
Submitted:
03 September 2023
Posted:
05 September 2023
You are already at the latest version
Abstract
The main aim of this study is to examine the effects of Total Quality Management (TQM) practices (leadership of management, decision making, continuous improvement, customer focus, employee involvement, process management and relations with suppliers) on the financial and operational performance of hospitals in service industry. The data of the study were collected by the questionnaire prepared in the light of published studies and the suggestions of medical and administrative staff. Medical and administrative staff were chosen as target participants that reflect perspectives of hospitals. 1069 questionnaires were answered in 6 private and 26 public hospitals in the Marmara region in Turkey. The results claim that “customer focus” affects both operational performance as well as the financial performance of hospitals more than other TQM practices. While “process management” and “customer focus” explain the variance of financial performance significantly. “Process management” does not explain variance of operational performance.
Keywords:
total quality management
; performance
; hospitals
; structural equation modelling
1. Introduction
There has been scant empirical research on the multidimensional perspective of TQM [1]. Success of total quality management practices are confirmed in the manufacturing industry. Commitment of top management, employee involvement, data driven performance, understanding variation, continuous improvement contribute to assure quality as a result of interdependent processes [2]. Despite these positive outcomes, implementation of these practices in the healthcare industry are hesitating. Lack of standard uniform product in healthcare, lack of an assembly line in healthcare, difference in cultural setting, difficulty of measuring or defining healthcare quality, belief that higher quality would lead to higher cost are some of the reasons of this hesitation [2].
On the other hand, it is rather difficult to have satisfied customers in hospitals. This is because evaluating the quality of health care services might be perceived as more complex and risky. Reasons of these difficulties to evaluate quality of healthcare services can be ordered as; firstly, the intangible nature of healthcare services make it difficult to determine customer expectations. Secondly, the skills and manners of employees who offer service to customers are evaluated as important criteria [3]. Thirdly, customers may not have technical expertise to assess the service quality in the hosptial. Some participants take into consideration the price of health services to evaluate quality. Some participants consider the level to which his or her health recovers [4]. Another evaluation criterion in the sight of customers is that a good doctor or nurse is expected to be competent, courteous, empathetic and expected to communicate and relate well to [5]. These service characteristics can be decisive among customers when they are choosing a healthcare [6]. As such, the involvement of many participants with different interests makes it difficult to define quality.
Although there are concerns about quality in the healthcare industry, increased importance of quality in the healtcare industry lead to occurence of various methods to assure quality in the hospitals. Quality in the healthcare industry is improved and audited with different methods like accredition, continuous professional development, clinical audit, peer reviews [7]. Providing service quality concluded with positive effects on patient satisfaction and productivity. Awareness of organizations regarding these positive outcomes make quality issues more attractive.
Although evaluating the quality of health care services might be perceived as more complex and risky, implementing TQM becomes indispensable for hospitals to have competitive advantage and satisfied customers. Creating new products/services and delivering them to customers, better and faster than any other competitors, at a lower cost and higher quality are the proofs of competitive advantage. Other factors such as controlling costs, improving productivity, structuring flexible human resources, applying new technologies, and maintaining continuous improvement protect the competitive situation of hospitals [8].
In addition to role of implementing TQM to have competitive advantage, competition among hospitals trigger to represent quality in their services. In the US, England and the Netherlands, there has been significant attention paid to the potential for hospital competition to drive increases in quality and efficiency. According to wider economic theory gives a clear response: under a fixed regime, competition will improve quality. Like to previous work from Kessler and Geppert [9], Cooper et al. [10] supported that to current efforts in England to increase the amount of publicly available information on quality and promote hospital competition.
The aim of this study is to examine the effects of TQM practices (management leadership, decision making, continuous improvement, customer focus, employee involvement, process management, and supplier relationships) on the financial, operational performance of hospitals. Also the effect of operational performance on financial performance is investigated. Hospitals are determined as a field to examine. Because, they have different systems than manufacturing industries. Even, they are diffeent than some of the other service industries like finance and education. Health care services consist of interconnected processes and these processes can be separated into distinct processes [2]. In addition, hospitals have more complex organizational culture dominated by physicians and professional power [11]. Implementation of TQM practices within these processes and complexity may represent different findings.
In addressing these objectives, we emphasized service quality and its importance for hospitals. Then, TQM practices and performance dimensions were discussed depending on a literature review. Second, a theoretical framework and hypotheses were proposed that enable us to determine the effects of TQM on hospitals. In the research methodology section, basic information related to sampling, data collection, and the measurement instrument were given. Analysis procedure started with exploratory factor analysis to reveal the items related with the variables. After testing the validity and reliability of the variables, confirmatory factor analysis was used to test the fitness of the model. Finally, conclusions and discussions were shared.
2. Materials and Methods
Literature review and hypotheses development
Forces such as upgrading standards of living and education, competitive pressures, medical advancements, alternative healthcare delivery mechanisms, changing cost structures, monitoring by public and private groups, increased information availability, and better informed customers make it necessary to reevaluate strategies for hospitals [12]. Additionally, strengthening positions of the customers, increasing awareness on patient safety put pressure on hospitals to improve the efficieny in line with cost effectiveness and quality of care [11]. While hospitals are attempting to be in more powerful position, they search for different processes. TQM practices with their positive effects on customer satisfaction and competitive advantage have potential to response their needs.
At the initial stage of applying industrial model of quality to health care, professionals and managers consider that the concept of quality management has been beneficial for manufacturing industry. They believed, that it may not be beneficial for the hospital context. In particular, “zero defects” and “statistical process control” techniques have been given as reasons of difficulties of using. Applicability of quality management in the hospitals is encouraged in different studies by emphasizing different alternatives to implement and evaluate quality. Tomes and Peng [5] stated that patient satisfaction in addition to medical care and technical aspects should be added to define, implement and evalute quality. Rodger, Pendharkar and Paper [13] indicated measurements should include appropriateness, continuity, effectiveness, efficacy, efficiency, timeliness, availability, respect and caring, and safety. Nilsson, Johnson and Gustafsson [14] advocated that many services are individually intensive and they should be adaptable to very distinct needs.
Hospitals should be aware of the definition of the service quality firstly. Service quality is defined as the difference between customer expectations and customer perceptions [3,15,16]. Historically, the quality of a hospital defined in terms of the technical delivery of its care. Recently, however, patients’ perceptions and expectations play an important role on the quality of hospitals [17,18]. Service quality of hospitals has been distinguished into two categories [16]: technical quality and functional quality. Technical quality relates to the clinical and operating skills of doctors’, nurses’ familiarity with drugs, and laboratory technicians’ expertise. Functional quality is evaluated through which medical care is delivered such as the communication skills of the staff, the facilities, cleanliness, and the quality of food [3,6,16].
Indispensability of implementing TQM is studied in the literature by emphasizing its benefits. Douglas and Judge [19] confirmed that the greater degree of TQM practices, the greater probability of improving organizational performance. To measure and improve quality, some TQM practices are included in the literature. The decision regarding which management practices should be included for effective TQM implementation is a field of study. Wardhani et al. [11] examined 533 publication. Organizational culture, design, leadership for quality, physician involvement, quality structure and technical competence are indicated as supportive factors of TQM implementation in hospitals [11]. Sureshchander et al. [20] defined critical quality practices for service organizations as top management commitment, human resource management, technical system, information and analysis system, benchmarking, continuous improvement, customer focus, employee satisfaction, union intervention, social responsibility,service scapes, service culture. Yang [21] mentioned similar content that includes customer focus, continuous improvement, employees participation, teamwork, process focus, systemization, empowerment, leadership.
After we thoroughly reviewed the literature, the TQM practices included in our study are management leadership, employee involvement, decision making, supplier relationships, process management, customer focus, and continuous improvement based on the ISO 9001:2000 quality assurance system. Although not exhaustive, these factor areas have often been considered the critical factors of TQM [22,23,24]. Also, these practices have “synergistic” effect for successful TQM implementation [7] (p.544).
Research model firstly indicates these critical practices to conduct TQM successfully. And then, effects of these practices on operational performance and financial performance are investigated separately. Lastly, relationship between operational performance and financial performance is interrogated. Prior to explain hypotheses about these relationships, each of the TQM practices and their outcomes explained under this title.
Management leadership
Management leadership has an important role on implementation of TQM as stated by quality gurus [25,26]. Puffer and McCarthy [27] provided a framework for evaluating leadership in a TQM context and claimed that creating a vision and promoting change is an essential talent for top management to implement TQM successfully. For quality management, managers should put aside their traditional administrative status and become leaders who define goals and who direct the quality initiative in the right path [28].
Implementing TQM practices as strategy increases the role of leaders to execute these TQM strategies. Because leadership is related to quality planning, human resource management, learning and customer focus [29]. If managers want to manage these practices effectively, leadership is the primary key [30]. Leaders may influence the behavior of people to adopt new practices necessary for TQM. Motivated, persuaded employees by leaders are considerable in the service industry as in the hospitals. Service is executed by employees. Motivated, persuaded employees in hospitals with leadership skills of managers contributes to operational and financial performance. As stated by Mosadeghrad [7] leadership positively influence implementation of TQM practices successfully.
Decision making
Decision making is one of the major responsibilities of management and requires selecting from alternatives. Decision makers choose alternatives to realize organizational goals, strategic objectives, and adapt to the external environment. Service intangibility, however, makes it difficult to make decisions on how consumers perceive services and service quality. When a service provider knows how the consumer will evaluate the service, they will be able to suggest how to influence these evaluations in the desired direction [3]. Lee et al. [31] stated that the most important contributing factor for quality improvement in Korean hospitals is the use of scientific decision making procedures.
In TQM, the decision-making process does not belong simply to managers, but employees also play a role in this process. Participating in decision making can speed up the process, and this speed can affect different performance criteria in a positive way [32]. Operational and financial performance are some of them. Organizations face many managerial and adoption problems through TQM implementations. They should define their priorities to allocate their resources. Good decision making facilitates to solve problems, allocate resources and accomplish the goals [30]. Hospitals that race against time for the health of people, give importance to solve problems, choose the best. If they have well structured decision making processes, these processes contributes to execute different TQM practices within the organization.
Process management
Ittner and Larcker [33] (p.523) explained, “A process is a set of activities that, taken together, produce a result of value to a customer”. A process thus leads to actions as a structure. And, this structure should produce value that improves efficiency and thus result in satisfied customers [14,34]. Process management is very important for quality management system. Because, building processes means that leaders, individuals and teams day by day try to practice the needed values and competencies based on the principle of continuous improvement and the company’s mission, vision, goals and strategies [35].
Service process in the hospital context differs from manufacturing. However; this is because it includes complex and high-level interactive procedures, which are supervised by the customer. Employees, customers, and managers are part of this process. Thus, process orientations have a significant and direct impact on customers’ satisfaction with services [14,36]. Well managed processes may conclude with high operational quality performance. Sustainability of the operational and quality performance also intensively depend on process management. Because process management provides structure to represent same quality service any time.
Continuous improvement
Quality assessment is a process that requires consideration and continuous attention [17]. Therefore, continuous improvement is one of the significant elements of quality management. It is defined by Daft [30] (p.49) as “ the implementation of small incremental improvements in all areas of the organization on an ongoing basis”. Continuous improvement mean never-ending attention to detail, which reduces the effort and time that it takes to conduct operations [34].
Organizations must update their quality processes based on technical and administrative activities. Hospitals that aim to have long term success in the health care sector, should adopt main philosophy of continuous improvement. Improving things a little bit at a time, all the time contributes to high performance success [30]. Undeniable importance of continuous improvement programs appeared on the better performance results [8,37].
Employee involvement
Through the continuous improvement process, employees’ acceptance of responsibility is another requirement [38,39]. Widening boundaries of authority for employees contributes to their acceptance of responsibility [39]. At that point top management’s attempt to attract employees’ attention to the philosophy of quality management is essential [40].
Involving the employees through the TQM implementation process is an indispensable necessity for organizations [41]. As emphasized in the cited studies, healthcare management should begin to improve service quality by involving and adapting their employees in any quality programs and strategies [4,5,36,38]. They have an important role in quality management success in service industry [7,42]. Management literature discusses that the behavioral traits of employees can play an important role in the success of total quality management (TQM). However, little empirical research exists in this regard [43]. Failure on employees involvement to quality pratices may conclude with failure on all TQM practices. Especially in the service industries, managing employees requires more care. Employees are the face of organizations that encounter the customer directly. If they do not feel that their organization gives value to their suggestions, knowledge and experiences, their intention to represent their full potential to implement TQM practices will decrease.
Relations with suppliers
Producing quality products depends on the timely delivery of quality materials and suppliers who are devoted to quality and continuous improvement. From the supplier’s point of view, it is essential to meet the buyer’s specifications and standards for quality [44,45,46].
Kannan and Tan [47] indicated that managing the supply chain effectively can drive the decline in lead times and material costs and increase improvements in product quality and responsiveness. Krause, Handfield and Scannell [48] posited that to have a source of competitive advantage, suppliers’ performance must be managed and adapted to meet the buying firms’ needs. Close relationships with suppliers must be facilitated to fulfill this process. This also increases the possibility that the provider and the supplier are working toward the same goal based on the principles of total quality management. Effective supplier management enhances the quality of purchased products, reduces the cost [7] and positively influences process management [49]. A hospital may use hundreds of suppliers to conduct the service. Cooperative relationships with suppliers leads to lower cost, higher quality and faster service in the healthcare industry. Benefits of close relationships with suppliers can be seen on the operational and financial performance of hospitals.
Customer focus
To run a business more efficiently, organizations should include customers in all improvement processes. This provides added value and enhances long-term customer relationships [50]. Zineldin [50] demonstrated that a company must create a triangular relationship among quality, customer relationship management, and customer loyalty for better position in a competitive marketplace. Samson and Terziovski [51] found that customer focus is one of the strongest antecedents of organizational performance.
Patients that acquire services from the hospital are customers. Wu and Chan [52] defended perceived service quality by customer has a major impact on the purchase decisions and sustainability of business operations. Factors such as minimal waiting time, flexible operating hours, staff availability, and cost effective treatment, however, do not automatically lead to satisfied patients. Dimensions of patient satisfaction also include reliability, responsiveness, assurance, empathy, and other tangibles that contribute to improve the quality of service [53].
Evaluating the quality of service and getting feedback from customers, however, are difficult in hospitals. Lack of mechanisms for measuring satisfaction and low levels of information from customers about healthcare services create a performance evaluation problem [38]. Defining necessities and expectations of customers, measuring their satisfaction, getting their feedback lead organizations to improve quality of services [7]. An effective customer database, for example, helps hospitals understand customer needs and demands and also differentiate it from competitors. When hospitals develop solutions to find out what customers want and need, customer focus orientation may conclude with better financial performance.
Operational performance
Parkan and Wu [54] defined operational performance as a concept that defines how well a production unit uses its resources when converting them into output. To compare the relative operational performance of product unit may involve activities that have implications for consuming and generating resources. Organizations have operational goals in addition to their strategic goals like deliveries on time, fewer mistakes, less waiting time [30]. TQM practices enable to reach operational goals and increase operational performance. Samson and Terziovski [51] (p.393) explained “the categories of leadership, customer focus and management of people were the strongest significant predictors of operational performance”.
This study supposes that TQM practices affect the operational performance positively. Leadership, decision making, process management, continuous improvement, employee involvement, supplier relations, and customer focus create potential for well production unit based on organizational resources. This is because TQM practices create value, time-based competition, quality, and low prices, all of which are required for competition. Factors such as fewer mistakes, fewer delays, and less rework, increase productivity. Preventing the cost of fatal mistakes will also create competitive advantage, especially in hospitals [49,55]. With these assumptions, the following hypothesis is proposed:
H1: There is a positive relationship between “TQM practices (management leadership, decision making, process management, continuous improvement, employee involvement, relations with suppliers, customer focus)” and “operational performance”in hospitals of service industry
Financial performance
Organizations define goals to accomplish mission and create optimal value. One of these goals are related to financial performance. High revenues in existing and new markets, high productivity and efficiency are indicators of financial performance [30].
Although some organizations have cancelled TQM practices because of their negative impact on profits [56], TQM practices have potential to increase financial performance. Customer satisfaction has been shown to lead to positive financial performance [38,57,58,59]. Satisfied customers will contribute to profitability through increased spending and word of mouth communication [15,60,61]. Likewise, customer dissatisfaction leads to consumer complaints and negative word of mouth. These behaviors reduce business volume within the organization [15].
On the other hand, operationally well worked hospitals contributes to customer satisfaction with fewer mistakes, less waiting time, less rework. Improvements on operational performance of hospitals show its benefit on customer satisfaction. To be preferred hospital by customers creates improvement on financial performance.
In line with the aim of this study, TQM principles such as low costs, high quality, speedy service, and customer satisfaction, however, absolutely influence financial performance. In this context, we propose the following hypotheses:
H2: There is a positive relationship between “TQM practices (management leadership, decision making, process management, continuous improvement, employee involvement, relations with suppliers, customer focus)” and “financial performance” in hospitals of service industry
H3: There is a positive relationship between “operational performance” and “financial performance” in hospitals of service industry
3. Results
Research methodology
This section provides an overview of the research model, measurement instruments, sampling process, collecting data and analyzing.
The nature of the research
Research model of this study examines the effects of TQM practices (management leadership, decision making, process management, continuous improvement, employee involvement, supplier relations, and customer focus) on operational performance and financial performance of hospitals as illustrated in (Figure 1).
Based on the research model, hospitals that implement TQM practices will have chance to increase their financial performance in accordance with their operational performance.
Measurement instrument for TQM practices
Although many studies have examined total quality management, we found that no measurement instrument has validity and reliability of all components of TQM that we describe here. To fill this gap, we did not use a measurement instrument from any single study, but preferred to create a unique one.
To construct the measurement instrument, we applied the methodology to develop measurement scales in social sciences [62]. In general, the procedure that allows one to move from the concept to its measurement requires a four-stage process: 1) literary definition of the concept, 2) specification of dimensions, 3) selection of observed indicators, and 4) synthesis of indicators or elaboration of indexes.
TQM practices that were determined as management leadership, decision making, process management, continuous improvement, employee involvement, supplier relations and customer focus were derived from the quality management principles based on the ISO 9001:2000 quality assurance system.
To measure these TQM practices, items were generated based on the literature and interview with people from the healthcare industry. In determining questionnaire items from the literature, some questions were not applicable to implementing TQM for hospitals, as they were used in research for industrial context. Therefore, a group consisting of doctors, nurses, and administrative employees of hospitals brainstormed ways in which the questions could be integrated into the hospital context. Their experiences and notions contributed to the process of preparing the questionnaire.
Management leadership factor items were customized from the studies of Cua, McKone and Schroeder [63]; decision-making factor items were adapted from Cua et al. [63], Fuentes-Fuentes et al. [64], Saraph, Benson and Schroeder [65]; process management factor items were taken from the studies of Cua et al. [63], Kaynak [49]; continuous improvement factor items were drawn from the studies of Kaynak [49], Rahman and Bullock [66], Fuentes-Fuentes et al. [64]; employee involvement factor items were adapted from the studies of Cua et al. [63], Rahman and Bullock [66], Fuentes-Fuentes et al. [64]; supplier relations factor items were drawn from the studies of Kannan and Tan [47], Rahman and Bullock [66] and customer focus factor items were adapted from the studies of Rahman and Bullock [66], Fuentes-Fuentes et al. [64], Chong and Rundus [67].
Effects of TQM practices on performance was evaluated in two dimensions as operational performance and financial performance. Operational performance factor items were adapted from the studies of Kaynak [49] and Fuentes-Fuentes et al. [64], whereas financial performance factor items were taken from the studies of Fuentes-Fuentes et al. [64]. Fifty items were assessed using a 5-point Likert scale. Respondents indicated their disagreement (1 = strongly disagree) or agreement (5 = strongly agree) on TQM practices, operational and financial performance of hospitals.
Sample demographics
The sample of this study includes administrative and medical employees of hospitals. The cross-sectional survey methodology was implemented in 32 hospitals. To increase the response rate, the confidentiality of the responses was guaranteed. A total of 1,069 questionnaires were correctly completed and collected from 26 public and 6 private hospitals.
Among these, 69,1% (739) of the employees were from the public hospitals, and 30,9% (330) of the employees were from private hospitals. The size of these hospitals ranged from 50-2,300 employees. Approximately 71,6% (765) of the respondents were positioned in hospitals that employed 200-1,100 employees. These hospitals served in both regional (35,5%) and national (63,3%) areas.
Statistical analysis
For analysis, we used the statistic software program AMOS 5.0. First, all of the 50 items were included in the analysis to form a scale of TQM practices, financial, performance, and operational performance. We referred to Cronbach’s alpha to assure reliability of variables. As a result of the analysis, the Cronbach’s alpha value was high at 0,925. Second, we looked at the corrected inter-item correlation. It was found that the resulting values were 0,500 and above, except for one item (0,418), CF5 (“Managers and supervisors encourage patient satisfaction development activities”). According to these findings, variable CF5 was removed from the scale.
The specified structural validity of TQM practices, financial performance and operational performance instrument consisted of 49 items in nine basic components as a result of the principal component analysis. In the data reduction procedure, items having eigen-values greater than 1 were used to determine the number of factors in the data set. Principal component analysis was applied with promax rotation to identify key TQM practices, financial performance, and operational performance factors. Factor loadings of these variables that we took into account were 0,500 and above (0,630-0,964). According to the principal component analysis, the Kaiser-Meyer-Olkin measurement of sampling adequacy is 0,964.

Table 1.
Model Purification Process.
| Factor name | Reason for Elimination | CMIN/df | GFI | AGFI | NFI | IFI | TLI | CFI | RMSEA |
|---|---|---|---|---|---|---|---|---|---|
| CF5 | Eliminated in EFA | 3,937 | ,848 | ,829 | ,888 | ,914 | ,907 | ,914 | ,052 |
| PM6 | SR | 3,800 | ,859 | ,841 | ,894 | ,920 | ,913 | ,914 | ,051 |
| PM7 | SR | 3,743 | ,863 | ,845 | ,898 | ,923 | ,916 | ,923 | ,051 |
| RS1 | SR | 3,738 | ,865 | ,847 | ,900 | ,925 | ,918 | ,925 | ,051 |
| OQP1 | MI; SR | 3,503 | ,877 | ,861 | ,908 | ,932 | ,926 | ,932 | ,048 |
| OQP7 | MI; SR | 3,374 | ,884 | ,867 | ,912 | ,936 | ,930 | ,936 | ,047 |
| EI1 | MI; SR | 3,298 | ,889 | ,873 | ,915 | ,939 | ,933 | ,939 | ,046 |
| DM1 | MI; SR | 3,230 | ,895 | ,879 | ,919 | ,943 | ,937 | ,943 | ,046 |
| OQP2 | MI; SR | 3,072 | ,902 | ,886 | ,924 | ,948 | ,942 | ,948 | ,044 |
| L1 | MI; SR | 2,979 | ,907 | ,891 | ,929 | ,952 | ,946 | ,951 | ,043 |
| DM2 | MI | 2,975 | ,910 | ,894 | ,931 | ,953 | ,948 | ,953 | ,043 |
| OQP9 | SR | 2,950 | ,913 | ,897 | ,934 | ,955 | ,950 | ,955 | ,043 |
| CF 1 | MI; SR | 2,886 | ,918 | ,937 | ,957 | ,958 | ,952 | ,958 | ,042 |
(SR = Standard Residual Covariances; MI = Modification Index).
To assess the validity and reliability of the scale developed for this study, the following analyses suggested by Bagozzi and Philips [68] were used: content validity, unidimensionality, reliability, convergent validity, discriminant validity, and predictive validity.
Confirmatory factor analysis (CFA) was used to test model fitness. CFA is the most well-known statistical procedure used to test the structures with factorial component generated by establishing hypotheses. Model fitness was evaluated based on multiple fit indexes. In the framework of the CFA procedure, the chi-square statistic is the most popular index to evaluate goodness of fit between the specified and actual models. Wheaton et al. [69] suggested that the researcher also compute a relative chi-square (χ2/df). They suggested a ratio of approximately five or less as reasonable. This ratio indicates that the null model and data are appropriate with one another [70]. In our experience, however, the ratio of chi-square (χ2 ) to degrees of freedom (df) fell in the range of 2 to 1 or 3 to 1 indicated an acceptable fit between the hypothetical model and the sample data [71].
Because of the sensitivity of the chi-square test to the sample size, however, insufficient sample size makes it difficult to find existing differences between the groups and deviations from multiple variables normality. We therefore used multiple fit indexes to reduce measurement errors.
Goodness of fit indexes (GFI) were used determine the model fit when measuring the fitness of the entire model. The GFI indicates the relative quantity of variance and covariance described in common. The adjusted goodness of fit index (AGFI) differs from GFI. AGFI adjusts to the number of degrees of freedom (df) in the model. AGFI and GFI values measured between 0,80 and 0,89, indicating a moderate fit, whereas values measured above 0,90 indicated a good fit [72].
The comparative fit index (CFI) indicates the fitness of the tested model and assumed model with one another [73]. The normal fit index (NFI) and incremental fit index (IFI) evaluate the degree of the freedom of the evaluated model relative to the initial model [74]. An IFI value close to 1 indicates a very good fit [75]. The typical range for TLI lies between 0 and 1, but is not limited to that range. A TLI value close to 1 indicates a very good fit.
The following findings were obtained as a result of the fitness analysis of the initial and last model as a result of principal component analysis is displayed in (Table 2).
To assess the reliability, Cronbach’s alpha coefficient and composite reliability scores were calculated (Table 2). According to critical levels indicated by Fornell and Larcker [76] and Nunnaly [77], scales showed acceptable levels of reliability because the Cronbach’s alpha coefficient and composite reliability scores were greater than ,70. Factor loadings shown in (Table 2) are large and all significant (p < 0,01) providing evidence for convergent validity. Shared variance between pairs of latent factors in the structural measurement model were compared with AVE scores that were calculated for each component of pairs to evaluate the discriminant validity [76]. Average variance extracted was found to be greater, signaling the discriminant validity.
Inter-correlations among variables are represented in (Table 3) with means and standard deviations (SD). The highest mean is 3,94, which reflects customer focus; the lowest mean is 3,20, which reflects employee involvement. The standard deviations of all variables are higher than ,70. Pearson correlations are indicated in Table 3. Notably, Cronbach’s alpha values are higher than Pearson correlation coefficients for all variables. This is important for construct validity, which evaluates how each item is measured on the scale. Thus, the instrument has convergent and discriminates validities, satisfying construct validity [49]. On the other hand, we also consider that the instrument has content validity too. This is because they were incorporated based on quality management principles of ISO 9001:2008 quality management system, and the scale items were gathered from a literature review.
We tried to find the best fitting model based on structural equation modeling. Relationships among the variables are represented in (Figure 2). Among the seven TQM practices, management leadership, decision making, continuous improvement, customer focus, and supplier relations were significantly related to operational performance. On the other hand, only customer focus and process management were significantly related to financial performance.
4. Discussion
Total quality management practices and dimensions of performance are significantly and positively related with one another. Correlation coefficients are significant at the 0.01 level. The lowest significant coefficient (.394) is between financial performance and decision making. The highest significant and positive coefficient (.761) is between leadership and decision making. Based on financial performance, customer focus has the highest correlation coefficient (.512) among the TQM practices. Also, the correlation coefficient (.651) between customer focus and operational performance is higher than the others. Other empirical findings support a significant and positive relationship between performance and customer focus [45,63,64,67,78,79,80].
Regression weights show that variance of operational performance (H1) is explained significantly by customer focus (35,7%); supplier relations (20,1%); leadership (13,4%); decision making (9,5%); and continuous improvement (7.7%). Process management and employee involvement do not explain variance of operational performance. On the other hand, variance of financial performance (H2) is explained significantly only by customer focus (21,3%) and process management (8%). In this position, other TQM practices do not explain the variance of financial performance. The influence of operational performance (H3) on the variance of financial performance is 26,6%. Thus, acceptance of H3 is supported. Overall, TQM practices explained the 53,4% variance of operational performance and 34,3% variance of financial performance.
Table 4.
Results of Hypothesis Testing.
| Hypothesized link | Estimate | Standardized Estimate | SE | CR | p | ||
|---|---|---|---|---|---|---|---|
| Leadership | → | Operational-Quality Performance |
,151 | ,134 | ,058 | 2,601 | ,009*** |
| Decision Making | → | Operational-Quality Performance |
,111 | ,095 | ,063 | 1,755 | ,079* |
| Continuous Improvement | → | Operational-Quality Performance |
,076 | ,077 | ,045 | 1,711 | ,087* |
| Customer Focus | → | Operational-Quality Performance |
,387 | ,357 | ,044 | 8,792 | ,000*** |
| Employee Involvement | → | Operational-Quality Performance |
,021 | ,026 | ,033 | ,639 | ,523 |
| Process Management | → | Operational-Quality Performance |
,006 | ,006 | ,044 | ,136 | ,892 |
| Relations with Suppliers | → | Operational-Quality Performance |
,163 | ,201 | ,031 | 5,214 | ,000*** |
| Leadership | → | Financial Performance | ,108 | ,078 | ,079 | 1,357 | ,175 |
| Decision Making | → | Financial Performance | -,008 | -,005 | ,087 | -,090 | ,929 |
| Continuous Improvement | → | Financial Performance | ,035 | ,029 | ,061 | ,580 | ,562 |
| Customer Focus | → | Financial Performance | ,285 | ,213 | ,063 | 4,513 | ,000*** |
| Employee Involvement | → | Financial Performance | ,025 | ,025 | ,045 | ,556 | ,578 |
| Process Management | → | Financial Performance | ,102 | ,080 | ,061 | 1,669 | ,095* |
| Relations with Suppliers | → | Financial Performance | ,028 | ,028 | ,043 | ,657 | ,511 |
| Operational-Quality Performance | → | Financial Performance | ,330 | ,266 | ,058 | 5,728 | ,000*** |
*p<0.10 **p<0.01 ***p<0.001.
Customer focus affects both operational performance and financial performance of hospitals more than other TQM practices. If hospitals successfully satisfy their customers, their performance [4,53,57,81,82,83,84,85,86]. Patients’ appraisals of quality are important, and hospitals should monitor patients’ perceptions and expectations regularly. In addition to heterogeneity, inseparability and intangibility features of services, patients’ participation to the process requires customer focus to result in better performance. Satisfied patients recommend hospital services, and their positive word of mouth impacts hospital performance. On the other hand, patient complaints force hospitals to address their service standards.
Relations with suppliers are important to explain better operational performance [45,46,87]. Hospitals should thus have closer relationships with their suppliers to fulfill quality requirements. Effective communication between suppliers and hospitals helps both parties understand what they want from each other in relation to producing services to deliver to patients. Furthermore, hospitals’ requirements for service quality lead to improved processes among suppliers. If any kind of problem occurs between suppliers and hospitals, it affects operational performance.
Results of this study also suggest that continuous improvement is significantly and positively related with operational performance. There are examples in the literature that confirms positive relationship between continuous improvement and performance [7,8]. In our results, employee involvement has no significant influence on performance. In the literature, however, there are positive relations between employee involvement and performance of hospitals [7,38,85,88]. Reason of our finding can be related to involvement of employees to medical organizational processes may require to be more educated and experienced. If organizations have lack of education and training, positive relationship may not be occurred [7].
5. Conclusions
Competition creates pressure on healthcare organizations to gain cost-effective and higher quality care. Also actors in the external environmet of hospitals like government, other agencies and customers put pressure on hospitals for quality. TQM is one of the perspective organizations can use to improve their service quality. Kennedy and Fiss [89] explained TQM adoption based on the institutional theory and they indicated that early and late adopters have different motivators to implement TQM. While efficiency motivete early adopters, legitimacy motivate late adopters to implement TQM.
Recently, total quality management implementation seems to have had a substantial impact on businesses’ effectiveness [90]. In this study, we focus on the relationship between TQM practices and identifying their effects on the various dimensions of performance in the hospitals. We gained important findings that will help hospitals to have better performance. Operational performance is determined as an antecedent of financial performance. For better service quality and positive financial results, various activities and procedures should be implemented. Higher productivity rates, fewer mistakes, shorter delivery and waiting time, fewer complaints raise tendecy of customers to pay more and to give priority among alternative hospitals. This study confirmed that customer focus and process management influence financial performance of hospitals positively. On the other hand, Macinati [91] stated lack of significant relationship between financial performance and quality management in the Italian health care industry. Reason is explained as difficulty of simultaneously conducting quality and efficieny.
Customer focus is the strongest practice to improve both operational performance and financial performance. Mosadeghrad [7] stated similar finding regarding positive relationship between customer management and performance for Iranian hospitals. If hospitals meet customers’ necessities and expectations and organize activities related to customer relationship management, the contribution of customer focus on operational and financial performance will be realized. This result supports customer focus as a facilitator of gaining competitive advantage. Beyond this, hospitals should try to develop customer loyalty. Satisfied patients and loyalty will help hospitals not only gain competitive advantage, but also help hospitals become more sustainable.
In addition to customer focus, supplier relations and management leadership are more likely to be useful than efforts to improve process management, employee involvement, and continuous improvement.
Findings of this study contribute to present a perspective to implement TQM practices in developing country. As stated by Mosadeghrad [7] different countries may need different TQM models to implement. Secondly, both quality management and healthcare literature may take advantage of these findings. Thirdly, valid and reliable questionnaire was developed. Fourthly, hospitals in the country may use findings as guideline to constitute quality management structure and define priorities to manage quality practically. Therefore, hospitals must begin their paths with being customer focus that will enhances their operational and financial performance. Lastly, this study was conducted in the service industry. In a broad perspective, providing service quality is not only necessary for long term profitability of service industry but also manufacturing industry may use these findings as an initial stage of offering service quality. Manufacturing industry may differentiate their position based on their service quality.
Based on this study, we can suggest that hospitals should support their patients to lead them in evaluating processes of service quality. Beyond patient satisfaction surveys, hospitals can establish patient suggestion boxes to allow customers to become more involved in service. Developing and using an effective customer database can help hospitals understand customer needs. It helps them to realize how their services can differ from their competitors. Not only satisfaction of patients but also families of patients should be taken into consideration to improve service quality.
Like all studies, this study has some limitations. Our sample includes both private and public hospitals. We are unable, however, to compare results from the two types of institutions, because the representation of private hospitals in the sample was much lower than public hospitals. Future studies should investigate the differences between private and public hospitals. Collecting data from different countries may also shed more light on the role of TQM practices on facets of performance. Influence of culture on adoption of TQM may represent different patterns. As a future study suggestion, cultural issues can be added to research model. We were also unable to test the differences between the time before TQM was implemented and after TQM was implemented. This is another limitation of our study. Longitudinal studies are suggested to measure TQM practices across a period of time.
Author Contributions
Conceptualization,S.Z. and C.Z. methodology, S.Z.; software, C.Z.; validation,C.Z.,. and S.Z.; formal analysis, S.Z.; investigation, S.Z.; resources, S.Z.; data curation, C.Z.; writing—original draft preparation, S.Z.; writing—review and editing, C.Z.; visualization, S.Z.; supervision, S.Z.; project administration,C.Z.; funding acquisition,S.Z. All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A. Measurement scales, survey items, and their sources
A.1. Leadership of management
L.1. Managers of all departments of the hospitals accept their responsibilities for quality.*
L.2. Hospital management provides individual leadership to improve service quality.
L.3. In the hospital, all managers encourage employees to serve on time.
L.4. Top management encourages employees to attend to service processes.
L.5. Hospital management creates a vision focused on quality improvement.
L.6. Hospital management attends to quality improvement project individually.
A.2. Decision Making
DM1. Knowledge about quality is a tool to manage quality.*
DM2. Knowledge about quality is handled to assess managers and supervisors.*
DM3. Before creating service and serving the customer, innovations are revised attentively.
DM4. Coordination is provided between departments that are effective in creating quality service.
DM5. New service and quality is emphasized based on the cost and objectives of the department.
A.3. Continuous Improvement
CI1. In the hospital, professional and technical training is given to employees. CI2. In the hospital, quality training is given to employees.
CI3. In the hospital, quality managers and quality supervisors have been trained.
CI4. In the hospital Total Quality Management training is given (philosophy of quality responsibility).
A.4. Customer focus
CF1. The needs of the patient are provided to disseminate and be understandable in the hospital.*
CF2. We know the current and future needs of patients.
CF3. We often communicate closely with our patients.
CF4. Our patients express their pleasures verbally.
CF5. Managers and supervisors encourage patient satisfaction development activities. **
CF6. The most important thing is to provide patient satisfaction and meet expectations.
CF7. Managers always emphasize the importance of patient satisfaction.
A.5. Employee Involvement
EI1. We try to evaluate the ideas of team members before decision making to solve problems.*
EI2. We implement a team problem-solving system.
EI3. Many problems have been solved by small team sessions for the last three years.
EI4. Problem solving teams contribute to developing service process.
EI5. Employees are encouraged to solve their problems on their own.
A.6. Process Management
PM1. Processes in the hospital are managed with statistical quality.
PM2. Comprehensive statistical methods are used to decrease incompatibility among processes.
PM3. Charts are handled based on whether service processes are under control.
PM4. Process is followed by statistical process.
PM5. Processes are often audited, revised, and controlled.
PM6. Distribution of service programs or service is balanced.*
PM7. Job or process definitions are given directly to employees. *
A.7. Relations with suppliers
RS1. We help suppliers enhance their performance for just-in-time manufacturing and delivery capability.*
RS2. We give importance to quality instead of price when choosing a supplier.
RS3. We consider quality dependency when choosing a supplier.
RS4. We consider process ability when choosing a supplier.
RS5. We consider commitment to “continuous improvement” when choosing a supplier.
A.8. Operational and quality performance
OQP1. Service quality is increasing.*
OQP2. Productivity rates are increasing.*
OQP3. Rate of faulty transactions are decreasing.
OQP4. Delivery time of buying materials is becoming shorter.
OQP5. Presentation time of treatment services is becoming shorter.
OQP6. Patient complaints are decreasing.
OQP7. The degree of patient satisfaction is increasing.*
OQP8. Rate of faulty services in clinics is decreasing.
OQP9. Quality in clinics meets or exceeds patient demands.*
A.9. Financial performance
FP1. Hospital revenues are increasing.
FP2. The market share of the hospital is increasing.
* omitted items because of low factor loading.
**corrected inter-item correlation coefficient (0,418) is lower than (0,500).
References
- Ali, K.; Johl, S. K.; Muneer, A.; Alwadain, A.; Ali, R. F. Soft and Hard Total Quality Management Practices Promote Industry 4.0 Readiness: A SEM-Neural Network Approach. Sustainability 2022, 14 (19), 11917. https://doi.org/10.3390/su141911917. [CrossRef]
- Anderson, J. A. Evolution of the Health Care Quality Journey. Journal of Legal Medicine 2010, 31 (1), 59–72. https://doi.org/10.1080/01947641003598252. [CrossRef]
- Parasuraman, A.; Zeithaml, V. A.; Berry, L. L. A Conceptual Model of Service Quality and Its Implications for Future Research. Journal of Marketing 1985, 49 (4), 41–50. https://doi.org/10.1177/002224298504900403. [CrossRef]
- Zabada, C.; Rivers, A. P.; Munchus, G. Obstacles to the Application of Total Quality Management in Health Care Organizations. Total Quality Management 1998, 9, 57–66. [CrossRef]
- Tomes, A. E.; Chee Peng Ng, S. Service Quality in Hospital Care: The Development of an in-Patient Questionnaire. Int. J. Health Care Qual. Assur. 1995, 8 (3), 25–33. https://doi.org/10.1108/09526869510089255. [CrossRef]
- Rashid, W. E. W.; Jusoff, H. K. Service Quality in Health Care Setting. Int. J. Health Care Qual. Assur. 2009, 22 (5), 471–482. https://doi.org/10.1108/09526860910975580. [CrossRef]
- Mosadeghrad, A. Developing and Validating a Total Quality Management Model for Healthcare Organizations. The TQM Journal 2015, 27 (5), 544–564. [CrossRef]
- Swinehart, K.; Green, R. F. Continuous Improvement and TQM in Health Care: An Emerging Operational Paradigm Becomes a Strategic Imperative. Int. J. Health Care Qual. Assur. 1995, 8 (1), 23–27. https://doi.org/10.1108/09526869510078031. [CrossRef]
- Kessler, D.; Geppert, J. The Effects of Competition on Variation in the Quality and Cost of Medical Care; National Bureau of Economic Research: Cambridge, MA, 2005.
- Cooper, Z.; Gibbons, S.; Jones, S.; McGuire, A. Does Hospital Competition Save Lives? Evidence from the English NHS Patient Choice Reforms. London School of Economics Working Paper 2010, 16/2010, https://doi.org/10.1111/j.1468-0297.2011.02449.x. [CrossRef]
- Wardhani, V.; Utarini, A.; Van Dijk, J.; Post, D.; Groothoff, J. Determinants of Quality Management Systems Implementation in Hospitals. Health Policy 2009, 89, 239–251. [CrossRef]
- Lim, P. C.; Tang, N. The Development of a Model for Total Quality Healthcare. Managing Service Quality 2000, 10, 103–111. [CrossRef]
- Rodger, J. A.; Pendharkar, P. C.; Paper, D. J. Management of Information Technology and Quality Perfor-Mance in Healthcare Facilities. Int. J of Applied Quality Management 1999, 2, 251–269.
- Nilsson, L.; Johnson, M. D.; Gustafsson, A. The Impact of Quality Practices on Customer Satis-Faction and Business Results: Product versus Service Organizations. J of Quality Management 2001, 6, 5–27. [CrossRef]
- Zeithaml, V. A.; Berry, L. L.; Parasuraman, A. The Behavioral Consequences of Service Quality. J. Mark. 1996, 60 (2), 31. https://doi.org/10.2307/1251929. [CrossRef]
- Grönroos, C. A Service Quality Model and Its Marketing Implications. Eur. J. Mark. 1984, 18 (4), 36–44. https://doi.org/10.1108/eum0000000004784. [CrossRef]
- Andaleeb, S. S. Public and Private Hospitals in Bangladesh: Service Quality and Predictors of Hospital Choice. Health Policy Plan. 2000, 15 (1), 95–102. https://doi.org/10.1093/heapol/15.1.95. [CrossRef]
- Donabedian, A. The Quality of Care: How Can It Be Assessed? J. of the American Medical Association 1988, 260, 1743–1748. [CrossRef]
- Douglas, T. J.; Judge, W. Q. Total Quality Management Implementation and Competitive Advantage: The Role of Structural Control and Exploration. Acad. Manage. J. 2001, 44 (1), 158–169. https://doi.org/10.2307/3069343. [CrossRef]
- Sureshchander, G.; Rajendran, C.; Anantharaman, R. A Conceptual Model for Total Quality Management in Service Organizations. Total Quality Management 2001, 12 (3), 343–363. [CrossRef]
- Yang, C.-C. The Establishment of a TQM System for the Health Care Industry. TQM Mag. 2003, 15 (2), 93–98. https://doi.org/10.1108/09544780310461107. [CrossRef]
- Claver, E.; Tarí, J. J.; Molina, J. F. Critical Factors and Results of Quality Management: An Empirical Study. Total Qual. Manage. Bus. Excel. 2003, 14 (1), 155–157. https://doi.org/10.1080/1478336032000044852. [CrossRef]
- Sila, I.; Ebrahimpour, M. Examination and Comparison of the Critical Factors of Total Quality Management (TQM) across Countries. Int. J. Prod. Res. 2003, 41 (2), 235–268. https://doi.org/10.1080/0020754021000022212. [CrossRef]
- Conca, F. J.; Llopis, J.; Tarı́, J. J. Development of a Measure to Assess Quality Management in Certified Firms. Eur. J. Oper. Res. 2004, 156 (3), 683–697. https://doi.org/10.1016/s0377-2217(03)00145-0. [CrossRef]
- Deming, W. Quality, Productivity and Competitive Position. Cambridge, M.A.: MIT Center for Advanced Engineering; 1982.
- Juran, J. On Planning for Quality. London: Collier Macmillian.1988.
- Puffer, S. M.; McCarthy, D. J. A Framework for Leadership in a TQM Context. J. Qual. Manag. 1996, 1 (1), 109–130. https://doi.org/10.1016/s1084-8568(96)90008-5. [CrossRef]
- Koumoutzis, N. Make Behavioral Considerations Your First Priority in Quality Improvements. Industrial Engineering 1994, 26, 63–65.
- Tarí, J. J.; Molina, J. F.; Castejón, J. L. The Relationship between Quality Management Practices and Their Effects on Quality Outcomes. Eur. J. Oper. Res. 2007, 183 (2), 483–501. https://doi.org/10.1016/j.ejor.2006.10.016. [CrossRef]
- Daft, R. New Era of Management. South Western: Cengage Learning. 2008.
- Lee, S.; Choi, K.-S.; Kang, H.-Y.; Cho, W.; Chae, Y. M. Assessing the Factors Influencing Continuous Quality Improvement Implementation: Experience in Korean Hospitals. Int. J. Qual. Health Care 2002, 14 (5), 383–391. https://doi.org/10.1093/intqhc/14.5.383. [CrossRef]
- Zehir, C.; Ozsahin, M. A Field Research on the Relationship Between Strategic Decision Making Speed and Innovation Performance in the Case of Turkish Large Scale Firms. Management Decision 2008, 46, 709–724. [CrossRef]
- Ittner, C. D.; Larcker, D. F. The Performance Effects of Process Management Techniques. Manage. Sci. 1997, 43 (4), 522–534. https://doi.org/10.1287/mnsc.43.4.522. [CrossRef]
- Reed, R.; Lemak, D. J.; Montgomery, J. C. Beyond Process: TQM Content and Firm Performance. Acad. Manage. Rev. 1996, 21 (1), 173–202. https://doi.org/10.5465/amr.1996.9602161569. [CrossRef]
- Park, D.; Dahlgaard, S. M. Organizational Learnability and Innovability”,A System for Assessing, Diagnosing and Improving Innovations. Academy of Management Review 1994, 19, 392–418.
- Bowen, D. E. Managing Customers as Human Resources in Service Organizations. Hum. Resour. Manage. 1986, 25 (3), 371–383. https://doi.org/10.1002/hrm.3930250304. [CrossRef]
- Shortell, S. M.; Obrien, J. L.; Carman, J. M.; Foster, R. W.; Hughes, E.; Boerstler, H.; Connor, O. Assessing the Impact of Continuous Quality Improvement / Total Quality Management: Concept versus Implementation. Health Serv Res 1995, 30, 377–401.
- Rad, A. A Survey of Total Quality Management in Iran: Barriers to Successful Implementation in Hospitals. Leadership in Health Services 2005, 18, 12–34. [CrossRef]
- Anderson, H. C. Teamwork Brings TQM to Health Care. Managing Service Quality. 1994, 4, 35–38. [CrossRef]
- Matej, Z.; Matjaz, M.; Damjan, M.; Bostjan, G. Quality Management Systems as a Link between Management and Employees. Total Quality Management & Business Excellence 2012, 23 (1), 45–62. [CrossRef]
- Welikala, D.; Sohal, A. Total Quality Management and Employees’ Involvement: A Case Study of an Australian Organisation. Total Quality Management & Business Excellence 2008, 19 (6), 627–642. [CrossRef]
- Agus, A. An Empirical Test of TQM in Public Service Sector and Its Impact on Customer Satisfaction. Journal of Quality Measurement and Analysis 2005, 1 (1), 47–60.
- Ahmad, S.; Schroeder, R. G. The Importance of Recruitment and Selection Process for Sustainability of Total Quality Management. Int. J. Qual. Reliab. Manag. 2002, 19 (5), 540–550. https://doi.org/10.1108/02656710210427511. [CrossRef]
- Flynn, B. B.; Schroeder, R. G.; Sakakibara, S. The Impact of Quality Management Practices on Performance and Competitive Advantage. Decis. Sci. 1995, 26 (5), 659–691. https://doi.org/10.1111/j.1540-5915.1995.tb01445.x. [CrossRef]
- Forza, C.; Filippini, R. TQM Impact on Quality Conformance and Customer Satisfaction: A Causal Model. Int. J. Prod. Econ. 1998, 55 (1), 1–20. https://doi.org/10.1016/s0925-5273(98)00007-3. [CrossRef]
- Trent, R. J.; Monczka, R. M. Achieving World-Class Supplier Quality. Total Qual. Manag. 1999, 10 (6), 927–938. https://doi.org/10.1080/0954412997334. [CrossRef]
- Kannan, V. R.; Tan, K. C. Just in Time, Total Quality Management, and Supply Chain Management: Understanding Their Linkages and Impact on Business Performance. Omega 2005, 33, 153–162. [CrossRef]
- Krause, D. R.; Handfield, R. B.; Scannell, T. V. An Empirical Investigation of Supplier Development: Reactive and Strategic Processes. J. Oper. Manage. 1998, 17 (1), 39–58. https://doi.org/10.1016/s0272-6963(98)00030-8. [CrossRef]
- Kaynak, H. The Relationship between Total Quality Management Practices and Their Effects on Firm Performance. J. Oper. Manage. 2003, 21 (4), 405–435. https://doi.org/10.1016/s0272-6963(03)00004-4. [CrossRef]
- Zineldin, M. The Royalty of Loyalty: CRM, Quality and Retention. J. Consum. Mark. 2006, 23 (7), 430–437. https://doi.org/10.1108/07363760610712975. [CrossRef]
- Samson, D.; Terziovski, M. The Relationship between Total Quality Management Practices and Operational Peformance. J of Operations Management 1999, 17, 393–409. [CrossRef]
- Wu, S.-I.; Chan, H.-J. Perceived Service Quality and Self-Concept Influences on Consumer Attitude and Purchase Process: A Comparison between Physical and Internet Channels. Total Qual. Manage. Bus. Excel. 2011, 22 (1), 43–62. https://doi.org/10.1080/14783363.2010.529645. [CrossRef]
- Sajid, M. S.; Baig, M. K. Quality of Health Care: An Absolute Necessity for Public Satisfaction. Int. J. Health Care Qual. Assur. 2007, 20 (6), 545–548. https://doi.org/10.1108/09526860710819477. [CrossRef]
- Parkan, C.; Wu, M. L. On the Equivalence of Operational Performance Measurement and Multiple Attribute Decision Making. Int. J. Prod. Res. 1997, 35 (11), 2963–2988. https://doi.org/10.1080/002075497194246. [CrossRef]
- Ho, S. K. M. Total Quality Management Transfer to Small and Medium Industries in Malaysia by SIRIM. Total Qual. Manag. 1995, 6 (3), 273–286. https://doi.org/10.1080/09544129550035440. [CrossRef]
- Hubiak, W. A.; Odonnell, S. J. Do Americans Have Their Minds Set against TQM?(Abstract). National Productivity Review 1996, 15, 19–32. [CrossRef]
- Cronin, J. J., Jr; Taylor, S. A. Servperf versus Servqual: Reconciling Performance-Based and Perceptions-Minus-Expectations Measurement of Service Quality. J. Mark. 1994, 58 (1), 125–131. https://doi.org/10.1177/002224299405800110. [CrossRef]
- Singh, J. Consumer Complaint Intentions and Behavior: Definitional and Taxonomical Issues. J. Mark. 1988, 52 (1), 93. https://doi.org/10.2307/1251688. [CrossRef]
- Alexander, J. A.; Weiner, B. J.; Griffith, J. Quality Improvement and Hospital Financial Performance. J. Organ. Behav. 2006, 27 (7), 1003–1029. https://doi.org/10.1002/job.401. [CrossRef]
- Rust, R. T.; Zahorik, A. J.; Keiningham, T. L. Return on Quality: Making Service Quality Financially Accountable. The J of Marketing 1995, 59, 58–70. [CrossRef]
- Zeithaml, V. A. Service Quality, Profitability and the Economic Worth of Customers: What We Know and What We Need to Learn. Journal of Academy of Marketing Science 2000, 28, 67–85. [CrossRef]
- Churchill, G. A., Jr. A Paradigm for Developing Better Measures of Marketing Constructs. J. Mark. Res. 1979, 16 (1), 64–73. https://doi.org/10.1177/002224377901600110. [CrossRef]
- Cua, K. O.; McKone, K. E.; Schroeder, R. G. Relationships between Implementation of TQM, JIT, and TPM and Manufacturing Performance. J. Oper. Manage. 2001, 19 (6), 675–694. https://doi.org/10.1016/s0272-6963(01)00066-3. [CrossRef]
- Fuentes-Fuentes, M. M.; Ca, A.-S. Llorens-Montes FJ. The Impact of Environmental Characteristics on TQM Principles and Organizational Performance. Omega 2004, 32, 425–442. [CrossRef]
- Saraph, J. V.; Benson, P. G.; Schroeder, R. G. An Instrument for Measuring the Critical Factors of Quality Management. Decis. Sci. 1989, 20 (4), 810–829. https://doi.org/10.1111/j.1540-5915.1989.tb01421.x. [CrossRef]
- Rahman, S.; Bullock, P. Soft TQM, Hard TQM and Organizational Performance Relationships: An Empirical Investigation. Omega 2005, 33, 73–83. [CrossRef]
- Chong, V. K.; Rundus, M. J. Total Quality Management, Market Competition and Organizational Performance. The British Accounting Review 2004, 36, 155–172. [CrossRef]
- Bagozzi, R.; Philips, L. Representing and Testing Organizational Theories: A Holistic Construct. Administrative Science Quarterly 1982, 27, 459–489. [CrossRef]
- Wheaton, B.; Muthen, B.; Alwin, D. F.; Summers, G. F. Assessing Reliability and Stability in Panel Models. Sociol. Methodol. 1977, 8, 84. https://doi.org/10.2307/270754. [CrossRef]
- Marsh, H.; Hocevar, D. Application of Confirmatory Factor Analysis to the Study of Self-Concept: First and Higher Order Factor Structures and Their Invariance Across Groups. Psychological Bulletin 1995, 97, 562–582.
- Carmines, E.; Mciver, J. Analyzing Models with Unobserved Variables: Analysis of Covariance Structures. G. Bohrnstedt, & E. Borgatta, In Social Measurement: Current Issues 1981, 65–115.
- Chau, P. Y. K. Reexamining a Model for Evaluating Information Center Success Using a Structural Equation Modeling Approach. Decis. Sci. 1997, 28 (2), 309–334. https://doi.org/10.1111/j.1540-5915.1997.tb01313.x. [CrossRef]
- Bentler, P. M.; Kano, Y. On the Equivalence of Factors and Components. Multivariate Behav. Res. 1990, 25 (1), 67–74. https://doi.org/10.1207/s15327906mbr2501_8. [CrossRef]
- Bentler, P.; Bonett, D. Significant Test Goodness of Fit in the Analysis of Covariance Structures. Psychological Bulletin 1980, 88, 588–606. [CrossRef]
- Arbuckle, J. L. AMOS 16.0. SpringHouse, PA: Amos Development Corporation. 2007.
- Fornell, D.; Larcker, D. Evaluating Structural Equation Models with Unobservable Variables and Measurement Error. Journal of Marketing Research 1981, 18 (1), 39–50. [CrossRef]
- Nunnaly, J. Psychometric Theory (2 b.). New York: McGraw Hill. 1978.
- Grandzol, J. R.; Gershon, M. Which TQM Practices Really Matter: An Empirical Investigation. Qual. Manag. J. 1997, 4 (4), 43–59. https://doi.org/10.1080/10686967.1998.11919147. [CrossRef]
- Ahire, S. L.; O’Shaughnessy, K. C. The Role of Top Management Commitment in Quality Management: An Empirical Analysis of the Auto Parts Industry. Int. J. Qual. Sci. 1998, 3 (1), 5–37. https://doi.org/10.1108/13598539810196868. [CrossRef]
- Nair, A. Meta-Analysis of the Relationship between Quality Management Practices and Firm Performance Implications for Quality Management Theory Development. J of Operations Management 2006, 24, 948–975. [CrossRef]
- Dagger, T. C.; Sweeney, J. C.; Johnson, L. W. A Hierarchical Model of Health Service Quality: Scale Development and Investigation of Integrated Model. J of Serv Res 2007, 10, 123–142. [CrossRef]
- Tanninen, K.; Puumalainen, K.; Sandström, J. The Power of TQM: Analysis of Its Effects on Profitability, Productivity and Customer Satisfaction. Total Qual. Manage. Bus. Excel. 2010, 21 (2), 171–184. https://doi.org/10.1080/14783360903549949. [CrossRef]
- Andaleeb, S. S.; Siddiqui, N.; Khandakar, S. Patient Satisfaction with Health Services in Bangladesh. Health Policy Plan. 2007, 22 (4), 263–273. https://doi.org/10.1093/heapol/czm017. [CrossRef]
- Naidu, A. Factors Affecting Patient Satisfaction and Healthcare Quality. Int. J. Health Care Qual. Assur. 2009, 22 (4), 366–381. https://doi.org/10.1108/09526860910964834. [CrossRef]
- Homburg, C.; Wieseke, J.; Hoyer, W. D. Social Identity and Service Profit Chain. J. of Marketing 2009, 73, 38–54. [CrossRef]
- Fotopoulos, C.; Psomas, E. & Vouzas, F, Investigating Total Quality Management Practice’s in-Ter-Relationships in ISO 9001:2000 Certified Organisations. Total Quality Management & Business Excellence 2010, 21 (5), 503–515. [CrossRef]
- Sadikoglu, E.; Zehir, C. Investigating the Effects of Innovation and Employee Performance on the Relationship between Total Quality Management Practices and Firm Performance: An Empirical Study of Turkish Firms. Int J of Production Economics 2010, 127, 13–26. [CrossRef]
- Newman, K.; Maylor, U.; Chansarkar, B. The Nurse Retention, Quality of Care and Patient Satisfaction Chain. Int. J. Health Care Qual. Assur. Inc. Leadersh. Health Serv. 2001, 14 (2–3), 57–68. https://doi.org/10.1108/09526860110386500. [CrossRef]
- Kennedy, M. T.; Fiss, P. C. Institutionalization, Framing, and Diffusion: The Logic of TQM Adoption and Implementation Decisions among U.s. Hospitals. Acad. Manage. J. 2009, 52 (5), 897–918. https://doi.org/10.5465/amj.2009.44633062. [CrossRef]
- Niyi Anifowose, O.; Ghasemi, M.; Olaleye, B. R. Total Quality Management and Small and Medium-Sized Enterprises’ (SMEs) Performance: Mediating Role of Innovation Speed. Sustainability 2022, 14 (14), 8719. https://doi.org/10.3390/su14148719. [CrossRef]
- Macinati, M. S. The Relationship between Quality Management Systems and Organizational Performance in the Italian National Health Service. Health Policy 2008, 85 (2), 228–241. https://doi.org/10.1016/j.healthpol.2007.07.013. [CrossRef]
Figure 1.
Research model.
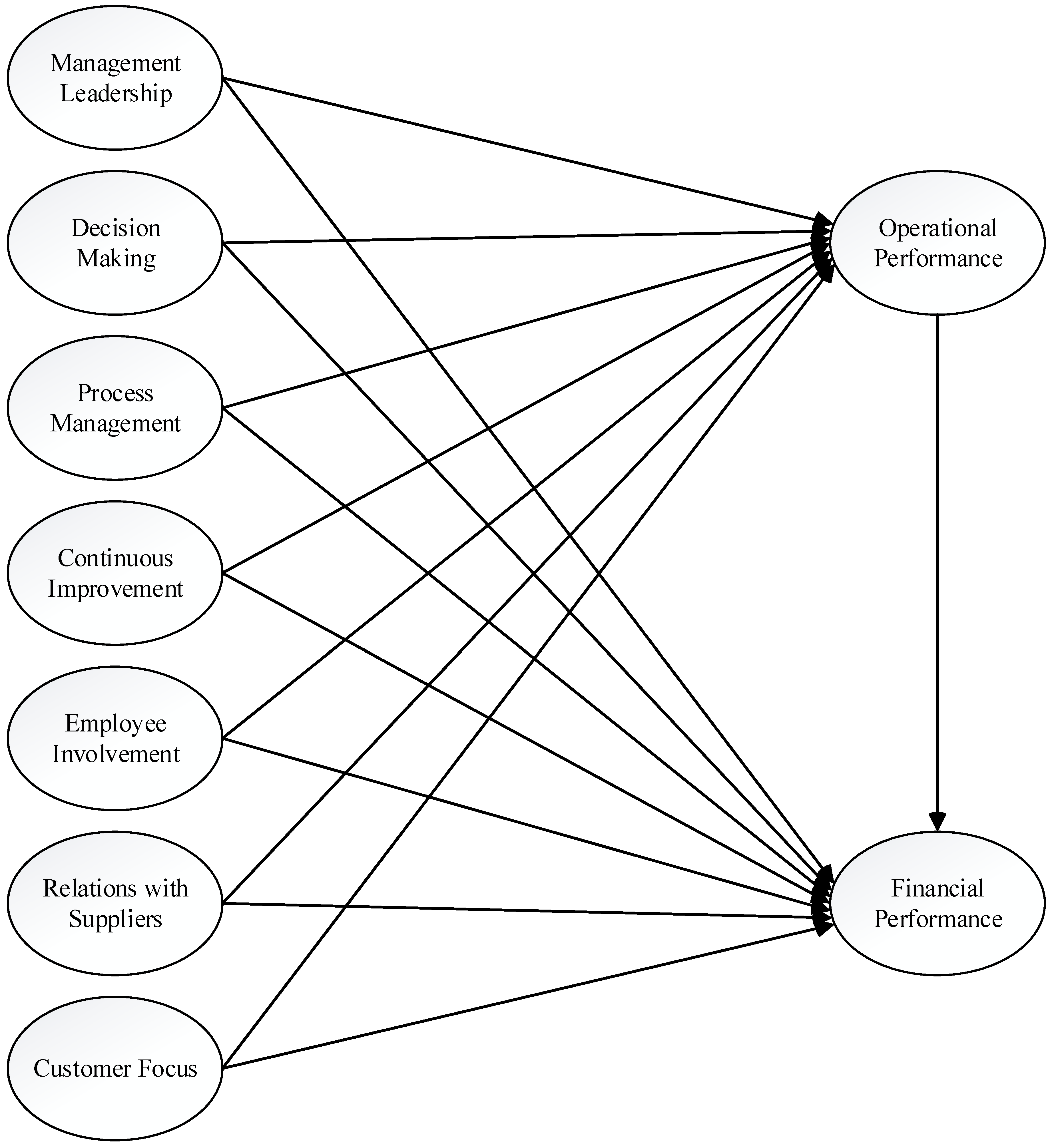
Figure 2.
Structural model.
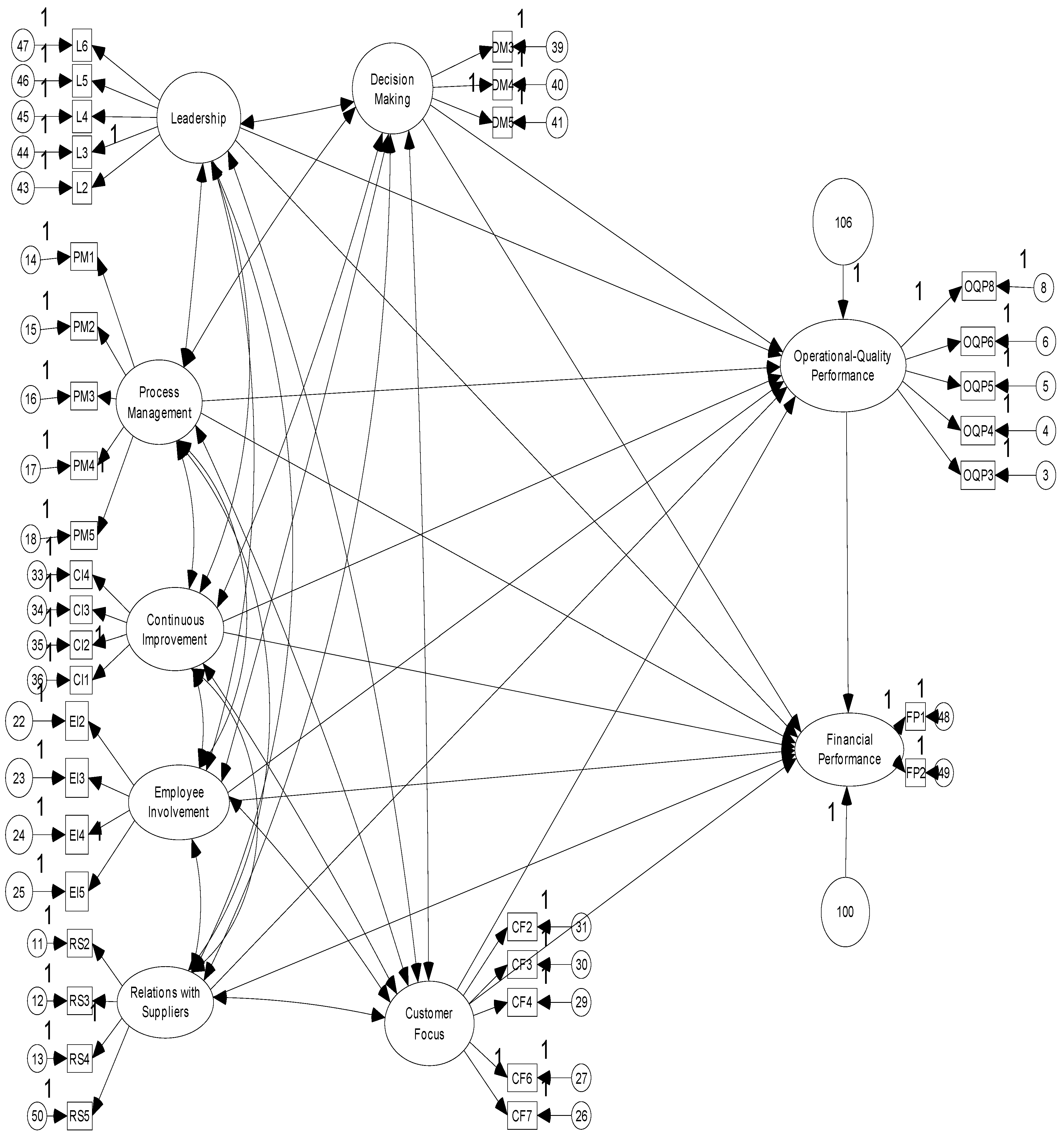
Table 2.
The Results of the Confirmatory Factor Analysis.
| Std.Regression Weights | S.E. | C.R. | p | Cronbach’sAlpha | Composite reliabity | A.V.E | ||
|---|---|---|---|---|---|---|---|---|
| Leadership | .873 | .875 | .585 | |||||
| L2 | .679 | |||||||
| L3 | .778 | .057 | 22.685 | *** | ||||
| L4 | .838 | .056 | 24.137 | *** | ||||
| L5 | .834 | .051 | 24.047 | *** | ||||
| L6 | .682 | .051 | 20.184 | *** | ||||
| Decision Making | .807 | .810 | .586 | |||||
| DM3 | .804 | .052 | 23.040 | *** | ||||
| DM4 | .782 | .052 | 22.568 | *** | ||||
| DM5 | .709 | |||||||
| Continuous Improvement | .873 | .878 | .644 | |||||
| CI1 | .698 | |||||||
| CI2 | .845 | .044 | 25.115 | *** | ||||
| CI3 | .832 | .043 | 24.785 | *** | ||||
| CI4 | .827 | .045 | 24.665 | *** | ||||
| Customer Focus | .876 | .877 | .587 | |||||
| CF2 | .752 | |||||||
| CF3 | .784 | .044 | 25.473 | *** | ||||
| CF4 | .76 | .043 | 24.633 | *** | ||||
| CF6 | .808 | .045 | 26.281 | *** | ||||
| CF7 | .727 | .044 | 23.474 | *** | ||||
| Employee Involvement | .917 | .918 | .738 | |||||
| EI2 | .865 | .035 | 31.746 | *** | ||||
| EI3 | .881 | .034 | 32.508 | *** | ||||
| EI4 | .901 | .033 | 33.466 | *** | ||||
| EI5 | .786 | |||||||
| Process Management | .847 | .871 | .580 | |||||
| PM1 | .781 | .060 | 17.285 | *** | ||||
| PM2 | .818 | .063 | 17.681 | *** | ||||
| PM3 | .801 | .060 | 17.507 | *** | ||||
| PM4 | .837 | .062 | 17.865 | *** | ||||
| PM5 | .532 | |||||||
| Relations with Suppliers | .923 | .925 | .756 | |||||
| RS2 | .809 | .029 | 35.181 | *** | ||||
| RS3 | .904 | .024 | 43.952 | *** | ||||
| RS4 | .894 | |||||||
| RS5 | .869 | .024 | 40.475 | *** | ||||
| Financial Performance | .893 | .895 | .810 | |||||
| FP1 | .856 | |||||||
| FP2 | .943 | .040 | 26.947 | *** | ||||
| Operational-Quality Performance | .879 | .879 | .593 | |||||
| OQP3 | .757 | .036 | 26.481 | *** | ||||
| OQP4 | .745 | .036 | 25.932 | *** | ||||
| OQP5 | .762 | .035 | 26.695 | *** | ||||
| OQP6 | .779 | .036 | 27.434 | *** | ||||
| OQP8 | .806 |
S.E.: Standard error of regression weight; C.R.: Critical ratio for regression weight; A.V.E: Average variance extracted ***: p<0, 001.
Table 3.
Descriptive statistics and intercorrelations of all variables.
| Variables | Mean | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Leadership | 3.68 | .784 | ||||||||
| 2. Decision Making | 3.77 | .739 | .761** | |||||||
| 3. Continuous Improvement | 3.82 | .802 | .583** | .558** | ||||||
| 4. Customer Focus | 3.94 | .721 | .545** | .482** | .616** | |||||
| 5. Employee Involvement | 3.20 | .969 | .619** | .570** | .584** | .530** | ||||
| 6. Process Management | 3.71 | .781 | .563** | .627** | .672** | .496** | .526** | |||
| 7. Relations with Suppliers | 3.46 | .902 | .527** | .523** | .509** | .550** | .644** | .548** | ||
| 8. Financial Performance | 3.64 | .952 | .434** | .394** | .431** | .512** | .401** | .405** | .411** | |
| 9.Operational-Quality Performance | 3.75 | .719 | .571** | .536** | .549** | .651** | .530** | .493** | .576** | .531** |
** Correlation is significant at the 0.01 level (2-tailed).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



