
Submitted:
29 August 2023
Posted:
31 August 2023
You are already at the latest version
Abstract
Feeling pain means feeling oneself, as the body feels discomfort as a kind of "disturbance experi-ence". Endometriosis is a disease in which the predominant symptom is pain felt by women pri-marily within the pelvis, but also outside of the body. The clinical biomarker used in the diagnosis of this disease is microRNAs. Treatment of endometriosis is complex and is based mainly on phar-macotherapy. Physiotherapy can complement pharmacological treatment in reducing pain using non-invasive treatments for the body. Therefore, databases have been searched to find the most effective forms of physiotherapy for the treatment of endometriosis. The literature review conducted here suggests that it is necessary to perform multicentre studies in order to establish which forms of physical therapy may be most effective in reducing pain and improving the quality of life of women suffering from endometriosis. Certainly, this type of research in conjunction with the assessment of pain and endometriosis markers would be of great clinical value in order to develop an interdisci-plinary treatment model.
Keywords:
pain
; endometriosis
; physiotherapy
1. Introduction
In the general medical sense, feeling pain means simultaneously feeling oneself, finding yourself changed in relation to the world, or more precisely, changed in the context of somatic communication with the world. In other words, the body experiences discomfort as a kind of "disturbance experience." This experience differs from the concept of disease explained from a scientific point of view. Discomfort is not yet a scientific symptom, but a signal generated in the sphere of somatics. This signal is not an object but a shift of meaning between itself and the other symptoms. "Discomfort" is a symbol of dysfunction or the inability to cope with everyday life. Discomfort is a sign of dysfunction. As such, it is highly evaluative.
Researchers at the Indiana University School of Medicine have identified several specific blood biomarkers that can help to objectively determine the severity of a patient's pain. The biomarkers MFAP3, GNG7, CNTN1, LY9, CCDC144B, and GBP1 have been shown to have the most solid empirical evidence for functional involvement in pain, and therefore can be considered as determinants of pain sensation, which allows clinicians to plan a treatment that can be characterized in a manner that is measurable [1]. The biomarkers identified are not only compatible with specific pain relievers, but can also help predict whether a patient will suffer from chronic pain in the future [1]. Biomarkers have been found that identify pain independently of gender or diagnosis. It identified those that are better predictors in men and those that are better predictors in women. CNTN1 is associated with chronic pain in women, while LY9 (lymphocyte antigen 9) and MFAP3 are associated with post-traumatic stress disorder (PTSD) in men [1].
Endometriosis is defined as the presence of endometrial tissue outside the uterus. Endometrial implants are most often found in the pelvic peritoneal cavity, on the ovaries, fallopian tubes in the rectovaginal septum, on the urinary bladder and the intestine [2-5]. In very rare cases, there are changes in the diaphragm or lungs [2,3,4,5].
This is nowadays one of the most common gynecological diseases, and can affect as much as 10-15% of all women of reproductive age and 70% of women with chronic pelvic pain [2,3,4,5]. Although it may affect as many as 176 million women around the world, we still do not know much about the disease and its causes are still being sought [2,3,4]. Most women with endometriosis report symptoms as early as puberty, and diagnosis is often delayed. Consequently, this delay may reduce their reproductive potential. Moreover, early identification and treatment of endometriosis can alleviate pain, prevent disease progression and organ damage, and preserve fertility [5].
According to the European Association of Urology, endometriosis is categorised under Internal Pelvic Pain Syndromes. The disease is often associated with negative cognitive, behavioural, sexual or emotional consequences, with symptoms that suggest lower urinary tract, sexual, bowel or gynecological dysfunction [6]. Many patients may experience pain above and beyond the endometriotic tissue [6]. Multiple mechanisms have been regarded as the cause of pain in endometriosis: nociception, inflammation and changes in how pain is processed by the peripheral and central nervous systems [7]. In a chronic condition such as endometriosis, the pain from the disease is often associated with psychological stress and fatigue, which can magnify the pain [7]. This has a negative impact on sexual health, becoming a cause of dyspareunia (painful intercourse), which also impacts on relationships between partners. Dyspareunia is defined as tenderness felt during sexual intercourse without coexisting shrinkage of vulva or vagina. It is a common sexual disorder in women, and can be caused by endometriosis.
Specific microRNA is a potential biomarker of endometriosis [8,9,10,11]. Recent studies have shown that microRNAs and their targeted microRNAs have a different expression in women suffering from endometriosis than in healthy women [8,9,10,11]. MicroRNA controls a wide spectrum of normal and pathological cellular functions and, according to researchers, may play a key role in the pathogenesis of this disease [8,9,10,11]. However, the usefulness of microRNA biomarkers in detecting endometriosis is still uncertain [12], and the search for a biomarker or set of biomarkers remains open.
So far, no optimal way to diagnose endometriosis has been found, nor is there a single effective method for a full recovery. The main symptom influencing the quality of life of women with endometriosis is their perception of pain [13,14] and pharmacological treatment is the dominant treatment in endometriosis, which also aims to reduce pain [15,16,17,18,19]. In justified situations, surgery is the treatment of choice [20,21,22].
There is no single interdisciplinary treatment algorithm for endometriosis accepted among medical specialists, physiotherapists and midwives, therefore the authors would like to draw attention to the use of physiotherapy in the treatment of endometriosis, which could be an effective complementary treatment method for reducing pain sensations and thus improving the women’s quality of life.
2. Materials and Methods
In the article, the authors consider the use of physiotherapy as a means of reducing the aspect of pain in endometriosis, and analyze this aspect on the basis of the available literature. Two independent reviewers have searched medical and public databases such as PubMed, Scopus and PEDro using search terms and MeSH such as endometriosis, pain, physiotherapy, physical activity, marker miRNA. Subsequently, the data obtained after the queries were then evaluated with regard to the titles in order to remove works with other keywords.
The inclusion and exclusion criterion was an article published in a peer-reviewed journal, limited as to the scope of the publication year 2020-2022. Another restriction was that it had to be an English-language publication. Failure to meet the inclusion criterion was treated as exclusion from the analysis. A review of journal databases was carried out between September and October 2022.
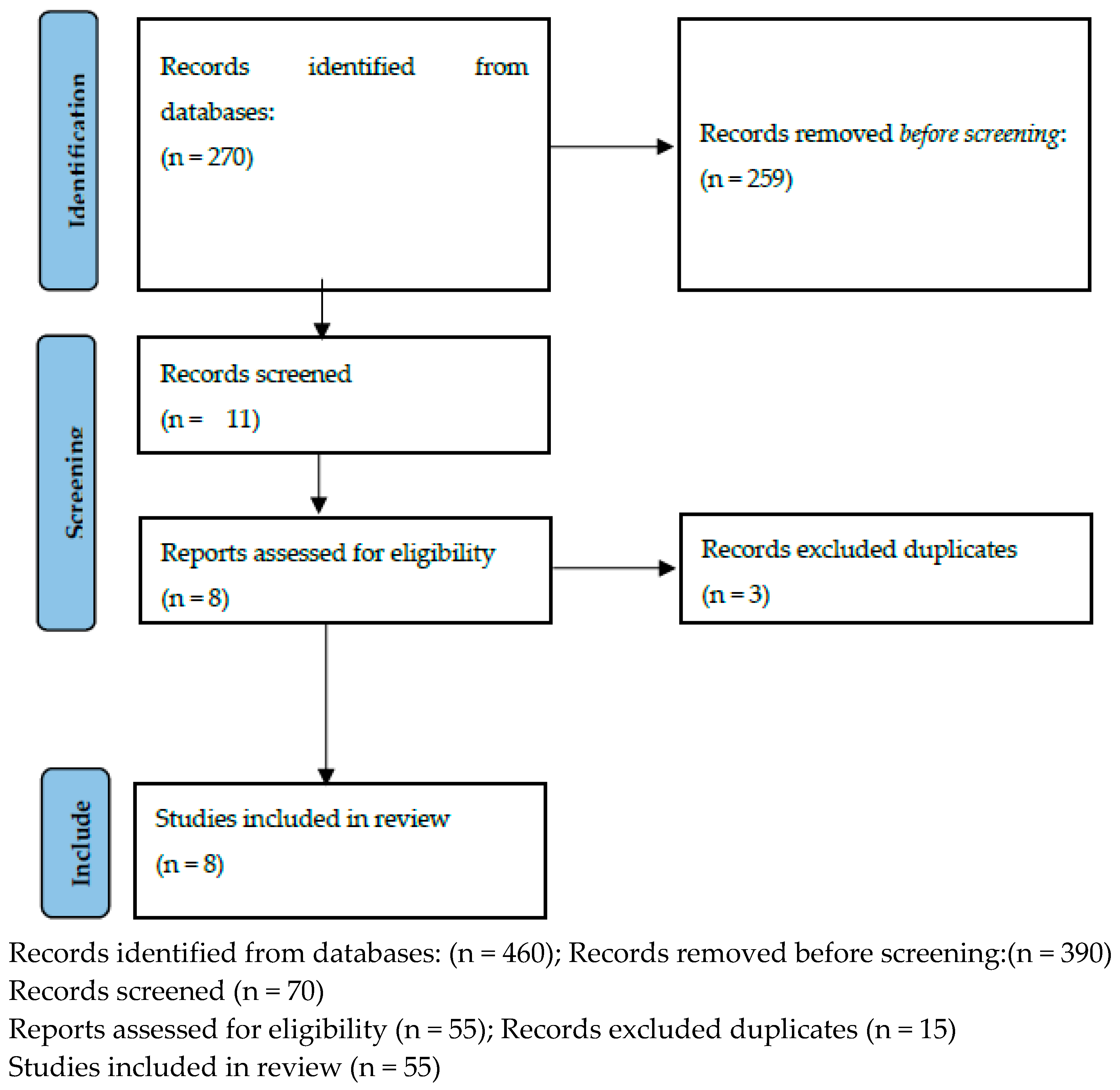
These records were then assessed for compliance with the inclusion and exclusion criteria on the basis of abstract analysis. Of the 270 articles initially shortlisted for further analysis, 259 were rejected at this stage. The 11 remaining articles were subjected to content analysis and a further 3 were rejected on the basis of further analysis due to duplication. The remaining 8 articles were subjected to further analysis (Figure 1).
All the articles collected were analysed in terms of the following parameters/content: which form/measure/physiotherapy modality was used in the treatment of endometriosis to reduce pain, what conclusion was obtained as a result of the review, and whether there was an assessment of a biomarker used for diagnosing endometriosis (to infer whether the form/measure/physiotherapy used affects the course of endometriosis).
3. Physiotherapy
The use of physical factors, physical activity and complex therapies to reduce pain in women with endometriosis.
3.1. Exercise
Hansen et al. (2021) reviewed articles to check whether exercise has an effect on pain reduction in women with endometriosis. Based on their review, the authors concluded that exercise does not have a positive effect on pain and suggested that randomised trials with correctly calculated power, well-defined study groups and training programmes should be conducted to answer the question of whether exercise can alleviate pain in patients with endometriosis. The articles reviewed did not determine the marker microRNA [23]. In this article, the literature list consisted of 27 publications [23] (Table 1).
Tennford et al. (2021) also reviewed the impact of exercise and physical activity. The authors were unable to conclude that exercise and physical activity have an effect on pain reduction in endometrial patients. Moreover, they believe that these subjects require studies with a well-designed methodology, using reliable and validated tools [24]. This article did not determine an microRNA marker either. The literature list comprised 40 items [24] (Table 1).
3.2. Balneotherapy
Habek et al. point to the use of balneoclimatology in gynaecological diseases in their review published in 2021. The authors point out that in endometriosis, the use of balneotherapy and hyperthermic hydrotherapy is contraindicated, due to the strong congestion effect following these treatments [25]. The review did not show that a microRNA marker was determined. The literature list totalled 36 entries [25] (Table 1).
3.3. Treatment recommendations for the management of persistent pelvic pain
Mardon et al. provided treatment recommendations for persistent pelvic pain in their 2022 Puliked review. The literature review provided information that the most commonly recommended treatments including for women with endometriosis are surgical treatment, pharmacotherapy, psychological care and physiotehrapy. The authors indicate that there is currently no consensus on what should be recommended in clinical practice for persistent pelvic pain [26]. The review did not identify microRNA. In their publication, the authors referred to 69 items from the literature [26] (Table 1).
3.4. Myofascial trigger points, visceral manual therapy
In a review published in 2022, Goździewicz et al. highlight the use of physiotherapy in the form of working with myofascial trigger points and visceral manual therapy to reduce symptoms of endometriosis disease. The authors also note prospective studies relating to surgical treatment and visceral therapy in endometriosis patients [27]. The review did not report the determination of a microRNA marker. The authors referred to 44 items from the literature [27] (Table 1).
3.5. TENS - Transcutaneous Electrical Nerve Stimulation
Mira et al. (2020) conducted a study to evaluate the clinical effectiveness of TENS (Transcutaneous Electrical Nerve Stimulation) versus standard hormone-only treatment for DIE (Deep Infiltrating Endometriosis) [28]. Only in the group in which TENS electrostimulation was performed was a reduction in CPP (Chronic Pelvic Pain) observed, with with a statistically significant improvement in the FSFI (Female Sexual Function Index) score also being found, with regard to sexual function. In terms of profound dyspareunia, improvements were observed in both groups. Considering secondary outcomes, a higher post-treatment total score for the EHP-30 (Endometriosis Health Profile) was observed in both groups [28] (Table 1). Pizyxane results indicate that TENS eletrostimulation is a good method for reducing CPP pain and deep dyspareunia, thereby improving women's quality of life and sexual function [28]. In this study, no assessment was made of the levels of the endometriosis biomarker microRNA.
3.6. Pelvic Floor Physiotherapy - Pelvic Floor Muscle Physiotherapy
Del Forno et al. (2021) conducted a study among women with Deep Infiltrating Endometriosis (DIE), who had chronic pelvic pain, dyspareunia and pelvic floor muscle hypertonia. The aim of the study was to assess PFP (Pelvic Floor Physiotherapy) and how it affects the area of levator ani muscle occlusion during the Valsalva manoeuvre, which was assessed by transabdominal ultrasonography, in women with DIE suffering from superficial dyspareunia [29]. Before and after the physiotherapy sessions, the participants of the study underwent a 3D/4D transperineal ultrasound. The study women had individual PFP sessions by a qualified physiotherapist. The results indicated that there was a marked reduction in pelvic pain in the group in which PFP was performed, thus achieving pelvic floor muscle relaxation [29] (Table 1). The microRNA marker was not assessed in this study.
3.7. Physio-EndEA’ Study
Del Salinas-Asensio et al. (2022) conducted a study called 'Physio-EndEA' on the Health-Related Quality of Life (HRQoL) of women with symptomatic endometriosis. Its was designed to check what benefits may occur using a therapy exercise programme (focused on lumbo-pelvic stabilisation and exercise tolerance). The 'Physio-EndEA' programme consisted of a one-week lumbo-pelvic stabilisation learning phase, followed by an eight-week phase of stretching, aerobic and resistance exercises focused on the lumbo-pelvic area, which included sequential instruction and supervision by a trained physiotherapist (with a progression of volume and intensity), with exercises adjusted daily according to the woman's needs and each participant's capabilities [30]. The following were also assessed: pain levels, muscle thickness and strength and flexibility, body balance and cardiorespiratory fitness) and outcomes described by the participants (pain intensity, physical fitness, chronic fatigue, sexual function, gastrointestinal function and sleep quality). The 'Physio-EndEA' programme has a positive effect on HRQoL in women with endometriosis [30] (Table 1). The microRNA marker was not determined in this study either.

Table 1.
Physiotherapy (types/forms) used in endometriosis.
| Study | Treatments | Conclusion | Marker assessment (microRNA) |
|---|---|---|---|
| Hansen et al., 2021 [23] | Exercise | Exercise has no positive effect on pain. The authors suggest that randomised trials with properly calculated power, well-defined study groups and training programmes should be conducted. | No |
| Tennford et al., 2021 [24] | Exercise Physical therapy |
Exercise and physical activity have no effect on pain reduction in endometritis patients. The authors also believe that the topic requires a study with a well-designed methodology, using reliable and validated tools. | No |
| Habek et al., 2021 [25] | Balneotherapy | The use of balneotherapy and hyperthermic hydrotherapy in endometriosis is contraindicated. | No |
| Mardon et al., 2022 [26] | Surgical treatment, pharmacotherapy, psychological care, physiotherapy | The most commonly recommended treatment including that for women with endometriosis is surgery, pharmacotherapy, psychological care and physiotherapy. The authors indicate that there is currently no consensus on what should be recommended in clinical practice for persistent pelvic pain. | No |
| Goździewicz et al., 2022 [27] | Myofascial trigger points, visceral manual therapy | The importance of using physiotherapy in the form of working with myofascial trigger points and visceral manual therapy to reduce symptoms of endometriosis disease. The authors note prospective studies in relation to surgical treatment and visceral therapy in patients with endometriosis. | No |
| Mira et al., 2020 [28] | TENS Applied TENS and hormonal therapy for 8 weeks at the S3–S4 region, 30 minutes session. Included a hundred-one participants with DIE in electrotherapy (n=53) (hormonal treatment + electrotherapy) or control group (n=48) (only hormonal treatment) by 8 weeks of follow-up. The primary measurement was chronic pelvic pain (CPP) using a visual analogue scale (VAS) and deep dyspareunia. The secondary outcomes were the quality of life by endometriosis health profile (EHP-30) and sexual function by female sexual function index (FSFI). |
Alleviation of CPP was observed only in the electrotherapy group. In terms of profound dyspareunia, improvement was observed for both groups. Considering the secondary outcomes, a higher post-treatment total score for EHP-30 was observed in both groups.With regard to sexual function, a statistically significant improvement in the FSFI score was observed in the electrotherapy group, with an increase in scores in the domains of lube and pain. | No |
| Del Forno et al., 2021 [29] | Pelvic Floor Muscle Physiotherapy Before the start of therapy, the participants received information on pelvic floor anatomy and function, with the help of anatomical illustrations. In addition, the physiotherapist, experienced in pelvic floor muscle dysfunction, performed a digital evaluation of the pelvic floor muscle tone. This was performed after the TPU, given that digital examination may induce pain with consequent contraction of the pelvic floor, which could affect the LHA assessment. Pubococcygeus and ischiococcygeus muscle tone were assessed bilaterally at rest, and during pelvic floor contraction and relaxation. After the first examination, the women in the study group underwent five individual sessions of PFP, of 30 min each, on weeks 1, 3, 5, 8 and 11. In each session, the women underwent a Thiele massage, which consists of digital pressure and subsequent stretching of the muscles in order to relax them, restoring normal pelvic floor tone and the ability to coordinate muscle behavior. Participants were assigned randomly to no intervention (control group) or to receive PFP sessions (study group) in a 1:1 ratio. Block randomization was computer generated and the allocation was hidden in opaque envelopes until randomized. following inclusion criteria: age between 18 and 45 years, clinical and ultrasound diagnosis of DIE and associated superficial dyspareunia. Exclusion criteria included previous or current genital malignancy, pelvic organ prolapse, previous surgery for DIE, current or previous pregnancy, congenital or acquired abnormalities of the pelvis or pelvic floor, history of sexual abuse, current genitourinary infection and presence of other causes of CPP; written informed consent was obtained from all participating women. Four months after randomization, all participants underwent a second examination, in which they were asked to rank again their endometriosis-related pain symptoms and underwent another 3D/4D-TPU assessment of the LHA at rest, on maximum PFMC and on maximum Valsalva maneuver. In addition, the women in the study group were asked to rate their satisfaction with their physiotherapy treatment using a 5-item scale (1, very dissatisfied; 2, dissatisfied; 3, neither satisfied nor dissatisfied; 4, satisfied; and 5, very satisfied). |
In conclusion PFP seems to be effective in improving pelvic floor muscle relaxation, superficial dyspareunia and CPP in women with DIE. As such, the studied physiotherapy protocol may improve patients’ quality of life and sexual life, which are often compromised in women with DIE11,43. 3D/4D-TPU is a reliable, objective and non-invasive method for assessing the pelvic floor muscles in these women. In the current context of tailored, multidisciplinary care40, PFP may represent an additional valid, minimally invasive, innovative and well-tolerated therapeutic option for women with DIE, particularly those with superficial dyspareunia and CPP. | No |
| del Mar Salinas-Asensio et al., 2022 [30] | Physio-EndEA’ Study A total of 22 symptomatic endometriosis women will be randomized 1:1 to the Physio-EndEA or usual care groups. The Physio-EndEA’ program consist of a one-week lumbopelvic stabilization learning phase followed by an eight-week phase of stretching, aerobic and resistance exercises focused on the lumbopelvic area that will be sequentially instructed and supervised by a trained physiotherapist (with volume and intensity progression) and adapted daily to the potential of each participant. The primary outcome measure is HRQoL. The secondary outcome measures included clinician-reported outcomes (pressure pain thresholds, muscle thickness and strength, flexibility, body balance and cardiorespiratory fitness) and patient-reported outcomes (pain intensity, physical fitness, chronic fatigue, sexual function, gastrointestinal function and sleep quality). |
The establishment of this type of intervention could benefit the HRQoL of symptomatic women with endometriosis. Moreover, it might reduce the direct and indirect costs of this health problem. | No |
4. Discussion
Despite the high incidence of endometriosis in women, the review indicates that physiotherapy is not widely used in the management of pain in women with endometriosis. Exercise and physical activity were most commonly used, but these have not been shown to be effective in reducing pain in endometriosis [23,24].
The Pelvic Floor Physiotherapy and the Physio-EndEA' Study is worth noting. These studies showed the positive effects of exercising selected pelvic floor and trunk muscles [29,30]. Performing exercises for the muscles of the pelvic floor and trunk requires a thorough discussion with a physiotherapist on this should be done; certainly, supervision by a physiotherapist during exercise is important - it allows the woman’s starting position to be corrected during exercise. Furthermore, it should be noted that the effectiveness of the exercises is related to their regular implementation [29,30] .
Baneoclimatology can be a good form of complementary treatment in gynaecological diseases, but in the case of endometriosis its use is contraindicated, due to the deep congestion effect achieved [25].
In physiotherapy, musculo-fascial therapy, which includes the deactivation of myofascial trigger points, is significant [27]. This therapy is also used in gynaecological physiotherapy, achieving an improvement in women's pelvic pain experience [31].
In physiotherapy clinical practice, the use of visceral manual therapy is noteworthy [32,33]. However, despite patients reporting improvements after its use, the efficacy of visceral manual therapy needs to be confirmed based on research, with a well-designed methodology.
When carefully instructed by a physiotherapist, TENS electrostimulation can be performed by the woman at home, which will translate into more regular treatments [28]. This is possible due to the availability of a small and therefore lightweight device, while newer devices also have a preloaded programme for TENS electrostimulation [28] .The most common treatment for women with endometriosis is surgical and pharmacological treatment [26].
Depending on the surgical technique selected, surgical treatment leaves a scar in and on the patient's body, which also requires physiotherapy intervention by mobilising it [34,35]. Pre- and postoperative physiotherapy to prepare the woman's musculoskeletal system to function after surgery should, of course, be kept in mind [36].
Despite their widespread use for pelvic pain caused by endometriosis, there is a lack of evidence of the efficacy of NSAIDs [37]. The surgical treatment used is challenging and still debatable as pain relief after removal of endometrial tissue has not been demonstrated [6,38,39]. It has been suggested that vitamin C and E should be supplemented in women with endometriosis I norder to reduce oxidative stress and pelvic pain sensations [40] .It is thought that noninvasive biomarkers, proteomics, genomics, and miRNA microarray could be very useful in diagnosing endometriosis. However, this requires further research involving large study groups, along with a better understanding of the pathophysiological mechanisms [41]. During endometriosis, due to chronic pelvic pain, women often experience an unfavourable psychological state, depressive states, anxiety symptoms and psychosomatic disorders [42] .In the reviews presented here, physiotherapy in the form of treatments, e.g., magnetotherapy, electrotherapy, light therapy, laser therapy as complementary treatment for women with endometriosis seems to be highly underestimated [28, 43-47]. The clinically used endometriosis marker microRNA [8-11] is not used by physiotherapists, which is certainly due to their professional competence. Nevertheless, controlling the treatment by determining this marker would allow the effectiveness of the physiotherapeutic interventions used to be monitored. Due to the complexity of this disease, the treatment of women with endometriosis should be an interdisciplinary treatment involving close cooperation between gynaecologists and physiotherapists.
In view of the high cost of treatment in each country, it is certainly the case that non-pharmacological methods/procedures to reduce pain among women with endometriosis and thus physiotherapeutic methods/procedures to improve the quality of life of women can be a good solution for the economics of medical care but especially for the affected women. Physiotherapy methods/symptoms are also non-invasive treatment procedures and the authors therefore emphasise their signifance for practical application.
5. Conclusion
The literature review conducted here suggests that it is necessary to carry out multicentre studies in order to ascertain which forms of physiotherapy may be most effective in reducing pain and improving the quality of life of women suffering from endometriosis.
It would certainly be useful to conduct multi-centre studies in different countries to prepare a treatment algorithm for women with endometriosis. Without doubt, this type of research in conjunction with the assessment of pain and endometriosis markers would be of great clinical value for developing an interdisciplinary treatment model. It might be the case that the failure to determine microRNA marker levels in publications demonstrating physiotherapy interventions was due to limited research funding.
Author Contributions
conceptualization, M.W. and K.P.; methodology, M.W. and K.P.; resources, M.W. and K.P.; writing—original draft preparation, M.W.; K.P.; M.D.; T.G.; M.P-K.; D.W.; K.P-R.; W.K.; and G.J.B.; writing—review and editing, M.W.; K.P.; M.D.; T.G.; M.P-K.; D.W.; K.P-R.; W.K.; and G.J.B.; visualization, M.W.; M.D.; K.P.; T.G.; and G.J.B.; supervision, M.W.; M.D.; K.P.; T.G.; and G.J.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive any specific grant from any funding agencies in the public, commercial or not-for-profit sectors.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Niculescu, A.B.; Le-Niculescu, H.; Levey, D.F.; Roseberry, K.; Soe, K.C.; Rogers, J. White, F. A. Towards precision medicine for pain: diagnostic biomarkers and repurposed drugs. Molecular psychiatry. 2019, 24, 501–522. [Google Scholar] [CrossRef] [PubMed]
- Mehedintu, C.; Plotogea, M.N.; Ionescu, S.; Antonovici, M. Endometriosis still a challenge. Journal of Medicine and Life. 2014, 7, 349–357. [Google Scholar] [PubMed]
- Greene, A.D.; Lang, S.A.; Kendziorski, J.A.; Sroga-Rios, J.M.; Herzog, T.J.; Burns, K.A. Endometriosis: Where are We and Where are We Going? Reproduction. 2016, 152, R63–R78. [Google Scholar] [CrossRef] [PubMed]
- Giudice, L.C. Clinical practice. Endometriosis. N Engl J Med. 2010, 362, 2389–98. [Google Scholar] [CrossRef] [PubMed]
- Dun, E.C.; Kho, K.A.; Morozov, V.V.; Kearney, S.; Zurawin, J.L.; Nezhat, C.H. Endometriosis in adolescents. Journal of the Society of Laparoendoscopic Surgeons. 2015, 19, e2015.00019. [Google Scholar] [CrossRef]
- Engeler, D.; Baranowski, A.P.; Borovicka, J.; Cottrell, A.M.; Dinis-Oliveira, P.; Elneil, S.; Hughes, J.; Messelink, E.J.; de C Williams, A.C. Guidelines Associates: Goonewardene, S.; Schneider, M.P. EAU Guidelines on Chronic Pelvic Pain. 2017. [Google Scholar]
- Morotti, M.; Vincent, K.; Becker, Ch.M. Mechanisms of pain in endometriosis. Eur J Obstet Gynecol Reprod Biol. 2017, 209, 8–13. [Google Scholar] [CrossRef]
- Ahn, S.H.; Singh, V.; Tayade, C. Fertil Steril Biomarkers in endometriosis: challenges and opportunities. Fertil Steril. 2017, 107, 523–532. [Google Scholar] [CrossRef]
- Bjorkman, S.; Taylor, H.S. MicroRNAs in endometriosis: biological function and emerging biomarker candidates†. Biol Reprod. 2019, 100, 1135–1146. [Google Scholar] [CrossRef]
- Wang, J.; Cong, S.; Wu, H.; He, Y.; Liu, X.; Sun, L.; Zhao, X.; Zhang, G. Identification and Analysis of Potential Autophagy-Related Biomarkers in Endometriosis by WGCNA. Front Mol Biosci. 2021, 8, 743012. [Google Scholar] [CrossRef]
- Jiang, L.; Zhang, M.; Wu, J.; Wang, S.; Yang, X.; Yi, M.; Zhang, X.; Fang, X. Exploring diagnostic m6A regulators in endometriosis. Aging (Albany NY). 2020, 12, 25916–25938. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, L.M.; Ferreira, M.C.; Rocha, A.L.L.; Carneiro, M.M.; Reis, F.M. New biomarkers in endometriosis. Adv Clin Chem. 2019, 89, 59–77. [Google Scholar] [PubMed]
- Saunders, P.T.K.; Horne, A.W. Endometriosis: Etiology, pathobiology, and therapeutic prospects. Cell. 2021, 27, 2807–2824. [Google Scholar] [CrossRef] [PubMed]
- As-Sanie, S.; Black, R.; Giudice, L.C.; Gray Valbrun, T.; Gupta, J.; Jones, B.; Laufer, M.R.; Milspaw, A.T.; Missmer, S.A.; Norman, A.; Taylor, R.N.; Wallace, K.; Williams, Z.; Yong, P.J.; Nebel, R.A. Assessing research gaps and unmet needs in endometriosis. Am J Obstet Gynecol. 2019, 221, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Buggio, L.; Dridi, D.; Barbara, G.; Merli, C.E.M.; Cetera, G.E. Vercellini P.Novel pharmacological therapies for the treatment of endometriosis. Expert Rev Clin Pharmacol. 2022, 15, 1039–1052. [Google Scholar] [CrossRef]
- Zajec, V.; Mikuš, M.; Vitale, S.G.; D'alterio, M.N.; Gregov, M.; Šarić, M.J.; Carugno, J.; Angioni, S.; Ćorić, M. Current status and challenges of drug development for hormonal treatment of endometriosis: a systematic review of randomized control trials. Gynecol Endocrinol. 2022, 38, 713–720. [Google Scholar] [CrossRef]
- Linzagolix: a new GnRH-antagonist under investigation for the treatment of endometriosis and uterine myomas. Dababou S, Garzon S, Laganà AS, Ferrero S, Evangelisti G, Noventa M, D'Alterio MN, Palomba S, Uccella S, Franchi M, Barra F. Expert Opin Investig Drugs. 2021, 30, 903–911. [CrossRef]
- Donnez, J.; Dolmans, M.M. GnRH Antagonists with or without Add-Back Therapy: A New Alternative in the Management of Endometriosis? Int J Mol Sci. 2021, 22, 11342. [Google Scholar] [CrossRef]
- Legendre, G.; Delbos, L.; Hudon, E.; Chabbert-Buffet, N.; Geoffron, S.; Sauvan, M.; Fernandez, H.; Bouet, P.E.; Descamps, P. New medical treatments for painful endometriosis: CNGOF-HAS Endometriosis Guidelines. Gynecol Obstet Fertil Senol. 2018, 46, 256–263. [Google Scholar]
- Kho, R.M.; Andres, M.P.; Borrelli, G.M.; Neto, J.S.; Zanluchi, A.; Abrão, M.S. Surgical treatment of different types of endometriosis: Comparison of major society guidelines and preferred clinical algorithms. Best Pract Res Clin Obstet Gynaecol. 2018, 51, 102–110. [Google Scholar] [CrossRef]
- Rolla, E. Endometriosis: advances and controversies in classification, pathogenesis, diagnosis, and treatment. F1000 Res. 2019, 8, F1000. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, M.; Gibbons, T.; Armour, M.; Wang, R.; Glanville, E.; Hodgson, R.; Cave, A.E.; Ong, J.; Tong, Y.Y.F.; Jacobson, T.Z.; Mol, B.W.; Johnson, N.P.; Condous, G. When to Do Surgery and When Not to Do Surgery for Endometriosis: A Systematic Review and Meta-analysis. J Minim Invasive Gynecol. 2020, 27, 390–407. [Google Scholar] [CrossRef] [PubMed]
- Hansen, S.; Sverrisdóttir, U.A.; Rudnicki, M. Impact of exercise on pain perception in women with endometriosis: A systematic review. Acta Obstet Gynecol Scand. 2021, 100, 1595–1601. [Google Scholar] [CrossRef] [PubMed]
- Tennford, M.K.; Gabrielsen, R.; Tellum, T. Efect of physical activity and exercise on endometriosis-associated symptoms: a systematic review. BMC Women’s Health. 2021, 21, 355. [Google Scholar]
- Habek, D.; Cerovac, A.; Kamerić, L.; Nevačinović, E.; Šerak, A. Balneogynaecology in the 21st century: increasingly recommended primary and complementary treatment of chronic gynaecological diseases. Med Glas (Zenica). 2021, 18, 1–6. [Google Scholar]
- Mardon, A.K.; Leake, H.B.; Szeto, I.K.; Astill, T.; Hilton, S.; Moseley, G.L.; Chalmers, K.J. Treatment recommendations for the management of persistent pelvic pain: a systematic review of international clinical practice guidelines. BJOG. 2022, 129, 1248–1260. [Google Scholar] [CrossRef]
- Goździewicz, T.; Jarzabek-Bielecka, G.; Luwanski, D.; Wójcik, M.; Plagens-Rotman, K.; Mizgier, M.; Pisarska-Krawczyk, M.; Kędzia, W. The Role of Visceral Therapy in the Sexual Health of Women with Endometriosis during the COVID-19 Pandemic: A Literature Review. J. Clin. Med. 2022, 11, 5825. [Google Scholar] [CrossRef]
- Mira, T.A.A.; Yela, D.A.; Podgaec, S.; Baracat, E.C.; Benetti-Pinto, C.L. Hormonal treatment isolated versus hormonal treatment associated with electrotherapy for pelvic pain control in deep endometriosis: Randomized clinical trial. Eur. J. Obstet Gyneacol. Reprod. Biol . 2020, 255, 134–141. [Google Scholar] [CrossRef]
- Del Forno, S.; Arena, A.; Pellizzone, V.; Lenzi, J.; Raimondo, D.; Cocchi, L.; Paradisi, R.; Youssef, A.; Casadio, P.; Seracchioli, R. Assessment of levator hiatal area using 3D/4D transperineal ultrasound in women with deep infiltrating endometriosis and superficial dyspareunia treated with pelvic floor muscle physiotherapy: randomized controlled trial. Ultrasound Obstet Gynecol. 2021, 57, 726–732. [Google Scholar] [CrossRef]
- Del Mar Salinas-Asensio, M.; Ocón-Hernández, O.; Mundo-López, A.; Fernández-Lao, C.; Peinado, F.M.; Padilla-Vinuesa, C.; Álvarez-Salvago, F.; Postigo-Martín, P.; Lozano-Lozano, M.; Lara-Ramos, A.; Arroyo-Morales, M.; Cantarero-Villanueva, I.; Artacho-Cordón, F. 'Physio-EndEA' Study: A Randomized, Parallel-Group Controlled Trial to Evaluate the Effect of a Supervised and Adapted Therapeutic Exercise Program to Improve Quality of Life in Symptomatic Women Diagnosed with Endometriosis. Int J Environ Res Public Health. 2022, 19, 1738. [Google Scholar] [CrossRef]
- Ross, V.; Detterman, C.; Hallisey, A. Myofascial Pelvic Pain: An Overlooked and Treatable Cause of Chronic Pelvic Pain. J Midwifery Womens Health. 2021, 66, 148–160. [Google Scholar] [CrossRef] [PubMed]
- Stone, C.; Williams, A. Visceral and Obstetric Osteopathy; Churchill Livingstone: London, UK, 2007. [Google Scholar]
- Barral, J.P.; Mercier, P. Visceral Manipulation; Eastland Press: Seattle, WA, USA, 1988. [Google Scholar]
- Anthonissen, M.; Daly, D.; Janssens, T.; Van den Kerckhove, E. The effects of conservative treatments on burn scars: A systematic review. Burns. 2016, 42, 508–18. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.S.; Jeon, J.H.; Hong, A.; Yang, H.T.; Yim, H.; Cho, Y.S.; Kim, D.H.; Hur, J.; Kim, J.H.; Chun, W.; Lee, B.C.; Seo, C.H. The effect of burn rehabilitation massage therapy on hypertrophic scar after burn: a randomized controlled trial. Burns. 2014, 40, 1513–20. [Google Scholar] [CrossRef] [PubMed]
- Boden, I.; Sullivan, K.; Hackett, C.; Winzer, B.; Lane, R.; McKinnon, M.; Robertson, I. ICEAGE (Incidence of Complications following Emergency Abdominal surgery: Get Exercising): study protocol of a pragmatic, multicentre, randomised controlled trial testing physiotherapy for the prevention of complications and improved physical recovery after emergency abdominal surgery. World J Emerg Surg. 2018, 13, 29. [Google Scholar]
- Brown, J.; Crawford, T.J.; Allen, C.; Hopewell, S.; Prentice, A. Nonsteroidal anti-inflammatory drugs for pain in women with endometriosis. Cochrane Database Syst Rev. 2017, 23, 1–CD004753. [Google Scholar] [CrossRef]
- Jarrell, J.; Brant, R.; Leung, W.; Taenzer, P. Women's Pain Experience Predicts Future Surgery for Pain Associated With Endometriosis. J Obstet Gynaecol Can. 2007, 29, 988–991. [Google Scholar] [CrossRef]
- Jarrell, J.; Mohindra, R.; Ross, S.; Taenzer, P.; Brant, R. Laparoscopy and reported pain among patients with endometriosis. J Obstet Gynaecol Can. 2005, 27, 477–85. [Google Scholar] [CrossRef]
- Amini, L.; Chekini, R.; Nateghi, M.R.; Haghani, H.; Jamialahmadi, T.; Sathyapalan, T.; Sahebkar, A. The Effect of Combined Vitamin C and Vitamin E Supplementation on Oxidative Stress Markers in Women with Endometriosis: A Randomized, Triple-Blind Placebo-Controlled Clinical Trial. Pain Res Manag. 2021, 5529741. [Google Scholar] [CrossRef]
- Anastasiu, C.V.; Moga, M.A.; Neculau, A.E.; Bălan, A.; Scârneciu, I.; Dragomir, R.M.; Dull, A.M.; Chicea, L.M. Biomarkers for the Noninvasive Diagnosis of Endometriosis: State of the Art and Future Perspectives. Int J Mol Sci. 2020, 21, 1750. [Google Scholar] [CrossRef]
- Shcherbina, N.A.; Potapova, L.V.; Shcherbina, I.N.; Lipko, O.P.; Mertsalova, O.V.; Chekhunova, A.A. Modern methods of complex correction of psychosomatic disorders in patients with external genital endometriosis. Wiad Lek. 2020, 73, 2623–2626. [Google Scholar] [CrossRef]
- Thabet, A.A.E.; Alshehri, M.A. Effect of Pulsed High-Intensity Laser Therapy on Pain, Adhesions, and Quality of Life in Women Having Endometriosis: A Randomized Controlled Trial. Photomed Laser Surg. 2018, 36, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Mira, T.A.; Giraldo, P.C.; Yeala, D.A.; Benetti- Pinto, C. Effectiveness of complementary pain treatment for women with deep endometriosis through Transcutaneous Electrical Nerve Stimulation (TENS): randomized controlled trial. Eur. J. Obstet Gyneacol. Reprod. Biol. 2015, 194, 1–6. [Google Scholar] [CrossRef]
- Zhang, Z.Y.; Wang, J.; Fan, Y.L.; Wang, B.Y.; Zhang, W.T. Effectiveness of neuromuscular electrical stimulation for endometriosis-related pain: A protocol of systematic review and meta-analysis. Medicine (Baltimore). 2020, 99, e20483. [Google Scholar] [CrossRef] [PubMed]
- de Mira, T.A.A.; Yela, D.A.; Podgaec, S.; Baracat, E.C.; Benetti-Pinto, C.L. Reply to Letter to the Editor entitled Re: Hormonal treatment isolated versus hormonal treatment associated with electrotherapy for pelvic pain control in deep endometriosis: Randomized clinical trial. Eur J Obstet Gynecol Reprod Biol. 2021, 258, 463–464. [Google Scholar] [CrossRef]
- Jorgensen, W.A.; Frome, B.M.; Wallach, C. Electrochemical therapy of pelvic pain: effects of pulsed electromagnetic fields (PEMF) on tissue trauma. Eur J Surg Suppl. 1994, 574, 83–6. [Google Scholar]
Figure 1.
Diagram of the systematic literature review (n—number of records).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



