Submitted:
04 September 2023
Posted:
07 September 2023
You are already at the latest version
Abstract
Spondyloptosis is a condition where there is complete dislocation of L5 over sacrum. It is a form of spinal dislocation in which one spinal segment is lodged in the anterior or posterior space of another or advanced spondylolisthesis [1]. Treatment is usually spinal fusion depending on the level of lesion [2]. This clinical case is of a 15 year old male with a history of fall from auto-rickshaw followed by a blunt trauma from a heavy iron rod falling over his abdomen. There was no history of loss of consciousness, but the patient had an excruciating pain over back immediately after the incident. Patient is now paraplegic with loss of sensation below L5 along with loss bladder and bowel control since the time of injury. The T1 weighted MRI of spine revealed grade 5 anterior lysthesis of L5 over S1 level with complete spinal cord transaction. The patient was operated to restore the vertebral alignment with pedicle screws and rods. After 3 months, patient is now treated for neuro-musculoskeletal , genitourinary and genitointestinal function with biofeedback, pelvic floor exercises and timed voiding [3]. When a patient has issues with urine retention, Valsalva manoeuvres, Crede's method, suprapubic tapping, and anal stretching are employed to help them void more effortlessly [4].
Keywords:
Spondyloptosis
; Neurogenic bladder and bowel
; Physiotherapy
; SCI
; bladder training
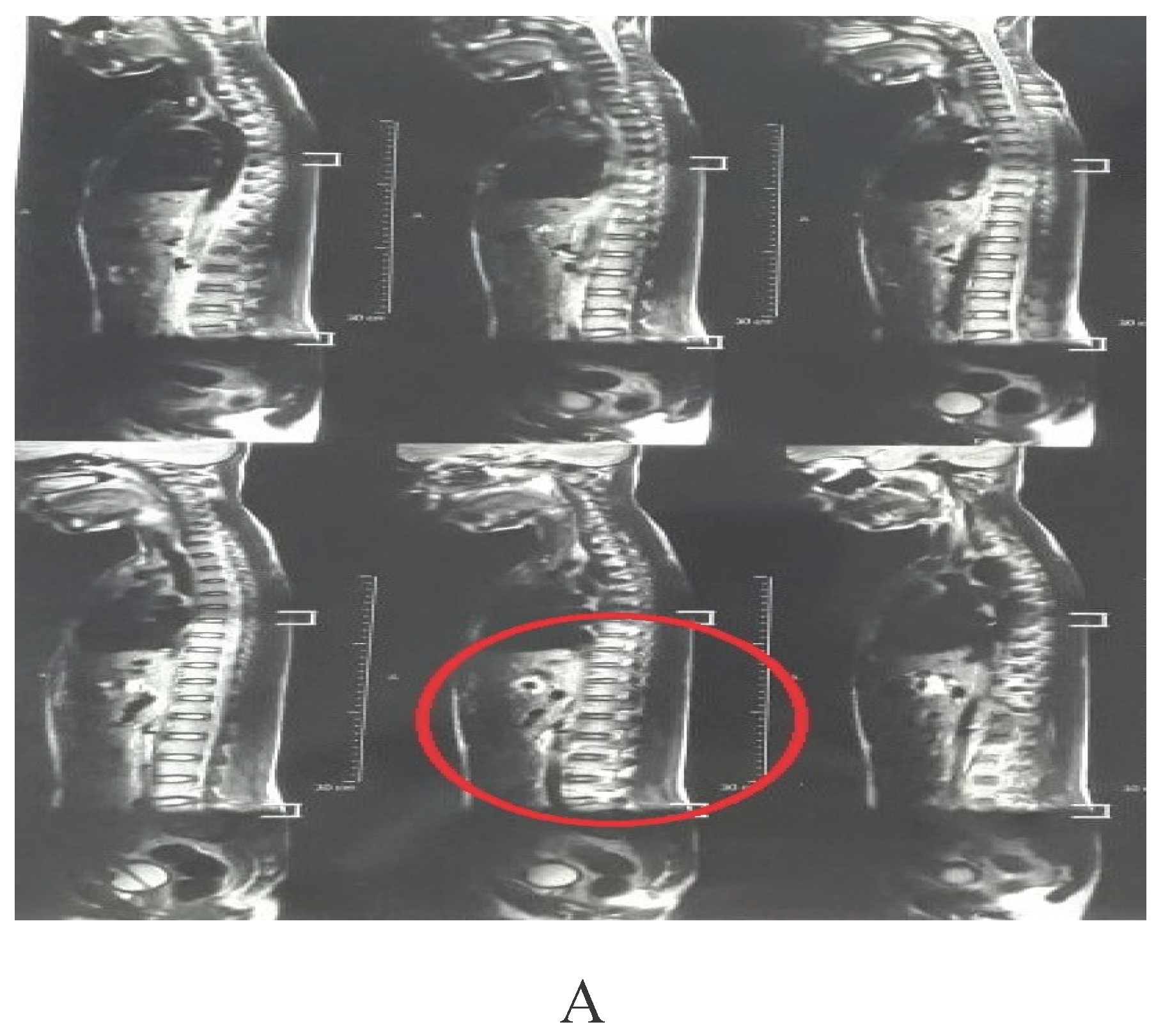
Figure 1.
weighted MRI of the Spine showing flattening of the dorso-lumbar spine. B T1 weighted MRI spine showing the Spondyloptosis of L5- S1 vertebra with cauda equine compression. According to Meyerding classification it comes under grade 5 i.e. >100% forward slip [5]. Cauda equine syndrome is a condition in which the lower segment of the spinal cord is compressed causing bladder and bowel dysfunction also sexual dysfunction. This patient experiences incontinence of bladder and bowel, also patient feels the filling of the bladder and bowel but there is loss of urge to void the urine and stool [6,7]. C- Showing the post-operative X-ray of Spinal fusion with rods and pedicle screws A-P view Surgical treatment is the only for traumatic spondyloptosis is reasonable. Surgery aims to reduce, decompress, stabilize, and fuse the spondyloptotic segment [8]. In this patient a posterior approach with decompression is used to re-align the vertebral segments and to maintain the integrity of the spinal cord. There is fixation of L5- S1 with pedicle screws and rods.
Figure 1.
weighted MRI of the Spine showing flattening of the dorso-lumbar spine. B T1 weighted MRI spine showing the Spondyloptosis of L5- S1 vertebra with cauda equine compression. According to Meyerding classification it comes under grade 5 i.e. >100% forward slip [5]. Cauda equine syndrome is a condition in which the lower segment of the spinal cord is compressed causing bladder and bowel dysfunction also sexual dysfunction. This patient experiences incontinence of bladder and bowel, also patient feels the filling of the bladder and bowel but there is loss of urge to void the urine and stool [6,7]. C- Showing the post-operative X-ray of Spinal fusion with rods and pedicle screws A-P view Surgical treatment is the only for traumatic spondyloptosis is reasonable. Surgery aims to reduce, decompress, stabilize, and fuse the spondyloptotic segment [8]. In this patient a posterior approach with decompression is used to re-align the vertebral segments and to maintain the integrity of the spinal cord. There is fixation of L5- S1 with pedicle screws and rods.

Author Contributions
Conceptualization, writing—original draft preparation by Swadha P. Udhoji writing review and editing by Raghuveer Raghumahanti. The author has read and agreed to the published version of the manuscript.
Funding
The present research received no external funding.
Institutional Review Board Statement
Not Applicable.
Informed Consent Statement
Informed consent was taken from the patient’s parent
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chandrashekhara, S.H.; Kumar, A.; Gamanagatti, S.; Kapoor, K.; Mukund, A.; Aggarwal, D.; Sinha, S. Unusual Traumatic Spondyloptosis Causing Complete Transaction of Spinal Cord. Int. Orthop. 2011, 35, 1671–1675. [CrossRef]
- Gaines, R.W. L5 Vertebrectomy for the Surgical Treatment of Spondyloptosis: Thirty Cases in 25 Years. Spine 2005, 30, S66–S70.
- Benevento, B.T.; Sipski, M.L. Neurogenic Bladder, Neurogenic Bowel, and Sexual Dysfunction in People with Spinal Cord Injury. Phys. Ther. 2002, 82, 601–612. [CrossRef]
- Park, Y.I.; Linsenmeyer, T.A. A Method to Minimize Indwelling Catheter Calcification and Bladder Stones in Individuals with Spinal Cord Injury. J. Spinal Cord Med. 2001, 24, 105–108. [CrossRef]
- Studnicka, K.; Ampat, G. Lumbosacral Spondylolisthesis. In StatPearls [Internet]; StatPearls Publishing, 2023.
- Fraser, S.; Roberts, L.; Murphy, E. Cauda Equina Syndrome: A Literature Review of Its Definition and Clinical Presentation. Arch. Phys. Med. Rehabil. 2009, 90, 1964–1968. [CrossRef]
- Lavy, C.; Marks, P.; Dangas, K.; Todd, N. Cauda Equina Syndrome—a Practical Guide to Definition and Classification. Int. Orthop. 2022, 1–5. [CrossRef]
- Daniels, A.H.; Deodhar, A.A.; Hart, R.A. Traumatic Spondyloptosis Resulting from High-Energy Trauma Concurrent with a Tonic-Clonic Seizure. Spine J. 2009, 9, e1–e4. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



