Submitted:
30 August 2023
Posted:
31 August 2023
You are already at the latest version
Abstract
Background: The oldest old people (≥ 85 years) represent the fastest growing age group in Western populations. Knowledge on early outcomes of acute ischemic stroke (AIS) in very old female patients remains limited. Methods: We assessed gender differences and female-specific clinical data and in-hospital mortality in very old patients with AIS. Acute cerebral infarction was diagnosed in 506 very old female patients from a total of 4,600 acute cerebrovascular infarctions available in an ongoing 24-year hospital stroke data bank. A comparative analysis of vital status at discharge (alive versus dead) was performed in terms of cardiovascular risk factors, clinical data, and early outcomes. Results: The overall in-hospital mortality rate was 20.4%. In multivariate analysis, sudden onset, altered level of consciousness, and neurological, respiratory, cardiological or hemorrhagic complications, and lacunar infarcts appeared to be independent predictors of in-hospital mortality. Conclusions: Female patients ≥85 years with AIS are an unfavorable subgroup of stroke patients with a high risk of early mortality, which may be due to comorbidity, stroke subtype distribution, and higher frequency of medical complications. However, the presence of lacunar infarcts showed a significant protective effect.
Keywords:
Aged
; 80 and over
; ischemic stroke
; cerebrovascular disorders
; female
; hospital mortality
; patient blood management
1. Introduction
Stroke is one of the leading causes of increase in acquired disability and, in turn, acute cerebrovascular diseases, mostly ischemic in nature, are the second leading cause of death in wealthy countries in both men and women, although deaths have been reduced by 21% [1,2,3,4]. Early detection and treatments to respond to the acute phase of the disease are essential to prevent the effects associated with acute ischemic stroke, i.e. premature death, dependency, recurrence, epilepsy, and vascular dementia, all of which require rehabilitation and support, placing a considerable economic burden on the patient, his or her family and the health care system [6,7,8,9,10].
Changes in population structure by age and the aging of industrialized and de-veloped populations, in which the very old (over 85 years) represent the fastest grow-ing segment, increase the importance of studies on acute stroke in the elderly [11,12,13,14]. The selection of 85 years or older is an arbitrary cut-off point for the exclusion of stroke patients from clinical trials and this leads to the arbitrary exclusion of elderly patients from clinical trials to, for example, the study of recombinant tissue plasminogen activator (rtPA) or anticoagulant therapy as a secondary stroke prevention in presumed cardioembolic cerebral infarction. Increasing life expectancy projects a higher percentage of elderly stroke victims [14,15]. Stroke was the first global cause of death in the oldest old in Spain in 2017, the second in men and the first in women [16].
Studies focused on the incidence of stroke in elderly patients agree with our data-base (Sagrat Cor Registry) in pointing out a high in-hospital mortality rate, longer duration of admission and less aggressive therapeutics compared with younger patients [14,17,18,19]. A comparative study between patients older and younger than 85 years indicated that older age was an overall predictor of early mortality in acute cerebrovascular victims (27% vs. 13.5%), as well as in-hospital death (25% vs. 11.5%) [14]. However, knowledge on early outcomes and predictive data on in-hospital mortality of acute stroke in very elderly patients remains limited.
Likewise, it has been found that men and women differ with regard to acute stroke in general and cerebral ischemia in particular. It has been shown that women have specific risk factors, clinical data and a characteristic natural history, in addition to a worse prognostic outcome [20]. Some preclinical studies suggest the sex specificity of some cell death pathways, suggesting that sex-differentiated therapeutic interventions may hold promise for a neuroprotective role in adult ischemic brain injury [21,22,23,24,25]. Despite all of which the analysis of the clinical characteristics of acute is-chemic stroke in the subgroup of elderly women with acute ischemic stroke remains understudied.
Most studies agree on promoting healthy lifestyle habits that control modifiable risk factors, such as smoking, obesity and overweight, sedentary lifestyle, dyslipidemia, hypertension, diabetes mellitus, alcohol consumption, and previous heart disease [26,27,28,29,30,31], although there are cardiovascular risk factors that cannot be modified, such as age, sex (female), family history, thrombophilias, and previous strokes. All factors being equal, the physiology of women in their different reproductive stages makes them especially sensitive to cerebrovascular problems, especially coagulation problems, which can lead to stroke.
It is essential to study and analyze the pathophysiological mechanisms of acute cerebrovascular disease from the different etiologies of the subtypes of ischemic stroke; this is intended to improve knowledge of the natural history of the disease, the expression of its clinical characteristics, with the result of increasing the therapeutic possibilities in cerebral reperfusion and neuronal protection, without forgetting secondary prevention. Thus, the validated subtypes of ischemic stroke are atherothrombotic, cardioembolic, lacunar, essential and cerebral infarction of unusual etiology [26,27]. Atherothrombotic and cardioembolic stroke are the subtypes with the most severe etiology [26,27,28,29,30,31,32]. In contrast, acute lacunar cerebral ischemia is caused by small infarcts (less than 20 mm in diameter) of the terminal branches of the perforating arteries, without anastomosis, that supply the subcortical region of the brain, the depth of the white matter, the basal ganglia and the pons, and approximately a quarter of acute strokes are of the lacunar type.
Emerging evidence suggests that acute lacunar cerebral ischemia, despite being a prevalent type of stroke with a favorable short-term prognosis, is not a benign entity and may represent the first clinical manifestation of cerebral small vessel disease, causing medium and long-term severe physical and vascular cognitive impairment or subcortical dementia [32,33,34,35,36,37,38]. However, there are no absolute data on the frequency and early prognosis of ischemic stroke subtypes in very elderly female patients.
Knowledge of the clinical and outcome differences between men and women could be of interest to improve prevention strategies and in-hospital treatment of very old women with acute cerebral infarction. To this end, we analyzed data from 4,600 consecutive patients with acute stroke included in our database, and compared the prevalence of demographics, cerebrovascular risk predictors, clinical features, and medical complications that developed during hospitalization, as well as neuroimaging data, in very elderly women with ischemic stroke on the basis of their vital condition at discharge (living versus dead) and by means of multiple regression analysis.
Although still controversial, the development of a predictive model of early in-hospital mortality in very elderly patients based on clinical neurological findings on admission would allow not only to establish the initial severity from bedside anamnesis, but also to identify those patients at high risk, with poor prognosis, in whom the relevance of new conventional treatments could be evaluated.
2. Materials and Methods
2.1. Study Population
We performed a retrospective analysis of data on stroke patients prospectively collected in the hospital stroke registry of the Hospital Universitari Sagrat Cor.
Our hospital is a 350-bed acute care university hospital in the city of Barcelona (Catalonia, Spain) serving an estimated population of 300,000 people [32]. For the present study, the data of all consecutive patients with cerebral infarction or primary cerebral hemorrhage admitted to the Department of Neurology, recorded over 24 years, were analyzed. This registry has been previously published and validated.
A protocolized 186-item questionnaire was used for each and every patient. Demographic data, cardiovascular risk factors, history and physical examination find-ings, laboratory data, chest x-ray, 12-lead electrocardiogram, neuroimaging data (noncontrast CT, CT angiography, angiography or MRI), complications and outcomes were collected.
For the classification of stroke subtypes, we used the criteria of the Catalan Society of Neurology and the Guidelines of the Cerebrovascular Study Group of the Spanish Society of Neurology [39,40]; both are similar to the classification of the National In-stitute of Neurological Disorders and Stroke [41] and have been used by our group in previous studies. The study obtained approval from the hospital's Clinical Research Ethics Committee.
A total of 4,600 consecutive patients with acute stroke were analyzed, with the following distribution of stroke subtypes: 955 cardioembolic strokes (20.8%), 944 atherothrombotic strokes (20.5%), 863 lacunar strokes (18.8%), 128 cerebral strokes of unusual etiology (2.8%), 373 cerebral strokes of unknown etiology (8. 1%), 761 transient ischemic attacks (TIAs) (16.5%), 473 intracerebral hemorrhagic strokes (10.3%), 52 subarachnoid hemorrhages (1.1%), and 44 spontaneous subdural hemorrhages/spontaneous epidural hemorrhages (1%).
For the purposes of this study, and as shown in the flow-chart in Figure 1, from the initial sample of patients diagnosed with acute cerebrovascular disease, only very elderly (≥ 85 years) women diagnosed with acute cerebral infarction (cardioembolic infarction, atherothrombotic infarction, lacunar infarction, cerebral infarction of unusual etiology, or cerebral infarction of unknown etiology) were selected from the stroke registry.
Thus, a total sample of 503 very old female with acute cerebral infarction was obtained, of whom 103 died and 403 dismissed alive.
Medical complications (neurological and non-neurological: infectious, hemorrhagic, vascular, respiratory, cardiac, urinary, sudden death) during the acute phase were assessed as well as the causes of early mortality. Neurological causes included recurrence of focal brain ischemia, cerebral herniation, or brain hemorrhage. Vascular complications were peripheral arterial embolism and deep venous thrombosis. Cardiac complications were arrhythmia, heart failure, and acute myocardial infarction. Pulmonary complications included aspiration pneumonia, superinfection, and pulmonary embolism. Mortality after stroke was assessed according to Silver et al criteria [42]. Modified Rankin Scale (mRs) for Neurologic disability was applied for evaluating the patient’s clinical status and degree of disability at discharge and scored as spontaneous neurological improvement or good prognosis (mRS grades 0-2) and poor prognosis or in-hospital death [43,44].
2.2. Statistical Analysis
Deceased and living very old women patients were analyzed comparatively. For univariate analysis, analysis of variance (ANOVA) and t-Student test for continuous variables and Chi-square test (with Yates correction) for categorical variables were used to assess demographics, frequency of risk factors, clinical and neuroimaging data, and outcome in relation to vital status at discharge (alive or dead). The level of statistical significance was established at p<0.05.
Next, a multivariate analysis was performed on those variables that were significantly related to vital status in the univariate analysis plus age. Age was used as a continuous variable, with a constant odds ratio [OR] for each year. In order to evaluate the independent predictive effect of each variable on in-hospital mortality, when p <0.10, a logistic regression procedure and forward stepwise selection were used.
Three predictive models were designed, and in all of them, the dependent variable was in-hospital mortality coded as "alive=0" and "dead=1".
The first model was structured on the basis of cardiovascular risk factors and clinical characteristics collected during the examination on admission. In the second model, variables related to medical complications occurring during the acute phase were added to cardiovascular risk factors and clinical characteristics and, finally, in the third model, the presence of lacunar infarction was evaluated together with the previous variables (cardiovascular risk factors, clinical characteristics, and medical complications).
In the analyses performed, the statistical significance threshold for remaining in the model was 0.15, and the tolerance threshold was set at 0.0001. The weight estimates of the variables in the model were based on the maximum likelihood method [45]. Odds ratios (OR) and confidence intervals (CI) were calculated from beta coefficients and standard deviations. The Chi-squared test was used to assess the goodness of fit of the logistic regression model. Each predictive model was evaluated using the receiver operating characteristic (ROC) curve and the area under the curve (AUC). The SPSS-PC+ and BMDP programs were used for statistical analysis [46].
3. Results
3.1. General Data
Overall, acute ischemic stroke in oldest old women was diagnosed in 506 patients, mean age of 88.6 years (SD 3.2 years), and the most frequent cardiovascular risk factors were hypertension in 56.5% of cases, atrial fibrillation in 42.9%, diabetes in 17.8 %, ischemic heart disease in 15%, heart failure in 13.8%, and hyperlipidemia in 12.8% of cases.
The frequency by different ischemic stroke subtypes was 37.7% of cardioembolic infarcts, 30.8% of atherothrombotic infarcts, 26.1% of cerebral infarcts of unknown cause, 26.1% of lacunar infarcts, and 11.5% of cerebral infarctions of unusual cause.
One hundred and three died, representing an in-hospital mortality of 20.4%. By subtype of ischemic stroke, in-hospital mortality rates were highest in cardioembolic infarct (30.4%) and the lowest frequency was observed in cerebral lacunar infarcts (1.2%) (Table 1).
Causes of mortality recorded were –from highest to lowest frequency- the following: brain herniation in 31%, pneumonia in 19.5%, infection in 19.5%, myocardial infarction in 5.5%, sudden death in 5.5%, recurrent cerebral ischemia in 3%, pulmonary thromboembolism in 1.5%, and unknown in 5%.
3.2. Comparative Clinical Study According to Vital Status at Discharge
Table 2 shows the distribution of statistically significant variables or clinically relevant data between deceased and discharged alive patients. Patients who died showed significantly more frequent presence of atrial fibrillation, sudden onset, consciousness disorders, limb weakness, sensory deficit, and neurological, respiratory, cardiac, hemorrhagic, and infectious complications in the univariate analysis.
3.3. Multivariate Analysis
The results of multivariate analysis for each predictive model indicated that sudden onset, altered consciousness, and limb weakness appeared to be independent clinical predictors of hospital death in the first predictive model based on cerebrovascular risk factors and clinical characteristics (Table 3). In addition to these variables, neurological, respiratory, cardiac, and hemorrhagic complications were selected in the second predictive model based on cerebrovascular risk factors, clinical features and medical complications. In the third model, lacunar infarcts were selected in association with sudden onset, altered consciousness, neurological, respiratory, cardiac, and hemorrhagic events.
For the three predictive models analyzed, the establishment of a cutoff point of 0.50 to predict vital status at hospital discharge yielded the following results: sensitivity of 62%, 77.7% and 80.6%; specificity of 81.1%, 83.1% and 80.4%; positive predictive values of 45.7%, 54% and 51.2%; negative predictive values of 89.3%, 93.6% and 94.2%; and total correct classifications of 77.3%, 82% and 80.4%.
Figure 2 illustrates the ROC curve for the accuracy of the regression model for predicting vital status at discharge, including the variables of cardiovascular risk factors, clinical data, medical complications and presence of lacunar infarct. The area under the receiver operating characteristic curve was 0.872. The sensitivity was 80.6%, the specificity was 80.4%, the positive predictive value was 51.2% and the negative predictive value was 94.2%.
4. Discussion
The results of the present study, based on the analysis of 506 very elderly female patients with ischemic stroke, according to data from our hospital registry, showed that they constituted a subgroup of stroke patients at high risk of early fatal outcome, revealing an in-hospital mortality rate of 20.4%. This higher risk seems to be related to comorbidity, the presence of subtypes of cerebral infarction with worse prognosis and a higher frequency of medical complications.
There are few studies and little published information on the clinical predictors of in-hospital mortality in the oldest old patients with acute cerebral infarction, so the optimal management of these patients remains a dilemma. Also, we have been unable to identify any previous studies that specifically examine the association between ischemic stroke in very elderly women and clinical predictors of in-hospital mortality.
Currently, one third of all patients with a first-ever acute cerebral infarction are 85 years of age or older [11,47,48]. Ischemic stroke causes great health and social impact due to its high incidence and prevalence, and because it is the leading cause of adult acquired disability and the second cause of dementia after Alzheimer's disease. It is a great burden, not only from the public health point of view, but also from the personal and family point of view, due to its impact on the lives of the people who suffer from it and their caregivers. The percentage of stroke patients among the elderly is increasing due to longer life expectancy and changes in the population pyramid in developed societies and it is becoming a major public health problem [49,50].
Analysis of our data, in line with other studies [51,52,53,54], reveals that the short-term prognosis of these patients with acute or hemorrhagic cerebrovascular infarct is poor compared to non-very old patients, showing higher in-hospital mortality (20.9% vs. 8.9%) and a lower percentage of symptom-free patients at discharge (9% vs. 13.7%), the latter being an indicator of disease burden.
The analysis of demographic data specifically related to female sex in the oldest old patients with acute ischemic cerebrovascular infarction is also limited. In this regard, the results based on the multivariate analysis presented here are novel.
The risk of acute cerebrovascular disease is lower in premenopausal women than in men of the same age [55,56,57]. It is known that endogenous estrogen acts as a protective factor, contributing to the maintenance of cardiovascular health through direct and indirect effects. During the climacteric period there is a decrease in ovarian estrogen levels, which causes an increase in the incidence of hypertension, diabetes, dyslipidemia and metabolic syndrome. In addition, there are alterations in weight, insulin sensitivity, lipid profile, sympathetic tone and vascular function. These changes interact with each other and increase the risk of cardiovascular disease in postmenopausal women [58,59]. Thus, gender-specific differences in the incidence of cerebrovascular disease disappear in the age group 65-84 years, increasing in women in the age range equal to or above ≥ 85 years, in acute strokes analyzed globally [60].
Data on the prognosis of ischemic infarction in oldest-old patients are scarce. In previous studies by our group we found that women were 67.2% of patients in the very old subgroup with first-ever acute stroke with a mean (SD) age of 88.6 (3.2) years [14] and that women differed from men in the distribution of risk factors and stroke subtypes, stroke severity, and outcome [61].
However, little is known about mortality rates in the different ischemic stroke subtypes in oldest old female patients (≥ 85 years) and we are not aware of a published predictive model of early in-hospital mortality in very elderly female patients.
One of the objectives of this study was to determine the existence of predictors of in-hospital mortality based on clinical data obtained after diagnosis of focal neurological deficit in the emergency department or within 48 hours of stroke onset. Our results confirm the existence of some predictors of early mortality during hospital admission. Multivariate analysis showed that using only clinical variables, the percentage of correct classification was 80.2%, contributing our clinical investigation to the knowledge of the little known natural history of this subgroup of very old female victims.
Specifically, our study highlights the dominant relevance of medical complications developed during hospital care in the prediction of in-hospital mortality in acute stroke victims. Neurological, respiratory, cardiac, and hemorrhagic complications were independent clinical factors, easily diagnosed at the patient’s bedside, associated with in-hospital death.
Contracting an infection of any type or origin is associated with severe neurological deterioration, which in turn increases both mortality and morbidity in acute stroke patients [62,63,64]. Stroke-associated infection, particularly pneumonia or respiratory superinfection, has been shown to be independently associated with poor functional outcome after cerebral infarction [65,66]. Urinary complications, whether urinary tract infection, incontinence, or urinary retention, are the most frequent in stroke patients and, in turn, can lead to bloodstream infection. Among the vascular complications, deep vein thrombosis stands out, which can cause pulmonary thromboembolism, which in turn is a common cause of death during the acute phase of cerebrovascular disease.
In view of these medical conditions, early diagnosis and appropriate pharmacological treatment are imperative, as they improve the prognosis of patients, as has been observed in other studies [65,66].
It should be emphasized that in-hospital mortality, as an independent variable, has been shown to decrease in hospitals that offer acute stroke unit services. These findings endorse the importance of careful and detailed cardiac and respiratory screening, together with the early institution of early therapy for cardiac and respiratory diseases and concurrent cardiopulmonary episodes.
In our study, altered consciousness was another clinical predictor related to in-hospital mortality, coinciding with the results of other studies [15,26,67,68]. In the study by Lee et al [51], very old Asian patients had the highest proportion of conscious impairment on admission and medical complications.
Motor neurological deficit was also a predictor of early mortality in our series. Appelros [69], in his study on predictors of length of admission in stroke patients, showed that the NIH stroke scale items that correlated with worse prognosis and longer length of stay were paresis, unilateral neglect, and level of consciousness. Most interestingly, lacunar infarction was the only acute infarction subtype that was inversely associated with in-hospital mortality. These patients have a good potential for recovery that may be due to the small infarct size (<2 cm in diameter) and the generally favorable short-term prognosis of lacunar cerebral infarction compared to other subtypes of non-lacunar ischemic stroke [34,70]. Consequently, the presence of lacunar stroke showed a significant protective effect versus other ischemic cerebra infarct subtypes.
Specifically in the objectives of the study, the data on elderly women reflect a greater probability of cardioembolic cerebrovascular infarction, together with a greater frequency of heart disease as comorbid condition. In this regard, it should be noted that cardioembolic cerebral infarction is the subtype of infarction associated with the highest in-hospital mortality (30.4%) in the acute phase of cerebral ischemia. It has been speculated that this may be due, on the one hand, to the high risk of early recurrence of infarction and, on the other, to the large infarct volume in cardiogenic cerebral embolism.
The possible limitations of the present study should be noted. A first limitation would be the potential bias of the retrospective design in a single center, which could contribute to selection bias. Although recruitment to the database was consecutive, this possibility cannot be dismissed out. It would therefore be desirable to design future multicenter studies that allow the study of a large sample size. The second limitation of the study is the lack of analysis of the prognostic value of sex in very old female patients with acute ischemic stroke in the medium or long term. And, finally, a third limitation would consist of not having analyzed the etiology of ischemic infarction of unusual cause in the sample [71], nor the relevance of vascular cognitive impairment in prognosis, with a negative predictive role in the older age group [72,73,74]. These points would represent interesting lines of research to be developed in future studies.
However, our study also has strengths and these are a large, homogeneous and well-characterized cohort, along with complete baseline and initial clinical outcomes with minimal loss to follow-up. In addition, the methods used in this study based on a stroke registry database on a large sample of 506 female patients older than 85 years collected over a 24-year period is more than less objective.
In summary, the poor health status prior to stroke and the greater disability and medical complications immediately following stroke might partly explain the poor clinical prognosis and high in-hospital mortality in oldest old women with acute ischemic stroke.
5. Conclusions
Acute ischemic cerebrovascular infarction in the oldest old (≥ 85 years) is more frequent in female patients and is a devastating situation that is associated with an increased risk of premature death.
In these patients, who constitute a subgroup with severe conditions and poorly understood natural history, the most determinant relevant clinical factors influencing in-hospital mortality after acute ischemic stroke are in-hospital medical complications, whether respiratory, cardiac, neurological, and hemorrhagic. However, the presence of lacunar infarcts showed a significant protective effect. This fact should condition clinicians to establish an early prognosis with greater precision.
The relevance of these findings lies in the fact that most medical complications are potentially avoidable and/or treatable conditions whose prevention, early diagnosis and aggressive treatment should be pursued. Doing so may reduce mortality and improve the prognosis of the oldest old female patients. Therefore, prevention and therapeutic management of avoidable risk factors for medical complications is essential in the early management of the oldest old female patients with acute cerebral ischemia.
As life expectancy increases, the elderly will constitute the majority of cerebrovascular casualties. Identifying particular patterns in cardiovascular factors of risk and outcomes in different age groups of patients with acute stroke has important preventive implications, in part because of the enormous challenges that demographic changes pose to both health and social care systems. A better understanding of the impact of sex-specific characteristics on acute cerebral infarction will improve out-comes for the entire population.
Finally, mention should be made of some of the most promising current lines of research, such as stroke genomics, possible determinant of recurrence in cerebral infarct, and biomarker-based diagnosis of subtypes of acute cerebral infarction. Not to mention the consolidation of new oral anticoagulants in long-term daily treatment of cardioembolic infarction in oldest old patients as the safest and most effective therapeutic management.
Author Contributions
Conceptualization, A.A. and S.T-R.; methodology, A.A.; software, L.G-E.; validation, A.A., S.T-R. and L.G-E.; formal analysis, L.G-E.; investigation, A.A.; resources, M.J.S-L.; data curation, M.J. S-L.; writing—original draft preparation, S.T-R.; writing—review and editing, A.A..; visualization, M.J.S-L.; supervision, A.A and L.G.-E.; project administration, M.J.S-L.;. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Sagrat Cor Hospital of Barcelona (protocol code 2022/07-NEU-HUSC and date of approval 22 February 2022).
Informed Consent Statement
Given the retrospective research setting, the informed consent form was waived.
Data Availability Statement
Not applicable.
Acknowledgments
The authors are grateful to J. Massons, E. Verges, F. Gil, and L. Diez, for their help in this study and the entire staff of the Department of Neurology for their valuable contribution. We also thank E. Grivé of the Department of Neuroradiology for the help and the excellent neuroimaging assistance. This article is dedicated to the memory of Josep Lluís Martí-Vilalta.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Tasso, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart disease and stroke statistics-2022 Update: A report from the American Heart Association. Circulation, 2022; 145, e153–e639. [Google Scholar]
- Mencl, S.; Garz, C.; Niklass, S.; Braun, H.; Göb, E.; Homola, G.; Heinze, H.J.; Reymann, K.G.; Kleinschnitz, C.; Schreiber, S. Early Microvascular Dysfunction in Cerebral Small Vessel Disease Is Not Detectable on 3.0 Tesla Magnetic Resonance Imaging: A Longitudinal Study in Spontaneously Hypertensive Stroke-Prone Rats. Exp Transl Stroke Med. 2013, 5, 8. [Google Scholar]
- Feigin, V.L.; Lawes, C.M.; Bennet, D.A.; Barker-Collo, S.L.; Parag, V. World-wide stroke incidence and early case fatality reported in 55 population-based studies: a systematic review. Lancet Neurol 2009, 8, 355–369. [Google Scholar] [CrossRef]
- Wang, W.X.; Springer, J.E.; Hatton, K.W. MicroRNAs as Biomarkers for Predicting Complications Following Aneurysmal Subarachnoid Hemorrhage. Int J Mol Sci 2021, 22, 9492. [Google Scholar]
- Mao, R.; Zong, N.; Hu, Y.; Chen, Y.; Xu, Y. Neuronal Death Mechanisms and Therapeutic Strategy in Ischemic Stroke. Neurosci Bull. 2022, 1–19. [Google Scholar]
- Arboix, A.; Oliveres, M.; Massons, J.; Pujades, R.; García-Eroles, L. Early differentiation of cardioembolic from atherothrombotic cerebral infarction: a multivariate analysis. Eur J Neurol 1999, 6, 677–683. [Google Scholar]
- Kim, K.Y.; Shin, K.Y.; Chang, K.A. Potential Biomarkers for Post-Stroke Cognitive Impairment: A Systematic Review and Meta-Analysis. Int J Mol Sci 2022, 23, 602. [Google Scholar] [CrossRef]
- Cullell, N.; Gallego-Fábrega, C.; Cárcel-Márquez, J.; Muiño, E.; Llucià-Carol, L.; Lledós, M.; Martín-Campos, J.M.; Molina, J.; Casas, L.; Almería, M.; et al. ICA1L is associated with small vessel disease: A proteome-wide association study in small vessel stroke and intracerebral haemorrhage. Int J Mol Sci 2022, 23, 3161. [Google Scholar]
- Wang, W.X.; Springer, J.E.; Hatton, K.W. MicroRNAs as Biomarkers for Predicting Complications Following Aneurysmal Subarachnoid Hemorrhage. Int J Mol Sci 2021, 22, 9492. [Google Scholar]
- Giralt-Steinhauer, E.; Jiménez-Baladó, J.; Fernández-Pérez, I.; Rey, L.A.; Rodríguez-Campello, A.; Ois, A.; Cuadrado-Godia, E.; Jiménez-Conde, J.; Roquer, J. Genetics and epigenetics of spontaneous intracerebral hemorrhage. Int J Mol Sci 2022, 23, 6479. [Google Scholar]
- Díaz-Guzmán, J.; Egido, J.A.; Gabriel-Sánchez, R.; Barberá-Comes, G.; Fuentes-Gimeno, B.; Fernández-Pérez, C.; et al. Stroke and Transient Ischemic Attack Incidence Rate in Spain: The IBERICTUS Study. Cerebrovasc Dis 2012, 34, 272–81. [Google Scholar]
- Luy, M.; Gast, K. Do women live longer or do men die earlier? Reflections on the causes of sex differences in life expectancy. Gerontology 2014, 60, 143–153. [Google Scholar]
- Kobayashi, L.C.; Beeken, R.J.; Meisel, S.F. Biopsychosocial predictors of perceived life expectancy in a national sample of older men and women. Plos One 2017, 12, e0189245. [Google Scholar]
- Arboix, A.; Pizarro, P.; Fontana, S.; Massons, J.; Garcia-Eroles, L.; Comes, E.; Oliveres, M. Changing profiles of acute stroke in very old patients: Results from the Sagrat Cor Hospital of Barcelona Stroke Registry over a 24-year period. Curr Trends Neurol 2015, 9, 27–35. [Google Scholar]
- Li, M.; Liu, X.; Wang, L.; Shu, L.; Luan, L.; Yin, J.; Zhang, J.; Wang, Q.; Zhang, Y.; Xie, T.; Liu, L.; Geng, T. Admission Hemoglobin Is Prognostic for In-Hospital Mortality in Oldest-Old Patients with Acute Ischemic Stroke. Gerontology 2021, 67, 687–694. [Google Scholar] [CrossRef]
- Ministerio de Sanidad, Consumo y Bienestar Social. Portal estadístico. Área de inteligencia de gestión. Mortalidad por causa de muerte [Internet]. España: Ministerio de Sanidad, Consumo y Bienestar Social; [citado 2018 oct 30]. Available from: https://pestadistico.inteligenciadegestion.mscbs.es/publicoSNS/comun/ArbolNodos.aspx?idNodo=106.
- Orzuza, G.; Zurrú, M.C. Epidemiological aspects of stroke in very old patients. Cardiovasc Hematol Disord Drug Targets 2011, 11, 2–5. [Google Scholar] [CrossRef]
- Erbguth, F. Schlaganfallakuttherapie im Alter. Z Gerontol Geriatr 2020, 53, 59–74. [Google Scholar] [CrossRef]
- Kauffmann, J.; Grün, D.; Yilmaz, U.; Wagenpfeil, G.; Faßbender, K.; Fousse, M.; Unger, M.M. Acute stroke treatment and outcome in the oldest old (90 years and older) at a tertiary care medical centre in Germany-a retrospective study showing safety and efficacy in this particular patient population. BMC Geriatr. 2021, 21, 611. [Google Scholar] [CrossRef]
- Eaker, E.D.; Chesebro, J.H.; Sacks, F.M.; Wenger, N.K.; Whisnant, J.P.; Winston, M. Cardiovascular disease in women. Circulation 1993, 88, 1999–2009. [Google Scholar]
- Gallego Fabrega, C.; Muiño, E.; Cullell, N.; Cárcel-Márquez, J.; Lazcano, U.; Soriano-Tárraga, C.; Lledós, M.; Llucià-Carol, L.; Aguilera-Simón, A.; Marín, R.; et al. Biological Age Acceleration Is Lower in Women With Ischemic Stroke Compared to Men. Stroke 2022, 53, 2320–2330. [Google Scholar] [CrossRef]
- Bousser, M.G. Stroke in women. Circulation. 1999, 99, 463–467. [Google Scholar]
- Wong, M.C.W.; Giuliani, M.J.; Haley, E.C. Cerebrovascular disease and stroke in women. Cardiology 1990, 77 (Suppl 2), 80–90. [Google Scholar]
- Tansey, M.J.B.; Opie, L.H.; Kenelly, B.M. High mortality in obese women diabetics with acute myocardial infarction. BMJ 1977, 1, 1624–1626. [Google Scholar]
- Roquer, J.; Rodríguez, A.C.; Gomis, M. Sex differences in first-ever acute stroke. Stroke 2003, 34, 1581–1585. [Google Scholar]
- Palomeras Soler, E.; Fossas Felip, P.; Casado Ruiz, V.; Cano Orgaz, A.; Sanz Cartagena, P.; Muriana Batiste, D. The Mataró Stroke Registry: a 10-year registry in a community hospital. Neurologia 2015, 30, 283–289. [Google Scholar]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. ; Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef]
- Di Stefano, V.; De Angelis, M.V.; Montemitro, C.; Russo, M.; Carrini, C.; di Giannantonio, M.; Brighina, F.; Onofrj, M.; Werring, D.J.; Simister, R. Clinical presentation of strokes confined to the insula: a systematic review of literature. Neurol Sci 2021, 42, 1697–1704. [Google Scholar] [CrossRef]
- Leventis, I.; Perlepe, K.; Sagris, D.; Sirimarco, G.; Strambo, D.; Georgiopoulos, G.; Eskandari, A.; Karagkiozi, E.; Vemmou, A.; Koroboki, E.; et al. Characteristics and outcomes of Embolic Stroke of Undetermined Source according to stroke severity. Int J Stroke 2020, 15, 866–871. [Google Scholar] [CrossRef]
- Tehrani, A.S.S.; Kattah, J.C.; Kerber, K.A.; Gold, D.R.; Zee, D.S.; Urrutia, V.C.; Newman-Toker, D.E. Diagnosing stroke in acute dizziness and vertigo. Pitfalls and pearls. Stroke 2018, 49, 788–795. [Google Scholar] [CrossRef]
- Choi, J.; Lee, S.; Kim, J. Central vertigo. Curr Opin Neurol 2018, 31, 81–89. [Google Scholar] [CrossRef]
- Arboix, A.; Massons, J.; Oliveres, M.; García, L.; Titus, F. An analysis of 1000 consecutive patients with acute cerebrovascular disease. The registry of cerebrovascular disease of La Alianza-Hospital Central of Barcelona. Med Clin (Barc), 1993; 101, 281–285. [Google Scholar]
- Bejot, Y.; Catteau, A.; Caillier, M.; Rouaud, O.; Durier, J.; Marie, C.; Di Carlo, A.; Osseby, G.V.; Moreau, T.; Giroud, M. Trends in incidence, risk factors, and survival in symptomatic lacunar stroke in Dijon, France, from 1989 to 2006. A population-based study. Stroke, 2008; 39, 1945–1951. [Google Scholar]
- Rudilosso, S.; Rodríguez-Vázquez, A.; Urra, X.; Arboix, A. The Potential Impact of Neuroimaging and Translational Research on the Clinical Management of Lacunar Stroke. Int J Mol Sci 2022, 23, 1497. [Google Scholar] [CrossRef]
- Chung, J.; Marini, S.; Pera, J.; Norrving, B.; Jimenez-Conde, J.; Roquer, J.; Fernandez-Cadenas, I.; Tirschwell, D.L.; Selim, M.; Brown, D.L.; et al. Genome-Wide Association Study of Cerebral Small Vessel Disease Reveals Established and Novel Loci. Brain 2019, 142, 3176–3189. [Google Scholar]
- Grau-Olivares, M.; Arboix, A.; Junqué, C.; Arenaza-Urquijo, E.M.; Rovira, M.; Bartrés-Faz, D. Progressive gray matter atrophy in lacunar patients with vascular mild cognitive impairment. Cerebrovasc Dis 2010, 30, 157–166. [Google Scholar] [CrossRef]
- Jacova, C.; Pearce, L.A.; Costello, R.; McClure, L.A.; Holliday, S.L.; Hart, R.G.; Benavente, O.R. Cognitive impairment in lacunar strokes: the SPS3 trial. Ann Neurol 2012, 72, 351–362. [Google Scholar]
- Rundek, T.; Tolea, M.; Ariko, T.; Fagerli, E.A.; Camargo, C. J;. Vascular Cognitive Impairment (VCI). Neurotherapeutics, 2022; 19, 66–88. [Google Scholar] [CrossRef]
- Arboix, A.; Alvarez-Sabin, J.; Soler, L.; Comité de Redacción ad hoc del Grupo de estudio de Enfermedades Cerebrovasculares de la SEN. Ictus. Clasificación y criterios diagnósticos. Neurologia. 1998, 13(Suppl 3), S3–S10.
- Societat Catalana de Neurologia. Guies mèdiques oficials de diagnòstic i tractament. En: Malalties vasculars cerebrals. Societat Catalana de Neurologia: Barcelona, 2011; 2a ed. pp. 159-240.
- Special Report from the National Institute of Neurological Disorders and Stroke: Classification of cerebrovascular diseases III. Stroke. 1990, 21, 637–676.
- Silver, F.L.; Norris, J.W.; Lewis, A.J.; Hachinski, V.C. Early mortality following stroke: a prospective review. Stroke 1984, 15, 492–496. [Google Scholar]
- Kumar, S.; Selim, M.; Caplan, L. Medical complications after stroke. Lancet Neurol 2010, 9, 105–18. [Google Scholar]
- Bamford, J.M.; Sandercock, P.A.G.; Warlow, C.P.; Slattery, J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1989, 20, 828. [Google Scholar]
- Armitage, P. Statistical methods in medical research. Wiley: New York, USA, 1977.
- Dixon, W.J. BMDP statistical software manual. Berkeley, CA. University of California Press: Berkeley, CA, USA, 1990; pp. 300-344.
- Smirnov, M.; Destrieux, C.; Maldonado, I.L. Cerebral White Matter Vasculature: Still Uncharted? Brain. 2021, 144, 3561–3575. [Google Scholar]
- Rabinstein, A.A. Update on Treatment of Acute Ischemic Stroke. Continuum (Minneap Minn), 2020; 26, 268–286. [Google Scholar] [CrossRef]
- Castagna, A.; Ferrara, L.; Asnaghi, E.; Colombo, V.; Rega, V.; Fiorini, G. Post-stroke dysphagia rehabilitation in the old and oldest old: outcome and relevance for discharge home. Int J Rehabil Res 2020, 43, 55–61. [Google Scholar] [CrossRef]
- Vannucchi, V.; Moroni, F.; Grifoni, E.; Marcucci, R.; Landini, G.; Prisco, D.; Masotti, L. Management of oral anticoagulation in very old patients with non valvular atrial fibrillation related acute ischemic stroke. J Thromb Thrombolysis 2020, 49, 86–93. [Google Scholar] [CrossRef]
- Lee, M.; Huang, W.Y.; Weng, H.H.; Lee, J.D.; Lee, T.H. First-ever ischemic stroke in very old Asians: clinical features, stroke subtypes, risk factors and outcome. Eur Neurol 2007, 58, 44–8. [Google Scholar] [CrossRef]
- Wang, Y.; Jing, J.; Pan, Y.; Wang, M.; Meng, X.; Wang, Y. Clinical characteristics and prognosis in oldest old patients with ischaemic stroke or transient ischaemic attack in China. Ann Palliat Med 2022, 11, 2215–2224. [Google Scholar] [CrossRef]
- Hamanaka, M.; Tanaka, E.; Yamada, T.; Kishitani, T.; Fujinami, J.; Nagakane, Y. Long-term effectiveness of anticoagulants in oldest-old stroke survivors with atrial fibrillation. J Clin Neurosci 2022, 102, 21–25. [Google Scholar] [CrossRef]
- Cocho, D.; Yarleque, S.; Boltes, A.; Espinosa, J.; Ciurans, J.; Pont-Sunyer, C.; Pons, J. Clinical Outcome of Ischemic Stroke in Old Patients Versus Oldest-Old. J Stroke Cerebrovasc Dis 2018, 27, 3657–3661. [Google Scholar] [CrossRef]
- Ayala, C.; Croft, J.B.; Greenlund, K.J.; Keenan, N.L.; Donehoo, R.S.; Malarcher, A.M.; Mensah, G.A. Sex differences in US mortality rates for stroke and stroke subtypes by race/ethnicity and age, 1995 to 1998. Stroke 2002, 33, 1197–1201. [Google Scholar]
- Ho, J.E.; Paultre, F.; Mosca, L. Is diabetes mellitus a cardiovascular disease risk equivalent for fatal stroke in women ?. Data from the Women’s Pooling Project. Stroke 2003, 34, 2812-2816.
- Soriano-Reixach, M.M.; Vivanco Hidalgo, R.M.; Ois, A.; Rodríguez Campello, A.; Roquer, J. Interaction of Sex and Diabetes on Outcome After Ischemic Stroke. Front Neurol. 2018, 9, 250. [Google Scholar] [CrossRef]
- Andersen, K.K.; Andersen, Z.J.; Olsen, T.S. Age-and gender-specific prevalence of cardiovascular risk factors in 40,102 patients with first-ever ischemic stroke: a Nationwide Danish Study. Stroke 2010, 41, 2768–2774. [Google Scholar] [CrossRef]
- Eriksson, M.; Åsberg, S.; Sunnerhagen, K.S.; von Euler, M. Sex Differences in Stroke Care and Outcome 2005-2018: Observations From the Swedish Stroke Register. Stroke 2021, 52, 3233–3242. [Google Scholar] [CrossRef]
- Paulus, J.K.; Lai, L.Y.; Lundquist, C.; Daneshmand, A.; Buettner, H.; Lutz, J.S.; Raman, G.; Wessler, B.S.; Kent, D.M. Field Synopsis of the Role of Sex in Stroke Prediction Models. J Am Heart Assoc 2016, 5, e002809. [Google Scholar] [CrossRef]
- Arboix A, Cartanyà A, Lowak M, García-Eroles L, Parra O, Oliveres M, Massons J. Gender differences and woman-specific trends in acute stroke: results from a hospital-based registry (1986-2009). Clin Neurol Neurosurg, 2014; 127, 19–24. [CrossRef]
- Chang, K.C.; Tseng, MC.; Weng, H.H.; Lin, Y.H.; Liou, C.W.; Tan, T.Y. Prediction of length of stay of first-ever ischemic stroke. Stroke 2002, 33, 2670–2674. [Google Scholar]
- Kumar, S.; Selim, M.; Caplan, L. Medical complications after stroke. Lancet Neurol. 2010, 9, 105–118. [Google Scholar]
- Tu, J.V.; Gong, Y. Trends in treatment and outcomes for acute stroke patients in Ontario, 1992-1998. Arch Intern Med 2003, 163, 293–297. [Google Scholar]
- Junttola, U.; Lahtinen, S.; Liisanantti, J.; Vakkala, M.; Kaakinen, T.; Isokangas, J.M. Medical complications and outcome after endovascular therapy for acute ischemic stroke. Acta Neurol Scand 2021, 144, 623–631. [Google Scholar] [CrossRef]
- Hung, S.H.; Ebaid, D.; Kramer, S.; Werden, E.; Baxter, H.; Campbell, B.C.; Brodtmann, A. Pre-stroke physical activity and admission stroke severity: A systematic review. Int J Stroke 2021, 16, 1009–1018. [Google Scholar] [CrossRef]
- Wise, F.M.; Harris, D.W.; Olver, J.H.; Davis, S.M.; Disler, P.B. Acute Predictors of Social Integration Following Mild Stroke. J Stroke Cerebrovasc Dis 2018, 27, 1025–1032. [Google Scholar] [CrossRef]
- Meissner, A. Hypertension and the brain: a risk factor for more than heart disease. Cerebrovasc Dis 2016, 42, 255–262. [Google Scholar]
- Appelros, P. Prediction of length of stay for stroke patients. Acta Neurol Scand 2007, 116, 15–19. [Google Scholar] [CrossRef]
- Arboix, A.; García-Plata, C.; García-Eroles, L.; Massons, J.; Comes, E. Clinical study of 99 patients with pure sensory stroke. J Neurol 2005, 252, 156–162. [Google Scholar]
- Arboix, A.; Jiménez, C.; Massons, J.; Parra, O.; Besses, C. Hematological disorders: a commonly unrecognized cause of acute stroke. Expert Rev Hematol 2016, 9, 891–901. [Google Scholar]
- Gąsecki, D.; Kwarciany, M.; Nyka, W.; Narkiewicz, K. Hypertension, brain damage and cognitive decline. Curr Hypertens Rep 2013, 15, 547–558. [Google Scholar]
- Carey, R.M.; Moran, A.E.; Whelton, P.K. Treatment of Hypertension: A Review. JAMA 2022, 328, 1849–1861. [Google Scholar] [CrossRef]
- Zonneveld, T.P.; Richard, E.; Vergouwen, M.D.I.; Nederkoorn, P.J.; de Haan, R.; Roos, Y.B.; Kruyt, N.D. Blood Pressure-Lowering Treatment for Preventing Recurrent Stroke, Major Vascular Events, and Dementia in Patients with a History of Stroke or Transient Ischaemic Attack. Cochrane Database Syst Rev 2018, 7, CD007858. [Google Scholar]
Figure 1.
Schematic flow-chart of the patients included in the study considering the early outcome in the very old female patients with acute cerebral infarction.
Figure 1.
Schematic flow-chart of the patients included in the study considering the early outcome in the very old female patients with acute cerebral infarction.

Figure 2.
ROC curve for the regression model. Variables adjusted for cerebrovascular risk factors, clinical features, medical complications, and presence of lacunar infarct. Area under the curve = 0.872. ROC: receiving operating characteristics.
Figure 2.
ROC curve for the regression model. Variables adjusted for cerebrovascular risk factors, clinical features, medical complications, and presence of lacunar infarct. Area under the curve = 0.872. ROC: receiving operating characteristics.
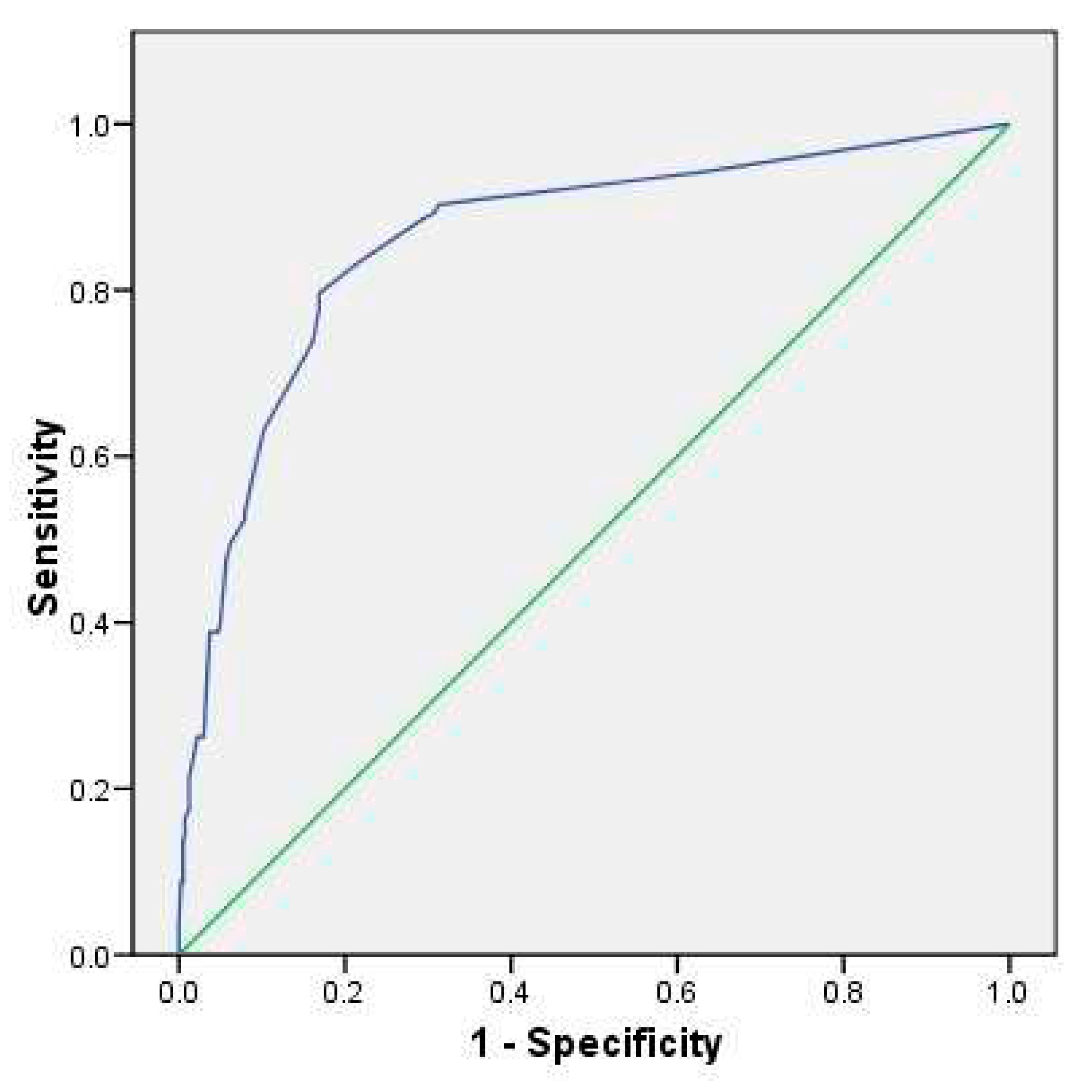

Table 1.
Mortality rates in the different ischemic stroke subtypes in oldest old female patients (≥ 85 years).
Table 1.
Mortality rates in the different ischemic stroke subtypes in oldest old female patients (≥ 85 years).
| Ischemic stroke subtypes | Alive | Dead | Total |
|---|---|---|---|
| Atherothrombotic infarct | 119 (82.1) | 26 (17.9) | 145 |
| Lacunar infarct | 81(98.8) | 1 (1.2) | 82 |
| Cardioembolic infarct | 158 (69.6) | 69 (30.4) | 227 |
| Cerebral infarcts of unknown cause | 39 (88.6) | 5 (11.4) | 44 |
| Cerebral infarctions of unusual cause | 6 (75) | 2 (25) | 8 |
| Total | 403 (79.6) | 103 (20.4) | 506 |
Table 2.
Results of univariate analysis in 506 female very old patients (≥ 85 years) with acute stroke according to vital status at discharge.
Table 2.
Results of univariate analysis in 506 female very old patients (≥ 85 years) with acute stroke according to vital status at discharge.
| Variable, coded | Alive (n=403) |
Deceased (n=103) |
P value |
|---|---|---|---|
| Cerebrovascular risk factors (%) | |||
| Hypertension Absent Present |
174 (79.1) 229 (80.1) |
46 (20.9) 57 (19.9) |
0.786 |
| Diabetes Mellitus Absent Present |
333 (80) 70 (77.8) |
83 (20) 29 (22.2) |
0.628 |
| Coronary heart disease Absent Present |
340 (79.1) 63 (82.9) |
90 (20.9) 13 (17.1) |
0.445 |
| Atrial fibrillation Absent Present |
244 (84.4) 159 (73.3) |
45 (15.6) 58 (26.7) |
0.002 |
| Congestive heart failure Absent Present |
353 (81) 50 (71.4) |
83 (19) 20 (28.6) |
0.066 |
| Previous cerebral stroke Absent Present |
363 (80.3) 40 (74.1) |
89 (19.7) 14 (25.9) |
0.282 |
| History of Transient Ischemic attack (TIA) Absent Present |
359 (80.3) 44 (74.6) |
88 (19.7) 15 (25.4) |
0.304 |
| Chronic obstructive pulmonary disease Absent Present |
381 (80.2) 22 (71) |
94 (19.8) 9 (29) |
0.216 |
| Obesity Absent Present |
385 (79.1) 18 (94.7) |
102 (20.9) 1 (5.3) |
0.169 |
| Anticoagulants Absent Present |
388 (80.2) 15 (68.2) |
96 (19.8) 7 (31.8) |
0.274 |
| Hyperlipidemia Absent Present |
346 (78.5) 57 (87.7) |
95 (21.5) 8 (12.3) |
0.084 |
| Clinical features (%) | |||
| Sudden onset Absent Present |
220 (85.6) 183 (73.5) |
37 (14.4) 66 (26.5) |
0.001 |
| Acute onset (hours) Absent Present |
279 (78.4) 124 (82.7) |
77 (21.8) 26 (17.3) |
0.273 |
| Headache Absent Present |
836 (78.6) 35 (92.1) |
100 (21.4) 3 (7.9) |
0.047 |
| Early seizures Absent Present |
399 (80) 4 (57.1) |
100 (20) 3 (42.9) |
0.310 |
| Altered consciousness Absent Present |
327 (89.3) 76 (54.3) |
39 (10.7) 64 (45.7) |
0.000 |
| Limb weakness Absent Present |
87 (88.8) 316 (77.5) |
11(11.2) 92 (22.5) |
0.012 |
| Sensory deficit Absent Present |
293 (83) 110 (71.9) |
60 (17) 43 (28.1) |
0.004 |
| Hemianopia Absent Present |
339 (81.1) 64 (72.7) |
24 (27.3) 103 (20.9) |
0.076 |
| Extrapyramidal disorders Absent Present |
391 (79.1) 12 (100) |
103 (20.9) 0 |
0.159 |
| In-hospital outcome (%) | |||
| Neurological complications Absent Present |
374 (84.8) 29 (44.6) |
67 (15.2) 36 (55.4) |
0.000 |
| Respiratory complications Absent Present |
361 (86.6) 42 (47.2) |
56 (13.4) 47 (52.8) |
0.000 |
| Digestive complications Absent Present |
391 (80.5) 12 (60) |
95 (19.5) 8 (40) |
0.052 |
| Cardiac events Absent Present |
390 (81.8) 13 (44.8) |
87 (18.2) 16 (55.2) |
0.000 |
| Hemorrhagic events Absent Present |
399 (80.8) 4 (33.3) |
95 (19.2) 8 (66.7) |
0.000 |
| Infectious complications Absent Present |
335 (84.6) 68 (61.8) |
61 (15.4) 42 (38.2) |
0.000 |
Table 3.
Multivariate logistic regression.
| Variable | β | SE (β) | OR (CI 95%) | p |
|---|---|---|---|---|
| Cerebrovascular risk factors and clinical features1 | ||||
| Sudden onset | 0.627 | 0.252 | 1.871 (1.143-3.065) | 0.013 |
| Altered consciousness | 1.953 | 0.245 | 7.049 (4.365-11.384) | 0.000 |
| Limb weakness | 0.757 | 0.367 | 2.132 (1.038-4.378) | 0.039 |
| Cerebrovascular risk factors, clinical features and medical complications2 | ||||
| Sudden onset | 0.680 | 0.278 | 1.974 (1.144-3.406) | 0.015 |
| Altered consciousness | 1.739 | 0.280 | 5.693 (3.290-9.850) | 0.000 |
| Neurological complications | 1.374 | 0.334 | 3.950 (2.053-7.601) | 0.000 |
| Respiratory complications | 1.752 | 0.304 | 5.765 (3.177-10.460) | 0.000 |
| Cardiac events | 1.107 | 0.503 | 3.025 (1.128-8.109) | 0.028 |
| Hemorrhagic events | 1.829 | 0.738 | 6.227 (1.466-26.440) | 0.013 |
| Cerebrovascular risk factors, clinical features, medical complications and presence of lacunar infarct3 | ||||
| Sudden onset | 0.671 | 0.281 | 1.957 (1.128-3.394) | 0.017 |
| Altered consciousness | 1.583 | 0.282 | 4.868 (2.800-8.466) | 0.000 |
| Neurological complications | 1.380 | 0.336 | 3.895 (2.017-7.521) | 0.000 |
| Respiratory complications | 1.725 | 0.305 | 5.610 (3.084-10.207) | 0.000 |
| Cardiac events | 0.987 | 0.497 | 2.709 (1.023-7.177) | 0.045 |
| Hemorrhagic events | 1.685 | 0.733 | 5.392 (1.281-22.698) | 0.022 |
| Lacunar infarct | -2.264 | 1.058 | 0.104 (0.013-0828). | 0.032 |
1β = -3.104, SE(β) = 0.376, Hosmer-Lemeshow goodness-of-fit test χ2 = 1.926, df = 4, p = 0.749, percentage correctly classified = 77.3%. 2β = -3.271, SE(β) = 0.286, Hosmer-Lemeshow goodness-of-fit test χ2 = 5.396, df = 4, p = 0.249, percentage correctly classified = 82%. 3β = -3.063, SE(β) = 0.296, Hosmer-Lemeshow goodness-of-fit test χ2 =6.468, df = 7, p = 0.486, percentage orrectly classified = 80.4%.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



