
Submitted:
31 August 2023
Posted:
31 August 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Omicron variants have higher infectivity, more immune escape but lower risk of severe clinical outcomes than the ancestral variants. However, people are still wondering whether SARS-CoV-2 may become lethal again or whether some highly-pathogenic strain may emerge in the future. Omicron is more selective proliferation in the upper respiratory tract (URT). The temperature of human URT is 33–34°C, and the virus strains other than Omicron cannot replicate effectively at this temperature. While Omicron adapted to the low temperature environment, so its distribution mainly depends on the expression levels of ACE2 in cells. Similar distribution switch from lungs to URT has been observed for the 1918 H1N1 influenza virus, who vanished after 1921 and has been turned to be the seasonal human influenza A viruses. However, some relatively high-pathogenic SARS-CoV-2 strains and influenza-virus strains may still emerge in the future. Dynamic changes in the viral virulence should be monitored constantly.
Keywords:
SARS-CoV-2
; 1918 H1N1 influenza virus
; immune escape
; upper respiratory tract
; pathogenicity
Introduction
The infections of respiratory viruses induce reactive oxygen species accumulation, causing hyper-immune responses to the viruses, which may have adverse effects on vital organs and result in high pathogenicity and mortality. For example, the avian influenza H5N1 virus may set off a cytokine storm, which leads to the acute respiratory distress syndrome and multi-organ failure (Yuan, 2013). While the coronavirus disease 2019 (COVID-19) also triggers cytokine storms and induces intravascular coagulation, ventilation–perfusion mismatch and life-threatening hypoxemia subsequently (Yuan et al., 2021a). High viral load but low clearance rate may be two of the key reasons (Yuan et al., 2021b).
So far, five severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variants (Alpha, Beta, Gamma, Delta, and Omicron) emerged and became dominant epidemic strains worldwide. Compared to the ancestral variants, the Omicron lineage has the most highly mutations in the spike protein, with more than 50 mutations occurred throughout the genome (Kandeel et al., 2022; Tian et al., 2022; Viana et al., 2022; Wang and Cheng, 2022; Zhou et al., 2023). Omicron variants have higher infectivity, more immune escape but attenuated fusogenicity (cell-cell fusion). Although higher binding affinity and more immune escape are usually associated with higher viral replication rate and lower clearance rate respectively, Omicron variants have lower risk of severe clinical outcomes than the ancestral variants (Suzuki et al., 2022; Zhou et al., 2023). The possible reasons for its lower pathogenicity are discussed in this perspective paper.
Increased binding to the receptor and enhanced immune escape in Omicron
The SARS-CoV-2 viruses have accumulated a lot of mutations to adapt to the human body, which have made the affinity between Omicron and the receptor angiotensin-converting enzyme 2 (ACE2) three times higher than that of the original strain (Cameroni et al., 2022; Yin et al., 2022). However the stronger affinity to the ACE2 may not be the evolutionary direction. The Alpha strain has a 6.2-fold increased binding affinity to human ACE2 (2.6 times of Omicron; Cameroni et al., 2022). However, the Alpha strain is not the circulating one.
Key residue mutations resulted in a sharp decline in antibody titer against Omicron receptor-binding domain (RBD; Cameroni et al., 2022; Cao et al., 2022a; Mannar et al., 2022; Planas et al., 2022). Moreover, for the original strain, a large part of the S protein surface is negatively charged or electrically neutral, but its RBD is partly positive-charged. However the surface of the S protein from the Omicron variant is uniformly positive-charged (Yuan et al., 2022a). The difference in antigen surface electrostatic distribution may result in charge-related heterogeneity in its corresponding monoclonal antibodies (Vlasak and Ionescu, 2008). Thus, the sharp decline in antibody titer against the Omicron may also be attributed to a change in surface charge of the S protein (Pascarella et al., 2022; Yuan et al., 2022a). Individuals immunized with mRNA vaccine (against ancestral variants) had more potent neutralizing activity against Wuhan-Hu-1 and retained detectable neutralization against Omicron with a decrease of 21-39 folds. However, reductions of neutralization potency were less pronounced (5 folds) in vaccinated individuals who had been previously infected with ancestral variants (Cameroni et al., 2022). Therefore, Omicron may escape the majority of the existing neutralizing antibodies (Cameroni et al., 2022; Cao et al., 2022a; Mannar et al., 2022; Planas et al., 2022). However, the viral strain with high immune escape capacity may not necessarily become the epidemic one. Although the Delta lineage exhibited immune escape property similar to the Omicron BA.1 strain (Arora et al., 2022), the Delta strain was replaced by the BA.1 variant. Relative to BA.4 and BA.5, BA.2.75 exhibited declined evasion of humoral immunity from BA.1/BA.2 infected convalescent plasma; nevertheless, due to its increased receptor-binding capability and distinct neutralizing antibody escape pattern, BA.2.75 prevailed after BA.4/BA.5 (Cao et al., 2022b).
Omicron is more selectively proliferated in the upper respiratory tract (URT)
The increase of binding with ACE2 and higher immune escape capacity did not lead to an increase in its pathogenicity, but the Omicron strain became much milder (Suzuki et al., 2022; Zhou et al., 2023). This is not due to the reduction in viral replication, but rather its more selective proliferation in the upper respiratory tract (URT; Figure 1; Granerud et al., 2022; Salmona et al., 2022; Salvagno et al., 2022). Omicron patients carried higher viral loads in the nasopharynx and showed more sustained viral shedding, when comparing with the Delta patients (Granerud et al., 2022). The viral load of Omicron in nasopharyngeal swabs increased by 8 times compared to Alpha or Delta; while the viral load of Omicron in saliva decreased by 8 times correspondingly (Salmona et al., 2022). Nevertheless, there are also contradictory reports showing that nasopharyngeal viral loads for Omicron were similar or lower than other variants (Migueres et al., 2022; Sentis et al., 2022).
Ancestral variants exhibited reduced viral replication (by 10 times) at 34°C compared to 37°C. Contrastingly, viral loads were either similar or (10 times) higher at 34°C for the Omicron variants (Stauft et al., 2023). The temperature of human URT is 33–34°C, and the virus strains other than Omicron replicate less-effectively at this temperature. Omicron replicates poorly in the lungs, which may be due to the higher temperature at 37°C. Nevertheless, Stauft et al., 2023 only performed in vitro studies with a non-small cell lung cancer cell line and a monkey kidney cell line. More solid evidences from in vivo studies are still required. Omicron adapted to the low temperature environment, so its distribution mainly depends on the expression levels of ACE2 in cells. In fact, although the expression level of ACE2 in alveolar type II epithelial cells was relatively high, it was much lower than those in nasal goblet cells and bronchial ciliated cells (Figure 1; Viera Braga et al., 2019; Hikmet et al., 2020; Salamanna et al., 2020). Thus, the distribution change of Omicron from the lung to the URT may be explained.
RNA-dependent RNA polymerase (RdRp) plays an essential role for the viral replication and some mutations may be associated with viral replication in a low temperature (Kim et al., 2022). Multiple intra-host single-nucleotide variations have been found in the RdRp coding region of the Omicron variant, such as A1892T, I189V, P314L, K38R, T492I and V57V (Bansal and Kumar, 2022). Although T4685A, N4992N, and G5063S in RdRp were associated with Delta mortality, no mutation in RdRp was found to be significantly associated with Omicron mortality (Saifi et al., 2022). SARS-CoV-2 variants containing the P323L or P323L/G671S mutation in RdRp exhibited enhanced replication at 33°C compared to 37°C and high transmissibility in ferrets (Kim et al., 2022). Detailed mechanisms for Omicron's adaptation to the low temperature require further studies.
Similar distribution switch from lungs to URT has been observed for the 1918 H1N1 influenza virus
To predict the evolutionary direction of SARS-CoV-2, we may retrospect to another worldwide pandemic, the 1918 H1N1 influenza virus infection. It was estimated that about 500,000,000 people or 1/3 of the world’s people were infected with the virus. The number of fatality was estimated to be more than 50,000,000 worldwide (Taubenberger et al., 2012; Short et al., 2018; Jester et al., 2019; Taubenberger et al., 2019; Scarpa et al., 2020). However, this highly pathogenic strain vanished after 1921 and has been turned to be the seasonal human influenza A viruses (Patrono et al., 2022).
The 1918 virus was likely originated from an avian virus, although people were not sure how long the virus had been adapting in mammalian hosts before emerging as a pandemic strain (Patrono et al., 2022). Watanabe et al. (2009) constructed a series of reassortants between the highly pathogenic 1918 H1N1 strain and a contemporary seasonal human H1N1 strain, and tested them in a ferret model. And they found that the 1918 virus could efficiently replicate in the lung tissue as well as the URT, but most reassortants and the contemporary human H1N1 virus grew predominantly in nasal turbinates, but only sporadically in the trachea and lungs (Figure 1; Watanabe et al., 2009).
A reassortant virus expressing the full 1918 RNA polymerase complex exhibited virulence property in both URT and the lower respiratory tract of ferrets that is similar to that of wild-type 1918 strain. These findings clearly implicated that the viral RNA polymerase is the main determinant of the pathogenicity of the 1918 H1N1 virus (Watanabe et al., 2009). Amino-acid mutations in the basic polymerase (PB) have also been shown to be important determinants of transmissibility and the host range (Resa-Infante et al., 2011). Whereas avian viruses, generally, replicate at temperatures of 41–42°C (the temperature of bird intestinal tract). For replication in humans, the virus needs to adapt to 33–34°C. The amino-acid substitution E627K in the basic polymerase 2 (PB2) has been suggested to be associated with efficient virus replication in human cells at such lower temperature (Tscherne and García-Sastre, 2011; Herfst et al., 2012; Russell et al., 2012; Lam et al., 2013). Amino-acid substitution S590G or R591Q in PB2 yields a similar phenotype to E627K (Mehle and Doudna, 2009). All the key mutations, E627K, S590G and R591Q, have been found in the 1918 H1N1 strain (Zhang et al., 2015).
The hemagglutinin (HA) of human-infective influenza viruses prefer to recognize α-2,6-linked sialic acids (SAs; the human-type receptor), however the HA of avian-infective influenza viruses prefer to recognize α-2,3-linked SAs (the avian-type receptor). Some amino acid substitutions in HA may switch the virus to human-infective influenza (Zhang et al., 2015). The α-2,3-linked SAs are mainly distributed on type II pneumocytes with a few number of epithelial cells of the URT; while the α-2,6-linked SAs are abundantly expressed in the URT and secondly in lungs (Figure 1; Yao et al., 2008; Kuchipudi et al., 2021). The 1918 H1N1 virus (such as the New York variant) bound both α-2,3 and α-2,6 receptors (Stevens et al., 2006). The relative lack of avian-type receptor in the upper airway may be another reason why the 1918 virus proliferated both in lungs and in the URT (Watanabe et al., 2009) and caused rapid and severe pneumonia, but the seasonal human influenza viruses proliferate mainly in the URT (Watanabe et al., 2009) and are usually non-lethal.
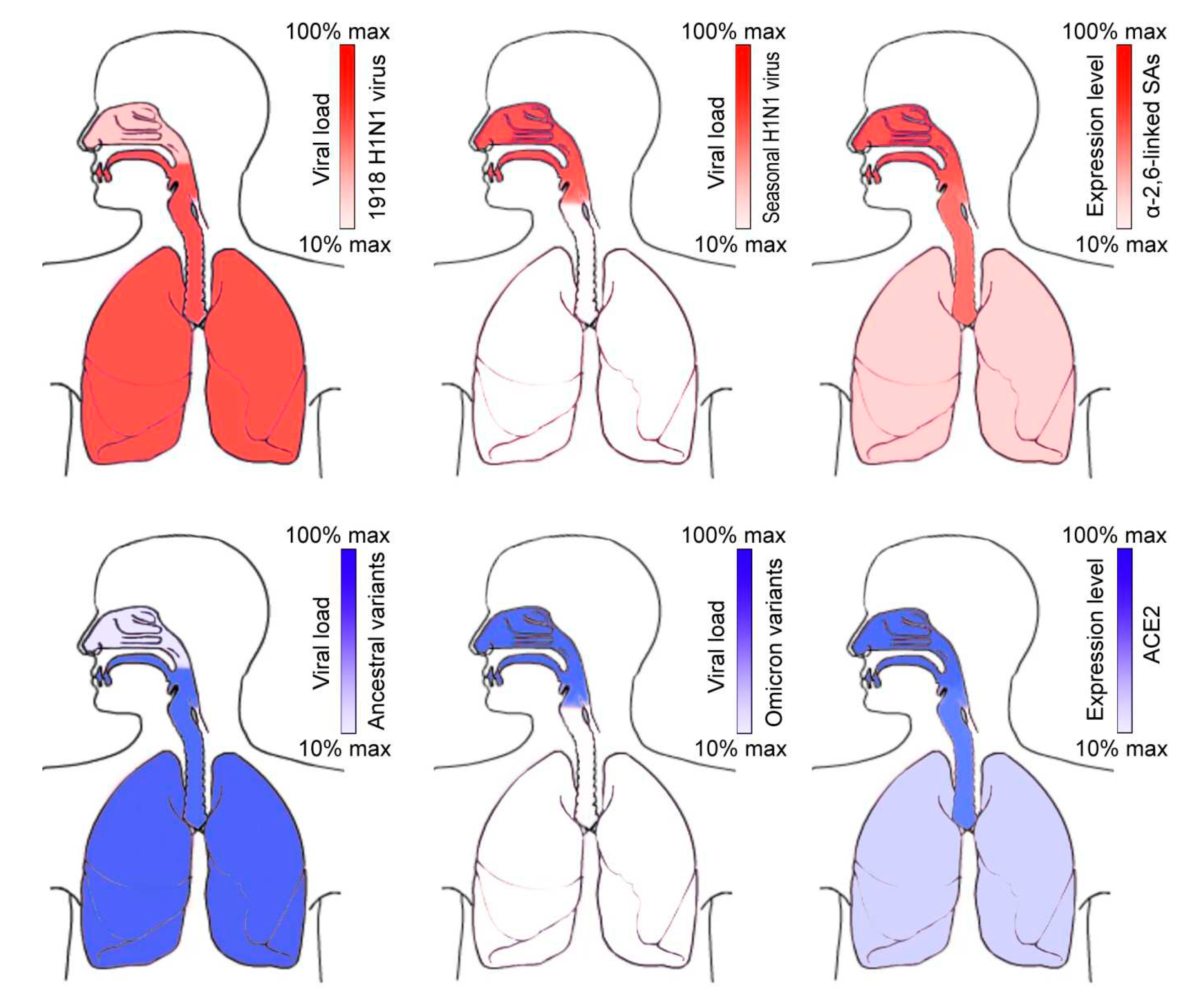
Putative viral loads of 1918 H1N1 virus, seasonal H1N1 virus, SARS-CoV-2 ancestral variants and Omicron variants in the whole respiratory tract are shown. And the expression levels of α-2,6-linked SAs (H1N1 virus receptor) and ACE2 (SARS-CoV-2 receptor) in the whole respiratory tract are shown.
Future evolutionary direction of SARS-CoV-2
URT infection enables viral shedding via abundant speech droplets (Yuan et al., 2020; Stadnytskyi et al., 2021). After the emergence of this evolutionary feature of URT distribution, the virus strain with the highest transmissibility would become the epidemic one. For example, the breath emission rate (viral copies in the exhaled aerosols per hour) of cases with BA.5 sub-variant infection was about 40 times higher than that of cases with BA.2 sub-variant (Li et al., 2023a). On the other hand, the BA.5 virus showed a significantly higher entry efficiency and enhanced immune evasion than the ancestral wild-type strain or B.1.1.529 (Li et al., 2023b). Therefore, BA.5 prevailed after BA.2 and B.1.1.529.
People are wondering whether SARS-CoV-2 may become lethal again or whether some highly-pathogenic strain may emerge in the future. The distribution on the URT also means that the viral loads in lungs are declined, the pathogenicity of the virus is reduced. This may be the evolutionary direction of most airborne viruses after they have infected humans. This evolutionary direction is irreversible, and therefore SARS-CoV-2 may not become lethal again, although new variants may still emerge after Omicron. However, the distribution on the URT does not necessarily mean that the virus will become further mild. The emergence of highly virulent influenza strains are usually due to the genetic reassortments (Joseph et al., 2017). Besides, certain key mutations may greatly enhance the viral replication efficiency and the virulence consequently (Zhang et al., 2015; Yuan et al., 2022b). Thus, some relatively high-pathogenic SARS-CoV-2 strains may still emerge in the future. Dynamic changes in the viral virulence should be monitored constantly.
Implications from the URT distribution
It is well-known that nose washing (nasal rinses) can reduce URT infections effectively (King et al., 2015; Farrell et al., 2020; Yuan et al., 2022c). Nasal rinses disrupt the viscous surface layer physically, and remove the mucus with its associated particulate matter (viruses). Moreover, the nasal saline increases hydration of the deeper aqueous layer, improves the underlying ciliary beat frequency and reduces local inflammatory factors (Farrell et al., 2020). A recent study showed that nasal irrigation significantly attenuated SARS-CoV-2 Omicron infection, transmissibility and lung injuries in the Syrian hamster model (Yuan et al., 2022c). So we recommend nasal irrigation to susceptible population, especially who just went to a crowded public place or just began to show some mild laryngopharyngeal symptoms. Nasal irrigation in the incubation period may relieve the symptoms, or even that the infected people may become asymptomatic. On the other hand, nasal irrigation would reduce Omicron's viral load effectively and therefore reduce the complication rate and mortality, which is of importance to children and old people, especially to those who have underlying diseases, like chronic obstructive pulmonary disease (COPD).
Nasal vaccines for COVID-19 treatments should also be developed. Efficient delivery of nasal sprays to ACE2-abundant regions is required urgently, especially in the context that some new strains may not be responsive to current vaccines and more refractory to current drug therapies (Xi et al., 2021; Abdoli et al., 2022; Feng et al., 2022).
Author Contributions
SY conceived the project. L-BX, TL, S-CJ, Z-WZ, Y-FF, and X-YY performed the literature search. SY wrote the manuscript with input from L-BX and TL. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the Sichuan Province Youth Science and Technology Innovation Team (20CXTD0062) to SY and the Applied Basic Research Program of Sichuan Province (2020YJ0410) to Z-WZ.
Conflicts of Interest
Ting Liu was employed by the Sichuan Kelun Pharmaceutical Comp. Ltd. Si-Cong Jiang was employed by the Haisco Pharmaceutical Group Comp. Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Abdoli M, Shafaati M, Ghamsari LK, Abdoli A (2022): Intranasal administration of cold-adapted live-attenuated SARS-CoV-2 candidate vaccine confers protection against SARS-CoV-2. Virus Res. 319, 198857. [CrossRef]
- Arora P, Zhang L, Rocha C, Graichen L, Nehlmeier I, Kempf A, Cossmann A, Ramos GM, Baier E, Tampe B, Moerer O, Dickel S, Winkler MS, Behrens GMN, Pöhlmann S, Hoffmann M (2022): The SARS-CoV-2 Delta-Omicron recombinant lineage (XD) exhibits immune-escape properties similar to the Omicron (BA.1) variant. Int. J. Mol. Sci. 23, 14057. [CrossRef]
- Bansal K, Kumar S (2022): Mutational cascade of SARS-CoV-2 leading to evolution and emergence of omicron variant. Virus Res. 315, 198765. [CrossRef]
- Cameroni E, Bowen JE, Rosen LE, Saliba C, Zepeda SK, Culap K, Pinto D, VanBlargan LA, De Marco A, di Iulio J, Zatta F, Kaiser H, Noack J, Farhat N, Czudnochowski N, Havenar-Daughton C, Sprouse KR, Dillen JR, Powell AE, Chen A, Maher C, Yin L, Sun D, Soriaga L, Bassi J, Silacci-Fregni C, Gustafsson C, Franko NM, Logue J, Iqbal NT, Mazzitelli I, Geffner J, Grifantini R, Chu H, Gori A, Riva A, Giannini O, Ceschi A, Ferrari P, Cippà PE, Franzetti-Pellanda A, Garzoni C, Halfmann PJ, Kawaoka Y, Hebner C, Purcell LA, Piccoli L, Pizzuto MS, Walls AC, Diamond MS, Telenti A, Virgin HW, Lanzavecchia A, Snell G, Veesler D, Corti D (2022): Broadly neutralizing antibodies overcome SARS-CoV-2 Omicron antigenic shiftNature 602, 664–670. [CrossRef]
- Cao Y, Wang J, Jian F, Xiao T, Song W, Yisimayi A, Huang W, Li Q, Wang P, An R, Wang J, Wang Y, Niu X, Yang S, Liang H, Sun H, Li T, Yu Y, Cui Q, Liu S, Yang X, Du S, Zhang Z, Hao X, Shao F, Jin R, Wang X, Xiao J, Wang Y, Xie XS (2022a): Omicron escapes the majority of existing SARS-CoV-2 neutralizing antibodies. Nature 602, 657–663. [CrossRef]
- Cao Y, Song W, Wang L, Liu P, Yue C, Jian F, Yu Y, Yisimayi A, Wang P, Wang Y, Zhu Q, Deng J, Fu W, Yu L, Zhang N, Wang J, Xiao T, An R, Wang J, Liu L, Yang S, Niu X, Gu Q, Shao F, Hao X, Meng B, Gupta RK, Jin R, Wang Y, Xie XS, Wang X (2022b): Characterization of the enhanced infectivity and antibody evasion of Omicron BA.2.75. Cell Host Microbe 30, 1527–1539.e5. [CrossRef]
- Farrell NF, Klatt-Cromwell C, Schneider JS (2020): Benefits and safety of nasal saline irrigations in a pandemic-washing COVID-19 away. JAMA Otolaryngol. Head Neck Surg. 146, 787–788. [CrossRef]
- Feng F, Wen Z, Chen J, Yuan Y, Wang C, Sun C (2022): Strategies to develop a mucosa-targeting vaccine against emerging infectious diseases. Viruses 14, 520. [CrossRef]
- Granerud BK, Ueland T, Lind A, Søraas A, Fevang B, Steffensen AK, Al-Baldawi H, Lund-Johansen F, Aukrust P, Halvorsen B, Dahl TB, Dudman S, Müller F, Holter JC (2022): Omicron variant generates a higher and more sustained viral load in nasopharynx and saliva than the Delta variant of SARS-CoV-2. Viruses 14, 2420. [CrossRef]
- Herfst, S., Schrauwen, E. J., Linster, M., Chutinimitkul, S., de Wit, E., Munster, V. J., et al. (2012). Airborne transmission of influenza A/H5N1 virus between ferrets. Science 336, 1534–1541. [CrossRef]
- Hikmet F, Méar L, Edvinsson Å, Micke P, Uhlén M, Lindskog C (2020): The protein expression profile of ACE2 in human tissues. Mol. Syst. Biol. 16, e9610. [CrossRef]
- Jester B, Uyeki TM, Jernigan DB, Tumpey TM (2019): Historical and clinical aspects of the 1918 H1N1 pandemic in the United States. Virology 527, 32–37. [CrossRef]
- Joseph U, Su YC, Vijaykrishna D, Smith GJ (2017): The ecology and adaptive evolution of influenza A interspecies transmission. Influenza Other Respir. Viruses 11, 74–84. [CrossRef]
- Kandeel M, Mohamed MEM, Abd El-Lateef HM, Venugopala KN, El-Beltagi HS (2022): Omicron variant genome evolution and phylogenetics. J. Med. Virol. 94, 1627–1632. [CrossRef]
- Kim SM, Kim EH, Casel MAB, Kim YI, Sun R, Kwack MJ, Yoo JS, Yu MA, Yu KM, Jang SG, Rollon R, Choi JH, Gil J, Eun K, Kim H, Ensser A, Hwang J, Song MS, Kim MH, Jung JU, Choi YK (2022): SARS-CoV-2 variants show temperature-dependent enhanced polymerase activity in the upper respiratory tract and high transmissibility. BioRxiv 2022.09.27.50 9689. [CrossRef]
- King D, Mitchell B, Williams CP, Spurling GK (2015): Saline nasal irrigation for acute upper respiratory tract infections. Cochrane Database Syst. Rev. 2015, CD006821. [CrossRef]
- Kuchipudi SV, Nelli RK, Gontu A, Satyakumar R, Surendran Nair M, Subbiah M (2021): Sialic acid receptors: the key to solving the enigma of zoonotic virus spillover. Viruses 13, 262. [CrossRef]
- Lam TT, Wang J, Shen Y, Zhou B, Duan L, Cheung CL, Ma C, Lycett SJ, Leung CY, Chen X, Li L, Hong W, Chai Y, Zhou L, Liang H, Ou Z, Liu Y, Farooqui A, Kelvin DJ, Poon LL, Smith DK, Pybus OG, Leung GM, Shu Y, Webster RG, Webby RJ, Peiris JS, Rambaut A, Zhu H, Guan Y (2013): The genesis and source of the H7N9 influenza viruses causing human infections in China. Nature 502, 241–244. [CrossRef]
- Li J, Zheng J, Chen P, Wang B, Zhang Y, Xiong J, You L, Jin Y, Jiang L, Tang F, Wen H, Hong C, Zeng X, Li L, Lu B, Rong B, Wang Z (2023a): Higher SARS-CoV-2 shedding in exhaled aerosol probably contributed to the enhanced transmissibility of Omicron BA.5 subvariant. J. Med. Virol. 95, e28365. [CrossRef]
- Li C, Huang J, Yu Y, Wan Z, Chiu MC, Liu X, Zhang S, Cai JP, Chu H, Li G, Chan JF, To KK, Yang Z, Jiang S, Yuen KY, Clevers H, Zhou J (2023b): Human airway and nasal organoids reveal escalating replicative fitness of SARS-CoV-2 emerging variants. Proc. Natl. Acad. Sci. U.S.A. 120, e2300376120. [CrossRef]
- Mannar D, Saville JW, Zhu X, Srivastava SS, Berezuk AM, Tuttle KS, Marquez AC, Sekirov I, Subramaniam S (2022): SARS-CoV-2 Omicron variant: Antibody evasion and cryo-EM structure of spike protein-ACE2 complex. Science 375, 760–764. [CrossRef]
- Mehle A, Doudna JA (2009): Adaptive strategies of the influenza virus polymerase for replication in humans. Proc. Natl. Acad. Sci. U.S.A. 106, 21312–21316. [CrossRef]
- Migueres M, Dimeglio C, Trémeaux P, Abravanel F, Raymond S, Lhomme S, Mansuy JM, Izopet J (2022): Influence of immune escape and nasopharyngeal virus load on the spread of SARS-CoV-2 Omicron variant. J. Infect. 84, e7–e9. [CrossRef]
- Pascarella S, Ciccozzi M, Bianchi M, Benvenuto D, Cauda R, Cassone A (2022): The value of electrostatic potentials of the spike receptor binding and N-terminal domains in addressing transmissibility and infectivity of SARS-CoV-2 variants of concern. J. Infect. 84, e62–e63. [CrossRef]
- Patrono LV, Vrancken B, Budt M, Düx A, Lequime S, Boral S, Gilbert MTP, Gogarten JF, Hoffmann L, Horst D, Merkel K, Morens D, Prepoint B, Schlotterbeck J, Schuenemann VJ, Suchard MA, Taubenberger JK, Tenkhoff L, Urban C, Widulin N, Winter E, Worobey M, Schnalke T, Wolff T, Lemey P, Calvignac-Spencer S (2022): Archival influenza virus genomes from Europe reveal genomic variability during the 1918 pandemic. Nat. Commun. 13, 2314. [CrossRef]
- Planas D, Saunders N, Maes P, Guivel-Benhassine F, Planchais C, Buchrieser J. Bolland WH, Porrot F, Staropoli I, Lemoine F, Péré H, Veyer D, Puech J, Rodary J, Baele G, Dellicour S, Raymenants J, Gorissen S, Geenen C, Vanmechelen B, Wawina-Bokalanga T, Martí-Carreras J, Cuypers L, Sève A, Hocqueloux L, Prazuck T, Rey FA, Simon-Loriere E, Bruel T, Mouquet H, André E, Schwartz O (2022): Considerable escape of SARS-CoV-2 Omicron to antibody neutralization. Nature 602, 671–675. [CrossRef]
- Resa-Infante P, Jorba N, Coloma R, Ortin J (2011): The influenza virus RNA synthesis machine: advances in its structure and function. RNA Biol. 8, 207–215. [CrossRef]
- Russell CA, Fonville JM, Brown AE, Burke DF, Smith DL, James SL, Herfst S, van Boheemen S, Linster M, Schrauwen EJ, Katzelnick L, Mosterín A, Kuiken T, Maher E, Neumann G, Osterhaus AD, Kawaoka Y, Fouchier RA, Smith DJ (2012): The potential for respiratory droplet–transmissible A/H5N1 influenza virus to evolve in a mammalian host. Science 336, 1541–1547. [CrossRef]
- Saifi S, Ravi V, Sharma S, Swaminathan A, Chauhan NS, Pandey R (2022): SARS-CoV-2 VOCs, Mutational diversity and clinical outcome: Are they modulating drug efficacy by altered binding strength? Genomics 114, 110466. [CrossRef]
- Salamanna F, Maglio M, Landini MP, Fini M (2020): Body localization of ACE-2: on the trail of the keyhole of SARS-CoV-2. Front. Med. 7:594495. [CrossRef]
- Salmona M, Chaix ML, Feghoul L, Mahjoub N, Maylin S, Schnepf N, Jacquier H, Walle EM, Helary M, Mellon G, Osinski N, Zebiche W, Achili Y, Amarsy R, Mahé V, Le Goff J, Delaugerre C (2022): Detection of SARS-CoV-2 in saliva and nasopharyngeal swabs according to viral variants. Microbiol. Spectr. 10, e0213322. [CrossRef]
- Salvagno GL, Henry BM, Pighi L, De Nitto S, Montagnana M, Lippi G (2022): SARS-CoV-2 Omicron infection is associated with high nasopharyngeal viral load. J. Infect. 84, 834–872. [CrossRef]
- Scarpa R, Caso F, Costa L, Passavanti S, Vitale MG, Trojaniello C, Del Puente A, Ascierto PA (2020): May the analysis of 1918 influenza pandemic give hints to imagine the possible magnitude of Corona Virus Disease-2019 (COVID-19)? J. Transl. Med. 18, 489. [CrossRef]
- Sentis C, Billaud G, Bal A, Frobert E, Bouscambert M, Destras G, Josset L, Lina B, Morfin F, Gaymard A, The Covid-Diagnosis Hcl Study Group (2022): SARS-CoV-2 Omicron variant, lineage BA.1, is associated with lower viral load in nasopharyngeal samples compared to Delta variant. Viruses 14, 919. [CrossRef]
- Short KR, Kedzierska K, van de Sandt CE (2018): Back to the future: Lessons learned from the 1918 influenza pandemic. Front. Cell. Infect. Microbiol. 8, 343. [CrossRef]
- Stadnytskyi V, Anfinrud P, Bax A (2021): Breathing, speaking, coughing or sneezing: What drives transmission of SARS-CoV-2? J. Intern. Med. 290, 1010–1027. [CrossRef]
- Stauft CB, Sangare K, Wang TT (2023): Differences in new variant of concern replication at physiological temperatures in vitro. J. Infect. Dis. 227, 202–205. [CrossRef]
- Stevens J, Blixt O, Glaser L, Taubenberger JK, Palese P, Paulson JC, Wilson IA (2006): Glycan microarray analysis of the hemagglutinins from modern and pandemic influenza viruses reveals different receptor specificities. J. Mol. Biol. 355, 1143–1155. [CrossRef]
- Suzuki R, Yamasoba D, Kimura I, Wang L, Kishimoto M, Ito J, Morioka Y, Nao N, Nasser H, Uriu K, Kosugi Y, Tsuda M, Orba Y, Sasaki M, Shimizu R, Kawabata R, Yoshimatsu K, Asakura H, Nagashima M, Sadamasu K, Yoshimura K; Genotype to Phenotype Japan (G2P-Japan) Consortium; Sawa H, Ikeda T, Irie T, Matsuno K, Tanaka S, Fukuhara T, Sato K (2022): Attenuated fusogenicity and pathogenicity of SARS-CoV-2 Omicron variant. Nature 603, 700–705. [CrossRef]
- Taubenberger JK, Baltimore D, Doherty PC, Markel H, Morens DM, Webster RG, Wilson IA (2012): Reconstruction of the 1918 influenza virus: unexpected rewards from the past. mBio 3, e00201-12. [CrossRef]
- Taubenberger JK, Kash JC, Morens DM (2019): The 1918 influenza pandemic: 100 years of questions answered and unanswered. Sci. Transl. Med. 11, eaau5485. [CrossRef]
- Tian D, Sun Y, Xu H, Ye Q (2022): The emergence and epidemic characteristics of the highly mutated SARS-CoV-2 Omicron variant. J. Med. Virol. 94, 2376–2383. [CrossRef]
- Tscherne DM, García-Sastre A (2011) Virulence determinants of pandemic influenza viruses. J. Clin. Invest. 121, 6–13. [CrossRef]
- Viana R, Moyo S, Amoako DG, Tegally H, Scheepers C, Althaus CL, Anyaneji UJ, Bester PA, Boni MF, Chand M, Choga WT, Colquhoun R, Davids M, Deforche K, Doolabh D, du Plessis L, Engelbrecht S, Everatt J, Giandhari J, Giovanetti M, Hardie D, Hill V, Hsiao NY, Iranzadeh A, Ismail A, Joseph C, Joseph R, Koopile L, Kosakovsky Pond SL, Kraemer MUG, Kuate-Lere L, Laguda-Akingba O, Lesetedi-Mafoko O, Lessells RJ, Lockman S, Lucaci AG, Maharaj A, Mahlangu B, Maponga T, Mahlakwane K, Makatini Z, Marais G, Maruapula D, Masupu K, Matshaba M, Mayaphi S, Mbhele N, Mbulawa MB, Mendes A, Mlisana K, Mnguni A, Mohale T, Moir M, Moruisi K, Mosepele M, Motsatsi G, Motswaledi MS, Mphoyakgosi T, Msomi N, Mwangi PN, Naidoo Y, Ntuli N, Nyaga M, Olubayo L, Pillay S, Radibe B, Ramphal Y, Ramphal U, San JE, Scott L, Shapiro R, Singh L, Smith-Lawrence P, Stevens W, Strydom A, Subramoney K, Tebeila N, Tshiabuila D, Tsui J, van Wyk S, Weaver S, Wibmer CK, Wilkinson E, Wolter N, Zarebski AE, Zuze B, Goedhals D, Preiser W, Treurnicht F, Venter M, Williamson C, Pybus OG, Bhiman J, Glass A, Martin DP, Rambaut A, Gaseitsiwe S, von Gottberg A, de Oliveira T (2022): Rapid epidemic expansion of the SARS-CoV-2 Omicron variant in southern Africa. Nature 603, 679–686. [CrossRef]
- Viera Braga FKG, Berg M, Carpaij OA, Polanski K, Simon LM, Brouwer S, Gomes T, Hesse L, Jiang J, Fasouli ES, Efremova M, Vento-Tormo R, Talavera-López C, Jonker MR, Affleck K, Palit S, Strzelecka PM, Firth HV, Mahbubani KT, Cvejic A, Meyer KB, Saeb-Parsy K, Luinge M, Brandsma CA, Timens W, Angelidis I, Strunz M, Koppelman GH, van Oosterhout AJ, Schiller HB, Theis FJ, van den Berge M, Nawijn MC, Teichmann SA (2019): A cellular census of human lungs identifies novel cell states in health and in asthma. Nat. Med. 25, 1153–1163. [CrossRef]
- Vlasak J, Ionescu R (2008): Heterogeneity of monoclonal antibodies revealed by charge-sensitive methods. Curr. Pharm. Biotechnol. 9, 468–481. [CrossRef]
- Wang L, Cheng G (2022): Sequence analysis of the emerging SARS-CoV-2 variant Omicron in South Africa. J. Med. Virol. 94, 1728–1733. [CrossRef]
- Watanabe T, Watanabe S, Shinya K, Kim JH, Hatta M, Kawaoka Y (2009): Viral RNA polymerase complex promotes optimal growth of 1918 virus in the lower respiratory tract of ferrets. Proc. Natl. Acad. Sci. U.S.A. 106, 588–592. [CrossRef]
- Xi J, Lei LR, Zouzas W, April Si X (2021): Nasally inhaled therapeutics and vaccination for COVID-19: Developments and challenges. MedComm 2, 569–586. [CrossRef]
- Yao L, Korteweg C, Hsueh W, Gu J (2008): Avian influenza receptor expression in H5N1-infected and noninfected human tissues. FASEB J. 22, 733–740. [CrossRef]
- Yin W, Xu Y, Xu P, Cao X, Wu C, Gu C, He X, Wang X, Huang S, Yuan Q, Wu K, Hu W, Huang Z, Liu J, Wang Z, Jia F, Xia K, Liu P, Wang X, Song B, Zheng J, Jiang H, Cheng X, Jiang Y, Deng SJ, Xu HE (2022): Structures of the Omicron spike trimer with ACE2 and an anti-Omicron antibody. Science 375, 1048–1053. [CrossRef]
- Yuan S (2013): Drugs to cure avian influenza infection--multiple ways to prevent cell death. Cell Death Dis. 4, e835. [CrossRef]
- Yuan S, Jiang SC, Li ZL (2020): Do humidity and temperature impact the spread of the novel coronavirus? Front. Public Health. 8, 240. [CrossRef]
- Yuan S, Jiang SC, Zhang ZW, Fu YF, Hu J, Li ZL (2021a): The role of alveolar edema in COVID-19. Cells 10, 1897. [CrossRef]
- Yuan S, Jiang SC, Zhang ZW, Fu YF, Hu J, Li ZL (2021b): Quantification of cytokine storms during virus infections. Front. Immunol. 12, 659419. [CrossRef]
- Yuan S, Jiang SC, Zhang ZW, Fu YF, Yang XY, Li ZL, Hu J, Du JB, Yuan M, Chen YE (2022a): Surface electrostatic shift on spike protein decreased antibody activities against SARS-CoV-2 Omicron variant. J. Infect. 85, 208–211. [CrossRef]
- Yuan S, Jiang SC, Zhang ZW, Fu YF, Zhu F, Li ZL, Hu J (2022b): Abuse of amantadine in poultry may be associated with higher fatality rate of H5N1 infections in humans. J. Med. Virol. 94, 2588–2597. [CrossRef]
- Yuan L, Zhu H, Zhou M, Ma J, Liu X, Wu K, Ye J, Yu H, Chen P, Chen R, Wang J, Zhang Y, Ge S, Yuan Q, Cheng T, Guan Y, Xia N (2022c): Nasal irrigation efficiently attenuates SARS-CoV-2 Omicron infection, transmission and lung injury in the Syrian hamster model. iScience 25, 105475. [CrossRef]
- Zhang ZW, Liu T, Zeng J, Chen YE, Yuan M, Zhang DW, Zhu F, Yuan S (2015): Prediction of the next highly pathogenic avian influenza pandemic that can cause illness in humans. Infect. Dis. Poverty 4, 50. [CrossRef]
- Zhou Y, Zhi H, Teng Y (2023): The outbreak of SARS-CoV-2 Omicron lineages, immune escape, and vaccine effectivity. J. Med. Virol. 95, e28138. [CrossRef]
Figure 1.
Distribution changes of 1918 H1N1 influenza virus and SARS-CoV-2 after human adaptations.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



