
Submitted:
15 September 2023
Posted:
18 September 2023
You are already at the latest version
Abstract
Meckel’s diverticulum (MD) is the most common congenital anomaly of the gastrointestinal tract with a 1-3% prevalence in general population. The surgical management of symptomatic MD is well described in the literature, but there is still no consensus on the indication for prophylactic resection of incidental asymptomatic MD. To address this issue, we extensively reviewed the current literature and report our experience with laparoscopic management of an unusual case of MD causing ileal volvulus and acute peritonitis two weeks after a laparoscopic appendectomy for acute gangrenous appendicitis performed in another hospital. A 50-year-old man presented to the emergency department with acute and severe abdominal pain, vomiting and constipation. He had undergone a laparoscopic appendectomy for acute appendicitis two weeks before in another hospital. The patient was apyretic, distressed, and sought an antalgic position. The abdomen was mildly distended, tender, and the Blumberg sign was mildly positive in the central quadrants. The clinical picture deteriorated with fever, peritonismus, and leukocytosis. A CT scan showed an ileo-ileal adhesion near the ileocolic junction and dilatation of the upstream loops with air-fluid levels. Through an urgent laparoscopy, a necrotic mass, the MD, was wedge-resected and the surrounding ileal volvulus derotated. The postoperative course was uneventful. There is no definitive consensus on the appropriate management of incidental asymptomatic MD, although several studies have attempted to identify guiding criteria. Features of the MD, patient’s risk factors, clinical presentation, and surgical approach need to be considered to establish definitive guidelines for the management of incidental asymptomatic MD. In the absence of definitive guidelines, personal expertise and judgement are the main resources for the surgeon approaching an incidental asymptomatic MD.
Keywords:
Meckel’s Diverticulum
; Laparoscopy
; Peritonitis
; Emergency surgery
; Volvulus
; Appendectomy
1. Introduction
Meckel’s diverticulum (MD) is the most common congenital anomaly of the gastrointestinal (GI) tract, with a prevalence of 1-3% in the general population [1,2,3,4,5]. It is the result of incomplete obliteration of the vitelline (omphalomesenteric) duct, which connects the primitive intestine to the yolk sac in early fetal life [2,6]. By definition, MD is a true diverticulum as it is surrounded by all the layers of the small bowel wall [7]. The right vitelline artery, which arises from the superior mesenteric artery, supplies the MD [8]. When present, the MD is located along the antimesenteric margin of the ileum at a mean distance of 52.4 cm (range, 7 - 100) from the ileocecal valve (ICV) and has a mean length and diameter of 3 and 1.58 cm, respectively [1]. In about half of cases, MD contains heterotopic mucosa within its wall: most commonly gastric mucosa (60%), followed by pancreatic acinar tissue (16%), and the remainder Brunner’s glands, pancreatic islets, colonic mucosa, hepatobiliary tissue, or a combination of these [3,9]. The presence of ectopic tissue within, especially the gastric type and at younger age, tend to increase the risk of clinical manifestation from MD, mostly in the form of bleeding [1,10,11]. According to the literature, MD becomes symptomatic in 4-71% of cases, predominantly in the first three to four decades of life, and up to four times more frequently in men [1,12,13]. Symptomatic adult patients usually present with intestinal obstruction (35.6%), inflammation (29.4%) or intestinal bleeding (27.3%) [1]. In paediatric symptomatic patients, these clinical manifestations occur in 46.7%, 19.5% and 25.3% of cases, respectively [1]. Elderly patients most commonly develop neoplastic degeneration within the MD tissue [1,14,15], often with a poor prognosis [16]. Complications of MD are hemorrhage, intestinal obstruction, volvulus, inflammation, and perforation [14]. Perforation or inflammation of the MD is occasionally misdiagnosed as acute appendicitis [1,17]. Mortality of MD is around 0.1% [18]. We report our experience of laparoscopic management of an unusual case of MD causing ileal volvulus and acute peritonitis only 15 days after laparoscopic appendectomy for acute appendicitis. The surgical management of MD has been widely described in the literature, but there is no definitive consensus regarding its prophylactic resection. To address this issue, we conducted a comprehensive review of the literature.
2. Case presentation
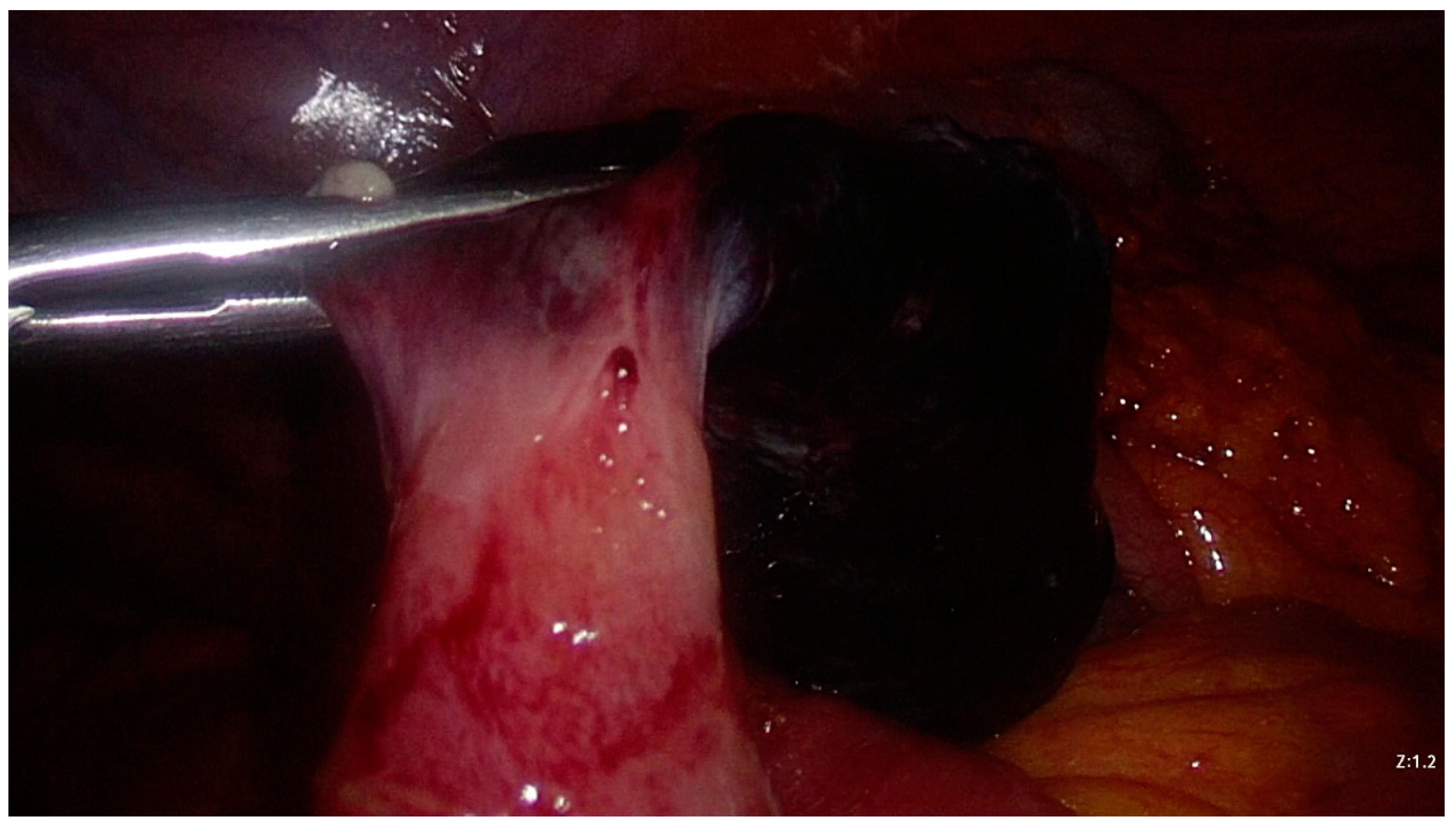
A 50-year-old man presented to the emergency department (ED) of our hospital (Ospedale di Circolo e Fondazione Macchi, Varese, Italy) with acute, cramping, diffuse and severe (Numeric Pain Rating Scale 8) abdominal pain, associated with vomiting and constipation. He had undergone a laparoscopic appendectomy (LAE) for acute appendicitis two weeks before in another hospital. His past medical history includes an ischaemic stroke and a patent foramen ovale, currently treated with low-dose aspirin. The patient was apyretic, had a distressed and anxious appearance and sought an antalgic position. On physical examination, scars from previous surgery were physiologically healed; peristalsis was present on auscultation; the abdomen was mildly distended, tender all over, and the Blumberg sign was mildly positive in the central quadrants. The patient reported the passage of gas, but there was no fecal material on digital rectal examination. Initial laboratory tests were within normal limits (leukocytes 6.3*109 units/L, PCR 1.0 mg/dL), except for a slight elevation in transaminases. A plain thoraco-abdominal x-ray showed a dilated stomach, coprostasis, no free air in the abdomen, and metallic clips from previous surgery. Computed tomography (CT) scan showed adhesion between two distal ileal loops near the ileocolic junction, thickening of the surrounding peritoneum, dilatation of the upstream intestinal loops with internal air-fluid levels, no free fluid in the abdomen [Figure 1, Figure 2 and Figure 3]. Initial conservative management (analgesic, antispasmodic, antiemetic and gastroprotective drugs with parenteral hydration) failed as the clinical condition rapidly deteriorated. The patient developed a fever and his abdominal pain worsened with onset of diffuse peritonismus. Blood tests showed significant leukocytosis (12.53*109 units/L). An urgent abdominal ultrasound (US) showed free fluid in the lower abdominal quadrants. An urgent laparoscopy was performed. The trocars were placed in the same positions as the previous LAE. On exploration, there was abundant serosanguinous fluid in the abdominal cavity. Approximately 30 cm proximal to the ileocolic junction, there was an ileal volvulus around a necro-hemorrhagic mass originating from the ileal wall [Figure 4]. The surgeon derotated the volvulus and performed a wedge-resection of the necro-hemorrhagic mass [Figure 5]. On anatomopathological examination, the mass was identified as a MD measuring 3 x 2.5 x 2 cm, with ischemic and infarcted areas and no evidence of heterotopic tissue. No neoplastic cells were found in an intraperitoneal fluid sample. The postoperative course was uneventful, and the patient was discharged on postoperative day (POD) 7. Follow-up was unremarkable.
3. Materials and Methods
We extensively examined past publications using the Database PubMed – United States National Library of Medicine. We considered 58 publications, including case series, case reports, and reviews, ranging from 1976 to 2023.
4. Discussion
Meckel’s diverticulum is a diagnostic challenge for clinicians because of its non-specific clinical manifestations. Meckel’s diverticulum is frequently discovered incidentally or during work-up for clinical conditions initially attributed to another cause (e.g., during videolaparoscopy). According to the literature, surgical resection, either open or laparoscopic, is the treatment of choice for a symptomatic MD, when appropriate [1,19]. The extent of resection should be guided by the clinical presentation and intraoperative findings, ranging from a stapled diverticulectomy or a limited wedge resection with closure of the ileal defect [20], to a more extensive bowel resection with subsequent loop anastomosis [21]. Meckel’s diverticulectomy has been demonstrated to be a safe method in the management of symptomatic MD in both adult and paediatric cohorts [19,22]. Morbidity was found to be higher after bowel resection than after simple diverticulectomy [23,24]. However, some advocate segmental bowel resection followed by anastomosis to ensure that no ectopic mucosa is left behind [25]. Taking a middle ground, Brungardt et al. in 2021 stated that diverticulectomy and small bowel resection are both likely to be appropriate approaches to the management of symptomatic MD when used in conjunction with surgeon discretion, as there is no difference in outcomes between the two techniques [26]. Laparoscopic diverticulectomy is technically safe, cost-effective, and efficient in both emergency and elective settings [20,22,27], avoiding the morbidity associated with both open surgery and small bowel resection, with the added benefits of precise operative diagnosis and shorter recovery time [24,28].
However, despite decades of research, there is no consensus on the management and indication for possible prophylactic resection of incidental asymptomatic MD [29]. Most of the evidence on MD comes from retrospective studies. There are only a few randomized studies, mostly single center, on complications, and none on incidental MD.
Early studies about asymptomatic MD were not in favor of prophylactic surgical resection. In 1962, Weinstein et al. reviewed 560 incidental MDs, of which 158 were left in situ on the basis that wide-mouthed diverticula (average width and length 1.92 cm x 2.99 cm, respectively) were not considered dangerous, and therefore their resection would only add to the risk of surgical complications and not provide any benefit [30]. In 1976, Soltero et al. estimated the lifetime risk of complications from MD to be 4.2%, eventually falling to 0% in old age; from then published data, they calculated that it would be necessary to resect approximately 800 asymptomatic MDs to save one patient’s life [31]. In 1986, considering that the calculated lifetime risk of complications from MD is very low and the risk of complications after diverticulectomy is not negligible, Leijonmarck et al. concluded that an incidental asymptomatic MD in adults should be left in situ [12]. In addition, they reported 28 cases of MD left in situ with no further clinical manifestations after an average of almost 8 years of follow up [12]. In 1993, DiGiacomo et al. stated that any incidental MD whose resection with a stapler would be unsafe and difficult because it is wide and short, should be left in situ because of the low risk of complications [32]. In 1995, Peoples et al. stated that incidental diverticulectomy in adults should be abandoned, because the lifetime risk of developing complications does not significantly outweigh the surgical morbidity and mortality of resection [33].
In 1994, Cullen et al. concluded that incidental MDs should be removed to avoid future potential complications unless an additional condition (e.g., generalized peritonitis) would make resection hazardous [34]. In 1995, Matsagas et al. studied a population of 2074 patients undergoing AE with intraoperative evaluation for MD; they concluded that resection of the unexpected MD can be performed safely with a low complication rate, regardless of the patient’s age [35].
In 2004, Bani-Hani et al. stated that resection of incidentally found MDs does not increase operative morbidity and mortality and was therefore worthy, especially in young patients with long and narrow (diameter ≤ 2 cm) MD [36]. Since then, many authors have advocated prophylactic resection of asymptomatic MD [11,37,38,39,40,41,42,43,44,45,46], also, but not exclusively, to prevent potential future neoplastic degeneration [39,40,41,42,44,45]. A recent multi-center retrospective study by Tree et al. supports laparoscopic stapled resection of incidental asymptomatic MD, considering the overall low complication rate and the potential for malignant transformation [24].
On the other hand, some other authors in the 2000s still prefer to leave an asymptomatic MD in situ. According to a 2004 observational study of 47 patients by Stone et al., removal of any asymptomatic MD should not be supported because complications of such a procedure, although uncommon, are often life-threatening [47]. In a 2008 review of the literature, Zani et al. did not support prophylactic resection of an incidental asymptomatic MD, noting that MD resection carried a 5.3% morbidity rate, mostly wound infections, while leaving MD in situ had an overall lower morbidity rate and long-term risk of complications [18].
A risk-based approach was first proposed in 1983 by Mackey et al.: they reviewed over 400 symptomatic MDs and identified some risk factors for complications such as age ≤40 years, length of the diverticulum ≥2 cm, presence of heterotopic tissue, and male sex [48].
In 2005, Park et al., after reviewing 1476 patients found to have an MD during surgery from 1950 to 2002, could neither definitively support nor reject the recommendation that every incidental asymptomatic MD should be removed, but recommended removal of any incidental MD that had any of the four features (patient age younger than 50 years, male sex, diverticulum length greater than 2 cm, and the presence of histologically abnormal tissue) most commonly associated with clinical manifestations [14]. In the same year, after reviewing 233 cases of MD incidentally discovered during an appendectomy, Ueberrueck et al. stated that in cases of gangrenous or perforated appendicitis, an incidentally discovered MD should be left in place, whereas in an only mildly inflamed appendix it should be removed [49]. In 2006, Robijn et al. proposed a scoring system based on four risk factors (male sex, age <45 years, diverticula >2 cm, and the presence of a fibrous band), to guide the decision for surgery in incidental asymptomatic MDs [50]. This risk-based approach has been supported by a growing number of authors [25,51,52,53,54,55,56,57,58]. According to Mackey [48], Park [14], Robijn [50] and other more recent authors, some characteristics of the patient and the MD were clear indications to perform a prophylactic diverticulectomy. According to DiGiacomo, only the intra-operatively tested fit of the MD within the mechanical stapler could lead to a decision [32]. Considering the work of Hansen, although the size of the MD was an indication for prophylactic resection due to the risk of future complications, the severe intercurrent gangrenous appendicitis validly discouraged such an adjunctive surgical act [1]. According to Leijonmack, the size of our reported MD was not an indication for prophylactic diverticulectomy [12]. According to the conclusions of both Cullen [34] and Ueberrueck [49], gangrenous appendicitis with peritonitis was a contraindication for incidental removal of the MD, as the surgical act would have been riskier than leaving it in situ. Looking a posteriori at our reported case, not removing the MD during the previous LAE seems to be a mistake, but an a priori decision regarding its resection at such a time would have been controversial and could only have been based on the judgement, expertise, and competence of the treating surgeon.
5. Conclusions
In conclusion, MD occurs in a minority of the population and its clinical manifestations are largely non-specific. We managed life-threatening small bowel volvulus and peritonitis in a patient who had undergone LAE two weeks earlier, with the MD left in situ. There is no definitive consensus on the appropriate management of incidental asymptomatic MD. Over the decades, several studies have attempted to identify criteria that would allow a decision to be made whether to resect or leave in situ an incidental asymptomatic MD. After a thorough review of the literature, we could not definitively state whether the MD of our reported patient should have been resected or left in situ at the time of the previous LAE. According to our analysis, MD characteristics, patient’s risk factors and the clinical presentation, and the surgical approach (open VS laparoscopic) need to be considered to establish definitive guidelines for the management of incidental asymptomatic MD. Considering the surgical approach, complications that might discourage open surgery and resection are less common with laparoscopic diverticulectomy. In the absence of definitive guidelines, expertise and common sense remain the main resources for the surgeon approaching an incidental asymptomatic MD.
Author Contributions
M.Z.: planned and wrote the original draft; D.I.: involved in the planning and revision of the manuscript; V.P.: involved in the planning and revision of the manuscript; N.G.: revised the manuscript; M.M.: revised the manuscript; G.S.: revised the manuscript; G.C.: involved in the planning and revision of the manuscript, supervised; G.I.: involved in the planning and revision of the manuscript, supervised. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
The patient verbally agreed and gave consent to publish this paper.
Data Availability Statement
Patients’ data registry of Ospedale di Circolo e Fondazione Macchi (VA).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hansen CC, Søreide K. Systematic review of epidemiology, presentation, and management of Meckel’s diverticulum in the 21st century. Medicine (Baltimore). 2018 Aug;97(35):e12154. [CrossRef] [PubMed Central]
- Sagar J, Kumar V, Shah DK. Meckel’s diverticulum: a systematic review. J. R. Soc. Med. 2006; 99: 501–5.
- Sancar S, Demirci H, Sayan A, Arıkan A, Candar A. Meckel’s diverticulum: Ten years’ experience. Ulus Cerrahi Derg. 2015 Jun 1;31(2):65-7. [CrossRef] [PubMed] [PubMed Central]
- Srisajjakul S, Prapaisilp P, Bangchokdee S. Many faces of Meckel’s diverticulum and its complications. Jpn J Radiol. 2016 May;34(5):313-20. Epub 2016 Mar 1. [CrossRef] [PubMed]
- Kuru S, Kismet K. Meckel’s diverticulum: clinical features, diagnosis, and management. Rev Esp Enferm Dig. 2018 Nov;110(11):726-732. [CrossRef] [PubMed]
- Turgeon DK, Barnett JL. Meckel’s diverticulum. Am J Gastroenterol. 1990 Jul;85(7):777-81. [PubMed]
- Schaedlich DS, Borges PC, Lacombe A, Moron RA. Intestinal intussusception of Meckel’s diverticulum, a case report and literature review of the last five years. einstein (São Paulo). 2023;21:eRC0173.
- Kovacs M, Botstein J, Braverman S. Angiographic diagnosis of Meckel’s diverticulum in an adult patient with negative scintigraphy. J Radiol Case Rep. 2017 Mar 31;11(3):22-29. [CrossRef] [PubMed] [PubMed Central]
- Uppal K, Tubbs RS, Matusz P, Shaffer K, Loukas M. Meckel’s diverticulum: a review. Clin Anat. 2011 May;24(4):416-22.
- Chen JJ, Lee HC, Yeung CY, Chan WT, Jiang CB, Sheu JC, Wang NL. Meckel’s Diverticulum: Factors Associated with Clinical Manifestations. ISRN Gastroenterol. 2014 Apr 1;2014:390869. [CrossRef] [PubMed] [PubMed Central]
- Chen, Q.; Gao, Z.; Zhang, L.; Zhang, Y.; Pan, T.; Cai, D.; Xiong, Q.; Shu, Q.; Qian, Y. Multifaceted behavior of Meckel’s diverticulum in children. J. Pediatr. Surg. 2018, 53, 676–681.
- Leijonmarck CE, Bonman-Sandelin K, Frisell J, Räf L. Meckel’s diverticulum in the adult. Br J Surg. 1986 Feb;73(2):146-9. [CrossRef] [PubMed]
- Fa-Si-Oen PR, Roumen RM, Croiset van Uchelen FA. Complications and management of Meckel’s diverticulum--a review. Eur J Surg. 1999 Jul;165(7):674-8. [CrossRef] [PubMed]
- Park JJ, Wolff BG, Tollefson MK, Walsh EE, Larson DR. Meckel diverticulum: the Mayo Clinic experience with 1476 patients (1950-2002). Ann Surg. 2005 Mar;241(3):529-33. [CrossRef] [PubMed] [PubMed Central]
- Alemayehu H, Hall M, Desai AA, St Peter SD, Snyder CL. Demographic disparities of children presenting with symptomatic Meckel’s diverticulum in children’s hospitals. Pediatr Surg Int. 2014 Jun;30(6):649-53. Epub 2014 May 9. [CrossRef] [PubMed]
- Kabir SA, Raza SA, Kabir SI. Malignant neoplasms of Meckel’s diverticulum; an evidence based review. Ann Med Surg (Lond). 2019 Jun 4;43:75-81. [CrossRef] [PubMed] [PubMed Central]
- Kloss, B.T., Broton, C.E. & Sullivan, A.M. Perforated Meckel diverticulum. Int J Emerg Med 3, 455–457 (2010). [CrossRef]
- Zani A, Eaton S, Rees CM, Pierro A. Incidentally detected Meckel diverticulum: to resect or not to resect? Ann Surg. 2008 Feb;247(2):276-81. [CrossRef] [PubMed]
- Ruscher KA, Fisher JN, Hughes CD, Neff S, Lerer TJ, Hight DW, Bourque MD, Campbell BT. National trends in the surgical management of Meckel’s diverticulum. J Pediatr Surg. 2011 May;46(5):893-6.
- Sharma RK, Jain VK. Emergency surgery for Meckel’s diverticulum. World J Emerg Surg. 2008 Aug 13;3:27. [CrossRef] [PubMed] [PubMed Central]
- Mukai M, Takamatsu H, Noguchi H, Fukushige T, Tahara H, Kaji T. Does the external appearance of a Meckel’s diverticulum assist in choice of the laparoscopic procedure? Pediatr Surg Int. 2002 May;18(4):231-3. [CrossRef] [PubMed]
- Ding Y, Zhou Y, Ji Z, Zhang J, Wang Q. Laparoscopic Management of Perforated Meckel’s diverticulum in adults. Int. J. Med. Sci. 2012; 9: 243–7.
- Piñero A, Martínez-Barba E, Canteras M, Rodriguez JM, Castellanos G, Parrilla P. Surgical management and complications of Meckel’s diverticulum in 90 patients. Eur J Surg. 2002;168(1):8-12. [CrossRef] [PubMed]
- Tree K, Kotecha K, Reeves J, Aitchison L, Noeline Chui J, Gill AJ, Mittal A, Samra JS. Meckel’s diverticulectomy: a multi-centre 19-year retrospective study. ANZ J Surg. 2023 Feb 23. Epub ahead of print. [CrossRef] [PubMed]
- Lequet J, et al. Meckel’s diverticulum in the adult. Journal of Visceral Surgery (2017). [CrossRef]
- Meckel’s: A National Surgical Quality Improvement Program Survey in Adults Comparing Diverticulectomy and Small Bowel Resection Joseph G. Brungardt, MD1, Brian R. Cummiskey, MD1, and Kurt P. Schropp, MD1.
- Palanivelu C, Rangarajan M, Senthilkumar R, Madankumar MV, Kavalakat AJ. Laparoscopic management of symptomatic Meckel’s diverticula: a simple tangential stapler excision. JSLS. 2008 Jan-Mar;12(1):66-70. [PubMed] [PubMed Central]
- Ezekian B, et al., Outcomes of laparoscopic resection of Meckel’s diverticulum are equivalent to open laparotomy, J Pediatr Surg (2018). [CrossRef]
- Rahmat S, Sangle P, Sandhu O, Aftab Z, Khan S. Does an Incidental Meckel’s Diverticulum Warrant Resection? Cureus. 2020 Sep 8;12(9):e10307. [CrossRef] [PubMed] [PubMed Central]
- WEINSTEIN EC, CAIN JC, REMINE WH. Meckel’s diverticulum: 55 years of clinical and surgical experience. JAMA. 1962 Oct 20;182:251-3. [CrossRef] [PubMed]
- Soltero MJ, Bill AH. The natural history of Meckel’s Diverticulum and its relation to incidental removal. A study of 202 cases of diseased Meckel’s Diverticulum found in King County, Washington, over a fifteen year period. Am J Surg. 1976 Aug;132(2):168-73. [CrossRef] [PubMed]
- DiGiacomo JC, Cottone FJ. Surgical treatment of Meckel’s diverticulum. South Med J. 1993 Jun;86(6):671-5. [CrossRef] [PubMed]
- Peoples JB, Lichtenberger EJ, Dunn MM. Incidental Meckel’s diverticulectomy in adults. Surgery 1995;118:649-52.
- Cullen JJ, Kelly KA, Moir CR, Hodge DO, Zinsmeister AR, Melton LJ 3rd. Surgical management of Meckel’s diverticulum. An epidemiologic, population-based study. Ann Surg. 1994 Oct;220(4):564-8; discussion 568-9. [CrossRef] [PubMed] [PubMed Central]
- Matsagas MI, Fatouros M, Koulouras B, Giannoukas AD. Incidence, complications, and management of Meckel’s diverticulum. Arch Surg. 1995 Feb;130(2):143-6. [CrossRef] [PubMed]
- Bani-Hani KE, Shatnawi NJ. Meckel’s diverticulum: comparison of incidental and symptomatic cases. World J Surg. 2004Sep;28(9):917-20. [CrossRef] [PubMed]
- Chiu EJ, Shyr YM, Su CH, Wu CW, Lui WY. Diverticular disease of the small bowel. Hepatogastroenterology. 2000 Jan-Feb;47(31):181-4. [PubMed]
- Zulfikaroglu B, Ozalp N, Zulfikaroglu E, Ozmen MM, Tez M, Koc M. Is incidental Meckel’s diverticulum resected safely? N Z Med J. 2008 Sep 22;121(1282):39-44. [PubMed]
- Thirunavukarasu P, Sathaiah M, Sukumar S, Bartels CJ, Zeh H 3rd, Lee KK, Bartlett DL. Meckel’s diverticulum--a high-risk region for malignancy in the ileum. Insights from a population-based epidemiological study and implications in surgical management. Ann Surg. 2011 Feb;253(2):223-30. [CrossRef] [PubMed] [PubMed Central]
- Caracappa D, Gullà N, Lombardo F, Burini G, Castellani E, Boselli C, Gemini A, Burattini MF, Covarelli P, Noya G. Incidental finding of carcinoid tumor on Meckel’s diverticulum: case report and literature review, should prophylactic resection be recommended? World J Surg Oncol. 2014 May 8;12:144. [CrossRef] [PubMed] [PubMed Central]
- Kilius, A., Samalavicius, N.E., Danys, D. et al. Asymptomatic heterotopic pancreas in Meckel’s diverticulum: a case report and review of the literature. J Med Case Reports 9, 108 (2015). [CrossRef]
- Jadlowiec CC, Bayron J, Marshall WT 3rd. Is an Incidental Meckel’s Diverticulum Truly Benign? Case Rep Surg. 2015;2015:679097. Epub 2015 Feb 9. [CrossRef] [PubMed] [PubMed Central]
- Gezer HÖ, Temiz A, İnce E, Ezer SS, Hasbay B, Hiçsönmez A. Meckel diverticulum in children: Evaluation of macroscopic appearance for guidance in subsequent surgery. J Pediatr Surg. 2016 Jul;51(7):1177-80. Epub 2015 Sep 15. [CrossRef] [PubMed]
- Mora-Guzmán I, Muñoz de Nova JL, Martín-Pérez E. Neuroendocrine tumours within a Meckel’s diverticulum. Ann R Coll Surg Engl. 2018 Jan;100(1):e10-e11. Epub 2017 Oct 19. [CrossRef] [PubMed] [PubMed Central]
- Ismael Mora-Guzmán, José Luis Muñoz de Nova & Elena Martín-Pérez (2018): Meckel’s diverticulum in the adult: surgical treatment, Acta Chirurgica Belgica. [CrossRef]
- Demirel B. D. , Hancıoglu S. , Bicakci U. , Bernay F. , Ariturk E. Complications of Meckel’s diverticulum in children: A 10-years experience. J. Exp. Clin. Med.. 2020; 36(3): 67-71.
- Stone PA, Hofeldt MJ, Campbell JE, Vedula G, DeLuca JA, Flaherty SK. Meckel diverticulum: ten-year experience in adults. South Med J. 2004 Nov;97(11):1038-41. [CrossRef] [PubMed]
- Mackey WC, Dineen P. A fifty year experience with Meckel’s diverticulum. Surg Gynecol Obstet. 1983 Jan;156(1):56-64. [PubMed]
- Ueberrueck T, Meyer L, Koch A, Hinkel M, Kube R, Gastinger I. The significance of Meckel’s diverticulum in appendicitis--a retrospective analysis of 233 cases. World J Surg. 2005 Apr;29(4):455-8. [CrossRef] [PubMed]
- Robijn J, Sebrechts E, Miserez M. Management of incidentally found Meckel’s diverticulum a new approach: resection based on a Risk Score. Acta Chir Belg. 2006 Jul-Aug;106(4):467-70. [CrossRef] [PubMed]
- Vane DW, West KW, Grosfeld JL. Vitelline duct anomalies. Experience with 217 childhood cases. Arch Surg. 1987 May;122(5):542-7. [CrossRef] [PubMed]
- St-Vil D, Brandt ML, Panic S, Bensoussan AL, Blanchard H. Meckel’s diverticulum in children: a 20-year review. J Pediatr Surg. 1991 Nov;26(11):1289-92. [CrossRef] [PubMed]
- Onen A, Ciğdem MK, Oztürk H, Otçu S, Dokucu AI. When to resect and when not to resect an asymptomatic Meckel’s diverticulum: an ongoing challenge. Pediatr Surg Int. 2003 Apr;19(1-2):57-61. Epub 2003 Jan 17. [CrossRef] [PubMed]
- Groebli Y, Bertin D, Morel P. Meckel’s diverticulum in adults: retrospective analysis of 119 cases and historical review. Eur J Surg. 2001 Jul;167(7):518-24. [CrossRef] [PubMed]
- Dumper J., Mackenzie S., Mitchell P., Sutherland F., Quan M.L., Mew D. Complications of Meckel’s diverticula in adults. Can. J. Surg. 2006;49:353–357.
- McKay R. High incidence of symptomatic Meckel’s diverticulum in patients less than fifty years of age: an indication for resection. Am Surg. 2007 Mar;73(3):271-5. Erratum in: Am Surg. 2007 Dec;73(12):1293. [PubMed]
- Blouhos K, Boulas KA, Tsalis K, et al. Meckel’s diverticulum in adults: surgical concerns [J]. Front Surg 2018; 5: 55.
- Chen Y, Liu Y, Jiang L, Jiang F, Zhu T. Axially torsional b Meckel’s diverticulum accompanied by small bowel volvulus: a case report. J Int Med Res. 2021 Oct;49(10):3000605211053554. [CrossRef] [PubMed] [PubMed Central]
Figure 1.
CT scan: MD (arrow) and suturing clips of previous appendectomy (circle).
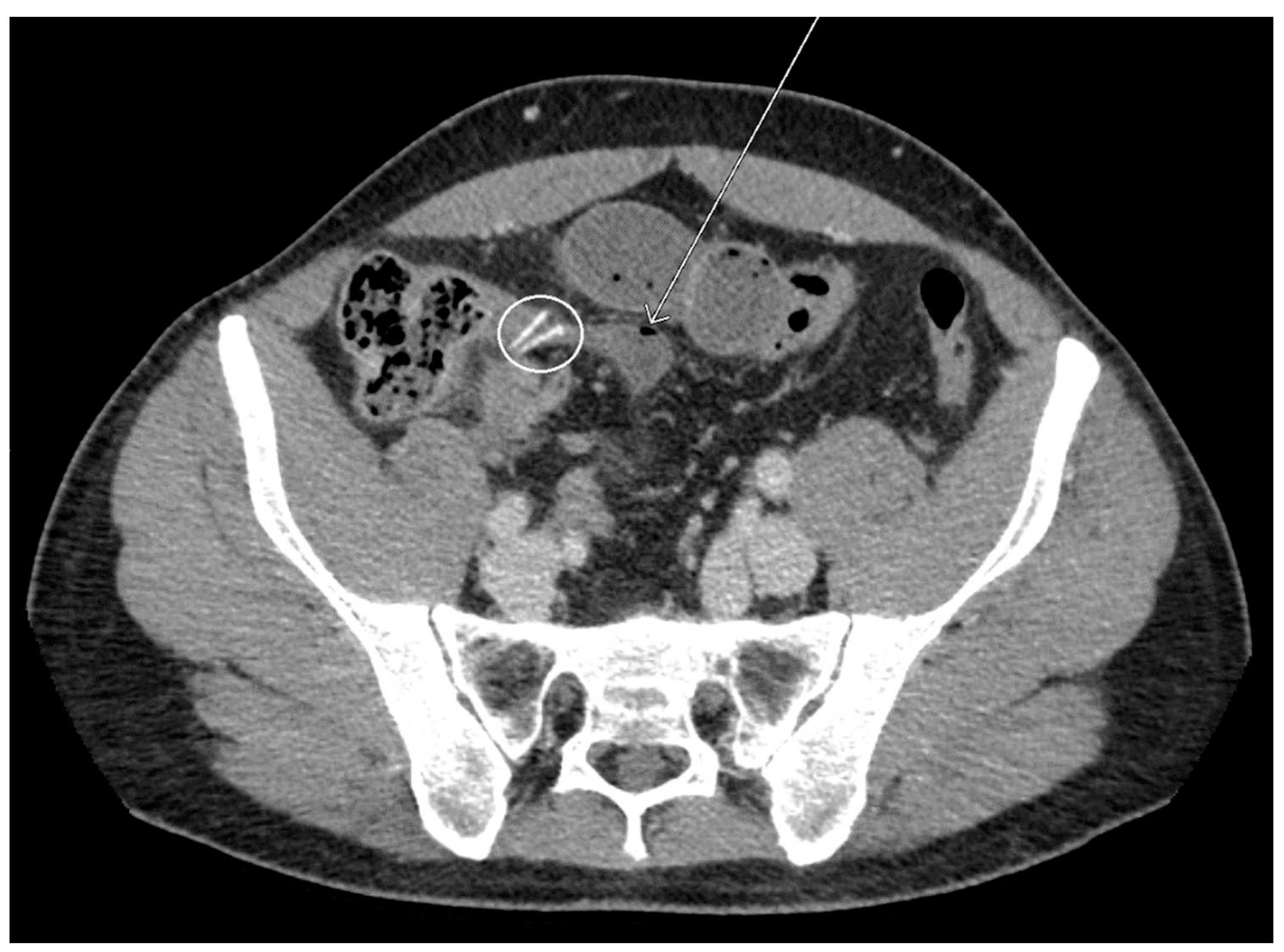
Figure 2.
CT scan: Pedunculated base of the MD (arrow) and MD (star).
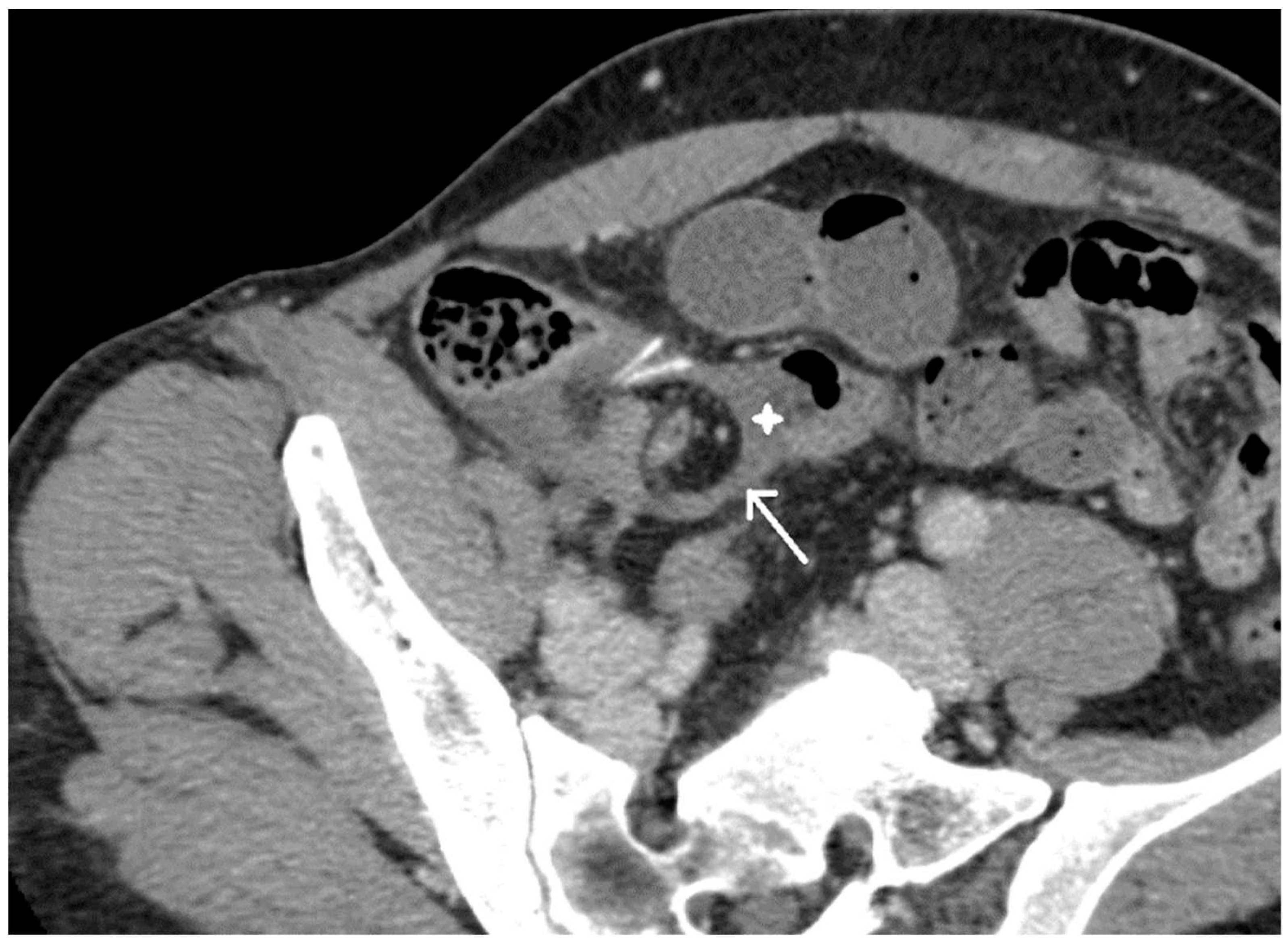
Figure 3.
CT scan: pre-op coronal view, congested mesentery (circle).

Figure 4.
Intraoperative image: ileal volvulus and clips of previous laparoscopic appendectomy.
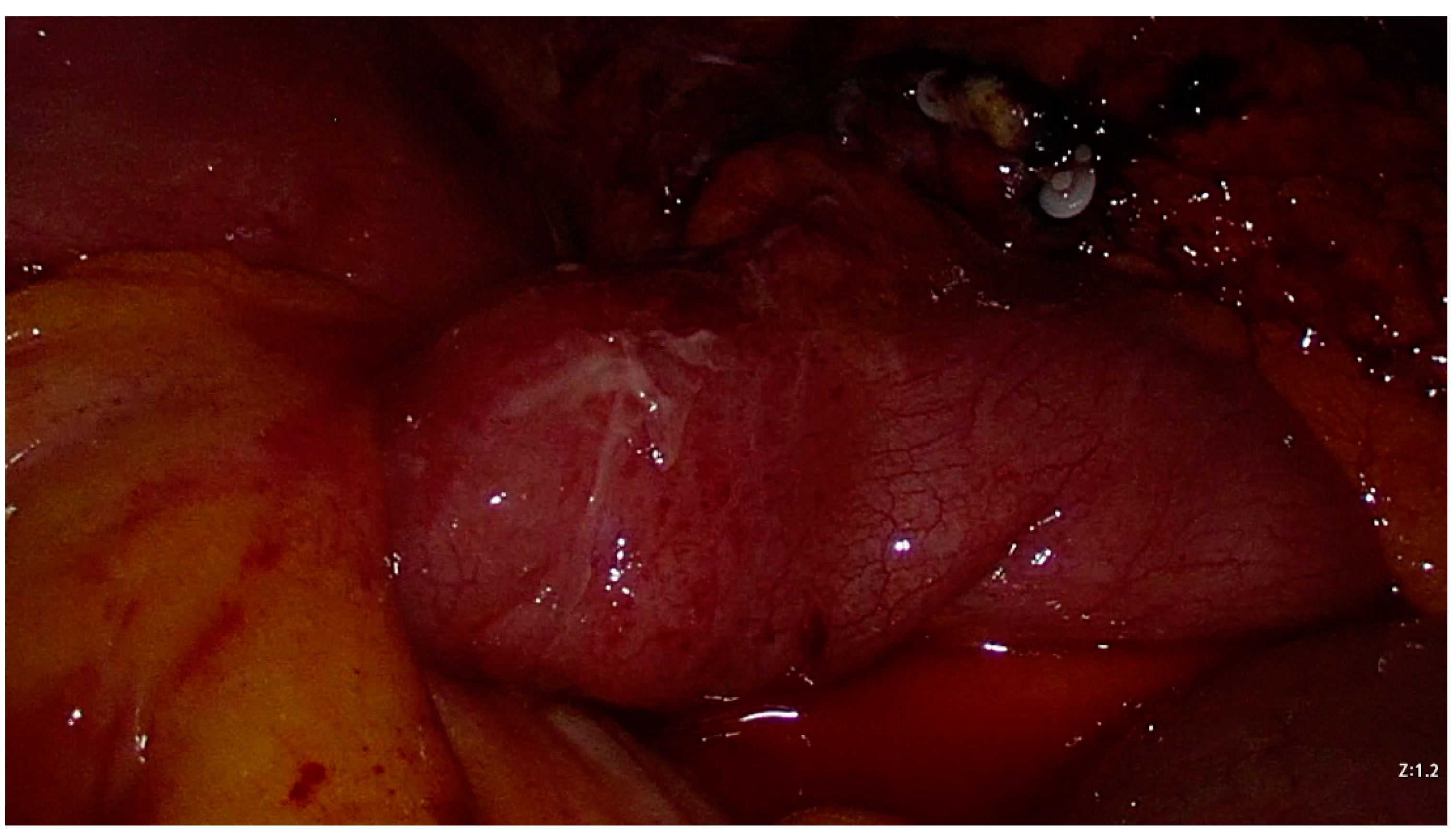
Figure 5.
Intraoperative image: mechanical stapler on MD base (necrotic mass).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



