
Submitted:
28 August 2023
Posted:
29 August 2023
You are already at the latest version
Preprints.org 2023 Most Popular Preprints Award Winner Collection
Abstract
Maxillofacial defects, arising from trauma, oncological disease or congenital differences, detrimentally affect everyday life. Prosthetic repair offers the aesthetic and functional reconstruction with the help of materials mimicking natural tissues, among which polymers take unprecedented role. The three-dimensional (3D) printing techniques based on the computer-aided design, where polymers are essential, provide a rapid and cost-effective workflow protocol to perfectly restore patient-specific anatomy for prosthetics. This review discusses the main 3D printing approaches to maxillofacial prostheses fabrication: extrusion and lithography, which are radically preferable to the traditional methods. The main assessment criteria, affording the polymer implementation in 3D printing of prostheses, as well as the characteristics of the key advanced polymers, are considered. The success of the prosthesis is shown to be largely dependent on the retention system, predominantly using polymers in the form of adhesives and osseointegrated implants as a support for the prosthesis. The approaches and technological prospects are also discussed in the context of specific aesthetic restoration on the example of the nasal, auricle and ocular prostheses. 3D printing techniques determine the development of personalized approaches to improve aesthetic and functional effect of prosthetics in patients with maxillofacial defects.
Keywords:
3D printing
; polymers for maxillofacial prostheses
; adhesives
; osseointegrated implants
; nasal
; auricle and ocular prostheses
1. Introduction
Every year, approximately 69 million persons worldwide suffer from maxillofacial defects due to cancer, trauma or congenital diseases [1], which represent significant psychological, social, and economic disadvantages, and, above all, are the cause of death and disability [2]. In many cases, the reconstruction of maxillofacial defects is a challenging, and it is difficult to achieve a satisfactory result, because of the anatomical complexity, the risk of infection, and disruption of critical anatomical structures. This bottleneck also relates to the desire to get a positive aesthetic outcome and the presence of various tissue types (bone, cartilage, muscle, and skin) and structures (auricle, orbit, nose, oral cavity) in the immediate vicinity. Some of the critical factors also contributing to complexity include the deficits of soft or bone tissues, the mobility of the affected tissue, the uniqueness of each defect and the chances of infection.
Prosthetics is aimed at restoring the aesthetics and function using materials that mimic the native tissue features, along with high-quality prosthetic fixation. In maxillofacial reconstruction, the prostheses are typically required to replace structures in the dental, oral, orbital, and nasal regions [3,4]. The ideal prosthesis should mimic the visual, textural, and mechanical characteristics very similar to the missing or damaged tissue [4,5].
The first prosthetics date back to ≈2300 BC, when Egyptians reconstructed mummies with molded plaster filled with mud, sand, linen, butter, or soda [6]. Until the 16th century, the choice of materials for elementary prostheses was limited by wood, cloth, natural waxes, resins, and metals. Prostheses of noses and eyes made from parchment, wax, wood, rubber, gold, silver, and copper prevailed and remained relatively unchanged for thousands of years. The main materials throughout the 19th century were metals due to their ability to be easy molded into various shapes [6,7]. Although metals have been utilized successfully for many years, metal implants do not meet all biomechanical requirements: tissue stress occurs around the implant, they may corrode and cause cytotoxic reactions by releasing metallic ions [8]. At the beginning of the 20th century, the first ocular polymer prosthesis based on poly(methyl methacrylate) (PMMA) was developed. This polymer found application as the most common prosthetic material of that time, and is still in use today[9]. Further progress in polymer chemistry in the 20thcentury have delivered a lot of new synthetic polymer materials that can be classified according to their properties, such as hetero- and homopolymers, copolymers of diverse compositions and structure, elastomers and plastics, thermoplasts and thermosets, etc. These materials represent wide variety of physical properties ranging from hard, stiff to soft, flexible polymers, as well as in the form of particles and plastisol. Special place belongs to silicone, which remains a main prosthetic material today due to its soft tissue-like properties, ease of processing, chemical inertness, durability, and excellent biocompatibility[10,11]. Synthetic polymers have provided significant advances in manufacturing, great similarity to substituted tissues and utility [12].
Digital prosthetic planning using 3D printing represents one of the most outstanding technological achievements of the recent decades. Traditional methods of maxillofacial prosthesis fabrication are now radically affected by advanced 3D manufacturing techniques, rational design of the new materials, and prosthetic methods. Although the traditional and advanced processes follow the same basic route: acquire morphology of the patient tissue loss site, model and fabricate the prosthesis, the traditional prosthesis preparation requires the implication of high-skilled and intensive labor [13]. (Figure 1). Traditional approaches start from taking a physical impression of the patient anatomy, which can be traumatic for the patient [14]. These impressions are employed for mold fabrication as a basis for hand-sculpting a prosthetic prototype, usually made from wax [15]. The final prosthesis material is then casted into the mold produced with the wax prototype. The wide variety of casting conditions mainly determines the level of complexity and detail of manufacturing. For example, room temperature processing can be applied for some prosthetic materials allowing the use of plaster, acrylic or epoxy molds, while others require high temperature for their treatment demanding more expensive molds and complicated processing [7]. After casting, prostheses usually need to be hand-painted to achieve an aesthetic effect, which complicates material selection and increases labor costs.
3D-printing techniques, involving 3D scanning, computer modeling, and 3D printing, make it possible to create the most complex maxillofacial prosthesis with high precision, tailored to personal needs [16]. Advanced manufacturing, along with the high degree of personalization and realistic appearance, is associated with computer-aided facility and easier patient access to high quality prosthesis through lower costs. The overall process is not labor-intensive and takes a shorter treatment time [17]. At present, a very limited number of 3D printed prostheses are available for clinical utilizations, although digital technology has been implemented in prosthetic field for the past 30 years [17,18]. It is only the last decade, the significant outcome of 3D technologies has seen in prosthesis manufacturing, as evidenced by growing number of reports in the literature [19]. The combination of both the innovations in 3D printing and advanced new materials and blends, especially polymers, has led to the rapid adoption of 3D technologies in practice and the replacement of traditional approaches to prosthesis fabrication.
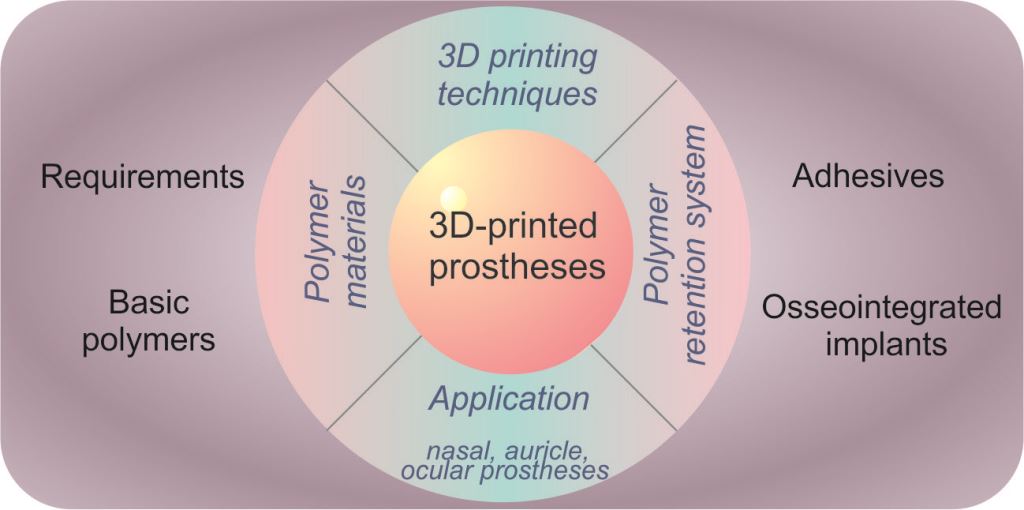
This review aims to demonstrate the recent advances in 3D-printing of polymer materials for more effective personalized reconstruction of complex maxillofacial defects. We consider the 3D-printing techniques based on extrusion and lithography, highlighting the main approaches suitable for polymer prosthesis fabrication. The design of materials mimicking natural tissue is the important task in prosthetics and the main characteristics of such materials with the specificity of polymers is overviewed here, as well as the avenues for further research. The number of the most common polymer materials and their blends are described in the context of their utilization in 3D printing. The reconstruction effect of prostheses is associated with the fixation system, among which polymer adhesives and supporting implants are considered the most popular. 3D-printed polymer implants are at an early stage of development and are poorly represented in the literature, but we show some applications of these osseointegrated implants in the section devoted to the reconstruction of the nasal, auricle and ocular areas with 3D-printed prostheses. The presented polymer prostheses illustrate the possibilities and significant advantages of 3D printing in terms of aesthetic effects, accuracy, comfort, less time, and labor consuming for individual adjustment.
2. 3D printing technology
2.1. Background
3D printing technology, also known as rapid prototyping or additive manufacturing, was first described by Hull in 1984 using stereolithography or “printing” by depositing materials layer by layer to form a 3D-object [20]. To date, the broad scope of 3D bioprinting governs its application in multiple disciplines, including maxillofacial prosthesis.
This advanced technology is based on the creation of an object from materials in a liquid, powdery or molten states as a result of their solidification in the course of fusing layer upon layer [21]. The first step in 3D printing is the medical imaging or 3D scanning of the target location for prosthesis attachment, as well as any normal contralateral anatomy to model the prosthesis. Tomographic imaging is predominant in the collection of data on the deficient facial structure in order to assess the features of the previously intact tissue [22]. However, despite the popularity of conventional imaging techniques (exploiting radiation) in prosthesis design, there is a need for a safer modality for data acquisition, such as optical modeling [23]. In more complex cases, included larger defects or the need to bypass delicate vital structures, a digital prosthetic model should be delivered using the healthy contralateral surface as a template [24].
In the next step, the scan data is transferred into modeling software for the digital design of the final prosthetics. There are a number of computer-aided design (CAD) packages[94 p-p] based on engineering modeling on the market, such as Mimics, Amira, Rhino, SurgiCase, ITK-Snap, InVesalius, and 3D Slicer [13]. The modeling product then is converted for utilization in printers according to the used materials and the differences in resolution between software and printing capabilities. Despite a great variety, all 3D printing technologies build up a 3D object using a layer-by-layer approach with each layer representing a 2D slice of the object [25]. The fashion of each layer formation predominantly determines the final properties of the prosthesis. Typically, 3D printing methods can be divided into two groups: those in which material is selectively supplied or deposited from an extrusion device, and those in which a layer of liquid or powdered material is selectively melted (sintered), bonded, or polymerized, similar to lithography [26] (Figure 2).
2.2. Extrusion-based 3D printing
The most popular extrusion-based printers are based on fused deposition modeling (FDM). Such a printer feeds a solid thermoplastic filament into a hot extruder nozzle, where filament is melted into a semi-fluid state and deposited either on a platform or on top of an already formed layer. Then, the build plate moves down (or the nozzle up), providing the fabrication of the next layer[27] (Figure 2). A solidification at room temperature leads to a continuous structure material due the fusion of the layers together. Variation in the printing speed, thickness of layer and construct orientation drives the desired change in the tissue construct quality.
Extrusion-based 3D printers exploit a broad range of low-cost materials, and, compared to others, can provide rapid fabrication of both large-scale constructs and constructs made of composite materials. These printers can also be tailored for dosing a variety of material with proven ability to induce osteoblast growth, such as calcium phosphate, ceramics, or cell-laden hydrogel, etc. [28]. They also have a broad range of available low-cost materials, including both rigid and flexible polymers [29]. The main advantages relate to the cost efficiency and the ability to print multicomponent materials using a multi-nozzle printer [30]. FDM printing implies the utilization of only thermoplastic material, namely, biocompatible materials with low melting points, such as polycarbonate (PC), copolymer of acrylonitrile, butadiene and styrene (ABS), polycaprolacton (PCL), or polylactide (PLA) [31].
In the other extrusion-based approaches, the construct layer is formed similar to FDM, however viscous material is forced out by the applied pressure using pneumatic or mechanical means. The individual layer is then exposed to UV light or heated on the stage in order to cure after printing, resulting in the desired construct [32]. The main advantage of this technique is a wide variety of the materials, including hydrogel, plastics, pastes, photopolymers, solutions [30,33,34]. However, this method is characterized by the low resolution and speed, as compared to FDM technique. Besides, materials must possess a high viscosity or have a high polymer content to maintain integrity, shape and structure under the action of external forces [35].
Adaptations of this approach to bioprinting and curing via multipart mixing of the material enabled the development of multi-head deposition system (MHDS) [36]. 3D material extrusion is also the basis for several direct 3D printing of silicone approaches [11], two-photon polymerization processes [37].
On the basis of extrusion, including MHDS, the concept of 4D printing has been developed. The main feature of 4D printing is the ability to print 3D objects that can change its shape, properties or function over time in response to external stimuli, such as temperature, light, water, etc. [38]. Changing the shape of structures is based on the use of either stimuli responsive materials, or on the creation of localized self-deformation inside the printed object during or after printing [39].
2.3. Lithography-based 3D printing
To date, there are a lot of different 3D printing technologies that are based on the lithography process, when the formation of two-dimensional layer occurs on the surface of the material in the vat. Typically, the material solidification proceeds under laser irradiation, and the non-irradiated liquid composition is removed from the work area. Laser-assisted bioprinters do not have nozzles that makes it possible to escape the direct contact between the materials and the dispenser, preventing clogging and material constricting. The layer can be formed on the surface of a liquid or powder material under the laser irradiation resulted in selectively sintering, bonding or polymerization according to the CAD model [13] (Figure 2).
Selective laser sintering (SLS) fabricates objects under laser action by sequentially fusing a thin layer of polymer powder, filling the vat. After creation of one layer, the platform with powder is lowered, the next layer is rolled over it and the whole process repeats. Following the CAD model, the selective powder fusion ensures the formation of the desired solid construction (Figure 2) [40]. SLS has the unique advantage of providing internal support for ready-made layers. When the layer is printed, all the remaining raw plastic powder remains on the assembly platform and serves to "support" the features of the printed project. SLS is a rapid, high resolution technique compatible with diverse polymers, from rigid and strong to flexible materials. Products made through powder-based 3D printing, in contrast to filament-based, are more isotropic in their properties, so the mechanical characteristics are the same across all directions. The usually used materials are metals, bioceramics, and synthetic polymers like polylactic acid (PLA), polycaprolactone (PCL), polyethyl-ether-ketone (PEEK), and polyether-ketone-ketone (PEKK), which can be reinforced with ceramics. The main disadvantage of SLS is that it is much more expensive compared to 3D printing methods that use plastic filament or resin [41].
Another technique, similar to SLS, is binder jetting (BJ), which, instead of the powder sintering, enables solid construct formation without a laser, but due to dispensing liquid binding agent onto the powder with print-head jets to form a two-dimensional pattern on a layer. After each layer, the build platform is lowered, and the next layer is prepared [42]. BJ systems are also characterized by a relatively high rate compared to other 3D printing like extrusion, since only a fraction of the total volume, namely the binder, needs to print. The semi-crystalline polymers appeared to be more preferable over amorphous polymers for utilization as the binder phase due to their higher density compared with amorphous polymers[43]. However, semi-crystalline polymers must be preheated to just below Tm before binder jetting, since they can shrink upon solidification, causing component distortion [44]. After SLS, the object must be cooled to room temperature slowly.
Stereolithography (SLA) is one of the oldest 3D printing technologies, using a laser irradiation to cure a liquid resin photocomposition in a layer-by-layer manner [45]. A laser beam located above/below the vat scans the surface, curing the composition on the platform in the form of a 2D- layer as a cross-section of the 3D model. Then the platform is lowered/raised to the thickness of the next layer and the scanning is repeated (Figure 2). A variation of SLA is masked SLA printing technology, when a photocomposition is applied in a thin layer to a physical photomask or "mask" of the corresponding contour. The formation of each layer is governed by the laser beam movement over a large surface area, printing constructs of a relatively large size (up to 50x50 cm) with high precision. However, SLA significant restrictions is the limited choice of photopolymers, since they mainly allow the manufacture of rigid 3D construction that do not meet the requirements of maxillofacial prosthetics [46].
The innovative SLA methods, such as digital light projection (DLP) method and the liquid crystal display method (LCD), provide high resolution (10 ± 50 m) at faster print speed. These methods exploit simultaneous irradiation of the entire polymer layer, producing objects according to the mask formed by the DLP or LCD matrixes, unlike traditional SLA technology, where point scanning occurs [26] (Figure 2).
The desire to improve print quality and speed is driving the design of new SLA techniques, among which can be distinguished computed axial lithography (CAL) [47], continuous liquid interface production (CLIP) [48], holographic 3D printing, as well as techniques based on two photon polymerization (2PP) [49].
Despite the widespread utilization of 3D printing technology in prosthesis creation, there are some limitations that should be mentioned. The entire 3D printing technique from the image acquisition to the maintenance of the printing process requires the participation of skilled technical staff. The important limiting factor is the printer costs, mainly determined by the implication of digital systems and large-scale yields. Besides, not all 3D printers can imply all types of polymers and maintain a consistent quality of 3D-printed structures [50]. Post-processing and sterilization methods should be thoroughly adjusted to prevent deterioration of the biomechanical and biological properties of the final 3D products [51]. For the desired application, some 3D printing techniques cannot provide structures with required mechanical strength resulting in gradual deformation, exhibit low production resolution [52]. These factors are critical for clinical application and should be carefully evaluated.
3. Polymers for 3D printing of prostheses
3.1. Relevant characteristics of prostheses
Recently, the progress in 3D printing have guided the development of new materials, specialized material blends and crosslinking methods to fine-tune their mechanical and visual properties suitable for3D printing. The leading place among materials actively used in maxillofacial prosthetic, such as metals, their alloys, ceramics, belongs to polymers and their blends. Their advantages are associated with the ability to simulate native tissue both functionally and aesthetically, providing excellent safety, adjustability, reliability, and robustness. There are numerous polymers available for 3D printing from soft elastomeric polymers to rigid nylons and acrylonitrile butadiene styrene copolymers, as well as blends of methacrylates, urethanes, siloxanes and other engineered polymers [53].
The desirable properties of maxillofacial prosthetic material can be divided on:
1. Physical properties, such as flexibility, dimensional stability, light weight, low thermal conductivity, and mechanical strength.
2. Biological and chemical properties, including biocompatibility, non-toxicity, hypoallergenicity. Moreover, materials must remain unchanged both in environmental surroundings, and when exposed to adhesives and their solvents, have lifetime of at least six months without significant damage to aesthetic and physical properties.
3. Fabrication conditions, which are associated with polymerization conditions, namely, the temperature ensuring the reusability of molds, suitable duration, the chance of dye embedding or coating, as well as the easy blending of individual components.
4. Aesthetic characteristics, implying the unnoticeable prosthesis properties in public, accurate reproduction of the lost structure in the finest detail, imitating the color, texture, form and transparency of missing structure and adjacent skin [12].
One of the important issues in prosthetics is the imitation of visual, textural, and mechanical characteristics of missing or damaged tissue [18]. The corresponding ranges of characteristic parameters are summarized in Table 1. The prosthesis should be fabricated strong and tough, but at the same time soft and flexible enough to respond to the motions of the patient face. Living organisms often consist of tissues with a Young’s modulus of 103–109 Pa (for example, skin or muscle tissue), so it is desirable that the prosthetic polymers have modulus in the range of biological materials [54]. Tensile strength, elongation at break, modulus of elongation, and tear strength determine the resistance of a prosthesis to rupture during the use and maintenance, as well as its compliance to facial movement. High values of strength, toughness, and tear strength are desirable along with low values of hardness and elongation modulus. Modulus of elongation at 100% extension is normally measured, although values of initial modulus are likely to be more substantial, since facial movements rarely exceed 10% [55].
The glass-transition temperature must be low enough to ensure the flexibility of the prosthesis on cold days, since noticeable stiffening can occur at 10 to 20oC above this temperature. The heat distortion temperature should be above 120°C, as boiling the prosthesis in water or steam sterilization should not cause distortion, even if neither procedure is recommended. The material can be doped with dye and must retain intrinsic and extrinsic coloration [56]. A relatively low critical surface tension is necessary for the application of oil-based cosmetics, while tension should also be high enough to facilitate their removal with soap and water. The prosthesis should demonstrate skin-like values of friction and hardness. Environmental factors (rainy or dry weather, sunlight, wind, etc.) should not affect the prosthesis properties [13].
Moreover, the material must be easily accessible at a reasonable price, have a sufficient life time, and be well stored and repaired. The prosthesis should not release plasticizer or additives, be compatible with strong adhesives, or well adhere to surgical tapes [57]. The preference is given to lightweight prostheses, as well as hollow or foamed ones. Finally, it is extremely important that prosthesis is biocompatible, non-toxic, non-allergenic, non-immunogenic, breathable [58].
The biggest challenge in prosthetics relates to mimicking the human skin, consisting of several layers with various cells, glands, vessels, and follicles, which give the skin its diverse properties and complex function. Synthetic polymer can replicate the skin structure only to some extent, though some of vital characteristics can be reproduced. The focus is on aesthetics such as translucency, texture, matching the intrinsic skin tone, as well as tactile properties such as elasticity and softness. [18]. A modern soft-tissue prosthesis typically contains a skin-like layer, which attaches to a foundation, maintaining shape and mechanical characteristics, responsible, in some cases, for magnetic or mechanical clips attachment [59]. Traditional polymers, such as poly(vinyl chloride), polyurethane elastomer, chlorinated polyethylene, and silicone were utilized to create skin-like layers of prostheses [60].
Substructures and eye prostheses are typically fabricated from rigid polymers, such as acrylic resins (e.g. PMMA) and rigid 3D printable polymers. Modern 3D printers enable formation of multicomponent prostheses, which is particularly a challenge in the case of silicones lacking the adhesion to other materials. The most advanced printers can selectively mix several components to fine-tune the final material properties. For example, a 3D object can be printed rigid and transparent at one end with a smooth transfer to flexible and opaque at the other end.The potential of 3D printed polymers for prosthesis is enormous for governing the precise design of constructions that meet the requirements of personalized mechanical and aesthetic properties [61].
In the next section, we demonstrate the chemistry and properties of synthetic polymers for 3D printing tissue prostheses, presented in three groups: traditional polymers, silicone, and their blends. The polymers exploited in 3D techniques usually come in one of three forms: photocurable resins, thermoplastic filaments, and polymer powders.
3.2. Basic polymers
The final properties of prosthesis are determined not only by the material used, but also the type of 3D printing technique. To fabricate soft (elastomeric) materials exploiting 3D printing, the polymers can be utilized in one of three forms: photocurable resins, thermoplastic monofilaments, and polymer powders, usually consisting of photopolymers, thermoplastic urethanes or other thermoplastic elastomers, silicones [62].
Filaments are thermoplastic materials that are commercially available on the market in the form of spools, where the filament is wrapped in several layers. There are many filaments, characterized with their specific chemical–physical properties, such as mechanical resistance, elasticity, and deformability. Filaments are able to withstand extreme temperatures in the wide range: from subzero to high positive temperatures. The medical-grade filaments can be implemented in prosthetics and implanted in the human body. A wide variety of filament diameters ensures their compatibility with most extruders [53].
Resins for 3D printers found on the market are polymer materials in a liquid form, whose composition is very complex and can differ from manufacturer to manufacturer. This chemical variety results in different behaviors in terms of elasticity, resistance, transparency, and physical behaviors. The resins are typically cured during 3D printing by exposure to laser light (usually UV-vis light) or by using binders. In this scenario, the resins are commonly referred to as “ink”. The limited range of 3D printable inks that ensure the fabrication of prostheses with compatibility with biotissues and the required chemical and mechanical properties remains the most problematic [26].
There is a wide variety of plastic materials which are generally not available in filament form, for example, silicates or polystyrene, but can be manufactured in powder. A powder-based method is one of the most versatile, compared to other 3D printing methods for plastics. Since plastic does not require much energy to melt, the 3D printing technology for plastic powder does not need as much diversity as others [25].
In this section, the most common polymers capable of acting in one or more forms are discussed and represented in Table 2.
3.2.1. Acrylic polymers (resins)
Acrylic polymers have been successfully employed to correct facial defects, especially with slight movement of tissue during function [81]. They are mainly produced from vinyl monomers using various types of polymerization, such as free-radical, controlled radical, anionic, cationic, etc. The main advantage of acrylic resins is their availability, chemical and technological properties, sufficient biocompatibility, the possibility of implementing external and internal coloring. However, the rigidity of acrylic polymer limits their use in highly movable tissue resulting in localized discomfort and edge exposure. Acrylic polymers are extensively employed in 3D printing involving sintering (e.g., SLS) or photopolymerization (e.g., SLA, DLP) ( Figure 2) [82].
Poly(methyl methacrylate) (PMMA) is the most commonly used transparent polymer in 3D printing due to the ease of its processing, low cost, lightweight, stability in the oral environment, and aesthetic properties. PMMA is highly suitable for use as orbital prostheses, since it is in glassy state at physiological temperature (Tg ~105oC) and can act as a reinforcing material. However, PMMA has easily damaged surface and weak mechanical properties, which can be improved by using additives such as nanoparticles, for example, SiO2, Al2O3, TiO2 [83].
PMMA is typically obtained from methyl methacrylate monomer or oligomer by free radical or anionic polymerization, as well as photopolymerization. Significant number of PMMA prostheses were fabricated by molding of PMMA using computer-aided design and 3D mold prototyping. The limitations of this material include shrinkage of material and the absence of pores, especially if tissue repair is necessary. Fiaschi et al. [84] improved traditional nonporous PMMA by crosslinking with aqueous carboxymethyl cellulose resulting in hydrogel formation in 3D pre-printable mold acquired by virtual CAD model. Porous PMMA offered sufficient impact resistance and provided cell growth in prosthesis. Another major problem with PMMA are residues of toxic chemical, which may occur as a result of incomplete polymerization [85].
PMMA is available in filament form (melting point ~160oC), which is suitable for direct FDM printing with rapid PMMA processing, ensuring complex geometries and various porosities for medical implants using medical imaging data [86]. PMMA resin of medical grade was also 3D printed using a material jetting approach (Polyjet 3D printing) to directly print personalized ocular prosthetics, which were subsequently hand painted [87].
PMMA composites as a combination of two or more phases, have been investigated to improve the properties of the final material [88]. PMMA composites with bioactive glasses, silicates, and hydroxyapatite (HA) improve the mechanical properties [89] and impart to shape memory of PMMA and, in addition to its bioactivity [90]. For example, Hamizah et al. reported about PMMA composites with HA and glass–ceramic that showed improved bending strength and enhanced thermal properties in simulated body fluid [91]. Stansbury et al. [82] reported on a new generation of acrylic oligomers, introducing a block of other polymers, such as polyurethane, polyfluorocarbon, polysiloxane, etc., in polymer chain, which can eliminate the drawbacks of traditional acrylic copolymers and meet the requirements of a maxillofacial elastomer.
3.2.2. Polyurethane Elastomer (Thermoset)
Polyurethanes (PU) are elastic polymers with excellent flexibility, good edge strength, ability to external and internal coloration and fine cosmetic results. PU is synthesized in the course of reaction between isocyanates and polyols, changing the ratio of which enables fabrication of polymers with diverse physical and chemical properties ranging from plastic to fiber items [92]. For example, a soft skin-like polymers can be produced in the excess of polyols, such as aliphatic diols, polyesters, or hydroxyl-terminated polyethers. The long chain molecules form the soft segments responsible for elasticity, flexibility, softness, and resistance to hydrolytic degradation. Resistance to UV damage and hydrolysis can be enhanced by using aliphatic groups, while improved mechanical properties are achieved by the addition of aromatic groups. Hard polymer chain with isocyanate groups either di- or polyfunctional improves the life time of prosthesis. An important drawback is associated with the sensitivity of isocyanate chains to moisture. Curing PU in molds contaminated with water leads to bubble formation, causing defects and reducing the material quality. This requires thorough dehydration during processing, which makes procedure more complicated [93].
PUs are actively employed for prosthesis mold fabrication owing to possibility of crosslinking at 100 °C that significantly decreasing the cost of molds compared to higher-temperature crosslinking. Medical grade PUs are available in filament rolls (melting point~ 160oC) suitable for low-cost FDM technique, which enables the production of PU materials with better mechanical properties [94]. Prosthesis based on PUs can be obtained using SLS printing techniques, since PU materials have very unique and adaptable qualities: well-flowing powders, low melt viscosities, and little shrinkage during the hardening process. PU materials after printing possess many relevant properties, such as flexibility, durability, and is available as a medical grade polymer [63].
Numerous studies focus on the blending of PU with other polymers and ceramics. It can successfully tune and correct PU properties improving mechanical, electrical, thermal, and physical characteristics to create more prospective materials [95]. For example, biodegradable polymer poly(lactide) (PLA) can be blended with PU to deliver outstanding shape memory effect and viscosity enhancement defined their great potential in 3D printing technology [96] Of particular interest are also PU composites with poly(acrylonitrile-butadiene-styrene), poly(vinylidene fluoride), polytetrafluoroethylene, polyethylene terephthalate, etc.[97].
3.2.3. Polyesters
Polyesters refer to a group of thermoplastic polymers that contain ester or ether group in the main chain. They are synthesized by polycondensation accompanied by the release of side -product. The three most popular polyesters are polycaprolactone (PCL), polylactic acid (PLA) and polyether-ether-ketone (PEEK) [13]
Polycaprolactone
PCL is aliphatic semi-crystalline polymer with glass transition temperature of -600C. Hence, at physiological temperature, PCL is in elastomeric state demonstrating high toughness and superior mechanical properties (high strength, elasticity depending on its molecular weight) [98]. PCL is a highly biocompatible polyester with long degradation time (2-3 years) and high stability in vivo due to its hydrophobicity. Good mechanical properties with high flexibility and great elongation underlie the PCL involvement in craniofacial bone repair [42] The presence of five hydrophobic –CH2 moieties in its repeating units determines PCL slowest degradation rate among all the polyesters. PCL is synthesized by ring-opening polymerization of ɛ - caprolactone monomers in the presence of a catalyst such as stannous octanoate [99].
PCL attracts a lot of attention for utilization in 3D printing due to its low melting temperature ( ∼63 °C), which allows PCL to be implicated in the filament form in printing techniques such as FDM. SLS is another technique for PCL-based prosthesis fabrication using a laser beam sintering the PCL powder. Note that SLS is more accurate but more expensive than FDM [100].
Despite biocompatibility and easy processability, PCL hydrophobic features and low bioactivity limit its applications in the biomedical field. Composite of PCL with bioactive inorganic particles (e.g. tricalcium phosphate, hydroxyapatite) oxides, polymers provides a promising way to overcome these shortcomings and improve properties [101,102]. Chen et al. [103] reported that ring-opening copolymerization in the presence of Sn(Oct)2 as catalyst and octanol as initiator resulted in poly( L-lactide-co-caprolactone-co-acryloyl carbonate), exhibiting high rigidity after extrusion and cross-linking after UV irradiation. The combination of PCL with hydrogel can improve mechanical properties, as demonstrated by Stichler et al. [104] on blends of PVC with hyaluronic acid/poly(glycolic acid) hydrogel cured with UV light.
Polylactide
PLA (exists in three isomeric form D-, L- and DL) is one of the most extensively used thermoplastic polymer in human body-related applications. It is typically synthesized by polycondensation, and in some cases by ring-opening polymerization [105]. The latter results in lower molecular weight and more brittle PLA suitable for low-stress applications. PLA has relatively low melting temperature (~160°C) that enables printing at lower temperature compared to other thermoplastics (for example, ~250°C of ABS) with better surface details and sharper features. PLA is highly biocompatible and possesses tunable physicochemical properties. It can stay in contact with the skin for a long time without any negative effects. The decomposition products of PLA are also non-toxic. PLA is commonly presented in the form of a filament, which is the easiest material to FDM printing, where PLA demonstrates the excellent processability. The material easily adheres to a variety of surfaces and does not require to heat the build plate for the first few layers making it easy to use. PLA is a durable material that crystallizes quickly, as well as does not release smelly fumes during processing. PLA is easily colored and comes with diverse range of colors, which can have glossy, matte, and metallic finishes. The shrinkage of PLA is very low, in the order of 2–3% maximum, providing the ability to print very large objects, as they deform less [106].
However, PLA has low heat resistance, which limits exploitation at high temperature, since the rapid deformation observed, especially under stress. The low impact strength of PLA is due to the brittleness of the material, which tends to break rather than bend, and does not withstand impact. This makes PLA more suitable to aesthetic rather than mechanical purposes. It is necessary to take in account PLA permeability both for gases and for waters, which can pass through the material.
The material properties can be significantly changed by the fabrication of blends nanoparticles, polymers, ceramics, metals, pigments etc. [4,107,108] For example, 3D printing of PLA composite with such polymer as poly(L-lactide-co-trimethylene carbonate) led to materials with sufficiently high mechanical properties. This makes the choice of PLA blends virtually endless [109].
Polyether-ether-ketone
In the late 1990s, PEEK gained attention as important high strength polymer due to its exceptional mechanical, thermal, and chemical properties, as well as biological stability and biocompatibility. Among materials available for 3D printing, PEEK ranks highest in terms of its performance properties. PEEK (-C6H4-O-C6H4-O-C6H4-CO-)n is a semi-crystalline thermoplastic polymer that have found various biomedical applications, particularly in maxillofacial surgery [110].
PEEK offers remarkable mechanical properties, including high strength, stiffness, and toughness. Its mechanical characteristics (tensile strength up to 100 MPa, flexural modulus ~4100 MPa) are comparable to metals such aluminum and steel, making an attractive alternative for lightweight components requiring strength and rigidity. Additionally, PEEK has an impressive impact strength, which means the resistance to significant stress without breaking. Therefore, PEEK became a potential candidate as an alternative to metals capable of reinforcing materials. Low friction coefficient and high resistance to deformation define PEEK excellent resistance to wear and abrasion. Moreover, PEEK exhibits minimal creep under stress, providing dimensional stability in printed parts [110].
PEEK demonstrates remarkable resistance to a wide range of solvents, acids, and bases, allowing it to utilize in aggressive environment. It is also resistant to hydrolysis, even in hot water, which is important both in sterilization processes for medical and dental products and in extending the service life of components [111]. PEEK is resistant to gamma radiation, while only moderately resistant to UV radiation [112].
PEEK has a high glass transition temperature (Tg ~143 °C) and a melting temperature (Tm ~343 °C) along with low thermal expansion coefficient, which ensures dimensional stability under varying temperatures [113]. These thermal properties make PEEK a highly versatile material capable of meeting the stringent requirements of various industries that operate in extreme temperature conditions. However, these excellent thermal properties make 3D printing of PEEK extremely challenging since high extrusion temperatures are required to melt the material. PEEK 3D printing research was sparse till recently owing to the higher temperatures required for melting and the lack of suitable raw materials [114].
Despite all, PEEK found application in FDM and SLS 3D printing methods. Recent years have witnessed the significant efforts and optimization made on the 3D printing of PEEK [115]. For example, it turned out that the fracture mechanics in FDM can be controlled by raster angle with an appropriate setting [116]. Vaezi et al. [117], Yang et al. [118] studied the mechanical properties, thermal processing conditions, and tensile properties of the printed PEEK products, respectively.
The study of SLS showed that the morphology, structure, and granulometry of the PEEK powder are highly crucial parameters [119]. In addition, various process parameters, including laser beam, affect the mechanical properties, dimensional shrinkage, structural characteristics, surface roughness, and other material characteristics of SLS products [120,121].
PEEK is biologically inert, but often results in the improper fixation of implants at defect sites and their loosening [122]. Being chemically inert, PEEK can be adopted to performance standards by using physical methods, e.g. coating, reinforcement, plasma treatment, surface modifications, etc.[123]. 3D printing of composites with hydroxyapatite, chitosan, and other bioceramics can improve material properties, enabling better control on distribution of bioactive phase, such as hydroxyapatite (HA) within PEEK matrix. In [124], the composite materials created with SLS by using various combinations of PEEK and HA showed high level of interconnectivity between components. Graphene oxide can improve interfacial bonding between PEEK and HA by forming a conjugated structure with graphene oxide having strong π-π bonds [125].
3.2.4. Styrene-based polymers
The most popular styrene polymers include polystyrene (PS) and acrylonitrile-butadiene-styrene copolymer (ABS). These polymers belong to rigid materials that have found their applications in the prosthesis fabrication both for the mold production, which are then implied for flexible polymer casting, and for 3D printing of rigid supports for composite prostheses. The relatively short period of thermoplastics in 3D printing of prostheses means that almost all recent publications on 3D printed soft tissue prostheses have used some form of rigid polymer for the mold manufacture [126].
PS is thermoplastic and is predominantly obtained by free radical polymerization of styrene monomer. It is structurally non-crystalline amorphous transparent polymer (Tg ~100oC), exhibiting stiffness, brittleness with a tendency to stress cracking. PS shows valuable surface properties, high dimensional stability, good processing, low water uptake and shrinkage. On the other hand, it has a limited chemical resistance to organic substances [127]. The use of various additives can modify PS properties. High impact polystyrene (HIPS) is a very promising material, which has a higher impact resistance. HIPS is typically produced by adding about 5 to 10 percent of rubber copolymer or butadiene, which increases strength and durability, but reduces transparency. HIPS is referred as a material that is similar to ABS (see below), but it is stronger and more flexible than ABS [128]. Mechanical properties and ease of processing make HIPS a good candidate for a wide range of applications in prosthetics, especially for mold fabrication. Processing and, consequently, final material characteristics are controlled by the temperature dependent viscosity of the melt. Appropriated melting temperature (~210-230oC) and availability of HIPS filaments enable 3D printing by using FDM, provided improved properties of the resulting products. For example, Kaveh et al. reported [129] on calibration factors made it possible to increase accuracy of the dimension of parts, holes, and thicknesses.
Another rigid material actively used in 3D printing is ABS, a block copolymer of acrylonitrile, butadiene, and styrene, which was the first thermoplastic implicated in 3D printing as a filament. ABS inherits its heat tolerance, high impact strength, and rigidity from acrylonitrile, butadiene, and styrene, respectively [130]. ABS is typically synthesized by free radical polymerization. It is characterized by an easy post-processing, a suitable melting point (~220°C), but there is a deformation effect (upward curvature of first material layer). ABS has a higher impact strength, higher resistance to stress cracking compared to PS, and less brittleness than PLA. This copolymer offers an increased breaking strength, a high mechanical strength, great rigidity, hardness, scratch resistance, dimensional stability under heat, relatively low water absorption and chemical resistance [127]. However, ABS plastic has poor UV resistance, resulting in shape change and discoloration. It is commercially available in many colors and is fairly easy to print in FDM from filaments. ABS is suitable for a wide range of 3D printing techniques, as it is available in the form of powders (for SLS and binder jetting) and resins (for SLA and material jetting)[131,132] To increase the mechanical resistance characteristics, increased hardness and reduced shrinkage, the composite materials have been developed, which takes the name of ABS + [133].
3.2.5. Silicones
The silicones (polysiloxanes) are known from 1946, but for the manufacture of maxillofacial prostheses, they came only past decade [134]. Silicone is elastomeric material made of semi-inorganic polymers of general structure –[SiRR’–O–]n with various alkyl or aryl R and R’ groups with diverse crosslinking degree (Figure 3c). To date, silicone is the most widely used facial prosthetic material due to its skin-like flexibility, heat resistance, radically low viscosity-temperature coefficients, biocompatibility, and intrinsic transparency [135]. The most studied and produced silicone is poly(dimethyl siloxane) (PDMS) –[Si(CH3)2–O–]n, which relatively poor mechanical properties can be improved by crosslinking in the course of polycondensation, free radical polymerization, and addition polymerization. Crosslinking (vulcanization) also provides silicone resistant to ultraviolet (UV) light. Crosslinking can be further divided into room temperature (RTV) or high-temperature (HTV) vulcanizing, both of which exhibit advantages and disadvantages [136].
Room temperature vulcanizing (RTV) silicones
The advantage of RTV vulcanizing concerns the low curing temperature, allowing molds to be fabricated from low-cost plaster and gypsum for silicone casting and curing [137]. RTV silicones are of two types according to the type of reaction:
1. Crosslinking occurs by polycondensation reaction between reactive silanol groups of hydroxyl terminated polysiloxanes, crosslinking agent, e.g. tetraethyl silicate, and a catalyst, e.g. methyl triacetoxy silane. After mixing, the resulting product is still liquid and stored in sealed vessel. Upon opening and exposure to atmospheric moisture, the functional groups (such as alkyloxy and acetoxy groups) are hydrolyzed, resulting in silanol groups responsible for condensation. Two chains are linked, and the reaction proceeds from the remaining acetoxy groups. However, during this process, acetic acid is released as a by-product of the reaction [138].
One of the RTV limitations for prosthesis fabrication is the production of parts with thicker cross-sections since moisture cannot penetrate deep enough to polycondensation occurs. This process also characterized by long polymerization time and the release acetic acid, which is a skin irritant. However, these systems have found application as medical adhesives and external colorants for prostheses [139].
2. Crosslinking of polysiloxanes by addition reactions is based on the interaction of silyl hydride groups (-SiH) with vinyl groups (CH2==CH-), attached to the silicone, in the presence of platinum catalyst. These RTV systems can contain either one or two siloxanes and are cured at a higher temperature in order to reduce reaction time. This polymerization approach provides products with reduced shrinkage due to the lack of by-product in this reaction. The RTV drawbacks for prosthetics include selective adhesion, hydrophobicity, troubles with external staining, and impurities reducing curing efficiency (e.g., amines, sulfides, or other catalyst poisons). These RTV limitations do not diminish the high popularity of platinum-catalyzed silicones among the most commonly used material in maxillofacial prosthetics [140].
High temperature vulcanizing (HTV) silicones
HTV silicones can be prepared by addition or free radical polymerization, carried out at high temperature between 100 and 200 °C. HTV silicones after addition polymerization, similar to the RTV reaction, but at a higher temperature, are typically transparent, odorless, have relatively high tensile and tear strength, are easily removed from the mold, and do not require post-processing. They are available as one or two-component systems, where adjusting the amounts of each components changes the final silicone flexibility. An example of addition reaction product at a two-part crosslinking is liquid silicone rubbers, which can be fabricated from low molecular weight silicones and have various viscosity, from low to high. The curing rate is controlled by temperature, the increase of which accelerates the process [141].
Efficient free-radical cross-linking, which gives HTV, requires the presence of vinyl groups in the polymer chains and the radical generation, generally from organic peroxides at elevated temperature. The peroxide usually is added before processing (extrusion, injection molding, etc.) that can lead to the formation of peroxide volatile residues, as a probable cause of the void formation. This determines the need for post-curing to remove these volatiles. HTV are produced in the form of heat-resistant, high-consistency silicone rubbers with high tear resistance. They have highest tensile strength, high percent elongation, excellent thermal, color and chemical stability, making them more biologically inert. However, they appear yellowing after curing, have a strong odor both during and after production, and are sticky to the touch with high surface friction [141,142].
The properties of silicones can be significantly extended by creating blends and copolymer materials. Silicones can be reinforced with fillers, which contribute to the dissipation of energy during deformation of the material associated with easier slipping of the chains relative to each other. The most common silicone filler is silica with hydrophobic surface, capable of increasing strength, hydrophobicity, loss and storage modulus, and damping factor, but reducing elasticity [143]. Nanoparticles of titanium, zinc, and cerium oxides have also been implicated as fillers [144]. Silicone block copolymers are new materials synthesized to overcome some of disadvantages of silicone vulcanized elastomers, such as relatively, thin margin tear strength, low elasticity and hardness, bacterial film formation. For example, block copolymer, containing a PDMS block and a poly [2-(dimethylamino)ethyl methacrylate] block demonstrated more tear-resistant behavior than conventional cross – linked silicone polymers [55].
Current approaches to 3D printing of silicon can be broadly divided into indirect and direct. In indirect approaches, silicone is typically cured in rigid polymer molds made using low-cost 3D extrusion printers [145]. Direct approaches are based on the layer-by-layer extrusion, jetting, or polymerization of silicone. Despite the easy fabrication, direct 3D printing suffered from the visible layers from the progressive polymerization that did not meet aesthetics requirements [11]. Now, direct 3D printing approaches are actively developed for manufacture of silicon prosthesis with optimal characteristics. For 3D printing of silicone is typically employed SLA techniques (vat polymerization), material jetting, and material extrusion with crosslinking via addition polymerization or UV curing [54]. One approach utilizes scheme similar to FDM, but without heating of nozzle and print plate. Two-component RTV silicones extruded in the presence of platinum catalyst have demonstrated the hardness, tear, and tensile strength within acceptable ranges for utilization as facial prostheses [10]. Silicon 3D printing can also be performed by extruding moisture-cured silicone elastomer RTV instead of a two-component mixture[11] or by using photocurable silicone, which is then cross-linked using a UV lamp.[110] Vat photopolymerization is another approach to direct 3D printing of silicone using the DLP technique to selectively photocure each polymer layer [146].
4. Polymers in retention systems
The success of utilizing a maxillofacial prosthesis is principally determined by the retention system. A wide range of intervention types and the complexity of the process provide numerous information about retention systems for prostheses. Various methods can be used to retain maxillofacial polymer prostheses, basically including adhesives, anatomical undercuts, spectacles, magnets, or fixation implants [147]. After assessing the surrounding anatomical tissues, the method was chosen depending on the shape and size of the defect, systemic condition, remnants of hard and soft tissues in case of trauma or postoperative defect, and the age of the patient. Retention methods based on the adhesive and implant implication are the most widely used [148].
4.1. Adhesives
The type of adhesive to fix maxillofacial prosthesis should be chosen carefully, taking into account a possible undesirable effect on the physical and optical properties of polymer-based prostheses.[8] To ensure the required level adhesion of prosthesis to skin, the adhesive compositions should be easy to apply, being biocompatible, non-toxic, odorless, moisture-resistant, preferably with a porous structure to maintain the secretion drainage. The main functions of adhesives can be outlined as follows [68]:
- -
- hold the prosthesis in place for at least 12 h a day;
- -
- do not cause tissue irritation;
- -
- do not damage tissue when adhesive peels off the skin;
- -
- dry quickly after application
Adhesive in maxillofacial prostheses is easily accepted by patients due to its cost-effectiveness, non-invasiveness, and the absence of aggressive side effects. It is worth noting that it is advisable to remove the prosthesis once a day to clean the surrounding tissues and before resting in order to avoid the risk of disturbing contact with the skin and to allow the tissues to rest [149].
One of the usually exploited approach to prosthesis retention concerns the implementation of pressure-sensitive adhesives (PSAs), which are soft permanently tacky polymeric materials. They form strong adhesive bonds with substrates of various chemical nature at a short-term (1-5 s) low force (pressure up to 10 Pa) [150]. Such materials must have a certain set of physicochemical properties, in particular mobility and fluidity during bonding, in order to form a good adhesive contact in combination with high intermolecular cohesive strength and elasticity. This requirement is necessary to resist the separation stress. Thus, these adhesive materials are characterized by their adhesion (i.e., adhesion strength to a surface) and cohesion (i.e., resistance to shear and destruction of the adhesive layer along the adhesive material), namely PSAs should have cohesive strength that is much higher than its adhesion strength to the substrate. The balance of adhesion-cohesion is essential in the case of PSA contact with physiological sensitive tissues (skin) that have low surface energy. The popularity of PSAs is mainly related to the low weight compared to other joining techniques (often using metal parts), as well as their low cost and easy application [151].
The most commonly used adhesives include hydrophobic polymers such as polyalkyl acrylates and their copolymers, natural rubber, polyvinyl ethers, polyisoprene, polyisobutylene, polybutadiene, styrene-isoprene copolymers, styrene-butadiene copolymers, polychloroprene, etc. [151] Acrylic-based PSAs dominate the adhesive market every year more and more due to their characteristics, such as high tack and peel adhesion along with excellent cohesion, exhibiting a high resistance towards UV, heat and humidity. Their easy manufacturing according to the user demands, suitability in various applications and their competitive cost also gain their active market [152].
The medical use of hydrophobic polymers that are not able to absorb moisture is limited, since the tack decreases, when applied to a hydrated surface, which is the skin. In contrast, the hydrophilic polymers as an adhesive component exhibit "stickiness" to the skin due to water absorption. However, this leads to a significant swelling of the composition and, accordingly, a significant decrease in cohesion. To meet these conflicting properties, PSAs should contain hydrophobic and hydrophilic parts. An example of such a composition is a blend of polyacrylic acid with polyvinyl alcohol, to which polyethylene glycol, polypropylene glycol, and glycerin are added [68]. This approach gives rise to an increase of the composition hydrophilicity but reduces the adhesive properties and requires complex procedures for mixing components with low affinity for each other. In some cases PSAs can be presented in the form of weakly cross-linked copolymers with 70 - 90 wt.% soft monomers (their polymers possess low glass transition temperature, Tg ) and 10 - 30 wt.% of a harder monomer (their polymers possess high Tg) [152]. Figure 3a shows examples of the most popular polyacrylates used as PSA.
The most promising material for creating adhesives are silicone compositions. They provided a prosthesis position on the skin, kept in place during the entire treatment period and then removed without leaving residue or damaging the skin. Silicone adhesives have the surface tension lower than that of the skin, which determines the rapid and intensive surface wetting. Besides, silicone rapidly spreads under low deformation rate, enhanced by light pressure and moderate heat. In addition, the main feature of silicone is the tunable viscoelastic properties with adjustable rheological parameters to ensure the required adhesion level [153].
Medical grade silicone PSAs are viscoelastic compounds, representing the resin-in-polymer concept, typically fabricated by using condensation reaction of hydroxyl terminated polydimethylsiloxanes (PDMS) (Figure 3b) from medium to low viscosity into MQ resin in the presence of ammonia. The MQ resin is obtained as a soluble three-dimensional network consisting of SiO4/2 (Q) units and R1R2R3SiO1/2 (M) units, where R1, R2 and R3 are mainly methyl or hydroxyl groups (Figure 3c).
Unlike organic adhesives, they do not require additives such as antioxidants, stabilizers, or other potentially extractable ingredients. Hydroxyl terminated PDMS as a liquid affects the viscoelastic properties, wetting and spreading of the adhesive. The MQ resin acts as a reinforcing agent, imparting tackiness, and elasticity. Resin content is the main factor that increases cohesion to a level, afforded the optimal balance of tack, adhesion, and peel. A blend of PDMS and MQ resin can provide the initial connection, but in the absence of covalent bonds between the components, low cohesive properties are revealed, which can be improved by reducing the concentration of hydroxyl groups.
To increase a cohesion, the PSA silicone network can be further cross-linked using two cure routes: peroxide-initiated free-radical curing and platinum-catalyzed curing. Since the peroxide cure route involves working with volatile solvents, peroxide by-products and high curing temperature, the platinum-catalyzed route appears to be more perspective for medical purpose. Platinum-catalyzed hydrosilylation reaction is carried out via addition polycondensation of vinyl-functionalized silicone and hydrogen (SiH)-functionalized silicone. The curing can be accomplished in a single zone at a relatively lower temperature without the formation of by-products (Figure 3) [153].
Despite widely spread adhesive retention system, there are some disadvantages, such as possible damage both prosthesis surface and the skin in the course of insertion and removal, as well as can cause dermatitis after prolonged contact. Retention problems can be associated with the insufficient strength against gravity and sweating, as well as limited tissue. Adhesives can lead to discoloration of the prosthesis, disruption of its structure and abrasion of the edges. All adhesive systems are insufficient to ensure the rigid fixation of facial prostheses movement. One way to partially improve retention properties of adhesives is to combine adhesives [149,154].
4.2. Implants
Osseointegrated implants can be utilized to improve the hold and retention of prostheses in the external craniofacial regions. They can offer excellent treatment option in prosthetic rehabilitation and can also eliminate or diminish the adhesive application. Implant-retained prostheses are comfortable to wear, easier to put in place with appropriate orientation, and convenient for patient to maintain hygiene. However, a satisfactory result can only be achieved with careful consideration of the number, position, and orientation of the implants, as well as with correct attachment system between the prosthesis and the implant retention structure. The surgical treatment for osseointegrated implants is rather simple and associated with a low level of perioperative and long-term complications [149]. The retention systems in the form of bar-clip retention, ball attachment, magnetic retention, locator abutment attachment and tilt lock system provide the prosthesis fixation on the implants [68,155].
In maxillofacial implantology, osseointegration, referring to a stable fixation by direct implant-to-bonе contact, is the only one that has demonstrated high success rates [156]. In 1979, the first implants were implemented to retain an auricular prosthesis [157], paving the way to international osseointegration utilization in facial reconstruction with facial prostheses. To date, osseointegrated implants were designed to anchor prostheses for the nose, ear, orbit, and midface in the reconstruction of maxillofacial defects [158]. The numerous conditions determine the integrity of the bone-implant interface during osseointegration, predominantly related to the bone ability to remodel. The most significant problem in the placement of facial implant setting concerns an insufficient bone volume. For example, suitable places for implant fixation are the temporal and supraorbital regions, where the bone thickness is in the range of 2.5 to 6 mm, so the external implants should be 3–4 mm long and 5 mm thick [68].
Recent advances in CAD have offered innovative options for fabricating osseointegrated implants with high precision, better adaptation for contour remodeling. Using CT and MRI scan, the CAD software make it possible to design a 3D implant model that precisely fits the defect. 3D implant objects are then produced using 3D printing techniques, such as SLS, FDM, SLA [159].
The preferable implant material for prosthesis retention is inexpensive, durable, radiolucent, lightweight, and biocompatible. Maxillofacial implants are usually made from metals and polymers. Titanium was the first material chosen for implants due to its high tensile strength, light weight and osseointegration property. Moreover, protective oxide layer is formed on titanium implants, which endows them corrosion resistance. Implants can be fabricated from pure titanium or an alloy. Their significant disadvantage is the high cost, which is unbearable for surgical practice[159].
Polymers commonly used for maxillofacial prosthesis include silicone, polycaprolactone, polylactide, PMMA, PEEK, etc. Silicone is one of the first polymer employed as an implant material. Silicone can be in a solid, liquid or gel state depending on the type of polymerization (see Section 3.2), among which solid silicone used as an osseointegrated implant. Silicone implants can be precisely produced by casting into 3D printed molds and easily modified intraoperatively [160]. PEEK is highly strength polymer, initially actively exploited for manufacturing orthopedic implants, and now is successfully adopted for 3D printing of both molds for implants and maxillofacial implants [161,162]. PMMA, also well established in the production of orthopedic implants, appeared to be important in the reconstruction of maxillofacial defects, especially for 3D printed ocular prostheses [163].
In summary, the main tendency of practitioner preferences can be estimated from the literature. Implants are the first choice for fixation of extraoral maxillofacial prostheses with predominantly bar-clip system for an auricular prosthesis, as well as either a bar-clip or magnets for the oculopalpebral and nasal regions. Adhesive-based prostheses are difficult to fit properly, and they can shift or dislocate during daily activities. Although in some cases, the mechanical and adhesive retention techniques are preferable, since they are the least expensive and have no side effects [164]. Future work on the maxillofacial prosthesis fixation should look for a standard design with common variables using the results reported by patients [149].
5. Special features of polymers
Chemical and mechanical changes in materials affect the shelf life of prosthesis, which are often exposed to mechanical tensions, ultraviolet radiation, , acidic or alkaline excretion, sebum, biological contamination, disinfectants and soaps, water, dust, extreme temperatures, adhesives, chemical interactions, fractures, etc. [165]. These factors of deterioration of aesthetic properties, perception and functionality of prostheses must be taken into account when developing new polymers and polymer composites for prosthetics.
Chemical degradation is one of the intrinsic processes of polymers, since they can degrade over time via chain bond cleavage which promotes polymer softening. For example, acrylic resin-based prosthesis can undesirably change color, deform or even crack over time [166]. This is aggravated by mechanical stress during normal use, when material fatigue begins and cracks spread. Internal and surface stresses in acrylic materials can also result from different thermal expansion between the resin and other attached materials [167]. Moreover, the reactions can continue within polymers long after the end of 3D printing delivering negative impacts on their mechanical properties. This scenario is observed in silicone curing due to continued crosslinking accompanied by an increases in elastic modulus, glass transition temperature, and viscoelasticity [168]. Also, the maximum stress and strain are reduced, as well as the tensile strength decreases [56,165].
Exposure to UV radiation and weather with effects of sunlight, rain, wind, and aerosol pollutants, etc. lead to the degradation of polymers over time, especially of skin-like components [169]. UV-radiation usually induces photooxidation, involving free radical formation, followed by chain crosslinking. As a result, an increase in maximum stress and deformation were observed, as well as a reduction in yield and strain strength, compression and tensile elastic modulus, and hardness. Additionally, weather factor can cause hydrolytic degradation, mechanical damages with opening of the weaker internal layers of prosthesis [170]. The problem of described types of degradation can be solved by development of composite and copolymer materials based on the aforementioned widely used polymers.
Skin secretions, including sweat and sebum, also have effect on polymer properties. For example, studies of different commercial silicones immersed in simulated skin secretions in the form of an aqueous salt solution and sebum in the form of an oil solution for 6 months showed their hardness and elasticity increase probably owing to the propagation of cross-linking reaction during aging. However, in a solution mimicking sebum, several silicon samples became softer and more plastic likely because of some compound extraction [171].
Prosthesis contact with skin can lead to microbial growth, capable of impairing both mechanical and aesthetic properties, which can cause skin irritation and infection. Silicone materials do not promote the growth of microorganisms, although surface irregularity and porosity can drive the colonization of commensal microorganisms with biofilm formation [172]. Sanitary procedures can prolong the lifetime of a prothesis, but various disinfection methods, e.g. UV radiation, microwaves, etc. and reagents, e.g. sodium hypochlorite solution, commercial disinfectants, chlorhexidine gluconate, soaps are capable to cause silicone degradation [173]. For example, neutral soap and disinfectants increase silicone hardness and elastic modulus in silicone, especially of surface layer. The microwave exposure also makes the silicon material harder, exhibiting greater changes at the small depth [174]. Acrylic materials can also change under cleaning, since they have the ability to absorb water. These responses of polymer materials on sanitary procedure stimulate the development of materials with biocidal properties, e.g. by including bactericidal reagents, such as poly(diallyldimethylammonium chloride) into silicone, recovering surface roughness of acrylic prostheses using photopolymerized glaze [175].
One of the visible deteriorating property of prostheses is discoloration. Many factors, including the pigment type and its affinity to polymer, manufacturer, original color, skin secretions, environment, etc. affect the rate of color change. For example, organic pigments in silicone appeared to be more prone to color change than inorganic pigments [166]. Discoloration is process, specific for each person, and may occur at different rates for the identical prostheses [170]. In silicones, color stability can be achieved using additives, such as barium sulfate [176], titanium dioxide nanoparticles [177], and commonly used opacifiers, which, however, make worse the mechanical properties [178].
6. Application of 3D-printed prostheses
The implication of maxillofacial prostheses aimed at reconstruction of acquired or congenitally missing facial structures, such as ears, eyes, the nose, etc., is a challenging task for the social reintegration of patients. One of the main causes of maxillofacial deformities are tumors, which are basically revealed at an advanced stage of the illness, when treatment is associated with mutilation. The loss or disfigurement of tissues have negative effects on the body image, which leads to psychological, social, and financial problems. The method of reconstruction is guided by many factors, primarily the lesion location, its size, etiology, severity along with the patient age and social factors [179]. Although the conventional reconstructive surgery can achieve excellent results for many cases, the relatively high costs and frequently negative patient experience give rise to the fact that non-permanent prostheses are preferred for many people. Moreover, the complex anatomy of structures, such as the ear and nose, tends to be difficult to reconstruct and almost impossible to reproduce using reconstructive surgery. It is worth noting that surgical intervention is highly invasive with potential complications and possible irreversible changes in the face after implementation. On the contrary, prosthesis application is typically minimally invasive, provides an immediate aesthetic amendment, enables multiple design options without impact on the patient [180].
3D printing has a great potential for reproducing tissues and anatomical elements for maxillofacial abnormalities. There are reports in the literature on the exploitation of modern CAD and 3D printing technologies in a number of patient-specific medical applications, from design [181] to facial prosthesis [182,183] However, unlike intraoral rehabilitation, there is still no simple software solution with digital retention elements for maxillofacial prosthesis, such as DentalCAD (Exocad GmbH) [184]. Although, numerous tissue prostheses are still fabricated using traditional handcrafting processes and 3D printing is still in its early development stage, the reports on 3D printing approaches to practical application are on the rise [185]. 3D technologies are implemented as adjuncts, and in some cases as a complete replacement for traditional manufacturing of facial prostheses in order to improve the existing methods. Herein, we briefly demonstrate the key details of recent reports on 3D printing of maxillofacial prostheses for ear, nose, eye and adjacent facial tissue.
6.1. Nasal prostheses
Nasal prostheses offer great benefit for the patient recovering from trauma, with congenital malformations or cancer-caused defects of the nose. Historically, such prostheses have been fixed largely by non-permanent methods, including spectacles and adhesive products. Nasal prostheses may also have a functional purpose, especially in the case of damage to the maxilla or palate. 3D printing has great potential for prosthetics of the nose and adjacent anatomical regions. Numerous researchers around the world are developing approaches to implement rapid prototyping in all its forms, as a support for rhinoplasty or for nose and facial reconstructions [53].
One of 3D printing approaches concerns the design of a support for their everyday surgery, using 3D photographs of patients to consider the possible surgical outcomes. The printed models provide visual and tactile support during surgical intervention to achieve the results agreed with patients. For example, Anton de Vez et al. [186] have fabricated the customized guides to assist in the reduction of the cartilage hump. The design of these small tools is simple and easy to implement using conventional 3D modeling programs. Choi et al. [187] reported on the specific guides or templates created by computer simulation that can govern the accuracy and precision during the planning of the nose formation, modeled in 3D modeled computer simulation.
3D creating and printing supports can be implied as a guide not only for surgical planning but also during rhinoplasty. This approach minimizes errors by evaluating the changes step by step and avoids using memory to obtain the results. Guevara et al. [66] used the common software for dental implant stent fabrication in order to select precise landmarks, such as the superior brow, the upper lip, or dental incisor edges, on which to build 3D model of the patient nose. Before the surgery operation, this model was printed in the liquid photopolymer using SLA, then sterilized and placed on the patient nose to assess and correct changes during surgery.
The creation of customized prostheses using 3D printing in molds is relatively simple and straightforward procedure. Molds give advantages to 3D printing of silicone[188], the most suitable material for facial prosthesis, since printable silicone materials are not available and direct-printable silicones have only recently been reported [189]. Denour et al. [80] demonstrated the prosthesis fabrication utilizing the models and molds made using conventional 3D printers. The patient refused surgical reconstruction after massive removal of the cartilage structures associated with nasal cancer and opted for a silicone prosthesis similar to the original nose. 3D surface imaging using the VECTRA-M5 360 Head System (Canfield Scientific Inc., Fairfield, NJ) was taken to create a digital model of the patient face instead of data from CT or MRI scans. Photocurable resin molds were prototyped by SLA according to this model, and prosthesis was fabricated in the conventional way by placing Silastic Medical Adhesive Silicone and RTV silicone (Dow Corning Corp, Midland, MI), fiber for reinforcement, specific dyes to achieve the skin tones in the mold. Silicone Adhesive (Factor II Inc) was used for retention. The 3D printed nasal mold makes the prosthesis creation easier, reduces production time and efficiency, and also provides a comprehensive analysis of external soft tissue.
There are numerous research reports on the best polymer in this area, such as silicone, using customized techniques, which allow the reduction of production time. For example, Choi et al. [76] showed a system with appropriate software called “3D carving system” for the preparation of implant models based on patient landmarks, namely a specific patient model of implant for the back of the nose. Negative molds obtained from ABS filaments using FDM were filled with medical-grade silicon (NuSil MED4-4420). After curing, the final implant was introduced through a skin incision under local anesthesia, placing the prosthesis on a subperiosteal plane. The custom model practically replicated the CT scan models, exhibiting correct placement due to the precise modeling of the ventral surface, which exactly conformed with the shape of the nasal bone. Note that a specific implant design took only 8.5 min on average, and final product was ready for implantation in 2.4 days.
The direct 3D printing of nasal prostheses is challenging, but their application is still insignificant. Nuseir et al. [67] reported on prosthesis for patient who lost the nasal pyramid after a facial injury and refused any reconstructive surgery. The nose was digitally designed using modeling software such as ZBrush software (ZBrush Software; Pixologic Inc., Los Angeles, CA) for 3D reconstruction of a facial defect recorded by CT. The final 3D model restored nose and facial aesthetics, anatomy, shape, and skin color, and was printed using a flexible color photocurable acrylate resins (TangoPlus, Stratasys Ltd) on a PolyJet system (J750; Stratasys Ltd., Eden Prairie, MN). The prosthesis exhibited an excellent aesthetic result and good patient tolerance, as well as a workflow provided enhanced prosthesis reproducibility and acceptability.
Direct silicone printing has a great potential for the fabrication of maxillofacial prostheses, although its clinical feasibility is at an early stage. Unkovskiy et al. [78] developed new technology for the rehabilitation of a nasal defect using a directly printed silicone nasal prosthesis. Prosthesis was designed for the patient with defect associated with the absence of the entire nasal pyramid due to extensive squamous cell carcinoma, and complete reconstructive surgery was impossible. Software reconstruction for the face and defect was based both on two extraoral scanning systems resulting in a 3D image of the entire face, including a highly detailed defect anatomy, and on photographs provided by the patient. The 3D image gave the necessary volumes and proportions to start the reconstruction, while the photos of the patient helped to recreate the external anatomy of the nose implicating modeling software used by industrial designers (ZBrush Software; Pixologic Inc). Assistance from CT imaging of bones or soft tissues was not required. Direct printing proceeded according to the digital model on 3D printer ((Drop-on-Demand ACEO; Wacker Chemie AG) using platinum-catalyzed addition polymerization of free-solvent silicone (ACEO Silicone General Purpose; Wacker Chemie AG). After exiting the printer nozzles, each silicone layer on the substrate is polymerized under the action of UV irradiation. The polished and painted prosthesis, fixed with skin adhesive, passively set into place and adhered well to the patient defect. This approach can be considered as a valid nasal defect rehabilitation with an aesthetic and functional result, appreciated by the patient.
6.2. Auricular prostheses
The ear cartilage architecture, differed by their complexity and uniqueness for each patient, has always been a challenge for reconstructive surgery. The search for the best technique capable of reconstructing the tissue shape, restoring the lost structure as a result of trauma or tumor treatment is crucial for both plastic surgery, and cosmetic surgery, which require improving the final results in terms of shape, size, and position of the pinna and ear lobe. The 3D printing technology seems to be very promising for auricular reconstruction that mimic the native ear. Traditional methods to restore auricular defects are based on a surgical intervention using autologous donor cartilage as a support for soft tissues. These techniques are difficult due to the complex 3D geometry of the auricular cartilage, which is limited in availability at the donor site and differs from the native cartilage in terms of biophysical properties. In addition, the presence of two surgical sites, the donor and graft recipient ones, is associated with significant morbidity [190]. These shortcomings can be solved after implementation of 3D printing approaches.
In particular, studies are focused on serious malformed pathological conditions such as, for example, microtia, which is congenital nature and characterized by incomplete development and even total absence of the ear auricle [71], predominantly unilateral. This disease is associated with hearing problems, and can also have a significant impact on social, psychological life, violating self-esteem, mental well-being, and quality of life in general. To create an ear prosthesis, two fundamental positions should be considered: i) the source of costal cartilage replicas (autological or synthetic) and formation of the ear framework; ii) the reference ear as a copy pattern. 3D printing enables the treatment of the microtia using ear prostheses, prepared in molds, and fixed through osseointegrated implants or adhesive.
The mold-tailored prostheses were presented by Berens et al. [72], who fabricated a 3D-printed ear model and used it as a reference tool to simplify microtia reconstruction. CAD and 3D printing made it possible to create the pediatric costal cartilage model for reconstruction, from which the negative model was constructed and 3D-printed with polylactic acid. This model acted as a mold for prosthesis fabrication by filling with blend of RTV silicone (GE Silicone II) with starch, capable of simulating skin characteristics such as pigmentation, hardness, and tensile strength. Complex models, also used in reconstruction, provide the recreation of the ear skin using various materials. For example, mold with costal cartilage can be 3D printed by Thermojet wax machine with gypsun, harden and applied to the impression with high consistency polyvinyl siloxane (Extrude Extra; Kerr Corp) and stabilized with light-activated polyurethane gel. The object was then duplicated in wax and converted into silicon elastomer [191].
Reconstruction of only external ear shape can be proceeded using 3D surface scanning or photogrammetry techniques, which are cheaper, than medical imaging and mainly radiation-free, in order to prepare a mirror-transformed cast of their normal ear [192]. Jeon et al. [193] prepared 3D template by scanning the normal ear cast, making a mirror image of the cast using CAD and printing a 3D ear model for reconstruction. This technique was applied for young patient, who could not sit still during the scanning process. The authors fixed an acrylic box on the little patient ear to introduce alginate impression material after protected the ear canal with a cotton swab. The mold was pushed inward, and a dental stone material (Neo plum stone, Mutsumi, Japan) was placed inside to obtain 3D scan of the ear model. Then a mirror model of ear was designed with the modeling software (MeshLab) for printing in the FDM 3D printer (Edison, Rokit, Korea) at a resolution of 0.05 mm. Microtia reconstruction was performed according to the Nagata technique [194], based on gathering the ear individual counterparts from the rib cartilage, and a 3D-printed ear model was implicated as a reference for the fabrication of framework. The details of the 3D-printed ear shape models were consistently and accurately collected and helped surgeons assemble the cartilage elements, while reducing surgery time and efforts.
Direct 3D printing was utilized by Nishimoto et al. [77] to produce 3D mock-up model for a chondral framework, implied the famous Nagata method [77] published in 1993. The authors created the groups of models, containing three basal parts and three upper parts, which were then printed using FDM (MakerBot Replicator 2X; Makerbot Industries,) in ABS plastics. These parts can be modified in shape and size and used as a reference in the operating room. Witek et al. [71] focused on separation of the model into its components, including helix, antihelical fold, superior and inferior crus and lobule, to have the entire model in the operating room. The authors showed that 3D model created with open-source software such as Blender (The Blender Foundation, The Netherlands) contains more anatomical details making their work easier and more accurate than a conventional 2D model. The completed auricular prosthesis was individually 3D printed on FDM printer (Builder Premium 3D Printer, The Netherlands) using polylactic acid filament.
The developed approaches provide a concrete assistance even in the daily practice of any plastic and reconstructive surgeon. Basic knowledge of modeling software (e.g. Rhino Version 7.0, Robert McNeel & Associates Seattle, WA) is enough to profile ear structures, separating their main components and creating ear model followed by 3D printing with light-curing resins. The acquired model can be used for various purposes both during planning and during surgery. In addition, the model components can be printed separately to facilitate the reconstruction of each individual fragment, for example, for carving cartilage [53].
The aesthetic appearance of auricular prosthesis, on which silicone spectacularly fits, can improve the patient perception of the entire outcome of rehabilitation. Unkovskiy et al. [79] demonstrated the direct multimaterial 3D printing of implant-supported auricular prosthesis utilizing a silicone of various grades of flexibility and hardness. The anatomy and position of the intact ear were acquired with 3D photogrammetry and intraoral scanner, followed by transfer all scans to CAD software programs (DentalCAD; Exocad GmbH; ZBrush; Pixologic Inc) for the virtual design mirrored ear model. The prosthesis was printed (Drop-on-Demand ACEO; Wacker Chemie AG) as 3 part-construction with a skin-like color silicone in various Shore hardness: prosthesis bulk (60A), concha (40 A), and lobula (20 A). After post-processing and coloring, the prosthesis was fixed using retention system with magnets. The final prosthesis matched the patient facial anatomy well and was satisfactory in terms of overall aesthetics, comfort and replication of the intact ear. Compared to the conventional workflow, the direct 3D silicone printing requires less production time. However, 3D approach needs technical development to enable high-resolution multicolor printing with minimal analog steps.
6.3. Ocular prostheses
Eye loss is commonly caused by trauma, glaucoma, or cancer and has more psychological implications than the actual lack of function. Indicated surgical enucleation results in the elimination of the entire globe of the eye, portion of the optic nerve, usually accompanied with orbital wall fractures, removal of bone supports in dependence with the degree of malignancy or injury [195]. This leads to the decrease in aesthetics and volume, which requires not only an eyeball prosthesis, but a reconstruction to restore surrounding tissues. The great difference between the eye and adjacent tissue in terms of visual and mechanical properties guides the implication of multiple materials, including polyurethanes , silicone, and rigid materials, such as acrylic resin [64]. Prosthesis retention is dependent on patient conditions, and can involve the eye socket, the spectacles, adhesives, or implants. The literature survey makes it possible to conclude that 3D printing for orbital and ocular prosthetics is in its infancy due to the small number of samples in each study, typically presented by only one prosthesis or specific case that is difficult to verify. In addition, the broad range of design methods, 3D printers and materials also suggests that this field is at an early stage of research [196].
Only eyeball replacement can be treated with the standard prostheses, the variations in colors and sizes of which, however, are limited [197]. An imperfect fit can cause irritation, which can potentially trigger an infection. Creating a well-fitting personalized prosthesis reduces this risk. The main materials for creation of eye globe prosthesis remain the acrylic polymers due to its lightweight, strength, versatility and transparency, as well as the possibility of coloring [16]. 3D printing determines the new level in development of eyeball prosthesis. Kim et al. [65] showed that the scleral prosthesis can be fabricated after acquiring 3D model with CAD and printing on DLP system (DS131, Carima, Seoul, Korea) using biocompatible photopolymer resin (FotoTec DLP.A; Dreve, Unna, Germany). It is worth noting that 3D printing technology was limited to printing only the scleral form, while the iris and vessels were painted manually. In this study, the authors first described a new approach. The iris and blood vessels were presented as a digital image of the patient other eye, generated using a color diagnostic tool and transferred by a sublimation transcription technique onto the scleral surface, followed by coating with transparent PMMA. This approach, being less time and labor consuming, imparts the objectivity and consistency to the personalized production of ocular prostheses.
Reconstruction of the orbital wall structures and surrounding tissue involves similar processes as with facial prostheses, emphasizing that orbital implants are essential for this process, although their correct placement is challenging. Implants help to fix prosthesis perfectly, focusing on the natural eye position, lid contour, and aesthetic details that mimic the contralateral eye [22]. Unfortunately, orbital implants often have a worse prognosis in comparison with implants for auricular and nasal prostheses. This may be attributed to the thin periosteum complicating the implantation, and problems in maintaining healthy soft tissues surrounding the implant. Another limitation for the current use of ocular prosthesis is the cost of implant preparation, for example a custom made titanium implant is still very expensive [53]. 3D printing has a great potential for this specific surgery.
CAD-designed implant model is typically obtained using the MRI and computed tomography [198], although a 3D facial scanner combined with an intraoral scanner also finds application [199]. For example, Callahan et al.[73] reported on orbital reconstructions with 4 samples of molded implants of high-density polyethylene sheet reinforced with titanium mesh (Medpor Titan mesh, Stryker, Kalamazoo, MI) and 1 sample of titanium mesh. After acquiring digital model of site using CT scans, the mock implants were printed on conventional FDM 3D printers with the two actively used filaments: polylactic acid filament (printer Makerbot Industries, Brooklyn, NY) and ABSplus (printer Stratasys, Edenprairie, MN). After printing and sterilization, the mock implant was then utilized intraoperatively as a stencil to model and cut the implants. The implant material was chosen in accordance with the specific requirements of the reconstruction. This 3D printing technique demonstrates the feasibility of utilizing a low-cost routine material, including Medpor Titan, for implants in orbital reconstructions extending to complex secondary reconstructions.
In [69], author demonstrated that 3D printed mesh implants can be fabricated using custom multi-head deposition printer from hydrophobic biodegradable polycaprolactone (PCL) to repair orbital fractures. Digital model based on CT scans enabled 3D printing of PCL mesh implants with optimal porosity, which can provide the additional benefit from biocompatibility associated with the cell ingrowth and even regeneration of the surrounding tissue. This effect was confirmed on 22 patients suffering from various orbital trauma, exhibiting satisfactory result in 95.4% of cases without implant infection, inflammation, implant migration, or bleeding. In orbital reconstruction, the PCL mesh maintains the functional ocular motility and demonstrates the absence of enophthalmos during the entire period of study. Han et al. [70] also restored the periorbital region and maxilla with PCL. Although, the PLC degradation period is believed to be about 2–3 years, good tissue regeneration can be induced despite a limited stimulation activity in relation to bone regrowth. Authors demonstrated a satisfactory increase in tissue density according to CT scans during the implant utilization. These results offer hope that biocompatible polymers can promote true bone regeneration.
7. Conclusions and Future Outlook
In this review, we demonstrate 3D printing techniques as a vital tool to assist maxillofacial prosthetics, which positively impacts in emotional, psychosocial, and functional well-being. Facial deformities are difficult to treat due to their complexity including anatomical structures, multiplicity of tissue types, deficit of bone and soft tissues, etc. Recent advances in 3D printing techniques and new approaches to the implication of the polymer materials both traditional and new, as well as their blends, govern the enormous promise in the treatment options available to patients. 3D printing technologies can offer the development of individual treatment plans and rational design, leading to higher aesthetic and functional outcomes in patient with maxillofacial defects.
The most commonly used materials for fabrication prostheses are polymers, which have almost all desirable physical, chemical, biological properties. The important requirements relate to aesthetic features, since prostheses must be invisible in public, reproduce in detail the lost tissues and adjacent skin, mimicking their color, texture, form. A review of the latest data shows that the currently available materials still do not fully meet all the requirements for an ideal material.
The main tasks of future research can be represented as follows: i) improvement of the physical and mechanical properties of existing materials or the development of new materials in order to achieve behavior closer to human tissue and increase the prosthesis life time; ii) the design of color-resistant dyes compatible with various polymers and scientifically selected to match the human skin and skin tones; iii) the creation of an adhesive composition for prosthesis retention without loss of adhesive strength; iv) the development of the prosthesis retention system based on the biodegradable osseointegrated implants providing the regeneration of bone to which they are attached; v) the improvement of direct 3D printing of prostheses with silicon as the most promising material for maxillofacial prosthetics.
Although 3D printing has numerous advantages, some vital components of the technology require significant refinement. This concerns 3D scanning and computer modeling, which determine the prosthesis characteristics necessary for processing and expression in the final product. For example, high-resolution scanners remain expensive and are designed for highly skilled personnel. Other shortcomings relate to the scanning time, up to several minutes, leading to errors due to the patient movement. The multicamera photogrammetry lacks these disadvantages, but often it is very expensive. In addition, the computer software currently available is not specifically designed for prosthetics and, being very complex and intended only for specialists, is limited for design purposes. Besides, some types of modern 3D printers are very expensive, and often researches are forced to customized simple 3D printers for their purposes.
In summary, future progress in 3D printing of polymer prosthesis and their retention system, associated with affordable and simple new materials, design and manufacturing capabilities will enable improving the life quality of people suffering from malformation or tissue loss.
Author Contributions
Conceptualization, A.N.G., A.G.S..; methodology, A.N.G., A.I.P.; writing—original draft preparation, A.I.P., A.A.V., M.S.M.; writing—review and editing, A.N.G.; visualization, A.N.G.; supervision, A.N.G., S.V.A.; funding acquisition, S.V.A., A.G.S All authors have read and agreed to the published version of the manuscript.
Funding
This publication has been supported by the RUDN University Scientific Projects Grant System projects №036500-2-000, №036501-2-000.
Informed Consent Statement
Not applicable.
Data Availability Statement
Available upon request.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the conceptualization; the collection, analyses, or interpretation of literature data; the writing of the manuscript; or the decision to publish the review.
References
- Dewan:, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.-C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the global incidence of traumatic brain injury. Journal of Neurosurgery 2019, 130, 1080–1097. [Google Scholar] [CrossRef]
- Maas, A.I.R.; Menon, D.K.; Adelson, P.D.; Andelic, N.; Bell, M.J.; Belli, A.; Bragge, P.; Brazinova, A.; Büki, A.; Chesnut, R.M.; et al. Traumatic brain injury: integrated approaches to improve prevention, clinical care, and research. The Lancet Neurology 2017, 16, 987–1048. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, E.L.; Farris, A.L.; Hung, B.P.; Dias, M.; Garcia, J.R.; Dorafshar, A.H.; Grayson, W.L. 3D-Printing Technologies for Craniofacial Rehabilitation, Reconstruction, and Regeneration. Annals of Biomedical Engineering 2017, 45, 45–57. [Google Scholar] [CrossRef]
- Bhaskar, B.; Owen, R.; Bahmaee, H.; Wally, Z.; Sreenivasa Rao, P.; Reilly, G.C. Composite porous scaffold of PEG/PLA support improved bone matrix deposition in vitro compared to PLA-only scaffolds. Journal of Biomedical Materials Research Part A 2018, 106, 1334–1340. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, K. Poly(trimethylene carbonate)-based polymers engineered for biodegradable functional biomaterials. Biomaterials Science 2016, 4, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Finch, J. The ancient origins of prosthetic medicine. The Lancet 2011, 377, 548–549. [Google Scholar] [CrossRef]
- Lai, J.H.; Hodges, J.S. Effects of processing parameters on physical properties of the silicone maxillofacial prosthetic materials. Dental Materials 1999, 15, 450–455. [Google Scholar] [CrossRef]
- Sawyer-Glover, A.M.; Shellock, F.G. Pre-MRI Procedure Screening: Recommendations and Safety Considerations for Biomedical Implants and Devices. Journal of Magnetic Resonance Imaging 2000, 12, 92–106. [Google Scholar] [CrossRef]
- Ring, M. Special Topic: PDF Only The History of Maxillofacial Prosthetics. Plastic and Reconstructive Surgery 1991, 87, 174–184. [Google Scholar] [CrossRef] [PubMed]
- Jindal, S.K.; Sherriff, M.; Waters, M.G.; Smay, J.E.; Coward, T.J. Development of a 3D printable maxillofacial silicone: Part II. Optimization of moderator and thixotropic agent. The Journal of Prosthetic Dentistry 2018, 119, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Liravi, F.; Toyserkani, E. A hybrid additive manufacturing method for the fabrication of silicone bio-structures: 3D printing optimization and surface characterization. Materials & Design 2018, 138, 46–61. [Google Scholar]
- Lanzara, D.R.; Viswambaran, D.M.; Kumar, D.D. Maxillofacial prosthetic materials: current status and recent advances: A comprehensive review. International Journal of Applied Dental Sciences 2021, 7, 255–259. [Google Scholar] [CrossRef]
- Powell, S.K.; Cruz, R.L.J.; Ross, M.T.; Woodruff, M.A. Past, Present, and Future of Soft-Tissue Prosthetics: Advanced Polymers and Advanced Manufacturing. Advanced Materials 2020, 32, 2001122. [Google Scholar] [CrossRef]
- Goel, G.K.; Jain, D.; Goel, D.; Juneja, P. Rehabilitation after Surgical Treatment for Retinoblastoma: Ocular Prosthesis for a 6-Month-Old Child. Journal of Prosthodontics 2012, 21, 408–412. [Google Scholar] [CrossRef]
- Lemon, J.C.; Chambers, M.S.; Wesley, P.J.; Martin, J.W. Technique for fabricating a mirror-image prosthetic ear. The Journal of Prosthetic Dentistry 1996, 75, 292–293. [Google Scholar] [CrossRef] [PubMed]
- Cruz, R.L.J.; Ross, M.T.; Powell, S.K.; Woodruff, M.A. Advancements in Soft-Tissue Prosthetics Part A: The Art of Imitating Life. Frontiers in Bioengineering and Biotechnology 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Pritham, C.H. Fundamentals of Facial Prosthetics. JPO Journal of Prosthetics and Orthotics 1995, 7, 22A. [Google Scholar] [CrossRef]
- Lewis, D.H.; Castleberry, D.J. An assessment of recent advances in external maxillofacial materials. The Journal of Prosthetic Dentistry 1980, 43, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Murtezani, I.; Sharma, N.; Thieringer, F.M. Medical 3D printing with a focus on Point-of-Care in Cranio- and Maxillofacial Surgery. A systematic review of literature. Annals of 3D Printed Medicine 2022, 6, 100059. [Google Scholar] [CrossRef]
- Schubert, C.; van Langeveld, M.C.; Donoso, L.A. Innovations in 3D printing: a 3D overview from optics to organs. British Journal of Ophthalmology 2014, 98, 159–161. [Google Scholar] [CrossRef]
- Hadad, H.; Boos Lima, F.B.; Shirinbak, I.; Porto, T.S.; Chen, J.E.; Guastaldi, F.P. The impact of 3D printing on oral and maxillofacial surgery. Journal of 3D Printing in Medicine 2023, 7. [Google Scholar] [CrossRef]
- Jazayeri, H.E.; Kang, S.; Masri, R.M.; Kuhn, L.; Fahimipour, F.; Vanevenhoven, R.; Thompson, G.; Gheisarifar, M.; Tahriri, M.; Tayebi, L. Advancements in craniofacial prosthesis fabrication: A narrative review of holistic treatment. The Journal of Advanced Prosthodontics 2018, 10, 430. [Google Scholar] [CrossRef] [PubMed]
- Reitemeier, B.; Notni, G.; Heinze, M.; Schöne, C.; Schmidt, A.; Fichtner, D. Optical modeling of extraoral defects. The Journal of Prosthetic Dentistry 2004, 91, 80–84. [Google Scholar] [CrossRef]
- Feng, Z.; Dong, Y.; Zhao, Y.; Bai, S.; Zhou, B.; Bi, Y.; Wu, G. Computer-assisted technique for the design and manufacture of realistic facial prostheses. British Journal of Oral and Maxillofacial Surgery 2010, 48, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Khorsandi, D.; Fahimipour, A.; Abasian, P.; Saber, S.S.; Seyedi, M.; Ghanavati, S.; Ahmad, A.; De Stephanis, A.A.; Taghavinezhaddilami, F.; Leonova, A.; et al. 3D and 4D printing in dentistry and maxillofacial surgery: Printing techniques, materials, and applications. Acta Biomaterialia 2021, 122, 26–49. [Google Scholar] [CrossRef]
- Generalova, A. N.; Demina, P.A.; Akasov, R.A.; Khaydukov, E.V. Photopolymerization in 3D printing of tissue-engineered constructs for regenerative medicine. Russian Chemical Reviews 2023, 92, RCR5068. [Google Scholar]
- Phogat, A.; Chhabra, D.; Sindhu, V.; Ahlawat, A. Analysis of wear assessment of FDM printed specimens with PLA, multi-material and ABS via hybrid algorithms. Materials Today: Proceedings 2022, 62, 37–43. [Google Scholar] [CrossRef]
- Ozbolat, I.T.; Hospodiuk, M. Current advances and future perspectives in extrusion-based bioprinting. Biomaterials 2016, 76, 321–343. [Google Scholar] [CrossRef]
- Dwivedi, R.; Mehrotra, D. 3D bioprinting and craniofacial regeneration. Journal of Oral Biology and Craniofacial Research 2020, 10, 650–659. [Google Scholar] [CrossRef]
- Baca, D.; Ahmad, R. The impact on the mechanical properties of multi-material polymers fabricated with a single mixing nozzle and multi-nozzle systems via fused deposition modeling. The International Journal of Advanced Manufacturing Technology 2020, 106, 4509–4520. [Google Scholar] [CrossRef]
- Wang, X.; Jiang, M.; Zhou, Z.; Gou, J.; Hui, D. 3D printing of polymer matrix composites: A review and prospective. Composites Part B: Engineering 2017, 110, 442–458. [Google Scholar] [CrossRef]
- Liu, Q.; Zhang, N.; Wei, W.; Hu, X.; Tan, Y.; Yu, Y.; Deng, Y.; Bi, C.; Zhang, L.; Zhang, H. Assessing the dynamic extrusion-based 3D printing process for power-law fluid using numerical simulation. Journal of Food Engineering 2020, 275, 109861. [Google Scholar] [CrossRef]
- Savelyev, A.G.; Sochilina, A. V.; Akasov, R.A.; Mironov, A. V.; Kapitannikova, A.Y.; Borodina, T.N.; Sholina, N. V.; Khaydukov, K. V.; Zvyagin, A. V.; Generalova, A.N.; et al. Facile Cell-Friendly Hollow-Core Fiber Diffusion-Limited Photofabrication. Frontiers in Bioengineering and Biotechnology 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Ngo, T.D.; Kashani, A.; Imbalzano, G.; Nguyen, K.T.Q.; Hui, D. Additive manufacturing (3D printing): A review of materials, methods, applications and challenges. Composites Part B: Engineering 2018, 143, 172–196. [Google Scholar] [CrossRef]
- Kyle, S.; Jessop, Z.M.; Al-Sabah, A.; Whitaker, I.S. Biofabrication: ‘Printability’’ of Candidate Biomaterials for Extrusion Based 3D Printing: State-of-the-Art (Adv. Healthcare Mater. 16/2017).’ Advanced Healthcare Materials 2017, 6.
- Ozbolat, I.T.; Hospodiuk, M. Current advances and future perspectives in extrusion-based bioprinting. Biomaterials 2016, 76, 321–343. [Google Scholar] [CrossRef]
- Ovsianikov, A.; Schlie, S.; Ngezahayo, A.; Haverich, A.; Chichkov, B.N. Two-photon polymerization technique for microfabrication of CAD-designed 3D scaffolds from commercially available photosensitive materials. Journal of Tissue Engineering and Regenerative Medicine 2007, 1, 443–449. [Google Scholar] [CrossRef]
- Kuang, X.; Roach, D.J.; Wu, J.; Hamel, C.M.; Ding, Z.; Wang, T.; Dunn, M.L.; Qi, H.J. Advances in 4D Printing: Materials and Applications. Advanced Functional Materials 2019, 29, 1805290. [Google Scholar] [CrossRef]
- Momeni, F.; Mehdi, M.; Hassani, N.S.; Liu, X.; Ni, J. A review of 4D printing. Materials & Design 2017, 122, 42–79. [Google Scholar]
- Mazzoli, A. Selective laser sintering in biomedical engineering. Medical & Biological Engineering & Computing 2013, 51, 245–256. [Google Scholar]
- Dwivedi, R.; Mehrotra, D. 3D bioprinting and craniofacial regeneration. Journal of Oral Biology and Craniofacial Research 2020, 10, 650–659. [Google Scholar] [CrossRef]
- Ziaee, M.; Crane, N.B. Binder jetting: A review of process, materials, and methods. Additive Manufacturing 2019, 28, 781–801. [Google Scholar] [CrossRef]
- Billiet, T.; Vandenhaute, M.; Schelfhout, J.; Van Vlierberghe, S.; Dubruel, P. A review of trends and limitations in hydrogel-rapid prototyping for tissue engineering. Biomaterials 2012, 33, 6020–6041. [Google Scholar] [CrossRef] [PubMed]
- Shahzad, K.; Deckers, J.; Zhang, Z.; Kruth, J.-P.; Vleugels, J. Additive manufacturing of zirconia parts by indirect selective laser sintering. Journal of the European Ceramic Society 2014, 34, 81–89. [Google Scholar] [CrossRef]
- Hull, W.C. Apparatus for Production of Three-Dimensional Objects by Stereolithography 1984.
- Levato, R.; Lim, K.S.; Li, W.; Asua, A.U.; Peña, L.B.; Wang, M.; Falandt, M.; Bernal, P.N.; Gawlitta, D.; Zhang, Y.S.; et al. High-resolution lithographic biofabrication of hydrogels with complex microchannels from low-temperature-soluble gelatin bioresins. Materials Today Bio 2021, 12, 100162. [Google Scholar] [CrossRef] [PubMed]
- Kelly, B.E.; Bhattacharya, I.; Heidari, H.; Shusteff, M.; Spadaccini, C.M.; Taylor, H.K. Volumetric additive manufacturing via tomographic reconstruction. Science 2019, 363, 1075–1079. [Google Scholar] [CrossRef] [PubMed]
- Tumbleston, J.R.; Shirvanyants, D.; Ermoshkin, N.; Janusziewicz, R.; Johnson, A.R.; Kelly, D.; Chen, K.; Pinschmidt, R.; Rolland, J.P.; Ermoshkin, A.; et al. Continuous liquid interface production of 3D objects. Science 2015, 347, 1349–1352. [Google Scholar] [CrossRef]
- Torgersen, J.; Qin, X.-H.; Li, Z.; Ovsianikov, A.; Liska, R.; Stampfl, J. Hydrogels for Two-Photon Polymerization: A Toolbox for Mimicking the Extracellular Matrix. Advanced Functional Materials 2013, 23, 4542–4554. [Google Scholar] [CrossRef]
- Shahrubudin, N.; Koshy, P.; Alipal, J.; Kadir, M.H.A.; Lee, T.C. Challenges of 3D printing technology for manufacturing biomedical products: A case study of Malaysian manufacturing firms. Heliyon 2020, 6, e03734. [Google Scholar] [CrossRef]
- Bandyopadhyay, A.; Bose, S.; Narayan, R. Translation of 3D printed materials for medical applications. MRS Bulletin 2022, 47, 39–48. [Google Scholar] [CrossRef]
- Tanveer, W.; Ridwan-Pramana, A.; Molinero-Mourelle, P.; Koolstra, J.H.; Forouzanfar, T. Systematic Review of Clinical Applications of CAD/CAM Technology for Craniofacial Implants Placement and Manufacturing of Nasal Prostheses. International Journal of Environmental Research and Public Health 2021, 18, 3756. [Google Scholar] [CrossRef]
- 3D Printing in Plastic Reconstructive and Aesthetic Surgery; Di Rosa, L., Ed.; Springer International Publishing: Cham, 2022. ISBN 978-3-031-10557-9.
- Zhou, L.; Fu, J.; He, Y. A Review of 3D Printing Technologies for Soft Polymer Materials. Advanced Functional Materials 2020, 30, 2000187. [Google Scholar] [CrossRef]
- Aziz, T.; Waters, M.; Jagger, R. Analysis of the properties of silicone rubber maxillofacial prosthetic materials. Journal of Dentistry 2003, 31, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Al-Harbi, F.A.; Ayad, N.M.; Saber, M.A.; ArRejaie, A.S.; Morgano, S.M. Mechanical behavior and color change of facial prosthetic elastomers after outdoor weathering in a hot and humid climate. The Journal of Prosthetic Dentistry 2015, 113, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Younis, I.; Gault, D.; Sabbagh, W.; Kang, N. V. Patient satisfaction and aesthetic outcomes after ear reconstruction with a Branemark-type, bone-anchored, ear prosthesis: A 16 year review. Journal of Plastic, Reconstructive & Aesthetic Surgery 2010, 63, 1650–1655. [Google Scholar]
- Frade, J.P.; Arthington-Skaggs, B.A. Effect of serum and surface characteristics on Candida albicans biofilm formation. Mycoses 2011, 54, e154–e162. [Google Scholar] [CrossRef]
- Fantini, M.; De Crescenzio, F.; Ciocca, L. Design and Rapid Manufacturing of anatomical prosthesis for facial rehabilitation. International Journal on Interactive Design and Manufacturing (IJIDeM) 2013, 7, 51–62. [Google Scholar] [CrossRef]
- Reddy, Jr.; Kumar, Bm.; Ahila, S.; Rajendiran, S. Materials in maxillo-facial prosthesis. Journal of Indian Academy of Dental Specialist Researchers 2015, 2, 1. [Google Scholar] [CrossRef]
- Sanohkan, S.; Kukiattrakoon, B.; Peampring, C. Tensile bond strength of facial silicone and acrylic resin using different primers. Journal of Orofacial Sciences 2017, 9, 48. [Google Scholar] [CrossRef]
- Zhou, L.; Fu, J.; He, Y. A Review of 3D Printing Technologies for Soft Polymer Materials. Advanced Functional Materials 2020, 30, 2000187. [Google Scholar] [CrossRef]
- Desai, S.M.; Sonawane, R.Y.; More, A.P. Thermoplastic polyurethane for three-dimensional printing applications: A review. Polymers for Advanced Technologies 2023, 34, 2061–2082. [Google Scholar] [CrossRef]
- Lemon, J.C.; Kiat-amnuay, S.; Gettleman, L.; Martin, J.W.; Chambers, M.S. Facial prosthetic rehabilitation: preprosthetic surgical techniques and biomaterials. Current Opinion in Otolaryngology & Head and Neck Surgery 2005, 13, 255–262. [Google Scholar]
- Kim, B.R.; Kim, S.H.; Ko, J.; Baek, S.W.; Park, Y.K.; Kim, Y.J.; Yoon, J.S. A Pilot Clinical Study of Ocular Prosthesis Fabricated by Three-dimensional Printing and Sublimation Technique. Korean Journal of Ophthalmology 2021, 35, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Guevara, C.; Matouk, M. In-office 3D printed guide for rhinoplasty. International Journal of Oral and Maxillofacial Surgery 2021, 50, 1563–1565. [Google Scholar] [CrossRef] [PubMed]
- Nuseir, A.; Hatamleh, M.M.; Alnazzawi, A.; Al-Rabab’ah, M.; Kamel, B.; Jaradat, E. Direct 3D Printing of Flexible Nasal Prosthesis: Optimized Digital Workflow from Scan to Fit. Journal of Prosthodontics 2019, 28, 10–14. [Google Scholar] [CrossRef]
- Diken Türksayar, A.; Saglam, S.; Bulut, A. Retention systems used in maxillofacial prostheses: A review. Nigerian Journal of Clinical Practice 2019, 22, 1629. [Google Scholar] [PubMed]
- Kim, S.Y. Application of the three-dimensionally printed biodegradable polycaprolactone (PCL) mesh in repair of orbital wall fractures. Journal of Cranio-Maxillofacial Surgery 2019, 47, 1065–1071. [Google Scholar] [CrossRef]
- Han, H.H.; Shim, J.-H.; Lee, H.; Kim, B.Y.; Lee, J.-S.; Jung, J.W.; Yun, W.-S.; Baek, C.H.; Rhie, J.-W.; Cho, D.-W. Reconstruction of Complex Maxillary Defects Using Patient-specific 3D-printed Biodegradable Scaffolds. Plastic and Reconstructive Surgery - Global Open 2018, 6, e1975. [Google Scholar] [CrossRef]
- Witek, L.; Khouri, K.S.; Coelho, P.G.; Flores, R.L. Patient-specific 3D Models for Autogenous Ear Reconstruction. Plastic and Reconstructive Surgery - Global Open 2016, 4, e1093. [Google Scholar] [CrossRef]
- Berens, A.M.; Newman, S.; Bhrany, A.D.; Murakami, C.; Sie, K.C.Y.; Zopf, D.A. Computer-Aided Design and 3D Printing to Produce a Costal Cartilage Model for Simulation of Auricular Reconstruction. Otolaryngology–Head and Neck Surgery 2016, 155, 356–359. [Google Scholar] [CrossRef]
- Callahan, A.B.; Campbell, A.A.; Petris, C.; Kazim, M. Low-Cost 3D Printing Orbital Implant Templates in Secondary Orbital Reconstructions. Ophthalmic Plastic & Reconstructive Surgery 2017, 33, 376–380. [Google Scholar]
- Borghi, A.; Ruggiero, F.; Tenhagen, M.; Schievano, S.; Ponniah, A.; Dunaway, D.; O’Hara, J.; Ong, J.; Britto, J.A. Design and manufacturing of a patient-specific nasal implant for congenital arhinia: Case report. JPRAS Open 2019, 21, 28–34. [Google Scholar] [CrossRef]
- Adhitya, M.; Sunarso, S.; Muis, A. Comparison of Popular Three-Dimensional Printing Materials for Oral and Maxillofacial Surgical Guidance Model Oral and Maxillofacial Surgical Guidance Model. Journal of Dentistry Indonesia 2020, 27. [Google Scholar] [CrossRef]
- Choi, Y.D.; Kim, Y.; Park, E. Patient-Specific Augmentation Rhinoplasty Using a Three-Dimensional Simulation Program and Three-Dimensional Printing. Aesthetic Surgery Journal 2017, 37, 988–998. [Google Scholar] [CrossRef] [PubMed]
- Nishimoto, S.; Sotsuka, Y.; Kawai, K.; Fujita, K.; Kakibuchi, M. Three-Dimensional Mock-Up Model for Chondral Framework in Auricular Reconstruction, Built with a Personal Three-Dimensional Printer. Plastic and Reconstructive Surgery 2014, 134, 180e–181e. [Google Scholar] [CrossRef] [PubMed]
- Unkovskiy, A.; Spintzyk, S.; Brom, J.; Huettig, F.; Keutel, C. Direct 3D printing of silicone facial prostheses: A preliminary experience in digital workflow. The Journal of Prosthetic Dentistry 2018, 120, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Unkovskiy, A.; Wahl, E.; Huettig, F.; Keutel, C.; Spintzyk, S. Multimaterial 3D printing of a definitive silicone auricular prosthesis: An improved technique. The Journal of Prosthetic Dentistry 2021, 125, 946–950. [Google Scholar] [CrossRef] [PubMed]
- Denour, E.; Woo, A.S.; Crozier, J.; Van Dongen, C. The Use of Three-Dimensional Photography and Printing in the Fabrication of a Nasal Prosthesis. Journal of Craniofacial Surgery 2020, Publish Ah.
- Moore, D.J.; Glaser, Z.R.; Tabacco, M.J.; Linebaugh, M.G. Evaluation of polymeric materials for maxillofacial prosthetics. The Journal of Prosthetic Dentistry 1977, 38, 319–326. [Google Scholar] [CrossRef]
- Stansbury, J.W.; Idacavage, M.J. 3D printing with polymers: Challenges among expanding options and opportunities. Dental Materials 2016, 32, 54–64. [Google Scholar] [CrossRef]
- Goiato, M.; Freitas, E.; dos Santos, D.; de Medeiros, R.; Sonego, M. Acrylic Resin Cytotoxicity for Denture Base: Literature Review. Advances in Clinical and Experimental Medicine 2015, 24, 679–686. [Google Scholar] [CrossRef]
- Fiaschi, P.; Pavanello, M.; Imperato, A.; Dallolio, V.; Accogli, A.; Capra, V.; Consales, A.; Cama, A.; Piatelli, G. Surgical results of cranioplasty with a polymethylmethacrylate customized cranial implant in pediatric patients: a single-center experience. Journal of Neurosurgery: Pediatrics 2016, 17, 705–710. [Google Scholar] [CrossRef]
- Goiato, M.; Freitas, E.; dos Santos, D.; de Medeiros, R.; Sonego, M. Acrylic Resin Cytotoxicity for Denture Base: Literature Review. Advances in Clinical and Experimental Medicine 2015, 24, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Espalin, D.; Arcaute, K.; Rodriguez, D.; Medina, F.; Posner, M.; Wicker, R. Fused deposition modeling of patient-specific polymethylmethacrylate implants. Rapid Prototyping Journal 2010, 16, 164–173. [Google Scholar] [CrossRef]
- Alam, M.S.; Sugavaneswaran, M.; Arumaikkannu, G.; Mukherjee, B. An innovative method of ocular prosthesis fabrication by bio-CAD and rapid 3-D printing technology: A pilot study. Orbit 2017, 36, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Vu, C.C.; Nguyen, T.T.; Kim, S.; Kim, J. Effects of 3D Printing-Line Directions for Stretchable Sensor Performances. Materials 2021, 14, 1791. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, Y.; Guo, Y.; Li, J.; Yu, Y.; Jiang, K.; Zhang, H.; Guo, S. Study on the forming and sensing properties of laser-sintered TPU/CNT composites for plantar pressure sensors. The International Journal of Advanced Manufacturing Technology 2021, 112, 2211–2222. [Google Scholar] [CrossRef]
- Yang, Y.; Chen, Y.; Wei, Y.; Li, Y. 3D printing of shape memory polymer for functional part fabrication. The International Journal of Advanced Manufacturing Technology 2016, 84, 2079–2095. [Google Scholar] [CrossRef]
- Sanei, S.H.R.; Popescu, D. 3D-Printed Carbon Fiber Reinforced Polymer Composites: A Systematic Review. Journal of Composites Science 2020, 4, 98. [Google Scholar] [CrossRef]
- Covolan, V.L.; Di Ponzio, R.; Chiellini, F.; Grillo Fernandes, E.; Solaro, R.; Chiellini, E. Polyurethane Based Materials for the Production of Biomedical Materials. Macromolecular Symposia 2001, 169, 273–282. [Google Scholar] [CrossRef]
- Touchet, T.J.; Cosgriff-Hernandez, E.M. Advances in Polyurethane Biomaterials. In; Cooper, S.L., Guan, J., Eds.; Elsevier, New York, 2016; pp. 3–22.
- Xiao, J.; Gao, Y. The manufacture of 3D printing of medical grade TPU. Progress in Additive Manufacturing 2017, 2, 117–123. [Google Scholar] [CrossRef]
- Kennedy, Z.C.; Christ, J.F. Printing polymer blends through in situ active mixing during fused filament fabrication. Additive Manufacturing 2020, 36, 101233. [Google Scholar] [CrossRef]
- Rahmatabadi, D.; Ghasemi, I.; Baniassadi, M.; Abrinia, K.; Baghani, M. 3D printing of PLA-TPU with different component ratios: Fracture toughness, mechanical properties, and morphology. Journal of Materials Research and Technology 2022, 21, 3970–3981. [Google Scholar] [CrossRef]
- Desai, S.M.; Sonawane, R.Y.; More, A.P. Thermoplastic polyurethane for three-dimensional printing applications: A review. Polymers for Advanced Technologies 2023, 34, 2061–2082. [Google Scholar] [CrossRef]
- Mondal, D.; Griffith, M.; Venkatraman, S.S. Polycaprolactone-based biomaterials for tissue engineering and drug delivery: Current scenario and challenges. International Journal of Polymeric Materials and Polymeric Biomaterials 2016, 65, 255–265. [Google Scholar] [CrossRef]
- Yang, X.; Wang, Y.; Zhou, Y.; Chen, J.; Wan, Q. The Application of Polycaprolactone in Three-Dimensional Printing Scaffolds for Bone Tissue Engineering. Polymers 2021, 13, 2754. [Google Scholar] [CrossRef] [PubMed]
- Youssef, A.; Hollister, S.J.; Dalton, P.D. Additive manufacturing of polymer melts for implantable medical devices and scaffolds. Biofabrication 2017, 9, 012002. [Google Scholar] [CrossRef]
- Nyberg, E.; Rindone, A.; Dorafshar, A.; Grayson, W.L. Comparison of 3D-Printed Poly-ɛ-Caprolactone Scaffolds Functionalized with Tricalcium Phosphate, Hydroxyapatite, Bio-Oss, or Decellularized Bone Matrix. Tissue Engineering Part A 2017, 23, 503–514. [Google Scholar] [CrossRef] [PubMed]
- Liao, G.; Jiang, S.; Xu, X.; Ke, Y. Electrospun aligned PLLA/PCL/HA composite fibrous membranes and their in vitro degradation behaviors. Materials Letters 2012, 82, 159–162. [Google Scholar] [CrossRef]
- Chen, F.; Hochleitner, G.; Woodfield, T.; Groll, J.; Dalton, P.D.; Amsden, B.G. Additive Manufacturing of a Photo-Cross-Linkable Polymer via Direct Melt Electrospinning Writing for Producing High Strength Structures. Biomacromolecules 2016, 17, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Stichler, S.; Böck, T.; Paxton, N.; Bertlein, S.; Levato, R.; Schill, V.; Smolan, W.; Malda, J.; Teßmar, J.; Blunk, T.; et al. Double printing of hyaluronic acid/poly(glycidol) hybrid hydrogels with poly( ε -caprolactone) for MSC chondrogenesis. Biofabrication 2017, 9, 044108. [Google Scholar] [CrossRef] [PubMed]
- Pretula, J.; Slomkowski, S.; Penczek, S. Polylactides—Methods of synthesis and characterization. Advanced Drug Delivery Reviews 2016, 107, 3–16. [Google Scholar] [CrossRef]
- Farah, S.; Anderson, D.G.; Langer, R. Physical and mechanical properties of PLA, and their functions in widespread applications — A comprehensive review. Advanced Drug Delivery Reviews 2016, 107, 367–392. [Google Scholar] [CrossRef]
- Esposito Corcione, C.; Gervaso, F.; Scalera, F.; Padmanabhan, S.K.; Madaghiele, M.; Montagna, F.; Sannino, A.; Licciulli, A.; Maffezzoli, A. Highly loaded hydroxyapatite microsphere/ PLA porous scaffolds obtained by fused deposition modelling. Ceramics International 2019, 45, 2803–2810. [Google Scholar] [CrossRef]
- Ritz, U.; Gerke, R.; Götz, H.; Stein, S.; Rommens, P.M. A New Bone Substitute Developed from 3D-Prints of Polylactide (PLA) Loaded with Collagen I: An In Vitro Study. International Journal of Molecular Sciences 2017, 18, 2569. [Google Scholar] [CrossRef] [PubMed]
- Marchewka, J.; Laska, J. Processing of poly-l-lactide and poly(l-lactide-co-trimethylene carbonate) blends by fused filament fabrication and fused granulate fabrication using RepRap 3D printer. The International Journal of Advanced Manufacturing Technology 2020, 106, 4933–4944. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Devine, J.N. PEEK biomaterials in trauma, orthopedic, and spinal implants. Biomaterials 2007, 28, 4845–4869. [Google Scholar] [CrossRef] [PubMed]
- Tekin, S.; Cangül, S.; Adıgüzel, Ö.; Değer, Y. Areas for use of PEEK material in dentistry. International Dental Research 2018, 8, 84–92. [Google Scholar] [CrossRef]
- Mylläri, V.; Ruoko, T.-P.; Järvelä, P. The effects of UV irradiation to polyetheretherketone fibres – Characterization by different techniques. Polymer Degradation and Stability 2014, 109, 278–284. [Google Scholar] [CrossRef]
- Atkinson, J. Enthalpic relaxation in semi-crystalline PEEK. Polymer 2002, 43, 731–735. [Google Scholar] [CrossRef]
- Termoplasti, Z.; Modeliranje, N. Processing poly (ether etherketone) on a 3D printer for thermoplastic modelling, Materiali in Tehnologije 2013, 47, 715–721. [Google Scholar]
- Cicala, G.; Latteri, A.; Del Curto, B.; Lo Russo, A.; Recca, G.; Farè, S. Engineering Thermoplastics for Additive Manufacturing: A Critical Perspective with Experimental Evidence to Support Functional Applications. Journal of Applied Biomaterials & Functional Materials 2017, 15, 10–18. [Google Scholar]
- Xiaoyong, S.; Liangcheng, C.; Honglin, M.; Peng, G.; Zhanwei, B.; Cheng, L. Experimental Analysis of High Temperature PEEK Materials on 3D Printing Test. In Proceedings of the 2017 9th International Conference on Measuring Technology and Mechatronics Automation (ICMTMA); IEEE, 2017; pp. 13–16.
- Vaezi, M.; Yang, S. Extrusion-based additive manufacturing of PEEK for biomedical applications. Virtual and Physical Prototyping 2015, 10, 123–135. [Google Scholar] [CrossRef]
- Yang, C.; Tian, X.; Li, D.; Cao, Y.; Zhao, F.; Shi, C. Influence of thermal processing conditions in 3D printing on the crystallinity and mechanical properties of PEEK material. Journal of Materials Processing Technology 2017, 248, 1–7. [Google Scholar] [CrossRef]
- Dupin, S.; Lame, O.; Barrès, C.; Charmeau, J.-Y. Microstructural origin of physical and mechanical properties of polyamide 12 processed by laser sintering. European Polymer Journal 2012, 48, 1611–1621. [Google Scholar] [CrossRef]
- Rong-Ji, W.; Xin-hua, L.; Qing-ding, W.; Lingling, W. Optimizing process parameters for selective laser sintering based on neural network and genetic algorithm. The International Journal of Advanced Manufacturing Technology 2009, 42, 1035–1042. [Google Scholar] [CrossRef]
- Fatemi, S.A.; Ashany, J.Z.; Aghchai, A.J.; Abolghasemi, A. Experimental investigation of process parameters on layer thickness and density in direct metal laser sintering: a response surface methodology approach. Virtual and Physical Prototyping 2017, 12, 133–140. [Google Scholar] [CrossRef]
- Deng, F.; Wu; Liu, X.; Guo; Wei Nano-TiO2/PEEK bioactive composite as a bone substitute material: in vitro and in vivo studies. International Journal of Nanomedicine, 2012; 1215. [CrossRef] [PubMed]
- Monich, P.R.; Henriques, B.; Novaes de Oliveira, A.P.; Souza, J.C.M.; Fredel, M.C. Mechanical and biological behavior of biomedical PEEK matrix composites: A focused review. Materials Letters 2016, 185, 593–597. [Google Scholar] [CrossRef]
- An, J.; Teoh, J.E.M.; Suntornnond, R.; Chua, C.K. Design and 3D Printing of Scaffolds and Tissues. Engineering 2015, 1, 261–268. [Google Scholar] [CrossRef]
- Roskies, M.; Jordan, J.O.; Fang, D.; Abdallah, M.-N.; Hier, M.P.; Mlynarek, A.; Tamimi, F.; Tran, S.D. Improving PEEK bioactivity for craniofacial reconstruction using a 3D printed scaffold embedded with mesenchymal stem cells. Journal of Biomaterials Applications 2016, 31, 132–139. [Google Scholar] [CrossRef]
- McHutchion, L.; Aalto, D. Simulation of tissue-prosthesis margin interface by using surface scanning and digital design for auricular prostheses. The Journal of Prosthetic Dentistry 2021, 125, 361–372. [Google Scholar] [CrossRef]
- Jockusch, J.; Ozcan, M. Additive manufacturing of dental polymers: An overview on processes, materials and applications. Dental Materials Journal 2020, 39, 345–354. [Google Scholar] [CrossRef]
- Kumar, R.; Singh, R.; Farina, I. On the 3D printing of recycled ABS, PLA and HIPS thermoplastics for structural applications. PSU Research Review 2018, 2, 115–137. [Google Scholar] [CrossRef]
- Kaveh, M.; Badrossamay, M.; Foroozmehr, E.; Hemasian Etefagh, A. Optimization of the printing parameters affecting dimensional accuracy and internal cavity for HIPS material used in fused deposition modeling processes. Journal of Materials Processing Technology 2015, 226, 280–286. [Google Scholar] [CrossRef]
- Harris, M.; Potgieter, J.; Archer, R.; Arif, K.M. Effect of Material and Process Specific Factors on the Strength of Printed Parts in Fused Filament Fabrication: A Review of Recent Developments. Materials 2019, 12, 1664. [Google Scholar] [CrossRef] [PubMed]
- Echte, A. Rubber-Toughened Styrene Polymers. In; 1989; pp. 15–64.
- Quan, H.; Zhang, T.; Xu, H.; Luo, S.; Nie, J.; Zhu, X. Photo-curing 3D printing technique and its challenges. Bioactive Materials 2020, 5, 110–115. [Google Scholar] [CrossRef]
- Rocha, C.R.; Torrado Perez, A.R.; Roberson, D.A.; Shemelya, C.M.; MacDonald, E.; Wicker, R.B. Novel ABS-based binary and ternary polymer blends for material extrusion 3D printing. Journal of Materials Research 2014, 29, 1859–1866. [Google Scholar] [CrossRef]
- Polyzois, G.L. Evaluation of a New Silicone Elastomer for Maxillofacial Prostheses. Journal of Prosthodontics 1995, 4, 38–41. [Google Scholar] [CrossRef] [PubMed]
- Goiato, M.C.; Haddad, M.F.; Santos, D.M. dos; Pesqueira, A.A.; Moreno, A. Hardness evaluation of prosthetic silicones containing opacifiers following chemical disinfection and accelerated aging. Brazilian Oral Research 2010, 24, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Mitra, A. Maxillofacial Prosthetic Materials- An Inclination Towards Silicones. JOURNAL OF CLINICAL AND DIAGNOSTIC RESEARCH 2014. [CrossRef]
- Chalian, V.A.; Phillips, R.W. Materials in maxillofacial prosthetics. Journal of Biomedical Materials Research 1974, 8, 349–363. [Google Scholar] [CrossRef] [PubMed]
- Bakirov, A. V.; Krasheninnikov, S. V.; Shcherbina, M.A.; Meshkov, I.B.; Kalinina, A.A.; Gorodov, V. V.; Tatarinova, E.A.; Muzafarov, A.M.; Chvalun, S.N. True Molecular Composites: Unusual Structure and Properties of PDMS-MQ Resin Blends. Polymers 2022, 15, 48. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, Z.; Mark, J.E. Biomimetic materials: recent developments in organic-inorganic hybrids. Materials Science and Engineering: C 1998, 6, 183–196. [Google Scholar] [CrossRef]
- Zare, M.; Ghomi, E.R.; Venkatraman, P.D.; Ramakrishna, S. Silicone-based biomaterials for biomedical applications: Antimicrobial strategies and 3D printing technologies. Journal of Applied Polymer Science 2021, 138. [Google Scholar] [CrossRef]
- Colas, A.; Curtis, J. Silicones. In Handbook of Polymer Applications in Medicine and Medical Devices; Elsevier, 2013; pp. 131–143.
- Muslov, S.A.; Polyakov, D.I.; Lotkov, A.I.; Stepanov, A.G.; Arutyunov, S.D. Measurement and Calculation of Mechanical Properties of Silicone Rubber. Russian Physics Journal 2021, 63, 1525–1529. [Google Scholar] [CrossRef]
- Santawisuk, W.; Kanchnavasita, W.; Sirisisna, C.; Harniattisai, C. Dynamic viscoelastic properties of experimental silicone soft lining materials. Dental Materials Journal 2010, 29, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Kiat-amnuay, S.; Powers, J.M.; Zhao, Y. Effect of nano-oxide concentration on the mechanical properties of a maxillofacial silicone elastomer. The Journal of Prosthetic Dentistry 2008, 100, 465–473. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Yang, F.; Zhao, H.; Gao, Q.; Xia, B.; Fu, J. Research on the printability of hydrogels in 3D bioprinting. Scientific Reports 2016, 6, 29977. [Google Scholar] [CrossRef] [PubMed]
- Rekštytė, S.; Malinauskas, M.; Juodkazis, S. Three-dimensional laser micro-sculpturing of silicone: towards bio-compatible scaffolds. Optics Express 2013, 21, 17028. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, P.G.; Disa, J.J. Challenges in midface reconstruction. Seminars in Surgical Oncology 2000, 19, 218–225. [Google Scholar] [CrossRef]
- Abu-Serriah, M.M.; McGowan, D.A.; Moos, K.F.; Bagg, J. Extra-oral craniofacial endosseous implants and radiotherapy. International Journal of Oral and Maxillofacial Surgery 2003, 32, 585–592. [Google Scholar] [CrossRef]
- Cobein, M.V.; Coto, N.P.; Crivello Junior, O.; Lemos, J.B.D.; Vieira, L.M.; Pimentel, M.L.; Byrne, H.J.; Dias, R.B. Retention systems for extraoral maxillofacial prosthetic implants: a critical review. British Journal of Oral and Maxillofacial Surgery 2017, 55, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Feldstein, M.M.; Dormidontova, E.E.; Khokhlov, A.R. Pressure sensitive adhesives based on interpolymer complexes. Progress in Polymer Science 2015, 42, 79–153. [Google Scholar] [CrossRef]
- Applications of Pressure-Sensitive Products; Benedek, I., Feldstein, M.M., Eds.; CRC Press, 2008. ISBN 9780429150517.
- Droesbeke, M.A.; Aksakal, R.; Simula, A.; Asua, J.M.; Du Prez, F.E. Biobased acrylic pressure-sensitive adhesives. Progress in Polymer Science 2021, 117, 101396. [Google Scholar] [CrossRef]
- Lin, S.B.; Durfee, L.D.; Ekeland, R.A.; McVie, J.; Schalau, G.K. Recent advances in silicone pressure-sensitive adhesives. Journal of Adhesion Science and Technology 2007, 21, 605–623. [Google Scholar] [CrossRef]
- Kiat-amnuay, S.; Gettleman, L.; Goldsmith, L.J. Effect of multi-adhesive layering on retention of extraoral maxillofacial silicone prostheses in vivo. The Journal of Prosthetic Dentistry 2004, 92, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Goiato, M.C.; Delben, J.A.; Monteiro, D.R.; dos Santos, D.M. Retention Systems to Implant-Supported Craniofacial Prostheses. Journal of Craniofacial Surgery 2009, 20, 889–891. [Google Scholar] [CrossRef]
- Albrektsson, T.; Brånemark, P.-I.; Hansson, H.-A.; Lindström, J. Osseointegrated Titanium Implants: Requirements for Ensuring a Long-Lasting, Direct Bone-to-Implant Anchorage in Man. Acta Orthopaedica Scandinavica 1981, 52, 155–170. [Google Scholar] [CrossRef]
- Tjellström, A. Osseointegrated implants for replacement of absent or defective ears. Clinics in Plastic Surgery 1990, 17, 355–366. [Google Scholar] [CrossRef]
- Hu, S.; Arnaoutakis, D.; Kadakia, S.; Vest, A.; Sawhney, R.; Ducic, Y. Osseointegrated Implants and Prosthetic Reconstruction Following Skull Base Surgery. Seminars in Plastic Surgery 2017, 31, 214–221. [Google Scholar] [CrossRef]
- Owusu, J.A.; Boahene, K. Update of patient-specific maxillofacial implant. Current Opinion in Otolaryngology & Head and Neck Surgery 2015, 23, 261–264. [Google Scholar]
- Binder, W.J. Custom-Designed Facial Implants. Facial Plastic Surgery Clinics of North America 2008, 16, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Scolozzi, P. Maxillofacial Reconstruction Using Polyetheretherketone Patient-Specific Implants by “Mirroring” Computational Planning. Aesthetic Plastic Surgery 2012, 36, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.M.; Boahene, K.D.O.; Byrne, P.J. Use of Customized Polyetheretherketone (PEEK) Implants in the Reconstruction of Complex Maxillofacial Defects. Archives of Facial Plastic Surgery 2009, 11, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Fernandes da Silva, A.L.; Borba, A.M.; Simão, N.R.; Pedro, F.L.M.; Borges, A.H.; Miloro, M. Customized Polymethyl Methacrylate Implants for the Reconstruction of Craniofacial Osseous Defects. Case Reports in Surgery 2014, 2014, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Haug, S.P.; Richard, G.E.; Margiotti, E.; Winkler, M.M.; Moore, D.J. An In Vivo Evaluation of Adhesives Used in Extraoral Maxillofacial Prostheses. Journal of Prosthodontics 1995, 4, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Hatamleh, M.M.; Polyzois, G.L.; Nuseir, A.; Hatamleh, K.; Alnazzawi, A. Mechanical Properties and Simulated Aging of Silicone Maxillofacial Elastomers: Advancements in the Past 45 Years. Journal of Prosthodontics 2016, 25, 418–426. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, D.M.; Goiato, M.C.; Sinhoreti, M.A.C.; Fernandes, A.Ú.R.; Ribeiro, P. do P.; Dekon, S.F. de C. Color Stability of Polymers for Facial Prosthesis. Journal of Craniofacial Surgery 2010, 21, 54–58.
- Bettencourt, A.F.; Neves, C.B.; de Almeida, M.S.; Pinheiro, L.M.; Oliveira, S.A. e; Lopes, L.P.; Castro, M.F. Biodegradation of acrylic based resins: A review. Dental Materials 2010, 26, e171–e180. [Google Scholar] [CrossRef]
- Eleni, P.N.; Krokida, M.K.; Polyzois, G.L.; Charitidis, C.A.; Koumoulos, E.P.; Tsikourkitoudi, V.P.; Ziomas, I. Mechanical behaviour of a poydimethylsiloxane elastomer after outdoor weathering in two different weathering locations. Polymer Degradation and Stability 2011, 96, 470–476. [Google Scholar] [CrossRef]
- Rahman, A.M.; Jamayet, N. Bin; Nizami, M.M.U.I.; Johari, Y.; Husein, A.; Alam, M.K. Effect of Aging and Weathering on the Physical Properties of Maxillofacial Silicone Elastomers: A Systematic Review and Meta-Analysis. Journal of Prosthodontics 2019, 28, 36–48. [Google Scholar] [CrossRef]
- Eleni, P.N.; Krokida, M.; Polyzois, G.; Gettleman, L.; Bisharat, G.I. Effects of outdoor weathering on facial prosthetic elastomers. Odontology 2011, 99, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Eleni, P.N.; Krokida, M.K.; Polyzois, G.L. Effects of Storage in Simulated Skin Secretions on Mechanical Behavior and Color of Polydimethylsiloxanes Elastomers. Journal of Craniofacial Surgery 2011, 22, 830–836. [Google Scholar] [CrossRef] [PubMed]
- Ariani, N.; Vissink, A.; van Oort, R.P.; Kusdhany, L.; Djais, A.; Rahardjo, T.B.W.; van der Mei, H.C.; Krom, B.P. Microbial biofilms on facial prostheses. Biofouling 2012, 28, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Hatamleh, M.M.; Polyzois, G.L.; Silikas, N.; Watts, D.C. Effect of Extraoral Aging Conditions on Mechanical Properties of Maxillofacial Silicone Elastomer. Journal of Prosthodontics 2011, 20, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Eleni, P.N.; Perivoliotis, D.; Dragatogiannis, D.A.; Krokida, M.K.; Polyzois, G.L.; Charitidis, C.A.; Ziomas, I.; Gettleman, L. Tensile and microindentation properties of maxillofacial elastomers after different disinfecting procedures. Journal of the Mechanical Behavior of Biomedical Materials 2013, 28, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Nagay, B.E.; Goiato, M.C.; da Silva, E.V.F.; Andreotti, A.M.; Bitencourt, S.B.; Duque, C.; dos Santos, P.H.; dos Santos, D.M. Effect of photopolymerized glaze application on bacterial adhesion on ocular acrylic resin surfaces submitted to accelerated ageing. Letters in Applied Microbiology 2019, 68, 120–127. [Google Scholar] [CrossRef]
- dos Santos, D.M.; Goiato, M.C.; Moreno, A.; Pesqueira, A.A.; Haddad, M.F. Influence of Pigments and Opacifiers on Color Stability of an Artificially Aged Facial Silicone. Journal of Prosthodontics 2011, 20, 205–208. [Google Scholar] [CrossRef]
- Han, Y.; Zhao, Y.; Xie, C.; Powers, J.M.; Kiat-amnuay, S. Color stability of pigmented maxillofacial silicone elastomer: Effects of nano-oxides as opacifiers. Journal of Dentistry 2010, 38, e100–e105. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Powers, J.M.; Kiat-amnuay, S. Effect of opacifiers and UV absorbers on pigmented maxillofacial silicone elastomer, part 1: Color stability after artificial aging. The Journal of Prosthetic Dentistry 2013, 109, 397–401. [Google Scholar] [CrossRef]
- Koster, M.E.T.A.; Bergsma, J. Problems and coping behaviour of facial cancer patients. Social Science & Medicine 1990, 30, 569–578. [Google Scholar]
- Mohammed, M.I.; Cadd, B.; Peart, G.; Gibson, I. Augmented patient-specific facial prosthesis production using medical imaging modelling and 3D printing technologies for improved patient outcomes. Virtual and Physical Prototyping 2018, 13, 164–176. [Google Scholar] [CrossRef]
- Yap, Y.L.; Tan, Y.S.E.; Tan, H.K.J.; Peh, Z.K.; Low, X.Y.; Yeong, W.Y.; Tan, C.S.H.; Laude, A. 3D printed bio-models for medical applications. Rapid Prototyping Journal 2017, 23, 227–235. [Google Scholar] [CrossRef]
- Bos, E.J.; Scholten, T.; Song, Y.; Verlinden, J.C.; Wolff, J.; Forouzanfar, T.; Helder, M.N.; van Zuijlen, P. Developing a parametric ear model for auricular reconstruction: A new step towards patient-specific implants. Journal of Cranio-Maxillofacial Surgery 2015, 43, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Palousek, D.; Rosicky, J.; Koutny, D. Use of digital technologies for nasal prosthesis manufacturing. Prosthetics & Orthotics International 2014, 38, 171–175. [Google Scholar]
- Kincade, C.; McHutchion, L.; Wolfaardt, J. Digital design of patient-specific abutments for the retention of implant-retained facial prostheses. The Journal of Prosthetic Dentistry 2018, 120, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.J.; Singh, D. 3D printing for developing patient specific cosmetic prosthetics at the point of care. International Journal of Surgery 2020, 80, 241–242. [Google Scholar] [CrossRef] [PubMed]
- Herrero Antón de Vez, H.; Herrero Jover, J.; Silva-Vergara, C. Personalized 3D Printed Surgical Tool for Guiding the Chisel during Hump Reduction in Rhinoplasty. Plastic and Reconstructive Surgery - Global Open 2018, 6, e1668. [Google Scholar] [CrossRef]
- Choi, J.W.; Kim, M.J.; Kang, M.K.; Kim, S.C.; Jeong, W.S.; Kim, D.H.; Lee, T.H.; Koh, K.S. Clinical Application of a Patient-Specific, Three-Dimensional Printing Guide Based on Computer Simulation for Rhinoplasty. Plastic & Reconstructive Surgery 2020, 145, 365–374. [Google Scholar]
- Yadav, S.; Narayan, A.I.; Choudhry, A.; Balakrishnan, D. CAD/CAM-Assisted Auricular Prosthesis Fabrication for a Quick, Precise, and More Retentive Outcome: A Clinical Report. Journal of Prosthodontics 2017, 26, 616–621. [Google Scholar] [CrossRef]
- Unkovskiy, A.; Brom, J.; Huettig, F.; Keutel, C. Auricular Prostheses Produced by Means of Conventional and Digital Workflows: A Clinical Report on Esthetic Outcomes. The International Journal of Prosthodontics 2018, 31, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Zopf, D.A.; Mitsak, A.G.; Flanagan, C.L.; Wheeler, M.; Green, G.E.; Hollister, S.J. Computer Aided–Designed, 3-Dimensionally Printed Porous Tissue Bioscaffolds for Craniofacial Soft Tissue Reconstruction. Otolaryngology–Head and Neck Surgery 2015, 152, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Watson, J.; Hatamleh, M.M. Complete integration of technology for improved reproduction of auricular prostheses. The Journal of Prosthetic Dentistry 2014, 111, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Mussi, E.; Furferi, R.; Volpe, Y.; Facchini, F.; McGreevy, K.S.; Uccheddu, F. Ear Reconstruction Simulation: From Handcrafting to 3D Printing. Bioengineering 2019, 6, 14. [Google Scholar] [CrossRef] [PubMed]
- Jeon, B.; Lee, C.; Kim, M.; Choi, T.H.; Kim, S.; Kim, S. Fabrication of three-dimensional scan-to-print ear model for microtia reconstruction. Journal of Surgical Research 2016, 206, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Nagata, S. A New Method of Total Reconstruction of the Auricle for Microtia. Plastic and Reconstructive Surgery 1993, 92, 187–201. [Google Scholar] [CrossRef]
- Borrelli, M.; Geerling, G.; Spaniol, K.; Witt, J. Eye Socket Regeneration and Reconstruction. Current Eye Research 2020, 45, 253–264. [Google Scholar] [CrossRef]
- Puls, N.; Carluccio, D.; Batstone, M.D.; Novak, J.I. The rise of additive manufacturing for ocular and orbital prostheses: A systematic literature review. Annals of 3D Printed Medicine 2021, 4, 100036. [Google Scholar] [CrossRef]
- Kavlekar, A.; Aras, M.; Chitre, V. An innovative and simple approach to fabricate a hollow ocular prosthesis with functional lubricant reservoir: A solution to artificial eye comfort. The Journal of Indian Prosthodontic Society 2017, 17, 196. [Google Scholar] [CrossRef] [PubMed]
- Dave, T.; Tiple, S.; Vempati, S.; Palo, M.; Ali, M.; Kaliki, S.; Naik, M. Low-cost three-dimensional printed orbital template-assisted patient-specific implants for the correction of spherical orbital implant migration. Indian Journal of Ophthalmology 2018, 66, 1600. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Bai, S.; Yu, X.; Zhao, Y. Combined use of a facial scanner and an intraoral scanner to acquire a digital scan for the fabrication of an orbital prosthesis. The Journal of Prosthetic Dentistry 2019, 121, 531–534. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The illustration showing both traditional and advanced manufacture of maxillofacial prostheses. The main steps are input, processing, and output, while 3D printing demonstrating significant advances over traditional methods.
Figure 1.
The illustration showing both traditional and advanced manufacture of maxillofacial prostheses. The main steps are input, processing, and output, while 3D printing demonstrating significant advances over traditional methods.
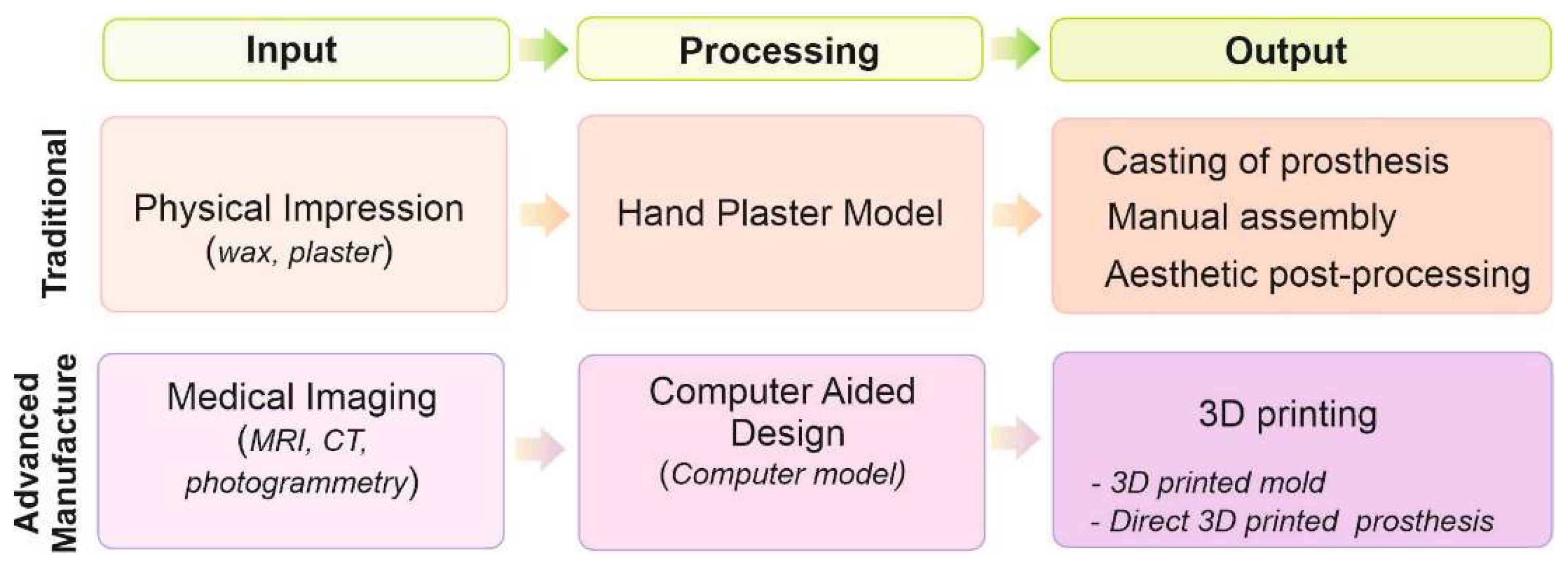
Figure 2.
Schematic illustration of the most common polymer 3D printing technologies. All techniques build up a 3D object layer-by-layer.
Figure 2.
Schematic illustration of the most common polymer 3D printing technologies. All techniques build up a 3D object layer-by-layer.
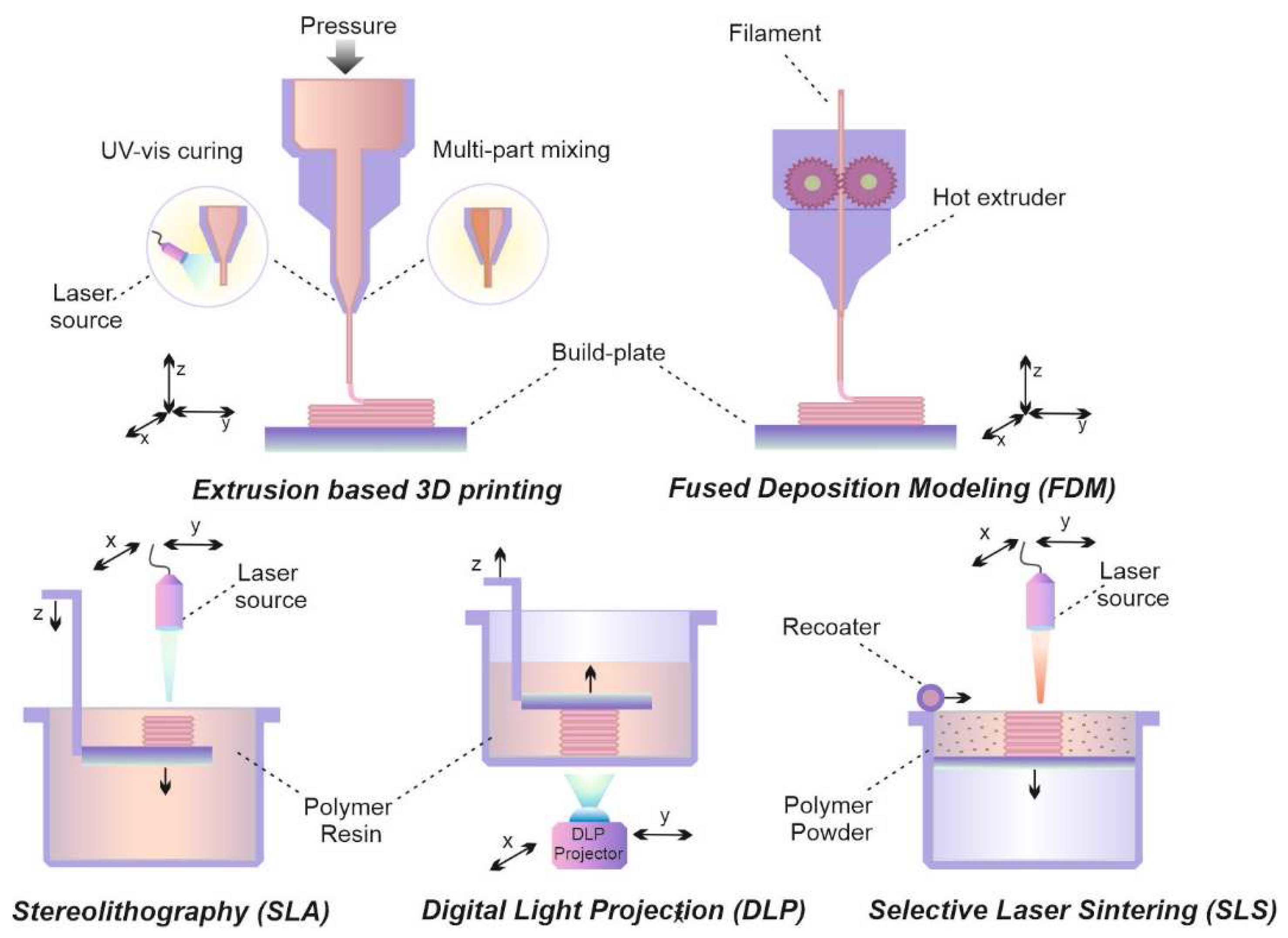
Figure 3.
Typical chain of acrylic PSA copolymer (a); General structure of silicone polymer, where polydimethylsiloxane (PDMS) contains R1=methyl (b); Structural units of MQ siloxane resin (c); Solvent-free platinum-catalyzed addition polycondensation (d).
Figure 3.
Typical chain of acrylic PSA copolymer (a); General structure of silicone polymer, where polydimethylsiloxane (PDMS) contains R1=methyl (b); Structural units of MQ siloxane resin (c); Solvent-free platinum-catalyzed addition polycondensation (d).
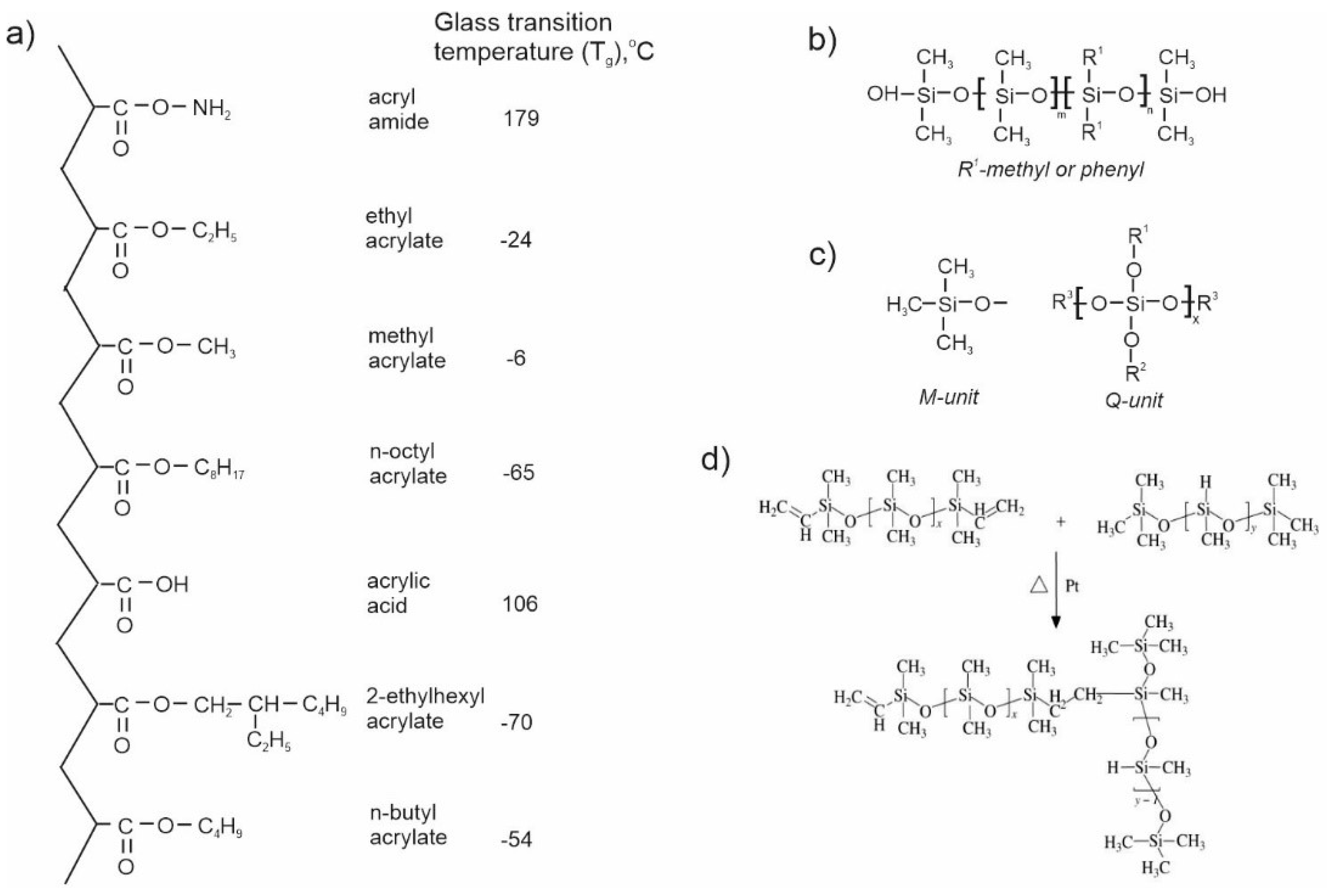

Table 1.
Desirable performance characteristics of prostheses [18].
Table 1.
Desirable performance characteristics of prostheses [18].
| Mechanical and physical properties |
Goal | Units | |
|---|---|---|---|
| min | max | ||
| Tear strength | 0.005 | 0.018 | kN/mm |
| Tensile strength | 6900 | 13800 | kPa |
| Modulus at 100% elongation | 345 | 1720 | kPa |
| Elongation at break | 400 | 800 | % |
| Glass transition temperature | less 0 | °С | |
| Heat distortion temperature | above 120 | °С | |
| Critical surface tension | 30 | 45 | mN/m |
| Coefficient of friction | 0.4 | 0.6 | none |
| Hardness | 25 | 35 | Shore A scale |
| Water absorption | None | ||
Table 2.
The most used polymers in prosthetics.
| Polymer | Description | 3D printing | Advantages | Disadvantages | Application | Ref |
| PU | Thermoset, high elastic properties | FDM, SLS, casting in 3D-printed molds | Excellent flexibility, ability to external and internal staining, fine cosmetic results | Sensitivity to moisture, limited mechanical properties | Ocular prostheses, molds, skin-like coating | [63] [64] |
| Polyacrylates | ||||||
| PMMA | Thermoplast, easy to blend, copolymerization to improve properties | FDM, SLS, casting in 3D-printed molds | low cost, lightweight, transparency, easy to manipulation | Brittle, scratched, unstable in organic solvent, limited mechanical properties | Ocular prostheses, eyeballs, surface coating, implant-supports, molds | [16] [65] |
| Photocurable resins | Acryic-based copolymer, cured by light (λ ~365nm) e.g. FotoTec DLP.A, TangoPlus |
SLA, DLP, casting in 3D-printed molds | Easy to manipulation, diversity of samples with various properties | Shrinkage, distortion, side-product under curing, fracture | Auricular, nasal, ocular prostheses, implants, molds | [65] [66] [67] |
| Adhesives | Polyalkyl acrylates with soft and hard segments, viscoelastic | - | Diversity of samples, easy tuned adhesion-cohesion, low cost | Contain solvents, insufficient wetting strength | Attachment of prostheses | [68] |
| Polyesters | ||||||
| PCL | Thermoplast, easy to blend, high strength, elasticity. | FDM, SLS, casing in 3D-printed molds | Low melting point, biodegradable, mechanically strong, easy processing, tissue regeneration | Slow biodegradation with acid release, impossibility of thermal sterilization | Implant-supports of orbital prostheses, molds | [69] [70] |
| PLA | Thermoplast, easy to blend, high strength, permeability for gases and water | FDM, SLS, casting in 3D-printed molds | Low melting point, low shrinkage, mechanically strong, easy processing | Low heat resistance, brittleness, slow biodegradation with acid release | Implant-supports of auricular prostheses, molds, mock implants | [71] [72] [73] |
| PEEK | Thermoplast, exceptional mechanical, thermal, and chemical properties, capable of blending. | FDM, SLS, | High strength, stiffness, and toughness | High melting point, high melt viscosity, moderately resistant to UV radiation, processing affects mechanical properties. | Reinforcement of auricular prostheses | [74] |
| Polystyrenes | ||||||
| PS | Thermoplast, rigid, hard, easy to blend, copolymerization to improve properties. | FDM | High dimensional stability, good processing, low water uptake and shrinkage, chemically resistant | Brittle, limited chemical resistance to organic solvents | Molds | [75] |
| ABS | Thermoplast, rigid, hard, easy to blend | SLA, FDM,SLS , binder jetting | Chemically resistant, heat tolerance, high impact strength, rigidity, high resistance to stress cracking | Poor resistance to chlorinated solvents, UV-light | Molds, mock implants | [73] [76] [77] |
| Silicones | ||||||
| Silicone RTV | Elastomer, easy to blend | Casting in 3D-printed molds, extrusion, jetting, SLA, DLP | Skin-like flexibility, heat resistance, radically low viscosity-temperature coefficients, biocompatibility, and intrinsic transparency, easy processing | Poor mechanical properties, hydrophobicity, troubles with external staining, and impurities. | All types of facial prostheses | [76] [78] [72] |
| Silicone HTV | Elastomer, easy to blend | Casting in 3D-printed molds, extrusion, jetting, SLA, DLP | Transparent, odorless polycondensation samples, have relatively high tensile and tear strength, easy processing | Volatile residues, yellowing after curing, Pt-catalyzed have a strong odor, sticky to the touch | Auricular prostheses, molds | [79] |
| Adhesives | Elastomer, viscoelastic, formed MQ resins | - | Spread and rapid, intensive surface wetting, easy tuned adhesion- cohesion, low cost | Possible damage of skin, insufficient wetting strength | Attachment of prostheses | [80] |
PU-polyurethane, PMMA-poly(methyl methacrylate), PCL – polycaprolactone, PLA – polylactide, PEEK - polyether-ether-ketone, PS – polystyrene, ABS - acrylonitrile-butadiene-styrene copolymer, ), FotoTec DLP.A - 2-hydroxyethyl methacrylate/diurethane dimethacrylate/hydroxypropyl methacrylate, TangoPlus - exo-1,7,7-trimethylbicyclo[2.2.1]hept-2-yl acrylate.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



