
Submitted:
02 September 2023
Posted:
05 September 2023
You are already at the latest version
Abstract
BACKGROUND: Retinoblastoma is a malignant tumour that develops from the immature cells of the retina. It is the most frequent type of paediatric intraocular cancer and is curable. Clinical and histological findings after enucleation of the affected eye dictate not only the patient's secondary care but also their prognosis. We assessed the clinical and histopathologic predictors of survival among children with retinoblastoma from two tertiary health facilities in Uganda. METHODS: This retrospective research utilized archived formalin fixed & paraffin embedded blocks of eye specimens enucleated between 2014 to 2016 at Mbarara University, pathology department and Ruharo Eye Centre. The specimens were then processed and stained with haematoxylin and eosin. The confirmation of retinoblastoma was made to include histologic stage and features of the tumor. Biographic data of the patients and the clinical features such as leukocoria, proptosis, phthisis, staphyloma, buphthalmos were retrieved from the records.RESULTS: Males (55.1%) dominated the study population (N=78). The median age was 31 months. The commonest clinical sign was leukocoria (69.2%) and the most abundant histopathological stage was stage 1 (41%). Optic nerve invasion 39.5%, choroidal invasion 29.5%, scleral invasion 7.7% and orbital extension 16.7% were seen. Flexner-Wintersteiner rosettes were seen in 24.6%. Necrosis was a prominent feature (71.2%). The two-year survival was estimated to be 62%. Leukocoria (RR 1.1), female gender (RR 1.4), intralaminar optic nerve invasion (RR 7.6) and a lack of orbital extension (RR- 7) were significant predictors of survival.CONCLUSION: Leukocoria and proptosis are noticeable clinical signs of retinoblastoma. Most patients present while in stage one although stage four presentation is also common. Leukocoria, optic nerve invasion, orbital extension, and gender are significant factors predictive of survival in patients with retinoblastoma.
Keywords:
clinical features
; histopathologic features
; retinoblastoma
; survival
; children
Introduction
Retinoblastoma (RB) is a malignant tumour that develops from the immature cells of the retina [1]. It is the most common intraocular cancer of childhood affecting approximately 1 in 15,000 – 20,000 births, for an incidence of 7000 – 8000 new cases annually worldwide and 4000 deaths annually [2,3]. It is an important cause of blindness, morbidity and mortality particularly in the underdeveloped countries of sub-Saharan Africa [4]. The greatest disease burden is recorded in large populations that have high birth rates, such as in Asia and Africa [5] [6]. Regions with greatest prevalence have the highest mortality with up to 70% mortality in Asia and Africa, compared with 3–5% in Europe, Canada, and the USA [6]. In Uganda, retinoblastoma is the 5th commonest cancer after lymphomas, Kaposi sarcoma, leukemia and nephroblastoma [7].
The survival of retinoblastoma patients in Africa, Uganda in particular is low largely because of delayed presentation [8]. The advanced stage of disease is found to be associated with very poor outcome. Survival majorly depends on severity of disease at presentation. Survival rates in the UK and US approach 100% [9] with survival in other continents, primarily developing nations, much lower. Survival rates in developed Latin America countries has been reported to be 80–89%, 48% in India, and as low as 20–46% in Africa [10]. In Uganda, survival rose from 45% in the pre-chemotherapy era to 65% in the post chemotherapy era [8].
A worldwide issue is poor access to comprehensive retinoblastoma pathology [6]. Histological examination of the enucleated globes in the region has also been inconsistent as shown in studies done in Uganda and in Kenya [11,12]. Retinoblastoma management not informed by histological examination could impede development of a rational management plan and lead to unsatisfactory clinical outcomes.
There is paucity of data on the association between clinical and histopathological features and survival so as to guide appropriate retinoblastoma management and ultimately improve survival, this study intended to address this gap.
Methods
Study design and site
This was a retrospective study carried out at two health facilities in south western Uganda. Mbarara Regional Referral Hospital (MRRH) is a tertiary hospital with a 350-bed capacity, located along Kampala-Kabale highway, 286kms from Kampala the capital city. The facility serves as a general referral hospital with pathology, surgical, medical, obstetrical and gynaecological, Pediatric services, and ear, nose, and throat (ENT), dental, orthopaedic, and other specialized units also on site. It is government funded through the Ministry of Health intended to provide free service and covers the districts of Mbarara, Isingiro, Sheema, Bushenyi, Ibanda, Kiruhura, Lyantonde and Ntungamo. It also receives patients from the neighbouring nations of Democratic Republic of Congo (DRC), Rwanda and Tanzania. It is a teaching hospital for Mbarara University of Science and Technology (MUST) and other health training institutions in the region.
Another study site was Ruharo Eye Center (REC). The patients with suspected retinoblastoma are referred to Ruharo Eye Center, a mission owned Ophthalmology centre for specialised care where the patients are managed. REC is one of the referral centres for retinoblastoma cases in the country and receives over 90 cases of retinoblastoma annually.
The enucleated specimens were taken to MUST histopathology laboratory in the MUST pathology department, which is the only government aided histopathology laboratory in the southern and western part of Uganda. The MUST pathology department is a referral unit for cases which require histologic diagnosis in the region.
Study variables
Clinical features were retrieved from archived records. These included leukocoria, strabismus, proptosis, uveitis, cataract, staphyloma, phthisis, laterality and treatment. Clinical outcome data was recorded as either alive or dead. The Staging was by the AJCC TNM8 staging system as pT1, PT2, pT3 and pT4.
The following histologic features were noted: Growth patterns as exophytic, endophytic and mixed; Invasion of lens, conjunctiva and corneal epithelium; Invasion of anterior segment structures as present or absent (iris, ciliary body and trabecular meshwork); Necrosis as none, mild (involving less than 25%), moderate (25-50%) and extensive (more than 50%); Calcification as none, mild (involving less than 25%), moderate (25-50%) and extensive (more than 50%); Flexner-Wintersteiner rosettes as mild (0-25%), moderate (25- 50%) and many (more than 50%).
The well differentiated tumours were those with more than 50%, moderately differentiated as those less than 50% and poorly differentiated as those without any rosettes; Homer-Wright rosettes as absent or present; Mitosis as present or absent; Presence of inflammation as chronic (lymphohistiocytic) or acute inflammation.
Data analysis
Stata Version 13 was used for analysis. Baseline participants’ characteristics were described using appropriate summary statistics, which is, mean or median for continuous variables and proportions for categorical variables. The histopathological stages of retinoblastoma among children were presented as proportions in a bar graph. The Survival after 2 years in care was computed as a cumulative measure and expressed as a proportion of all children still alive by two years out of all that were admitted with retinoblastoma at REC. The corresponding 95% confidence interval (CI) was also reported.
Independent variables included sociodemographic factors like age, gender and geographical region of residence, in-hospital care, histopathologic features of the tumor and clinical presentation of the children. Unadjusted risk-ratios were reported together with their corresponding 95% CI. A significance level of 5% was used. All independent variables with p<0.1 were included in the multivariate model building using a manual backward-stepwise selection method. Variables that lost their association with survival at 2-years were excluded from the final multivariate model. Also, variables that could not allow for convergence of the model were excluded. For all variables in the final model, adjusted risk-ratios were presented with their corresponding 95% Confidence Intervals.
Results
We included 78 eye specimens in the study. As shown in Table 1, the median age of diagnosis was 31 months and most of the participants were between 12-59 months (78.4%). Majority were males (55.1%) while most of them originated from western Uganda (33.3%). In most cases, only one eye was affected at the time of diagnosis (70.5%).
The commonest clinical sign was leukocoria (69.2%) which was followed by proptosis (32.1%). See Figure 1 below.
The commonest pathologic stage was stage 1 (41.0%) followed by 4 (26.9%), then 2 (26.9%) and then 3 (5.1%). Stage 2 was further classified as 2A (24.4) and 2B (2.6) while stage 3 would be further classified as 3A (1.3), B (2.6), C (1.3), D (0). See Figure 2 below.
Choroidal invasion was seen in 29.5% (23) of the specimens, more than half of these were massive. Optic nerve invasion was seen in 31.5% (30) cases with almost half of these having invasion to the surgical end/margin. Orbital extension was seen in 16.7 % (13) cases while scleral invasion seen in a paltry 7.7%. Iris, trabecular meshwork and ciliary body invasion accounted for 16.7% (13) each. Lens, corneal, conjunctival and vascular invasion accounted for a combined paltry 7.8% (6). Endophytic tumor was seen in 71.8% (56) cases. Flexner-Wintersteiner rosettes were seen in 34.6% (27) cases while Homer-Wright rosettes in only 6.4% (5) cases. Necrosis was seen in 71.8% cases while calcification was seen in 41% cases while mitoses were seen in only 9% cases. See Table 2 below.
The 2-year survival was estimated to be 62% as shown in Table 3 below.
At univariate analysis, gender, region of origin, leukocoria, proptosis, cataract, choroidal invasion, orbital invasion and necrosis were significant factors in predicting survival. Age, laterality, chemoreduction, buphthalmos, growth pattern, calcification, vascularity, mitosis, differentiation were not significant. Scleral invasion and anterior segment invasion were not able to produce a risk ratio because the alive category had zeroes. See Table 4 below.
Female gender, leukocoria, proptosis, choroidal invasion, optic nerve invasion orbital invasion, region, cataract and necrosis were run in the final model however region, cataract, choroidal invasion, proptosis and necrosis would not bring convergence so they were eliminated from the final model.
Female gender, leukocoria, orbital extension, optic nerve invasion were significant predictors of survival with female being able to survival 1.4 times, better than males, patients without leukocoria being able to survive 1.1 times better than those without.
Patients without optic nerve invasion will survive better than those with optic nerve invasion depending on the degree of invasion and patients without orbital extension will be able to survive 7 times better than those with orbital extension. See Table 5 below.
Discussion
The median age of the patients at presentation was 31 months which is comparable to a study at a tertiary centre in Kinshasa, Democratic Republic of Congo who found the median age at 32 months and 29 in months in an Indian population. However, this is not comparable to studies done in developed countries who report a median age of 12 months such as in the UK. This is attributed to the late presentation and delayed diagnosis of these cases in our setting and other developing countries [9,13,14].
The prevalence of males and females vary widely from studies. Male were 55.1% which was comparable to a Kenyan study at 54% as well as other studies in both developed and developing countries such as Turkey and Pakistan [12] [15,16]. However, studies done in Malaysia and Nigeria have reported a higher prevalence of females. This could be attributed to the genetic differences in the different populations and referral selection due to differences in cultural beliefs [17,18].
The commonest age groups involved was the 12-59 months (78.4%), Delayed diagnosis is commonly encountered in developing countries with 90% of cases diagnosed before the age of 5 years as evidenced by a study done in Cameroon which is consistent with our study at 91.2% and 85% in Nigeria [4,17]. Those less than 12 months were 12.8% which is comparable to a study in Kenya [19]. On the contrary most children diagnosed with RB in developed countries are less than 24 months because of the early presentation and diagnosis [1].
Unilateral cases were 70.5% and this is comparable to many studies which reported unilateral cases to be 72%, 74% 71.2% in Kenya, Uganda and Pakistan respectively [11,12,20]. Sub-Saharan Africa studies have found 11% to 33% of patients with retinoblastoma to have bilateral disease as seen in a study done in Republic of Côte d’Ivoire and the Democratic Republic of the Congo which is in keeping with our study [13,21].
Leukocoria (69.2%) and proptosis (37.2%) were the commonest presenting symptoms. This was comparable to a study done at Kenyatta Hospital in Kenya at 71% and 37% respectively [12]. Also, leukocoria was the commonest presenting sign Republic of Côte d’Ivoire and the Democratic Republic of the Congo [13,21]. However, this is different from data in middle income to upper income countries who present with leukocoria and strabismus as the commonest signs, such as in Egypt and in the UK [9,22]. This is because symptoms such as proptosis symptoms are signs of advanced RB and present when there is most likely orbital extension. The frequency of other less common symptoms such as buphthalmos, phthisis, cataracts and staphyloma were similar to a study done in India[23].
Intraocular tumours (stages pT1-3) constituted 73.1% while extraocular tumours (stage pT4) were 26.9%. This was comparable to a study done in India which found intraocular tumours and extraocular tumours to be 72.3% and 27.7% respectively [14]. PT4 was our second most common stage which was consistent with findings of a study done in India that showed pT1 of 48.1% and pT4 in 26% [24]. However, this is lower than the percentage found in a study done at Ruharo Eye Centre, Uganda that showed that almost half the tumours were extraocular (46%). This is due to the introduction of an effective safe chemotherapy regimen in Uganda which presumably reduced the progression of disease to advanced stages [8].
Endophytic pattern was seen in 71.8% while exophytic pattern 17.9% and mixed pattern in 10.3%. The incidence of growth patterns varies widely with the endophytic and mixed types being more predominant. This difference could be attributed to a difference in the biologic nature of these tumors [24,25].
Choroidal invasion was seen in 29.5% which is comparable to that of Shields et al., (1993) of 23% [26]. Though the incidence of choroidal invasion varies greatly in various reported series, ranging from 15.2% to 62%, it is lower than of findings in other developing countries such as in India of 47.4% [23]. This has been attributed to the limited peripheral calottes that were taken during the sectioning. However massive choroidal invasion was seen in 12.8% cases which is comparable to the 18% seen in Jordan, but was still lower than that from other studies such as in India at 24.6% because of the limited sectioning [15,23].
Reports indicate that 24% to 45% of eyes have any degree of optic nerve invasion. Optic nerve invasion was seen in 39.5% which was comparable with the study in America of 38.7% and at 32% in India [25,27]. However, it was higher than that a much earlier study in the USA, probably reflecting to the advanced stage of the tumours in our study [28]. Retrolaminar ON invasion was seen in 3.9 % cases which is comparable to Shields et al., (1994) of 5.5%, however studies from developing countries have shown a higher percentage such as Gupta et al., (2009) with 17% and Ralph Eagle (2009) with 10.4% [27,28,29]. Invasion of resected margin of optic nerve was seen in 16.7% cases. This was comparable to other studies in the developing world, however this is higher than for developed countries such as in USA of 1% [28].
Scleral invasion was seen in 7.7% cases which was in keeping with other studies such as that of Argentina at 8.8%, and 7% of Pakistan [30,31]. Orbital extension was seen in 16.7% which is comparable to 18% in Indian study [32]. This is due to the advanced stages of the tumours in developing countries. Invasion of the iris was seen in 16.7% which is in keeping with a study done in India of 10.7% [23]. The higher incidence of these risk factors in developing world might be related to later presentation (more advanced stage) in relation to the lower socioeconomic status and the delay in seeking and getting treatment [11].
Tumour differentiation is highly variable between different reports from the developing world. Many tumours showed higher incidence of poorly differentiated (up to 80%) compared to well differentiated tumours which was comparable to our study of 65% probably reflecting the late age of presentation of the undifferentiated tumours [23].
Generally, necrosis was seen in 71.2% cases which was higher than in most studies because of the fact that most cases had undergone chemoreduction before enucleation in our study as compared to other studies who examined primarily enucleated eyes, however, extensive necrosis seen is 33.3% was comparable to 31% of an Indian study[23].
Calcification in retinoblastoma is a frequent histologic finding with a reported frequency between 40% and 95%, although the subject has not been studied in depth. Our study found calcification in 41%of the cases, which is similar to the 48% in Malaysia but this is lower than seen in Israel at 84% [18,33].
Two- year survival was estimated to be 62 % and this was comparable to a study done Taiwan at 64.4% [34]. This is higher than those of surrounding countries such as Kenya of 22.6% and 23% in Tanzania and this difference is assumed to be due to the development of an effective safe chemotherapy regimen in Uganda[8,12,35]. However, this is lower than for the developed countries such as UK where survival is estimated at 95% [9]. The poorer survival in LMIC is attributed to a combination of many factors including diagnostic delays resulting in advanced stage of disease at presentation, lack of availability of chemotherapeutic agents, cost of treatment leading to abandonment of care and limited access to surgery and radiotherapy[12,35].
Age was not found to be a predictor in our study as it is in many studies, however studies in India and in Singapore have shown that age less than 24 months a significant predictor with these children being able to survive most likely because children who present at a younger age may have tumours diagnosed at earlier stages of the disease [23,36].
Our study showed that sex had significant influence on survival (RR 1.4) with females having a 1.4-fold chance of survival compared to males. Though most studies have not shown any difference in survival between males and females with RB, many studies have shown that females have a better cancer survival than males [37,38]. Though environmental and hormonal factors have been implicated in adulthood cancer, genetics have been thought to be the commonest cause for this difference in childhood cancers as evidenced in some studies [39].
Most studies have shown that people with leukocoria have a better survival (RR 1.1) with our study showing that these people are almost 1.1 times more likely to be alive at 2 years than those without leukocoria. This is because leukocoria can easily be seen as an abnormal sign and hence patients will present when tumour is less advanced [12,40]. Most studies from developing countries such as in Kenya have shown that proptosis is associated with a poor survival as it is a sign of more advanced disease, and this was consistent with this study which showed a significant association, however this was not included in final model as it would not achieve convergency.at multivariate analysis[12].
Cataract was a significant predictor at univariate analysis but lost significance at multivariate analysis. Cataract was a significant factor on univariate analysis and is this is in keeping with some studies in India and USA which show that orbital cellulitis, phthisis bulbi, staphyloma, and cataract are clinical predictors of high risk pathology [23,41].
The rate of survival in patients with ON invasion depends on degree of ON invasion. Survival rates increase as the degree of invasion reduces and this was evidenced at univariate analysis where absent ON invasion, prelaminar ON and intralaminar ON invasion was significant [24]. However, at multivariate analysis, there was statistical significance for only intralaminar ON probably due to fewer numbers.
Scleral invasion has been shown to be an independent factor of survival in most studies however, this study did not provide a risk ratio as there was no one in the alive group [24,30]. Choroidal invasion was seen to be significant in univariate analysis but could not be included it in the multivariate model because it could not allow for convergence, though mortality is higher in those with massive choroidal invasion.
Survival in patients with anterior segment invasion has been shown to be low, however our analysis couldn’t produce risk ratios as there was no one in the exposure group, though mortality associated with these patients was very high.
Our study showed that orbital extension was significantly predictive of survival. Patients without orbital extension being able to survive 7 times better than those with orbital extension. Orbital extension is a major cause of death in children with retinoblastoma in the developing countries with mortalities of up to 100%. The presence of orbital invasion was associated with a 10–27 times higher risk of systemic metastasis as compared to cases without orbital invasion. This is in agreement with studies done in USA and in India [32,42].
Necrosis was a significant factor at univariate analysis though it lost significance at multivariate analysis. Most studies including ours have not found necrosis to be associated with survival however, a study done in USA showed that patients with extensive necrosis are associated with high risk pathology and mortality [43]. Our study did not show that differentiation is a predictive factor as it is in many other studies, however a study in Jordan has shown that poorly differentiated tumours are associated with more advanced tumor pathology [15]. Growth type has not been associated with survival though a study in Jordan illustrated that the mixed type independently affects survival as it would be found in advanced tumours[44]. Calcification was not shown be a significant factor of survival, nevertheless no studies have been done to see its impact on survival.
Conclusion
Leukocoria and proptosis are the most common clinical signs of Retinoblastoma. The dominant pathologic stage is stage 1 though late presentation (stage 4) is also observed. Survival is still low though generally higher than neighbouring countries. Leukocoria, optic nerve invasion, orbital extension, and gender were the significant factors predictive of survival in patients at Mbarara Regional Referral Hospital. Sensitisation of health workers and community on identification and referral of any child with leukocoria to improve histopathology reporting in order as well as to identify patients at risk is highly recommended.
Author Contributions
Conceptualization, RA, DL and KW.; methodology, RA and AB.; software, RA.; validation, DL and KW; formal analysis, RA.; investigation, RA, AB and RK.; resources, RK.; data curation, RA and RK.; writing—original draft preparation, RA and AB.; writing—review and editing, RA and RK; visualization, RA.; supervision, DL and KW.; project administration, RA. All authors have read and agreed to the publication of this manuscript.
Funding
This study did not receive any external funding.
Institutional Review Board Statement
The study was conducted in accordance with the declaration of Helsinki. Ethical review and approval were obtained from the Faculty of Medicine Research Committee (FRC) and Research Ethics Committee of Mbarara University of Science and Technology (MUST-REC Number: 07/06-17).
Informed Consent Statement
Individual patient consent was waived because we reviewed records and obtained archived block eye specimen. There was no real time involvement with the patients.
Data Availability Statement
Data used in this study is available from the corresponding author upon request.
Acknowledgments
The authors would like to acknowledge the staff and administrative management of the two tertiary hospitals for supporting this research.
Conflicts of Interest
The authors and funders declare no conflict of interest in this study.
References
- Yun, J.; Li, Y.; Xu, C.-T.; Pan, B.-R. Epidemiology and Rb1 gene of retinoblastoma. International Journal of Ophthalmology 2011, 4, 103. [Google Scholar]
- Aerts, I.; Lumbroso-Le Rouic, L.; Gauthier-Villars, M.; Brisse, H.; Doz, F.; Desjardins, L. Retinoblastoma. Orphanet journal of rare diseases 2006, 1, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.; Deng, Y.-P. Retinoblastoma: concerning its initiation and treatment. International journal of ophthalmology 2013, 6, 397. [Google Scholar] [PubMed]
- Epee, E.; Moukouri, E.; Koki, G.; Pondy, A.; Mbassi, K. Clinical features and prognosis of retinoblastoma at the University Teaching Hospital of Yaounde-Cameroon. HEALTH SCIENCES AND DISEASE 2014, 15. [Google Scholar]
- Jain, M.; Rojanaporn, D.; Chawla, B.; Sundar, G.; Gopal, L.; Khetan, V. Retinoblastoma in Asia. Eye 2019, 33, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Dimaras, H.; Kimani, K.; Dimba, E.A.; Gronsdahl, P.; White, A.; Chan, H.S.; Gallie, B.L. Retinoblastoma. The Lancet 2012, 379, 1436–1446. [Google Scholar] [CrossRef]
- Wabinga, H.R.; Nambooze, S.; Amulen, P.M.; Okello, C.; Mbus, L.; Parkin, D.M. Trends in the incidence of cancer in Kampala, Uganda 1991–2010. International journal of cancer 2014, 135, 432–439. [Google Scholar] [CrossRef]
- Waddell, K.M.; Kagame, K.; Ndamira, A.; Twinamasiko, A.; Picton, S.V.; Simmons, I.G.; Revill, P.; Johnston, W.T.; Newton, R. Improving survival of retinoblastoma in Uganda. British Journal of Ophthalmology 2015, 99, 937–942. [Google Scholar] [CrossRef]
- MacCarthy, A.; Draper, G.; Steliarova-Foucher, E.; Kingston, J. Retinoblastoma incidence and survival in European children (1978–1997). Report from the Automated Childhood Cancer Information System project. European Journal of Cancer 2006, 42, 2092–2102. [Google Scholar] [CrossRef]
- Houston, S.K.; Murray, T.G.; Wolfe, S.Q.; Fernandes, C.E. Current update on retinoblastoma. International ophthalmology clinics 2011, 51, 77. [Google Scholar] [CrossRef]
- Waddell, K.M.; Kagame, K.; Ndamira, A.; Twinamasiko, A.; Picton, S.V.; Simmons, I.G.; Johnston, W.T.; Newton, R. Clinical features and survival among children with retinoblastoma in Uganda. British Journal of Ophthalmology 2015, 99, 387–390. [Google Scholar] [CrossRef] [PubMed]
- Nyawira, G.; Kahaki, K.; Kariuki-Wanyoike, M. Survival among retinoblastoma patients at the Kenyatta National Hospital, Kenya. 2013.
- Kazadi Lukusa, A.; Aloni, M.N.; Kadima-Tshimanga, B.; Mvitu-Muaka, M.; Gini Ehungu, J.L.; Ngiyulu, R.; Ekulu Mfutu, P.; Budiongo Nzazi, A. Retinoblastoma in the democratic republic of congo: 20-year review from a tertiary hospital in kinshasa. Journal of cancer epidemiology 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
- Chawla, B.; Hasan, F.; Azad, R.; Seth, R.; Upadhyay, A.D.; Pathy, S.; Pandey, R. Clinical presentation and survival of retinoblastoma in Indian children. British Journal of Ophthalmology 2016, 100, 172–178. [Google Scholar] [CrossRef]
- Yousef, Y.A.; Hajja, Y.; Nawaiseh, I.; Mehyar, M.; Sultan, I.; Deebajah, R.; Rawashdeh, K.; Khurma, S.; Jaradat, I.; Al-Hussaini, M. A histopathologic analysis of 50 eyes primarily enucleated for retinoblastoma in a tertiary cancer center in Jordan. Turk Patoloji Derg 2014, 30, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Adhi, M.I.; Kashif, S.; Muhammed, K.; Siyal, N. Clinical pattern of Retinoblastoma in Pakistani population: Review of 403 eyes in 295 patients. JPMA. The Journal of the Pakistan Medical Association 2018, 68, 376–380. [Google Scholar] [PubMed]
- Musa, K.O.; Aribaba, O.T.; Oluleye, T.S.; Olowoyeye, A.O.; Akinsete, A.M. Challenges of Retinoblastoma management at a Nigerian tertiary eyecare facility. 2017.
- Reddy, S.; Anusya, S. Clinical presentation of retinoblastoma in Malaysia: a review of 64 patients. International Journal of Ophthalmology 2010, 3, 64. [Google Scholar] [PubMed]
- Gichigo, N.; Kariuki-Wanyoike, M.; Kimani, K. Clinico-surgical histopathological findings of retinoblastoma cases treated at Kenyatta National Hospital. East African Medical Journal 2011, 88, 423–429. [Google Scholar]
- Khan, A.A.; Bukhari, M.H.; Mehboob, R. Association of retinoblastoma with clinical and histopathological risk factors. 2013.
- Lukamba, R.M.; Yao, J.-J.A.; Kabesha, T.A.; Budiongo, A.N.; Monga, B.B.; Mwembo, A.T.; Bey, P.; Chenge, G.B.; Desjardins, L.; Luboya, O.N. Retinoblastoma in sub-Saharan Africa: case studies of the Republic of Côte d’Ivoire and the Democratic Republic of the Congo. Journal of global oncology 2018, 4, 1–8. [Google Scholar] [CrossRef]
- El Zomor, H.; Nour, R.; Alieldin, A.; Taha, H.; Montasr, M.M.; Moussa, E.; El Nadi, E.; Ezzat, S.; Alfaar, A.S. Clinical presentation of intraocular retinoblastoma; 5-year hospital-based registry in Egypt. Journal of the Egyptian National Cancer Institute 2015, 27, 195–203. [Google Scholar] [CrossRef]
- Kashyap, S.; Meel, R.; Pushker, N.; Sen, S.; Bakhshi, S.; Sreenivas, V.; Sethi, S.; Chawla, B.; Ghose, S. Clinical predictors of high risk histopathology in retinoblastoma. Pediatric blood & cancer 2012, 58, 356–361. [Google Scholar]
- Suryawanshi, P.; Ramadwar, M.; Dikshit, R.; Kane, S.V.; Kurkure, P.; Banavali, S.; Viswanathan, S. A study of pathologic risk factors in postchemoreduced, enucleated specimens of advanced retinoblastomas in a developing country. Archives of pathology & laboratory medicine 2011, 135, 1017–1023. [Google Scholar]
- Biswas, J.; Das, D.; Krishnakumar, S.; Shanmugam, M.P. Histopathologic analysis of 232 eyes with retinoblastoma conducted in an Indian tertiary-care ophthalmic center. Slack Incorporated Thorofare, NJ: 2003; Vol. 40, pp 265-267.
- Shields, C.L.; Shields, J.A. Recent developments in the management of retinoblastoma. Journal of Pediatric Ophthalmology & Strabismus 1999, 36, 8–9. [Google Scholar]
- Eagle Jr, R.C. High-risk features and tumor differentiation in retinoblastoma: a retrospective histopathologic study. Archives of pathology & laboratory medicine 2009, 133, 1203–1209. [Google Scholar]
- Shields, C.L.; Shields, J.A.; Baez, K.; Cater, J.R.; de Potter, P. Optic nerve invasion of retinoblastoma. Metastatic potential and clinical risk factors. Cancer 1994, 73, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Vemuganti, G.K.; Reddy, V.A.P.; Honavar, S.G. Histopathologic risk factors in retinoblastoma in India. Archives of pathology & laboratory medicine 2009, 133, 1210–1214. [Google Scholar]
- Cuenca, A.; Giron, F.; Castro, D.; Fandino, A.; Guitter, M.; de Dávila, M.T.; Chantada, G. Microscopic scleral invasion in retinoblastoma: clinicopathological features and outcome. Archives of ophthalmology 2009, 127, 1006–1010. [Google Scholar] [CrossRef]
- Ali, M.J.; Honavar, S.G.; Reddy, V.A. Orbital retinoblastoma: Present status and future challenges–A review. Saudi Journal of Ophthalmology 2011, 25, 159–167. [Google Scholar] [CrossRef]
- Honavar, S.G.; Manjandavida, F.P.; Reddy, V.A.P. Orbital retinoblastoma: An update. Indian Journal of Ophthalmology 2017, 65, 435. [Google Scholar] [CrossRef]
- Levy, J.; Frenkel, S.; Baras, M.; Neufeld, M.; Pe’er, J. Calcification in retinoblastoma: histopathologic findings and statistical analysis of 302 cases. British journal of ophthalmology 2011, 95, 1145–1150. [Google Scholar] [CrossRef]
- Chen, Y.; Lin, H.; Hsu, W.; Lee, S.; Cheng, C. Retinoblastoma in Taiwan: incidence and survival characteristics from 1979 to 2003. Eye 2010, 24, 318–322. [Google Scholar] [CrossRef]
- Bowman, R.; Mafwiri, M.; Luthert, P.; Luande, J.; Wood, M. Outcome of retinoblastoma in east Africa. Pediatric blood & cancer 2008, 50, 160–162. [Google Scholar]
- Saw, S.-M.; Tan, N.; Lee, S.-B.; Eong, K.-G.A.; Chia, K.-S. Incidence and survival characteristics of retinoblastoma in Singapore from 1968-1995. Slack Incorporated Thorofare, NJ: 2000; Vol. 37, pp 87-93.
- Cook, M.B.; McGlynn, K.A.; Devesa, S.S.; Freedman, N.D.; Anderson, W.F. Sex disparities in cancer mortality and survival. Cancer epidemiology, biomarkers & prevention 2011, 20, 1629–1637. [Google Scholar]
- Tulla, M.; Berthold, F.; Graf, N.; Rutkowski, S.; Von Schweinitz, D.; Spix, C.; Kaatsch, P. Incidence, trends, and survival of children with embryonal tumors. Pediatrics 2015, 136, e623–e632. [Google Scholar] [CrossRef] [PubMed]
- Dorak, M.T.; Karpuzoglu, E. Gender differences in cancer susceptibility: an inadequately addressed issue. Frontiers in genetics 2012, 3, 268. [Google Scholar] [CrossRef] [PubMed]
- Abramson, D.H.; Beaverson, K.; Sangani, P.; Vora, R.A.; Lee, T.C.; Hochberg, H.M.; Kirszrot, J.; Ranjithan, M. Screening for retinoblastoma: presenting signs as prognosticators of patient and ocular survival. Pediatrics 2003, 112, 1248–1255. [Google Scholar] [CrossRef]
- Kopelman, J.E.; McLean, I.W.; Rosenberg, S.H. Multivariate analysis of risk factors for metastasis in retinoblastoma treated by enucleation. Ophthalmology 1987, 94, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Finger, P.T.; Harbour, J.W.; Karcioglu, Z.A. Risk factors for metastasis in retinoblastoma. Survey of ophthalmology 2002, 47, 1–16. [Google Scholar] [CrossRef]
- Chong, E.-M.; Coffee, R.E.; Chintagumpala, M.; Hurwitz, R.L.; Hurwitz, M.Y.; Chévez-Barrios, P. Extensively necrotic retinoblastoma is associated with high-risk prognostic factors. Archives of pathology & laboratory medicine 2006, 130, 1669–1672. [Google Scholar]
- Nawaiseh, I.; Al-Hussaini, M.; Alhamwi, A.; Meyar, M.; Sultan, I.; Alrawashdeh, K.; Jaradat, I.; Yousef, Y.A. The impact of growth patterns of retinoblastoma (Endophytic, Exophytic, and Mixed Patterns). Turk Patoloji Derg 2015, 31, 45–50. [Google Scholar] [CrossRef]
Figure 1.
Bar graph showing clinical characteristics of the specimen participants.
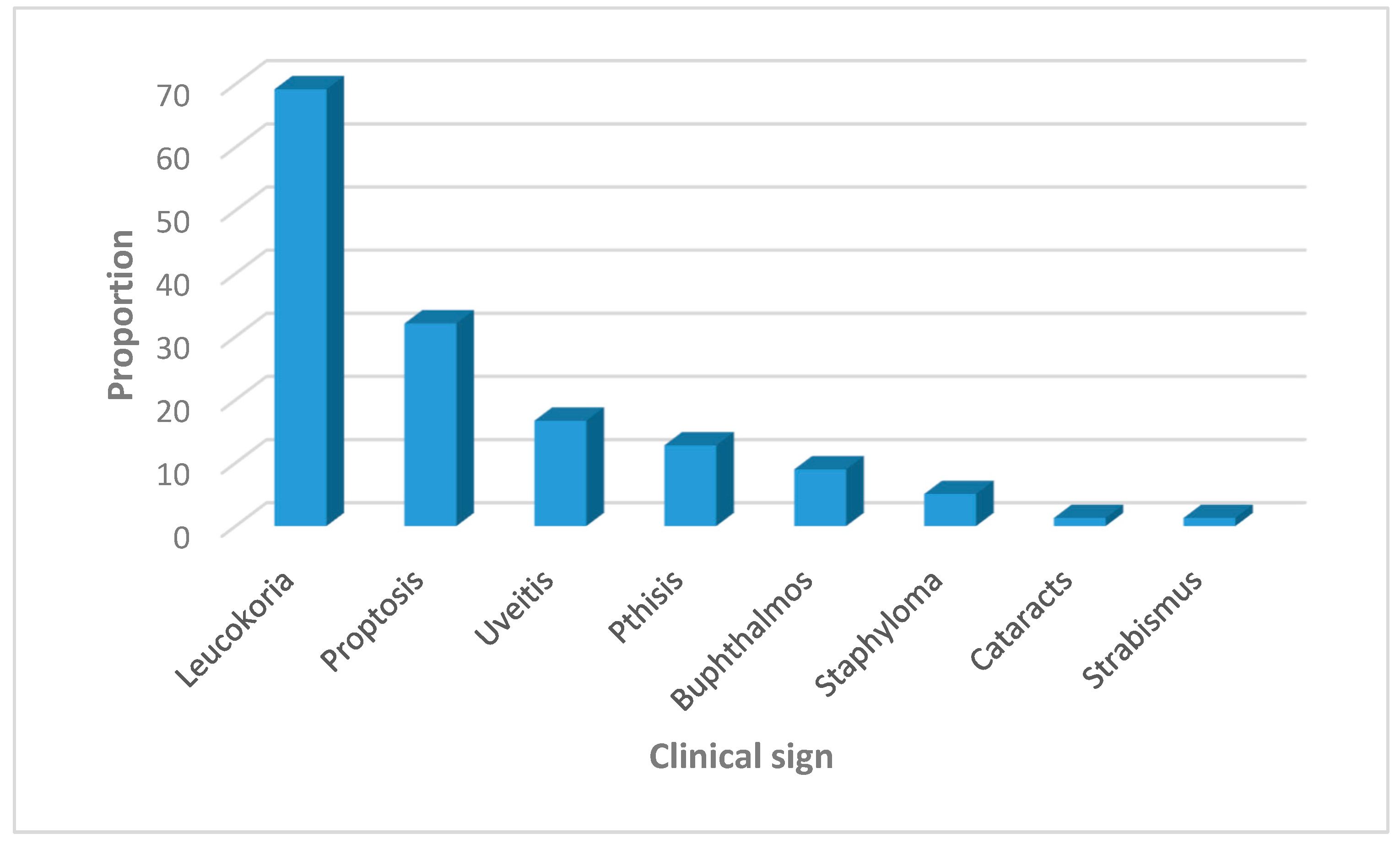
Figure 2.
Bar graph showing histopathologic stages of the specimens.
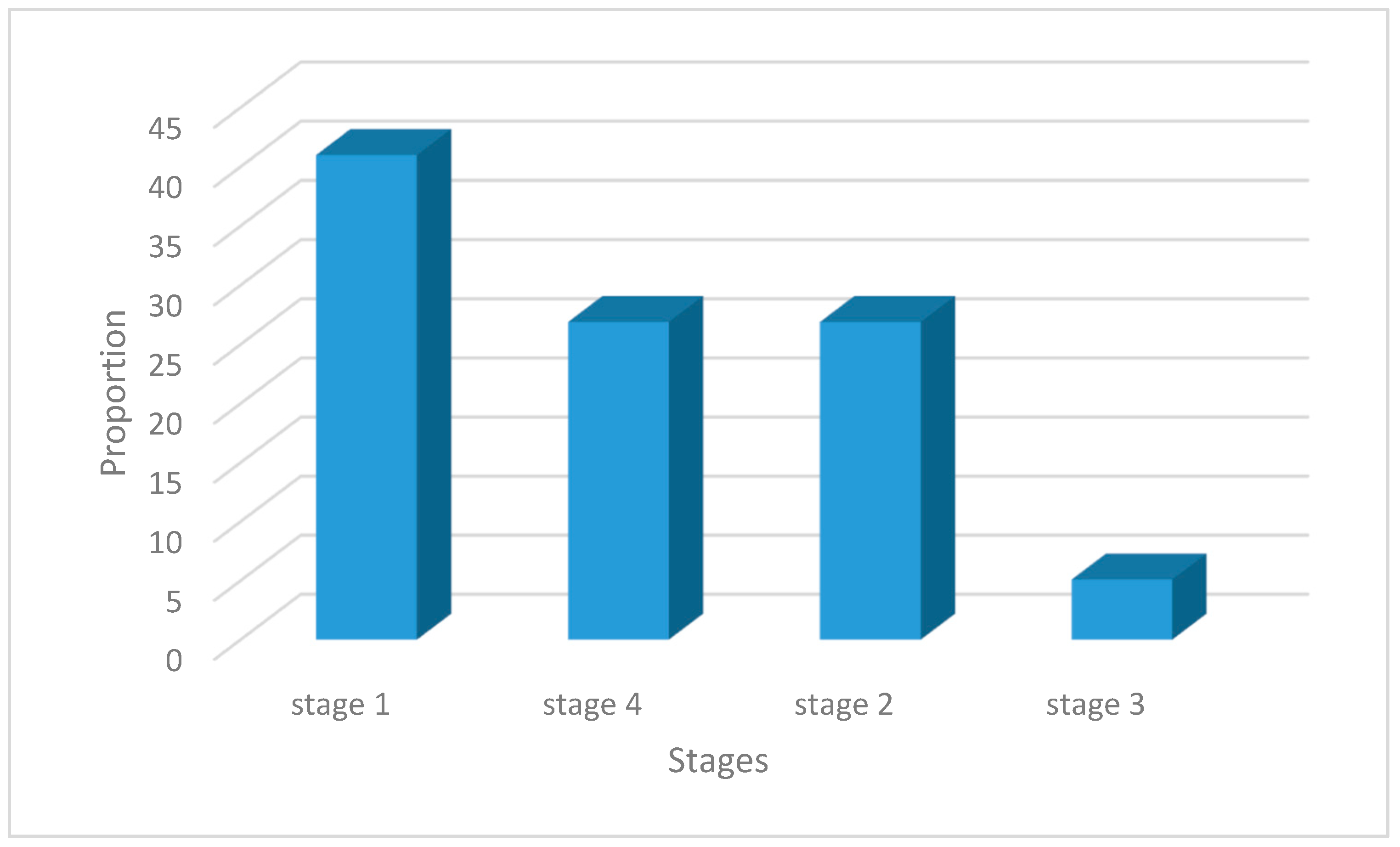

Table 1.
Baseline characteristics of sample source patients.
| Characteristic | n(%) |
|---|---|
| Age in months, median (IQR) | 31 (18-39) |
| Age categories (months) <12 12-59 ≥60 |
10 (12.8) 58 (78.4) 10 (12.8) |
| Gender Male Female |
43 (55.1) 35 (44.9) |
| Region Western Eastern Central Northern International |
26 (33.3) 21 (26.9) 22 (28.2) 5 (6.4) 4 (5.1) |
| Laterality Unilateral Bilateral |
55 (70.5) 23 (29.5) |
| Chemoreduction therapy Given Not given |
63 (80.8) 15 (19.2) |
Table 2.
Histopathologic features of the samples.
| Characteristic | n(%) |
|---|---|
| Choroidal invasion Absent Focal Massive |
55 (70.5) 13 (16.7) 10(12.8) |
| Optic nerve invasion Absent Prelaminar Intra-laminar Retrolaminar Surgical margin/cut end |
48 (61.5) 10 (12.8) 4 (5.1) 3 (3.9) 13 (16.7) |
| Scleral invasion Absent Partial thickness Full thickness |
72 (92.3) 1 (1.3) 5 (6.4) |
| Orbital extension | 13 (16.7) |
| Iris | 13 (16.7) |
| Trabecular meshwork | 13 (16.7) |
| Growth pattern Endophytic Exophytic Mixed |
56 (71.8) 14 (17.9) 8 (10.3) |
| Lens Invasion | 1 (1.3) |
| Ciliary body invasion | 13 (16.7) |
| Corneal epithelium invasion | 2(2.6) |
| Conjunctival invasion | 1 (1.3) |
| Vascular invasion | 2(2.6) |
| Flexner-Wintersteiner rosettes None Mild Moderate Many |
51 (65.4) 12 (15.4) 7 (9.0) 8 (10.2) |
| Homer-Wright rosettes None Present |
73 (93.6) 5 (6.4) |
| Necrosis None Mild Moderate Massive |
22 (28.2) 18 (23.1) 12 (15.4) 26 (33.3) |
| Calcification None Mild Moderate Massive |
46 (59.0) 13 (16.6) 12 (15.4) 7 (9.0) |
Table 3.
Estimation of survival at 2 years.
| Status at 2 years | n (%) | Proportion (CI) |
|---|---|---|
| Dead | 30 (38.5) | 38 (28- 50) |
| Alive | 48 (61.5) | 62 (50- 72) |
Table 4.
Results of univariate analysis showing predictors of 2year survival.
| Characteristic | Dead n (%) |
Alive n (%) |
Unadjusted (95% CI) | RR p value |
|---|---|---|---|---|
| Gender Female Male |
7 (20) 23 (53.5) |
28 (80) 20 (46.5) |
1.7 (1.20- 2.47) 1.0 |
0.003 |
| Region Eastern Central Southern International Western |
11 (52.4) 7 (61.8) 0 (0) 2 (50) 10 (38.5) |
10 (47.6) 15 (38.2) 5 (100) 2 (50) 16 (61.5) |
0.8 (0.45- 1.33) 1.1 (0.73- 1.68) 1.7 (1.26- 2.30) 0.8 (0.29- 2.27) 1.0 |
0.354 0.630 0.001 0.692 |
| Leukocoria Present Absent |
15 (27.8) 15 (62.5) |
39 (72.2) 9 (37.5) |
1.9 (1.12- 3.31) 1.0 |
0.018 |
| Proptosis Present Absent |
20 (80) 10 (18.9) |
5 (20) 43 (81.1) |
4.1 (1.83- 8.98) 1.0 |
0.001 |
| Cataract Present Absent |
0 (0) 30 (38) |
1 (100) 47 (61) |
1.7(1.43- 2.05) 1.0 |
0.000 |
| Choroidal invasion Absent Focal Massive |
17 (30.9) 4 (30.8) 9 (90) |
38 (69.1) 9 (69.2) 1 (10) |
6.9 (1.07- 44.72) 6.9 (1.04- 46.03) 1.0 |
0.043 0.045 |
| Optic nerve invasion Absent Prelaminar Intralaminar retrolaminar Surgical margin/ cut end |
14 (29.2) 2 (20) 0 (0) 2 (66.7) 12 (92.3) |
34 (70.8) 8 (80) 4 (100) 1 (33.3) 1 (7.7) |
9.2 (1.39- 61.06) 10.4 (1.4- 70.12) 13.6 (2.07- 89.4) 4.3 (0.37- 51.29) 1.0 |
0.021 0.016 0.007 0.245 |
| Orbital extension Absent Present |
18 (27.7) 12 (92.3) |
47 (72.3) 1 (7.7) |
9.4 (1.42- 62.16) 1.0 |
0.020 |
| Necrosis None Mild Moderate Severe |
3 (13.6) 8 (44.4) 3 (25) 16 (61.5) |
19 (83.4) 10 (55.6) 9 (75) 10 (38.5) |
2.3 (1.34- 2.75) 1.4 (0.76- 2.73) 1.95 (1.08- 3.50) 1.0 |
0.002 0.259 0.025 |
Table 5.
Shows predictors of 2- year survival at multivariate analysis.
| Variable | Adjusted RR (95% CI) | P value |
|---|---|---|
| Gender Female Male |
1.4 (1.07- 1.70) 1.0 |
0.009 |
| Leukocoria Present Absent |
1.1 (1.10- 1.11) 1.0 |
0.000 |
| Optic nerve (ON) invasion Absent Prelaminar ON invasion Intralaminar ON Retrolaminar ON Surgical margin ON |
6.0 (0.85- 42.3) 7.0 (0.99- 49.27) 7.6 (1.08- 53.98) 2.4 (0.18- 31.04) 1.0 |
0.072 0.052 0.042 0.504 |
| Orbital extension Absent Present |
7.0 (1.00- 49.25) 1.0 |
0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



