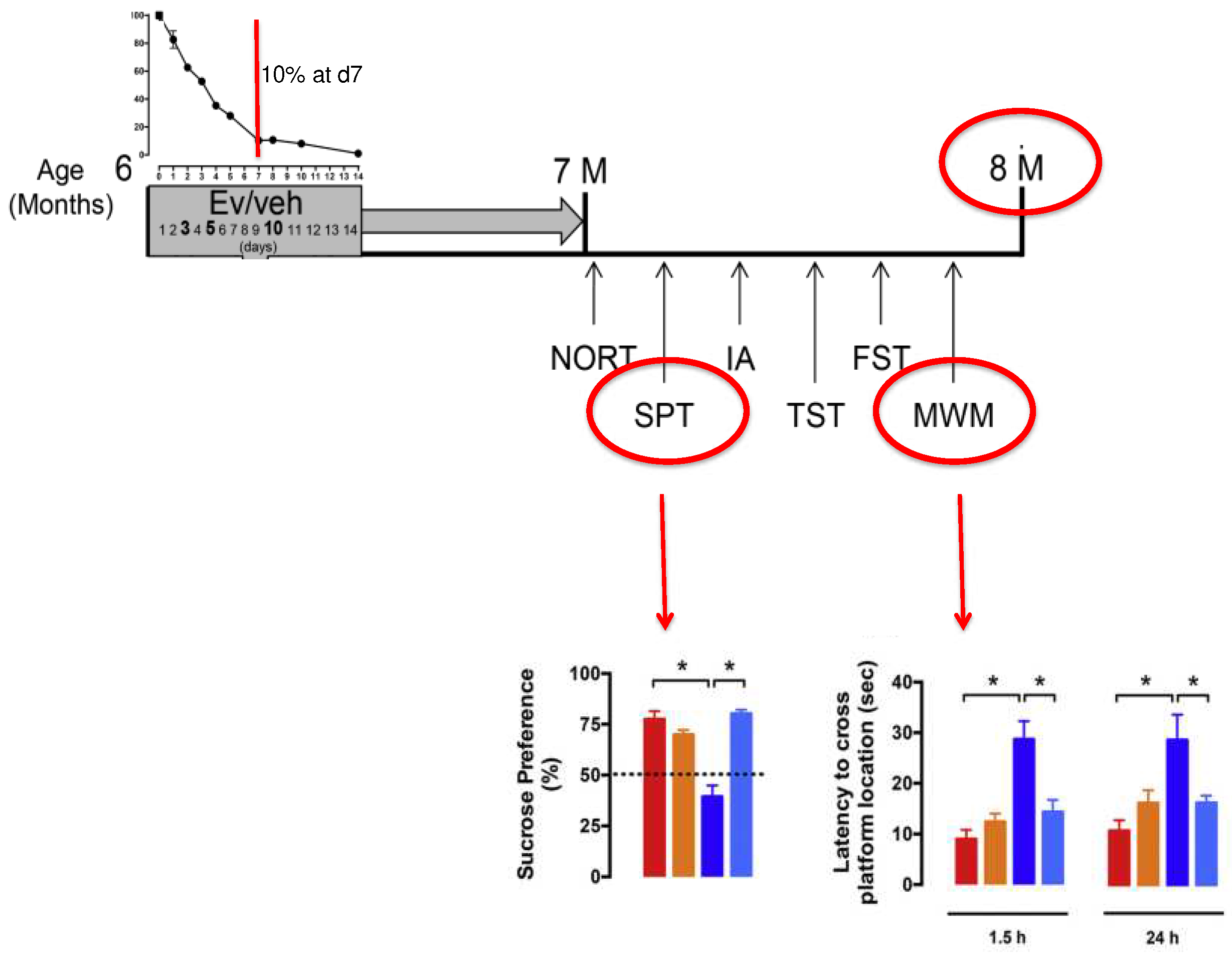
Figure 3.
Rapamycin and everolimus decay, in DMSO solution, at body temperature (%/day). (from Cassano et al., Experimental Neurology, 2019 Jan;311:88-105 [30], Copyright Elsevier, 2019, with permission).
Figure 3.
Rapamycin and everolimus decay, in DMSO solution, at body temperature (%/day). (from Cassano et al., Experimental Neurology, 2019 Jan;311:88-105 [30], Copyright Elsevier, 2019, with permission).
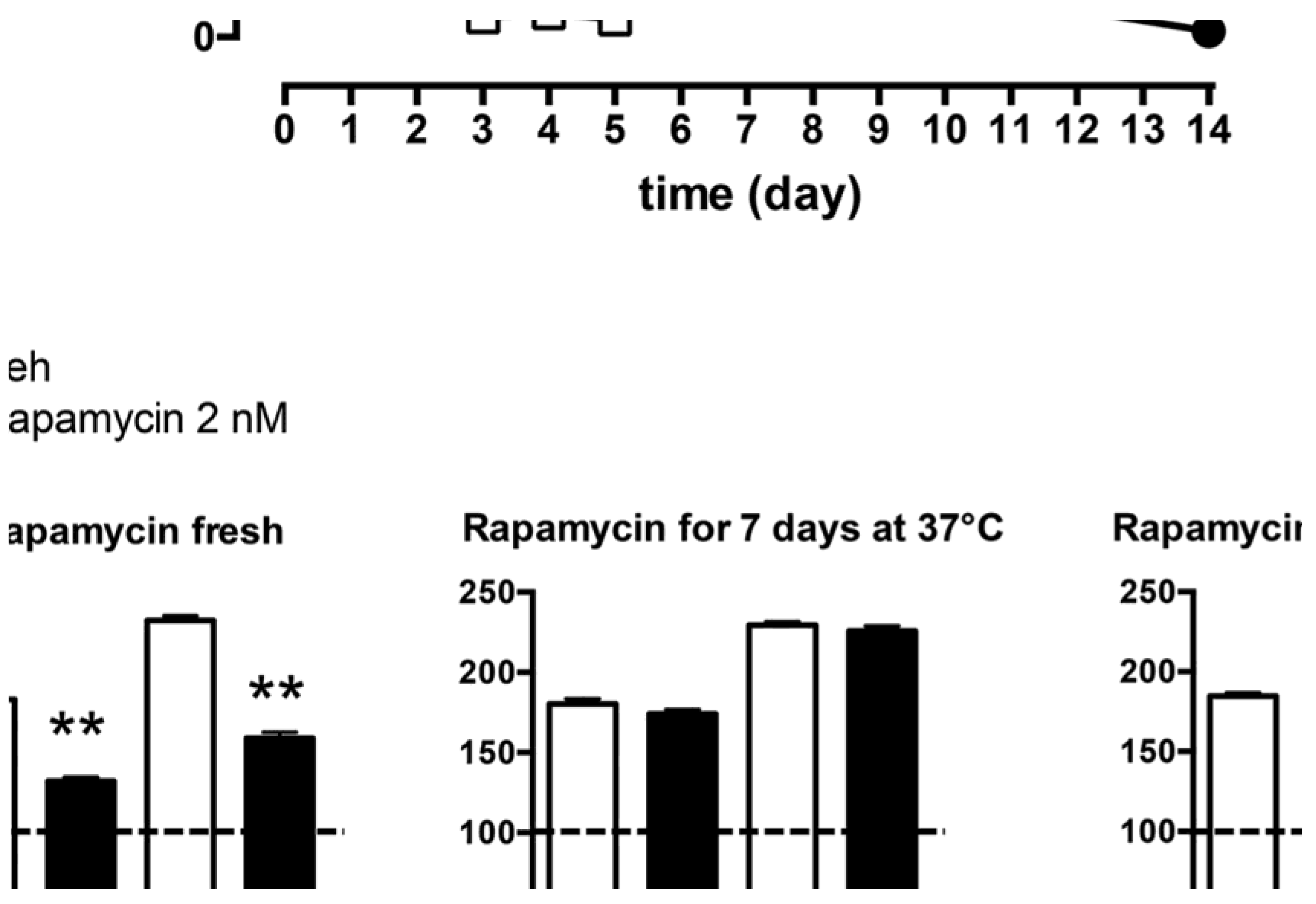
Figure 4.
Ommaya device is the most common instrument for delivering drugs in the ventricular cerebrospinal fluid (CSF). Here a “basic” model is represented. The rubber reservoir is surgically placed under the scalp skin and it is connected with a catheter reaching the lateral ventricle of one side. The reservoir is in fact a pump that can be refilled many times with a normal syringe, in accurate sterility.
Figure 4.
Ommaya device is the most common instrument for delivering drugs in the ventricular cerebrospinal fluid (CSF). Here a “basic” model is represented. The rubber reservoir is surgically placed under the scalp skin and it is connected with a catheter reaching the lateral ventricle of one side. The reservoir is in fact a pump that can be refilled many times with a normal syringe, in accurate sterility.
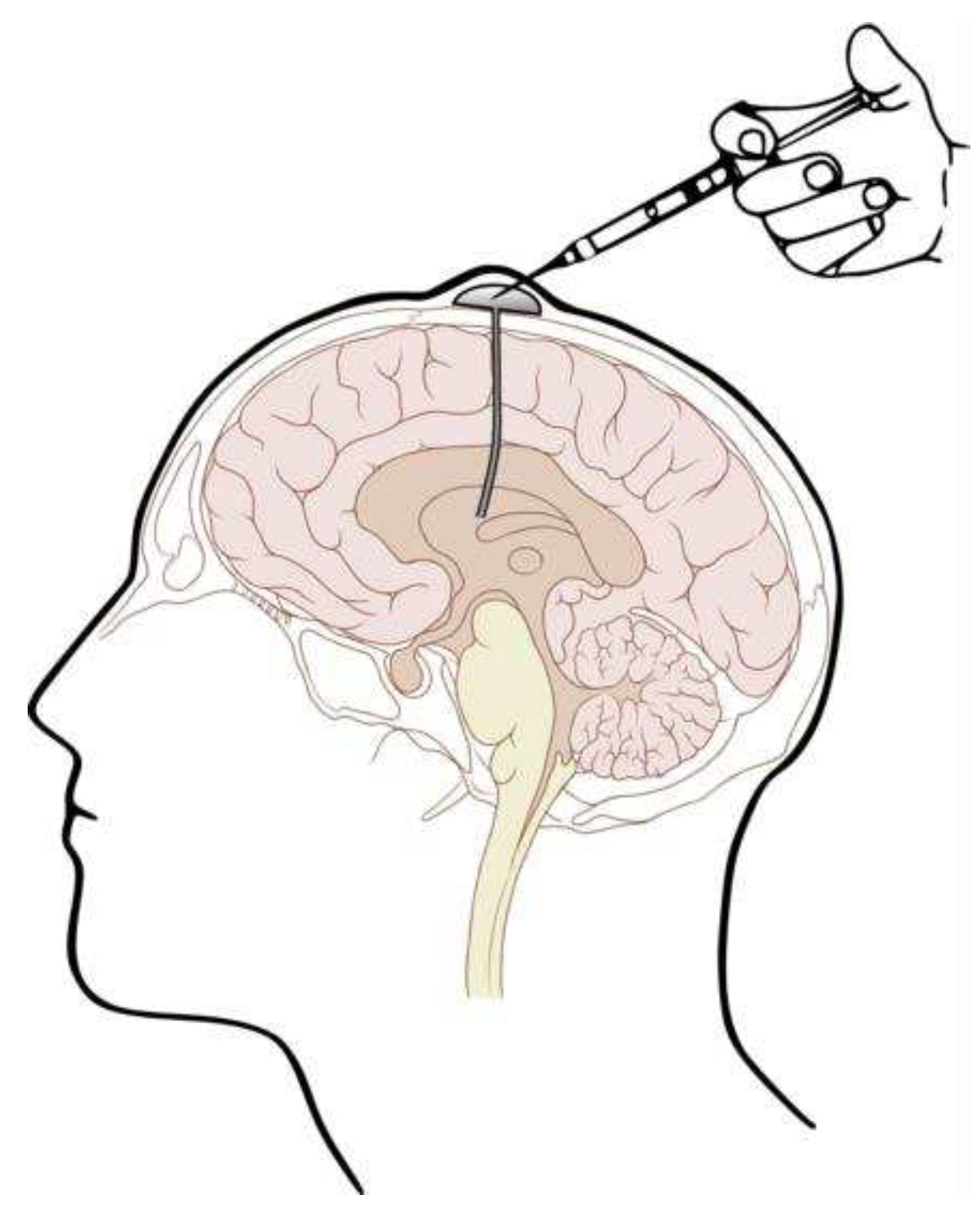
Figure 5.
Everolimus decay in DMSO solution (grey) and in micelles (black) (A). At Body Temperature (BT, 37° C). (B). At Room Temperature (RT, 25° C). (C). At 4° C. After 15 days at BT (A), over 95% of the Ev-mic activity was still maintained, while Ev-sol decayed completely.
Figure 5.
Everolimus decay in DMSO solution (grey) and in micelles (black) (A). At Body Temperature (BT, 37° C). (B). At Room Temperature (RT, 25° C). (C). At 4° C. After 15 days at BT (A), over 95% of the Ev-mic activity was still maintained, while Ev-sol decayed completely.
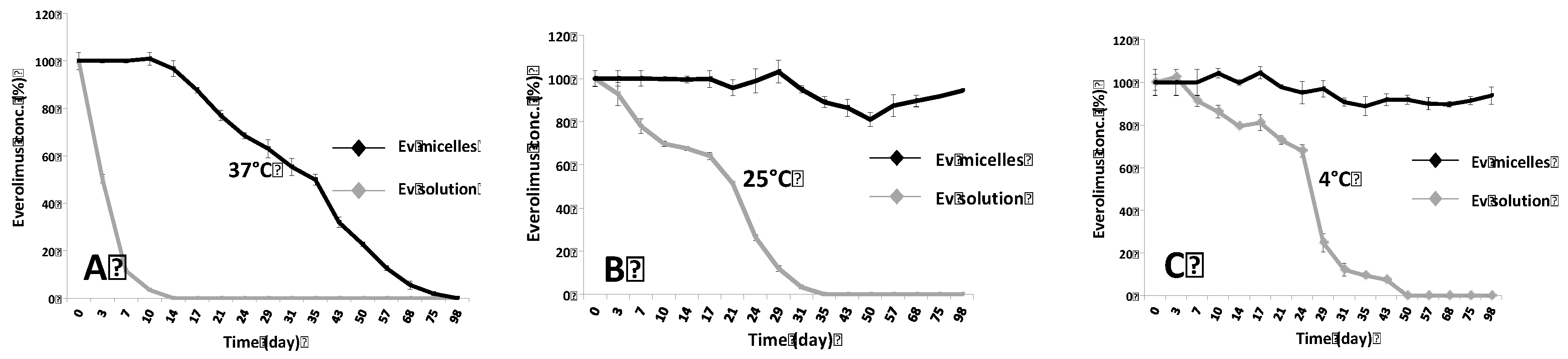
Figure 6.
(A). Evaluation of Ev-sol and Ev-mic activity on HeLa cells. The activity was measured by the MTT method. HeLa (3000 cells/well) cells were seeded in a 96-well plate for 24h at 37°C. Ev-sol and Ev-mic (both 5nM) were used fresh or maintained at 37°, 25° and 4°C for 7, 14, 35, 50 and 77 days. The data obtained are normalized using untreated, DMSO- treated (Veh) and empty micelles-treated (Empty mic) cells, as controls. Results on SH-SY5Y cells (6000/well) confirmed those on HeLa (data not shown). (B). A simplified detail of Figure 4A shows here the improved thermostability of micellar everolimus (Ev-mic) compared to that of the DMSO everolimus solution (Ev-sol), both maintained 14 days at Body Temperature. Empty micelles (Empty mic) represent the negative control, and freshly prepared DMSO everolimus solution (Ev-sol fresh) the positive control. #: p-value = 0,003.
Figure 6.
(A). Evaluation of Ev-sol and Ev-mic activity on HeLa cells. The activity was measured by the MTT method. HeLa (3000 cells/well) cells were seeded in a 96-well plate for 24h at 37°C. Ev-sol and Ev-mic (both 5nM) were used fresh or maintained at 37°, 25° and 4°C for 7, 14, 35, 50 and 77 days. The data obtained are normalized using untreated, DMSO- treated (Veh) and empty micelles-treated (Empty mic) cells, as controls. Results on SH-SY5Y cells (6000/well) confirmed those on HeLa (data not shown). (B). A simplified detail of Figure 4A shows here the improved thermostability of micellar everolimus (Ev-mic) compared to that of the DMSO everolimus solution (Ev-sol), both maintained 14 days at Body Temperature. Empty micelles (Empty mic) represent the negative control, and freshly prepared DMSO everolimus solution (Ev-sol fresh) the positive control. #: p-value = 0,003.
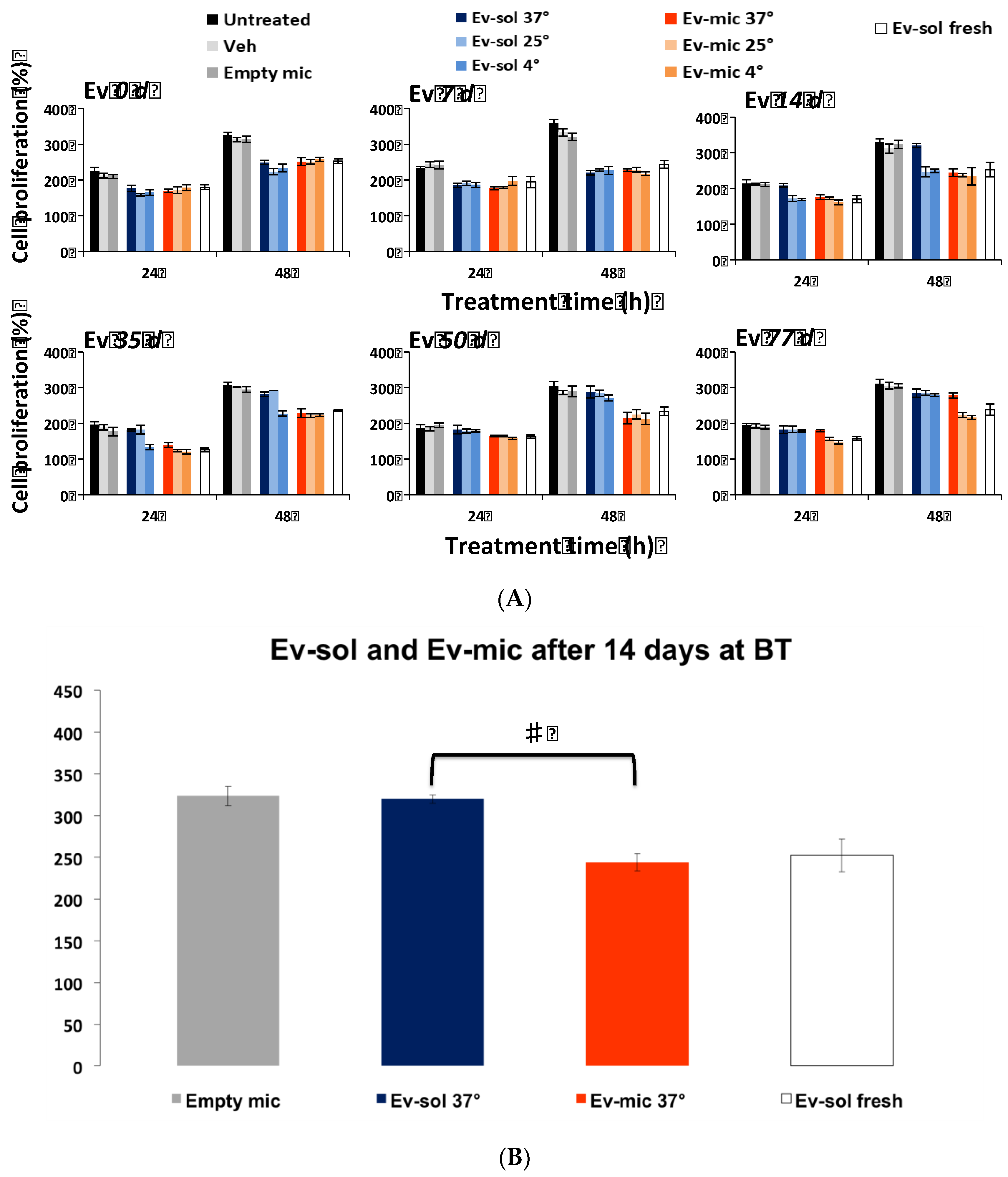
Figure 7.
Hypothetical explanation of the prolonged recovery observed in the AD mouse treated with everolimus ICV (see Figure 2 and Figure 3 and Cassano et al., 2019). (A), cognitively impaired 3xTg-AD mouse (but the EAE model - obtained by injecting under the skin a mixture of inflammatory agents and a brain myelin peptide—might perform equally). (B), the infusion pump gradually infused the thermolabile rapalog for 7-12 days (see Figure 2 and Figure 3): the DCs patrolling the brain found themselves as in Macedo’s in vitro conditions (see Figure 1, Introduction and ref [8,9,10,11,12,13]), namely in the contemporary presence of the βA “antigen” and the rapalog. (C), rapalog-conditioned DCs left the brain and reached the cervical lymph nodes, where they found a competent immune system (IS), and (D), might have given in AD, and might give in EAE, origin to specific Tregs, restoring the previously broken tolerance.
Figure 7.
Hypothetical explanation of the prolonged recovery observed in the AD mouse treated with everolimus ICV (see Figure 2 and Figure 3 and Cassano et al., 2019). (A), cognitively impaired 3xTg-AD mouse (but the EAE model - obtained by injecting under the skin a mixture of inflammatory agents and a brain myelin peptide—might perform equally). (B), the infusion pump gradually infused the thermolabile rapalog for 7-12 days (see Figure 2 and Figure 3): the DCs patrolling the brain found themselves as in Macedo’s in vitro conditions (see Figure 1, Introduction and ref [8,9,10,11,12,13]), namely in the contemporary presence of the βA “antigen” and the rapalog. (C), rapalog-conditioned DCs left the brain and reached the cervical lymph nodes, where they found a competent immune system (IS), and (D), might have given in AD, and might give in EAE, origin to specific Tregs, restoring the previously broken tolerance.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



