
Submitted:
28 August 2023
Posted:
01 September 2023
You are already at the latest version
Abstract
The rapid introduction of DAAs has revolutionized the treatment of chronic HCV infection, however some concerns have been arose about their early and long term safety in real life settings. Therefore, these drugs achieve a robust and sustained virological response in a short duration of treatment, being a quick winning option, but, what then? At now an extensive follow-up in real life settings does not exist particularly on HCC occurrence as recently suggested in a Cochrane review . In this regard from February 2015 to December 2017 a group of 5 Hospital and Academic Centers in Southern Italy (Campania Region) managed an observational, prospective, real-life study on efficacy and safety of DAAs treatment schedule enrolling 1022 consecutive HCV patients treated with IFN-free DAAs regimens being followed-up for 24 months. Our preliminary data on the first 360 patients out of 1022 whose completed at least 66 weeks follow-up, based on clinical, laboratory and expert ultrasonography every three months, showed an SVR in 342 out 360 (95%) patients of which 9 had a new diagnosed HCC (2.63%). Specifically HCC developed in mean after 16,2 months after end of treatment as one or more nodules (2-3 cm in mean) with an increase in alpha-fetoprotein 10 x u.n.v (n.v. <15 UI/mL) in patients with F4 fibrosis staging at the time of treatment enrolment. In conclusion, in view of our findings and literature evidences, regular clinical, laboratory and expert ultrasonography follow-up should carefully performed also on these patients and the current Faster, Higher, Stronger approach to the new antivirals development should strongly be revisited in the light of possible late adverse events like HCC occurrence and the relative economic impact on health care system cost.
Keywords:
HCC
; DAAs
; Antivirals
; HCV
; Immunesurveillance
; Immunity
; Liver stiffness
Introduction
Hepatitis C virus (HCV) infection has been characterized, in the last years, by a significant advancement in treatment schedule with the advent of the new direct-acting antivirals (DAA). These drugs are characterized by a rate of sustained viral response (SVR) higher than 90%, relative few adverse events and short length of treatment reported in clinical trials (1-3). However, in the last few years some concerns have raised according to several reports on HCC occurrence in those cirrhotic patients achieving SVR (4-6) whereas other reports suggest lower risk (7, 8). Indeed, among patient with HCV infection and cirrhosis, the risk of hepatocellular carcinoma (HCC) is estimated to be 3% to 7% per year (9-10) while previous reports have shown that cirrhotic patients achieving the SVR, after IFN schedule treatment, had a lower risk of HCC development, with an incidence rate per year of 1.2–1.4% (11-12). Nevertheless, the risk of HCC remains because advanced fibrosis or cirrhosis, which are the most important risk factors for liver cancer, is not completely resolved by antiviral treatment (13). Thus, even if these new antivirals have demonstrated their great value in terms of treatment for the Hepatitis C eradication in the next future some issues still remain to be evaluated, particularly:
- (1)
- Does Viral clearance really mean a disease resolution? That would be mandatory to determine to really weight a significant long term impact on natural history of HCV.
- (2)
- We now have more then 5 years follow-up however still remain unknown a long-term follow-up) more than 10 years about clinical evolution of viral disease (ascites, variceal bleeding, hepato-renal syndrome, hepatic encephalopathy, and hepatocellular carcinoma). Particularly, we do not have decisive findings regarding these outcomes in real life settings and this would be fundamental in the health care system management.
According to our previous research protocol on long-term follow-up of patients undergoing first generation DAAs (referenza WJHEPA), we managed a long-term follow-up to verify disease natural history of patients who underwent second generation DAAs with achieved SVR. Here we will present our data on 48 months real life follow-up.
Methods
Study design and patients’ population
From February 2015 to December 2018 a group of 4 Hospital and Academic Centres in Southern Italy (Campania Region) on behalf of CLEO (Italian Society of Hospital Hepatologist) conducted an observational, prospective, real-life study on efficacy and safety of DAAs treatment schedule recruiting all consecutive HCV patients treated with IFN-free DAAs regimens, local ethical committee n674. According to Italian ministerial guidelines for DAAs treatment, the inclusion criteria were HCV-RNA serum positivity, fibrosis stage ≥F3 according to Metavir score (the Italian reimbursement criteria, at the time of enrolment, were applicable only for patients with F3-F4 fibrosis) assessed by liver biopsy or transient elastography (TE) (14). The TE was performed by Fibroscan® (Echosens, Paris, France), according to standard criteria and only reliable tests according to Boursier’s criteria were considered optimal for enrolment (15).
In this real-life population study, patients with any of the following features were excluded: active HCC on imaging or history of previous treated HCC, HBV or HIV co-infection, or liver transplant recipients. All patients were followed up every month during treatment and thereafter every 3 months for at least 48 months.
The baseline HCC screening for all patients enrolled in our cohort was performed according to the European guidelines of the European Association for the Study of Liver (EASL) (16).
An abdominal ultrasound (US) was performed before starting the antiviral therapy (within two weeks); each US was performed by two expert experienced operators (defined with more than 5000 exams with certification at SIUMB (Italian Society of Ultrasound Medicine) for each Centre). This approach was managed in order to minimize the bias of a multicenter, unmonitored study. A contrast-enhanced ultrasonography (CEUS), a dynamic computed tomography (CT) scan or dynamic magnetic resonance imaging (MRI) was managed to characterize incidental hepatic lesions. Patients showing nodular patterns suggestive of HCC or with uncertain dynamic vascular behaviour at the time of treatment enrolment were excluded from further follow-up.
HCV-RNA was assessed by real-time PCR (COBAS®TaqMan, AmpliPrep, Roche) with a detection limit of 15 IU/mL.
The diagnosis of cirrhosis was based on clinical, biochemical, ultrasonographic, elastographic and, when available, histological features. In particular, for cirrhotic patients, liver function was graded according to the Child-Turcotte-Pugh (CTP) score system.
Demographic characteristics and clinical parameters at baseline, including age, sex, body mass index (BMI), alcohol consumption, tobacco smoking, presence of comorbidities, and biochemical parameters were recorded.
The study was performed according to the Declaration of Helsinki and was approved by the local Ethic Committee (Vanvitelli-Ospedali dei COlli Local Ethical Committee; Approval number: 674); all patients gave informed consent to the study as for previous research protocol.
Patients follow-up
Virological response to therapy was assessed by real-time PCR with HCV-RNA detection at the end of treatment, 12 and 24 weeks after the end of treatment. The SVR, defined as the persistent absence of detectable serum HCV-RNA 12 weeks after the end of treatment (SVR12), was assessed for all the enrolled patients. Any relapse of serum HCV-RNA during follow-up was recorded.
At least three ultrasound examinations per year were performed for every enrolled patient during the established follow-up period (at the end of therapy, 12 weeks after the end of therapy and six months later) according to the HCC surveillance program and study design. Any detected liver lesion was evaluated by imaging technique workup (CEUS, or dynamic CT scan or dynamic MRI) according to EASL guidelines (16).
The diagnosed HCC were recorded and scored according to Barcelona Clinic Liver Cancer (BCLC) staging system (17). Once a patient had a diagnosis of HCC, the follow-up was stopped.
Liver stiffness evaluation
TE by FibroScan was carried out using the M probe experienced operators (>1000 exams), according to the manufacturer’s instructions. The LSM, expressed in Kilopascal (Kpa), range 2.5-75, was assessed for reliability by the interquartile range (IQR)/median ratios (IQR/M). IQR represents an index of the intrinsic variability of the LSM. Moreover, the operators were blinded to the clinical and biochemical data of the patients. The IQR corresponds to the interval of LSM results containing 50% of the valid measurement between the 25th and 75th percentiles. Advanced fibrosis was defined by a FibroScan ≥ 10 kPa but < 14 kPa. Cirrhosis was defined by a FibroScan ≥ 14 kPa in combination with clinical, laboratory and ultrasound parameters.
Endpoints of study
Primary endpoint was to evaluate the late occurrence rate of HCC in HCV patients with SVR after DAAs treatment schedule, defined as carcinoma onset after 48 months from SVR. Secondary end point was to evaluate the risk factors associated to late HCC occurrence. As additional end-point, a sub-analysis focused only on cirrhotic patients, to reduce any possible selection bias, assessing difference between Child A and Child B.
Statistical Analysis
Data are shown as either median or range, in the case of continuous variables or number and percentage, for categorical variables. Differences between groups have been analysed by Fisher’s exact test or Chi square test for categorical variables. Mann–Whitney U test or Kruskal–Wallis test have instead been performed to compare continuous variables. As multivariate analysis, a logistic regression with the stepwise Wald statistic input was performed.
Finally, a ROC curve analysis was built to measure the real risk of development of HCC based on liver stiffness values (kPa).
P values below 0.05 were considered statistically significant. All analyses were performed with the SPSS software (IBM, Armonk, New York), version 24.
Results
Nine hundred and eighty-five patients completed the treatment and 306 were followed-up for at least 48 months after end of treatment according to study design. Ten patients were excluded from the analysis due to incomplete follow-up data, and one patient died during the antiviral therapy (the causes of death were not related to DAAs).
Data were equally distributed among the single Centers. The baseline demographic characteristics of the enrolled population are reported in Table 1.
The median age was 67 years, and most patients were male (55.1%). Type 2 diabetes was reported in 13.3% of patients. The great majority of enrolled patients had a genotype 1 HCV infection (77.8%) and an HBV co-infection was observed in less than 2% of population. The liver stiffness median value was 21 Kpa (range 16-29). a cut-off of 22 KPa was associated with a significant increase in the risk of HCC onset (Figure 1). The presence of cirrhosis was recorded in all patients; of which 94.4% having CTP class A and 5.6% showing class B.
A SOF-based regimen was administered in 72.5% out of the patients, while ribavirin was used in 20%. All enrolled patients achieved SVR. During the follow-up, a late HCC onset was reported in 20 patients with a cumulative incidence rate of 6.55%. The pattern of HCC occurrence was heterogeneous: thirty-two patients had a nodular profile, while 3 patients developed infiltrative HCC (4 of them with macro-vascular invasion as portal vein thrombosis). No patient showed extrahepatic metastases. All patients with HCC occurrence did not show any viral relapse achieving SVR. The median diameter of the lesions was 24 mm (range 15-37 mm). None of the patients with HCC was an active alcohol consumer. Three patients (8.5%) were smokers of about 10 cigarettes/day. According to BCLC classification, patients were classified as follow: 13 patients as stage A, 4 patients as stage B, 3 patients as stage C. Among the enrolled patients, 18 out of them (90%) underwent a SOF-based treatment, and 12 of them (60%) were treated without RBV. Based on univariate analysis, CTP B stage (p 0.001), comorbidity of diabetes (p 0.007), presence of cirrhosis (p 0.002), and liver
stiffness value (p 0.0001) were significantly associated with HCC occurrence. At multivariate analysis we found that liver stiffness, diabetes, BMI as well as platelet levels before antiviral therapy were factors related to late HCC occurrence (Table 2).
Discussion
The pathogenesis and natural history of HCV are characterized by several factors, including immune system activity with regulatory and effector environments since the early phase of infection (18-19). Chronic infection underlies a persistent activity of immune system with a specific cytokines environment that leads to a liver necro-inflammation and then to HCC onset that may still occur over the years as previously suggested (20-21), due to the continuous damage of inflammation and related fibrosis (22).
Indeed, in interferon-based regimens, the significant reduction of HCC incidence but not its disappearance in those with viral clearance have been associated to several factors including: the cirrhotic persistence architecture, advanced age, presence of latent mutations of HCV, presence of comorbidities such as diabetes, and the consumption of alcohol and tobacco (11-12, 23-24). The approval of second wave DAA is a recent event and it still does not allow a long-term assessment of the impact of SVR on HCC incidence. This is independent, spontaneous, real-life study on a long term follow-up aimed to verify disease natural history after viral clearance. Our findings showed that late HCC may occur after viral clearance and that interestingly, this association with neoplastic onset seems to be strongly occurring in CTP A patients, suggesting that fibrosis could not be the only factor possibly associated to HCC occurrence in this setting of patients. Intriguingly all HCC cases were in those treated with an antiviral SOF-Based regimen, while more enigmatically no HCC developed in those not achieving SVR. Therefore, SVR by DAAs does not seem to completely prevent the occurrence of late HCC recurring. These findings, theoretically, should not occur since the carcinogenic effect of HCV proteins is related to necroinflammation in the presence of active viral replication, which deregulate host cell cycle checkpoints and the virus and immune-mediated oxidative stress leading to DNA mutations in liver cells (25-26). Despite this scientific evidence, mechanisms related to the late HCC occurrence are still unclear even considering possible pathogenetic models that could explain the possible reason of the onset of late HCC in patients with SVR. Indeed, the reason why those who underwent DAAS schedule including SOF seems to be likely associated to early and late HCC may be related to several factors as the low level of immunosurveillance in patients with advanced fibrosis due to possible downregulation of interferon genes during DAA therapy, and increased cell proliferation. In absence of an appropriate checkpoints, this mechanism could promote tumor development. Therefore, according to previous data (27) and our findings on late HCC occurrence, it seems obvious that further studies are mandatory to better address the potential role of DAA therapy on long term results. In conclusion, HCC is still the most fearsome complication of cirrhosis HCV and that requires both surgical therapies with the possibility of liver transplantation and last generation drugs (28-29). In view of our findings, in addition to previous experiences as well as literature evidence, we have confirmed that the viral clearance by DAAs regimen does not remove the risk of late HCC onset. Therefore, a long-term regular clinical, laboratory and expert ultrasonography follow-up should carefully be performed also on these patients and the current Faster, Higher, Stronger approach to the new antivirals’ development should strongly consider possible late adverse events like those we have reported.
References
- Sulkowski, M.S.; Vargas, H.E.; Di Bisceglie, A.M.; Kuo, P.A.; Reddy, K.R.; Lim, J.K.; et al. Effectiveness of Simeprevir plus Sofosbuvir, With or Without Ribavirin, in Real-World Patients with HCV Genotype 1 Infection. Gastroenterology 2015, 150, 419–429. [Google Scholar] [CrossRef]
- Ioannou, G.N.; Beste, L.A.; Chang, M.F.; Green, P.K.; Lowey, E.; Tsui, J.I.; Su, F.; Berry, K. Effectiveness of Sofosbuvir, Ledipasvir/Sofosbuvir, or Paritaprevir/Ritonavir/Ombitasvir and Dasabuvir Regimens for Treatment of Patients With Hepatitis C in the Veterans Affairs National Healthcare System. Gastroenterology 2016, 151, 457–471. [Google Scholar] [CrossRef] [PubMed]
- Kwo, P.; Gane, E.J.; Peng, C.Y.; Pearlman, B.; Vierling, J.M.; Serfaty, L.; Buti, M.; Shafran, S.; Stryszak, P.; Lin, L.; Gress, J.; Black, S.; Dutko, F.J.; Robertson, M.; Wahl, J.; Lupinacci, L.; Barr, E.; Haber, B. Effectiveness of Elbasvir and Grazoprevir Combination, With or Without Ribavirin, for Treatment-Experienced Patients With Chronic Hepatitis C Infection. Gastroenterology 2017, 152, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Mariño, Z.; Perelló, C.; Iñarrairaegui, M.; Ribeiro, A.; Lens, S.; Díaz, A.; Vilana, R.; Darnell, A.; Varela, M.; Sangro, B.; Calleja, J.L.; Forns, X.; Bruix, J. Unexpected early tumor recurrence in patients with hepatitis C virus –related hepatocellular carcinoma undergoing interferon-free therapy: A note of caution. J Hepatol 2016, 65, 719–726. [Google Scholar] [CrossRef]
- Cardoso, H.; Vale, A.M.; Rodrigues, S.; et al. High incidence of hepatocellular carcinoma following successful interferon-free antiviral therapy for hepatitis C associated cirrhosis. J Hepatol 2016, 65, 1070–1071. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, L.; Perrella, A.; Guarino, M.; De Luca, M.; Piai, G.; Coppola, N.; Pafundi, P.C.; Ciardiello, F.; Fasano, M.; Martinelli, E.; Valente, G.; Nevola, R.; Monari, C.; Miglioresi, L.; Guerrera, B.; Berretta, M.; Sasso, F.C.; Morisco, F.; Izzi, A.; Adinolfi, L.E. Incidence and risk factors of early HCC occurrence in HCV patients treated with direct acting antivirals: A prospective multicentre study. J Transl Med. 2019, 17, 29. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B.; Kanwal, F.; Richardson, P.; Kramer, J. Risk of hepatocellular carcinoma after sustained virological response in Veterans with hepatitis C virus infection. Hepatology. 2016, 64, 130–137. [Google Scholar] [CrossRef]
- Nahon, P.; Bourcier, V.; Layese, R.; et al. Eradication of hepatitis C virus infection in patients with cirrhosis reduces risk of liver and non-liver complications. Gastroenterology. 2017, 152, 142–156. [Google Scholar] [CrossRef]
- Alazawi, W.; Cunningham, M.; Dearden, J.; Foster, G.R. Systematic review: Outcome of compensated cirrhosis due to chronic hepatitis C infection. Aliment Pharmacol Ther 2010, 32, 344–355. [Google Scholar] [CrossRef]
- Fattovich G, Pantalena M, Zagni I et al. Effect of hepatitis B and C virus infections on the natural history of compensated cirrhosis: A cohort study of 297 patients. Am J Gastroenterol 2002, 97, 2886–2895. [Google Scholar] [CrossRef]
- D’Ambrosio, R.; Della Corte, C.; Colombo, M. Hepatocellular Carcinoma in Patients with a Sustained Response to Anti-Hepatitis C Therapy. Int. J. Mol. Sci. 2015, 16, 19698–19712. [Google Scholar] [CrossRef] [PubMed]
- Morgan, R.L.; Baack, B.; Smith, B.D.; Yartel, A.; Pitasi, M.; Falck-Ytter, Y. Eradication of hepatitis C virus infection and the development of hepatocellular carcinoma: A meta-analysis of observational studies. Ann Intern Med. 2013, 158, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Kanwal, F.; Khaderi, S.; Singal, A.G.; Marrero, J.A.; Loo, N.; Asrani, S.K.; Amos, C.I.; Thrift, A.P.; Gu, X.; Luster, M.; Al-Sarraj, A.; Ning, J.; El-Serag, H.B. Risk factors for HCC in contemporary cohorts of patients with cirrhosis. Hepatology 2023, 77, 997–1005. [Google Scholar] [CrossRef] [PubMed]
- Associazione Italiana per lo Studio del Fegato. Documento di indirizzo dell’Associazione Italiana per lo Studio del Fegato per l’uso razionale di antivirali diretti di seconda generazione nelle categorie di pazienti affetti da epatite C cronica ammesse alla rimborsabilità in Italia. Available at webaisf.org/pubblicazioni/documento-aisf-hcv-2016.aspx.
- Boursier, J.; Zarski, J.P.; de Ledinghen, V.; Rousselet, M.C.; Sturm, N.; Lebail, B.; Fouchard-Hubert, I.; Gallois, Y.; Oberti, F.; Bertrais, S.; Calès, P.; Multicentric Group from ANRS/HC/EP23 FIBROSTAR Studies. Determination of reliability criteria for liver stiffness evaluation by transient elastography. Hepatology 2013, 57, 1182–1191. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver, European Organisation for Research and Treatment of Cancer. EASL-EORTC clinical practice guidelines: Management of hepatocellular carcinoma. J Hepatol 2012, 56, 908–943. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Reig, M.E.; de Lope, C.R.; Bruix, J. Current strategy for staging and treatment: The BCLC update and future prospects. Semin Liver Dis 2010, 30, 61–74. [Google Scholar] [CrossRef]
- Buchanan, R.; Hydes, T.; Khakoo, S.I. Innate and adaptive genetic pathways in HCV infection. Tissue Antigens. 2015, 85, 231–240. [Google Scholar] [CrossRef]
- Shi, J.; Li, Y.; Chang, W.; Zhang, X.; Wang, F.S. Current progress in host innate and adaptive immunity against hepatitis C virus infection. Hepatol Int. 2017. [CrossRef]
- Perrella, A.; Sbreglia, C.; Atripaldi, L.; Esposito, C.; D'Antonio, A.; Perrella, O. Rapid virological response in peripheral blood mononuclear cells with an increase of hepatitis C virus-specific interferon-gamma production predisposes to sustained virological response in patients with chronic hepatitis C genotype 1 undergoing treatment with pegylated-interferon alpha 2a plus ribavirin. Scand J Gastroenterol. 2010, 45, 250–255. [Google Scholar]
- van der Ree, M.H.; Stelma, F.; Willemse, S.B.; Brown, A.; Swadling, L.; van der Valk, M.; Sinnige, M.J.; van Nuenen, A.C.; de Vree, J.M.L.; Klenerman, P.; Barnes, E.; Kootstra, N.A.; Reesink, H.W. Immune responses in DAA treated chronic hepatitis C patients with and without prior RG-101 dosing. Antiviral Res. 2017, 146, 139–145. [Google Scholar] [CrossRef]
- Yue, M.; Deng, X.; Zhai, X.; Xu, K.; Kong, J.; Zhang, J.; Zhou, Z.; Yu, X.; Xu, X.; Liu, Y.; Zhu, D.; Zhang, Y. Th1 and Th2 cytokine profiles induced by hepatitis C virus F protein in peripheral blood mononuclear cells from chronic hepatitis C patients. Immunol Lett. 2013, 152, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Hou, X.J.; Ye, F.; Li, X.Y.; Liu, W.T.; Jing, Y.Y.; Han, Z.P.; Wei, L.X. Immune response involved in liver damage and the activation of hepatic progenitor cells during liver tumorigenesis. Cell Immunol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Werner, J.M.; Adenugba, A.; Protzer, U. Immune Reconstitution After HCV Clearance With Direct Antiviral Agents: Potential Consequences for Patients With HCC? Transplantation. 2017, 101, 904–909. [Google Scholar] [CrossRef] [PubMed]
- Aroucha, D.C.; do Carmo, R.F.; Moura, P.; Silva, J.L.; Vasconcelos, L.R.; Cavalcanti, M.S.; Muniz, M.T.; Aroucha, M.L.; Siqueira, E.R.; Cahú, G.G.; Pereira, L.M.; Coêlho, M.R. High tumor necrosis factor-α/interleukin-10 ratio is associated with hepatocellular carcinoma in patients with chronic hepatitis C. Cytokine. 2013, 62, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Lemon, S.M.; McGivern, D.R. Is hepatitis C virus carcinogenic? Gastroenterology 2012, 142, 1274–1278. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi L, Di Francia R, Coppola N, Guerrera B, Imparato M, Monari C; et al. Hepatocellular carcinoma in HCV cirrhosis after viral clearance with direct acting antiviral therapy: Preliminary evidence and possible meanings. WCRJ. 2016, 3, e748. [Google Scholar]
- Valente, G.; Rinaldi, L.; Sgambato, M.; Piai, G. Conversion from twice-daily to once-daily tacrolimus in stable liver transplant patients: Effectiveness in a real-world setting. Transplant Proc. 2013, 45, 1273–1275. [Google Scholar] [CrossRef]
- Caturano, A.; Galiero, R.; Vetrano, E.; Giorgione, C.; Mormone, A.; Rinaldi, M.; Marfella, R.; Sasso, F.C.; Rinaldi, L. Current hepatocellular carcinoma systemic pharmacological treatment options. WCRJ 2023, e2570. [Google Scholar]
Figure 1.
ROC curve describing the discriminant power of the liver stiffness value (kPa) on the risk of developing late HCC in cirrhotic patients [n=306, AUROC score = 0.646, 95% C.I.: 0.519 – 0.774]. The p value for the significance of liver stiffness on the risk of HCC was 0.029 (Kruskal–Wallis test).
Figure 1.
ROC curve describing the discriminant power of the liver stiffness value (kPa) on the risk of developing late HCC in cirrhotic patients [n=306, AUROC score = 0.646, 95% C.I.: 0.519 – 0.774]. The p value for the significance of liver stiffness on the risk of HCC was 0.029 (Kruskal–Wallis test).
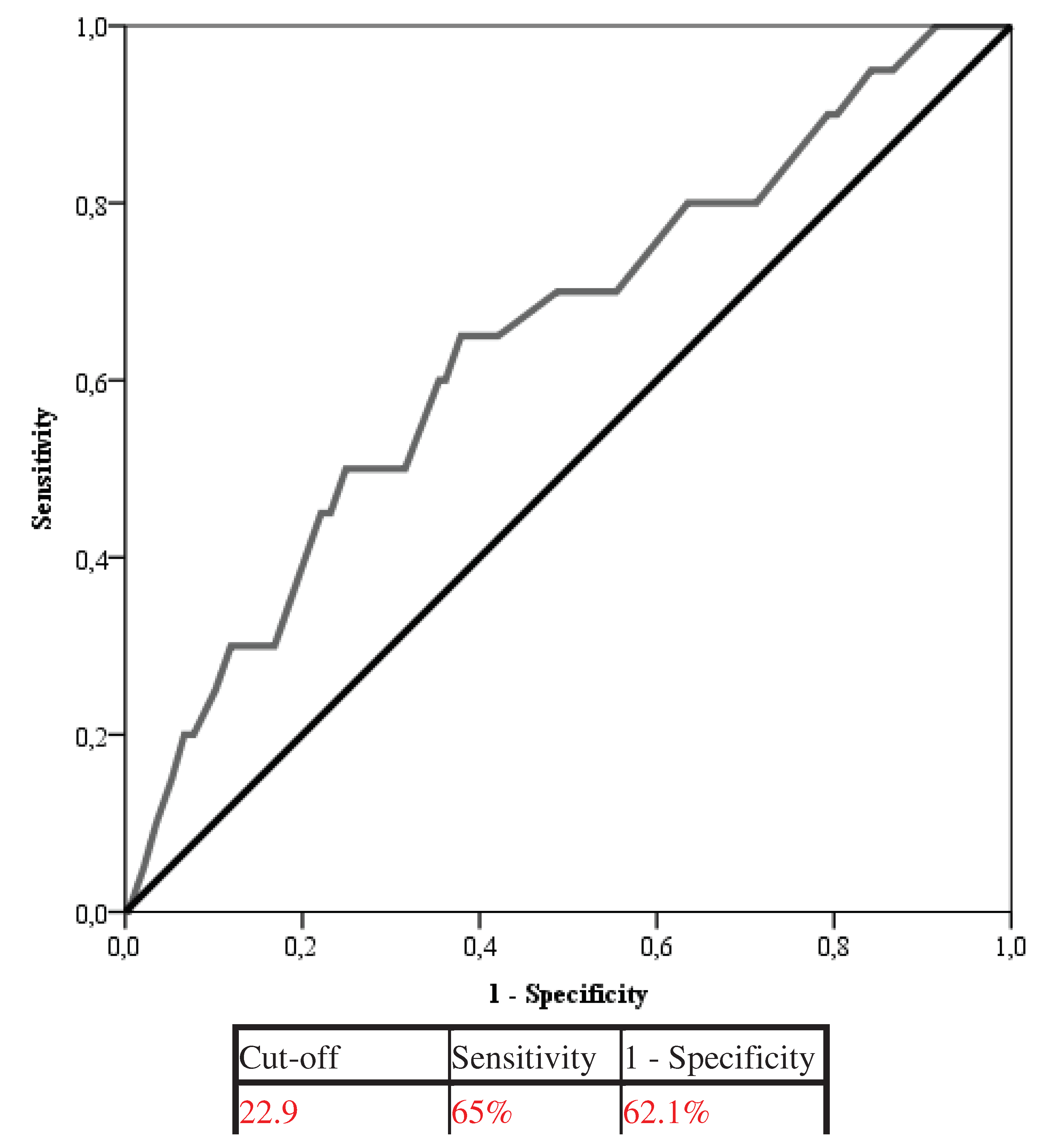

Table 1.
Baseline characteristics of the entire cohort of study (n = 306).
| Parameter | |
|---|---|
| Age (yrs.), median [IQR] | 67 [60 – 73] |
| Sex, n (%) Male Female |
165 (53.9) 141 (46.1) |
| BMI, median [IQR] | 26.1 [24.3 – 28] |
| Smoke, n (%) | 2 (0.7) |
| Potus, n (%) | 2 (0.7) |
| Diabetes, n (%) | 59 (19.3) |
| Metabolic syndrome, n (%) | 22 (7.2) |
| Number of lesions, n (%) 0 1 ≥2 |
286 (93.5) 15 (4.9) 5 (1.6) |
| Portal invasion, n (%) | 5 (1.6) |
| Bright liver, n (%) | 22 (7.2) |
| Liver stiffness (kPa), median [IQR] | 21 [16 – 29] |
| Duration of therapy, median [IQR] | 12 [12 – 24] |
| Platelets, median [IQR] T0 SVR12 |
108000 [73000 – 153000] 103500 [65250 – 122000] |
| Genotype, n (%) 1 2 3 4 |
243 (79.4) 50 (16.3) 11 (3.6) 2 (0.7) |
| Child-Pugh Score T0, n (%) A B |
289 (94.4) 17 (5.6) |
| Child-Pugh Score SVR12, n (%) A B |
298 (97.4) 8 (2.6) |
| Therapy, n (%) Sofosbuvir Sofosbuvir/Ledipasvir Sofosbuvir/Daclatasvir Sofosbuvir/Simeprevir 3D |
80 (26.1) 69 (22.5) 23 (7.5) 50 (16.3) 84 (27.5) |
| Late HCC, n (%) | 20 (6.5) |
* Data are expressed ad either number and percentage or median and interquartile range (IQR).
Table 2.
Baseline Characteristics of Cirrhotic Patients According to late HCC Development: univariate and multivariate analysis (n = 306).
Table 2.
Baseline Characteristics of Cirrhotic Patients According to late HCC Development: univariate and multivariate analysis (n = 306).
| Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|
| HCC | |||||
| Parameter | Yes (n = 20) | No (n = 286) | P | O.R. [95% C.I.] | p |
| Age (yrs), median [IQR] | 70 [68.2 – 75] | 67 [59.5 – 72] | 0.026 | ||
| Sex, n (%) M/F |
15 (75)/5 (25) |
150 (52.4)/136 (47.6) |
0.050 | ||
| BMI, median [IQR] | 25 [23.2 – 26.7] | 26.2 [24.7 – 28.4] | 0.026 | 0.712 [0.537 – 0.943] | 0.018 |
| Smoke, n (%) | 2 (10) | 0 (-) | 0.000 | ||
| Potus, n (%) | 2 (10) | 0 (-) | 0.000 | ||
| Diabetes, n (%) | 9 (45) | 50 (17.5) | 0.003 | 0.180 [0.045 – 0.713] | 0.015 |
| Metabolic syndrome, n (%) | 3 (15) | 19 (6.6) | 0.162 | ||
| Liver stiffness (kPa), median [IQR] | 26.5 [18 – 44.5] | 20.4 [16 – 28.7] | 0.028 | 1.070 [1.020 – 1.122] | 0.006 |
| Duration of therapy (months), median [IQR] | 12 [12 – 12] | 12 [12 – 24] | 0.007 | ||
| Platelets, median [IQR] T0 SVR |
75000 [48000 – 109500] n.a. |
115000 [80000 – 166000] n.a. |
0.001 n.a. |
0.975 [0.954 – 0.996] |
0.019 |
| Genotype, n (%) 1 2 3 4 |
15 (75) 3 (15) 1 (5) 1 (5) |
228 (79.7) 47 (16.4) 10 (3.5) 1 (0.3) |
0.095 |
0.007 [0.000 – 0.417] 0.003 [0.000 – 0.280] |
0.017 0.012 |
| Number of lesions, n (%) 0 1 ≥2 |
0 (-) 15 (75) 5 (25) |
286 (100) 0 (-) 0 (-) |
0.000 | ||
| Portal invasion, n (%) | 4 (11.4) | 0 (-) | 0.000 | ||
| Bright liver, n (%) | 1 (5) | 21 (16.8) | 0.172 | ||
| Child-Pugh Score T0, n (%) A B |
15 (75) 5 (25) |
274 (95.8) 12 (4.2) |
0.000 | ||
| Child-Pugh Score SVR12, n (%) A B |
17 (85) 3 (15) |
281 (98.3) 5 (1.7) |
0.000 | ||
| Therapy, n (%) Sofosbuvir Sofosbuvir/Ledipasvir Sofosbuvir/Daclatasvir Sofosbuvir/Simeprevir 3D |
16 (80) 0 (-) 1 (5) 1 (5) 2 (10) |
64 (22.4) 69 (24.1) 22 (7.7) 49 (17.1) 82 (28.7) |
0.000 | ||
* Data are expressed ad either number and percentage or median and interquartile range (IQR).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



