
Submitted:
12 September 2023
Posted:
14 September 2023
You are already at the latest version
Abstract
Background: Myocardial infarction (MI) is a major cause of mortality worldwide. Its presentation as ST-segment elevation MI (STEMI) and non-ST-segment elevation MI (NSTEMI) is influence by atherosclerosis risk factors.
Aim: To assess the patterns of presentation and predicting risk factors of acute MI in Kosovo.
Methods: This is a cross sectional study from the Clinic of Cardiology of the University Clinical Center of Kosovo, which included all patients hospitalized with acute MI over a period of 7 years (January 1st, 2014 to December 31st, 2020). Data was collected using a structured questionnaire and epidemiological patterns and risk factors were analyzed.
Results: Among 7353 patients admitted with acute MI (age 63 ± 12 years, 29% female), 4366 (59.4%) patients had STEMI, and 2987 (40.6%) NSTEMI. Patients age was not different between the two groups (p=0.077). NSTEMI patients smoked less (48.3% vs. 54%, p<0.001), but were more diabetics (37.8% vs. 33.6%, p<0.001), more hypertensives (69.6% vs. 63%, p<0.001), frequently had family history for coronary artery disease (CAD) (40% vs 38%, p=0.009), and included more females compared to STEMI patients (32% vs 27%, p<0.001). The two groups of patients, did not differ in the prevalence of significant CAD on angiography (66.8% vs. 67.8%, p = 0.396), but NSTEMI patients underwent less primary percutaneous interventions compared with STEMI patients (43.6% vs. 55.2%, p < 0.001).
Conclusion: In Kosovo, STEMI is commoner than NSTEMI, who were mostly males, more likely to have diabetes, hypertension and family history for CAD compared to those with NSTEMI. Smoking and arterial hypertension proved the strongest predictors of acute MI, in Kosovo, thus highlighting the urgent need for better atherosclerosis risk control and education strategy.
Keywords:
Myocardial infarction
; risk factors
; smoking
; diabetes
; arterial hypertension
; age
; gender
1. Introduction
In the past decades, epidemiological patterns of coronary artery disease (CAD) and acute myocardial infarction (MI) have changed worldwide (1) with some European countries showing a significant fall in the incident of acute CAD cases (2). However, CAD remains the main global cause of death, particularly in low- and middle-income countries (3,4). Moreover, the epidemiology and the risk factors for CAD differ, is impacted by differences in geographic, socio-economic and environmental conditions between regions (5-11). The last decades witnessed significant improvement in the diagnosis and treatment of acute MI, emphasizing immediate diagnosis and risk stratification, as well as introducing interventional revascularization treatment in all patients with acute MI (12, 13). This resulted in a significant decline in the incidence of ST-segment elevation MI (STEMI) over the years, whereas that of non-ST-segment elevation MI (NSTEMI) gradually increased, most likely due to the advent of high-sensitivity biomarkers (14-16). The epidemiology and risk factors of CAD and acute MI in the general population and in patients with known CAD in the Republic of Kosovo remain ill determined (17). Therefore, the objective of this study was to assess the occurrence, clinical characteristics, and impact of risk factors in patients with different types of acute MI in Kosovo.
2. Methods
This study was conducted at the Clinic of Cardiology of the University Clinical Center of Kosovo, Prishtina, using a cross sectional descriptive analysis. All patients hospitalized with acute MI (a total of 7353 patients) over a period of 7 years (from 1stJanuary 2014 to 31st December 2020) were included in the study. After receiving approval from the University Clinical Service's Ethics Council, data were collected by a researcher who administered a structured questionnaire, for all patients with acute MI. The epidemiological data from patients’ records, including age, gender, risk factors (smoking, arterial hypertension, diabetes, dyslipidemia and family history for CAD), clinical data (cardiogenic shock, duration of hospitalization, outcome), biochemical data (glycemia at admission, cholesterol, triglycerides, urea, creatinine, hemoglobin, troponin), electrocardiogram, medications and data from an echocardiographic examination at admission were collected. In addition, conventional coronary angiographic data and the results of the interventional treatment were registered. Acute MI was diagnosed based on electrocardiogram and conventional raised levels of myocardial biomarkers. Patients were divided into two groups based on the ST-segment elevation at admission: 1) non-ST-segment elevation myocardial infarction (NSTEMI) and 2) ST-segment elevation myocardial infarction (STEMI) (16).
We compared the data of our acute MI, Kosovo patients with those from Northern (Finland) and Southern (Greece) Europe (17).
Statistical analysis
Patients' clinical characteristics were collected retrospectively from the medical records, which then underwent several thorough statistical analyses. Continuous variables are presented as mean ± SD and categorical variables as frequencies and percentages. Logistic regression analysis was performed to determine the predictors of in-hospital mortality among patients with acute MI, as well as in those with STEMI and NSTEMI. Significance was determined based on a p-value <0.05. Statistical analyses were performed using IBM SPSS Statistics for Windows Operating System, version 24.0 software (IBM Corp., Armonk, N.Y., USA).
3. Results
General data of patients with AMI
In this study, we included 7353 patients admitted with acute MI (mean age 63 ± 12 years, 29% female) during the seven years period (2014 - 2022). According to the final discharge diagnosis, 4366 (59.4%) patients were identified with STEMI, and 2987 (40.6%) with NSTEMI. Among all patients admitted with acute MI, 1188 (16%) were transferred to another primary PCI hospital, whereas 84% remained for treatment at our Center.
STEMI versus NSTEMI patients
Patients’ age was not different between the two groups (p=0.077), but the NSTEMI cohort had less smokers (48.3% vs. 54%, p<0.001), more diabetics (37.8% vs. 33.6%, p<0.001), more hypertensives (69.6% vs. 63%, p<0.001), more patients with family history for CAD (40% vs 38%, p=0.009), and more females (32% vs 27%, p<0.001) compared to the STEMI cohort (Table 1). At admission, patients with NSTEMI had lower glucose (9.2 ± 5 vs. 9.8 ± 6 mmol/L, p < 0.001), and higher triglycerides (2.0 ± 1.2 vs. 1.88± 1.3 mmol/L, p=0.001) levels compared with STEMI patients, whereas cholesterol, urea, creatinine and hemoglobin did not differ between the two cohorts (Table 1). Also at admission, patients with NSTEMI had less atrial fibrillation (3.9% vs. 5%, p = 0.035), less left bundle branch block (2.6% vs. 5.3%, p < 0.001), higher left ventricular ejection fraction (51.6 ± 9% vs. 49.8 ± 9%, p<0.001) and less cardiogenic shock (2.1% vs. 4.9%, p < 0.001) compared to STEMI patients (Table 1).
There was no difference between the two cohorts with respect to the presence of significant CAD on diagnostic coronary angiography (66.8% vs. 67.8%, p = 0.396), but patients with NSTEMI underwent less primary percutaneous interventions compared with STEMI patients (43.6% vs. 55.2%, p < 0.001) (Table 2).
Risk factors predicting STEMI and NSTEMI
Arterial hypertension and smoking were the two independent predictors of both presentations of acute MI. However, female gender independently predicted the occurrence of STEMI and diabetes mellitus independently predicted the occurrence of NSTEMI (Table 3).
The age and gender in patients with acute AMI
The highest percentage of patients with acute MI belonged to the 60–69-year age group (29.6%), followed by the 50-59-year age group (26%) (Figure 1). These percentages were not influenced by the type of acute MI patients had, NSTEMI or STEMI (Figure 1). The highest percentage of female patients with acute MI belonged to the 70-79-year age group (32.3%), followed by 60–69-year age group (29%), whereas the highest percentage of male patients was among the 60–69-year age group (29.9%), followed by 50–59-year age group (29.3%) (Figure 2). Thus, there was a 10 years difference as a gender determined occurrence of acute MI.
Comparison between acute MI patients in Kosovo and North and South Europe
STEMI was significantly more frequently occurring in patients with acute MI in Kosovo compared to those in Finland and Greece (Table 4, Figure 3), there was no difference between the latter two countries. Kosovo patients with acute MI were younger than those in Finland and Greece (P<0.001, Figure 4A). The percentage of females admitted with acute MI in Kosovo was lower than in Finland and higher than in Greece (P<0.001, Figure 4B). The prevalence of smoking, diabetes mellitus and arterial hypertension was higher in Kosovo compared to Finland and Greece (P<0.001, Figure 4 C, D, E). While the prevalence of diabetes and hypertension did not differ between Finland and Greece, smoking was more in Greece compared to Finland (Figure 4 C, D, E).
4. Discussion
The aim of this observational study was to provide a real contemporary descriptive picture of patients presenting with acute MI, admitted to the University Clinical Centre of Kosova, the only tertiary healthcare center in Kosovo during a 7 years period, with an aim of identifying the areas requiring improvement of the overall management strategy of such patients. The findings of this study also reflect the pattern of atherosclerosis risk factors these patients had and its relationship with acute MI as well as the extent of differences in comparison with other European countries. This study represents the largest real population survey of almost all patients referred with acute MI from all regional hospitals of Kosovo, to our heart center, for optimum treatment. This study deserves to be described as consecutive.
Findings:
Our data analysis shows that in Kosovo, females suffered less MIs than males. The majority of cases presenting with acute MI had STEMI who were less commonly having diabetes, arterial hypertension and family history for CAD, but smoked more, compared to those presenting with NSTEMI. Also, Kosovo STEMI patients had higher incidence of atrial fibrillation, left bundle branch block, lower left ventricular ejection fraction and more cardiogenic shock compared to NSTEMI patients. In addition, females were more prevalent among the NSTEMI compared to STEMI patients. Moreover, the highest percentage of patients with acute MI belonged to the 60–69-year age group, with the highest percentage of females in the 70-79-year age group. Finally, Kosovo patients admitted with acute MI had specific characteristics when compared with other European countries, irrespective of their geographical location, north (Finland) or south (Greece). The majority of Kosovo patients presented with STEMI compared with the rest of Europe who presented with NSTEMI. Kosovo patients were younger by an average of 8 years from Finland patients and 4 years compared to Greek patients. Over 50% of Kosovo patients smoked compared to only 20% Finish and 40% Greeks. The prevalence of diabetes and hypertension was also significantly higher in Kosovo patients compared to the other two European cohorts.
Data interpretation:
Our analysis shows that smoking and hypertension are the strongest predictors of acute MI irrespective of presentation, STEMI or NSTEMI. This reflects a cultural issue when compared with predictors in other countries, where dyslipidemia is a well-established factor (30). In the absence of a significant role of diabetes in predicting acute MI in our cohort, the accumulative risk of smoking and hypertension explains even the difference in MI presentation being mostly STEMI compared with other European countries, in which smoking and hypertensin are well controlled and most MI presentation is in the form of NSTEMI. This difference also reflects better established health services and patient education programs in the other European countries, particularly the northern ones, where smoking prevalence is significantly lower than that in the Mediterranean counterparts, as our analysis showed. The above interpretation could also explain the high prevalence of females admitted with acute MI compared with Greece, who are expected to lag behind males in developing atherosclerosis by approximately 10 years (31). Furthermore, the above proposed interpretation likely explains the significant young age at admission, we found, in our Kosovo patients compared with Finland and Greece. People usually start smoking early in life, hence its contribution to the significant young age at presentation with acute MI, our analysis showed.
Clinical Implications:
The findings of this large cohort of acute MI patients from Kosovo paves the way for a serious need for better atherosclerosis risk factors control with its well-tested beneficial impact on reducing the incidence of acute MI with its short- and long- term complications. Such control needs multidisciplinary strategy between health professionals and politicians, and also should have national implication, irrespective of population size, at least with serious revolution against smoking and various hypertension related risks. It would be of interest to analyze the pattern of risk factors contributing to acute strokes in Kosovo, the results of which should strengthen the atherosclerosis disease prevention strategy.
Limitations:
The data collected in this study was retrospective, but fulfilled all required and recognized criteria used before in other national registries. We would have liked to have more biomarkers to enrich the predictors search, but those were limited to conventionally analyzed ones used in daily practice, because of the retrospective nature of the study. Despite that, we succeeded to collect data from all patients admitted with acute MI, with no single case missed.
Conclusion:
In Kosovo, most patients present with STEMI, who were mostly males, were more likely to have diabetes, arterial hypertension and positive family history for CAD, but smoked less, compared to those with NSTEMI. Smoking and arterial hypertension proved the strongest predictors of acute MI, in Kosovo, thus highlighting the urgent need for better atherosclerosis risk control and education strategy.
Acknowledgments
We acknowledge nurses and doctors of the Clinic of Cardiology, at University Clinical Centre of Kosova, in Prishtina, for their contribution in the treatment of patients included in this study and for their support in collecting the data from the records.
References
- GBD 2017 Mortality Collaborators. Global, regional, and national age-sex-specific mortality and life expectancy, 1950-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1684–1735. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Hashim, M.J.; Mustafa, H.; Baniyas, M.Y.; Al Suwaidi, S.K.B.M.; Alkatheeri, R.; Alblooshi, F.M.K.; Almatrooshi, M.E.A.H.; Alzaabi, M.E.H.; Al Darmaki, R.S.; et al. Global Epidemiology of Ischemic Heart Disease: Results from the Global Burden of Disease Study. Cureus 2020, 12, e9349. [Google Scholar] [CrossRef] [PubMed]
- Nowbar, A.N.; Gitto, M.; Howard, J.P.; Francis, D.P.; Al-Lamee, R. Mortality from Ischemic Heart Disease. Circ Cardiovasc Qual Outcomes. 2019, 12, e005375. [Google Scholar] [CrossRef] [PubMed]
- Seligman, B.; Vedanthan, R.; Fuster, V. Acute coronary syndromes in low- and middle-income countries: Moving forward. Int. J. Cardiol. 2016, 217, S10–S12. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; et al. GBD-NHLBI-JACC Global Burden of Cardiovascular Diseases Writing Group. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update from the GBD 2019 Study. J Am Coll Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Zeymer, U.; Ludman, P.; Danchin, N.; Kala, P.; Laroche, C.; Sadeghi, M.; Caporale, R.; Shaheen, S.M.; Legutko, J.; Iakobsishvili, Z.; et al. Reperfusion therapies and in-hospital outcomes for ST-elevation myocardial infarction in Europe: the ACVC-EAPCI EORP STEMI Registry of the European Society of Cardiology. Eur. Hear. J. 2021, 42, 4536–4549. [Google Scholar] [CrossRef] [PubMed]
- Poloński, L.; Gasior, M.; Gierlotka, M.; Kalarus, Z.; Cieśliński, A.; Dubiel, J.S.; Gil, R.J.; Ruzyłło, W.; Trusz-Gluza, M.; Zembala, M.; Opolski, G. Polish Registry of Acute Coronary Syndromes (PL-ACS). Characteristics, treatments and outcomes of patients with acute coronary syndromes in Poland. Kardiol Pol. 2007, 65, 861–872. [Google Scholar] [PubMed]
- Mohanan, P.P.; Mathew, R.; Harikrishnan, S.; Krishnan, M.N.; Zachariah, G.; Joseph, J.; Eapen, K.; Abraham, M.; Menon, J.; Thomas, M.; et al. Presentation, management, and outcomes of 25 748 acute coronary syndrome admissions in Kerala, India: results from the Kerala ACS Registry. Eur. Hear. J. 2012, 34, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Insam, C.; Paccaud, F.; Marques-Vidal, P. Trends in hospital discharges, management and in-hospital mortality from acute myocardial infarction in Switzerland between 1998 and 2008. BMC Public Heal. 2013, 13, 270. [Google Scholar] [CrossRef] [PubMed]
- Hanssen, M.; Cottin, Y.; Khalife, K.; Hammer, L.; Goldstein, P.; Puymirat, E.; Mulak, G.; Drouet, E.; Pace, B.; Schultz, E.; et al. French Registry on Acute ST-elevation and non ST-elevation Myocardial Infarction 2010. FAST-MI 2010. Hear. 2012, 98, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Sanchis-Gomar, F.; Perez-Quilis, C.; Leischik, R.; Lucia, A. Epidemiology of coronary heart disease and acute coronary syndrome. Ann. Transl. Med. 2016, 4, 256. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Ludman, P.; Zeymer, U.; Danchin, N.; Kala, P.; Laroche, C.; Sadeghi, M.; Caporale, R.; Shaheen, S.M.; Legutko, J.; Iakobishvili, Z.; et al. Care of patients with ST-elevation myocardial infarction: an international analysis of quality indicators in the acute coronary syndrome STEMI Registry of the EURObservational Research Programme and ACVC and EAPCI Associations of the European Society of Cardiology in 11 462 patients. Eur. Hear. Journal. Acute Cardiovasc. Care 2022, 12, 22–37. [Google Scholar] [CrossRef]
- McManus, D.D.; Gore, J.; Yarzebski, J.; Spencer, F.; Lessard, D.; Goldberg, R.J. Recent Trends in the Incidence, Treatment, and Outcomes of Patients with STEMI and NSTEMI. Am. J. Med. 2011, 124, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Meyers, H.P.; Bracey, A.; Lee, D.; Lichtenheld, A.; Li, W.J.; Singer, D.D.; Kane, J.A.; Dodd, K.W.; Meyers, K.E.; Thode, H.C.; et al. Comparison of the ST-Elevation Myocardial Infarction (STEMI) vs. NSTEMI and Occlusion MI (OMI) vs. NOMI Paradigms of Acute MI. J. Emerg. Med. 2020, 60, 273–284. [Google Scholar] [CrossRef] [PubMed]
- André, R.; Bongard, V.; Elosua, R.; Kirchberger, I.; Farmakis, D.; Häkkinen, U.; et al. International differences in acute coronary syndrome patients' baseline characteristics, clinical management and outcomes in Western Europe: the EURHOBOP study. Heart. 2014, 100, 1201–1207. [Google Scholar] [CrossRef]
- Bajraktari, G.; Thaqi, K.; Pacolli, S.; Gjoka, S.; Rexhepaj, N.; Daullxhiu, I.; Sylejmani, X.; Elezi, S. In-hospital mortality following acute myocardial infarction in Kosovo: a single center study. Ann Saudi Med. 2008, 28, 430–434. [Google Scholar] [PubMed]
- Khraishah, H.; Alahmad, B.; Alfaddagh, A.; Jeong, S.Y.; Mathenge, N.; Kassab, M.B.; Kolte, D.; Michos, E.D.; Albaghdadi, M. Sex disparities in the presentation, management and outcomes of patients with acute coronary syndrome: insights from the ACS QUIK trial. Open Hear. 2021, 8, e001470. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, S.; Watanabe, T.; Arimoto, T.; Takahashi, H.; Shishido, T.; Miyashita, T.; Miyamoto, T.; Nitobe, J.; Shibata, Y.; Konta, T.; et al. Trends in Coronary Risk Factors Among Patients with Acute Myocardial Infarction Over the Last Decade: The Yamagata AMI Registry. J. Atheroscler. Thromb. 2010, 17, 989–998. [Google Scholar] [CrossRef] [PubMed]
- Boden, W.E.; O’rourke, R.A.; Teo, K.K.; Hartigan, P.M.; Maron, D.J.; Kostuk, W.; Knudtson, M.; Dada, M.; Casperson, P.; Harris, C.L.; et al. The Evolving Pattern of Symptomatic Coronary Artery Disease in the United States and Canada: Baseline Characteristics of the Clinical Outcomes Utilizing Revascularization and Aggressive DruG Evaluation (COURAGE) Trial. Am. J. Cardiol. 2007, 99, 208–212. [Google Scholar] [CrossRef] [PubMed]
- Malik, R.; Begum, S.; Afridi, M.N. ACUTE MYOCARDIAL INFARCTION; FREQUENCY OF MODIFIABLE RISK FACTORS. Prof. Med J. 2016, 23, 293–297. [Google Scholar] [CrossRef]
- Robert, W. Yeh, Stephen Sidney, Malini Chandra, Michael Sorel, Joseph V. Selby, and Alan S. Go. Population Trends in the Incidence and Outcomes of Acute Myocardial Infarction. N. Engl. J. Med. 2010, 362, 2155–2165. [Google Scholar]
- Rogers, W.J.; Frederick, P.D.; Stoehr, E.; Canto, J.G.; Ornato, J.P.; Gibson, C.M.; Pollack, C.V.; Gore, J.M.; Chandra-Strobos, N.; Peterson, E.D.; et al. Trends in presenting characteristics and hospital mortality among patients with ST elevation and non-ST elevation myocardial infarction in the National Registry of Myocardial Infarction from 1990 to 2006. Am. Hear. J. 2008, 156, 1026–1034. [Google Scholar] [CrossRef] [PubMed]
- Shyu, K.-G. Improvement of Outcomes in Acute Coronary Syndrome (ACS) by Getting with the Guidelines: From Taiwan ACS-full Spectrum Registry to Taiwan ACS-DM Registry. J Taiwan Cardiovasc Interv 2019, 8. [Google Scholar]
- Martínez, M.J.; Rueda, F.; Labata, C.; Oliveras, T.; Montero, S.; Ferrer, M.; El Ouaddi, N.; Serra, J.; Lupón, J.; Bayés-Genís, A.; et al. Non-STEMI vs. STEMI Cardiogenic Shock: Clinical Profile and Long-Term Outcomes. J. Clin. Med. 2022, 11, 3558. [Google Scholar] [CrossRef] [PubMed]
- Kirchberger, I.; Meisinger, C.; Heier, M.; Kling, B.; Wende, R.; Greschik, C.; von Scheidt, W.; Kuch, B. Patient-reported symptoms in acute myocardial infarction: differences related to ST-segment elevation. J. Intern. Med. 2011, 270, 58–64. [Google Scholar] [CrossRef]
- Martínez, M.J.; Rueda, F.; Labata, C.; Oliveras, T.; Montero, S.; Ferrer, M.; El Ouaddi, N.; Serra, J.; Lupón, J.; Bayés-Genís, A.; et al. Non-STEMI vs. STEMI Cardiogenic Shock: Clinical Profile and Long-Term Outcomes. J. Clin. Med. 2022, 11, 3558. [Google Scholar] [CrossRef] [PubMed]
- Takeji, Y.; Shiomi, H.; Morimoto, T.; Yamamoto, K.; Matsumura-Nakano, Y.; Nagao, K.; Taniguchi, R.; Yamaji, K.; Tada, T.; Kato, E.T.; et al. Differences in mortality and causes of death between STEMI and NSTEMI in the early and late phases after acute myocardial infarction. PLOS ONE 2021, 16, e0259268. [Google Scholar] [CrossRef] [PubMed]
- Elbadawi, A.; Elgendy, I.Y.; Mahmoud, K.; Barakat, A.F.; Mentias, A.; Mohamed, A.H.; Ogunbayo, G.O.; Megaly, M.; Saad, M.; Omer, M.A.; et al. Temporal Trends and Outcomes of Mechanical Complications in Patients with Acute Myocardial Infarction. JACC: Cardiovasc. Interv. 2019, 12, 1825–1836. [Google Scholar] [CrossRef] [PubMed]
- Bradley, S.M.; Borgerding, J.A.; Wood, G.B.; Maynard, C.; Fihn, S.D. Incidence, Risk Factors, and Outcomes Associated with In-Hospital Acute Myocardial Infarction. JAMA Netw. Open 2019, 2, e187348. [Google Scholar] [CrossRef] [PubMed]
- Nicoll, R.; Wiklund, U.; Zhao, Y.; Diederichsen, A.; Mickley, H.; Ovrehus, K.; Zamorano, J.; Gueret, P.; Schmermund, A.; Maffei, E.; et al. Gender and age effects on risk factor-based prediction of coronary artery calcium in symptomatic patients: A Euro-CCAD study. Atherosclerosis 2016, 252, 32–39. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Age distribution of the sample in STEMI and NSTEMI patients.
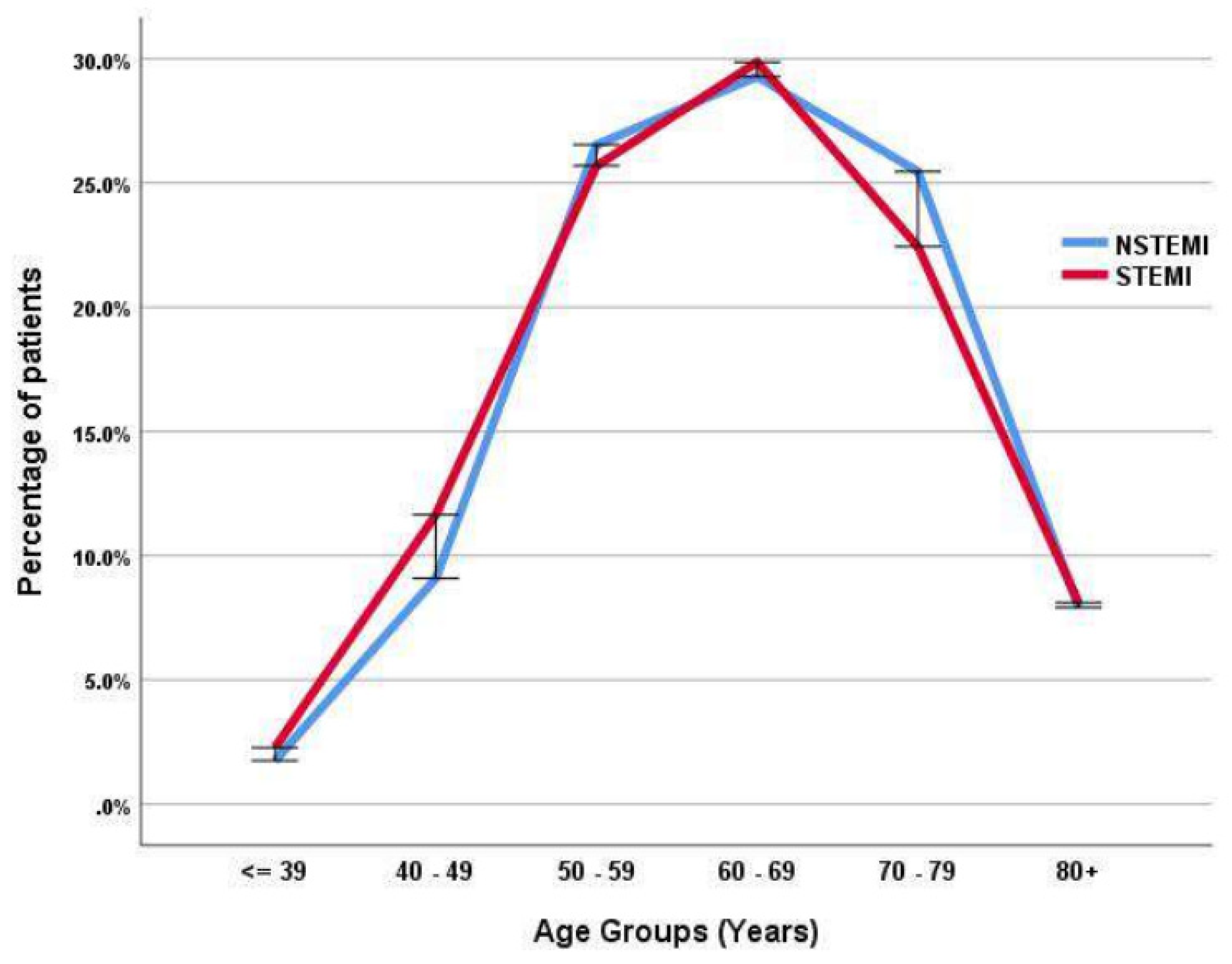
Figure 2.
Age distribution of the sample in male and female patients with acute myocardial infarction.
Figure 2.
Age distribution of the sample in male and female patients with acute myocardial infarction.
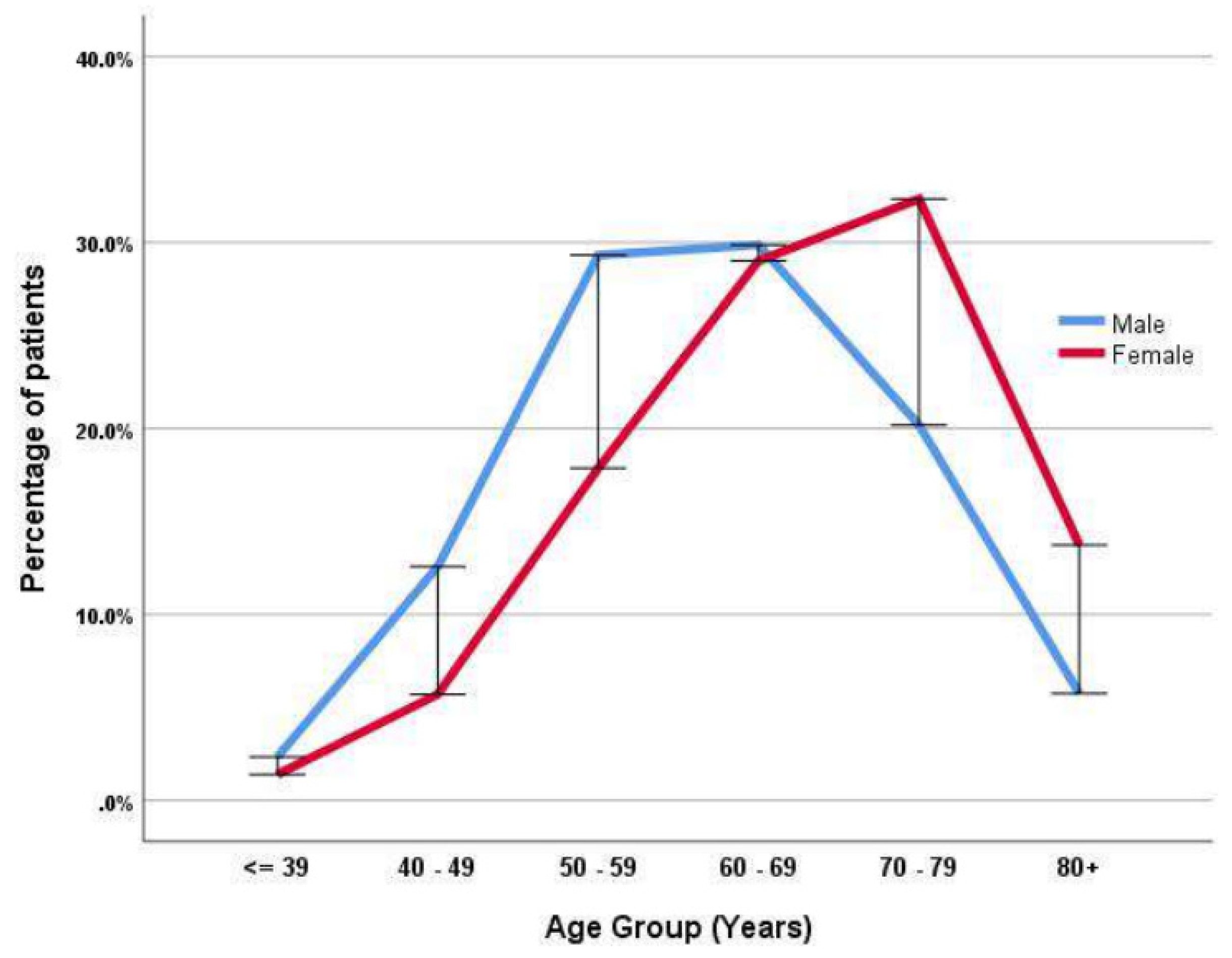
Figure 3.
Prevalence of STEMI and NSTEMI in patients with acute myocardial infarction in Kosovo, Finland and Greece.
Figure 3.
Prevalence of STEMI and NSTEMI in patients with acute myocardial infarction in Kosovo, Finland and Greece.
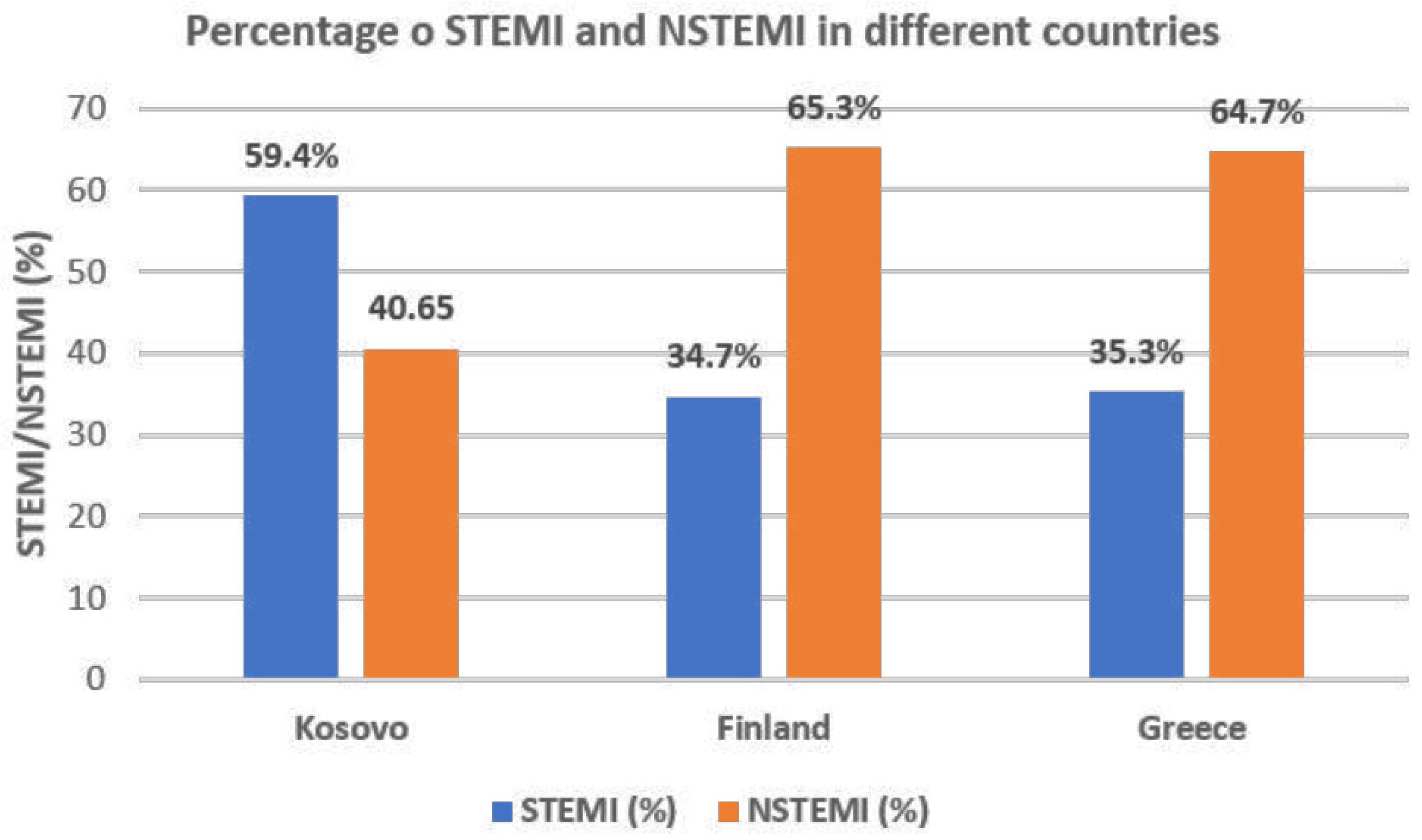
Figure 4.
Age (A) and gender (B) differences, and smoking (C), diabetes (D) and arterial hypertension (E) prevalences of patients with acute myocardial infarction between Kosovo, Finland and Greece.
Figure 4.
Age (A) and gender (B) differences, and smoking (C), diabetes (D) and arterial hypertension (E) prevalences of patients with acute myocardial infarction between Kosovo, Finland and Greece.
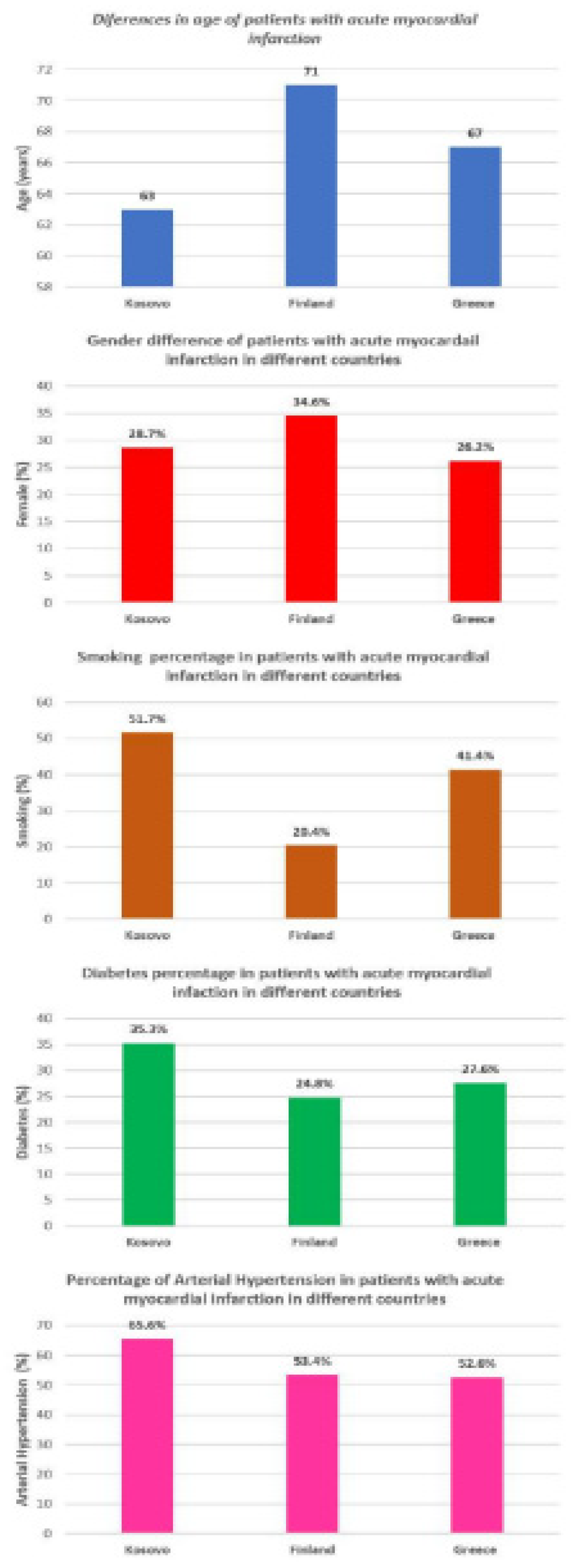

Table 1.
Clinical and biochemical data in patients with acute myocardial infarction.
| Variable | All included patients | Patients with NSTEMI | Patients with STEMI | P value |
|---|---|---|---|---|
| (n = 7353) | (n = 2987) | (n =4366) | ||
| Age (years) Female (%) |
63 ± 12 28.7 |
63 ± 11 31.7 |
64 ± 12 26.6 |
0.077 ˂0.001 |
| Smoking (%) Diabetes (%) |
51.7 35.3 |
48.3 37.8 |
54 33.6 |
˂0.001 ˂0.001 |
| Hypercholesterolemia (%) | 40.1 | 39.4 | 40.1 | 0.099 |
| Arterial hypertension (%) Family history for CAD (%) |
65.6 38.1 |
69.6 39.9 |
63 36.9 |
<0.001 0.009 |
| Atrial fibrillation (%) | 4.4 | 3.9 | 5.0 | 0.036 |
| Left bundle branch block (%) | 3.7 | 2.6 | 5.3 | <0.001 |
| Cardiogenic shock (%) | 3.7 | 2.1 | 4.9 | <0.001 |
| Fasting glucose (mmol/L) | 9.5 ± 5.5 | 9.2 ± 5 | 9.8 ± 6 | <0.001 |
| Total cholesterol (mmol/L) | 4.8 ± 1.6 | 4.8 ± 1.6 | 4.5 ± 1.5 | 0.939 |
| Triglycerides (mmol/L) | 1.9 ± 1.3 | 2.0 ± 1.3 | 1.88 ± 1.2 | 0.001 |
| Creatinine (μmol/L) Urea |
118 ± 74 9.2 ± 6 |
118 ± 74 9.2 ± 6 |
117 ± 73 9.1 ± 6 |
0.632 0.652 |
| Hemoglobin (g/dl) | 13.7 ± 3.2 | 13.7 ± 3.4 | 13.7 ± 3 | 0.942 |
| Heart rate at admission (beats/min) | 82.6 ± 23 | 82.5 ± 26 | 82.6 ± 20 | 0.822 |
| Left ventricular ejection fraction (%) | 50.6 ± 9 | 51.6 ± 9 | 49.8 ± 9 | <0.001 |
Legend: STEMI: ST-segment-elevation myocardial infarction; NSTEMI: Non-ST-segment elevation myocardial infarction, CAD: coronary artery disease.
Table 2.
Invasive treatment of patients with acute myocardial infarction.
| Variable | All included patients | Patients with NSTEMI | Patients with STEMI | P value |
|---|---|---|---|---|
| (n = 7353) | (n = 2987) | (n =4366) | ||
| Coronary angiography (%) | 67.3 | 66.8 | 67.8 | 0.396 |
| Primary Percutaneous Intervention (%) | 50.1 | 43.6 | 55.2 | <0.001 |
Legend: STEMI: ST-segment-elevation myocardial infarction; NSTEMI: Non-ST-segment elevation myocardial infarction.
Table 3.
Multivariate predictors of the type of Acute Myocardial Infarction.
| STEMI patients | NSTEMI patients | |||||
|---|---|---|---|---|---|---|
| Variable | OR | (CI 95%) | P value | OR | (CI 95%) | P value |
| Age Female gender Smoking Diabetes Arterial hypertension |
0.998 0.875 1.148 0.911 0.791 |
(0.994 - 1.002) (0.783 – 0.976) (1.037 - 1.271) (0.824 - 1.007) (0.714 - 0.878) |
0.412 0.017 0.008 0.069 <0.001 |
1.003 1.103 0.891 1.113 1.265 |
(0.999 - 1.008) (0.986 – 1.233) (0.804 - 0.988) (1.005 - 1.232) (1.139 - 1.405) |
0.151 0.086 0.028 0.039 <0.001 |
Legend: STEMI: ST-segment-elevation myocardial infarction; NSTEMI: Non-ST-segment elevation myocardial infarction.
Table 4.
The prevalence of conventional risk factors in Kosovo compared to Finland and Greece in patients admitted with acute myocardial infarction.
Table 4.
The prevalence of conventional risk factors in Kosovo compared to Finland and Greece in patients admitted with acute myocardial infarction.
| Variable | Kosovo | Finland | Kosovo | Greece | ||
|---|---|---|---|---|---|---|
| (n = 7353) | (n = 1813) | P value | (n = 7353) | (n =1185) | P value | |
| Age (years) Female (%) |
63 ± 12 28.7 |
71 ± 13 34.6 |
<0.000 <0.001 | 63 ± 12 28.7 |
67 ± 13 26.2 |
<0.001 <0.001 |
| Smoking (%) Diabetes (%) |
51.7 35.3 |
20.4 24.8 |
<0.001 <0.001 | 51.7 35.3 |
41.4 27.6 |
<0.001 <0.001 |
| Arterial hypertension (%) STEMI (%) |
65.6 59.4 |
53.4 34.7 |
<0.001 <0.001 | 65.6 59.4 |
52.6 35.3 |
<0.001 <0.001 |
| NSTEMI (%) | 40.6 | 65.3 | <0.001 | 40.6 | 64.7 | <0.001 |
Legend: STEMI: ST-segment-elevation myocardial infarction; NSTEMI: Non-ST-segment elevation myocardial infarction.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



