
Submitted:
19 September 2023
Posted:
20 September 2023
You are already at the latest version
Abstract
Nurses focus more on curative aspects rather than health promotion and disease prevention, thus weakening primary health care and lessening engagement with the community. Providing a learning environment that can support the professional growth of nurses through engagement with local communities and educational institutions would strengthen primary health care in the community; however, this poses challenges due to the traditional mindset of nurses towards primary health care. This integrative review aimed to explore key features of the potential of the nursing center model as a contracting-out approach to strengthen primary health care services. This integrative review provides lessons for implementing the Nursing Centre model for any country, mainly where nurses are not fully utilized for health promotion and disease prevention.
Keywords:
Contracting-out
; Nursing Center
; Health Promotion
; Disease Prevention
1. Introduction
Schools of nursing establish academic Nursing Centres (NCs) to address the gap between education and practice in nursing [1] in order to achieve their missions including education, research, and clinical practice [2]. Therefore, the NC has a three-fold mission namely the education of nurses, being a practice site for lecturers and other members of faculty and providing nursing services to the community [2]; as well as research that advances healthcare [3]. Schools in either a medical centre setting or a research-intensive/extensive setting were more likely to have developed NCs [2].
Despite the similarity in the purpose of the NCs establishment, the characteristics and emphasis of the operation of these centres is somewhat varied [4]. The variety of characteristics and approaches used in NCs may be influenced by the differing organisational characteristics of the particular School of Nursing (SON) operating these centres. Pohl, Sebastian [2] surveyed the characteristics of the SONs operating NCs in the USA. They found that 92 out of 565 SONs indicated that they had one or more NCs. Of the 92 SONs, 59 responded to the survey. The findings showed that the overall proportion of SONs operating NCs was very low (16%). The survey results also outlined the characteristics of the NCs. As well, many NCs serve as educational and clinical sites for nursing students at the baccalaureate, masters, and doctoral levels. The number of nursing academics practicing in these centres ranged from one to ten academics. In terms of funding, most of the centres identified that grants and SONs are the most common sources of funding for the NCs ([2]. In terms of location, the most common was space in another agency (38.8%), followed by location in a free-standing building (21.4%), while only 12% were located within SONs. In terms of the number of years the NCs have been open ranged from two to 35 years, with an average of nine years whereas only four centres had been open for more than 20 years.
The literature reports on the wide variety of models or approaches to the NC, starting with community-based services [5], the Lundeen community nursing centre [6], the Betty Neuman model [7], primary health care [8] and the evidence-based model [9], community as client [10], through to the business plan model [11, 12]. These models show that the NC has potential to contribute and strengthen the primary health care service in the community through contracting out. Contracting out entails the public sector acting as the buyer while a private supplier provides a public service. The term "privatization," frequently used when a private actor gains complete control over the service in question and public assets are sold, does not apply to this situation [13]. Collaboration is a powerful tool to integrate primary healthcare into the academic system in order to improve the quality of education through knowledge-sharing and synergies between the health services and education institutions [14]. The major challenge for such integration is to provide a learning environment that can support professional growth [15] through engagement with local communities to promote health and disease prevention in the population [14]. However, this variable has not been fully articulated in the literature. Therefore, the question asked in this review is that “what are the potential of contracting out through the Nursing Center Model that can strengthen primary health care services and health promotion in the community?
2. Materials and Methods
The integrative review method of Whittemore and Knafl [16] was used for this review. Integrative reviews are part of the group of research review methods which include both quantitative and qualitative research in order to enhance the rigour of the evaluation of a phenomenon of interest [16, 17]. The literature search was conducted systematically using a number of databases, and the snowball technique [18]. The results are documented in Table 1 as a summary of the number of included retrieved articles. A total of 41 studies were included in the review. A flowchart of the search results is presented in Figure 1.
2.1. Conducting a quality appraisal of the retrieved literature
Studies were not appraised individually as it is anticipated that the findings of the review will come from a diverse range of literature. As a result, it is anticipated that quality will be highly variable. While this is a limitation of the review, given that the aim is to develop a description of the phenomena of interest rather that to evaluate a specific treatment, it was anticipated the findings would still provide important information regarding the academic NC model.
2.2. Data analysis
After the articles had been gathered, the synthesis process consisted of three phases [19]:
- Identification of the key findings by reading and re-reading the articles to develop a sense of the studies as a whole.
- The differences and commonalities in the lists of major findings across the studies were compared and contrasted.
- Data display matrices were developed to display all the coded data from each report by category and then were iteratively compared. These categories were used to develop a functional definition of service learning. The product of the synthesis was then written up in the form of a table and a model.
In addition to three analysis phases, a bibliometric analysis was conducted using VOS Viewer [20] to map concepts and visualise the correlation between some ideas used in the included papers.
3. Results
Of 41 papers, 33 are from the USA, three are from Australia, two are from Indonesia, and one from Taiwan. Most papers used descriptive design, and three papers used case study design. Regarding the integrated approach, 33 papers mentioned integration between nursing education, health services, and research within the nursing centre. In addition, 31 papers mentioned collaboration with community organisations or interinstitutional collaboration. These can be a potential for contracting out models for the nursing centres. Table 2 summarises Nursing Centre Models and their potential for contracting out.
Figure 2 shows that nurse-managed centers (NC) can enhance nursing education and provide a clinical learning environment for nursing students and faculty practice. Apart from nursing education, nurse-managed centers (NC) also have the potential to provide health promotion through community-institutional relations and interinstitutional relations.
4. Discussion
4.1. Strengthening health promotion and primary prevention
One of the earliest NCs in the US was established in 1979 at the University of Wisconsin-Milwaukee [5]. In this centre, Lundeen [5] used the following four elements: 1) community-based services located in the community using a small humanistic organisational structure to provide a sense of familiarity; 2) a comprehensive range of services that focus on the multiple risk factors that influence families; 3) collaborative relationships with various health disciplines, agencies, and multiple funders; and 4) coordination of services for families to reduce overlaps in service provision.
In addition to this model, Lundeen published a study on the application of the Lundeen Community Nursing Centre Model. This is a model that uses a collaborative and multidisciplinary approach with organisational partners in the public health and social service sectors and community residents in order to provide health promotion and primary prevention as key components of nursing roles. The Lundeen Community Nursing Centre Model is based on the principle of integration and collaboration between nursing, public health, social services, and community-based organisations. The services provided in these centres comprise assessment and screening, health education, counselling, community outreach, case management, community assessment and development, and clinic-based primary care [6]. This model emphasis on the collaboration and integration of multiple discipline, professional education, and research activities, however, there was no specific information of how this integration was conducted and measured.
In the subsequent publication of the NC Wisconsin, Hong and Lundeen [29] reported that the Automated Community Health Information System (ACHIS) was used to code client problems and nursing interventions based on the Omaha system [29]. They further found that the majority of nursing diagnoses in this centre were coded as actual problems, but 38% of client problems were documented as potential problems and health promotion issues. The actual nursing interventions provided in this centre were health teaching, guidance, and counselling (38.9%) and case management (25.8%). This study showed the contribution of the NC towards health promotion for vulnerable populations, and that ACHIS could be used as a clinical information system in the NC. However, there was no information in the paper in relation to evaluation of education and research within the NC. As well, there was no information regarding the numbers of the NC that used the Lundeen’s model and the sustainability of this NC up to now because the latest publication was in 2009.
A different model of the NC was reported by Oros, Johantgen [9] who looked at the Open Gates Health Centre in inner city Baltimore which was established by the University Of Maryland School Of Nursing in 1993. The mission of this centre is to provide quality healthcare to individuals and families who are uninsured, underinsured, or who are having difficulty accessing the traditional healthcare system. The centre was established by a non-profit organisation, Open Gates, Inc., with board representation from the community, a religious organisation, and the school of nursing. The Open Gates received an initial grant from the Middendorf Foundation and a special project grant from the Division of Nursing, U.S Department of Health and Human Services. This centre used the Evidence-Based Clinical Practice Model, which applied “system theory to define the set of relationships between community and student needs, the clinical practice program, and student and community outcomes” [9]. The Evidence-Based Clinical Practice model started with the understanding the needs of student and the community as the foundation for the development a clinical practice program that include primary healthcare, health education and promotion, and community outreach strategy. Clinical education of students and research were integral components of the entire care delivery approach [9]. Despite the authors’ claim of integration of primary healthcare, education, and research in the Open Gate Health Centre, there was no reported evaluation of this integration in the paper.
The Open Gate model was the prototype of nurse-managed community-based model which was used by other centres, such as five mobile treatment units, 15 school-based health centres, a nursing centre for frail seniors, a teen parent education and support centre, a large interdisciplinary paediatric ambulatory practice, and a state-wide consultation and training program for child care providers. The interventions in such centres consist of primary healthcare, health education and promotion programs, and community outreach provided by students and advanced-practice nursing academics [9]. The NCs demonstrated that they provide comprehensive quality healthcare in an efficient and effective way. However, this NC model faced challenges in relation to balancing conflicting community needs and accountability of public health practices. These are including practice management/clinical operations, community, and research challenges [9]. The major challenge in practice management is the staffing of the centre because this centre mainly runs by faculty members who also have other commitments to teach and conduct research. In term of community challenges, the priority of community needs often in conflict with academic interests which sometimes reduce the community trust towards a university. In terms of research, the main challenge is to integrate and balance the competing demands of practice, education and research in order to achieve mutual goals of community health and academic [9]
Another NC model is that described by Newman [7] using the Betty Neuman systems model which views the client as a system in interaction with environmental stressors that may have either positive or negative impacts on the client. This centre was established in 1997 in Chester, Pennsylvania to meet the health promotion needs of underserved senior citizens. This centre was funded by the Independence Foundation of Philadelphia as the result of collaboration between the Health Advisory Committee of Chester, Neumann College Division of Nursing and Health Sciences, and Widener University School of Nursing. The centre was located in two different sites to accommodate students and faculty practice from these two nursing education institutions. The goal of the centre was to “establish a nurse-managed centre to provide health promotion activities, research, and placement of nursing students to focus on the health of elderly men and women”[7]. Nursing interventions in such NCs were characterised by prevention strategies in order to change the interaction between the client and the environmental stressor. The author reported that a total of 400 clients were seen in the NC between 1997 and 2001.
Miller, Bleich [12] proposed the use of a business plan as a blueprint for the NC should be used to determine the feasibility of clinical services, faculty development requirements, and expected returns on investment of time and resources. This business plan would include the mission and goals of the centre, strategic and business planning processes, marketing, recruitment, and the development of incentives to reward professional employees. The dimensions of academic practice within the NC, including direct care where the nurse practitioners deliver primary care services to clients at a particular site, the opportunity to use nurse academics to develop a consulting practice in the clinical, administrative, and research areas, and a new educational development approach to institutions and individual patient consumers[12].
A similar approach was also reported by Branstetter and Holman [11] for a NC that was established in 1977 by academics from the Arizona State University College of Nursing. This centre used a model based on the primary care role of the nurse focusing on the provision of healthcare for people in the community. After 11 years of operation, this centre was threatened with closure due to financial constraints. In response, the centre employed six strategies to maintain viability. These strategies were to: initiate a policy of direct, full pay for services at the time of the visit; develop a realistic business management plan; aggressive use of planned marketing strategies; obtain contracts and agreements with other community agencies; cooperate with other agencies to address specific local health needs; and to solicit obtaining provider status with selected health maintenance organisations. In this way, the NC at Arizona State University has survived as a freestanding nursing clinic[11].
Persily [38] reported a different approach on academic practice within the West Virginia Rural Health Education Partnerships (WVRHEP) program to address the problem of critically limited levels of primary healthcare in rural and medically underserved areas in the US. This program has integrated academic nursing practice, student learning, and research. The results showed that women used the WVRHEP services for prenatal care as well also for the continuing care of their families. Nursing education was also integrated into the practice, as this centre also served as a laboratory to provide deeper understandings to nursing students of rural nursing practice. In terms of research, this centre has received research grants, and has also disseminated their research findings in the form of publications and presentations [38].
The positive impact of integrating education with research in the NC was also reported by Marek, Rantz [37] who described the establishment of Senior Care, a practice based in the University of Missouri-Sinclair School of Nursing (MUSSON), which has an emphasis on the combination of research, education, and practice. This program generated more than US$1.25 million of service revenue in 2003, with more than 300 students using Senior Care as a clinical or service-learning site, and has received more than US$3 million in research funding. The Senior Care program used the principles of Ageing in Place which promotes independence, dignity, and health [37].
Apart from the wide use of NCs model in the US, this model has also been adopted in other countries. Yeh, Rong [47] reported that a new academic-based, nurse-managed community centre program was established and implemented in Taiwan over more than two years. The findings demonstrated that teachers, students, and residents in the apartment complex perceived high levels of satisfaction with this model. The academic-based, nurse-managed community centre could be sustained using a systematic integrated educational partnership with stable resources sourced through industrial, government, academic, and private institutions [47].
A review of these studies has shown that various models and approaches have been used by NCs in some countries. Most of the papers in this review claimed that the NC is integrating health services, education, and research. However, most of these publications reported on the service aspect of the NC while there is little information regarding the specific educational approach as well as the evaluation of framework of the integration that are reported in these papers. NC teams need to document extensive data relating to best practice and outcomes of care, and to identify the important factors in establishing and maintaining a NC so that the SON can gain the benefit of the services, education, and research in the NC [2].
4.2. Collaborative Approach
The NC has been recognised as an innovative model that integrates nursing services, education, and research. As academic NCs evolve, ongoing clinical and health services research and development are necessary to identify the strengths and weaknesses of NCs, and to document their implications and disseminate these research findings in order to inform other nursing academics, healthcare providers, consumers, and policy-makers [6].
Collaboration and partnership between academics and the community are needed in order to maintain the sustainability of NCs [31]. Collaboration defined as the ways in which various resources, such as health professionals, are brought together, while integration is defined as the ways in which services are delivered and practices are organised and managed. Therefore collaboration and integration in the NC can be defined as the ways in which students, lecturers, nurses, and other health professionals are brought together in order to organise and manage health services, education, and research in an integrated way. Collaboration and partnership in initial planning of the NC is particularly important for those that have partnerships with the community or with other healthcare organisations in order to determine the compatibility of mission and mutual goals of the organisations [6].
Organisations that are involved in the NCs need to clarify the philosophy and goals of their collaboration with the NCs so that the vision and mission of each organisation can be aligned to the purpose of the NC, and they need to review these missions and goals on a regular basis [6]. As NCs offer holistic care and patient-centred health promotion and disease prevention [3], partnerships between academics and the community, or the healthcare organisation, serve to increase trust from people in the community towards NCs, and thus, increase the chances of integration of health promotion activities into the daily activities of members of the community. A study demonstrated that the Lundeen Community NC model supported nursing practice that was oriented toward the promotion of health as the key element that differentiated the NC from other health delivery models [6].
The strength of the NC is that it combines nursing expertise with other disciplines such as medicine, public health, mental health and social work, and community development [31], as the traditional primary medical service alone is insufficient to address the integrated and holistic care needs of people in the community [3].
Even though nursing education institutions do not have direct connections with healthcare service organisations, the World Health Organisation (WHO) acknowledges a need for inter-sectoral and close collaboration between health, social care, education, and other sectors in the community in order to achieve better health goals for individuals, families, and the community. Collaboration and partnerships in the NCs enables the fulfilment of a greater number of community needs, as long as each organisation allocates sufficient time to develop trust and to understand each other’s needs and goals [23].
In order to improve the integration of NCs, five strategies for a people-centred and integrated health services approach, developed by the World Health Organisation can be implemented by NCs. These strategies include “empowering and engaging people, strengthening governance and accountability, reorienting the model of care, coordinating services, creating an enabling environment”. In terms of empowering and engaging people, people as resources need to be empowered, engaged, and involved in the production of healthcare in equal and reciprocal relationships between health professionals and people who use the service. In addition to empowering people, health providers could strengthen governance and accountability by involving people in the community to develop a population-oriented health policy [49]. The NC can become a way of re-orienting the model of care in order to provide efficient and effective healthcare services through balancing the service needs of the clients and the academic needs of the nursing programs using the primary and community care services).
The WHO (2015) further emphasises the importance of shifting the medical model to a more holistic form of care which includes health promotion and illness prevention strategies. Strategies for coordinating services focus on ways of reducing the fragmentation of care delivery through improving continuity of care and relationships with people and different healthcare providers, and creating effective networks between health and other sectors [49]. Finally, the strategy of people-centred and integrated healthcare seeks to create an environment that enables stakeholders to become involved in the process of transformation towards people-centred and integrated health services [49]. Even though these strategies provide a general direction for an integrated healthcare approach at the national and international levels, they can also be applied to the NC through involving stakeholders in the process of integration.
5. Conclusions
This integrative review showed key features of the potential of the nursing center model as a contracting-out approach to strengthen primary health care services. This integrative review provides lessons for the implementation of the Nursing Centre model for any country, particularly where nurses are not fully utilized for health promotion and disease prevention.
Author Contributions
Conceptualization, NJ, ML, and ADP; methodology, NJ, ML, and ADP.; formal analysis, NJ, ML, and ADP; writing—original draft preparation, NJ; writing—review and editing, NJ, ML, and ADP. All authors have read and agreed to the published version of the manuscript.”.
Funding
This study was funded by Universitas Padjadjaran under the scheme Unpad Research Grants.
Data Availability Statement
The data are available upon request to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- King, ES. A 10-Year Review of Four Academic Nurse-Managed Centers: Challenges and Survival Strategies. Journal of Professional Nursing. 2008, 24, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Pohl JM, Sebastian JG, Barkauskas VH, Breer ML, Williams CA, Stanhope M, et al. Characteristics of schools of nursing operating academic nurse-managed centers. Nursing Outlook. 2007, 55, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Humphreys J, Martin H, Roberts B, Ferretti C. Strengthening an academic nursing center through partnership. Nursing Outlook. 2004, 52, 197–202. [Google Scholar] [CrossRef]
- Barger, SE. Academic nursing centers: the road from the past, the bridge to the future. Journal of Nursing Education. 2004, 43, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Lundeen, SP. Comprehensive, collaborative, coordinated, community-based care: A community nursing center model. Family & Community Health. 1993, 16, 57–65. [Google Scholar]
- Lundeen, SP. An Alternative Paradigm for Promoting Health in Communities: The Lundeen Community Nursing Center Model. Family & Community Health. 1999, 21, 15–28. [Google Scholar]
- Newman DML. A community nursing center for the health promotion of senior citizens: based on the Neuman Systems Model. Nursing Education Perspectives. 2005, 26, 221–223. [Google Scholar]
- Neff DF, Mahama N, Mohar DR, Kinion E. Nursing care delivered at academic community-based nurse-managed center. Outcomes Management. 2003, 7, 84–89. [Google Scholar] [PubMed]
- Oros M, Johantgen M, Antol S, Heller BR, Ravella P. Community-based nursing centers: a model for health care delivery in the 21st century. Community-based nursing centers: challenges and opportunities in implementation and sustainability. Policy, Politics & Nursing Practice. 2001, 2, 277–287. [Google Scholar]
- Glick, DF. Advanced practice community health nursing in community nursing centers: A holistic approach to the community as client. Holistic Nursing Practice. 1999, 13, 19–27. [Google Scholar] [CrossRef]
- Branstetter E, Holman EJ. An academic nursing clinic's financial survival. Nursing Economics. 1997, 15, 248–252. [Google Scholar]
- Miller KL, Bleich MR, Hathaway D, Warren C. Developing the academic nursing practice in the midst of new realities in higher education. Journal of Nursing Education. 2004, 43, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Bhatti Y, Olsen AL, Pedersen LHJG. The effects of administrative professionals on contracting out. 2009, 22, 121–137.
- Frenk J, Chen L, Bhutta ZA, Cohen J, Crisp N, Evans T, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. The lancet. 2010, 376, 1923–1958. [Google Scholar] [CrossRef]
- Frenk, J. Reinventing primary health care: the need for systems integration. The Lancet. 2009, 374, 170–173. [Google Scholar] [CrossRef]
- Whittemore R, Knafl K. The integrative review: Updated methodology. Journal of Advanced Nursing. 2005, 52, 546–553. [Google Scholar] [CrossRef]
- Evans, D. Overview of Methods. In: Webb C, Roe B, editors. Reviewing Research Evidence for Nursing Practice: Systematic Reviews. Oxford, UK: Blackwell Publishing Ltd; 2007. p. 135-48.
- Kable AK, Pich J, Maslin-Prothero SE. A structured approach to documenting a search strategy for publication: A 12 step guideline for authors. Nurse Education Today. 2012, 32, 878–886. [Google Scholar] [CrossRef] [PubMed]
- Evans, D. Systematic reviews of interpretive research: Interpretive data synthesis of processed data. Australian Journal of Advanced Nursing. 2002, 20, 22–26. [Google Scholar] [PubMed]
- van Eck NJ, Waltman L. VOSViewer: Visualizing Scientific Landscapes [Software]. 2010.
- Acord LG, Dennik-Champion G, Lundeen SP, Schuler SG. Vision, Grit, and Collaboration: How the Wisconsin Center for Nursing Achieved Both Sustainable Funding and Established Itself as a State Health Care Workforce Leader. Policy, Politics, & Nursing Practice. 2010, 11, 126–131. [Google Scholar] [CrossRef]
- Andresen PA, McDermott MA. Client satisfaction with student care in a nurse-managed center. Nurse Educator. 1992, 17, 21–23. [Google Scholar] [CrossRef]
- Aponte J, Egues AL. A school of nursing-wellness center partnership: creating collaborative practice experiences for undergraduate US senior nursing students. Holistic Nursing Practice. 2010, 24, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Barkauskas VH, Schafer P, Sebastian JG, Pohl JM, Benkert R, Nagelkerk J, et al. Clients Served and Services Provided by Academic Nurse-Managed Centers. Journal of Professional Nursing. 2006, 22, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Connolly PM, Mao C, Yoder M, Canham D. Evaluation of the Omaha System in an academic nurse managed center. Online Journal of Nursing Informatics. 2006, 10, 14. [Google Scholar] [PubMed]
- Connolly, PM. Services for the underserved: a nurse-managed center for the chronically mentally ill. Journal of Psychosocial Nursing & Mental Health Services. 1991, 29, 15. [Google Scholar] [PubMed]
- Henry, JK. Community nursing centers: Models of nurse managed care. Journal of Obstetric, Gynecologic & Neonatal Nursing. 1997, 26, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Hildebrandt E, Baisch MJ, Lundeen SP, Bell-Calvin J, Kelber S. Eleven years of primary health care delivery in an academic nursing center. Journal of Professional Nursing. 2003, 19, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Hong W-HS, Lundeen SP. Using ACHIS to Analyze Nursing Health Promotion Interventions for Vulnerable Populations in a Community Nursing Center: A Pilot Study. Asian Nursing Research. 2009, 3, 130–138. [Google Scholar] [CrossRef]
- Kent F, Keating J. Patient outcomes from a student-led interprofessional clinic in primary care. Journal of interprofessional care. 2013, 27, 336–338. [Google Scholar] [CrossRef]
- Krothe JP, Flynn B, Ray D, Goodwin S. Community development through faculty practice in a rural nurse-managed clinic. Public Health Nursing. 2000, 17, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Lough, MA. An academic-community partnership: a model of service and education. Journal of Community Health Nursing. 1999, 16, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Lundeen, SP. Leadership strategies for organizational change: Applications in community nursing centers. Nursing administration quarterly. 1992, 17, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Lundeen, SP. Community Nursing Centers-Issues for Managed Care. Nursing management. 1997, 28, 35–37. [Google Scholar] [CrossRef]
- Lundeen SP, Harper E, Kerfoot K. Translating nursing knowledge into practice: An uncommon partnership. Nursing Outlook. 2009, 57, 173–175. [Google Scholar] [CrossRef] [PubMed]
- Lutz J, Herrick CA, Lehman BB. Community partnership: a school of nursing creates nursing centers for older adults. Nursing & Health Care Perspectives. 2001, 22, 26–29. [Google Scholar] [PubMed]
- Marek KD, Rantz MJ, Porter RT. Academic practice exemplars. Senior care: making a difference in long-term care of older adults. Journal of Nursing Education. 2004, 43, 81–83. [Google Scholar] [PubMed]
- Persily, CA. Academic practice exemplars. Academic nursing practice in rural West Virginia. Journal of Nursing Education. 2004, 43, 75–77. [Google Scholar] [CrossRef] [PubMed]
- Pohl JM, Breer ML, Tanner C, Barkauskas VH, Bleich M, Bomar P, et al. National consensus on data elements for nurse managed health centers. Nursing Outlook. 2006, 54, 81–84. [Google Scholar] [CrossRef]
- Pohl JM, Tanner C, Barkauskas VH, Gans DN, Nagelkerk J, Fiandt K. Toward a national nurse-managed health center data set: Findings and lessons learned over 3 years. Nursing Outlook. 2010, 58, 97–103. [Google Scholar] [CrossRef]
- Resick LK, Leonardo M, McGinnis K, Stewart J, Goss C, Ellison T. A Retrospective Data Analysis of Two Academic Nurse-Managed Wellness Center Sites. Journal of Gerontological Nursing. 2011, 37, 42–52. [Google Scholar] [CrossRef]
- Shiber S, D'Lugoff M. A win-win model for an academic nursing center: Community partnership faculty practice. Public Health Nursing. 2002, 19, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Stewart A, Coulon L, Kavanagh K. The role of a nurse-managed health-care centre in health promotion: A feasibility study. Health Promotion Journal of Australia. 1997, 7, 189–195. [Google Scholar]
- Thompson C, Feeney E. Student-client relationships in a community health nursing clinical setting. Nursing Education Perspectives. 2004, 25, 137–138. [Google Scholar] [PubMed]
- Tuaoi L-A, Cashin A, Hutchinson M, Graham I. Nurse practitioners in academic nurse managed centres: A new and emergent opportunity for Australian nurses. Australasian Emergency Nursing Journal. 2011, 14, 40–44. [Google Scholar] [CrossRef]
- Van Zandt SE, Sloand E, Wilkins A. Caring for vulnerable populations: role of academic nurse-managed health centers in educating nurse practitioners. Journal for Nurse Practitioners. 2008, 4, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Yeh M, Rong J, Chen M, Chang S, Chung U. Development of a new prototype for an educational partnership in nursing. Journal of Nursing Education. 2009, 48, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Zachariah R, Lundeen SP. Research and Practice in an Academic Community Nursing Center. Image: the Journal of Nursing Scholarship. 1997, 29, 255–260. [Google Scholar] [CrossRef]
- World Health Organization. WHO global strategy on people-centred and integrated health services: interim report. World Health Organization, 2015.
Figure 1.
Flow chart of search results.
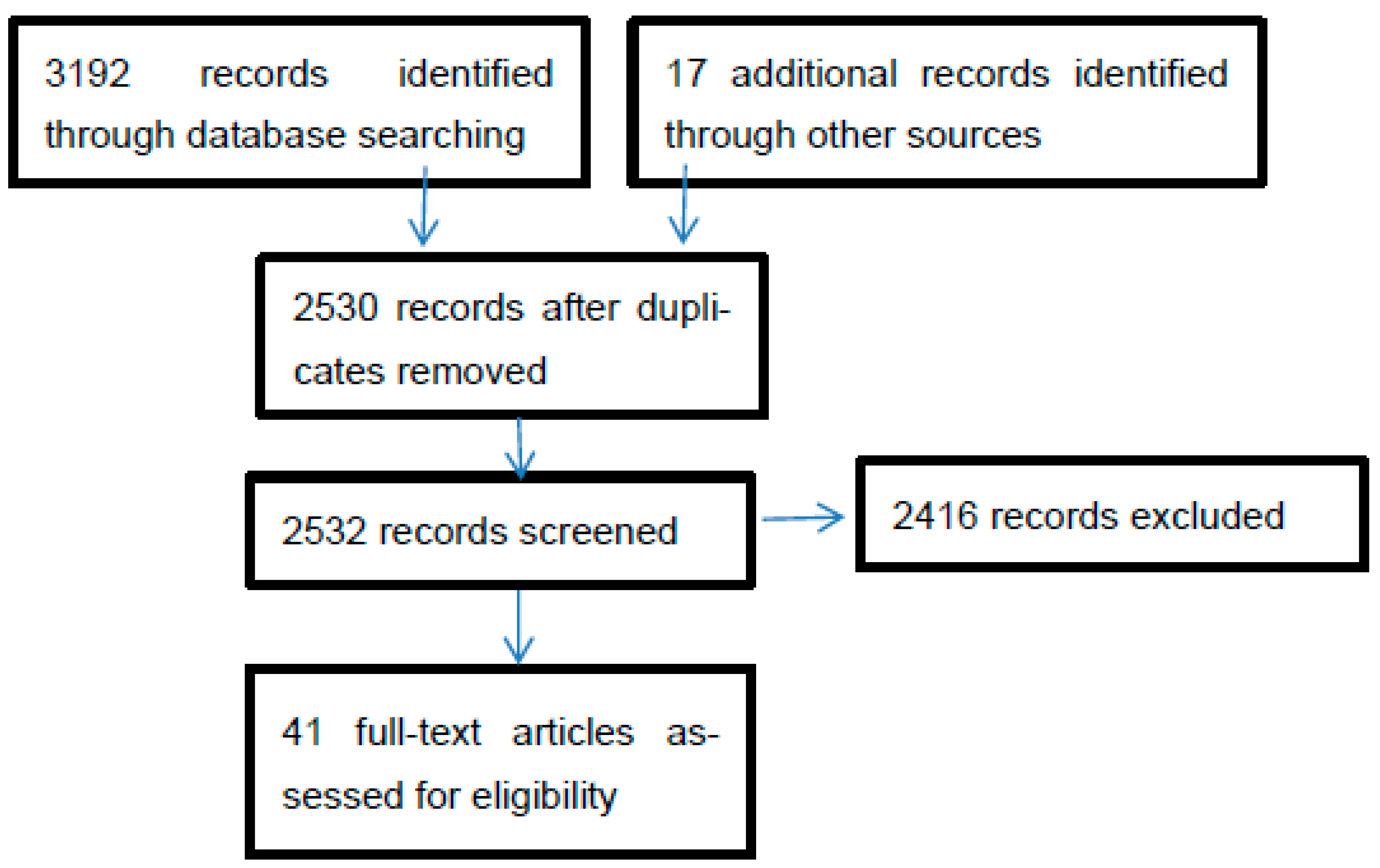
Figure 2.
Bibliometric Analysis of the Nursing Centre.
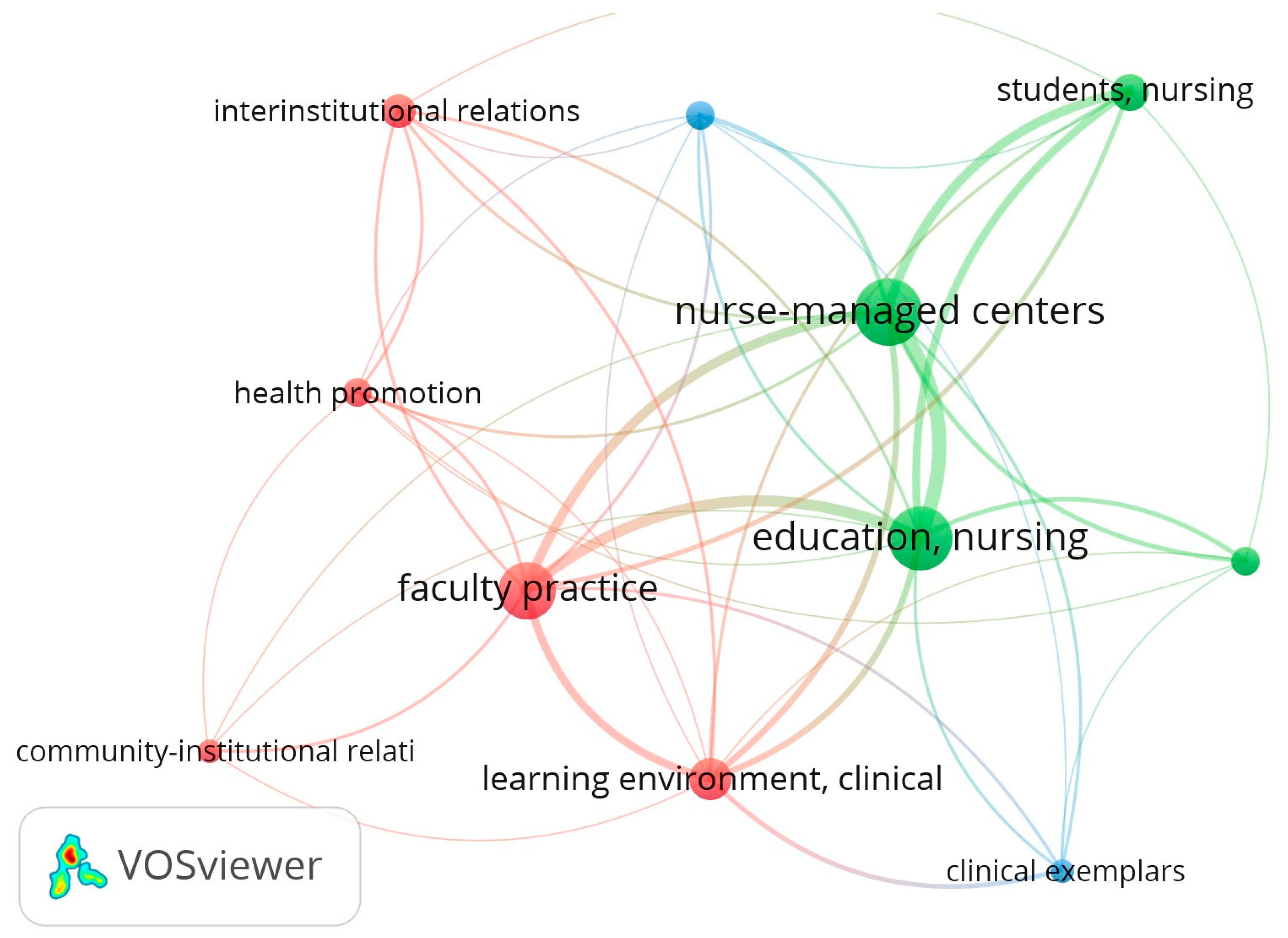

Table 1.
Summary of number of included retrieved articles.
| Literature Search | # Retrieved papers | # Met inclusion criteria |
|---|---|---|
| CINAHL | 2454 | 21 |
| MEDLINE | 723 | 8 |
| Snowball technique | 17 | 12 |
| Total | 3192 | 41 |
Table 2.
Summary of Nursing Centre Models (n=41).
| No | Study (n=39) | Research design | Country | Model | Integration | Contracting Out |
|---|---|---|---|---|---|---|
| 1. | Acord, Dennik-Champion [21] | Not mentioned | USA | The Wisonsin centre for nursing | V | - |
| 2. | Andresen and McDermott [22] | Descriptive | USA | - | V | V |
| 3. | Aponte and Egues [23] | Survey | USA | Wellness centre and SoN partnership | V | V |
| 4. | Barger [4] | Not mentioned | USA | Four era of academic NC | V | - |
| 5. | Barkauskas, Schafer [24] | Cross-sectional survey | USA | Academic nurse-managed centre | - | V |
| 6. | Branstetter and Holman [11] | Not mentioned | USA | Business oriented NC | V | V |
| 7. | Connolly, Mao [25] | Practice exemplars | USA | Academic-nurse managed centre | V | V |
| 8. | Connolly [26] | Pilot project | USA | A nurse managed centre for the chronically mentally ill | V | V |
| 9. | Glick [10] | Discussion paper | USA | Community as client | V | V |
| 10. | Henry [27] | Descriptive | USA | Community nursing centre and service learning | V | V |
| 11. | Hildebrandt, Baisch [28] | Retrospective review | USA | Academic community NC | V | V |
| 12. | Hong and Lundeen [29] | Descriptive | USA | The Lundeen’s comprehensive community-based primary healthcare model | V | V |
| 13. | Humphreys, Martin [3] | Not mentioned | USA | Nurse-managed academic health centre for children and adolescents | V | V |
| 14. | Juniarti et al. 2015 | Case study | Indonesia | Community NC | V | - |
| 15. | Juniarti et al. 2019 | Case study | Indonesia | Community NC | V | - |
| 16. | Kent and Keating [30] | Descriptive | Australia | Student-led inter-professional clinic | V | - |
| 17. | King [1] | 10 years review of 10 academic NCs | USA | Business model | V | V |
| 18. | Krothe, Flynn [31] | Descriptive | USA | Community development model | V | V |
| 19 | Lough [32] | Descriptive | USA | Academic-community partnership | V | V |
| 20. | Lundeen [33] | Not mentioned | USA | Community NC | - | - |
| 21. | Lundeen [5] | Not mentioned | USA | Community NC | V | - |
| 22. | Lundeen [34] | Not mentioned | USA | Community NC | - | V |
| 23. | Lundeen, Harper [35] | Not mentioned | USA | Lundeen Community NC | V | V |
| 24. | Lutz, Herrick [36] | Not mentioned | USA | NC for older adults and service learning | V | V |
| 25. | Marek, Rantz [37] | Descriptive | USA | - | V | V |
| 26. | Miller, Bleich [12] | Not mentioned | USA | Business plan | V | V |
| 27. | Neff, Mahama [8] | Retrospective descriptive | USA | Academic community based nurse-managed centre | - | V |
| 28. | Newman [7] | Descriptive | USA | Neuman Systems model | V | - |
| 29. | Oros, Johantgen [9] | Not mentioned | USA | Community-based NC | V | V |
| 30. | Persily [38] | Practice exemplars | USA | Academic nursing practice | V | V |
| 31. | Pohl, Breer [39] | Survey | USA | Nurse-managed health centres | V | V |
| 32. | Pohl, Sebastian [2] | Survey | USA | - | V | V |
| 33. | Pohl, Tanner [40] | Survey | USA | Primary care nurse-managed centre | - | V |
| 34. | Resick, Leonardo [41] | Retrospective | USA | Nurse-managed wellness centre | - | V |
| 35. | Shiber and D'Lugoff [42] | Descriptive | USA | Academic-community partnership | V | V |
| 36. | Stewart, Coulon [43] | Feasibility study | Australia | Nurse-managed healthcare centre | - | - |
| 37. | Thompson and Feeney [44] | Not mentioned | USA | Academic nursing centre/CHN clinical setting | V | V |
| 38. | Tuaoi, Cashin [45] | Discussion paper | Australia | - | V | - |
| 39. | Van Zandt, Sloand [46] | Case study | USA | Academic nurse managed centre | V | V |
| 40 | Yeh, Rong [47] | Action research | Taiwan | NC and service learning | V | V |
| 41 | Zachariah and Lundeen [48] | Descriptive | USA | Community NC | V | V |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



