
Submitted:
18 September 2023
Posted:
19 September 2023
You are already at the latest version
Abstract
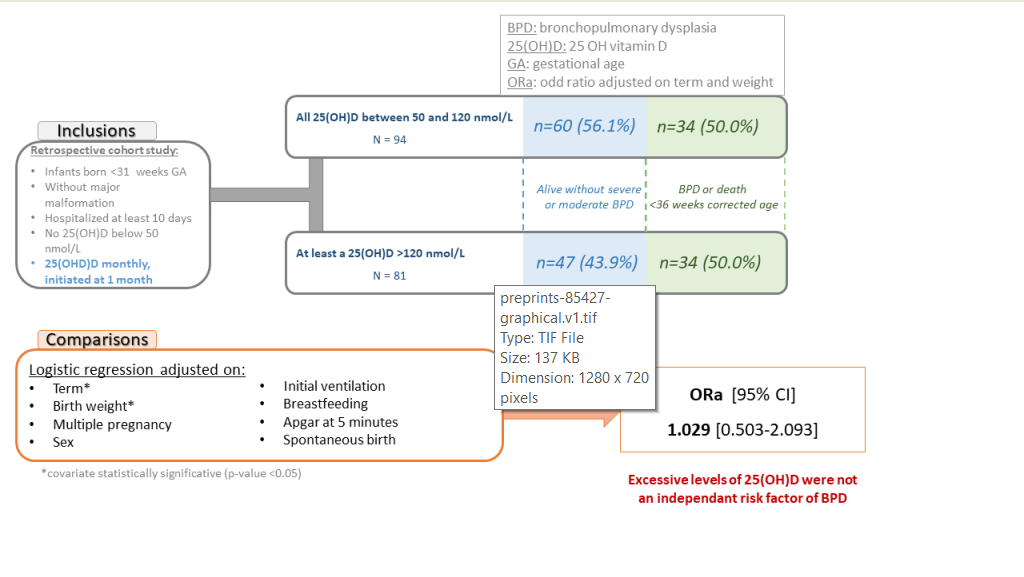
Low 25 OH vitamin D (25(OH)D) in preterm infants is a risk factor of bronchopulmonary dysplasia (BPD), but increased supplementation failed to demonstrate beneficial effect on BPD. In neonatal animal models, deficiency and excessive vitamin D exposure have been associated with increased mortality and lung histological alterations evocative of BPD. Our hypothesis is that 25(OH)D levels ≥ 120nmol/L is also a risk factor for BPD or death. This retrospective single-center cohort study included all infants born <31 weeks gestational age without major malformation with at least a determination of 25(OH)D <36 weeks corrected age and no determination <50 nmol/L. Routine 25(OH)D determination was performed at 1 month and monthly thereafter. A total of 175 infants were included. Infants with BPD or who died had a significantly lower term and weight, but a similar frequency of 25(OH)D ≥120nmol/L (50.5% vs 43.9%, p=0.53). The logistic regression identified weight (OR 0.997, 95%CI [0.995-0.998]) and term (OR 0.737, 95%CI [0.551-0.975]) as significantly associated with BPD or death; the occurrence of excessive 25(OH)D was not significantly associated (OR 1.029, 95%CI [0.503-2.093]). The present study did not demonstrate any significant association between excessive 25(OH)D after one month of age and BPD or death.
Keywords:
vitamin D
; premature infants
; bronchopulmonary dysplasia
; low birth weight infant
; very low birth weight infant
1. Introduction
Bronchopulmonary dysplasia (BPD) is a frequent and sometimes severe complication of premature infants with long-term consequences [1]. Vitamin D is implicated in lung development as demonstrated by multiple animal studies in rodents [2]. Low concentrations of 25 OH vitamin D (25(OH)D) at birth and at one month of age have been associated with increased risk of BPD [3,4,5]. However, studies investigating high-dose supplementation (compared to low-dose) failed to demonstrate any significant effect on the frequency of BPD [6,7] but have found high 25(OH)D concentrations in the groups exposed to high intake [7,8,9]. The data on the consequence of vitamin D excess in this population (except for the risk of nephrocalcinosis and/or hypercalcemia) are sparse [10]. In rodents receiving vitamin D in excess during gestation and lactation, pups had an abnormal lung histology; there was an greater mean linear intercept, greater total respiratory system resistance, as well as a lower basal proliferation of their lung mesenchymal stem cells with a lower adipogenic and an greater myogenic potential [11,12]. Furthermore, in a model of bronchopulmonary dysplasia, neonatal pups exposed to oxygen receiving high doses of 1,25 OH vitamin D from the first day of life exhibited a higher mortality and an altered lung histology (increased mean linear intercept, a decreased angiogenesis, and increased proinflammatory factors) when compared to animals receiving low doses [13]. Recent studies have demonstrated a high frequency of excessive level of 25(OH)D in preterm infants with supplementation recommended at that time [14,15,16]. Our hypothesis was that these excessive 25(OH)D levels in very and extremely preterm infants may be deleterious to pulmonary development and may therefore be implicated in the pathogenesis of BPD. The primary objective of this study was therefore to determine whether excessive 25(OH)D levels are an independent risk factor of BPD or death.
2. Materials and Methods
In this retrospective cohort study all infants born <31 weeks gestational age between January 2018 and December 2019 were eligible for inclusion if they were hospitalized before 3 days of life and for at least 10 days in neonatal intensive care unit (NICU) from Hospital Femme Mere Enfant, Bron, France, and presented no major congenital malformation. They were included if they had at least a 25(OH) D determination <36 weeks corrected age. They were excluded if they had presented at least a 25(OH) D determination < 50 nmol/L.
In this NICU, preterm infants receiving parenteral nutrition were supplemented with Cernevit (Baxter, Guyancourt, France) ¼ vial daily (containing 55IU cholecalciferol,). When parenteral nutrition was stopped, infants with a weight below 1 kg received Sterogyl (DB pharma, La Varenne-St- Hilaire, France) 3 drops daily (1200IU ergocalciferol) when infants above 1kg received Uvesterol ADEC (Crinex, Montrouge, France) 0.3 mL daily (containing 1000IU ergocalciferol). A routine determination of 25(OH)D was recommended at one month of age and monthly thereafter until discharge with a protocol for adaptation of the dose (Figure 1). The objective was to maintain 25(OH)D ≥ 50 and <120 nmol/L.
The main outcome was BPD or death at 36 weeks corrected age. BPD was defined as the need of supplemental oxygen or respiratory support to maintain a saturation equal to or above 90% at 36 weeks corrected age. In the description of the population it was classified into three grades according to Jobe et al. [17].
The main early predictive factors of BPD reported in recent studies were collected [18,19,20,21]: multiple gestation, antenatal corticosteroids, spontaneous delivery, gestational age at birth, birthweight, Apgar at 5 minutes (in categories: 8 to 10, 4 to 7, 0 to 3), sex, respiratory support during the first 24 hours (classified in 3 groups: mild FiO2<30% and non-invasive ventilation, moderate FiO2<30% and mechanical ventilation, severe FiO2≥30% and mechanical ventilation), and breastfeeding defined as receiving any mother milk. The ethnic origin was not available; however, Baud et al. excluded it from their final predictive model in a French population [18].
Small for gestational age was defined as a weight below the tenth percentile according to the Fenton curves [22]. Enterocolitis was considered as present if a grade 2 or above was observed.
Data were extracted from electronic medical charts (IntelliSpace Critical Care and Anesthesia prescription software, Philips, Suresne, France) and completed with the discharge letter when infants had been transferred to another hospital or another unit.
The number of subjects was calculated based on the unpublished results of a pilot study[23]. Based on the results of the multiple logistic regression simulation taking into account confounding parameters (term, spontaneous birth, and sex) and excessive 25(OH)D concentration, the number of infants necessary was 176 to find an OR of 2.8 for BPD and 25(OH)D concentration association, with power of 80% and alpha risk of 0.05.
The quantitative variables were described by the mean and standard deviation (SD), and qualitative variables by the number of patients and frequency (%) of each modality.
Patients were stratified according to the maximal 25(OH)D concentration between 1 month of life and 36 weeks corrected age (excessive any determination ≥ 120nmol/L] [24] or normal [all determinations ≥50 to <120nom/L]). Patients with BPD or who died at 36 weeks corrected age were compared to other patients using the Wilcoxon or Chi2 test, as appropriate. The analysis of the association between BPD and excessive 25(OH)D concentration was investigated using a logistic regression model constructed using backward stepwise selection.
25(OH)D concentration was measured using a Chemiluminescent Microparticle Immuno Assay on an Isys analyser (Immunodiagnostic Systems, Pouilly-en-Auxois, France).
The study was approved by the institutional review board (Comité Scientifique et Éthique) of the Hospices Civils de Lyon on January 18, 2023 (number 23_076). It also received the approval of the national data protection commission (Commission Nationale de l'Informatique et des Libertés; number 23_5076). According to French law parental informed consent was not necessary, but all parents were informed and could refuse the participation of their infant.
The study is registered in ClinicalTrials.gov (NCT05944055).
3. Results
3.1. Population
3.1.1. Study flow-chart
The study flow chart is presented on Figure 2.
3.1.2. Description of the population
The obstetrical characteristics of the included population and according to 25(OH)D concentration are described in Table 1 (Table 1).
The main neonatal characteristics of the included population and according to 25(OH)D concentration are presented in Table 2.
3.2. Outcomes
The main outcomes of the cohort according to 25(OH)D concentration are presented in Table 3.
3.3. Analysis
Univariate analysis found that term (BPD or death: median 26.50, interquartile range (25.57-27.79) versus no BPD or death: median 28.29 interquartile range (27.36-29.43), p<0.001), and weight (BPD or death: median 775g, interquartile range (635-892) versus no BPD or death: median 1050g, interquartile range (900-1232), p<0.001) were significantly different between infants with BPD or death and those without. The occurrence of 25(OH)D ≥ 120 nmol/l (50.0% vs 43.9%, Chi2, p=0.53) was not significantly different between the two groups (with BPD or death and without). Multiple pregnancy, Apgar score, sex, any mother milk given, spontaneous birth, and maximum ventilation during the first 24 hours of life were not significantly different between groups.
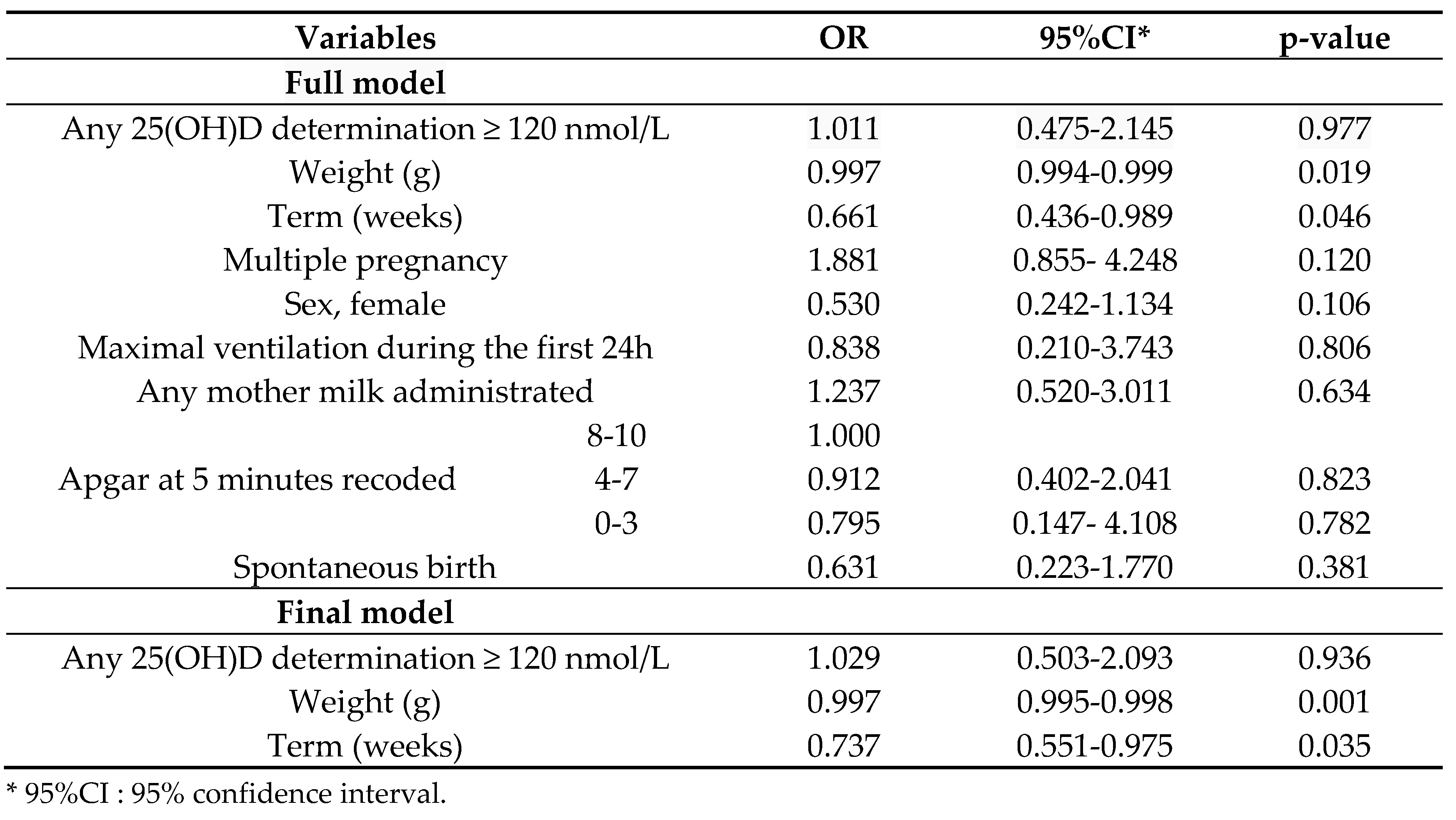
The results of the multivariable analysis are presented in Table 4. In the final model term (OR 0.737, 95%CI [0.551-0.975], p=0.035) and weight (OR 0.997, 95%CI [0.995-0.998], p=0.001) were significantly associated with BPD or death; there was no significant association with any 25(OH)D determination ≥ 120 nmol/L (OR 1.029, 95%CI [0.503-2.093], p=0.936).
A post hoc analysis was performed to evaluate whether the occurrence of a 25(OH)D above 150 nmol/L was associated with the occurrence of BPD or death. Again, only term (OR 0.736, 95%CI [0.551-0.971], p=0.033) and weight (OR 0.997, 95%CI [0.995-0.999], p=0.001) were significantly associated; there was no significant effect of 25(OH)D >150 nmol/L (OR 1.291, 95%CI [0.558-2.982], p=0.548).
4. Discussion
Unlike the results obtained in an animal model [11,12,13], the present study did not find that excessive 25(OH)D concentration was risk factor for BPD or death. This result may be related to the temporality of the excessive concentration, as in animal studies native vitamin D was administrated throughout the gestation [11,12] or 1,25(OH)2D immediately at birth [13]. With such early administration the lungs are more immature and their development may be severely impaired. We chose to study 25(OH)D at the first month because the frequency of excessive concentrations at birth in preterm infants is very low [25,26,27]. In France, Courbebaisse et al. reported that in the general population of newborns 93% of cord blood concentrations were below 75 nmol/L [28], and Papalia et al. reported that in infants born below 29 weeks gestational age 74% had a cord blood concentration ≤ 75 nmol/L [29]. In France, the current recommendation for vitamin D supplementation during pregnancy is to administer 100 000IU once during the 7th month of pregnancy. This recommendation was followed in 88% of the pregnant patients in a recent large cohort study [28] and may explain these results. Furthermore, the vitamin D intakes during parenteral nutrition was low herein (55IU daily), and the median duration of parenteral nutrition was 14 days. Taking into account these aspects and the results of the study reported by Fort et al. (who described the increase of 25(OH)D in preterm receiving 200, 400 and 1000IU daily) [8], we estimated that the risk of early excessive concentration was low in the study population.
The upper limit of normal 25(OH)D was established in accordance with the current recommendation of the European Society for Paediatric Nephrology for infants with chronic kidneys disease [24,30] and recent French and European recommendations for preterm infants [31,32]. It was justified by an increase in mortality with higher concentrations in the general population [33,34]. This threshold is reinforced by the results of a case series study that identified 16 preterm infants referred to nephrology clinics for symptomatic hypervitaminosis D with 25(OH)D concentrations between 119–350 nmol/L [10]. In two previous studies, higher concentrations have been associated with a high frequency of hypercalciuria [14,15]. However, it remains possible that the effect of excessive 25(OH)D concentration on lung development necessitates concentrations above 120 nmol/L, although the results of the post hoc analysis with concentrations above 150 nmol/L do not support this hypothesis.
The main limitation of this study is the absence of determination of 25(OH)D at birth, some infants from both groups may have experienced an early deficiency in 25(OH)D which is a recognized risk factor of BPD [3,4] and they may not be equally distributed between groups, decreasing the difference between groups for the primary outcome. Despite this limitation this result is important because it shows that in the absence of an early determination of 25(OHD), a 25(OH)D concentration above 120 nmol/L before 36 weeks corrected age is not a significant risk factor of BPD or death. In addition, there does not seem to be a great difference in terms of morbidity according to 25(OH)D concentration herein, although this was not formally tested to avoid multiplicity of comparisons.
Further studies are necessary to determine the appropriate modalities of administration of native vitamin D in extremely and very preterm infants as it is a modifiable factor that could impact the risk of BPD [3,4] and the risk of sepsis [35,36,37,38], two essential factors for the future of premature infants, but also nephrological and bone-related outcomes.
Author Contributions
Conceptualization, S. Laborie and J. Bacchetta; methodology, M Bonjour and S Laborie; validation, S. Laborie, M. Butin; formal analysis, M Bonjour; investigation, M. Mauras and S. Laborie; data curation, M. Mauras and S Laborie.; writing—original draft preparation, S .Laborie; writing—review and editing, S Laborie, M Bonjour, M Mauras, J Bacchetta and M Butin; visualization, S Laborie and M Bonjour.; supervision, M. Butin, J. Bacchetta; project administration, M. Butin. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Hospices civils de Lyon (protocol code 23_076 and date of approval: 01/18/2023).
Informed Consent Statement
Parent consent was waived due to the French law regarding retrospective studies. However, according to the law, the parents were informed by a letter or an email and could refuse to participate in the study, which was taken into account.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
We acknowledge Dr Frank Plaisant for his help to extract the data from the electronic medical charts.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Cheong, J.L.Y.; Doyle, L.W. An Update on Pulmonary and Neurodevelopmental Outcomes of Bronchopulmonary Dysplasia. Semin. Perinatol. 2018, 42, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Lykkedegn, S.; Sorensen, G.L.; Beck-Nielsen, S.S.; Christesen, H.T. The Impact of Vitamin D on Fetal and Neonatal Lung Maturation. A Systematic Review. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2015, 308, L587–L602. [Google Scholar] [CrossRef]
- Yu, H.; Fu, J.; Feng, Y. Utility of Umbilical Cord Blood 25-Hydroxyvitamin D Levels for Predicting Bronchopulmonary Dysplasia in Preterm Infants with Very Low and Extremely Low Birth Weight. Front. Pediatr. 2022, 10, 956952. [Google Scholar] [CrossRef]
- Park, H.W.; Lim, G.; Park, Y.-M.; Chang, M.; Son, J.S.; Lee, R. Association between Vitamin D Level and Bronchopulmonary Dysplasia: A Systematic Review and Meta-Analysis. PLOS ONE 2020, 15, e0235332. [Google Scholar] [CrossRef]
- Byun, S.Y.; Bae, M.H.; Lee, N.R.; Han, Y.M.; Park, K.H. Association between Vitamin D Deficiency at One Month of Age and Bronchopulmonary Dysplasia. Medicine (Baltimore) 2021, 100, e27966. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, Z.; Yan, G.; Jie, Q.; Rui, C. Effect of Different Doses of Vitamin D Supplementation on Preterm Infants – an Updated Meta-Analysis. J. Matern. Fetal Neonatal Med. 2018, 31, 3065–3074. [Google Scholar] [CrossRef]
- Aristizabal, N.; Holder, M.P.; Durham, L.; Ashraf, A.P.; Taylor, S.; Salas, A.A. Safety and Efficacy of Early Vitamin D Supplementation in Critically Ill Extremely Preterm Infants: An Ancillary Study of a Randomized Trial. J. Acad. Nutr. Diet. 2023, 123, 87–94. [Google Scholar] [CrossRef]
- Fort, P.; Salas, A.A.; Nicola, T.; Craig, C.M.; Carlo, W.A.; Ambalavanan, N. A Comparison of 3 Vitamin D Dosing Regimens in Extremely Preterm Infants: A Randomized Controlled Trial. J. Pediatr. 2016, 174, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, C.K.; Sankar, M.J.; Agarwal, R.; Pratap, O.T.; Jain, V.; Gupta, N.; Gupta, A.K.; Deorari, A.K.; Paul, V.K.; Sreenivas, V. Trial of Daily Vitamin D Supplementation in Preterm Infants. Pediatrics 2014, 133, e628–e634. [Google Scholar] [CrossRef] [PubMed]
- Vierge, M.; Laborie, S.; Bertholet-Thomas, A.; Carlier, M.-C.; Picaud, J.-C.; Claris, O.; Bacchetta, J. Intoxication néonatale à la vitamine D chez des anciens prématurés : une série de 16 cas. Arch. Pédiatrie 2017, 24, 817–824. [Google Scholar] [CrossRef]
- Sakurai, R.; Singh, H.; Wang, Y.; Harb, A.; Gornes, C.; Liu, J.; Rehan, V.K. Effect of Perinatal Vitamin D Deficiency on Lung Mesenchymal Stem Cell Differentiation and Injury Repair Potential. Am. J. Respir. Cell Mol. Biol. 2021, 65, 521–531. [Google Scholar] [CrossRef]
- Yurt, M.; Liu, J.; Sakurai, R.; Gong, M.; Husain, S.M.; Siddiqui, M.A.; Husain, M.; Villarreal, P.; Akcay, F.; Torday, J.S.; et al. Vitamin D Supplementation Blocks Pulmonary Structural and Functional Changes in a Rat Model of Perinatal Vitamin D Deficiency. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2014, 307, L859–L867. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Weng, H.; Zhang, X.; Wang, S.; Lu, C.; Jin, H.; Chen, S.; Liu, Y.; Sheng, A.; Sun, Y. Low-Dose Vitamin D Protects Hyperoxia-Induced Bronchopulmonary Dysplasia by Inhibiting Neutrophil Extracellular Traps. Front. Pediatr. 2020, 8, 335. [Google Scholar] [CrossRef] [PubMed]
- Laborie, S.; Denis, A.; Raverot, V.; Claris, O.; Bacchetta, J.; Butin, M. A Third of Premature Neonates Displayed Inadequate 25-hydroxyvitamin D Levels before Being Discharged from a French Neonatal Intensive Care Unit. Acta Paediatr. 2022, 111, 104–106. [Google Scholar] [CrossRef] [PubMed]
- Mathilde, M.; Butin, M.; Pascal, R.; Plaisant, F.; Laborie, S.; Bacchetta, J. Local Protocol Helped to Deliver Vitamin D Levels More Accurately in Preterm Infants. Acta Paediatr. 2022, 111, 76–85. [Google Scholar] [CrossRef]
- Kołodziejczyk-Nowotarska, A.; Bokiniec, R.; Seliga-Siwecka, J. Monitored Supplementation of Vitamin D in Preterm Infants: A Randomized Controlled Trial. Nutrients 2021, 13, 3442. [Google Scholar] [CrossRef] [PubMed]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary Dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef]
- Baud, O.; Laughon, M.; Lehert, P. Survival without Bronchopulmonary Dysplasia of Extremely Preterm Infants: A Predictive Model at Birth. Neonatology 2021, 118, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Laughon, M.M.; Langer, J.C.; Bose, C.L.; Smith, P.B.; Ambalavanan, N.; Kennedy, K.A.; Stoll, B.J.; Buchter, S.; Laptook, A.R.; Ehrenkranz, R.A.; et al. Prediction of Bronchopulmonary Dysplasia by Postnatal Age in Extremely Premature Infants. Am. J. Respir. Crit. Care Med. 2011, 183, 1715–1722. [Google Scholar] [CrossRef]
- Lapcharoensap, W.; Gage, S.C.; Kan, P.; Profit, J.; Shaw, G.M.; Gould, J.B.; Stevenson, D.K.; O’Brodovich, H.; Lee, H.C. Hospital Variation and Risk Factors for Bronchopulmonary Dysplasia in a Population-Based Cohort. JAMA Pediatr. 2015, 169, e143676. [Google Scholar] [CrossRef]
- Spiegler, J.; Preuß, M.; Gebauer, C.; Bendiks, M.; Herting, E.; Göpel, W.; Bendiks, M.; Berghäuser, M.A.; Böckenholt, K.; Bohnhorst, B.; et al. Does Breastmilk Influence the Development of Bronchopulmonary Dysplasia? J. Pediatr. 2016, 169, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Fenton, T.R.; Kim, J.H. A Systematic Review and Meta-Analysis to Revise the Fenton Growth Chart for Preterm Infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef] [PubMed]
- Laborie, S. Les Surdosages En 25 OHD Pendant Les Premiers Mois de Vie Sont-Ils Un Facteur de Risque de Dysplasie Bronchopulmonaire ? Presented at the JFRN 2022, France, 2022. [Google Scholar]
- Shroff, R.; Wan, M.; Nagler, E.V.; Bakkaloğlu, S.; Fischer, D.-C.; Bishop, N.; Cozzolino, M.; Bacchetta, J.; Edefonti, A.; Stefanidis, C.J.; et al. Clinical Practice Recommendations for Native Vitamin D Therapy in Children with Chronic Kidney Disease Stages 2–5 and on Dialysis. Nephrol. Dial. Transplant. 2017, 32, 1098–1113. [Google Scholar] [CrossRef] [PubMed]
- Burris, H.H.; Van Marter, L.J.; McElrath, T.F.; Tabatabai, P.; Litonjua, A.A.; Weiss, S.T.; Christou, H. Vitamin D Status among Preterm and Full-Term Infants at Birth. Pediatr. Res. 2014, 75, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Kassai, M.S.; Cafeo, F.R.; Affonso-Kaufman, F.A.; Suano-Souza, F.I.; Sarni, R.O.S. Vitamin D Plasma Concentrations in Pregnant Women and Their Preterm Newborns. BMC Pregnancy Childbirth 2018, 18. [Google Scholar] [CrossRef]
- Onwuneme, C.; Martin, F.; McCarthy, R.; Carroll, A.; Segurado, R.; Murphy, J.; Twomey, A.; Murphy, N.; Kilbane, M.; McKenna, M.; et al. The Association of Vitamin D Status with Acute Respiratory Morbidity in Preterm Infants. J. Pediatr. 2015, 166, 1175–1180. [Google Scholar] [CrossRef] [PubMed]
- Courbebaisse, M.; Souberbielle, J.-C.; Baptiste, A.; Taieb, J.; Tsatsaris, V.; Guibourdenche, J.; Senat, M.-V.; Haidar, H.; Jani, J.; Guizani, M.; et al. Vitamin D Status during Pregnancy and in Cord Blood in a Large Prospective French Cohort. Clin. Nutr. 2019, 38, 2136–2144. [Google Scholar] [CrossRef]
- Papalia, H.; Samonini, A.; Buffat, C.; Gras, E.; des Robert, C.; Landrier, J.-F.; Pauly, V.; Boubred, F. Low Vitamin D Levels at Birth and Early Respiratory Outcome in Infants With Gestational Age Less Than 29 Weeks. Front. Pediatr. 2022, 9, 790839. [Google Scholar] [CrossRef]
- Bacchetta, J.; Schmitt, C.P.; Bakkaloglu, S.A.; Cleghorn, S.; Leifheit-Nestler, M.; Prytula, A.; Ranchin, B.; Schön, A.; Stabouli, S.; Van de Walle, J.; et al. Diagnosis and Management of Mineral and Bone Disorders in Infants with CKD: Clinical Practice Points from the ESPN CKD-MBD and Dialysis Working Groups and the Pediatric Renal Nutrition Taskforce. Pediatr. Nephrol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Bacchetta, J.; Edouard, T.; Laverny, G.; Bernardor, J.; Bertholet-Thomas, A.; Castanet, M.; Garnier, C.; Gennero, I.; Harambat, J.; Lapillonne, A.; et al. Vitamin D and Calcium Intakes in General Pediatric Populations: A French Expert Consensus Paper. Arch. Pédiatrie 2022, 29, 312–325. [Google Scholar] [CrossRef] [PubMed]
- Embleton, N.D.; Moltu, S.J.; Lapillonne, A.; van den Akker, C.H.P.; Carnielli, V.; Fusch, C.; Gerasimidis, K.; van Goudoever, J.B.; Haiden, N.; Iacobelli, S.; et al. Enteral Nutrition in Preterm Infants (2022): A Position Paper from the ESPGHAN Committee on Nutrition and Invited Experts. J. Pediatr. Gastroenterol. Nutr. 2022, Publish Ahead of Print. [CrossRef]
- Durup, D.; Jørgensen, H.L.; Christensen, J.; Schwarz, P.; Heegaard, A.M.; Lind, B. A Reverse J-Shaped Association of All-Cause Mortality with Serum 25-Hydroxyvitamin D in General Practice: The CopD Study. J. Clin. Endocrinol. Metab. 2012, 97, 2644–2652. [Google Scholar] [CrossRef] [PubMed]
- Sempos, C.T.; Durazo-Arvizu, R.A.; Dawson-Hughes, B.; Yetley, E.A.; Looker, A.C.; Schleicher, R.L.; Cao, G.; Burt, V.; Kramer, H.; Bailey, R.L.; et al. Is There a Reverse J-Shaped Association Between 25-Hydroxyvitamin D and All-Cause Mortality? Results from the U.S. Nationally Representative NHANES. J. Clin. Endocrinol. Metab. 2013, 98, 3001–3009. [Google Scholar] [CrossRef] [PubMed]
- Dhandai, R.; Jajoo, M.; Singh, A.; Mandal, A.; Jain, R. Association of Vitamin D Deficiency with an Increased Risk of Late-Onset Neonatal Xepsis. Paediatr. Int. Child Health 2018, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Cizmeci, M.N.; Kanburoglu, M.K.; Akelma, A.Z.; Ayyildiz, A.; Kutukoglu, I.; Malli, D.D.; Tatli, M.M. Cord-Blood 25-Hydroxyvitamin D Levels and Risk of Early-Onset Neonatal Sepsis: A Case–Control Study from a Tertiary Care Center in Turkey. Eur. J. Pediatr. 2015, 174, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Say, B.; Uras, N.; Sahin, S.; Degirmencioglu, H.; Oguz, S.S.; Canpolat, F.E. Effects of Cord Blood Vitamin D Levels on the Risk of Neonatal Sepsis in Premature Infants. Korean J. Pediatr. 2017, 60, 248. [Google Scholar] [CrossRef] [PubMed]
- Cetinkaya, M.; Cekmez, F.; Buyukkale, G.; Erener-Ercan, T.; Demir, F.; Tunc, T.; Aydın, F.N.; Aydemir, G. Lower Vitamin D Levels Are Associated with Increased Risk of Early-Onset Neonatal Sepsis in Term Infants. J. Perinatol. 2015, 35, 39–45. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Local protocol of adaptation of vitamin in extremely and very preterm infants.
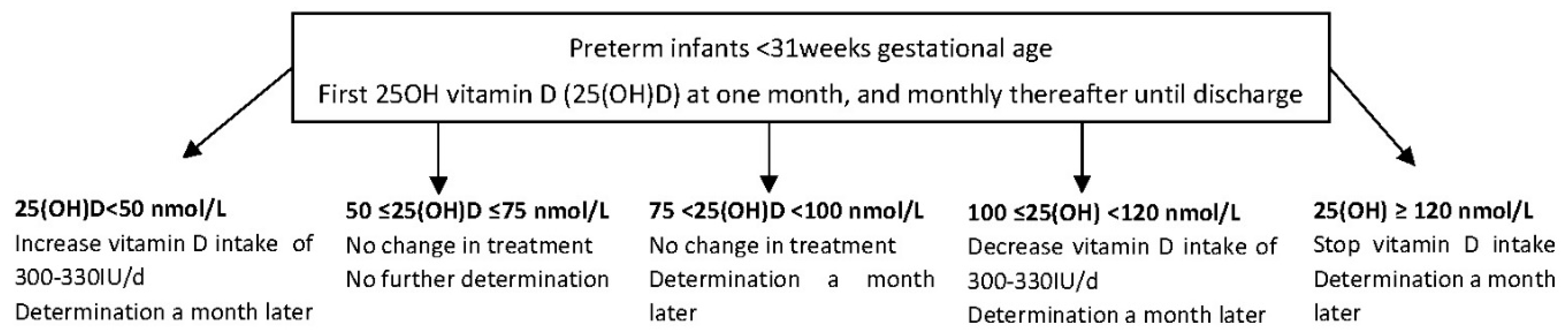
Figure 2.
Study flow-chart.
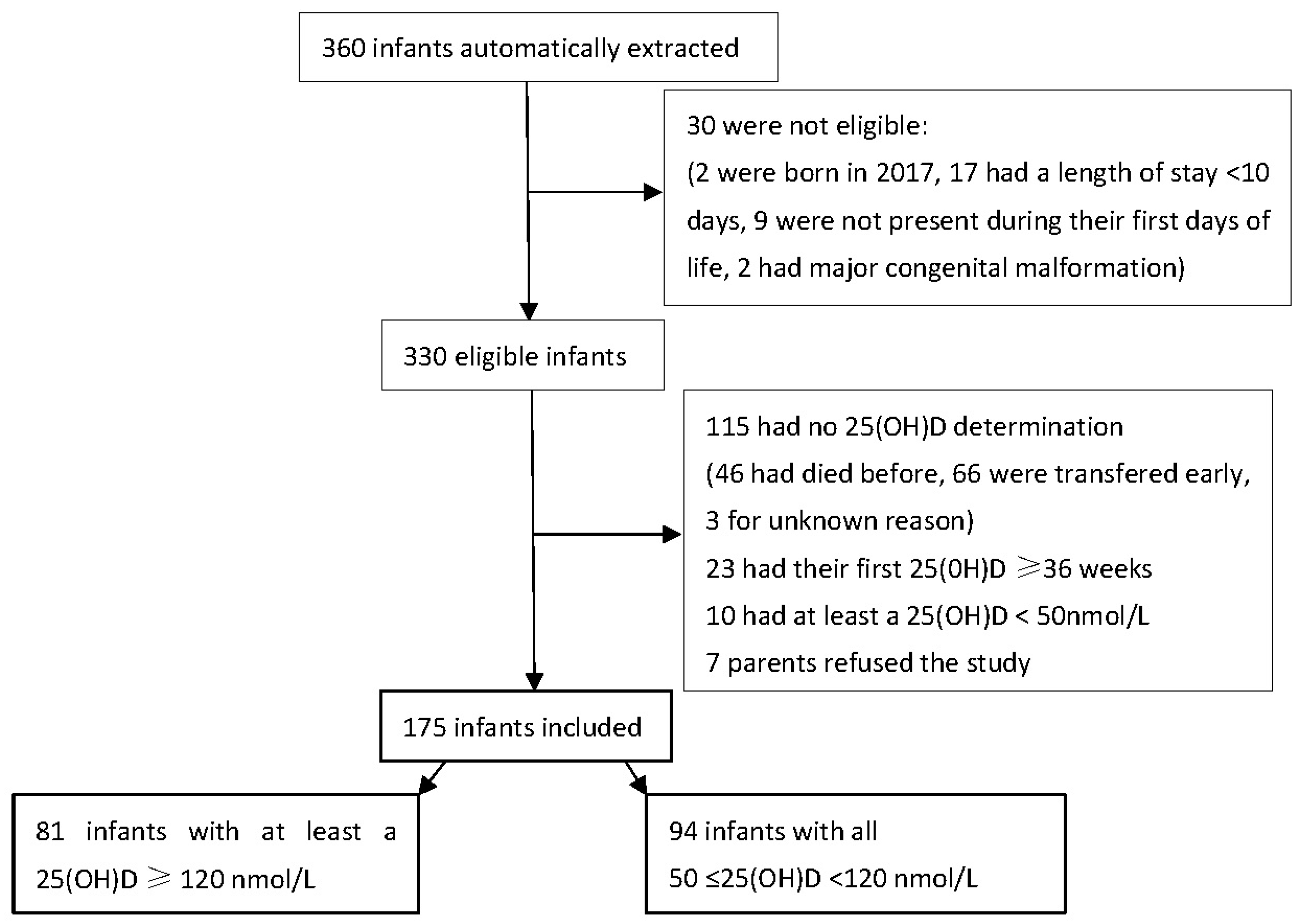

Table 1.
Main obstetrical characteristics of the studied population.
| Pregnancy characteristics* | Excessive 25(OH)D N=81 | Normal 25(OH)D N=94 |
Total N=175 |
||
|---|---|---|---|---|---|
| Parity | 1 | 29 (35.8%) | 40 (42.6%) | 69 (39.4%) | |
| 2 | 25 (30.9%) | 31 (33.0%) | 56 (32.0%) | ||
| 3 | 19 (23.5%) | 14 (14.9%) | 33 (18.9%) | ||
| ≥4 | 8 (9.9%) | 8 (8.5%) | 16 (9.1%) | ||
| Unknown | 0 (0.0%) | 1 (1.1%) | 1 (0.6%) | ||
| Multiple pregnancy | 30 (37.5%) | 25 (26.6%) | 56 (32.0%) | ||
| Any hypertension during pregnancy | 19 (23.5%) | 21 (22.3%) | 40 (22.9%) | ||
| Preterm premature rupture of membranes | 26 (32.1%) | 27 (28.7%) | 53 (30.3%) | ||
| Any diabetes during pregnancy | 8 (9.9%) | 13 (13.8%) | 21 (12.0%) | ||
| Histological chorioamnionitis | 21 (25.9%) | 13 (13.8%) | 34 (19.4%) | ||
| Unavailable | 0 (0%) | 3 (3.2%) | 3 (1.7%) | ||
| Clinical chorioamnionitis | 11 (13.6%) | 7 (7.4%) | 18 (10.3%) | ||
| Unknown | 1/1.2%) | 3 (3.2%) | 4 (2.3%) | ||
| Any antenatal corticosteroids | 76 (93.8%) | 83 (88.3%) | 159 (90.9%) | ||
*Data were available for all infants except if specified.
Table 2.
Main neonatal characteristics of the studied population.
| Neonatal characteristics* | N (%), except if specified | Excessive 25(OH)D N=81 | Normal 25(OH)D N=94 |
Total N=175 |
|---|---|---|---|---|
| Birth Season | Summer | 19 (23.5%) | 32 (34.0%) | 51 (29.1%) |
| Fall | 20 (24.7%) | 26 (27.7%) | 46 (26.3%) | |
| Winter | 21 (25.9%) | 18 (19.1%) | 39 (22.3%) | |
| Spring | 21 (25.9%) | 18 (19.1%) | 39 (22.3%) | |
| Sex | Male | 39 (48.1%) | 51 (54.3%) | 90 (51.4%) |
| Term (weeks) | Mean (SD) | 27.58 (1.84) | 27.88 (1.56) | 27.74 (1.70) |
| Weight (g) | Mean (SD) | 938 ( 272) | 998 ( 305) | 970 (291) |
| Height (cm) | Mean (SD) | 35.05 (3.11) | 35.15 ( 3.98) | 35.11 (3.60) |
| Head circumference (cm) | Mean (SD) | 24.83 ( 2.19) | 25.44 (2.72) | 25.16 (2,50) |
| Small for gestational age* | 14 (17.3%) | 17 (18.1%) | 31 (17.7%) | |
| Apgar at 5 minutes | 8-10 | 55 (67.9%) | 52 (55.3%) | 107 (61.1%) |
| 4-7 | 21 (25.9%) | 37 (39.4%) | 58 (33.1%) | |
| 0-3 | 4 (4.9%) | 4 (4.3%) | 8 (4.6%) | |
| Not available | 1 (1.2%) | 1 (1.1%) | 2 (1.1%) | |
| Maximum ventilation during the first 24h | FiO2<30% and non invasive ventilation | 7 (8.6%) | 6 (6.4%) | 13 (7.4%) |
| Assisted ventilation and FiO2<30% | 0 (0.0%) | 1 (1.1%) | 1 (0.6%) | |
| Assisted ventilation or FiO2≥ 30% | 74 (91.4%) | 87 (92.6%) | 161 (92.0%) | |
| Parenteral nutrition (days) | Median | 14 | 13 | 14 |
| Interquartile range | 7 -23 | 7 -20 | 7 -21 | |
| Enteral feeding | Maternal or donor milk | 17 (21.0%) | 19 (20.2%) | 36 (20.6%) |
| Mixed | 50 (61.7%) | 49 (52.1%) | 99 (56.6%) | |
| Formula or donor milk | 14 (17.3%) | 26 (27.7%) | 40 (22.9%) | |
| Any mother milk given | 66 (81.5%) | 68 (72.3%) | 134 (76.6%) | |
| First determination of 25(OH)D (nmol/L) | Mean (SD) | 139.4 (43.1) | 86.1 (19.6) | 110.8 (42.1) |
| Corrected age at first 25(OH)D determination | Mean (SD) | 32.4 (1.9) | 32.5 (1.5) | 32.4 (1.7) |
| Second determination of 25(OH)D (nmol/L) | 25 (30.9%) | 20 (21.3%) | 45 (25.7%) | |
| Mean (SD) | 144.40 (29.58) | 85.20 (17.76) | 118.1 (38.7) | |
| Corrected age at second determination of 25(OH)D | Mean (SD) | 34.2 (1.2) | 34.2 (1.5) | 34.2 (1.3) |
* Data were available for all infants except if specified ,*Weight below the tenth percentile according to Fenton curves[22], SD: standard deviation.
Table 3.
Main outcomes of the studied population.
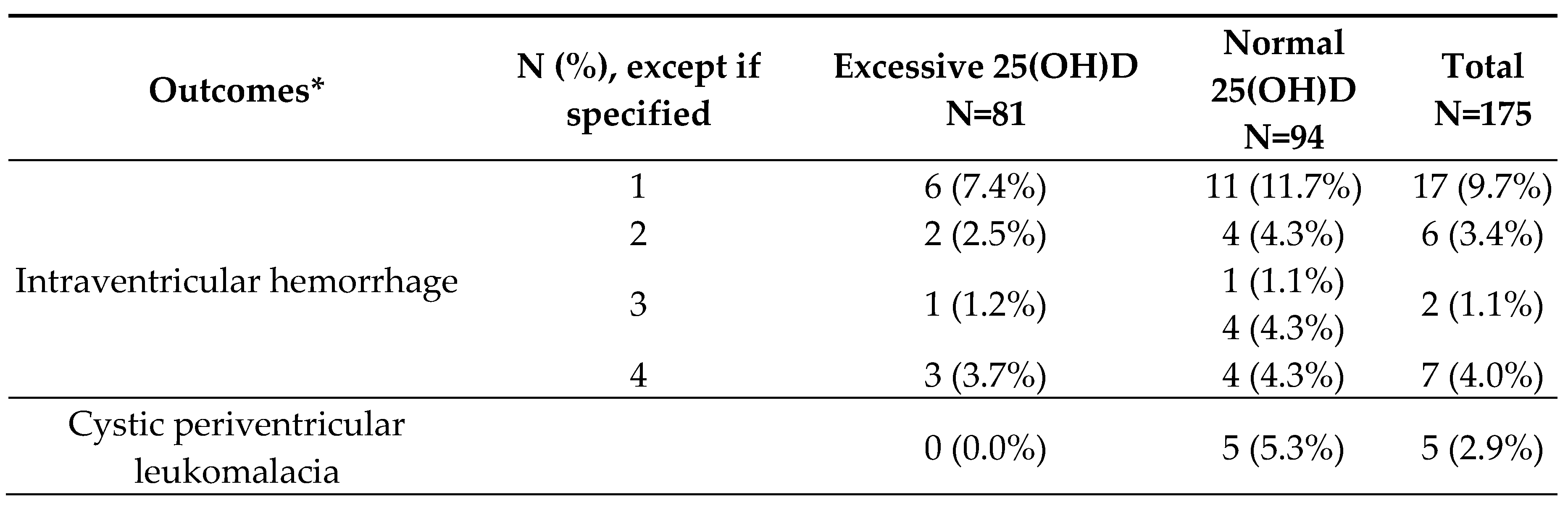
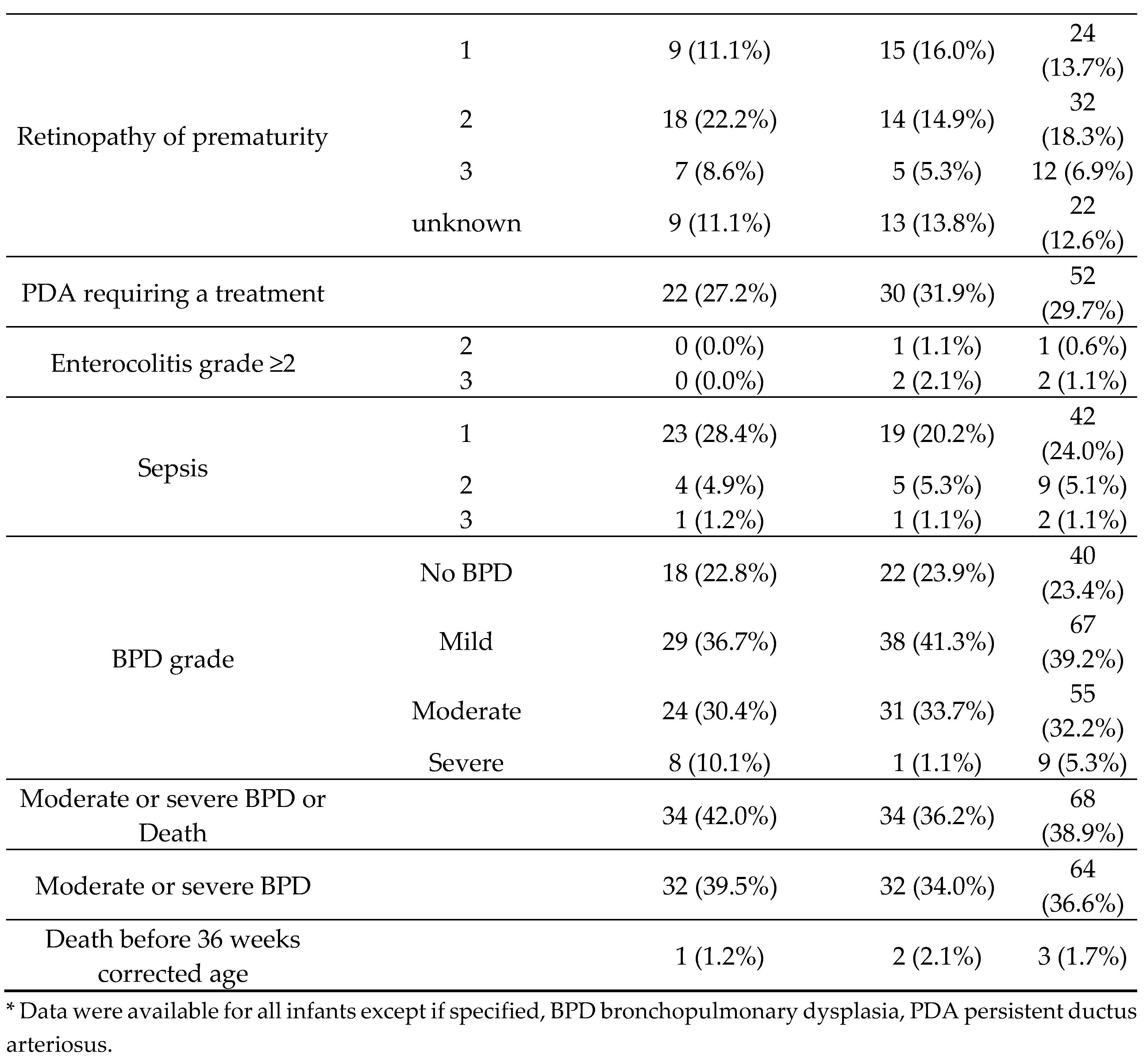
Table 4.
Multivariable analysis to evaluate the risk of bronchopulmonary dysplasia or death taking into account the classically described factors and the occurrence of a 25(OH)D >120nmol/L.
Table 4.
Multivariable analysis to evaluate the risk of bronchopulmonary dysplasia or death taking into account the classically described factors and the occurrence of a 25(OH)D >120nmol/L.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



