Submitted:
13 September 2023
Posted:
14 September 2023
You are already at the latest version
Abstract
To the best of the author’s knowledge, studies of mature plasmacytoid dendritic cell proliferation associated with T lymphoblastic lymphoma were extremely rare in the literature. Here, we report a patient who underwent both mature plasmacytoid dendritic cell proliferation and T lymphoblastic lymphoma. With the findings of lymph node biopsy taken from the right cervical and inguinal regions, we identified eye-catching mature plasmacytoid dendritic cells that were considered to be responsible for this lesion at the beginning, until the immunostaining of Ki67 and TDT showed a small group of positive cells hiding in these plasmacytoid dendritic cells. Bone marrow biopsy was also performed in this patient. Microscopically, the hematopoietic tissue was almost completely replaced by lymphoblastoid cells with condensed chromatin, inconspicuous nucleoli and scanty cytoplasm, which were basically the same as those seen in the lymph nodes in morphology. However, there was no sign of plasmacytoid dendritic cells or Langerhans cells in the bone marrow biopsy. With the help of bone marrow biopsy, our final diagnosis of the lymph node was T lymphoblastic lymphoma coexisting with mature plasmacytoid dendritic cell proliferation . Although accumulations of plasmacytoid dendritic cells may occur in some infections or reactive lymphadenopathy, the presence of extensive nodules or infiltration of plasmacytoid dendritic cells strongly reminds the pathologist to carefully evaluate the bone marrow or peripheral blood status of the patient to exclude a hidden myeloid or other neoplasm.
Keywords:
mature plasmacytoid dendritic cell proliferation
; T lymphoblastic lymphoma
; myeloid neoplasms
; case report
1. Introduction
Plasmacytoid dendritic cells (PDCs), first described by Lennert and Remmele in reactive lymphoid hyperplasia in 1958[1], were initially called ‘plasmacytoid T cells’, ‘T-associated plasma cells’ or ‘plasmacytoid monocytes’. They represent a specialized branch of the dendritic cell (DC) family with ‘plasmacytoid’ morphology, a large capacity for producing type I interferon, and the ability to differentiate into antigen-presenting dendritic cells in particular conditions, which was confirmed by the Liu and Colonna groups until the late 1990s[2,3]. Increased PDCs have been observed in a wide range of inflammatory conditions, including infection, hyaline-vascular Castleman disease and Kikuchi-Fujimoto lymphadenopathy, and sometimes involved in a variety of malignancies and autoimmune diseases [4].
Attributing to the differences in clinical course and pathological features, neoplasms derived from PDCs have been divided into two distinct forms: mature PDC proliferations associated with myeloid neoplasms (MPDMN) and blastic plasmacytoid dendritic cell neoplasm (BPDCN). Patients with mature PDC proliferation often suffer from chronic myelomonocytic leukemia, but acute myeloid leukemia or other myeloproliferative disorders may also be reported [5]. To the best of the author’s knowledge, cases of mature PDC proliferation associated with T lymphoblastic lymphoma have been seldomly reported in the literature. Here, we report a patient who underwent both mature PDC proliferation and T lymphoblastic lymphoma.
2. Case presentation
A 65-year-old woman suffered from cough, lymphadenopathy and intermittent high fever for 8 months. The patient was admitted to our hospital after ineffective treatment with anti-inflammatory and anti-tuberculosis therapy at an external medical facility. Her peripheral blood analysis showed leukocytopenia (2.68*109/L), erythrocyte (2.84*1012/L), normochromic anemia (hemoglobin 91 g ⁄ L; mean corpuscular volume 95.1 fl), and a normal platelet count (215*109 ⁄ L). Differential counts of white blood cells revealed a relatively high percentage of lymphocytes (72.7%) and a low percentage of neutrophils (21.29%). Meanwhile, her physical examinations showed enlarged lymph nodes over the clavicular, cervical, axillary and inguinal regions, without hepatomegaly or splenomegaly. The PET-CT imaging results show Multiple enlarged lymph nodes and increased metabolism in bilateral neck, armpits, retroperitoneum, mesenteric roots, abdominal cavity, bilateral iliac vessels, and bilateral inguinal regions. A bone marrow aspiration examination demonstrated that bone marrow was invaded by the tumor cells. After diagnosis, the patient received chemotherapy of Cyclophosphamide+ Doxorubicin hydrochloride + Vindesine +Dexamethasone, after 2 cycles of treatment, the patient developed myelosuppression accompanied by lung infection, and then she was unable to tolerate the side effects of chemotherapy and chose to be discharged, unfortunately, she was lost to follow-up after that.
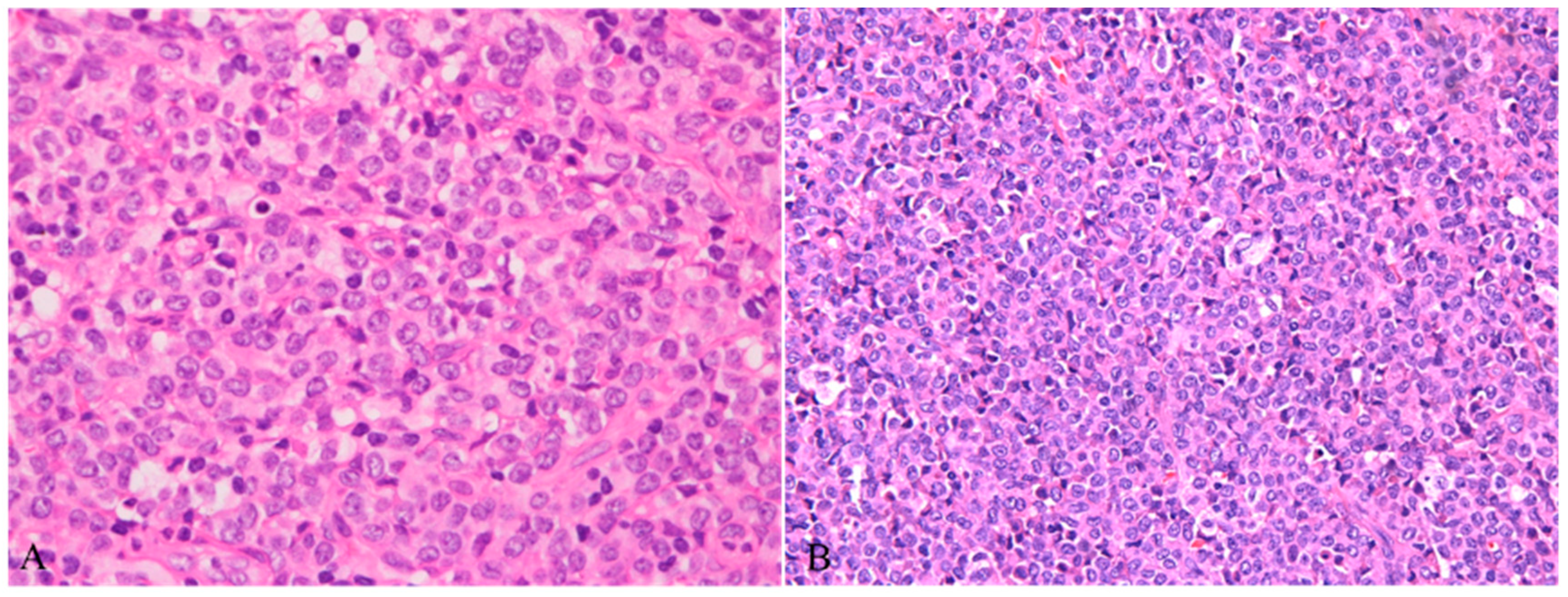
Lymph node biopsy samples were taken from the right cervical and inguinal regions of this patient. All tissues were fixed in 10% buffered formalin, and then the paraffin-embedded sections were stained with hematoxylin and eosin. Histological examination showed that the normal structure of the lymph nodes was effaced, and the inguinal lymph node was almost entirely replaced by sheets of small- to medium-sized cells with amphophilic cytoplasm, round to ovoid nuclei, finely dispersed chromatin and inconspicuous or small nucleoli(Figure 1A,2). Immunohistochemistry indicated that these cells expressed CD123, CD68, CD4, TCF4, CD43, CD31 and LCA but were negative for CD3, CD8, CD20, CD56, CD34, TCL1,S100, CD1a, Langerin, CD61, CD15, CD163, CD117, MPO, ALK and TDT. The proliferation rate of these cells was very low, and only 5% of cells showed nuclear staining for Ki-67. According to the morphology and immunophenotype, these cells were believed to be mature plasmacytoid dendritic cells (PDCs).
Figure 1.
A: Normal structure of lymph nodes was effaced by sheets of tumor cells with amphophilic cytoplasm (HE ×40). B: Clusters of PDCs mixed with some cells characterized by abundant and pale cytoplasm, forming a ‘dark-light’ pattern (HE ×100).
Figure 1.
A: Normal structure of lymph nodes was effaced by sheets of tumor cells with amphophilic cytoplasm (HE ×40). B: Clusters of PDCs mixed with some cells characterized by abundant and pale cytoplasm, forming a ‘dark-light’ pattern (HE ×100).
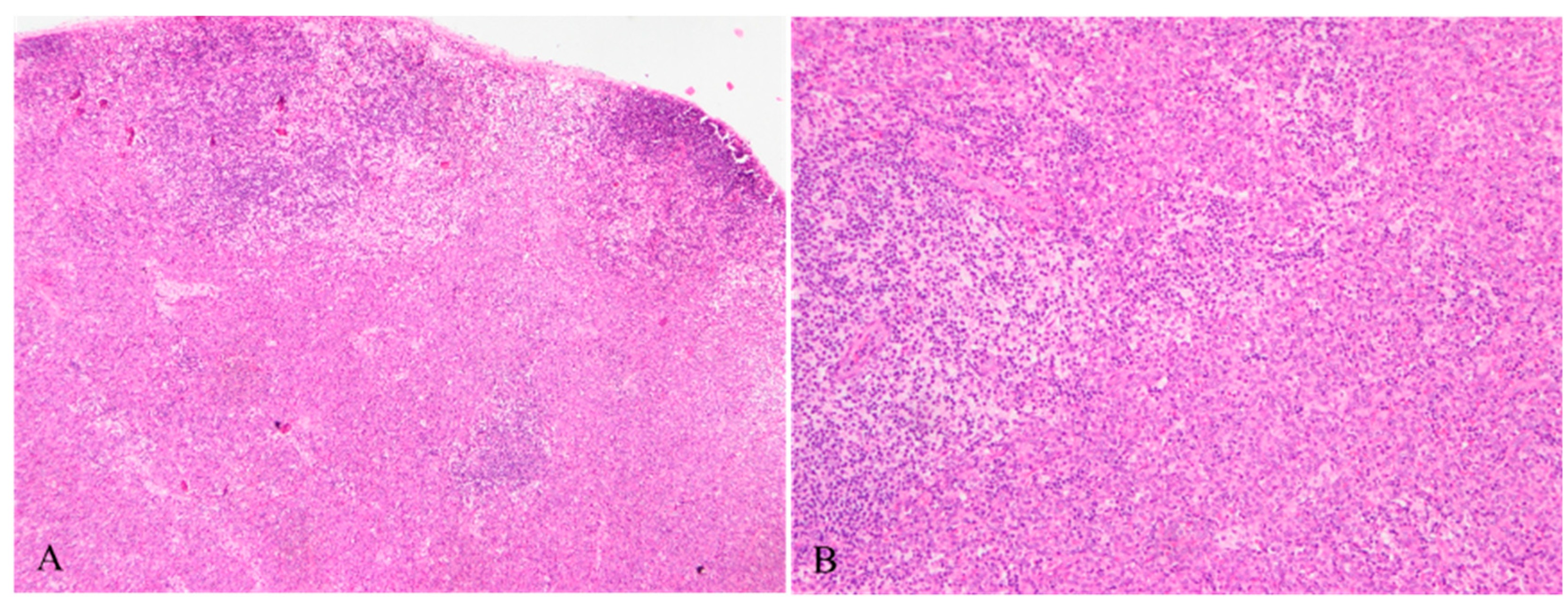
Figure 2.
Mature plasmacytoid dendritic cells with amphophilic cytoplasm, round to ovoid nuclei, finely dispersed chromatin and inconspicuous or small nucleoli (HE ×400).
Figure 2.
Mature plasmacytoid dendritic cells with amphophilic cytoplasm, round to ovoid nuclei, finely dispersed chromatin and inconspicuous or small nucleoli (HE ×400).
These eye-catching mature plasmacytoid dendritic cells were considered to be responsible for this lesion at the beginning, until the immunostaining of Ki67 and TDT showed a small group of positive cells hiding in these PDCs. Mostly, they were scattered in the paracortex of the lymph nodes, and a few of them formed small clusters. Morphologically, these cells resembled lymphoblasts, characterized by condensed chromatin, inconspicuous nucleoli and scanty cytoplasm(Figure 3A). Immunostaining confirmed that these were T lymphoblasts positive for CD3, CD5, CD7, CD34, LCA, and CD31 and negative for CD4, CD8, CD2, MPO, and CD117(Figure 3B). The proliferation rate was very high. However, it was difficult to differentiate reactive lymphoblast proliferation from bona fide lymphoblastic lymphoma in this situation due to the scarcity of these lymphoblasts.
In a few areas of the lymph node, clusters of PDCs mixed with some cells that had abundant, pale cytoplasm, forming a ‘dark-light’ pattern(Figure 1B). The pale cells had distinctively complex folded and grooved nuclei, inconspicuous nucleoli, and finely dispersed chromatin. Binucleated or multinucleated cells may also be found occasionally. The expression of S100, langerin and CD1a revealed that these cells were proliferative Langerhans cells.
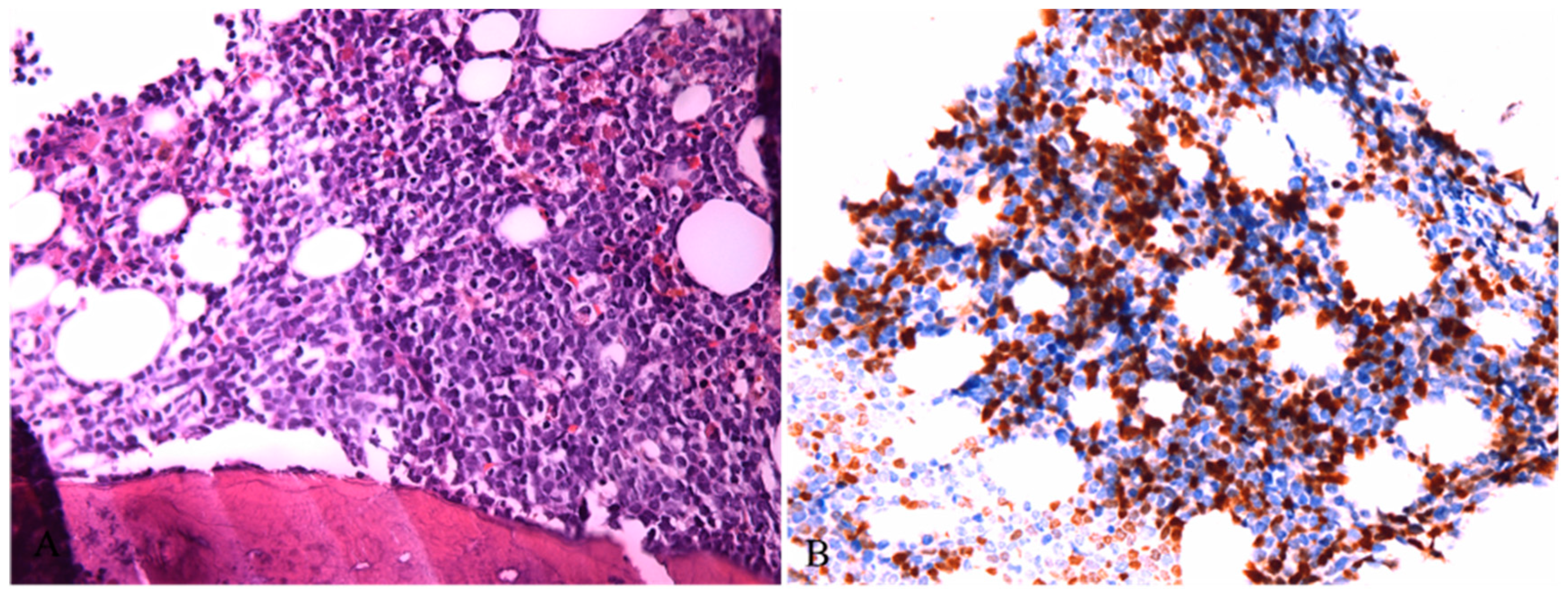
The pathological features of cervical lymph nodes were milder than those of inguinal lymph nodes, but the growth pattern and cell composition were quite the same. In conclusion, these lesions are mainly composed of mature PDCs, along with a relatively small amount of Langerhans cells and T lymphoblasts. Bone marrow biopsy was also performed in this patient. Microscopically, the hematopoietic tissue was almost completely replaced by lymphoblastoid cells with condensed chromatin, inconspicuous nucleoli and scanty cytoplasm, which were basically the same as those seen in the lymph nodes in morphology(Figure 4A). However, there was no sign of PDCs or Langerhans cells in the bone marrow biopsy. These lymphoblastoid cells expressed TDT, CD3, CD5, CD7, CD34, and LMO2 but were negative for CD20, CD4, CD117, MPO, CD68, CD123, S100, CD235, and CD61(Figure 4B). The proliferation rate reached approximately 80%.Flow cytometry showed 85.06% abnormal T lymphoblasts, which had the same immunophenotype of bone marrow biopsy and no sign of PDCs. Next-generation sequencing (NGS) of the PDCs revealed a few mutations: DNMT3A p.Cys549Phe (32.18% VAF), DNMT3A p.Glu774Ala (28.20% VAF), NF1 p.Arg1534Ter (1.61% VAF) and ERCC1 p.Phe321Ser (1.35% VAF). While the NGS results of the T lymphoblasts was quite different from PDCs, which demonstrating mutations as follows: CSF3R p.Q730X(47.56%,VAF), NOTCH1 p.L1574Q (31.85%,VAF) and NOTCH1 p.I1718T(4.01%,VAF). Collectively, the diagnosis of bone marrow biopsy was T lymphoblastic lymphoma/lymphoblastic leukemia. With the help of bone marrow biopsy, our final diagnosis of the lymph node was T lymphoblastic lymphoma coexisting with mature PDC proliferation.
3. Discussion and Conclusions
The origin and characteristics of PDCs have perplexed scientists for decades since they were first described by Lennert and Remmele in 1958. The physiologic, immunologic roles and pathologic states of PDCs have been well studied during the past two decades. They are characterized by a ‘plasmacytoid’ morphology resembling plasma cells, the production of high levels of type I interferons (IFN-I) and the ability to differentiate into antigen-presenting dendritic cells in particular situations[6]. PDCs originate in the bone marrow, where they comprise 0.1%–0.5% of nucleated cells and then circulate in the peripheral blood as mature cells, which means they remain in a nonproliferative state and survive for only several days[7]. PDCs normally reside in small amounts in lymphoid organs, such as lymph nodes and tonsils, and are seldomly found in bone marrow, spleen, thymic medulla, or mucosa-associated lymphoid tissue[8].
Morphologically, PDCs are medium-sized cells with round to ovoid, sometimes slightly elongated nuclei, fine chromatin and moderately abundant cytoplasm that is eosinophilic with hematoxylin/eosin staining and basophilic with Giemsa staining. They are usually situated in the paracortex in lymph nodes, around high endothelial venules as clusters or dispersed cells, while the clusters are scarcely seen in other lymph tissues or bone marrow[9]. PDCs are more readily identified by immunostaining, which are distinguishable by the expression of CD123, CD4, CD68, TCL1 and CD303 (BDCA2). CD2, CD5, CD7 or CD56 may be seen in small proportions of PDCs, usually with only focal and weak reactivity.
In many kinds of inflammatory conditions, such as tumors, autoimmunity, and infections, PDCs may home to the diseased tissue, usually lymph nodes and skin. In lymph nodes, the increase in PDCs is most commonly seen in three special forms of reactive lymphadenopathy: Kikuchi-Fujimoto lymphadenopathy (histiocytic necrotizing lymphadenitis, Castleman disease (hyaline-vascular subtype) and Kimura disease. In addition, PDCs may infiltrate a variety of malignancies, such as melanoma, squamous cell carcinoma, basal cell carcinoma, and breast carcinoma. Many studies have suggested that PDCs may enhance an antitumor immune response by using TLR7 and TLR9 agonists[10,11,12].
Owing to the large differences both in clinical course and pathology, neoplasms derived from PDCs have been divided into two distinct forms: mature PDC proliferations associated with myeloid neoplasms (MPDMN) and blastic plasmacytoid dendritic cell neoplasms (BPDCN), a newly recognized highly aggressive neoplasms, which most likely arise from PDC precursor cells that characteristically express CD123, CD4 and CD56. The former comprises large numbers of mature PDCs with a very low proliferation rate (Ki67<10%) and is invariably associated with myeloid neoplasms[5]. In most cases, mature PDCs express CD123, CD4, CD68, TCL1, and CD303 and usually form compact, well-defined nodules in the lymph nodes, bone marrow, spleen or skin, but diffuse infiltration may also be seen in a few cases. The MPDMN was first described as “plasmacytoid T-cell lymphoma” in 1983[13]. To date, fewer than 100 cases have been reported as single case or small case series. Most of these cases occurred in the bone marrow, followed by the skin, lymph nodes and, more rarely, spleen. Focusing on lymph node lesions, 19 reported cases were found until May 2020 by a literature search[14,15,16,17,18,19,20,21,22,23]. Detailed clinical and pathological features from all 20 (the present case and 19 reported cases) patients are provided in Table 1. Elderly patients accounted for the majority of cases (ranging from 6-86 years, mean age 59 years), with the exception of a 6-year-old girl. Tumors were more common in male patients (70%). All patients presented with lymphadenopathy (20/20), followed by hepatomegaly (13/20) and splenomegaly (11/20). Other commonly observed symptoms include weakness, night sweats, weight loss, skin lesions and so on. Most patients (18/20) had myeloid disorders, including chronic myelomonocytic leukemia (6/18), myeloproliferative disorder (6/18), acute myelomonocytic leukemia (3/18), acute monocytic leukemia (2/18), and acute myeloid leukemia (1/18). However, there were two exceptions: Facchetti et al. reported a case of mature PDC proliferation coexisting with acute non-B non-T lymphoblastic leukemia, and the present patient showed mature PDC proliferation with T lymphoblastic lymphoma/leukemia.
| Report | Case | Gender | Age | Pattern | Destruction of normal structure | Location | Nodular Myeloid or lymphoid tumor | Associated tumor | Presentation | Follow-up time | Outcome |
| Muller et al. 1983 | 1 | M | 65 | NM | NM | NM | NM | Acute myelomonocytic leukemia | fatigu, weight loss,L,H,S | 7M | Dead |
| Grizzle et al.1985 | 2 | M | 86 | D | YES | NM | NO | Chronic myelogenous leukemia | weight loss,L,H,S | 3W | Dead |
| Beiske et al.1986 | 3 | M | 74 | N | NM | P | YES | Acute myelomonocytic leukemia | Weight loss,night sweat,L | 6M | Dead |
| Thomas et al.1991 | 4 | F | 6 | D | YES | P | NO | Atypical myeloproliferative disorder | L,H,S | NM | NM |
| Koo et al.1990 | 5 | F | 58 | D | YES | P,M | YES | Myeloproliferative disorder | aneimia,night sweat,L,H,S | 28M | Dead |
| Facchetti et al.1990 | 6 | M | 75 | N D | YES | P,C | YES | Chronic myelomonocytic leukemia | Weight loss,L,H,S | 16M | Dead |
| 7 | M | 66 | N | NO | P | YES | Acute nonB nonT lymphoblastic leukiemia | dyspnea fever,L,H,S | 20D | Dead | |
| Baddoura et al.1992 | 8 | M | 58 | D | YES | P,C,M | YES | Chronic myeloproliferative disorder | Fatigue fever weight loss ,L,H,S | Lost | Lost |
| 9 | M | 73 | N | NM | NM | NM | Acute monocytic leukemia | weight loss,fatigue ,L | Lost | Lost | |
| Harris et al.1991 | 10 | F | 54 | N | YES | P | YES | Chronic myelomonocytic leukaemia | fatigue ,weight loss,L,S | 84M | Dead |
| Vermi et al.2004 | 11 | M | 24 | N D | YES | NM | YES | Chronic myelomonocytic leukaemia | L,H,S | 8M | Dead |
| 12 | M | 50 | N | YES | NM | YES | Acute myelomonocytic leukaemia | L,H,S | 11M | Alive | |
| 13 | M | 58 | N | YES | NM | YES | Chronic myelomonocytic leukaemia | L,H | 84M | Dead | |
| 14 | F | 63 | N | YES | NM | YES | Unclassifiable chronic myeloproliferative disorder; | L,H | 15M | Dead | |
| 15 | M | 80 | D | YES | NM | NO | Unclassifiable myeloproliferative/myelodysplastic disorder | L,H,S | 43M | Dead | |
| 16 | F | 62 | N | YES | NM | YES | Acute monocytic leukemia | L | 15M | Dead | |
| 17 | M | 52 | N | YES | NM | YES | Chronic myelomonocytic leukaemia | L,H | 13M | Alive | |
| Song et al.2012 | 18 | M | 55 | N D | YES | NM | YES | Acute myeloid leukaemia | weigh loss,L | 17D | Dead |
| Bodmer et al.2017 | 19 | M | 65 | N | NM | P | NM | Myelodysplastic syndromes | L | 28M | Dead |
| present | 20 | F | 65 | D | YES | P,C,M | YES | T lymphoblastic lymphoma/leukemia | L | 3M | Alive |
Histologically, PDCs in all the cases were easily identified by their plasmacytoid morphology with medium-sized cells, round to ovoid, sometimes slightly elongated nucleus, fine chromatin and moderately abundant cytoplasm. Lymph node architecture effacement was observed in over 90% of these cases (15/16). Only one case showed clusters of PDCs with a nondestructive growth pattern. In other cases, the pattern of PDC accumulation can be roughly divided into two groups: nodular and diffuse patterns. Usually, PDCs formed compact and well-demarcated nodules (10/19), and a diffuse pattern of infiltration was observed in 33.3% (6/19) of these cases. In addition, a mixed pattern of both nodular and diffuse growth was revealed in three patients. Its site of predilection was the paracortical area, while the cortex and medulla area can also be involved in a few cases. Of interest, although the diagnosis of myeloid neoplasms or lymphoblastic lymphoma/leukemia was confirmed by bone marrow biopsy, more than 80% (14/17) of cases showed lymph node involvement of myeloid or lymphoblastic tumors. These myeloid or lymphoblastic tumor cells usually accounted for a small number, were dispersed or formed small clusters along the trabecular septa and medulla, sometimes within the paracortical area or capsule. In a few rare cases, large numbers of myeloid or lymphoblastic tumor cell infiltration can also be found. The expression of immunohistochemical markers was similar to that in normal plasmacytoid dendritic cells, and the most useful markers were CD4, CD68, CD123 and Ki67 (low proliferation rate). B cell or T cell markers were often negative, with occasional aberrant expression of CD2, CD5, CD7 and CD10. It is worth noting that, unlike its counterpart BPDCN, CD56 was negative in the majority of the cases, with only focal and weak reactivity observed in a few cases. Although the PDCs may be superior in number, the prognosis relies on the patient’s underlying myeloid neoplasm rather than the expansion of PDCs. All patients underwent chemotherapy, but the prognosis was usually dismal. The median follow-up duration was 26 months, ranging from 17 days to 7 years, and 14 (82%) of 17 patients had died. Thus, the five-year OS rate was 11.7%.
The nature of nodal accumulations of PDCs in patients with myeloid neoplasms has perplexed the pathologist and clinician for quite a long time. Lymph node parenchyma effacement can be seen in almost all patients, and aberrant expression of CD2, CD5, CD7, CD10 or CD56 in some cases favors a neoplastic origin of these cells[5]. Recently, via fluorescence in situ hybridization, an increasing number of studies have suggested that neoplastic mature plasmacytoid dendritic cells and their associated myeloid neoplasm cells share similar and clonal chromosomal abnormalities. A case from Vermi et al. demonstrated monosomy 7 in both myeloid leukemia and PDC nodules[16]. Monosomy 7 was also observed in two kinds of cellular components in one case reported by Chen et al., and they reported another case showing loss of 20q12 in both populations[24]. One case of cutaneous PDCs associated with CMML also presented with trisomy 13 in both leukemia cells and neoplastic PDCs[21]. In addition, with the development of massive parallel sequencing (NGS), Bodmer et al. revealed a common PTPN11 gene mutation shared by the MDS and PDC populations[23]. Despite this genetic evidence, hints provided by the clinical course of PDCs paved the way for the coming truth. Follow-up of a patient by Harris et al. showed that the nonbiopsied lymph node did not enlarge but regressed after being given prednisone and busulphan [19]. In addition, Dargent et al revealed an interesting phenomenon of simultaneous regression of cutaneous PDC accumulation and reduction of peripheral leukemia cells after therapy aimed at leukemia[21]. All of these findings led some researchers to consider PDC proliferation as part of the entire tumor process, other than an independent tumor component, and both components may share a common myeloid precursor-cell origin[25].
Apart from the present case, only two case of mature PDC proliferation with lymphoblastic leukemia was reported[15,29]. However, due to the nondestructive growth pattern of the PDC part, the author considered the PDC part as the reactive component of the tumor in one case. Different from the former case, the grow pattern and pathogenic mutation of demonstrated the neoplastic origin of these PDCs. Another case of mature PDC proliferations associated with T-lymphoblastic leukemia was recently reported by Oscar Sliva et al in bone marrow, while the limitation of this report lies on the unsorting NGS of PDCs and T lymphoblasts components. By definition, MPDMN is a tumor characterized by mature plasmacytoid dendritic cell proliferation invariably associated with a myeloid neoplasm[5]. While in the present case, the tumor was mainly composed of neoplastic PDC proliferation, along with a relatively small amount of T lymphoblast lymphoma cells and Langerhans cells, the question of whether to put the case into MPDMN remains to be answered. Of interest, Langerhans cells mixed with PDCs seen in the present case were also observed in some reports of MPDMN[26,27,28]. Therefore, initially we hypothesized that there may be a hematopoietic stem cell at the very beginning of those mature PDC proliferation-associated tumors. It may have multilineage potential to give rise to neoplastic cells of different lineages under different microenvironments. However, the mutations detected by NSG were completely different in PDCs and T lymphoblasts components, which goes against the initial assumption, the mature PDC proliferations and T lymphoblastic lymphoma may be genetically unrelated to each other. Thorough researches about mutational clonality between mature PDC proliferations and lymphoid neoplasms are still need to illustrate the uncommon condition. Although studies focused on mature PDC proliferation have lasted more than 30 years, the cell lineage is still not definitely understood. Whether mature PDC proliferation can occur in both lymphoid and myeloid tumors also remains to be elucidated in the future. The significance of our case lies in two aspects: 1) to report a rare case of mature PDC proliferation coexisting with T lymphoblastic lymphoma/leukemia and reveal different mutations between mature PDC proliferation and T lymphoblastic lymphoma/leukemia; 2) although accumulations of PDCs may occur in some infections or reactive lymphadenopathy, the presence of extensive nodules or infiltration of PDCs strongly reminds the pathologist to carefully evaluate the bone marrow or peripheral blood status of the patient to exclude a hidden myeloid or other neoplasm.
Author Contributions
Cong Deng , Bei-bei Gao and Tian-li Wang wrote the manuscript. Xiao-Na Chang , Gui-xiang Xiao and Qin Xia systematically consulted the pathological sections. Hua-Xiong Pan and Xiu Nie critically commented and edited the manuscript.
Funding
The work was supported by grants from the National Natural Science Foundation of China (No. 81773022).
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
Data availability is not applicable to this article as no new data were created or analyzed in this study.
Acknowledgments
We acknowledge the work and contribution of all the health providers from Wuhan Union Hospital.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Lennert, K.; Remmele, W. [Karyometric research on lymph node cells in man. I. Germinoblasts, lymphoblasts & lymphocytes]. Acta Haematol 1958, 19, 99–113. [Google Scholar]
- Siegal, F.P.; Kadowaki, N.; Shodell, M.; Fitzgerald-Bocarsly, P.A.; Shah, K.; Ho, S.; Antonenko, S.; Liu, Y.J. The nature of the principal type 1 interferon-producing cells in human blood. Science 1999, 284, 1835–1837. [Google Scholar] [CrossRef]
- Cella, M.; Jarrossay, D.; Facchetti, F.; Alebardi, O.; Nakajima, H.; Lanzavecchia, A.; Colonna, M. Plasmacytoid monocytes migrate to inflamed lymph nodes and produce large amounts of type I interferon. Nat Med 1999, 5, 919–923. [Google Scholar] [CrossRef]
- Jegalian, A.G.; Facchetti, F.; Jaffe, E.S. Plasmacytoid dendritic cells: Physiologic roles and pathologic states. Adv Anat Pathol 2009, 16, 392–404. [Google Scholar] [CrossRef]
- Facchetti, F.; Cigognetti, M.; Fisogni, S.; Rossi, G.; Lonardi, S.; Vermi, W. Neoplasms derived from plasmacytoid dendritic cells. Mod Pathol 2016, 29, 98–111. [Google Scholar] [CrossRef]
- Mathan, T.S.; Figdor, C.G.; Buschow, S.I. Human plasmacytoid dendritic cells: From molecules to intercellular communication network. Front Immunol 2013, 4, 372. [Google Scholar] [CrossRef]
- Zhan, Y.; Chow, K.V.; Soo, P.; Xu, Z.; Brady, J.L.; Lawlor, K.E.; Masters, S.L.; O'Keeffe, M.; Shortman, K.; Zhang, J.G.; et al. Plasmacytoid dendritic cells are short-lived: Reappraising the influence of migration, genetic factors and activation on estimation of lifespan. Sci Rep 2016, 6, 25060. [Google Scholar] [CrossRef]
- Facchetti, F.; Vermi, W.; Mason, D.; Colonna, M. The plasmacytoid monocyte/interferon producing cells. Virchows Arch 2003, 443, 703–717. [Google Scholar] [CrossRef]
- Facchetti, F.; De Wolf-Peeters, C.; van den Oord, J.J.; De Vos, R.; Desmet, V.J. Plasmacytoid T cells: A cell population normally present in the reactive lymph node. An immunohistochemical and electronmicroscopic study. Hum Pathol 1988, 19, 1085–1092. [Google Scholar] [CrossRef]
- Stary, G.; Bangert, C.; Tauber, M.; Strohal, R.; Kopp, T.; Stingl, G. Tumoricidal activity of TLR7/8-activated inflammatory dendritic cells. J Exp Med 2007, 204, 1441–1451. [Google Scholar] [CrossRef]
- Chaperot, L.; Blum, A.; Manches, O.; Lui, G.; Angel, J.; Molens, J.P.; Plumas, J. Virus or TLR agonists induce TRAIL-mediated cytotoxic activity of plasmacytoid dendritic cells. J Immunol 2006, 176, 248–255. [Google Scholar] [CrossRef]
- Urosevic, M.; Dummer, R.; Conrad, C.; Beyeler, M.; Laine, E.; Burg, G.; Gilliet, M. Disease-independent skin recruitment and activation of plasmacytoid predendritic cells following imiquimod treatment. J Natl Cancer Inst 2005, 97, 1143–1153. [Google Scholar] [CrossRef]
- Muller-Hermelink, H.K.; Stein, H.; Steinmann, G.; Lennert, K. Malignant lymphoma of plasmacytoid T-cells. Morphologic and immunologic studies characterizing a special type of T-cell. Am J Surg Pathol 1983, 7, 849–862. [Google Scholar] [PubMed]
- Koo, C.H.; Mason, D.Y.; Miller, R.; Ben-Ezra, J.; Sheibani, K.; Rappaport, H. Additional evidence that "plasmacytoid T-cell lymphoma" associated with chronic myeloproliferative disorders is of macrophage/monocyte origin. Am J Clin Pathol 1990, 93, 822–827. [Google Scholar] [CrossRef] [PubMed]
- Facchetti, F.; De Wolf-Peeters, C.; Kennes, C.; Rossi, G.; De Vos, R.; van den Oord, J.J.; Desmet, V.J. Leukemia-associated lymph node infiltrates of plasmacytoid monocytes (so-called plasmacytoid T-cells). Evidence for two distinct histological and immunophenotypical patterns. Am J Surg Pathol 1990, 14, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Vermi, W.; Facchetti, F.; Rosati, S.; Vergoni, F.; Rossi, E.; Festa, S.; Remotti, D.; Grigolato, P.; Massarelli, G.; Frizzera, G. Nodal and extranodal tumor-forming accumulation of plasmacytoid monocytes/interferon-producing cells associated with myeloid disorders. Am J Surg Pathol 2004, 28, 585–595. [Google Scholar] [CrossRef]
- Baddoura, F.K.; Hanson, C.; Chan, W.C. Plasmacytoid monocyte proliferation associated with myeloproliferative disorders. Cancer 1992, 69, 1457–1467. [Google Scholar] [CrossRef]
- Prasthofer, E.F.; Prchal, J.T.; Grizzle, W.E.; Grossi, C.E. Plasmacytoid T-cell lymphoma associated with chronic myeloproliferative disorder. Am J Surg Pathol 1985, 9, 380–387. [Google Scholar]
- Harris, N.L.; Demirjian, Z. Plasmacytoid T-zone cell proliferation in a patient with chronic myelomonocytic leukemia. Histologic and immunohistologic characterization. Am J Surg Pathol 1991, 15, 87–95. [Google Scholar] [CrossRef]
- Beiske, K.; Langholm, R.; Godal, T.; Marton, P.F. T-zone lymphoma with predominance of 'plasmacytoid T-cells' associated with myelomonocytic leukaemia--a distinct clinicopathological entity. J Pathol 1986, 150, 247–255. [Google Scholar] [CrossRef]
- Dargent, J.L.; Henne, S.; Pranger, D.; Balzarini, P.; Sartenaer, D.; Bulliard, G.; Rack, K.; Facchetti, F. Tumor-forming plasmacytoid dendritic cells associated with myeloid neoplasms. Report of a peculiar case with histopathologic features masquerading as lupus erythematosus. J Cutan Pathol 2016, 43, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.O.; Beiske, K.; Hann, I.; Koo, C.; Mason, D.Y. Immunohistological diagnosis of "plasmacytoid T cell lymphoma" in paraffin wax sections. J Clin Pathol 1991, 44, 632–635. [Google Scholar] [CrossRef] [PubMed]
- Bodmer, A.; Menter, T.; Juskevicius, D.; Arranto, C.; Wenzel, F.; Dirnhofer, S.; Tzankov, A. Sharing of a PTPN11 mutation by myelodysplastic bone marrow and a mature plasmacytoid dendritic cell proliferation provides evidence for their common myelomonocytic origin. Virchows Arch 2017, 470, 469–473. [Google Scholar] [CrossRef]
- Chen, Y.C.; Chou, J.M.; Ketterling, R.P.; Letendre, L.; Li, C.Y. Histologic and immunohistochemical study of bone marrow monocytic nodules in 21 cases with myelodysplasia. Am J Clin Pathol 2003, 120, 874–881. [Google Scholar] [CrossRef]
- Dargent, J.L.; Delannoy, A.; Pieron, P.; Husson, B.; Debecker, C.; Petrella, T. Cutaneous accumulation of plasmacytoid dendritic cells associated with acute myeloid leukemia: A rare condition distinct from blastic plasmacytoid dendritic cell neoplasm. J Cutan Pathol 2011, 38, 893–898. [Google Scholar] [CrossRef] [PubMed]
- Shon, W.; Peters, M.S.; Reed, K.B.; Ketterling, R.P.; Dogan, A.; Gibson, L.E. Atypical generalized eruptive histiocytosis clonally related to chronic myelomonocytic leukemia with loss of Y chromosome. J Cutan Pathol 2013, 40, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Breton, G.; Oliveira, T.Y.; Zhou, Y.J.; Aljoufi, A.; Puhr, S.; Cameron, M.J.; Sekaly, R.P.; Nussenzweig, M.C.; Liu, K. Restricted dendritic cell and monocyte progenitors in human cord blood and bone marrow. J Exp Med 2015, 212, 385–399. [Google Scholar] [CrossRef]
- Song, H.L.; Huang, W.Y.; Chen, Y.P.; Chang, K.C. Tumorous proliferations of plasmacytoid dendritic cells and Langerhans cells associated with acute myeloid leukaemia. Histopathology 2012, 61, 974–983. [Google Scholar] [CrossRef]
- Fei, F.; Liedtke, M.; Silva, O. Case Report: Mature Plasmacytoid Dendritic Cell Proliferation Associated With a Lymphoid Neoplasm. Front Oncol. 2022, 12, 903113. [Google Scholar] [CrossRef]
Figure 3.
A: Lymphoblasts hiding in mature plasmacytoid dendritic cells, featuring condensed chromatin, inconspicuous nucleoli and scanty cytoplasm (HE ×400); B: Scattered lymphoblasts highlighted by TDT stain (IHC ×40).
Figure 3.
A: Lymphoblasts hiding in mature plasmacytoid dendritic cells, featuring condensed chromatin, inconspicuous nucleoli and scanty cytoplasm (HE ×400); B: Scattered lymphoblasts highlighted by TDT stain (IHC ×40).
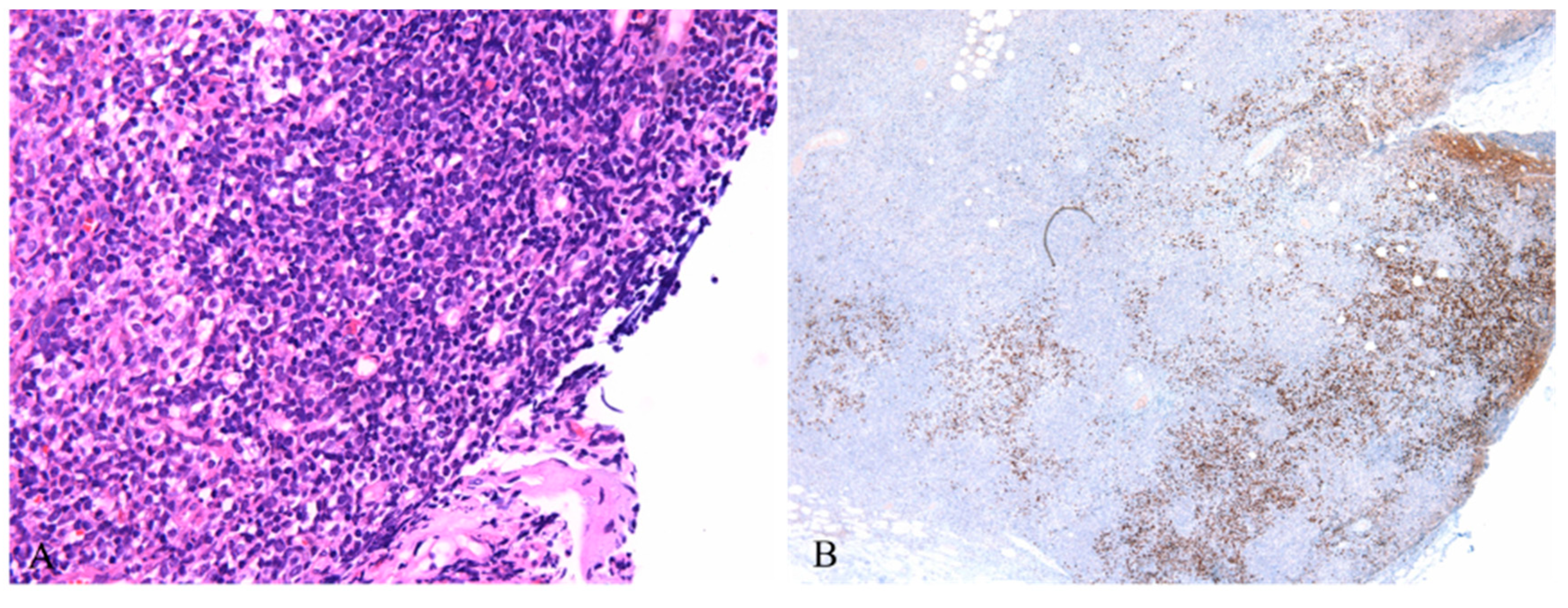
Figure 4.
A: Hematopoietic tissue in bone marrow was replaced by lymphoblasts (HE ×400); B: Tumor cells showed nuclear expression of TDT (IHC ×400).
Figure 4.
A: Hematopoietic tissue in bone marrow was replaced by lymphoblasts (HE ×400); B: Tumor cells showed nuclear expression of TDT (IHC ×400).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



