
Submitted:
12 September 2023
Posted:
13 September 2023
You are already at the latest version
Abstract
The health of inmates living in a restricted environment are affected by oral health behaviours and is related to their oral health-related quality of life (OHRQoL). We investigated oral health behaviours and oral symptoms among male inmates and analysed factors related to OHRQoL. Three hundred and seventy-six male inmates in two prisons were investigated using a self-reported questionnaire. The survey items included oral health behaviours, oral symptoms, self-esteem, and OHRQoL level. We analysed cross-correlations and factors related to OHRQoL. Toothbrushing after lunch and dinner was practiced by 83.5% of male inmates. ‘Food impaction’ was experienced by 45.4%. The OHRQoL level among male inmates was low, at 39.90 points. A hierarchical multiple regression model that controlled for general characteristics identified the following OHRQoL factors, in order of significance: trouble biting/chewing (β = -0.307), toothache (β = -0.154), temporomandibular joint disorder (β = -0.099), and periodontal health (β = 0.089). Self-esteem and OHRQoL were not significantly correlated. To ensure oral health in male inmates, the results of this study suggests that an oral health education programme, as well as provision of adequate dental care services, is required to increase appropriate oral health practice rates.
Keywords:
Inmate
; Oral health behaviour
; Oral health-related quality of life
; Oral symptom awareness
; Toothbrushing
1. Introduction
Since prison inmates are members of the public who will eventually return to society, healthcare management is crucial in maintaining their physical and mental health [1]. Inmates in Korea are more likely to have poor health due to the significant healthcare gap compared to even the low-income group of the general population [2]. According to a report based on a survey of the right to health in detention facilities, ‘dental consultation and treatment’ ranked first in terms of the services considered most necessary in relation to health in the current Korean prison system, followed by ‘periodic health examination’ and ‘expansion of the use of external hospital treatment’ [3]. In addition, the prevalence of major diseases was high among those with dental diseases (6.3%), along with hypertension (14.4%) and diabetes (8.5%); in particular, tooth diseases (4.6%) and gum diseases (2.2%) accounted for the majority [3].
The oral cavity plays a vital role as a link between the external environment and the body [4,5]. Poor oral hygiene causes various oral diseases, such as dental caries, periodontal disease, and tooth loss, which significantly affects oral health [6,7]. Moreover, oral health is strongly associated with systemic health, and oral diseases are associated with major systemic diseases, including hypertension and diabetes [4,5,6,8]. Considering this relationship, oral health behaviours and related factors should be investigated among inmates to resolve their health problems.
Oral health status and oral hygiene habits affect Oral Health-Related Quality of Life (OHRQoL) [9]. To evaluate OHRQoL, the Oral Health Impact Profile 14 (OHIP-14) questionnaire is typically used. It consists of concepts such as functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicaps. Factors affecting OHIP-14 have been reported to include not only socio-demographic characteristics, but also socio-psychological factors, such as oral health status and self-esteem [10,11,12].
A recent study from India, reported a high level of oral disease among inmates; additionally, the length of imprisonment affected the degree of dental caries experienced [13]. Thirty-three percent of female inmates in Brazil experienced tooth loss after imprisonment, and 65.6% subjectively perceived that prison dental services were of below-average quality, which negatively affected their quality of life [14]. Deterioration in inmates’ quality of life was associated with caries, dental pain, deep periodontal pockets, prosthesis use, and age [15]. Moreover, adult male inmates had worse oral health than did the general adult male population, with 7.37 times more oral problems affecting their daily life [16]. Among imprisoned male adolescents, the tooth-loss rate was 47.06% [17], the prevalence of dental caries was high, and oral hygiene conditions were poor, requiring special attention from a policy perspective [18]. On the other hand, intervention for improving oral health among inmates has been reported to have a positive effect on oral health-related behavioural changes [19]. According to a review article on oral health among inmates in Europe, oral health among this population should be understood from an organisational perspective, due to its complexity, and more studies are needed to address gaps in the literature on oral health in inmates [20].
A comparison of the prevalence of dental caries among detention centre inmates based on the Korea National Health and Nutrition Examination Survey (KNHANES), as a study on the oral health among detention centre inmates in Korea, showed that the oral health among the inmate group was worse than that among the general population [21]. In addition, conservative infection control in a case of acute mandibular pericoronitis in an inmate [22] and the oral health status and awareness of oral health among adolescents in juvenile protection facilities and detention centre inmates have been reported [1,23,24]. Nevertheless, currently, insufficient studies have investigated factors related to oral health in adult inmates. Considering the results of several previous studies, oral health behaviours, perceived oral symptoms, and self-esteem among inmates are predicted to be significantly related to OHRQoL [12,14,15,16].
This study investigated oral health behaviours, perceived oral symptoms, and OHRQoL levels among inmates in Korean prisons, and sought to identify cross-correlations and factors affecting OHRQoL, to be utilised as a basis for developing programmes to improve oral health in inmates.
2. Materials and Methods
2.1. Study Design
This cross-sectional, correlational survey study investigated oral health behaviours and perceived oral symptoms among male inmates, and sought to identify factors associated with OHRQoL. The study adhered to the tenets of the Declaration of Helsinki, and the Institutional Review Board of D University (IRB: DKU IRB 2021-08-029) approved the study. Data were registered with the Clinical Research Information Service in Korea (CRIS) (KCT 0008129) [25]. Participant consent was obtained before conducting the survey.
2.2. Participants
The study participants were male inmates from two prisons in the Chungcheong Region of Korea. The appropriate sample size was calculated using G-power 3.1.7 (https://download.cnet.com/G-Power/3000-2054_4-10647044.html). With the effect size set at 0.10, power at 0.90, and 27 predictive factors, we calculated that 313 participants were required. Estimating a dropout rate due to incomplete survey responses of approximately 20%, we determined that approximately 376 participants were required.
The participants selected were inmates who voluntarily agreed to respond to the questionnaire. We excluded those who withdrew from participation during the course of the survey as they felt too uncomfortable with the questions asked to proceed further, as well as those who were unable to participate due to quarantine or punishment.
2.3. Variables
The questionnaires included items on socio-demographic characteristics (age) and oral health behaviours (two items for oral health awareness, two items for use of dental treatment, and three items for oral health care), and OHRQoL (14 items), self-esteem (11 items), and perceived oral symptoms (8 items).
2.3.1. Dependent Variables
For the OHRQoL scale, the OHIP-14 scale, reported by Slade and Spencer in 1994, was used [10,26]. The OHIP-14 scale was scored as follows: very often, 0 points; fairly often, 1 point; occasionally, 2 points; hardly ever, 3 points; and never, 4 points. The sum was calculated by inverse transformation processing. The highest possible score was 56 points. The higher the score, the higher was the OHRQoL. The internal consistency of this tool, as assessed by Cronbach’s alpha, was 0.88.
2.3.2. Independent Variables
As for the perceived oral symptom scale, eight items included in the 2021 Youth Health Risk Behaviour Web-based Survey were used [27]. These items were as follows: Q1. Does food get stuck between your teeth? Q2. Are you sensitive to hot or cold food? Q3. Have you ever experienced bleeding gums or gum disease? Q4. Do you feel like you have an unpleasant bad breath (oral malodour) in your mouth? Q5. Is your mouth often dry? Q6. Do you have trouble chewing or biting food? Q7. Have you ever felt that your jaw is dislocated or hurts when you open your mouth wide or chew? Q8. Have you ever had tooth pain (toothache) even when your mouth is still? Perceived oral symptoms were measured on a 5-point Likert scale, as follows: not at all, 1 point; very rarely, 2 points; sometimes, 3 points; often, 4 points; and always, 5 points. The mean score of the eight items was calculated. The highest possible score was 5 points. The higher the score, the more severe were the perceived oral symptoms. The internal consistency of this tool, as calculated by Cronbach’s alpha, was 0.83.
For the self-esteem scale, the tool developed by Rosenberg (1965) was used [28,29]. Each item was scored on a 5-point Likert scale, as follows: strongly disagree, 1 point; disagree, 2 points; neutral, 3 points; agree, 4 points; and strongly agree, 5 points. The mean of the scores of the 11 items was calculated. The highest possible score was 5 points. The higher the score, the higher was the individual’s level of self-esteem. The internal consistency of this tool, as assessed using Cronbach’s alpha, was 0.92.
2.3.3. Covariables
Age, a socio-demographic characteristic, was investigated as a continuous variable and was then re-coded as a categorical variable (aged between 20 and 29 years = 1; aged between 30 and 39 years = 2; aged between 40 and 49 years = 3; aged between 50 and 59 years = 4; aged 60 years or older = 5).
Oral health behaviour was investigated with multiple responses for the timing of brushing teeth during the previous day (before breakfast = 1; after breakfast = 2; before lunch = 3; after lunch = 4; before dinner = 5; after dinner = 6; after snack time = 7; before sleeping = 8), in reference to a previous study [30]. Dental treatment experience and dental examination in the past year (yes = 1; no = 2; do not know = 3), toothbrushing time (less than 1 min = 1; 1 min to less than 2 min = 2; 2 min to less than 3 min = 3; more than 3 min = 4), use of fluoride toothpaste, and ability to chew food with increasing hardness levels (tofu & rice, apple, kimchi, meat, dried squid, hard candy) were investigated as categorical items. Subjective health and oral health awareness were measured on a 5-point Likert scale (strongly agree = 5 points to strongly disagree = 1 point). Higher scores were considered to correspond to higher subjective health and oral health awareness in participants.
2.4. Data Collection
From September 23–30, 2021, the researcher visited the prison in person, explained the purpose of the study through the warden of the correctional institution to obtain consent, and delivered a structured questionnaire to the correctional officers. The questionnaire was distributed to inmates who voluntarily agreed to respond to the survey during lunchtime through a study participant recruitment notice displayed at the cafeteria. The survey process was performed anonymously, and a toothbrush and toothpaste set was provided as a reward for responding to the survey. A total of 376 inmates participated. The completed questionnaires were collected by putting them in a prepared questionnaire collection box. No incomplete questionnaires were included; thus, 376 questionnaires were included for analysis.
2.5. Statistical Analyses
SPSS software (Version 23.0; IBM Corp., Armonk, NY, USA) was used to obtain frequencies, percentages, and descriptive statistics of all variables. Differences in the OHIP-14 according to general characteristics were analysed using an independent t-test or one-way analysis of variance, and Scheffe’s multiple comparison test was performed as a post-hoc test. Pearson’s correlation analysis was performed to evaluate the relationship between OHIP-14 scores and perceived oral symptoms. Hierarchical multiple regression analysis was performed to identify factors related to the OHIP-14. The significance level of this study was set at α = 0.05.
3. Results
3.1. Toothbrushing Behaviour and Perceived Oral Symptoms in Male Inmates
Among the participating male inmates, 83.5% brushed their teeth after lunch and after dinner, and 82.6% brushed their teeth after breakfast; however, only 38.0% of inmates brushed their teeth before sleeping (Figure 1). In addition, 35.5% of inmates brushed their teeth before breakfast. Oral symptoms that were perceived to occur ‘often’ or more were as follows, in order: ‘food impaction (45.4%)’, ‘periodontal health (23.5%)’, ‘sensitivity to cold/hot food (21.7%)’, ‘trouble in biting/chewing (19.1%)’, and ‘malodour (15.9%).’ Among the perceived oral symptoms, the incidence of ‘TMJ disorder (8.4%)’ and ‘toothache (8.7%)’ was relatively low (Figure 2).
3.2. OHIP-14 According to the General Characteristics of Male Inmates
The OHIP-14 score among male inmates was low, at 39.9 points. Table 1 shows the comparison of the differences according to the general characteristics of the male inmates.
OHIP-14 scores decreased significantly with increasing inmate age (p < 0.001). The OHIP-14 score was higher for those in their 20s (46.89) than for those in their 40s (39.84), 50s (36.15), and 60s or older (36.39), and the scores of those in their 30s (43.60) was significantly different from that of those in their 40s or older.
The OHIP-14 score was lower in the group who reported brushing teeth for less than 2 min than in the group who reported brushing for more than 2 mins (p = 0.020). This score also increased as toothbrushing lengthened, in the order: ‘2 to less than 3 mins (41.87),’ ‘more than 3 mins (41.73),’ and ‘1 to less than 2 mins (38.10)’ (p = 0.020).
OHIP-14 increased depending on chewing discomfort with harder food (p < 0.001). The group that could chew tofu & rice (25.81) and apple (26.22) had a lower OHIP-14 score than the group that could chew meat (37.30), dried squid (36.45), and hard candy (45.46). In addition, the group that could chew kimchi (29.06) had a lower OHIP-14 score than the group that could chew hard candy.
The perceived level of subjective health and oral health was found to be directly proportional to the OHIP-14 score (p < 0.001).
Furthermore, self-esteem was also found to increase with an increase in OHIP-14 score, in the order of ‘high’ (41.10), ‘usual’ (40.12), and ‘low’ (38.65); however, this correlation was not statistically significant (p > 0.05). In addition, the OHIP-14 score did not differ significantly depending on dental treatment experience, dental examination in the past year, and use of fluoride toothpaste (p > 0.05).
3.3. Correlation between Perceived Oral Symptoms and Self-Esteem and OHIP-14 in Male Inmates
Table 2 shows the results of the correlation analysis of perceived oral symptoms and self-esteem with OHIP-14 scores in male inmates. Although perceived oral symptoms had a negative relationship with the OHIP-14 score, the relationship with self-esteem was not statistically significant (p > 0.05). The OHIP-14 score correlated negatively with perceived oral symptoms in the order of ‘trouble biting/chewing (r = –0.749),’ ‘toothache (r = –0.649),’ ‘periodontal health (r = –0.570),’ ‘sensitivity to cold/hot food (r = –0.546),’ ‘dry mouth (r = –0.523),’ ‘TMJ disorder (r = –0.488),’ and ‘food impaction (r = –0.338).
A strong positive correlation was found among the eight items of perceived oral symptoms. In particular, oral malodour was an oral symptom that was related to self-esteem in inmates (r = –0.114): the worse the oral malodour, the lower was their self-esteem.
3.4. Factors Related to OHIP-14 in Male Inmates
Table 3 shows the results of the hierarchical multiple linear regression analysis to identify factors affecting OHIP-14 scores in male inmates. Correlation analysis of the eight items of perceived oral symptoms revealed a correlation coefficient of less than 0.8; thus, all items were used for regression analysis. Age, subjective health awareness, and oral health awareness, which showed significant associations with the OHIP-14 score, were included as independent variables. In addition, ‘tofu & rice’ was set as the reference category for chewable food, a categorical variable, and dummy variables were used for the remaining five items. The assumptions of the regression analysis were tested, and all of them were found to be satisfied. Since the Durbin–Watson statistic was 2.030, autocorrelation of errors was deemed absent. Tolerance was less than 0.1, and the variance inflation factor value was 1.155–6.167, i.e., less than 10, indicating the absence of multicollinearity.
Model 1 yielded 49.9% (Adj. R2 = 0.499) explanatory power when the independent variable was adjusted for the dependent variable, OHIP-14 score, and the regression model was found to be statistically significant (F = 44.754, p < 0.001). The size of the influence of factors on the OHIP-14 score was in the following order: subjective oral health awareness (β = 0.278), subjective health awareness (β = 0.200), and age (β = -0.099). For chewable food, hard candy (β= 0.522), meat (β= 0.270), and squid (β= 0.126) were found to be factors affecting the OHIP-14 score, as compared to tofu & rice.
Model 2 was analysed by adding eight items of perceived oral symptoms to model 1. The model’s goodness of fit was significant (F = 51.631, p < 0.001). The adjusted explanatory power of the model was 69.8% (Adj. R2 = 0.698), indicating that the influence on OHIP-14 increased by19.9% as compared with model 1. The factor most significantly affecting the OHIP-14 score in male inmates was trouble biting/chewing (β = –0.307), followed by toothache (β = –0.154), age (β = –0.146), malodour (β = –0.131), subjective health (β = 0.131), TMJ disorder (β= –0.099), and periodontal health (β = –0.089). Among chewable foods in model 1, meat and squid, which were factors affecting the OHIP-14 score, were not significant, and only hard candy (β = 0.175) was a significant affecting factor. In particular, high subjective health and being able to bite candy were found to affect the OHIP-14 score positively, whereas trouble biting/chewing, toothache, age, malodour, TMJ disorder, and periodontal health were found to negatively affect OHIP-14 scores.
4. Discussion
This study examined oral health behaviours and perceived subjective symptom levels in male inmates and determined factors related to OHRQoL. We found that the OHRQoL level among male inmates was low (39.90 points). In a hierarchical multiple regression model that controlled for general characteristics, we identified the following factors as affecting OHRQoL, in order: trouble biting/chewing, toothache, age, subjective health, oral malodour, TMJ disorder, and periodontal health. We did not find a statistically significant correlation between self-esteem and OHRQoL.
Previous studies found that the level of oral health among prison inmates was poor as compared to that in the general population [31,32], and that oral health status affected self-esteem [33,34]. Moreover, considering the report that oral health problems are related to decreased quality of life, perceived subjective symptoms have been reported to affect OHRQoL [35].
Although the mean practice rate of toothbrushing after meals among male inmates in Korea was 83.2%, the practice rate before breakfast (35.5%) was higher, and the practice rate before sleeping (38.8%) was rather low. Hence, education on appropriate oral health care is necessary. However, the practice rate of toothbrushing after lunch was 83.5%, approximately 15% higher than that obtained in the 2022 Community Health Survey (68.3%) [36]. In addition, when compared to the practice rate of toothbrushing after lunch among Korean workers aged 19 years or older (51.6%) in the 6th KNHANES (2013–2015), the rate of toothbrushing after lunch among male inmates was relatively high [37]. These findings were thought to be influenced by the laws stipulated, such as maintaining the cleanliness of inmates (Article 32 [1] of the Act on Execution of Sentences and Treatment of Inmates) and regular exercise and bathing for health maintenance (Article 33 [1] of the Act on Execution of Sentences and Treatment of Inmates), so that inmates can lead healthy and regular lives in an enclosed environment [38].
In terms of perceived oral symptoms, inmates responded to ‘often’ or ‘always’ having the following, in order: ‘food impaction’, ‘periodontal health’, and ‘sensitivity to cold/hot food.’ However, in a study on perceived oral symptoms in older individuals, the order was ‘subjective oral health awareness’ (49.4%) and ‘chewing discomfort’ (49.2%) [39]. Nevertheless, the items included in perceived oral symptoms differed between these studies. On the other hand, all items for perceived oral symptoms and the level of OHRQoL showed a negative correlation. This finding was similar to the results of studies on non-medical hospital workers [40], industrial workers [27,41], and middle-aged people in Korea [42]. Against this background, customised oral healthcare programmes are needed in correctional facilities to alleviate the perceived oral symptoms among inmates [14].
The OHIP-14 score among the participants was rather low (39.9 out of 55 points). Except for participants in their 60s or older, the mean OHIP-14 score decreased as age increased. This finding was similar to the results of studies on industrial workers [41], middle-aged adults [43], and female inmates [15]. Toothbrushing time of ‘2 min to less than 3 mins’ was associated with the highest OHIP-14 score among our participants, similar to the results of studies on foreign workers [44] and patients visiting the dentist [45]. Since oral health care with correct toothbrushing can be related to quality of life, this result suggested that inmates should be motivated to use oral health education, and that the facilities and environment for brushing teeth should be improved [1].
Among male inmates, 246 (67.8%) responded ‘no’ to the use of dental treatment over the past year, which was more than twice as many as those who responded ‘yes’ (110, 30.3%). In addition, 59% (214) responded ‘no’ to oral examination over the past year, approximately 1.5 times the percentage of those who responded ‘yes’ (145, 39.8%). These values were approximately twice as high as that of those who had not used dental hospitals and clinics in the past year in a study on the relationship between health check-ups and unmet dental care needs among Korean adults (31.5%) [46]. The result of this study was somewhat high, with 57.4% of individuals responding that they had not undergone an oral examination in the last year . In addition, in a study on dental check-ups and unmet dental care needs based on the 7th KNHANES [47], 31.7% reported unmet dental care needs, while 56.5% of people did not undergo oral check-ups. Thus, the proportions of those who did not use dental treatment and of those who did not undergo oral examination were higher among inmates in the present study than among adults in the general Korean population.
As for the difference in the OHIP-14 score depending on the ability to chew food, the OHIP-14 scores of inmates who could chew tougher food was higher in the order of meat, dried squid, and hard candy, as compared to tofu & rice and apple. This finding was similar to the results of studies on non-medical hospital workers [40], the KNHANES population [48], and OHRQoL in some adults [48,49]. Thus, the chewing-related indicator may be useful as an indicator of OHRQoL in inmates in future [22].
In terms of the OHIP-14 score, the more positively health or oral health were subjectively perceived, the higher was the OHRQoL. This finding was similar to the results of studies on patients of dental hospitals and clinics [45,51] and the general adult population, based on the KNHANES [48]. Hence, subjective health and oral health awareness are also worth considering as indicators of oral health and quality of life among inmates in future [21]. Furthermore, continuous customised oral health education is required for inmates to perceive their oral health positively [1].
This study showed that inmates with high self-esteem (41.10 points) had higher OHIP-14 scores than did inmates with low self-esteem (38.65 points), but the difference was not statistically significant. This finding was similar to that of previous studies in childcare teachers [52], a general adult population [53], and orthodontic patients [54,55].
Clinical strengths, Limitations and Future Research
Article 10 of the UN International Covenant on Civil and Political Rights stipulates that ‘all persons deprived of their liberty shall be treated with humanity and with respect for the inherent dignity of the human person’ [56,57]. In addition, the ‘United Nations Standard Minimum Rules for the Treatment of Prisons (the Nelson Mandela Rules)’ clearly state that prisoners, as citizens, should receive the same level of healthcare services as people in the general population [58].
The correctional healthcare delivery system and health management in Korea are critical to the right to health of inmates and the right to healthcare in correctional facilities [1,59]. Thus, a comprehensive correctional healthcare delivery system, emphasising primary healthcare but providing other forms of care as well, is needed [1,59,60]. By emphasizing primary healthcare, the direction should be set to prevent progression of mild diseases, that can be cured in correctional facilities, to a level requiring secondary or tertiary medical care [59].
This study analysed the factors related to OHRQoL in adult male inmates in Korea, which have not been reported previously. The results of this study may facilitate provision of dental care services to inmates and can help to improve the oral healthcare system. In particular, chewing discomfort and toothache among the perceived oral symptoms of male inmates were found to be important factors influencing OHRQoL. This finding may help to prioritise the dental care services needed for male inmates.
The limitations of this study were as follows. First, since this study was performed only with a self-reported questionnaire, without oral examination, the relationship between OHRQoL and objective indicators of oral health status could not be identified. Further studies need to perform oral examinations simultaneously to identify objective oral health indicators, such as dental caries experience, periodontal health, and chewing discomfort. Second, since only male inmates were selected as study participants, we were unable to compare the results in female inmates. Further studies on female inmates are required to compare sex differences. Third, the causality of the factors affecting OHRQoL could not be assessed as this was a cross-sectional study performed in two prisons in Korea. In future, a large-scale longitudinal study is required to expand the number of study participants and determine changes in the oral health level in inmates.
5. Conclusions
In this study, the practice rate of toothbrushing among male prison inmates in Korea was high, at 83.2%; however, the OHRQoL was somewhat low, at 39.9 points. In addition, food impaction, sensitivity to cold/hot food, periodontal health, malodour, dry mouth, trouble biting/chewing, TMJ disorder, and toothache, which are perceived oral symptoms, were found to be positively correlated with each other, indicating the need for integrated management of oral healthcare. In particular, factors affecting OHIP-14 score were strongly negatively related to chewing discomfort and toothache. Although no significant relationship between self-esteem and OHIP-14 scores was found, inmates with high self-esteem (41.10 points) had higher OHIP-14 scores than did inmates with lower self-esteem (38.65 points). To guarantee the right to health among inmates in future, our findings suggest the need for establishment of a healthcare system that can provide appropriate dental care services and operate an oral health education programme to promote appropriate oral health awareness.
Author Contributions
Conceptualization, J.-H.J.; methodology, J.-H.J., and K.-S.K.; software, H.-S.Y.; validation, J.-H.J., K.-S.K., and H.-S.Y.; formal analysis, H.-S.Y.; investigation, H.-S.Y., and J.-H.J.; resources, H.-S.Y.; data curation, H.-S.Y. writing—original draft preparation, H.-S.Y., and J.-H.J.; writing—review and editing, J.-H.J., K.-S.K., and H.-S.Y.; visualization, J.-H.J., and H.-S.Y.; supervision, J.-H.J., and K.-S.K.; project administration, J.-H.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Dankook University (IRB: DKU IRB 2021-08-029).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
The data presented in this study are available on reasonable request from the corresponding author.
Acknowledgments
We thank the prison warden and officials who cooperated with data collection.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ryu, D.-Y.; Song, K.-S.; Han, S.-Y. Oral health condition, recognition, and practice in prisoners. J. Dent. Hyg. Sci. 2015, 15, 153–159. [Google Scholar] [CrossRef]
- Yeon, S.-J.; Roh, Y.-J.; Kim, A.-S.; Jung, Y.- J. Health and medical services for inmates in Korean correctional facilities. KICJ. 2008, 12, 1–228. [Google Scholar]
- Ju, Y. Survey on the Right to Health in Detention Facilities, 2016. National Human Rights Commission of Korea 2017.
- Darnaud, C.; Thomas, F.; Pannier, B.; Danchin, N.; Bouchard, P. Oral health and blood pressure: The IPC Cohort. Am. J. Hypertens. 2015, 28, 1257–1261. [Google Scholar] [CrossRef] [PubMed]
- Salcedo-Rocha, A.L.; Garca-de-Alba-Garcia, J.E.; Velsquez-Herrera, J.G.; Barba-Gonzlez, E.A. Oral health: Validation of a questionnaire of self-perception and self-care habits in diabetes mellitus 2, hypertensive and obese patients. The UISESS-B scale. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e834–839. [Google Scholar] [CrossRef]
- Jahangiry, L.; Bagheri, R.; Darabi, F.; Sarbakhsh, P.; Sistani, M.M.N.; Ponnet, K. Oral health status and associated lifestyle behaviors in a sample of Iranian adults: An exploratory household survey. BMC Oral Health 2020, 82. [Google Scholar] [CrossRef]
- Arantes, R.; Santos, R.V.; Frazo, P. Oral health in transition: the case of indigenous peoples from Brazil. Int. Dent. J. 2010, 60, 235–240. [Google Scholar]
- Banyai, D.; Vegh, D.; Vegh, A.; Ujpal, M.; Payer, M.; Biczo, Z.; Rzsa, N. Oral health status of children living with type 1 diabetes mellitus. Int. J. Environ. Res. Public Health 2022, 19, 545. [Google Scholar] [CrossRef]
- Ferruzzi, L.P.D.C.; Davi, L.R.; Lima, D.C.B.D.; Tavares, M.; Castro, A.M.D. Oral health-related quality of life of athletes with disabilities: a cross sectional study. J. Biosci. 2021, 37, e37008. [Google Scholar] [CrossRef]
- Slade, G.D.; Spencer, A.J. Development and evaluation of the oral health impact profile. Community Dent. Health 1994, 11, 3–11. [Google Scholar]
- Slade, GD. Derivation and validation of a short-form oral health impact profile. Community Dent. Oral Epidemiol. 1997, 25, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.-J.; Yoon, M.-S. Relationship of depression, stress, and self-esteem with oral health-related quality of life of middle-aged women. J. Korean Soc. Dent. Hyg. 2015, 15, 825–835. [Google Scholar] [CrossRef]
- Balkrishna, A.; Singh, K.; Sharma, A.; Parkar, S.M.; Oberoi, G. Oral health among prisoners of district jail, Haridwar, Uttarakhand, India-A cross-sectional study. Rev. Esp. Sanid. Penit. 2022, 24, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Moraes, L.R.; Duarte de Aquino, L.C.; Cruz, D.T.d.; Leite, I.C.G. Self-perceived impact of oral health on the quality of life of women deprived of their liberty. Int. J. Dent. 2021, 2021, 5520652. [Google Scholar] [CrossRef]
- Soares, G.H.; Mendona, I.; Michel-Crosato, E.; Moyss, S.J.; Moyss, S.T.; Werneck, R.I. Impact of oral conditions on the quality of life of incarcerated women in Brazil. Health Care Women Int. 2019, 40, 776–787. [Google Scholar] [CrossRef]
- Bukhari, R.; Al-Sulaimi, A.; Fadaak, A.; Balhaddad, A.; AlKhalfan, A.; El Tantawi, M.; Al-Ansari, A. Oral health amongst male inmates in Saudi prisons compared with that of a sample of the general male population. S. Afr. Dent. J. 2017, 72, 402–407. [Google Scholar] [CrossRef]
- Casarin, M.; Nolasco, W.d.S.; Colussi, P.R.G.; Piardi, C.C.; Weidlich, P.; Rösing, C.K.; Muniz, F.W.M.G. Prevalence of tooth loss and associated factors in institutionalized adolescents: A cross-sectional study. Cien. Saude Colet. 2021, 26, 2635–2642. [Google Scholar] [CrossRef]
- Alkhadra, T. Prevalence of dental caries and oral hygiene status among juvenile prisoners in the kingdom of Saudi Arabia. J. Contemp. Dent. Pract. 2017, 18, 991–995. [Google Scholar] [CrossRef]
- Evensen, K.B.; Bull, V.H. Oral health in prison: An integrative review. Int. J. Prison. Health 2023, 19, 251–269. [Google Scholar] [CrossRef]
- Evensen, K.B.; Bull, V.H.; Ness, L. A health promotion intervention to improve oral health of prisoners: Results from a pilot study. Int. J. Prison. Health 2021, 17, 546–559. [Google Scholar] [CrossRef]
- Hwang, I.; Park, K.; Park, H.-K. Prevalence of dental caries and associated factors of detention center inmates in South Korea compared with Korea National Health and Nutrition Examination Survey (KNHANES) respondents: a retrospective study. BMC Oral Health 2022, 22, 383. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-U.; Yoo, J.-H.; Choi, B.-H.; Sul, S.-H.; Kim, H.-R.; Mo, D.-Y.; Kim, J.-B. Conservative infection control on acute pericoronitis in mandibular third molar patients referred from the prison. J. Korean Oral Maxillofac. Surg. 2010, 36, 57–61. [Google Scholar] [CrossRef]
- Hong, S.-H. A research on recognition of oral health based on oral health education for adolescents in some reformatories. J. Dent. Hyg. Sci. 2007, 7, 187–191. [Google Scholar]
- Jung, Y.-J.; Jeong, S.-Y.; Kang, B.-J.; Baek, K.-W. Oral health status and self-perceived oral health status of students in juvenile protection education institutions. J. Korean Acad. Pediatr. Dent. 2009, 36, 539–549. [Google Scholar]
- Clinical Research Information System(CRIS). Available online: https://cris.nih.go.kr/cris/index.jsp (accessed on 13 Jul 2023).
- Bana, K.F.M.A.; Shadab, S.; Hakeem, S.; Ilyas, F. Comparing oral health-related quality of life (OHIP-14) and masticatory efficiency with complete denture treatment. J. Coll. Physicians Surg. Pak. 2021, 30, 694–698. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.-I.; Han, S.-J. Factors which affect the oral health-related quality of life of workers. J. Dent. Hyg. Sci. 2013, 13, 480–486. [Google Scholar]
- Rosenberg, M. Society and the adolescent self-image. Princeton, United states, 1965, 16-36. [CrossRef]
- Nasiriziba, F.; Saati, M.; Haghani, H. Correlation between self-efficacy and self-esteem in patients with an intestinal stoma. Br. J. Nurs. 2020, 29, S22–S29. [Google Scholar] [CrossRef]
- Choi, C.-H.; Choi, Y.-H.; Jeong, S.-H.; Cho, H.-J.; Son, C.-K.; Jeong, S.-H. Korea national children’s oral health survey. National Center for Medical Information and Knowledge (NCMIK), Korea, 2018.
- Public Health England. Survey of prison dental services England, Wales and Northern Ireland 2017 to 2018. Public Health England, 2022.
- The Scottish Government. Oral Health Improvement and Dental Services in Scottish Prisons. The Scottish Government, 2015.
- Billa, A.L.; Sukhabogi, J.R.; Doshi, D.; Jummala, S.; Turaga, S.S. Correlation of self-esteem with oral hygiene behaviour and oral health status among adult dental patients. Ann. Ig. 2023, 35, 534–545. [Google Scholar]
- Ibigbami, O.I.; Folayan, M.O.; Oginni, O.; Lusher, J.; Sam-Agudu, N.A. Moderating effects of resilience and self-esteem on associations between self-reported oral health problems, quality of oral health, and mental health among adolescents and adults in Nigeria. PLoS one 2023, 18, e0285521. [Google Scholar] [CrossRef]
- Melbye, E.L. Dimensional structure of the OHIP-14 and associations with self-report oral health-related variables in home-dwelling Norwegians aged 70+. Acta Odontol. Scand. 2023, 81, 66–72. [Google Scholar] [CrossRef]
- Korea Centers for Disease Control and Prevention. 2022 Community health survey [Internet]. Korea Centers for Disease Control and Prevention. 2022. Available online: https://chs.kdca.go.kr/chs/ststs/statsMain.do (accessed on 15 Jul 2023).
- Korea Centers for Disease Control and Prevention. Korean National Health and Nutrition Examination Surveys 2013~2015. Available online: https://knhanes.cdc.go.kr/knhanes/sub01/sub01_02.do#s2_01 (accessed on 15 Jul 2023).
- The Korean Law Information Center. Act on the Execution of Penalties and Treatment of Inmates. The Korean Law Information Center, 2022 Available online: Act on Execution of Sentences and Treatment of Prisoners (law.go.kr) (accessed on 15 Jul 2023).
- Park, C.-S.; Kim, I.-J. Oral health behaviour according to perceived oral symptoms in the elderly. J. Korean Soc. Dent. Hyg. 2016, 16, 955–968. [Google Scholar] [CrossRef]
- Hong, M.-H.; Lee, J.-M.; Jang, K.-W. Effect of oral health status and work loss on oral health-related quality of life of non-medical hospital workers. J. Converg. Inf. Technol. 2022, 12, 163–173. [Google Scholar]
- Kim, A.-J.; Kang, E.-J. A study on the oral symptoms and oral health-related quality of life (OHIP-14) of industrial workers. J. Dent. Hyg. Sci. 2014, 14, 51–58. [Google Scholar]
- Moon, B.; Jeong, S.-R.; Jang, J.-Y.; Kim, K.-Y. Health-related quality of life by oral health behaviour and oral health status for the middle-aged people. J. Korean Soc. Dent. Hyg. 2015, 15, 197–204. [Google Scholar] [CrossRef]
- Park, E.-S.; Choi, J.-S. The effect of health status on general quality of life and oral health related quality of life in the middle-aged adults. J. Dent. Hyg. Sci. 2012, 12, 624–633. [Google Scholar]
- Yoon, S.-U.; Nam, I.-S. Oral health impact profile (OHIP) according to the oral health behaviour of foreign workers. J. Korean Soc. Dent. Hyg. 2015, 15, 451–459. [Google Scholar] [CrossRef]
- Yoon, H.-S. Relationship of oral health status and oral health care to the quality of life in patients of dental hospitals and clinics. J. Dent. Hyg. Sci. 2015, 15, 594–602. [Google Scholar] [CrossRef]
- Kim, J.-L.; Kim, J.-H.; Jang, J.-H. Relationship between dental checkups and unmet dental care needs in Korean adults. J. Korean Soc. Dent. Hyg. 2020, 20, 581–591. [Google Scholar]
- Jang, J.-H.; Kim, J.-L.; Kim, J.-H. Associations between dental checkups and unmet dental care needs: An examination of cross-sectional data from the seventh Korea National Health and Nutrition Examination Survey (2016–2018). Int. J. Environ. Res. Public Health 2021, 18, 3750. [Google Scholar] [CrossRef]
- Lee, E.-J.; Kim, M.-G. The effect of oral function on the quality of kife of Korean adults by age group. Korean J. Heal. Serv. Manag. 2016, 10, 99–110. [Google Scholar] [CrossRef]
- Lee, M.-R.; Choi, J.-S. Relationship of self-perceived symptoms of periodontal disease to quality of life in adults. J. Dent. Hyg. Sci. 2012, 12, 115–121. [Google Scholar]
- Lee, J.-Y.; Kim, G.-P.; Yu, B.-C. Relationship between periodontal disease and quality of life. J. Korean Soc. Dent. Hyg. 2013, 13, 835–843. [Google Scholar] [CrossRef]
- Park, M.-S.; Jang, J.-H. Relationship between health risk behaviors, oral health-related quality of life (OHIP-14) and happiness in soldiers. J. Korean Soc. Dent. Hyg. 2017, 17, 1159–1169. [Google Scholar]
- Lee, S.-L.; Kwag, J.-S.; Choi, J.-H. Correlation and influencing factors on oral health awareness, oral health behaviour, self-esteem and OHIP-14 in childcare teachers. J. Korean Soc. Dent. Hyg. 2015, 15, 261–269. [Google Scholar] [CrossRef]
- Grecu, A.G.; Balazsi, R.; Dudea, D.; Mesaro, A.; Strmbu, M.; Dumitracu, D.L. Oral health related quality of life and self-esteem in a general population. Med. Pharm. Rep. 2019, 92, S65–S72. [Google Scholar] [CrossRef]
- Park, Y.-N.; Lee, M.-R. Main cause of influencing oral health impact profile (OHIP) and self-esteem of orthodontic patients. J. Korean Soc. Dent. Hyg. 2010, 10, 513–522. [Google Scholar]
- Gobic, M.B.; Kralj, M.; Harmicar, D.; Cerovic, R.; Maricic, B.M.; Spalj, S. Dentofacial deformity and orthognathic surgery: Influence on self-esteem and aspects of quality of life. J. Craniomaxillofac. Surg. 2021, 49, 277–281. [Google Scholar] [CrossRef]
- United Nations (UN). Available online: https://treaties.un.org/Pages/ViewDetails.aspx?src=TREATY&mtdsg_no=IV-4&chapter=4&clang=_en (accessed on 21 Sep 2022).
- Korean Ministry of Government Legislation. Available online: https://www.law.go.kr/ Laws/Constitution of the Republic of Korea (accessed on 04 Nov 2022).
- Chun, J.-H. A study on correctional medical treatment for disabled prisoners and sick prisoners. J. Welf. Corr. 2021, 73, 175–202. [Google Scholar] [CrossRef]
- Lee, S.-G.; Sun, J.-G.; Park, I.-K.; Kang, H.-H.; Kim, S.-Y.; Sohn, M.-S. Correctional health care delivery system and prisoners’ human rights. Korean J. Med. L. 2009, 17, 121–150. [Google Scholar]
- Park, Y.-K. Medical treatment for prisoners. Correct. Rev. 2010, 48, 73–104. [Google Scholar]
Figure 1.
Toothbrushing behaviour in a day among adult male inmates
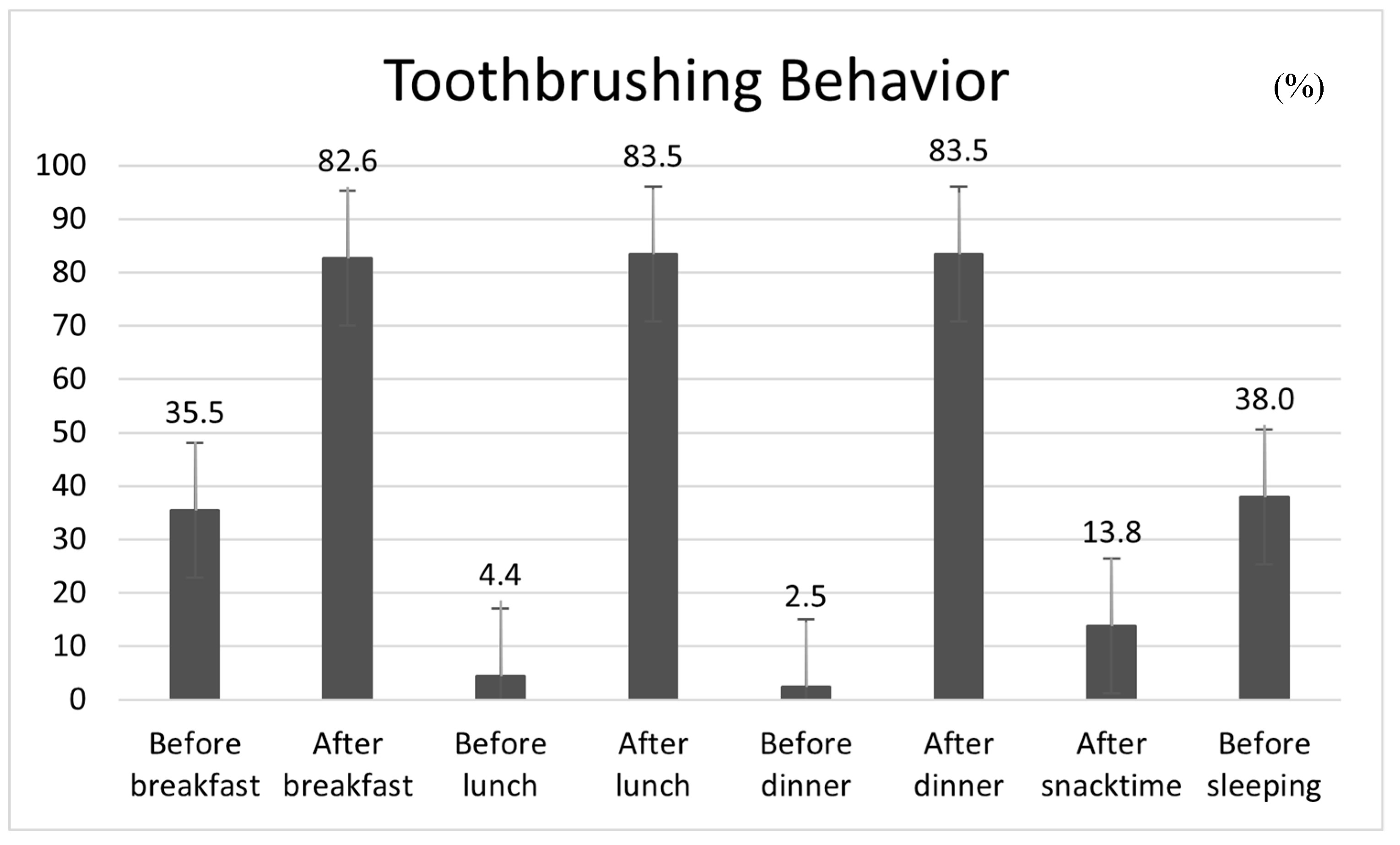
Figure 2.
Perceived oral symptoms among adult male inmates. TMJ, temporomandibular joint
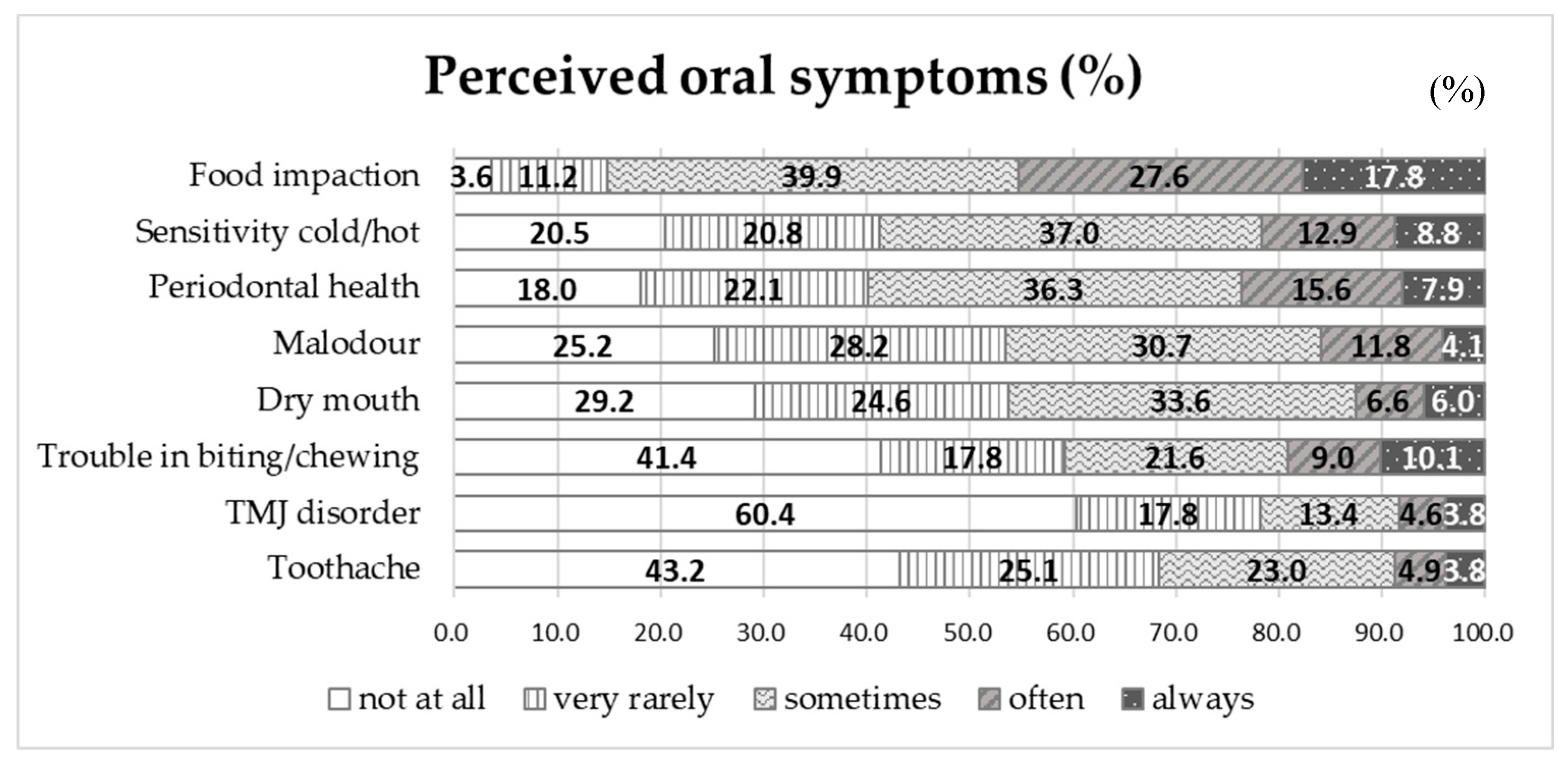

Table 1.
The OHP-14 scores according to the generalized characteristics in adult male inmates.
| Variables | Division | N (%) | OHIP-14 | |
|---|---|---|---|---|
| M ± SD | p-Value* | |||
| Age (years) | 20–29 a | 37 (10.2) | 46.86 ± 10.57 | < 0.001 |
| 30–39 ab | 80 (22.0) | 43.60 ± 10.84 | ||
| 40–49 bc | 85 (23.4) | 39.84 ± 13.39 | ||
| 50–59 c | 99 (27.3) | 36.15 ± 12.07 | ||
| ≥ 60 c | 62 (17.1) | 36.39 ± 11.28 | ||
| EDT (for last year) | Yes | 110 (30.3) | 38.26 ± 13.39 | 0.265 |
| No | 246 (67.8) | 40.59 ± 12.06 | ||
| Don’t know | 7 (1.9) | 39.71 ± 4.79 | ||
| EDE (for last year) | Yes | 145 (39.8) | 41.19 ± 12.04 | 0.247 |
| No | 214 (59.0) | 38.96 ± 12.70 | ||
| Don’t know | 5 (1.4) | 40.60 ± 5.59 | ||
| Toothbrushing time (min) | < 1 a | 51 (14.01) | 37.12 ± 12.37 | 0.02 |
| 1 to less than 2 ab | 126 (34.62) | 38.10 ± 13.06 | ||
| 2 to less than 3 b | 121 (33.24) | 41.87 ± 10.84 | ||
| ≥ 3 b | 66 (18.13) | 41.73 ± 13.12 | ||
| Use of fluoride toothpaste | Use | 173 (47.92) | 39.90 ± 11.89 | 0.432 |
| No use | 73 (20.22) | 38.60 ± 11.67 | ||
| Don’t know | 115 (31.86) | 40.97 ± 13.15 | ||
| Chewing discomfort | Tofu & Ricea | 21 (5.8) | 25.81 ± 13.04 | < 0.001 |
| Applea | 9 (2.5) | 26.22 ± 15.47 | ||
| Kimchiab | 36 (10.0) | 29.06 ± 12.80 | ||
| Meatbc | 61 (16.9) | 37.30 ± 90.4 | ||
| Dried squidbc | 29 (8.1) | 36.45 ± 11.53 | ||
| Hard candyc | 204 (56.7) | 45.46 ± 8.80 | ||
| Subjective health | Strongly disagreea | 56 (15.38) | 26.41 ± 13.86 | < 0.001 |
| Disagreeb | 93 (25.55) | 36.47 ± 10.17 | ||
| Neutralbc | 123 (33.79) | 43.22 ± 8.95 | ||
| Agreec | 82 (22.53) | 46.89 ± 9.38 | ||
| Strongly agreec | 10 (2.75) | 48.10 ± 12.77 | ||
| Subjective oral health | Strongly disagreea | 78 (21.49) | 27.77 ± 13.58 | < 0.001 |
| Disagreeb | 130 (35.81) | 38.68 ± 9.78 | ||
| Neutralbc | 117 (32.23) | 46.01 ± 8.00 | ||
| Agreebc | 34 (9.37) | 49.26 ± 7.57 | ||
| Strongly agreec | 4 (1.10) | 54.75 ± 1.89 | ||
| Self-esteem | High | 49 (13.39) | 41.10 ± 15.64 | 0.547 |
| Usual | 252 (68.85) | 40.12 ± 11.97 | ||
| Low | 65 (17.76) | 38.65 ± 10.55 | ||
| Total | 376 (100.0) | 39.90 ± 12.38 | ||
*by one way ANOVA test at α = 0.05; a,b,c Means followed by different letters are statistically significantly different by Scheffe test at α=0.05; EDT = Experience of dental treatment; EDE = Experience of dental examination.
Table 2.
Correlation between main variables and OHIP-14 in adult male inmates.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Food impaction | 1 | |||||||||
| 2. Sensitivity cold/hot | 0.492** | 1 | ||||||||
| 3. Periodontal health | 0.434** | 0.566** | 1 | |||||||
| 4. Malodour | 0.373** | 0.507** | 0.633** | 1 | ||||||
| 5. Dry mouth | 0.316** | 0.446** | 0.499** | 0.622** | 1 | |||||
| 6. Trouble biting/chewing | 0.366** | 0.570** | 0.555** | 0.520** | 0.514** | 1 | ||||
| 7. TMJ disorder | 0.176** | 0.340** | 0.386** | 0.431** | 0.426** | 0.447** | 1 | |||
| 8. Toothache | 0.318** | 0.509** | 0.548** | 0.536** | 0.520** | 0.628** | 0.583** | 1 | ||
| 9. Self-esteem | 0.018 | 0.008 | -0.050 | -0.114* | -0.063 | -0.040 | -0037 | -0.023 | 1 | |
| 10. OHIP-14*** | -0.338** | -0.546** | -0.570** | -0.552** | -0.523** | -0.749** | -0.488** | -0.649** | 0.057 | 1 |
*p < 0.05, **p < 0.01 by Pearson’s correlation coefficient at α = 0.01; OHIP-14 = Oral health impact profile-14; TMJ = temporomandibular joint.
Table 3.
Factors related to OHIP-14 in adult male inmates.
| Model 1 | Model 2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | ß | t | p-Value* | B | SE | ß | t | p-Value* | |
| (Constant) | 20.705 | 2.998 | 6.905 | < 0.001 | 53.394 | 3.381 | 15.790 | < 0.001 | ||
| Age | -0.093 | 0.038 | -0.099 | -2.436 | 0.015 | -0.138 | 0.031 | -0.146 | -4.412 | < 0.001 |
| Subjective health | 2.259 | 0.597 | 0.200 | 3.785 | < 0.001 | 1.482 | 0.471 | 0.131 | 3.146 | 0.002 |
| Subjective oral health | 3.493 | 0.676 | 0.278 | 5.168 | < 0.001 | 0.755 | 0.570 | 0.060 | 1.326 | 0.186 |
| Chewing discomfort (ref. = Tofu & Rice) | ||||||||||
| Apple | -2.735 | 3.569 | -0.034 | -0.766 | 0.444 | -4.808 | 2.809 | -0.060 | -1.712 | 0.088 |
| Kimchi | 3.100 | 2.400 | 0.077 | 1.292 | 0.197 | 0.273 | 1.908 | 0.007 | 0.143 | 0.886 |
| Meat | 8.629 | 2.207 | 0.270 | 3.910 | < 0.001 | 3.196 | 1.778 | 0.100 | 1.798 | 0.073 |
| Squid | 5.675 | 2.548 | 0.126 | 2.228 | 0.027 | 1.279 | 2.041 | 0.028 | 0.627 | 0.531 |
| Candy | 12.665 | 2.080 | 0.522 | 6.089 | < 0.001 | 4.255 | 1.768 | 0.175 | 2.407 | 0.017 |
| Perceived oral symptoms | ||||||||||
| Food impaction | 0.212 | 0.423 | 0.018 | 0.502 | 0.616 | |||||
| Sensitivity cold/hot | 0.400 | 0.429 | 0.039 | 0.931 | 0.353 | |||||
| Periodontal health | -0.936 | 0.463 | -0.089 | -2.021 | 0.044 | |||||
| Malodour | -1.423 | 0.481 | -0.131 | -2.957 | 0.003 | |||||
| Dry mouth | -0.008 | 0.425 | -0.001 | -0.018 | 0.985 | |||||
| Trouble biting/chewing | -2.735 | 0.429 | -0.307 | -6.376 | < 0.001 | |||||
| TMJ disorder | -1.086 | 0.409 | -0.099 | -2.656 | 0.008 | |||||
| Toothache | -1.687 | 0.491 | -0.154 | -3.439 | 0.001 | |||||
| F (p-Value) | 44.754 (< 0.001) | 51.631 (< 0.001) | ||||||||
| R2 | 0.511 | 0.711 | ||||||||
| Adj. R2 | 0.499 | 0.698 | ||||||||
*by hierarchical multiple linear regression at α = 0.05; TMJ = temporomandibular joint.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



