Submitted:
08 September 2023
Posted:
18 September 2023
You are already at the latest version
Abstract
The aim of our study was to evaluate the impact of T. gondii status on eosinophils count (PNE), eosinophil to lymphocyte ratio (ELR) and eosinophil to neutrophil to lymphocytes ratio (ENLR) before and after can-nabis cessation in patients with psychiatric disorders. One hundred and eighty-eight patients were includ-ed in the study. T. gondii, PNE, ELR, ENLR, and urinary cannabis were measured at baseline and after 4 weeks of cannabis cessation. Highest PNE (p = .02), ELR (p = .03) and ENLR levels (p = .031) and highest increase of PNE (p = .044), and ENLR (p = .036) levels were found in patients after cannabis cessation only in the Toxo+ group. At four weeks, significant interactions between cannabis and T. gondii status for PNE (p = .038), and for ENLR (p = .043) levels were found, as well as for the evolution between baseline and 4 weeks for ENLR level (p = .049). After cannabis cessation, we found a positive correlation between negative symptoms and PNE levels at 4 weeks in the Toxo+ group. This study shows that the increase of inflammation after cannabis cessation might be modulated by T. gondii seropositivity status in patient after cannabis cessation.
Keywords:
inflammation
; T. gondii
; cannabis use
; eosinophils counts
1. Introduction
Toxoplasma Gondii is an intracellular parasite which affects approximately 30% of humans worldwide, with a higher heterogeneity depending on geographic location [1,2]. Indeed, the seroprevalence in the USA or the UK was estimated between 8 and 22% but in central and south America and Europe the estimates range from 30 to 90% [3]. There is a higher prevalence of toxoplasma among psychiatric populations. A recent meta-analysis found a mean seroprevalence of 37% and 28% respectively in patients with bipolar disorder and in healthy controls [4] however considering single studies, the seroprevalence can reach 76.9% in France [5]. Interestingly, the geographic variations of the seroprevalence was more important in healthy controls than in patients with psychiatric disorders [4]. Unfortunately, few studies have investigated the highest seroprevalence of T. gondii in addictive disorders, excepted a meta-analysis [6].
The hypothesis of immuno-inflammation induced by T. gondii could explain the particular link with psychiatric disorders and addictions [7,8]. The secretion of pro-inflammatory cytokines following T. toxoplasma gondii infection (such as IL-6, IL-1B and TNF-a) could affect the microglie and thereby affect the neurotransmitter secretion of serotonin and dopamine [9]. A link with cognitive deterioration has therefore raised as cognitive impairment (processing speed, working memory, executive functions) was found among healthy and psychiatric populations [1,10] which can be correlated to the degree of inflammation among patients (IL-6) [10,11].
Substance use disorders have an impact on inflammatory markers [12]. Some studies suggested that cannabis use was associated with lower inflammation in patients with psychiatric disorders (IL-6, IFN-G and CRP) [13,14,15] however with inconsistant data [16,17]. One study found that cannabis use was not associated with specific inflammatory profiles but a composite score representing the systemic inflammation state, might moderate the cannabis-psychosis association in first-episode of psychosis patients [18]. Finally, cannabis cessation in patients with psychosis is associated with an increase of leucocyte, lymphocyte and monocyte counts [17].
Eosinophils counts have been suggested as a key player of innate and adaptive immune response [19]. Indeed Eosinophil/lymphocyte ratio and eosinophil neutrophil/lymphocytes ratio have been proposed as indicators of systemic inflammation in patients with cancer or with autoimmune rheumatic diseases [20]. They found that highest ratios are associated with poorer prognosis [21]. These associations have also been found among smokers in psychiatric populations as compared to non-smokers [20] and alcohol use disorder patients with comorbid bipolar disorder [22].
Eosinophils are thought to be effector cells in the body’s defense against parasites infections and the mechanism of action may differ depending on the parasite [23] but to our knowledge, no study had investigated the link between eosinophils, T.gondii serological status and cannabis use and cessation.
The aim of our study is to evaluate the impact of T.gondii serological status on eosinophils count (PNE), eosinophil/lymphocyte ratio (ELR) and eosinophil-neutrophil /lymphocyte ratio (ENLR) before and after cannabis cessation in patients with psychiatric disorders. The second objective of our work is to study the associations between these ratios, T. gondii status and clinical symptoms.
2. Materials and Methods
2.1. Participants
This retrospective study included one hundred and eighty-eight inpatients in the psychiatry and addictology department at Paul Brousse Hospital (Paris) between July 2019 and November 2022. The inclusion criteria were: (i) inpatients during an acute phase of a psychiatric disorder as defined by the ICD 10 classification (F10-99). The diagnosis was performed by the psychiatrists in charge of the patients and was extracted from hospitalization records; (ii) being over 18 years old. Exclusion criteria included neurological disorders (F00 to F10 ICD 10 diagnosis) and use of anti-inflammatory treatments. In this non-interventional retrospective cohort study only using existing data from routine care were added. According to the Jarde law (2012) modifying the public health law (2004), a complete information was given to all patients on the possible retrospective use of their routine care data for research purposes. All patients were informed that they could refuse the study without consequences on the care provided. None of the included patients refused. This MR-004 non interventional study was conducted in accordance with the data-processing and freedom law 1978 modified, the declaration of Helsinki and was approved by the CNIL (N°1980120), a French institution devoted to the protection of participants.
2.2. Data collected
Socio-demographic data, comorbidities, undergoing treatments, smoking status, and body mass index (BMI) were collected. Positive and Negative Syndrome Scale (PANSS) scale [24] was assessed by trained psychiatrists. These PANSS scores were only extracted for patients with psychosis (i.e. diagnosis of schizophrenia, schizoaffective disorder, other psychotic disorder, bipolar disorder or major depressive disorder with psychotic symptoms). T. gondii serology was assessed by chemiluminescence enzyme immunoassay (Liaison ® XL DiaSorin) at baseline. WBC results were collected at baseline and 4 weeks later. Urinary cannabis was also collected upon admission and 4 weeks later using an immuno-enzymatic method (C800 Abbott ®). All biological samples were analyzed in the laboratory of Paul Brousse Hospital. All data were extracted from the computerized medical records and stored in an anonymized file in accordance with the CNIL declaration.
2.3. Data analyses
Analyses were performed with Jamovi (Version 2.2), a graphic user to the R statistical analysis software for scientific medical publications (Available on: https://www.jamovi.org). To compare PNE, ELR, ENLR levels between cannabis user (THC+) and non-users (THC-) among positive patients for T. gondii serology (Toxo +) vs negative patients (Toxo -), a Shapiro-Wilk test was performed to confirm the normal distribution of the samples. For samples including more than 30 patients with normal distribution of parameters, a t-test was used to compare THC+ versus THC- in patients Toxo + and in patients Toxo – and paired sample t-test was used to compare the intra-group changes. We used a Mann-Whitney non parametric test, and a Wilcoxon test was used to compare the intra-changes in small samples (< 30 patients) and/or if the data distribution was not normal. For categorical variables, a Chi-square test was used. To assess the association between PNE, ELR and ENLR and sociodemographic or PANSS score, Spearman or Pearson correlations were computed.
Two multivariate analyses were performed using linear regression. At baseline and at 4 weeks, we included age, gender, use of antipsychotics (Yes/No), use of mood stabilizers (Yes/No), use of antidepressants (Yes/No), use anxiolytic (Yes/No), BMI, smoking status (Yes/No), cannabis status (Yes/No), presence of illness that may impact inflammation (Yes/No) and diagnosis of psychosis (Yes/No).
To evaluate the interaction between Toxoplasma Gondii and cannabis status on PNE, ELR and ENLR, a general linear model was performed at baseline and 4 weeks using the same confounding factors used in the linear regression.
3. Results
3.1. Description of the population
One hundred and eighty-eight inpatients were included in this study (106 Toxo +, 82 Toxo -) at baseline and one hundred and nineteen attended follow-up at 4 weeks (58 Toxo+ vs 61 Toxo -). The main characteristics of this population are described in Table 1. Toxo + patients were older than Toxo- patients (p < .01). There were more smokers in the Toxo + group (p < .01). No difference was found for BMI, gender, cannabis status, diagnosis and PANSS score at baseline between the two groups. Concerning medication at baseline, there were no difference considering the number of drug-free patients, drug-naïve patients, antipsychotic, antidepressant or anxiolytic treatment between the two groups. Highest use of mood stabilizer was found in the Toxo+ group (p = .01).
3.2. Comparison of PNE, ELR and ENLR levels between cannabis users and non-users in patients according to the seropositivy of T. Gondii
At baseline, no difference was found for PNE, ELR and ENLR in univariate or multivariate analysis between the two groups (Figure 1).
At four weeks, in the univariate analysis, a highest PNE level was found in the cannabis cessation group (p = .035) but no difference was found for ELR and ENLR levels. However, in the multivariate analysis, highest PNE (p = .02), ELR (p = .03) and ENLR levels (p = .031) were found in the cannabis cessation group (Figure 1). Between baseline and 4 week-follow up, we found in the group THC + a significant increase in PNE (p < .01), ELR (p < .01) and ENLR (p < .01) levels (Figure 1). We found similar results in the group THC- with a significant increase of PNE (p < .01), ELR (p < .01) and ENLR (p < .01) levels (Figure 1). However, we found that the increase levels of PNE (p = .044), and ENLR (p = .036) were greater in the THC+ group as compared to the THC- group. We also found a trend significant increase of ELR level in the THC+ group (p = .071) (Figure 2).
3.3. Comparison of PNE, ELR and ENLR levels between cannabis users and non-users in patients seronegative for T. gondii
At baseline, no difference was found between the two groups for PNE, ELR and ENLR considering univariate or multivariate analysis (Figure 1).
At four weeks, in the univariate analysis, highest PNE (p < .01), ELR (p = .036), ENLR (p = .043) levels were found in the cannabis cessation group but these differences did not remain significant in the multivariate analysis (Figure 1). Between baseline and 4 weeks, we found a significant increase in PNE (p < .01), ELR (p < .01) and ENLR (p < .01) levels (Figure 1) in the THC + group. We found similar results in the group THC- with a significant increase in PNE (p < .01), ELR (p < .01) and ENLR (p < .01) levels (Figure 1). PNE (p = .33), ELR (p = .47) and ENLR (p = .11) were similar between the two groups (Figure 2).
3.4. Interaction between cannabis and T. gondii status and PNE, ELR and ENLR
At baseline, we did not find an interaction between cannabis and T. gondii status regarding the PNE, ELR and ENLR levels.
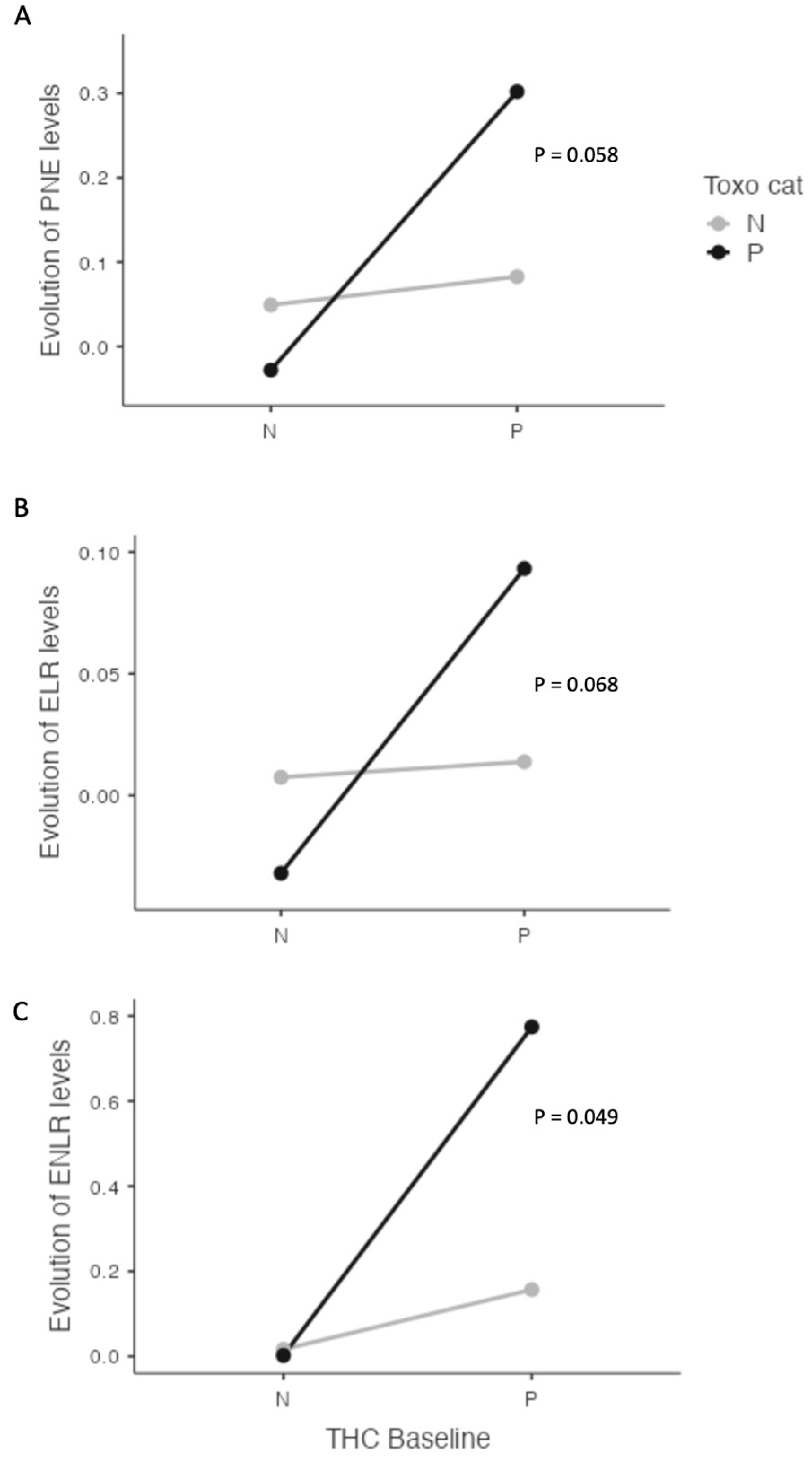
At four weeks, we found significant interactions between cannabis and T. gondii status for PNE (p = .038), and for ENLR (p = .043) levels and a statistical trend for ELR level (p = .072) (Figure 3). Further, we found a significant interaction between cannabis and T. gondii status regarding the evolution between baseline and four weeks of ENLR level (p = .049) and a statistical trend for the evolution of PNE (p = .058) and ELR (p = .068) levels (Figure 3).
3.5. Correlation between IgG antibodies against T. gondii, PNE, ELR, ENLR and clinical variables
At baseline, in the THC+ Toxo+ group, a positive correlation was found between IgG antibodies against T. gondii and ENLR level (r =.492; p = .024) whereas no correlation was found in the THC- group. In the psychosis subgroup no correlation was found between IgG antibodies against T. gondii, PNE, ELR, ENLR and PANSS score, considering the cannabis status.
At four weeks, no correlation was found between IgG antibodies against T. gondii and PNE, ELR, ENLR, nor with PNE, ELR, ENLR between baseline and four weeks, regardless the cannabis status. Patients with psychosis who stopped using cannabis showed a positive correlation between PANSS negative subscale and PNE (r = .87; p < .01) or ELR (r = .74; p = .024) at 4 weeks. Moreover, in the same group, we found a positive correlation between the evolution (between baseline and 4 weeks) of PANSS negative subscale and the evolution of PNE (r = .08; p = .018) or of ELR (r = 0.75; p = .032). In the Toxo+ THC- group, negative correlations were found between PNE level at 4 weeks and PANSS general subscale at 4 weeks (r = -.44; p = .018) but also between the evolution of PNE levels and PANSS total score (r = -.61; p < .01), PANSS positive subscale score (r = -.4; p = .035), PANSS negative subscale score (r = -.46; p = .015), and PANSS general subscale score (r = -.66; p < .01) at four weeks. A negative correlation was also found between PNE level at 4 weeks and the evolution of PANSS total score (r = -.66; p < .01), PANSS positive subscale score (r = -.56; p < .01), and PANSS general subscale score (r = -.65; p < .01) between baseline and four weeks.
4. Discussion
In this study, we found that cannabis cessation in patients with psychiatric disorders was associated with an increase of indirect inflammatory markers such as PNE, ELR and ENLR. Moreover, we found that these disorders seem to be modulated by T. gondii seropositivity. Indeed, we found increased levels of PNE, ELR and ENLR at 4 weeks among T. gondii positive patients as compared to T. gondii negative patients. Furthermore, T. gondii status and cannabis cessation were associated with highest of PNE, ELR and ENLR. Finally, we found a positive correlation between negative symptoms and PNE levels at 4 weeks in the group of Toxo+ and THC+ patients.
The role of eosinophils in innate immunity may partly explain our results. Indeed, eosinophils have traditionally been considered as end- stage cells in innate immunity that contribute to anti-parasitic immunity or allergy by their pro-inflammatory and destructive effects [19]. In addition to direct secretion of pro-inflammatory cytokines [25], eosinophils participate in innate immunity by secreting various eosinophils-derived cationic granules including eosinophil derived neurotoxin, eosinophil cationic protein, and eosinophil peroxidase. With a highly basic nature, these cationic proteins are highly toxic to parasitic because they can damage cells by binding to negatively charged cell membranes and thus disordering the lipid bilayer or by affecting the activity of enzymes within tissues [26].
Previous studies have already evaluated the impact of cannabis use on inflammatory markers in patients with psychiatric disorders [13,14,15,16,17,18]. Few studies have investigated the specific impact of cannabis cessation on CRP levels and white blood cell counts [15,17]. Lowest levels of CRP were found at baseline in schizophrenic patients, with increased levels of CRP after cannabis cessation, suggesting a restoration of low grade inflammation after cannabis cessation [15]. This result was confirmed in a larger second study [17]. Despite the fact that CRP levels were not different in our study, we did not found a difference between cannabis users and non users considering PNE ELR and ENLR, ratios that had not been tested in previous studies to our knowledge. These results are in line with other studies, which also found no differences between these two populations [13,16]. However, we found again that cannabis cessation was associated with an increase of PNE, ELR and ENLR levels regarding the T. gondii status. This result is in accordance with our previous results which found that cannabis cessation was associated with increased levels of leucocyte and monocyte [17].
Moreover, we found that the inflammatory enhancement after cannabis cessation is modulated by the T. gondii infection. Indeed, we found an interaction between T. gondii and cannabis cessation for PNE and ENLR levels and a positive correlation between IgG antibody levels against T. gondii and ENLR levels. The link found between T. gondii and eosinophils levels is not surprising because eosinophils are thought to be a major effector cells in the body’s defense against parasitic infections [23]. Moreover, seropositivity to T. gondii has been known to interact with inflammation markers in patients with psychiatric disorders [5,11]. During T. gondii infection, cytokines such as IL-6 and IL-27 play a critical role [5]. The first is required for the development of protective immunity against T. gondii infection, and the second is crucial for limiting infection-induced inflammatory damage [27]. Eosinophils play a key role in the innate anti-parasite immune response, notably through the secretion of pro-inflammatory cytokines such as IL-6 and Tumor Necrosis Factor α [19,25]. The increase of inflammation found in patients seropositive for T. gondii [5,28] could explain the different kinetic of inflammation markers after cannabis cessation between patients positive or negative patients.
To our knowledge, our study is the first to investigate the link between cannabis consumption and T. gondii infection. Endocannabinoid anandamide levels and mRNA transcripts for CB2 receptors are higher during acute episodes of schizophrenia [29,30], during which inflammation is known to be greater [31]. It is also known that chronic T. gondii infection, or other brain infections, may increase endocannabinoid levels [32] with neuroprotective effects. We can therefore hypothesize that in patients with psychiatric disorders with latent T. gondii infection, cannabis consumption may enhance the anti-inflammatory effect of endocannabinoids.
We found positive a correlation between PNE and ELR levels and PANSS negative subscale only in patients with psychosis who stopped using cannabis and who were seropositive for T. gondii. A link between T. gondii infection and negative symptoms has been found in patients with schizophrenia [11,33] and more precisely considering alogia (defined by a poverty of speech) [11]. This association can be explained by the decreased neural activity in the ventral striatum and the reduced connectivity in reward-relevant neural circuitry [34] observed in negative symptoms. Our hypothesis is that the negative symptoms are induced by increased inflammation after cannabis cessation, which is modulated by T. gondii infection.
Our study has several limitations. First, the retrospective design of the cohort does not allow us to conclude for a potential causal relationship. Furthermore, because of the retrospective design of our study, we were unable to characterize specifically each addiction of our patients. Missing information such as the frequency of cannabis use, the cannabis potency, or the exact THC/cannabidiol ratio, could bias our results. Secondly, most of the data were collected from medical records, which could cause an important bias. Finally, we did not evaluate other inflammatory markers such as cytokine levels. These limitations can be explained by the naturalistic, non-interventional design of our study using existing data from routine care. Our study thus needs to be replicated by others to confirm the veracity of our results.
5. Conclusions
In conclusion, this study shows that the increase of inflammation after cannabis cessation could be modulated by seropositivity for T. gondii leading to an activation of the innate system highlighted by an over secretion of eosinophils (PNE, ELR and ENLR). Studying the different factors before and after cannabis cessation could be useful to better understand the dual diagnosis between cannabis use disorder and psychiatric disorder and enable future specific treatment or intervention.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, B.R., A.B. and NH.; data curation, B.R.; V.L. ; methodology, B.R. and A.A.; validation, N.H., and A.B.; formal analysis, B.R. A.A.; writing—original draft preparation, B.R. ; writing—review and editing, V.L.; C.M.; A.A., A.B., N.H.; supervision, N.H. and A.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This MR-004 non interventional study was conducted in accordance with the data-processing and freedom law 1978 modified, the declaration of Helsinki and was approved by the CNIL (N°1980120), a French institution devoted to the protection of participants.
Informed Consent Statement
According to the Jarde law (2012) modifying the public health law (2004), a complete information was given to all patients on the possible retrospective use of their routine care data for research purposes. All patients were informed that they could refuse the study without consequences on the care provided. None of the included patients refused.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
Bruno Romeo, Valentine Lestra, Catherine Martelli, Ammar Amirouche and Nora Hamdani have no conflict of interest. Amine Benyamina has given talk for Lundbeck, Mylan, Merck-Serono and Bristol-Myers Squibb and member of bord Indivior.
References
- de Haan L, Sutterland AL, Schotborgh JV, Schirmbeck F, de Haan L. Association of Toxoplasma gondii Seropositivity With Cognitive Function in Healthy People: A Systematic Review and Meta-analysis. JAMA Psychiatry 2021;78:1103. [CrossRef]
- Nogareda F, Le Strat Y, Villena I, De Valk H, Goulet V. Incidence and prevalence of Toxoplasma gondii infection in women in France, 1980–2020: model-based estimation. Epidemiol Infect 2014;142:1661–70. [CrossRef]
- Aguirre AA, Longcore T, Barbieri M, Dabritz H, Hill D, Klein PN, et al. The One Health Approach to Toxoplasmosis: Epidemiology, Control, and Prevention Strategies. EcoHealth 2019;16:378–90. [CrossRef]
- Cossu G, Preti A, Gyppaz D, Gureje O, Carta MG. Association between toxoplasmosis and bipolar disorder: A systematic review and meta-analysis. J Psychiatr Res 2022;153:284–91. [CrossRef]
- Hamdani N, Daban-Huard C, Lajnef M, Richard J-R, Delavest M, Godin O, et al. Relationship between Toxoplasma gondii infection and bipolar disorder in a French sample. J Affect Disord 2013;148:444–8. [CrossRef]
- Sutterland AL, Fond G, Kuin A, Koeter MWJ, Lutter R, van Gool T, et al. Beyond the association. Toxoplasma gondii in schizophrenia, bipolar disorder, and addiction: systematic review and meta-analysis. Acta Psychiatr Scand 2015;132:161–79. [CrossRef]
- Chaudhury A, Ramana B. Schizophrenia and bipolar disorders: The Toxoplasma connection. Trop Parasitol 2019;9:71. [CrossRef]
- Johnson SK, Johnson PTJ. Toxoplasmosis: Recent Advances in Understanding the Link Between Infection and Host Behavior. Annu Rev Anim Biosci 2021;9:249–64. [CrossRef]
- Tyebji S, Seizova S, Hannan AJ, Tonkin CJ. Toxoplasmosis: A pathway to neuropsychiatric disorders. Neurosci Biobehav Rev 2019;96:72–92. [CrossRef]
- Hamdani N, Daban-Huard C, Lajnef M, Gadel R, Le Corvoisier P, Delavest M, et al. Cognitive deterioration among bipolar disorder patients infected by Toxoplasma gondii is correlated to interleukin 6 levels. J Affect Disord 2015;179:161–6. [CrossRef]
- Fond G, Boyer L, Schürhoff F, Berna F, Godin O, Bulzacka E, et al. Latent toxoplasma infection in real-world schizophrenia: Results from the national FACE-SZ cohort. Schizophr Res 2018;201:373–80. [CrossRef]
- Herrera-Imbroda J, Flores-López M, Ruiz-Sastre P, Gómez-Sánchez-Lafuente C, Bordallo-Aragón A, Rodríguez de Fonseca F, et al. The Inflammatory Signals Associated with Psychosis: Impact of Comorbid Drug Abuse. Biomedicines 2023;11:454. [CrossRef]
- Gibson CL, Bassir Nia A, Spriggs SA, DeFrancisco D, Swift A, Perkel C, et al. Cannabinoid use in psychotic patients impacts inflammatory levels and their association with psychosis severity. Psychiatry Res 2020;293:113380. [CrossRef]
- Miller BJ, Buckley PF, McEvoy JP. Inflammation, substance use, psychopathology, and cognition in phase 1 of the clinical antipsychotic trials of intervention effectiveness study. Schizophr Res 2018;195:275–82. [CrossRef]
- Romeo B, Lestra V, Martelli C, Benyamina A, Hamdani N. Cannabis Cessation, Inflammatory Markers and Schizophrenia. J Dual Diagn 2022;18:33–41. [CrossRef]
- Goetz RL, Miller BJ. Total and Differential White Blood Cell Counts, Cocaine, and Marijuana Use in Patients With Schizophrenia. J Nerv Ment Dis 2019;207:633–6. [CrossRef]
- Romeo B, Lestra V, Martelli C, Amirouche A, Benyamina A, Hamdani N. Increased markers of inflammation after cannabis cessation and their association with psychotic symptoms. Acta Neuropsychiatr 2023:1–10. [CrossRef]
- Corsi-Zuelli F, Marques L, da Roza DL, Loureiro CM, Shuhama R, Di Forti M, et al. The independent and combined effects of cannabis use and systemic inflammation during the early stages of psychosis: exploring the two-hit hypothesis. Psychol Med 2021:1–11. [CrossRef]
- Long H, Liao W, Wang L, Lu Q. A Player and Coordinator: The Versatile Roles of Eosinophils in the Immune System. Transfus Med Hemotherapy 2016;43:96–108. [CrossRef]
- Çekici Y, Yılmaz M, Seçen Ö. New inflammatory indicators: association of high eosinophil-to-lymphocyte ratio and low lymphocyte-to-monocyte ratio with smoking. J Int Med Res 2019;47:4292–303. [CrossRef]
- Holub K, Biete A. New pre-treatment eosinophil-related ratios as prognostic biomarkers for survival outcomes in endometrial cancer. BMC Cancer 2018;18. [CrossRef]
- Dirani E, Bou Khalil R, Raad G, Richa S. Eosinophils to Lymphocytes Ratio (ELR) as a Potential Inflammatory Biomarker in Patients with Dual Diagnosis of Bipolar and Alcohol Use Disorders: A Retrospective Cohort Study. J Dual Diagn 2022;18:144–52. [CrossRef]
- Kuang, FL. Approach to Patients with Eosinophilia. Med Clin North Am 2020;104:1–14. [CrossRef]
- Kay SR, Fiszbein A, Opler LA. The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia. Schizophr Bull 1987;13:261–76. [CrossRef]
- Aceves SS, Ackerman SJ. Relationships Between Eosinophilic Inflammation, Tissue Remodeling, and Fibrosis in Eosinophilic Esophagitis. Immunol Allergy Clin North Am 2009;29:197–211. [CrossRef]
- Acharya KR, Ackerman SJ. Eosinophil Granule Proteins: Form and Function. J Biol Chem 2014;289:17406–15. [CrossRef]
- Silver JS, Stumhofer JS, Passos S, Ernst M, Hunter CA. IL-6 Mediates the Susceptibility of Glycoprotein 130 Hypermorphs to Toxoplasma gondii. J Immunol 2011;187:350–60. [CrossRef]
- Fabiani S, Pinto B, Bonuccelli U, Bruschi F. Neurobiological studies on the relationship between toxoplasmosis and neuropsychiatric diseases. J Neurol Sci 2015;351:3–8. [CrossRef]
- Melamede, R. Parasitic brain infection, endocannabinoids, and schizophrenia. Med Hypotheses 2009;72:220–2. [CrossRef]
- De Marchi N, De Petrocellis L, Orlando P, Daniele F, Fezza F, Di Marzo V. Endocannabinoid signalling in the blood of patients with schizophrenia. Lipids Health Dis 2003;2:5. [CrossRef]
- Lestra V, Romeo B, Martelli C, Benyamina A, Hamdani N. Could CRP be a differential biomarker of illness stages in schizophrenia? A systematic review and meta-analysis. Schizophr Res 2022;246:175–86. [CrossRef]
- Eljaschewitsch E, Witting A, Mawrin C, Lee T, Schmidt PM, Wolf S, et al. The Endocannabinoid Anandamide Protects Neurons during CNS Inflammation by Induction of MKP-1 in Microglial Cells. Neuron 2006;49:67–79. [CrossRef]
- Esshili A, Thabet S, Jemli A, Trifa F, Mechri A, Zaafrane F, et al. Toxoplasma gondii infection in schizophrenia and associated clinical features. Psychiatry Res 2016;245:327–32. [CrossRef]
- Goldsmith DR, Rapaport MH. Inflammation and Negative Symptoms of Schizophrenia: Implications for Reward Processing and Motivational Deficits. Front Psychiatry 2020;11. [CrossRef]
Figure 1.
T. gondii and cannabis status and Eosinophils (PNE) (A), Eosionophils lymphocytes ratio (ELR) (B), Eosinophils neutrophils lymphocytes ratio (ENLR) (C). No difference was found at baseline concerning these three markers. Higher levels of PNE, ELR and ENLR levels were found in the Toxo + group at four weeks. Significant increase between baseline and four weeks were found for PNE, ELR and ENLR levels in Toxo+ and Toxo – groups according to cannabis status.
Figure 1.
T. gondii and cannabis status and Eosinophils (PNE) (A), Eosionophils lymphocytes ratio (ELR) (B), Eosinophils neutrophils lymphocytes ratio (ENLR) (C). No difference was found at baseline concerning these three markers. Higher levels of PNE, ELR and ENLR levels were found in the Toxo + group at four weeks. Significant increase between baseline and four weeks were found for PNE, ELR and ENLR levels in Toxo+ and Toxo – groups according to cannabis status.
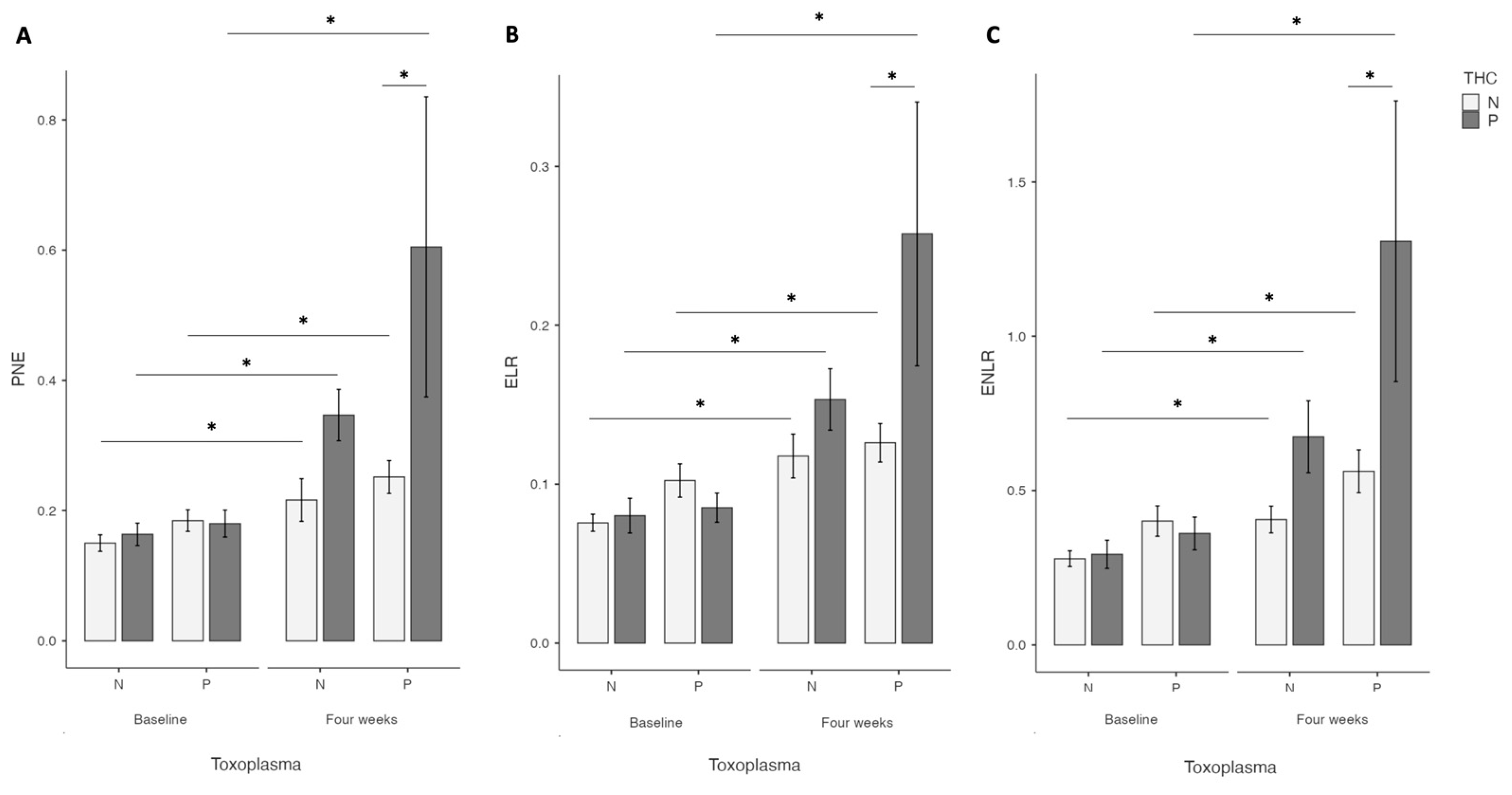
Figure 2.
Prospective evaluation of Eosinophils (PNE) (A), Eosionophils lymphocytes ratio (ELR) (B) and Eosinophils neutrophils lymphocytes ratio (ENLR) (C) evolution according to cannabis and T. gondii status at four weeks. A higher increase of PNE, ELR and ENLR levels after cannabis cessation versus non-users was found in the Toxo+ group.
Figure 2.
Prospective evaluation of Eosinophils (PNE) (A), Eosionophils lymphocytes ratio (ELR) (B) and Eosinophils neutrophils lymphocytes ratio (ENLR) (C) evolution according to cannabis and T. gondii status at four weeks. A higher increase of PNE, ELR and ENLR levels after cannabis cessation versus non-users was found in the Toxo+ group.
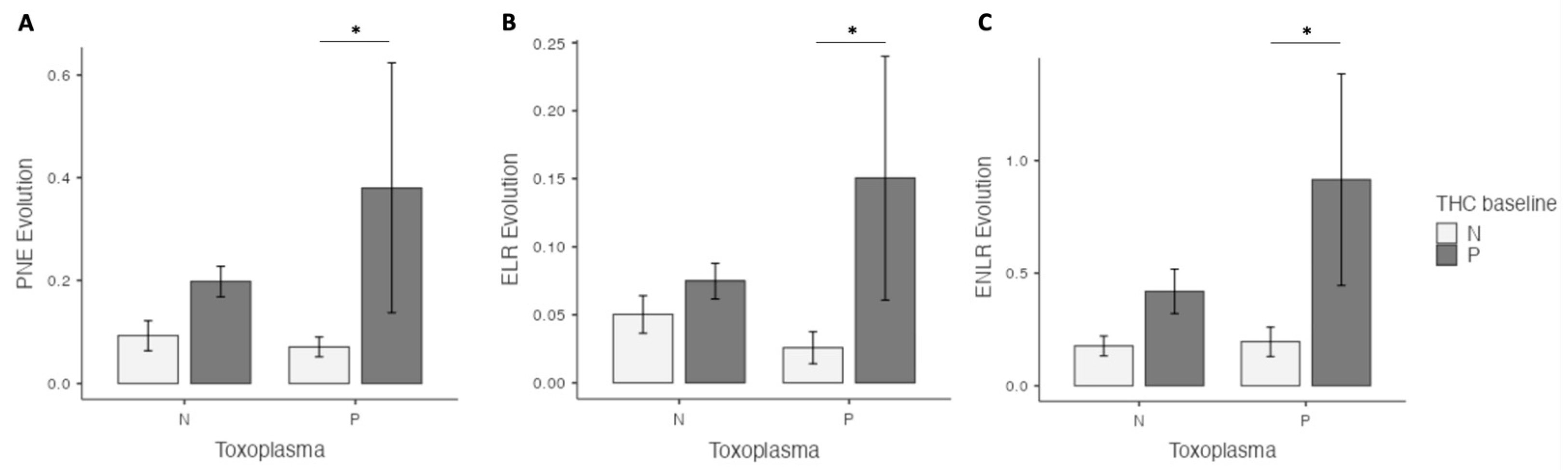
Figure 3.
Interactions between cannabis and T. gondii status for Eosinophils (PNE) (A), Eosionophils lymphocytes ratio (ELR) (B) and Eosinophils neutrophils lymphocytes ratio (ENLR) (C) at four weeks after cannabis cessation. Significant interactions were found between cannabis and T. gondii status for PNE and ENLR levels four weeks after cannabis cessation with a statistical trend for ELR level.
Figure 3.
Interactions between cannabis and T. gondii status for Eosinophils (PNE) (A), Eosionophils lymphocytes ratio (ELR) (B) and Eosinophils neutrophils lymphocytes ratio (ENLR) (C) at four weeks after cannabis cessation. Significant interactions were found between cannabis and T. gondii status for PNE and ENLR levels four weeks after cannabis cessation with a statistical trend for ELR level.
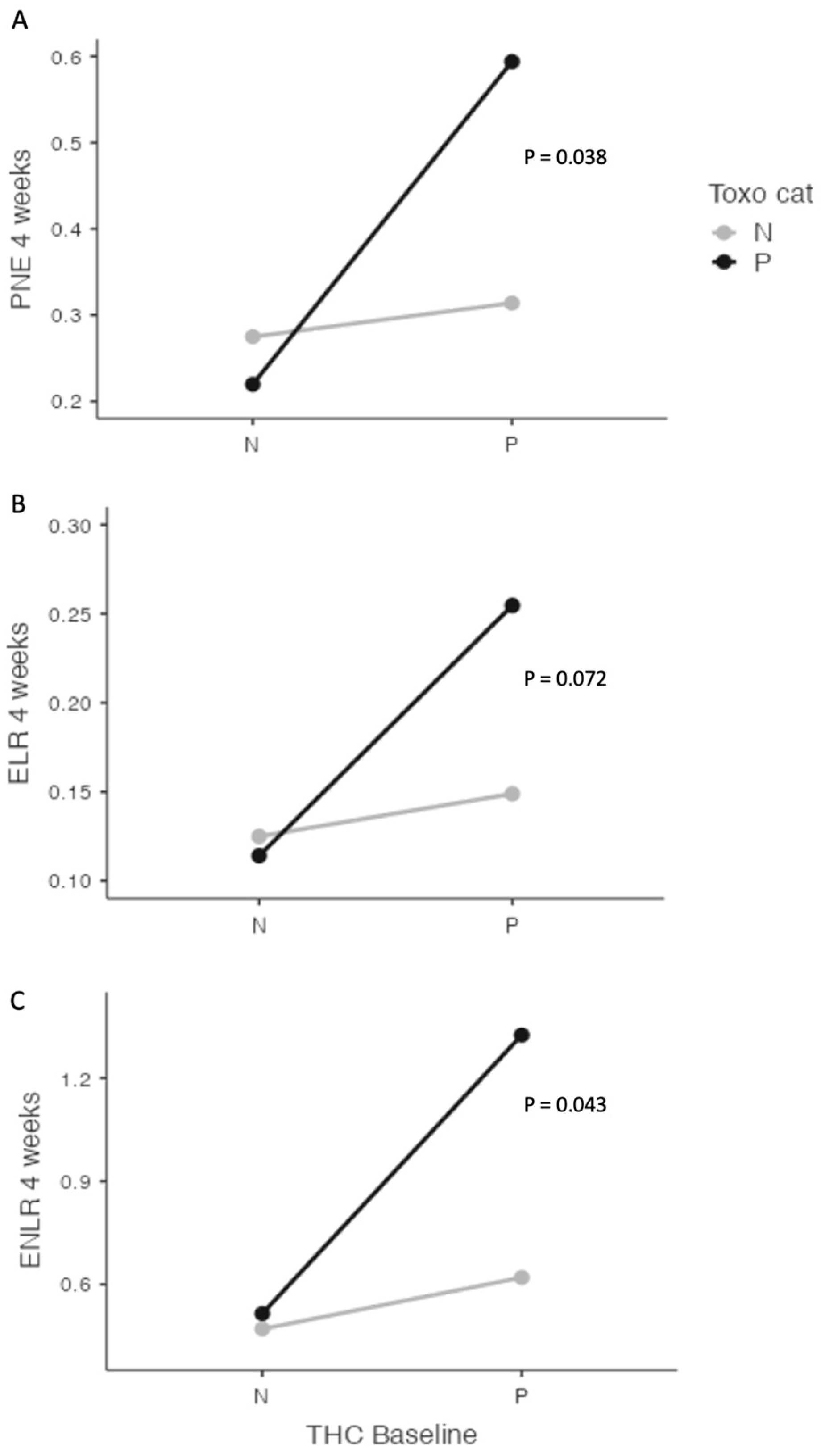
Figure 4.
Interactions between cannabis and T. gondii status for Eosinophils (PNE) (A), Eosionophils lymphocytes ratio (ELR) (B) and Eosinophils neutrophils lymphocytes ratio (ENLR) (C) between baseline and four weeks after cannabis cessation. A significant interaction was found between cannabis and T. gondii status and ENLR level evolution with a statistical trend for PNE and ELR levels.
Figure 4.
Interactions between cannabis and T. gondii status for Eosinophils (PNE) (A), Eosionophils lymphocytes ratio (ELR) (B) and Eosinophils neutrophils lymphocytes ratio (ENLR) (C) between baseline and four weeks after cannabis cessation. A significant interaction was found between cannabis and T. gondii status and ENLR level evolution with a statistical trend for PNE and ELR levels.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



