Submitted:
06 September 2023
Posted:
08 September 2023
You are already at the latest version
Abstract
In the last decade, an increasing awareness was directed to the role of Vitamin D in non-skeletal and preventive roles for chronic diseases. Vitamin D is a key hormone involved in the regulation of calcium/phosphorous balance and it has been implicated in the pathogenesis of inflammation, insulin resistance and obesity. Cholecalciferol (Vitamin D3) and Ergocalciferol (Vitamin D2) are the main form of vitamin D: the active form (1,25-dihydroxyvitamin D) is the result of two hydroxylations that take place in liver, kidney, pancreas and immune cells. Some anti-inflammatory cytokines are produced at higher levels by vitamin D, while some pro-inflammatory cytokines are released at lower levels. Toll-Like Receptor (TLR) expression is increased and a pro-inflammatory state is also linked to low levels of vitamin D. Regardless of how it affects inflammation, various pathways suggest that vitamin D directly improves insulin sensitivity and secretion. The level of vitamin D in the body may change the ratio of pro- to anti-inflammatory cytokines, which would impact insulin action, lipid metabolism, and the development and function of adipose tissue. Many studies have demonstrated an inverse relationship between vitamin D concentrations and pro-inflammatory markers, insulin resistance, glucose intolerance, metabolic syndrome, obesity and cardiovascular disease. It's interesting to note that several long-term studies also revealed an inverse correlation between vitamin D level and the occurrence of diabetes mellitus. Vitamin D supplementation in people has controversial effects, in fact while some studies demonstrated improvements in insulin sensitivity, glucose and lipid metabolism, others revealed no significant effect on glycemic control and inflammation. The aim of this review is to provide insight into the molecular basis of the relationship between vitamin D, insulin-resistance, metabolic syndrome, type 1 and 2 diabetes, gestational diabetes, and cardiovascular diseases.
Keywords:
vitamin D
; insulin-resistance
; metabolic syndrome
; type 1 and 2 diabetes
; gestational diabetes
; cardiovascular diseases and metabolism
INTRODUCTION
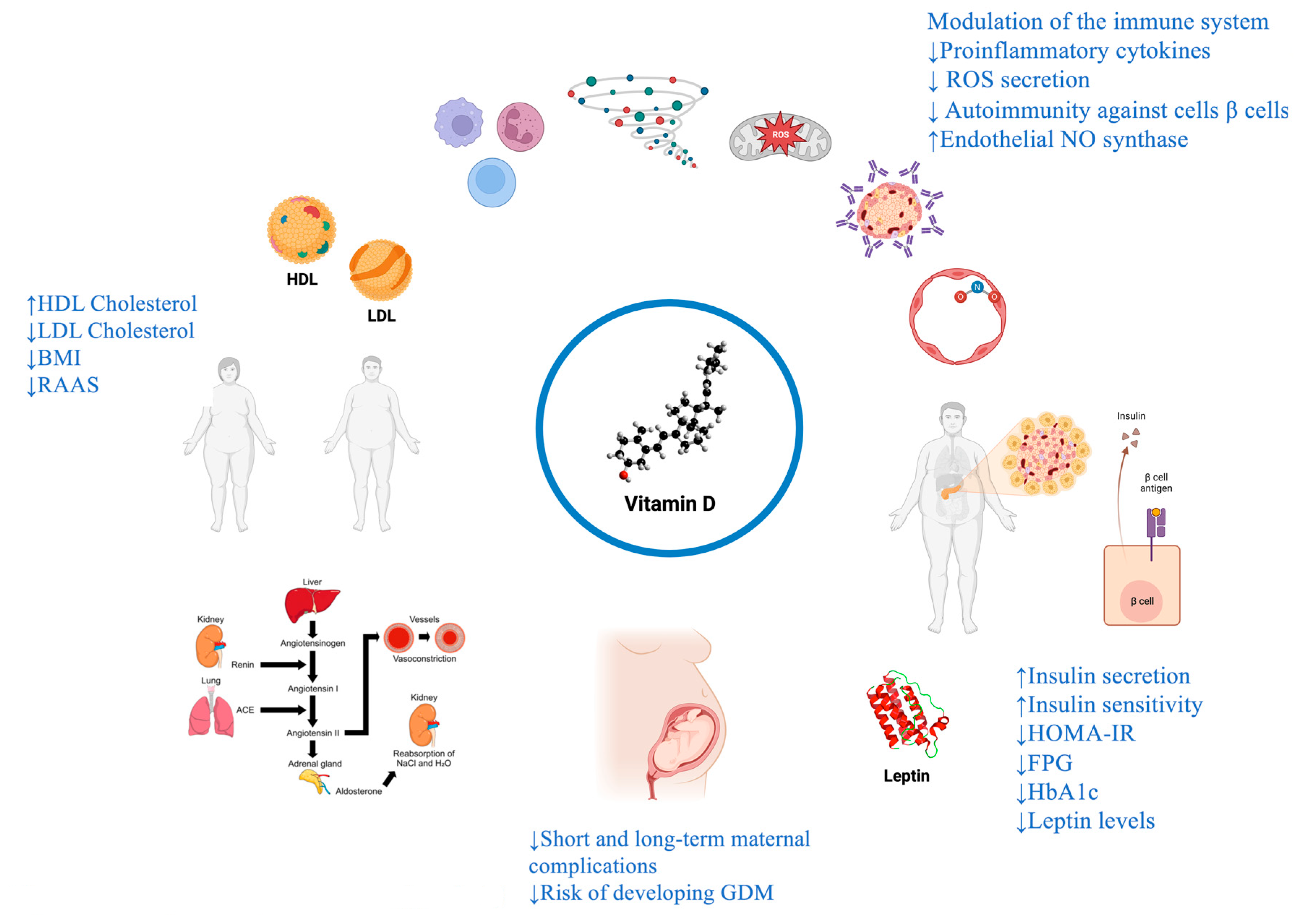
In recent years, the attention to the role of vitamin D in different fields is growing. Vitamin D is a liposoluble prohormone with endocrine, autocrine, and paracrine functions and is fundamental to bone metabolism [1]. Vitamin D has a role in extra-skeletal functions; consequentially, there is a relationship between vitamin D deficiency and some pathologic conditions, including diabetes, metabolic syndrome, non-alcoholic liver disease, autoimmune diseases, hypertension, cardiovascular disease and cancer [2,3,4,5,6,7,8,9] (Figure 1). Moreover, the recent pandemic of COVID-19 has underlined the possible therapeutic role of Vitamin D in some aspects of the infection and the association between severe vitamin D deficiency and COVID-19-related health outcomes [10,11,12]. Many studies have reported the existence of immuno-modulatory effects of vitamin D and that its deficiency may be associated with a sub-inflammatory state [13]. Diabetes and metabolic syndrome represent a major clinical and public health problem. The disease burden related to diabetes and metabolic syndrome is increasing significantly, particularly in older subjects [14,15]. According to the International Diabetes Federation, data released in 2021 showed that 537 million adults live with diabetes worldwide. The total number is predicted to rise to 643 million by 2030 and to 783 million by 2045, instead of the previous estimation of 693 million [16]. Many epidemiological and observational studies have found an association between vitamin D insufficiency and the incidence of type 1 and type 2 Diabetes [17,18,19,20,21]. In this sense, many studies reported the existence of different mechanisms able to explain the potential role of vitamin D in glucose metabolism, such as preservation of the β-cell function and slow failure of residual β-cell function in patients with type 1 diabetes and latent autoimmune diabetes [22,23]. Furthermore, vitamin D determines direct stimulation of insulin secretion and improves peripheral insulin resistance by reducing systemic inflammation through the vitamin D receptor on pancreatic beta cells and in muscles and liver [24,25,26]. This last mechanism also plays a key role in metabolic syndrome development [27]. The lack of vitamin D receptors in cardiovascular tissue increased ventricular mass dysregulation of metalloproteinases and fibroblasts, promoting the fibrotic process and ventricular dilatation [28].
Given this background, an extensive search of SCOPUS, PubMed, and CENTRAL was performed using the following string ((vitamin d) OR (calcifediol)) OR (ergocholecalciferol)) AND (systematic review [pt] OR meta-analysis [pt]) AND 2017:2023 [dp]). This review aims to explore the molecular basis of the role of vitamin D in insulin resistance, type 1 and 2 diabetes, gestational diabetes, metabolic syndrome and cardiovascular disease.
Figure 1.
the pleiotropic effect of vitamin D.
1. VITAMIN D METABOLISM
Vitamin D is a liposoluble prohormone that humans can acquire through nutrition and by synthesis in the skin during exposure to UV radiation [29]. Vitamin D3 (Cholecalciferol) is the main source of vitamin D, and vitamin D2 (Ergocalciferol) are the forms through which vitamin D exists.
Most of the amount of Cholecalciferol comes from the endogenous production in the skin after sun exposure; a small amount of Cholecalciferol has an exogenous origin and derives from foods. Ergocalciferol is contained in dairy products and nutritional supplements and is the vegetal form of vitamin D [30].
Once in the circulation, Cholecalciferol and Ergocalciferol are converted in liver tissue by the action of vitamin D-25-hydroxylase (CYP2R1) to 25-hydroxyvitamin D or calcifediol [25 (OH) D]; subsequently, 25(OH)D undergoes a second conversion, by the enzyme 25-hydroxyvitamin D-1α-hydroxylase (CYP27B1), into active and bioavailable vitamin D (1,25-dihydroxyvitamin or calcitriol - CT) [1,25 (OH)2 D] [31,32,33]. This reaction takes place mainly in the kidney. At that point, 1,25 (OH)2 D performs its functions by binding to the vitamin D receptor (VDR), expressed in the cytoplasm of cells, forming a VDR-RXR-hormone complex (vitamin D receptor - retinoid X receptor) through the stimulation of the heterodimerization of the VDR with the retinoid X receptor [15]. In the nucleus, it regulates the expression of many genes through their up or downregulation [32]. 1,25 (OH)2 D has about 1000-fold higher affinity than 25(OH) for the VDR. CYP27B1 is also expressed in other tissues, like activated macrophages, microglia, parathyroid glands, breast, colon and keratinocytes; 1,25 (OH)2 D has autocrine and paracrine effects [34,35]. It is known that vitamin D is associated with bone health and can play an essential role in other systems, including the immune system. These extra skeletal actions are available because of the presence of VDR and hydroxylation enzymes in different tissues such as the pancreas, kidney, muscles, liver and others. Vitamin D supplementation (VDS) has hormonal, anti-inflammatory, anti-apoptotic, anti-fibrotic activities, antioxidant and immune-modulatory effects [36,37], as well as plays a role in insulin resistance, through the reduction of the expression of some pro-inflammatory cytokines, like interleukin-1 (IL-1) and IL-6 [38].
2. VITAMIN D AND INSULIN RESISTANCE
2.1. Vitamin D, Insulin-resistance and molecular mechanisms
Vitamin D is involved in several non-skeletal health diseases, including common metabolic disorders like Metabolic Syndrome (MetS), Type 2 Diabetes (T2DM), Impaired Fasting Glucose (IFG), Non-Alcoholic Fatty Liver Disease (NAFLD) and Polycystic ovarian syndrome (PCOS), that are all characterized by insulin resistance (IR) [39,40,41]. It has been demonstrated that there is an inverse association between vitamin D deficiency and Homeostatic Model Assessment of Insulin Resistance (HOMA-IR), which is used as the measure of insulin resistance, defined as an increase in insulin secretion necessary for the maintenance of glycemic homeostasis [42]. Therefore, supplementation of vitamin D reduces the risk of insulin resistance and circulating levels of insulin [42,43]; the inverse correlation between vitamin D and HOMA-IR gets more robust with increasing Body Mass Index (BMI) [42].
Molecular mechanisms underlying the pathophysiological hypothesis of the possible association between hypovitaminosis D and insulin resistance are mainly associated with the expression of insulin-receptors and the production of inflammatory cytokines and polymorphism of VDR expressed in the β-cells of the pancreas. Based on the above, hypovitaminosis D and insulin resistance are genetically interrelated [40,42,43].
Concerning insulin receptor expression, it was found that vitamin D increases receptor expression in muscle, liver and adipose tissue, improving insulin sensitivity [42]. In detail, it was shown that vitamin D works as an epigenetic factor, affecting the transcription level of many genes involved in insulin sensitivity, like Insulin Receptor Substrate (IRS), which is increased by 2.4-fold in high-fat mice models treated with vitamin D [42]. As a result, insulin sensitivity improves in the target tissues because IRS protein increases insulin sensitivity [42]. In addition, vitamin D improves the sensitivity of insulin receptors to insulin and glucose transport and promotes the conversion of proinsulin to insulin [43,44,45].
Vitamin D deficiency increases the expression of pro-inflammatory cytokines, which can be the cause of insulin resistance in patients with relatively higher BMI, it has been observed that obesity is associated with hypovitaminosis D because of three reasons: the less exposure to sunlight, the low intake of vitamin D through nutrition and the sequestration of vitamin D in the adipose tissue [42]. In addition to this mechanism, it was found that high secretion of the anti-diabetic hormone leptin, whose levels are deregulated by abdominal adiposity, is associated with insulin resistance. That means that high doses of vitamin D supplements can decrease leptin levels and reduce BMI in insulin-resistant patients [42]. This effect would be linked to a reduced caloric intake mediated by the binding of vitamin D to its receptors in the paraventricular nucleus of the hypothalamus.
As regards VDR, it is an endocrine member of the nuclear receptor superfamily for steroid hormones, and it works as a transcription factor that mediates the action of vitamin D through control of the expression of hormone-sensitive genes, like Calmodulin-Dependent Kinase (CaMKs), which in turn stimulates VDR-Mediated transcription by phosphorylation levels of VDR [40]. The function of β-cells may be affected by vitamin D through direct and indirect mechanisms: the direct mechanism consists of binding of vitamin D to VDR in β-cells, helping in the release of insulin secretion [42,46]; the indirect mechanism is related to the regulation by vitamin D of calcium flux through the pancreatic β-cell because insulin secretion is strongly dependent on calcium [46]. This could be the reason why tissue calcium levels (adipose tissue and skeletal muscle) affect IR [46]. It was recently discovered that deletion of macrophage VDR promotes insulin resistance [40].
Recently, it was found that the enzyme activating vitamin D, 1-α-hydroxylase, is present in β-cells [46]. Other elements that support the role of vitamin D in the secretion of insulin are the presence of vitamin D response elements (VDRE) in the promoter region of the insulin gene and the activation of the insulin gene by vitamin D [42].
2.2. Studies and research
A recent meta-analysis, which included 9232 participants, has studied genetic associations of four polymorphisms in the VDR with insulin-resistance diseases, particularly TaqI, BsmI, ApaI, and FokI variants. It was found that there is an association between insulin-resistance-related diseases (mostly with PCOS and MetS than T2DM) and VDR ApaI variant (mostly G allele than T allele) in Asians and population who lived in middle latitude district, BsmI (mostly A allele than G allele) and TaqI variant (T/C allele) in dark-pigmented Caucasian. At the same time, there was no association between VDR FokI variant and insulin-resistance-related diseases in populations with different skin pigments and in different latitudes [40].
Beneficial effects of high-dose (vitamin D ≥ 2000 mg/day and calcium ≥ 1000 mg/day) and in both short-term and long-term (> 12 weeks) combined vitamin D and calcium supplementation were found [46]. However, the results obtained so far are conflictive because some trials reported that supplementation of vitamin D does not reduce insulin resistance [29]. Further studies, like long-term and large-scale randomized controlled trials, are needed.
3. VITAMIN D AND TYPE 2 DIABETES MELLITUS (T2DM)
3.1. Vitamin D, T2DM and molecular mechanisms
It is well known that T2DM is a public health challenge worldwide, accounting for approximately 87%–91% of all cases of diabetes. Type 2 Diabetes Mellitus is a chronic metabolic disorder characterized by inadequate insulin production and consequentially high blood glucose [47]. T2DM constitute an essential risk factor for premature death and adverse complications, micro and macrovascular, such as blindness, stroke, heart attack, amputation, and kidney failure [48], and also determines and impairs quality of life [49]. According to OMS, 762 million people worldwide suffer from prediabetes [50], which is strongly connected with obesity [51].
3.2. Studies and research
According to a recent meta-analysis, vitamin D supplementation improves glycemic homeostasis and insulin sensitivity [55]. It seems also to work as an anti-diabetic factor by regulating insulin sensitivity and production, controlling parathyroid hormone levels and anti-inflammatory cytokine effects [56,57]. Vitamin D has been identified as a potential prevention and treatment strategy [58]. Low 25-hydroxyvitamin D (25(OH) D) levels are highly prevalent among T2DM patients [59]. The effects of vitamin D supplementation may explain the association between vitamin D and T2DM, because it prevented the increase in plasma HbA1c levels and in IR [60,61,62].
The Gold Standard for evaluating glycemic control in T2DM is represented by glycated hemoglobin (HbA1c) in line with The UK Prospective Diabetes Study [63].
In line with recent studies, vitamin D supplementation is implicated in plasma HbA1c reduction, suggesting that vitamin D can contribute in reducing the development of diabetic complications [64]. Also, studies have found that vitamin D supplementation improved beta cell function [65] and insulin sensitivity [54,66,67,68], especially in persons at high risk for diabetes.
In particular, vitamin D has a role in lipid metabolism in adipose tissue [69] and may decrease inflammation [70]. In pancreatic tissue, Vitamin D protects β-cells function, reducing local inflammation [71,72]. A key role is represented by the activation of the VDR expressed in the pancreatic beta-cell. Indeed, mice lacking VDR have impaired insulin secretion [73], and the addition of Vitamin D stimulates pancreatic cells, resulting in increased insulin secretion [74]. It is worth outlining that the human insulin receptor gene promoter contains a Vitamin D response element, suggesting that transcriptional activation of the gene may be favoured by calcitriol administration [75,76]. A calcium-dependent mechanism mediates insulin secretion. Vitamin D may play a role [77] in regulating the opening and closure of calcium channels, mediating the calcium flux in beta cells and interacting with receptors (VDR and 1,25D3-MARRS). Therefore, vitamin D deficiency causing an alteration in calcium flux could interfere with normal insulin secretion [78,79]. In addition, vitamin D is involved in skeletal muscle metabolism, insulin sensitivity, and lipid composition [80]. Consequently, increasing circulating vitamin D concentration could affect tissue energy and metabolism, improving systemic insulin sensitivity. The skeletal muscle is crucial in insulin sensitivity, involving postprandial period 70%–90% of total glucose disposal [81,82,83]. Thus, vitamin D supplementation might improve skeletal muscle glucose handling and, as a consequence, insulin sensitivity [84]. Vitamin D also regulates the adipose tissue, and hypovitaminosis may play a role in obesity and fat mass due to the restoration of Vitamin D, a fat-soluble vitamin, in the adipose tissue. [85]. According to Bajaj et al., hypovitaminosis also seems to increase microvascular complications such as diabetes retinopathy, diabetic neuropathy, diabetic nephropathy, and diabetic foot ulcers [86], and a meta-analysis demonstrated that increased circulating vitamin D levels protect the kidney from injury and ameliorate proteinuria in T2DM patients [87]. Concerning microvascular complications, vitamin D deficiency may be involved in diabetic neuropathy interfering with nociceptor functions by causing diabetic nerve damage [88], and diabetic retinopathy increasing the severity and playing a role in the pathogenesis through its effects on the immune system and angiogenesis [89]. Lastly, lack of Vitamin D promotes macrovascular complications such as endothelial dysfunction and arterial stiffness [90,91], peripheral arterial disease and carotid arterial plaque [92]. Hence, hypovitaminosis D (as deficiency or insufficiency) embrace several complications in diabetic patients; therefore, screening for vitamin D levels in T2DM patients may play a crucial role in defining the outcomes.
4. VITAMIN D AND TYPE 1 DIABETES MELLITUS (T1DM)
4.1. Vitamin D, T1DM and molecular mechanisms
Type 1 Diabetes Mellitus (T1DM) is a chronic autoimmune disease related to an immune system alteration that destroys pancreatic ß cells with a consequent quantitative or qualitative dysfunction of insulin [93]. The prevalence of T1DM has steadily increased over the past few decades in most countries [94]. Patients with T1DM are genetically susceptible to developing autoimmune diseases, with an increased risk of developing the disease among first-degree relatives [95,96]. Currently, the research aims to identify genetic and environmental factors predisposing to the onset of the disease. Current knowledge suggests that an important role could be played by vitamin D, which in the first years of life modulates the still-growing immune system, which plays a crucial role in the development of self-tolerance [97,98,99]. Vitamin D signalling impairment, especially in the first years of life, increases the risk of autoimmunity [100,101,102]. Given the role that vitamin D plays in the immune system, it is believed that it may have a protective role in the development of T1DM [103].
The discovery of vitamin D receptors throughout the body has opened up new reflections on its possible implication in other diseases, including autoimmune diseases such as T1DM and multiple sclerosis [104]. Indeed, VDR is also expressed in immune cells, effectively regulating innate and adaptive immune responses [105].
The expression of 1α-hydroxylase CYP27B1 in specific immune system cells explains how these can regulate vitamin D levels [106]. Some studies have shown that the activity of macrophages/monocytes, antigen pre-transmitter cells, T cells, and B cells is regulated by vitamin D [107]. Vitamin D stimulates the innate immune system by inducing antimicrobial substances, but an overall opposite effect on adaptive immunity has been reported [108]. Indeed, it plays a role in the modulation of the activity of dendritic cells [109]. In the presence of 1,25(OH)2D3, dendritic cells produce fewer inflammatory factors such as tumor necrosis factor-α and interleukin-12, producing a less anti-inflammatory tolerance state characterized by increased production of interleukin-10 [109].
In the same way, in late immune responses, 1,25(OH)2D3 promotes macrophage differentiation, which is essential for the activation of involutional inflammation in animal models of T1DM, to the anti-inflammatory phenotype (M1→M2) via the VDR- PPARgamma signalling pathway [110]. More recently, vitamin D metabolites have also been reported to act directly on various T cell populations. After activation, T cells begin to express VDRs and are the primary targets of calcitriol in regulating immune responses [107]. Vitamin D differentiates naive T cells into T helper two cells and regulatory T cells (T-reg) [111]. In this sense, a randomized controlled trial showed that monthly supplementation of healthy humans with 140,000 IU cholecalciferol for three months significantly increased peripheral blood T-reg cell counts compared to placebo [112]. In addition, the binding between vitamin D and VDRs expressed in active B lymphocytes leads to the inhibition of immunoglobulin production [113]. These properties of vitamin D, on the regulation of the inflammatory response are very interesting in T1DM because, in the pancreas of affected patients, there is an inflammatory infiltrate composed of T lymphocytes, B lymphocytes and macrophages. In animal models of T1DM, such as nonobese diabetic mice, high doses of calcitriol and non-high calcium vitamin D analogues arrest involutional inflammation, as indicated by reduced effector T cell numbers and induction of T-reg cells [114,115,116].
Fronczak et al. reported that increased maternal intake of vitamin D in food reduced the risk of autoimmunity against pancreatic beta cells in their offspring; there is no effect of 1alpha,25-dihydroxyvitamin D3 on residual beta cell function and insulin requirements in adults [117].
4.2. Studies and research
According to evidence (systematic reviews, meta-analyses) [118,119] on the link between vitamin D levels and T1DM, adequate vitamin D status in the first years of life reduces the risk of diabetes [17,97,99,120], and vitamin D deficiency is more common in people with T1DM [121,122]. A cross-sectional study revealed that 70% of children with T1DM had a vitamin D deficiency [123], and rickets are associated with an increased risk of T1DM [124]. Also, the TEDDY study reported that a higher infant concentration of 25(OH)D is associated with lower islet autoimmunity [125]. In contrast, a birth-cohort study in Finland suggested that sufficient vitamin D supplementation could assist in decreasing T1DM risk [124].
The risk of developing T1DM before 15 age is associated with a reduction in serum vitamin D levels as demonstrated by a case-control study that was part of EURODIAB (OR 0.63) [126]. Human studies report the relationship between VDR polymorphisms and T1DM risk and β cell function. Although 25D is the major circulating form, pancreatic β cells can convert 25D to 1,25D [127]. This implies that a small role in beta cell survival in T1DM can be played by exogenous and circulating 1,25 D. Anyhow, rising 25D levels could be helpful to as a substrate for the formation of 1,25D by beta cells while circulating 1,25 D could exert autocrine and paracrine effects. Considering beta cell injury at the clinical diagnosis, vitamin D is much less likely to be helpful after disease onset [128]. A meta-analysis conducted by Najjar et al. found no critical effect of a genetically determined reduction in 25(OH)D concentrations by selected polymorphisms on T1DM risk. However, a strong association was shown in some observational studies [129].
5. VITAMIN D AND GESTATIONAL DIABETES MELLITUS (GDM)
5.1. Pathophysiology of vitamin D levels in pregnancy
In pregnancy, numerous physiological alterations of the maternal metabolism are necessary for the normal development of the fetus. During pregnancy, a relationship between the maternal and fetal vitamin D status underlines the importance of an adequate vitamin D level in this period. Gestational vitamin D metabolism adaptations include a characteristic physiological growing of 1,25(OH)2D in maternal blood. It rises at the beginning of gestation and reaches its highest levels in the third trimester when it presents two to three times the levels found in non-pregnant women. Several studies have shown a correlation between vitamin D levels and GDM [130]. GDM is defined as glucose intolerance, and IR was first diagnosed in pregnant women [131]. GDM affects up to 14% of pregnancies [132]. Inadequate glycemic control in women with GDM leads to short- and long-term maternal complications, including gestational hypertension, preeclampsia, macrosomia, congenital abnormalities, hypoglycemia in the newborn, and an increased risk of T2DM after pregnancy [133,134]. GDM is compared a form of impaired glucose tolerance, similar to prediabetes in non-pregnant individuals, and represents a global public health problem related to serious health problems in the mother and newborn [135]. Women with a history of GDM have an increased risk of developing IR syndrome (IRS) and cardiovascular disease (CVD) later in their lives [136]. The rate of women who develop T2DM within 5-10 years ranges from 20 to 60% [137,138]. The risks of occurrence of MetS and CVD are three times higher in women with GDM. Indeed, children born to women with GDM have a higher risk of developing impaired glucose tolerance and obesity. The pathogenesis of GDM has not yet been cleared. Some studies [139,140] suggest that the onset and development of GDM are closely related to genetic factors (insulin resistance, family history of diabetes and immune dysfunction) and environmental (dietary structure and pancreatic β cell damage).
5.2. Vitamin D, GDM and molecular mechanisms
Vitamin D can support insulin secretion and normal glucose tolerance [141]. Vitamin D deficiency seems closely related to the onset of GDM. Among the factors that may play a role in the onset of GDM is chronic low-grade inflammation [142]. The increased degree of inflammation in early pregnancy is related to an increased risk of GDM and the development of hyperglycemia [143]. Moreover, in women with GDM, oxidative stress has been found [144,145,146], while antioxidant status is down-regulated [147]. Oxidative stress plays an important role in both the pathogenesis and complications of GDM [148]. A significant inverse association exists between serum vitamin D concentrations and low-grade inflammation [149]. The low levels of vitamin D trigger inflammatory responses through the NF-kB pathway by regulating p-p65/RelB in pancreas tissue [150] upwards. Excessive Ca2+ and reactive oxygen species (ROS) in ß cells, both in vitamin D deficiency, result in cell death and promote diabetes [151].
Furthermore, some genes that protect against the onset of diabetes are inactivated by hypermethylation [152]. Vitamin D prevents hypermethylation by increasing the expression of DNA demethylases in more regions of genes that protect against diabetes [151]. In addition, a significant inverse association was also found between serum calcium concentrations, which is positively regulated by vitamin D, and obesity risk, as another diabetes risk factor [153].
5.3. Studies and research
Several longitudinal prospective cohort studies have reported the risk of GDM with serum vitamin D concentrations in early pregnancy [154]. A meta-analysis conducted by Chunfeng Wu et al. [155] showed that vitamin D supplementation has a beneficial effect on lipidic assessment: increasing HDL-Cholesterol (HDL-C) levels and is useful for reducing serum Total Cholesterol (TC) and LDL-Cholesterol (LDL-C) levels of patients with GDM. However, no single opinion exists between this meta-analysis and the previous ones [156,157]. Preceding meta-analyses [157] pointed out that vitamin D can improve LDL-C levels but does not affect triglycerides (TG), TC and HDL-C. The short duration of the studies could explain this. Several studies [158,159,160] have shown that when GDM patients have abnormal lipid metabolism, their risk of pregnancy complications increases. Studies [161,162] proved that vitamin D deficiency is associated with a higher incidence of T2DM, and vitamin D supplementation can dramatically increase insulin sensitivity in people with IR and vitamin D deficiency. IR and insufficient secretion underlie the pathogenesis of GDM [163]. According to a network-metanalysis conducted by Shixiao Jin et al. to evaluate the effects of vitamin D supplementation was the best for reducing fast plasma glucose (FPG) and improving HOMA-IR compared to the effects of other nutritional strategies [164]. Vitamin D deficiency is a frequent phenomenon after pregnancy; one study showed that at 25-28 weeks of gestation, the concentration of 25(OH)D (the active form of the vitamin within the body) in GDM patients is significantly reduced [165]. Another Systematic Review and Meta-Analysis conducted by Wang M. et al. has shown how vitamin D supplementation in a population of women with GDM can statistically significantly reduce serum FPG, insulin, HOMA-IR, as well as complications related to childbirth (cesarean section, maternal hospitalization and postpartum haemorrhage) and newborn (hyperbilirubinemia, giant children, hypoglycemia, polyhydramnios, fetal distress, and premature delivery). Vitamin D deficiency is considered a potential risk factor for abnormal glucose metabolism; Zhang et al. [166] conducted a study that showed that low vitamin D levels in the blood may increase the risk of GDM and that adequate vitamin D supplementation may improve GDM status. 25(OH)D can not only regulate insulin secretion but also stimulate insulin receptor expression to promote insulin sensitivity [167], achieving the effect of lowering blood sugar. In addition, vitamin D has antioxidant effects, which can reduce β islet cell damage and apoptosis β of islet cells through active oxidative groups [168]. Patients with GDM can increase their 25(OH)D concentration through vitamin D supplementation, thereby improving insulin resistance and decreasing blood sugar [169].
6. VITAMIN D, METABOLIC SYNDROME (MetS) AND CARDIOVASCULAR DISEASE (CVD)
6.1. MetS and CVD: burden of the problem
MetS is related to abdominal obesity, IR, hypertension, and dyslipidemia [170]. The diagnosis of MetS including waist circumference (WC), FPG, TG levels, HDL-C levels, total cholesterol levels, and blood pressure (BP) [171]. The MetS increases the risk of developing T2DM associated with long-term microvascular and macrovascular damage [172] and CVDs. CVDs are one of the significant causes of disability and death worldwide [173]. Atherosclerosis is the primary aetiology of CVDs, and it is considered a chronic inflammatory condition [174]. Several studies have also documented that a decrease in antioxidant levels and an increase in inflammatory and oxidative stress biomarkers may be involved in the pathophysiology of T2DM complications [175] and the onset of CVDs [176]. The inflammatory process can be triggered by metabolic disorders such as atherogenic dyslipidemia (higher TG and apolipoprotein B, small low-density lipoprotein cholesterol LDL-C particles, and low HDL-C concentrations), T2DM, and increased inflammatory cytokines [177]. Consequently, the inflammatory cascade may initiate plaque formation, endothelial damage, and, ultimately, plaque rupture [174]. The pathophysiology of endothelial dysfunction includes overproduction of reactive oxidative species, inflammatory cytokines and pro-atherogenic lipoproteins, and an imbalance between vasodilating and vasoconstricting molecules. Impairment of vasodilatation may be due to reduced bioavailability of nitric oxide (NO), produced by the endothelial cells and involved in multiple physiological processes, including vasodilation, inflammation and platelet aggregation [178]. On the other hand, dyslipidemia is associated with insulin resistance and elevated risk of CVD events [179,180]. There are numerous risk factors for MetS e CVDs; among these, the dietary factor is among the most important [181], such as high-calorie and high-fat diets [182].
6.2. Vitamin D, MetS and CVD and molecular mechanisms
Vitamin D deficiency patients are a risk factor for MetS [183]. Vitamin D deficiency can affect insulin secretion and sensitivity and play an essential role in the onset of MetS [27]. Furthermore, a study found that vitamin D supplementation had a positive effect on lipid profile, IR, hyperglycemia, obesity and hypertension and then on the treatment of MetS-related disorders [184].
Vitamin D can reduce Oxidative Stress (OS) using upregulating cellular Glutathione (GSH) and antioxidant systems such as glutathione peroxidase and superoxide dismutase [185]. Also, vitamin D can inhibit Reactive Oxygen Species (ROS) secretion [186]. VDRs are expressed in different tissues, notably endothelial cells, vascular smooth muscle cells and cardiomyocytes and regulate the expression of the target gene [187]. Vitamin D3, furthermore is a direct transcriptional regulator of endothelial Nitric Oxide (NO) synthase. In this pathophysiological situation, OS plays a crucial role in cellular injury in which the production of reactive ROS suppresses the antioxidant defence system of the cells, which consequently causes cellular death [188]. Under the physiologic conditions, the antioxidant defence systems maintain the oxidant-antioxidant balance by adjusting the altering levels of oxidants [189]. The antioxidant defence systems include enzymes such as glutathione peroxidase, catalase, superoxide dismutase, and other compounds (albumin, GSH).
Furthermore, different nutrients such as vitamins and minerals can also affect the antioxidant balance [190,191,192]. Accordingly, vitamin D has been proposed to have antioxidant properties. The association between VDS and MetS is controversial. The benefits of VDS in the treatments of MetS and its disorders connected include improved arterial stiffness, mitochondrial oxidation and phospholipid metabolism; increased lipoprotein lipase activity, peripheral insulin sensitivity and β-cell function; decreased inflammatory cytokines and parathyroid hormone levels, and renin-angiotensin-aldosterone system activity [193,194,195,196].
6.3. Studies and research
Zhu and Heil reported that serum 25D level was linked to the risk factors for MetS [197]. In a meta-analysis study, Jafari et al. [198] reported that vitamin D supplementation improved the lipid profile of patients with T2DM. In another meta-analysis, vitamin D intake significantly decreased insulin resistance in people with T2DM [199]. Several RCTs have studied the impact of vitamin D supplements on lipid profiles, glucose homeostasis, and C-reactive protein (CRP) in persons with CVD [200]. Some studies reported no significant relationship between VDS and MetS in adults [201,202,203]. Therefore, the association between VDS and MetS still needs evidence to demonstrate whether VDS helps treat MetS. In a meta-analysis, Ostadmohammadi, Milajerdi, et al. demonstrated the beneficial effects of vitamin D supplementation on reductions in fasting glucose, insulin concentrations, and HOMA-IR. In addition, the pooled analysis revealed a significant increase in serum HDL-C concentrations after vitamin D therapy and a significant reduction in CRP levels. However, supplementation did not affect TG, TC, and LDL-C levels [204]. Kai-Jie, Zhong-Tao et al. have realized a meta-analysis to study the effect of vitamin D on MetS in adults using relevant biomarkers such as anthropometric parameters, BP, blood lipid profile, blood sugar, OS and vitamin D toxicity. Vitamin D did not affect waist circumference, body mass index, body fat percentage and BP. VDS significantly reduced FPG, but did not affect HDL-C, LDL-C, TC and TG blood levels. For OS parameters, VDS significantly lowered malondialdehyde and hypersensitive CRP [205]. Tatiana P., Caroline K, et al. [206] in a systematic review and meta-analysis, randomized clinical trials (RCTs) investigated the effects of micronutrients on BP in patients with T2DM. In this systematic review, a reduction in BP, especially systolic BP, has been demonstrated. Observational and experimental data favour the concept that vitamin D is associated with the pathogenesis of arterial hypertension [207,208]. A possible mechanism for this link involves the inhibition of the renin-angiotensin-aldosterone system by vitamin D. Additionally, in the presence of hypovitaminosis D, an alternative mechanism could be related to the secondary hyperparathyroidism and relative hypocalcemia that are commonly seen in these patients [209]. In a meta-analysis, Hajhashemy Z, Shahdadian F, et al. illustrated that the highest level of blood vitamin D, compared with the lowest level, was significantly linked to lower odds of MetS in cross-sectional studies on the adult population. In addition, based on dose–response analysis, each 25 nmol/L (or 10 ng/ml) increment in 25(OH)D was associated with a 15% decreased chance of MetS.
DISCUSSION AND CONCLUSIONS
Data reported in our review support the notion that Vitamin D levels are associated with T1DM and T2DM, GDM, MetS and CVDs. There is some experimental and epidemiological evidence for the administration of Vitamin D in these different diseases. In Table 1, we have summarized the results of Meta-Analyses and Systematic Reviews on the effectiveness of vitamin D administration and their dosages in the various conditions that we have dealt with in this review. However, data from randomized clinical trials, very highly heterogeneous, have yielded contrasting data. Although the possibility of preventing the onset of the disease, vitamin D administration should be started very early in life or even during pregnancy in T1DM and GDM; moreover, different data showed that vitamin D administration improves glucose metabolism and the risk T2DM and metabolic syndrome, randomized clinical studies showed contradictory results for vitamin D supplementation in the management of altered metabolic states. In this sense, further studies are necessary to determine the fundamental role of vitamin D deficiency and if it can be considered a causal factor in altered metabolism.
References
- Dattola, A.; Silvestri, M.; Bennardo, L.; Passante, M.; Scali, E.; Patruno, C.; Nisticò, S.P. Role of Vitamins in Skin Health: A Systematic Review. Curr Nutr Rep 2020, 9, 226–235. [CrossRef]
- Umar, M.; Sastry, K.S.; Chouchane, A.I. Role of Vitamin D Beyond the Skeletal Function: A Review of the Molecular and Clinical Studies. Int J Mol Sci 2018, 19, 1618. [CrossRef]
- Maddaloni, E.; Cavallari, I.; Napoli, N.; Conte, C. Vitamin D and Diabetes Mellitus. Front Horm Res 2018, 50, 161–176. [CrossRef]
- Mitri, J.; Muraru, M.D.; Pittas, A.G. Vitamin D and Type 2 Diabetes: A Systematic Review. Eur J Clin Nutr 2011, 65, 1005–1015. [CrossRef]
- Targher, G.; Bertolini, L.; Scala, L.; Cigolini, M.; Zenari, L.; Falezza, G.; Arcaro, G. Associations between Serum 25-Hydroxyvitamin D3 Concentrations and Liver Histology in Patients with Non-Alcoholic Fatty Liver Disease. Nutr Metab Cardiovasc Dis 2007, 17, 517–524. [CrossRef]
- Chen, X.; Zhou, M.; Yan, H.; Chen, J.; Wang, Y.; Mo, X. Association of Serum Total 25-Hydroxy-Vitamin D Concentration and Risk of All-Cause, Cardiovascular and Malignancies-Specific Mortality in Patients with Hyperlipidemia in the United States. Front Nutr 2022, 9, 971720. [CrossRef]
- Wimalawansa, S.J. Non-Musculoskeletal Benefits of Vitamin D. J Steroid Biochem Mol Biol 2018, 175, 60–81. [CrossRef]
- Teleni, L.; Baker, J.; Koczwara, B.; Kimlin, M.G.; Walpole, E.; Tsai, K.; Isenring, E.A. Clinical Outcomes of Vitamin D Deficiency and Supplementation in Cancer Patients. Nutr Rev 2013, 71, 611–621. [CrossRef]
- Khademi, Z.; Hamedi-Shahraki, S.; Amirkhizi, F. Vitamin D Insufficiency Is Associated with Inflammation and Deregulation of Adipokines in Patients with Metabolic Syndrome. BMC Endocrine Disorders 2022, 22, 223. [CrossRef]
- Argano, C.; Mallaci Bocchio, R.; Natoli, G.; Scibetta, S.; Lo Monaco, M.; Corrao, S. Protective Effect of Vitamin D Supplementation on COVID-19-Related Intensive Care Hospitalization and Mortality: Definitive Evidence from Meta-Analysis and Trial Sequential Analysis. Pharmaceuticals (Basel) 2023, 16, 130. [CrossRef]
- Corrao, S.; Mallaci Bocchio, R.; Lo Monaco, M.; Natoli, G.; Cavezzi, A.; Troiani, E.; Argano, C. Does Evidence Exist to Blunt Inflammatory Response by Nutraceutical Supplementation during COVID-19 Pandemic? An Overview of Systematic Reviews of Vitamin D, Vitamin C, Melatonin, and Zinc. Nutrients 2021, 13, 1261. [CrossRef]
- Argano, C.; Mallaci Bocchio, R.; Lo Monaco, M.; Scibetta, S.; Natoli, G.; Cavezzi, A.; Troiani, E.; Corrao, S. An Overview of Systematic Reviews of the Role of Vitamin D on Inflammation in Patients with Diabetes and the Potentiality of Its Application on Diabetic Patients with COVID-19. Int J Mol Sci 2022, 23, 2873. [CrossRef]
- Barragan, M.; Good, M.; Kolls, J.K. Regulation of Dendritic Cell Function by Vitamin D. Nutrients 2015, 7, 8127–8151. [CrossRef]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr Hypertens Rep 2018, 20, 12. [CrossRef]
- Argano, C.; Natoli, G.; Mularo, S.; Nobili, A.; Monaco, M.L.; Mannucci, P.M.; Perticone, F.; Pietrangelo, A.; Corrao, S. Impact of Diabetes Mellitus and Its Comorbidities on Elderly Patients Hospitalized in Internal Medicine Wards: Data from the RePoSi Registry. Healthcare (Basel) 2022, 10, 86. [CrossRef]
- Diabetes Is “a Pandemic of Unprecedented Magnitude” Now Affecting One in 10 Adults Worldwide. Diabetes Research and Clinical Practice 2021, 181. [CrossRef]
- Dong, J.-Y.; Zhang, W.; Chen, J.J.; Zhang, Z.-L.; Han, S.-F.; Qin, L.-Q. Vitamin D Intake and Risk of Type 1 Diabetes: A Meta-Analysis of Observational Studies. Nutrients 2013, 5, 3551–3562. [CrossRef]
- Littorin, B.; Blom, P.; Schölin, A.; Arnqvist, H.J.; Blohmé, G.; Bolinder, J.; Ekbom-Schnell, A.; Eriksson, J.W.; Gudbjörnsdottir, S.; Nyström, L.; et al. Lower Levels of Plasma 25-Hydroxyvitamin D among Young Adults at Diagnosis of Autoimmune Type 1 Diabetes Compared with Control Subjects: Results from the Nationwide Diabetes Incidence Study in Sweden (DISS). Diabetologia 2006, 49, 2847–2852. [CrossRef]
- Song, Y.; Wang, L.; Pittas, A.G.; Del Gobbo, L.C.; Zhang, C.; Manson, J.E.; Hu, F.B. Blood 25-Hydroxy Vitamin D Levels and Incident Type 2 Diabetes: A Meta-Analysis of Prospective Studies. Diabetes Care 2013, 36, 1422–1428. [CrossRef]
- Afzal, S.; Bojesen, S.E.; Nordestgaard, B.G. Low 25-Hydroxyvitamin D and Risk of Type 2 Diabetes: A Prospective Cohort Study and Meta-analysis. Clin Chem 2013, 59, 381–391. [CrossRef]
- Lee, C.J.; Iyer, G.; Liu, Y.; Kalyani, R.R.; Bamba, N.; Ligon, C.B.; Varma, S.; Mathioudakis, N. The Effect of Vitamin D Supplementation on Glucose Metabolism in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Intervention Studies. J Diabetes Complications 2017, 31, 1115–1126. [CrossRef]
- Sharma, S.; Biswal, N.; Bethou, A.; Rajappa, M.; Kumar, S.; Vinayagam, V. Does Vitamin D Supplementation Improve Glycaemic Control In Children With Type 1 Diabetes Mellitus? - A Randomized Controlled Trial. J Clin Diagn Res 2017, 11, SC15–SC17. [CrossRef]
- Ataie-Jafari, A.; Loke, S.-C.; Rahmat, A.B.; Larijani, B.; Abbasi, F.; Leow, M.K.S.; Yassin, Z. A Randomized Placebo-Controlled Trial of Alphacalcidol on the Preservation of Beta Cell Function in Children with Recent Onset Type 1 Diabetes. Clin Nutr 2013, 32, 911–917. [CrossRef]
- Contreras-Bolívar, V.; García-Fontana, B.; García-Fontana, C.; Muñoz-Torres, M. Mechanisms Involved in the Relationship between Vitamin D and Insulin Resistance: Impact on Clinical Practice. Nutrients 2021, 13, 3491. [CrossRef]
- Gysemans, C.A.; Cardozo, A.K.; Callewaert, H.; Giulietti, A.; Hulshagen, L.; Bouillon, R.; Eizirik, D.L.; Mathieu, C. 1,25-Dihydroxyvitamin D3 Modulates Expression of Chemokines and Cytokines in Pancreatic Islets: Implications for Prevention of Diabetes in Nonobese Diabetic Mice. Endocrinology 2005, 146, 1956–1964. [CrossRef]
- Park, S.; Kim, D.S.; Kang, S. Vitamin D Deficiency Impairs Glucose-Stimulated Insulin Secretion and Increases Insulin Resistance by Reducing PPAR-γ Expression in Nonobese Type 2 Diabetic Rats. The Journal of Nutritional Biochemistry 2016, 27, 257–265. [CrossRef]
- Melguizo-Rodríguez, L.; Costela-Ruiz, V.J.; García-Recio, E.; De Luna-Bertos, E.; Ruiz, C.; Illescas-Montes, R. Role of Vitamin D in the Metabolic Syndrome. Nutrients 2021, 13, 830. [CrossRef]
- Mancuso, P.; Rahman, A.; Hershey, S.D.; Dandu, L.; Nibbelink, K.A.; Simpson, R.U. 1,25-Dihydroxyvitamin-D3 Treatment Reduces Cardiac Hypertrophy and Left Ventricular Diameter in Spontaneously Hypertensive Heart Failure-Prone (Cp/+) Rats Independent of Changes in Serum Leptin. J Cardiovasc Pharmacol 2008, 51, 559–564. [CrossRef]
- Pieńkowska, A.; Janicka, J.; Duda, M.; Dzwonnik, K.; Lip, K.; Mędza, A.; Szlagatys-Sidorkiewicz, A.; Brzeziński, M. Controversial Impact of Vitamin D Supplementation on Reducing Insulin Resistance and Prevention of Type 2 Diabetes in Patients with Prediabetes: A Systematic Review. Nutrients 2023, 15, 983. [CrossRef]
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium Dietary Reference Intakes for Calcium and Vitamin D; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; The National Academies Collection: Reports funded by National Institutes of Health; National Academies Press (US): Washington (DC), 2011;
- Haussler, M.R.; Haussler, C.A.; Jurutka, P.W.; Thompson, P.D.; Hsieh, J.C.; Remus, L.S.; Selznick, S.H.; Whitfield, G.K. The Vitamin D Hormone and Its Nuclear Receptor: Molecular Actions and Disease States. J Endocrinol 1997, 154 Suppl, S57-73.
- Adams, J.S.; Rafison, B.; Witzel, S.; Reyes, R.E.; Shieh, A.; Chun, R.; Zavala, K.; Hewison, M.; Liu, P.T. Regulation of the Extrarenal CYP27B1-Hydroxylase. J Steroid Biochem Mol Biol 2014, 144PA, 22–27. [CrossRef]
- Klopot, A.; Hance, K.W.; Peleg, S.; Barsony, J.; Fleet, J.C. Nucleo-Cytoplasmic Cycling of the Vitamin D Receptor in the Enterocyte-Like Cell Line, Caco-2. J Cell Biochem 2007, 100, 617–628. [CrossRef]
- Charoenngam, N.; Shirvani, A.; Holick, M.F. Vitamin D for Skeletal and Non-Skeletal Health: What We Should Know. J Clin Orthop Trauma 2019, 10, 1082–1093. [CrossRef]
- Battault, S.; Whiting, S.J.; Peltier, S.L.; Sadrin, S.; Gerber, G.; Maixent, J.M. Vitamin D Metabolism, Functions and Needs: From Science to Health Claims. Eur J Nutr 2013, 52, 429–441. [CrossRef]
- Chagas, C.E.A.; Borges, M.C.; Martini, L.A.; Rogero, M.M. Focus on Vitamin D, Inflammation and Type 2 Diabetes. Nutrients 2012, 4, 52–67. [CrossRef]
- Hewison, M. An Update on Vitamin D and Human Immunity. Clin Endocrinol (Oxf) 2012, 76, 315–325. [CrossRef]
- Selvaraj, P.; Harishankar, M.; Afsal, K. Vitamin D: Immuno-Modulation and Tuberculosis Treatment. Can J Physiol Pharmacol 2015, 93, 377–384. [CrossRef]
- Wang, S.; Cai, B.; Han, X.; Gao, Y.; Zhang, X.; Wang, R.; Zhang, Y.; Chen, Q. Vitamin D Supplementation for Non-alcoholic Fatty Liver Disease in Type 2 Diabetes Mellitus: A Protocol for a Systematic Review and Meta-Analysis. Medicine (Baltimore) 2020, 99, e20148. [CrossRef]
- Han, F.; Lv, Y.; Gong, L.; Liu, H.; Wan, Z.; Liu, L. VDR Gene Variation and Insulin Resistance Related Diseases. Lipids Health Dis 2017, 16, 157. [CrossRef]
- Sindhughosa, D.A.; Wibawa, I.D.N.; Mariadi, I.K.; Somayana, G. Additional Treatment of Vitamin D for Improvement of Insulin Resistance in Non-Alcoholic Fatty Liver Disease Patients: A Systematic Review and Meta-Analysis. Sci Rep 2022, 12, 7716. [CrossRef]
- Rafiq, S.; Jeppesen, P.B. Vitamin D Deficiency Is Inversely Associated with Homeostatic Model Assessment of Insulin Resistance. Nutrients 2021, 13, 4358. [CrossRef]
- Mo, M.; Shao, B.; Xin, X.; Luo, W.; Si, S.; Jiang, W.; Wang, S.; Shen, Y.; Wu, J.; Yu, Y. The Association of Gene Variants in the Vitamin D Metabolic Pathway and Its Interaction with Vitamin D on Gestational Diabetes Mellitus: A Prospective Cohort Study. Nutrients 2021, 13, 4220. [CrossRef]
- Wang, M.; Chen, Z.; Hu, Y.; Wang, Y.; Wu, Y.; Lian, F.; Li, H.; Yang, J.; Xu, X. The Effects of Vitamin D Supplementation on Glycemic Control and Maternal-Neonatal Outcomes in Women with Established Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis. Clin Nutr 2021, 40, 3148–3157. [CrossRef]
- Huang, S.; Fu, J.; Zhao, R.; Wang, B.; Zhang, M.; Li, L.; Shi, C. The Effect of Combined Supplementation with Vitamin D and Omega-3 Fatty Acids on Blood Glucose and Blood Lipid Levels in Patients with Gestational Diabetes. Ann Palliat Med 2021, 10, 5652–5658. [CrossRef]
- Asbaghi, O.; Khosroshahi, M.Z.; Kashkooli, S.; Abbasnezhad, A. Effect of Calcium-Vitamin D Co-Supplementation on Insulin, Insulin Sensitivity, and Glycemia: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Horm Metab Res 2019, 51, 288–295. [CrossRef]
- Muoio, D.M.; Newgard, C.B. Mechanisms of Disease:Molecular and Metabolic Mechanisms of Insulin Resistance and Beta-Cell Failure in Type 2 Diabetes. Nat Rev Mol Cell Biol 2008, 9, 193–205. [CrossRef]
- Lotfy, M.; Adeghate, J.; Kalasz, H.; Singh, J.; Adeghate, E. Chronic Complications of Diabetes Mellitus: A Mini Review. Curr Diabetes Rev 2017, 13, 3–10. [CrossRef]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global Aetiology and Epidemiology of Type 2 Diabetes Mellitus and Its Complications. Nat Rev Endocrinol 2018, 14, 88–98. [CrossRef]
- Rooney, M.R.; Fang, M.; Ogurtsova, K.; Ozkan, B.; Echouffo-Tcheugui, J.B.; Boyko, E.J.; Magliano, D.J.; Selvin, E. Global Prevalence of Prediabetes. Diabetes Care 2023, 46, 1388–1394. [CrossRef]
- Blaak, E.E.; Antoine, J.-M.; Benton, D.; Björck, I.; Bozzetto, L.; Brouns, F.; Diamant, M.; Dye, L.; Hulshof, T.; Holst, J.J.; et al. Impact of Postprandial Glycaemia on Health and Prevention of Disease. Obes Rev 2012, 13, 923–984. [CrossRef]
- Zakharova, I.; Klimov, L.; Kuryaninova, V.; Nikitina, I.; Malyavskaya, S.; Dolbnya, S.; Kasyanova, A.; Atanesyan, R.; Stoyan, M.; Todieva, A.; et al. Vitamin D Insufficiency in Overweight and Obese Children and Adolescents. Front Endocrinol (Lausanne) 2019, 10, 103. [CrossRef]
- Kabadi, S.M.; Lee, B.K.; Liu, L. Joint Effects of Obesity and Vitamin D Insufficiency on Insulin Resistance and Type 2 Diabetes. Diabetes Care 2012, 35, 2048–2054. [CrossRef]
- Gagnon, C.; Lu, Z.X.; Magliano, D.J.; Dunstan, D.W.; Shaw, J.E.; Zimmet, P.Z.; Sikaris, K.; Grantham, N.; Ebeling, P.R.; Daly, R.M. Serum 25-Hydroxyvitamin D, Calcium Intake, and Risk of Type 2 Diabetes after 5 Years: Results from a National, Population-Based Prospective Study (the Australian Diabetes, Obesity and Lifestyle Study). Diabetes Care 2011, 34, 1133–1138. [CrossRef]
- Mirhosseini, N.; Vatanparast, H.; Mazidi, M.; Kimball, S.M. Vitamin D Supplementation, Glycemic Control, and Insulin Resistance in Prediabetics: A Meta-Analysis. J Endocr Soc 2018, 2, 687–709. [CrossRef]
- Borissova, A.M.; Tankova, T.; Kirilov, G.; Dakovska, L.; Kovacheva, R. The Effect of Vitamin D3 on Insulin Secretion and Peripheral Insulin Sensitivity in Type 2 Diabetic Patients. Int J Clin Pract 2003, 57, 258–261.
- Fadda, G.Z.; Akmal, M.; Lipson, L.G.; Massry, S.G. Direct Effect of Parathyroid Hormone on Insulin Secretion from Pancreatic Islets. Am J Physiol 1990, 258, E975-984. [CrossRef]
- Sherman, M.H.; Yu, R.T.; Engle, D.D.; Ding, N.; Atkins, A.R.; Tiriac, H.; Collisson, E.A.; Connor, F.; Van Dyke, T.; Kozlov, S.; et al. Vitamin D Receptor-Mediated Stromal Reprogramming Suppresses Pancreatitis and Enhances Pancreatic Cancer Therapy. Cell 2014, 159, 80–93. [CrossRef]
- Pittas, A.G.; Lau, J.; Hu, F.B.; Dawson-Hughes, B. The Role of Vitamin D and Calcium in Type 2 Diabetes. A Systematic Review and Meta-Analysis. J Clin Endocrinol Metab 2007, 92, 2017–2029. [CrossRef]
- Cigolini, M.; Iagulli, M.P.; Miconi, V.; Galiotto, M.; Lombardi, S.; Targher, G. Serum 25-Hydroxyvitamin D3 Concentrations and Prevalence of Cardiovascular Disease among Type 2 Diabetic Patients. Diabetes Care 2006, 29, 722–724. [CrossRef]
- Scragg, R.; Sowers, M.; Bell, C.; Third National Health and Nutrition Examination Survey Serum 25-Hydroxyvitamin D, Diabetes, and Ethnicity in the Third National Health and Nutrition Examination Survey. Diabetes Care 2004, 27, 2813–2818. [CrossRef]
- Di Cesar, D.J.; Ploutz-Snyder, R.; Weinstock, R.S.; Moses, A.M. Vitamin D Deficiency Is More Common in Type 2 than in Type 1 Diabetes. Diabetes Care 2006, 29, 174. [CrossRef]
- Intensive Blood-Glucose Control with Sulphonylureas or Insulin Compared with Conventional Treatment and Risk of Complications in Patients with Type 2 Diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998, 352, 837–853.
- Hu, Z.; Chen, J.; Sun, X.; Wang, L.; Wang, A. Efficacy of Vitamin D Supplementation on Glycemic Control in Type 2 Diabetes Patients: A Meta-Analysis of Interventional Studies. Medicine (Baltimore) 2019, 98, e14970. [CrossRef]
- Mitri, J.; Dawson-Hughes, B.; Hu, F.B.; Pittas, A.G. Effects of Vitamin D and Calcium Supplementation on Pancreatic β Cell Function, Insulin Sensitivity, and Glycemia in Adults at High Risk of Diabetes: The Calcium and Vitamin D for Diabetes Mellitus (CaDDM) Randomized Controlled Trial. Am J Clin Nutr 2011, 94, 486–494. [CrossRef]
- Nazarian, S.; St Peter, J.V.; Boston, R.C.; Jones, S.A.; Mariash, C.N. Vitamin D3 Supplementation Improves Insulin Sensitivity in Subjects with Impaired Fasting Glucose. Transl Res 2011, 158, 276–281. [CrossRef]
- Pramono, A.; Jocken, J.W.E.; Blaak, E.E. Vitamin D Deficiency in the Aetiology of Obesity-Related Insulin Resistance. Diabetes Metab Res Rev 2019, 35, e3146. [CrossRef]
- Alvarez, J.A.; Ashraf, A. Role of Vitamin D in Insulin Secretion and Insulin Sensitivity for Glucose Homeostasis. Int J Endocrinol 2010, 2010, 351385. [CrossRef]
- Larrick, B.M.; Kim, K.-H.; Donkin, S.S.; Teegarden, D. 1,25-Dihydroxyvitamin D Regulates Lipid Metabolism and Glucose Utilization in Differentiated 3T3-L1 Adipocytes. Nutr Res 2018, 58, 72–83. [CrossRef]
- Karkeni, E.; Bonnet, L.; Marcotorchino, J.; Tourniaire, F.; Astier, J.; Ye, J.; Landrier, J.-F. Vitamin D Limits Inflammation-Linked MicroRNA Expression in Adipocytes in Vitro and in Vivo: A New Mechanism for the Regulation of Inflammation by Vitamin D. Epigenetics 2018, 13, 156–162. [CrossRef]
- Altieri, B.; Grant, W.B.; Della Casa, S.; Orio, F.; Pontecorvi, A.; Colao, A.; Sarno, G.; Muscogiuri, G. Vitamin D and Pancreas: The Role of Sunshine Vitamin in the Pathogenesis of Diabetes Mellitus and Pancreatic Cancer. Crit Rev Food Sci Nutr 2017, 57, 3472–3488. [CrossRef]
- Cade, C.; Norman, A.W. Vitamin D3 Improves Impaired Glucose Tolerance and Insulin Secretion in the Vitamin D-Deficient Rat in Vivo. Endocrinology 1986, 119, 84–90. [CrossRef]
- Zeitz, U.; Weber, K.; Soegiarto, D.W.; Wolf, E.; Balling, R.; Erben, R.G. Impaired Insulin Secretory Capacity in Mice Lacking a Functional Vitamin D Receptor. FASEB J 2003, 17, 509–511. [CrossRef]
- Bouillon, R.; Carmeliet, G.; Verlinden, L.; van Etten, E.; Verstuyf, A.; Luderer, H.F.; Lieben, L.; Mathieu, C.; Demay, M. Vitamin D and Human Health: Lessons from Vitamin D Receptor Null Mice. Endocr Rev 2008, 29, 726–776. [CrossRef]
- Maestro, B.; Campión, J.; Dávila, N.; Calle, C. Stimulation by 1,25-Dihydroxyvitamin D3 of Insulin Receptor Expression and Insulin Responsiveness for Glucose Transport in U-937 Human Promonocytic Cells. Endocr J 2000, 47, 383–391. [CrossRef]
- Maestro, B.; Molero, S.; Bajo, S.; Dávila, N.; Calle, C. Transcriptional Activation of the Human Insulin Receptor Gene by 1,25-Dihydroxyvitamin D(3). Cell Biochem Funct 2002, 20, 227–232. [CrossRef]
- Pittas, A.G.; Harris, S.S.; Stark, P.C.; Dawson-Hughes, B. The Effects of Calcium and Vitamin D Supplementation on Blood Glucose and Markers of Inflammation in Nondiabetic Adults. Diabetes Care 2007, 30, 980–986. [CrossRef]
- Bland, R.; Markovic, D.; Hills, C.E.; Hughes, S.V.; Chan, S.L.F.; Squires, P.E.; Hewison, M. Expression of 25-Hydroxyvitamin D3-1alpha-Hydroxylase in Pancreatic Islets. J Steroid Biochem Mol Biol 2004, 89–90, 121–125. [CrossRef]
- Reusch, J.E.; Begum, N.; Sussman, K.E.; Draznin, B. Regulation of GLUT-4 Phosphorylation by Intracellular Calcium in Adipocytes. Endocrinology 1991, 129, 3269–3273. [CrossRef]
- Ryan, Z.C.; Craig, T.A.; Folmes, C.D.; Wang, X.; Lanza, I.R.; Schaible, N.S.; Salisbury, J.L.; Nair, K.S.; Terzic, A.; Sieck, G.C.; et al. 1α,25-Dihydroxyvitamin D3 Regulates Mitochondrial Oxygen Consumption and Dynamics in Human Skeletal Muscle Cells. J Biol Chem 2016, 291, 1514–1528. [CrossRef]
- Baron, A.D.; Brechtel, G.; Wallace, P.; Edelman, S.V. Rates and Tissue Sites of Non-Insulin- and Insulin-Mediated Glucose Uptake in Humans. Am J Physiol 1988, 255, E769-774. [CrossRef]
- DeFronzo, R.A.; Jacot, E.; Jequier, E.; Maeder, E.; Wahren, J.; Felber, J.P. The Effect of Insulin on the Disposal of Intravenous Glucose. Results from Indirect Calorimetry and Hepatic and Femoral Venous Catheterization. Diabetes 1981, 30, 1000–1007. [CrossRef]
- Jefferson, G.E.; Schnell, D.M.; Thomas, D.T.; Bollinger, L.M. Calcitriol Concomitantly Enhances Insulin Sensitivity and Alters Myocellular Lipid Partitioning in High Fat-Treated Skeletal Muscle Cells. J Physiol Biochem 2017, 73, 613–621. [CrossRef]
- Krul-Poel, Y.H.M.; Ter Wee, M.M.; Lips, P.; Simsek, S. MANAGEMENT OF ENDOCRINE DISEASE: The Effect of Vitamin D Supplementation on Glycaemic Control in Patients with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Eur J Endocrinol 2017, 176, R1–R14. [CrossRef]
- Earthman, C.P.; Beckman, L.M.; Masodkar, K.; Sibley, S.D. The Link between Obesity and Low Circulating 25-Hydroxyvitamin D Concentrations: Considerations and Implications. Int J Obes (Lond) 2012, 36, 387–396. [CrossRef]
- Bajaj, S.; Singh, R.P.; Dwivedi, N.C.; Singh, K.; Gupta, A.; Mathur, M. Vitamin D Levels and Microvascular Complications in Type 2 Diabetes. Indian J Endocrinol Metab 2014, 18, 537–541. [CrossRef]
- Zhao, J.; Dong, J.; Wang, H.; Shang, H.; Zhang, D.; Liao, L. Efficacy and Safety of Vitamin D3 in Patients with Diabetic Nephropathy: A Meta-Analysis of Randomized Controlled Trials. Chin Med J (Engl) 2014, 127, 2837–2843.
- Shehab, D.; Al-Jarallah, K.; Mojiminiyi, O.A.; Al Mohamedy, H.; Abdella, N.A. Does Vitamin D Deficiency Play a Role in Peripheral Neuropathy in Type 2 Diabetes? Diabet Med 2012, 29, 43–49. [CrossRef]
- Assy, M.H.; Draz, N.A.; Fathy, S.E.; Hamed, M.G. Impact of Vitamin D Level in Diabetic People with Peripheral Neuropathy. The Egyptian Journal of Neurology, Psychiatry and Neurosurgery 2021, 57, 117. [CrossRef]
- Al-Shoumer, K.A.; Al-Essa, T.M. Is There a Relationship between Vitamin D with Insulin Resistance and Diabetes Mellitus? World J Diabetes 2015, 6, 1057–1064. [CrossRef]
- Mohd Saffian, S.; Jamil, N.A.; Mohd Tahir, N.A.; Hatah, E. Vitamin D Insufficiency Is High in Malaysia: A Systematic Review and Meta-Analysis of Studies on Vitamin D Status in Malaysia. Front Nutr 2022, 9, 1050745. [CrossRef]
- Ding, Y.-H.; Wei, T.-M.; Qian, L.-Y.; Ma, Y.; Lao, D.-B.; Yao, B.; Pang, J. Association between Serum 25-Hydroxyvitamin D and Carotid Atherosclerotic Plaque in Chinese Type 2 Diabetic Patients. Medicine (Baltimore) 2017, 96, e6445. [CrossRef]
- Paschou, S.A.; Papadopoulou-Marketou, N.; Chrousos, G.P.; Kanaka-Gantenbein, C. On Type 1 Diabetes Mellitus Pathogenesis. Endocr Connect 2018, 7, R38–R46. [CrossRef]
- Soltesz, G.; Patterson, C.C.; Dahlquist, G.; EURODIAB Study Group Worldwide Childhood Type 1 Diabetes Incidence--What Can We Learn from Epidemiology? Pediatr Diabetes 2007, 8 Suppl 6, 6–14. [CrossRef]
- Cernea, S.; Dobreanu, M.; Raz, I. Prevention of Type 1 Diabetes: Today and Tomorrow. Diabetes Metab Res Rev 2010, 26, 602–605. [CrossRef]
- Huber, A.; Menconi, F.; Corathers, S.; Jacobson, E.M.; Tomer, Y. Joint Genetic Susceptibility to Type 1 Diabetes and Autoimmune Thyroiditis: From Epidemiology to Mechanisms. Endocr Rev 2008, 29, 697–725. [CrossRef]
- Mathieu, C.; Badenhoop, K. Vitamin D and Type 1 Diabetes Mellitus: State of the Art. Trends Endocrinol Metab 2005, 16, 261–266. [CrossRef]
- Takiishi, T.; Gysemans, C.; Bouillon, R.; Mathieu, C. Vitamin D and Diabetes. Endocrinol Metab Clin North Am 2010, 39, 419–446, table of contents. [CrossRef]
- Storm, T.L.; Sørensen, O.H.; Lund, B.; Lund, B.; Christiansen, J.S.; Andersen, A.R.; Lumholtz, I.B.; Parving, H.H. Vitamin D Metabolism in Insulin-Dependent Diabetes Mellitus. Metab Bone Dis Relat Res 1983, 5, 107–110. [CrossRef]
- Luong, K. vinh quoc; Nguyen, L.T.H.; Nguyen, D.N.P. The Role of Vitamin D in Protecting Type 1 Diabetes Mellitus. Diabetes Metab Res Rev 2005, 21, 338–346. [CrossRef]
- Danescu, L.G.; Levy, S.; Levy, J. Vitamin D and Diabetes Mellitus. Endocrine 2009, 35, 11–17. [CrossRef]
- Yang, C.-Y.; Leung, P.S.C.; Adamopoulos, I.E.; Gershwin, M.E. The Implication of Vitamin D and Autoimmunity: A Comprehensive Review. Clin Rev Allergy Immunol 2013, 45, 217–226. [CrossRef]
- Norris, J.M.; Johnson, R.K.; Stene, L.C. Type 1 Diabetes-Early Life Origins and Changing Epidemiology. Lancet Diabetes Endocrinol 2020, 8, 226–238. [CrossRef]
- Jiang, X.; Kiel, D.P.; Kraft, P. The Genetics of Vitamin D. Bone 2019, 126, 59–77. [CrossRef]
- Holick, M.F. Vitamin D Deficiency. N Engl J Med 2007, 357, 266–281. [CrossRef]
- Bikle, D.D. Vitamin D Metabolism, Mechanism of Action, and Clinical Applications. Chem Biol 2014, 21, 319–329. [CrossRef]
- Dankers, W.; Colin, E.M.; van Hamburg, J.P.; Lubberts, E. Vitamin D in Autoimmunity: Molecular Mechanisms and Therapeutic Potential. Front Immunol 2016, 7, 697. [CrossRef]
- Metabolic Bone Disease Available online: https://accessmedicine.mhmedical.com/content.aspx?sectionid=166248750&bookid=2178 (accessed on 23 August 2023).
- Penna, G.; Adorini, L. 1 Alpha,25-Dihydroxyvitamin D3 Inhibits Differentiation, Maturation, Activation, and Survival of Dendritic Cells Leading to Impaired Alloreactive T Cell Activation. J Immunol 2000, 164, 2405–2411. [CrossRef]
- Zhang, X.; Zhou, M.; Guo, Y.; Song, Z.; Liu, B. 1,25-Dihydroxyvitamin D₃ Promotes High Glucose-Induced M1 Macrophage Switching to M2 via the VDR-PPARγ Signaling Pathway. Biomed Res Int 2015, 2015, 157834. [CrossRef]
- Unger, W.W.J.; Laban, S.; Kleijwegt, F.S.; van der Slik, A.R.; Roep, B.O. Induction of Treg by Monocyte-Derived DC Modulated by Vitamin D3 or Dexamethasone: Differential Role for PD-L1. Eur J Immunol 2009, 39, 3147–3159. [CrossRef]
- Bock, G.; Prietl, B.; Mader, J.K.; Höller, E.; Wolf, M.; Pilz, S.; Graninger, W.B.; Obermayer-Pietsch, B.M.; Pieber, T.R. The Effect of Vitamin D Supplementation on Peripheral Regulatory T Cells and β Cell Function in Healthy Humans: A Randomized Controlled Trial. Diabetes Metab Res Rev 2011, 27, 942–945. [CrossRef]
- Lemire, J.M.; Adams, J.S.; Sakai, R.; Jordan, S.C. 1 Alpha,25-Dihydroxyvitamin D3 Suppresses Proliferation and Immunoglobulin Production by Normal Human Peripheral Blood Mononuclear Cells. J Clin Invest 1984, 74, 657–661. [CrossRef]
- Casteels, K.M.; Mathieu, C.; Waer, M.; Valckx, D.; Overbergh, L.; Laureys, J.M.; Bouillon, R. Prevention of Type I Diabetes in Nonobese Diabetic Mice by Late Intervention with Nonhypercalcemic Analogs of 1,25-Dihydroxyvitamin D3 in Combination with a Short Induction Course of Cyclosporin A. Endocrinology 1998, 139, 95–102. [CrossRef]
- Mathieu, C.; Waer, M.; Laureys, J.; Rutgeerts, O.; Bouillon, R. Prevention of Autoimmune Diabetes in NOD Mice by 1,25 Dihydroxyvitamin D3. Diabetologia 1994, 37, 552–558. [CrossRef]
- Zella, J.B.; McCary, L.C.; DeLuca, H.F. Oral Administration of 1,25-Dihydroxyvitamin D3 Completely Protects NOD Mice from Insulin-Dependent Diabetes Mellitus. Arch Biochem Biophys 2003, 417, 77–80. [CrossRef]
- Fronczak, C.M.; Barón, A.E.; Chase, H.P.; Ross, C.; Brady, H.L.; Hoffman, M.; Eisenbarth, G.S.; Rewers, M.; Norris, J.M. In Utero Dietary Exposures and Risk of Islet Autoimmunity in Children. Diabetes Care 2003, 26, 3237–3242. [CrossRef]
- Corrao, S.; Colomba, D.; Arnone, S.; Argano, C.; Di Chiara, T.; Scaglione, R.; Licata, G. Improving Efficacy of PubMed Clinical Queries for Retrieving Scientifically Strong Studies on Treatment. J Am Med Inform Assoc 2006, 13, 485–487. [CrossRef]
- Corrao, S.; Colomba, D.; Argano, C.; Calvo, L.; Scaglione, R.; Licata, G. Optimized Search Strategy for Detecting Scientifically Strong Studies on Treatment through PubMed. Intern Emerg Med 2012, 7, 283–287. [CrossRef]
- Hou, Y.; Song, A.; Jin, Y.; Xia, Q.; Song, G.; Xing, X. A Dose–Response Meta-Analysis between Serum Concentration of 25-Hydroxy Vitamin D and Risk of Type 1 Diabetes Mellitus. Eur J Clin Nutr 2021, 75, 1010–1023. [CrossRef]
- Bener, A.; Alsaied, A.; Al-Ali, M.; Al-Kubaisi, A.; Basha, B.; Abraham, A.; Guiter, G.; Mian, M. High Prevalence of Vitamin D Deficiency in Type 1 Diabetes Mellitus and Healthy Children. Acta Diabetol 2009, 46, 183–189. [CrossRef]
- Omar, D.F.; Kamal, M.M.; El-Hefnawy, M.H.; El-Mesallamy, H.O. Serum Vitamin D and Its Upregulated Protein, Thioredoxin Interacting Protein, Are Associated With Beta-Cell Dysfunction in Adult Patients With Type 1 and Type 2 Diabetes. Can J Diabetes 2018, 42, 588–594. [CrossRef]
- ALkharashi, N.A. Estimation of Vitamin D Deficiency Prevalence among Saudi Children in Armed Forces Hospital and Riyadh Care Hospital in Riyadh, Kingdom of Saudi Arabia and Its Relation to Type 1 Diabetes Mellitus. Saudi Med J 2019, 40, 1290–1293. [CrossRef]
- Hyppönen, E.; Läärä, E.; Reunanen, A.; Järvelin, M.R.; Virtanen, S.M. Intake of Vitamin D and Risk of Type 1 Diabetes: A Birth-Cohort Study. Lancet 2001, 358, 1500–1503. [CrossRef]
- Norris, J.M.; Lee, H.-S.; Frederiksen, B.; Erlund, I.; Uusitalo, U.; Yang, J.; Lernmark, Å.; Simell, O.; Toppari, J.; Rewers, M.; et al. Plasma 25-Hydroxyvitamin D Concentration and Risk of Islet Autoimmunity. Diabetes 2018, 67, 146–154. [CrossRef]
- Vitamin D Supplement in Early Childhood and Risk for Type I (Insulin-Dependent) Diabetes Mellitus. The EURODIAB Substudy 2 Study Group. Diabetologia 1999, 42, 51–54. [CrossRef]
- Wei, Z.; Yoshihara, E.; He, N.; Hah, N.; Fan, W.; Pinto, A.F.M.; Huddy, T.; Wang, Y.; Ross, B.; Estepa, G.; et al. Vitamin D Switches BAF Complexes to Protect β Cells. Cell 2018, 173, 1135-1149.e15. [CrossRef]
- Yu, J.; Sharma, P.; Girgis, C.M.; Gunton, J.E. Vitamin D and Beta Cells in Type 1 Diabetes: A Systematic Review. Int J Mol Sci 2022, 23, 14434. [CrossRef]
- Najjar, L.; Sutherland, J.; Zhou, A.; Hyppönen, E. Vitamin D and Type 1 Diabetes Risk: A Systematic Review and Meta-Analysis of Genetic Evidence. Nutrients 2021, 13, 4260. [CrossRef]
- von Websky, K.; Hasan, A.A.; Reichetzeder, C.; Tsuprykov, O.; Hocher, B. Impact of Vitamin D on Pregnancy-Related Disorders and on Offspring Outcome. J Steroid Biochem Mol Biol 2018, 180, 51–64. [CrossRef]
- American Diabetes Association 2. Classification and Diagnosis of Diabetes. Diabetes Care 2017, 40, S11–S24. [CrossRef]
- Jenum, A.K.; Mørkrid, K.; Sletner, L.; Vangen, S.; Torper, J.L.; Nakstad, B.; Voldner, N.; Rognerud-Jensen, O.H.; Berntsen, S.; Mosdøl, A.; et al. Impact of Ethnicity on Gestational Diabetes Identified with the WHO and the Modified International Association of Diabetes and Pregnancy Study Groups Criteria: A Population-Based Cohort Study. Eur J Endocrinol 2012, 166, 317–324. [CrossRef]
- Noctor, E.; Crowe, C.; Carmody, L.A.; Kirwan, B.; O’Dea, A.; Glynn, L.G.; McGuire, B.E.; O’Shea, P.M.; Dunne, F.P. ATLANTIC-DIP: Prevalence of Metabolic Syndrome and Insulin Resistance in Women with Previous Gestational Diabetes Mellitus by International Association of Diabetes in Pregnancy Study Groups Criteria. Acta Diabetol 2015, 52, 153–160. [CrossRef]
- Milajerdi, A.; Tehrani, H.; Haghighatdoost, F.; Larijani, B.; Surkan, P.J.; Azadbakht, L. Associations between Higher Egg Consumption during Pregnancy with Lowered Risks of High Blood Pressure and Gestational Diabetes Mellitus. Int J Vitam Nutr Res 2018, 88, 166–175. [CrossRef]
- Groof, Z.; Garashi, G.; Husain, H.; Owayed, S.; AlBader, S.; Mouhsen, H.; Mohammad, A.; Ziyab, A.H. Prevalence, Risk Factors, and Fetomaternal Outcomes of Gestational Diabetes Mellitus in Kuwait: A Cross-Sectional Study. Journal of Diabetes Research 2019, 2019, e9136250. [CrossRef]
- Verma, A.; Boney, C.M.; Tucker, R.; Vohr, B.R. Insulin Resistance Syndrome in Women with Prior History of Gestational Diabetes Mellitus. J Clin Endocrinol Metab 2002, 87, 3227–3235. [CrossRef]
- Andersson-Hall, U.; Gustavsson, C.; Pedersen, A.; Malmodin, D.; Joelsson, L.; Holmäng, A. Higher Concentrations of BCAAs and 3-HIB Are Associated with Insulin Resistance in the Transition from Gestational Diabetes to Type 2 Diabetes. J Diabetes Res 2018, 2018, 4207067. [CrossRef]
- Nutrition Therapy in Gestational Diabetes Mellitus: Time to Move Forward | Diabetes Care | American Diabetes Association Available online: https://diabetesjournals.org/care/article/41/7/1343/36441/Nutrition-Therapy-in-Gestational-Diabetes-Mellitus (accessed on 23 August 2023).
- Ismail, N.A.; Mohamed Ismail, N.A.; Bador, K.M. Vitamin D in Gestational Diabetes Mellitus and Its Association with Hyperglycaemia, Insulin Sensitivity and Other Factors. J Obstet Gynaecol 2021, 41, 899–903. [CrossRef]
- Magnusdottir, K.S.; Tryggvadottir, E.A.; Magnusdottir, O.K.; Hrolfsdottir, L.; Halldorsson, T.I.; Birgisdottir, B.E.; Hreidarsdottir, I.T.; Hardardottir, H.; Gunnarsdottir, I. Vitamin D Status and Association with Gestational Diabetes Mellitus in a Pregnant Cohort in Iceland. Food & nutrition Research 2021. [CrossRef]
- Agüero-Domenech, N.; Jover, S.; Sarrión, A.; Baranda, J.; Quesada-Rico, J.A.; Pereira-Expósito, A.; Gil-Guillén, V.; Cortés-Castell, E.; García-Teruel, M.J. Vitamin D Deficiency and Gestational Diabetes Mellitus in Relation to Body Mass Index. Nutrients 2021, 14, 102. [CrossRef]
- Khambule, L.; George, J.A. The Role of Inflammation in the Development of GDM and the Use of Markers of Inflammation in GDM Screening. Adv Exp Med Biol 2019, 1134, 217–242. [CrossRef]
- Wolf, M.; Sauk, J.; Shah, A.; Vossen Smirnakis, K.; Jimenez-Kimble, R.; Ecker, J.L.; Thadhani, R. Inflammation and Glucose Intolerance: A Prospective Study of Gestational Diabetes Mellitus. Diabetes Care 2004, 27, 21–27. [CrossRef]
- López-Tinoco, C.; Roca, M.; García-Valero, A.; Murri, M.; Tinahones, F.J.; Segundo, C.; Bartha, J.L.; Aguilar-Diosdado, M. Oxidative Stress and Antioxidant Status in Patients with Late-Onset Gestational Diabetes Mellitus. Acta Diabetol 2013, 50, 201–208. [CrossRef]
- Shang, M.; Zhao, J.; Yang, L.; Lin, L. Oxidative Stress and Antioxidant Status in Women with Gestational Diabetes Mellitus Diagnosed by IADPSG Criteria. Diabetes Res Clin Pract 2015, 109, 404–410. [CrossRef]
- Peuchant, E.; Brun, J.-L.; Rigalleau, V.; Dubourg, L.; Thomas, M.-J.; Daniel, J.-Y.; Leng, J.-J.; Gin, H. Oxidative and Antioxidative Status in Pregnant Women with Either Gestational or Type 1 Diabetes. Clin Biochem 2004, 37, 293–298. [CrossRef]
- Grissa, O.; Atègbo, J.-M.; Yessoufou, A.; Tabka, Z.; Miled, A.; Jerbi, M.; Dramane, K.L.; Moutairou, K.; Prost, J.; Hichami, A.; et al. Antioxidant Status and Circulating Lipids Are Altered in Human Gestational Diabetes and Macrosomia. Transl Res 2007, 150, 164–171. [CrossRef]
- Maged, A.M.; Torky, H.; Fouad, M.A.; GadAllah, S.H.; Waked, N.M.; Gayed, A.S.; Salem, A.K. Role of Antioxidants in Gestational Diabetes Mellitus and Relation to Fetal Outcome: A Randomized Controlled Trial. J Matern Fetal Neonatal Med 2016, 29, 4049–4054. [CrossRef]
- Haidari, F.; Zakerkish, M.; Karandish, M.; Saki, A.; Pooraziz, S. Association between Serum Vitamin D Level and Glycemic and Inflammatory Markers in Non-Obese Patients with Type 2 Diabetes. Iran J Med Sci 2016, 41, 367–373.
- Wang, W.; Zhang, J.; Wang, H.; Wang, X.; Liu, S. Vitamin D Deficiency Enhances Insulin Resistance by Promoting Inflammation in Type 2 Diabetes. Int J Clin Exp Pathol 2019, 12, 1859–1867.
- Berridge, M.J. Vitamin D Deficiency and Diabetes. Biochem J 2017, 474, 1321–1332. [CrossRef]
- Johannesson, B.; Sui, L.; Freytes, D.O.; Creusot, R.J.; Egli, D. Toward Beta Cell Replacement for Diabetes. EMBO J 2015, 34, 841–855. [CrossRef]
- Taheri, E.; Saedisomeolia, A.; Djalali, M.; Qorbani, M.; Madani Civi, M. The Relationship between Serum 25-Hydroxy Vitamin D Concentration and Obesity in Type 2 Diabetic Patients and Healthy Subjects. J Diabetes Metab Disord 2012, 11, 16. [CrossRef]
- Milajerdi, A.; Abbasi, F.; Mousavi, S.M.; Esmaillzadeh, A. Maternal Vitamin D Status and Risk of Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. Clin Nutr 2021, 40, 2576–2586. [CrossRef]
- Wu, C.; Song, Y.; Wang, X. Vitamin D Supplementation for the Outcomes of Patients with Gestational Diabetes Mellitus and Neonates: A Meta-Analysis and Systematic Review. Int J Clin Pract 2023, 2023, 1907222. [CrossRef]
- Akbari, M.; Moosazaheh, M.; Lankarani, K.B.; Tabrizi, R.; Samimi, M.; Karamali, M.; Jamilian, M.; Kolahdooz, F.; Asemi, Z. The Effects of Vitamin D Supplementation on Glucose Metabolism and Lipid Profiles in Patients with Gestational Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Horm Metab Res 2017, 49, 647–653. [CrossRef]
- Wang, H.; Xia, N.; Yang, Y.; Peng, D.-Q. Influence of Vitamin D Supplementation on Plasma Lipid Profiles: A Meta-Analysis of Randomized Controlled Trials. Lipids Health Dis 2012, 11, 42. [CrossRef]
- Kron-Rodrigues, M.R.; Rudge, M.V.C.; Lima, S.A.M. Supplementation of Vitamin D in the Postdelivery Period of Women with Previous Gestational Diabetes Mellitus: Systematic Review and Meta-Analysis of Randomized Trials. Rev Bras Ginecol Obstet 2021, 43, 699–709. [CrossRef]
- Saha, S.; Saha, S. Changes in Anthropometric and Blood 25-Hydroxyvitamin D Measurements in Antenatal Vitamin Supplemented Gestational Diabetes Mellitus Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Turk Ger Gynecol Assoc 2021, 22, 217–234. [CrossRef]
- Wang, M.M.; Chen, Z.J.; Wang, Y.; Xu, X.R.; Li, H.J.; Yang, J. [Effects of Vitamin D Supplementation on Serum Lipid Profiles and Neonatal Outcomes in Gestational Diabetes Mellitus:a Meta-analysis]. Zhongguo Yi Xue Ke Xue Yuan Xue Bao 2021, 43, 82–91. [CrossRef]
- Yang, C.; Jing, W.; Ge, S.; Sun, W. Vitamin D Status and Vitamin D Deficiency Risk Factors among Pregnancy of Shanghai in China. BMC Pregnancy and Childbirth 2021, 21, 431. [CrossRef]
- Chatzakis, C.; Sotiriadis, A.; Tsakmaki, E.; Papagianni, M.; Paltoglou, G.; Dinas, K.; Mastorakos, G. The Effect of Dietary Supplements on Oxidative Stress in Pregnant Women with Gestational Diabetes Mellitus: A Network Meta-Analysis. Nutrients 2021, 13, 2284. [CrossRef]
- Wang, L.; Zhang, C.; Song, Y.; Zhang, Z. Serum Vitamin D Deficiency and Risk of Gestational Diabetes Mellitus: A Meta-Analysis. Arch Med Sci 2020, 16, 742–751. [CrossRef]
- Jin, S.; Sha, L.; Dong, J.; Yi, J.; Liu, Y.; Guo, Z.; Hu, B. Effects of Nutritional Strategies on Glucose Homeostasis in Gestational Diabetes Mellitus: A Systematic Review and Network Meta-Analysis. J Diabetes Res 2020, 2020, 6062478. [CrossRef]
- Soheilykhah, S.; Mojibian, M.; Rashidi, M.; Rahimi-Saghand, S.; Jafari, F. Maternal Vitamin D Status in Gestational Diabetes Mellitus. Nutr Clin Pract 2010, 25, 524–527. [CrossRef]
- Vitamin D and Gestational Diabetes Mellitus: A Systematic Review Based on Data Free of Hawthorne Effect - Zhang - 2018 - BJOG: An International Journal of Obstetrics & Gynaecology - Wiley Online Library Available online: https://obgyn.onlinelibrary.wiley.com/doi/abs/10.1111/1471-0528.15060 (accessed on 23 August 2023).
- Vaidya, A.; Williams, J.S. Vitamin D and Insulin Sensitivity: Can Gene Association and Pharmacogenetic Studies of the Vitamin D Receptor Provide Clarity? Metabolism 2012, 61, 759–761. [CrossRef]
- Lu, M.; Xu, Y.; Lv, L.; Zhang, M. Association between Vitamin D Status and the Risk of Gestational Diabetes Mellitus: A Meta-Analysis. Arch Gynecol Obstet 2016, 293, 959–966. [CrossRef]
- Chen, Y.; Zhu, B.; Wu, X.; Li, S.; Tao, F. Association between Maternal Vitamin D Deficiency and Small for Gestational Age: Evidence from a Meta-Analysis of Prospective Cohort Studies. BMJ Open 2017, 7, e016404. [CrossRef]
- Licata, G.; Argano, C.; Di Chiara, T.; Parrinello, G.; Scaglione, R. Obesity: a main factor of metabolic syndrome? Panminerva Med. 2006 Jun;48(2):77-85. PMID: 16953145.
- Fahed, G.; Aoun, L.; Bou Zerdan, M.; Allam, S.; Bou Zerdan, M.; Bouferraa, Y.; Assi, H.I. Metabolic Syndrome: Updates on Pathophysiology and Management in 2021. Int J Mol Sci 2022, 23, 786. [CrossRef]
- 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2022 | Diabetes Care | American Diabetes Association Available online: https://diabetesjournals.org/care/article/45/Supplement_1/S17/138925/2-Classification-and-Diagnosis-of-Diabetes (accessed on 23 August 2023).
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, Regional, and National Life Expectancy, All-Cause Mortality, and Cause-Specific Mortality for 249 Causes of Death, 1980–2015: A Systematic Analysis for the Global Burden of Disease Study 2015. The Lancet 2016, 388, 1459–1544. [CrossRef]
- Zhu, Y.; Xian, X.; Wang, Z.; Bi, Y.; Chen, Q.; Han, X.; Tang, D.; Chen, R. Research Progress on the Relationship between Atherosclerosis and Inflammation. Biomolecules 2018, 8, 80. [CrossRef]
- Hojs, R.; Ekart, R.; Bevc, S.; Hojs, N. Markers of Inflammation and Oxidative Stress in the Development and Progression of Renal Disease in Diabetic Patients. Nephron 2016, 133, 159–162. [CrossRef]
- Flaim, C.; Kob, M.; Di Pierro, A.M.; Herrmann, M.; Lucchin, L. Effects of a Whey Protein Supplementation on Oxidative Stress, Body Composition and Glucose Metabolism among Overweight People Affected by Diabetes Mellitus or Impaired Fasting Glucose: A Pilot Study. J Nutr Biochem 2017, 50, 95–102. [CrossRef]
- Mannarino, E.; Pirro, M. Molecular Biology of Atherosclerosis. Clin Cases Miner Bone Metab 2008, 5, 57–62.
- Hussin, A.M.; Ashor, A.W.; Schoenmakers, I.; Hill, T.; Mathers, J.C.; Siervo, M. Effects of Vitamin D Supplementation on Endothelial Function: A Systematic Review and Meta-Analysis of Randomised Clinical Trials. Eur J Nutr 2017, 56, 1095–1104. [CrossRef]
- Jacobson, T.A.; Maki, K.C.; Orringer, C.E.; Jones, P.H.; Kris-Etherton, P.; Sikand, G.; La Forge, R.; Daniels, S.R.; Wilson, D.P.; Morris, P.B.; et al. National Lipid Association Recommendations for Patient-Centered Management of Dyslipidemia: Part 2. J Clin Lipidol 2015, 9, S1-122.e1. [CrossRef]
- Cholesterol Treatment Trialists’ (CTT) Collaboration; Fulcher, J.; O’Connell, R.; Voysey, M.; Emberson, J.; Blackwell, L.; Mihaylova, B.; Simes, J.; Collins, R.; Kirby, A.; et al. Efficacy and Safety of LDL-Lowering Therapy among Men and Women: Meta-Analysis of Individual Data from 174,000 Participants in 27 Randomised Trials. Lancet 2015, 385, 1397–1405. [CrossRef]
- Bovolini, A.; Garcia, J.; Andrade, M.A.; Duarte, J.A. Metabolic Syndrome Pathophysiology and Predisposing Factors. Int J Sports Med 2021, 42, 199–214. [CrossRef]
- Castro-Barquero, S.; Ruiz-León, A.M.; Sierra-Pérez, M.; Estruch, R.; Casas, R. Dietary Strategies for Metabolic Syndrome: A Comprehensive Review. Nutrients 2020, 12, 2983. [CrossRef]
- Pan, G.-T.; Guo, J.-F.; Mei, S.-L.; Zhang, M.-X.; Hu, Z.-Y.; Zhong, C.-K.; Zeng, C.-Y.; Liu, X.-H.; Ma, Q.-H.; Li, B.-Y.; et al. Vitamin D Deficiency in Relation to the Risk of Metabolic Syndrome in Middle-Aged and Elderly Patients with Type 2 Diabetes Mellitus. J Nutr Sci Vitaminol (Tokyo) 2016, 62, 213–219. [CrossRef]
- Faraji, S.; Alizadeh, M. Mechanistic Effects of Vitamin D Supplementation on Metabolic Syndrome Components in Patients with or without Vitamin D Deficiency. J Obes Metab Syndr 2020, 29, 270–280. [CrossRef]
- Sepidarkish, M.; Farsi, F.; Akbari-Fakhrabadi, M.; Namazi, N.; Almasi-Hashiani, A.; Maleki Hagiagha, A.; Heshmati, J. The Effect of Vitamin D Supplementation on Oxidative Stress Parameters: A Systematic Review and Meta-Analysis of Clinical Trials. Pharmacol Res 2019, 139, 141–152. [CrossRef]
- Jain, S.K.; Micinski, D. Vitamin D Upregulates Glutamate Cysteine Ligase and Glutathione Reductase, and GSH Formation, and Decreases ROS and MCP-1 and IL-8 Secretion in High-Glucose Exposed U937 Monocytes. Biochem Biophys Res Commun 2013, 437, 7–11. [CrossRef]
- Brandenburg, V.M.; Vervloet, M.G.; Marx, N. The Role of Vitamin D in Cardiovascular Disease: From Present Evidence to Future Perspectives. Atherosclerosis 2012, 225, 253–263. [CrossRef]
- Siti, H.N.; Kamisah, Y.; Kamsiah, J. The Role of Oxidative Stress, Antioxidants and Vascular Inflammation in Cardiovascular Disease (a Review). Vascul Pharmacol 2015, 71, 40–56. [CrossRef]
- Sies, H. Total Antioxidant Capacity: Appraisal of a Concept. J Nutr 2007, 137, 1493–1495. [CrossRef]
- Namazi, N.; Larijani, B.; Azadbakht, L. Alpha-Lipoic Acid Supplement in Obesity Treatment: A Systematic Review and Meta-Analysis of Clinical Trials. Clin Nutr 2018, 37, 419–428. [CrossRef]
- Heshmati, J.; Farsi, F.; Shokri, F.; Rezaeinejad, M.; Almasi-Hashiani, A.; Vesali, S.; Sepidarkish, M. A Systematic Review and Meta-Analysis of the Probiotics and Synbiotics Effects on Oxidative Stress. Journal of Functional Foods 2018, 46, 66–84. [CrossRef]
- Slominski, A.T.; Kim, T.-K.; Hobrath, J.V.; Janjetovic, Z.; Oak, A.S.W.; Postlethwaite, A.; Lin, Z.; Li, W.; Takeda, Y.; Jetten, A.M.; et al. Characterization of a New Pathway That Activates Lumisterol in Vivo to Biologically Active Hydroxylumisterols. Sci Rep 2017, 7, 11434. [CrossRef]
- Mahmood, S.F.; Idiculla, J.; Joshi, R.; Joshi, S.; Kulkarni, S. Vitamin D Supplementation in Adults with Vitamin D Deficiency and Its Effect on Metabolic Syndrome - A Randomized Controlled Study. Int J Vitam Nutr Res 2016, 86, 121–126. [CrossRef]
- Teixeira, J.S.; Bull Ferreira Campos, A.; Cordeiro, A.; Pereira, S.E.; Saboya, C.J.; Ramalho, A. Vitamin D Nutritional Status and Its Relationship with Metabolic Changes in Adolescents and Adults with Severe Obesity. Nutr Hosp 2018, 35, 847–853. [CrossRef]
- Ferreira, P.P.; Cangussu, L.; Bueloni-Dias, F.N.; Orsatti, C.L.; Schmitt, E.B.; Nahas-Neto, J.; Nahas, E. a. P. Vitamin D Supplementation Improves the Metabolic Syndrome Risk Profile in Postmenopausal Women. Climacteric 2020, 23, 24–31. [CrossRef]
- Xu, Y.; Zhou, Y.; Liu, J.; Wang, C.; Qu, Z.; Wei, Z.; Zhou, D. Genetically Increased Circulating 25(OH)D Level Reduces the Risk of Type 2 Diabetes in Subjects with Deficiency of Vitamin D. Medicine (Baltimore) 2020, 99, e23672. [CrossRef]
- Zhu, W.; Heil, D.P. Associations of Vitamin D Status with Markers of Metabolic Health: A Community-Based Study in Shanghai, China. Diabetes Metab Syndr 2018, 12, 727–732. [CrossRef]
- Jafari, T.; Fallah, A.A.; Barani, A. Effects of Vitamin D on Serum Lipid Profile in Patients with Type 2 Diabetes: A Meta-Analysis of Randomized Controlled Trials. Clin Nutr 2016, 35, 1259–1268. [CrossRef]
- Li, X.; Liu, Y.; Zheng, Y.; Wang, P.; Zhang, Y. The Effect of Vitamin D Supplementation on Glycemic Control in Type 2 Diabetes Patients: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 375. [CrossRef]
- Wu, Z.; Wang, T.; Zhu, S.; Li, L. Effects of Vitamin D Supplementation as an Adjuvant Therapy in Coronary Artery Disease Patients. Scand Cardiovasc J 2016, 50, 9–16. [CrossRef]
- Ganji, V.; Sukik, A.; Alaayesh, H.; Rasoulinejad, H.; Shraim, M. Serum Vitamin D Concentrations Are Inversely Related to Prevalence of Metabolic Syndrome in Qatari Women. Biofactors 2020, 46, 180–186. [CrossRef]
- Wang, N.; Wang, C.; Chen, X.; Wan, H.; Chen, Y.; Chen, C.; Han, B.; Lu, Y. Vitamin D, Prediabetes and Type 2 Diabetes: Bidirectional Mendelian Randomization Analysis. Eur J Nutr 2020, 59, 1379–1388. [CrossRef]
- Zheng, J.-S.; Luan, J.; Sofianopoulou, E.; Sharp, S.J.; Day, F.R.; Imamura, F.; Gundersen, T.E.; Lotta, L.A.; Sluijs, I.; Stewart, I.D.; et al. The Association between Circulating 25-Hydroxyvitamin D Metabolites and Type 2 Diabetes in European Populations: A Meta-Analysis and Mendelian Randomisation Analysis. PLoS Med 2020, 17, e1003394. [CrossRef]
- Ostadmohammadi, V.; Milajerdi, A.; Ghayour-Mobarhan, M.; Ferns, G.; Taghizadeh, M.; Badehnoosh, B.; Mirzaei, H.; Asemi, Z. The Effects of Vitamin D Supplementation on Glycemic Control, Lipid Profiles and C-Reactive Protein Among Patients with Cardiovascular Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Curr Pharm Des 2019, 25, 201–210. [CrossRef]
- Qi, K.-J.; Zhao, Z.-T.; Zhang, W.; Yang, F. The Impacts of Vitamin D Supplementation in Adults with Metabolic Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Frontiers in Pharmacology 2022, 13.
- de Paula, T.P.; Kramer, C.K.; Viana, L.V.; Azevedo, M.J. Effects of Individual Micronutrients on Blood Pressure in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Sci Rep 2017, 7, 40751. [CrossRef]
- McGreevy, C.; Williams, D. New Insights about Vitamin D and Cardiovascular Disease: A Narrative Review. Ann Intern Med 2011, 155, 820–826. [CrossRef]
- Grossman, E. Ambulatory Blood Pressure Monitoring in the Diagnosis and Management of Hypertension. Diabetes Care 2013, 36 Suppl 2, S307-311. [CrossRef]
- Hajhashemy, Z.; Shahdadian, F.; Moslemi, E.; Mirenayat, F.S.; Saneei, P. Serum Vitamin D Levels in Relation to Metabolic Syndrome: A Systematic Review and Dose-Response Meta-Analysis of Epidemiologic Studies. Obes Rev 2021, 22, e13223. [CrossRef]

Table 1.
Synthesis of Meta-Analyses and Systematic Reviews on the effectiveness of various dosages of vitamin D administration in pathologic conditions analyzed.
Table 1.
Synthesis of Meta-Analyses and Systematic Reviews on the effectiveness of various dosages of vitamin D administration in pathologic conditions analyzed.
| AUTHOR/YEAR | DESIGN | DURATION | PARTICIPANTS (I/C) |
DOSE OF VITAMIN D | RESULTS |
|---|---|---|---|---|---|
| VITAMIN D AND INSULIN-RESISTANCE (IR) | |||||
|
Asbaghi et al. 2019 46 |
MT (12 RCTs) | From 6 to 312 weeks | 8946 healthy subjects or patients with overweight/obesity, IFG, prediabetes, GDM, T2DM, PCOS, HIV infection (4395/4551) |
From 200 IU/day Vitamin D3 to 50.000 IU/week Vitamin D3 (with supplementation dose of calcium, that ranged from 500 mg/day to 1000 mg/day) | Reducing effects on FBG, circulating levels of insulin and HOMA-IR |
| Sindhughosa et al. 2022 41 | MT (7 RCTs) | From 10 to 52 weeks | 735 patients with NAFLD (423/312) | From 1.000 IU/day Vitamin D3 to 50.000 IU/week Vitamin D3 | Improvement on IR (marked by decrease of HOMA-IR), decrement in ALT levels |
| Pienkowska et al. 202329 | SR (8 RCTs) | From 12 to 260 weeks | From 66 to 2423 patients with prediabetes | From 1.000 IU/day Vitamin D3 to 88.000 IU/week Vitamin D3 | Only one trial showed improvements in FBG and HOMA-IR |
| VITAMIN D AND TYPE 2 DIABETES MELLITUS (T2DM) | |||||
|
Pittas et al. 2007 59 |
MT (13 Case Control Studies; 15 Cross-sectional studies; 12 RCTs) | N/A | Patients with T2DM or prediabetes | 2.000 IU/day Vitamin D3 or Vitamin D3 700 IU/day with supplementation dose of 500 mg/day calcium citrate |
Vitamin D and calcium insufficiency may negatively influence glycemia, whereas combined supplementation with both nutrients may be beneficial in optimizing glucose metabolism |
| Krul-Poel et al. 2017 84 | MT (23 RCTs) | From 4 to 52 weeks | 1797 patients with T2DM: for the effect on HbA1c 1475 patients (755/720), for the effect on FBG 1180 patients (608/572) | From 1.000 IU/day Vitamin D3 to 45.000 IU/week Vitamina D3 or 11.200 IU/day Vitamin D3 for 2 weeks followed by 5.600 IU/day for 10 weeks or from 100.000 to 300.000 IU Vitamin D3 single dose | Significant effect on FBG in a subgroup of studies (n = 4); no significant effect in change of HbA1c |
| Mirhosseini et al. 2018 55 | MT (28 RCTs) | From 8 to 260 weeks | 3848 healthy subjects or patients with prediabetes and/or overweight or obesity, NAFLD, arterial hypertension, cervical intraepithelial neoplasia, premenopausal and postmenopausal women | From 420 IU/day to 88.880 IU/week Vitamin D3 | Significant reduction in HbA1c, FBG and HOMA-IR |
|
Hu et al. 2019 64 |
MT (19 RCTs) | From 4 to 24 weeks | 1374 patients with T2DM (747/627) |
Up to 50.000 UI/weekly Vitamin D3 or 300.000 UI single injection Vitamin D3 | Significant reduction in HbA1c, IR (marked by decrease of HOMA-IR) and insulin levels in the short-term vitamin D supplementation group |
| VITAMIN D AND TYPE 1 DIABETES MELLITUS (T1DM) | |||||
| Najjar et al. 2021129 | MT (10 studies: 3 Cohort; 5 Case-control; 2 Matched case-control) |
N/A | 39884 patients with T1DM (16370/23514) |
N/A | No large effect of a genetically determined reduction in 25(OH)D concentrations by selected polymorphisms on T1D risk |
|
Hou et al. 2021120 |
MT (16 studies: 12 case-control studies; 1 cross-sectional case-control study; 2 nested case- control study; 1 case-cohort study) |
N/A | 10605 patients with T1DM (3913/6692) | N/A | Results demonstrated a significant inverse association between the 25(OH)D concentration in circulation and the risk of T1DM |
|
Yu et al. 2022 128 |
SR (13 studies: 9 RCTs; 2 Open label case-control; 1 Open label; 1 Cohort ) |
From 4 to 12 weeks | 527 patients with T1DM | The following therapeutic regimens were used: 1,25D 0.25 μg 2nd daily; 25D 2.000 IU daily; 25D to achieve serum 25D > 125 nmol/L; Alfacalcidol 0,25 μg bd 25D; 60.000 IU monthly; Ergocalciferol (D2) 2 m of 50.000 IU/w; 25D 2.000 IU/d; 25D. 3.000 IU/d; Calciferol 2.000 IU/d + etanercept + GAD-alum |
The maintenance of optimal circulating 25D levels may reduce the risk of T1D and that it may have potential for benefits in delaying the development of absolute or near-absolute C-peptide deficiency |
| VITAMIN D AND GESTATIONAL DIABETES MELLITUS (GDM) | |||||
|
Rodrigues et al. 2019 158 |
MT (6 studies RCTs) | From 6 to 24 weeks and a study until delivery | 456 pregnant women with GDM diagnosed in the second or third trimester of pregnancy |
50.000 IU of vitamin D3 every 2 weeks or 1.000 UI daily |
Improves adverse maternal and neonatal outcomes related to GDM |
|
Milajerdi et al. 2021 134 |
MT (29 studies: 18 Cohort; 9 Nested case-control;1 Prospective cross-sectional; 1 Retrospective cohort) |
N/A | 42668 patients with GDM or not | Blood vitamin D levels | The lowest risk of GDM was found among those with a serum vitamin D levels of 40 and 90 nmol/L |
|
Wang et al. 2021 44 |
MT (19 RCTs of these 13 concerned GDM) | From 6 to 12 weeks | 1198 patients with GDM | From 50.000 IU of vitamin D3 2 times/day to 1.200 IU daily |
The results showed that vitamin D supplementation during pregnancy could significantly reduce maternal cesarean section rate, maternal hospitalization rate, and postpartum hemorrhage in women with GDM |
|
Chatzakis et al 2021 162 |
MT (15 studies: 9 Cohort; 6 Nested case- control) |
N/A | 42636 pregnant women (1848/40788) |
Blood vitamin D levels | The result showed that lower levels of serum 25(OH)D were associated with a higher chance of GDM |
|
Wu et al. 2023 155 |
MT (20 studies RCTs) | From 2 to 16 weeks | 1682 pregnant women with GDM diagnosed (837/845) |
From 50.000 IU of vitamin D3 2 times/day to 1.200 IU daily |
Reduce serum LDL-C, TG, and TC levels and increase the serum HDL-C level. Reduce maternal and neonatal hyperbilirubinemia and hospitalization risk. |
| VITAMIN D, METABOLIC SYNDROME (MetS) AND CARDIOVASCULAR DISEASE (CVD) | |||||
|
De Paula TP et al. 2017 205 |
MT (7 RCTs) | From 3 to 52 weeks | 542 patients with T2DM (472/70) | A single dose of vitamin D2 (100.000 IU) or vitamin D3 (100.000 IU or 200.000 IU) | Reduction in BP, especially in systolic BP |
|
Ostadmohammadi et al. 2019 203 |
MT (8 RCTs) | From 8 to 24 weeks | 630 adults with CVD (305/325) | 50.000 IU/week Vitamin D3 or 50.000 IU every two weeks or 300.000 IU single dose |
Improving glycemic control, HDL-C and CRP levels; it did not affect TG, TC and LDL-C levels |
|
Hajhashemy Z et al. 2021208 |
Dose–response MT (43 epidemiological studies: 38 cross-sectional 1 nested case control, and 4 cohorts studies) |
N/A | 309.206 adults with o without MetS | Blood Vitamin D levels in adults | Inverse association between serum vitamin D concentrations and risk of MetS |
|
Qi KJ et al. 2022 204 |
MT (13 RCTs) | From 8 to 24 weeks | 1.076 adults with MetS (530/546) | From 1.000 IU/day Vitamin D3 to 50.000 IU/week | Decreased BP, FPG, HOMA-IR and CRP levels; it did not affect HDL-C, LDL-C, TC, and TG levels |
I/C: Intervention/Control; IR: Insulin-Resistance; MT: Meta-Analysis; RCT: Randomized Controlled Trials; IFG: Impaired fasting Glucose; GDM: Gestational Diabetes Mellitus; T2DM: Type 2 Diabetes Mellitus; PCOS: PolyCystic Ovary Syndrome; FBG: Fasting Blood Glucose; HOMA-IR: Homeostatic Model Assessment of Insulin Resistance; NAFLD: Non-alcoholic Fatty Liver Disease; HbA1c: Glycated Hemoglobin; SR: Systematic Review; IR: Insulin-Resistance; T1DM: Type 1 Diabetes Mellitus; N/A: Not Applicable; MetS: Metabolic Syndrome; CVD: Cardiovascular Disease; BP: Blood Pressure; TG: Triglycerides; TC: Total-cholesterol; LDL-C: LDL-cholesterol; HDL-C: HDL-cholesterol; CRP: C-Reactive Protein.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



