
Submitted:
09 September 2023
Posted:
13 September 2023
You are already at the latest version
Abstract
Resistance training is beneficial to adults for improving muscle strength and reducing the body composition. Nevertheless, little is known regarding online resistance training on anthropometric parameters and muscular strength (MS) in overweight female adolescents. This study aimed to examine the effects of online resistance training on anthropometric parameters and muscular strength (MS) in overweight female adolescents. This prospective, single-center, single-blinded, randomized controlled study included 60 overweight female adolescents who were divided into a control group (n=30) and an intervention group (n=30). The intervention group performed online resistance training, which focused on body weight training of 12 components (4 sets, 12 repetitions) for 45 min, three times per week, for 12 weeks. The intensity of training was 65–75%. Anthropometric parameters, including body weight (BW), body mass index (BMI), body circumference measurements (BCM), and muscle strength (MS), were assessed. All parameters were measured at weeks 0, 8, and 12. Within-group and between-group comparisons were performed. The results revealed improvements in MS, BW, BMI, and BCM in the intervention group. However, chest circumference was not significant. These findings suggest that online resistance training was effective in improving MS and reducing the body composition and circumference.
Keywords:
anthropometric parameters
; female adolescent
; online resistance training
; muscle strength
; overweight
1. Introduction
The World Health Organization (WHO) reported that there is a large number of overweight people, accounting for 1,900 million people [1]. More importantly, this overweight crisis could lead to obesity because there are over 650 million people who are obese. Approximately 40% of adults and 20% of children are now overweight or obese [2]. WHO also identified the negative effects of overweight people, including heart disease, respiratory disease, diabetes, and high blood pressure [1]. Those diseases are the leading cause of death in the world's population. The reason why the world's population is becoming overweight is because people consume too much without exercising. This could imply that the body needs less energy, but the amount of food consumed remains the same. This also leads to an overweight issue.
The prevalence of overweight is increasing globally, impacting individuals across all regions. Notably, this phenomenon has a disproportionately negative impact on women and adolescent girls. Regrettably, no nation has effectively managed to halt or reverse this prevailing trend [3]. In Thailand, the Ministry of Public Health reported that 17.4 million people are overweight. A higher percentage of overweight women (41.80%) than overweight men (32.92%) was shown in the report. This gives children, particularly women and females, greater autonomy over their food preferences. They are more likely to consume low-quality, energy-dense, or highly processed foods with appealing flavors or appearances, such as fast food, soft drinks, sugary beverages, and packaged munchies [4]. These foods negatively impact their health and eventually cause them to become overweight. More importantly, overweight and obesity not only affect a person's health and chance of dying, but they also add to the cost of health care and society as a whole [5,6]. In Thailand, the impact of being overweight on economic loss is over 12,000 million Thai baht, equivalent to 2.2% of all health expenditures in Thailand [7]. One of the best ways to light up the issue of being overweight or obese is exercising or doing active physical activities.
Girls and women are physically inactive due to their hectic lifestyles and limited access to exercise spaces [4]. Those who are overweight or obese appear to have low physical activity and fitness levels. The structured exercise training programs would be beneficial to them. Oppert, et al. [8] indicated that detailed physical activity recommendations and the implementation of structured exercise training programs are recognized as integral components of the management of overweight and obesity, behavioral support, and medication. As a result, increasing physical activity and fitness levels in people who are overweight or obese often has a significant positive effect on a variety of important clinical outcomes, including favorable changes in body composition, improved physical fitness, eating behavior, and health-related quality of life.
As mentioned about the advantages of physical activities, one of the factors is anthropometry. It entails the systematic measurement of the physical characteristics of the human body, especially the dimensions of body size and shape. The body mass index (BMI), waist-to-hip ratio, skin-fold test, and bioelectrical impedance analysis are commonly used to accomplish such measurements. It is important to be aware of the effects of changes in body size, structure, and composition and to be able to measure them [9]. Because health and body composition are related. Several research studies indicated the benefits of various physical activities and exercises, such as exercise training [10], aerobic training [11], and resistance training [12]. The focus of this study was resistance training.
This study focused on resistance training (RT), also known as strength training. RT involves the voluntary contraction of specific skeletal muscles against external resistance provided by body weight, free weights (such as barbells and dumbbells), or various exercise modalities (such as machines, springs, elastic bands, and traditional resistance) and is particularly beneficial for adults [13,14,15]. Strength training is carried out by sustaining or repeating muscular actions to increase muscle strength (MS) and muscle mass [16]. As an intervention, RT has profound impacts and reduces risk factors for cardiovascular disease, diabetes, and cancer [17]. The efficacy of RT as a treatment has been shown by earlier investigations. Strength exercise has been demonstrated to enhance body composition (i.e., a lower level of inflammation of the markers, higher levels of muscle mass) through increasing MS [18,19,20]. The American College of Sports Medicine recommends strength training as an auxiliary strategy for weight loss, with the aim of improving functional capacity via an increase in strength, muscle power, and daily energy expenditure [21]. Thus, RT inevitably became important and necessary for survival during the overweight crisis.
Traditionally, RT is usually conducted at gyms and fitness centers in order to increase MS and reduce anthropometry. Besides, the RT programs were identified as having benefits for adults [13,14,15]. However, online RT programs designed for young female adolescents are still limited. In 2021 and 2022, the American College of Sports Medicine has identified online training as the leading and third most popular phrase [15,16]. Online platforms allow people to connect with information and other people anywhere and anytime. Therefore, the present research aimed to investigate the effects of an online RT program on young female adolescents on their MS, BMI, and anthropometry.
2. Materials and Methods
2.1. Study Design
This present study employed quantitative research design [22]. The data gathered in this research were calculated to compare the effects of an online RT program on young female adolescents on their MS, BMI, and anthropometry using pre-test, middle-test, and post-test.
2.2. Participants
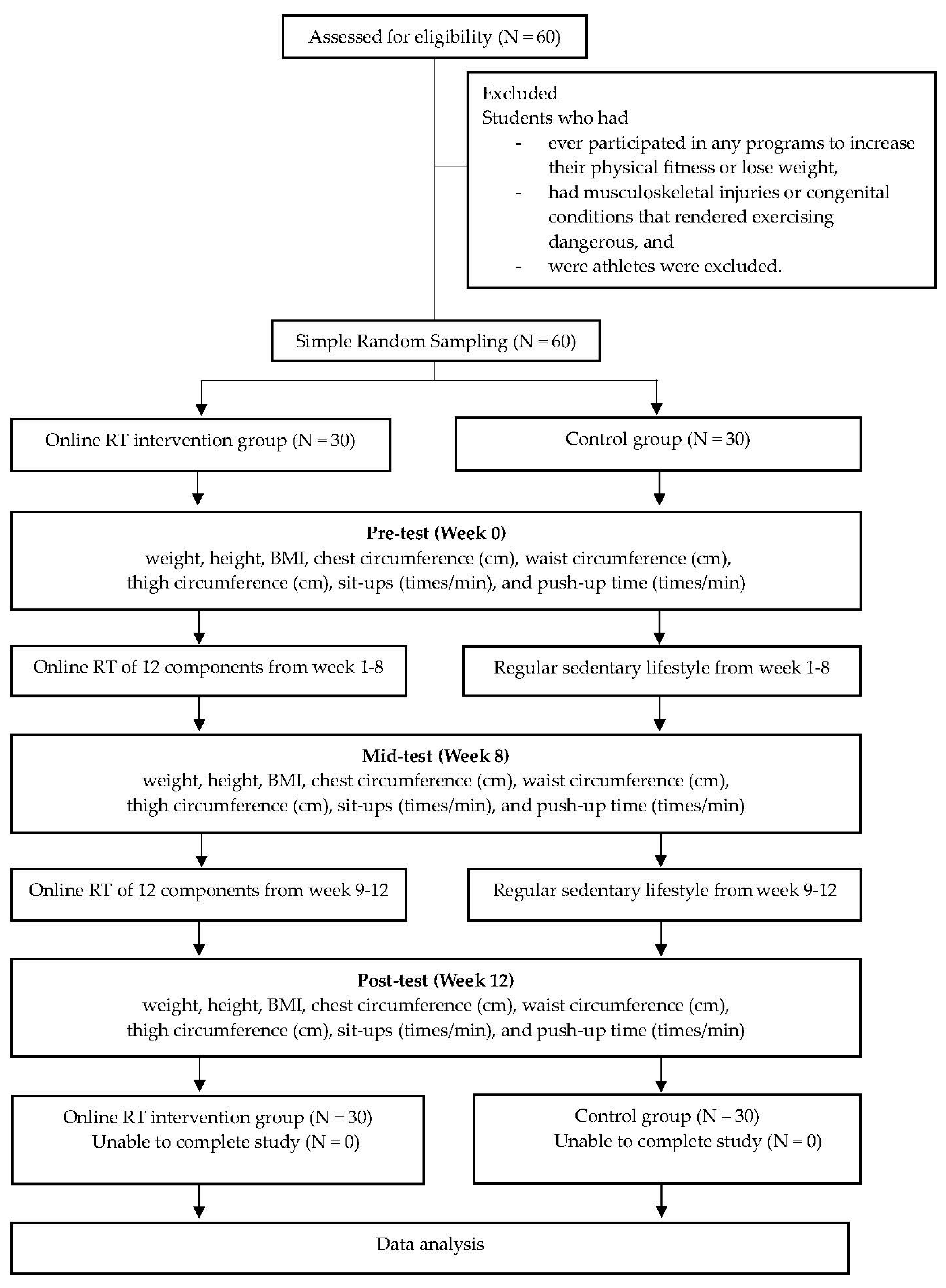
This study included 60 female adolescents at a university in the south of Thailand (1) who were between 18 and 22 years of age, (2) who had BMI between 23 and 26 kg/m2 according to recommendations for those in the World Health Organization Western Pacific Region [23], and (3) who had physical ability to exercise. Students who had ever participated in any programs to increase their physical fitness or lose weight, who had musculoskeletal injuries or congenital conditions that rendered exercising dangerous, and who were athletes were excluded.
The sample size for the randomized controlled experiment with continuous outcomes was calculated using the n4Studies program [24]. The difference in body mass was 3.30 ± 4.40 (mean ± standard deviation [25]) in the treatment group and 0.70 ± 0.10 in the control group, with a precision of 0.05, confidence level of 95%, and power of 80% (with β% of type II error) [26]. Consequently, the minimum sample size required to identify a difference between the two means was 23. The researchers divided the 60 selected and invited individuals into the online RT intervention group and control group by simple random and purposive sampling [22]. The study required 30 participants in each group (RT intervention and control groups), assuming a dropout rate of 30%.
In this present study, 30 students participated in the intervention group using the online RT program. On the contrary, another 30 students in the control group did not have control on them such as diet, rest, living conditions etc.
2.2. Intervention and Assessment
Anthropometric parameters (BW, BMI, and BCM) and MS (sit-ups and push-ups) were tested before, during, and after the online RT intervention in this prospective study, which involved a control group as well. This study was conducted between January and December 2021, with an intervention period of 12 weeks (between August and October 2021). In the experimental investigation, the online resistance training was conducted online for 45 min. In contrast, the control group adhered to their regular routine.
The research was carried out in compliance with the 1975 Declaration of Helsinki, with the amended version from 2013. The study received approval from the Ethics Committee on Human Research at Walailak University, located in Nakhon Si Thammarat, Thailand. The approval number assigned to the study was WUCE-21-076-01, and it was granted on May 14, 2021. Prior to the commencement of the trial, signed informed consent was collected from all participants.
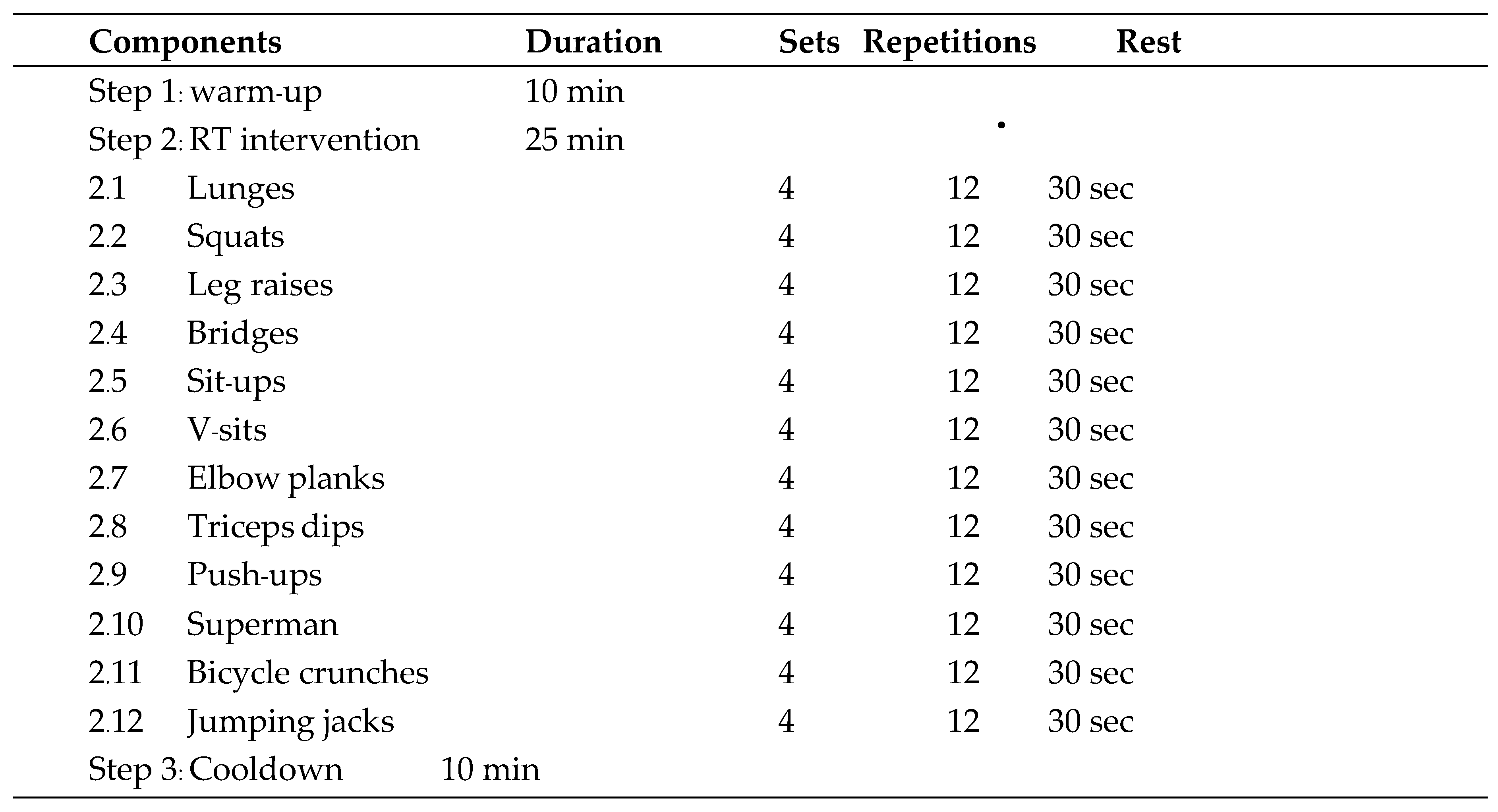
The online resistance training focused on performing core body and body weight training of 12 components, which included exercises such as lunges, squats, sit-ups, V-sits, elbow planks, triceps dips, bridges, leg raises, push-ups, superman, bicycle crunches, and jumping jacks (4 sets, 12 repetitions), during a continuous training period with a 20–30-sec break. The training lasted for 45 min, including 10–15 min of warm-up and cooldown. Exercises were performed for 12 weeks at an intensity of 65–75% of the maximum heart rate. The online RT program was validated by the five experts in sports science and physical education. In addition, the researcher conducted a pilot study with 10 female adolescents who have the same characteristics with the participants. The results from the pilot study were applied to adjust the online RT program according to the comments from the experts and the findings from the pilot study.

Table 1.
Online RT interventional components (three times/week for 12 weeks).
 |
Anthropometric parameters, including BW, BMI, BCM (e.g., chest circumference, waist circumference, hip circumference, thigh circumference), and MS (e.g., 30-sec sit-ups, 30-sec push-ups), were measured at weeks 0, 8, and 12.
Height was measured to the closest 0.1 cm in centimeters (cm), without socks or shoes. Weight in kilograms (kg) was measured using a digital electronic weighing scale. BMI was determined by multiplying the weight in kilograms by the square of height in meters. Body circumference was measured to the nearest 0.1 cm in centimeters (cm) using a non-elastic measuring tape. The lowest rib and iliac crest were used as landmarks to measure the waist circumference, whereas the center of the nipple was used to measure the chest circumference. The largest circumference below the waist and anterior superior iliac spine was utilized to calculate the hip circumference. Thigh circumference was measured on the right side of the mid-thigh.
Regarding sit-ups, the participants were instructed to lay on their back with flexed knees and with their feet flat on the floor. Their arms were crossed across their chest, and their hands were placed on either side of their shoulders. Their feet were tightly held to a mat by a partner. The participants were instructed to curl into a sitting position with their arms resting across their chests while using the cues “Prepare” and “Start.” One sit-up was considered complete when the elbows of the participants made contact with their thighs, and sit-ups were repeated for 60 sec.
As for push-ups, the participants lay face down with their arms straight and their palms placed slightly wider than the shoulder width. The legs were maintained equidistant from the floor, and both elbows were bent down to the floor. Once their elbows were 90° away from the spine, the participants paused to complete one repetition. Push-ups were repeated for 60 sec, with the body pushed back up to the starting position.
2.3. Statistical Analysis
Using IBM SPSS Statistics for Windows (version 23.0; SPSS Inc., Chicago, IL, USA), all data analyses were carried out. Both descriptive and inferential statistics were used to analyze the data. The median and interquartile range (quartile 1, quartile 3) were used to describe continuous variables such as weight, height, BMI, chest circumference, waist circumference, hip circumference, thigh circumference, sit-ups, and push-ups. The Shapiro-Wilk test was used to determine whether the data were normal. The medians between the groups were compared using the Mann-Whitney U test. The Friedman's test was used to examine changes in the means for each group from the baseline to the eighth and twelfth weeks. Additionally, the Wilcoxon test was used for pairwise comparisons to determine whether there were any notable differences between the baseline and the 8th and 12th weeks as well as between the 8th and 12th weeks within the group. Statistical significance was set at p < 0.05.
Figure 1.
Schematic representation of the experimental procedure.
3. Results
3.1. Demographic Characteristics of the Study Participants
As presented Table 2, no statistically significant differences in mean weight, height, BMI, chest circumference (cm), waist circumference (cm), thigh circumference (cm), and sit-ups (times/min) were observed at baseline between the control and the online RT intervention groups. At baseline, the mean push-up time (times/min) of the online RT intervention group was considerably greater than that of the control group (Table 2).
3.2. Effects on BW
In both the online RT intervention and control groups, BW revealed a statistically significant variation across time points (p < 0.001). BW showed a significant difference in the online RT intervention group, with a greater decrease at weeks 8 and 12 (p = 0.001 for both; compared to baseline values) and at week 12 (p < 0.001; compared to the value at week 8). In the control group, BW exhibited a significant difference, with a greater increase at week 12 (p = 0.005; compared to the baseline value) as illustrated in Table 3.
3.3. Effects on BMI
BMI indicated a statistically significant difference between time points in both the online RT intervention group (p < 0.001) and control group (p = 0.002). The BMI was significantly more decreased in the online RT intervention group at weeks 8 and 12 (p = 0.001 for both; compared to the values at baseline) and at week 12 (p < 0.001; compared to the value at week 8). In the control group, BMI showed a significant difference, with a greater increase at week 12 (p = 0.005; compared to the baseline value). At weeks 8 (p = 0.015) and 12 (p < 0.001), inter-group analysis revealed statistically significant differences between the online RT intervention and control groups. At weeks 8 and 12, the mean BMI of the online RT intervention group was lower than that of the control group (Table 4).
3.4. Effects on Chest Circumference
No significant difference in chest circumference was detected between time points in the online RT intervention and control groups (Table 5).
3.5. Effects on Waist Circumference
Waist circumference indicated a statistically significant variation across time points in the online RT intervention group (p < 0.001) and control group (p < 0.001). Waist circumference was significantly more decreased in the online RT intervention group at weeks 8 and 12 (p = 0.002 and p < 0.001, respectively; compared to baseline values) and at week 12 (p = 0.005; compared to the baseline value). Conversely, waist circumference was significantly more increased in the control group at week 12 (p = 0.017; compared to baseline values). At week 8 (p = 0.006) and week 12 (p < 0.001), inter-group analysis revealed statistically significant differences between the online RT intervention and control groups. At weeks 8 and 12, the mean waist circumference in the online RT intervention group was smaller than that in the control group (Table 6).
3.6. Effects on Hip Circumference
In the online RT intervention group, there was a statistically significant difference in hip circumference between time points (p < 0.001). Hip circumference showed a significant difference in the online RT intervention group, with a greater decrease at week 12 (p < 0.001; compared to the baseline value) and at week 12 (p = 0.002; compared to the value at week 8). In the control group, hip circumference did not change from baseline. At week 12, inter-group comparisons revealed statistically significant differences between the RT intervention and control groups (p = 0.044). At week 12, the mean hip circumference in the online RT intervention group was lower than that in the control group (Table 7).
3.7. Effects on Thigh Circumference
The difference in thigh circumference between time points was statistically significant in the online RT intervention group (p = 0.001) and control group (p = 0.013). The online RT intervention group showed a significant difference in thigh circumference, with a greater decrease at week 12 (p < 0.001; compared to the baseline value) and at week 12 (p < 0.001; compared to the value at week 8). In contrast, hip circumference in the control group did not change from baseline. When compared to the control group, inter-group analysis revealed statistically significant differences in weight training at week 8 (p = 0.035) and week 12 (p < 0.001). At weeks 8 and 12, the mean thigh circumference in the online RT intervention group was smaller than that in the control group (Table 8).
3.8. Effects on Sit-ups
In the online RT intervention group, sit-ups showed a statistically significant difference between time points (p = 0.001). Sit-ups indicated a significant difference in the online RT intervention group, with a greater increase at weeks 8 and 12 (p < 0.001 for both; compared to baseline values) and at week 12 (p = 0.001; compared to the value at week 8). Sit-ups in the control group were constant from baseline. At week 8 (p < 0.001) and week 12 (p < 0.001), inter-group analysis revealed statistically significant differences between the online RT intervention and control groups. At weeks 8 and 12, the online RT intervention group performed more sit-ups than the control group (Table 9).
3.9. Effects on Push-ups
Push-ups exhibited a statistically significant difference between time points in the online RT intervention group (p < 0.001) and control group (p = 0.003). Push-ups indicated a significant difference in the online RT intervention group, with a greater increase at weeks 8 and 12 (p < 0.001 for both; compared to baseline values) and at week 12 (p < 0.001; compared to the value at week 8). Push-ups in the control group showed a significant difference, with a greater increase at week 8 (p = 0.035; compared to the baseline value) and a decrease at week 12 (p = 0.020; compared to the value at week 8). At week 8 (p < 0.001) and week 12 (p < 0.001), inter-group analysis revealed statistically significant differences between the online RT intervention and control groups. At weeks 8 and 12, the mean number of push-ups in the online RT intervention group was higher than that in the control group (Table 10).
4. Discussion
The primary purpose of this study was to investigate the effects of online RT on MS and anthropometric parameters in overweight female students. The main finding from this study revealed that the participants had the significant health improvement in BW, BMI, waist, hip, and thigh circumference, sit-ups, and push-ups. On the contrary, there was no significant differences in chest circumference because the chest muscles are the main muscles, and the online RT did not focus on the pectoral muscles.
Since there was no significant different shown in chest circumference, this could be due to variances in muscle fiber distribution throughout the body. That is, the majority of muscle fibers in the upper body are fast-twitch, which is proportionally more than muscle fibers in the lower body. While most lower body muscles have slow-twitch muscle fibers, adaptation to training may differ depending on muscle fiber type [27,28]. Additionally, the muscles of the upper body, with the exception of the abdominal and lower back muscles, are continually strained by daily movement. These two muscles may be the only ones that can respond to training when compared to the entire upper body's muscles. Including those for chest muscles [29,30]. In order to gain chest circumference, specific exercises should be performed with intensity and volume of training as well as controlling the nutritional status [31,32].
Such results from the present study suggested that the online RT program could decrease the BW and BMI and that all parameters (excluding chest circumference) did not differ after RT. This is consistent with the findings of Riberio et al. [33] concluded that resistance was an effective treatment for improving MS and cardiovascular fitness in obese children. Additionally, RT interventions appeared to reduce body fat, BMI, and waist circumference. Most of these findings indicated that RT was essential for controlling body composition [34]. Moreover, RT contributes to the maintenance of muscle mass [35]. Similarly, Burrup et al. [36] found that resistance strength training was an effective method for improving body composition. Hence, an RT program could possibly represent the primary component of performance and health exercise programs because it potentially increases multiple sclerosis, potency, stamina and hypertrophy, all of which are beneficial for the improvement of motor performance.
Numerous studies have examined the impact of resistance training (RT) on various physiological parameters, including body mass index (BMI), lean mass, body fat percentage, metabolic syndrome (MS), and cardiorespiratory fitness, among a population of overweight students [37,38,39]. The results demonstrated that RT was a successful treatment for obese adolescents and were consistent with results from treatments in the adult population. In addition to improving MS, RT Interventions targeting obesity in adolescents were found to yield favorable outcomes, as evidenced by reductions in body fat, waist circumference, and body mass index (BMI). The aforementioned studies also documented beneficial changes in body composition following a resistance training (RT) program. These changes included a notable reduction in body fat and waist circumference, an increase in lean mass, and a drop in BMI. Additionally, it is noteworthy that MS also shown good benefits in response to the RT program.
According to certain research, RT may be crucial for enhancing athletic performance and physical fitness as well as for regulating body composition. In other words, RT improves maintain or enhance muscle mass [40]. However, the effects of age, diet, menopausal status, and physical activity on the relationship between strength training and body composition remain unclear. The study also found that the more days, time, and effort devoted to strength training, the more body fat and higher fat-free mass tended to be visible. A significant portion of the differences in body composition seemed to result from people who participate in more physical activity than those who do not. Additionally, some studies suggested that RT may lead to beneficial improvements in cardiorespiratory endurance in children [40,41]. Some studies showed an increase in cardiorespiratory fitness was linked to the previously overweight nature of children [39,41]. Therefore, it can be implied that for sedentary overweight children, RT could be taken for fat loss. More specifically, the RT was used for further muscle gain and maintenance of muscle mass to improve body composition, BW, BMI, chest, waist, hip, and thigh circumference, and MS using sit-up and push-up measurements. More importantly, some findings reveal that it may be essential to improve the quality of life.
Based on the findings of present study, individuals staying at home can utilize an online RT program to improve their physical performance while increasing their strength and losing weight. It is important to increase the physical activity or exercise levels. Additionally, the current study revealed the strength in that it showed the benefits of a home-based resistance exercise regimen in improving health. Nevertheless, the participants were required to check their target heart rate (THR) during exercise because the exercise intensity was regulated in this study.
This study found some limitations. All participants underwent the online RT program on anthropometric assessments. As this was an online study and all participants received measurement training as part of the program introduction, the researchers were unable to confirm the use of the same measuring techniques. However, the camera not only was turned on to view and track the training but was also under the control of a research assistant.
5. Conclusions
This study aims to investigate the effects of online RT program included 12 weeks on MS and anthropometric parameters in overweight female adolescents. The results suggested that the online RT program appeared to be effective in improving the MS and anthropometric parameters and could serve as an efficient strategy for reducing body fat, waist, hip, and thigh circumference, and BMI in overweight female adolescents in the south of Thailand. However, this study did not reveal the significant differences in chest circumference. Therefore, this may provide important information for the development of useful tools and for designing online RT programs to improve chest circumference. More importantly an online RT program is a suitable method for improving the body composition, given that training at least three times per week for 12 weeks can increase or considerably improve the MS and anthropometric measurements in overweight participants. It could be an excellent way to exercise while staying at home, as no special equipment is necessary to practice alone at home owing to its simplicity. Consequently, an online RT program has the potential to improve health, to aid overweight individuals in losing weight, and to increase muscle strength as well as elevating the quality of life.
Author Contributions
Conceptualization, N.M.P.; methodology, N.M.P.; software, N.M.P. and N.U.; validation, N.M.P. and N.U.; formal analysis, N.M.P., and N.U; investigation, N.M.P., N.U., and K.R.; resources, N.M.P.; data curation, N.M.P. and N.U.; writing—original draft preparation, N.M.P., N.U., P.W., T.R., K.R., and M.T.; writing—review and editing, N.M.P., N.U., P.W., T.R., K.R., and M.T.; visualization, N.M.P., N.U., and K.R.; supervision, N.M.P.; project administration, N.M.P.; funding acquisition, N.M.P. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Walailak University, Thailand (grant number: WU-IRG-64-035).
Institutional Review Board Statement
The study was conducted in accordance with the 1975 Declaration of Helsinki (as revised in 2013) and was approved by the Ethics Committee on Human Research at Walailak University, Nakhon Si Thammarat, Thailand (approval no.: WUCE-21-076-01; date of approval: May 14, 2021).
Informed Consent Statement
Informed and written consent was obtained from all participants involved in the study.
Acknowledgments
The authors are grateful for all financial support and research facilities provided by Walailak University.
Conflicts of Interest
The authors declare that they have no conflicts of interest. The funders did not contribute to the study's design, data collection, analysis, interpretation, or article writing.
References
- Organization, W.H. Global strategy on diet, physical activity and health. Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 10 July).
- World Health Organization. Overweight and Obesity. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 17 July).
- Global Nutrition Report. 2018 Global Nutrition Report. Available online: https://globalnutritionreport.org/documents/355/2018_Global_Nutrition_Report_-_London.pdf (accessed on 17 July).
- Trübswasser, U.; Verstraeten, R.; Salm, L.; Holdsworth, M.; Baye, K.; Booth, A.; Feskens, E.J.; Gillespie, S.; Talsma, E.F. Factors influencing obesogenic behaviours of adolescent girls and women in low-and middle-income countries: A qualitative evidence synthesis. Obes. Rev. 2021, 22, e13163. [Google Scholar] [CrossRef] [PubMed]
- WHO, G. Global status report on noncommunicable diseases 2010. 2011.
- Rtveladze, K.; Marsh, T.; Webber, L.; Kilpi, F.; Levy, D.; Conde, W.; McPherson, K.; Brown, M. Health and economic burden of obesity in Brazil. PloS One 2013, 8, e68785. [Google Scholar] [CrossRef] [PubMed]
- Ninyaporn, J.; Anukool, M. Effecttiveness of applying the concept of health belife model in modifyling obesity reduction behavior of Sukhothai personel, muang district, Sukhothai province. Acad. J. Comminuty Public Health 2023, 9. [Google Scholar]
- Oppert, J.m.; Bellicha, A.; van Baak, M.A.; Battista, F.; Beaulieu, K.; Blundell, J.E.; Carraça, E.V.; Encantado, J.; Ermolao, A.; Pramono, A. Exercise training in the management of overweight and obesity in adults: Synthesis of the evidence and recommendations from the European Association for the Study of Obesity Physical Activity Working Group. Obes. Rev. 2021, 22, e13273. [Google Scholar] [CrossRef]
- Ojo, O.R.; Babalola, J.F. Effect of variable resistance training on anthropometric parameters of in-school early adolescents in Ondo Municipality. West Afr. J. Phys. Health Educ. 2018, 22, 91–103. [Google Scholar]
- ARDIC, F. Anthropometry and exercise in obesity. In Handbook of Anthropometry: Physical Measures of Human Form in Health and Disease; Springer: 2012; pp. 1919–1935.
- Saghebjoo, M.; Nezamdoost, Z.; Ahmadabadi, F.; Saffari, I.; Hamidi, A. The effect of 12 weeks of aerobic training on serum levels high sensitivity C-reactive protein, tumor necrosis factor-alpha, lipid profile and anthropometric characteristics in middle-age women patients with type 2 diabetes. Diabetes Metab. Syndr. : Clin. Res. Rev. 2018, 12, 163–168. [Google Scholar] [CrossRef]
- Campa, F.; Maietta Latessa, P.; Greco, G.; Mauro, M.; Mazzuca, P.; Spiga, F.; Toselli, S. Effects of different resistance training frequencies on body composition, cardiometabolic risk factors, and handgrip strength in overweight and obese women: A randomized controlled trial. J. Funct. Morphol. Kinesiol. 2020, 5, 51. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Kojima, K.; Kearns, C.; Yohena, H.; Fukuda, J. Whole body muscle hypertrophy from resistance training: distribution and total mass. Br. J. Sport. Med. 2003, 37, 543–545. [Google Scholar] [CrossRef]
- Westcott, W.L. Resistance training is medicine: effects of strength training on health. Curr. Sport. Med. Rep. 2012, 11, 209–216. [Google Scholar] [CrossRef]
- Bharti, N.; Hrubeniuk, T.; Mayo, A.; Senechal, M.; Bouchard, D.R. Resistance training contribute to the aerobic components of an exercise session in adults but not as much in older adults. Int. J. Exerc. Sci. 2017, 10, 406. [Google Scholar]
- Dean, R.N.; Farrell, J.M.; Kelley, M.L.; Taylor, M.J.; Rhodes, R.E. Testing the efficacy of the theory of planned behavior to explain strength training in older adults. J Aging Phys Act 2007, 15, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Winett, R.A.; Carpinelli, R.N. Potential health-related benefits of resistance training. Prev. Med. 2001, 33, 503–513. [Google Scholar] [CrossRef]
- Baillet, A.; Vaillant, M.; Guinot, M.; Juvin, R.; Gaudin, P. Efficacy of resistance exercises in rheumatoid arthritis: meta-analysis of randomized controlled trials. Rheumatology 2011, 51, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Morsley, K.; Berntzen, B.; Erwood, L.; Bellerby, T.; Williamson, L. Progressive resistance training (PRT) improves rheumatoid arthritis outcomes: A district general hospital (DGH) model. Musculoskelet. Care 2018, 16, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Sul, B.; Lee, K.B.; Joo, Y.B.; Hong, B.Y.; Kim, J.S.; Kim, K.J.; Park, K.S.; Park, Y.J.; Lim, S.H. Twelve Weeks of Strengthening Exercise for Patients with Rheumatoid Arthritis: A Prospective Intervention Study. J Clin Med 2020, 9. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sport. Exerc 2009, 41, 459–471. [Google Scholar] [CrossRef]
- Creswell, J.W.; Creswell, J.D. Research design: Qualitative, quantitative, and mixed methods approaches; Sage publications: 2017.
- Na Nongkhai, M.P.; Huntula, S.; Kumar, R.; Narkkul, U. Effects of an online yoga program on anthropometric parameters among overweight female students during the COVID-19 pandemic. Heliyon 2022, 8, e10661. [Google Scholar] [CrossRef]
- Ngamjarus, C. n4Studies: sample size calculation for an epidemiological study on a smart device. Siriraj Med. J. 2016, 68, 160–170. [Google Scholar]
- Tunmer, W.E.; Nesdale, A.R.; Wright, A.D. Syntactic awareness and reading acquisition. Br. J. Dev. Psychol. 1987, 5, 25–34. [Google Scholar] [CrossRef]
- Branco, B.H.M.; Valladares, D.; De Oliveira, F.M.; Carvalho, I.Z.; Marques, D.C.; Coelho, A.A.; De Oliveira, L.P.; Bertolini, S.M.M.G. Effects of the order of physical exercises on body composition, physical fitness, and cardiometabolic risk in adolescents participating in an interdisciplinary program focusing on the treatment of obesity. Front. Physiol. 2019, 10, 1013. [Google Scholar] [CrossRef]
- Sanchis-Moysi, J.; Idoate, F.; Olmedillas, H.; Guadalupe-Grau, A.; Alayon, S.; Carreras, A.; Dorado, C.; Calbet, J. The upper extremity of the professional tennis player: muscle volumes, fiber-type distribution and muscle strength. Scand. J. Med. Sci. Sport. 2010, 20, 524–534. [Google Scholar] [CrossRef]
- Bottinelli, R.; Reggiani, C. Human skeletal muscle fibres: molecular and functional diversity. Prog. Biophys. Mol. Biol. 2000, 73, 195–262. [Google Scholar] [CrossRef] [PubMed]
- Snow-Harter, C.; Bouxsein, M.L.; Lewis, B.T.; Carter, D.R.; Marcus, R. Effects of resistance and endurance exercise on bone mineral status of young women: a randomized exercise intervention trial. J. Bone Miner. Res. 1992, 7, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, W.D.; Simão, R.; Polito, M.D.; Santana, C.A.; Chaves, R.B.; Bezerra, E.; Fleck, S.J. Influence of strength training on adult women's flexibility. J. Strength Cond. Res. 2008, 22, 672–677. [Google Scholar] [CrossRef] [PubMed]
- Orange, S.T.; Madden, L.A.; Vince, R.V. Resistance training leads to large improvements in strength and moderate improvements in physical function in adults who are overweight or obese: a systematic review. J. Physiother. 2020, 66, 214–224. [Google Scholar] [CrossRef]
- Shaw, B.S.; Brown, G.A.; Shaw, I. Importance of resistance training in the management of cardiovascular disease risk. In Risk Factors for Cardiovascular Disease; IntechOpen: 2021.
- Ribeiro, B.; Forte, P.; Vinhas, R.; Marinho, D.A.; Faíl, L.B.; Pereira, A.; Vieira, F.; Neiva, H.P. The Benefits of Resistance Training in Obese Adolescents: A Systematic Review and Meta-analysis. Sport. Med Open 2022, 8, 109. [Google Scholar] [CrossRef]
- Peitz, M.; Behringer, M.; Granacher, U. A systematic review on the effects of resistance and plyometric training on physical fitness in youth- What do comparative studies tell us? PLoS One 2018, 13, e0205525. [Google Scholar] [CrossRef]
- Foureaux, G.; Pinto, K.M.d.C.; Dâmaso, A. Effects of excess post-exercise oxygen consumption and resting metabolic rate in energetic cost. Rev. Bras. De Med. Do Esporte 2006, 12, 393–398. [Google Scholar] [CrossRef]
- Burrup, R. Strength training and body composition in middle-age women; Brigham Young University: 2015.
- Wewege, M.A.; Desai, I.; Honey, C.; Coorie, B.; Jones, M.D.; Clifford, B.K.; Leake, H.B.; Hagstrom, A.D. The effect of resistance training in healthy adults on body fat percentage, fat mass and visceral fat: a systematic review and meta-analysis. Sport. Med. 2022, 52, 287–300. [Google Scholar] [CrossRef]
- Lopez, P.; Taaffe, D.R.; Galvão, D.A.; Newton, R.U.; Nonemacher, E.R.; Wendt, V.M.; Bassanesi, R.N.; Turella, D.J.; Rech, A. Resistance training effectiveness on body composition and body weight outcomes in individuals with overweight and obesity across the lifespan: A systematic review and meta-analysis. Obes. Rev. 2022, 23, e13428. [Google Scholar] [CrossRef]
- Ribeiro, B.; Forte, P.; Vinhas, R.; Marinho, D.A.; Faíl, L.B.; Pereira, A.; Vieira, F.; Neiva, H.P. The Benefits of Resistance Training in Obese Adolescents: A Systematic Review and Meta-analysis. Sport. Med. -Open 2022, 8, 109. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.C.; Torode, M.; Fiatarone Singh, M. Effects of resistance training on metabolic fitness in children and adolescents: a systematic review. Obes. Rev. 2008, 9, 43–66. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Song, Y.W.; Kim, H.S.; Lee, S.Y.; Jeong, H.S.; Suh, S.-H.; Park, J.K.; Jung, J.W.; Kim, N.S.; Noh, C.I. The effects of an exercise program on anthropometric, metabolic, and cardiovascular parameters in obese children. Korean Circ. J. 2010, 40, 179–184. [Google Scholar] [CrossRef] [PubMed]
Table 2.
Demographic characteristics of the participants at baseline.
| Characteristics | Groups | p-value* | |
|---|---|---|---|
| RT intervention (n = 30) |
Control (n = 30) |
||
| Weight (kg) | 56.5 (55,65) | 56 (54,60) | 0.199 |
| Height (cm) | 158 (155,161) | 156 (153,161) | 0.207 |
| BMI (kg/m2) | 22.88 (22.43,23.88) | 22.88 (22.6,23.15) | 0.813 |
| Chest circumference (cm) | 34 (33,36) | 34 (34,36) | 0.690 |
| Waist circumference (cm) | 29 (27,32) | 30 (28,32) | 0.568 |
| Hip circumference (cm) | 36.25 (34,39) | 36 (34,38) | 0.703 |
| Thigh circumference (cm) | 20 (19,21.5) | 21 (19.5,22) | 0.248 |
| Sit-up (times/min) | 17 (15,21) | 16.5 (13,20) | 0.150 |
| Push-up (times/min) | 11 (8,13) | 8 (7,10) | 0.007 |
Data are presented as median (quartile 1, quartile 3). *p < 0.05, significantly different when compared with the control group.
Table 3.
Body weight of the RT intervention and control groups.
| Characteristics | Groups | p-value* | |
|---|---|---|---|
| RT intervention (n = 30) |
Control (n = 30) |
||
| Week 0 | 56.5 (55,65) | 56 (54,60) | 0.199 |
| Week 8 | 55 (53,63)† | 56 (55,60) | 0.795 |
| Week 12 | 54.5 (52,61)††, ††† | 57 (55,61)†† | 0.061 |
| p-value** | <0.001 | 0.002 | |
Data are presented as median (quartile 1, quartile 3). Statistical analysis: *Mann–Whitney U test, **Friedman’s test. †Significant difference between weeks 0 and 8 within the group (p < 0.05). ††Significant difference between weeks 0 and 12 within the group (p < 0.05). †††Significant difference between weeks 8 and 12 within the group (p < 0.05).
Table 4.
BMI of the online RT intervention and control groups.
| Characteristics | Groups | p-value* | |
|---|---|---|---|
| RT intervention (n = 30) |
Control (n = 30) |
||
| Week 0 | 22.88 (22.43,23.88) | 22.88 (22.6,23.15) | 0.813 |
| Week 8 | 22.4 (21.63,23.59)† | 23.24 (22.72,23.44) | 0.015 |
| Week 12 | 21.64 (21.22,22.76)††, ††† | 23.47 (22.89,23.81)†† | <0.001 |
| p-value** | <0.001 | 0.002 | |
Data are presented as median (quartile 1, quartile 3). Statistical analysis: *Mann-Whitney U test, **Friedman’s test. †Significant difference between weeks 0 and 8 within the group (p < 0.05). ††Significant difference between weeks 0 and 12 within the group (p < 0.05). †††Significant difference between weeks 8 and 12 within the group (p < 0.05).
Table 5.
Chest circumference of the online RT intervention and control groups.
| Characteristics | Groups | p-value* | |
|---|---|---|---|
| RT intervention (n = 30) |
Control (n = 30) |
||
| Week 0 | 34 (33,36) | 34 (34,36) | 0.690 |
| Week 8 | 34 (33,36) | 34 (34,36) | 0.654 |
| Week 12 | 34 (33,36) | 34 (34,36) | 0.600 |
| p-value** | 0.358 | 1.000 | |
Data are presented as median (quartile 1, quartile 3). Statistical analysis: *Mann-Whitney U test, **Friedman’s test. †Significant difference between weeks 0 and 8 within the group (p < 0.05). ††Significant difference between weeks 0 and 12 within the group (p < 0.05). †††Significant difference between weeks 8 and 12 within the group (p < 0.05).
Table 6.
Waist circumference of the online RT intervention and control groups.
| Characteristics | Groups | p-value* | |
|---|---|---|---|
| RT intervention (n = 30) |
Control (n = 30) |
||
| Week 0 | 29 (27,32) | 30 (28,32) | 0.568 |
| Week 8 | 28 (26,30)† | 30.5 (28,32) | 0.006 |
| Week 12 | 26.5 (25,28)††, ††† | 30.5 (28,33)†† | <0.001 |
| p-value** | <0.001 | <0.001 | |
Data are presented as median (quartile 1, quartile 3). Statistical analysis: *Mann-Whitney U test, **Friedman’s test. †Significant difference between weeks 0 and 8 within the group (p < 0.05). ††Significant difference between weeks 0 and 12 within the group (p < 0.05). †††Significant difference between weeks 8 and 12 within the group (p < 0.05).
Table 7.
Hip circumference of the online RT intervention and control groups.
| Characteristics | Groups | p-value* | |
|---|---|---|---|
| RT intervention (n = 30) |
Control (n = 30) |
||
| Week 0 | 36.25 (34,39) | 36 (34,38) | 0.703 |
| Week 8 | 35.75 (33.5,38) | 36 (34,38) | 0.777 |
| Week 12 | 34.5 (33,36)††, ††† | 36 (34,38) | 0.044 |
| p-value** | <0.001 | 0.368 | |
Data are presented as median (quartile 1, quartile 3). Statistical analysis: *Mann-Whitney U test, **Friedman’s test. †Significant difference between weeks 0 and 8 within the group (p < 0.05). ††Significant difference between weeks 0 and 12 within the group (p < 0.05). †††Significant difference between weeks 8 and 12 within the group (p < 0.05).
Table 8.
Thigh circumference of the online RT intervention and control groups.
| Characteristics | Groups | p-value* | |
|---|---|---|---|
| RT intervention (n = 30) |
Control (n = 30) |
||
| Week 0 | 20 (19,21.5) | 21 (19.5,22) | 0.248 |
| Week 8 | 20 (18.5,21) | 21 (20,22) | 0.035 |
| Week 12 | 18 (17,20)††, ††† | 21 (20,22) | <0.001 |
| p-value** | <0.001 | 0.013 | |
Data are presented as median (quartile 1, quartile 3). Statistical analysis: * Mann-Whitney U test, **Friedman’s test. †Significant difference between weeks 0 and 8 within the group (p < 0.05). ††Significant difference between weeks 0 and 12 within the group (p < 0.05). †††Significant difference between weeks 8 and 12 within the group (p < 0.05).
Table 9.
Sit-ups in the online RT intervention and control groups.
| Characteristics | Groups | p-value* | |
|---|---|---|---|
| RT intervention (n = 30) |
Control (n = 30) |
||
| Week 0 | 17 (15,21) | 16.5 (13,20) | 0.150 |
| Week 8 | 23.5 (18,26)† | 16 (13,21) | <0.001 |
| Week 12 | 27 (22,33)††, ††† | 15.5 (14,21) | <0.001 |
| p-value** | <0.001 | 0.314 | |
Data are presented as median (quartile 1, quartile 3). Statistical analysis: *Mann-Whitney U test, **Friedman’s test. †Significant difference between weeks 0 and 8 within the group (p < 0.05). ††Significant difference between weeks 0 and 12 within the group (p < 0.05). †††Significant difference between weeks 8 and 12 within the group (p < 0.05).
Table 10.
Push-up of the online RT intervention and control groups.
| Characteristics | Groups | p-value* | |
|---|---|---|---|
| RT intervention (n = 30) |
Control (n = 30) |
||
| Week 0 | 11 (8,13) | 8 (7,10) | 0.007 |
| Week 8 | 15.5 (12,18)† | 8.5 (7,11)† | <0.001 |
| Week 12 | 20 (18,23)††, ††† | 8 (7,10)††† | <0.001 |
| p-value** | <0.001 | 0.003 | |
Data are presented as median (quartile 1, quartile 3). Statistical analysis: *Mann-Whitney U test, **Friedman’s test. †Significant difference between weeks 0 and 8 within the group (p < 0.05). ††Significant difference between weeks 0 and 12 within the group (p < 0.05). †††Significant difference between weeks 8 and 12 within the group (p < 0.05).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



