
Submitted:
11 September 2023
Posted:
12 September 2023
You are already at the latest version
Abstract
Cancer theragnostics is a novel approach that combines diagnostic imaging and radionuclide therapy. It is based on the use of a pair of radiopharmaceuticals, one optimized for positron emission tomography imaging, through linkage to a proper radionuclide, and the other bearing a beta-emitter isotope that can induce significant damage to cancer cells. In recent years, the use of theragnostics in nuclear medicine clinical practice has increased considerably, and thus investigation has focused on the identification of novel radionuclides that can bind to molecular targets which are typically dysregulated in different cancers. The major advantages of the theragnostic approach include elimination of multi-step procedures, reduced adverse effects to normal tissues, early diagnosis, better predicting responses and personalized patient care. This review aims to discuss emerging theragnostic molecules that have been investigated in a series of human malignancies, including gliomas, thyroid cancer, neuroendocrine tumors, cholangiocarcinoma and prostate cancer, as well as potent and recently introduced molecular targets, like cell-surface receptors, kinases, and cell adhesion proteins. Furthermore, special reference has been made to copper radionuclides as theragnostic agents, and their radiopharmaceutical applications since they present promising alternatives to the well-studied gallium-68 and lutetium-177.
Keywords:
Theragnostics
; nuclear medicine
; thyroid cancer
; neuroendocrine tumors
; prostate cancer
; colorectal cancer
; cholangiocarcinoma
; glioma
1. Introduction
Cancer consists of one primary cause of death globally. Given its recurring and lethal nature, its cure remains unsuccessful for most patients. In recent years there has been a great expansion of theragnostics, which consists of a comprehensive therapeutic process that encompasses identification of the cancer using a specific radioactive molecule that binds to the tumor, following by the administration of a similar radioactive molecule designed to kill the malignant cells (Figure 1). In addition, another diagnostic post-therapy scan is usually performed that confirms the therapeutic response of the selected sites [1]. In certain cases, nuclear theragnostic agents with comparable molecular features are utilized, whereas in others, theragnostic compounds that are not biologically similar but have equal biodistribution are used [2]. The rapid evolving field of theragnostics includes some already approved treatments such as 177Lu-PSMA (prostate-specific membrane antigen) for prostate cancer, 223Ra for osseous metastases, 177Lu-DOTATATE for neuroendocrine tumors, and 131I for thyroid cancer, and several other which are under development [3].The concept of theragnostics was initiated at the early days of nuclear medicine.
One such example represents the administration of iodine-131 followed by SPECT to diagnose thyroid cancer and subsequent administration of higher dose of the same radioactive molecule to attack and extinguish the cancer. However, during the last two decades there has been tremendous progress in the actual construction and development of theragnostic molecules for personalized cancer diagnosis and therapy [4]. Examples of such recent molecules include [68Ga/177Lu]-labeled somatostatin peptides for theragnostics of neuroendocrine tumors. A similar molecule, [68Ga/177Lu] PSMA, may be used for metastatic prostate cancer. While these applications are very promising, there are significant practical challenges that must be solved for creative theragnostics to be implemented. For instance, the biodistribution of the theragnostic drugs should demonstrate adequate accumulation in the tumor, but very low concentration in the normal tissues; the diagnostic and therapeutic radionuclide half-lives must be appropriate for imaging and targeted cell killing, respectively; finally, the therapeutic radionuclides should be available to the patient within the time frame suggested by half-life and stability. In any event, recent evidence suggests that theragnostics is becoming an important contribution to cancer therapy [4]. In the present review we summarize recent theragnostic molecules that have been investigated in various types of malignancies.
2. Theragnostics
2.1. Thyroid cancer
Usage of theragnostics in thyroid cancer comprises a combination of a diagnostic scan to localize the primary thyroid tumor and any metastases prior to surgically removed of the thyroid tumor and subsequent targeted 131I therapy to treat any remaining macroscopic or microscopic disease [12]. In fact, therapy with iodine-131 (131I) following thyroidectomy is one of the oldest theragnostic application, introduced in 1946. It was based on sodium iodide symporter that thyroid cells express and traps131I, metabolize it and aids in treatment of residual and metastatic disease [1], (Figure 2A).
Figure 2A.
A whole-body scan and planar images of a 42 year old male with thyrois cancer who had initial radioactive iodine (RAI) therapy is depicted. The underlying principle of a 131I thyroid therapy consists of ablation postoperative thyroid tissue residuals following thyroidectomy and treating metastatic disease after incomplete or total thyroidectomy. Dosing over 30 mCi result in obliteration of the thyroid by the beta particles causing ionization. This patient received 125 mCi 131I ablation therapy, due to Hurtle cell carcinoma (oncocytic cell follicular thyroid carcinoma) in left lobe and 8 days post therapy, a whole-body imaging was performed to look for any nodal/distant metastases. A region of intense uptake was observed in the lower cervical region, on the left of the midline, giving an image like a star, a sign known as “star sign” seen in the anterior images (this is due to the high uptake of RAI of the remnant thyroid tissue after surgery - arrow). The high uptake of 131I in the remnant thyroid tissue was seen also in the posterior images (arrowheads). No abnormal accumulation was noted elsewhere.
Figure 2A.
A whole-body scan and planar images of a 42 year old male with thyrois cancer who had initial radioactive iodine (RAI) therapy is depicted. The underlying principle of a 131I thyroid therapy consists of ablation postoperative thyroid tissue residuals following thyroidectomy and treating metastatic disease after incomplete or total thyroidectomy. Dosing over 30 mCi result in obliteration of the thyroid by the beta particles causing ionization. This patient received 125 mCi 131I ablation therapy, due to Hurtle cell carcinoma (oncocytic cell follicular thyroid carcinoma) in left lobe and 8 days post therapy, a whole-body imaging was performed to look for any nodal/distant metastases. A region of intense uptake was observed in the lower cervical region, on the left of the midline, giving an image like a star, a sign known as “star sign” seen in the anterior images (this is due to the high uptake of RAI of the remnant thyroid tissue after surgery - arrow). The high uptake of 131I in the remnant thyroid tissue was seen also in the posterior images (arrowheads). No abnormal accumulation was noted elsewhere.
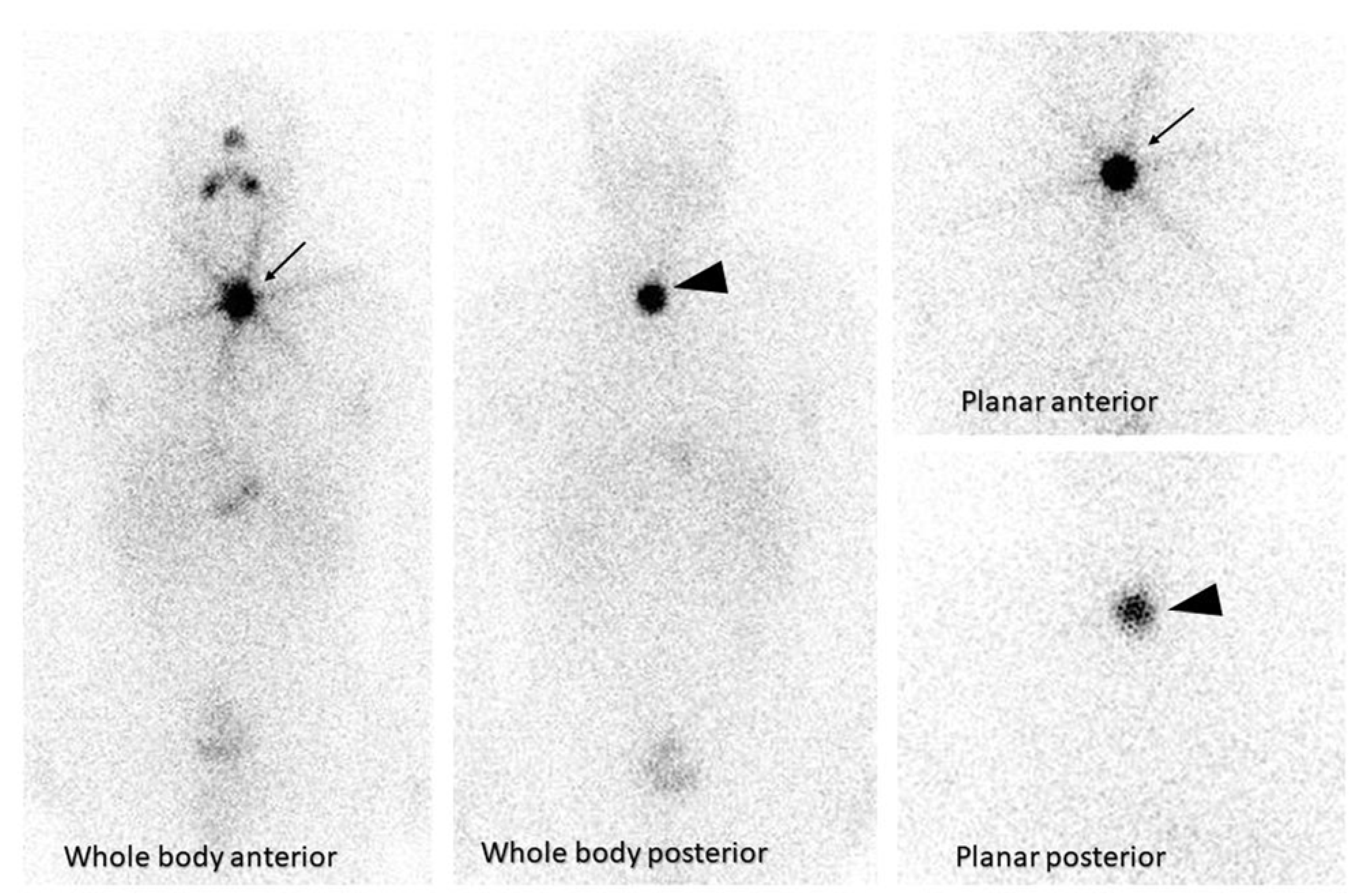
Figure 2B.
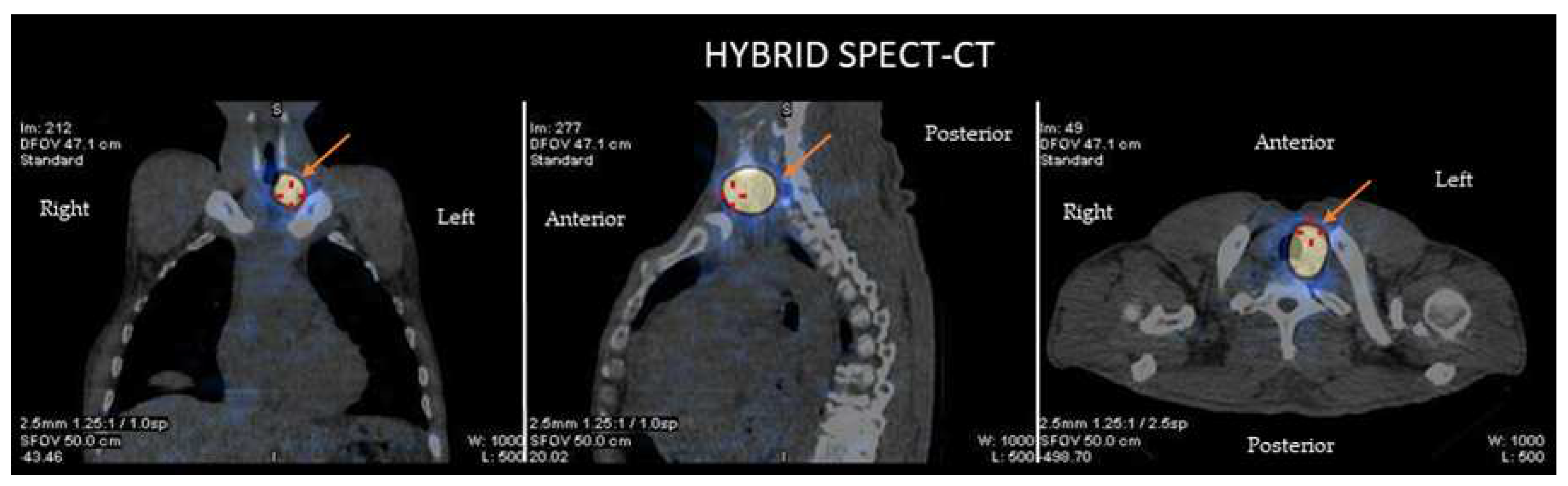
This figure demostrates the hybrid single photon emission tomography (SPECT) and low dose computed tomography (CT) images for anatomical verification of the finding and disclosure of any nodal uptake near the star sign. The combination of the CT with the iodine scan, accurately localizes the thyroid tissue uptake (arrow) from the metastatic lesions providing a three-dimensional view.
The explosive development in the in the nuclear imaging technology during the last several years, consisted of SPECT/CT and PET/CT systems, has allowed achievement of precision diagnostic imaging localizing primary and metastatic tumors for remnant ablation or adjuvant 131I treatment of the tumor avoiding the non-target healthy tissues [13,14], (Figure 2B).
Figure 2B.
This figure demostrates the hybrid single photon emission tomography (SPECT) and low dose computed tomography (CT) images for anatomical verification of the finding and disclosure of any nodal uptake near the star sign. The combination of the CT with the iodine scan, accurately localizes the thyroid tissue uptake (arrow) from the metastatic lesions providing a three-dimensional view.
The explosive development in the in the nuclear imaging technology during the last several years, consisted of SPECT/CT and PET/CT systems, has allowed achievement of precision diagnostic imaging localizing primary and metastatic tumors for remnant ablation or adjuvant 131I treatment of the tumor avoiding the non-target healthy tissues [13,14], (Figure 2B).
124IPET/CT consists of an important imaging tool for staging of differentiated thyroid cancer but 18F-fluorodeoxyglucose (FDG) PET/CT is more precise for high-risk differentiated thyroid cancer or noniodine recurrences. However, poorly differentiated thyroid carcinoma is better evaluated by 18F-FDG PET/CT, or the 68Ga/177Lu-prostate-specific membrane antigen. As a new generation imaging technique, novel molecular radiotracers based on PSMA ligand uptake evaluated with PET/CT have evolved. PSMA is a type II transmembrane glycoprotein that is extensively expressed in prostate cancer (PCa) and is the next imaging modality for PCa staging, re-staging, and response assessment. [15]When paired with 177Lu, it demonstrated greater diagnostic accuracy than traditional imaging in high-risk PCa patients, as well as treatment benefits (in terms of safety and efficacy). Despite its name, PSMA is not limited to the prostate; it has been reported to be expressed in the neovasculature of a variety of solid tumors, and enhanced uptake of 68Ga-PSMA PET/CT has been demonstrated in a variety of non-prostatic malignancies, including thyroid cancer. [16,17]Histological investigations, in particular, have confirmed the expression of PSMA in the microvasculature of thyroid tumors, where PSMA expression was associated with malignant disease, poor prognostic markers, and a lower progression free survival (PFS).[18]This evidence implies that PSMA PET/CT could be used as a theragnostic and prognostic imaging biomarker.The medullary thyroid carcinoma may be assessed by various PET tracers, such as [18F]-DOPA, [18F]-FDG, DOTA-octreotate (DOTATATE) and 68Ga-1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid [19,20]. For diagnosis of distant metastases of medullary thyroid cancer, the use of [68Ga] Ga-DOTA.SA.FAPi had significantly higher sensitivity compared to[68Ga]Ga-DOTANOC PET/CT [21]. 18F-DOPA is a PET drug that targets the L-type amino acid transporter, which is expressed in both MTC and pheochromocytomas [22]. While it is thought to be the most accurate method for detecting recurrent/metastatic MTC [23], particularly liver and cervical lymph node metastases, it is only available at specialist academic institutions. With an overall sensitivity of 47-83% [247], 18F -DOPA PET is most likely to detect uptake in MTC metastases in individuals with high calcitonin (>150 ng/mL). The sensitivity of 18F-FDG PET for MTC metastases is moderate (59-69%) [25]with the highest yield among individuals with short tumor marker doubling periods (one year). A study of -18F FDG PET indicated that in MTC with high calcitonin, the sensitivity was 92% and the specificity was 86%, with a significant impact on management decisions [26].
Finally, 68Ga- DOTATATE, a somatostatin analogue with strong affinity for SSTR2 that is widely available for neuroendocrine imaging, may be employed to screen for metastatic MTC. In comparison to other neuroendocrine neoplasms, this tracer has less dependable absorption, with relatively modest sensitivity for MTC (64%)[27], notably bone metastases. A recent research of 68Ga -DOTATATE PET indicated that it performed better than traditional imaging in 37% of 14/38 patients, changing patient care by finding neck nodes and bone metastases [28] Despite this, detecting somatostatin receptor type 2 expression may qualify a patient with refractory disease for 177Lu-PRRT: a recent small series indicated that 62% of patients with verified DOTATATE uptake (27/43) demonstrated imaging evidence of disease response following PRRT [29]. Targeted novel PET drugs using Ga-68/Lu-177 theranostic pairings, such as those targeting cholecystokinin-2 (CCK2R) receptors (DOTA-PPF11) and minigastrin (DOTA-MGS5), are also being studied.In any event, there are several radiotracers that aid in the effective diagnosis and therapy of the various types of thyroid cancers.
2.2. Neuroendocrine tumors
Neuroendocrine tumors are typically characterized by increased expression of somatostatin receptors (SSTRs).Several clinical studies have demonstrated that targeting of the somatostatin receptor (SSTR) produced sufficient imaging for diagnosis and staging of neuroendocrine tumors. Furthermore, therapeutic intervention of these tumors includes treatment with either cold somatostatin analogs or radionuclide therapy against the somatostatin receptor. PET with somatostatin analogs labelled with 68Ga demonstrated high sensitivity for diagnosis and staging of neuroendocrine tumors (NETs). In such patients, FDG PET/CT complemented molecular imaging with 68Ga-SSTR PET/CT [30]. A large study of 495 patients with metastatic neuroendocrine neoplasms had FDG PET/CT prior to treatment with peptide receptor radiotracer and found that the presence of positive lesions on FDG PET/CT was an independent predictor of outcome. The best long-term survival was associated with high expression of SSTR and negative FDG PET/CT [31].
Gastrointestinal NETs appearing either in intestines, appendix, or pancreas exhibit a variety of malignant transformation, with clinical activities depended on the mitotic activity calculated by the Ki-67 proliferative index and cell differentiation. Presence of SSTR expression in NET allows SSTR imaging with 68Ga-DOTATATE PET/CT and radiotracer therapy against the somatostatin receptor. In addition, the 68Ga-DOTATATE PET/CT may be occasionally used for staging and selection of patients for peptide receptor radionuclide therapy [32].177Lu-DOTATOC has also been studied as a promising therapeutic option for patients with metastatic bronchial NETs expressing high levels of SSTRs in a large study of 1,200 patients. [33]In another recent study, where patients with advanced midgut NET received 177Lu -DOTATATE and Sandostatin-LAR, longer progression-free survival and an overall survival benefit was observed for the combination compared to high-dose Sandostatin treatment alone. [34] The safety and efficacy of 177Lu -DOTATATE as pointed out in different studies has resulted in its approval by the FDA for the treatment of advanced SSTR-positive GEP neuroendocrine tumors.[35]
In recent years, research has also, focused on the use of alpha particle therapy with the radionuclides 225Ac, 213Bi and 212Pb. The latter has been recently investigated in patients with metastatic NETsin a phase I clinical trial after being labeled with DOTAMTATE, however the results of the study are not yet published.[36] The efficacy and safety profile of 225Ac-DOTATATE has been investigated in patients with metastatic NETs in terms of objective tumor response. The results showed that 37,5 % of patients experienced stabilization of disease, whereas the rest showed partial response.[37]
2.3. Prostate cancer
PSMA (prostate-specific membrane antigen), also known as glutamate carboxypeptidase II, is a zinc metalloenzyme encoded by FOLH1, and is localized in the cellular membrane. PSMA is expressed up to 1,000 times more in prostate cancer cells compared to normal prostate cells, and even higher in advanced prostate tumors. Although PSMA does not represent a selective marker of prostate cells or malignancies, its pattern of expression in the prostate prologs it as a theragnostic target for both imaging and therapeutic purposes [38]. Tumor characterization using PSMA-ligand for positron emission tomography (PET) imaging is important for subsequent PSMA radioligand therapy. Recently, the FDA approved two new drugs for PSMA PET imaging [39].
The radiopharmaceutical agent 68Ga-PSMA-HBED-CC (N, N′-bis-[2-hydroxy-5-(carboxyethyl)benzyl] ethylenediamine-N, N′-diacetic acid) represents a universal agent for PSMA-PET imaging. In this sector, a radiotracer targeting prostate-specific membrane antigen (PSMA) has showed interesting results. PSMA is a protein expressed ondysplastic prostate cells at levels 100-1000 times greater than on normal cells, with levelsincreasing even more with higher stages and grades.[40] Recent meta-analyses, such as the one by Han S. et al., reveal that 68Ga-PSMA positron emission tomography (PET) offers outstanding diagnostic performance for primary and secondary staging due to its capacity to detect lesions even at very low serum PSA levels.[41] The following was the study question for this meta-analysis: “What proportion of patients experience change in their management when 68Ga-PSMA PET is used versus conventional imaging modalities (CT, MRI)?” Utilizing 68Ga-PSMA-PET for initial staging of prostate cancer may result in modification of initial treatment plans in a significant number of patients. The pooled proportion of patients experiencing change in management was 54%. Similarly, 68Ga-PSMA-PET can detect patients with early recurrence, with higher sensitivity and specificity compared to conventional imaging modalities [42]. In addition, when new metastatic lesions were identified, 68Ga-PSMA-PET could suggest alternative treatment options for these metastases, such as stereotactic radiation therapy or surgical resection resulting in a better outcome. Thus, this treatment approach may result in reduction of anti-androgen therapy in some patients, avoiding its side effects [38]. For radioimmunotherapy, the diagnostic isotope is replaced by a therapeutic beta-emitting radioisotope coupled to the PSMA ligand and it is administered to the site of metastasis where it binds to PSMA on prostate cancer cells and kills them. In a meta-analysis of 9 clinical trials utilizing the 177Lu-PSMA-617 as the PSMA-radioisotope conjugate, it was shown over 50% reduction of PSA in 37% of prostate cancer patients [43]. Similar results of 50% reduction in PSA in 44.2% patients with castration resistant prostate cancer were reported in another study of 177Lu-PSMA-617 therapy and increased overall survival in responder patients in comparison to non-responders. In addition, there was noted improved radiologic progression-free survival and overall survival, as well as better objective response rate and disease control rate [44]. Apart from beta-emitting isotopes, alpha-emitting radioisotopes such as 213Bi and 225Ac conjugated with PSMA-617 showed a favorable response in non-responders to 177Lu-PSMA-617 treatment [45].
The FDG PET/CT has only limited use for advanced prostate carcinoma. Even though the PET radiotracer choline labeled with either 18F or 11C may detect early recurrence of prostate carcinoma, it has been replaced by other more specific radiotracers [46]. Other considered radiotracers include bombesin analogs that showed a positive diagnostic rate of 71.8% in patients that exhibited a negative conventional imaging [47]. Bombesin analogues labeled with 68Ga can target the gastrin-releasing peptide receptors and used for PET imaging with advantages of its availability, half-life, and relative low expenditure [48].
2.4. Colorectal cancer
Although early non-metastatic colorectal cancer is curable, metastatic colorectal cancer usually represents an incurable tumor. Thus, early diagnosis prior to metastases remains crucial for cure. Even though limited clinical data exists for these tumorsafter the appearance of metastatic lesions, characterization of genomic changes of metastatic lesions from the original tumor may modify a considered therapeutic intervention to a more personalized therapy. In such cases, a biopsy of the metastatic disease is recommended to examine any genomic alterations of the primary to metastatic tumor.
PET employing 18F-2-deoxy-2-fluoro-d-glucose (FDG) has emerged as a potential diagnostic method for recurrent colorectal cancer. The inclusion of FDG-PET affects disease management in up to 30% of patients with possibly resectable liver metastases, primarily by finding previously undisclosed extrahepatic illness, according to published data.Furthermore, because it is extremely sensitive in detecting residual or relapse malignancy in scarred liver tissue following both resection and local ablative treatments, FDG-PET is beneficial in the follow-up of patients who have undergone liver surgical procedures. Early FDG-PET appears to predict responsiveness to therapy during systemic therapy follow-up. For example, there is recent data showing that FDG-PET/MRI may change management in 19% of oligometastatic colorectal cancer.[49] Moreover, FDG PET/MRI enables local tumor evaluation and provides better N staging, particularly when evaluating low rectal tumors. [50]FDG-PET and computed tomography are complementary modalities for staging and restaging advanced colorectal cancer patients. The combination of these two approaches has a substantial impact on patient management. [51]
2.5. Cholangiocarcinoma
Cholangiocarcinoma or bile duct carcinoma is an infrequent malignancy of the bile ducts. Cholangiocarcinoma may be intrahepatic (rare) or extrahepatic (more common). The extrahepatic cholangiocarcinoma is divided into perihilar, localized in the area where the right and left hepatic ducts join to form the common hepatic duct, and the distal cholangiocarcinoma located in the area where the common hepatic duct joins with the gallbladder cystic duct to form the common bile duct. Several biomarkers in the bile have been investigated as potential diagnostic and treatment targets because tumor fluid in that area is secreted directly into the bile and should possess markers that potentially can be identified. However, the mere presence of a biomarker in the vicinity of a tumor does not essentially qualify it as a molecule for theragnostics. The appropriate theragnostic biomarker should be in the tumor cell surface, to be able to bind easily with a systemically administered drug [52]. One such secretome biomarker present in the bile secreted by the cholangiocarcinoma is the neutrophil gelatinase-associated lipocalin (NGAL), a 25-kDa glycoprotein that forms a covalently linked complex with the 92-kDa type-IV gelatinase matrix metalloproteinase-9 (MMP9). NGAL possesses anti-microbial properties and is involved in the regulation of various types of cancer, such as stomach, colon, and pancreas. The regulatory function of NGAL on cancer growth is mediated through its regulatory and stabilizing role on extracellular MMP9 and its anti-apoptotic effects on malignant cells. Thus, NGAL represents a biomarker overexpressed in the bile of patients with cholangiocarcinoma and generally, in patients with any pancreatobiliary malignancy [53]. The production and secretion of NGAL in significantly larger amounts in cell lines of cholangiocarcinoma compared to normal cholangiocytes makes NGAL a potential candidate biomarker for use in theragnostic systems [54].
Another interesting biomarker in cholangiocarcinomais PSMA that has been found in the tumor-associated neovasculature of the majority of cholangiocarcinoma cases (79.3%) in a large sample set recently for the first time. PSMA expression was limited to the cholangiocarcinoma neovasculature, while normal liver and peritumoral tissues were mostly PSMA-negative. Although a premature finding, PSMA may have diagnostic power in cholangiocarcinoma and can be used as a treatment target.[55]
2.6. Gliomas
Glioma is a type of tumor arising from glia. Glioblastoma (GBM) is the most malignant glioma with a median survival time of affected patients of approximately 16 months. Diagnosis is based on imaging tools, mainly MRI, PET, and CT scan [56]. The current therapy for recently diagnosed malignant gliomas consist of maximal surgical resection if the tumor is accessible, followed by radiation therapy, and chemotherapy [57]. Although temozolomide is the most effective chemotherapeutic drug, other chemotherapies may be also used upon failure of temozolomide. However, there are significant difficulties during chemotherapy treatment of gliomas, consisted of the presence of the blood-brain barrier, the diffuse structure of the neural tissue, and the presence of malignant cells within the glioma having multiple and different genetic abnormalities [58]. The blood – brain barrier hinders the entrance of most therapeutic drugs into the tumor, allowing only small, lipid soluble substances to pass freely. In addition, the diffuse infiltrating structure of the tumor within the intermixed presence of normal glial and neuronal cells, impedes chemotherapeutics to reach the vicinity of most tumor. Furthermore, most systemically administered antineoplastic drugs have modest pharmacokinetics and can also accumulate in healthy organs, and thus, increase the severity of side effects [59]. Finally, the presence of multiple and different genetic abnormalities within the same tumor, make it difficult to treat, since some parts of the tumor may respond to a certain drug and other are unresponsive resulting in the development of resistance of chemotherapy [60]. Theragnostic agents based on radionuclides can play an important role in the management and treatment of gliomas, including glioblastoma which remains the most aggressive type of primary tumor in the central nervous system. Several molecular targets have been explored for theragnostics in glioblastoma, including cell-surface receptors, kinases, and cell adhesion proteins, and other promising targets implicated in different pathways affecting tumor growth, survival, and progression. Some of the most prominent targets for glioblastoma are summarized in Table 1.
In glioblastoma, radiolabeled small molecules are the most popular choices as potential theragnostic agents since they present a more favorable pharmacokinetic profile and can cross the BBB. A molecular target that has been widely investigated for the development of this type of theragnostics is the enzyme PARP1 that is implicated in DNA repair. This enzyme is overexpressed in glioblastoma as opposed to non-tumoral cells. Since PARP becomes activated in response to DNA damage, inhibiting its actions pharmacologically or genetically may be a promising therapeutic option for cancers, including glioblastoma. Apart from the therapeutic potential, PARP inhibitors have also, been explored as PET imaging agents.18F-olaparib is a PARP-1 inhibitor designed in that accord, whereas another specific target, 18F-PARPi primarily binds to peripheral tumors [70,71].
PSMA radioligands, primarily used in the management of prostate cancer, as mentioned before, have also gained attention as potential diagnostic tools for gliomas. Different studies have explored the efficacy of PSMA as a radioligand when combined with 68Ga. Nomura et al. were the first to report that grade IV gliomas showed increased PSMA staining [72]. The utility of 68Ga-68 PSMA molecule as a diagnostic tool has been recently examined by Kumar et al. in recurrent high-grade glioma patients. The results showed that this compound is a promising imaging tool for evaluating recurrence in glioblastoma [73]. In another study, the use of 68Ga-PSMA-11 brain PET/CT for the evaluation of recurrent glioma showed also increased PSMA uptake, and the absence of normal brain uptake resulted in a much better visualization of glioma lesions [74]. Interestingly, when compared to conventional 18F-FDG PET, PSMA-targeting radiopharmaceuticals have the advantage of lower uptake in the normal brain [75]. However, despite the efficacy of PSMA-based molecules as diagnostic tools, there are still no clinical studies to evaluate their potential therapeutic role in glioma patients.
Chemokine receptor-4 (CXCR4) is highly expressed in different cancers, including gliomas, and is related to neo-angiogenesis, migration, and survival of malignant cells. A preferential expression of this molecule by high-grade glioma cells and a relationship with poor patient survival have been previously reported [76]. In that regard, Lapa et al. made a radiolabeled pentapeptide showing high affinity to CXCR4, named 68Ga-Pentixafor which was then tested as a PET imaging tool. Interestingly, the tracer showed high specificity towards high-grade glioma cells and presented a higher tumor uptake compared to popular tracers, like 18F-FET [77]. CXCR4-directed anti-glioma therapy using cytotoxic radionuclides, like 177Lu may thus, be a promising therapy for glioblastoma.
Two promising radionuclides that can be conjugated with chelators and act as antibody-based theragnostic are 89Zr and 177Lu. Recently, Foster et al. developed a bifunctionalchelator, named Lumi804 to be used in combination with either of the metals mentioned above as a theragnostic agent in glioblastoma. This radiolabeled molecule targets the tumor microenvironment and may significantly improve immunotherapy [78]. Another promising radionuclide that has been explored for its PET-imaging properties in glioblastoma is 99mTc. When linked to tetrofosmin, 99mTc-TF showed an increased uptake by glioblastoma cells. Given the fact that this radiotracer appears to be less affected by the existence of the elimination and uptake mechanism of chemotherapeutic substances, which certain cancer cells possess through p-glycoprotein, it may be a promising agent for the development of novel theragnostic agents through chelation with an appropriate cytotoxic agent [79,80].
2.7. Neuroblastoma and other pediatric tumors
Neuroblastoma is a common extracranial malignancy in young children originating from neural crest progenitor cells. [81] Atheranostic approach for these pediatric patients includes iodine-labeled metaiodobenzylguanidine (MIBG). This norepinephrine analog has the ability to accumulate into the neuroendocrine cells by primarily utilizing the cells’ normal norepinephrine transporters. Another minor mechanism of MIBG cell uptake includes passive diffusion. [82]MIBG is labeled with 123I or 131I. In a past study, 13 children with advanced neuroblastoma were treated with 131I-MIBG combined with chemotherapy. The results showed that the addition of the theranostic agent did not induce any additional toxicity compared to chemotherapy alone. Moreover, most patients responded very well to the combined treatment, and only one patient exhibited a mixed response.[83] In another study, where pediatric patients with relapsed neuroblastoma were treated with high doses of 131I-MIBG, no significant toxicity was observed, whereas the overall survival rate 1-year post-treatment was measured at 58%.[84]Apart from neuroblastoma, MIBG has been used in other types of pediatric malignancies, including paraganglioma and pheochromocytoma. These rare tumors are primarily treated by surgery, however in case of diffuse metastases or non-accessible anatomical region, the use of 131I-MIBG has shown promising results.[85] Apart from iodine-labeled MIBG, there has recently been designed a PET tracer based on fluorine ([18F]-meta-fluorobenzylguanidine). When 40 pediatric patients with a mean age of 6 years old and a history of neuroblastoma underwent [18F]MFBG PET/CT and [123I]MIBG SPECT/CT studies, a more favorable lesion detection rate was observed with [18F]MFBG PET/CT, implying that this radiolabeled agent may be a promising alternative to the well-studied 123I-MIBG theragnostic.[86]
3. Copper radionuclides as theragnostic agents
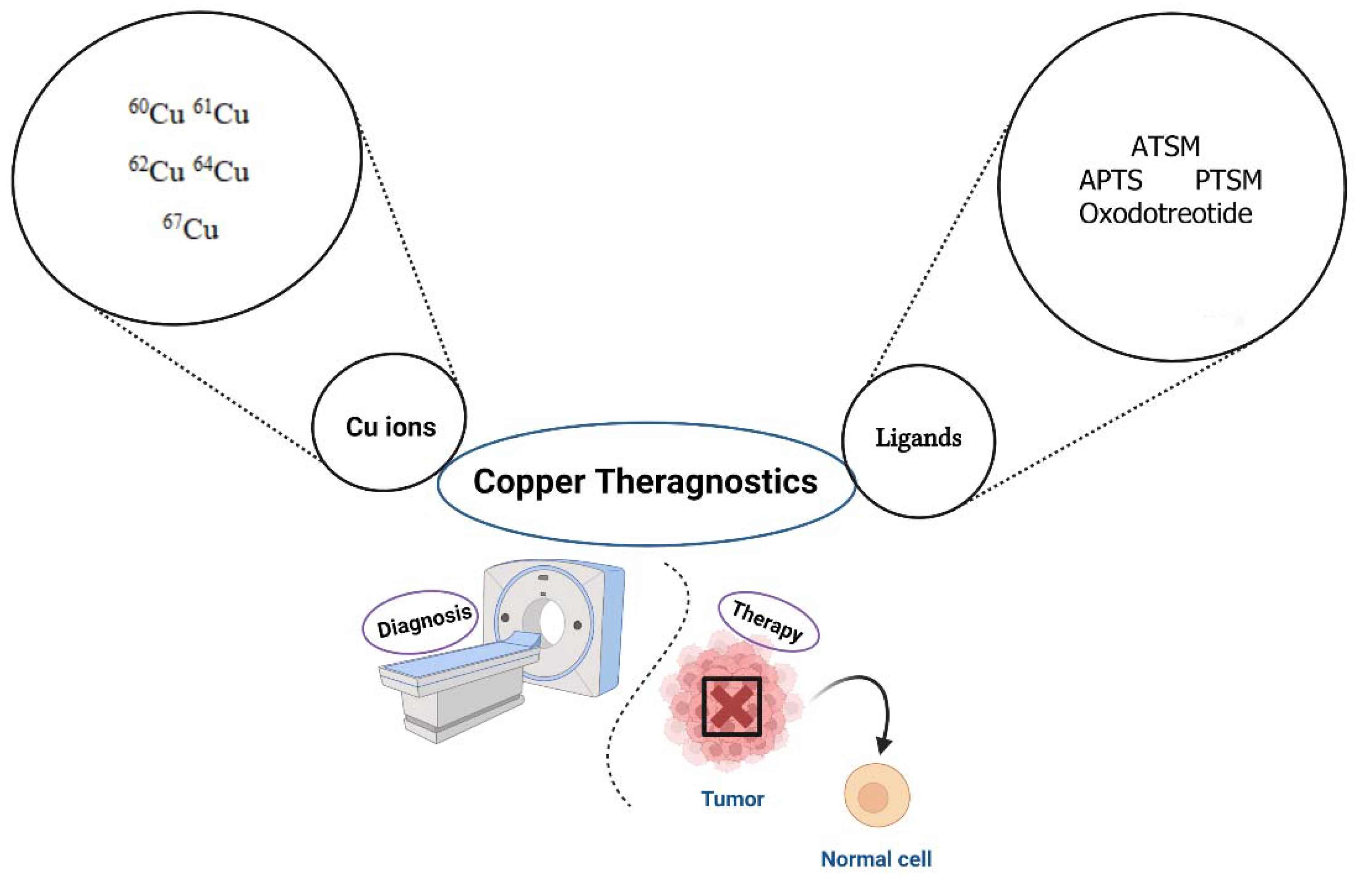
Copper radionuclides have been studied as promising theragnostic agents and the most effective copper isotope appears to be 64Cu. Several efforts have been made to evaluate the potential of this radioisotope as a diagnostic PET/CT tracer in clinical oncology. The nuclear properties of 64Cu make it a great example of theragnostic radionuclide and an interesting alternative to the well-studied gallium-68 (68Ga) and lutetium-177 (177Lu). In PET, the radionuclide decays through different routes. The resulting positrons destroy upon contact with electrons in the body producing photons that can be detected and analyzed by computers to locate the exact source of the annihilationevent [87]. Specifically, 64Cu is implicated in a complex decay scheme, involving three different processes. It can emit low-energy positrons, β- particles and Auger electrons. The combination of these emission routes makes this metallic radionuclide ideal for capturing high-resolution PET images, and in addition, as a therapeutic agent [88]. Μoreover, an interesting alternative to the single 64Cu radionuclide is the radionuclide pair 64Cu/67Cu. Copper-67 decays with beta emissions that are long enough to induce cell death in tumor cells. The coordination chemistry of this pair is also ideal for the linkage of a variety of chelators. Moreover, the ionic forms of copper, including the dicationic form Cu2+ are involved in several cellular processes, among which are cell proliferation and metastasis [89]. Therefore, the preparation of radiopharmaceuticals using copper has gained a lot of attention over the last decade (Figure 3).
Figure 3.
Major Cu ions and their ligands as promising theragnostic radionuclides for the diagnosis and treatment of different tumors. 60Cu, 61Cu, 62Cu are labeling with ATSM, APTS, PTSM. 64Cu is labeling with oxodotreotide (Dotatate). 67Cu as a β+ and γ emitter can be used for both SPECT imaging and radiotherapy. ATSM: N4-methylthiosemicarbazone; APTS: 2-acetylpyridine thiosemicarbazone; PTSM: N4-methylthiosemicarbazoneCreated using Biorender (https://www.biorender.com/
Figure 3.
Major Cu ions and their ligands as promising theragnostic radionuclides for the diagnosis and treatment of different tumors. 60Cu, 61Cu, 62Cu are labeling with ATSM, APTS, PTSM. 64Cu is labeling with oxodotreotide (Dotatate). 67Cu as a β+ and γ emitter can be used for both SPECT imaging and radiotherapy. ATSM: N4-methylthiosemicarbazone; APTS: 2-acetylpyridine thiosemicarbazone; PTSM: N4-methylthiosemicarbazoneCreated using Biorender (https://www.biorender.com/
3.1. Biological effects of copper ions in cancer
Copper ions are involved in different biological processes during cancer progression. Normal and malignant cells exhibit significant differences in copper metabolism and preclinical studies have demonstrated the multifaceted effects of copper on cancer development. The major mechanism of copper entrance to both normal and malignant cells is through specific transporters, named human copper transporter 1 (hCTR1). Prior to entrance, Cu2+ ions are reduced to Cu+ by reductases. Different studies have shown that hCTR1 transporters are overexpressed in tumors, including prostate cancer, breast cancer, melanoma and glioblastoma compared to normal cells [90,91,92] Moreover, RNA-mediated knockdown of this transporter has resulted in reduced uptake of 64Cu in the tumor site, resulting in inhibition of tumor development [93]. For this reason, this transporter has been proposed as an effective target for copper-based radiopharmaceuticals with the aim to visualize the tumor’s site.
4. Radiopharmaceutical applications of 64Cu isotope
64Cu isotope has been proposed as an effective metallic radionuclide for the development of theragnostic radiopharmaceuticals. 64CuCl2 is a promising agent for different types of tumors, including prostate cancer and glioblastoma. Ferrari et al. investigated the effect of this molecule against U87MG glioma cells using a xenografted GBM tumor mouse model. The investigators demonstrated that 64CuCl2 not only exhibits high affinity for GBM cells compared to normal cells, but is also, a potent anti-cancer agent, with the ability to inhibit cell proliferation after single or multiple-dose treatments [94]. In another study performed by Qin et al, the use of 64CuCI2 as a theragnostic agent for malignant melanoma was investigated. The authors reported that 64CuCI2 showed high uptake in the studied melanoma cell lines and the tumors were clearly visualized using 64CuCI2 PET imaging. It was also, observed that this molecule could effectively reduce tumor growth in the same cell lines, thus acting as a promising theragnostic agent [95].
The use of 64CuCl2 as a PET imaging tool in a clinical environment was first introduced by Panichelli et al. back in 2016 in glioblastoma patients. The clinical study included 19 patients, of which 18 were diagnosed with glioblastoma and 1 with grade 2 astrocytoma. The findings of this study demonstrated that all 18 patients with high-grade glioma showed a significantly higher tumor uptake of 64CuCl2 compared to the patient with low-grade malignancy [96]. Moreover, recent studies have demonstrated that hCTR1-expressing tumor cells or xenografts show elevated 64CuCl2 uptake, meaning that this compound can be a helpful theragnostic tool for these types of tumors. For example, it has been found that 64CuCl2 can act as a promising imaging tool for the diagnosis of recurrent prostate cancer in small-scale human studies, with the additional benefit that no adverse effects were recorded in those participating in the studies. Back in 2018, Guerreiro et al. investigated the effects of 64CuCl2 on different prostate Ca cell lines compared to normal cells. Interestingly, their results showed that not only the uptake of this compound was higher in tumor cells, but it was significantly more cytotoxic against cancer cells, compared to the non-tumoral prostate cell line [97]. Recently, an inhibitor of SGK1, a serine/threonine protein kinase named SI113 has been investigated in combination with 64CuCl2 for its therapeutic role against glioblastoma cell lines. The results presented by the investigators show that co-treatment with SI113 and 64CuCl2 increases cell death and enhances the effects of ionizing radiation. Thus, such a combination could be the basis of developing novel theragnostic tools for the diagnosis and treatment of GBM [98].
As mentioned above, the radionuclide pair 64Cu/67Cu may be a promising theragnostic solution due to the concurrent PET imaging properties of 64Cu and therapeutic potential of 67Cu. In a recent study, where patients with unresectable multifocal meningioma were injected with [64Cu] Cu-SARTATE (with SARTATE being a somatostatin analogue chelated to the sarcophagineMeCOSARchelator) prior to treatment with [67Cu] Cu-SARTATE, near identical targeting to tumors was observed between patients, implying that this combination of copper radionuclides can be an effective theragnostic option [99]. In another study, where the molecular target was the gastrin releasing peptide receptor (GRPR) that’s highly expressed in tumors, like prostate cancer, a complex made of the pair of radionuclides 64Cu/67Cu, a bombesin (BBN) analogue and a sarcophagine-based amine was used in a PC-3 xenograft prostate cancer mouse model. The results showed that [64/67Cu] Cu(SAR-BBN) displayed increased tumor uptake and retention, followed by a significant tumor growth inhibition [100].
5. Conclusion
In the last years, nuclear medicine has significantly contributed to the development of new tools for the concurrent diagnosis and treatment of different tumors. A wide variety of radionuclides can be linked to appropriate chelators and cytotoxic agents to design novel radiopharmaceuticals with theragnostic properties. The major advantages of this approach include improved diagnosis, reduced adverse effects to normal tissues, elimination of multi-step procedures and better patient care. Moreover, advancements in the field of nuclear medicine, such as the introduction of long-axial field-of-view PET/CT scanners can improve current imaging and diagnostic tools, by increasing sensitivity and resolution, as well as by reducing the level of injected radiopharmaceuticals while maintaining a high-resolution image quality. However, further research is needed to better understand the exact mechanism underlying the effects of theragnostic molecules in human cancer, and ultimately develop novel theragnostic agents with improved properties.
Acknowledgments
This research has been co-financed by the European Regional Development Fund of the European Union and Greek national funds through the Operational Program Competitiveness, Entrepreneurship and Innovation, under the call RESEARCH—CREATE—INNOVATE (project code: TAEDK-06189, MIS: 5149205).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Choudhury, P.S.; Gupta, M. Differentiated thyroid cancer theranostics: radioiodine and beyond. Br J Radiol. 2018, 91, 20180136. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, A.; Annunziata, S.; Salvatori, M. Side effects of theragnostic agents currently employed in clinical practice. Q J Nucl Med Mol Imaging. 2021, 65, 315–326. [Google Scholar] [CrossRef] [PubMed]
- Pomykala, K.; Hadaschik, B.A.; Sartor, O.; Gillessen, S.; Sweeney, C.J.; Maughan, T.; Hofman, M.S.; Herrmann, K. Next generation radiotheranostics promoting precision medicine. Ann Oncol. 2023, 34, 507–519. [Google Scholar] [CrossRef] [PubMed]
- Koziorowski, J.; Ballinger, J. Theragnostic radionuclides: a clinical perspective. Q J Nucl Med Mol Imaging. 2021, 65, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.; Rousseau, J.; Ramogida, C.F.; Celler, A.; Rahmim, A.; Uribe, C.F. Implications of physics, chemistry and biology for dosimetry calculations using theranostic pairs. Theranostics. 2022, 12, 232–259. [Google Scholar] [CrossRef] [PubMed]
- Jadvar, H.; Chen, X.; Cai, W.; Mahmood, U. Radiotheranostics in Cancer Diagnosis and Management. Radiology. 2018, 286, 388–400. [Google Scholar] [CrossRef] [PubMed]
- Vahidfar, N.; Eppard, E.; Farzanehfar, S.; Yordanova, A.; Fallahpoor, M.; Ahmadzadehfar, H. An Impressive Approach in Nuclear Medicine: Theranostics. PET Clin. 2021, 16, 327–340. [Google Scholar] [CrossRef]
- Klain, M.; Ricard, M.; Leboulleux, S.; Baudin, E.; Schlumberger, M. Radioiodine therapy for papillary and follicular thyroid carcinoma. Eur J Nucl Med Mol Imaging. 2002, 29 (Suppl. S2)), S479–S485. [Google Scholar] [CrossRef]
- Schlumberger, M.; Garcia, C.; Hadoux, J.; Klain, M.; Lamartina, L. Functional imaging in thyroid cancer patients with metastases and therapeutic implications. Presse Med. 2022, 51, 104113. [Google Scholar] [CrossRef] [PubMed]
- Klain, M.; Zampella, E.; Piscopo, L.; Volpe, F.; Manganelli, M.; Masone, S.; Pace, L.; Salvatore, D.; Schlumberger, M.; Cuocolo, A. Long-Term Prognostic Value of the Response to Therapy Assessed by Laboratory and Imaging Findings in Patients with Differentiated Thyroid Cancer. Cancers. 2021, 13, 4338. [Google Scholar] [CrossRef]
- Qaim, S.M.; Scholten, B.; Neumaier, B. New developments in the production of theranostic pairs of radionuclides. J Radioanal Nucl Chem. 2018, 318, 1493–1509. [Google Scholar] [CrossRef]
- Avram, A.M.; Dewaraja, Y.K. Thyroid Cancer Radiotheragnostics: the case for activity adjusted 131I therapy. ClinTransl Imaging. 2018, 6, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Sioka, C.; Kouraklis, G.; Zafirakis, A.; Manetou, A.; Dimakopoulos, N. Menstrual cycle disorders after therapy with iodine-131. FertilSteril. 2006, 86, 625–628. [Google Scholar] [CrossRef] [PubMed]
- Sioka, C.; Fotopoulos, A. Effects of I-131 therapy on gonads and pregnancy outcome in patients with thyroid cancer. FertilSteril. 2011, 95, 1552–1559. [Google Scholar] [CrossRef] [PubMed]
- Maurer, T.; Eiber, M.; Schwaiger, M.; Gschwend, J.E. Current use of PSMA-PET in prostate cancer management. Nat Rev Urol. 2016, 13, 226–35. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, Y.; Kuratsukuri, K.; Landas, S.; Imaida, K.; Rovito, P.M.; Wang, C.Y.; Haas, G.P. Expression of prostate-specific membrane antigen in normal and malignant human tissues. World J Surg. 2006, 3, 628–36. [Google Scholar] [CrossRef]
- Vargas, J.; Perez, F.G.; Gomez, E.; Pitalua, Q.; Ornelas, M.; Ignacio, E.; et al. Histopathologic Correlation With 68Ga PSMA PET/CT in Non Prostate Tumors. J Nucl Med. J Nucl Med., 61, 472. [Google Scholar]
- Ciappuccini, R.; Saguet-Rysanek, V.; Giffard, F.; Licaj, I.; Dorbeau, M.; Clarisse, B.; et al. PSMA Expression in Differentiated Thyroid Cancer: Association With Radioiodine, 18F-FDG Uptake and, Patient Outcome. J ClinEndocrinolMetab 2021, 106, 3536–45. [Google Scholar] [CrossRef] [PubMed]
- Roseland, M.E.; Dewaraja, Y.K.; Wong, K.K. Advanced imaging and theranostics in thyroid cancer. CurrOpinEndocrinol Diabetes Obes. 2022, 29, 456–465. [Google Scholar] [CrossRef]
- Giovanella, L.; Deandreis, D.; Vrachimis, A.; Campenni, A.; PetranovicOvcaricek, P. Molecular Imaging and Theragnostics of Thyroid Cancers. Cancers (Basel). 2022, 14, 1272. [Google Scholar] [CrossRef]
- Ballal, S.; Yadav, M.P.; Roesch, F.; Raju, S.; Satapathy, S.; Sheokand, P.; Moon, E.S., Martin, M.; Agarwal, S.; Tripathi, M.; Bal, C. Head-to-head comparison of [68Ga] Ga-DOTA.SA.FAPi and [68Ga]Ga-DOTANOC PET/CT imaging for the follow-up surveillance of patients with medullary thyroid cancer. Thyroid. 2023, 10.1089.
- Bal, C.; Chakraborty, D.; Khan, D. Positron emission tomography/computed tomography in thyroid cancer. PET Clin. 2022, 17, 265–283. [Google Scholar] [CrossRef]
- Asa, S.; Sonmezoglu, K.; Uslu-Besli, L.; et al. Evaluation of F-18 DOPA PET/CT in the detection of recurrent or metastatic medullary thyroid carcinoma: comparison with GA-68 DOTA-TATE PET/CT. Ann Nucl Med. 2021, 35, 900–915. [Google Scholar] [CrossRef] [PubMed]
- Treglia, G.; Tamburello, A.; Giovanella, L. Detection rate of somatostatin receptor PET in patients with recurrent medullary thyroid carcinoma: a systematic review and a meta-analysis. Hormones 2017, 16, 362–372. [Google Scholar] [PubMed]
- Rubello, D.; Rampin, L.; Nanni, C.; et al. The role of 18F-FDG PET/CT in detecting metastatic deposits of recurrent medullary thyroid carcinoma: a prospective study. Eur J SurgOncol. 2008, 34, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Saponjski, J.; Macut, D.; Saranovic, D.S.; et al. Clinical relevance of (18)F-FDG PET/CT in the postoperative follow-up of patients with history of medullary thyroid cancer. RadiolOncol. 2020, 55, 18–25. [Google Scholar]
- Pajak, C.; Cadili, L.; Nabata, K.; Wiseman, S.M. (68)Ga-DOTATATE-PET shows promise for diagnosis of recurrent or persistent medullary thyroid cancer: A systematic review. Am J Surg. 2022.224, 670–675.
- Tuncel, M.; Kılıçkap, S.; Süslü, N. Clinical impact of (68)Ga-DOTATATE PET-CT imaging in patients with medullary thyroid cancer. Ann Nucl Med. 2020, 34, 663–674. [Google Scholar] [CrossRef]
- Parghane, R.V.; Naik, C.; Talole, S.; et al. Clinical utility of (177) Lu-DOTATATE PRRT in somatostatin receptor-positive metastatic medullary carcinoma of thyroid patients with assessment of efficacy, survival analysis, prognostic variables, and toxicity. Head Neck 2020, 42, 401–416. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.; Svirydenka, H.; Virgolini, I. Theragnostics in Neuroendocrine Tumors. PET Clin. 2021, 16, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Liu, Q.; Singh, A.; Schuchardt, C.; Kulkarni, H.R.; Baum, R.P. Prognostic Value of 18F-FDG PET/CT in a Large Cohort of Patients with Advanced Metastatic Neuroendocrine Neoplasms Treated with Peptide Receptor Radionuclide Therapy. J Nucl Med. 2020, 61, 1560–1569. [Google Scholar] [CrossRef]
- Kandathil, A.; Subramaniam, R.M. Gastroenteropancreatic Neuroendocrine Tumor Diagnosis: DOTATATE PET/CT. PET Clin. 2023, 18, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Brabander, T.; van der Zwaan, W.A.; Teunissen, J.J.M.; et al. Long-term efficacy, survival, and safety of [177Lu-DOTA0,Tyr3]octreotate in patients with gastroenteropancreatic and bronchial neuroendocrine tumors. ClinCancerRes. 2017, 23, 4617–4624. [Google Scholar] [CrossRef] [PubMed]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors. N Engl J Med. 2017, 376, 125–135. [Google Scholar] [CrossRef]
- Sheikhbahaei, S.; Sadaghiani, M.S.; Rowe, S.P.; Solnes, L.B. Neuroendocrine Tumor Theranostics: An Update and Emerging Applications in Clinical Practice. AJR Am J Roentgenol. 2021, 2021. 217, 495–506. [Google Scholar] [CrossRef]
- NIH website. Phase 1 study of AlphaMedix in adult subjects with SSTR (+) NET (NCT03466216). clinicaltrials.gov/ct2/show/NCT03466216. UpdatedJuly 10, 2020. AccessedApril 10, 2021.
- Kratochwil, C.; Giesel, i.L.; Bruchertseifer, F.; Mier, W.; Apostolidis, C.; Boll, R.; et al. Bi-DOTATOC receptor-targeted alpha-radionuclide therapy induces remission in neuroendocrine tumours refractory to beta radiation: a first-in-human experience. Eur J Nucl Med Mol Imaging. 2014, 41, 2106–19.
- Jeong, S.H.; Kwak, C. Prostate-specific membrane antigen-mediated theragnostics in prostate cancer. Investig Clin Urol. 2021, 62, 497–499. [Google Scholar] [CrossRef]
- Farolfi, A.; Mei, R.; Ali, S.; Castellucci, P. Theragnostics in prostate cancer. Q J Nucl Med Mol Imaging. 2021, 65, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Montori, V.; Akl, E.A.; Djulbegovic, B.; Falck-Ytter, Y. GRADE guidelines: 4. Rating the quality of evidence--study limitations (risk of bias). J Clin Epidemiol. 2011, 64, 407–15. [Google Scholar] [PubMed]
- Beresford, M.J.; Gillatt, D.; Benson, R.J.; Ajithkumar, T. A systematic review of the role of imaging before salvage radiotherapy for post-prostatectomy biochemical recurrence. Clin Oncol (R Coll Radiol). 20, 2, 46-55.
- Han, S.; Woo, S.; Kim, Y.J.; Suh, C.H. Impact of 68Ga-PSMA PET on the management of patients with prostate cancer: a systematic review and meta-analysis. Eur Urol. 2018, 74, 179–190. [Google Scholar] [CrossRef]
- Calopedos, R.J.S.; Chalasani, V.; Asher, R.; Emmett, L.; Woo, H.H. Lutetium-177-labelled anti-prostate-specific membrane antigen antibody and ligands for the treatment of metastatic castrate-resistant prostate cancer: a systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2017, 20, 352–360. [Google Scholar] [CrossRef]
- Sartor O, de Bono J, Chi KN, Fizazi K, Herrmann K, Rahbar K, Tagawa ST, Nordquist LT, Vaishampayan N, El-Haddad G, Park CH, Beer TM, Armour A, Pérez-Contreras WJ, DeSilvio M, Kpamegan E, Gericke G, Messmann RA, Morris MJ, Krause BJ; VISION Investigators. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer.N Engl J Med. 2021, 385, 1091-1103.
- Afshar-Oromieh, A.; Babich, J.W.; Kratochwil, C.; Giesel, F.L.; Eisenhut, M.; Kopka, K.; Haberkorn, U. The rise of PSMA ligands for diagnosis and therapy of prostate cancer. J Nucl Med. 2016, 57, 79S–89S. [Google Scholar] [CrossRef] [PubMed]
- Annunziata, S.; Pizzuto, D.A.; Treglia, G. Diagnostic performance of pet imaging using different radiopharmaceuticals in prostate cancer according to published meta-analyses. Cancers (Basel). 2020, 12, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Liberini, V.; Laudicella, R.; Balma, M.; Nicolotti, D.G.; Buschiazzo, A.; Grimaldi, S.; Lorenzon, L.; Bianchi, A.; Peano, S.; Bartolotta, T.V.; Farsad, M.; Baldari, S.; Burger, I.A.; Huellner, M.W.; Papaleo, A.; Deandreis, D. Radiomics and artificial intelligence in prostate cancer: new tools for molecular hybrid imaging and theragnostics. EurRadiol Exp. 2022, 6, 27. [Google Scholar] [CrossRef]
- Sonni, I.; Baratto, L.; Iagaru, A. Imaging of Prostate Cancer Using Gallium-68-Labeled Bombesin. PET Clin. 2017, 12, 159–171. [Google Scholar] [CrossRef] [PubMed]
- Furtado, F.S., Suarez-Weiss, K.E., Vangel, M. et al. Clinical impact of PET/MRI in oligometastatic colorectal cancer. Br J Cancer 2021, 125, 975–982.
- Catalano, O.A., Lee, S.I., Parente, C. et al. Improving staging of rectal cancer in the pelvis: the role of PET/MRI. Eur J Nucl Med Mol Imaging 2021, 48, 1235–1245.
- Wiering, B.; Ruers, T.J.; Oyen, W.J. Role of FDG-PET in the diagnosis and treatment of colorectal liver metastases. Expert Rev Anticancer Ther. 2004, 4, 607–13. [Google Scholar] [CrossRef]
- Van Oosten, M.; Crane, L.M.; Bart, J.; van Leeuwen, F.W.; van Dam, G.M. Selecting potential targetable biomarkers for imaging purposes in colorectal cancer using target selection criteria (TASC): A novel target identification tool. Transl Oncol. 2011, 4, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, S.; Kaur, S.; Guha, S.; Batra, S.K. The multifaceted roles of neutrophil gelatinase associated lipocalin (NGAL) in inflammation and cancer. Biochim Biophys Acta. 2012, 1826, 129–69. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.; Ingram, N.; Verghese, E.T.; Wijetunga, I.; Markham, A.F.; Wyatt, J.; Prasad, K.R.; Coletta, P.L. Neutrophil Gelatinase-associated Lipocalin as a Theragnostic Marker in Perihilar Cholangiocarcinoma. Anticancer Res. 2018, 38, 6737–6744. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.X.; Zou, S.J.; Li, D.; Zhou, J.Y.; Cheng, Z.T.; Zhao, J.; Zhu, Y.L.; Kuang, D.; Zhu, X.H. Prostate-specific membrane antigen expression in hepatocellular carcinoma, cholangiocarcinoma, and liver cirrhosis. World J Gastroenterol. 2020, 26, 7664–7678. [Google Scholar] [CrossRef]
- Kaba, S.E.; Kyritsis, A.P. Recognition and management of gliomas. Drugs. 1997, 53, 235–244. [Google Scholar] [CrossRef]
- Groves, M.D.; Maor, M.H.; Meyers, C.; Kyritsis, A.P.; Jaeckle, K.A.; Yung, W.K.; Sawaya, R.E.; Hess, K.; Bruner, J.M.; Peterson, P.; Levin, V.A. A phase II trial of high-dose bromodeoxyuridine with accelerated fractionation radiotherapy followed by procarbazine, lomustine, and vincristine for glioblastoma multiforme. Int J Radiat Oncol Biol Phys. 1999, 45, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Kyritsis, A.P.; Levin, V.A. An algorithm for chemotherapy treatment of recurrent glioma patients after temozolomide failure in the general oncology setting. Cancer Chemother Pharmacol. 2011, 67, 971–983. [Google Scholar] [CrossRef] [PubMed]
- Fueyo, J.; Gomez-Manzano, C.; Puduvalli, V.K.; Martin-Duque, P.; Perez-Soler, R.; Levin, V.A.; Yung, W.K.; Kyritsis, A.P. Adenovirus-mediated p16 transfer to glioma cells induces G1 arrest and protects from paclitaxel and topotecan: implications for therapy. Int J Oncol. 1998, 12, 665–669. [Google Scholar] [CrossRef] [PubMed]
- Fueyo, J.; Gomez-Manzano, C.; Yung, W.K.; Kyritsis, A.P. The functional role of tumor suppressor genes in gliomas: clues for future therapeutic strategies. Neurology. 1998, 51, 1250–1255. [Google Scholar] [CrossRef]
- Marei, H.E.; Althani, A.; Afifi, N.; Hasan, A.; Caceci, T.; Cifola, I.; Caratelli, S.; Sconocchia, G.; D'Agnano, I.; Cenciarelli, C. Glioma extracellular vesicles for precision medicine: prognostic and theragnostic application. DiscovOnc. 2022, 13, 49. [Google Scholar] [CrossRef]
- Oprita, A.; Baloi, S.C.; Staicu, G.A.; Alexandru, O.; Tache, D.E.; Danoiu, S.; Micu, E.S.; Sevastre, A.S. Updated Insights on EGFR Signaling Pathways in Glioma. Int J Mol Sci. 2021, 22, 587. [Google Scholar] [CrossRef] [PubMed]
- Gagner, J.P.; Sarfraz, Y.; Ortenzi, V.; Alotaibi, F.M.; Chiriboga, L.A.; Tayyib, A.T.; Douglas, G.J.; Chevalier, E.; Romagnoli, B.; Tuffin, G.; Schmitt, M.; Lemercier, G.; Dembowsky, K.; Zagzag, D. Multifaceted C-X-C Chemokine Receptor 4 (CXCR4) Inhibition Interferes with Anti-Vascular Endothelial Growth Factor Therapy-Induced Glioma Dissemination. Am J Pathol. 2017, 187, 2080–94. [Google Scholar] [CrossRef]
- Lamszus, K.; Meyerhof, W.; Westphal, M. Somatostatin and somatostatin receptors in the diagnosis and treatment of gliomas. J Neurooncol. 1997, 35, 353–364. [Google Scholar] [CrossRef]
- Martins, E.P.; Gonçalves, C.S.; Pojo, M.; Carvalho, R.; Ribeiro, A.S.; Miranda-Gonçalves, V.; Taipa, R.; Pardal, F.; Pinto, A.A.; Custódia, C.; Faria, C.C.; Baltazar, F.; Sousa, N.; Paredes, J.; Costa, B.M. Cadherin-3 is a novel oncogenic biomarker with prognostic value in glioblastoma. MolOncol. 2022, 16, 2611–2631. [Google Scholar] [CrossRef] [PubMed]
- Afshari, A.R.; Motamed-Sanaye, A.; Sabri, H.; Soltani, A.; Karkon-Shayan, S.; Radvar, S.; Javid, H.; Mollazadeh, H.; Sathyapalan, T.; Sahebkar, S. Neurokinin-1 Receptor (NK-1R) Antagonists: Potential Targets in the Treatment of Glioblastoma Multiforme. Curr Med Chem. 2021, 28, 4877–4892. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Patel, C.B.; Xu, G.; Iagaru, A.; Zhu, Z.; Zhang, L.; Cheng, Z. Visualization of Diagnostic and Therapeutic Targets in Glioma with Molecular Imaging. Frontiers in Immunology. 2020, 11, 592389. [Google Scholar] [CrossRef]
- Zhao, L.; Chen, J.; Pang, Y.; Fu, K.; Shang, Q.; Wu, H.; Sun, L.; Lin, Q.; Chen, H. Fibroblast activation protein-based theranostics in cancer research: A state-of-the-art review. Theranostics. 2022, 12, 1557–1569. [Google Scholar] [CrossRef] [PubMed]
- Pommier, Y.; O'Connor, M.J.; de Bono, J. Laying a trap to kill cancer cells: PARP inhibitors and their mechanisms of action. SciTransl Med. 2016, 8, 362. [Google Scholar] [CrossRef] [PubMed]
- Reiner, T.; Lacy, J.; Keliher, E.J.; Yang, K.S.; Ullal, A.; Kohler, R.H.; Vinegoni, C.; Weissleder, R. Imaging therapeutic PARP inhibition in vivo through bioorthogonally developed companion imaging agents. Neoplasia. 2012, 14, 169–177. [Google Scholar] [CrossRef]
- Carney, B.; Carlucci, G.; Salina, B.; Di Gialleonardo, V.; Kossatz, S.; Vansteene, A.; Longo, V.A.; Bolaender, A.; Chiosis, G.; Keshari, K.R.; Weber, W.A.; Reiner, T. Non-invasive PET imaging of PARP1 expression in glioblastoma models. Mol Imaging Biol. 2016, 18, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Nomura, N.; Pastorino, S.; Jiang, P.; Lambert, G.; Crawford, J.R.; Gymnopoulos, M.; Piccioni, D.; Juarez, T.; Pingle, S.C.; Makale, M.; Kesari, S. Prostate specific membrane antigen (PSMA) expression in primary gliomas and breast cancer brain metastases. Cancer Cell Int. 2014, 14, 26. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; ArunRaj, S.T.; Bhullar, K.; Haresh, K.P.; Gupta, S.; Ballal, S.; Yadav, M.; Singh, M.; Damle, N.A.; Garg, A. , Tripathi, M.; Bal C. Ga-68 PSMA PET/CT in recurrent high-grade gliomas: Evaluating PSMA expression in vivo. Neuroradiology. 2022, 64, 969–979. [Google Scholar] [CrossRef] [PubMed]
- Sasikumar, A.; Kashyap, R.; Joy, A.; Patro, K.C.; Bhattacharya, P.; Pilaka, V.K.R.; Oommen, K.E.; Pillai, M.R.A. Utility of 68Ga-PSMA-11 PET/CT in Imaging of Glioma—A Pilot Study. ClinNucl Med. 2018, 43, e304–e309. [Google Scholar] [CrossRef]
- Rizzo, A.; Dall'Armellina, S.; Pizzuto, D.A.; Perotti, G.; Zagaria, L.; Lanni, V.; Treglia, G.; Racca, M.; Annunziata, S. PSMA Radioligand Uptake as a Biomarker of Neoangiogenesis in Solid Tumours: Diagnostic or Theragnostic Factor? Cancers (Basel). 2022, 14, 4039. [Google Scholar] [CrossRef] [PubMed]
- Bian, X.W.; Yang, S.X.; Chen, J.H.; Ping, Y.F.; Zhou, X.D.; Wang, Q.L.; Jiang, X.F.; Gong, W.; Xiao, H.L.; Du, L.L.; Chen, Z.Q.; Zhao, W.; Shi, J.Q.; Wang, J.M. Preferential expression of chemokine receptor CXCR4 by highly malignant human gliomas and its association with poor patient survival. Neurosurgery. 2007, 61, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Lapa, C.; Lückerath, K.; Kleinlein, I.; Monoranu, C.M.; Linsenmann, T.; Kessler, A.F.; Rudelius, M.; Kropf, S.; Buck, A.K.; Ernestus, R.I.; Wester, H.J.; Löhr, M.; Herrmann, K. (68) Ga-Pentixafor-PET/CT for Imaging of Chemokine Receptor 4 Expression in Glioblastoma. Theranostics. 2016, 6, 428–34. [Google Scholar] [CrossRef] [PubMed]
- Foster, A.; Nigam, S.; Tatum, D.S.; Raphael, I.; Xu, J.; Kumar, R.; Plakseychuk, E.; Latoche, J.D.; Vincze, S.; Li, B.; Giri, R.; McCarl, L.H.; Edinger, R.; Ak, M.; Peddagangireddy, V.; Foley, L.M.; Hitchens, T.K.; Colen, R.R.; Pollack, I.F.; Panigrahy, A.; Magda, D.; Anderson, C.J.; Edwards, W.B.; Kohanbash, G. Novel theranostic agent for PET imaging and targeted radiopharmaceutical therapy of tumour-infiltrating immune cells in glioma. EBioMedicine. 2021, 71, 103571. [Google Scholar] [CrossRef]
- Alexiou, G.A.; Xourgia, X.; Gerogianni, P.; Vartholomatos, E.; Kalef-Ezra, J.A.; Fotopoulos, A.D.; Kyritsis, A.P. 99mTc-Tetrofosmin Uptake Correlates with the Sensitivity of Glioblastoma Cell Lines to Temozolomide. World J Nucl Med. 2017, 16, 45–50. [Google Scholar] [CrossRef] [PubMed]
- lexiou GA, Tsiouris S, Kyritsis AP, Fotakopoulos, K.; Goussia, A.; Voulgaris, S.; Fotopoulos, A.D. The value of 99mTc-tetrofosmin brain SPECT in predicting survival in patients with glioblastoma multiforme. J Nucl Med. 2010, 51, 1923-1926.
- Mahapatra, S.; Challagundla, K.B. Neuroblastoma. 2023 Feb 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023.
- Cimini, A.; Ricci, M.; Chiaravalloti, A.; Filippi, L.; Schillaci, O. Theragnostic Aspects and Radioimmunotherapy in Pediatric Tumors. Int J Mol Sci. 2020, 21, 3849. [Google Scholar] [CrossRef] [PubMed]
- Mastrangelo, S.; Rufini, V.; Ruggiero, A.; Di Giannatale, A.; Riccardi, R. Treatment of Advanced Neuroblastoma in Children Over 1 Year of Age: The Critical Role of 131I-metaiodobenzylguanidine Combined with Chemotherapy in a Rapid Induction Regimen. Pediatr. Blood Cancer. 2011, 56, 1032–1040. [Google Scholar] [CrossRef] [PubMed]
- Kayano, D.; Wakabayashi, H.; Nakajima, K.; Kuroda, R.; Watanabe, S.; Inaki, A.; Toratani, A.; Akatani, N.; Yamase, T.; Kunita, Y.; et al. High-dose 131I-metaiodobenzylguanidine Therapy in Patients with High-Risk Neuroblastoma in Japan. Ann. Nucl. Med. 2020, 34, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Hasse-Lazar, K.; Krajewska, J.; Paliczka-Cieślik, E.; Jurecka-Lubieniecka, B.; Michalik, B.; Handkiewicz-Junak, D.; Roskosz, J.; Jarzab, B. Terapia 131I-MIBG w leczeniuguzówchromochłonnych u dzieci--doświadczeniawłasne [131I-MIBG therapy in the treatment of pheochromocytoma in children--own experiences]. Endokrynol Pol. 2008, 5, 235–40. [Google Scholar]
- Wang, P.; Li, T.; Liu, Z.; et al. [18F]MFBG PET/CT outperforming [123I]MIBG SPECT/CT in the evaluation of neuroblastoma. EurJ Nucl Med MolImag. 2023, 50, 3097–3106. [Google Scholar] [CrossRef] [PubMed]
- Ametamey, S.M.; Honer, M.; Schubiger, P.A. Molecular imaging with PET. Chem Rev. 2008, 108, 1501–1516. [Google Scholar] [CrossRef] [PubMed]
- Capriotti, G.; Piccardo, A.; Giovannelli, E.; Signore, A. Targeting Copper in Cancer Imaging and Therapy: A New Theragnostic Agent. J Clin Med. 2022, 12, 223. [Google Scholar] [CrossRef]
- Boschi, A.; Martini, P.; Janevik-ivanoska, E.; Duatti, A. The emerging role of copper-64 radiopharmaceuticals as cancer theranostics. Drug Discov Today. 2018, 23, 1489–1501. [Google Scholar] [CrossRef] [PubMed]
- Denoyer, D.; Masaldan, S.; La Fontaine, S.; Cater, M.A. Targeting copper in cancer therapy: ‘Copper That Cancer’ Metallomics. 2015, 7, 1459–1476.
- Bolzati, C. ,’ Duatti, A. The emerging value of 64Cu for molecular imaging and therapy. Q J Nucl Med Mol Imaging. 2020, 64, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Gutfilen, B.; Souza, S.A.; Valentini, G. Copper-64: a real theranostic agent. Drug Des DevelTher. 2018, 12, 3235–3245. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Wu, J.S.; Muzik, O.; Hsieh, J.T.; Lee, R.J.; Peng, F. Reduced 64Cu uptake and tumor growth inhibition by knockdown of human copper transporter 1 in xenograft mouse model of prostate cancer. J Nucl Med. 2014, 55, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, C.; Niccoli, A.; Villano, C.; Giacobbi, B.; Coccetti, D.; Panichelli, P.; Giuseppe, R. Copper-64 Dichloride as Theranostic Agent for Glioblastoma Multiforme: A Preclinical Study. Bio Med Res Int. 2015, 2015, 129764. [Google Scholar] [CrossRef]
- Qin, C.; Liu, H.; Chen, K.; Hu, X.; Ma, X.; Lan, X. Theranostics of malignant melanoma with 64CuCl2. J Nucl Med. 2014, 55, 812–817. [Google Scholar] [CrossRef] [PubMed]
- Panichelli, P.; Villano, C.; Cistaro, A.; Bruno, A.; Barbato, F.; Piccardo, A. Imaging of brain tumors with copper-64 chloride: Early experience and results. Cancer BiotherRadiopharm. 2016, 31, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Guerreiro, J.F.; Alves, V.; Abrunhosa, A.J.; Paulo, A.; Gil, O.M.; Mendes, F. Radiobiological characterization of 64CuCl2 as a simple tool for prostate cancer theranostics. Molecules. 2018, 23, 2944. [Google Scholar] [CrossRef] [PubMed]
- Catalogna, G.; Talarico, C.; Dattilo, V.; Gangemi, V.; Calabria, F.; D’Antona, L.; Schenone, S.; Musumeci, F.; Bianco, C.; Perrotti, N.; et al. The SGK1 kinase inhibitor SI113 sensitizes theranostic effects of the 64CuCl2 in human glioblastoma Multiforme cells. CellPhysiolBiochem. 2017, 43, 108–119. [Google Scholar] [CrossRef] [PubMed]
- Bailey, D.L.; Willowson, K.P.; Harris, M.; Biggin, C.; Aslani, A.; Lengkeek, N.A.; Stoner, J.; Eslick, M.E.; Marquis, H.; Parker, M.; et al. 64Cu Treatment Planning and 67Cu Therapy with Radiolabeled [64Cu/67Cu]MeCOSar-Octreotate in Subjects with Unresectable Multifocal Meningioma: Initial Results for Human Imaging, Safety, Biodistribution, and Radiation Dosimetry. J Nucl Med. 2023, 64, 704–710. [Google Scholar] [CrossRef]
- Huynh, T.; Van Dam, E.; Houston, Z.; McInnes, L.; Mpoy, C.; Harris, M.; Thurecht, K.; Donnelly, P.; Rogers, B. A Cu-64/Cu-67 Bombesin ligand as a theranostic for cancer. J Nucl Med. 2021, 62 (supplement 1), 1237. [Google Scholar]
Figure 1.
The use of radiopharmaceuticals as theragnostic tools. Depending on their decay properties radioisotopes could possess either diagnostic or therapeutic capabilities. Specifically, γ-emitters may be utilized for diagnostic SPECT and PET imaging. [5]. In contrast, α- and β radionuclides that emit low-range but highly ionizing radiation, are specific for therapeutic purposes.[6,7]. One commonly used theragnostic agent is Iodine-131 (131I), for diagnosis and treatment of patients with differentiated thyroid cancer [8,9,10]. Several other commonly used theragnostic pairs include,68Ga/177Lu, 43Sc/44Sc/47Sc, 83Sr/89Sr, 86Y/90Y, 110In/111In, 90Y/177Lu, and 152Tb/161Tb [11]. Created using Biorender (https://www.biorender.com/).
Figure 1.
The use of radiopharmaceuticals as theragnostic tools. Depending on their decay properties radioisotopes could possess either diagnostic or therapeutic capabilities. Specifically, γ-emitters may be utilized for diagnostic SPECT and PET imaging. [5]. In contrast, α- and β radionuclides that emit low-range but highly ionizing radiation, are specific for therapeutic purposes.[6,7]. One commonly used theragnostic agent is Iodine-131 (131I), for diagnosis and treatment of patients with differentiated thyroid cancer [8,9,10]. Several other commonly used theragnostic pairs include,68Ga/177Lu, 43Sc/44Sc/47Sc, 83Sr/89Sr, 86Y/90Y, 110In/111In, 90Y/177Lu, and 152Tb/161Tb [11]. Created using Biorender (https://www.biorender.com/).
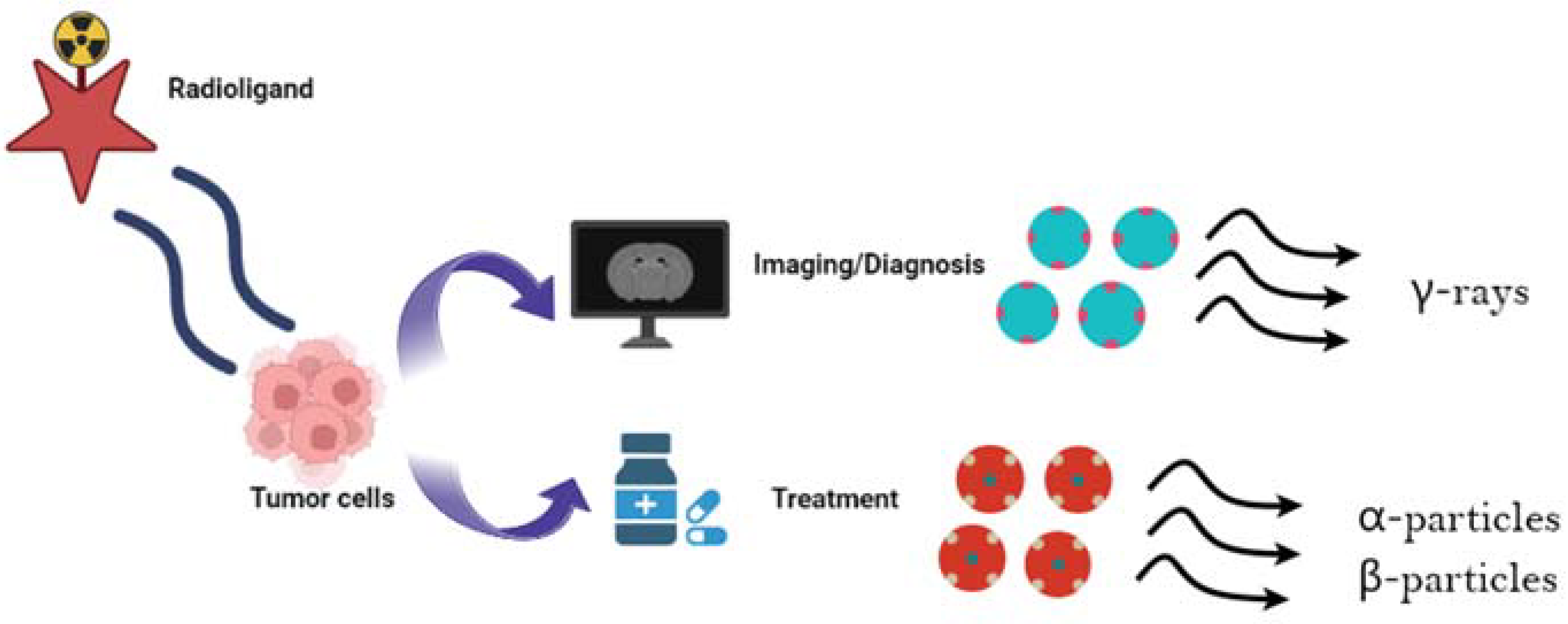

Table 1.
Molecular targets for theragnostics in GBM1.
| Molecular Target | Biological process in GBM | Reference |
|---|---|---|
| Tenascin-C | Cell adhesion/extracellular matrix (ECM) | [61] |
| Epidermal growth factor receptor (EGFR) | Cell growth/survival | [62] |
| Chemokine Receptor-4 (CXCR4) | Cell migration | [63] |
| Somatostatin Receptor 2 (SSTR2) | Cell signalling/cell survival | [64] |
| Cadherin-3 | Cell adhesion/extracellular matrix (ECM) | [65] |
| Neurokinin-1 receptor (NK1R) | Cell growth/survival | [66] |
| Integrin alpha-V beta-3 (αvβ3) | Angiogenesis | [67] |
| Fibroblast activation protein (FAP) | Inflammation | [68] |
| Poly (ADP-ribose) polymerase 1 (PARP1) | Cellular repair of DNA | [69] |
1GBM: Glioblastoma Multiforme.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



