
Submitted:
04 September 2023
Posted:
06 September 2023
You are already at the latest version
Abstract
Although the frequency of myocarditis in the general population is very difficult to accurately determine due to the large number of asymptomatic cases, the incidence of this disease is increasing significantly due to better defined criteria for diagnosis and the development of modern diagnostic method. The multitude of different etiological factors, the diversity of the clinical picture and the variability of the diagnostic findings make this disease often demanding both for the selection of the diagnostic modality and for the proper therapeutic approach. The previously known most common viral etiology of this disease is today overshadowed by new findings based on immune-mediated processes, associated diseases that in their natural course can lead to myocardial involvement, but also the iatrogenic cause of myocarditis due to use of immune checkpoint inhibitors in the treatment of cancer patients. Suspecting that a patient with polymorphic and non-specific clinical signs and symptoms, changes in ECG and echocardiography has myocarditis is the starting point in the diagnostic algorithm. Cardio magnetic resonance imaging is non-invasive diagnostic gold standard for diagnosis and clinical follow-up of thses patients. Endomyocardial biopsy as an invasive method is the diagnostic choice in life-threatening patients with suspicion of fulminant myocarditis where the diagnosis has not yet established or there is no adequate response to the applied therapeutic regimen. The treatment of myocarditis is increasingly demanding and includes conservative methods of treating heart failure, immunomodulatory and immunospressive therapy, methods of mechanical circulatory support and heart transplantation. The goal of developing new diagnostic and therapeutic methods is to reduce mortality from this complex disease, which is still high.
Keywords:
acute myocarditis
; chronic inflammatory cardiomyopahty
; heart failure
; cardiac magnetic resonance
; endomyocardial biopsy
1. Definition and epidemiology of myocarditis
Myocarditis is a disease of the heart muscle caused by inflammation, which is the most often the result of an infectious process, but it can also be caused by hypersensitivity to drugs, radiation, metabolic disorders, collagenoses, sarcoidosis, Kawasaki disease, exposure to excessive heat and chemicals [1,2]. The prevalence of myocarditis in the general population is difficult to determine because a large number of patients remain undiagnosed, but it roughly ranges from 10.2 to 105.6 per 100,000 worldwide, and its annual occurrence is estimated at about 1.8 million cases [3]. A Swedish study by Fu M. and associates indicated an increase in the incidence of myocarditis from 6.3 to 8.6 pet 100,000 from 2000 to 2014 [4]. This increase in incidence can be explained by better diagnosis of myocarditis and better defined criteria for diagnosing myocarditis. Autopsy studies have shown the presence of myocardial inflammation in 6-42% of autopsies after sudden cardiac death [5,6]. According to modern registries, myocarditis is a disease of the younger population with an average age between 30 and 45 years of age and is considered one of main causes of sudden cardiac death in young people. Myocardial disease is the cause of death in 25% of suddenly deceased patients under the age of 21, and in 20% of cases this disease is a precursor to dilated cardiomyopathy (DCM), which is the most common reason for heart transplantation today [7,8].
Special attention was paid to this disease by the world public during the outbreak of the SARS-CoV-2 virus pandemic, considering that as many as 28% of patients had myocardial damage accompanied by an increase in the value of cardio specific troponin [9]. Data from a respective cohort study indicate that 54% of patients after confirmed COVID-19 infection had an cardiac magnetic resonance (CMR) finding that indicated myocarditis (myocardial edema or late gadolinium accumulation)[10]. There is evidence that the probability of occurrence of myocarditis is up to seven times higher in unvaccinated patients compared to patients who received the SARS-CoV-2 virus vaccine [11].
Men are 2 to 4 times more likely to suffer from myocarditis than women [12]. Affected men are more often younger than women, and the highest rate of occurrence of the disease in men is between 16 and 20 years of age, while women were the most affected at the age of 56-60 [13,14,15].
Myocarditis is a very common disease in children, and due to the heterogeneity of symptoms of the clinical picture, the diagnosis is made only in 17% of patients during the first examination [16]. Today, the incidence rate in children aged 0-15 years is estimated at 1.95/100,000 persons per year [17]. In the children’s population, myocarditis is most common in boys.
2. Etiological factors and pathophysiological mechanisms of myocarditis
2.1. Infectious causes of myocarditis
Cardiotropic viruses are the most common causes of myocarditis, which lead to cardiomyocyte damage through direct cardio toxic effects. These viruses primarily include enteroviruses (Coxsackie A and Coxsackie B virus, echoviruses) and adenoviruses [18]. Genetic predisposition can affect the increased susceptibility to infection caused by cardiotropic viruses and the development of the chronic course of the disease [19]. In addition to cardiotropic viruses, the causative agents of myocarditis are vasculotropic viruses (erythroviruses – parvovirus B19) and lymphotropic viruses (herpes viruses, Epstein Barr virus; Cytomegalovirus) [18]. Cytomegalovirus and Toxoplasma gondii are potential causes of myocarditis in heart transplant patients [20,21]. Viruses mostly act through the activation of the immune system, the appearance of a cytotoxic storm of immune mimicry [22]. Such viruses are human immunodeficiency virus, hepatitis C virus, influenza A and B viruses as well as SARS-CoV 1and 2 viruses [18]. A special mechanism of action was discovered in the SARS-CoV-2 virus, which causes direct damage to cardiomyocytes by acting on Angiotensin II receptors [23,24]. Enteroviruses, which are one of the most common causes of viral myocarditis, bind to specific receptors on cardiomyocytes, multiply, and cell lysis follows. In about 50% of these patients, there is a spontaneous clinical recovery, while the persistence of the virus genome in the myocardium most often leads to left ventricular dysfunction and a worse clinical outcome [25]. Today, with the development of molecular technology, other viral agents of acute myocarditis (AM) such as PVB19 and HHV61 have emerged [26,27]. PVB19 is a virus that can cause both virus-mediated and virus-induced myocarditis. In children, PVB19 causes systemic infection associated with AM where PVB19 can be detected in both plasma and myocardium [28].
There are two mechanisms of myocardial damage during viral infection:
(1) direct cytotoxic effect (Murine model: virus penetration into myocytes, their binding to a specific receptor, virus replication and consequent necrosis of myocites, binding to intracellular agents (myosin) and activation of the immune system characterized by the invasion of natural killer cells and macrophages accompanied by T lymphocytes.
(2) secondary phase (autoimmune reaction).
After the acute phase of viral-mediated myocarditis, there are three generally accepted clinical possibilities: (1) the virus clears without residual inflammation, resulting in complete healing; (2) viral infection persists with or without inflammation; or (3) viral infection results in autoimmune-mediated inflammation that persists despite viral clearance [29]. If the infectious agent is quickly eliminated and the inflammatory process ends, the disease will be cured with only minor changes in myocardium. If irreversible myocardial damage has developed, the clinical picture evolves into DCM [29].
Infection with the human immunodeficiency virus (HIV) is a global problem. A large percentage of patients with HIV infection suffer from myocarditis, although the incidence of myocarditis associated with HIV infection has been declining in recent years [30]. However, in contrast, the incidence of heart failure (HF) is increasing, primarily due to HF with preserved ejection fraction [31,32]. Today, the estimated incidence of DCM associated with HIV-disease is 1.6% [33]. It has been shown that there is no clear association between HIV infection and cardiomyocyte dysfunction. However, it has been shown that the presence of the virus can condition the appearance of an inflammatory response and the activation of cytokines and consequent damage to cardiomyocytes [34]. An additional important factor in the occurrence of myocarditis and DCM associated with HIV infection are opportunistic infections [35]. Of course, the toxic effects of ARV therapy cannot be ignored either [36]. According to autopsy data published before the ART era, myocarditis was diagnosed in 40-52% of patients who died of AIDS [37].
Although in patients with myocarditis the viral etiology of the disease is always thought of first, other infectious agents should also be considered. A detailed travel history must be taken to assess the possible risk of schistosomiasis (primarily in Africa, but also in Japan, China, the Middle East, South America, the Caribbean) Chagas disease (North America, Europe, Japan, Australia), tuberculosis (Asia and Africa, Eastern Europe), or Hepatitis C (Japan). In endemic areas, the presence of dengue fever must also be considered [3,38].
2.2. Eosinophilic myocarditis
Eosinophilic myocarditis (EM) is characterized by the presence of eosinophilic infiltration in myocardial tissue. EM may be accompanied by a hematologic disorder (hypereosinophilic syndrome (idiopathic form) or myeloproliferative form of the disease) characterized by persistent eosinophilia (>1,5 x109/L for more than 6 months) and organ damage [39,40]. About 20% of patients with this syndrome have myocardial involvement [41]. EM has been observed to be associated with hypersensitivity reaction to chemical and some drugs (b-lactam antibiotics, clozapine, carbamazepine, minocycline, etc.) [42,43,44,45]. Sometimes parasitic infections and malignancies can be associated with EM [46,47]. EM can occur with some systemic diseases such as the association of eosinophilic granulomatosis with polyangiitis [48].
2.3. Giant cell myocarditis
Giant cell myocarditis is a rare type of rapidly progressive myocarditis. The incidence of giant cell myocarditis (GCM) ranges from 0.007% to 0.051% [49]. A large post-mortem study reported that GCM is responsible for approximately 10% of fulminant form of myocarditis (FM) [50]. Pathohistologically, significant destruction of the myocardium mediated by a large number of cytotoxic T cells, macrophages, giant cells and eosinophilis was observed within this myocarditis. It is believed that there is an association of this type of myocarditis with immune/allergic processes [51]. It is characterized by sudden onset of HF and refractory malignant ventricular forms of arrhythmia (about 55%) [52]. In the differential diagnosis, it is necessary to distinguish it from myocarditis in sarcoidosis.
2.4. Myocarditis associated with immune checkpoint inhibitors
The use of immune checkpoint inhibitors (ICIs) as anticancer drugs has increased significantly in recent years. As part of their application, an increased incidence of myocarditis was observed, up to 1.9% [33,53]. Acute myocarditis the most often occurs in the first month after the start of drug administration [54]. Patients with AM after administration of ICI have a high mortality rate [53,55].
2.5. Myocarditis associated with systemic diseases
The pathogenesis of myocarditis with autoimmune systemic diseases is based on the deposition of immune complexes, activation of complement, etc. Systemic diseases most often caused the appearance of myocarditis in patients between 25 and 60 years of age. Cardiac lesions are found in 40-60% of autopsy patients who suffered from systemic lupus erythematosus, 50-80% of patients suffering from scleroderma, and in 38% of patients previously suffering from dermatomyositis [39,56].
3. Division of myocarditis
Myocarditis can be classified according to the etiological factor that causes it, the severity of the disease, the dominant symptoms and the pathohistological findings [1,38]. Sometimes a combination of the aforementioned criteria classifies the patient in a certain phenotype.
According to the traditional pathohistological Dallas criteria, examination of the biopsy obtained by endomyocardial biopsy (EMB) with a light microscope can initially indicate whether it is active myocarditis or borderline myocarditis. Active myocarditis is presented by the presence of an inflammatory infiltrate in the myocardium with necrosis and/or degeneration of adjacent myocytes, unlike borderline myocarditis where there is an inflammatory cell infiltrate in the myocardium but without cell necrosis [57].
Based on the histopathological diagnosis of the myocardium and according to the type of cellular infiltrate, we distinguish between lymphocytic, eosinophilic and polymorphic myocarditis, giant cell myocarditis, and granuloma [38].
According to the etiological factor, myocarditis can be divided into those caused by infectious and non-in factious agents. Infectious myocarditis is caused by viruses, protozoa, bacteria, fungi, pathogens that cause direct injury to the myocardium [58]. When myocarditis is cause by a viral infection, the result of which is a direct cytotoxic effect on the myocardium, then we are talking about virus-mediated myocarditis. It occurs under the influence of myocardiotropic viruses, such as Coxackie virus. Non-infectious myocarditis occurs as a result of damage to cardiomyocytes through the direct effect of toxic noxa (drugs, chemicals, vaccines) as a result of hypersensitivity reactions, immune processes, under the influence of radiation or as a part of systemic disease [59,60]. In the case of immune-mediated lymphocytic myocarditis (Virus-triggered myocarditis), we do not have the presence of a viral genome in the myocardium, but the connection between viral infection and the appearance of AM is clearly correlated (e.g. in the case of influenza) [29]. Immune-mediated myocarditis caused by damage to cardiomyocytes in autoimmune processes (seen in heart transplantation – alloantigenes or in systemic diseases – systemic lupus erythematosus, rheumatoid arthritis, Churg-Strauss syndrome, thyrotoxicosis, sarcoidosis, Wegener’s granulomatosis – autoantigens) [38,61,62].
Myocarditis caused by hypersensitivity reactions primarily due to the use of drugs are classified as Hypersensitivity myocarditis (allergic myocarditis) [61,63]. Myocarditis caused by the direct cytotoxic effect of the drug is called Drug-induced myocarditis [1].
Based on clinical features, myocarditis can be divided into AM, chronic myocarditis (CM) and chronic inflammatory cardiomyopathy (CIC) [1]. According to the consensus of experts of the American HF Association, subcute myocarditis (SM) is also included in the clinical division, while in the Japanese Association of Cardiology guidelines, chronic active myocarditis (CAM) and postmyocarditis cardiomyopathy (PMC) are included in the clinical division [1,39]. In both of these documents, inflammatory dilated cardiomyopathy (IDC) is conceptually included in the frame work of HIC. Recent views and consensuses of experts have shown a tendency to classify all myocarditis clinically in one of two forms – AM and CIC [1,39].
3.1. Acute myocarditis
AM is predominantly a clinical diagnosis of myocarditis, which includes a time frame until the diagnosis is made and, if EMB was performed, the presence of findings that are characteristic of active myocarditis. According to the more recent criteria of the American Heart Association (AHA) and the Japanese Association of Cardiology (JAC) AM is that myocarditis in which symptoms started within one month of diagnosis (according to the earlier guidelines of the European Society of Cardiology (ESC), AHA and JAC up to 3 months) [1,38,39,64]. AM is accompanied by an increase in the level of high sensitive troponin, the presence of myocardial edema diagnosed on CMR and infiltration of mononuclear cells with fusion or necrosis of cardiomyocytes proven by the finding of EMB [65,66].
3.2. Subacute myocarditis
SM is a myocarditis in which the symptoms are present or have worsened more than 3 months before the diagnosis (according to the ESC consensus). According to the AHA expert consensus, SM is considered myocarditis when the diagnosis is made between 1 and 3 months after the onset of symptoms. According to clinical and histopathological characteristics, it can also be defined as myocarditis in healing, with previously clear evidence of AM [67].
3.3. Chronic myocarditis
CM may represent as intermediate stage between AM and CIC. It is defined as an ongoing inflammatory process with fibrosis, but also without necrosis or abnormality of cardiomyocytes [1,39]. The diagnosis is established if the symptomatology lasts longer than 3 months until the diagnosis according to the ESC guidelines, i.e. longer than 1 month according to the JAC guidelines [38,39]. The AHA consensus does not clearly define the time frame for CM [1]. The term chronic active myocarditis is only described within JAC recommendations and is defined as myocarditis after 30 days from the onset of symptoms with a histopathological picture of active myocarditis [39].
3.4. Chronic inflammatory cardiomyopathy
It indicates a chronic inflammatory condition in which there is a constant infiltration of the myocardium with inflammatory cells, without clear signs of myocardial necrosis [39]. Cardiomyocyte abnormality with local or diffuse fibrosis is expected. This finding is present more than 30 days after the onset of symptoms. Ventricular remodeling accompanied by cardiac failure is present. It can present with dilated cardiomyopathy (inflammatory dilated cardiomyopathy) or a form without dilated cardiomyopathy (hypokinetic phenotype) [1].
4. CLINICAL PICTURE
Myocarditis is a disease characterized by polymorphic signs and symptoms. The reason for this lies both in the different etiological factors that led to myocarditis on the one hand and on the other hand in symptomatology, which is different depending on the stage of the disease in which the patient was first examined. The clinical picture can vary from asymptomatic cases to sudden cardiac death due to cardiogenic shock and malignant rhythm disorders [68]. The disease can occur in patients of all age groups, although it is most common in young people [69].
None of the symptoms in patients with myocarditis are specific to this disease. Apart from the symptoms related to the damage and inflammation of the myocardium itself, the symptoms of other organ systems that can be affected by the infectious agent are also important. According to all guidelines, the most important first point in the diagnostic algorithm is to suspect that the patient has myocarditis, given the polymorphism and non-specificity of the symptoms.
- Acute (non-fulminant) myocarditis – about 65% of patients have this form of myocarditis [70]. This phenotype includes asymptomatic cases, cases in which some degree of cardiac damage may occur with partial or complete regression [33]. These patients have a clinical, electrocardiographic picture and biohumoral syndrome similar to acute myocardial infarction (AMI). In rare cases, death occurs [71].
- Fulminant myocarditis (FM) – there are about 8.6% of all patients with myocarditis [72]. It is characterized by an acute onset of the disease, which is characterized by rapid deterioration and usually death [33]. Usually, patients present with symptoms and signs of HF (up to pulmonary edema) and not infrequently up to cardiogenic shock, and the clinical course is accompanied by malignant arrhythmias. In these patients, inotropic stimulation or mechanical circulatory support is usually required [39,73]. Patients with FM compared to patients with a non-fulminant form of this disease have a higher early mortality ((28.0% vs. 1.8%, p=0.0001) and late mortality during 7 years of follow-up (47.7% vs. 10.4%, p<0.0001) respectively [71]. Earlier studies that monitored the prognosis of patients with FM showed conflicting results regarding the long-term prognosis [74,75,76]. Ammirati E. et al also showed a correlation between the histological subtype of FM and patient prognosis. Giant cell FM is associated with a significantly worse patient prognosis compared to eosinophilic and lymphocytic subtypes of myocarditis [71].
- Chronic persistent myocarditis (7% of cases) – it is characterized by a mild onset of the disease, usually without cardiac decompensation [33].
4.1. Symptoms related to the previous infectious agent
In the case of viral infectious etiological factors, patients usually have symptoms related to respiratory, gastrointestinal system or symptoms similar to a common cold two weeks before the appearance of specific symptoms [77,78]. General symptoms are present in about 80% of patients, and the most common are: chills, fever, elevated body temperature, headache, myalgias, atralgias, fatigue, sweating. Signs of upper respiratory tract infection (sore throat, cough) and gastrointestinal symptoms (loss of appetite, nausea/vomiting, diarrhea, nonspecific abdominal pain) are not uncommon [72,79,80,81]. According to the HERMES-HF register, 60%of patients with AM have symptoms related to infections of the respiratory system (90% - elevated body temperature, 50% - sore throat, 44.3% - cough) 15% of patients have gastrointestinal symptoms (100% - diarrheal syndrome, 78% - fever, 56% - abdominal pain, 30% - vomiting) [82].
4.2. Chest pain
In patients who report chest pain at initial presentation, the suspicion of myocarditis can be aroused by the anamnestic data of a respiratory or gastrointestinal infection present 1-4 weeks before the onset of symptoms. Chest pain in the case of myocarditis or myopericarditis occurs in 75-95% of patients [81,83,84,85]. The pain may resemble typical angina when it is very important to make a differential diagnosis in relation to AMI [86]. When the pericardium is affected by inflammation, the pain can have different characteristics. The pain is then usually sharp, intensifies during inspiration, forced coughing, and decreases when sitting [87]. In patients with myocarditis, chest pain can also occur as a result of microvascular dysfunction [88]. Spasm of coronary blood vessels caused by inflammation can also be the cause of pain [89]. Among the first descriptions of transient spasm of coronary blood vessels in patients with proven lymphocytic myocarditis was given by Mc Culli et al. [90].
4.3. Symptoms and signs of heart failure
Patients with HF may present first with fatigue, both during normal physical exertion until fatigue and at the slightest physical exertion. In AM patients have dyspnea and orthopnea in 19-49% [82,91]. Studies have shown that in patients with reduced left ventricular ejection fraction (EF LK<45%) dyspnea is present in as many as 98.1% of patients, and that patients with preserved EF have less dyspnea and that the dominant symptom is chest pain [92]. Late inhaling crackles over lung fields are registered during physical examination of the patient. Auscultation of the heart registers the presence of the third heart sound – S3, tachycardia, systolic murmur of mitral and tricuspid regurgitation. In some patients, we have signs (swollen neck veins, pretibial edema) and symptoms of right heart failure. In the most severe cases, the patient will present with a picture of cardiogenic shock, the need for inotropic stimulation or mechanical support [93,94].
According to data from the multicenter Lombardy registry, about 26% of patients with AM are complicated by the appearance of HF with reduced EF [72]. The results of this registry suggest that patients with AM can be effectively stratified based on their initial clinical presentation. For patients who have HF with EF <50% (assessed by initial echocardiographic examination), the occurrence of self-sustaining ventricular tachycardia or the need for inotropes or mechanical circulatory support, it can be said that they have complicated AM with high short-term and long-term mortality (11.9% vs. 18%) [72]. Other studies also showed a negative predictive value of the occurrence of HF and the presence of malignant ventricular arrhythmias on the outcome of patients with AM [93,94].
4.4. Arrhythmias
The development of arrhythmias in myocarditis is most often a consequence of the development of focal foci in the sensitive and damaged part of the myocardium [95]. Dysfunction of ion channels as well as myocardial ischemia potentiates the electrical instability of cardiomyocytes [96]. Myocarditis can be complicated by both atrial and ventricular arrhythmias. Different types of potentially life-threatening bradyarrhythmias and tachyarrhythmias can be registered at any stage of the disease as an expression of electrical instability of the myocardium [95,97,98].
Sinus tachycardia is registered in about 26.7- 57% of patients [82,99]. Atrial fibrillation is not rare and is registered with a frequency of 3% to 14% [39,100]. It is more often registered in patients with a more severe clinical picture and previous heart diseases [100].
Patients with ventricular rhythm disturbances can have a wide range of symptoms from palpitations (14.4%), syncope to sudden cardiac death [97,101]. Ventricular arrhythmias are most often registered in the acute phase and vary from isolated extra systoles to complex and life-threatening ventricular tachycardia that can lead to sudden death. Ventricular arrhythmias are particular common in patients with FM, especially in patients with GCM (29%) and sarcoidosis (55%) [95].
In the event of conduction disturbances, patients may complain of unsteadiness while walking, dizziness, lightheadedness or loss of consciousness. Atrioventricular blocks are most often registered in patients with GCM, patients with sarcoidosis or Lyme disease [102,103,104]. In the chronic phase of myocarditis, life-threatening arrhythmias occur due to the development of recurrent myocarditis, residual dysfunction of the left ventricle, and the formation of a post-inflammatory scar of the myocardium.
4.5. Syncope
Syncope is reported in 6% of patients with myocarditis during the initial presentations [72]. Syncope occurs more often in patients with the fulminant form of the disease [71]. It can be a consequence of the development of severe HF and consequent cardiogenic shock, but it can also occur as a consequence of ventricular rhythm disorders or conduction disorders.
4.6. Myocarditis in children
In about 83% of children’s cases, the diagnosis of myocarditis is not made at the first visit to the doctor, but usually takes two or more visits to the doctor before the diagnosis of myocarditis is made [105]. As in adults, the symptoms and signs of myocarditis can be non-specific. General signs and symptoms such as fever, chills, increased sweating and loss of appetite may precede. The clinical picture may include dyspnea, vomiting and the appearance of diarrhea stools [106]. The occurrence of dysrhythmias is common in the pediatric population with myocarditis and indicates a worse prognosis of the disease [105]. According to the studies of S Aliaa et al., the largest number of children (76.5%) presents with symptoms and signs of congestive HF without hemodynamic instability, while 11.8% of patients develop a fulminant form of the disease [105].
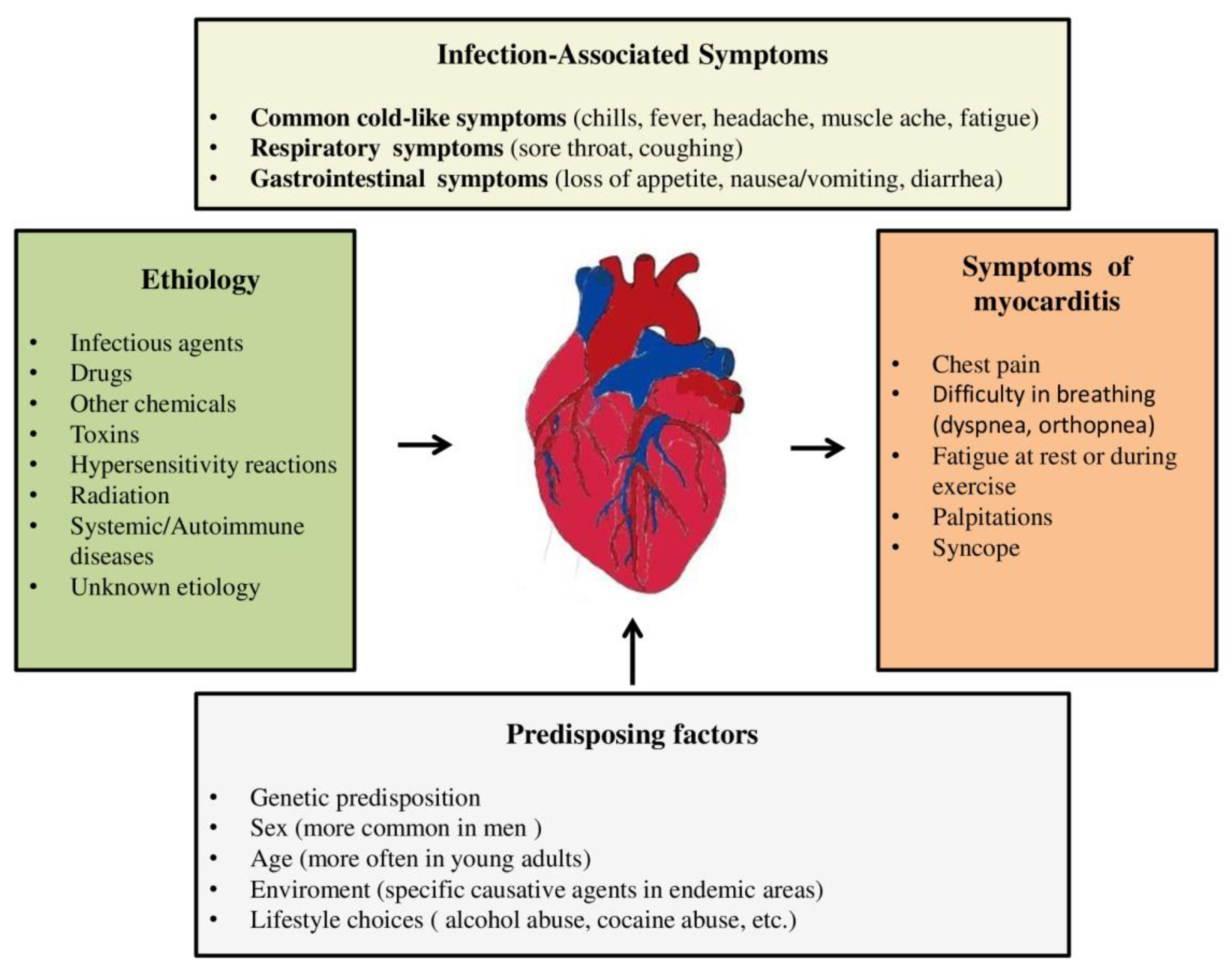
According to the ESC recommendations, clinically suspected myocarditis requires one or more clinical criteria (acute chest pain or new-onset dyspnea or palpitations/unexplained arrhythmia cardiogenic shock) and ≥1 diagnostic criteria from different categories (ECG features of heart injury, elevated markers of myocardial necrosis, functional/structural abnormalities on echocardiogram/angiogram or CMR), in the absence of angiographically detectable cause that could explain the existing syndrome [38]. In addition to anamnestic data on previous on previous infection, it is important to pay attention to other potential causes of myocarditis, such as recent exposure to medications, taking drugs, consuming raw meat, or travelling in areas where there are specific viral or bacterial pathogens. Also, data on previous disease and conditions that could be associated with the occurrence of myocarditis are of a great importance (Figure 1).
Figure 1.
Etiology, predisposing factors and symptoms of myocarditis.
5. DIAGNOSIS OF MYOCARDITIS
As myocarditis is a disease with a wide clinical spectrum, from asymptomatic cases to sudden cardiac death, a large number of patients remain undiagnosed. The lack of non-invasive tests with high specificity and sensitivity is another reason why the diagnosis of myocarditis is often missed. Diagnostic includes physical examinations, teleradiography of the heart and lungs, echocardigraphic examination, 24-hour ECG Holter monitoring, CMR heart examination, cardiac catheterization and EMB. Non-invasive diagnostic methods such as CMR can be useful in diagnosing myocarditis and monitoring the progression of the disease. EMB is the gold standard in the final diagnosis of myocarditis, but not all patients with suspected myocarditis should undergo EMB, but only patients with an unconfirmed diagnosis, especially with a pseudoinfraction image [69,107].
5.1. ECG in myocarditis
Changes in the electrocardiogram can be seen in approximately 90% of patients with AM [81,108]. A 12-lead ECG should be performed in all patients with clinically suspected myocarditis despite its low sensitivity (47%) for myocarditis [33,109]. Both supraventricular arrhythmias (sinus tachycardia, atrial fibrillation/flutter) and ventricular arrhythmias (ventricular extra systoles, ventricular tachycardia and ventricular fibrillation) are common. Conduction disorders (atrioventricular blocks, bundle branch block, defects in interventricular conduction) are also not rare [110,111,112].
Of all the arrhythmias, sinus tachycardia occurs most often with variable frequency [113]. Studies suggest that the occurrence of sinus tachycardia is often associated with the development of HF, especially in FM [114]. Repolarization changes at the level of the ST segment and T waves, changes in the height of the R teeth, the appearance of pathological Q teeth are also often registered in these patients. ST segment elevation is registered more often (prevalence between 24-75%) than ST depression [115]. ST elevation in myocarditis most often occurs when the pericardium is also affected. ST elevation is presented in almost all leads in the ECG and is not accompanied by reciprocal ST depression in the contra lateral leads (except in aVR and V1) [116]. ST elevation in myopericarditis is concave while in AMI is convex upwards [117]. Patients with initial ST elevation in the electrocardiogram may develop further evolutionary changes in the form of negative T waves (81.6% of patients), most often on the fourth day after the initial ST segment elevation [114]. However, the evolutionary appearance of negative T waves in the electrocardiogram is not associated with a worse clinical outcome. One condition, which can also be confused with acute perimyocarditis, is benign diffuse ST elevation, called “early repolarization with ST elevation” (ERSTE) [118]. ERSTE is accompanied by diffuse ST segment elevation in the inferior and anterolateral leads. ST depression is present in about 9-18% of patients with acute myocarditis [119,120].
Isolated T wave changes are seen in 9-48% of patients with AM [114,120,121]. Most often, it is an inversion of the T wave. The importance of this change is also reflected in the differential diagnosis, because patients with AMI can also have symmetrical, deep, negative T waves. In the study by De Lazzari et al., it was determined that the presence of negative T waves in the electrocardiogram correlates with the extent of myocardial edema assessed by T2-weighed CMR sequences [122].
Depression of the PR segment can occur in about 2% of cases of myocarditis [4]. It occurs quite often in myopericarditis [123].
Reduction in the amplitude of the QRS complex is seen in about 10% of patients with acute myocarditis [39]. The most common reason for low QRS voltage is the occurrence of pericardial effusion. Nakashima H. et al. showed in their study that 18% of patients with AM have a significant reduction of QRS amplitude during the acute phase of the disease regardless of the presence of pericardia effusion [110]. From a pathophysiological point of view, myocardial edema can be one of the causes of low QRS complex voltage [115,124]. Also, a study by Chen J. et al, showed that low QRS complex voltage was present in 44 out of 274 patients and this sign was associated with the occurrence of FM [114]. Low voltage of the QRS complex in the ECG was an independent predictive factor for the occurrence of FM.
The prevalence of a wide QRS complex in AM is variable and depends on the severity of the clinical picture (12%-25%) [39,125]. According to some studies, that percentage goes up to 70% if it is about FM [126]. A QRS complex of ≥120 msec duration (including the block of the left and right branches of the bundle of His) is an independent predictive marker for FM [71,114]. Ukene et al. pointed out that prolonged duration of the QRS complex is a significant independent predictor of cardiac death or the need for a heart transplant [125]. In a study by Nakashima H. et al., bundle branch blocks of His occurred in 55% of patients with equal prevalence of right and left bundle branch blocks [110,115].
Ventricular tachycardia (VT) is registered in 6.2% of patients with AM, and the results of the study showed that its occurrence is an independent predictive factor of FM and a worse outcome [114]. VT occurs with a much higher frequency in GCM (up to 55%), in EM (11%) and cardiac sarcoidosis (29%) [52,127,128].
The prevalence of first-degree AV block I occurs with a frequency of 4-11% [39,129]. A study by Morger T. et al. showed a prevalence of advanced or complete AV block of 15.5% [129]. Ogunbayo GO et al. showed that the incidence of cardiogenic shock, respiratory failure and renal failure were higher in patients with high degree AV block compared to patients without conduction disorders (26.2% vs. 5.0%, 33.9% vs. 5.9% and 29.2% vs. 5.5%, p<0.001 respectively) [111]. A high frequency of AV blocks was seen in Lyme carditis (40%), cardiac sarcoidosis (30%), GCM (31%) [130,131,132,133]. In their study, Chen J. et al. showed by multivariate logistic regression analysis that independent predictive factors associated with FM were the occurrence of ventricular tachycardia, high degree AV block, low QRS complex amplitude and QRS complex duration of ≥120 ms. The appearance of pathological Q wave and prolonged QT interval >440 ms were also identified as predictors of poor outcome [114].
5.2. Biomarkers
Today, a large number of laboratory parameters are used for both diagnostic and prognostic purposes in myocarditis.
- Markers of inflammation: high-sensitivity C-reactive protein (hs-CRP), elevated leukocyte count and accelerated sedimentation.
Leukocytosis, elevated CRP values and accelerated sedimentation are always found in patients with myocarditis, but their diagnostic value is low due to their presence in many other diseases [134]. Elevated CRP values and accelerated sedimentation are present as many as 80-99% of patients [39]. The presence of eosinophilia can be indicated on EM (it occurs in 75.9% of patients) [127]. New inflammatory biomarkers under investigation include necrosis factor of tumor-alpha, interleukin 10, interleukin 6, interferon-g, serum soluble Fas, and soluble Fas ligand levels. Elevation of these markers indicates a worse prognosis, although they are not taken as part of routine laboratory analyses [135,136]. More recent studies have shown elevated levels of heparin-binding protein (HBP) in patients with myocarditis [137]. Also, proinflammatory molecules released from monocytes and neutrophils (alarmin S100A8 and S100A9) proved to be significant predictors of myocardial damage, and the highest values in myocarditis were observed in the acute phase of the disease [138]. Serum S100A8/A9 levels in patients with recent-onset myocarditis have been shown to reflect inflammatory disease activity in cardiac tissue independent of viral persistence, age, or sex [138]. Sera soluble ST2 affects the reduction of the proinflammatory activity of IL 33. In a study conducted on 330 male patients younger than 50 years of age with myocarditis, significantly elevated values of sST2 were registered. Elevated values of sST2 correlated with the severity of HF (the same was nor proven for patients older than 50 years) [139]. In their studies, Mirna M and al. examined the ratio of neutrophils and lymphocytes as well as the ratio of neutrophils and monocytes on the severity of myocarditis. Both ratios have been shown to correlate with disease severity followed by longer hospital stay [140].
- b.
- Markers of myocardial damage
None of the markers of myocardial damage available so far are specific enough to demonstrate myocardial inflammatory processes. The diagnostic value of these markers varies depending on the time they are taken relative to the onset of the disease. Within AM, the levels of aspartate aminotransferase (AST), lactate dehydrogenase (LDH), creatine kinase (CK-MB), highly sensitive troponins (troponin T and troponin I) and myoglobin are elevated [141,142]. Troponins can be used to demonstrate cardiomyocyte degradation due to myocardial infarction, myocarditis, cardiac arrhythmias, etc. However, on the basis of troponin values, a distinction cannot be made between ischemic and inflammatory cardiomyocyte injury. Elevated troponin values can also be found in other diseases such as aortic dissection, pulmonary thromboembolism, injures sepsis, etc [143]. When it comes to myocarditis, troponin is elevated in at least 50% of patients with proven EMB myocarditis. Most often, troponin values are negative due to the delay in taking a blood sample compared to the onset of the disease. Liu C. et al. examined the absolute and relative changes in hs-cTnI within 24 h and 48 h after admission to the hospital in patients with AM. They showed that absolute changes and relative changes in hs-cTnI within 24 h and 48 h were strong predictors of in-hospital mortality by Cox regression analysis after adjustment for sex, time from onset to admission, and occurrence of VT or VF [144]. Most FM patients who survived experienced a decline in hs-cTnI within 24 h [144]. Today, in the era of ICI use and associated myocarditis, Tn values have been shown to be indispensable for monitoring these patients. High-sensitive TnI levels are significantly elevated in patients with ICI-induced myocarditis [145]. Early detection of this myocarditis is essential because timely treatment greatly improves the outcome.
- c.
- Dysfunction markers
B-type natriuretic peptide (BNP) and N-terminal pro BNP (NT-proBNP) are widely used as diagnostic biomarkers for HF and cardiac dysfunction in clinical medicine. They are released from cardiomyocytes when there are elevated values of ventricular filling pressure. Their measurement in patients with myocarditis and suspected HF is recommended [1]. A more recent study by Sara B. et al. showed that NT-proBNP is significantly correlated with markers of inflammation (leukocyte count and CRP value) in patients with AM [146]. A study by Uken C. and colleagues showed that a high value of NT-pro BNP in patients with myocarditis was predictive for cardiac death of heart transplantation (hazard ratio 9.2; 95% confidence interval 1.7-50; p=0.011) [147].
- d.
- Anti cardiac antibodies
Heart-specific autoantibodies (anti-cardiac autoantibodies) are found in the peripheral blood of patients with myocarditis. The expression of autoantibodies against the heart is the result of the induction of autoimmunity during the process of the immune reaction in order to eliminate the causative agent. In fact, in case of myocarditis and DCM, there may be anti-cardiac autoantibodies against various tissues, including the contractile structure of the heart (myosin), the extracellular matrix (laminin) [148]. Autoantibodies against the heart are detected in about 60% of all patients with myocarditis in the chronic phase [18]. In patients who do not have myocarditis, they are detected in 1-3% [149]. Therefore, their use in screening for myocarditis is expected. The presence of anti cardiac antibodies strongly correlates with the prognosis of patients with myocarditis [150]. In AM, their presence may indicate the risk of cardiac death or the need for a heart transplant [151]. The presence of anti-cardiac antibodies in patients with chronic myocarditis is associated with possible deterioration of cardiac function in the future and transition to DCM.
- e.
- Micro RNA
MicroRNAs (miRNAs) are single-stranded, non-coding RNAs that are not translated into protein, and act on protein-coding mRNA and regulate gene expression. An increase in blood mRNAs was observed in patients with AM [152]. Various clinical studies have shown that the levels of multiple miRNAs can be increased or decreased in serum and tissue obtained from patients suffering from myocarditis [153,154,155]. It has been demonstrated that mRNA expression is higher in AM patients than in healthy individuals or in AMI patients. The expression of mRNA allows the differentiation of AM from AMI with an accuracy of ≈93% [39]. miRNA levels were often different in patients suffering from myocarditis compared to patients with other heart diseases, making them promising diagnostic biomarkers [156]. Determination of micro RNA is particularly important in order to obtain gene therapy in the treatment of myocarditis.
- f.
- Viral antibodies
In the acute and convalescent phase of the disease, virus titers are positive in less than 40% of cases. The diagnosis of myocarditis cannot be made by determining only the titer of antibodies to cardiotropic viruses in the serum. The diagnosis of possible viral myocarditis is established by the presence of a fourfold increase in the titer of virus antibodies in two samples 3-4 weeks apart with the corresponding clinical picture, echocardiographic findings and CMR findings. Routine viral serology testing is not recommended.
Today, new biomarkers such as pentraxin 3, galectin 3 and growth differentiation factor are also in use. Total and microribonucleic acid transcriptomic biomarkers promise to improve the diagnostic and prognostic assessment of myocarditis in the future.
5.3. Echocardiography
Echocardiography is a standard diagnostic method that should be performed in all patients with suspected myocarditis in order to exclude other causes of HF, reveal the presence of intracardiac thrombi and associated valvular disease. Echocardiography quantifies the degree of systolic and diastolic dysfunction of the left ventricle. It is used to visualize the thickness of the left ventricular wall and to measure the endocavitary dimensions of the chambers. An echocardiographic examination in patients with myocarditis can reveal thicker walls of the left ventricle with abnormal echogenicity of the myocardium due to interstitial myocardial edema, global ventricular dysfunction, segmental outbursts in the kinetics of the left ventricle (especially hypokinesia of the inferior or inferolateral wall of the left ventricle), the presence of diastolic dysfunction of the right ventricle, the presence of pericardial effusion [157,158]. Thickening of the walls of the ventricle and segmental outbursts in the kinetics are usually transient and last during the acute phase of the disease [39]. Particular attention should be paid to whether segmental breaks in kinetics correspond to the revascularization area of one coronary artery, which is more common in ischemic heart disease and not in myocarditis.
In addition to assessing the function of the left ventricle, it is also important to assess the right ventricle (estimation of its size, systolic excursion of the tricuspid annulus – TAPSE, etc.)[159]. A significant reduction in right ventricular function is a powerful predictor of death and the need for heart transplantation in patients with proven myocarditis [39]. In patients with FM, the dimensions of the heart cavities are normal and the walls are edematous, while in patients with AM, we have pronounced dilatation of the left ventricle with normal thickness of the heart walls. The importance of the finding of reduced EF during the initial examination in patients with myocarditis is reflected in its prognostic significance, which suggests worse patient outcome [75,160]. The results of the study by Meindl C. et al. showed that the presence of myocarditis in both the acute and subacute phases can be most reliably proven by longitudinal left ventricular strain (LV-GLS), rather than by determining EF or diastolic volume of the LK by transthoracic echocardiography (p<0.05) [161]. As the differential diagnosis of AM and AMI still represents a great challenge, the application of newer echocardiographic techniques, especially Speckle tracking echocardiography (STE) technology, has increased not only the accuracy in the diagnosis of systolic and diastolic dysfunction of the left ventricle, but also in distinguishing these two diseases [162]. The results of various studies have shown that STE measurements are more sensitive than two-dimensional transthoracic echocardiography in the identification of minor regional disturbances in the kinetics of the left ventricular walls and in the diagnosis of acute viral myocarditis [163,164]. It was shown that in children and adolescents with FM and normal EF, subclinical abnormality in LK systolic function was proven by 2DE STE examination to correlate with CMR findings of epicardial edema [165]. Also STE can provide significant information about the lack of regional recovery of left ventricular systolic function during follow-up time.
5.4. Cardiac magnetic resonance (CMR)
Today, it is considered the non-invasive gold standard for the diagnosis of myocarditis [166]. CMR is recommended in patients with clinically suspected AM to confirm the diagnosis or in patients with chest pain, normal coronary angiogram, and elevated troponin to resolve the differential diagnosis. It is recommended that CMR be performed in all clinically stable patients [1]. In 2018, the earlier Lake Louise criteria for diagnosing myocarditis were updated [167]. According to these criteria, in patients with high pretest probability, myocardial inflammation is suspected when at least one of the criteria is met: 1. There are positive findings on T2-weighted images or T2 mapping as markers of myocardial edema. 2. There is at least 1 positive finding among late gadolinium enhancement (LGE), T1 mapping, and ECV as markers of myocardial injury. With the introduction of mentioned novelties, the sensitivity and specificity of CMR for the diagnosis of myocarditis is 87.5% and 96.2% respectively [168]. However, the diagnostic accuracy may vary depending on the clinical picture, the time of the patient’s examination and the extent of the necrosis of cardiomyocytes. The study by Francona M. et al. showed that the diagnostic sensitivity of CMR of the heart is high for a clinical picture similar to myocardial infarction (80%), low for a clinical picture similar to cardiomyopathy (57%) and very low for patients presenting with arrhythmias (40%) [169]. Studies have shown that CMR tissue characterization plays major role in risk stratification in patients with suspected myocarditis [80,170,171]. Progression of LGE and greater extent of focal fibrosis on CMR predict the risk of hospitalization and adverse cardiovascular events in patients with suspected myocarditis [172]. According to the ITAMY study, the anteroseptal accumulation of LGE in the midwall layer in patients with AM is associated with a worse outcome compared to other patterns of presentations [84,173]. Also, the study by Gräni C. and associates showed that regarding location and pattern, septal and midwall LGE showed strongest associations with MACE (HR: 2.55; 95% CI: 1.77 to 3.83 and HR: 2.39; 95% CI: 1.54 to 3.69, respectively; both p<0.001) [80].
It is best to use CMR or to identify acute, active inflammation of the myocardium, and the highest sensitivity is achieved if the examination is performed within 2-3 weeks from the onset of symptoms [1,174]. Myocardial edema is best seen on T2 imagining. CMR can be repeated during patient follow-up, usually 6-12 months in order to identify post-inflammatory scars.
The disadvantages of CMR ate that it is difficult to perform in patients who cannot hold their breath for a long time, who are hemodynamically unstable, as well as in patients on mechanical ventilation or other intracorporeal devices. Claustrophobia is also one of the contraindications for the application of this modern diagnostic method. Although the importance of performing CMR in AM has been widely demonstrated, this technology remains underutilized, in part due to the limited availability of CMR in standard clinical practice [175].
5.5. FDG-PET Myocarditis
Consumption of 18F-fluorodeoxyglucose (18F-FDG) is a quantitative surrogate parameter of increase glucose metabolism, which is a hallmark of the inflammatory process. The use of PET-CT in various forms of myocarditis cause by sarcoidosis , virus, GCM and post-infraction myocarditis has long been known [157,176,177,178]. 18F-FDG PET proved to be important both in establishing a diagnosis and in monitoring the response to the application of therapeutic regimen, especially in patients with cardiac sarcoidosis [179]. A study by Nensa F. and colleagues showed that the use of FDG-PET in diagnosis of myocarditis has sensitivity of 74% and a specificity of 97% [180]. Novel PET radiopharmaceuticals with affinity for somatostatin receptors, such as the 68Ga-lebeled peptides DOTATOC, DOTATATE and DOTANOC, have been shown to have a higher diagnostic accuracy than 18F-FDG for cardiac sarcoidosis [181]. Some studies have shown that the sensitivity and specificity of FDG-PET and CMR in the diagnosis of myocarditis show strong complementarities [182,183]. One of the potential advantages of PET-CT over CMR is that it can quantify the degree of inflammation [157].
5.6. Endomyocardial biopsy (EMB)
Endomyocardial biopsy (EMB) has long been considered the gold standard, but has variable sensitivity and specificity [38]. Although EMB is often indicated for the diagnosis of myocarditis, the sensitivity of this method is debatable given the limited possibility of myocardial sampling. Currently, the only way to identify and characterize the inflammatory cell infiltrate is to perform EMB. According to the Dallas criteria, acute myocarditis is defined by lymphocytic infiltrates associated with myocyte necrosis [57,184]. Borderline myocarditis is characterized by inflammatory infiltrates without the presence of myocyte necrosis. Histological criteria of myocarditis are present in only 5-30% of patient with clinically suspected myocarditis and up to half of patients with DCM. EMB provides unique useful information related to diagnosis, prognosis, and its results help in the selection of therapeutic modalities. However, the use of EMB has decreased over time, probably due to its invasive nature, so only its rational application gives an optimal result. EMB is of particular importance in patients with an acute clinical picture, in life-threatening patients who require rapid diagnosis and adequate treatment [184]. Although EMB in a large number of cases confirms the diagnosis of myocarditis, its results should be interpreted in the context of (1) clinical probability before testing, (2) sample collection time, (3) sample collection quality, (4) sample collection site, (5) historical type of myocarditis, and (6) analytical methods that are applied [1].
6. Differential diagnosis
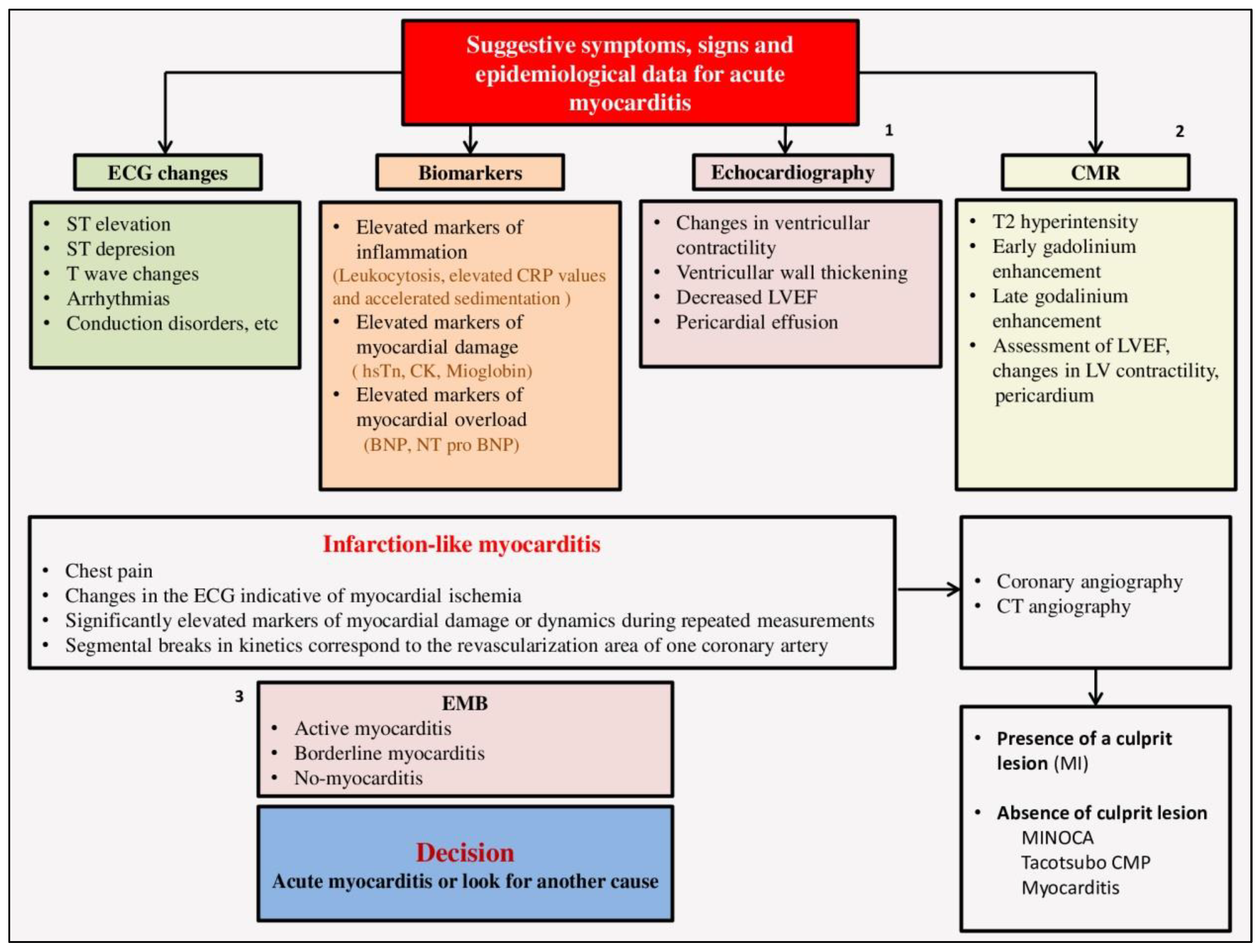
The most difficult differential diagnosis from AMI is when the patient presents with severe chest pain, ECG changes, elevated markers of cardiac necrosis and heart failure. For patients with myocarditis who have chest pain and changes in the ECG, the term infarction-like myocarditis was introduced [1]. According to the registries, the clinical picture occurs in up to 45.8% of patients with myocarditis. According to the prospective observational study Pasupathy S. et al. it was shown that in as many as 33% of patients who were initially recognized as having a myocardial infarction without coronary vessel obstruction, the underlying cause was myocarditis [185]. In the differential diagnosis, we must take into account that patients with myocarditis are usually younger, the presence of a history of recent viremia, slow-developing ECG changes involving more than one vascular territory, the lack of reciprocal ST depression, and echocardiographic disturbances in kinetics are global rather than segmental. Also ST elevation in myocarditis is usually transient and can disappear within 24h (49%) or 48h (74%) [115]. If there is still a differential diagnostic dilemma between these two diseases, it is necessary to perform cardiac catheterization [38]. Coronary angiography is usually normal in myocarditis, and if there is still a dilemma, it is removed by EMB. Patients with acute myocarditis and acute pericarditis may complain of similar symptoms. It is sometimes difficult to make a differential diagnosis between acute myocarditis and non-ischemic cardiomyopathy (Takotcubo cardiomyopathy) or drug-induced cardiomyopathy [186,187] (Figure 2).
Figure 2.
Diagnostic algorithm in acute myocarditis. 1. If there are possibilities, Speckle tracking echocardiography (STE) technology should be done; 2. CMR of the heart can only be done in hemodynamically stable patients; 3. EMB is indicated in case of severe forms of the disease; Abbreviations. ECG, electrocardiogram; CRP, C-reactive protein; hsTn, high sensitive troponin; CK, creatine kinase; BNP, brain natriuretic peptide; NT pro BNP, N-terminal prohormone of brain natriuretic peptide, LVEF, left ventricular ejection fraction; CMR, cardiac magnetic resonance; LV, left ventricle; CT, computerized tomography; EMB, endomyocardial biopsy; MI, myocardial infarction; MINOCA, myocardial infarction with non-obstructive coronary arteries; CMP, cardiomyopathy;.
Figure 2.
Diagnostic algorithm in acute myocarditis. 1. If there are possibilities, Speckle tracking echocardiography (STE) technology should be done; 2. CMR of the heart can only be done in hemodynamically stable patients; 3. EMB is indicated in case of severe forms of the disease; Abbreviations. ECG, electrocardiogram; CRP, C-reactive protein; hsTn, high sensitive troponin; CK, creatine kinase; BNP, brain natriuretic peptide; NT pro BNP, N-terminal prohormone of brain natriuretic peptide, LVEF, left ventricular ejection fraction; CMR, cardiac magnetic resonance; LV, left ventricle; CT, computerized tomography; EMB, endomyocardial biopsy; MI, myocardial infarction; MINOCA, myocardial infarction with non-obstructive coronary arteries; CMP, cardiomyopathy;.
7. Treatment
Spontaneous recovery of left ventricular function is common in patients with acute myocarditis. It is necessary to treat such patients symptomatically because specific treatment options have not yet been found. Autoimmune myocarditis (large cell myocarditis) is treated with immunosuppressive therapy. A smaller number of patients require mechanical circulatory support or heart transplantation within a year. The prognosis of patients treated for myocarditis is variable with a five-year survival rate of 60-90% [188].
- A.)
- Classical treatment
Hemodynamically stable patients
Patients with myocarditis and reduced EFLK are treated according to current guidelines for the treatment of HF [189]. Hemodynamically stable patients with AM and developed HF should be treated with diuretics, ACE inhibitors or AT receptor blockers and beta adrenergic blockers. Treatment should be continued at least 6 months in patients with reduced LVEF even if LVEF improves (>50%) and according to guideline-guided recommendations [39,190]. Nonsteroid anti-inflammatory drugs, especially acetylsalicylic acid, should not be used in myocarditis accompanied by HF, because their use is associated with an increase in mortality [38]. They are reserved in the smallest possible dose for patients with perimyocarditis. Recent case-control studies show that their use is not associated with increased mortality in patients with myocarditis [191,192].
Hemodynamically unstable patients
Hemodynamically unstable patients with HF should be treated in intensive care units in accordance with existing recommendations for the treatment of HF. In acute/fulminant cases with cardiogenic shock and severe ventricular dysfunction, administration of inotropic and vasopressor drugs is necessary [73,193]. In the event that the intravenous administration of inotropes does not lead to hemodynamic improvement of the patient, and the signs and symptoms of shock are still maintained, the use of mechanical circulatory support is advised for the purpose of bridging until healing or heart transplantation [73]. Heart transplantation should be postponed in the acute phase due to possible cure, but should be considered in hemodynamically unstable patients with GCM.
Arrhythmias
There are no special recommendations for the treatment of arrhythmias in myocarditis, so the treatment should be according to current recommendations [194]. Malignant arrhythmias should be treated with antiarrhythmias, and implantation of an implantable cardioverter defibrillator should be delayed in an acute episode of myocarditis and considered usually 3-6 months after the onset of the acute phase of the disease. Patients with GCM and malignant ventricular arrhythmias who have a life expectancy without heart transplantation of >1 year should receive an ICD [39]. On case of complete atrioventricular block, it may be necessary to install a temporary pacemaker [69]. Atrioventricular block is transient and in many cases resolves within about one week of starting treatment [39,195]. Immunosuppressive therapy with steroids can promote recovery of atrioventricular nodal conduction. In some patients, however, complete atrioventricular block may persist even after the acute phase, requiring permanent pacemaker implantation [196]. Resynchronization therapy and the application of mechanical pumps enable longer survival of patients with severe DCM. The indication for implantation of an ICD and cardiac resynchronization defibrillator (CRT-D) should be considered in the chronic phase of the disease to prevent sudden cardiac death, even in recovering patients, if ventricular arrhythmia persists [197]. Primary prevention of sudden cardiac death is based on the SCD-Heft study criteria: chronic heart failure, NYHA>II and left ventricular ejection fraction (LVEF) <35% [198].
Avoidance of intensive physical activities
In the acute phase of myocarditis, intense physical activity is prohibited until the disease is completely cured (at least 6 months) [199]. Athletes should be temporarily excluded from professional sports activity regardless of age, sex, severity of symptoms or therapeutic regimen.
- B.)
- Immunomodulatory therapy
Antiviral therapy
Antiviral therapy can theoretically be effective for the treatment of viral myocarditis because viral infection in an integral part of the pathological process. For example, interferon-b may be effective in treating myocarditis caused by enterovirus (coxsackie virus) or adenovirus infection, and acyclovir may be effective in treating myocarditis caused by human herpes virus infection [38,200,201]. In Murino coxsacke virus B3 induced myocarditis, interferon beta and alpha therapy protects myocytes from damage and reduces the inflammatory response [202].
High doses of intravenous immunoglobulins
Intravenous immunoglobulins are a source of passive immunity and help to clear the virus. Intravenous administration of high doses of immunoglobulin leads to faster recovery of left ventricular function and higher survival during the first year of the disease. Immunoglobulins should be used in patients with DCM whose left ventricular function is progressively deteriorating despite full drag therapy [203,204]. Multicenter study by Kishimoto C. et al. showed that IVIG 1-2 g/kg for 2 days significantly increased 1-month survival rate and significantly reduced cytokines, including TNF-a and IL-6 [204]. An American observational study showed that high-dose IVIG can significantly increase LVEF in patients with myocarditis with EF LK (LVEF) <30% [203].
Immunoabsorption
The basic principle of immunoabsorption is to remove cardiotoxic auto antibodies from the patient’s plasma by plasmapheresis [205]. The complete amount of IgG antibodies found in the plasma is absorbed during repeated cycles at certain time intervals (daily during the first three days, and then four cycles with an interval of one month). After each session, plasma IgG must be replenished by injection of 0.5g/kg polyclonal IgG.
- C.)
- Immunosuppressive therapy
Patients with DCM and immunohistologically proven chronic inflammation, but without persistent viral infection, benefit from immunosuppression. A six-month immunosuppressive treatment in these patients can lead to a significant improvement in HF symptoms. Immunosuppressive therapy may be considered when patient has a relapse, recurrent exacerbation, or persistent infiltration of inflammatory cells (e.g. when chronic active myocarditis is suspected) [39]. Patients with EM respond particularly favorably to immunosuppressive therapy, with increased survival rates [206]. Currently, no evidence is available to support the efficiency of immunosuppressive therapy for acute lymphocytic myocarditis. Patients with DCM and persistent infection with cardiotropic viruses should not undergo immunosuppression, as they are candidates for antiviral treatment. So far, treatment with immunosuppressive drugs has shown controversial results. The use of azathiopyrine and prednisone in patients with chronic DCM has been shown to improve left ventricular function, while in GCM combined treatment with immunosuppressant (cyclosporine and corticosteroids with or without azathiopyrine or muronomab-CDs) can extend the average survival time to 12 months compared to untreated patients whose average survival time is 3 months [69]. Patients treated with tacrolimus (target serum concentration, 8-12 ng/mL in short-term treatment and 6-8 ng/mL in long-term treatment) have fewer adverse reactions that those treated with the old immunosuppressive regimen [39].
8. Prognosis
The mortality rate in patients with myocarditis is still high despite advances in diagnostic and therapeutic modalities (one-year mortality is around 20% and five-year mortality is 50%) [7]. Studies have shown that mortality from acute non-fulminant myocarditis is about 8-12%. Study data from the registry of the Spanish National Health Service show that hospital mortality in patients with AM is 3% (data analyzed from 2003 to 2015) [207]. Predictors of mortality in these patients were shown to be: decreased EFLK, presence of syncope at initial presentation, right ventricular dysfunction, presence of pulmonary hypertension and prolongation of the QRS complex for more than 120s. Extremely elevated levels of IL10 as well as soluble Fas have been shown to be predictors of poor outcome in patients with FM. Although up to 80% of patients with AM have normalized left ventricular size and systolic function, the incidence of DCM among patients with histologically positive AM ranges between 14% and 50%. When it comes to children, after acute myocarditis, about 21% of patients develop DCM [208]. Long-term mortality (up to 90 days of follow-up) after myocarditis is about 4.9% [97].
Conclusions
Myocarditis is still a disease with high mortality and morbidity, especially in the young population. Establishing as accurate and timely diagnosis in myocarditis is still challenging due to the huge number of etiological agents and associated diseases that in their natural course can lead to this disease.
However, by improving diagnostic modalities and searching for increasingly sensitive biomarkers (S100A8/A9, sST2, anti-cardiac antibodies, miRNA, pentraxin 3, galectin 3 and growth differentiation factor), we are getting closer to the possibility of early non-invasive diagnostic and adequate monitoring of these patients. In hemodynamically stable patients, the gold standard in diagnosis of this disease is CMR, which should be used more, i.e. to work on its greater availability in standard clinical practice. EMB is the main invasive diagnostic method, especially in patients with fulminant form of the disease. Although only this diagnostic method can identify, and characterize the infiltrate of inflammatory cells, its use has decreased over time, probably due to its invasive character, so only its rational application provides an optimal result. It is necessary to perform early risk stratification in patients with myocarditis and single out the most vulnerable group of patients in order to prevent possible adverse events and provide an adequate therapeutic regimen. Reduced EF at initial presentation, occurrence of malignant ventricular arrhythmias with circulatory collapse are significant predictors of poor prognosis in patients with myocarditis.
New therapeutic modalities, the development of immunomodulatory and immunosuppressive therapy, improving the education of doctors in the field of mechanical circulatory support and timely heart transplantation are just some of the therapeutic aspects that will improve the survival of these patients. Large additional test ate still needed both in the field of diagnostics and in the field of therapy in order to improve treatment, prevent the transition from an acute to a chronic form of the disease, prevent the recurrence of the disease and ultimately reduce the mortality of these patients.
Author Contributions
Conceptualization, methodology, investigation, data curation, writing, and original draft preparation, R.L. and L.D.; original draft preparation, L.S. and G.K.; visualization, M.Z.; investigation, M.R. and A.L..; supervision, M.A. and A.R.. All authors have read and agreed to the published version of the manuscript
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare that there is no conflict of interest.
References
- Ammirati, E.; Frigerio, M.; Adler, E.D.; Basso, C.; Birnie, D.H.; Brambatti, M.; Friedrich, M.G.; Klingel, K.; Lehtonen, J.; Moslehi, J.J.; et al. Management of Acute Myocarditis and Chronic Inflammatory Cardiomyopathy: An Expert Consensus Document. Circ Heart Fail. 2020, 13, e007405. [Google Scholar] [CrossRef]
- Ikegami, Y.; Tase, C. ; Acute Myocarditis in Emergency Medicine. JACC 2012, 59, 779–792. [Google Scholar]
- Golpour, A.; Patriki, D.; Hanson, P.J.; McManus, B.; Heidecker, B. Epidemiological Impact of Myocarditis. J Clin Med. 2021, 10, 603. [Google Scholar] [CrossRef] [PubMed]
- Fu, M.; Kontogeorgos, S.; Thunström, E.; Zverkova, S.T.; Kroon, C.; Bollano, E.; Schaufelberger, M.; Rosengren, A. Trends in myocarditis incidence, complications and mortality in Sweden from 2000 to 2014. Sci Rep. 2022, 12, 1810. [Google Scholar] [CrossRef] [PubMed]
- Basso, C.; Calabrese, F.; Corrado, D.; Thiene, G. Postmortem diagnosis in sudden cardiac death victims: macroscopic, microscopic and molecular findings. Cardiovasc Res. 2001, 50, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Doerer, J.J.; Haas, T.S.; Tierney, D.M.; Mueller, F.O. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980-2006. Circulation. 2009, 119, 1085–1092. [Google Scholar] [CrossRef] [PubMed]
- Jouriles, N.J; Chapter 80. In: Marx, J.A.; Hockberger, R.S.; Walls, R.M.; editors. Rosen’s emergency medicine: concepts and clinical practice. 7th ed. Philadelphia: Mosby; 2009. p. 1064-1068.
- Maron, B.J.; Towbin, J.A.; Thiene, G.; Antzelevitch, C.; Corrado, D.; Arnett, D.; Moss, A.J.; Seidman, C.E.; Young, J.B.; American Heart Association; Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; Council on Epidemiology and Prevention. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation 2006, 113, 1807–1816. [Google Scholar]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular Implications of Fatal Outcomes of Patients with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–818. [Google Scholar] [CrossRef]
- Altay, S. COVID-19 myocarditis cardiac magnetic resonance findings in symptomatic patients. Acta Radiol. 2022, 63, 1475–1480. [Google Scholar] [CrossRef]
- Voleti, N.; Reddy, S.P.; Ssentongo, P. Myocarditis in SARS-CoV-2 infection vs. COVID-19 vaccination: A systematic review and meta-analysis. Front Cardiovasc Med. 2022, 9, 951314. [Google Scholar] [CrossRef]
- Fairweather, D.; Beetler, D.J.; Musigk, N.; Heidecker, B.; Lyle, M.A.; Cooper, L.T., Jr.; Bruno, K.A. Sex and gender differences in myocarditis and dilated cardiomyopathy: An update. Front Cardiovasc Med. 2023, 10, 1129348. [Google Scholar] [CrossRef]
- Kytö, V.; Sipilä, J.; Rautava, P. The effects of gender and age on occurrence of clinically suspected myocarditis in adulthood. Heart. 2013, 99, 1681–1684. [Google Scholar] [CrossRef]
- Laufer-Perl, M.; Havakuk, O.; Shacham, Y.; Steinvil, A.; Letourneau-Shesaf, S.; Chorin, E.; Keren, G.; Arbel, Y. Sex-based differences in prevalence and clinical presentation among pericarditis and myopericarditis patients. Am J Emerg Med. 2017, 35, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Lynge, T.H.; Nielsen, T.S.; Gregers Winkel, B.; Tfelt-Hansen, J.; Banner, J. Sudden cardiac death caused by myocarditis in persons aged 1-49 years: a nationwide study of 14 294 deaths in Denmark. Forensic Sci Res. 2019, 4, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Durani, Y.; Egan, M.; Baffa, J.; Selbst, S.M.; Nagar, A.L. Pediatric myocarditis: presenting clinical characteristics. Am J Emerg Med. 2009, 27, 942–947. [Google Scholar] [CrossRef] [PubMed]
- Arola, A.; Pikkarainen, E.; Sipilä, J.O.; Pykäri, J.; Rautava, P.; Kytö, V. Occurrence and Features of Childhood Myocarditis: A Nationwide Study in Finland. J Am Heart Assoc. 2017, 6, e005306. [Google Scholar] [CrossRef] [PubMed]
- Tschöpe, C.; Ammirati, E.; Bozkurt, B.; Caforio, A.L.P.; Cooper, L.T.; Felix, S.B.; Hare, J.M.; Heidecker, B.; Heymans, S.; Hübner, N.; et al. Myocarditis and inflammatory cardiomyopathy: current evidence and future directions. Nat Rev Cardiol. 2021, 18, 169–193. [Google Scholar] [CrossRef] [PubMed]
- Lévêque, N.; Garcia, M.; Bouin, A.; Nguyen, J.H.C.; Tran, G.P.; Andreoletti, L.; Semler, B.L. Functional Consequences of RNA 5'-Terminal Deletions on Coxsackievirus B3 RNA Replication and Ribonucleoprotein Complex Formation. J Virol. 2017, 91, e00423–17. [Google Scholar] [CrossRef] [PubMed]
- Strabelli, T.M.; Siciliano, R.F.; Vidal Campos, S.; Bianchi Castelli, J.; Bacal, F.; Bocchi, E.A.; Uip, D.E. Toxoplasma gondii Myocarditis after Adult Heart Transplantation: Successful Prophylaxis with Pyrimethamine. J Trop Med. 2012, 2012, 853562. [Google Scholar] [CrossRef]
- Mylvaganam, R.; Glaser, A.; Moss, N.; Rana, M. A case of late-onset cytomegalovirus myocarditis in an orthotopic heart transplant recipient; case report and review of the literature. Diagn Microbiol Infect Dis. 2018, 91, 153–155. [Google Scholar] [CrossRef]
- Massilamany, C.; Huber, S.A.; Cunningham, M.W.; Reddy, J. Relevance of molecular mimicry in the mediation of infectious myocarditis. J Cardiovasc Transl Res. 2014, 7, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Pannucci, P.; Jefferson, S.R.; Hampshire, J.; Cooper, S.L.; Hill, S.J.; Woolard, J. COVID-19-Induced Myocarditis: Pathophysiological Roles of ACE2 and Toll-like Receptors. Int J Mol Sci. 2023, 24, 5374. [Google Scholar] [CrossRef] [PubMed]
- Lasica, R.; Djukanovic, L.; Mrdovic, I.; Savic, L.; Ristic, A.; Zdravkovic, M.; Simic, D.; Krljanac, G.; Popovic, D.; Simeunovic, D.; Rajic, D.; Asanin, M. Acute Coronary Syndrome in the COVID-19 Era-Differences and Dilemmas Compared to the Pre-COVID-19 Era. J Clin Med. 2022, 11, 3024. [Google Scholar] [CrossRef] [PubMed]
- Dennert, R.; Crijns, H.J.; Heymans, S. Acute viral myocarditis. Eur Heart J. 2008, 29, 2073–2082. [Google Scholar] [CrossRef]
- Andréoletti, L.; Lévêque, N.; Boulagnon, C.; Brasselet, C.; Fornes, P. Viral causes of human myocarditis. Arch Cardiovasc Dis. 2009, 102, 559–568. [Google Scholar] [CrossRef]
- Seitz, A.; Martínez Pereyra, V.; Hubert, A.; Klingel, K.; Bekeredjian, R.; Sechtem, U.; Ong, P. Epicardial and microvascular coronary artery spasm in biopsy-proven viral myocarditis. Int J Cardiol. 2022, 360, 1–4. [Google Scholar] [CrossRef]
- Keramari, S.; Poutoglidis, A.; Chatzis, S.; Keramaris, M.; Savopoulos, C.; Kaiafa, G. Parvovirus B19-Associated Myocarditis: A Literature Review of Pediatric Cases. Cureus. 2022, 14, e21726. [Google Scholar] [CrossRef]
- Schultheiss, H.P.; Baumeier, C.; Aleshcheva, G.; Bock, C.T.; Escher, F. Viral Myocarditis-From Pathophysiology to Treatment. J Clin Med. 2021, 10, 5240. [Google Scholar] [CrossRef] [PubMed]
- Palecek, T.; Ganame, J.; Di Salvo, G. Myocardial Diseases: Current Views on Etiopathogenesis, Diagnostic Modalities, and Therapeutic Options. Biomed Res Int. 2016, 2016, 1720405. [Google Scholar] [CrossRef]
- Saad, H.A.B.; Ntusi, N. HIV-Associated Cardiovascular Disease. Advances in HIV and AIDS Control. IntechOpen; 2018. [CrossRef]
- Freiberg, M.S.; Chang, C.H.; Skanderson, M.; Patterson, O.V.; DuVall, S.L.; Brandt, C.A.; So-Armah, K.A.; Vasan, R.S.; Oursler, K.A.; Gottdiener, J.; et al. Association Between HIV Infection and the Risk of Heart Failure with Reduced Ejection Fraction and Preserved Ejection Fraction in the Antiretroviral Therapy Era: Results from the Veterans Aging Cohort Study. JAMA Cardiol. 2017, 2, 536–546. [Google Scholar] [CrossRef]
- Rroku, A.; Kottwitz, J.; Heidecker, B. Update on myocarditis - what we know so far and where we may be heading. Eur Heart J Acute Cardiovasc Care. 2020, 2048872620910109. [Google Scholar] [CrossRef] [PubMed]
- Lumsden, R.H.; Bloomfield, G.S. The Causes of HIV-Associated Cardiomyopathy: A Tale of Two Worlds. Biomed Res Int. 2016, 2016, 8196560. [Google Scholar] [CrossRef] [PubMed]
- Bloomfield, G.S.; Alenezi, F.; Barasa, F.A.; Lumsden, R.; Mayosi, B.M.; Velazquez, E.J. Human Immunodeficiency Virus and Heart Failure in Low- and Middle-Income Countries. JACC Heart Fail. 2015, 3, 579–590. [Google Scholar] [CrossRef] [PubMed]
- Sinha, A.; Feinstein, M. Epidemiology, pathophysiology, and prevention of heart failure in people with HIV. Prog Cardiovasc Dis. 2020, 63, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Kaul, S.; Fishbein, M.C.; Siegel, R.J. Cardiac manifestations of acquired immune deficiency syndrome: a 1991 update. Am Heart J. 1991, 122, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Caforio, A.L.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2013, 34, 2636–2648. [Google Scholar]
- Nagai, T.; Inomata, T.; Kohno, T.; Sato, T.; Tada, A.; Kubo, T.; Nakamura, K.; Oyama-Manabe, N.; Ikeda, Y.; Fujino, T.; et al. Japanese Circulation Society Joint Working Group. JCS 2023 Guideline on the Diagnosis and Treatment of Myocarditis. Circ J. 2023, 87, 674–754. [Google Scholar] [CrossRef]
- Tefferi, A.; Gotlib, J.; Pardanani, A. Hypereosinophilic syndrome and clonal eosinophilia: point-of-care diagnostic algorithm and treatment update. Mayo Clin Proc. 2010, 85, 158–164. [Google Scholar] [CrossRef]
- Ogbogu, P.U.; Bochner, B.S.; Butterfield, J.H.; Gleich, G.J.; Huss-Marp, J.; Kahn, J.E.; Leiferman, K.M.; Nutman, T.B.; Pfab, F.; Ring, J. Hypereosinophilic syndrome: a multicenter, retrospective analysis of clinical characteristics and response to therapy. J Allergy Clin Immunol. 2009, 124, 1319–1325e3. [Google Scholar] [CrossRef]
- Datta, T.; Solomon, A.J. Clozapine-induced myocarditis. Oxf Med Case Reports. 2018, 2018, omx080. [Google Scholar] [CrossRef]
- Garty, B.Z.; Offer, I.; Livni, E.; Danon, Y.L. Erythema multiforme and hypersensitivity myocarditis caused by ampicillin. Ann Pharmacother. 1994, 28, 730–731. [Google Scholar] [CrossRef] [PubMed]
- Çetin, M.; Mis, M.D.; Karaman, K.; Yavuz, Í.H.; Geylan, H.; Tunçdemir, P.; Demir, F. Carbamazepine-induced DRESS syndrome leading to reversible myocarditis in a child. Cent Eur J Immunol. 2019, 44, 102–105. [Google Scholar] [CrossRef] [PubMed]
- Shaughnessy, K.K.; Bouchard, S.M.; Mohr, M.R.; Herre, J.M.; Salkey, K.S. Minocycline-induced drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome with persistent myocarditis. J Am Acad Dermatol. 2010, 62, 315–318. [Google Scholar] [CrossRef]
- Bryde, R.E.; Ray, J.C.; Sacco, K.A.; Shapiro, B.; Cooper, L. Eosinophillic Myocarditis Secondary to Metastatic Melanoma. Radiol Cardiothorac Imaging. 2019, 1, e190076. [Google Scholar] [CrossRef]
- Epelboin, L.; Jauréguiberry, S.; Estève, J.B.; Danis, M.; Komajda, M.; Bricaire, F.; Caumes, E. Myocarditis during acute schistosomiasis in two travelers. Am J Trop Med Hyg. 2010, 82, 365–367. [Google Scholar] [CrossRef]
- Pakbaz, M.; Pakbaz, M. Cardiac Involvement in Eosinophilic Granulomatosis with Polyangiitis: A Meta-Analysis of 62 Case Reports. J Tehran Heart Cent. 2020, 15, 18–26. [Google Scholar] [CrossRef]
- Xu, J.; Brooks, E.G. Giant Cell Myocarditis: A Brief Review. Arch Pathol Lab Med. 2016, 140, 1429–1434. [Google Scholar] [CrossRef]
- Hu, Y.; Ren, J.; Dong, X.; Zhang, D.; Qu, Y.; Yang, C.; Sun, Y.; Li, J.; Luo, F.; Wang, W.; et al. Fulminant Giant Cell Myocarditis vs. Lymphocytic Myocarditis: A Comparison of Their Clinical Characteristics, Treatments, and Outcomes. Front Cardiovasc Med. 2021, 8, 770549. [Google Scholar] [CrossRef]
- Gadela, N.V.; Krishnan, A.M.; Mukarram, O.; Sthalekar, N. Giant cell myocarditis. Proc (Bayl Univ Med Cent). 2021, 34, 401–402. [Google Scholar] [CrossRef]
- Ghaly, M.; Schiliro, D.; Stepczynski, J. Giant Cell Myocarditis: A Time Sensitive Distant Diagnosis. Cureus. 2020, 12, e6712. [Google Scholar] [CrossRef]
- Al-Kindi, S.G.; Oliveira, G.H. Reporting of immune checkpoint inhibitor-associated myocarditis. Lancet. 2018, 392, 382–383. [Google Scholar] [CrossRef] [PubMed]
- Ma, R.; Wang, Q.; Meng, D.; Li, K.; Zhang, Y. Immune checkpoint inhibitors-related myocarditis in patients with cancer: an analysis of international spontaneous reporting systems. BMC Cancer. 2021, 21, 38. [Google Scholar] [CrossRef] [PubMed]
- Vasbinder, A.; Chen, Y.; Procureur, A.; Gradone, A.; Azam, T.U.; Perry, D.; Shadid, H.; Anderson, E.; Catalan, T.; Blakely, P.; et al. Biomarker Trends, Incidence, and Outcomes of Immune Checkpoint Inhibitor-Induced Myocarditis. JACC CardioOncol. 2022, 4, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Perel-Winkler, A.; Bokhari, S.; Perez-Recio, T.; Zartoshti, A.; Askanase, A.; Geraldino-Pardilla, L. Myocarditis in systemic lupus erythematosus diagnosed by 18F-fluorodeoxyglucose positron emission tomography. Lupus Sci Med. 2018, 5, e000265. [Google Scholar] [CrossRef]
- Aretz, H.T. Myocarditis: the Dallas criteria. Hum Pathol. 1987, 18, 619–624. [Google Scholar] [CrossRef]
- Brociek, E.; Tymińska, A.; Giordani, A.S.; Caforio, A.L.P.; Wojnicz, R.; Grabowski, M.; Ozierański, K. Myocarditis: Etiology, Pathogenesis, and Their Implications in Clinical Practice. Biology 2023, 12, 874. [Google Scholar] [CrossRef]
- Pandey, S.; Rajasurya, V. Nonviral Myocarditis. Treasure Island (FL): StatPearls Publishing; 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK536928/.
- Nguyen, L.S.; Cooper, L.T.; Kerneis, M.; Funck-Brentano, C.; Silvain, J.; Brechot, N.; Hekimian, G.; Ammirati, E.; Ben M'Barek, B.; Redheuil, A.; et al. Systematic analysis of drug-associated myocarditis reported in the World Health Organization pharmacovigilance database. Nat Commun. 2022, 13, 25. [Google Scholar] [CrossRef]
- Kounis, N.G.; Koniari, I.; Mplani, V.; Plotas, P.; Velissaris, D. Hypersensitivity Myocarditis and the Pathogenetic Conundrum of COVID-19 Vaccine-Related Myocarditis. Cardiology 2022, 147, 413–415. [Google Scholar] [CrossRef]
- Bracamonte-Baran, W.; Čiháková, D. Cardiac Autoimmunity: Myocarditis. Adv Exp Med Biol. 2017, 1003, 187–221. [Google Scholar]
- Park, Y.; Ahn, S.G.; Ko, A.; Ra, S.H.; Cha, J.; Jee, Y.G.; Lee, J.H. Hypersensitivity myocarditis confirmed by cardiac magnetic resonance imaging and endomyocardial biopsy. Korean J Intern Med. 2014, 29, 236–240. [Google Scholar] [CrossRef]
- JCS Joint Working Group. Guidelines for diagnosis and treatment of myocarditis (JCS 2009): digest version. Circ J. 2011, 75, 734–743. [Google Scholar] [CrossRef] [PubMed]
- Ammirati, E.; Moslehi, J.J. Diagnosis and Treatment of Acute Myocarditis: A Review. JAMA 2023, 329, 1098–1113. [Google Scholar] [CrossRef] [PubMed]
- Ammirati, E.; Buono, A.; Moroni, F.; Gigli, L.; Power, J.R.; Ciabatti, M.; Garascia, A.; Adler, E.D.; Pieroni, M. State-of-the-Art of Endomyocardial Biopsy on Acute Myocarditis and Chronic Inflammatory Cardiomyopathy. Curr Cardiol Rep. 2022, 24, 597–609. [Google Scholar] [CrossRef] [PubMed]
- Lampejo, T.; Durkin, S.M.; Bhatt, N.; Guttmann, O. Acute myocarditis: aetiology, diagnosis and management. Clin Med 2021, 21, e505–e510. [Google Scholar] [CrossRef] [PubMed]
- Daniels, C.J.; Rajpal, S.; Greenshields, J.T.; Rosenthal, G.L.; Chung, E.H.; Terrin, M.; Jeudy, J.; Mattson, S.E.; Law, I.H.; Borchers, J.; et al. Big Ten COVID-19 Cardiac Registry Investigators. Prevalence of Clinical and Subclinical Myocarditis in Competitive Athletes with Recent SARS-CoV-2 Infection: Results from the Big Ten COVID-19 Cardiac Registry. JAMA Cardiol. 2021, 6, 1078–1087. [Google Scholar] [CrossRef] [PubMed]
- Caforio, A.L.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2013, 34, 2636–2648. [Google Scholar]
- Al-Akchar, M.; Shams, P.; Kiel, J. Acute Myocarditis. Treasure Island (FL): StatPearls Publishing; 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK441847/.
- Ammirati, E.; Veronese, G.; Brambatti, M.; Merlo, M.; Cipriani, M.; Potena, L.; Sormani, P.; Aoki, T.; Sugimura, K.; Sawamura, A.; et al. Fulminant Versus Acute Nonfulminant Myocarditis in Patients with Left Ventricular Systolic Dysfunction. J Am Coll Cardiol. 2019, 74, 299–311. [Google Scholar] [CrossRef]
- Ammirati, E.; Cipriani, M.; Moro, C.; Raineri, C.; Pini, D.; Sormani, P.; Mantovani, R.; Varrenti, M.; Pedrotti, P.; Conca, C.; et al. Registro Lombardo delle Miocarditi. Clinical presentation and outcome in a contemporary cohort of patients with acute myocarditis: multicenter lombardy registry. Circulation. 2018, 138, 1088–1099. [Google Scholar] [CrossRef]
- Kociol, R.D.; Cooper, L.T.; Fang, J.C.; Moslehi, J.J.; Pang, P.S.; Sabe, M.A.; Shah, R.V.; Sims, D.B.; Thiene, G.; Vardeny, O. American Heart Association Heart Failure and Transplantation Committee of the Council on Clinical Cardiology. Recognition and Initial Management of Fulminant Myocarditis: A Scientific Statement from the American Heart Association. Circulation. 2020, 141, e69–e92. [Google Scholar] [CrossRef]
- McCarthy, R.E., 3rd; Boehmer, J.P.; Hruban, R.H.; Hutchins, G.M.; Kasper, E.K.; Hare, J.M.; Baughman, K.L. Long-term outcome of fulminant myocarditis as compared with acute (nonfulminant) myocarditis. N Engl J Med. 2000, 342, 690–695. [Google Scholar] [CrossRef]
- Anzini, M.; Merlo, M.; Sabbadini, G.; Barbati, G.; Finocchiaro, G.; Pinamonti, B.; Salvi, A.; Perkan, A.; Di Lenarda, A.; Bussani, R.; et al. Long-term evolution and prognostic stratification of biopsy-proven active myocarditis. Circulation. 2013, 128, 2384–2394. [Google Scholar] [CrossRef] [PubMed]
- Ammirati, E.; Cipriani, M.; Lilliu, M.; Sormani, P.; Varrenti, M.; Raineri, C.; Petrella, D.; Garascia, A.; Pedrotti, P.; Roghi, A.; et al. Survival and Left Ventricular Function Changes in Fulminant Versus Nonfulminant Acute Myocarditis. Circulation. 2017, 136, 529–545. [Google Scholar] [CrossRef] [PubMed]
- Jeserich, M.; Konstantinides, S.; Olschewski, M.; Pavlik, G.; Bode, C.; Geibel, A. Diagnosis of early myocarditis after respiratory or gastrointestinal tract viral infection: insights from cardiovascular magnetic resonance. Clin Res Cardiol. 2010, 99, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Vohra, S.; Yadav, A.; Sharma, P.; Khan, S.; Jaiswal, V. Acute myocarditis masquerading as anterior wall myocardial infarction: A case report. Ann Med Surg 2022, 84, 104884. [Google Scholar] [CrossRef] [PubMed]
- White, J.A.; Hansen, R.; Abdelhaleem, A.; Mikami, Y.; Peng, M.; Rivest, S.; Satriano, A.; Dykstra, S.; Flewitt, J.; Heydari, B.; et al. Natural History of Myocardial Injury and Chamber Remodeling in Acute Myocarditis. Circ Cardiovasc Imaging. 2019, 12, e008614. [Google Scholar] [CrossRef] [PubMed]
- Gräni, C.; Eichhorn, C.; Bière, L.; Murthy, V.L.; Agarwal, V.; Kaneko, K.; Cuddy, S.; Aghayev, A.; Steigner, M.; Blankstein, R.; et al. Prognostic value of cardiac magnetic resonance tissue characterization in risk stratifying patients with suspected myocarditis. J Am Coll Cardiol. 2017, 70, 1964–1976. [Google Scholar] [CrossRef] [PubMed]
- Younis, A.; Matetzky, S.; Mulla, W.; Masalha, E.; Afel, Y.; Chernomordik, F.; Fardman, A.; Goitein, O.; Ben-Zekry, S.; Peled, Y.; et al. Epidemiology characteristics and outcome of patients with clinically diagnosed acute myocarditis. Am J Med. 2020, 133, 492–499. [Google Scholar] [CrossRef]
- Adamopoulos, S.; Miliopoulos, D.; Karavidas, A.; Nikolaou, M.; Lazaros, G.; Gkouziouta, A.; Manginas, A.; Sevastos, G.; Karvounis, H.; Karamitsos, T.D.; et al. HEllenic Registry on Myocarditis SyndromES on behalf of Hellenic Heart Failure Association: The HERMES-HF Registry. ESC Heart Fail. 2020, 7, 3676–3684. [Google Scholar] [CrossRef]
- Dries, D.J. Chest Pain. Air Med J. 2016, 35, 107–110. [Google Scholar] [CrossRef]
- Aquaro, G.D.; Perfetti, M.; Camastra, G.; Monti, L.; Dellegrottaglie, S.; Moro, C.; Pepe, A.; Todiere, G.; Lanzillo, C.; Scatteia, A.; et al. Cardiac Magnetic Resonance Working Group of the Italian Society of Cardiology. Cardiac MR With Late Gadolinium Enhancement in Acute Myocarditis with Preserved Systolic Function: ITAMY Study. J Am Coll Cardiol. 2017, 70, 1977–1987. [Google Scholar] [CrossRef]
- Cannata, A.; Bhatti, P.; Roy, R.; Al-Agil, M.; Daniel, A.; Ferone, E.; Jordan, A.; Cassimon, B.; Bradwell, S.; Khawaja, A.; et al. Prognostic relevance of demographic factors in cardiac magnetic resonance-proven acute myocarditis: A cohort study. Front Cardiovasc Med. 2022, 9, 1037837. [Google Scholar] [CrossRef] [PubMed]
- Angelini, A.; Calzolari, V.; Calabrese, F.; Boffa, G.M.; Maddalena, F.; Chioin, R.; Thiene, G. Myocarditis mimicking acute myocardial infarction: role of endomyocardial biopsy in the differential diagnosis. Heart. 2000, 84, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Khandaker, M.H.; Espinosa, R.E.; Nishimura, R.A.; Sinak, L.J.; Hayes, S.N.; Melduni, R.M.; Oh, J.K. Pericardial disease: diagnosis and management. Mayo Clin Proc. 2010, 85, 572–593. [Google Scholar] [CrossRef] [PubMed]
- Aota, H.; Suzuki, H.; Godo, S.; Kuniyoshi, S.; Fujishima, F.; Tahakashi, J.; Yasuda, S. A teenage boy with acute myocarditis and reversible microvascular angina: A case report. J Cardiol Cases. 2023, 27, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.; Marques, P.; Martins, S.; Bordalo, E.; Sá, A.L.; Nóbrega, J.; Duarte, J.; Almeida, A.G.; Gabriel, H.M.; Correia, M.J.; Diogo, A.N. Coronary artery vasospasm and acute myocarditis: a rare association. Rev Port Cardiol. 2010, 29, 1879–1888. [Google Scholar] [PubMed]
- McCully, R.B.; Cooper, L.T.; Schreiter, S. Coronary artery spasm in lymphocytic myocarditis: a rare cause of acute myocardial infarction. Heart. 2005, 91, 202. [Google Scholar] [CrossRef] [PubMed]
- Khan, Z.; Pabani, U.K.; Gul, A.; Muhammad, S.A.; Yousif, Y.; Abumedian, M.; Elmahdi, O.; Gupta, A. COVID-19 Vaccine-Induced Myocarditis: A Systemic Review and Literature Search. Cureus. 2022, 14, e27408. [Google Scholar] [CrossRef]
- Bonanni, M.; Angelini, G.; Leo, L.A.; Schlossbauer, S.A.; Bergamaschi, L.; Landi, A.; Sangiorgi, G.M.; Forleo, C.; Pasotti, E.; Pedrazzini, G.; et al. Multimodality Imaging Evaluation to Detect Subtle Right Ventricular Involvement in Patients with Acute Myocarditis and Preserved Left Ventricular Ejection Fraction. J Clin Med. 2023, 12, 4308. [Google Scholar] [CrossRef]
- Duncan, B.W.; Bohn, D.J.; Atz, A.M.; French, J.W.; Laussen, P.C.; Wessel, D.L. Mechanical circulatory support for the treatment of children with acute fulminant myocarditis. J Thorac Cardiovasc Surg. 2001, 122, 440–448. [Google Scholar] [CrossRef]
- Pages, O.N.; Aubert, S.; Combes, A.; Luyt, C.E.; Pavie, A.; Léger, P.; Gandjbakhch, I.; Leprince, P. Paracorporeal pulsatile biventricular assist device versus extracorporal membrane oxygenation-extracorporal life support in adult fulminant myocarditis. J Thorac Cardiovasc Surg. 2009, 137, 194–197. [Google Scholar] [CrossRef]
- Peretto, G.; Sala, S.; Rizzo, S.; De Luca, G.; Campochiaro, C.; Sartorelli, S.; Benedetti, G.; Palmisano, A.; Esposito, A.; Tresoldi, M.; et al. Arrhythmias in myocarditis: State of the art. Heart Rhythm. 2019, 16, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Karki, R.; Janga, C.; Deshmukh, A.J. Arrhythmias Associated with Inflammatory Cardiomyopathies. Curr Treat Options Cardiovasc Med. 2020, 22, 76. [Google Scholar] [CrossRef] [PubMed]
- Kragholm, K.H.; Lindgren, F.L.; Zaremba, T.; Freeman, P.; Andersen, N.H.; Riahi, S.; Pareek, M.; Køber, L.; Torp-Pedersen, C.; Søgaard, P.; et al. Mortality and ventricular arrhythmia after acute myocarditis: a nationwide registry-based follow-up study. Open Heart. 2021, 8, e001806. [Google Scholar] [CrossRef] [PubMed]
- Sozzi, F.B.; Gherbesi, E.; Faggiano, A.; Gnan, E.; Maruccio, A.; Schiavone, M.; Iacuzio, L.; Carugo, S. Viral Myocarditis: Classification, Diagnosis, and Clinical Implications. Front Cardiovasc Med. 2022, 9, 908663. [Google Scholar] [CrossRef] [PubMed]
- Law, Y.M.; Lal, A.K; Chen, S.; Čiháková, D.; Cooper, L.T.; Deshpande, S.; Godown, J.; Grosse-Wortmann, L.; Robinson, J.D.; Towbin, J.A. American Heart Association Pediatric Heart Failure and Transplantation Committee of the Council on Lifelong Congenital Heart Disease and Heart Health in the Young and Stroke Council. Diagnosis and Management of Myocarditis in Children: A Scientific Statement from the American Heart Association. Circulation 2021, 144, e123–e135. [Google Scholar] [PubMed]
- Subahi, A.; Akintoye, E.; Yassin, A.S.; Abubakar, H.; Adegbala, O.; Mishra, T.; Abdelrahman, M.; Shokr, M.; Afonso, L. Impact of atrial fibrillation on patients hospitalized for acute myocarditis: Insights from a nationally-representative United States cohort. Clin Cardiol. 2019, 42, 26–31. [Google Scholar] [CrossRef]
- Rosier, L.; Zouaghi, A.; Barré, V.; Martins, R.; Probst, V.; Marijon, E.; Sadoul, N.; Chauveau, S.; Da Costa, A.; Badoz, M.; et al. High Risk of Sustained Ventricular Arrhythmia Recurrence After Acute Myocarditis. J Clin Med. 2020, 9, 848. [Google Scholar] [CrossRef]
- Okura, Y.; Dec, G.W.; Hare, J.M.; Kodama, M.; Berry, G.J.; Tazelaar, H.D.; Bailey, K.R.; Cooper, L.T. A clinical and histopathologic comparison of cardiac sarcoidosis and idiopathic giant cell myocarditis. J Am Coll Cardiol. 2003, 41, 322–329. [Google Scholar] [CrossRef]
- Kandolin, R.; Lehtonen, J.; Kupari, M. Cardiac sarcoidosis and giant cell myocarditis as causes of atrioventricular block in young and middle-aged adults. Circ Arrhythm Electrophysiol. 2011, 4, 303–309. [Google Scholar] [CrossRef]
- Wan, D.; Baranchuk, A. Lyme carditis and atrioventricular block. CMAJ. 2018, 190, E622. [Google Scholar] [CrossRef]
- Alamri, A.S.; Khayat, L.T.; Alzahrani, A.J.; Kurdi, L.K.; Alkhameesi, N.F.; Bahaidarah, S.A. Clinical Presentation of Myocarditis in the Pediatric Age Group and Predictors of Poor Early and Late Outcomes: Academic Hospital Experience. Cureus. 2022, 14, e31643. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Tsuda, E.; Miyazaki, A.; Ishibashi-Ueda, H.; Yamada, O. Clinical characteristics and long-term outcome of acute myocarditis in children. Heart Vessels. 2013, 28, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2013, 128, 1810–1852. [Google Scholar] [CrossRef] [PubMed]
- Károlyi, M.; Kolossváry, M.; Weber, L.; Matziris, I.; Polacin, M.; Sokolska, J.M.; Gotschy, A.; Alkadhi, H.; Manka, R. Association between ECG parameters and late gadolinium enhancement along the course of myocarditis. Int J Cardiovasc Imaging. 2023, 39, 1169–1178. [Google Scholar] [CrossRef]
- Cooper, L.T.Jr. Myocarditis. N Engl J Med. 2009, 360, 1526–1538. [Google Scholar] [CrossRef]
- Nakashima, H.; Honda, Y.; Katayama, T. Serial electrocardiographic findings in acute myocarditis. Intern Med. 1994, 33, 659–666. [Google Scholar] [CrossRef]
- Ogunbayo, G.O.; Elayi, S.C.; Ha, L.D.; Olorunfemi, O.; Elbadawi, A.; Saheed, D.; Sorrell, V.L. Outcomes of Heart Block in Myocarditis: A Review of 31,760 Patients. Heart Lung Circ. 2019, 28, 272–276. [Google Scholar] [CrossRef]
- Stulova, M.A.; Konstantinova, E.V. Ventricular extrasystole as manifestation of viral myocarditis and myopericarditis in young patients. Ter Arkh. 2007, 79, 28–34. [Google Scholar]
- Baksi, A.J.; Kanaganayagam, G.S.; Prasad, S.K. Arrhythmias in viral myocarditis and pericarditis. Card Electrophysiol Clin. 2015, 7, 269–281. [Google Scholar] [CrossRef]
- Chen, J.; Chen, S.; Li, Z.; Zhou, P.; Huang, W.; Wang, H.; Shi, J.; Ni, Y.; Lin, L.; Lei, Y. Role of electrocardiograms in assessment of severity and analysis of the characteristics of ST elevation in acute myocarditis: A two-centre study. Exp Ther Med. 2020, 20, 20. [Google Scholar] [CrossRef]
- Buttà, C.; Zappia, L.; Laterra, G.; Roberto, M. Diagnostic and prognostic role of electrocardiogram in acute myocarditis: A comprehensive review. Ann Noninvasive Electrocardiol. 2020, 25, e12726. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.C.; Brady, W.J.; Pollack, M. Electrocardiographic manifestations: acute myopericarditis. J Emerg Med. 1999, 17, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, A.; Birnbaum, Y. ST-segment elevation: Distinguishing ST elevation myocardial infarction from ST elevation secondary to nonischemic etiologies. World J Cardiol. 2014, 6, 1067–1079. [Google Scholar] [CrossRef] [PubMed]
- Birnbaum, Y.; Perez Riera, A.R.; Nikus, K. PR depression with multi lead ST elevation and ST depression in aVR: Is it always acute pericarditis? J Electrocardiol. 2019, 54, 13–17. [Google Scholar] [CrossRef]
- Sarda, L.; Colin, P.; Boccara, F.; Daou, D.; Lebtahi, R.; Faraggi, M.; Nguyen, C.; Cohen, A.; Slama, M.S.; Steg, P.G.; Le Guludec, D. Myocarditis in patients with clinical presentation of myocardial infarction and normal coronary angiograms. J Am Coll Cardiol. 2001, 37, 786–792. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Dai, Q.; Wu, H.; Chen, J.; Zhang, J.; Wei, Z. The diagnostic capability of electrocardiography on the cardiogenic shock in the patients with acute myocarditis. BMC Cardiovasc Disord. 2020, 20, 502. [Google Scholar] [CrossRef]
- Di Bella, G.; Florian, A.; Oreto, L.; Napolitano, C.; Todaro, M.C.; Donato, R.; Calamelli, S.; Camastra, G.S.; Zito, C.; Carerj, S.; et al. Electrocardiographic findings and myocardial damage in acute myocarditis detected by cardiac magnetic resonance. Clin Res Cardiol. 2012, 101, 617–624. [Google Scholar] [CrossRef]
- De Lazzari, M.; Zorzi, A.; Baritussio, A.; Siciliano, M.; Migliore, F.; Susana, A.; Giorgi, B.; Lacognata, C.; Iliceto, S.; Perazzolo Marra, M.; Corrado, D. Relationship between T-wave inversion and transmural myocardial edema as evidenced by cardiac magnetic resonance in patients with clinically suspected acute myocarditis: clinical and prognostic implications. J Electrocardiol. 2016, 49, 587–595. [Google Scholar] [CrossRef]
- Ahluwalia, M.; O'Quinn, R.; Ky, B.; Callans, D.; Kucharczuk, J.; Carver, J.R. Persistent PR segment change in malignant pericardial disease. Cardiooncology. 2016, 2, 6. [Google Scholar] [CrossRef]
- Madias, J.E. Transient attenuation of the amplitude of the QRS complexes in the diagnosis of Takotsubo syndrome. Eur Heart J Acute Cardiovasc Care. 2014, 3, 28–36. [Google Scholar] [CrossRef]
- Ukena, C.; Mahfoud, F.; Kindermann, I.; Kandolf, R.; Kindermann, M.; Böhm, M. Prognostic electrocardiographic parameters in patients with suspected myocarditis. Eur J Heart Fail. 2011, 13, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Dai, Q.; Wu, H.; Chen, J.; Zhang, J.; Wei, Z. The diagnostic capability of electrocardiography on the cardiogenic shock in the patients with acute myocarditis. BMC Cardiovasc Disord. 2020, 20, 502. [Google Scholar] [CrossRef] [PubMed]
- Brambatti, M.; Matassini, M.V.; Adler, E.D.; Klingel, K.; Camici, P.G.; Ammirati, E. Eosinophilic Myocarditis: Characteristics, Treatment, and Outcomes. J Am Coll Cardiol. 2017, 70, 2363–2375. [Google Scholar] [CrossRef] [PubMed]
- Viwe, M.; Nery, P.; Birnie, D.H. Management of ventricular tachycardia in patients with cardiac sarcoidosis. Heart Rhythm O2. 2021, 2, 412–422. [Google Scholar] [CrossRef] [PubMed]
- Morgera, T.; Di Lenarda, A.; Dreas, L.; Pinamonti, B.; Humar, F.; Bussani, R.; Silvestri, F.; Chersevani, D.; Camerini, F. Electrocardiography of myocarditis revisited: clinical and prognostic significance of electrocardiographic changes. Am Heart J. 1992, 124, 455–467. [Google Scholar] [CrossRef]
- Bhattacharya, I.S.; Dweck, M.; Francis, M. Lyme carditis: a reversible cause of complete atrioventricular block. J R Coll Physicians Edinb. 2010, 40, 121–122. [Google Scholar] [CrossRef]
- Kandolin, R.; Lehtonen, J.; Salmenkivi, K.; Räisänen-Sokolowski, A.; Lommi, J.; Kupari, M. Diagnosis, treatment, and outcome of giant-cell myocarditis in the era of combined immunosuppression. Circ Heart Fail. 2013, 6, 15–22. [Google Scholar] [CrossRef]
- Sekhri, V.; Sanal, S.; Delorenzo, L.J.; Aronow, W.S.; Maguire, G.P. Cardiac sarcoidosis: a comprehensive review. Arch Med Sc 2011, 7, 546–554. [Google Scholar] [CrossRef]
- Kaczmarek, K.A.; Szwabe, K.; Urbanek, I.; Ptaszynski, P.; Strzelecki, A.; Wranicz, J.K.; Cygankiewicz, I. Prevalence of Lyme Carditis in Patients with Atrioventricular Blocks. Int J Environ Res Public Health. 2022, 19, 14893. [Google Scholar] [CrossRef]
- Suresh, A.; Martens, P.; Tang, W.H.W. Biomarkers for Myocarditis and Inflammatory Cardiomyopathy. Curr Heart Fail Rep. 2022, 19, 346–355. [Google Scholar] [CrossRef]
- Amioka, N.; Nakamura, K.; Kimura, T.; Ohta-Ogo, K.; Tanaka, T.; Toji, T.; Akagi, S.; Nakagawa, K.; Toh, N.; Yoshida, M.; et al. Pathological and clinical effects of interleukin-6 on human myocarditis. J Cardiol. 2021, 78, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Fuse, K.; Kodama, M.; Okura, Y.; Ito, M.; Hirono, S.; Kato, K.; Hanawa, H.; Aizawa, Y. Predictors of disease course in patients with acute myocarditis. Circulation. 2000, 102, 2829–2835. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Zhang, X.; Shen, J.; Jiang, B.; Hu, D.; Zhao, M. Heparin-Binding Protein: A Novel Biomarker Linking Four Different Cardiovascular Diseases. Cardiol Res Pract. 2020, 15, 9575373. [Google Scholar] [CrossRef] [PubMed]
- Müller, I.; Vogl, T.; Kühl, U.; Krannich, A.; Banks, A.; Trippel, T.; Noutsias, M.; Maisel, A.S.; van Linthout, S.; Tschöpe, C. Serum alarmin S100A8/S100A9 levels and its potential role as biomarker in myocarditis. ESC Heart Fail. 2020, 7, 1442–1451. [Google Scholar] [CrossRef] [PubMed]
- Coronado, M.J.; Bruno, K.A.; Blauwet, L.A.; Tschöpe, C.; Cunningham, M.W.; Pankuweit, S.; van Linthout, S.; Jeon, E.S.; McNamara, D.M.; Krejčí, J.; et al. Elevated Sera sST2 Is Associated with Heart Failure in Men ≤50 Years Old With Myocarditis. J Am Heart Assoc. 2019, 8, e008968. [Google Scholar] [CrossRef]
- Mirna, M.; Schmutzler, L.; Topf, A.; Hoppe, U.C.; Lichtenauer, M. Neutrophil-to-lymphocyte ratio and monocyte-to-lymphocyte ratio predict length of hospital stay in myocarditis. Sci Rep. 2021, 11, 18101. [Google Scholar] [CrossRef]
- Kanda, T.; Kobayashi, I.; Suzuki, T.; Murata, K.; Radio, S.J.; McManus, B.M. Elevation of ALT to AST ratio in patients with enteroviral myocarditis. J Med. 1995, 26, 153–162. [Google Scholar]
- Omran, F.; Kyrou, I.; Osman, F.; Lim, V.G.; Randeva, H.S.; Chatha, K. Cardiovascular Biomarkers: Lessons of the Past and Prospects for the Future. Int J Mol Sci. 2022, 23, 5680. [Google Scholar] [CrossRef]
- Jeremias, A.; Gibson, C.M. Narrative review: alternative causes for elevated cardiac troponin levels when acute coronary syndromes are excluded. Ann Intern Med. 2005, 142, 786–791. [Google Scholar] [CrossRef]
- Liu, C.; Wang, Z.; Chen, K.; Cui, G.; Chen, C.; Wang, L.; Jiang, J. The absolute and relative changes in high-sensitivity cardiac troponin I are associated with the in-hospital mortality of patients with fulminant myocarditis. BMC Cardiovasc Disord. 2021, 21, 571. [Google Scholar] [CrossRef]
- Lehmann, L.H.; Heckmann, M.B.; Bailly, G.; Finke, D.; Procureur, A.; Power, J.R.; Stein, F.; Bretagne, M.; Ederhy, S.; Fenioux, C.; et al. Cardiomuscular Biomarkers in the Diagnosis and Prognostication of Immune Checkpoint Inhibitor Myocarditis. Circulation. 2023, 148, 473–486. [Google Scholar] [CrossRef] [PubMed]
- Sara, B.; Monteiro, J.; Carvalho, P.; Ribeiro Carvalho, C.; Chemba, J.; Ferreira, C.; Moreira, J.I. Are high NT-proBNP levels more related to inflammation than to left ventricular systolic dysfunction in acute myocarditis? Eur Heart J Acute Cardiovasc Care. 2021, 10, 189. [Google Scholar] [CrossRef]
- Ukena, C.; Kindermann, M.; Mahfoud, F.; Geisel, J.; Lepper, P.M.; Kandolf, R.; Böhm, M.; Kindermann, I. Diagnostic and prognostic validity of different biomarkers in patients with suspected myocarditis. Clin Res Cardiol. 2014, 103, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Heuser, J.S.; Cunningham, L.C.; Kosanke, S.D.; Cunningham, M.W. Mimicry and antibody-mediated cell signaling in autoimmune myocarditis. J Immunol. 2006, 177, 8234–8240. [Google Scholar] [CrossRef]
- Tymińska, A.; Ozierański, K.; Skwarek, A.; Kapłon-Cieślicka, A.; Baritussio, A.; Grabowski, M.; Marcolongo, R.; Caforio, A.L. Personalized Management of Myocarditis and Inflammatory Cardiomyopathy in Clinical Practice. J Pers Med. 2022, 12, 183. [Google Scholar] [CrossRef] [PubMed]
- Blagova, O.; Varionchik, N.; Zaidenov, V.; Savina, P.; Sarkisova, N. Anti-heart antibodies levels and their correlation with clinical symptoms and outcomes in patients with confirmed or suspected diagnosis COVID-19. Eur J Immunol. 2021, 51, 893–902. [Google Scholar] [CrossRef]
- Caforio, A.L.; Tona, F.; Bottaro, S.; Vinci, A.; Dequal, G.; Daliento, L.; Thiene, G.; Iliceto, S. Clinical implications of anti-heart autoantibodies in myocarditis and dilated cardiomyopathy. Autoimmunity 2008, 41, 35–45. [Google Scholar] [CrossRef]
- Goldberg, L.; Tirosh-Wagner, T.; Vardi, A.; Abbas, H.; Pillar, N.; Shomron, N.; Nevo-Caspi, Y.; Paret, G. Circulating MicroRNAs: a Potential Biomarker for Cardiac Damage, Inflammatory Response, and Left Ventricular Function Recovery in Pediatric Viral Myocarditis. J Cardiovasc Transl Res. 2018, 11, 319–328. [Google Scholar] [CrossRef]
- Besler, C.; Urban, D.; Watzka, S.; Lang, D.; Rommel, K.P.; Kandolf, R.; Klingel, K.; Thiele, H.; Linke, A.; Schuler, G.; et al. Endomyocardial miR-133a levels correlate with myocardial inflammation, improved left ventricular function, and clinical outcome in patients with inflammatory cardiomyopathy. Eur J Heart Fail. 2016, 18, 1442–1451. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Domínguez, R.; Sánchez-Díaz, R.; de la Fuente, H.; Jiménez-Borreguero, L.J.; Matesanz-Marín, A.; Relaño, M.; Jiménez-Alejandre, R.; Linillos-Pradillo, B.; Tsilingiri, K.; Martín-Mariscal, M.L.; et al. A Novel Circulating MicroRNA for the Detection of Acute Myocarditis. N Engl J Med. 2021, 384, 2014–2027. [Google Scholar] [CrossRef]
- Aleshcheva, G.; Pietsch, H.; Escher, F.; Schultheiss, H.P. MicroRNA profiling as a novel diagnostic tool for identification of patients with inflammatory and/or virally induced cardiomyopathies. ESC Heart Fail. 2021, 8, 408–422. [Google Scholar] [CrossRef] [PubMed]
- Grodzka, O.; Procyk, G.; Gąsecka, A. The Role of MicroRNAs in Myocarditis-What Can We Learn from Clinical Trials? Int J Mol Sci. 2022, 23, 16022. [Google Scholar] [CrossRef] [PubMed]
- Adeboye, A.; Alkhatib, D.; Butt, A.; Yedlapati, N.; Garg, N. A Review of the Role of Imaging Modalities in the Evaluation of Viral Myocarditis with a Special Focus on COVID-19-Related Myocarditis. Diagnostics 2022, 12, 549. [Google Scholar] [CrossRef] [PubMed]
- Felker, G.M.; Boehmer, J.P.; Hruban, R.H.; Hutchins, G.M.; Kasper, E.K.; Baughman, K.L.; Hare, J.M. ; Echocardiographic findings in fulminant and acute myocarditis. J Am Coll Cardiol. 2000, 36, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Hameed, A.; Condliffe, R.; Swift, A.J.; Alabed, S.; Kiely, D.G.; Charalampopoulos, A. Assessment of Right Ventricular Function-a State of the Art. Curr Heart Fail Rep. 2023, 20, 194–207. [Google Scholar] [CrossRef] [PubMed]
- Grossman, S.M.; Pravda, N.S.; Orvin, K.; Hamdan, A.; Vaturi, M.; Bengal, T.; Kornowski, R.; Weissler-Snir, A. Characterization and long-term outcomes of patients with myocarditis: a retrospective observational study. Postepy Kardiol Interwencyjnej. 2021, 17, 60–67. [Google Scholar] [CrossRef]
- Meindl, C.; Paulus, M.; Poschenrieder, F.; Zeman, F.; Maier, L.S.; Debl, K. Patients with acute myocarditis and preserved systolic left ventricular function: comparison of global and regional longitudinal strain imaging by echocardiography with quantification of late gadolinium enhancement by CMR. Clin Res Cardiol. 2021, 110, 1792–1800. [Google Scholar] [CrossRef]
- Tünnemann-Tarr, A.; Stöbe, S.; Laufs, U.; Hagendorff, A.; Tayal, B. Speckle tracking echocardiography in a patient with viral myocarditis and acute myocardial infarction. J Cardiol Cases. 2020, 22, 184–191. [Google Scholar] [CrossRef]
- Løgstrup, B.B.; Nielsen, J.M.; Kim, W.Y.; Poulsen, S.H. Myocardial oedema in acute myocarditis detected by echocardiographic 2D myocardial deformation analysis. Eur Heart J Cardiovasc Imaging. 2016, 17, 1018–1026. [Google Scholar] [CrossRef]
- Sturmberger, T.; Niel, J.; Aichinger, J.; Ebner, C. Acute myocarditis with normal wall motion detected with 2D speckle tracking echocardiography. Echo Res Pract. 2016, 3, K15–K19. [Google Scholar] [CrossRef]
- Chinali, M.; Franceschini, A.; Ciancarella, P.; Lisignoli, V.; Curione, D.; Ciliberti, P.; Esposito, C.; Del Pasqua, A.; Rinelli, G.; Secinaro, A. Echocardiographic two-dimensional speckle tracking identifies acute regional myocardial edema and sub-acute fibrosis in pediatric focal myocarditis with normal ejection fraction: comparison with cardiac magnetic resonance. Sci Rep. 2020, 10, 11321. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, M.G.; Marcotte, F. Cardiac magnetic resonance assessment of myocarditis. Circ Cardiovasc Imaging. 2013, 6, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.T.; Liu, P.; et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert Recommendations. J Am Coll Cardiol. 2018, 72, 3158–3176. [Google Scholar] [CrossRef] [PubMed]
- Luetkens, J.A.; Faron, A.; Isaak, A.; Dabir, D.; Kuetting, D.; Feisst, A.; Schmeel, F.C.; Sprinkart, A.M.; Thomas, D. Comparison of Original and 2018 Lake Louise Criteria for Diagnosis of Acute Myocarditis: Results of a Validation Cohort. Radiol Cardiothorac Imaging. 2019, 1, e190010. [Google Scholar] [CrossRef] [PubMed]
- Francone, M.; Chimenti, C.; Galea, N.; Scopelliti, F.; Verardo, R.; Galea, R.; Carbone, I.; Catalano, C.; Fedele, F.; Frustaci, A. CMR sensitivity varies with clinical presentation and extent of cell necrosis in biopsy-proven acute myocarditis. JACC Cardiovasc Imaging. 2014, 7, 254–263. [Google Scholar] [CrossRef]
- Polte, C.L.; Bobbio, E.; Bollano, E.; Bergh, N.; Polte, C.; Himmelman, J.; Lagerstrand, K.M.; Gao, S.A. Cardiovascular Magnetic Resonance in Myocarditis. Diagnostics 2022, 12, 399. [Google Scholar] [CrossRef]
- Ferreira, V.M.; Piechnik, S.K.; Robson, M.D.; Neubauer, S.; Karamitsos, T.D. Myocardial tissue characterization by magnetic resonance imaging: novel applications of T1 and T2 mapping. J Thorac Imaging. 2014, 29, 147–154. [Google Scholar] [CrossRef]
- Mewton, N.; Liu, C.Y.; Croisille, P.; Bluemke, D.; Lima, J.A. Assessment of myocardial fibrosis with cardiovascular magnetic resonance. J Am Coll Cardiol. 2011, 57, 891–903. [Google Scholar] [CrossRef]
- Jiang, L.; Zuo, H.; Liu, J.; Wang, J.; Zhang, K.; Zhang, C.; Peng, X.; Liu, Y.; Wang, D.; Li, H.; et al. The pattern of late gadolinium enhancement by cardiac MRI in fulminant myocarditis and its prognostic implication: a two-year follow-up study. Front Cardiovasc Med. 2023, 10, 1144469. [Google Scholar] [CrossRef]
- Friedrich, M.G.; Strohm, O.; Schulz-Menger, J.; Marciniak, H.; Luft, F.C.; Dietz, R. Noninvasive diagnosis of acute myocarditis by contrast-enhanced magnetic resonance imaging - response to the author. Circulation. 1999, 99, 459–460. [Google Scholar]
- Menacho, K.D.; Ramirez, S.; Perez, A.; Dragonetti, L.; Perez de Arenaza, D.; Katekaru, D.; Illatopa, V.; Munive, S.; Rodriguez, B.; Shimabukuro, A. Improving cardiovascular magnetic resonance access in low- and middle-income countries for cardiomyopathy assessment: rapid cardiovascular magnetic resonance. Eur Heart J. 2022, 7, 2496–2507. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.; Batrice, A.; Rischpler, C.; Eiber, M.; Ibrahim, T.; Nekolla, S.G. Utility of multimodal cardiac imaging with PET/MRI in cardiac sarcoidosis: Implications for diagnosis, monitoring and treatment. Eur. Heart J. 2014, 35, 312. [Google Scholar] [CrossRef] [PubMed]
- von Olshausen, G.; Hyafil, F.; Langwieser, N.; Laugwitz, K.L.; Schwaiger, M.; Ibrahim, T. Detection of acute inflammatory myocarditis in Epstein Barr virus infection using hybrid 18F-fluoro-deoxyglucose-positron emission tomography/magnetic resonance imaging. Circulation 2014, 130, 925–926. [Google Scholar] [CrossRef] [PubMed]
- Lamacie, M.M.; Almufleh, A.; Nair, V.; Stadnick, E.; Birnie, D.; Beanlands, R.; Chih, S. Serial 18F-Fluorodeoxyglucose Positron Emission Tomography Imaging in a Patient with Giant Cell Myocarditis. Circ. Cardiovasc. Imaging 2020, 13, e009940. [Google Scholar] [CrossRef] [PubMed]
- Mathijssen, H.; Tjoeng, T.W.H.; Keijsers, R.G.M.; Bakker, A.L.M.; Akdim, F.; van Es, H.W.; van Beek, F.T.; Veltkamp, M.V.; Grutters, J.C.; Post, M.C. The usefulness of repeated CMR and FDG PET/CT in the diagnosis of patients with initial possible cardiac sarcoidosis. EJNMMI Res. 2021, 11, 129. [Google Scholar] [CrossRef] [PubMed]
- Nensa, F.; Kloth, J.; Tezgah, E.; Poeppel, T.D.; Heusch, P.; Goebel, J.; Nassenstein, K.; Schlosser, T. Feasibility of FDG-PET in myocarditis: Comparison to CMR using integrated PET/MRI. J Nucl Cardiol. 2018, 25, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Castiglione, V.; Aimo, A.; Todiere, G.; Barison, A.; Fabiani, I.; Panichella, G.; Genovesi, D.; Bonino, L.; Clemente, A.; Cademartiri, F. Role of Imaging in Cardiomyopathies. Card Fail Rev. 2023, 9, e08. [Google Scholar] [CrossRef]
- Chen, W.; Jeudy, J. Assessment of Myocarditis: Cardiac MR, PET/CT, or PET/MR? Curr Cardiol Rep. 2019, 21, 76. [Google Scholar] [CrossRef]
- Vita, T.; Okada, D.R.; Veillet-Chowdhury, M.; Bravo, P.E.; Mullins, E.; Hulten, E.; Agrawal, M.; Madan, R.; Taqueti, V.R.; Steigner, M.; et al. Complementary Value of Cardiac Magnetic Resonance Imaging and Positron Emission Tomography/Computed Tomography in the Assessment of Cardiac Sarcoidosis. Circ Cardiovasc Imaging. 2018, 11, e007030. [Google Scholar] [CrossRef]
- Ammirati, E.; Veronese, G.; Bottiroli, M.; Wang, D.W.; Cipriani, M.; Garascia, A.; Pedrotti, P.; Adler, E.D.; Frigerio, M. Update on acute myocarditis. Trends Cardiovasc Med. 2021, 31, 370–379. [Google Scholar] [CrossRef]
- Pasupathy, S.; Air, T.; Dreyer, R.P.; Tavella, R.; Beltrame, J.F. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation. 2015, 131, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Taghavi, S.; Chenaghlou, M.; Mirtajaddini, M.; Naderi, N.; Amin, A. Takotsubo syndrome without major stress mimicking myocarditis. Anatol J Cardiol. 2020, 23, 349–350. [Google Scholar] [CrossRef] [PubMed]
- Lasica, R.; Spasic, J.; Djukanovic, L.; Trifunovic-Zamaklar, D.; Orlic, D.; Nedeljkovic-Arsenovic, O.; Asanin, M. Case report: Acute toxic myocardial damage caused by 5-fluorouracil-from enigma to success. Front Cardiovasc Med. 2022, 9, 991886. [Google Scholar] [CrossRef] [PubMed]
- Rapezzi, C.; Arbustini, E.; Caforio, A.L.; Charron, P.; Gimeno-Blanes, J.; Heliö, T.; Linhart, A.; Mogensen, J.; Pinto, Y.; Ristic, A.; et al. Diagnostic work-up in cardiomyopathies: bridging the gap between clinical phenotypes and final diagnosis. A position statement from the ESC Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2013, 34, 1448–1458. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Peretto, G.; Sala, S.; Rizzo, S.; Palmisano, A.; Esposito, A.; De Cobelli, F.; Campochiaro, C.; De Luca, G.; Foppoli, L.; Dagna, L. Ventricular Arrhythmias in Myocarditis: Characterization and Relationships with Myocardial Inflammation. J Am Coll Cardiol. 2020, 75, 1046–1057. [Google Scholar] [CrossRef] [PubMed]
- Mirna, M.; Schmutzler, L.; Topf, A.; Boxhammer, E.; Sipos, B.; Hoppe, U.C.; Lichtenauer, M. Treatment with Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) Does Not Affect Outcome in Patients with Acute Myocarditis or Myopericarditis. J Cardiovasc Dev Dis. 2022, 19, 32. [Google Scholar] [CrossRef]
- Berg, J.; Lovrinovic, M.; Baltensperger, N.; Kissel, C.K.; Kottwitz, J.; Manka, R.; Patriki, D.; Scherff, F.; Schmied, C.; Landmesser, U.; et al. Non-steroidal anti-inflammatory drug use in acute myopericarditis: 12-month clinical follow-up. Open Heart. 2019, 6, e000990. [Google Scholar] [CrossRef]
- Montero, S.; Abrams, D.; Ammirati, E.; Huang, F.; Donker, D.W.; Hekimian, G.; García-García, C.; Bayes-Genis, A.; Combes, A.; Schmidt, M. Fulminant myocarditis in adults: a narrative review. J Geriatr Cardiol. 2022, 19, 137–151. [Google Scholar]
- Zeppenfeld, K.; Tfelt-Hansen, J.; de Riva, M.; Winkel, B.G.; Behr, E.R.; Blom, N.A.; Charron, P.; Corrado, D.; Dagres, N.; de Chillou, C.; et al. ESC Scientific Document Group. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J. 2022, 43, 3997–4126. [Google Scholar] [CrossRef]
- Bang, V.; Ganatra, S.; Shah, S.P.; Dani, S.S.; Neilan, T.G.; Thavendiranathan, P.; Resnic, F.S.; Piemonte, T.C.; Barac, A.; Patel, R.; et al. Management of Patients with Giant Cell Myocarditis: JACC Review Topic of the Week. J Am Coll Cardiol. 2021, 77, 1122–1134. [Google Scholar] [CrossRef] [PubMed]
- Maury, P.; Chilon, T.; Dumonteil, N.; Fontan, A. Complete atrioventricular block persisting after regression of infectious myocarditis. J Electrocardiol. 2008, 41, 665–667. [Google Scholar] [CrossRef] [PubMed]
- Pelargonio, G.; Pinnacchio, G.; Narducci, M.L.; Pieroni, M.; Perna, F.; Bencardino, G.; Comerci, G.; Dello Russo, A.; Casella, M.; Bartoletti, S.; et al. Long-Term Arrhythmic Risk Assessment in Biopsy-Proven Myocarditis. JACC Clin Electrophysiol. 2020, 6, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Bardy, G.H.; Lee, K.L.; Mark, D.B.; Poole, J.E.; Packer, D.L.; Boineau, R.; Domanski, M.; Troutman, C.; Anderson, J.; Johnson, G.; et al. Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT) Investigators. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005, 352, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, A.; Solberg, E.E.; Papadakis, M.; Adami, P.E.; Biffi, A.; Caselli, S.; La Gerche, A.; Niebauer, J.; Pressler, A.; Schmied, C.M.; et al. Recommendations for participation in competitive and leisure time sport in athletes with cardiomyopathies, myocarditis, and pericarditis: position statement of the Sport Cardiology Section of the European Association of Preventive Cardiology (EAPC). Eur Heart J. 2019, 40, 19–33. [Google Scholar] [CrossRef]
- Kühl, U.; Pauschinger, M.; Schwimmbeck, P.L.; Seeberg, B.; Lober, C.; Noutsias, M.; Poller, W.; Schultheiss, H.P. Interferon-beta treatment eliminates cardiotropic viruses and improves left ventricular function in patients with myocardial persistence of viral genomes and left ventricular dysfunction. Circulation. 2003, 107, 2793–2798. [Google Scholar] [CrossRef]
- Abdenasser, D.; Amine, E. Rare case of subacute herpetic myocarditis. IDCases. 2023, 33, e01828. [Google Scholar] [CrossRef]
- Deonarain, R.; Cerullo, D.; Fuse, K.; Liu, P.P.; Fish, E.N. Protective role for interferon-beta in coxsackievirus B3 infection. Circulation. 2004, 110, 3540–3543. [Google Scholar] [CrossRef]
- Goland, S.; Czer, L.S.; Siegel, R.J.; Tabak, S.; Jordan, S.; Luthringer, D.; Mirocha, J.; Coleman, B.; Kass, R.M.; Trento, A. Intravenous immunoglobulin treatment for acute fulminant inflammatory cardiomyopathy: series of six patients and review of literature. Can J Cardiol. 2008, 24, 571–574. [Google Scholar] [CrossRef]
- Kishimoto, C.; Shioji, K.; Hashimoto, T.; Nonogi, H.; Lee, J.D.; Kato, S.; Hiramitsu, S.; Morimoto, S.I. Therapy with immunoglobulin in patients with acute myocarditis and cardiomyopathy: analysis of leukocyte balance. Heart Vessels. 2014, 29, 336–342. [Google Scholar] [CrossRef]
- Fuchs, K.; Rummler, S.; Ries, W.; Helmschrott, M.; Selbach, J.; Ernst, F.; Morath, C.; Gauly, A.; Atiye, S.; Stauss-Grabo, M.; et al. Performance, clinical effectiveness, and safety of immunoadsorption in a wide range of indications. Ther Apher Dial. 2022, 26, 229–241. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Z.; Yang, Z.; Peng, Y.; Wang, L.; Yuan, X. Diagnosis and treatment of eosinophilic myocarditis. J Transl Autoimmun. 2021, 4, 100118. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Ortiz, M.; Anguita-Sánchez, M.; Bonilla-Palomas, J.L.; Fernández-Pérez, C.; Bernal-Sobrino, J.L.; Cequier-Fillat, A.; Bueno-Zamora, H.; Marín, F.; Elola-Somoza, F.J. Incidence and outcomes of hospital treated acute myocarditis from 2003 to 2015 in Spain. Eur J Clin Invest. 2021, 51, e13444. [Google Scholar] [CrossRef] [PubMed]
- Alamri, A.S.; Khayat, L.T.; Alzahrani, A.J.; Kurdi, L.K.; Alkhameesi, N.F.; Bahaidarah, S.A. Clinical Presentation of Myocarditis in the Pediatric Age Group and Predictors of Poor Early and Late Outcomes: Academic Hospital Experience. Cureus. 2022, 14, e31643. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



