
Submitted:
05 September 2023
Posted:
07 September 2023
You are already at the latest version
Abstract
Alveolar bone atrophy after tooth extraction presents significant difficulties when planning delayed-immediate implant treatment to replace a lost tooth. Socket augmentation is an effective therapy that limits the post extraction volumetric changes and facilitates implant placement whilst reducing the need for staged grafting. However, socket augmentation and osteoconductive graft conversion is a slow process that could take 4-6 months. PRF and its variants have significant bio-enhancement effect on wound healing and regeneration through release of platelet drived growth factors, bioactive substances, cytokines. Leukocytes in PRF also play a significant role in enhancing tissue regeneration as part of osteo-immune response. Use of PRF during socket augmentation is highly effective in enhancing extraction site healing and graft integration by angiogenesis, cell proliferation, recruitment, and differentiation through release of growth factors and bioactive substances mediated by platelets and leukocytes. PRF with SA is recommended as an adjunct to SA as a sole biomaterial or in combination with xenograft or allograft bone substitutes to enhance tissue regeneration and to reduce risk of infection, osteitis and postoperative pain in extraction sockets
Keywords:
platelet-rich fibrin
; ridge augmentation
; socket augmentation
; grafting
; cytokines
; growth factors
; tissue regeneration
; bio-enhancement
; PRF
; platelet concentrate
; accelerated implant treatment
1. Introduction
1.1. Use of Platelet-Rich Fibrin (PRF) in Dentistry:
Autologous platelet concentrates have been used in dentistry for many years to promote hard and soft tissue healing. Numerous clinical studies, including randomized clinical trials (RCT), have reported on the benefits and bioactive role of platelet concentrates on angiogenesis, cell recruitment, differentiation, mineralization, and tissue regeneration during wound healing. Since the application by Marx et al in 1998 of platelet-rich plasma (PRP) in oral defects, this technology has seen increasing use in oral surgery and implantology, particularly since the introduction of new, less complex, and more effective second and third-generation platelet concentrate preparation protocols in recent years [1]. A recent systematic review by Yu et al 2022 showed a rapid increase in annual publications on PRF including original research articles (58.01%), reviews (17.08%), and case reports (10.14%). In dentistry, PRF was reported to be frequently used in oral surgery (31.14%), periodontal regeneration (22.42%), and implant therapy (18.68%) [1,2]. The purpose of using PRF is to support natural wound healing and to enhance tissue regeneration for improved clinical outcomes. In oral surgery, the reported benefits of PRF therapy include less morbidity and pain, faster wound healing, and regeneration of new bone and soft tissue following tissue injury. The aim of this paper was to demonstrate the use of PRF in conjunction with SA in reducing the overall duration of staged implant treatment following tooth extractions, in two case studies, using objective outcome measures. Additionally, a narrative review of the current evidence supporting the bioenhancement role of PRF when applied alongside socket augmentation (SA) is presented.
The basic mechanism by which platelet concentrates accelerate wound healing is related to their ability to provide 6 – 8 times more supraphysiological doses of platelet derived substances including growth factors, cytokines, and immune system messengers which are involved in the stimulation of mesenchymal stem cell recruitment, differentiation, and activation for enhanced tissue healing and regeneration [3]. Whereas the original protocol by Marx et al (1998) involved the addition of bovine thrombin to obtain PRP [4], Anitua described a protocol of producing platelet-rich plasma (PRP) concentrate using CaCl and heat treatment which he termed as “platelet rich growth factors” (PRGF) [5,6]. These products excluded the leukocytes from the fibrin matrix and the anticoagulant additive used in preparing PRP was later shown to be detrimental for tissue regeneration [3,4]. A simpler second-generation plasma concentrates protocol (PRF) that involved obtaining a fibrin clot by employing a novel centrifuge spinning technique was introduced by Choukroun [5,6,7] This more streamlined method did not require the addition of an anticoagulant or chemicals to the autologous blood sample [8,9,10]. A search of the literature was carried out using the search words PRF, SA, bioenhancement, and accelerated implant treatment after tooth loss with the inclusion criteria of randomized clinical trials (RCTs) only. The search results did not allow a systematic review as the RCTs did not have structured study designs or homogenous outcome measures. Most importantly, the papers included various different PRF preparation methods with the use of a variety of biomaterials in SA. Therefore, the authors have chosen to carry out a comprehensive narrative review and critical analysis of the current evidence available for SA with PRF along with case studies as proof of concept.
1.2. Improved PRF protocols- A-PRF, A-PRF+ and i-PRF
Depending on individual surgical requirements, PRF can be prepared in solid and/or liquid form (e.g. a-PRF, iPRF, a-PRF+) by altering the G-force during centrifugation (Table 1 and Table 2). Both matrices are rich in growth factors and the differences between different second-generation platelet concentrates have been shown to be small and probably clinically not significant [11,12]. The second-generation PRF concentrates such as advanced platelet rich fibrin (A-PRF), A-PRF+ and injectable PRF (i-PRF) use lower centrifugal “g-forces” to obtain higher growth factor release compared with the original PRF protocol. The slower centrifugation reduces cell loss and increases the concentration of leukocytes in the PRF matrix (mostly in the buffy coat layer). The effect is to increase the concentration of the total number of cells (neutrophils, lymphocytes, undifferentiated monocytes, and immune cells) as well as the growth factors that are actively involved in bone and soft tissue regeneration. Advanced PRF (A-PRF) is obtained using reduced g-forces; at 1,500 rpm (230g) for 14 min or at 1,300 rpm (200g) for 14 min [11] (see Table 1.)

Table 1.
Protocols for producing different formulations (solid and liquid) of PRF [12].
Table 1.
Protocols for producing different formulations (solid and liquid) of PRF [12].
| PRF Preparation | Tube | RCF (g) | Time (mins) | Speed (rpm) | Evidence |
| Solid Matrix | |||||
| L-PRF | Glass or Silica coated | 408 | 12 | 2700 | Choukroun, 2001 [7] |
| A-PRF | Glass or Silica coated | 194 | 14 | 1500 | Ghanaati et al, 2014 [14] |
| A-PRF+ | Glass or Silica coated | 145 | 8 | 1300 | Fujioka-Kobayashi et al 2017 [15] |
| Liquid/Flowable matrix | |||||
| i-PRF | Plastic (PET) | 60 | 3 | 700 | Miron et al 2017 [9] |
| C-PRF | Plastic (PET) | 408 | 12 | 2700 | Miron et al 2020 [10] |
Table 2.
Conversion table for calculating g-force from rpm and radius arm of the centrifuge device. (Adapted from Sigma Aldrich).
Table 2.
Conversion table for calculating g-force from rpm and radius arm of the centrifuge device. (Adapted from Sigma Aldrich).
| Radius (cm) | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
| Speed (rpm) | ||||||||||
| 1000 | 45 | 56 | 67 | 78 | 89 | 101 | 112 | 123 | 134 | 145 |
| 1500 | 101 | 126 | 151 | 176 | 201 | 226 | 252 | 277 | 302 | 327 |
| 2000 | 179 | 224 | 268 | 313 | 358 | 402 | 447 | 492 | 537 | 581 |
| 2500 | 280 | 349 | 419 | 489 | 559 | 629 | 699 | 769 | 839 | 908 |
| 3000 | 402 | 503 | 604 | 704 | 805 | 906 | 1006 | 1107 | 1207 | 1308 |
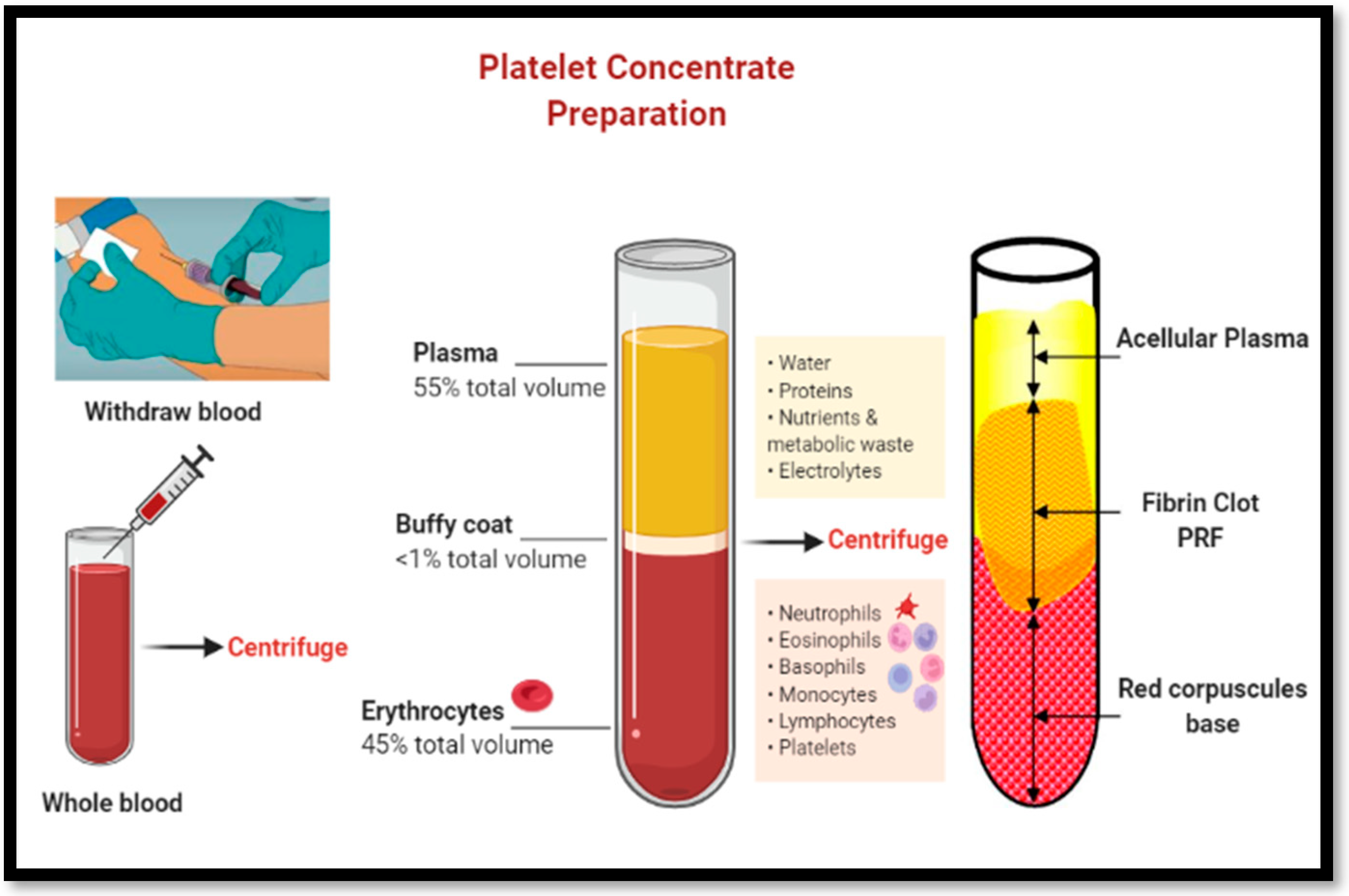
The spin protocols change between different centrifuge devices and can be calculated using a formula that is based on the radius of the rotor arm of the device and the speed of rotation (see Table 2) Generally, slower centrifugation protocols of 1300 rpm × 8 min produce more evenly distributed number of platelets compared with the original PRF protocol of 2700 rpm x 14 min. Furthermore, Kobayashi et al, 2016 have demonstrated much-sustained release of GFs from slower preparation of PRF (e.g. a-PRF) compared with the original PRP or PRF protocols [17,18]. Injectable-PRF (i-PRF) protocol (60g g-force at 3 mins) produces the highest concentration of leukocytes/platelets in a smaller volume of liquid matrix. Plastic (PET) tubes used in i-PRF protocol do not activate the coagulation process since they have hydrophobic surfaces with no coatings thus a liquid plasma concentrate rich in growth factors, platelets, and bioactive substances forms quickly at the top of the tube [13–16 and 18,19].
Buffy coat layer, at the interface, histologically contains a highly dense layer of leukocytes or white blood cells (WBC). When collecting the PRF clot the face should be carefully separated from the red zone of RBC to preserve the WBC layer [19,20]. The solid fibrin matrix (PRF membrane) can be sutured or applied as a wound dressing in conjunction with guided bone regeneration (GBR) technique or can be packed into a fresh extraction site (fibrin plug) or a large bony defect to enhance tissue repair as part of SA. PRF membranes remain solid and release large quantities of GFs for 7 to 14 days. Liquid PRF can be mixed with a bone substitute material (e.g. xenograft or allograft) to produce a coagulated mixture known as “sticky bone” (Figure 2). This mixture acts not only as a physical scaffold to support new bone formation but also releases bioactive substances such as cytokines and growth factors (e.g. VEGF, PDGF, TGF) to enhance tissue regeneration (see Table 3).
Table 3.
Platelet Derived Growth Factors found in PRF that have direct role in early wound healing. These factors and cytokines released from processed platelets are involved in mesenchymal cell recruitment, cell differentiation and activation, angiogenesis, and wound healing processes.
Table 3.
Platelet Derived Growth Factors found in PRF that have direct role in early wound healing. These factors and cytokines released from processed platelets are involved in mesenchymal cell recruitment, cell differentiation and activation, angiogenesis, and wound healing processes.
| Growth factors | Functions |
| Transforming Growth factor (TGF) | Growth of endothelial vascular cells, cell recruitment and proliferation in wound healing. Inhibits osteoclast formation and bone resorption. Stimulates fibronectin and collagen production. |
| Epidermal Growth Factor (EGF) | Promotion of mesenchymal cell proliferation and differentiation, epithelial cell growth and angiogenesis |
| Vascular Endothelial Growth Fcator (VEGF) | Restores oxygen supply to the injured tissue. Promotes repair and growth of vascular endothelial cells, angiogenesis |
| Platelet Derived Growth Factors (PDGF) | Cell growth, proliferation of smooth muscle cells within vascular tissue, angiogenesis, collagen production Provokes proliferation of mesenchymal cell lineage, enablers macrophage chemotaxis |
| Insulin-like Growth Factor (IGF) | Cell proliferation, cell to cell communications, stimulates chemotaxis and activation of osteoblasts and bone formation, induces mitogenesis of mesenchymal cells |
| Fibroblast Growth Factor (FGF) | Tissue Repair, Cell Growth, Hyaluronic acid and Collagen production |
More recently, Miron et al (2020) managed to further increase the platelet and leukocytes concentration by over 10-fold using a new method of harvesting platelet-rich fibrin (C-PRF) from the buffy coat portion of the platelet concentrate [22]. Tunali et al (2014) described titanium-prepared platelet-rich fibrin protocol (T-PRF) using an identical centrifugal protocol to A-PRF but using titanium tubes arguing that titanium would help to activate platelets more effectively [23]. However, the benefit of this technique remains to be demonstrated clinically. PRF has been used in conjunction with socket augmentation, alveolar ridge grafting, GBR procedures, maxillary sinus grafting, treatment of periodontal and peri-implantitis defects, and soft tissue grafting in dentistry successfully. Although a PRF membrane does not act as a true barrier membrane it contributes directly to repair and regeneration at all stages of wound healing. Clinical and histomorphometric research has shown significantly more bone regeneration within bone defects when PRF is combined with xenografts (demineralized bovine matrix/ Bioss®) or allografts (demineralized freeze-dried bone) [24,25,26,27]. The reported benefits also included no need for primary wound closure, less ridge resorption, and improved bone quality histologically and density radiologically with less incidence of pain and alveolitis [28].
1.3. Mode of action and biological effects of PRF:
Platelets and leukocytes are the main cells that are responsible for the biological activity of PRF (Pavlovic et al 2021, Quirynen and Pinto, 2022) [11,29]. Activated platelet concentrate (PRF) initiates an immune cell response via anti-inflammatory and pro-inflammatory processes that include leukocytes (neutrophils, monocytes and lymphocytes). In addition to the activated platelets and leukocytes, the fibrin network acts as a reservoir for platelet-derived growth factors (Table 1) that are known to be involved in all stages of wound healing including angiogenesis, cell recruitment, cell differentiation, mineralization, and tissue regeneration [30,31]. The GF and bioactive substances are stored in alpha, delta, and lambda granules within the platelets. In addition to GFs, PRF is also enriched with leukocytes and immune cytokines (e.g. interleukin) which are the main drivers of bone and soft tissue regeneration [32].
Leukocytes regulate cell proliferation and cell differentiation and play a key in response to tissue injury at all stages of healing and regeneration, inflammatory proliferation, tissue remodeling and maturation. During the inflammatory phase neutrophils are recruited to remove bacteria and necrotic tissue. They also produce inflammatory cytokines and GFs which are essential for early phases of wound healing. Monocytes are the second type of leukocytes that are the precursors to macrophages. Normally they are provided from bone marrow. PRF matrix, in addition to platelets, provides a highly concentrated cell line of leukocytes which enhance all phases of tissue healing, angiogenesis, mesenchymal stem cell activation and tissue regeneration including osteogenesis. PRF matrix has also been shown to exhibit a strong antibacterial capacity to most oral pathogens [33]. Both liquid and solid matrices of PRF release growth factors up to 10 days after reaching a peak at day 7. [29,34]. Protocols for producing PRF variants are shown in Table 1.
Figure 1.
PRF protocol: distinct stages from blood drawing, centrifugation, and clotting process. Buffy coat is a thin layer of highly concentrated leukocytes and platelets at the “face” of the PRF matrix bordering the RBC zone below. Studies have shown significantly higher release of GFs and cytokines from the cells in buffy coat layer.
Figure 1.
PRF protocol: distinct stages from blood drawing, centrifugation, and clotting process. Buffy coat is a thin layer of highly concentrated leukocytes and platelets at the “face” of the PRF matrix bordering the RBC zone below. Studies have shown significantly higher release of GFs and cytokines from the cells in buffy coat layer.
PRF and its variants have been shown to enhance wound healing during SA. Alissa et al (2010), reported a denser trabecular pattern and less pain sensation along with better soft tissue healing when PRP was used for ridge augmentation. Anitua et al 2015 [35] reported that PRGF yielded good outcomes such as regenerated socket volume, bone density and soft tissue healing along with the percentage of new bone formation when PRGF was used in mandibular extraction sockets. However, when PRGF, which is depleted of leucocytes, is used the results cannot be translated to PRF due to their different properties. Production of PRGF requires the addition of CaCl solution followed by heat treatment. Others have reported beneficial SA results with increased crestal ridge width and a higher percentage of vital bone [36,37]. Wu et al 2012 found that PRF stimulates PDLF proliferation, as well as osteoblast and gingival fibroblast proliferation by 1.28-fold collectively (P<0.05)- thus increasing post-operative bone regeneration. PRF is also shown to reduce the overall wound healing time [38].
There is strong biological evidence to support the application of PRF as a bioactive material to enhance tissue regeneration and wound repair. Numerous biochemical studies have shown that PRF exhibits significant concentration of biologically active-matrix proteins and growth factors (GF) which are released slowly due to the three-dimensional architecture of glycoproteins in the fibrin clot (see Table 1). Furthermore, PRF is thought to play a role in an osteo-immune response that occurs as a result of an interplay between bone and the immune system. GFs are expressed in both matrices of PRF and contribute to enhancement of angiogenesis and early wound healing [39,40]. In an animal study Yuan et al (2021) applied PRF with a resorbable gel and found it to be effective in ridge preservation by facilitating blood clotting and promotion of angiogenesis and osteogenesis and recommended it as a cost-effective graft material for SA [41].
Hauser et al used PRF preparations in 168 post extraction sockets in fifty cardiac surgery patients without modification of their anticoagulant therapy (mean international normalized ratio = 3.16 ± 0.39). In all cases, no alveolitis or painful events were reported, and wound closure was complete at the time of suture removal one week after surgery. They proposed using PRF protocol as a reliable therapeutic option to avoid significant bleeding after dental extractions without the suspension of the continuous oral anticoagulant therapy in heart surgery patients [42]. In a case study, Chenchev et al 2017 reported the benefits of using a-PRF and i-PRF in conjunction with a bone substitute on augmentation of the alveolar ridge before implant placement [43]. In a rare split-mouth randomized controlled clinical trial Temmerman et al (2016) investigated the effect of using a preparation of platelet-rich fibrin as a socket-filling material on ridge preservation. In twenty-two patients in need of single bilateral and closely symmetrical tooth extractions in the maxilla or mandible, they reported significant differences (p < 0.005) in total width reduction between test (-22.84%) and control sites (-51.92%) at 1 mm below crest level and significant differences were found for socket fill between test (94.7%) and control sites (63.3%). They concluded that use of PRF was effective in preservation of horizontal and vertical ridge dimensions at three months after tooth extraction is beneficial [44].
In another split mouth RCT Castro et al (2021) studied the effect of different platelet-rich fibrin preparations (A-PRF+ and LPRF) and reported that although the mean horizontal and vertical changes at 1-mm below the crest (buccal and palatal side) were similar for the test and control sites (p > 0.05) both PRF matrices showed radiographically a significant superiority for the socket fill (L-PRF (85.2%) and A-PRF+ (83.8%) compared with the controls (67.9%) [44,37]. A SR by Al-Maawi (2021) of 20 RCT and controlled studies showed that PRF was effective in reducing post-operative pain, accelerating soft tissue healing and preventing dimensional bone loss, especially in the early time period of 2–3 months. Dimensional bone loss was significantly lower in the PRF group compared with the unaided wound healing after 8-15 weeks but not after 6 months. Socket fill was significantly higher in the PRF group compared with spontaneous wound healing. The authors concluded that based on the analyzed studies, PRF was most effective in the early healing period of 2-3 months after tooth extraction, and allowing a longer healing period may not provide any benefits. However, the authors found heterogeneity between the included studies and assessed a relatively high risk of bias in blinding of participant and personnel as well as blinding of outcome assessment [44,39]. In a multi-arm parallel randomized controlled clinical trial, Clark et al (2018) evaluated the efficacy of platelet rich fibrin (A-PRF) alone or mixed with freeze-dried bone allograft (FDBA) in improving vital bone formation and alveolar dimensional stability during SA, in fresh extraction sites [40].
In forty patients, non-molar extraction sites were randomized into one of four ridge preservation approaches: A-PRF, A-PRF+FDBA, FDBA, or blood clot They concluded that A-PRF alone or augmented with FDBA is a suitable biomaterial for ridge preservation [40]. This finding supports recommendations by Miron et al (2021) of using of PRF alone in intact premolar and molar sites to prevent dimensional changes, reduce pain and infection, and enhance wound healing. However, when the buccal wall of an extraction socket is missing, the use of a bone graft mixed with PRF is advisable. Bernnardo et al 2023, evaluated the use of platelet-rich fibrin (PRF) as a natural carrier for antibiotics delivery. Different antibiotics were added to PRF and their release and antimicrobial activity were analyzed against various microorganisms. Gentamicin and linezolid were released from PRF without affecting its physical properties and showed massive antibacterial activity against all microorganisms. Vancomycin interfered with PRF formation. PRF loaded with antibiotics allowed the release of effective concentrations of antimicrobial drugs and could potentially reduce the risk of post-operative infection after oral surgery. However, further studies are needed to confirm its efficacy as a topical antibiotic delivery tool [40,41,42]. The above-mentioned studies demonstrate the benefits of using PRF alone or in combination with bone substitute materials to promote healing and tissue regeneration. However, it should be noted that as there is a general lack of randomized clinical trials using standardized protocols for different PRF preparation and homogeneous outcome measures, the evidence for clinical efficiency of PRF and it’s variants, in bone regeneration in dental implantology, has not yet been fully established [44]. Future studies are urgently needed to demonstrate the optimum SA and PRF protocols using standardized protocols and outcome measures. In summary, there is emerging evidence that supports the biological and clinical benefits of using PRF during SA to enhance all stages of wound healing and tissue regeneration.
2. Materials and Methods
All cases were treated by a single Oral and Maxillofacial Surgeon (CU) in an outpatient setting under local anesthetic. Clinical and radiographical follow-up was performed to assess healing. As the procedures are carried out in ICE postgraduate institute and hospital, full consent process of the patients were taken as usual and no ethical approval process was necessary as it was a routine procedure followed in the hospital by the surgeon CU. To demonstrate the concept of accelerated implant treatment following SA in conjunction with PRF treatment, two case studies were included as a proof of concept. The case studies were selected from patients attending our center requiring tooth extraction and SA when immediate implant placements were not feasible or contraindicated according to criteria. The surgical procedures involved extraction of the teeth under a local inaesthetic (articanine). Teeth were extracted using a minimally invasive extraction technique without raising a periosteal flap. The sockets were immediately grafted with a xenograft (Bioss® small particles) mixed with i-PRF (liquid) to construct a coagulum of “sicky bone” (Figure 2) (Table 1). i-PRF (liquid) concentrate was prepared by collecting 10 ml venous blood and using a centrifugation protocol at 700 rpm for 3 minutes (see Table 1). Centrifugation was started within 90 seconds of drawing blood as recommended by Miron et al (2021). No barrier membranes were used, and the site was covered with a PRF membrane of fibrin clot which was sutured to the edges of the socket using 3.0 vicryl® rapid (Figure 3). No primary closure was carried out and the sockets were allowed to heal in a semi-open fashion by secondary intention. After 8 weeks, implants (Megagen® Anyridge) were placed (1 mm sub-crestally) with excellent primary stability (insertion torque >60 Ncm). Implants were fitted with transmucosal healing abutments (5 mm diameter and collar height of 3 mm) and allowed to heal transmucosally before being loaded 6 weeks after placement. Clinical and radiological follow-up examination at six months revealed satisfactory peri-implant soft tissue parameters with no radiological sign of marginal bone loss.
Figure 2.
“Sticky bone” is produced by mixing PRF liquid fraction with a bone substitute material (BioOss® Geistlich).
Figure 2.
“Sticky bone” is produced by mixing PRF liquid fraction with a bone substitute material (BioOss® Geistlich).
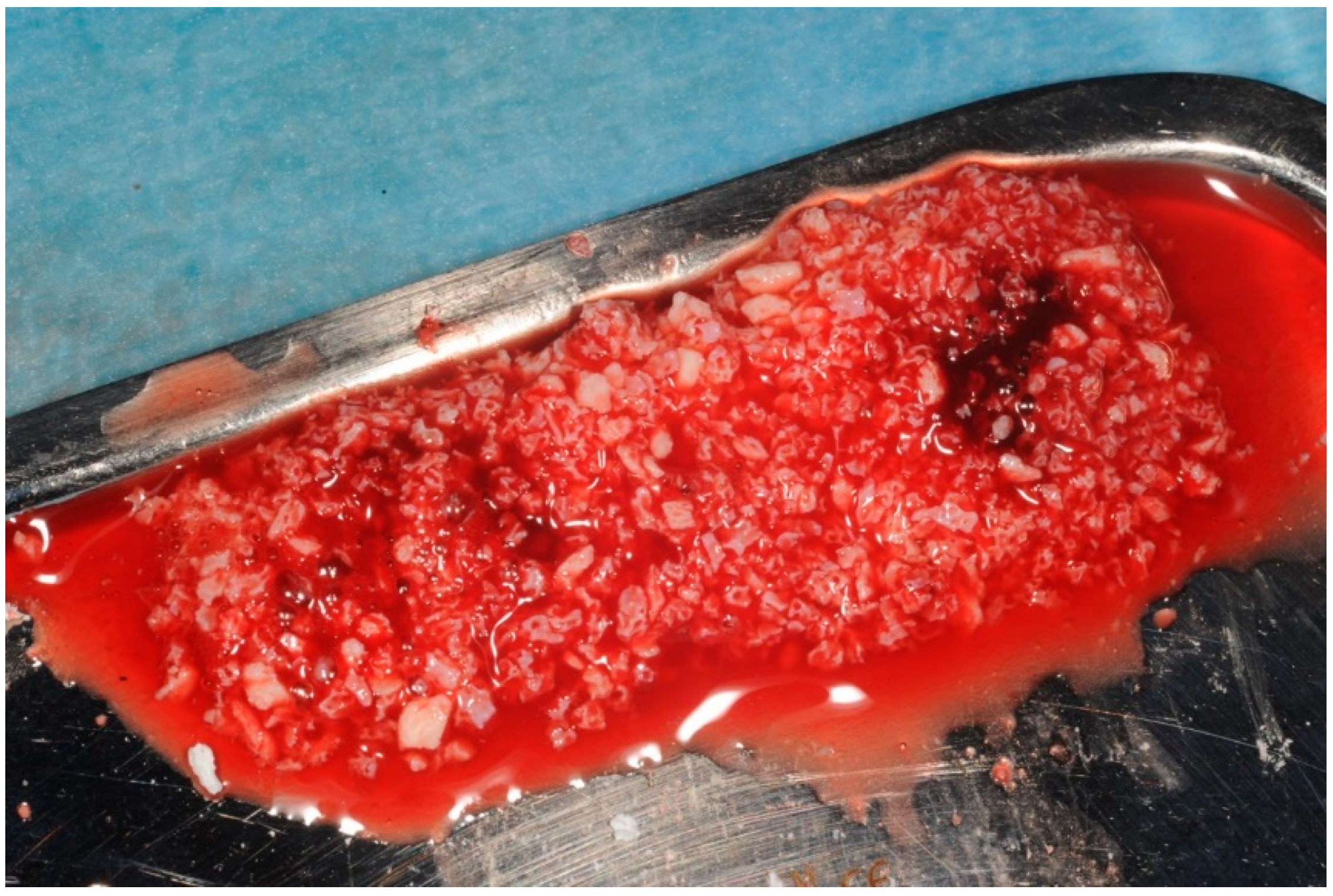
Figure 3.
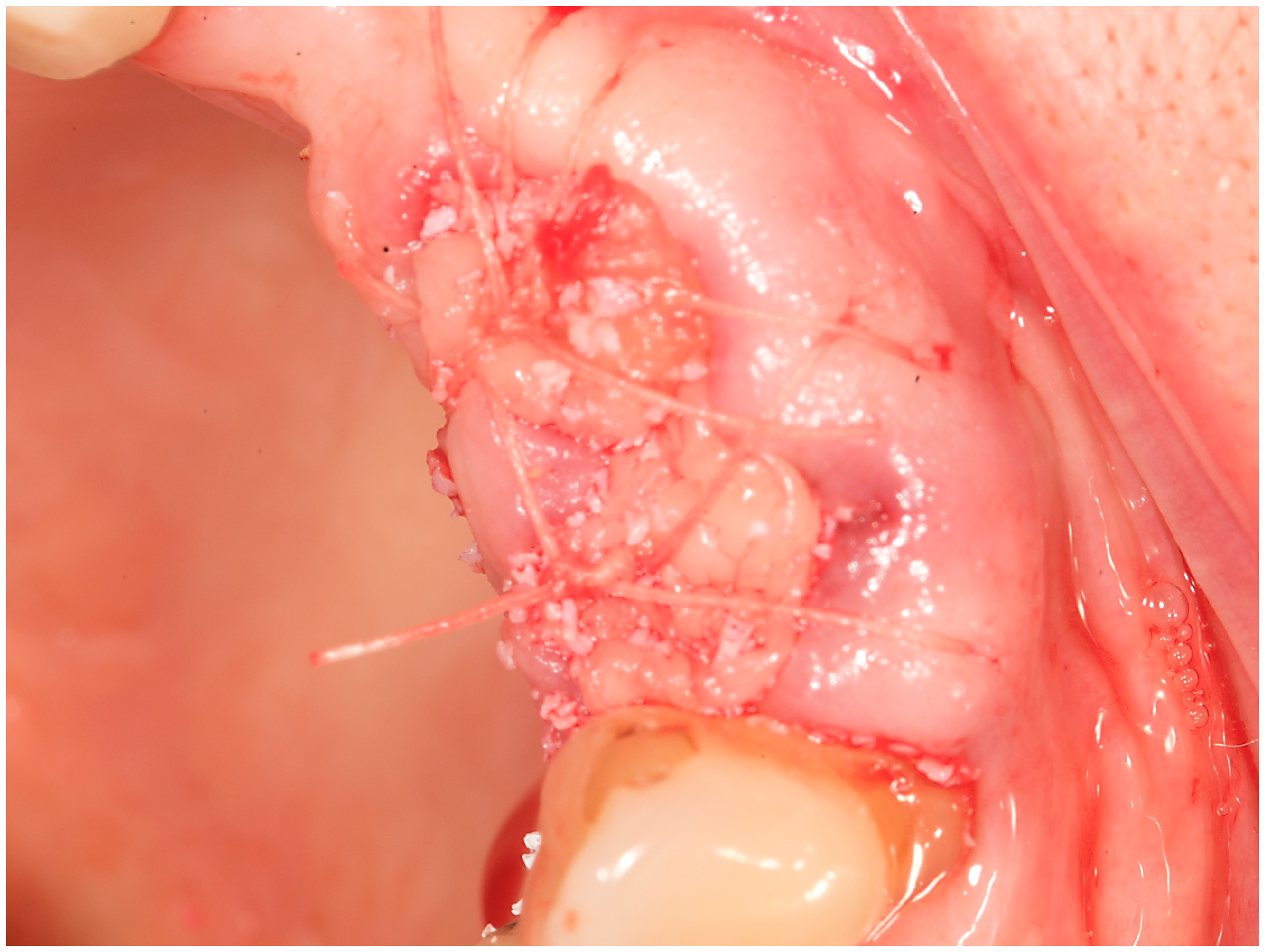
Semi-open minimally invasive socket augmentation technique with PRF fibrin: tooth extraction is carried out with a periotome to prevent fracture/loss of the thin buccal plate. A soft tissue flap is not raised to avoid damage to the periosteum and the blood supply. The socket is degranulated and irrigated with saline. The socket is augmented with sticky bone produced by mixing a bone substitute material (e.g. BioOss® Geistlich) and iPRF liquid. The graft is covered with a A-PRF fibrin which is sutured to the edges of the socket without any attempt to achieve primary closure. When using a “sticky bone” mixture of PRF and a biomaterial, it may not be essential to cover the extraction site with PRF fibrin membrane although evidence suggests that using 2 layers of PRF over the SA would be highly beneficial.
Figure 3.
Semi-open minimally invasive socket augmentation technique with PRF fibrin: tooth extraction is carried out with a periotome to prevent fracture/loss of the thin buccal plate. A soft tissue flap is not raised to avoid damage to the periosteum and the blood supply. The socket is degranulated and irrigated with saline. The socket is augmented with sticky bone produced by mixing a bone substitute material (e.g. BioOss® Geistlich) and iPRF liquid. The graft is covered with a A-PRF fibrin which is sutured to the edges of the socket without any attempt to achieve primary closure. When using a “sticky bone” mixture of PRF and a biomaterial, it may not be essential to cover the extraction site with PRF fibrin membrane although evidence suggests that using 2 layers of PRF over the SA would be highly beneficial.
The outcome measures used to assess the success of socket healing, bone conversion, and implant survival included:
- I)
-
Primary outcome measures:
- a)
- radiological assessment of bone quality and quantity after SA using cone beam computerized tomography (CBCT),
- b)
- bone quality and primary implant stability during implant placement surgery,
- c)
- early placement and loading of implants and
- II)
-
Secondary outcome measures:
- a)
- implant mobility at the time of loading
- b)
- need for additional grafting at the time of implantation
- c)
- radiological assessment of implant integration and marginal bone integrity after loading.
Results
Two case studies are presented in this paper to highlight the bio-enhancement effect of PRF when used alongside SA in fresh extraction sites followed by the rehabilitation of the augmented sites with dental implants 8 weeks post-grafting. The objectives were to show, as a proof of concept, that when PRF is used in conjunction with SA, graft healing and consolidation could be enhanced to allow for earlier implant placement (e.g. at 8 weeks vs 24 weeks) and early implant loading ( e.g 6 weeks after implant placement in SA sites).
Case study 1
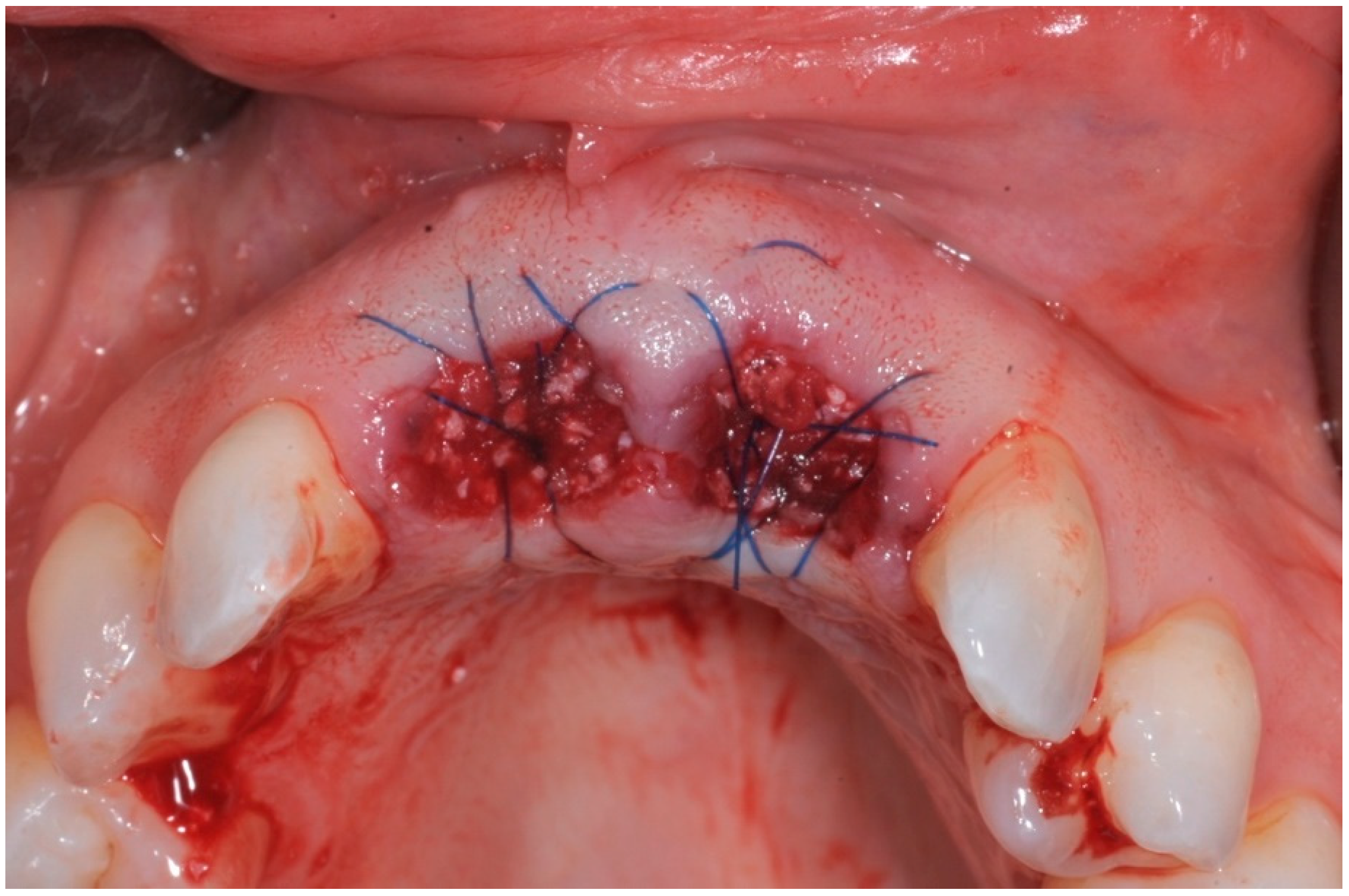
In this case study the first author has used SA technique in conjunction with PRF and a particulate xenograft (BioOss® Gesitlich) to enhance fresh extraction site healing prior to delayed implant placements after 8 weeks. A 40-year male generally fit and well and no smoking history presented complaining of the poor aesthetics associated with his anterior teeth. He gave a recurring history of infection from these teeth with the last episode being 6 months earlier. Clinically his oral hygiene was fair to poor with marginal plaque deposits and probing depths generally up to 4mm. The upper incisor teeth, however, had probing depths extending to the root end with grade 2/3 mobility and recession (Figure 4a,b). A diagnosis of chronic periodontitis with possible perio-endo lesions on the upper anterior teeth made. The prognosis of the teeth was poor and after a course of initial treatment, the extraction of the upper anterior teeth was planned with interim replacement using an Essix retainer. Due to the labial bone defect, the decision was made to extract the teeth and carry out SA using a xenograft (Bioss Geistlich®) mixed with i-PRF. The extraction defect was treated with a double layer of A-PRF fibrin matrix membrane which was sutured to the mucosa surrounding the edges of the extraction sockets (Figure 4c,d).
The four incisor teeth were extracted using the minimally invasive extraction technique as described in part 1 of this paper, and all granulation tissue removed. The extraction sockets were augmented using a xenograft (Bio-Oss®/ Geistlich Biomaterials) mixed with i-PRF (see Table 1). Two Megagen Anyridge® implants were subsequently placed and restored with a 4-unit bridge after successful control of the periodontal disease. Good incorporation of graft particles surrounded by newly formed bone was noted at the time of implant placement.
Figure 4.
Extraction sockets of periodontally involved upper incisor teeth which were augmented with a xenograft (BioOss ®, Geistlich Biomaterials) mixed with i-PRF and closed with double layer of A-PRF membrane using vicryl ® sutures.
Figure 4.
Extraction sockets of periodontally involved upper incisor teeth which were augmented with a xenograft (BioOss ®, Geistlich Biomaterials) mixed with i-PRF and closed with double layer of A-PRF membrane using vicryl ® sutures.
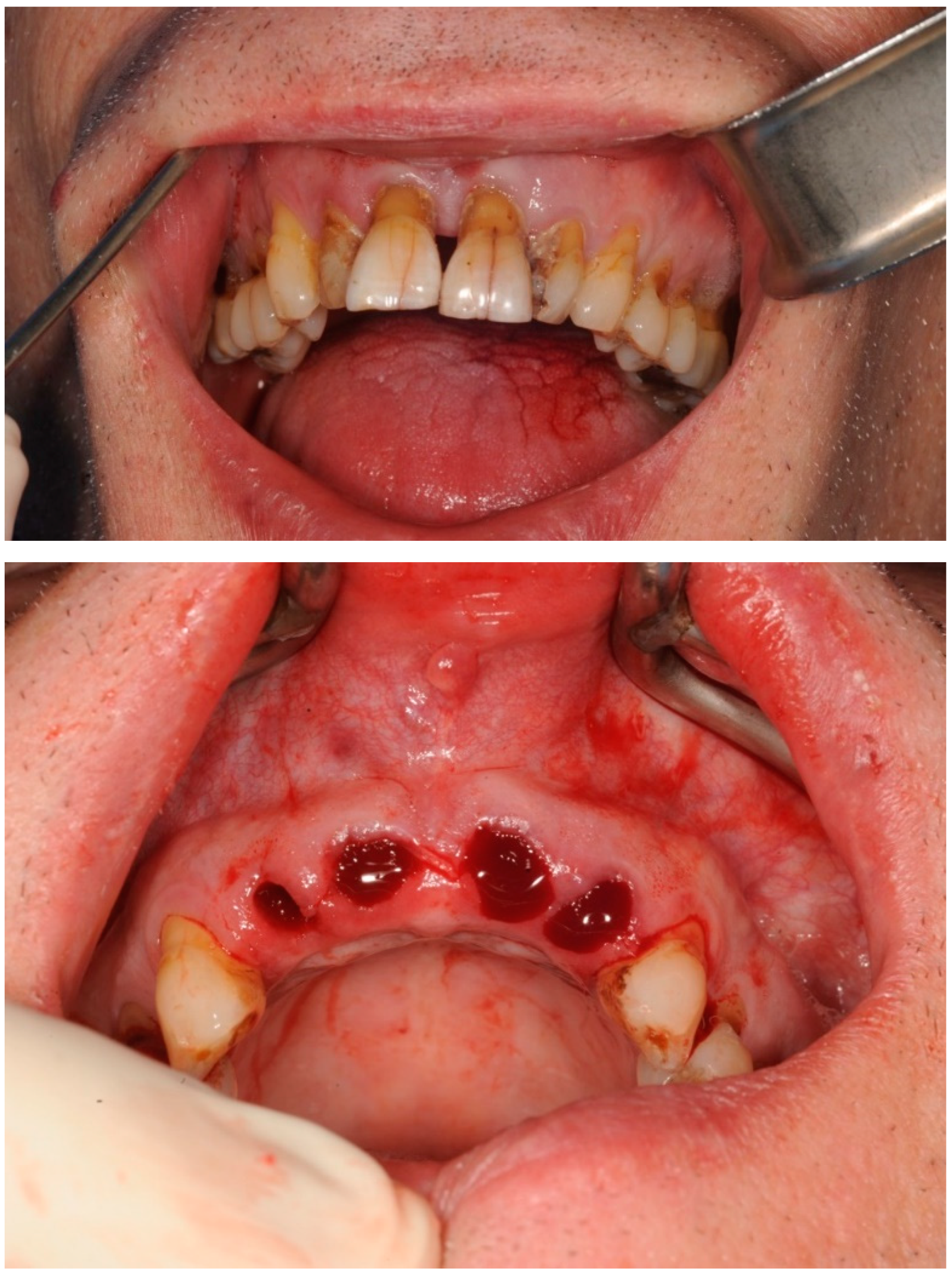
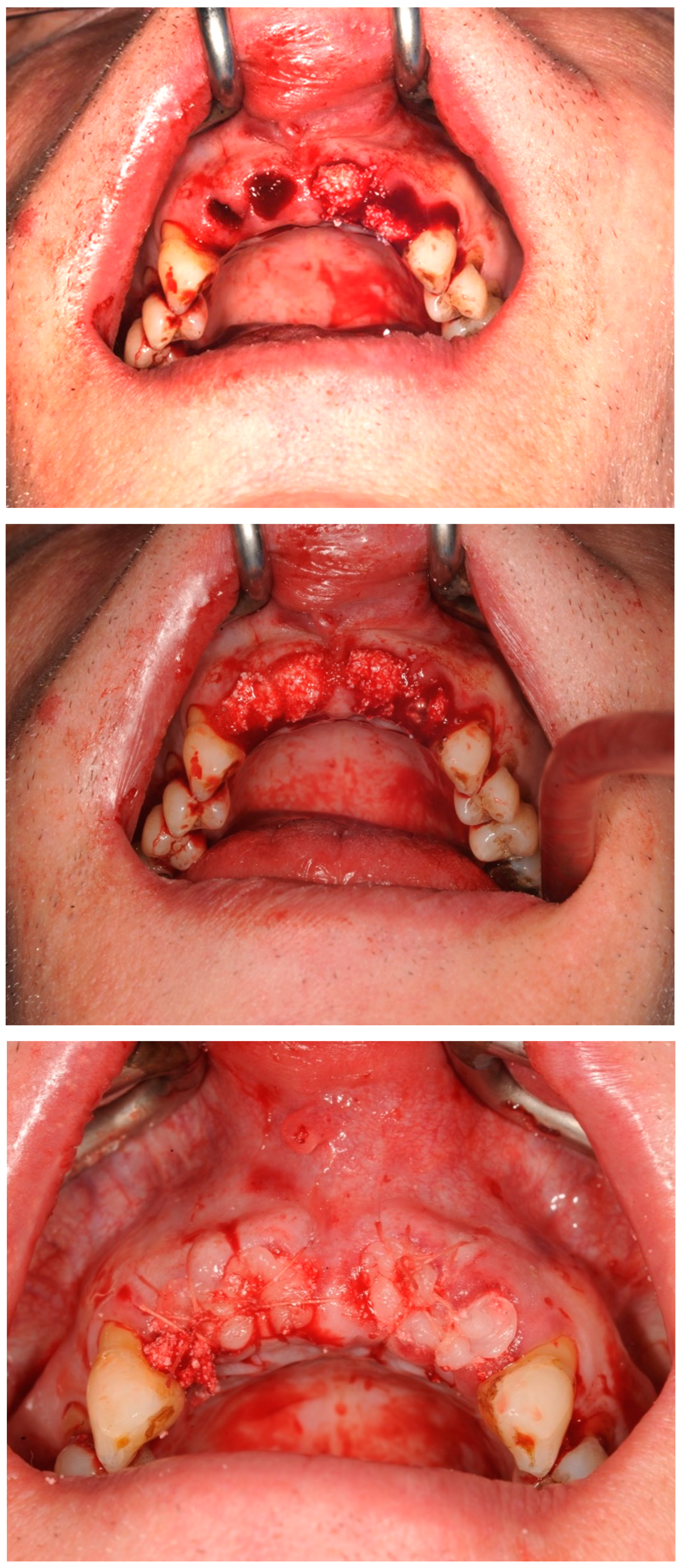
Figure 5a.
Radiographs showing socket augmentation dense radiopacity and contour preservation, 8 weeks after SA.
Figure 5a.
Radiographs showing socket augmentation dense radiopacity and contour preservation, 8 weeks after SA.
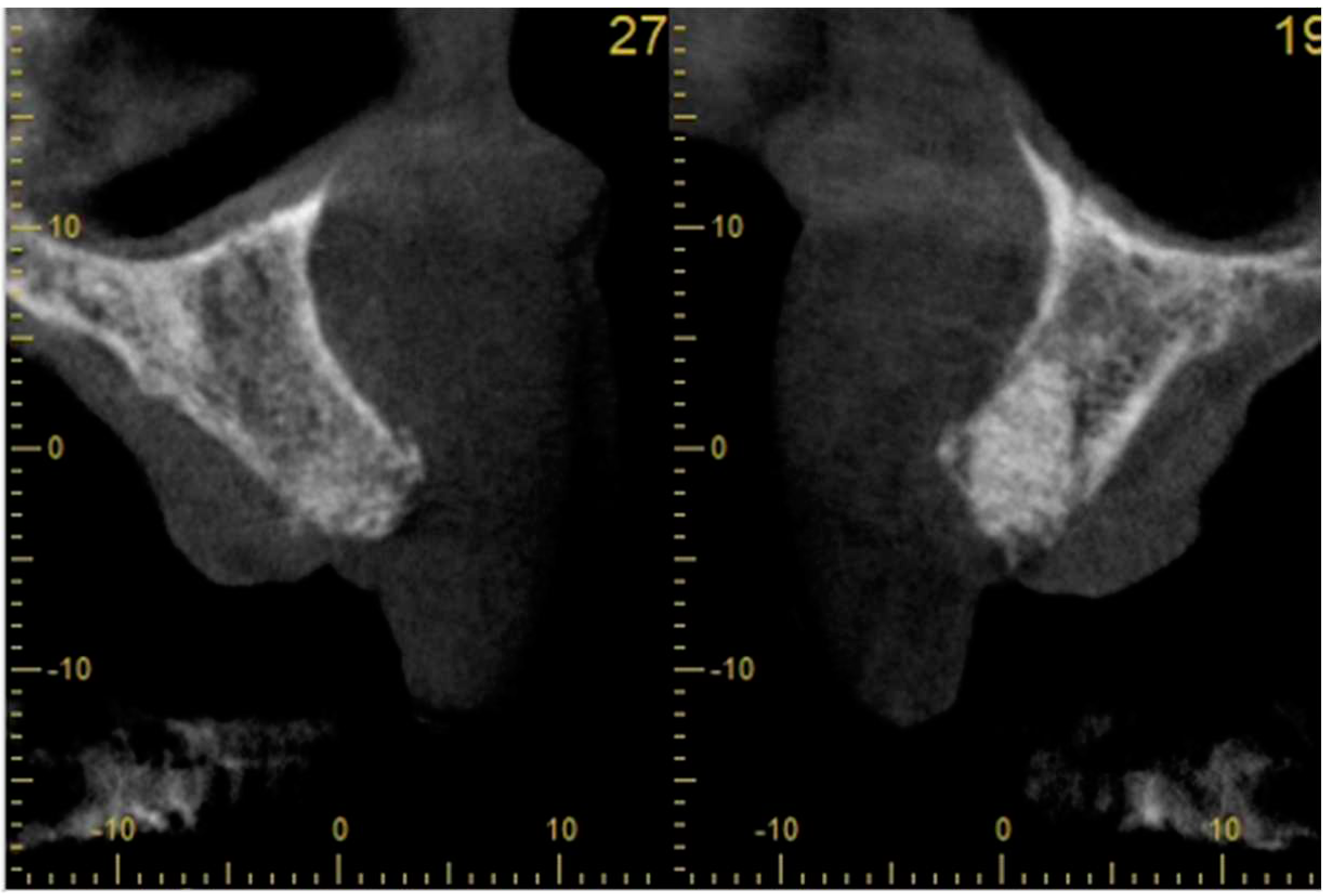
Figure 5b.
Control periapical radiograph shows the stability of marginal bone support around the two Megagen Anyridge® implants in function. Although the implant: crown ratio appears to be unfavourable in this radiograph, the internationally recognized restorative guidelines were used in selection of implant lengths.
Figure 5b.
Control periapical radiograph shows the stability of marginal bone support around the two Megagen Anyridge® implants in function. Although the implant: crown ratio appears to be unfavourable in this radiograph, the internationally recognized restorative guidelines were used in selection of implant lengths.
3.2. Case Study 2
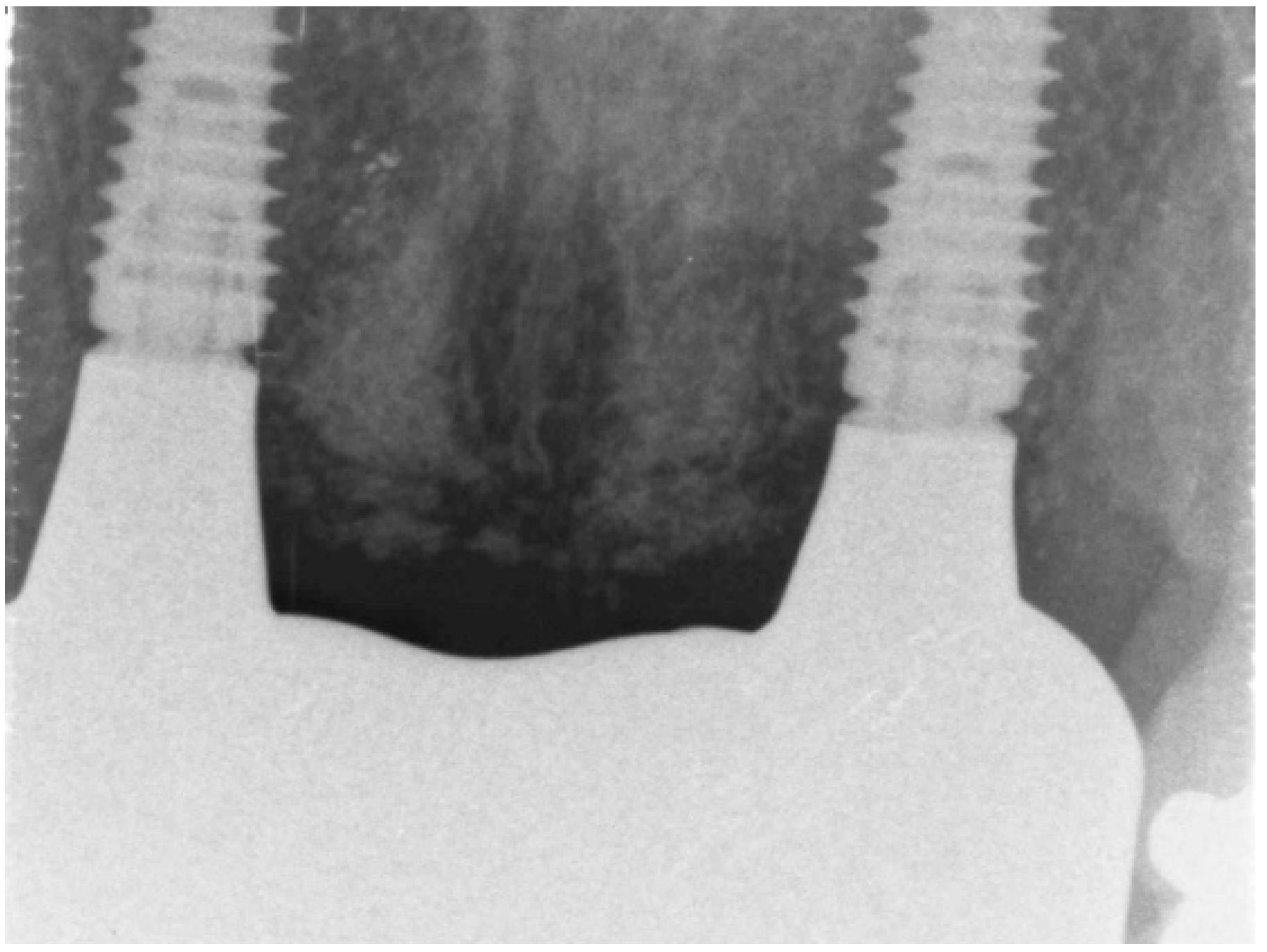
UR1 was removed with SA using BioOss® and A-PRF. Eight weeks post-SA, a CBCT scan revealed outstanding preservation of the alveolar bone shape with radiographically dense bone. A Megagen Anyridge® implant was inserted eight weeks post-SA. Before the implants were inserted, the implant bed was drenched with i-PRF solution using a one-time use syringe. A periapical X-ray indicated successful implant integration and preservation of the newly formed bone at the UR1 extraction site during a subsequent follow up see (Figure 6 and Figure 7 and Table 4).
Figure 6.
Extraction of UR1 and SA using BioOss ® and A-PRF. A CBCT was taken 8 weeks after SA showing excellent maintenance of alveolar bone contour with radiologically dense bone.
Figure 6.
Extraction of UR1 and SA using BioOss ® and A-PRF. A CBCT was taken 8 weeks after SA showing excellent maintenance of alveolar bone contour with radiologically dense bone.
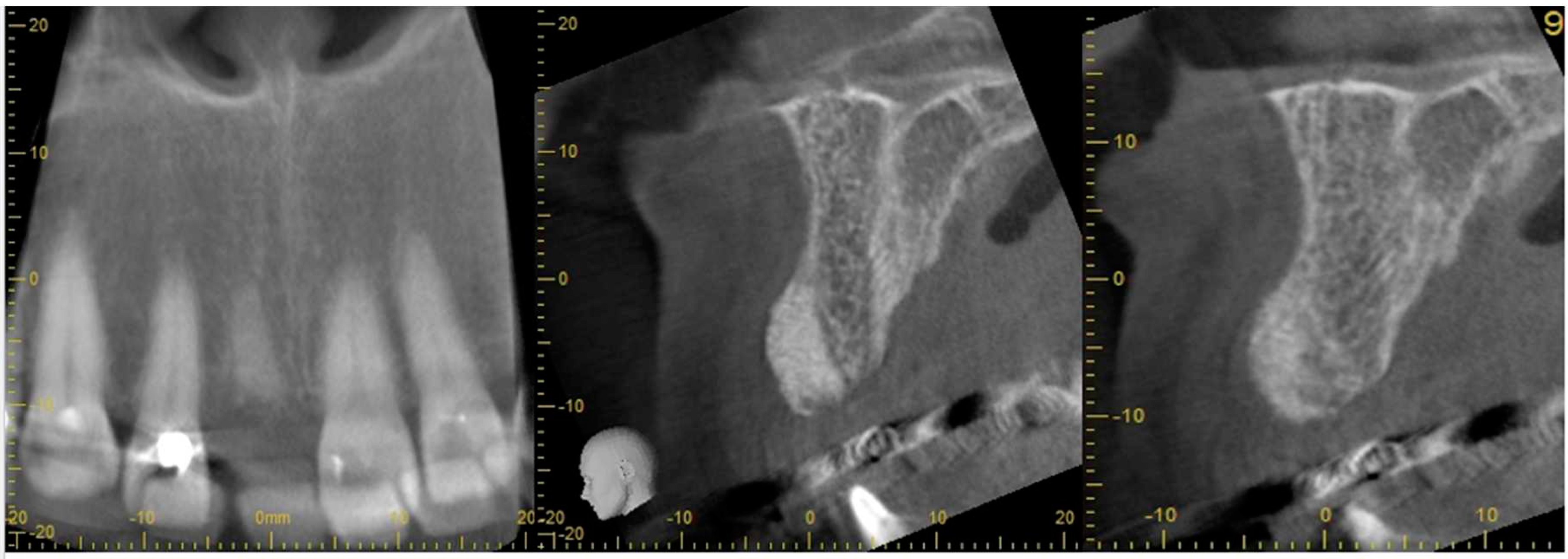
Figure 7.
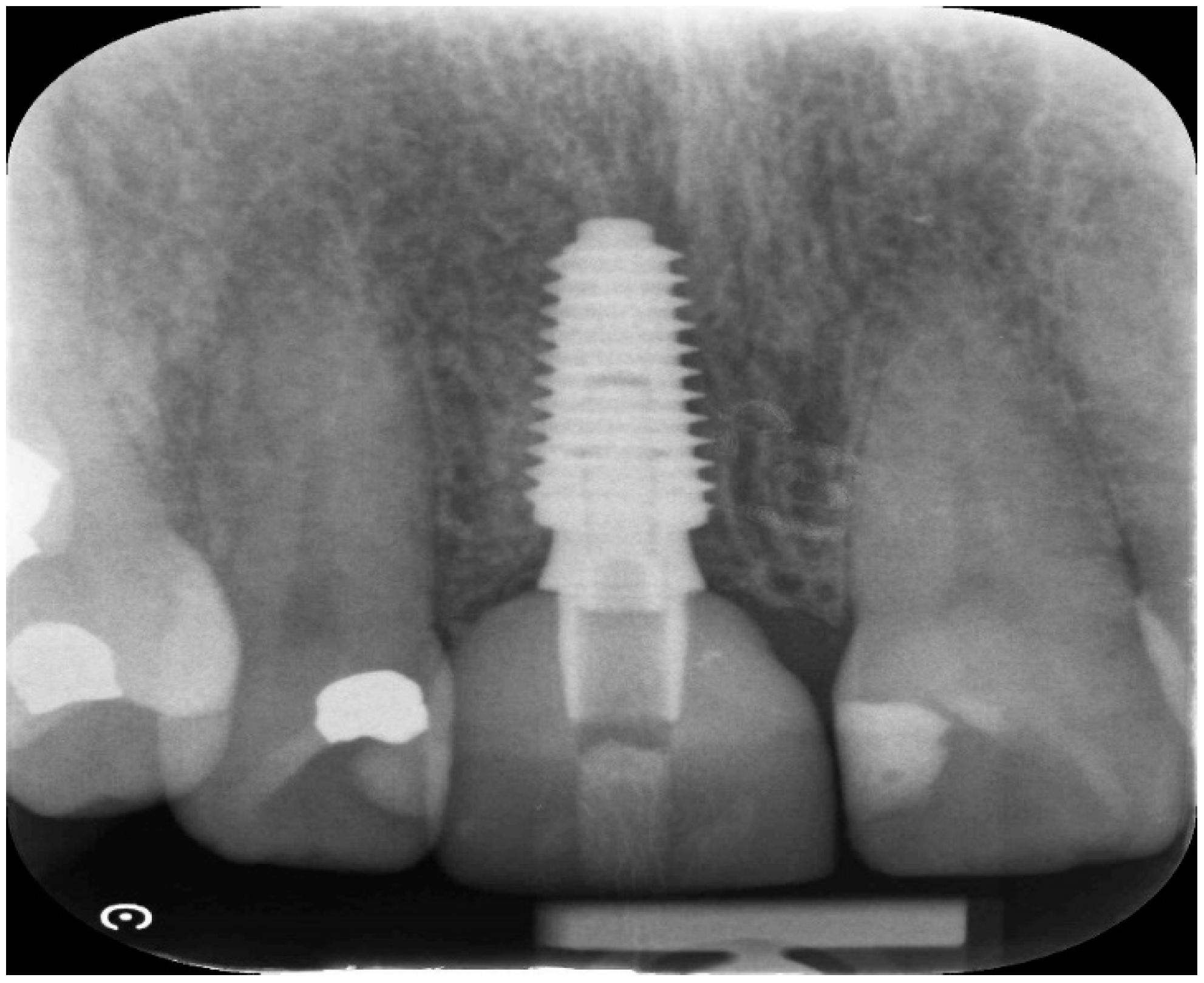
A Megagen Anyridge® implant was placed at 8 weeks after SA. Implant bed was soaked with i-PRF solution using a disposable syringe just prior to insertion of the implants. Periapical radiograph shows good implant integration and maintenance of the newly generated bone within the extraction site at UR1 at a follow up appointment.
Figure 7.
A Megagen Anyridge® implant was placed at 8 weeks after SA. Implant bed was soaked with i-PRF solution using a disposable syringe just prior to insertion of the implants. Periapical radiograph shows good implant integration and maintenance of the newly generated bone within the extraction site at UR1 at a follow up appointment.
The success of the two case studies presented in this paper were evaluated using specific primary and secondary outcome measures seen inable 4 summarises the results.
Table 4.
Outcomes of case studies presented in our study.
| Case No | Outcomes: | ||||||||
| Case No: | SA | BQn | BQ | PS | Surgery BQ | Secondary Grafting | Time since SA | Early Loading | CBS |
| Case 1 | open SA | Full contour | excellent | high | D2-3 | None | 8 weeks | 6 weeks | No crestal bone loss |
| Case 2 implant 1 | open SA | Full contour | excellent | high | D2-4 | None | 9 weeks | 7 weeks | No crestal bone loss |
| Case 2 implant 2 | open SA | Full contour | excellent | high | D2-5 | None | 10 weeks | 8 weeks | No crestal bone loss |
Table 4: SA: Socket Augmentation, BQn: Bone quality/ Full contour preservation, BQ: excellent/good/poor; PS: Primary Stability on implant placement High/medium/Low; Surgery BQ: bone density at surgery D1, D2, D3, D4; Secondary Grafting: Need for additional grafting at the time of implant placement; SA: Time since SA (weeks); Early Loading: Time since implant placement (weeks); CBS: Crestal bone stability.
4. Discussion
Socket augmentation is indicated to prevent dimensional changes occurring to an extraction socket and to facilitate staged implant placement at a later date. (The XV European Workshop in Periodontology (2019). SA is specifically indicated in case of thin gingival biotype or reduced extraction socket wall thickness of <2 mm in the aesthetic zone. SA is also highly indicated when the extraction socket morphology is not optimum for restoratively driven immediate implant placement with adequate primary stability. Several studies have reported better crest maintenance using graft materials in fresh extraction sites [43]. A randomized controlled trial conducted by Sisti et al (2012) showed radiographically near complete vertical and horizontal maintenance of the grafted volume with flapless socket augmentation (SA) [44]. They further showed that the application of particulate socket grafts without barrier membranes minimized alveolar crest resorption in large fresh extraction sites and resulted in better horizontal regeneration of the deficient buccal bone wall compared with non-grafted sites. Mardas et al (2015) concluded in a SR that SA procedures could decrease the need for further augmentation procedures during staged implant placement, at a later date, compared with unassisted socket healing [45]. Significantly, the success rate as well as the marginal bone levels of implants placed in alveolar ridges following SA were found to be comparable with that of implants placed in untreated sockets. A review of the rationale for SA with PRF was presented by the current authors Ucer et al [46]. The results of the current case studies are consistent with the findings of Sisti et al [44] and Marda et al [45].
The ideal graft material should be osteoinductive to induce new bone formation such as an autologous graft which is still the gold standard in bone reconstructive surgery. However, the use of autologous bone as a graft material in socket augmentation is not always practical as it has many disadvantages including a need for a donor site. The alternative biomaterials are typically osteoconductive which act as a space maintaining scaffold. These include allogeneic, xenogeneic, and synthetic derivatives. The main disadvantage of using scaffold biomaterials is their slow remodeling and graft consolidation time which delays the placement of implants after SA for several months. Biologically active molecules such as BMPs can be added to osteoconductive scaffolds to enhance new bone formation. In the two case studies presented in the current paper, implants have been placed within 8 weeks after SA in conjunction with second-generation PRF products (i-PRF). The implants were loaded after a reduced integration period of 6 weeks. Consistent with the studies mentioned above, the current results have demonstrated excellent alveolar bone preservation after tooth extractions and SA in the anterior maxilla. This allowed successful placement, integration, and early loading of implants in these cases. Furthermore, there was no need for secondary grafting at the time of implant placements 8 weeks after tooth removal when SA was used in conjunction with PRF. The initial implant and marginal bone stability were good with no detectable crestal bone loss during the first 6 months follow-up time. These results are consistent with reports in the current literature. Although, the optimum timing for implant placement after SA is currently not known, there is consensus that implant placement after SA should be deferred for a period of up to 6 months to allow slow incorporation of graft materials such as xenografts. This view was supported by a recent umbrella review of randomized controlled clinical trials, analyzing the outcomes of flapless socket grafting, which found less than 45% vital bone in SA grafted with xenografts and allografts after a healing period of 12 weeks [47,48].
As demonstrated by the current paper, use of PRF in conjunction with SA may allow earlier rehabilitation of patients due to enhanced healing and bone regeneration. There is emerging biological and clinical evidence to show that the second generation PRF products can provide a significant bio-enhancement effect when applied in conjunction with SA and as demonstrated in the current case studies this could help to reduce the overall duration of staged implant treatment after tooth extractions. Furthermore, coating implant surfaces (or soaking the implant bed) with liquid PRF could provide additional benefits on the osteointegration process when used in augmented or native implant sites [48]. This view that osseointegration could be enhanced by wetting the implants surface with PRF or placing a piece of PRF membrane in the osteotomy site is supported by laboratory and in vivo RCTs reported by Oncu and Alaaddinogluet al , Oncu, and Erbeyoglu et al and(Quirynen and Pinto, 2022 [11,49,50]. These researchers have demonstrated higher implant stability quotient values and significantly less bone loss due to post-implantation bone remodeling (Boora et al) when RCF was applied during implant placement. Nevertheless, currently there is a general lack of comparative RCTs to show the clinical significance of different preparations of PRF or the ideal timing of interventions during SA in conjunction with PRF. A review of the literature on this subject highlighted the differences at many levels in study methodologies as well as the lack of homogeneity of outcome measures (e.g. implant success/survival, marginal bone loss, implant stability) making it impossible to carry out a comprehensive analysis. Whilst current evidence and our clinical experience, as highlighted in current case studies, support the use of PRF in conjunction with a biomaterial (e.g. xenograft) to enhance healing during SA, further research is needed to demonstrate the optimum protocols and bio-enhancement properties of PRF when used in SA.
Conclusion
Two case studies presented in this paper have demonstrated that it may be possible to reduce the overall duration of implant treatment when PRF is used alongside SA. Furthermore, good primary stability was achieved and there was no need for secondary grafting when implants were placed 8 weeks after SA. Whilst there is strong biological evidence for the mode of action of PRF in oral wound healing, histomorphometric analysis of the newly formed tissues and standardized randomized clinical trials (RCT) with long-term follow-ups are urgently required to further substantiate the bio-enhancement role of PRF in socket augmentation. Alveolar bone atrophy after tooth extraction presents significant difficulties when planning delayed-immediate implant treatment to replace a lost tooth. Socket augmentation is an effective therapy that limits the post extraction volumetric changes and facilitates implant placement whilst reducing the need for staged grafting. However, socket augmentation and osteoconductive graft conversion is a slow process that could take 4-6 months. PRF has been shown to have important bio-active properties such as angiogenesis, cell proliferation, recruitment, and differentiation through release of growth factors mediated by platelets and leukocytes. When applied alongside SA, PRF may have a bio-enhancement role in socket graft healing and could help to reduce the overall duration of implant treatment after tooth loss.
Author Contributions
“Conceptualization, methodology, by CU, formal analysis, investigation, resources, data curation, writing—original draft preparation, writing—review and editing, supervision, project administration, funding acquisition, by CU and RK. All authors have read and agreed to the published version of the manuscript.
Funding
“This research received no external funding”.
Institutional Review Board Statement
“Not applicable”.
Informed Consent Statement
“Informed consent was obtained from all subjects involved in the study.”.
Data Availability Statement
“Not applicable”.
Acknowledgments
ICE dental hospital.
Conflicts of Interest
“The authors declare no conflict of interest.”.
References
- Yu, H. Y., & Chang, Y. C. (2022). A Bibliometric Analysis of Platelet-Rich Fibrin in Dentistry. International journal of environmental research and public health, 19(19), 12545. https://doi.org/10.3390/ijerph191912545. [CrossRef]
- Wang, X., Zhang, Y., Choukroun, J., Ghanaati, S., & Miron, R. J. (2018). Effects of an injectable platelet-rich fibrin on osteoblast behavior and bone tissue formation in comparison to platelet-rich plasma. Platelets, 29(1), 48–55. https://doi.org/10.1080/09537104.2017.1293807. [CrossRef]
- Pavlovic V, Ciric M, Jovanovic V, Trandafilovic M, Stojanovic P. Platelet-rich fibrin: Basics of biological actions and protocol modifications. Open Med (Wars). 2021 Mar 22;16(1):446-454. doi: 10.1515/med-2021-0259. PMID: 33778163; PMCID: PMC7985567. [CrossRef] [PubMed]
- Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85(6):638-646.
- ANITUA, E., TEJERO, R., ALKHRAISAT, M. H. & ORIVE, G. 2013. Platelet-rich plasma to improve the bio-functionality of biomaterials. BioDrugs, 27, 97-111.
- Miron, R. J., Zucchelli, G., Pikos, M. A., Salama, M., Lee, S., Guillemette, V., Fujioka-Kobayashi, M., Bishara, M., Zhang, Y., Wang, H. L., Chandad, F., Nacopoulos, C., Simonpieri, A., Aalam, A. A., Felice, P., Sammartino, G., Ghanaati, S., Hernandez, M. A., & Choukroun, J. (2017). Use of platelet-rich fibrin in regenerative dentistry: a systematic review. Clinical oral investigations, 21(6), 1913–1927. https://doi.org/10.1007/s00784-017-2133-z. [CrossRef]
- Choukroun, J., & Ghanaati, S. (2018). Reduction of relative centrifugation force within injectable platelet-rich-fibrin (PRF) concentrates advances patients’ own inflammatory cells, platelets and growth factors: the first introduction to the low speed centrifugation concept. European journal of trauma and emergency surgery : official publication of the European Trauma Society, 44(1), 87–95. https://doi.org/10.1007/s00068-017-0767-9. [CrossRef]
- Fujioka-Kobayashi, M., Miron, R. J., Hernandez, M., Kandalam, U., Zhang, Y., & Choukroun, J. (2017). Optimized Platelet-Rich Fibrin With the Low-Speed Concept: Growth Factor Release, Biocompatibility, and Cellular Response. Journal of periodontology, 88(1), 112–121. https://doi.org/10.1902/jop.2016.160443. [CrossRef]
- Miron, R. J., Fujioka-Kobayashi, M., Hernandez, M., Kandalam, U., Zhang, Y., Ghanaati, S., & Choukroun, J. (2017). Injectable platelet rich fibrin (i-PRF): opportunities in regenerative dentistry?. Clinical oral investigations, 21(8), 2619–2627. https://doi.org/10.1007/s00784-017-2063-9. [CrossRef]
- Miron, R. J., Chai, J., Zhang, P., Li, Y., Wang, Y., Mourão, C. F. A. B., Sculean, A., Fujioka Kobayashi, M., & Zhang, Y. (2020). A novel method for harvesting concentrated platelet-rich fibrin (C-PRF) with a 10-fold increase in platelet and leukocyte yields. Clinical oral investigations, 24(8), 2819–2828. https://doi.org/10.1007/s00784-019-03147-w. [CrossRef]
- Quirynen M, Pinto NR. Leukocyte-and Platelet-Rich Fibrin in Oral Regenerative Procedures: Evidence-Based Clinical Guidelines. Quintessenz Verlag; 2022 Jun 14.
- (adapted from https://www.sigmaaldrich.com/deepweb/assets/sigmaaldrich/marketing/global/documents/232/100/rpm-converted-to-g-force-mk.pdf last accessed 06 04 2023 ).
- Xuzhu Wang, Yufeng Zhang, Joseph Choukroun, Shahram Ghanaati & Richard J. Miron (2017): Effects of an injectable platelet-rich fibrin on osteoblast behavior and bone tissue formation in comparison to platelet-rich plasma, Platelets, DOI: 10.1080/09537104.2017.1293807. [CrossRef]
- Choukroun, J., & Ghanaati, S. (2018). Reduction of relative centrifugation force within injectable platelet-rich-fibrin (PRF) concentrates advances patients’ own inflammatory cells, platelets and growth factors: the first introduction to the low speed centrifugation concept. European journal of trauma and emergency surgery : official publication of the European Trauma Society, 44(1), 87–95. https://doi.org/10.1007/s00068-017-0767-9. [CrossRef]
- Fujioka-Kobayashi, M., Miron, R. J., Hernandez, M., Kandalam, U., Zhang, Y., & Choukroun, J. (2017). Optimized Platelet-Rich Fibrin With the Low-Speed Concept: Growth Factor Release, Biocompatibility, and Cellular Response. Journal of periodontology, 88(1), 112–121. https://doi.org/10.1902/jop.2016.160443. [CrossRef]
- Kobayashi E, Flückiger L, Fujioka-Kobayashi M, Sawada K, Sculean A, Schaller B, Miron RJ. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin Oral Investig. 2016 Dec;20(9):2353-2360. doi: 10.1007/s00784-016-1719-1. Epub 2016 Jan 25. PMID: 26809431. [CrossRef] [PubMed]
- Fujioka-Kobayashi M, Miron RJ, Hernandez M, Kandalam U, Zhang Y, Choukroun J. Optimized Platelet-Rich Fibrin With the Low-Speed Concept: Growth Factor Release, Biocompatibility, and Cellular Response. J Periodontol. 2017 Jan;88(1):112-121. doi: 10.1902/jop.2016.160443. Epub 2016 Sep 2. PMID: 27587367. [CrossRef] [PubMed]
- Miron RJ, Dham A, Dham U, Zhang Y, Pikos MA, Sculean A. The effect of age, gender, and time between blood draw and start of centrifugation on the size outcomes of platelet-rich fibrin (PRF) membranes. Clin Oral Investig. 2019 May;23(5):2179-2185. doi: 10.1007/s00784-018-2673-x. Epub 2018 Oct 2. PMID: 30280327. [CrossRef] [PubMed]
- Miron, R. J., Chai, J., Zheng, S., Feng, M., Sculean, A., & Zhang, Y. (2019). A novel method for evaluating and quantifying cell types in platelet rich fibrin and an introduction to horizontal centrifugation. Journal of biomedical materials research. Part A, 107(10), 2257–2271. https://doi.org/10.1002/jbm.a.36734. [CrossRef]
- Miron, R. J., Fujioka-Kobayashi, M., Hernandez, M., Kandalam, U., Zhang, Y., Ghanaati, S., & Choukroun, J. (2017). Injectable platelet rich fibrin (i-PRF): opportunities in regenerative dentistry?. Clinical oral investigations, 21(8), 2619–2627. https://doi.org/10.1007/s00784-017-2063-9. [CrossRef]
- Kobayashi, E., Flückiger, L., Fujioka-Kobayashi, M., Sawada, K., Sculean, A., Schaller, B., & Miron, R. J. (2016). Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clinical oral investigations, 20(9), 2353–2360. https://doi.org/10.1007/s00784-016-1719-1. [CrossRef]
- Miron, R. J., Chai, J., Zhang, P., Li, Y., Wang, Y., Mourão, C. F. A. B., Sculean, A., Fujioka Kobayashi, M., & Zhang, Y. (2020). A novel method for harvesting concentrated platelet-rich fibrin (C-PRF) with a 10-fold increase in platelet and leukocyte yields. Clinical oral investigations, 24(8), 2819–2828. https://doi.org/10.1007/s00784-019-03147-w. [CrossRef]
- Tunalı M, Özdemir H, Küçükodacı Z, Akman S, Yaprak E, Toker H, Fıratlı E. A novel platelet concentrate: titanium-prepared platelet-rich fibrin. Biomed Res Int. 2014;2014:209548. doi: 10.1155/2014/209548. Epub 2014 Jan 21. PMID: 24563860; PMCID: PMC3915853. [CrossRef] [PubMed]
- You JS, Kim SG, Oh JS, Kim JS. Effects of Platelet-Derived Material (Platelet-Rich Fibrin) on Bone Regeneration. Implant Dent. 2019 Jun;28(3):244-255. doi: 10.1097/ID.0000000000000877. PMID: 31124821. [CrossRef] [PubMed]
- Şimşek S, Özeç İ, Kürkçü M, Benlidayı E. Histomorphometric Evaluation of Bone Formation in Peri-Implant Defects Treated With Different Regeneration Techniques: An Experimental Study in a Rabbit Model. J Oral Maxillofac Surg. 2016 Sep;74(9):1757-64. doi: 10.1016/j.joms.2016.05.026. Epub 2016 Jun 7. PMID: 27351696. [CrossRef] [PubMed]
- Oliveira MR, deC Silva A, Ferreira S, Avelino CC, Garcia IR Jr, Mariano RC. Influence of the association between platelet-rich fibrin and bovine bone on bone regeneration. A histomorphometric study in the calvaria of rats. Int J Oral Maxillofac Surg. 2015 May;44(5):649-55. doi: 10.1016/j.ijom.2014.12.005. Epub 2014 Dec 30. PMID: 25553712. [CrossRef] [PubMed]
- Miron, R. J., Zucchelli, G., Pikos, M. A., Salama, M., Lee, S., Guillemette, V., Fujioka-Kobayashi, M., Bishara, M., Zhang, Y., Wang, H. L., Chandad, F., Nacopoulos, C., Simonpieri, A., Aalam, A. A., Felice, P., Sammartino, G., Ghanaati, S., Hernandez, M. A., & Choukroun, J. (2017). Use of platelet-rich fibrin in regenerative dentistry: a systematic review. Clinical oral investigations, 21(6), 1913–1927. https://doi.org/10.1007/s00784-017-2133-z. [CrossRef]
- Phuong Tran TT, Vu Pham TA. Effect of advanced and injectable platelet-rich fibrins against Aggregatibacter actinomycetemcomitans in subjects with or without periodontal diseases. J Dent Sci. 2023 Apr;18(2):491-496. doi: 10.1016/j.jds.2022.09.014. Epub 2022 Oct 6. PMID: 37021261; PMCID: PMC10068356. [CrossRef] [PubMed]
- Zwittnig, K., Kirnbauer, B., Jakse, N., Schlenke, P., Mischak, I., Ghanaati, S., Al-Maawi, S., Végh, D., Payer, M., & Zrnc, T. A. (2022). Growth Factor Release within Liquid and Solid PRF. Journal of clinical medicine, 11(17), 5070. https://doi.org/10.3390/jcm11175070. [CrossRef]
- ANITUA, E., TEJERO, R., ALKHRAISAT, M. H. & ORIVE, G. 2013. Platelet-rich plasma to improve the bio-functionality of biomaterials. BioDrugs, 27, 97-111.
- Sammartino, G., Dohan Ehrenfest, D. M., Carile, F., Tia, M., & Bucci, P. (2011). Prevention of hemorrhagic complications after dental extractions into open heart surgery patients under anticoagulant therapy: the use of leukocyte- and platelet-rich fibrin. The Journal of oral implantology, 37(6), 681–690. https://doi.org/10.1563/AAID-JOI-D-11-00001. [CrossRef]
- Yuan, S., Li, Q., Chen, K. et al. Ridge preservation applying a novel hydrogel for early angiogenesis and osteogenesis evaluation: an experimental study in canine. J Biol Eng 15, 19 (2021). https://doi.org/10.1186/s13036-021-00271-8. [CrossRef]
- Temmerman, A., Vandessel, J., Castro, A., Jacobs, R., Teughels, W., Pinto, N., & Quirynen, M. (2016). The use of leucocyte and platelet-rich fibrin in socket management and ridge preservation: a split-mouth, randomized, controlled clinical trial. Journal of clinical periodontology, 43(11), 990–999. https://doi.org/10.1111/jcpe.12612. [CrossRef]
- Chenchev IL, Ivanova VV, Neychev DZ, Cholakova RB. Application of Platelet-Rich Fibrin and Injectable Platelet-Rich Fibrin in Combination of Bone Substitute Material for Alveolar Ridge Augmentation - a Case Report. Folia Med (Plovdiv). 2017 Sep 1;59(3):362-366. doi: 10.1515/folmed-2017-0044. PMID: 28976904. [CrossRef] [PubMed]
- Anitua E, Murias-Freijo A, Alkhraisat MH, Orive G. Clinical, radiographical, and histological outcomes of plasma rich in growth factors in extraction socket: a randomized controlled clinical trial. Clin Oral Investig. 2015 Apr;19(3):589-600. doi: 10.1007/s00784-014-1278-2. Epub 2014 Jul 8. PMID: 24998770. [CrossRef] [PubMed]
- Chappuis, V., Engel, O., Reyes, M., Shahim, K., Nolte, L. P., & Buser, D. (2013). Ridge alterations post-extraction in the esthetic zone: a 3D analysis with CBCT. Journal of dental research, 92(12 Suppl), 195S–201S. https://doi.org/10.1177/0022034513506713. [CrossRef]
- Castro, A. B., Van Dessel, J., Temmerman, A., Jacobs, R., & Quirynen, M. (2021). Effect of different platelet-rich fibrin matrices for ridge preservation in multiple tooth extractions: A split-mouth randomized controlled clinical trial. Journal of clinical periodontology, 48(7), 984–995. https://doi.org/10.1111/jcpe.13463. [CrossRef]
- Wu CL, Lee SS, Tsai CH, Lu KH, Zhao JH, Chang YC. Platelet-rich fibrin increases cell attachment, proliferation and collagen-related protein expression of human osteoblasts. Aust Dent J. 2012 Jun;57(2):207-12. doi: 10.1111/j.1834-7819.2012.01686.x. PMID: 22624763. [CrossRef] [PubMed]
- Al-Maawi, S., Becker, K., Schwarz, F., Sader, R., & Ghanaati, S. (2021). Efficacy of platelet-rich fibrin in promoting the healing of extraction sockets: a systematic review. International journal of implant dentistry, 7(1), 117. https://doi.org/10.1186/s40729-021-00393-0. [CrossRef]
- Clark D, Rajendran Y, Paydar S, Ho S, Cox D, Ryder M, Dollard J, Kao RT. Advanced platelet-rich fibrin and freeze-dried bone allograft for ridge preservation: A randomized controlled clinical trial. J Periodontol. 2018 Apr;89(4):379-387. doi: 10.1002/JPER.17-0466. PMID: 29683498; PMCID: PMC6483085. [CrossRef] [PubMed]
- Yu, H. Y., & Chang, Y. C. (2022). A Bibliometric Analysis of Platelet-Rich Fibrin in Dentistry. International journal of environmental research and public health, 19(19), 12545. https://doi.org/10.3390/ijerph191912545. [CrossRef]
- Bennardo, F., Gallelli, L., Palleria, C. et al. Can platelet-rich fibrin act as a natural carrier for antibiotics delivery? A proof-of-concept study for oral surgical procedures. BMC Oral Health 23, 134 (2023). https://doi.org/10.1186/s12903-023-02814-5. [CrossRef]
- Hauser F, Gaydarov N, Badoud I, Vazquez L, Bernard JP, Ammann P. Clinical and histological evaluation of postextraction platelet-rich fibrin socket filling: a prospective randomized controlled study. Implant Dent. 2013 Jun;22(3):295-303. doi: 10.1097/ID.0b013e3182906eb3. PMID: 23644909. [CrossRef] [PubMed]
- Sisti A, Canullo L, Mottola MP, Covani U, Barone A, Botticelli D. Clinical evaluation of a ridge augmentation procedure for the severely resorbed alveolar socket: multicenter randomized controlled trial, preliminary results. Clin Oral Implants Res. 2012 May;23(5):526-35. doi: 10.1111/j.1600-0501.2011.02386.x. Epub 2011 Dec 8. PMID: 22150876. [CrossRef] [PubMed]
- Mardas N, Trullenque-Eriksson A, MacBeth N, Petrie A, Donos N. Does ridge preservation following tooth extraction improve implant treatment outcomes: a systematic review: Group 4: Therapeutic concepts & methods. Clin Oral Implants Res. 2015 Sep;26 Suppl 11:180-201. doi: 10.1111/clr.12639. Epub 2015 Jun 16. PMID: 26078004. [CrossRef] [PubMed]
- Ucer, C.; Khan, R.S. Extraction Socket Augmentation with Autologous Platelet-Rich Fibrin (PRF): The Rationale for Socket Augmentation. Dent. J. 2023, 11, 196. https://doi.org/10.3390/dj11080196. [CrossRef]
- Chenchev IL, Ivanova VV, Neychev DZ, Cholakova RB. Application of Platelet-Rich Fibrin and Injectable Platelet-Rich Fibrin in Combination of Bone Substitute Material for Alveolar Ridge Augmentation - a Case Report. Folia Med (Plovdiv). 2017 Sep 1;59(3):362-366. doi: 10.1515/folmed-2017-0044. PMID: 28976904. [CrossRef] [PubMed]
- Temmerman A, Vandessel J, Castro A, Jacobs R, Teughels W, Pinto N, Quirynen M. The use of leucocyte and platelet-rich fibrin in socket management and ridge preservation: a split-mouth, randomized, controlled clinical trial. J Clin Periodontol. 2016 Nov;43(11):990-999. doi: 10.1111/jcpe.12612. Epub 2016 Sep 21. PMID: 27509214. [CrossRef] [PubMed]
- Öncü E, Alaaddinoğlu EE. The effect of platelet-rich fibrin on implant stability. Int J Oral Maxillofac Implants. 2015 May-Jun;30(3):578-82. doi: 10.11607/jomi.3897. PMID: 26009908. [CrossRef] [PubMed]
- Öncü E, Erbeyoğlu AA. Enhancement of Immediate Implant Stability and Recovery Using Platelet-Rich Fibrin. Int J Periodontics Restorative Dent. 2019 March/April;39(2):e58–e63. doi: 10.11607/prd.2505. Epub 2017 Feb 14. PMID: 28196154. [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



