
Submitted:
25 August 2023
Posted:
25 August 2023
You are already at the latest version
Abstract
Background: Identity diffusion plays a central role in the onset of borderline personality and disorders. The Dialectical Behavioral Therapy for Adolescents (DBT-A) is a treatment program for adolescents with emotional instability and dysregulation. The interest of this study is to examine the influence of a standardized and certified DBT-A therapy program on identity development of adolescents with emotion dysregulation in an inpatient setting.
Methods:
138 adolescents aged 13 to 18 years with symptoms of emotional instability were assessed before and after a curricular 12-weeks in-patient DBT-A program with standardized instruments for the assessment of identity (AIDA), emotion regulation (FEEL-KJ, SEE) and general psychopathology (SCL-90-R, DIKJ).
Results: The results indicate a significant change in identity development, emotion regulation and general symptoms of psychopathology after treatment with DBT-A.
A connection between identity scales and psychopathological symptoms of adolescents with diagnosed borderline disorders and impaired emotion regulation could be established.
Conclusion: In this large sample of adolescents, DBT-A significantly improved identity and reduced identity diffusion. As identiy disturbance is a core symptom of borderline personality disorder, our results may become clinically relevant for the prevention of personality disorders in emotionally unstable adolescents
Keywords:
emotion regulation
; identity
; DBT-A
; adolescents
; Borderline Personality Personality disorders
1. Introduction
Dialectical Behavioral Therapy (DBT) was developed by Marsha M. Linehan [1,2,3] as a disorder-specific therapeutic approach for the treatment of adults with borderline personality disorder (BPD). The effectiveness of DBT has been demonstrated in numerous studies [2,4,5,6,7] A central criterion of BPD is the disturbance of emotional regulation as well as disturbed cognitions and maladaptive behavior. An adaptation specifically designed for the treatment of adolescents (DBT-A) was developed by Miller and Rathus [8,9,10] and a German version by Fleischhaker and colleagues [11]. Evidence-based data indicates promising efficacy of DBT-A for adolescents with BPD symptoms and its effectiveness has been demonstrated by numerous studies and reviews [7,8,10,12].
During adolescence, there are numerous developmental tasks to be addressed, including dealing with adaptive and maladaptive emotional regulation strategies. The possibility of diagnosing BPD in adolescence is considered reliable and valid [13]. Based on the assumption that adolescents with deficits in emotional regulation are a particularly vulnerable group for the development of mental disorders, early interventions are indicated to counteract the chronification of mental disorders [14].
DBT-A can be applied to a variety of disorders focusing on unstable emotional regulation [15].
In DBT-A, the goal is to convey adaptive skills to adolescents as alternatives to maladaptive behavior like self-injurious behavior, impulsive behavior etc. through targeted skills training [15,16]. The Interventions are characterized by a clear structure and a high practical relevance. The basic attitude is dialectical, validating, and mindful. In modules such as skills training, specific abilities are trained with the adolescents, e.g. to increase stress resilience, regulation of strong inner states of tension and emotional regulation [16,17,18].
With regard to the development of personality disorders, identity diffusion is understood to be a pathological development [19,20,21,22], in fact, a central criterion of BPD is a disturbance of emotional regulation and identity development [10]. Identity development plays a central role in healthy and disturbed development from childhood on [7,23] and identity diffusion is related to personality disorders [24] oftentimes associated with unstable attachments, experiences of invalidation, and negative childhood experiences [25]. Identity is described in DSM 5 as a core symptom (criterion 3) of borderline personality disorder [26,27,28]. Moreover, studies indicate a significant relationship between disturbed identity experience and severity of psychopathology [5,19]. The sense of self is determined by coherence and continuity [19,23,27,28]and has a significant influence on the development of e.g. autonomy [29].
Research results imply, that stable identity development is of great importance for personality development and emotional development in adolescence [28]. An unstable identity development can significantly contribute to the development of personality disorders, in particular borderline personality disorder (BPD) [26,30].
Identity, according to [31] can be fundamentally defined on one hand by focusing on the self-referential aspect and, along with it, the idea of being unique as a person, more specifically to be a person with past and future and to be different from others. But on the other hand, identity also includes the experience of being similar to others or sharing with others. Identity has also been reported to significantly impact autonomy development and implies comparison with others involving a dimension in the social context of "belonging" and "differentiation" [32]. Thus, identity is also to be considered in the social context depending on social roles such as occupation, peer group, nationality, child, mother, father, friend, etc. The sense of self is determined by coherence and continuity [24,31]. Many child and adolescent psychiatric disorders (e.g., eating disorders, borderline personality disorder, depression) are accompanied by or even caused by a clinically relevant impairment of identity development [5,33]. As with these findings, it is relevant to know, wheter central apsects of identity development in adolescents can be targeted effectively by a standardized DBT-tretmant program.
The present pilot study therefore examines the influence of a structured DBT-A program on identity development in adolescents diagnosed with BPD or severe emotional dysregulation.
2. Materials and Methods
2.1. Inclusion and exclusion criteria
Inclusion criteria:
- age 13–18
- inpatient referral for non-suicidal self-harming behavior, aggressive/impulsive behavior, emotional crises
- voluntary participation in the structured 3 –month DBT-A- in-patient program
Exclusion criteria:
- diagnoses of schizophrenic or affective psychosis
2.2. Sample description
A total of 188 adolescents were enrolled in the study, referred to inpatient treatment for emotional dysregulation such as emotional instability, self-harming behavior, or impulsive and aggressive behavior.
The study inclusion procedure consisted of a session with a child and adolescent psychiatrist evaluating admissibility regarding indication for elective inpatient treatment and to deliver information about DBT-A and the group-intervention as well as informed consent. All patients received a handout with information and worksheets at the beginning of the study. After informed consent, adolescents were included in the treatment group. The psychometric instruments described below were administered before and after treatment.
A total of 138 patients completing the entire 12 weeks DBT-treatment were finally included for analysis consisting of 17 male and 121 female patients aged between 13 and 18 years (M=16.5; SD = 1.3) who completed the DBT-A-program.

Table 1.
Sample description.
| Sample description | |
|---|---|
| Participants (n) | n = 138 |
| gender % (n) male female |
12,3 (17) 87,7 (121) |
|
M (±SD) Age (min. – max.) |
16,5 (1,3) 13,7 – 18,8 |
|
M (±SD) (Duration of treatment in weeks) |
14,9 (5,9) |
2.3. Diagnoses
Confirmation of the ICD-10-diagnoses (see Table 2) follows a clinical routine workflow with standardized diagnostic procedures specific for the disorder in question.
Although diagnoses (ICD-10) were collected, they were not a prerequisite for participating in the study.
2.4. Statistical analyses
All analyses were conducted using IBM Statistics SPSS, version 27.0.
In the present study, it was of interest whether DBT-A could influence identity development (AIDA) and emotional regulation as well as measures of general psychopathology and also depression.
Only data from 138 participants who completed the DBT-A therapy program and answered all questionnaires completely, thus called "completer", were included in the analysis. Multivariate analysis of variance (MANOVA) was used to examine possible differences between completers and non-completers (n= 50) in the interval-scaled dependent variables of interest.
Identity (AIDA), general psychopathology (SCL-90-R), depression (DIKJ), and emotion regulation (FEEL-KJ, SEE).
Dependent-samples T-tests were performed for within-group comparisons of pre-post scores measuring treatment outcomes. Cohen's d (pooled effect size) was calculated to determine the effect size of the pre-/post-tests. For this purpose, Cohen recommends values of .20 for small effects, .50 for medium effects, and .80 for large effects. Statistical Power Analysis for the Behavioral Sciences (revised edition).
Standardized norm values (t-values) were used for all statistical analyses and descriptive plots.
Pearson's correlation coefficients were calculated to determine the linear relationship between identity development scores, general psychopathology scores, and emotion regulation scores.
2.5. Experimental Intervention and Instruments
Experimental Intervention
DBT-A is a manualized program based on previous research. It comprises different modules within a 12 week time span. DBT-A was administered in single sessions by therapists twice a week and an additional session with a nurse for psychoeducation and skill training promotion.
The skills group trainings took place twice a week for 60 minutes and were held by one therapist and one nurse. The group was conducted with 6-8 adolescents between the ages of 13 and 18. All participants obtained worksheets for the treatment program. Overall, parents and key caregivers were offered facultative skills training (8 sessions).
Each module is structured and follows a standard sequence of activities and tasks, including tools for mindfulness, stress regulation, emotion regulation, interpersonal skills and walking the middle path.
2.6. Psychometric Assessments:
Adolescents were asked to complete the following questionnaires using a PC in a quiet setting accompanied by a therapist in case of comprehensive issues regarding the material or other questions.
Assessment of Identity Development in Adolescence (AIDA)
AIDA [31] (is a self-report questionnaire and a reliable and valid diagnostic instrument to detect disturbed identity development. This questionnaire distinguishes between identity diffusion, consolidates and stable identity.
In clinical practice, it supports the differentiation between normal and severely disturbed identity as the core component of BPD.
AIDA assessment can serve as a tool for indication and evaluation of treatment methods, which focus on identity. It takes into account influences from social-cognitive self-concept research. The main scales "Continuity" and "Coherence" consider emotionally intuitive and cognitive-definition-related areas [19,28,32,34].
In clinical practice, it supports the differentiation between severely disturbed identity as one of the core components of personality disorders like BPD and identity crisis or stable identity development that can be found in other mental disorders. AIDA is developed as a self-screening instrument for adolescents between the age of 12 - 18 years. The goal is the differentiation between a healthy identity development, simple identity crisis and clinically noticeable identity diffusion.
Reliability:
Cronbach's alpha is used to determine reliability with .94 for the overall identity diffusion scale, .87 and .92 for the two main scales discontinuity and incoherence, and between .69 and .84 for the subscale level.
Validity:
The overall identity diffusion scale differentiated highly significantly and with relevant effect size between the school sample and the patient sample. The AIDA total score provides a very large effect size of d = 2.6 standard deviations.
Depression inventory for children and adolescents (DIKJ) [35]
This method is used to record the severity of depressive symptoms in children and adolescents aged 8 to 16 years. All essential symptoms of a depressive disorder according to the criteria of the DSM-5 are being screened for. The DIKJ is also sensitive to changes in the severity of a depressive disorder. The internal consistency (Cronbach's alpha) was found to be .92 in a clinical sample (N = 139) and .87 in an unscreened school sample (N = 3,403).
Symptom Checklist (SCL-90-R) [36]
SCL-90-R general psychopathology was measured via the german version of the revised Symptom Checklist (consisting of the scales somatization, depression, compulsions, general anxiety, social anxiety, phobic anxiety, psychotizism, paranoia, hostility and global severity index. The symptomatic distress is recorded on a five-point Likert scale ("not at all", "a little", "fairly", "strongly", "very strongly"). Three global parameters provide information about the overall level of psychological stress experienced.
It is a self-assessment procedure for adolescents and adults aged 12 and older. Internal consisteny of the nine scales (Cronbachs α) reaches = .64 and = .84 as established in a sample of n = 857 adolescents aged 12-17 years. Three global characteristic values provide information about the overall level of psychological stress experienced. According to the author, the objectivity of implementation, evaluation, and interpretation is given). Content validity is assumed by the author on the basis of interviews with experts.
Questionnaire for the Assessment of Emotional Regulation in Children and Adolescents (FEEL-KJ) [37]
The FEEL-KJ questionnaire is designed for children and adolescents aged 10 to 19,11 years (1,2) and quantifies 15 strategies for emotional regulation and regulation of the specific emotions (all of which are multi-dimensional and specific to a certain emotion): anxiety, sadness, and anger. In two secondary scales, this instrument identifies seven adaptive and five maladaptive emotional regulation strategies. Adaptive strategies include the following sub-scales: problem-oriented acting, distraction, mood improvement, acceptance, forgetting, cognitive problem solving, dealing with anger, anxiety, and grief. Maladaptive strategies include the sub-scales: giving up, aggressive behavior, self-devaluation, withdrawal, perseveration as well as dealing with anger, anxiety, and grief. The additional scales are composed of social support, expression, and emotional control.
Internal consistency of the 15 scales ranges between α =0.69 and α = 0.91. Secondary scales show a consistency of α = 0.93 (adaptive strategies) and α = 0.82 (maladaptive strategies). The Range of the retest-reliability (6-week-stability) is between r = 0.62 and r = 0.81, and for the secondary scales between r = 0.81 (adaptive strategies) and r = 0.73 (maladaptive strategies). The secondary scale called “adaptive scales” for specific emotions shows a very good internal consistency α = 0.88 for sadness, α = 0.83 for anxiety, and α = 0.83 for anger. The maladaptive scale shows internal consistency for anxiety α = 0.59, for sadness α = 0.59 and for anger α = 0.58.
Scales for Experiencing Emotions (SEE) [39]
The Emotional Experience Scales are designed for use in individual and group examinations with adolescents aged 14years and older, as well as adults. It is a theory-based, multidimensional measuring instrument for the central constructs of patient-centered personality theory and the concept of emotional intelligence. The questionnaire is divided into 7 scales obtained through factor analysis and independent of each other. The scales contain 42 items, which include the following seven independent scales: 1. Acceptance of own emotions, 2. Experience of emotion transfer, 3. Experiencing emotional deficiency, 4. Body-related symbolization of emotions, 5. Imaginative symbolization of emotions, 6. Experiencing regulation of emotions, 7. Experiencing self-control.
The scales aim to measure how patients perceive, evaluate, and address their emotions.
The internal consistency of the scales lies between 0.70 and 0.86 (Cronbach’s alpha). Additionally, retest reliability is reported to range from 0.60 to 0.090 between intervals of 2, 3, 4, 10 and 14 weeks.
3. Results
Comparison “completer versus non-completer”
In the final analyses, only those patients (n=138) were included who took part in the entire 12-week long program (completers). To examine possible differences at the beginning of treatment between completers and those patients who did not complete the therapy program (non-completers) a multivariate analysis of variance (MANOVA) with the dependent variables’ identity diffusion, general psychopathology and emotional regulation was carried out.
In the multivariate tests, there were no statistically significant differences at the beginning of the therapy between completers (n=138) and non-completers (n=50) based on the dependent variables, F(7, 180) = 1.621, p > .05, Wilk's Λ = .941, partial η2 = .059. However, the tests of the between-subjects effects and the individual contrasts revealed statistically significant differences (see Table 3) between the two groups on the following scales:
Identity Diffusion (AIDA): F(1) = 4.803, p<.05, η2 = .025
Global Severity Index GSI (SCL-90-R): F(1) = 6.274, p <.05, η2 = .033
This states, that significantly higher values were measured in the reported scales in the group of completers at the start of therapy than in the non-completers (M and SD see table).
There were no statistically significant differences between “completers and non-completers” at the start of therapy in the following scales:
Adaptive strategies (FEEL-KJ): F(1) = 2.822, p >.05, η2 = .015
Maladaptive strategies (FEEL-KJ): F(1) = 2.281, p >.05, η2 = .012
This states, that no significant differences in the reported scales were measured in the group of completers and non-completers at the start of therapy (M and SD see Table 3).
Table 3.
Differences completer vs. non completer at the beginning of therapy.
| completer n= 138 |
non completer n = 50 |
MANOVA | |||
|---|---|---|---|---|---|
| Mean (±SD) | Mean (±SD) | F(df) | Sig. | partial η2 | |
| Diffusion (AIDA) | 65,79 (13,130) | 60,92 (14,351) | 4,80 (1) | .030 | .025 |
| Depression (DIKJ) | 64,18 (11,68) | 57,78 (13,939) | 9,82 (1) | .002 | .050 |
| GSI (SCL-90-R) | 67,82 (11,706) | 62,88 (12,589) | 6,27 (1) | .013 | .033 |
| FEEL-KJ - adaptive strategies (total) | 37,29 (12,793) | 40,76 (11,701) | 2,82 (1) | .095 | .015 |
| FEEL-KJ - maladaptive strategies (total) | 62,19 (13,422) | 58,80 (14,054) | 2,28(1) | .133 | .012 |
Assessment of Impairment of Identity Development in Adolescence (AIDA)
The main scale and two subscales of the AIDA were examined using repeated measures t-tests before and after the standardized DBT-A-Program (see Table 4).
The t-test for the Diffusion subscale revealed a significant result, t(137) = 5.579 , p < .001, d = .67. Thus, higher values were measured in the patients before treatment (M T1 = 66, SD = 13.1) than after the treatment (M T2 = 59, SD = 15.9).
The t-test for the discontinuity subscale also revealed a significant result, t(137) = 5.104, p < .001, d = .63. Thus, higher values were measured in the patients before the hospital stay (M T1 = 67, SD = 12.9) than after treatment (M T2 = 61, SD = 15.5).
Finally, the t-test for the subscale 'incoherence' also revealed a significant result, t(137) = 4.997, p < .001, d = .68. Thus, higher impairment values were measured in the patients before the treatment program (M T1 = 63, SD = 13.4) than after the treatment program (M T2= 57, SD = 15.3).
Depression Inventory for Children and Adolescents (DIKJ)
The t-test for the 'severity of depressiveness' scale (see Table 4) reveals a significant result, t(137) = 7.085 , p < .001, d = .91, indicating that patients had a higher 'severity of depressiveness' score before treatment (M T1 = 68, SD = 11.7) than after treatment (M T2 = 60, SD = 14.6).
Symptom Checklist- (SCL-90-R: Global Severity Index)
The two scales measuring general psychopathology were tested with two repeated measures t-tests.
The t-test for the depression severity scale (see Table 4) revealed a significant result, t(137) = 7.085, p < .001, d = .91, indicating that a higher value for the ‘severity of depression’ was measured in the patients before teatment (M T 1= 68, SD = 11.7) than after treatment (M T= 60, SD = 14.6).
The t-test for the SCL-90-R scale (see Table 3) here for the Global Severity Index (GSI) also showed a significant result, t(137) = 7.282 , p < .001, d = .83, indicating that patients had higher scores in total general psychopathology before treatment (M T1 = 64, SD = 11.8) than after treatment (M T2= 56, SD = 14.6).
Questionnaire for the Assessment of Emotional Regulation in Children and Adolescents (FEEL-KJ) [37]
The two main scales of the FEEL-KJ - "Adaptive Strategies" and "Maladaptive Strategies" were examined using two repeated measures t-tests.
The t-test for the adaptive strategies scale shows a significant result in the pre-post comparison, t (137) = -7.256, p < .001, d = -1.02, indicating that patients had lower scores for the overall "Adaptive Strategies" scale before treatment (M = 37, SD = 12.8) than after treatment (MT2 = 46, SD = 14.5) (see Table 5, and Figure 1).
In addition, the t-test for the scale - "maladaptive strategies" also revealed significant result, t (137) = 4.809, p < .001, d = .48, indicating that patients had higher scores before DBT-A (MT1 = 62, SD = 13.4) than after DBT-A (M T2 = 56.5, SD = 15.3).
The subscales were also examined with repeated-measures t-tests.
Significant effects were also found with respect to the emotional regulation subscales for anger, anxiety, and sadness (see Table 5). There was a significant increase in scores for adaptive strategies and a significant reduction in scores for maladaptive strategies. Overall, small to moderate effects could be found (Cohens’ d) for the maladaptive strategies scales (d=.37 to d=.62) and large effect sizes (d= -.80 to d= -1.03) for the adaptive strategies.
Scales of Experience Emotions (SEE) [39]
The scales of the SEE were also examined using repeated measures t-tests before and after treatment with DBT-A. Significant results were found for the following scales (see Table 4; Figure 2):
Acceptance of own emotions: t (135) = -4.917, p < .001, d = -.66.
Experience of emotion regulation: t (135) = -5.458, p < .001, d = -.79.
Experience of self-control: t (135) = -3.884, p < .001, d = -.46.
This means that significantly lower values were measured before than after treatment (see Table 5)
Experience of emotional overload: t (135) = 5.619, p < .001, d = .82.
Experience of a lack of emotions: t (135) = 4.419, p < .001, d = .48.
This means that significantly higher values (M and SD) were measured before than after treatment (Table 6).
There was no significant change on the following scales:
Body symbolization of emotions: t (135) = 0.409, p > .05,
Imaginative symbolization of emotions: t (135) = -1.017, p > .05.
This means that the values before and after the therapy do not differ significantly from each other (M and SD) (see Table 6).
4. Discussion
This pilot study examined whether dialectical-behavioral therapy for adolescents (DBT-A) inpatient treatment has an impact on the identity development of patients and on measures of psychopathology and emotional regulation in our 12 week long certified structured and standardized DBT-A-Program. We were able to show an improvement on emotional regulation as reported by FEEL-KJ and SEE.
All included patients in this study appear to also benefit significantly from the standardized DBT-A in terms of their experience of identity, as indicated by the reduction of the identity diffusion values in the pre/ post comparison of the pilot evaluation study. These findings do not only have a diagnostic value, but also support the implementation of an early therapeutic intervention using DBT-A in unstable identity experience, to counteract further chronicity in the course of the disease of adolescents [40,41]
Furthermore, the detection of early antecedents of impaired identity development is an important step to allow for early intervention.
These results indicate a diagnostic assessment of identity development in emotionally unstable adolescents as an important apsect of a full clinical diagnosis. The improvement in identity might hypothetically be caused by the increase in adaptive emotion regulation strategies and the reduction of maladpative strategies as a better capability of handling one’s emotions might be directly reflecting on an adolescents’s self –concept. A stable and positive self-concept is of essential importance to counteract potential chronification and progradient disease progression fueled by a fundamentally negative self-concept [5,42,43].
Overall, all participants significantly benefited from standardized DBT-A in the inpatient setting.
Numerous studies in the past have investigated correlations and risk factors for the development of severe emotion regulation disorders and the development of identity diffusion. Bio-psychosocial therapy approaches considering neurobiological disposition and psycho-social risk factors in emergence such as BPD are needed, yet studies on treatment approaches are lacking.
The Assessment of Identity Development in Adolescence (AIDA) records a differentiated assessment of healthy and pathological identity development in adolescence [31,32].
The results also speak for an early therapeutic intervention using DBT-A in unstable identity experience, to counteract further chronicity in the course of the disease of adolescents.
In the long term, early stabilization of adolescents is important both in terms of counteracting the chronification of mental disorders and of social integration and participation [14]. Emotional regulation and a stable identity can be regarded as a central aspect of resilience[44] Early interventions such as DBT-A can contribute to a reduction in admissions and rehospitalizations to child and adolescent psychiatric hospitals. As in the present study, diagnosis and appropriate intervention programs such as DBT-A are of great importance. In DBT-A, the focus should be on symptomatology and levels of functioning and not exclusively on diagnosis [45].
Nevertheless, especially in the field of adolescents, further studies on novel therapy approaches are needed to offer the severely distressed adolescents therapies that validate their needs, especially in adapted methods such as DBT-A as a stepped care treatment approach [32,46,47]. This could validate the needs of the adolescents as well as develop and offer customized therapy approaches regarding the necessary complexity of the treatment (e.g. change between treatment settings - outpatient, partial inpatient, online therapy modules). Especially low-threshold therapy programs [12,14,48,49,50,51] promise to be early and preventive interventions to counteract a chronification of disorders such as BPD, PTSD [20], emotion regulation disorders.
Limitations:
Limitations of our study are the lack of a treatment—as usual—control group. This shall be addressed in future studies. The proven feasibility and large number of benefiting adolescents give rise for the construction of a randomized control trial.
Author Contributions
AD: conceptualization, implementation, data collection, conducted the statistical analysis. AD and EM: drafted the manuscript and the discussion, text creation AD and EM revised the manuscript. All authors contributed to the article and approved the submitted version.
Data Availability Statement
The data set can be assessed from the first author upon request andrea.dixius@uni-saarland.de.
Acknowledgments
The authors would like to thank the adolescents for their participation in the study.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethics Statement
The studies involving human participants were reviewed and approved by the regional Ethics Board of Medical Association Saarland, Germany (No:181/14).The study was performed in accordance with ethical standards laid down in the Declaration of Helsinki 1964 and its later amendments. All legal guardians gave their informed consent, and children and adolescents provided their informed assent prior to their inclusion in the study.
Abbreviations
AIDA: Assessment of Identity Development in Adolescence; BDP, Borderline Personality Disorder; DBT, Dialectical Behavior Therapy; DBT-A, Dialectical Behavior Therapy for Adolescents; DIKJ, Depression inventory for Children and Adolescents; FEEL-KJ, Fragebogen zur Erhebung der Emotionsregulation bei Kindern und Jugendlichen (Questionnaire for the assessment of the emotional regulation in children and adolescents); Global Severity Index (GSI); ICD, International Statistical Classification of Diseases; SEE, Scales of Experience Emotions; Symptom Checklist (SCL-90-R)
References
- Linehan, M.M. Naturalistic Follow-up of a Behavioral Treatment for Chronically Parasuicidal Borderline Patients. Arch Gen Psychiatry 1993, 50, 971. [Google Scholar] [CrossRef] [PubMed]
- Linehan, M.M. Behavioral Treatments of Suicidal Behaviors: Definitional Obfuscation and Treatment Outcomes; Centre for Reviews and Dissemination (UK), 1997.
- Linehan, M.M. DBT Skills Training Manual: Second Edition 2014.
- Copeland, W.E.; Shanahan, L.; Egger, H.; Angold, A.; Psych, M.R.C.; Costello, E.J. Adult Diagnostic and Functional Outcomes of DSM-5 Disruptive Mood Dysregulation Disorder. Am J Psychiatry 2014, 7. [Google Scholar] [CrossRef]
- Chapman, A.L. Borderline Personality Disorder and Emotion Dysregulation. Dev Psychopathol 2019, 31, 1143–1156. [Google Scholar] [CrossRef]
- Charlton, M.; Dykstra, E.J. Dialectical Behaviour Therapy for Special Populations: Treatment with Adolescents and Their Caregivers. Advances in Mental Health and Intellectual Disabilities 2011, 5, 6–14. [Google Scholar] [CrossRef]
- Sharp, C.; Wall, K. Personality Pathology Grows up: Adolescence as a Sensitive Period. Current Opinion in Psychology 2018, 21, 111–116. [Google Scholar] [CrossRef]
- Miller, A.L.; Wyman, S.E.; Huppert, J.D.; Glassman, S.L.; Rathus, J.H. Analysis of Behavioral Skills Utilized by Suicidal Adolescents Receiving Dialectical Behavior Therapy. Cognitive and Behavioral Practice 2000, 7, 183–187. [Google Scholar] [CrossRef]
- Miller, A.L.; Rathus, J.H.; Linehan, M.M. Dialectical Behavior Therapy with Suicidal Adolescents; Guilford Press, 2006; ISBN 978-1-60623-789-2.
- Rathus, J.; Campbell, B.; Miller, A.; Smith, H. Treatment Acceptability Study of Walking The Middle Path, a New DBT Skills Module for Adolescents and Their Families. APT 2015, 69, 163–178. [Google Scholar] [CrossRef]
- Fleischhaker, C.; Böhme, R.; Sixt, B.; Brück, C.; Schneider, C.; Schulz, E. Dialectical Behavioral Therapy for Adolescents (DBT-A): A Clinical Trial for Patients with Suicidal and Self-Injurious Behavior and Borderline Symptoms with a One-Year Follow-Up. Child Adolesc Psychiatry Ment Health 2011, 5, 3. [Google Scholar] [CrossRef]
- Sharp, C.; Fonagy, P. Practitioner Review: Borderline Personality Disorder in Adolescence – Recent Conceptualization, Intervention, and Implications for Clinical Practice. Journal of Child Psychology and Psychiatry 2015, 56, 1266–1288. [Google Scholar] [CrossRef]
- Kaess, M.; Brunner, R.; Chanen, A. Borderline Personality Disorder in Adolescence. PEDIATRICS 2014, 134, 782–793. [Google Scholar] [CrossRef]
- Chanen, A.; Sharp, C.; Hoffman, P. Prevention and Early Intervention for Borderline Personality Disorder: A Novel Public Health Priority. World Psychiatry 2017, 16, 215–216. [Google Scholar] [CrossRef] [PubMed]
- Von Auer, A.K.; Bohus, M. Interaktives Skillstraining für Jugendliche mit Problemen der Gefühlsregulation (DBT-A): Das Therapeutenmanual - Akkreditiert vom Deutschen Dachverband DBT; Klett-Cotta, 2018; ISBN 978-3-608-26934-5.
- Rathus, J.; Miller, A.; Paul, H. Rathus, J.H.; Miller, A.L.; Paul, H. DBT Skills Manual for Adolescents. Guilford Press Child & Family Behavior Therapy 2015, 37, 179–187. [Google Scholar] [CrossRef]
- Buerger, A.; Fischer-Waldschmidt, G.; Hammerle, F.; von Auer, K.; Parzer, P.; Kaess, M. Differential Change of Borderline Personality Disorder Traits During Dialectical Behavior Therapy for Adolescents. Journal of Personality Disorders 2019, 33, 119–134. [Google Scholar] [CrossRef] [PubMed]
- Moran, L.R.; Kaplan, C.; Aguirre, B.; Galen, G.; Stewart, J.G.; Tarlow, N.; Auerbach, R.P. Treatment Effects Following Residential Dialectical Behavior Therapy for Adolescents with Borderline Personality Disorder. Evid Based Pract Child Adolesc Ment Health 2018, 3, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Sollberger, D.; Gremaud-Heitz, D.; Riemenschneider, A.; Küchenhoff, J.; Dammann, G.; Walter, M. Associations between Identity Diffusion, Axis II Disorder, and Psychopathology in Inpatients with Borderline Personality Disorder. Psychopathology 2012, 45, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Schmeck, K.; Schlüter-Müller, S. Early Detection and Intervention for Borderline Personality Disorder in Adolescence. Socijalna psihijatrija 2017, 45, 30–35. [Google Scholar] [CrossRef]
- Schmid, M.; Schmeck, K.; Petermann, F. Persönlichkeitsstörungen im Kindes- und Jugendalter? Kindheit und Entwicklung 2008, 17, 190–202. [Google Scholar] [CrossRef]
- Sevecke, K.; Lehmkuhl, G.; Petermann, F.; Krischer, M.K. Persönlichkeitsstörungen Im Jugendalter. Kindheit und Entwicklung 2011, 20, 256–264. [Google Scholar] [CrossRef]
- Kernberg, P.F.; Weiner, A.S.; Bardenstein, K.K. Persönlichkeitsstörungen bei Kindern und Jugendlichen; Klett-Cotta, 2001; ISBN 978-3-608-94323-8.
- Foelsch, P. The Essentials of Identity – Differentiating Normal from Pathological. Neuropsychiatrie de l’Enfance et de l’Adolescence 2012, 60, S17. [Google Scholar] [CrossRef]
- Penner, F.; Gambin, M.; Sharp, C. Childhood Maltreatment and Identity Diffusion among Inpatient Adolescents: The Role of Reflective Function. Journal of Adolescence 2019, 76, 65–74. [Google Scholar] [CrossRef]
- Sevecke, K.; Schmeck, K.; Krischer, M. Das dimensional-kategoriale Hybridmodell für Persönlichkeits- störungen im DSM-5 aus jugendpsychiatrischer Perspektive: Kritik und klinischer Ausblick. Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie 2014, 42, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Schmeck, K.; Schlüter-Müller, S.; Foelsch, P.A.; Doering, S. The Role of Identity in the DSM-5 Classification of Personality Disorders. Child Adolesc Psychiatry Ment Health 2013, 7, 27. [Google Scholar] [CrossRef] [PubMed]
- Erikson, E.H. Identity: Youth and Crisis; Reissued as Norton paperback 1994.; W. W. Norton & Company: New York London, 1994; ISBN 978-0-393-31144-0. [Google Scholar]
- Foelsch, P.A.; Schlüter-Müller, S.; Odom, A.E.; Arena, H.T.; Borzutzky, H.A.; Schmeck, K. Adolescent Identity Treatment; Springer International Publishing: Cham, 2014; ISBN 978-3-319-06867-1. [Google Scholar]
- Gander, M.; Buchheim, A.; Bock, A.; Steppan, M.; Sevecke, K.; Goth, K. Unresolved Attachment Mediates the Relationship Between Childhood Trauma and Impaired Personality Functioning in Adolescence. Journal of Personality Disorders 2020, 1–20. [Google Scholar] [CrossRef]
- Goth, K.; Foelsch, P.; Schlüter-Müller, S.; Birkhölzer, M.; Jung, E.; Pick, O.; Schmeck, K. Assessment of Identity Development and Identity Diffusion in Adolescence - Theoretical Basis and Psychometric Properties of the Self-Report Questionnaire AIDA. Child Adolesc Psychiatry Ment Health 2012, 6, 27. [Google Scholar] [CrossRef] [PubMed]
- Goth, K.; Birkhölzer, M.; Schmeck, K. Assessment of Personality Functioning in Adolescents With the LoPF–Q 12–18 Self-Report Questionnaire. Journal of Personality Assessment 2018, 100, 680–690. [Google Scholar] [CrossRef]
- Paulus, F.W.; Ohmann, S.; Möhler, E.; Plener, P.; Popow, C. Emotional Dysregulation in Children and Adolescents With Psychiatric Disorders. A Narrative Review. Front. Psychiatry 2021, 12, 628252. [Google Scholar] [CrossRef]
- Euler, S.; Dammann, G.; Endtner, K.; Leihener, F.; Perroud, N.A.; Reisch, T.; Schmeck, K.; Sollberger, D.; Walter, M.; Kramer, U. Borderline-Störung: Behandlungsempfehlungen Der SGPP. Swiss Archives of Neurology, Psychiatry and Psychotherapy 2018, 169, 135–143. [Google Scholar] [CrossRef]
- Joachim Stiensmeier-Pelster; Monika Braune-Krickau, Karin Duda, Ed.; Martin Schürmann; Karin Duda Depressionsinventar Für Kinder Und Jugendliche; Hogrefe: Göttingen, 2014. [Google Scholar]
- Franke, G. Die Symptom-Checkliste von Derogatis (SCL-90-R) - Deutsche Version - Manual; Hogrefe: Göttingen, 2002. [Google Scholar]
- Grob, A.; Smolenski, C. Fragebogen Zur Erhebung Der Emotionsregulation Bei Kindern Und Jugendlichen (FEEL-KJ); 2nd ed.; Huber: Bern, 2009. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J Health Soc Behav 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Behr, M.; Becker, M. Skalen Zum Erleben von Emotionen; Hogrefe: Göttingen, 2004. [Google Scholar]
- Zimmermann, R.; Fürer, L.; Schenk, N.; Koenig, J.; Roth, V.; Schlüter-Müller, S.; Kaess, M.; Schmeck, K. Silence in the Psychotherapy of Adolescents with Borderline Personality Pathology. Personality Disorders: Theory, Research, and Treatment, 2020. [Google Scholar] [CrossRef]
- Jung, E.; Pick, O.; Schlüter-Müller, S.; Schmeck, K.; Goth, K. Identity Development in Adolescents with Mental Problems. Child Adolesc Psychiatry Ment Health 2013, 7, 26. [Google Scholar] [CrossRef]
- Thompson, K.N.; Jackson, H.; Cavelti, M.; Betts, J.; McCutcheon, L.; Jovev, M.; Chanen, A.M. The Clinical Significance of Subthreshold Borderline Personality Disorder Features in Outpatient Youth. Journal of Personality Disorders 2019, 33, 71–81. [Google Scholar] [CrossRef]
- Gross, J.J.; Thompson, R.A. Emotion Regulation: Conceptual Foundations. In Handbook of emotion regulation; The Guilford Press: New York, NY, US, 2007; pp. 3–24. ISBN 978-1-59385-148-4. [Google Scholar]
- Fergus, S.; Zimmerman, M.A. ADOLESCENT RESILIENCE: A Framework for Understanding Healthy Development in the Face of Risk. Annu. Rev. Public Health 2005, 26, 399–419. [Google Scholar] [CrossRef] [PubMed]
- Von Auer, A.K.; Bohus, M. Interaktives Skillstraining für Jugendliche mit Problemen der Gefühlsregulation (DBT-A): Das Therapeutenmanual - Akkreditiert vom Deutschen... - Inklusive Keycard zur Programmfreischaltung; 1.; Schattauer, 2017; ISBN 978-3-608-43116-2.
- Schrobildgen, C.; Goth, K.; Weissensteiner, R.; Lazari, O.; Schmeck, K. Der OPD-KJ2-SF – Ein Instrument zur Erfassung der Achse Struktur der OPD-KJ-2 bei Jugendlichen im Selbsturteil. Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie 2019, 47, 428–440. [Google Scholar] [CrossRef] [PubMed]
- Birkhölzer, M.; Goth, K.; Schrobildgen, C.; Schmeck, K.; Schlüter-Müller, S. Grundlagen Und Praktische Anwendung Des Assessments of Identity Development in Adolescence (AIDA)/ Background and Practical Use of the Assessment of Identity Development in Adolescence (AIDA). Praxis der Kinderpsychologie und Kinderpsychiatrie 2015, 64, 584–600. [Google Scholar] [CrossRef] [PubMed]
- Dixius, A.; Möhler, E. Feasibility and Effectiveness of a New Short-Term Psychotherapy Concept for Adolescents With Emotional Dysregulation. Front. Psychiatry 2021, 11, 585250. [Google Scholar] [CrossRef] [PubMed]
- Dixius, A.; Michael, T.; Altpeter, A.; Ramos Garcia, R.; Möhler, E. Adolescents in Acute Mental Health Crisis : Pilot-Evaluation of a Low-Threshold Program for Emotional Stabilization. 2023. [CrossRef]
- Dixius, A.; Möhler, E. START – Entwicklung einer Intervention zur Erststabilisierung und Arousal-Modulation für stark belastete minderjährige Flüchtlinge. Praxis der Kinderpsychologie und Kinderpsychiatrie 2017, 66, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Dixius, A.; Möhler, E. A Pilot Evaluation Study of an Intercultural Treatment Program for Stabilization and Arousal Modulation for Intensely Stressed Children and Adolescents and Minor Refugees, Called START (Stress-Traumasymptoms-Arousal-Regulation-Treatment). ARC Journal of Psychiatry 2017.
Figure 1.
Questionnaire for the Assessment of Emotional Regulation in Children and Adolescents (FEEL-KJ) (Grob & Smolenski, 2009) - adaptive and maladptive scales in total.
Figure 1.
Questionnaire for the Assessment of Emotional Regulation in Children and Adolescents (FEEL-KJ) (Grob & Smolenski, 2009) - adaptive and maladptive scales in total.
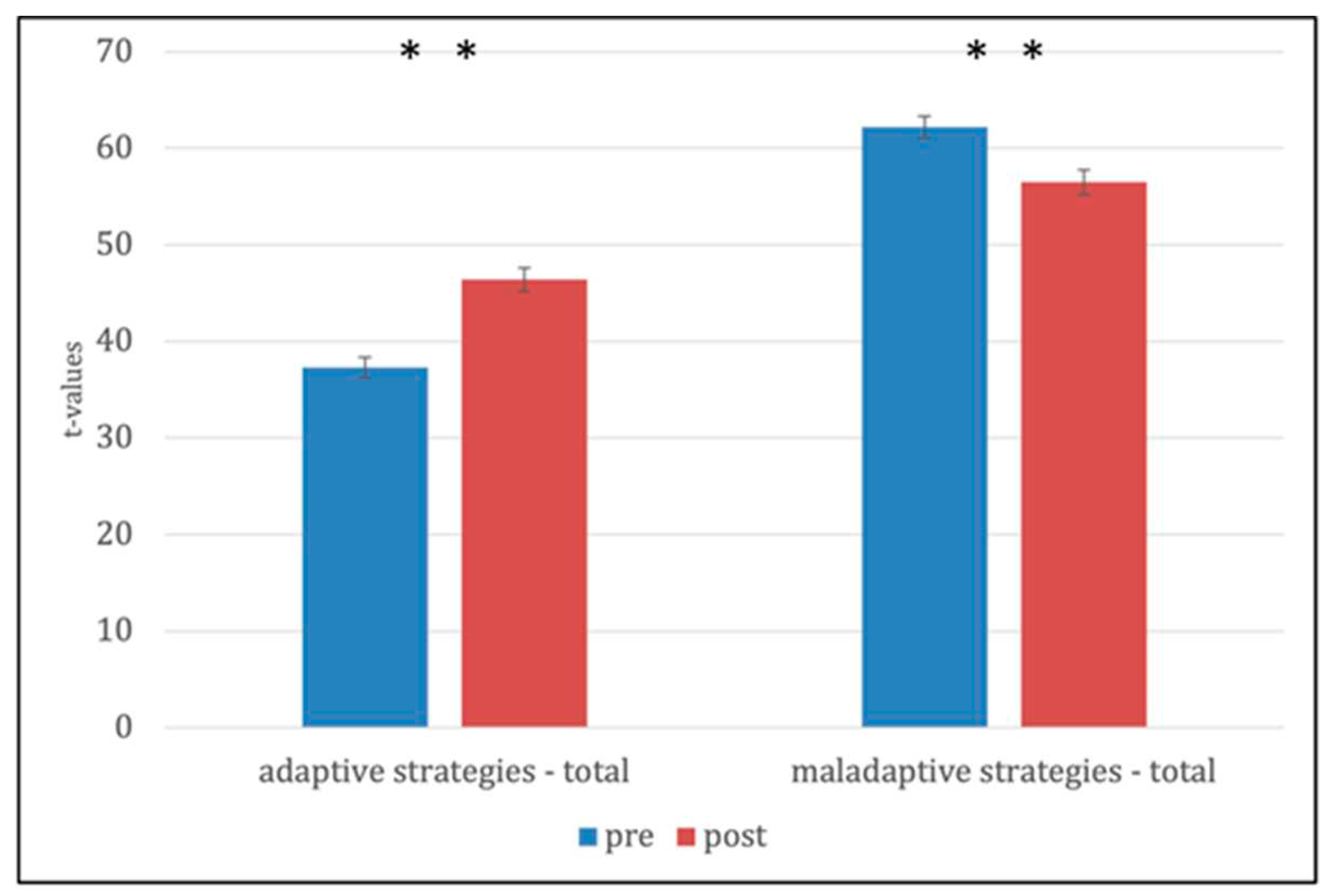
Figure 2.
Scales of Experience Emotions (SEE).
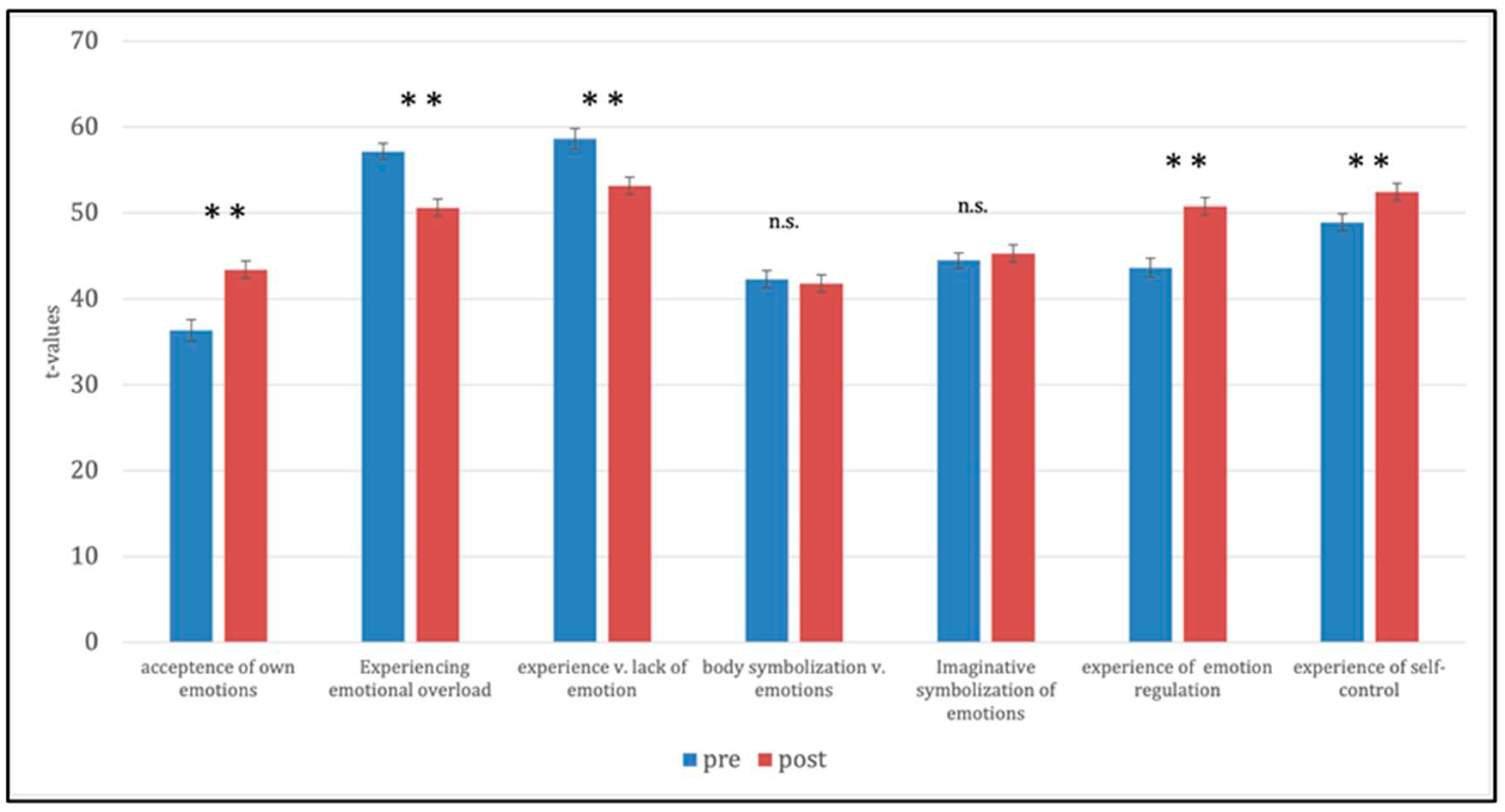
Table 2.
Diagnoses - International Statistical Classification of Diseases (ICD-10).
| Diagnosen | ICD-10 | Frequency(n) | Percentage (%) |
|---|---|---|---|
| Adjustment disorder | F43.2 | 4 | 3 |
| Anorexia nervosa | F50.1 | 25 | 18 |
| Bulimia nervosa | F50.2 | 7 | 5 |
| Dissociative convulsions | F44.5 | 1 | 1 |
| Emotionally unstable personality disorder | F60.31 | 47 | 34 |
| Moderate depressive episode | F32.1 | 15 | 11 |
| Other mixed disorders of conduct and emotions | F92.8 | 1 | 1 |
| Other specific personality disorders | F60.8 | 1 | 1 |
| Post-traumatic stress disorder | F43.1 | 34 | 24 |
| Social phobia | F40.1 | 2 | 1 |
| Somatization disorder | F45.0 | 1 | 1 |
Table 4.
Results: Pre-/ post comparison:.
| Assessment of Identity Development in Adolescence (AIDA) Depression Inventory for Children and Adolescents (DIKJ) Symptom Checklist- (SCL-90-R: Global Severity Index) | |||||||
| AIDA | M T1 (±SD) | M T2 (±SD) | M dif (±SD) | t | df | p | d |
| Diffusion | 65.8 (13.1) | 58.7 (15.9) | 7.1 (-2.8) | 5.579 | 137 | < .001 | .67 |
| Discontinuity | 67.2 (12.9) | 60.9 (15.5) | 6.3 (10.3) | 5.104 | 137 | < .001 | .63 |
| Incoherence | 63.2 (13.4) | 57.2 (15.3) | 6,0 (-1.9) | 4.997 | 137 | < .001 | .68 |
| DIKJ | 67.8 (11.7) | 59.7 (14.6) | 8.1 (-2.9) | 7,085 | 137 | < .001 | 0.91 |
| GSI (SCL-90-R) | 64.2 (11.8) | 55.5 (14.6) | 8.7 (-2.8) | 7,282 | 137 | < .001 | 0,83 |
Table 5.
Questionnaire for the Assessment of Emotional Regulation in Children and Adolescents (FEEL-KJ).
Table 5.
Questionnaire for the Assessment of Emotional Regulation in Children and Adolescents (FEEL-KJ).
| FEEL-KJ | M T1 (±SD) | M T2 (±SD) | M dif. (±SD) | t | df | p | d |
|---|---|---|---|---|---|---|---|
| adaptive strategies (total) | 37.3 (12.8) | 46.4 (14.5) | -9.1 (-1.7) | -7.256 | 137 | < .001 | -1.02 |
| Anger | 38.1 (12.1) | 46.7 (13.5) | -8.6 (-1.4) | -7.050 | 137 | < .001 | -1.03 |
| Anxiety | 38.2 (12.4) | 46.9 (14.1) | -8.7 (-1.7) | -6.135 | 137 | < .001 | -.80 |
| Grief | 38.9 (12.3) | 46.6 (13.8) | -7.7 (-1.5) | -6.249 | 137 | < .001 | -.86 |
| maladaptive strategies (total) | 62.2 (13.4) | 56.5 (15.3) | 5.7 (-1.9) | 4.809 | 137 | < .001 | .48 |
| Anger | 59.9 (13.0) | 55.3 (14.2) | 4.6 (-1.2) | 4.176 | 137 | < .001 | .49 |
| Anxiety | 60.5 (13.7) | 55.8 (15.3) | 4.7 (-1.6) | 3.644 | 137 | < .001 | .37 |
| Grief | 61.4 (12.2) | 55.6 (13.7) | 5.8 (-1.5) | 5.354 | 137 | < .001 | .62 |
Table 6.
Scales of Experience Emotions (SEE).
| SEE | M T1(±SD) | M T2(±SD) | M dif(±SD) | t | df | p | d |
|---|---|---|---|---|---|---|---|
| acceptance of own emotions | 36.1. (14.8) | 43.4 (17.2) | -7.3 (-2.4) | -4,917 | 137 | < .001 | -.66 |
| experience of emotion regulation | 57.3 (11.2) | 50.6 (12.4) | 6.7 (-1.2) | 5,619 | 137 | < .001 | .82 |
| experience of emotional overload | 58.9 (14.1) | 53.2 (13.3) | 5.7 (1.0) | 4,419 | 137 | < .001 | .48 |
| body symbolization of emotions | 42.2 (11.8) | 41.8 (11.8) | 0.4 (0,0) | 0.409 | 137 | > .05 | - |
| imaginative symbolization of emotions | 44.5 (10.4) | 45.3 (10.4) | -0.8 (0.0) | -1.017 | 137 | > .05 | - |
| experience v. Emotion regulation | 43.3 (12.7) | 50.8 (13.4) | -7.5 (-0.7) | -5.458 | 137 | < .001 | -.79 |
| experience v. self-control | 48.7 (11.6) | 52.5 (11.3) | -3.8 (0.3) | -3.884 | 137 | < .001 | -.46 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



